IMPLEMENTATION OF WORKPLACE HIV/AIDS POLICIES IN PRIVATE INSTITUTIONS IN UGANDA CASE STUDY OF REPRODUCTIVE HEALTH UGANDA AND UGANDA TELECOM LIMITED A DISSERTATION SUBMITTED TO UGANDA MARTYRS UNIVERSITY, NKOZI IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF THE DEGREE OF MASTER OF ARTS IN DEVELOPMENT STUDIES. OLOYA PAUL MAY, 2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
IMPLEMENTATION OF WORKPLACE HIV/AIDS POLICIES IN PRIVATE
INSTITUTIONS IN UGANDA
CASE STUDY OF REPRODUCTIVE HEALTH UGANDA AND UGANDA
TELECOM LIMITED
A DISSERTATION SUBMITTED TO UGANDA MARTYRS UNIVERSITY, NKOZI
IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF
THE DEGREE OF MASTER OF ARTS IN DEVELOPMENT STUDIES.
OLOYA PAUL
MAY, 2013

i
Declaration
I Oloya Paul hereby declare that this dissertation is my own work and that all sources that
have been referred to and quoted have been indicated and acknowledged with complete
references. This work has not been submitted to any other institution for the award of any
academic qualification.
Signed ……………………………. Date……………………………….
Oloya Paul
Signed………………………………Date………………………….
(Supervisor)

ii
Approval
This is to certify that this report has been prepared under my supervision and now is ready for
submission with my approval as a university supervisor for a requirement for the award of a
Master of Arts in Development Studies of Uganda Martyrs University, Nkozi.
Signature:......................................................... Date:..................................................

iii
Dedication
I dedicate this work to my family and friends and my colleagues at work who contributed
immensely through their moral and financial support to make my course manageable.

iv
Acknowledgements
I wish to extend my sincere appreciation and gratitude to the people who supported me and
provided the necessary encouragement to see the research to the end. I would also like to
thank the staff of Reproductive Health Uganda and Uganda Telecom, who so willingly
participated in the study, and provided the necessary data, without which the study would not
have been possible.
I would like to thank, my family and friends who encouraged and believed in me. To my
supervisor, Mr. Mubangizi Denis for guidance and his willingness to share his experience and
knowledge – Thank you very much and God bless you.
Lastly to my creator, for bestowing unto me the necessary courage, good health and mental
ability to complete the study.

v
Table of Contents
Declaration ............................................................................................................................................. i
Approval .................................................................................................................................... ii
Dedication ............................................................................................................................................ iii
Acknowledgements ............................................................................................................................. iv
Table of Contents ................................................................................................................................. v
List of Figures ...................................................................................................................................... ix
List of Tables ........................................................................................................................................ x
CHAPTER ONE: GENERAL INRODUCTION ........................................................................ 1
1.0 Introduction ..................................................................................................................................... 1
1.1 Background to the study ............................................................................................................... 1
1.2 Statement of the problem .............................................................................................................. 3
1.3 Purpose of the study ...................................................................................................................... 3
1.4 Objectives........................................................................................................................................ 3
1.5 Specific objectives ......................................................................................................................... 4
1.6 Research Questions ........................................................................................................................ 4
1.7 Significance of the study ............................................................................................................... 4
1.8 Scope of the study .......................................................................................................................... 5
1.9 Conceptual Framework ................................................................................................................. 5
CHAPTER TWO: LITERATURE REVIEW ............................................................................. 7
2.0 Introduction ..................................................................................................................................... 7
2.1 Global Situation of the HIV/AIDS Pandemic ............................................................................ 7

vi
2.2 Situation of HIV/AIDS in Sub-Saharan Africa .......................................................................... 9
2.3 HIV/AIDS Situation in Uganda ................................................................................................. 11
2.3.1 Factors Fuelling HIV Transmission in Uganda .................................................................... 13
2.4 Effects of HIV/AIDS in the workplace ..................................................................................... 16
2.5 Efforts by International Organizations and Employers in Combating HIV/AIDS in the
Workplace ........................................................................................................................................... 21
2.6 Salient Issues addressed by Workplace HIV/AIDS Policies ................................................. 23
2.7 Challenges facing implementation of workplace HIV/AIDS Policies.................................. 25
CHAPTER THREE: RESEARCH METHODOLOGY ......................................................... 27
3.0 Introduction ................................................................................................................................... 27
3.1 Research Design ........................................................................................................................... 27
3.2 Study area ...................................................................................................................................... 27
3.3 Population of the study ................................................................................................................ 27
3.4 Sample size ................................................................................................................................... 27
3.5 Sampling Techniques .................................................................................................................. 28
3.6 Data collection techniques and instruments ............................................................................. 29
3.7 Research Procedure ..................................................................................................................... 29
3.8 Quality control .............................................................................................................................. 30
3.9 Data analysis ................................................................................................................................. 30
3.9.1 Statistical Data Analysis using Statistical Packages for Social Scientists (SPSS)........... 30
CHAPTER FOUR: DATA PRESENTATION, ANALYSIS AND INTERPRETATION ............ 31
4.0 Introduction ................................................................................................................................... 31

vii
4.1 The Biographical Characteristics of the Respondents ............................................................ 31
4.1.1 Age bracket of respondents ..................................................................................................... 31
4.1.2 Sex of respondents .................................................................................................................... 32
4.1.3 Education level of respondents ............................................................................................... 33
4.1.4 Length of employment of respondents .................................................................................. 33
4.1.5 Job position of respondents ..................................................................................................... 34
4.2 Level of exposure of the employees to the HIV/AIDS workplace policy ............................ 34
4.2.1 Familiarity with the work place HIV/AIDS policy .............................................................. 35
4.2.2 Familiarity of HIV/AIDS Policy by Sex ............................................................................... 36
4.2.3 Familiarity of HIV/AIDS Policy by age ................................................................................ 37
4.3 The functionality of the workplace HIV/AIDS policies ......................................................... 37
4.3.1 Recognition of HIV/AIDS policy as a workplace issue ...................................................... 38
4.3.2 HIV/AIDs policy and the principle of non discrimination .................................................. 39
4.3.3 HIV/AIDS policy and the issue of a healthy work environment ........................................ 40
4.3.4 HIV/AIDS policy and encouragement of social dialogue on HIV/AIDS issues .............. 41
4.3.5 HIV/AIDS policy and strengthening confidentiality ........................................................... 42
4.3.6 HIV/AIDS policy and supporting prevention initiatives on HIV/AIDS ........................... 43
4.3.7 HIV/AIDS policy and staff care and support with regard to HIV/AIDS .......................... 44
4.3.8 HIV/AIDS policy and continuation of employment relationship ...................................... 45
4.4 Challenges faced in implementation of HIV/AIDS policy ..................................................... 46
CHAPTER FIVE: SUMMARY, CONCLUSION AND RECOMMENDATIONS ......... 48
5.0 Introduction ................................................................................................................................... 48

viii
5.1 Summary ....................................................................................................................................... 48
5.1.1 Level of exposure of the employees to the HIV/AIDS workplace policy ........................ 48
5.1.2 The functionality of the workplace HIV/AIDS policies ...................................................... 49
5.1.3 Challenges faced in implementation of HIV/AIDS policy ................................................. 50
5.2 Conclusion .................................................................................................................................... 50
5.3 Recommendations ........................................................................................................................ 51
References ........................................................................................................................................... 51
Appendix : Questionnaire.................................................................................................................. 58

ix
List of Figures
Figure 4.1: Age of respondents ................................................................................................ 31
Figure 4.2: Respondents‟ sex ................................................................................................... 32
Figure 4.3: Respondents‟ Education level ............................................................................... 33
Figure 4.4: Respondents‟ length of employment ..................................................................... 33
Figure 4.5: Job Position of respondents ................................................................................... 34

x
List of Tables
Table 4.1:Familiarity to HIV/AIDS policy..............................................................................35
Table 4.2 Sex and Familiarity to HIV/AIDS programme Cross tabulation ............................. 36
Table 4.3: Age Bracket and Familiarity to HIV/AIDS policy Cross tabulation ...................... 37
Table 4.4: Perceptions of respondents on Recognition of HIV/AIDS policy as a workplace
issue.......................................................................................................................................... 38
Table 4.5: Responses on organization‟s HIV/AIDS policy and the principle of non
discrimination .......................................................................................................................... 39
Table 4.6: Responses on HIV/AIDS policy and the issue of a healthy work environment ..... 40
Table 4.7: Responses on HIV/AIDS policy and encouragement of social dialogue on
HIV/AIDS ................................................................................................................................ 41
Table 4.8: Responses on HIV/AIDS policy and strengthening confidentiality ....................... 42
Table 4.9: Responses on HIV/AIDS policy and supporting prevention initiatives on
HIV/AIDS ................................................................................................................................ 43
Table 4.10: Responses on HIV/AIDS policy and staff care and support................................. 44
Table 4.11: Responses on HIV/AIDS policy and continuation of employment relationship .. 45
Table 4.12: Pair wise matrix ranking of challenges faced in implementation of HIV/AIDS
policy........................................................................................................................................ 46

1
CHAPTER ONE
GENERAL INRODUCTION
1.0 Introduction
The grapple of this research is set to analyze the Implementation of workplace HIV/AIDS
policies in private institutions in Uganda using Reproductive Health Uganda and Uganda
Telecom Limited as case studies. This chapter sets the base for the study. It contains the
background to the research, statement of the problem, purpose of the study, objectives of the
study, research questions which guided the study, the scope and the significance of the study.
It also gives the definitions of the key concepts used in this study, as well as the conceptual
framework.
1.1 Background to the study
HIV/AIDS is a major workplace issue often regarded as similar to other serious illnesses, but
due to its means of transmission it has created great social stigma. More than 42 million
people around the world are infected with HIV, including some 26 million workers aged
between 15 and 49 years who are in the prime of their productive lives. Sub-Saharan Africa
remains the region most heavily affected by HIV (Garcia – Calleja, Gouws, Ghys, 2006). In
2008, sub-Saharan Africa accounted for 67% of HIV infections worldwide, 68% of new HIV
infections among adults and 91% of total new HIV infections (UNAIDS 2008). While the
rate of new HIV infections in Sub-Saharan Africa has slowly declined – with the number of
new infections in 2008 approximately 25% lower than at the epidemic‟s peak in the region in
1995 – the number of people living with HIV in sub-Saharan Africa slightly increased in
2008, in part due to increased longevity stemming from improved access to HIV treatment
(UNDP, 2009). Adult HIV prevalence declined from 5.8% in 2001 to 5.2% in 2008. While,
an estimated 1.4 million AIDS – related deaths occurred in Sub-Saharan Africa, representing
and 18% decline in annual HIV-related mortality in the region since 2004 (UNDP, 2008;
Whiteside et al, 2006).
In Uganda, employers are facing a major threat from HIV/AIDS and that is eroding the
development of the economy; consequently, a number of organizations have developed
workplace HIV/AIDS policies, partnered to fight HIV/AIDS and supported their employees
who are infected with HIV (Asingwire & Birungi, 2006). The dramatic and widespread effect

2
of HIV/AIDS on communities across the country is having a major impact on employers in
Uganda where 70% of reported cases fall in the 15 and 49 year age group (Collins and Rau,
2000; Uganda HIV/AIDS Manual for Work Places, 2004).
According to the Uganda HIV/AIDS Manual for work places (2004), workplace HIV/AIDS
policies and programs that are in place such as the „Stop AIDS Now‟ Project: Managing HIV
and AIDS in the workplace in Uganda, (2008); Kasese Town Council‟s Workplace
HIV/AIDS Policy; and Agro Eco/EPOPA Uganda HIV/AIDS Workplace Policy (2006) have
attempted to deal with how to protect employees and their families from infection; the kind of
assistance to give employees suffering from HIV/AIDS, as well as the communities in which
they live. The manual states that private sector institutions are particularly well placed to deal
with HIV/AIDS because they have structures that can take quick and effective action; they
know their employees and are in close contact with their families; they have systems for
handling personnel matters including health issues; and are part of wider networks which
work closely (The Uganda HIV/AIDS Manual for Work places, 2004).
Uganda Telecom Limited (UTL) is the most experienced telecommunications organization in
Uganda. It was previously a government parastatal and the only telecommunications provider
until the liberalization policy took effect and saw in new market entrants that led to its
privatization in June 2000. At Uganda Telecom, although HIV/AIDS testing and screening of
employees for purposes of access to employment is not compulsory, employees are
encouraged to take the test privately and know their status; and the company is ready to assist
in cases of positive results. Confidentiality of HIV/AIDS information is upheld and within its
financial capability, UTL provides medication, including ARVs to staff and eligible family
members infected with HIV/AIDS; awareness and counselling sessions are also held for staff.
Reproductive Health Uganda (RHU) is a national, voluntary, non-discriminatory and not-for-
profit, Non-Governmental Organization promoting and providing Sexual and Reproductive
Health and Rights. Formerly known as Family Planning Association of Uganda, RHU is the
pioneer of family planning services in Uganda and has remained the lead NGO in the
provision of family planning services. At Reproductive Health Uganda, disclosure of HIV
status is voluntary. The principle of equal opportunity is adhered to in hiring and promoting
staff, without discriminating on the grounds of race, tribe, colour, creed, gender, sexual

3
orientation, physical handicap, HIV status or age, provided the prospective employee can
fulfil the requirements of the job (The RHU Policy Handbook, 2009).
The effects of HIV/AIDS are felt by employees, their families, their employers and ultimately
national economies. The population most affected are the youths and people within the
productive age bracket most of who constitute a nation‟s workforce. Having a written policy
in itself is not sufficient unless it is operationalized. Response to the HIV/AIDS pandemic
within the workplace is crucial if progress is to be made in the prevention, impact mitigation
and provision of care and support for People Living with HIV/AIDS (PLWHA) and People
affected by HIV/AIDS. However, such responses are not without obstacles, that is why this
study sought to unearth the challenges faced in implementing HIV/AIDS Workplace policies.
1.2 Statement of the problem
Despite the existence in many workplaces of the HIV/AIDS policy and formal commitment
to its values and objectives, practices that work against the spirit of the policy still abound.
Stigma and discrimination are obvious examples. Despite decades of awareness raising and
education, stigma and discrimination against infected and affected people continues to be a
concern in many societies. Job security is not assured and many people can be fired or let go
due to their HIV positive status. As a social contract in the workplace, policies are
fundamental to protect people‟s rights. Care must be taken when implementing workplace
policies that they adhere to the principles in the policy declarations as well as acknowledge
and address stigma and discrimination when they arise.
1.3 Purpose of the study
This study sought to assess the implementation of HIV/AIDS policies in the workplace by
private organisations. The institutions chosen as case studies were Reproductive Health
Uganda, and Uganda Telecom Limited.
1.4 Objectives
The major objective of this study was to assess the implementation of workplace HIV/AIDS
policies in private institutions in Uganda and establish the challenges faced.

