The University of Dodoma University of Dodoma Institutional Repository http://repository.udom.ac.tz Health Sciences Doctoral Theses 2020 Implementation of direct health facility financing in public primary health facilities in Tanzania: effects on health system performance. Kapologwe, Ntuli Angyelile The University of Dodoma Kapologwe, N. A. (2020). Implementation of direct health facility financing in public primary health facilities in Tanzania: effects on health system performance (Doctoral thesis). The University of Dodoma, Dodoma. http://hdl.handle.net/20.500.12661/2826 Downloaded from UDOM Institutional Repository at The University of Dodoma, an open access institutional repository.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The University of Dodoma
University of Dodoma Institutional Repository http://repository.udom.ac.tz
Health Sciences Doctoral Theses
2020
Implementation of direct health facility
financing in public primary health
facilities in Tanzania: effects on health
system performance.
Kapologwe, Ntuli Angyelile
The University of Dodoma
Kapologwe, N. A. (2020). Implementation of direct health facility financing in public primary
health facilities in Tanzania: effects on health system performance (Doctoral thesis). The
University of Dodoma, Dodoma.
http://hdl.handle.net/20.500.12661/2826
Downloaded from UDOM Institutional Repository at The University of Dodoma, an open access institutional repository.

IMPLEMENTATION OF DIRECT HEALTH FACILITY
FINANCING IN PUBLIC PRIMARY HEALTH
FACILITIES IN TANZANIA: EFFECTS ON HEALTH
SYSTEM PERFORMANCE
NTULI ANGYELILE KAPOLOGWE
DOCTOR OF PHILOSOPHY IN PUBLIC HEALTH
THE UNIVERSITY OF DODOMA
DECEMBER, 2020

IMPLEMENTATION OF DIRECT HEALTH FACILITY
FINANCING IN PUBLIC PRIMARY HEALTH FACILITIES IN
TANZANIA: EFFECTS ON HEALTH SYSTEM PERFORMANCE
BY
NTULI ANGYELILE KAPOLOGWE
A THESIS SUBMITTED IN FULFILLMENT OF THE
REQUIREMENTS FOR THE DEGREE OF DOCTOR OF
PHILOSOPHY IN PUBLIC HEALTH
THE UNIVERSITY OF DODOMA
DECEMBER, 2020

i
DECLARATION AND COPYRIGHT
I, Ntuli Angyelile Kapologwe, declare that this is my own original work and that it
has not been presented and will not be presented to any other University for a similar
or any other degree award.
Signature
No part of this thesis may be reproduced, stored in any retrieval system, or
transmitted in any form or by any means without prior written permission of the
author or the University of Dodoma (UDOM). If transformed for publication in any
other format shall be acknowledging that, this work has been submitted for degree
award at the University of Dodoma.

ii
CERTIFICATION
The undersigned certify that they have read and hereby recommend for acceptance
by the University of Dodoma thesis titled “Implementation of Direct Health Facility
Financing in the Public Primary Health Facilities in Tanzania: Effect on Health
System Performance” in fulfillment of the requirements for the degree of PhD in
Public Health of the University of Dodoma.
Dr. Stephen Kibusi
Signature _ Date_____03/12/2020__________
(SUPERVISOR)
Dr. Albino Kalolo
Signature Date______03/12/2020__________
(Co - SUPERVISOR)

iii
ACKNOWLEDGEMENTS
To Almighty God, may there always be Glory. I am grateful to Him and I thank Him
for His mercy and grace.
Contributions and moral support from several people, organization and institutions
made this thesis successful. I would like to give my sincere thanks and appreciation
to each and everyone who in one way or another made this journey successful. First,
I would like to give my thanks to the Permanent Secretary, President’s Office-
Regional Administration and Local Government Authority, for granting me
permission to pursue my PhD studies at the University of Dodoma.
I would also like to express my deep gratitude to Dr. Stephen Kibusi and Dr. Albino
Kalolo, my research supervisors, for their guidance, encouragement, and mentorship
towards achieving this research work. My special tributes go to Professors Josephine
Borghi and Tuntufye Mwamwenda for their scholarly comments and valuable time in
the evaluation and examination of the Thesis. From their national and international
University careers, I benefited immensely.
I wish to acknowledge and thank the Swiss Development Cooperation (SDC) and
UNICEF for sponsoring my PhD Studies. Furthermore, I would like to register my
gratitude to the Center for Reforms, Innovation, Health Policy and Implementation
Research (CeRIHI) for their massive support in making this thesis a success. I would
also like to extend my sincere thanks to Regional Administrative Secretaries of the
regions of Pwani, Mtwara, Dodoma, Mbeya, Shinyanga, Manyara and Katavi - for
their support of this study. I am grateful to the District Executive Directors of
Dodoma City Council and Bahi District Council, Kibaha Town Council and
Kisarawe District Council, Mtwara Municipal Council and Nanyumbu District
Council, Mbeya City Council and Rungwe City Council, Shinyanga Municipal
Council and Ushetu District Council, Babati Town Council and Hanang District
Council, Mpanda Municipal Council and Mlele District Council, District Medical
Officers and all the staff and participants of the respective primary health facilities in
respective District Councils for their support and assistance during baseline, mid line
and terminal data collection exercises.
iv
I would also like to send my sincere thanks to my friends, Sally Lake, Ally
Kananika, Hendry Samky, Ally Kinyanga and Abdallah Ally, for their tireless
support in shaping the thesis.
Lastly, I would like to thank Eng. Joseph M Nyamhanga with whom I shared my
ideas and who supported me to the end of this important journey of my life.

v
DEDICATION
This thesis is dedicated to my lovely wife, Dr. Julieth Simon Kabengula, and our
lovely daughters, Tusekile and Twitike, and to our son, Rodney. Without their
support, it would not have been possible to complete this dissertation.
I am also dedicating my work to my parents, Mr. Angyelile Mwasomola Kapologwe
and Mrs. Imani Ambakisye Mwasomola, and my siblings, Lugano, Rhoda and
Nisalile, for their moral support and encouragement in any step I took in making this
thesis a success. May Almighty God protect them and give them the strength they
need.
Lastly, I dedicate this work to all health care workers of United Republic of Tanzania
for their continued effort of offering services to the Tanzanians. To them, I will
always be grateful.

vi
ABSTRACT
Background: Tanzania, like many countries globally, has continuously been
implementing health sector reforms with the intent of ensuring affordable health
services to the population, in alignment with the shift towards Universal Health
Coverage as well as improving the quality of health services, among these reforms
has been the introduction of Direct Health Facility Financing (DHFF), which has
limited evidence on its implementation and outcomes with respect to its intended
goals. This study aimed to assess the implementation of DHFF in the Public Primary
Health Facilities (PPHFs) as well as its effects on health system performance in
Tanzania.
Methods: This study was conducted from January 2018 to September 2019 utilized a
before and after non-controlled study design with a process evaluation embedded at
midline. Both quantitative and qualitative methods were used for data collection. A
structured questionnaire was used to obtain the quantitative data from exiting
patients, and health care workers in 42 PPHFs. Qualitative data was collected using
an interview guide through 14 in depth interviews and seven focus group discussions
to health managers at council level from 14 councils in seven regions. Quantitaive
data analysis was done using SPSS™ version 25 while for qualitative NVIVO
QSR™ version 12 was used.
Results: A total of 844 exiting patients were studied on seven domains of Health
System Responsiveness (HSR) at baseline and endline. All but one domain (i.e.
communication) of HSR were found to have positive significant difference between
baseline and endline. Overall HSR improved significantly from 62.84% at baseline to
71.20% at end line (p<0.0001). In a multivariable logistic regression model, patients
who were studied at the end line were four times more likely to have experienced
positive responsiveness as compared to those at the baseline.
Forty-two (42) PPHFs were studied based on structural quality of maternal health
services (MHS). The majority (71%) of the facilities were within 10 kilometers of
participants’ residences. Of note, the majority (88.9%) of dispensaries and 60% of
health centers were below the required staffing level. There were significant

vii
differences on structural quality of MHS between baseline and endline (2.38% and
30.9% respectively).
With respect to maternal health services utilization, 42 facilities were studied on nine
maternal health service consumption indicators before and after the introduction of
the DHFF initiative. There were significant differences in all indicators after DHFF
introduction except those for intermittent presumptive treatment for malaria second
dose, use of modern family planning methods, and mebendazole use.
Of 238 health care providers who participated in the Fidelity of Implementation (FoI)
component of the study, the majority (76%) had adequate knowledge on the DHFF
implementation issues while only 28% had high Fidelity of Implementation (FoI
scores. For health service providers working in the rural settings, training and
knowledge on the DHFF and Facility Financial Accounting and Reporting System
(FFARS) were significantly associated with high FoI. In the multiple logistic
regression model, both positive HSR (AOR 3.4 [95%CI: 1.637, 7.064]), and high
maternal health service utilization (AOR 40.971[95%CI: 4.065, 412.927]) were
strongly associated with high structural quality of MHS.
Health service providers indicated an improvement in both governance and
accountability, especially in the areas of planning and budgeting, financial
management and transparency, with the implementation of the DHFF. However, the
majority of health care providers admitted to have not received adequate supportive
supervision and mentorship. The providers also felt that this initiative added an
additional burden to their routine work.
Conclusions: In general, the DHFF have affected the health system, specifically on
health system performance in Tanzania. FoI was low despite training being offered to
health care providers, which indicates a need for more investment on this aspect in
order to have a resilient health system. Improved governance and accountability have
been positive outcome on DHFF implementation, which indicate the merits in
ongoing efforts to invest on governance and accountability at PPHFs.
viii
TABLE OF CONTENTS
DECLARATION AND COPYRIGHT ........................................................... i
CERTIFICATION ........................................................................................ ii
ACKNOWLEDGEMENTS ......................................................................... iii
DEDICATION.............................................................................................. v
ABSTRACT ................................................................................................ vi
TABLE OF CONTENTS ........................................................................... viii
LIST OF TABLES ................................................................................... xviii
LIST OF FIGURES ................................................................................... xxi
LIST OF PUBLICATIONS ..................................................................... xxiii
LIST OF APPENDICES .......................................................................... xxiv
LIST OF ABBREVIATIONS .................................................................. xxvi
DEFINITIONS OF TERMS ..................................................................... xxix
CHAPTER ONE ......................................................................................... 1
INTRODUCTION ...................................................................................... 1
1.0 Overview ................................................................................................ 1
1.1 Background Information ......................................................................... 1
1.2 Problem Statement ................................................................................ 25
1.3 Objectives ............................................................................................. 26
1.3.1 Broad objective .................................................................................. 26

ix
1.3.2 Specific Objectives............................................................................. 26
1.3.3 Specific Research Questions ............................................................... 26
1.4 Significance of the Study ...................................................................... 27
CHAPTER TWO ...................................................................................... 29
LITERATURE REVIEW ......................................................................... 29
2.0 Overview .............................................................................................. 29
2.1 Theoretical Literature Review ............................................................... 29
2.1.1 Health System Performance Model (HSPM) ...................................... 31
2.1.2 Health System Reforms Model (HSRM) ............................................ 32
2.1.3 Fidelity of Implementation (FoI) ........................................................ 35
2.1.4 Fidelity of Implementation (Adherence) ............................................. 36
2.1.5 Participants’ Responsiveness towards DHFF implementation ............. 38
2.1.6 Context and Description of DHFF Implementation in Tanzania .......... 39
2.1.7 Implementation Research ................................................................... 41
2.1.8 Evaluation of Health Inteventions or Programs ................................... 43
2.2 Empirical Review .................................................................................. 45
2.2.1 Situation of Health Care Financing Reforms....................................... 45
2.2.2 Implementation of DHFF initiative in Tanzania .................................. 48
2.2.2.1 Delays in Disbursement of Funds .................................................... 48

x
2.2.2.2 Weaknesses in Planning and Budgeting of Activities ....................... 49
2.2.2.3 Weak Supportive Supervision and Mentorship ................................ 50
2.2.2.4 Failure to Maintain Buildings and Supply Chain of Medicines and
Supplies ........................................................................................... 50
2.2.3 HSR in PPHF ..................................................................................... 51
2.2.4 Structural Quality of MHS ................................................................. 51
2.2.5 Maternal Health Service Utilization .................................................... 53
2.2.6 Conceptual Frameworks Guiding the Study ........................................ 54
2.2.7 Theory of Change (ToC) .................................................................... 54
2.2.8 Governance and Accountability .......................................................... 57
2.2.9 Research or Knowledge Gap .............................................................. 59
CHAPTER THREE .................................................................................. 60
METHODOLOGY ................................................................................... 60
3.0 Overview .............................................................................................. 60
3.1 Study Settings ....................................................................................... 60
3.2 Research Approaches ............................................................................ 63
3.3 Study Design ......................................................................................... 63
3.4 Target Population .................................................................................. 64
3.5 Study Population ................................................................................... 64
3.5.1 Inclusion Criteria................................................................................ 65
xi
3.5.2 Exclusion Criteria .............................................................................. 65
3.6 Unit of Analysis .................................................................................... 65
3.7 Sampling Method and Sample Size Estimation ...................................... 66
3.7.1 Sampling Methods for Quantitative Data ............................................ 66
3.7.2 Quantitative Sample Size Determination ............................................ 69
3.7.3 Quantitative Data Collection .............................................................. 69
3.7.4 Sampling Methods for Qualitative Data .............................................. 70
3.7.5 Data Collection Methods and Tools for Qualitative ............................ 71
3.8 Sample Size Determination ................................................................... 72
3.9 Data Collection Tools............................................................................ 73
3.10 Pre-testing of Tools ............................................................................. 86
3.11 Data Collection Procedure ................................................................... 86
3.12 Data analysis.…………………………………………………………...87
3.12.1 Quantitative data analysis …………………………………………....87
3.12.1.1 Variables and their measures ......................................................…87
3.12.1.1.1 Dependent Variables................................................................... 87
i. HSR .................................................................................................... 87
ii. Structural quality of MHS ................................................................... 87
iii. MHS utilization
iv. Implementation fidelity of DHFF initiative

xii
v. Governance and accountability ............................................................ 87
3.12.1.1.2 Independent Variables ................................................................ 87
3.12.1.2 Categorization of Variables ........................................................... 88
3.12.1.2.1 Categorization of Health System Responsiveness ....................... 88
3.12.1.2.2 Categorization of Structural Quality of MHS .............................. 91
3.12.1.2.3 Categorization of Health Service Utilization ............................... 92
3.12.1.2.4 Categorization of Fidelity of Implementation (FoI) ..................... 92
3.13 Data Processing and Statistical Analysis .............................................. 93
3.13.1 Statistical analysis ........................................................................... 93
3.13.2 Governance and Accountability ....................................................... 94
3.14 Qualitative Data Analysis .................................................................... 94
3.15 Integration of Quantitative and Qualitative methods ............................ 95
3.16 Trustworthiness and Credibility ........................................................... 96
3.17 Validity and Reliability ....................................................................... 97
3.17.1 Validity ........................................................................................... 97
3.17.2 Reliability ........................................................................................ 97
3.18 Ethical Consideration ........................................................................ 102
CHAPTER FOUR................................................................................... 103
RESULTS ................................................................................................ 103

xiii
4.0 Introduction ........................................................................................ 103
4.1 Perception of Patients on Health System Responsiveness (HSR) in PPHF
...................................................................................................... 104
4.1.1 Socio-Demographic Characteristics of Patients in PPHFs ................. 104
4.1.2 Status of Health System Responsiveness (HSR) as perceived by patients
in PPHF (PPHFs) before and after implementation of Direct Health
Facility Financing (DHFF) ............................................................ 106
4.1.3 Factors Associated with change in overall perception of patients on
Health System Responsiveness in PPHF before and after
implementation of Direct Health Facility Financing. ...................... 110
4.2 Level of Structural Quality of MHS in the PPHF before and after Direct
Health Facility Financing Implementation ..................................... 119
4.2.1 Demographic Characteristics of PPHF before and after implementation
of Direct Health Facility Financing ................................................ 119
4.2.2 Level of Structural Quality of Maternal Health Service in PPHF before
and after implementation of Direct Health Facility Financing. ....... 128
4.2.3 Other factors that influenced change in structural quality of MHS in
PPHF before and after implementation of Direct Health Facility
Financing....................................................................................... 133
4.3 Level of maternal health service utilization in PPHF before and after
implementation of Direct Health Facility Financing ....................... 136
4.3.1 Other factors associated with Change of Maternal Health Service
Utilization in PPHF before and after implementation of Direct Health
Facility Financing. ......................................................................... 137
4.4 Level of Direct Health Facility Financing (DHFF) Fidelity of
Implementation (FoI) and its potential moderators ......................... 141

xiv
4.4.1 Socio-Demographic Characteristics of Health Service Providers in
PPHFs ........................................................................................... 141
4.4.2 Knowledge of Health Service Providers on the implementation of
Direct Health Facility Financing in PPHF. ..................................... 144
4.4.3 Fidelity of Implementation of DHFF by Health Service Providers . 149
4.5 The association between Fidelity of Implementation (FoI) and overall
Structural quality of maternal health service in PPHF. ................... 151
4.6 The association between Fidelity of Implementation (FoI) and overall
Maternal health service utilization in PPHF before and after
implementation of Direct Health Facility Financing. ...................... 153
4.6.1 Health Care Providers’ experience towards Direct Health Facility
Financing...........................................................................................154
4.6.2 Thematic Findings for Qualitative Research......................................155
4.6.2.1 Training on DHFF, FFARS, Planning and Budgeting .................... 156
4.6.2.2 Knowledge (Content) on DHFF initative ....................................... 157
4.6.2.3 Coordination of DHFF activities .................................................... 157
4.6.2.4 Attitude of Health care providers towards DHFF ........................... 159
4.6.2.5 Timeliness in addressing issues due to DHFF presence .................. 159
4.6.2.6 Timely availability of health service provider’s benefits, tools and
other resources .............................................................................. 160
4.6.2.7 Timely fund utilization and service provision ................................ 160
4.6.2.8 Capacity of health service providers on management of DHFF
initiative ........................................................................................ 161
4.6.2.9 Timeleness in disbursement of funds ............................................. 162

xv
4.6.2.10 Improvement in working environment ......................................... 162
4.7. Thematic Number 1: Governance…………………………………….162
4.7.1 Governance of DHFF ....................................................................... 163
4.7.2 Funds Management .......................................................................... 164
4.7.3 Capacity of Health Facility Governing Committee (HFGC) Members
...................................................................................................... 164
4.7.4 Planning and Budgeting ................................................................... 164
4.8 Thematic Area Number 2: Accountability ........................................... 165
4.8.1 Transparency and Community Involvement ..................................... 165
4.8.2 Financial and performance report review and approval ..................... 166
4.8.3 Oversight ......................................................................................... 166
4.9 Thematic Number 3: Supportive Supervision and Mentorship ............. 166
4.9.1 Regular monitoring of primary health facilities, Consistency provision
of guidance………………………………………………………….168
4.9.2 Clarification/ interpretation of policies, strategies and operational
guidelines…………………………………………………………..168
4.9.3 Integration of Quantitative and Qualitative Results ........................... 168
4.9.3.1 Framework for Integration ............................................................. 168
4.9.3.2 Interpretation of the Integrated Results .......................................... 169
CHAPTER FIVE .................................................................................... 170
DISCUSSION .......................................................................................... 170
xvi
5.0 Introduction ........................................................................................ 170
5.1 Health System’s Responsiveness ......................................................... 170
5.2 Structural Quality of MHS .................................................................. 172
5.3 Maternal Health Service Utilization .................................................... 173
5.4 FoI towards DHFF initiative................................................................ 174
5.5 Health Care Providers’ responsiveness towards implementation of Direct
Health Facility Financing in PPHF. ............................................... 177
5.6. Governance and Accountability on DHFF implementation....................178
5.6.1 Governance ...................................................................................... 178
5.6.2 Accountability .................................................................................. 179
5.6.3 Theoretical reviews .......................................................................... 181
5.6.4 Conceptual frameworks .................................................................... 182
CHAPTER SIX ....................................................................................... 184
CONCLUSION, RECOMMENDATIONS AND SUGGESTION FOR
FURTHER RESEARCH ............................................................. 184
6.1 Conclusion .......................................................................................... 184
6.2 Recommendations ............................................................................... 185
6.2.1 Recommendation to Policy makers ................................................... 185
6.2.2 Recommendation to Policy Implementers ......................................... 186
6.2.3 Recommendations to the DHFF Initiative ......................................... 188
xvii
6.3 Strengths of the Study ......................................................................... 189
6.4 Limitations of the Study ...................................................................... 189
6.5 Suggestions for Further Research ........................................................ 190
REFERENCES ......................................................................................... 192
PUBLICATIONS ..................................................................................... 217
APPENDICES .......................................................................................... 219

xviii
LIST OF TABLES
Table 1: Star Rating and Grading Criteria of Primary Health Facilities .................... 19
Table 2: Allocation of funds pre and post-introduction of DHFF ............................. 24
Table 3: Scoring Criteria/Cut-offs for HSR Performances ....................................... 74
Table 4: Health Care Responsiveness Performance Criteria and their Categorization
........................................................................................................................ 90
Table 5: Reliabilities of each Domain of HSR ......................................................... 90
Table 6: Data Analysis Plan and Measurement of Variables for Baseline and Endline
Study............................................................................................................... 98
Table 7: Objective number 4 ................................................................................. 101
Table 8: Social Demographic Characteristics of the Patients in PPHF (PPHFs) before
and after implementation of Direct Health Facility Financing (DHFF) (n=844)
...................................................................................................................... 104
Table 9: Two Sample Independent T-test for Perception of Patients towards Health
System Responsiveness before and after implementation of Direct Health
facility Financing (DHFF) in PPHF (PPHF) (n=844, p=0.05) ........................ 109
Table 10: Chi-squire test for factors associated with change in overall perception of
Health System Responsiveness among patients who attended in the public
primary health care facilities before and after DHFF implementation (n=844,
p=0.05). ........................................................................................................ 112
Table 11: Logistic regression model for factors associated with change in overall
perception of Health System Responsiveness before and after implementation of
Direct Health Facility Financing in PPHF (p<0.05, 95% CI). ........................ 115
Table 12: Characteristics of the Public Primary Health Facilities before and after
implementation of Direct Health Facility Financing (n=42). .......................... 120
xix
Table 13: Descriptive Results on Change of Structural quality of MHS in Tanzania
before and after DHFF implementation (n= 42). ............................................ 124
Table 14: Paired T-test Results for Change in Structural Quality of MHS in PPHFs
before and after implementation of DHFF (n=42, p=0.05, CI = 95%). ........... 130
Table 15: Fisher’s exact test results for other factors that attributed to change in
overall structural quality of MHS in PPHF before and after implementation of
Direct Health Facility Financing (n= 42). ...................................................... 134
Table 16: Cell analysis results for for other factors that attributed to change in overall
structural quality of MHS in PPHF before and after implementation of Direct
Health Facility Financing (n= 42) .................................................................. 135
Table 17: Wilcoxon signed rank test for Change in Maternal Health Service
Utilization before and after implementation of Direct Health Facility Financing
in PPHF (n=42, p= 0.05). .............................................................................. 138
Table 18: Poisson Regression Model for other factors associated with change of
maternal health service utilization in Public Primary Health Facilities before and
after implementation of DHFF. ..................................................................... 140
Table 19: Social Demographic characteristics of Health Care Workers (HCWs) in
PPHF implementing DHFF. .......................................................................... 142
Table 20: Descriptive results of knowledge among health care workers in PPHF
during the implementation of Direct Health Facility Financing ...................... 144
Table 21: Level of FoI among Health Service Providers in PPHFs ........................ 146
Table 22: Logistic regression model for factors associated knowledge (p=0.005) .. 147
Table 23: Chi-squire test for factors associated with FoI ....................................... 149
Table 24: Logistic regression results for factors associated with FoI in PPHF before
and after implementation of DHFF (n=234). .................................................. 151

xx
Table 25: Association between Changes of Structural Quality by Fidelity of
Implementation ............................................................................................. 152
Table 26: Logistic regression results for association between FOI and overall
structural quality of HS and in PPHFs before and after implementation of DHFF
(n= 42). ......................................................................................................... 152
Table 27: Association between overall changes of health service utilization and
Fidelity of Implementation of Direct Health facility financing in PPHFs. ...... 153
Table 28: Logistic regression results for the association between FoI and overall
maternal health service utilization in PPHFs before and after implementation of
DHFF. ........................................................................................................... 154
Table 29: Socio-demographic Characteristics of Interviewees ............................... 155
Table 30: Results from Indepth interviews by thematic and sub thematic areas ..... 155
Table 31: Characteristics of Interviewees .............................................................. 163
xxi
LIST OF FIGURES
Figure 1. Health System Building Blocks (Adam & Savigny, 2012) ...................... 10
Figure 2: Estimated health sector expenditures, projections and sources of funding
(million TZS). ................................................................................................. 15
Figure 3: Tanzania Health Sector Milestones and Reform Timelines from 1880s to
2019 ................................................................................................................ 17
Figure 4: Cascade Training on Direct Health Facility Financing (DHFF) across
Tanzania. ........................................................................................................ 21
Figure 5: Funds disbursement before and after DHFF implementation. ................... 24
Figure 6: Opening the ‘black box’ of the DHFF through assessing the
implementation processes. ............................................................................... 28
Figure 7: The health reform cycle (modified from Roberts et al., 2002)
31
Figure 8: Health System Performance Model (Berman & Bitran, 2011a) ................ 33
Figure 9: Direct Health Facility Financing Management Framework ...................... 41
Figure 10: Health Financing Arrangement, Intermediate Objectives and UHC goals
(WHO, 2013). ................................................................................................. 46
Figure 11: Direct Health Facility Financing (DHFF) Funds Flow and Stakeholders
Relationship in Tanzania (Kapologwe. et al., 2020). ........................................ 49
Figure 12: Theory of Change of DHFF Implementation in Tanzania ....................... 56
Figure 13: Conceptual Framework for Fidelity of Implementation .......................... 56
Figure 14: Map of Tanzania that depicts the distribution of District Councils and
PPHF that participated in the study (Kapologwe et al., 2019). ......................... 61

xxii
Figure 15: The Organization of Health System of Tanzania .................................... 62
Figure 16: Schematic Presentation of Sampling Technique ..................................... 68
Figure 17: Schematic Presentation of Data Collection Processes ............................. 70
Figure 18: Schematic Presentation of Process and Outcome Evaluation of the DHFF
Implementation ............................................................................................... 81
Figure 19: Modified Conceptual FoI Framework after the Midline Study (Modified
from Original Framework by Kapologwe et al., 2019). .................................... 85
Figure 20: Summary of Study Variables ................................................................ 88
Figure 21: Schematic Presentation of Integration of Mixed Methods Triangulation
Design for Measuring DHFF Fidelity of Implementation (FoI) ........................ 96
Figure 22: Regional pefromance on structural quality of MHS before and after
implementation of Direct Health Facility Financing (n=42). .......................... 108
Figure 23: Percentage Change of Structural Quality of Maternal Health service in
PPHF before and after implementation of Direct Health Facility Financing
(n=42). .......................................................................................................... 133

xxiii
LIST OF PUBLICATIONS
Publication Paper 1: Understanding the implementation of direct health facility
finacing and its effect on health system performance in Tanzania .................. 217
Publication Paper 2: Assessing health system responsiveness in primary health care
facilities in Tanzania ..................................................................................... 218

xxiv
LIST OF APPENDICES
Appendix I: A descriptive results of Health System Responsiveness as perceived by
patients in PPHF before and after implementation of DHFF .......................... 219
Appendix II: Prompt to Attention .......................................................................... 221
Appendix III: Respect to Dignity .......................................................................... 223
Appendix IV: Clear Communication ..................................................................... 224
Appendix V: Respect to Autonomy ....................................................................... 226
Appendix VI: Access to Care ................................................................................ 227
Appendix VII: Respect to Confidentiality ............................................................. 229
Appendix VIII: Basic Amenities ........................................................................... 230
Appendix IX: Association between Structural Quality and HSR in PPHF after
implementation of DHFF (p<0.05; CI = 95%) ............................................... 234
Appendix X: Table of Random Numbers .............................................................. 235
Appendix XI: Coding Table for Indepth Interviews ............................................... 236
Appendix XII: Coding table for Focus Group Discussion ...................................... 240
Appendix XIII: Objective number One: Health System Responsiveness as perceived
by the end users of PPHF .............................................................................. 244
Appendix XIV: Objective number two: Structural Quality of MHS in the PPHF ... 257
Appendix XV: Objective number three: Maternal Health Service Utilization in the
PPHF ............................................................................................................ 284
Appendix XVI: Objective Number Four: To explore Governance and Accountability
on DHHF in PPHFs ....................................................................................... 289