4
1.5 Specific objectives
The specific objectives of this study were:
1. To determine the level of exposure of the employees to the HIV/AIDS workplace
policy.
2. To assess the functionality of the workplace HIV/AIDS policies in private institutions
in Uganda.
3. To investigate the major challenges facing implementation of workplace HIV/AIDS
policies by private institutions.
4. To suggest recommendations towards the improvement of workplace HIV/AIDS
policy implementation.
1.6 Research Questions
1. To what extent are the employees of the two organisations exposed to the HIV/AIDS
workplace policy?
2. To what extent are the HIV/AIDS policies functional in the two study private
institutions?
3. What are the major challenges facing implementation of workplace HIV/AIDS
policies by private institutions?
1.7 Significance of the study
To academicians, it is hoped that the results of this study will help fill in some gaps that
previous similar studies could have left, and contribute to relevant body of information;
To policy makers and implementers, the researcher hopes that the results of the study will
inform the design and formulation of future workplace HIV/AIDS policies and refine existing
national policies.
To other organizations, it is hoped that the findings of the study can create a ripple effect for
other agencies to copy in the implementation of their related policies on HIV/AIDS.

5
1.8 Scope of the study
The study was limited to assessing the implementation of workplace HIV/AIDS policies in
two purposively selected private sector institutions in Kampala. It covered the period between
2005 and 2010 within which the researcher through his review of related literature feels
workplace HIV/AIDS policies took root especially in Uganda.
1.9 Conceptual Framework
Dependent Variable
Functionality of workplace HIV/AIDS
policies
- Reduction in stigmatization
- Increased disclosure of HIV/AIDS
status
- Availing HIV/AIDS health care
services
- Positive living
- Quality of working relationships
Intervening Variables
- Stigmatization
- Resistance to routine HIV
counselling and testing
- Low productivity of the HIV+
employees
Independent Variable
Workplace HIV/AIDS policies
- Non-discrimination on basis of
sero-status.
- Equal involvement of HIV+
employees.
- Confidentiality about
employees‟ sero-status.
- Routine workplace HIV
counseling and testing.
6
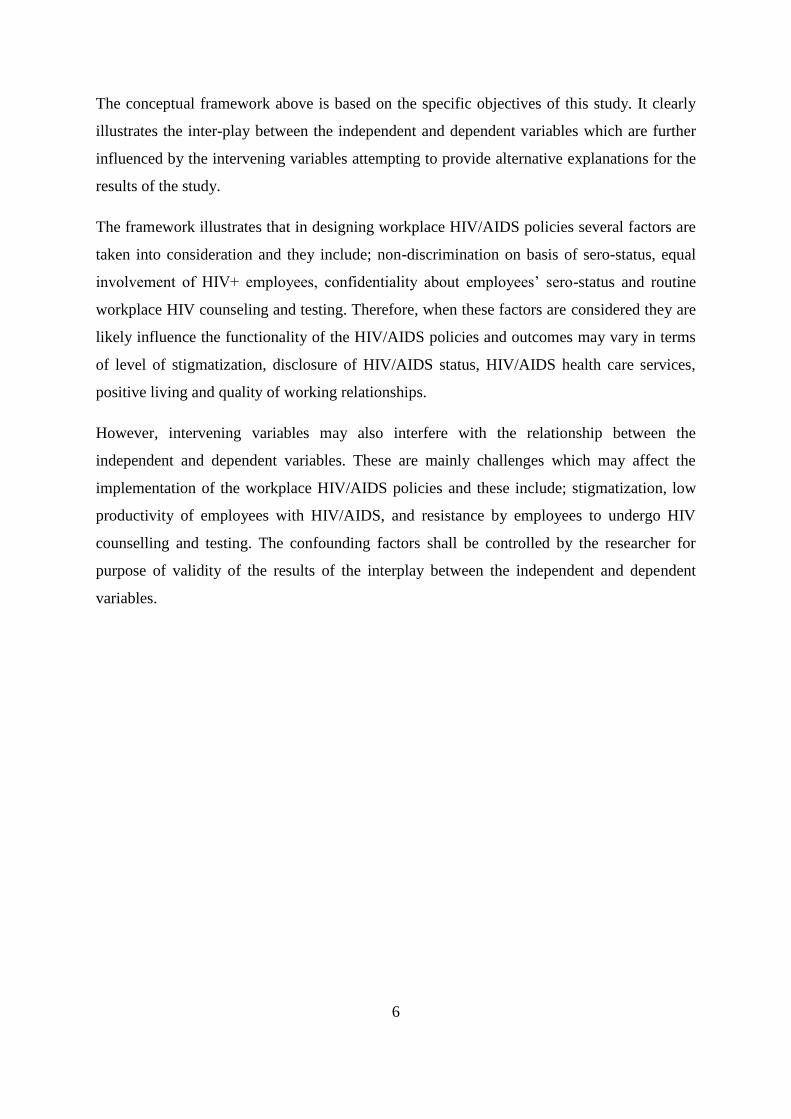
The conceptual framework above is based on the specific objectives of this study. It clearly
illustrates the inter-play between the independent and dependent variables which are further
influenced by the intervening variables attempting to provide alternative explanations for the
results of the study.
The framework illustrates that in designing workplace HIV/AIDS policies several factors are
taken into consideration and they include; non-discrimination on basis of sero-status, equal
involvement of HIV+ employees, confidentiality about employees‟ sero-status and routine
workplace HIV counseling and testing. Therefore, when these factors are considered they are
likely influence the functionality of the HIV/AIDS policies and outcomes may vary in terms
of level of stigmatization, disclosure of HIV/AIDS status, HIV/AIDS health care services,
positive living and quality of working relationships.
However, intervening variables may also interfere with the relationship between the
independent and dependent variables. These are mainly challenges which may affect the
implementation of the workplace HIV/AIDS policies and these include; stigmatization, low
productivity of employees with HIV/AIDS, and resistance by employees to undergo HIV
counselling and testing. The confounding factors shall be controlled by the researcher for
purpose of validity of the results of the interplay between the independent and dependent
variables.

7
CHAPTER TWO
LITERATURE REVIEW
2.0 Introduction
This study aimed at assessing the implementation of workplace HIV/AIDS policies in private
institutions in Uganda. The key concepts in the study were therefore the level of exposure of
the employees to HIV/AIDS workplace policy, the functionality of the workplace HIV/AIDS
policies in private institutions and the major challenges facing implementation of workplace
HIV/AIDS policies by private institutions. It was necessary to make reference to other studies
conducted in areas related to the concepts specifically and the study problem in general.
In this chapter, a discussion is made of such related literature under the themes: Global
situation of the HIV/AIDS pandemic, situation of HIV/AIDS in Sub-Saharan Africa,
HIV/AIDS situation in Uganda, factors fuelling HIV transmission in Uganda, effects of
HIV/AIDS in the workplace, efforts by International organizations and employers in
combating HIV/AIDS in the workplace, salient issues addressed by workplace HIV/AIDS
policies, and challenges facing implementation of workplace HIV/AIDS Policies.
2.1 Global Situation of the HIV/AIDS Pandemic
HIV stands for Human Immunodeficiency Virus. Viruses such as HIV cannot grow or
reproduce on their own, they need to infect the cells of a living organism in order to replicate
– make new copies of themselves. The human immune system usually finds and kills viruses
fairly quickly, but HIV causes AIDS by damaging the immune system cells until the immune
system can no longer fight off other infections that it would usually be able to prevent. It
takes around ten years on average for someone with HIV to develop AIDS (UNAIDS, 2002).
However, this average is based on the person with HIV having a reasonable diet; therefore,
someone who is malnourished may well progress from HIV to AIDS more rapidly.
With around 2.7 million people becoming infected with HIV in 2008, there are now an
estimated 3.3 million people around the world who are living with HIV, including millions

8
who have developed AIDS (WHO 2009, Unicef, 2009). The number of people living with
HIV worldwide continued to grow in 2008, reaching an estimated 33.4 million (31.1 million
– 35.8 million). The total number of people living with the virus in 2008 was more than 20%
higher than the number in 2000, and the prevalence was roughly threefold higher than in
1999. The continuing rise in the population of people living with HIV reflects the combined
effects of continued high rates of new HIV infections and the beneficial impact of
antiretroviral therapy. As of December 2008, approximately 4 million people in low-and
middle-income countries were receiving antiretroviral therapy – a 10 -fold increase over five
years (WHO 2009, Unicef, 2009). In 2008, an estimated 2.7 million new HIV infections and
two million deaths occurred due to AIDS–related illnesses worldwide. The latest
epidemiological data indicate that globally the spread of HIV appears to have peaked in 1996,
when 3.5 million new HIV infections occurred. In 2008, the estimated number of new HIV
infections was approximately 30% lower than at the epidemic‟s peak 12 years earlier (WHO
2009, Unicef, 2009).
Unknown before 1981, HIV/AIDS is now a worldwide pandemic that has claimed more than
28 million lives. An estimated 40 million others are living with HIV, including 19.2 million
women and 2.5 million children under 15 years old. In the U.S, more than 501,669
individuals had died of HIV/AID by the end of 2002, and 384,906 others were believed to be
living with AIDS (UNAIDS, 2002; U.S. Centres for Disease Control and Prevention (CDC)
2003). The Centres for Disease Control and Prevention (CDC) estimates that up to 600,000
additional U.S. residents are living with asymptomatic HIV infection and that one half are
unaware of their condition. The CDC also estimates that at least 40,000 U.S residents become
infected with HIV annually. Additionally, CDC information indicates that in 2002, the
number of diagnosed HIV/AIDS cases in the United States rose to more than 42,000, an
increase of about 1,000 cases from 2001 (UNAIDS, 2002).
In other parts of the world, however, HIV/AIDS can be likened only to the very worst disease
scourges in human history. Four nations in sub-Saharan Africa have general HIV infection
rates today higher than 30 percent. Botswana has 38.8%, Zimbabwe 33.7%, Swaziland 33.4%
and Lesotho 31%). Several others have infection rates above 20 percent, including South
Africa and Zambia. More than 13 million children have been orphaned and broad areas of
regions have been depopulated, with grave implications for entire economies and cultures.
These statistics, and the treatment and prevention challenges behind them, show the desperate

9
need for greater collaborative multi-sectoral strategies and extensive public and private
resources to limit the expansion of HIV/AIDS and address the critical needs of those infected
and directly affected by HIV/AIDS. This is especially true in light of interventions – both
therapeutic and preventive which have proven successful in the U.S. and increasingly in the
developing world (UNDP, 2008; Whiteside et al, 2006).
Notwithstanding its comparatively low HIV prevalence, Asia has not escaped the epidemic‟s
harmful consequences. The economic consequences of AIDS will force an additional 6
million households in Asia into poverty by 2015 unless national responses are significantly
strengthened (Commission on AIDS in Asia, 2008). The epidemic continues to have an
enormous impact on households, communities, businesses, public services and national
economies in the Sub-Sahara. In Swaziland, average life expectancy fell by half between
1990 and 2007 to 37 years largely due to the pandemic (UNDP, 2008; Whiteside et al, 2006).
2.2 Situation of HIV/AIDS in Sub-Saharan Africa
Developing countries have been severely affected by HIV and AIDS. Sub-Saharan Africa has
been declared as the region most severely hit by HIV and AIDS. It is home to just six percent
(6%) of the world population but, statistics indicate that two thirds of all the people living
with HIV worldwide are found in Sub-Saharan Africa (Desmond, Karam & Steinberg 2003).
Research has shown that HIV/AIDS and other infectious diseases thrive in the communities
where there is much poverty (Bendell, 2003). People from environments that are poverty-
stricken cannot afford basic needs, such as healthy food and clean water. The observations of
Kauffman and Lindauer (2004) concur that poverty exacerbates HIV and AIDS. Moreover,
HIV/AIDS affects all spheres of life including the workplace.
Africa‟s share of the horror of the estimated 40 million people worldwide infected with
HIV/AIDS at the end of 2001, at least 70 percent or 28.1 million were residing in Sub-
Saharan Africa (Development Management Associates; 2002). About 3.4 million new
infections occurred in 2001 and 2.3 million Africans died of AIDS in that year alone. The
epidemic caused the death of both parents of 1.7 million African children by the end of 1999.
Africa‟s share of total estimated deaths due to HIV\AIDS since the beginning of the epidemic
is above 85 percent. By comparison with other regions, this is a crisis.

10
Dr. EM Samba (2000), the director of the World Health Organisation‟s Regional Office in
Africa said the following regarding the impact of HIV/AIDS on the African continent:
“…the sad and gloomy scenario is becoming even more painfully
familiar: everyday, cemeteries and funeral service outfits in rural and
urban Africa brim with business – welcoming and handling new
arrivals…in some of our countries, at least 2000 people are buried
every week, victims, we now know of the HIV/AIDS pandemic”.
South Africa has been declared as the country worst affected by HIV/AIDS and Kauffman
and Lindauer (2004:17) go as far as referring to South Africa as “the HIV capital of the
world”. A number of factors have fuelled the spread of HIV in sub Saharan Africa as
summarised below:
Although individual worker‟s behaviour and decision do play major roles in reducing or
increasing the risk of infection, certain types of work situations are more susceptible to the
risk of infection than others. Work involving the mobility of a youthful workforce in
industrial enterprises such as mines, oilfields, and road and dam-building projects are for
example high on the list. Workers posted in geographically isolated environments with
limited social interaction and limited health facilities and those engaged in highway
transportation are also vulnerable. Work involving occupational risks such as contact with
human blood using inadequate equipment is equally susceptible to the risk. So is work that is
dominated by men, where women are in a small minority. Various studies have looked at the
role of truck drivers, both in Africa and in Asia, in the spread of HIV.
Behavioural practices continue to drive the probability curve that a worker and/or employer
may acquire the infection upwards. These include unprotected sexual relationships with
partners, whose HIV status is not known, lack of adherence to infection-control warnings and
cultural norms and values. Finally, a climate of discrimination and lack of respect for human
rights leaves workers more vulnerable to infection and less able to cope with AIDS because it
makes it difficult for them to seek voluntary testing, counselling, treatment or support; they
will also not be in position to take part in advocacy and prevention campaigns. Moreover,
individuals who suffer discrimination and lack of respect for their human rights are both more
vulnerable to becoming infected and less able to cope with the burdens of HIV/AIDS.

11
This spread comes with a number of consequences that include but are not limited to:
Along with the reduction in population size, the distribution of the working population profile
will change in terms of age, skills and work experience as a result of the epidemic. Three
interrelated factors could lead to rising number of widows and orphans, which will alter the
labour market structure as more and more widows and orphans enter to seek a livelihood.
Also as people living with AIDS (generally in the age group of 20-49 years) exit the labour
market, the tendency for early entry of poorly prepared and unskilled children into the active
labour force becomes greater. It is further envisaged that early withdrawal of people with
AIDS from the workplace will increase the need to retain older persons in the labour force
who may not have the necessary stamina to meet the corresponding rigorous labour market
demands.
Cohen sees the end result as the evolvement of a smaller and smaller active labour force and
a greater dependency ratio (Karen A. Stanecki & Peter O. Way; 1996). The US Bureau of
Census has predicted 8 to 31 years of life will have been lost in those countries most affected
by HIV\AIDS in sub-Saharan Africa by the year 2010 (ILO; June 2000) . Using population
data from Botswana, Cameroon, Ethiopia, Cote d‟Ivoire, Kenya, Malawi, Mozambique,
Namibia, Nigeria, South Africa, Tanzania, Uganda and Zimbabwe, the ILO made some
observations as well including the following two: (i) there would be about 24 million fewer
workers in hard hit countries alone in the year 2020 as a result of the AIDS epidemic; and (ii)
the labour force should be 10% to 22 % smaller in those countries with rates greater than
10% than it would have been if there had been no HIV/AIDS by the year 2020 (ILO;
December 2000).
Emanating from the guidelines set by United Nations and the World Health Organisation,
different continents and regions have crafted their own strategies applicable to their
respective regions to address the spread of HIV and the eventual severe impact of the AIDS
pandemic.
2.3 HIV/AIDS Situation in Uganda
Uganda is one of the countries in Sub-Saharan Africa that has demonstrably slowed down the
AIDS epidemic. According to the Ministry of Health HIV/AIDS surveillance report of June
2001, the number of adults with HIV in 2000 was 1,107,644 adults (543,753 women, 453,127

12
men and 110,880 children below 15 years). The decline in HIV prevalence has been
attributed to among others: - extensive national STD/HIV education and treatment
programmes, counselling of PHAs, treatment of opportunistic infections, voluntary HIV
counselling and testing, prevention programmes and a good political will as well as consistent
funding and technical assistance from international donors.
Almost three decades after the first reported cases in Uganda in 1982 (Serwadda, 1985),
AIDS has continued to pose a significant public health and development challenge. Uganda
has a generalized HIV epidemic with a prevalence of 6.4% in adults and 0.7% in children
(UAC, June 2009). Approximately 1.1 million people in Uganda are HIV-infected
(MoH/ORC Macro 2004-5). The incidence rate by far outstrips AIDS related mortality and
the numbers of clients enrolling into chronic AIDS care. The wave of new as well as old
infection has shifted to older age groups (Kirungi et al., 2008) with both HIV incidence and
prevalence in Uganda‟s mature HIV epidemic having stopped declining around 2000 and
hence remaining more or less stable (Kirungi et al., 2006).
The number of people with AIDS, is however on the rise as more people already infected
with HIV are falling sick. The results of the 2011 Uganda AIDS Indicator Survey (UAIS)
indicate that 7.3% of adults age 15-49 in Uganda are living with HIV. Among children under
age five, HIV prevalence is 0.6%. These results are based on a nationwide survey that was
conducted to provide estimates of HIV prevalence and other important HIV/AIDS
programme indicators.
“These results demonstrate indisputably that HIV/AIDS remains a significant health problem
for Uganda and should serve as a call to action for us all,” said Minister of Health Dr
Christine Ondoa. “The Ministry of Health along with our dedicated international partners
takes this as an opportunity to recommit ourselves to continued scale-up of proven HIV
interventions, to the goal of universal access to ARV treatment, and to our shared vision of a
future free of HIV.”
The survey shows that there has been a tremendous increase in voluntary HIV testing in
Uganda over the past 6 to 7 years. The proportion of women age 15-49 who have ever been
tested for HIV and received their results increased fivefold, from 13 percent in 2004-05 to 66
percent in 2011. The increase among men has been somewhat more modest, from 11 percent
in 2004-05 to 45 percent in 2011. The main reason for the gender difference is likely to be the

13
high level of testing of pregnant women. Survey results indicate that almost three in four
pregnant women (72 percent) were tested for HIV and received results as part of their
antenatal care.
Whereas male circumcision has been shown to have a protective effect on HIV transmission,
the proportion of Ugandan men age 15-49 that are circumcised has remained almost
unchanged at 26%. The proportion of men circumcised ranges from 2 percent in Mid
Northern region to 53 percent in Mid-Eastern region. Furthermore, the data indicates that
multiple sexual partnerships (proportion of respondents having two or more partners in the
previous 12 months), which is a key driver of Uganda‟s HIV epidemic, remains unacceptably
high at 25% among men and 4% among women.
The UAIS results demonstrate both the strengths and challenges of Uganda‟s HIV response.
The survey identifies a continued need for individual behaviour change, and scale-up of
evidence-based prevention interventions such as prevention of mother-to-child transmission
services and safe male circumcision, as well as increased treatment coverage for people living
with HIV. Interventions should be targeted to those most-at-risk populations and must pay
particular attention to those regions and districts most heavily impacted by the epidemic.
This tailored and enhanced approach should significantly impact future rates of HIV infection
in Uganda. Women, urban dwellers and residences of the post conflict northern Uganda
region are more disproportionately affected.
In Uganda, sexual transmission continues to contribute 76% of new HIV infections while
mother to child transmission contributes 22%. Currently, estimates indicate that over 100,000
new infections occur annually. During 2008, an estimated 110,694 new HIV infections
occurred countrywide and approximately 61,306 people died from AIDS related illnesses in
2008 (MoH, 2009).
2.3.1 Factors Fuelling HIV Transmission in Uganda
A review of assessments of the epidemiology of HIV infection in Uganda reveals evidence of
the factors associated with increased risk of HIV transmission (UAC, 2006). Sex with
multiple partners, HIV discordance among married and co-habiting couples, intact foreskin
and infection with genital herpes (HSV-2) and other STIs appear to be some of the current

14
key risk factors fuelling the HIV epidemic in Uganda. The perception that HIV&AIDS is
normal by some sections of the community has also contributed to some form of
disengagement from preventive behaviour, (UAC 2006; 2007).
There is increasing evidence according to the Uganda AIDS Commission (2007) to show that
the number of multiple sexual relationships increased between 2001 and 2005 from 25% to
29% in men and from 2% to 4% in women. Among married couples, the proportion reporting
extra-marital sex during the same period increased from 14% to 29% among men but
remained stable at 3% among women.
Historically, the zero grazing campaigns of the late 1980s had a great impact on HIV
transmission contributing to the decline in prevalence from 18% to 6.4%. Married and co-
habiting couples are thus a key population group that needs to be targeted with an HIV
prevention package specifically designed to suite the uniqueness of marital relationships.
Serwadda et.al, (1995) in a study conducted as part of the Rakai Health Sciences Program
showed that the risk of HIV transmission among discordant couples is as high as 10 times the
risk of transmission among the general population. A secondary analysis of the 2004-05
Uganda HIV Sero- Behavioural Survey (UHSBS) showed that among couples where one is
HIV positive, 40% have an HIV negative spouse and only 9% are aware of the HIV status of
their spouse (Bunnell et al. 2007). In addition, of their last unprotected sexual encounters,
84% were with their spouses and 13% with steady partners.
Available evidence suggests that overall, consistent condom use is very low. Between 2001
and 2005, condom use during the most recent sexual intercourse with casual sex partners
increased from 39% to 48% among women, but decreased from 61% to 53% among men.
This low use of condoms irrespective of type of partner increases vulnerability to HIV
transmission.
The evidence linking lack of circumcision with increased risk of HIV transmission is
overwhelming. Three randomized controlled trials including one in Uganda showed efficacy
of medical male circumcision as a prevention intervention against HIV transmission, a
vaccine with 50% - 60% efficacy (Gray et. al., 2007).
Thus, the most-at-risk behaviours that put people at greater risk of HIV infection include:
high rates of multiple sexual partnerships, low rates of condom use, high rates of concomitant

15
STIs, unprotected anal sex with multiple partners and injecting drug use with shared
equipment.
Whereas HIV&AIDs is now a generalized epidemic in Uganda, there are still population
groups in which most-at-risk behaviours are concentrated. These include commercial sex
workers and their partners, long distance truck drivers (see Morris and Ferguson 2006), fisher
folk, uniformed services, men who have sex with men (MSMs) and injecting drug users
(IDUs).
Whereas information on men who have sex with men (MSMs) and injecting drug users
(IDUs) is either scanty or unavailable in Uganda, one study on MSM (Kajubi et al. 2008) in
Uganda shows that 39% of the MSMs reported being bisexual, 37% had unprotected
receptive anal sex in the last six months and 11 % reported a history of urethral discharge.
The Modes of Transmission (MOT) study predicts that 43% of all new HIV infections
expected to occur in the next year will be among persons in mutually monogamous
relationships among the sexually active adult population aged 15 – 49 years (Odiit, 2008).
This proportion is only second to those in casual sexual relationships. Married and co-
habiting couples are thus a key population group that needs to be targeted with an HIV
prevention package specifically designed to suite the uniqueness of marital relationships. It is
not enough to assume that they will benefit from interventions targeting the general
population (Odiit, 2008).
Trends in prevalence among the adolescents and young people especially those aged 15 – 19
year olds reflect recent trends in HIV incidence since this age group has recently initiated sex,
duration of infection is short and mortality is low. Abstinence programs have been quite
successful in this age group. Life-skills training, for both in-school and out of school
children, have also been successful leading to a decline in HIV prevalence and an increase in
age of sexual debut (UHSBS, 2005).
In terms of sexual behaviour, the UHSBS showed that youth who are orphans or vulnerable
children were slightly more likely to have sex by age 15 than other youth. Young women
classified as orphans and vulnerable children (OVC) were 1.5 times more likely to initiate sex
before age 15 than other young women, while young men who were OVC are 1.1 times as

16
likely. These findings emphasize the need to protect OVCs from the risk of acquisition of
HIV.
Various factors associated with social and cultural values, beliefs, perceptions and practices
are known to influence dominant sexual behaviours that have a bearing on HIV prevention.
For instance, the value for children, even when people know they have HIV amid limited
social services such as PMTCT and ART, and the pressure exerted by society has tended to
influence adults to have diminished control over their sexuality (Oundo and Siu 2006).
Despite some progress in human rights protection, many women often have little say in all
matters concerning their lives including sex, and young girls are socialized likewise (Whyte
1997); thus the social impact of HIV infection has increased women's vulnerability (Porter,
2004).
In the event of a more urbanized mobile family, in relation to guidance against HIV&AIDS,
the role of peers has increased in importance as the role of parents has diminished (Neema et
al. 2000). These too are struggling with a plethora of new cultures and practices which have a
negative influence on young people‟s ability to prevent HIV infection.
Many studies (e.g. UNAIDS 2004; UNESCO 1999; PSI 2006) have long shown the linkages
between economic aspects especially poverty with transactional sex. Cases of sexual
exploitation, mostly unprotected cross-generational sex (Neema et al. 2004), in some cases
involving male adolescents with old women (Bohmer and Kirumira 2000), and unwanted
pregnancies for female youths (Kyaddondo et al. 2005) have been reported.
2.4 Effects of HIV/AIDS in the workplace
The epidemic‟s impact on the education system could affect the quality of future labour
inputs in the workplace mainly resulting from poor outflow of new entrants into the labour
market. Few studies have made the case forcefully. One school suggests that the epidemic‟s
effect on the school system is manifested in its impact on students‟ learning curves and
classroom performance. The hypothesis is that children who have to live daily carrying
within them the grief, trauma and/or experiences of seeing close relatives, friends and
teachers fall sick, suffer and die of AIDS, would be in a more vulnerable state of mind in
responding to learning. Furthermore, there are a number of students who would have lost
their parents or guardian to AIDS subjecting them to a lower living standard in the absence of

17
alternative source of income (Loewenson, R. & Kerkhoven, R.; May 1996). For these
children, balancing the demands of school and the demands of life could present a practical
problem. The problem could become even more disturbing for students who know that they
are infected with the virus, and will die of it someday. In addition to the fright of dying and
the loss of hope for living, the tendency is high for such students to shy away from active
participation in class work and therefore retard in learning and performance.
Teachers are not exempted from these trauma or loss of life either. Deaths among teachers are
occurring in large numbers in highly affected countries. For example, the number increased
by 60 % between 1994 and 1999 in Botswana including 84 primary school teachers who died
in 1999 as compared to only 8 in 1994. In Zambia, 40 % of teachers are infected with HIV
and are dying at a faster rate than the number of teacher graduations. Filling in the gap is
indeed a very difficult task. On the other hand, the quality of instruction diminishes as more
and more teachers fall sick. Frequent bouts of sickness of either teachers or family members
take away many person hours from classroom teaching. Worse still, the stress of sickness and
the knowledge of impending death reduces the quality of lecture preparation and delivery.
The end result is the poor quality of people flowing from the education system in relation to
the demands of the workplace and society (Loewenson, R. & Kerkhoven, R.; May 1996).
Many African governments have called upon the business community in their respective
countries to join in the fight against HIV/AIDS. Public sector institutions, NGOs and CBOs
are also involved in promoting a viable and supportive response to the epidemic. There are
direct and opportunity costs associated with each intervention taken in response to this call.
As the rate of infection increases, so are the costs associated with the epidemic. These
increasing costs may ultimately affect the level of benefits that a business is able to provide
for its workforce.
Cost increases come about through a variety of ways, three of which are worth mentioning.
Demand for recruitment and training rises as a result of increased staff turnover and loss of
skills. For example, 36 out of 1600 employees of Barclays Bank in Zambia died of AIDS-
related sicknesses. Situations like these, call for the employment of extra labour, multi-
skilling, succession strategies and extensive human resource monitoring only to cope with
staff fluctuations and losses. These are done mainly through training, re-training and
recruitment costs, which would mean falling rates of return on human capital formation. The
18
higher income and more skilled employee categories of staff involved, the greater the cost
(Sehgal, Jag M.; November 1999).
Secondly, the costs to enterprises, public or private, are those incurred in the provision of
health care for infected employees. A study (Rugalema, 1999) of a commercial agro-estate in
Kenya estimated that “medical expenditure rose to over 400 % above that of projected
expenditure without AIDS” (Sehgal, Jag M.; November 1999). However, the provision of
health care in countries where public health care provision is limited and private health care
expensive, the cost could be considered an investment, preventing or limiting
sickness\absenteeism and controlling workforce health risks.
Finally, company life insurance premiums and pension fund commitments will rise as a result
of early retirement or death. This is particularly problematic in those economies where such
benefits are more comprehensive. For example, in Zimbabwe, over a two-year period, life
insurance premiums quadrupled as a result of HIV\AIDS. Where businesses provide for the
funeral costs of employees, the operating cost component could get bigger as mortality rate of
HIV\AIDS gets bigger. Additional costs are incurred from frequent absenteeism due to illness
or attendance at funerals, as well as time spent on training. Whiteside (1999) calculated that
absenteeism accounted for anywhere between 25-54 percent of costs on average for a group
of businesses in East Africa (Karen A. Stanecki & Peter O. Way; 1996).
HIV/AIDS is a threat to enterprise delivery capacity and performance. The impact of the
epidemic has therefore raised a number of concerns for the employer and self-employed who
demand labour inputs to sustain their enterprises. A major area of concern is the high labour
turnover due to HIV/AIDS related deaths. The case is serious as the rapid turnover leads to a
less experienced workforce relative to the skills demanded (UNDP; “June 2001, p 10).
Another area of concern is the effect of the pandemic on the competitiveness of enterprises in
the production of quality goods and services. Losses in labour time and skills will reduce the
quantity and quality of outputs produced. This can directly affect the quality of products and
services, leading to reputation losses and ultimately a reduction in customers. Quality of
goods and services produced by small firms in the formal and informal sectors also suffer
from the effects of the epidemic. Loss of one or more key employees may be even more
catastrophic. It has been observed that food production reduced and food security declined in
rural sectors as labour and time are reallocated from agricultural work to non-agricultural
care activities. Maize outputs for small farmers in Zambia fell by 45 % due to all deaths.