xxv
Appendix XVII: Objective Number Five (Quantitative): Level of Fidelity of
Implementation and its potential moderators ................................................. 293
Appendix XVIII: Objective number five (Qualitative): Participant’s Responsiveness
to DHFF ........................................................................................................ 313
Appendix XIX: Consent Form .............................................................................. 315
Appendix XX: Ethical Clearance Forms................................................................ 317

xxvi
LIST OF ABBREVIATIONS
AIDS Acquired Immunodeficiency Syndrome
ANC Antenatal Care
AOR Adjusted Odds Ratio
ART Antiretroviral Therapy
CHF Community Health Fund
CHMT Council Health Management Team
CHS Community Health Syestem
CHSB Council Health Service Board
CHW Community Health Workers (CHWs)
CORPs Community Own Resource Persons
CTC Centre for Treatment and Counselling
D-by-D Decentralization by Devolution
DED District Executive Director
DFF Direct Facility Financing [Kenya]
DHFF Direct Health Facility Financing
DHIS -2 District Health Information System -2
DMO District Medical Officer
FFARS Facility Financial Accounting and Reporting System
FoI Fidelity of Implementation

xxvii
GoT Government of Tanzania
HCWs Health Care Workers
HF Health Facility
HFGC Health Facility Governance Committee
HIV Human Immunodeficiency Virus
HRH Human Resource for Health
IDI In-Depth Interview
IPD Inpatient Department
LGA Local Government Authority
LMIC Lower- and Middle-Income Countries
MOHCDGEC Ministry of Health, Community Development, Gender, Elderly
and Children
OPD Outpatient Department
PO-RALG President’s Office – Regional Administration and Local
Government
PPHF Public Primary Health Facility
PHC Primary Health Care
P4P Payment for Performance
RBF Results-Based Financing
RMNCH Reproductive, Maternal, Newborn, and Child Health
SDGs Sustainable Development Goals

xxviii
ToC Theory of Change
ToT Training of Trainers
URT United Republic of Tanzania
WHO World Health Organization
xxix
DEFINITIONS OF TERMS
Acceptability Determining how well an intervention will be received by the
target population and the extent to which the new intervention
meet the needs of the target population and organizational setting
(Ayala & Elder, 2011).
Attitude A settled way of thinking or feeling about something.
Caretakers
People from within the family environment taking care of basic
needs required by the patient.
Client Person who uses services available at health facility.
Cost Center Refers to levels of service provision and associated budgets. For
example, in the health sector there are 5 cost centers – Council
Health Management Team (CHMT), Council Hospital, Voluntary
Agency Hospital (VAH), Health Centre and Dispensaries.
Cost Sharing Money paid by clients ‘out of pocket’ and through various
insurance schemes
Decentralization
by Devolution (D
by D)
One of three types of decentralization; the other types are de-
concentration and delegation. Under D-by-D policy the central
government is expected to devolve functions, transfer authority for
decision-making, finance, and management to the local
government authorities. Responsibility for services to city,
municipalities and district councils that elect their own mayors and
councils, raise their own revenues, and have independent authority
to make investment decisions.
Direct Health
Facility
Financing
The process of disbursing funds directly to the health facilities by
the central Government of Tanzania (GoT).
xxx
Effect
Exercised
Outcomes or Results from implementation of DHFF initiative.
Means how implementation of DHFF in PPHF adhered to the
principles of Governance and Accountability.
Fidelity of
Implementation
Extent to which an intervention, initiative, or program is delivering
as intended by the intervention model (Carroll et al., 2007).
Health Basket
Fund
Joint funding mechanism in Tanzania whereby Development
partners pool un-earmarked resources to support non-salary
recurrent costs of primary level health services.
Health
Management
Information
System
Data collection and dissemination system specifically designed to
support planning, management, and decision making in
health facilities and organizations.
Health Planning Process of getting agreed priorities and direction for health sector
in the light of available resources.
Health service Any service (i.e. not limited to medical or clinical services) aimed
at contributing to improved health or to the diagnosis, treatment,
and rehabilitation of sick people.
Health System
Performance
Indicators
Indicators used to measure progress of the health care system. In
this study, the 5 indicators studied were health system
responsiveness, structural quality of maternal health services,
maternal health service utilization, governance, and accountability.
Health system
responsiveness
(HSR)
Assessment of how well the health system meets the legitimate
expectations of the population for the non-health enhancing
aspects of the health system. It includes seven domains: prompt to
attention, autonomy, dignity, quality of basic amenities of care,
communication, respect of confidentiality, and access to care.
Implementa-tion An integrated concept that links research and practice to accelerate

xxxi
Research the development and delivery of public health approaches.
Implementation research involves creation and application of
knowledge to improve the implementation of health policies,
programmes, and practices. Implementation research as a
“scientific inquiry into questions concerning implementation, i.e.,
the act of carrying an intention into effect which in health research
can be policies, programs or individual practices (collectively
called interventions)”(Peters, Tran, & Adam, 2013, p # please).
Knowledge
Information and skills acquired through experience or training on
DHFF, which can be either explicit or implicit.
Morbidity State of illness and disability in a population
Mortality rate Number of deaths within a specific population group and within a
particular period of time.
Outcome A quantitative or qualitative factor or variable that provides a
simple and reliable means to measure achievement, to reflect the
changes connected to an intervention, or to help assess the
performance of an institution.
PlanRep A web-based system designed to assist local government
authorities and public health facilities in planning, budgeting,
projecting revenue from all sources, and tracking of and reporting
on funds received, physical implementation, and expenditures.
Primary Health
Care
Essential preventive and curative health services offered from the
District Council level, Health Centers, Dispensaries up to the
Community level.
Public Health
Facility
All health facilities that are owned and managed by the GoT.

xxxii
Quality of Health
Care Services
Degree to which health services for individuals and populations
increase likelihood of desired health outcomes and consistent with
current professional knowledge (Mainz, 2003).
Results-Based
Financing (RBF)
A cash payment or non-monetary transfer made to a national or
sub-national government, manager, provider, payer, or consumer
of health services after predefined results have been attained and
verified. Payment is conditional on measurable actions being
undertaken." (www.rbfhealth.org). RBF is an umbrella term
because the definition is general and characterizes various
programs in many countries. Different labels exist for essentially
the same concept or are associated with different incentives and
payment arrangements. Any mode of payment that tries to base
financing beyond inputs is called results-based financing.

1
CHAPTER ONE
INTRODUCTION
1.0 Overview
This chapter presents background information on health system performance, health
care financing related reforms and implementation of a decentralization policy in the
health sector in Tanzania. In addition, this chapter introduces the concept of
implementation research, problem statements, research objectives, research and
evaluation questions and significance of the study.
1.1 Background Information
Health system performance and indicators measures
Health system performance, refers the measure of whether the health systems meet
expectation of the beneficiaries, is an important metric for any health care system in
the world. There is a multiplicity of models to measure health system performance,
but measures that consistently reflect the objectives of the system, the nature and
quality of the data, the incentives for stakeholders to scrutinize and act upon the data,
and the culture of the organization within which the data are deployed, are
considered to be more reliable (Smith, 2002; Smith & Busse, 2008). Indicators of a
perfoming system include: HSR, clinical quality, utilization, population health
outcomes, equity, and productivity. Other essential indicators for measuring health
system performance are structural outcomes and process indicators (Musgrove et al.,
2000; Smith, 2002; Smith & Busse, 2008).
Maternal Health Services (MHS)
Women and children are the main users of health services in any given settings. The
reason for their main use of services are due to their predisposition to different
disease conditions (Chakraborty, Islam, Chowdhury, Bari, & Akhter, 2003). This is
one of the reasons which accounts for their high level of attendences in the health
facilities. The empirical evidence has shown that when you address health challenges
that are maternal and child related tend to impact other groups in the general
population (Braveman & Gottlieb, 2014).

2
Globally, it is estimated that 295,000 maternal deaths occurred in the year 2017
(WHO & UNICEF, 2019), with haemorrhage (44,200 deaths) and abortions (43,700
deaths) being the leading causes of mortality (Kinney et al., 2010; Naghavi et al.,
2015). Sub-Saharan African women constitute about 66% (196, 000) of maternal
mortality worldwide (WHO, UNICEF, UNFPA, World Bank Group,
2019). Tanzania ranks among the countries with the highest maternal mortality rates
worldwide (WHO, UNICEF, UNFPA, World Bank Group, 2019). The current
Tanzanian estimated maternal mortality ratio is 556/100,000 live births
(MoHCDGEC et al., 2016).
Tanzania like many other Sub-Saharan Africa (SSA) countries, has been challenged
by high maternal mortality rates since 1990s despite significant government and
partner efforts to minimize the deaths. There have been several strategies,
interventions and reforms dedicated to reduction of mortality with negligible
successes such as use of traditional birth attendants (MOHCDGEC, 2016). In an
effort to reduce maternal deaths and to increase maternal health service utilization
among mothers, the GoT introduced exemptions of costs to cover for health services
among pregnant women and also subsidizing the cost of some essential commodities
like insecticides treated nets through the ‘Hati Punguzo’ program and anti malarial
medicines. Moreover, several strategies have been undertaken, such as One Plan I, II,
III and Health Sector Strategic Plan-IV (2015-2020), which have demonstrated some
success such as increase in immunization coverage and also increase in reproductive
and child health outreach and mobile clinics. Also there have been some programs
including the Results-Based Financing (RBF) which is currently implemented in
eight regions aimed at improving maternal health indicators (MOHSW, 2009).
Results-Based Financing as an intervention is aiming at improving the quantity and
quality of MHS, raising health facility utilization, and improving community
participation on maternal health related activities (MoHSW, 2015a).
In 2017/2018, the Direct Health Facility Financing (DHFF) initiative was introduced
with aim of improving quality of health service delivery at the PPHF with a main
focus being maternal and child health services.

3
Empirical evidence shows that poor quality facility-based health care for women and
their newborns contributes to increased deaths and morbidity in their respective areas
(MoHCDGEC, 2015; Naghavi et al., 2015).
Health System Responsiveness (HSR)
Health system responsiveness (HSR) ‘tends to measure the non-health aspect of care
relating to the environment and the way healthcare services are provided to clients’
(Robone, Rice, & Smith, 2011; Shé et al., 2020; Smith, Rice, Robone, & Smith,
2008, ). The intrinsic goal of responsiveness is to ensure “that people are treated
promptly, with respect for their dignity and their wishes, and that patients receive
adequate physical and effective support while undergoing treatment” (WHO, 2000)
while seeking meaningful improvement of the health care system for the well-being
of the population (Darby, Valentine, Murray, & de Silva, 2001; Smith et al., 2008).
Responsiveness, as it pertains to the health system, mainly focuses on seven domains
that have been divided into two major components: (a) respect for persons (including
dignity, clear communication, confidentiality and autonomy of individuals and
families to decide about their own health); and (b) client orientation (prompt
attention, access to social support networks during care and quality of basic
amenities) (Darby et al., 2001; Murray & Frenk, 2000). In Tanzania, the overall
health system performance by the PPHF has been low even before the introduction of
DHFF initiative (Kapologwe et al., 2020).
Structural Quality of Health Services
Quality of care can be defined as the “degree to which health services for individuals
and populations increase likelihood of desired health outcomes and consistent with
current professional knowledge” (Gary, 1990). Structural quality of MHS are all
structural quality issues that are related to maternal health service provision in the
health facilities. A study done in five countries in SSA including Tanzania showed
that the quality of the MHS in the majority of primary health care (PHC) facilities is
poor and needs improvement (Kruk et al., 2016; Yahya & Mohamed, 2018).

4
According to Mainz (2003), ‘structures’ refers to
Health system characteristics that affect the system’s ability to meet the
healthcare needs of individual patients or a community. Structural indicators
describe the type and amount of resources used by a health system or
organization to deliver programs and services, e.g. the presence or number of
staff, clients, funds, beds, supplies, and buildingsincluding those which offer
safe surgery facilities (p.525).
A body of evidence exists which suggests there is an association between health care
structures and the quality of health services being offered by those facilities (WHO &
OECD, 2018).
Poor quality of health services provision has been a central challenge affecting the
Tanzanian health system experienced by the health providers working in those health
facilities (Mboya et al., 2016; Renggli, 2017). This quality gap has consequently
resulted in dissatisfaction of service users. A study done in in Dar es Salaam at
Mwananyamala hospital among outpatients on quality of health services rendered to
them, they expressed the poor quality concerns (Khamis & Njau, 2014). Despite
those challenges, the GoT has been investing heavily in improving the structural
quality of the primary health facilities through several interventions including the
Primary Health Service Development Programme (PHSDP) commonly known as
MMAM (Mpango wa Maendeleo wa Afya ya Msingi) in Kiswahili. This has resulted
in renovation and construction of both old and new facilities respectively, as well as
equipping the facilities with essential medical equipment (Kapologwe et al., 2020).
Maternal Health Service Utilization
Health service utilization is the extent to which people are accessing and making use
of health services available within and outside their immediate catchment areas.
Access can be either through admission or through the outpatient services. Optimal
service utilization is a core indicator for any highly performing health care system in
any given setting. Patient service utilization is an important indicator of health
system performance or a proxy indicator for quality of services provision and HSR.
Additionally, health service utilization data can inform planning and budgeting as
well as forecasting and quantification of health commodities and supplies. Moreover,

5
the data can help to identify utilization trends and bypassing of health services by the
members of the community in their catchment areas.
Maternal health service utilization has been a challenge in many resource-limited
countries due to low education levels, poor income and wealth, and rurality (Alam,
Hajizadeh, Dumont, & Fournier, 2015; Kanyangarara, Munos, & Walker, 2017;
Saxena, Vangani, & Mavalankar, 2013). Many studies point to maternal health
service indicators as showing particularly low performance in areas of post-natal care
[i.e., within 3-7 days], institutional deliveries, use of modern family planning
methods, and uptake of a second and third dose of intermittent preventive treatment
for malaria during pregnancy (IPT2) (Kibusi, Kimunai, & Hines, 2015; Martin et al.,
2019; Saxena et al., 2013). Morever, one maternal health service utilisation indicator
that has increased in Tanzania over recent years is the prevalence of women
experiencing facility-based deliveries, shifting from 50% in 2010 to 63% in 2015.
However, this trend varies depending on the area of residence whereby those who are
in urban areas had an attendance of 86% while those in rural areas had an attendance
of 54% (MoHSW, 2015b).
Health System Governance and Accountability
As part of DHFF implementation, the PPHF are authorized to have a facility-level
account for the receipt of all type of funds from both government and non-state
actors. However, opening of these accounts needs authorization from the Bank of
Tanzania (BoT) (Kapologwe et al., 2019). Management of facility funds is done by
the health service providers together with Health Facility Governing Committee
(HFGC) members by following the guidelines for Comprehensive Health Facility
Plans (CHFP) and Comprehensive Council Health Plan (CCHP) (MoHSW, 2011;
United Republic of Tanzania (URT), 2016). The GoT has developed a simple
Facility Financial Accounting and Reporting System (FFARS) which is used as a
guide for public financial management for the public primary health facility
(MoHSW, 2014b). FFARS works alongside other financial systems, such as
Planning and Reporting System (PlanRep) and the LGA accounting software