19
When AIDS was factored out as the cause of death, maize production figures went down by
61%, cotton 47 %, vegetables 49 % and groundnuts 37 % respectively (UNDP; “June 2001, p
10).
Disruption in the production process due to the loss of skills from the workforce is another
area of concern for the renters of labour. Such disruption is severed if it is a loss of
“intellectual capital”, which has become increasingly important relative to “financial capital”
and with the progressive changes in the way companies are now valued. In other words, skills
losses could lead to lower value or lower quality products and decrease the value of goods
produced. Finally, what happens in one sector could impact events in another sector. For
example, skills losses and interruption of production in say the telecommunications and
electricity sectors may lead to production losses in all other sectors that use these services. In
the public sector, skills losses in an already skills deficit situation, will compound problems
of public administration and policy management (UNDP; “June 2001, p 10).
A direct link exists between HIV\AIDS and declining productivity and profits. The bottom
line is that declining levels of productivity could lead to declining profits especially when
production costs are not declining at an equal or higher rate, as is usually the case when the
prevalence rate of HIV/AIDS is high among the productive segment of the population. We
had reviewed earlier the increasing costs associated with the need for employers and
individual workers to redress the rising scourge of the epidemic. For example a transport
company in Zimbabwe incurred a total cost equal to 20 percent of profits to deal with
HIV/AIDS related issues in the company (Stover, J. & Bollinger, L. ; 2000).
One principal area in which HIV\AIDS impacts on productivity in addition to costs escalation
is increased organisational disruption within the workforce due to high rates of morbidity and
mortality. Usually making prompt and adequate adjustments to the erratic rate of staff
turnover coupled with the loss of skills and tacit knowledge can be very difficult. The main
problem is the passing on of acquired skills and knowledge, which has been such a major
factor in the growth of labour productivity, diminishes. Besides, staff morale can be severely
affected by the loss of colleagues; discrimination against people living with HIV\AIDS; and
the disruption of work activities to attend infected and affected workmates. These less visible
organisational factors are built up over longer time frames and are critical for a more
efficient, effective and ultimately productive workforce. While these factors may be

20
essentially invisible in nature and difficult to calculate, their impact on productivity levels is
nonetheless enormous (Stover, J. & Bollinger, L.; 2000).
As discussed earlier, HIV/AIDS could lead to less productive employment and lower earning
power. These would in turn depress domestic private savings. It should be noted that national
savings are the outcome of what happens to domestic savings and the balance of capital
inflow and outflow. Consequently, depressed domestic savings would lead to depressed
investments and eventually to depressed growth. Attempts to quantify this expected decline
in growth indicators as a result of HIV/AIDS have been made. One study using data from
Tanzania, Cameroon, Zambia, Swaziland, Kenya, KwaZulu-Natal and a few other Sub-
Saharan African countries found that the “rate of economic growth may be reduced by as
much as 25 percent over a 20-year period as a result of the HIV/AIDS pandemic” (ILO; June
2000, p. 12.] . Way and Over, (1992) also concluded that “AIDS could suppress gross
domestic product (GDP) by as much as 10 percent over a 15-year period” (Loewenson, R. &
Kerkhoven, R.; 1996).
HIV/AIDS has multiple implications for the smooth functioning of public services. Besides
causing prolonged absenteeism and the loss of key staff, the disease drains the organisations
of institutional memory, of tacit knowledge of the workings of institutions, and of new ideas
and energy that younger staff members could bring to the work environment (Rau, 2003).
HIV/AIDS affects the economically active age groups; therefore the implications for the
world of work are unlike those associated with any other disease. In addition, the fact that the
disease, in an infected employee, remains “invisible” for years and then follows an often
unpredictable pattern from symptomatic HIV disease to death means that it is very difficult to
plan for an organisation‟s human resource needs (Smart, 2004).
For the private sector, HIV/AIDS affects both productivity and profitability; the effects on
productivity include increased absenteeism, staff turnover and lower staff morale. The
impacts of HIV/AIDS on profitability include increased costs, declining investment and
threat to consumer base (Maphosa, 2003). It is argued that these effects will negatively
impact on tax revenues and domestic and foreign investment, levels of human capital and,
ultimately, the macro-economy as a whole (Pharoah, 2005).
Page et al., (2006) say that HIV/AIDS affect people in their economically active years which
are mostly the ages of 25 to 49 years. The HIV-infected person - depending on the

21
individual‟s lifestyle, access to treatment and the progression of the viral load - can become
less productive as fatigue and opportunistic infections set in. Should the HIV-infected person
die, his or her knowledge, training and experience will also be lost by the workplace.
In view of the foregoing points, the International Labour Organisation (ILO) declared
HIV/AIDS as a workplace issue (ILO, 2001). The effects of HIV/AIDS on the work
environment prompted the ILO to outline guidelines to be followed by its member states in
the mitigation of the impact of HIV/AIDS in the workplace.
Page et al., (2006) further observe that HIV/AIDS is a concern for the workplace because of
the consequences of HIV and AIDS, such as an inability to work due to poor health and
eventually death, the financial constraints placed on companies due to medical aid claims
absenteeism and loss of employees, the stress and trauma experienced by employees due to
the illness and deaths of colleagues, morale degeneration due to the loss of colleagues,
burnout experienced by the remaining employees due to ever growing amounts of work, a
potential decrease in productivity, the loss of skills and finally stigmatisation and
discrimination against people suspected to be infected or affected by HIV and AIDS.
2.5 Efforts by International Organizations and Employers in Combating HIV/AIDS
in the Workplace
According to the Joint United Nations Programme on HIV/AIDS and the International
Organisation of Employers (2002), the majority of employers are concerned with how to
protect their workforce from HIV infection and how to deal with those who are already
infected.
Actual initiatives taken by an employer to respond to HIV/AIDS in his or her company,
however, will depend on the following two key factors:
i. The HIV prevalence rate within the company and the surrounding community; and
ii. The level of knowledge and awareness by the management of the real and potential
impacts of the pandemic.
Understanding the potential impact on needs and capacity is essential in mobilizing
HIV/AIDS responses and enabling effective planning, action and efficient use of available
resources. This should clearly identify key areas of susceptibility and vulnerability of
employees and overall system function.

22
Informed planning in many severely affected countries requires projection of the scale of
various impacts (Lamptey & Gayle, 2001).
The Joint United Nations Programme on HIV/AIDS and the International Organisation of
Employers (2002) further mention five main initiatives that an organisation can take to
respond to HIV/AIDS in the workplace which are: developing a HIV/AIDS policy for the
company, providing HIV prevention education in the workplace, providing care and support
in the workplace, Implementing fair employment practices and community involvement.
Many countries now have HIV/AIDS policies and, increasingly, countries are also adopting
HIV/AIDS policies for the workplace; in some countries, specific ministries have designed
AIDS policies for their workforces. The rationale for a ministry developing an AIDS
workplace policy is to provide its employees with clear statements on expectations and
responsibilities (Rau, 2003).
These policies are based on the International Labour Organisation (ILO) Code of Practice on
“HIV/AIDS and the World of Work”, the code of practice contains fundamental principles
for policy development and practical guidelines from which concrete responses can be
developed at the enterprise, community and national levels (International Labour
Organization, 2001). The code is adaptable to a variety of situations and different levels of
resources (Joint United Nations Programme on HIV/AIDS (UNAIDS) and the International
Organisation of Employers (IOE), 2002).
A workplace policy provides a framework for action to reduce the spread of HIV/AIDS and
manage its impact. It defines an institution‟s position on HIV/AIDS, and outlines activities
for preventing the transmission of the virus and providing care and treatment for staff who
are infected. It also ensures that the response is balanced, activities complement each other,
and resources are used most effectively (Pharoah, 2005).
A good HIV and AIDS workplace policy always contains an outline or a description of how
the particular organisation, institution or business is going to manage HIV and AIDS on a
day-to-day basis. Establishing an HIV/AIDS programme and policy in the workplace is a
cost-effective solution and will help reduce the future spread and impact of the disease
(UNAIDS, 1998).
An HIV and AIDS workplace programme is an action-oriented plan that an organisation will

23
implement in order to prevent new HIV infections, provide care and support for employees
who are infected or affected by HIV or AIDS, and manage the impact of the epidemic on the
organisation. It outlines how all the different principles within the policy will be translated
into practice at the workplace (Stellenbosch University and the USAID Health Policy
Initiative, 2008).
Workplace HIV/AIDS programmes are most effective when they include a comprehensive
and coordinated set of prevention, care, and support components. Whether they are provided
directly by employer or by employer sponsored referrals to service providers in the
community, such programs are more likely to be strong, cost-effective, and sustainable
(Academy for Educational Development, 2004).
2.6 Salient Issues addressed by Workplace HIV/AIDS Policies
The International Labor Organization (ILO) provides a comprehensive framework which
addresses how Persons Living with HIV/AIDS should be handled at the workplace. It also
has a policy document which guides the design and development of workplace HIV/AIDS
issues and spells out the salient issues how they are to be observed by employers.
ILO‟s policy regarding personnel issues emphasises that employers should not engage in nor
permit any personnel policy or practice that discriminates against workers infected with or
affected by HIV/AIDS. In particular, it clearly spells out that employers should not require
HIV/AIDS screening or testing unless otherwise specified in section 8 of this code; ensure
that work is performed free of discrimination or stigmatization based on perceived or real
HIV status; encourage persons with HIV and AIDS-related illnesses to work as long as
medically fit for appropriate work; and provide that, where a worker with an AIDS-related
condition is too ill to continue to work and where alternative working arrangements including
extended sick leave have been exhausted, the employment relationship may cease in
accordance with anti-discrimination and labour laws and respect for general procedures and
full benefits.
To address issues pertaining to grievances and disciplinary procedures, the ILO Code of
Practice on HIV/AIDS and the World of Work (2001) provides that employers should have
procedures that can be used by workers and their representatives for work-related grievances.
These procedures should specify under what circumstances disciplinary proceedings can be

24
commenced against any employee who discriminates on the grounds of real or perceived HIV
status or who violates the workplace policy on HIV/AIDS. Regarding confidentiality,
HIV/AIDS-related information of workers should be kept strictly confidential and kept only
on medical files, whereby access to information complies with the Occupational Health
Services Recommendation, 1985 (No. 171), and national laws and practices. Access to such
information should be strictly limited to medical personnel and such information may only be
disclosed if legally required or with the consent of the person concerned. Organizations are
required by the code to adhere to the set standards of risk reduction and management, which
calls on employers to ensure a safe and healthy working environment, including the
application of Universal Precautions and measures such as the provision and maintenance of
protective equipment and first aid. To support behavioural change by individuals, employers
should also make available, where appropriate, male and female condoms, and counselling,
care, support and referral services. Where size and cost considerations make these difficult,
employers and/or their organizations should seek support from government and other relevant
institutions.
In the design and development of Workplace HIV Policies by organizations, workers and
their representatives are required to consult with their employers on the implementation of an
appropriate policy for their workplace, designed to prevent the spread of the infection and
protect all workers from discrimination related to HIV/AIDS. Workers and their
organizations should adhere to national law and practice when negotiating terms and
conditions of employment relating to HIV/AIDS issues, and endeavour to include provisions
on HIV/AIDS protection and prevention in national, sectoral and workplace/enterprise
agreements. Workers and their organizations should use existing union structures and other
structures and facilities to provide information on HIV/AIDS in the workplace, and develop
educational materials and activities appropriate for workers and their families, including
regularly updated information on workers‟ rights and benefits.
The effects of HIV/AIDS on the socio-economic status of individuals as well as on the
economy of nations cannot be underscored. And in cognizance of this fact, workers and their
organizations have the obligation to work together with employers to develop appropriate
strategies to assess and appropriately respond to the economic impact of HIV/AIDS in their
particular workplace and sector. They have also championed initiatives to work with
employers, their organizations and governments to raise awareness of HIV/AIDS prevention

25
and management. The ILO Code of Practice on HIV/Aids and the World of Work (2001)
provides that workers and their representatives should support and encourage employers in
creating and implementing personnel policy and practices that do not discriminate against
workers with HIV/AIDS. It also asserts that workers‟ representatives have the right to take up
issues at their workplaces through grievance and disciplinary procedures and/or should report
all discrimination on the basis of HIV/AIDS to the appropriate legal authorities.
Similarly, Stellenbosch University and the USAID Health Policy Initiative, (2008) have
identified that the key elements of an HIV and AIDS workplace programme include:
An impact assessment of HIV and AIDS on your organisation, HIV and AIDS awareness
programmes, voluntary counselling and HIV-testing programmes, HIV and AIDS education
and training, condom distribution, encouraging health treatment for STIs and TB, universal
infection-control Procedures, creating an open and accepting environment, wellness
programmes for employees affected by HIV and AIDS, the provision of antiretroviral or
referral to relevant service providers, education and awareness about antiretroviral and
treatment literacy programmes, counselling and other forms of social support for HIV-
positive employees, reasonable accommodation for HIV-positive employees, strategies to
address direct and indirect costs and other practical implications of HIV and AIDS
monitoring, evaluation and review of the programme.
2.7 Challenges facing implementation of workplace HIV/AIDS Policies
UNAIDS, (1998) says that organisations face enormous challenges in responding to
HIV/AIDS such as setting up comprehensive, sustained programmes, adopting relevant
policies, obtaining management commitment, ensuring confidentiality and non-
discrimination, supporting staff who are infected with HIV/AIDS, dealing with attitudes of
co-workers and sustaining involvement (UNAIDS, 1998).
Other challenges include strengthening existing structures as well as capacity to develop and
implement workplace programmes and having specific issues related to HIV/AIDS
incorporated into planning and implementation of departmental core functions (GTZ, 2003).
Among the greatest challenges in addressing HIV/AIDS are stigma and discrimination. They
often result from fear caused by myths, misinformation, and a lack of knowledge about how
HIV is and is not transmitted. The negative effects of workplace stigma and discrimination

26
can be substantial, both to the business and to workers themselves (Academy for Educational
Development, 2004).
In a study conducted by Chetty in 2006, despite the existence of the policy and formal
commitment to its values and objectives, practices that work against the spirit of the policy
often continue. Stigma and discrimination are an obvious example. Despite decades of
awareness raising and education, stigma and discrimination against infected and affected
people continues to be a concern in many societies. Job security is not assured and many
people can be fired or let go due to their HIV positive status.
As a social contract in the workplace, policies are fundamental to protect people‟s rights.
Care must be taken when implementing workplace policies that they adhere to the principles
in the policy declarations as well as acknowledge and address stigma and discrimination
when they arise. The segments of the population affected most are the youths and people
within the productive age bracket most of who constitute the nation‟s workforce. Response to
the HIV/AIDS pandemic within the workplace is crucial if progress is to be made in the
prevention, impact mitigation and the provision of care and support for People Living with
HIV/AIDS (PLWHA) and People affected by HIV/AIDS (Chetty, 2006).
The Interagency Coalition on AIDS and Development (2004), outlines some of the
challenges facing the development and implementation of Workplace HIV/AIDS policies as;
the level of staff participation required in terms of research and policy development,
implementation, communication, monitoring and adjustments; perceived costs involved in
training; the duty to accommodate altered work schedules; legal input and associated costs;
possible costs for consultant to research and develop policy; regular review necessary - who
will do this, when and who is responsible for tracking legislative or human rights up-dates?;
different codes and standards between organizations, union and non-union requirements;
considerations for parity; stigma and/or discrimination; and lack of human and financial
resources as well as attitude issues around willingness to develop such a policy.
The National Tripartite Committee of Ghana, 2004, complements that the fundamental rights
to workers infected by the AIDS virus or affected by HIV/AIDS is compromised with respect
to the pervasive discrimination and stigmatization that such workers face especially in the
case that fellow workers are not sensitized about the implications of stigma.

27
CHAPTER THREE
RESEARCH METHODOLOGY
3.0 Introduction
Chapter three presents a detailed description of the selected research design. It details what
was done and how it was done. It comprises several sub-sections which include the research
design, study population, sampling, data collection/instrumentation, data quality management
including validity and reliability, and data analysis, research procedure and data quality
control.
3.1 Research Design
The study employed a case study design to investigate the challenges of implementing the
Workplace HIV/AIDS policies at Uganda Telecom Limited and Reproductive Health
Uganda. Data collection strategy was both qualitative and quantitative, using structured and
semi-structured interviews, document analysis and FGDs. Probability and non-probability
sampling techniques were used for the study.
3.2 Study area
The study was carried out at the head offices of Reproductive Health Uganda and Uganda
Telecom Limited, both located in Kampala city.
3.3 Population of the study
This study was conducted at Reproductive Health Uganda and Uganda Telecom Limited
from where a population of seventy (70) respondents were targeted in both organisations. The
targeted respondents were those in the positions of managers, officers and assistants.
3.4 Sample size
The sample consisted of ninety sixty (60) respondents in total; selected from Reproductive
Health Uganda and Uganda Telecom Limited. The following formula was used to determine
the sample size;

28
Formula is: n = N
1+N (e) 2
Whereby “n” is unknown sample you want to arrive at
“N” is the total number of beneficiaries
1 is a constant
“e” is the acceptable error in research always expressed as 0.05 or 0.01
3.5 Sampling Techniques
This study employed both probability and non probability sampling techniques namely
purposive sampling and systematic random sampling to select the respondents for the study.
Sampling techniques refer to a description of the strategies which the researcher will use to
select representative respondents from the target population (Onen and Oso, 2005).
Purposive sampling was used to select the two private institutions from where the sixty (60)
respondents were drawn. This is because large institutions are more likely to have
comprehensive human resource management policies including HIV/AIDS workplace policy.
Purposive sampling is a non-probability type of sampling in which the researcher decides
who to include in the sample for the purpose of collecting focused information for the study
(Onen and Oso, 2005).
Systematic random sampling was used to select the sixty employees from the two institutions.
Every third (3rd
) employee from the list of each of the two institutions was a respondent. The
list was generated by randomly assigning a number of each of the other employees from each
organization. This was done in order for the researcher to obtain a representative sample. In
systematic random sampling, the researcher selects the „nth
‟ number of the population from a
randomized list of the population. It employs a probability sampling strategy (Onen and Oso,
2005). Purposive sampling was then used again to select ten (10) key informant respondents
from each of the two private institutions, after the systematic random sampling which
generated the sixty respondents.

29
3.6 Data collection techniques and instruments
Collection of the data involved the use of a number of methods including questionnaire
surveys, focused group discussions, and document analysis.
A Questionnaire survey was carried out to collect data about the level of exposure of the
employees to their workplace HIV/AIDS policy and to assess the functionality of the
workplace HIV/AIDS policies in the study organisations. The technique involved the use of
questionnaires developed by the researcher and administered to the respondents who
responded to the items in writing. The technique was appropriate because the respondents had
varying yet busy schedules; and it is cost effective and less time consuming.
Focussed group discussions (FGDs) were also used to explore group perceptions especially
with regard to the major challenges faced in the HV/AIDS policy implementation in the work
place. FGDs were used because they it allowed the researcher o obtain in-depth information
to supplement the responses yielded by questionnaires. A pair wise ranking matrix was used
for this purpose.
3.7 Research Procedure
This describes how the data was collected by using the instruments described above.
A letter of introduction was sought by the researcher from the school of postgraduate studies
to enable the researcher approach respondents. Both qualitative and quantitative data was
collected by the researcher using semi-structured and structured questionnaires. Qualitative
data was collected from the ten key informants using semi-structured and unstructured
questionnaires, while quantitative data from the forty other respondents was collected using
structured questionnaires. The data was collected by the researcher alone because of financial
constraints limiting the use of research assistants and in order for him to be able to capture
first hand other non verbal but observable communication cues given the sensitive nature of
the issue of HIV/AIDS. The raw data was checked for completeness, sorted coded and
analysed using Statistical Packages for Social Scientists (SPSS) in order for interpretation to
be made. Then the researcher concluded and accordingly made relevant recommendations.

30
3.8 Quality control
Validity and Reliability
The validity and reliability of the data collection tools was ensured by pre-testing them to
make sure they are easy to understand, have ability to capture the actual information and
generate the responses for which they have been designed and can replicate similar responses
whenever used under similar circumstances.
Eliminating extraneous variables was also done by the researcher as a quality control measure
against externalities such as noise, interruptions of other nature, interference from non
respondents and time. The researcher did this by carrying out the focus group discussions and
interviews in the conducive environment of a board room which was free from noise and
interference from non-respondents; and he allocated equal amount of time for each focus
group and key informant.
3.9 Data analysis
This section dealt with the organization, interpretation and presentation of collected data and
it postulates how the data was analyzed.
Being a predominantly qualitative study, thematic analysis was used to interpret and discuss
the findings and responses from the data gathered from respondents including the key
informants through focus group discussion and interview guides. A narrative was provided as
the basis for sound conclusion and recommendations by the researcher.
3.9.1 Statistical Data Analysis using Statistical Packages for Social Scientists (SPSS)
Data analysis and interpretation was done by the researcher using Statistical Packages for
Social Scientists (SPSS) in order to yield data that is accurate and simple to understand when
presented in percentile, graphical and chart forms.

31
CHAPTER FOUR
DATA PRESENTATION, ANALYSIS AND INTERPRETATION
4.0 Introduction
Chapter four explored the analyses and interpretation of the data collected through self-
administered questionnaires. The findings presented and discussed in this chapter are based
on the analysis of data derived from sixty research participants who are employees of
Reproductive Health Uganda and Uganda Telecom Limited who were randomly selected.
The objectives of the study were: to determine the level of exposure of the employees to their
workplace HIV/AIDS policy, to assess the functionality of the workplace HIV/AIDS policies
in private institutions in Uganda, to investigate the major challenges facing implementation
of workplace HIV/AIDS policies by private institutions and to suggest recommendations for
improving workplace HIV/AIDS policy implementation.
4.1 The Biographical Characteristics of the Respondents
4.1.1 Age bracket of respondents
Source: Questionnaire survey
Figure 4.1 shows the distribution of respondents according to age; where it is observed that
majority of the respondents are in the age group of 21-30 years accounting for 26 (43%), 14
(23%) were in the age group 31-40 years, 16 (27%) were in the age group 41-50 years
whereas the least number of respondents were above 50 years of age accounting for 4 (7%)
respondents. The results indicate that the respondents were relatively young people and are
Figure 4.1: Age of respondents
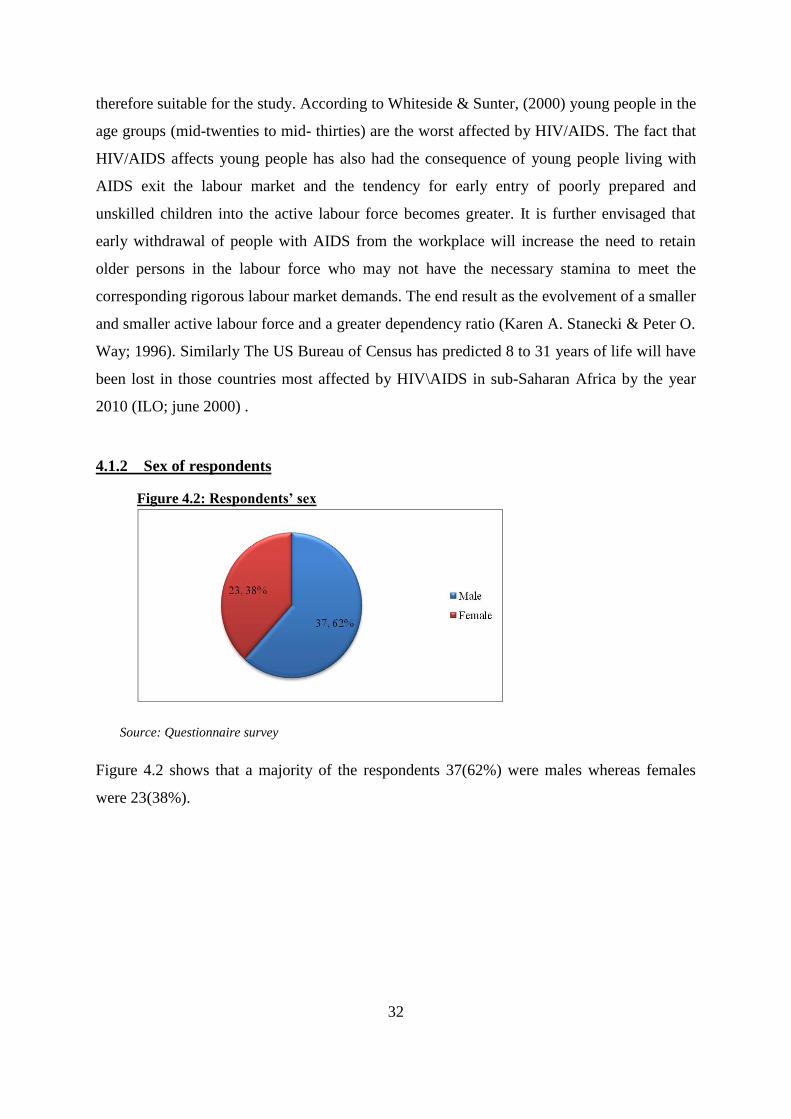
32
Figure 4.2: Respondents’ sex
therefore suitable for the study. According to Whiteside & Sunter, (2000) young people in the
age groups (mid-twenties to mid- thirties) are the worst affected by HIV/AIDS. The fact that
HIV/AIDS affects young people has also had the consequence of young people living with
AIDS exit the labour market and the tendency for early entry of poorly prepared and
unskilled children into the active labour force becomes greater. It is further envisaged that
early withdrawal of people with AIDS from the workplace will increase the need to retain
older persons in the labour force who may not have the necessary stamina to meet the
corresponding rigorous labour market demands. The end result as the evolvement of a smaller
and smaller active labour force and a greater dependency ratio (Karen A. Stanecki & Peter O.
Way; 1996). Similarly The US Bureau of Census has predicted 8 to 31 years of life will have
been lost in those countries most affected by HIV\AIDS in sub-Saharan Africa by the year
2010 (ILO; june 2000) .
4.1.2 Sex of respondents
Source: Questionnaire survey
Figure 4.2 shows that a majority of the respondents 37(62%) were males whereas females
were 23(38%).

33
Figure 4.3: Respondents’ Education level
4.1.3 Education level of respondents
Source: Questionnaire survey
Figure 4.3 shows a distribution of respondents according to education level; whereby a
majority of the respondents were bachelors degree holders accounting for 32(54%), diploma
and Advanced level qualifications had 11(18%) respondents each, whereas Respondents with
postgraduate training and Ordinary level both accounted for 3(5%) of the respondents. The
respondents of the study were therefore well educated and gave informed views about the
issues being investigated in the study.
4.1.4 Length of employment of respondents
Source: Questionnaire survey
Figure 4.4: Respondents’ length of employment

34
Figure 4.4 shows a distribution of respondents according to length of employment from
where it was observed that a majority of the respondents 28(46%) were employed for 1-3
years, 16 (27%) were employed for less than one year, 10 (17%) were employed for 3-5 years
whereas the least number of respondents 6 (10%) were employed for less than a year. The
results show that there is a variation in the length of employment amongst the respondents
with some respondents having worked in the organisations for a short period of time whereas
others worked for a long period. These results are an indicator that the views that they
presented were representative of the situation as it was at the time of the study and also how it
was in the past. The findings were therefore representative of a long period of time.
4.1.5 Job rank of respondents
Source: Questionnaire survey
Figure 4.5 shows a distribution of respondents according to job rank, where it was observed
that a majority of the respondents 42(70%) were officers/ facilitators, 11(18%) were
assistants whereas 7(12%) were managers. These results show that representative views were
got from all employee ranks right from management to junior staff. This was vital to the
study in that HIV/AIDS affects everyone in the work place irrespective of rank and therefore
the views from all categories of people in the workplace were needed for the study.
4.2 Level of exposure of the employees to the HIV/AIDS workplace policy
The first objective of this study was to establish the level of exposure of the employees to the
HIV/AIDS workplace policy in their respective organisations. The analysis for this objective
was presented under the themes of: familiarity with the work place HIV/AIDS policy,
familiarity of HIV/AIDS policy by sex and familiarity of HIV/AIDS policy by age.
Figure 4.5: Job rank of respondents