6
(EPICOR), to aid planning, budgeting, expenditures tracking and reporting as per
schedules (URT, 2016).
Governance can be defined as ‘how societies make and implement collective
decision’ (Saltman, Bankauskaite, & Vrangbaek, 2007), and is reflected in
Sustainable Development Goal (SDG) number 16 (UN, 2015). Governance helps to
enhance accountability and ownership of programs and initiatives (Savedoff, 2011).
The governance structures vary considerably across the globe. For example, in
Kenya, they have Health Facility Committees which are responsible for some
management and governance activities at the primary health facility level.
Governance in the Tanzanian health sector is guided by the existing governance
structures at central and lower levels of government. In Tanzania, health system
governance structures at all levels combine members from both technical and
political sides, which create checks and balances during implementation decision
points. For primary health care, this places governance at the district council level,
and lower level governments, such as wards and villages where the facilities are
based. At the district council level there is a standing committee for social services
with technocrats (composed of heads of departments for health, education,
agriculture, environment, accounts, internal audit, procurement, water, land, law,
human resources and planning) whose roles are to approve plan and report on all
technical issues that are implemented at the ward and village levels, they are also
answerable to councillors. Alongside this committee there are governing entities
from the regional level down to the local level, including the Council Health Service
Board (CHSB) that is composed of members from the community including the
chairperson, the other members include the chairperson to the Social Committee and
Council Management Team (CMT) members. The Secretariat to this meeting comes
from the Council Health Management Team (CHMT) (Kessy, 2014). At the facility
level, there is HFGC that serves a health system governance structure that links the
community’s decisions to that of the primary health facility within the catchment
area.
Accountability in the health system can be defined as “procedures and processes by
which one party justifies and takes responsibility for its activities such as for
7
achieving various organizational goals” (Emanuel & Emanuel, 1996). It is
considered to be one of the intermediate goals of attaining Universal Health
Coverage (UHC) along with transparency and equitable distribution of health
systems resources (Kutzin, 2013; Kutzin, Cashin, & Jakab, n.d.).
The concept of internal accountability mechanisms refers to the relationship within
and between different levels of the health care system. It is important to look into
how key players were involved in the planning and budgeting processes, adherence
to standards of submissions of technical and financial reports, and displays of
revenues and expenditures at the primary health facility level while complying to all
available instructions. The World Bank (2015) found that many HFGC members and
some health facility providers had limited knowledge on planning and budgeting and
few adhered to the budget guidelines (World Bank, 2015a, 2015b).
External accountability mechanisms refer to existing relationship between health care
workers and the communities within and around their catchment areas. The current
study assessed how implementation of the DHFF initiative has influenced the
performance of HFGCs and HSR. The HFGC are mainly responsible for oversight
of the health services provided by the primary health facilities. However, several
assessments conducted in Tanzania showed that they have limited capacities in terms
of their functionality and performance of their assigned roles and responsibilities
(Mayumana et al., 2017; World Bank, 2015b). Moreover, in many primary health
facilities, the complaints handling mechanism, display of revenues and expenditures,
and price list of services were non-existant (Mayumana et al., 2017; World Bank,
2015b).
The way health systems perform vary due to a number of factors which such as
expenditure rates in the health sector, disbursement modalities, and human resources
for health (Murray & Frenk, 2000; Tashobya et al., 2014). To improve health system
performance globally and specifically in low- and middle-income countries (LMIC),
several reforms have been implemented with varying levels of success. Such reforms
include introduction of a prime vendor system in order to ensure a constant supply of
health commodities and supplies, improved community health fund (CHF), and

8
direct health facility financing (Kalolo, Radermacher, Stoermer, Meshack, & De
Allegri, 2015b; Kapologwe et al., 2019; Wiedenmayer et al., 2019). These reforms
have been implemented and evaluated alongside the World Health Organization’s
(WHO) conceptual framework for health system performance assessements (HSPA).
The HSPA are conducted through selected indicators that reflects the performance of
the health care system (Murray & Frenk, 2000; Sun, Ahn, Lievens, & Zeng, 2017;
Tashobya et al., 2014).
The performance of the country’s health care system largely depends on the health
financing modality adopted in a given country (Murray & Frenk, 2000). The health
financing block, which is one of the six WHO health system building blocks (Figure
1) (WHO, 2010), is a cornerstone of health system performance and improvements in
health outcomes of the population. There are two types of health care financing
systems that include: 1) Bismarck model, which is based on social insurance; and 2)
Beveridge model, that is based on the tax collection (Liaropoulos & Goranitis, 2015).
The functions of the health care financing systems include: i) resource mobilization
from different sources such as out of pocket payment, community health financing,
social health insurance, general revenue and donor funding; ii) risk pooling; and iii)
resource allocation (payment mechanisms) [i.e. through global budget, fee-for-
service and capitation] (Kutzin et al., n.d.; WHO, 2017).
Although funds may be mobilized using different sources and ensuring risk-pooling
approaches, paying health services providers (organizations) and how to disburse the
payments presents a challenge (Frumence, Nyamhanga, Mwangu, & Hurtig, 2013).
Adopting innovative payment and fund disbursement approaches can solve these
challenges. The DHFF initiative represents an innovative fund disbursement
mechanism adopted by the GoT since 2017 (Kapologwe et al., 2019).
Direct Health Facility Financing represents a payment and disbursement mechanism
where mobilized funds are disbursed directly to the health facility from any funding
source or the government treasury without going through any other channel. The
objective is to improve efficiency, accountability, transparency, autonomy and
service delivery while also adhering to the financial guidelines, regulations, and

9
laws. Others define DHFF initiative as “the direct provision of government or
external funds to a health facility to meet the operational requirements of the health
facility”(Asian Development Bank, 2016). Direct Health Facility Financing is one of
the disbursement approaches within the health-financing component of the health
system and one of the approaches to facilitate fiscal decentralization. Evolving
evidence indicates that DHFF is linked to improvements in efficient use of resources
and promoting accountability (Kapologwe et al., 2019).
Under the DHFF initiative, funds are directly sent to the facilities instead of going
through a district council’s head office with the aim to address the delays and
misappropriation of funds that was experienced when funds were disbursed through
the district’s office. A setback of this approach is that the CHMTs are not likely to
own the disbursement process as they may feel that they have been disempowered
although upon disbursement of funds to the primary health facilities the Distict
Council also get an exchequer. This may lead to lower perfomance of the DHFF-
related interventions due to unacceptability by managers; hence, there is low fidelity
of implementation.
Given the intertwining and non–lineality of the health system building blocks (see
Figure 1) (Adam & Savigny, 2012), the DHFF initiative, although directly related to
the health financing block, is expected to impact all other blocks, such as service
delivery, human resources, and governance. DHFF is also viewed as a health sector
reform that aims to empower PHC actors by enhancing autonomy in decision making
to improve health system performance (Kapologwe et al., 2019).

10
Figure 1. Health System Building Blocks (Adam & Savigny, 2012)
Health Sector Reform
Health sector reform, defined as ‘sustained, purposeful change to improve the
efficiency, equity and effectiveness of the health sector’ (ANDREW, 1995). Reforms
have ostensibly been implemented globally to improve health system performance
(Berman & Bitran, 2011a; Shewade, 2012). Both LMICs and high income countries
are implementing different reforms and evaluations to improve effectiveness,
efficiency, accountability, responsiveness, and equity in service delivery and
coverage as a strategy to move towards the goal of UHC, particularly as addressed in
goal number three of the SDGs (Gilson & Mills, n.d.; Kruk et al., 2016; Tomson &
Biermann, 2015; WHO, 2016). The reform package for achieving UHC includes
health financing strategies particularly targeting health insurance schemes, user fee
removal or exemption, performance-based financing, and fiscal decentralization
(Kolehmainen-Aitken, 2004; Panda & Thakur, 2016). The WHO considers health
financing reforms to be important in the movement towards achieving UHC, with
such reforms influencing the intermediate UHC objectives of equity in the

11
distribution of health systems resources, efficiency, transparency, and accountability
(Kutzin, 2013; Kutzin et al., n.d.). Many on-going health financing reforms intend to
improve service delivery, especially at primary healthcare facilities given that these
facilities are critical as the gateway to health care for many and health for all.
Reforms are necessary opportunities for continuous improvement of health care
systems while paving the way for continuous evaluation of the on-going
implementation of various interventions for the better health outcome of the
population (Roberts, Reich, Hsiao, & Berman, 2002).
Tanzania, like any other LMICs, has undertaken numerous innovations and reforms
to ensure the health system delivers the best to its people through effective and
affordable approaches. Historically, the health agenda has been the main priority of
the GoT since its independence in 1961 (Semali, 2005; Massoi & Norman, 2009).
This agenda had been implemented through various trials, reforms, and evaluations
to make it responsive to people’s demand (WHO & World Bank, 2012) and has been
reaffirmed through the Tanzanian Vision 2025 document which identifies health as
sectors contributing to a higher quality livelihood for all Tanzanians (URT, 1999).
Improving services at the PHC facilities was one of the priorities after independence
(Semali, 2005). This goal first seriously conceived in 1967 and later it was
strengthened through the Decentralization Act of 1972 (Frumence et al., 2013;
Massoi & Norman, 2009) which led to construction of health posts across the
country with the aim of improving access of health care and equity to the general
public (Massoi & Norman, 2009; MOHSW, 2009). The PHC concept was cemented
by the Alma-Ata Declaration of 1978 that emphasized the importance of the ‘health
for all’ agenda (Rifkin, 2018). More than forty years later, after vigorous reviews and
evaluation, the ‘Health for All’ agenda has slightly changed and been re-affirmed in
the Astana Declaration of 2018. This declaration states that the ‘Health for All’
agenda should be a priority in all settings as the international community move
towards UHC (Walraven, 2019). In the Tanzanian context, primary health care
(PHC) is defined as ‘the essential promotive, preventive and curative health services

12
offered from the community level, Health Centers up to the district level facilities’
(URT, 2007).
Therefore, any investments that seek to promote a high performing health care
system should focus on the PHC system including their reforms and evaluations at
any given point. As the entry point to the health care system for many, primary
health facilities need to offer quality health services and must be responsive to the
people’s needs. In Tanzania, 95% of patients encounter the PHC facility before
moving to the next level (NIMR, 2010). Fortunately, the majority of countries
including Tanzania (Kress et al., 2016) are signatories to a number of international
agreements that promote primary health care, including the SDGs (UN, 2015) and
the Astana Declaration of 2018 which are essential for improvement of health care
delivery at the lower level (Rifkin, 2018; Walraven, 2019). Both agreements require
signatories to have sustainable health financing strategies and strong PHC system
that responds to the people’s needs towards achievement of UHC by 2030 (UN,
2015; WHO, 2013).
The evidence has suggested that primary health facilities need to be social enterprises
to attract patients including women to visit those health facilities when needs arises
so that they can access quality health care services (Addicott, 2011; Chang, Zangle,
& Hunter, n.d.). The ability of primary health facilities to deliver quality health
services requires sustainable and adequate financing coupled with good governance
and accountability (Wang et al., 2015; Macinko & Starfield, 2009). Moreover, PHC
systems, like many other cogs in the machinery of the health systems, should
continuously be subjected to reforms and evaluations so that they can respond to
evolving demands and needs of the general public.
The Tanzanian health sector has passed through several milestones and challenges,
which are reflected in Figure 3. The main challenge has been around health care
financing as an important health system building block. The health system in
Tanzania has not been able to sustain itself due to inadequate domestic tax funding
and over-reliance on the donor communities. In addition, inadequate collection of
user fees and community health funds, as well as delays in receipt of funds as a result

13
of long channels of disbursement have further contributed to low potential of self-
reliance (MoHCDGEC, MoH [Zanzibar], 2016). Following the Structural
Adjustment Programs (SAP) of 1993, the public sector embarked on its Health
Sector Reforms of 1994 which included, among other things, cost-sharing for select
health services which was a significant challenge for the lowest wealth quintile
(Abel-Smith & Rawal, 1992; Brunelli, 2007; Semali, 2005). The on-going litany of
reforms have all been geared towards improving Tanzania’s health sector delivery.
For example, piloting of the Community Health Fund in Igunga District (Tabora
Region) targeted people working in the informal sector so that they can afford health
care (MoHSW, 2015a). Additionally, the introduction of the National Health
Insurance Fund (NHIF) was intended for people working in the formal sector. These
schemes were institutionalised under Acts of 2001 and 1999 respectively (Kamuzora
& Gilson, 2007; Kamuzora, Maluka, Ndawi, Byskov, & Hurtig, 2013a). Another
reform was the introduction of HFGCs in 1999 as responsible for oversight of the
health facility affairs, planning and budgeting, and endorsement of requests and
transactions that are made at the health facility level (Kapologwe et al., 2019; Kessy,
2014; S. Maluka, 2017; S. Maluka et al., 2018). The communities have been
participating enthusiastically and materially towards ensuring availability and access
to health services through construction, renovation, and maintenance of health
facilities through their Health Boards and Health Facility Governing Committees.
Since the year 2000, there has been implementation of several health care reforms in
the area of health care financing. One of the areas which has undergone major
reforms is the Community Health Fund (CHF) which was revamped in 2011 by
improving the minimum benefit packages, introducing regional resource pooling
level, purcher and provider split. These reforms led to rebranding of CHF to be
called ‘improved Community Health Fund (iCHF)’ and is currently being rolled out
across the country. Under iCHF there is a separation of roles between the providers
and purchasers of the health services (Kalolo et al., 2015b; Kapologwe et al., 2017).
Another reform is the movement from input-based financing to results-based
financing. The Tanzanian RBF is a strategic program funded by the World Bank and
USAID launched as a pilot in Kishapu District Council in 2014 and since then it has
been rolled out to eight regions. The program relies on offering financial complement

14
other sources of funds in the primary health facilities based on their achievements
(MoHSW, 2014a; World Bank, 2013). Initiated as a pilot scheme in the Pwani
Region under the name “Payment for Performance (P4P)” through the support of the
Norwegian government, the program was transformed into RBF after having proven
its effectectiveness (Binyaruka et al., 2015; Borghi et al., 2015; Mayumana et al.,
2017; Olafsdottir et al., 2014). The achievements are usually obtained after quarterly
monitoring of agreed qualitative and quantitative indicators that are based on pre-
defined outputs to improve the delivery of health services (Grittner, 2013). The RBF
Program categorizes its resources for development grant for minor renovations and
constructions (75%) and incentives (25%) paid to health care providers with the dual
aim of improving provider performance and increasing utilization of maternal health
services by the local catchment population (World Bank, 2005, 2015b).
The concept of decentralization is derived from Article 8 of the Tanzanian
Constitution of 1977 that stipulates clearly that the government will derive its
mandate from the citizens. Most of the health reforms in Tanzania are in line with
decentralization processes. There have been notable success stories since re-
introduction of Decentralization by Devolution (D-by-D) policy in 1984. The re-
introduction of decentralization policy in 1984 was subsequently suspended for about
11 years following disappointing results due to circumstances such as low capacity
for resource management by the local government officials (Khaleghian, 2004;
Massoi & Norman, 2009). Financial decentralization entailed financial discretionary
powers to local councils, through a mandate to levy local taxes and the entitlement to
receive adequate unconditional and other forms of grants from the central
government. It warrants local councils to plan, budget, and spend financial resources
in the way that reflects their own priorities and complies with the national standards.
Prior to 1998, the government financed the provision of services and local
development through the Regional Administration. The enactment of the Regional
Administration Act No. 19 of 1997 reduced the role of the Regional Administration
and, as a result, some fiscal powers and service delivery functions were transferred to
Local Government Authorities. The amendment of the Local Government Finance
Act No. 9 of 1982 in 2000 redefined sources of revenue for local government
authorities.