35
With reference to a 5 point likert scale, descriptive statistics were generated to examine the
level of exposure of employees to their workplace policy. The parameters in the likert scale
included very high extent, high extent, moderate extent, low extent and very low extent.
These parameters served to show the degree to which respondents were familiar with the item
in question.
4.2.1 Familiarity with the work place HIV/AIDS policy
Table 4.1: Familiarity to HIV/AIDS policy
Response Frequency Percent
Very High Extent 8 13.3
High Extent 14 23.3
Moderate Extent 14 23.3
Low Extent 15 25
Very Low Extent 9 15
Total 60 100.0
Mean 3.05
Std. Deviation 1.281
Source: Questionnaire survey
Respondents were asked to state the extent to which they are familiar with their workplace
HIV/AIDS policy. Table 4.1 shows that a majority of the respondents 15(25%) reported that
they are familiar with their workplace HIV/AIDS policy to a low extent whereas the least
number 8(13.3%) mentioned that they were aware of the HIV/AIDS policy to a very low
extent. A mean score of 3.05 implies that the respondents were moderately familiar with their
work place HIV/AIDS policy.
However, a standard deviation of 1.281 implies a wide variation in familiarity of HIV/AIDS
policy by the respondents. The implication of this is that whereas there were many
respondents whose awareness of the work place HIV/AIDS policy was high, there were also
many respondents whose awareness of the HIV/AIDS policy was low. These results are not
encouraging because the respondents have been in employment with their organizations for
quite a long time and should have been exposed to the policy in some way or another given
the fact that HIV/AIDS are of great concern in the workplace. This can be a consequence of

36
poor implementation of the HIV/AIDS work place policy. Furthermore, even those who may
be familiar with the policy may not take it very seriously as shown by a study conducted by
Chetty in 2006 which showed that despite the existence of a policy and formal commitment
to its values and objectives, practices that work against the spirit of the policy often continue
especially Stigma and discrimination.
Esu-Williams et al., (2005) recommends that it is necessary for any company to; once it has
implemented an HIV/AIDS workplace programme, embark on an evaluation process of that
intervention. The reason for this is to determine if the programme is addressing the issues that
it was intended to deal with.
4.2.2 Familiarity with the workplace HIV/AIDS Policy by Sex
Table 4.2 Sex and Familiarity with the workplace HIV/AIDS policy Cross tabulation
Familiarity with the workplace HIV/AIDS Policy Total
Very High
Extent
High
Extent
Moderate
Extent
Low
Extent
Very Low
Extent
Sex Male 5 9 5 11 7 37
Female 3 5 9 4 2 23
Total 8 14 14 15 9 60
Source: Questionnaire survey
A cross-tabulation was carried out to find out familiarity levels of employees with their
workplace HIV/AIDS policy among males and females. Table 4.2 shows that males mostly
reported to be familiar with the organization‟s HIV/AIDS policy to a low extent whereas
females mostly mentioned that they are familiar to a moderate extent. The results are an
indication that more work is needed to make both sexes familiar with the policy and with
more attention given to the males.

37
4.2.3 Familiarity with the workplace HIV/AIDS Policy by Age
Table 4.3: Age Bracket and Familiarity with workplace HIV/AIDS policy Cross
tabulation
Familiarity to HIV/AIDS policy Total
Very
High
Extent
High
Extent
Moderate
Extent
Low
Extent
Very Low
Extent
Age
Bracket
21-30years 5 3 7 6 5 26
31-40years 2 4 1 4 3 14
41-50years 1 6 6 3 0 16
50years+ 0 1 0 2 1 4
Total 8 14 14 15 9 60
Source: Questionnaire survey
A cross tabulation was carried out to find out familiarity levels of respondents with their
workplace HIV/AIDS policy among the age groups. Table 4.3 shows that the respondents in
the age group of 21 to 30 years mainly reported that they were familiar to their workplace
HIV/AIDS policy to a moderate extent, those in the age group of 31 to 40 years mentioned
that they were aware of the policy to a high extent and low extent accounting for 4
respondents each, the respondents in the age group between 41-50 years were familiar with
the policy to a higher extent whereas those in the age group 50 and above were familiar with
the policy to a lower extent. The results are an indication the awareness of the HIV/AIDS
policy is lower among the younger people and yet HIV/AIDS problem affects them the more.
4.3 The functionality of the workplace HIV/AIDS policies
The second objective of the study was to investigate the functionality of the work place
HIV/AIDS policies. The analysis for this objective was presented under the following
themes: Recognition of HIV/AIDS policy as a workplace issue, HIV/AIDs policy and the
principle of non discrimination, HIV/AIDS policy and the issue of a healthy work
environment, HIV/AIDS policy and encouragement of social dialogue on HIV/AIDS issues,
HIV/AIDS policy and supporting prevention initiatives on HIV/AIDS, HIV/AIDS policy and

38
staff care and support with regard to HIV/AIDS and HIV/AIDS policy and continuation of
employment relationship.
With reference to a 5 point Likert scale, descriptive statistics were generated to examine the
functionality of the workplace HIV/AIDS policies according to the perceptions of the
employees. The parameters in the Likert scale included strongly agree, agree, don‟t know,
disagree, and strongly disagree. These parameters served to show the degree to which
respondents agreed or disagreed with the item in question.
4.3.1 Recognition of HIV/AIDS as a workplace issue
Table 4.4: Perceptions of respondents on Recognition of HIV/AIDS as a workplace issue
Response Frequency Percent
Strongly Agree 18 30
Agree 27 45
Don‟t know 5 8.3
Disagree 6 10
Strongly Disagree 4 6.7
Total 60 100
Mean 2.18
Std. Deviation 1.172
Source: Questionnaire survey
Respondents were asked whether their companies recognize HIV/AIDS as a workplace issue.
Table 4.4 shows that majority of the respondents agreed that their organization recognizes
HIV/AIDS as a work place issue, whereas the least 4 (6.7%) strongly disagreed. A mean on
2.18 shows that a majority of the respondents agreed that their organization recognizes
HIV/AIDS as a work place issue. A standard deviation of 1.172 shows a small variation
among the perceptions of the respondents. This implies the respondents generally felt that
their workplace recognizes HIV/AIDS as a work place issue. The fact that HIV/AIDS is
recognised as a work place issue is in line with The International Labor Organization (ILO)
which provides a comprehensive framework which addresses how Persons Living with
HIV/AIDS should be handled at the workplace. It also has a policy document which guides
the design and development of workplace HIV/AIDS issues and spells out the salient issues
and how they are to be observed by employers.

39
Similarly, Stellenbosch University and the USAID Health Policy Initiative, (2008) suggests
that recognition of HIV/AIDS should be carried out in an organization through awareness
programmes as one of the key elements of a workplace HIV/AIDS program.
However, the creation of awareness programmes is a big challenge to orgainsations as
indicated by UNAIDS, (1998) which says that organisations face enormous challenges in
responding to HIV/AIDS through processes such as setting up comprehensive, sustainable
programmes, adopting relevant policies, obtaining management commitment, ensuring
confidentiality and non-discrimination, supporting staff who are living with HIV/AIDS,
dealing with attitudes of co-workers and sustaining involvement.
4.3.2 HIV/AIDs policy and the principle of non-discrimination
Table 4.5: Responses on organizations’ HIV/AIDS policy and the principle of non-
discrimination
Response Frequency Percent
Strongly Agree 29 48.3
Agree 17 28.3
Don‟t Know 4 6.7
Disagree 4 6.7
Strongly disagree 6 10
Total 60 100
Mean 2.02
Std. Deviation 1.321
Source: Questionnaire survey
Respondents were asked whether their organization‟s HIV/AIDS policy promotes the
principle of non-discrimination. Table 4.5 shows that majority of the respondents 29 (48.3)
strongly agreed that their organization‟s HIV/AIDS policy promotes the principle of non-
discrimination. A mean of 2.02 is indicative that a majority of the respondents agreed that
their organizations HIV/AIDS policy promotes the principle of non-discrimination. A
standard deviation of 1.321 shows a relatively large variation among the perceptions of the
respondents, implying that whereas respondents generally felt that their workplace
HIV/AIDS policy promotes the principle of non-discrimination, a number of them disagreed.

40
Kauffman and Lindauer (2004), mention that the issue of discrimination is an important
aspect in workplace HIV/AIDs policy because a climate of discrimination and lack of respect
for human rights leaves workers more vulnerable to infection and less able to cope with
AIDS because it makes it difficult for them to seek voluntary testing, counselling, treatment
or support; they will also not be in a position to take part in advocacy and prevention
campaigns. Moreover, individuals who suffer discrimination and lack of respect for their
human rights are both more vulnerable to becoming infected and less able to cope with the
burdens of HIV/AIDS (Kauffman and Lindauer 2004).
ILO‟s policy regarding personnel issues emphasises that employers should not engage in nor
permit any personnel policy or practice that discriminates against workers infected with or
affected by HIV/AIDS.
4.3.3 HIV/AIDS policy and the issue of a healthy work environment
Table 4.6: Responses on HIV/AIDS policy and the issue of a healthy work environment
Response Frequency Percent
Strongly agree 18 30
Agree 23 38.3
Don‟t know 6 10
Disagree 10 16.7
Strongly disagree 3 5
Total 60 100
Mean 2.28
Std. Deviation 1.209
Source: Questionnaire survey
Respondents were asked whether their organization‟s HIV/AIDS policy addresses the issue
of a healthy work environment. Table 4.6 shows that Majority of the respondents 23 (38.3)
agreed, whereas the least number of respondents 3 (5%) strongly disagreed. A mean of 2.28
shows that a majority of the respondents agreed that their organization‟s HIV/AIDS policy
addresses the issue of a healthy work environment. A standard deviation of 1.209 shows a
relatively large variation among the perceptions of the respondents, implying that whereas

41
respondents generally felt that their workplace HIV/AIDS policy addresses the issue of a
healthy work environment, a number of them actually disagreed.
These findings show that the organisations‟ policies are in line with ILO‟s code of practice on
HIV/AIDS and the World of Work (2001) which provides that employers should ensure a
safe and healthy working environment, including the application of Universal Precautions
and measures such as the provision and maintenance of protective equipment and first aid.
The policy further provides that to support behavioural change by individuals, employers
should also make available, where appropriate, male and female condoms, and counselling,
care, support and referral services. Where size and cost considerations make these difficult,
employers and/or their organizations should seek support from government and other relevant
institutions
4.3.4 HIV/AIDS policy and encouragement of social dialogue on HIV/AIDS issues
Table 4.7: Responses on HIV/AIDS policy and encouragement of social dialogue on HIV/AIDS
Responses Frequency Percent
Strongly agree 9 15
Agree 21 35
Dont know 6 10
Disagree 14 23.3
Strongly disagree 10 16.7
Total 60 100
Mean 2.92
Std. Deviation 1.369
Source: Questionnaire survey
Respondents were asked whether their organization‟s HIV/AIDS policy encourages social
dialogue on HIV/AIDS issues among employees. Table 4.7 shows that Majority of the
respondents 21 (35%) agreed, while few respondents 6 (10%) did not know. A mean of 2.92
shows that a majority of the respondents were not sure if their organizations HIV/AIDS
policy encourages social dialogue on HIV/AIDS issues among employees. A standard
deviation of 1.369 shows a relatively large variation among the perceptions of the
respondents. The responses were evenly distributed across all perceptions.

42
The National Plan of Action for Implementing the National Policy on HIV/AIDS and the
World of Work, (2010) provides that private organizations have the responsibility of
promoting social dialogue and advocacy for inclusion of workplace HIV/AIDS programmes,
ensuring employers‟ involvement and participation in the HIV/AIDS campaign.
Apart from Social dialogue, other activities should be promoted and carried out such as
impact assessment of HIV/AIDS on an organisation, HIV and AIDS awareness programmes,
voluntary counselling and testing for HIV, HIV and AIDS education and training, condom
distribution, encouraging health treatment for STIs and TB, universal infection and control
procedures, creating an open and accepting environment, wellness programmes for
employees affected by HIV and AIDS, provision of anti-retroviral treatment or referral to
relevant service providers, education and awareness about anti-retroviral treatment and other
treatment literacy programmes, counselling and other forms of social support for HIV-
positive employees, reasonable accommodation for HIV-positive employees, strategies to
address direct and indirect costs and other practical implications of HIV and AIDS
monitoring, evaluation and review of the programme.
4.3.5 HIV/AIDS policy and strengthening confidentiality
Table 4.8: Responses on HIV/AIDS policy and strengthening confidentiality
Response Frequency Percent
Strongly Agree 18 30
Agree 24 40
Don‟t know 7 11.7
Disagree 8 13.3
Strongly disagree 3 5
Total 60 100
Mean 2.32
Std. Deviation 1.546
Source: Questionnaire survey
Respondents were asked whether they felt that their organization‟s HIV/AIDS policy
emphasizes the need to strengthen confidentiality. Table 4.8 shows that Majority of the
respondents 24 (40%) agreed whereas the lowest number of respondents 3 (5%) strongly
disagreed. A mean of 2.32 shows that a majority of the respondents agreed that their

43
organization‟s HIV policy emphasizes the need to strengthen confidentiality. A standard
deviation of 1.546 shows a relatively large variation among the perceptions of the
respondents. This implies that whereas some respondents agreed that their organization‟s
HIV policy emphasizes the need to strengthen confidentiality others felt the contrary. These
findings are in line with the World of Work (2001),which recommends that HIV/AIDS-
related information of workers should be kept strictly confidential and kept only on medical
files, whereby access to information complies with the Occupational Health Services
Recommendation, 1985 (No. 171), and national laws and practices. Access to such
information should be strictly limited to medical personnel and such information may only be
disclosed if legally required or with the consent of the person concerned.
4.3.6 HIV/AIDS policy and supporting prevention initiatives on HIV/AIDS
Table 4.9: Responses on HIV/AIDS policy and supporting prevention initiatives on HIV/AIDS
Response Frequency Percent
Strongly agree 22 36.7
Agree 15 25
Don‟t know 7 11.7
Disagree 11 18.3
Strongly disagree 5 8.3
Total 60 100
Mean 2.37
Std. Deviation 1.365
Source: Questionnaire survey
Respondents were asked whether they felt that their organizations‟ HIV/AIDS policy
supports prevention initiatives on HIV/AIDS at their work place. Table 4.9 shows that
Majority of the respondents 22 (36.7%) strongly agreed whereas the least number of
respondents 5(8.3%) strongly disagreed. A mean of 2.37 shows that a majority of the
respondents agreed that their organisation's HIV policy supports prevention initiatives on
HIV/AIDS at the work Place. A standard deviation of 1.365 shows a relatively large variation
among the perceptions of the respondents. This implies that whereas some respondents
agreed that their organisation's HIV policy supports prevention initiatives on HIV/AIDS at
the work Place a reasonable number of others felt the contrary. The 2011 Uganda AIDS

44
Indicator Survey (UAIS) identifies a continued need for individual behaviour change, and
scale-up of evidence-based prevention interventions such as prevention of mother-to-child
transmission services and safe male circumcision, as well as increased treatment coverage for
people living with HIV. Interventions should be targeted to those most-at-risk populations
and must pay particular attention to those regions and districts most heavily impacted by the
epidemic. Similarly prevention interventions should be carried out in workplaces as
recommended by the ILO Code of Practice on HIV/AIDS and the World of Work (2001)
provides that Workers and their organizations should endeavour to include provisions on
HIV/AIDS protection and prevention in national, sectoral and workplace/enterprise
agreements.
4.3.7 HIV/AIDS policy and staff care and support with regard to HIV/AIDS
Table 4.10: Responses on HIV/AIDS policy and staff care and support
Response Frequency Percent
Strongly agree 6 10
Agree 20 33.3
Don‟t know 9 15
Disagree 10 16.7
Strongly Disagree 15 25
Total 60 100
Mean 3.13
Std. Deviation 1.384
Source: Questionnaire survey
Respondents were asked whether they felt that their organization‟s HIV/AIDS policy deals
with staff care and support with regard to HIV/AIDS. Table 4.10 shows that Majority of the
respondents 20 (33.3%) agreed whereas the least number of respondents 6(10%) strongly
agreed. However, a mean of 3.13 shows that there was general uncertainty amongst the
respondents as regards to their perceptions on whether HIV/AIDS policy deals with staff care
and support with regard to HIV/AIDS. A standard deviation of 1.365 shows a relatively large
variation among the perceptions of the respondents. One of the five main initiatives
mentioned by the International Organisation of Employers (2002) that an organisation can

45
take to respond to HIV/AIDS in the workplace is providing care and support in the
workplace.
A good HIV and AIDS workplace programme is one that is action-oriented and one that an
organisation will implement in order to prevent new HIV infections, provide care and support
for employees who are infected or affected by HIV or AIDS, manage the impact of the
epidemic on the organisation and also outlines how all the different principles within the
policy will be translated into practice at the workplace.
4.3.8 HIV/AIDS policy and continuation of employment relationship
Table 4.11: Responses on HIV/AIDS policy and continuation of employment relationship
Responses Frequency Percent
Strongly agree 27 45.0
Agree 9 15.0
Don‟t know 5 8.3
Disagree 8 13.3
Strongly disagree 11 18.3
Total 60 100.0
Mean 2.45
Std. Deviation 1.599
Source: Questionnaire survey
Respondents were asked whether they felt that their organization‟s HIV/AIDS addresses the
continuation of employment relationship. Table 4.11 shows that Majority of the respondents
27(45%) strongly agreed whereas the least number of respondents 5(8.3%) did not know. A
mean of 2.45 shows that there was general agreement amongst the respondents as regards to
their perceptions on whether organization‟s HIV/AIDS addresses the continuation of
employment relationship. A standard deviation of 1.599 shows a relatively large variation
among the perceptions of the respondents.
According to the Kenya public sector workplace policy on HIV and AIDS, (2005) HIV
infection is not a cause for termination of employment. Persons with HIV related illnesses
should be allowed to work for as long as medically fit in available appropriate work.

46
4.4 Challenges faced in implementation of HIV/AIDS policy
The third objective of the study was to establish the most pressing problem faced in the
implementation of the work place policies by private organizations. A focused group
discussion was carried out with the respondents and a pair wise ranking matrix was used to
establish the challenges faced most in the implementation of the HIV/AIDS polices in the two
organizations. Pair wise ranking is a method in which each item on a list is compared in a
systematic way with each other. To construct this table, each problem was compared in turn
with each of the other problems.
Table 4.12: Pair wise matrix ranking of challenges faced in implementation of HIV/AIDS policy
Problem Problem number Score Rank
1 2 3 4 5 6 7 8 9 10
1. Lack of management commitment 2 3 4 5 6 7 8 9 10 0 10
2. Weak emphasis on confidentiality and non-
discrimination
2 4 2 2 2 8 2 2 7 3
3 Lack of support for staff with HIV/AIDS 4 3 3 3 8 3 3 6 4
4 Negative attitudes of co-workers and lack
of involvement in HIV/AIDS programs
4 4 4 8 4 4 8 2
5 Gender inequality in our organisation 5 5 8 9 10 3 7
6 The work environment is not socially well
maintained
6 8 9 10 2 8
7 Little money allocated for HIV/AIDS work 8 9 10 1 9
8 Stigma and discrimination against
employees who are HIV positive.
8 8 9 1
9 Social dialogue on HIV/AIDS issues is hard
to foster at work.
10 4 6
10 Prevention initiatives are quite costly for the
organisation in terms of time and money
5 5
Source: Focus group discussion
Table 4.12 shows a pair wise ranking of the most pressing challenges faced in the
implementation of the HIV/AIDS policies in the organizations. It can be seen that the highest
ranked problem is Stigma and discrimination of employees who are HIV/AIDS positive had a
score of 9 and was thus ranked number 1 by the respondents. These findings are in line with
the Academy for Educational Development, (2004) that found that among the greatest

47
challenges in addressing HIV/AIDS are stigma and discrimination which often result from
fear caused by myths, misinformation, and a lack of knowledge about how HIV is and is not
transmitted. The negative effects of workplace stigma and discrimination can be substantial,
both to the business and to workers themselves.
The second ranked challenge was negative attitudes of workers and lack of involvement in
the implementation of the HIV/AIDS policies with a score of 8. These findings are consistent
with UNAIDS, (1998) that says that organisations face enormous challenges in responding to
HIV/AIDS such as dealing with attitudes of co-workers and sustaining involvement.
Lack of confidentiality and non discrimination also ranked highly at number 3 with a score of
7. UNAIDS, (1998) further adds that organisations face enormous challenges ensuring
confidentiality and non-discrimination in the workplace.
Other problems included lack of support for HIV/AIDs workers ranked at number 4 with a
score of 6, Prevention initiatives being quite costly for the organisation in terms of time and
money rank 5 with a score of 5, Social dialogue on HIV/AIDS being hard to foster at work
,rank 6 with a score of 4, Gender inequality in the organization rank 7 with a score of 3, the
work environment not socially well maintained rank 8 with a score of 2, Little money
allocated for HIV/AIDS work was at rank 9 with a score of 1 whereas lack of commitment to
tackle the HIV/AIDS issue ranking last with no score.
These results are consistent with The Interagency Coalition on AIDS and Development
(2004), which gives a general outline of some of the challenges facing the development and
implementation of Workplace HIV/AIDS policies as; the level of staff participation required
in terms of research and policy development, implementation, communication, monitoring
and adjustments; perceived costs involved in training; the duty to accommodate altered work
schedules; legal input and associated costs; possible costs for consultant to research and
develop policy; regular review necessary; different codes and standards between
organizations, union and non-union requirements; considerations for parity; stigma and/or
discrimination; and lack of human and financial resources as well as attitude issues around
willingness to develop such a policy.

48
CHAPTER FIVE
SUMMARY, CONCLUSION AND RECOMMENDATIONS
5.0 Introduction
The purpose of the study was to assess the implementation of HIV/AIDS policies in private
institutions in Uganda with Reproductive Health Uganda, and Uganda Telecom Limited as
case studies. This final chapter comprises a summary, conclusions and recommendations
basing on the findings of the study.
5.1 Summary
The main findings are summarised in terms of the stated objectives and sub-sections of the
questionnaire.
5.1.1 Level of exposure of employees to their HIV/AIDS workplace policy
The first objective of this study was to establish the level of exposure of employees to the
workplace HIV/AIDS policy in their respective organizations.
The majority of respondents reported a low extent of familiarity with their workplace
HIV/AIDS policy, whereas the least reported that they were fully familiar with the policy. A
mean score of 3.05 showed that the respondents were moderately familiar with their work
place HIV/AIDS policy. However, a standard deviation of 1.281 showed a wide variation in
familiarity with the workplace HIV/AIDS policy by the respondents implying that whereas
the respondents were aware about their work place HIV/AIDS policy, the level of awareness
in a number of them was low.
Males mostly reported a low extent of familiarity with their organizations HIV/AIDS policy,
whereas females reported familiarity to a moderate extent.
In terms of awareness and age brackets, the younger people appeared to be less aware of the
existence of their workplace HIV/AIDS policy as compared to the older people.

49
5.1.2 The functionality of the workplace HIV/AIDS policies
The second objective of the study was to investigate the functionality of the work place
HIV/AIDS policies.
A mean of 2.18 and a standard deviation of 1.172 showed that majority of the respondents
agreed that their organization‟s policy recognizes HIV/AIDS as a work place issue.
With a mean of 2.02, the study also found that majority of the respondents agreed that their
organization‟s HIV/AIDS policy promotes the principle of non-discrimination. However with
a standard deviation of 1.321, there was a relatively large variation among the perceptions of
the respondents indicating that a good number of respondents disagreed.
The majority of the respondents agreed that their organization‟s HIV/AIDS policy addresses
the issue of a healthy work environment. This was represented by the mean score of 2.28.
But, whereas respondents generally felt that their workplace HIV/AIDS policy addresses the
issue of a healthy work environment, a relatively large variation in their perception
represented by a standard deviation of 1.209 was also reported.
A mean on 2.92 showed that majority of the respondents were not sure if their organization‟s
HIV/AIDS policy encourages social dialogue on HIV/AIDS issues among employees. With a
standard deviation of 1.369, a relatively large variation among the perceptions of the
respondents is seen; implying that the responses were evenly distributed on all perceptions.
A mean of 2.32 showed that majority of the respondents agreed that their organization‟s HIV
policy emphasizes the need to strengthen confidentiality. However, a standard deviation of
1.546 shows a relatively large variation among the perceptions of the respondents. This
implies that whereas some respondents agreed that their organization‟s HIV policy
emphasizes the need to strengthen confidentiality others felt the contrary.
A mean of 2.37 showed that a majority of the respondents agreed that their organisation's
HIV/AIDS policy supports prevention initiatives on HIV/AIDS at the workplace. However, a
standard deviation of 1.365 shows a relatively large variation among the perceptions of the
respondents. This implies that whereas some respondents agreed that their organisation's
HIV/AIDS policy supports prevention initiatives on HIV/AIDS at the workplace, a
reasonable number of others felt otherwise.

50
A mean of 3.13 showed that there was general uncertainty amongst the respondents on how
they felt their workplace HIV/AIDS policy addresses staff care and support with regard to
HIV/AIDS. However, a standard deviation of 1.365 shows a relatively large variation among
the perceptions of the respondents implying an even distribution of those who agreed and
disagreed that it is well addressed.
A mean of 2.45 shows that there was general agreement amongst the respondents as regards
their perceptions on whether their organization‟s HIV/AIDS policy addresses the
continuation of employment relationship. The standard deviation of 1.599 shows a relatively
large variation among the perceptions of the respondents implying that a good number of
respondents actually disagreed.
5.1.3 Challenges faced in implementation of HIV/AIDS policy
The third objective of the study was to establish the most pressing problem faced in the
implementation of the workplace policies by private organizations.
A pair wise ranking of the most pressing problems being faced in the implementation of the
HIV/AIDS policies of the organizations showed that the highest ranked problems were
stigma and discrimination of people with HIV/AIDS, negative attitudes of workers towards
employees living with HIV/AIDS; lack of involvement by employees in the implementation
of their workplace HIV/AIDS policies and Lack of confidentiality and non-discrimination in
addressing HIV/AIDS among employees.
Other problems included lack of support for HIV/AIDs positive employees, prevention
initiatives being quite costly for the organisation in terms of time and money, social dialogue
on HIV/AIDS being hard to foster at the workplace, gender inequality in the organization, the
work environment not socially well maintained, little money allocated for HIV/AIDS issues
and lack of commitment by management to tackle the issue of HIV/AIDS at work.
5.2 Conclusion
The purpose of the study was to assess the implementation of HIV/AIDS policies in private
institutions in Uganda. This was done by establishing the level of exposure of employees to
their workplace HIV/AIDS policies, the functionality of workplace HIV/AIDS policies and
the challenges faced in implementation of the workplace HIV/AIDS policies.

51
The study revealed that though majority of the respondents were familiar with their
organisation‟s HIV/AIDS policies, there was a disparity in familiarity in terms of gender and
age with women and the older people more familiar.
The study also revealed that most private organizations‟ workplace HIV/AIDS policies are
functional to a small extent; but some issues in the policies are not well addressed.
Finally, the study reveals that the effective implementation of workplace HIV/AIDS policies
in private organisations is hampered by a range of challenges.
It can therefore be concluded that despite the fact that private organisations strive to
implement their workplace HIV/AIDS policies, the capacity to meet their objectives is
influenced by gender, age, management of the implementation of those policies and the
unique challenges that arise from the implementation of such a unique policy.
5.3 Recommendations
It is recommended that the employees especially the males and the young should be
encouraged to orient themselves with their workplace HIV/AIDS policy and that they should
be encouraged to become familiar with its contents.
It is also recommended that private organisations should design well formulated programmes
and include the various HIV/AIDS policy instruments so as to ensure that the HIV/AIDS
policies are well implemented.
All the challenges that inhibit the success of the implementation of these policies should be
identified and addressed.
Private organisations should allocate adequate funding for their workplace HIV/AIDS policy
implementation.
References
ACADEMY FOR EDUCATIONAL DEVELOPMENT. (2004). A Workplace Guide for Managers
and Labor Leaders: HIV/AIDS Policies and Programs. Publisher, place of publication
do this for all references
ALAGARI, P., SUMMERS T, KATES J. Trends in U.S. Spending on HIV/AIDS. Henry J. Kaiser
Family Foundation. July 2002. www.kff.org.

52
ALAGARI, P., SUMMERS T, KATES, J. Federal HIV/AIDS Spending: A Budget Chartbook – Fiscal
Year 2002.
ATTIA, S. et al., (2009). Sexual Transmission of HIV according to viral load and antiretroviral
therapy: systematic review and meta – analysis. AIDS, 23:1397-1404.
BENDELL, J. 2003. Waking up to risk: corporate responses to HIV/AIDS in the workplace. Geneva:
UNRISD and UNAIDS.
BOLTON-MOORE, C, et al. (2007). Clinical outcomes and CD4 cell response in children receiving
antiretroviral therapy at primary health care facilities in Zambia. Journal of the
American Medical Association, 298(16):1888-1899.
BONG, C. et al. (2007). Risk factors for early mortality in children on adult fixed-dose combination
antiretroviral therapy in a central hospital in Malawi. AIDS, 2:1905-1810.
BOULLE, A, et al. (2008). Antiretroviral therapy and early mortality in South Africa. Bulletin of the
World Health Organization, 86:678-687.
BUSSMANN H et al. (2008). Five-year outcomes of initial patients treated in Botswana’s national
antiretroviral treatment program. AIDS, 22(17):2303-2311.
CENTERS FOR DISEASE CONTROL AND PREVENTION (2008). HIV prevalence estimates –
United States, 2006. Morbidity and Mortality Weekly Report, 57(39): 1073-1076.
COUNCIL ON FOUNDATIONS. “Trends in Grandmaking”. Corporate Update, Winter 2003, page
6.
DESMOND, C., KARAM, L. & STEINBERG, M. (2003). Still everybody’s business: the
enlightening truth about AIDS. Bellville: Metropolitan Group.