15
The DHFF is considered as one of the financial reforms that bypasses funds to be
channeled via the district while sending money directly the health facilities. Under
this arrangemen the district council headquarters are provided with exchequer,
whenever there is disbursement of funds to PHC facilities to help in coordination and
followup. Consequently, there has been an increase in the percentage of sectoral
block grants provided to LGAs over time for education, health, agricultural, water
supply and road sectors. For instance, for the health sector there has been an increase
in spending from 2005 – 2010 (Figure 2).
Figure 2: Estimated health sector expenditures, projections and sources of
funding (million TZS).
Financial decentralization to the public primary health facilities has been the difficult
one due to fact that majority of people at the central are concerned with capacity of
those working at the lower level despite its notably significant impact in terms of
bringing autonomy, transparency, creativity and innovation to the lower levels of
health care provision (Massoi & Norman, 2009; URT, 2001). Prior to DHFF
introduction in 2017/2018, the health sector financial decentralization had just
reached the level of the district council level but not the primary health facility level.
At this level, the District Executive Director (DED) and CHMTs through the
leadership of DMO decided on spending and planning on behalf of the facilities
(Boex, 2013; Boex, Fuller, & Malik, 2015a; 2015b) . This persistent top down

16
approach contributed to delays that affected quality of service delivery at the facility
level in areas, such as availability of health commodities, and minor rehabilitation of
health facilities to improve basic amenities, hygiene, and sanitation (Figure 3). With
DHFF initiative introduction these challenges are expected to be addressed.
Under decentralization policies, it is recognised that the local communities have a
better understanding and knowledge of their local needs and challenges than national
or regional authorities. Hence, local communities are better placed to make sound
decisions and propose innovative solutions to their existing challenges. However,
this challenge is not the case if they are granted autonomy, and equipped with the
authority and capacity to identify problems, to prioritize them, and to plan/manage
all resources at their facility level (Kress et al., 2016; Tsofa, Goodman, Gilson, &
Molyneux, 2017). The community structures, like the HFGC, have the mandate to
deliver tasks on behalf of the communities and they can act as social accountability
representatives.
Boex, et al. (2015a) and MoHCDGEC (2016) both revealed that disbursement of
funds into district council accounts instead of primary health facility accounts created
a loophole for reallocation and misuse of facility funds by LGAs rather than
improving the services delivery of health facilities and frontline workers.

17
Fig
ure 3
: Tan
zan
ia H
ealth
Secto
r Milesto
nes a
nd
Refo
rm T
imelin
es from
1880s to
2019
Source: K
apolo
gw
e et al., 2017.

18
Through fiscal decentralization, primary healthcare facilities are supposed to receive
adequate resources inplanning, management,and using resources; however, many of
these facilities are often underfunded in LMICs (Panda & Thakur, 2016).
Despite an increase in funding, service delivery at public PHC facilities was poor as
evidenced through a star rating exercises of 2014/2015 and 2017/2018. The star
rating approach for primary health facilities is a method to gauge PHC system
quality. Star rating assessment is usually based on the minimum score out of four
domains [(A = Facility management and staff performance (20); B = Service charters
& accountability (30); C = Safe and conducive facilities (20); D = Quality of care &
services (30)]. Zero-star facilities are those scoring less than 20% in any one of the
four domains (Table 1) (Yahya & Mohamed, 2018). There are percentage scores
attached to each grade in order to classify facilities into five grades starting with zero
star rated to five star rated facilities. For the zero-star rating, the scores are between
zero and below 20%. For one star, the score is between 20 and less than 40%. For
two stars, the score is between 40 and less than 60%. For three stars, it is between 60
and less than 80%. For four stars, it is between 80 and less than 90%, and for five
stars, it is between 90 and 100%. The star rating is used to grade all the primary
health facilities in Tanzania (Table 1).
In 2014/2015, fewer than 2% of primary healthcare facilities (131/6,993) met the
desired quality standard of three stars or above. Just over half (51%) of all assessed
facilities were rated one-star, and about one-third were rated zero-star (34%), with
the latter category requiring urgent attention (Yahya & Mohamed, 2018). The
repeated star rating assessment exercise of 2017/2018 findings showed that 456 (6%)
of primary health facilities scored zero; 2396 (33%) scored one star; 3067 (42%)
score two stars; 1276 (18%) scored three stars; 94 (1%) scored for stars and 0
facilities scored five stars (Yahya & Mohamed, 2018).

19
Table 1: Star Rating and Grading Criteria of Primary Health Facilities
Star Status Grade Scoring Criteria
0 <20 A = Facility management and staff performance
(20)
B = Service charters & accountability (30)
C = Safe and conducive facilities (20)
D = Quality of care & services (30)
Zero-star facilities are those scoring less than
20% in any one of the four domains
1 20 -39
2 40 – 59
3 60 – 79
4 80 – 89
5 90 -100
Source: MoHSW, 2014.
In addition to these star ratings, the Service Availability and Readiness Assessment
(SARA) of 2012 and Tanzania Service Provision Assessment (TSPA) of 2015/2016
revealed that the physical condition of the health facility buildings was poor, such as
electricity, piped water, and basic amenities (Kapologwe et al., 2020; MoHSW,
2015b; Tanzania MoHSW, 2013).
Reforms in the Tanzanian Health Financing System
Direct Health Facility Financing
As a result of the above-mentioned challenges, in 2017, the GoT decided to introduce
DHFF in order to ensure flexible and timely funding at the level of service delivery
points to ensure increased efficiency in financial use, accountability, transparency,
and quality of service delivery to the public. The DHFF initiative further aligns with
global health initiatives, such as the (UHC and SDGs).
As part of the DHFF implementation arrangement, the facility is required to prepare
a budget and plan that undergoes rigorous scrutiny. Once responsible authorities
approve the plan, in this case the HFGC, spending by facilities will not be subject to
pre-approval by the District Council. There is a requisite for a certain level of
20
approval for the set financial threshold by the District Executive Director (DED). As
part of financial accountability and compliance mechanisms, all PHC facilities will
be subject to audits by the Internal Auditor General (IAG) and the National Audit
Office as per Public Act Number 11 of 2008 (Opwora, Kabare, Molyneux, &
Goodman, 2010). Training on the DHFF initiative was delivered using a cascade
approach from the national to the community level. As part of preparation to DHFF
initiative implementation, training was conducted in December 2018 with the aim
being to impart knowledge and skill sets to enable health service providers to
implement DHFF accordingly. The diagram below shows every step of the training
and the associated activities (Figure 4).
The training involved teams from Ministry of Health, Community Development,
Gender, Elderly and Children (MoHCDGEC), Ministry of Finance and Planning
(MoFP), and President’s Office-Regional Administration and Local Government
(PORALG) who took part in the masters of training exercise. It also involved
Regional Health Management Teams (RHMTs) and CHMTs. Lastly, training was
conducted with the health service providers and members of the HFGCs. It was a
three days training session that involved introduction to the DHFF initiative, roles
and responsibilities of the DHFF, financial management and issues relating to the
supportive supervision and mentorship. All these events utilized the cascade
approach depicted in Figure 4.
The introduction of the DHFF intiative was expected to affect purchasing
arrangements, because it allows facilities to make local purchases for medical
supplies, employment of casual workers, to pay for health facility operational costs
including paying electricity and water bills, minor infrastructure renovations, and to
provide community outreach services of PPHF in Tanzania. These outcomes were
shown in Kenya’s parallel intervention (Kapologwe et al., 2020; Kapologwe et al.,
2019; Opwora et al., 2010, 2015; URT, 2001).

21
Figure 4: Cascade Training on Direct Health Facility Financing (DHFF) across
Tanzania.
Source: Kapologwe et al., 2017.
Master training on DHFF
Regional Trainers of Trainers
(ToTs)
Instructions were sent to the
Local Government Authorities
on DHFF
Training to Health Facility
Governing Committee on DHFF
Health Service Providers’
Training on DHFF
Local Government Authorities
Training in DHFF

22
PPHF countries, there is increased efficiency in financial use, and there are
transparency and accountability mechanisms instituted at all levels. These should be
accompanied by utilization levels relative to need and quality of services rendered
while ensuring that there is universal financial protection to the service users (Kutzin,
2013; Murray & Frenk, 2000; WHO, 2017).
At this point, DHFF is an approach that is envisaged to set a foundation and platform
for resource mobilization, utilization, and accountability for committed resources at
the PHC facility level. Its main aim is to improve the quality of services delivered to
the people while at the same time advancing towards achieving UHC. Under the
DHFF initiative it is expected that they will be leveraging of all resources at the PHC
levels and accountability of other sources of funds which are generated locally like
the National Health Insurance Fund (NHIF), RBF, Improved Community Health
Fund (iCHF) and user fees (Kapologwe et al., 2017).
Kenya is considered to have well implemented DFF program by starting it as a pilot
intervention in some counties. The Government of Kenya through the devolved
system started to disburse the Health Sector Service Fund (HSSF) to more than 6,000
health facilities with some notable successes (Opwora et al., 2010; Waweru et al.,
2013).
The WHO considers ‘better health’ as the main objective of any health system.
Improvement of health services has two social goals: the goal of ‘goodness’, which
means the health system responds well to what people need; and the goal of
‘fairness’, which implies that the response is equal to all without discrimination
(Musgrove et al., 2000). Both concepts should lead to better health outcomes as they
create an environment for improved access to the essential services at the affordable
cost. However, achievement of goodness in the health system is better off as
compared to fairness. A health outcome is defined as a change in the health of an
individual, group of people, or population that is attributable to an intervention or
series of interventions. Outcome measures (i.e., quality of health services, morbidity,
mortality etc.) are quality and cost targets that healthcare organizations are trying to
improve (Murray & Frenk, 2000; Robone, Rice, & Smith, 2011). Therefore, it is

23
important that, health system should be robust and able to respond to the challenges
that are faced by people with intent to access services at any health delivery point.
District council health funds are usually allocated through pre-determined cost
centers namely CHMT, District Council Hospitals, Health Centers, and Dispensaries.
However, prior to the introduction of DHFF, CHMT received a larger share allowing
them to conduct some of the activities that were initially meant for frontline facilities
(Table 2) (URT, 2016).
After introduction of DHFF initiative there has been a devolution of many tasks that
were initially done by the CHMT on behalf of frontline workers. This has been
accompanied by the reduction of funds allocation from the CHMT cost center to go
to the PHC facilities where most of activities are implemented. However, CHMTs
consolidate all health facility plans and budget to a Comprehensive Council Health
Plan (CCHP) before its submission to the regional level for scruitnization. The
Comprehensive Council Health planning process is conducted at two levels; Health
Facility level and CHMT level, whereby plans from these two levels are later
consolidated to CCHP. Thereafter, the plan is presented to the CHSB, Council
Management Team (CMT), Council Social Services Committee (CSSC), Council
Finance, Administration and Planning Committee (CFAPC) and Full Council (FC)
for endorsement. After endorsement at the Full Council level the plan is submitted to
the Regional Secretariat for assessment, approval, and forwarding to national level.
At the national level, the plan is assessed by national assessors comprised of
members from PORALG-Health and MoHCDGEC and then, if approved, it is
recommended for funding (MoHSW, 2011a; URT, 2016).