53
DEVELOPMENT MANAGEMENT ASSOCIATES (2002). “Situation Analysis of HIV/AIDS in
Botswana”; a report prepared for the Government of Botswana, July 2002.
ESU-WILLIAMS.2005. Strengthening workplace HIV/AIDS programs: The Eskom experience in
South Africa. Johannesburg: Population Council/Horizons.
GRAY, D. E. (2004). Doing Research in the Real World. SAGE.
GRAY, R.H, LI, X., KIGOZI, G., SERWADDA, D., NALUGODA, F., WATYA, S., REYNOLDS,
S.J, WAWER. M. (2007). The impact of male circumcision on HIV incidence and cost
per infection prevented: a stochastic simulation model from Rakai, Uganda. AIDS. Apr
23;21(7):845-50.
HALL, HI. et al. (2008). Estimation of HIV incidence in the United States. Journal of the American
Medical Association, 300(5):520-529.
HALLETT, T., et al. (2008). Estimating incidence from prevalence in generalized HIV epidemics:
methods and validation. PLoS Medicine, 5(4):e80.
HALLETT, T.B. et al, (in press). Estimates of HIV incidence from household-based prevalence
surveys in sub-Saharan Africa. AIDS.
HENRY, J. KAISER FAMILY FOUNDATION. September 2003.
www.kff.org/content/2003/6076/6076v2.pdf.
HERBS, A.J. et al. (2009). Adult mortality and antiretroviral treatment roll-out in rural KwaZulu-
Natal, South Africa. Bulletin of the World Health Organization, 87:754-762.
ILO (2000). “HIV/AIDS: A Threat to Decent Work, Productivity and Development” Mimeo, (A
discussion paper for high-level meeting on HIV/AIDS and the World of Work), Geneva,
June 2000.
ILO (2000). HIV/AIDS in Africa: The Impact on the World of Work, Addis Ababa, December 2000.
INTERNATIONAL LABOUR ORGANIZATION, 2001. An ILO code of practice on HIV / AIDS and
the world of work. Geneva: ILO.
JAHN, A. et al., (2008). Population – level effect of HIV on adult mortality and early evidence of
reversal after introduction of antiretroviral therapy in Malawi. Lancet, 371:1603-1611.

54
JOINT UNITED NATIONS PROGRAMME ON HIV/AIDS (UNAIDS) AND THE
INTERNATIONAL ORGANISATION OF EMPLOYERS (IOE). (2002). Employers’
Handbook on HIV/AIDS – A Guide for Action.
JOINT UNITED NATIONS PROGRAMME ON HIV/AIDS (UNAIDS). Press release:
Implementing the Declaration of Commitment on HIV/AIDS. 22 September 2003.
www.unaids.org/html/pub/Media/Pressreleases01/UNGASS_Pressrelease_2003_en_doc.
htm.
KAJUBI, P., KAMYA, M.R., RAYMOND, H.F., et al. (2008), Gay and Bisexual Men in Kampala,
Uganda, AIDS Behaviour 12:492-504.
KAREN A. STANECKI & PETER O.(1996). The Demographic Impacts of HIV/AIDS Reprinted from
World Population Profile: 1996, U.S. Bureau of the Census, Washington, D.C. June
1996.
KAUFFMAN, K.D. & LINDAUER, D.L. (2004). AIDS and South Africa: the social expression of a
pandemic. New York: Palgrave Macmillan.
KIRUNGI, W.L., MUSINGUZI, J., MADRAA, E., MULUMBA, N., CALLEJJA, T., GHYS, P.,
BESSINGER, R. (2006). Trends in antenatal HIV prevalence in urban Uganda
associated with uptake of preventive sexual behaviour. Sex Transm Infect. 2006 Apr; 82
Suppl 1:i36-41.
KYADDONDO, D., NAKKAZI, P. AND SIU, G. (2005). Causes and perceptions about child
marriages in Maddu sub county Mpigi District, Kampala: Child Health and
Development Center Makerere University.
LIMA, V.C. et al. (2008). Expanded access to highly active antiretroviral therapy: a potentially
powerful strategy to curb the growth of the HIV epidemic. Journal of Infectious
Diseases, 198:59-67.
LOEWENSON, R. & KERKHOVEN, R. (1996); The Socio-Economic Impact of AIDS: Issues and
Options in Zimbabwe, SafAIDS, Colon Press, May 1996.
MAPHOSA, F. (2003). HIV/AIDS at the workplace: A study of corporate responses to the HIV/AIDS
pandemic. CODESRIA Bulletin, 2, 56-58.
MERMIN, J. et al. (2008). Mortality in HIV-infected Ugandan adults receiving antiretroviral
treatment and survival of their HIV-uninfected children: a prospective cohort study.
Lancet, 371:752-759.

55
MoH. (2009). HIV/AIDS Epidemiological Surveillance Report, GoU/MoH/ACP, Kampala, Uganda.
MUSICCO, M. et al. (1994). Antiretroviral treatment of men infected with Human Immunodeficiency
Virus type 1 reduces the incidence of heterosexual transmission. Archives of Internal
Medicine, 154(17):1971-1976.
NATIONAL COMMITTEE FOR RESPONSIVE PHILANTHROPY. The NCRP Quarterly, Summer
2003. p7.
NATIONAL ORGANIZATIONS RESPONDING to AIDS (NORA). Fiscal Year 2003 HIV/AIDS
Appropriations Recommendations. May 2003.
NEEMA, S., SSEKIWANUKA, J. and SSEDYABULE D. (2000), Children living in difficult
circumstances: vulnerability and coping mechanisms of child-headed households in
Rakai, Uganda. Kampala, Straight Talk Foundation.
ODIIT, M. (2008). A Review of the sources of Incident HIV Infections in Uganda, Modes of
Transmission Study: Uganda, GoU/UNAIDS/UAC Oct.2008.
ONEN, D. and OSO, Y. W. (2005). A concise approach to research methodology: (1st ed.), Options
printers and publishers: Kisumu.
OU, C et al., (2007). Identification of HIV-1 infected infants and young children using real-time RT
PCR and dried blood sports from Uganda and Cameroon. Journal of Virological
Methods, 144:109-144.
OUNDO G. and SIU, G. (2006). Sexual and Reproductive Behavior Among People Living With
HIV/AIDS (PHA) In Busia District, A research report, funded by Child Health and
Development Centre.
PAGE, J, LOUW, S, PAKKIRI, D & JACOBS, M. (2006). Working with HIV/AIDS. Cape Town:
Juta And Company LTD.
PHARAOH, R. & SCHONTEICH, M. (2006). AIDS, Security and governance in Southern Africa:
exploring impact. Johannesburg: Institute for Security Studies.
PSI (2006), Uganda: Understanding Current Attitudes to Condoms and Pre- Testing Messages in
Uganda, A study commissioned by PSI/Uganda Research Division for MoH, conducted
by Asingwire, N., S. Kyomuhendo, J. Kiwanuka.

56
RAU, B, ROBERTS, M & EMERY, A. 2002. Workplace HIV/AIDS programs. Arlington: Family
Health International.
SEHGAL, JAG M. (1999). The Labour Implications of HIV/AIDS and the World of Work, published
by ILO, Geneva, November 1999.
SERWADDA D, MUGERWA, R.D., SEWANKAMBO, N.K., LWEGABA, A., CARSWELL, J.W.,
KIRYA, G.B. (1985), Slim disease: a new disease in Uganda and its association with
HTLV-III infection, Lancet; 2:849-852.
SHISANA, O. et al. (2009). South African National HIV prevalence, incidence, behavior and
communications survey 2008: a turning tide among teenagers? Cape Town, South
Africa, HSRC Press.
Smart, R. (2004). HIV/AIDS Guide for the Mining Sector - A Resource for Developing Stakeholder
Competency and Compliance in Mining Communities in Southern Africa.
STELLENBOSCH UNIVERSITY and the USAID HEALTH POLICY INITIATIVE. (2008).
Developing an HIV and AIDS Policy: Content, Process, Challenges and Implementation.
STOVER, J. & BOLLINGER, L. (2000). “The Economic Impact of AIDS”, the Policy Project.
Quoted in UNAIDS/ Global Business Council on HIV and AIDS; The Business Response
to HIV/AIDS: Impact and Lessons Learned, Geneva and London, 2000.
THE NATIONAL ALLIANCE OF STATE AND TERRITORIAL AIDS DIRECTORS (NASTAD),
NASTAD 2003 Policy Priorities, June 2003.
www.nastad.org/documents/public/Public/Policy/200364NASTAD2003PolicyPriorities.
pdf.
UNAIDS (2007). Practical guidelines for intensifying HIV prevention. Geneva, UNAIDS.
UNAIDS (2008). Report on the global AIDS epidemic. Geneva, UNAIDS.
UNAIDS (2009). Joint action for results: UNAIDS outcome framework 2009-2011. Geneva.
UNAIDS.
UNAIDS. (1998). HIV/AIDS and the workplace: forging innovative business responses. Geneva.
UNAIDS.
UNAIDS. 2004. Sub-Saharan Africa fact sheet. Geneva: UNAIDS.
UNAIDS. Fact Sheet 2002: The Impact of HIV/AIDS. Geneva. UNAIDS.

57
UNAIDS. Fact sheet: Meeting the need: June 2003. At www.unaids.org/fact_sheets . Geneva.
UNAIDS.
UNAIDS. Report on the State of HIV/AIDS Financing: Programme Coordinating Board, 14th
Meeting UNAIDS/PCB (14)/03. Conference Paper 2a 25 June 2003. www.unaids.org,
www.businessfightsaids.org. and www.hivatwork.org. Geneva. UNAIDS.
UNDP (2001). “HIV/AIDS: Implications for Poverty Reduction”, (Policy Paper), June 2001, p 10;
and ILO; “HIV/AIDS: A Threat to Decent Work, Productivity and Development”
Mimeo, (A discussion paper for high-level meeting on HIV/AIDS and the World of
Work), Geneva, June 2000, p 21.
VIOLARI, A. et al. (2008). Early antiretroviral therapy and mortality among HIV-infected infants.
New England Journal of Medicine, 359:2233-2244.
WHITESIDE, A. & SUNTER, C. (2000). AIDS: the challenge for South Africa. Cape Town: Human
& Tafelberg.
WILLIAMS, B. et al. (2001). Estimating HIV incidence rates from age prevalence data in epidemic
situations. Statistics in Medicine, 20(13):2003-2016.
WORLD HEALTH ORGANIZATION (2008). World health statistics 2008. Geneva, World Health
Organization.
WORLD HEALTH ORGANIZATION, UNITED NATIONS CHILDREN‟S FUND, UNAIDS
(2009). Universal access: scaling up.

58
Appendix : Questionnaire
Serial No:
Introduction:
My name is Paul OLOYA, a student of M.A Development Studies at Uganda Martyrs
University, Nkozi. As a course requirement, I am undertaking a study titled “The Challenges
Facing Organizations in Implementing Workplace HIV/AIDS Policies: A Case Study of
Uganda Telecom Limited and Reproductive Health Uganda”. You have been selected as a
respondent to participate in this study. This study is voluntary and purely for academic
purposes. Respondents‟ identities and responses shall be kept confidential. I therefore request
you to spare a few minutes and respond to these questions. Please respond according to the
instructions given, and kindly respond to all questions.
Section A: BIO-DATA (INSTRUCTION: For 1-5, Tick against the response that best
applies to you)
1. Age Bracket:
(a) 21-30yrs:……… (b) 31-40yrs:……..
(c) 41-50yrs:……… (d) 51yrs ++:……..
2. Sex: (a) Male: ……….. (b) Female: ………..
3. Job Rank:
a) Assistant Officer: ……………………..
b) Officer/Supervisor: ……………………
c) Manager/Head of Department: ……….
4. Length of employment in this Organization:
(a) Less than 1 yr ……… (b) 1-3yrs………

59
(c) 3-5yrs ……… (d) More than 5yrs:………
5. Highest level of Education: (a) O‟ Level:…………
(b) A‟ Level:…………. (c) Diploma:…………..
(d) Bachelors:………… (e) Postgraduate:.……..
Section B: level of exposure of the employees to the HIV/AIDS workplace policy.
How strongly do you agree or disagree with the following statements about the HIV/AIDS
policy of your organization? (Tick in the box below the number which best represents your
view using the following key: (Strongly Agree [1], Agree [2], Don’t Know [3], Disagree
[4], Strongly Disagree[5])
Statement
1
2
3
4
5
a) My organization‟s HIV Policy recognizes HIV/AIDS as a
workplace issue
b) Promotes the principle of non-discrimination
c) Takes into account gender equality at the workplace
d) Addresses the issue of a healthy work environment
e) Encourages social dialogue on HIV/AIDS issues among
employees
f) Discourages screening for purposes of exclusion from work or
work processes
g) Emphasizes the need to strengthen confidentiality
h) Handles the issue of continuation of employment relationship
i) Supports prevention initiatives on HIV/AIDS at the workplace
j) Deals with care and support with regard to HIV/AIDS
Section C: Functionality of the HIV/AIDS Policy of the Organization

60
How strongly do you agree or disagree with the following statements about the functionality
of the HIV/AIDS policy of your organization? (Tick in the box below the number which best
represents your view using the following key: (Strongly Agree [1], Agree [2], Don’t Know
[3], Disagree [4], Strongly Disagree[5])
Statement 1
2
3
4
5
a) HIV/AIDS is recognized as a workplace issue
b) HIV positive people are not discriminated against at my workplace
c) Gender equality is encouraged in our organization
d) The issue of a healthy work environment is addressed in our
organization
e) Social dialogue on HIV/AIDS issues takes place in our
organization
f) Workers are not screened for purposes of exclusion from work or
work processes
g) Workers HIV status is kept secret and not disclosed openly without
their permission
h) Handles the issue of continuation of employment relationship
i) Our organization is actively involved in prevention of HIV/AIDS
at the workplace
j) Care and support is offered by our organization with regard to
HIV/AIDS
Section D: Challenges Facing Implementation of Workplace HIV/AIDS Policies
How strongly do you agree or disagree with the following statements about the challenges
faced by your organization in the implementation the HIV/AIDS policy? (Tick in the box
below the number which best represents your view using the following key: (Strongly Agree
[1], Agree [2], Don’t Know [3], Disagree [4], Strongly Disagree [5]).
Statement
1
2
3
4
5
a) HIV/AIDS is not recognized as a workplace issue

61
Statement
1
2
3
4
5
b) Preventing discrimination against HIV positive people is hard
c) There is gender inequality in our organization
d) The work environment is not socially well maintained
e) Social dialogue on HIV/AIDS issues is hard to foster at work
f) Screening of employees is difficult since HIV testing is
voluntary
g) Keeping the records of employees secret especially regarding
their HIV status is difficult
h) Managing employment relationship with HIV positive workers
is difficult
i) Prevention initiatives are quite costly for the organization in
terms of time and money
j) High cost of providing care and support to HIV positive
workers
Thank you very much for your time!
Related Documents