24
Table 2: Allocation of funds before and after introduction of DHFF
SN Cost Centre Allocation
Before DHFF After DHFF
1 CHMT 15-20% 15 %
2 Council Hospital /Council
Designated Hospital
25-30% 20 %
3 Voluntary Agency Hospitals
(VAH)
10-15% 10 %
4 Health Centre 15-20% 25 %
5. Dispensary 20-25% 30%
The differences existing in funds allocation in the respective cost centre before and
after the introduction of the DHFF initiative have been shown in Table 2. With
resource allocation after DHFF more resources are directed to health centers and
dispensaries, with combined now both get 55% of the total allocation from the
Health Basket Fund (HBF) compared with a maximum of 45% before DHFF
introduction.
Figure 5: Funds disbursement before and after DHFF implementation.
Source: Kapologwe et al., 2017.
25
1.2 Problem Statement
Since the DHFF’s introduction in Tanzania, there has not been any attempt to
understand its effects on health system performance variables. While there is a
widespread belief that this initiative may solve challenges that exist in the PPHF,
there is no systematic evidence to substantiate this conjecture. Existing evidence on
the financial management system prior to DHFF introduction showed there were
leakage of funds in the process of disbursement to the target primary health facilities
(Boex et al., 2015b), this was coupled by insufficient decisions making at the district
level which resulted into erratic supply of health commodities and other health
system inputs that lead to poor quality of services rendered at the primary health
facilities (Kamuzora et al., 2013a; URT, 2016).
The delays and misappropriation of funds led to the compromise in the governance
and accountability mechanisms at the PHC level, and also led to poor HSR. There
has been some attempt to improve health system responsiveness through health
system reforms such implementation of RBF program that among other things
directed financial resources to the health facilities to address challenges that are
experienced at the lower level. However, these reforms have been implemented in
few (8) regions and they were not evaluated to know areas for improvement.
Moreover, there is limited evidence on the RBF program effects and how major
reforms can improve performance of health systems. This study is needed at this time
to understand whether the introduction of the DHFF initiative had any effects on the
health system performance and addressed problems that existed before its
introduction.
This study therefore evaluated both the processes after 6 months and outcomes of
DHFF 18 months after its introduction in order to understandits performance on
other health systems components. The process evaluation was conducted as it is
important for a better understanding of the ‘black box’ of the DHFF initiative and the
Fidelity of Implementation (FoI). The study also included the outcome evaluation to
understand the effects of DHFF on various indicators of health systems at PPHF in
Tanzania.
26
1.3 Objectives
1.3.1 Broad objective
To determine effects of DHFF on selected health system performance indicators
(HSR, governance and accountability, health service utilization and the structural
quality of maternal health services) and how DHFF is implemented in PPHF in
Tanzania.
1.3.2 Specific Objectives
1. To assess the level of HSR as perceived by patients attending the select PPHF
before and after DHFF implementation.
2. To assess the level of structural quality of MHS in the select PPHF before
and after DHFF implementation.
3. To assess the level of maternal health service utilization in the select PPHF
before and after DHFF implementation.
4. To measure FoI of DHFF and its potential moderators in select PPHF.
5. To measure the association between FoI and overall change of structural
quality of MHS before and after implementation of DHFF.
6. To measure the association between FoI and overall change of maternal
health service utilization in select PPHF.
7. To explore how governance and accountability of DHFF is exercised in the
select PPHF.
1.3.3 Specific Research Questions
1. What are patients’ perceptions on the level of health system responsiveness in
the PPHFselect PPHF before and after DHFF implementation?
2. What is the level of structural quality of MHS in the select PPHF before
anmaternal health service utilization in the PPHFselect PPHF before and after
DHFF implementation?
3. What is the level of FoI and its potential moderators towards DHFF
implementation?
4. What is the association existing between FoI and Structural quality?

27
5. What is the association existing between FoI and maternal health service
utilization?
6. How are governance and accountability of DHFF exercised in the PPHF?
1.4 Significance of the Study
The rationale for conducting this study is informed by the evidence that timely
funding at the level of service delivery can unlock important barriers to effective and
efficient healthcare delivery and contribute to better health outcome for the
population. There has been minimal research on the effects of DHFF on health
system performance.
DHFF is expected to improve the quality of health services including maternal health
that is crucial in Tanzania. It is expected that DHFF initiative will improve
efficiency, foster innovations. And bring more autonomy while promoting
accountability and governance structures such as HFGC.
Findings from this study may inform future designing of interventions and improve
the performance of the current initiative through use of this implementation science
experience. This may also help to strengthen the implementation research discipline
in Tanzania.
The findings may also help to re-design the DHFF initiative in this phase of the
implementation. Will also help to lay down strategies for other health system
interventions of this nature.
Therefore, this process and outcome evaluation was expected to find out the effect of
DHFF on some health system components (HSR, governance and accountability and
structural quality of MHS) and evaluated the processes and outcome by using
selected indicators for health service utilization, structural quality, responsiveness,
knowledge and practice of health service providers and HFGC members. The process
and outcome evaluation (Figure 6) were further achieved through development and
use of a Theory of Change (ToC) and application of the concept of Fidelity of
Implementation (FoI). Other researchers and policy makers who work to improve the
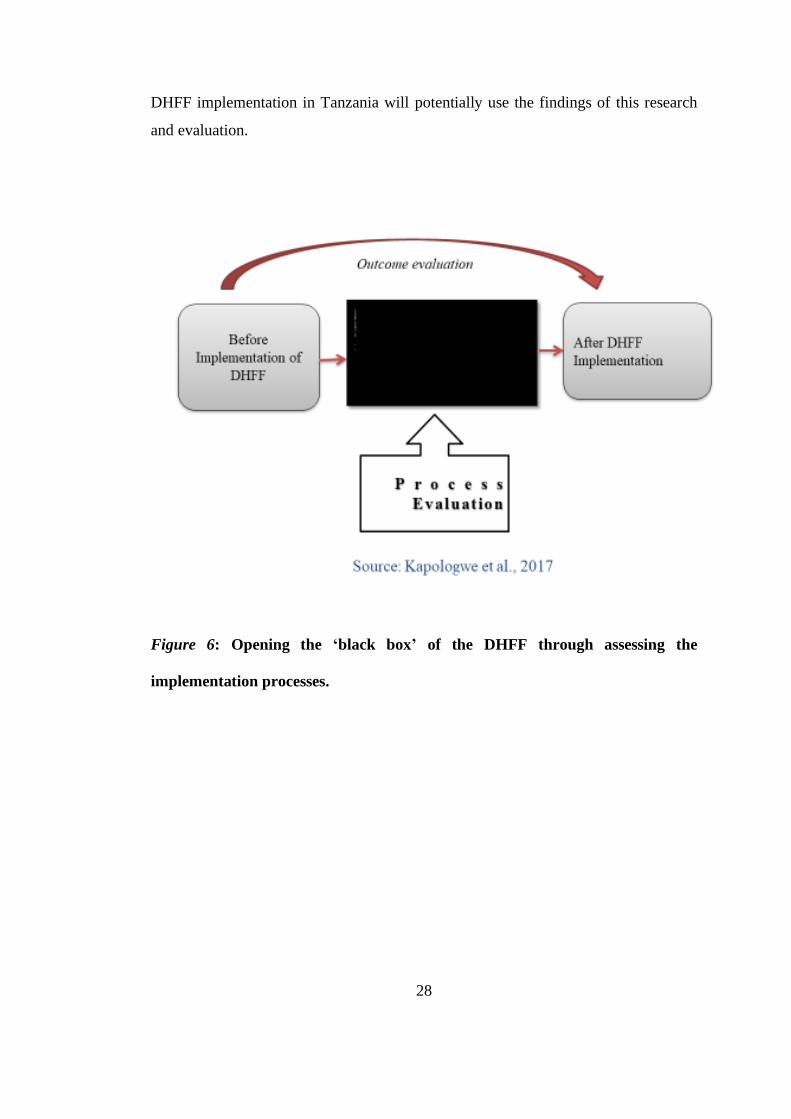
28
DHFF implementation in Tanzania will potentially use the findings of this research
and evaluation.
Figure 6: Opening the ‘black box’ of the DHFF through assessing the
implementation processes.

29
CHAPTER TWO
LITERATURE REVIEW
2.0 Overview
This chapter reviews literature relevant to this study. It starts with the presentation of
the definitions of key theories on health sector reforms and reform cycles, related
theoretical review, and empirical literature review. This chapter aims to reveal what
is known and not known on the topic globally, in Africa, and in Tanzania,
specifically. The second part provides a discussion of the two conceptual frameworks
that guided the conduct of this study, namely: the theory of change (ToC) and fidelity
of implementation (FoI) framework. Finally, the chapter presents a review of
evaluation (Process and Outcome) and a review of the current state of the
implementation of research on complex public health initiatives.
2.1 Theoretical Literature Review
In this study, two related models that help to understand health system performance
and reforms are reviewed. The two theoretical constructs (health system performance
model and health reforms model) are both integrated through the Health Reform
Cycle that has six components to show how DHFF reform was carried out (Figure 6)
(Roberts et al., 2002). These six components are:
1) Problem identification. This is an important step in the health reform process,
whereby the stakeholders identify the health sector problems that need to
have a reform solution. In this study, the main identified problem was delays
in timely disbursement of funds and misappropriation of funds that led to
poor quality health service delivery and lowered the level of autonomy
amongst frontline workers of the PHC facilities.
2) Problem diagnosis. This step enables the identification of the determinants or
causes of the identified health sector problem. To arrive at a diagnosis there
must be exploration of the control knobs that guide the performance of the
health care system. In this regard the control knobs that are used are in the
areas of: financing, payment, organization, regulation and behaviors or

30
persuasion (Roberts et al., 2002). Therefore, the DHFF initiative qualifies as a
major reform as it has incorporated all five control knobs.
3) Policy development. Under this step the health problems were diagnosed
through problem tree analysis and then reform was gauged by using control
knobs. As for this study, a policy meeting that took place in December 2016,
it was used to make resolution for the introduction of DHFF initiative as a
strategy to improve quality of health care services in the primary health
facility level in Tanzania. The performance of the Health Sector is reviewed
on annual basis under Sector Wide Approach (SWAp) by different
stakeholders. The review is conducted to determine Sector’s performance
against HSSP targets.
4) Political will and commitment. This is a critical input for addressing the
health problem or challenge. As for the introduction of DHFF initiative in
Tanzania there were series of meetings from both technical (technical
working group and annual joint technical review meeting) and political levels
(annual joint policy meeting and discussion with social services
parliamentary committee). Both sets of meetings aimed at ensuring political
decisions and commitment to the introduction of the DHFF initiative
(MOHCDGEC, 2016).
5) Implementation of the reform agenda. In this study, the reform is the DHFF
initiative that was implementated from the national to the primary health
facility level. The implementation started in 2017/2018 after the buy in from
all key stakeholders in Tanzania (Figure 4). Implementation started by
cascade training.
6) Evaluation of the implemented reform. Through this stage, we come to
understand how the outcome of interest changes over time. Moreover, this
stage helps to monitor progress of an initiative and also provides room for
modification while exploring necessary factors for sustainability (Roberts et
al., 2002). In this study, baseline and endline cross-sectional studies were
conducted to evaluate the effect of the DHFF on select health system areas. A
midline/midpoint study was done to evaluate processes and also the FoI of

31
DHFF to get a better understanding on how the initiative evolved over a
period of time (Kapologwe et al., 2019).
Figure 7: The health reform cycle (modified from Roberts et al., 2002)
In the next section, a review of theories (health system performance model and
health reforms model) used in this study and their relationship to the health reform
cycle is profferred.
2.1.1 Health System Performance Model (HSPM)
The health system performance model (HSPM) helps to identify the causes of poor
performance of any project/program or an approach and to propose policy changes to
improve performance (Berman & Bitran, 2011a). The HSPM is presented in the four
blocks of Figure 8 with each block is representing control knobs in health system
performance. Reading fromleft to right, the left-most positioned block contains
categories of ultimate and intermediate outcomes that are often used to measure
health system performance. Based on these measures, analysts assess performance
1. Problem identification
4. Political decision -
making
5. Implementation of
DHFF
6. Evaluation
(Process & Outcome)
2. Problem diagnosis
by using control
knobs
3. Policy
development and
resolution on DHFF

32
and identify problems (i.e., poor performance) that must be addressed by health
reforms of an organization or within thepublic sector. The second and third blocks
from the left portrays the analysis of the causes of health system performance and the
formulation of hypotheses. The fourth block focuses mainly on the policy
interventions which are necessary to improve health system performances through
implementation of each control knob, particularly, financing, payment, organization,
regulation and persuasions (FPORP). This DHFF initiative was approved during the
policy meeting of December 2016, and then started its implementation in 2017/2018.
This reform qualifies as major health financing reform as it has all five control
knobs. The model identifies more than one of these control knobs (health financing,
payment, organization, regulation and persuasion) as drivers in achieving major
reforms and performance of health sector of a state (Figure 8) (Berman & Bitran,
2011a).
2.1.2 Health System Reforms Model (HSRM)
Health system reforms are important for any growing health sector that is expected to
meet the people’s expectations. Direct Health Facility Financing is one of the health
financing reforms to be implemented in Tanzania, makes the health systems reform
model important for conceptualizing this study. The process and outcome study of
DHFF used the HSRM to gauge the magnitude of this health reform in which it
qualified as a big ‘R’.

33
Figure 8: Health System Performance Model (Berman & Bitran, 2011a)
Health system control knobs are things ‘that can be adjusted by government action.
And those adjustments or changes in the control knob must be significant causal
determinants of health system performance’(Roberts et al., 2002). Control knobs
describe the discrete areas of health system structures and functions that matter
significantly for health system performance and are subject to change as part of
health system reform.
Looking at the items in the Control Knob Blocks in Figure 8,
1. The financing knob determines the resources which are available to run the
health care system particulary in the primary health facilities. For this study,
funds came from health basket fund, block grants, national health insurance
funds, council own source and improved community health fund (iCHF).
2. The payment knob determines resources that are available to providers. As
for this study, payment knob referred to payments made by Ministry of
Finance and Planning (MoFP) directly to the primary health facilities.
3. The organization knob determines the kinds of provider organizations that
exist and their internal structures that shape how these organizations perform.
In this study, the organizational structures that are responsible for

34
implementation of DHFF are CHMT, CHSB, Health Facility Management
Teams (HFMT) and HFGC.
4. The regulation knob imposes constraints on desired behaviors to allow the
health system to perform. In this study we used circulars, standard operating
procedures and guidelines to implement the DHFF initiative. Direct Health
Facility Financing is governed by existing laws and legal framework present
in Tanzania, including the Constitution of 1977, Budget Act 2015 and its
regulations, annual budget guidelines, Public Procurement Act of 2011 (as
amended 2016) and its regulations of 2013, Local Government Authorities
Tender Board (Establishment and Proceedings Regulations, 2018, Local
Government Finances Act, 1982 (as amended in 2017), Local Government
Financial memorandum of 2009.
5. Finally, the efforts to change behavior knob influences how individuals
respond to health sector organizations, which, in turn, shapes the
opportunities that organizations confront (Roberts et al., 2002). In this study
that was checked through measuring process evaluation by using fidelity of
implementation framework of the DHFF implementers.
The analysis of introduction of DHFF initiative as the health financing reform shows
that; all five control knobs are key components of the DHFF initiative making it a
major reform and also helped in assessing the effects of the DHFF initiative on HSR,
governance, and accountability, and structural quality of MHS in Tanzania.
Hsiao (2000) reform models categorises reforms into two types i.e. ‘R’ and small ‘r’,
and explains that; big “R” reforms are those that are derived from strategic,
purposeful reform programs that introduced change in two or more of the control
knobs, thus affecting health system performance across several parts of the health
system. On the other hand, small “r” reforms may still be strategic and purposeful,
but are more narrowly focused on only one control knob and only one part of the
system (International Health System Group- Harvard School of Public Health, 2000).
Given these definitions, this study examined big “R” reform to explain DHFF
reforms because it touches more than one control knobs. This research studied issues
of current health financing modalities and payment mechanisms used in DHFF

35
initiative. The issues studied included: organizations benefiting from DHFF,
specifically the PPHF, compliance with regulations governing the operation of
DHFF, and behaviours of the health service providers towards DHFF implementation
since its introduction. The success of many reforms depends on the context, design,
policy and fidelity of implementation.
2.1.3 Fidelity of Implementation (FoI)
All policies/programs/initiatives around the globe have a higher likelihood of being
successful and impactful if they are implemented with fidelity (i.e. faithful to the
design). The concept of fidelity has been used to gauge the level of performance
against the design of the initiative and its intended modus operandi (mode of
operation).
Implementation fidelity refers to “the degree to which an intervention or program is
delivered as intended” (Carroll et al., 2007). Only by understanding and measuring
whether an intervention has been implemented with fidelity can researchers and
practitioners gain a better understanding of how and why an intervention works, and
the extent to which health outcomes improved. It is therefore important that fidelity
is measured for any implemented project or program (Carroll et al., 2007). Carroll et
al. (2007) developed a conceptual framework to measure the FoI by allocating a
score based on the adherence to the proposed intervention. The adherence is
understood as all those practices or actions that comply with the set standards.
However, within this conceptualisation of FoI, adherence is defined as whether "a
program service or intervention is being delivered as it was designed or written"
(Mihalic, 2002).
Implementation fidelity helps to establish the relationship between interventions and
their intended outcomes (Carroll et al., 2007). Evaluation of implementation fidelity
is important because this variable may not only moderate the relationship between an
intervention and its outcomes, but may prevent potential false conclusions from
being drawn about an intervention’s effectiveness. Fidelity of any program can be
assessed by conducting a process evaluation (Mihalic, 2002).

36
The concept of fidelity of implementation is currently described and defined in
terms of five elements, namely: adherence to intervention, exposure, quality of
delivery, participant responsiveness, and programme differentiation (Compaoré,
Yameogo, Millogo, Tougri, & Kouanda, 2017; Dusenbury, Brannigan, Falco, &
Hansen, 2003; Kalolo, Radermacher, Stoermer, Meshack, & De Allegri, 2015).
However, according to Carroll et al (2007), adherence is considered to be the
cornerstone to FoI measurement. A policy becomes successful if it adheres to content
and frequency, duration, and coverage, which are collectively grouped as ‘dose’
(Carroll et al., 2007). The content of an intervention is considered as skill sets and
the knowledge that the participants have to deliver the prescribed task.
The score of implementation fidelity can be obtained through measurement of the
adherence to the task that is related to the delivarence of outcomes of interest. Keith
et al. (2010) added contextual factors to other factors presented previously by Carroll
et al. (2007) and it has shown to be influencing the fidelity of implementation of the
programme and its outcomes (Keith et al., 2010). Implementation also offered
multiple insights into contextual factors affecting sustainability of program
implementation (Ojemeni et al., 2017). Despite being a relatively new study area in
Tanzania, there has been an increased interest in measuring FoI of different
initiatives, projects, and program in Tanzania (Mmari et al., 2019).
2.1.4 Fidelity of Implementation (Adherence)
According to Carrol et al (2007), adherence tends to measure who receives an
intervention, and the frequency and magnitude (size) of the given intervention
(Carroll et al., 2007). In this regard, adherence of any initiative can be measured by
looking at how the implementers are abiding to the design while at the same time
looking for amount of dose given and duration with which it was offered.
Adherence to the implementation of the programs or initiatives varies considerably
from one place to the other depending on the quality of delivery which depends on
the awareness and level of knowledge of the implementers (Hasson, 2010; Toomey,
Matthews, & Hurley, 2017). For the DHFF inititative the dose was considered as
funds that are disbursed from Ministry of Finance and Planning to the public primary
37
health facilities across the country. These funds are disbursed through use of
allocative efficiency formular by taking into account the issue of equity for district
councils and public primary health facilities. Therefore, resource allocation formular
takes into account several factors depending on whether is a district council or a
public primary health facility. For district council the following factors are put into
considerations which are: Population (60%): Funds are distributed in proportion to
the population of each district council by 60%; Poverty (10%): Councils receive
additional resources for the special needs of a poor population (10% of the grant
resources); Under-five mortality (10%): The 10% of resources are earmarked to
places with high burden of diseases; the under-five mortality (U5M) is considered as
an appropriate proxy for burden of diseases; Capped land factor (20%): The formula
recognizes the higher expenditure needs of rural areas by directing 20% for the route
mileage regularly travelled by health sector vehicles within their locality and to and
from the district council head office; For that case this formula takes into
consideration the issue of higher operational cost of delivering health services to a
rural population and to sparsely populated areas within Tanzania; this formula also
includes health commodities distribution costs.
Allocation ceiling for Dispensaries and Health centres (30% and 25% respectively) is
combined to provide a pool for lower level health facilities. Parameters used for
allocating the pooled Health Sector Basket Fund and Health Block Grant to health
facilities includes; Catchment Population (40%): Takes into account the population
expected to be served by the Health facility; Distance of the individual
Dispensary/Health Centre to the Council’s headquarter (10%): It is important in
budgeting funds to be used for referral, and logistics requiring health facility staff to
travel to head quarters; Service utilization (40%): Takes into consideration the
intention to improve quality of services. It is measured by a composite indicator, the
“Care unit”; that measures service outputs. The composite indicator consists of six
indicators and is calculated using DHIS2 data as total of (number of attendances x
weight). The six indicators and their weights are: Outpatient attendances – 01,
Antenatal attendances – 01, Institutional deliveries – 06, Postnatal attendances – 01,
Admissions – 10, C-sections – 27; Performance (10%): Takes into account facility’s
contribution towards LGAs performance. It is calculated based on two indicators

38
(use of modern family planning methods and availability of 30 tracer medicine)
using DHIS2 data. Each of the two indicators weight 0.5; Modern Family Planning
users are calculated as percentage of total Family Planning users of public Health
Centres and dispensaries.
On the other hand, duration of funds disbursement from the Ministry of Finance and
Planning to the public primary health facilities is done on quarterly basis for all
health facilities. Therefore, this study focused mainly on the quality of delivery by
looking into the level of knowledge (content), participation of HFGCs and
availability of working tools where as for fidelity of implementation of DHFF, this
study focused mainly on the adherence to the implementation design as dose and
duration was the same for all public primary health facilities.
2.1.5 Participants’ Responsiveness towards DHFF implementation
Several studies have tried to define participant responsiveness. Following review of
13 studies, Schaap et al. (2018) defined participant responsiveness as ‘satisfaction,
appreciation, acceptability, or enjoyment of the programme’ (Schaap, Bessems,
Otten, Kremers, & van Nassau, 2018).
Participant responsiveness is achieved when those who have been assigned to deliver
a certain initiative, deliver it with passion and enthusiasm thereby achieving high
fidelity (Dusenbury et al., 2003; Hasson, 2010). In this DHFF study, participants
were defined to be the health service providers and members of health facility
governing committee (Kapologwe et al., 2019).
Quality of Delivery
Quality of delivery is an important component of the FoI and reflects the way in
which an initiative was delivered according to the set protocols. For this study, the
quality of delivery was assessed by looking into the level of knowledge (content) of
health care workers, participation of HFGCs in decision making processes and
planning and budgeting and availability of working tools especially financial
management tools which are necessary for the implementation of DHFF initiative.
39
Program Differentiation
Program differentiation is ‘the degree to which the critical components of a program
are distinguishable from each other and from other programs’(Dusenbury,
Brannigan, Falco, & Hansen, 2003). Program differentiation can also be referred to
as the process of identifying the critical components of a program that are essential
for producing positive outcomes (Dusenbury, Brannigan, Falco, & Hansen, 2003),
which essentially discriminates between successful and unsuccessful programs. For
this study, the program differentiation was achieved through supportive supervision
and mentorship and also through participator decision making processes by
expanding decision making space.
Strengths of Implementation Fidelity in Initiative Management
Fidelity of Implementation (FoI) helps to measure how an implementation of an
initiative or intervention was achieved and its relationship to the outcomes of interest
(Hulleman & Cordray, 2009; Mowbray, Holter, Gregory, & Bybee, 2003), and
increase external validity of tools that are used for data collection (Stains & Vickrey,
2017). In other words, using FoI improves causal pathway of the program
implementation and its anticipated outcomes while identifying predictors for the
initiative’s success (Donnell, 2015). Stains and Vickrye (2017) outlined that, through
use of FoI, one can improve empirical and descriptive evidences of how and under
what circumstances the program can lead to the anticipated results. It is not easy to
establish the adherence of the program implementation if we do not monitor its
performance. However, it is difficult to establish whether failure to achieve the
outcomes reflects a failure of the model or failure to implement the model as
intended (Carroll et al., 2007; Linda Dusenbury et al., 2003; Mowbray et al., 2003).
2.1.6 Context and Description of DHFF Implementation in Tanzania
The DHFF initiative was launched in 2017/2018; however, actual disbursement and
receipt of funds to the public primary health facilities started in February 2018 across
all 184 district councils of Tanzania mainland. The DHFF initiative was a
government approach to facilitate financial decentralization in the health sector with

40
the aim to improve the quality of health service delivery and autonomy at the public
primary health facilities. Some of the DHFF essential implementation activities
included: 1) training about the program; 2) supportive supervision and mentorship; 3)
employment of assistant accountants; 4) dissemination of facility financing
accounting and reporting systems (FFARS) and guidelines; and 5) opening of bank
accounts that are approved by the BoT. The Regional Health Management Team
(RHMT) and CHMT where mandated to provide technical support and mentorship
on financial management, implementation of annual plans and budget to the health
facilities in accordance with the guidelines.
This study was conducted in PHC facilities (i.e., health centers and dispensaries) and
communities through HFGC as their representative. In Tanzania, health centers are
expected to have mixed set of skilled staff (i.e., doctors, nurses, assistant
accountants) from 39 to 52 workers. At the dispensary level, there is a range of 15 to
20 staff. The introduction of DHFF targeted these facilities to increase efficiency and
accountability and to improve health services provision. Finally, other moderating
factors were supportive supervision and mentorship, inclusiveness in decision-
making, functionality of HFGCs, and operation of BoT approved bank accounts. The
resource allocation for the public primary health facilities considers workload
(Service utilization 70% and health system performance 30%). As for Health centres
and Dispensaries, Service utilization are factored into six indicators (Outpatient
attendances (1), Antenatal attendances (1), Deliveries (6), Postnatal attendances (1),
Admissions (10) and C-section (27). Where as for the Council Hospital performance
are calculated on availability of 30 tracer medicines (0.5) and modern family
planning use (0.5).

41
Figure 9: Direct Health Facility Financing Management Framework
Link between theoretical frameworks and the study
In this study the expected effects of DHFF outcomes are:
1. Provision of structurally quality MHS;
2. Increased HFGC accountability and governance;
3. Increased HSR as perceived in the patient’s experience; and
4. Increased maternal health service utilization.
2.1.7 Implementation Research
Peters et al. (2013) define implementation research as “scientific inquiry into
questions concerning implementation, i.e., the act of carrying an intention into effect
which in health research can be policies, programs or individual practices
(collectively called interventions)”(Peters et al., 2013). The intent is to understand
42
what, why, and how an intervention works in real world settings and to test
approaches to improve it.
Health systems are complex in nature as their blocks are intertwined in nature, so
they need a clear and robust approach in dealing with its evaluations so that to get
clear picture of its processes and outcome of implementation of an initiative or
reform (Adam & Savigny, 2012; Moore, Audrey, Barker, & Bond, 2014). The
interventions that comprise multiple components like the DHFF initiative are
considered as complex interventions and needs holistic and robust approaches to be
successfully evaluated (Moore et al., 2014). Therefore, any design for the evaluation
of any intervention need a good crafting so that they can give results for initiative in
quest. The learnings from such applications are potentially transferrable to other
settings and may contribute to project sustainability. Through use of the FoI
framework, complex interventions will benefit from a rigorous process evaluation
that will enable the opening of a black box. The opening of the black box helps to
understand how the DHFF was implemented in the public primary health facilities.
The essence of the process evaluation is to explore the quality and quantity of the
project implemented and why and how. The inclusion of a process evaluation adds a
measure of accountability and integrity for an organization and individuals
participating in the implementation of the intervention (Moore et al., 2014).
Implementation research uses theories to conceptualize the ideas, therefore applying
a theory is an important component of any health system implementation research
(Brousselle & Champagne, 2011; Rogers, 2008). Theory application of any
intervention usually presents an important step in conducting a robust theory driven
implementation research. A theory of intervention refers to causal pathways through
which change is produced as a result of intervention strategies and implementation
actions (Rogers, 2008). The use of the theory of intervention helps to guide to test
evaluation questions in the course of conducting evaluations.
This study is an example of implementation research, as it studies the effects of an
ongoing initiative relatively recent implementation. Implementation research studies
aim to get a better understanding on what, why, and how an initiative like DHFF
works under normal conditions rather than trying to maneuver or controlling these

43
conditions or remove their influences as a cause and effect (Peters et al., 2013).
According to Peters et al. (2013), some of the studied variables under
implementation research are: fidelity, acceptability, sustainability, and coverage. As
implementation research tends to be conducted in the real world, studying health
systems which are complex in nature align with this approach (Peters et al., 2013).
As the introduction of DHFF has the potential to affect various health systems
building blocks, implementation research is an appropriate method to study the
effects of DHFF initiative on other health system building blocks and the complexity
of the system as a whole.
2.1.8 Evaluation of Health Inteventions or Programs
There have been many approaches that are used to classify different types of
evaluation (Sun, Ahn, Lievens, & Zeng, 2017; WHO, 2012). However, the common
types of evaluation are: (1) formative evaluation - used during the development of
new modification of an existing program; (2) process evaluation that be used to
measure if an initiative in implemented as per design or as per intent; (3) outcome
evaluation - can be used to measure the effect of an initiative or program to the
population in question; and (4) impact evaluation - used to assess whether the
initiative or program is effective enough to attain the ultimate goal.
Globally many studies have focused on the outcomes of an intervention but ignore
the processes that can explain the how and why for the outcomes. The importance of
investing in both the process and the outcome evaluation, it helps to know how the
initiatives are emplemented and the effects evolved from an initiative (Moore et al.,
2014; Nielsen & Randall, 2013). Outcome evaluations do not offer an opportunity to
open the “black box” of an initiative or program hence leading to constrained
knowledge on how the effect of the program or an initiative came into being
(Harachi, Abbott, Catalano, Haggerty, & Fleming, 1999; Nielsen & Randall, 2013).
Having the right frameworks for evaluation can uncover whether an initiative has
failed due to design or due to implementation (Carroll et al., 2007a; Harachi, 1999;
Health, Rychetnik, & Building, 2006; Patton, 2008).

44
The UK Medical Research Council (MRC) defines process evaluation as an
evaluation study that aims to understand the functioning of an intervention by
examining implementation processes, mechanisms of impact, and contextual factors
(Moore et al., 2014). There are several benefits of conducting implementation
process assessments. Four things that make assessment of the implementation
process beneficial are: 1) assists with interprtaton of the outcomes of the
intervention; 2) provides feedback that can help to improve intervention
improvement; 3) helps to replicate an intervention to other settings; and 4) it helps to
appraise the generalizability and the transferability of the intervention (Nielsen &
Randall, 2013).
For the process evaluation focusing on a FoI framework (which mainly focuses on
whether a project is implemented as per design), it can offer more information on the
outcome of interest, as FoI tends to mediate outcomes (Carroll et al., 2007; Hasson,
2010). Process evaluations that use the FoI framework can help to avoid type-III
errors, which falsely occurs due to lack of effect of a given measure to the
intervention rather than due to weaknesses in the course of its implementation
(Carroll et al., 2007; Hasson, 2010)
Research and evaluation contribute to the improvement of health services of the
general population (CDC, 2011). Globally, most countries have been implementing a
number of reforms, projects, and programs with the aim of improving health care
services. However, many organizations or institutions fail to conduct evaluations of
performance of such initiatives (WHO, 2010). Conducting an evaluation of the
initiative or program helps in measuring the performance and also tracks progress of
the implementation, while enhancing the accountability of the said implemented
initiative (Frieden, 2014; Lindeman, 2014; Nielsen & Randall, 2013).
A monitoring and evaluation framework is important when starting a new initiative
or program as it helps in the monitoring of progress towards the set targets or goals
and also offers room for the improvement of the program as it gives necessary
feedback to the decision makers and implementers.
45
2.2 Empirical Review
Most countries are striving to make sure that public sector systems are both effective
and responsive to the peoples’ need. This effort explains why there are a number of
innovations and reforms emerging and being implemented with the aim of improving
improve health service delivery to the public. Most of these reforms aim at
empowering people who are residing at the community level or empowering workers
who are working at the grassroots level. A frequent approach, which has met with
varying levels of success, has been decentralization policy which purport to bring
more autonomy to the lower levels of government and the communities at large.
The empirical review shares findings on the situation of implementation of various
form of reforms on health financing globally and regionally. Also help to understand
essential factors that are necessary for successful implementation of any reform in
any given settings. Thi section will mainly focus on situation of health financing,
HSR, Structural quality of maternal health services, maternal health service
utilization, fidelity of implementation and governance and accountability.
2.2.1 Situation of Health Care Financing Reforms
Health financing reforms are an important ingredient for achievement of UHC by
improving equity and access to the health services. The WHO acknowledges that, in
order to make progress towards achieving UHC, countries should embrace health
financing reforms through development of their national health financing strategies
(Kutzin, 2013). It is important to invest in health financing reforms as health
financing influences achievement of the intermediate objectives of UHC of equity in
distribution of health systems resources, efficiency, transparency, and accountability
(Kutzin, 2013; Kutzin et al., n.d.). WHO has defined three specific functions of a
health financing system, specifically revenue collection, pooling, and purchasing,
each of which may require definition of a reform strategy (Figure 10).

46
-
Figure 10: Health Financing Arrangement, Intermediate Objectives and UHC
goals (WHO, 2013).
The DHFF initiative, being a health financing reform, aligns well with the WHO’s
agenda of health financing reform as it encompasses all three specific functions of
health financing arrangement as seen in the Figure 10. It is also highlighted in the
SDG number three, under target 3c which states that “Substantially increase health
financing and the recruitment, development, training, and retention of the health
workforce in developing countries, especially in the least developed countries and
Small Island Developing States” (UN, 2015).
In SSA, there has been several policy decentralisations which are implemented in
different settings, however very few of these decentralizations is on financial
decentralization. For example, Kenya has been implementing financial
decentralization through local governments since 2008 (Opwora, Kabare, Molyneux,
& Goodman, 2009). The pilot phase was followed by a scale up at the the county
level through devolved government functions. Studies conducted in Kenya have
shown some improvement in terms of financial management and autonomy, quality

47
of health care, health worker staff motivation, and patient satisfaction (Waweru,
Molyneux, Goodman, & Tsofa, 2016). Urban facilities reported water, sanitation
(toilets and cleaners) and minor renovations as their most important uses of funds,
while rural facilities named casual labourers, essential drugs, food, and referrals
(Goodman, Waweru, Kedenge, Tsofa, & Molyneux, 2010; Opwora et al., 2009).
As part of the decentralization process, Ghana has been channelling funds to the
district through regions (Kolehmainen-Aitken, 2004).
The Decentralization by Devolution (D-by-D) policy implementation in the health
sector of Tanzania started in 1970s and was strengthened in the 1990s.
Implementation of these reforms laid foundation for the health sector reforms of
1994 which substantially altered health system financing mechanisms through re-
introduction of cost sharing, soon after initiation of the adjusted structural program
(Frumence et al., 2013; Maluka & Bukagile, 2016; URT, 1999). Under this D-by-D
policy and reform, powers to manage health services delivery at the council level
were devolved to Local Government Authorities (LGAs) and CHMTs. Thus CHMTs
became responsible for budgeting and planning, conducting supportive supervision
and mentorship to the lower level health facilities, and facilitating administrative
activities of the primary health facilities within their jurisdiction (MOHCDGEC
2017).
Under the D-by-D policy implementation, there were still some challenges. These
included: a top-down approach in management on different issues that denied the
frontline workers from exercising their full roles and responsibilities; delays in
disbursement of funds to the PHC facilities from CHMTs; the misappropriation of
some funds; and delays in distribution of medicines and supplies to reach health
facilities (Boex et al., 2015b). Other challenges were inadequate funding, delayed
disbursement from central government, insufficient and unqualified personnel at the
PHC level, and lack of community participation in the budgeting and planning
process. Of all the D-by-D policy achievements, health financing decentralization
has been the most difficult to implement due to worries around capacities and
accountability at the lower level (Fjeldstad, 2001; Panda & Thakur, 2016).
48
2.2.2 Implementation of DHFF initiative in Tanzania
The idea for the DHFF initiative originated from the Joint Annual Health Sector
Planning meeting of December 2016, where participants passed a resolution on the
introduction of DHFF in Tanzania. The decision was based on positive results from
the Results Based Financing that was being implemented in eight regions
(Kapologwe, et al., 2019; Maluka, et al., 2018; World Bank, 2013), as well as
experience from the Ministry of Education and Vocational Training of Tanzania,
that had started to send money directly to the both primary and secondary schools
(Komba, 2012). However, Kenya which is neighbouring Tanzania started
implementation this approach as a pilot intervention in 2008 (Opwora et al., 2009).
Some of the challenges that led to the introduction of DHFF in Tanzania were delays
in disbursement of funds; weak planning and budgeting activities by primary health
facilities; weak supportive supervision and mentorship; failure to carry out minor
renovation; and erratic supply of health commodities and supplies. The detailed
explanations of each challenge are in the following sections.
2.2.2.1 Delays in Disbursement of Funds
Several reports were issued on the delays of the funds reaching the frontline health
facilities challenging expenditures for important health activities (Boex et al.,
2015b). Delays in fund disbursement were observed by World Bank officials when
they were conducting fiduciary system assessments, with showed funds being
delayed up to 16 days enroute to the LGAs. This delay was amplified when it came
to availability of funds at the health facilities level as they were disbursed by LGAs
(World Bank, 2015). In most cases facilities that missed resources for some time
became reliant on other internal sources, such as Community Health Fund (CHF),
National Health Insurance Fund (NHIF) and user fees, to run services at the primary
health facility. Also, the burden for access to medical commodities was transferred to
district hospital where most of the primary health facilities went for support. All
these issues caused unnecessary referrals and poor service delivery at primary health
facilities (Boex et al., 2015b).

49
Figure 11 shows how funds were disbursed from the Ministry of Finance to the
respective health care facilities prior to the introduction of DHFF.
Figure 11: Direct Health Facility Financing (DHFF) Funds Flow and
Stakeholders Relationship in Tanzania (Kapologwe. et al., 2020).
2.2.2.2 Weaknesses in Planning and Budgeting of Activities
This was the common challenge that was presented at the PPHF as they were relying
on the CHMTs for the financial resources to implement their plans and budgets
(Boex et al., 2015b, 2015a; URT, 2016). This made implementation of budget and
plans very difficult. Some prior studies revealed poor accountability in terms of
budget transparency during implementation by the community and involved
individuals, with Tanzania scoring 15 out of 100 points on accountability

50
(International Budget Partnership, 2018). Other reports went further to explain the
minimal engagement of community in decision making especially in terms of the
governance structures like health facility governance committees that endorse
resource use and provide checks and balances (Frumence et al., 2013; Odd-Helge
Fjeldstad, 2010; World Bank, 2015). Community involvement, planning, and
budgeting are considered very important pillars of the DHFF implementation.
2.2.2.3 Weak Supportive Supervision and Mentorship
Supportive supervision from higher to the lower levels is part of health system
governance, as well as supervision within each level, is very important for ensuring
that there is constant provision of quality health services at the primary health care
facility. According to a report from the United Republic of Tanzania - MoHCDGEC
(2016) there was a slight drop of quality of cascade supervision from 64% in 2012/13
to 54% in 2014/15 among LGAs despite the fact that it was noted decrease in the
cost per supportive supervision. Through this cascade supervision superior health
facility is enabled to supervise other facilities in their catchment areas while adhered
to the standards and guidelines. Within the Tanzanian health system, it is expected
that health centers should be able to supervise the satellite dispensaries that are
within the locus or catchment area. With this approach capacities of people at the
health centers to supervise others are built, but, at the same time, it saves costs as the
distance between the supervisor and supervisee is reduce significantly (Olafsdottir et
al., 2014).
2.2.2.4 Failure to Maintain Buildings and Supply Chain of Medicines and
Supplies
Despite funds being disbursed to the district councils, there were a number of minor
activities like maintenance and renovations of infrastructure that were left
unattended. Also there was an erratic supply of medicines and other supplies due to
the inadequate funds being disbursed to the frontline facilities due to delays or
inadequate funding from the district level (Kapologwe et al., 2014; Wiedenmayer et
al., 2015; Wiedenmayer et al., 2019). This problem was also evident in Kenya prior
to the introduction of DHFF (Opwora et al., 2009).

51
2.2.3 HSR in PPHF
Health system responsiveness implies the existence of favourable environment that
promotes health seeking behaviours among people, improves transparency and
communication between heath care providers and users, and ensures adaptation to
quality health information (Njeru, Blystad, Nyamongo, & Fylkesnes, 2009).
This research adapted the domains of HSR as proposed by WHO and various studies
including those done by Mohammadi & Koorosh (2014), Murray & Frenk (2000),
and Njeru, et al., (2009) in measuring responsiveness in PPHF (Kapologwe et al.,
2020). Following a baseline study on HSR, it was found out that several domains did
not performed well some of them are access to care which had a percentage mean
scores of 50% while the overall baseline HSR was 69.1% (Kapologwe et al., 2020).
2.2.4 Structural Quality of MHS
Structural quality is an important aspect of the quality delivery of health services in
any health care system. Donabedian identified and proposed three quality
components for provision of quality of health services in any settings (Donabedian,
1973). Those components areprocesses, structures and outcome (Rourke, 1957;
Westaway, Rheeder, Van Zyl, & Seager, 2003). In the Donabedian model, the
process component examines the process of health care delivery which is an
important component during process evaluation in order to open up the black box
(Gilson & Mills, n.d.; Moore et al., 2014; Westaway et al., 2003). While the outcome
component helps to measure the health care outcomes, some researchers have
criticized this element as it does note independently reveal/explain the processes
which happen between the quality of care delivery and the outcomes (Vesel et al.,
2013; Waiswa et al., 2017). Looking into structure as the third component of the
Donabedian model, we see this component used to assess the infrastructure, medical
equipment, staffing level, and other health commodities. However, Many scholars
considers it, although it has some deficiencies in the sense that it cannot give an
attribution between the quality due to structure and the outcome in the certain
settings (Donabedian, 1973; Khamis & Njau, 2014; Westaway et al., 2003).
52
Tanzania like any other country in sub–Saharan Africa has been trying to improve
the quality of health service delivery to its people through implementation of number
of reforms like star rating program and big results now initiative. In 2012, Tanzania
through the MoHSW came up with the Quality Improvement Framework (2011 -
2016). The aim of this framework is to ensure that there is quality of health services
rendered to the people at each and every level of health care system in the country
(MOHSW, 2009). The publication of the quality improvement framework was
followed by the Service. Availability and Readiness Assessment (SARA) that was
conducted in the 2012. However, some of the shortfalls of this exercise dwelled on
just the assessment of physical status of infrastructure (structure) and never went into
assessing the relationship between the structural quality and processes and the health
outcome (Tanzania MoHSW, 2013). This was rectified by the Service Provision
Assessment (SPA) survey in 2015 which measured the effect of structural quality
and the processes (Kapologwe et al., 2020; MoHSW, 2015b). Both studies revealed
that there was poor quality of services rendered to the people who visit the health
facilities. In Tanzania more than 95% of people reside within 10 kilometres of public
primary health care facilities and more than 90% of people used primary health care
facilities as their first choice when entering the health care system (MoHSW, 2011b;
NIMR, 2010).
Furthermore, the majority of quality improvement interventions were done at the
national, zonal, and regional referral hospitals and less was done to address the
quality challenges at the primary health care levels (MOHSW, 2009; Shoo, Mboera,
Ndeki, & Munishi, 2017). As a result, it became evident that investment at the
primary health care level is vital for the better health outcomes of the majority of
people. Studying the effect of DHFF on the structural quality of MHS is important
because a study in five countries in SSA showed that quality of MHS was found to
be poor in PHC facilities regardless of the efforts which has been put by both
international and country’s effort to improve the MHS (Kruk et al., 2016).
53
2.2.5 Maternal Health Service Utilization
Health service utilization is referring to extent to which people or their
accompanying significant others are accessing and making use of health services that
are available in their communities within and outside their catchment population.
This can be either through admission or through use of the outpatient services.
Service utilization is one of the pre-requisites of any highly working and performing
health care system in any given setting. It can be considered as an important indicator
of performance of system or proxy indicator for quality of health services provision
and HSR by patients. There have been several studies conducted with the aim to
assess health services after the introduction of a certain interventions with some
notable successes (Ojemeni et al., 2017; Ramsey et al., 2013).
There have been several efforts put in place with the aim to improve the service
utilization in several countries around the globe and in Africa at large (Akowuah,
Agyei-Baffour, & Awunyo-Vitor, 2018; Basinga et al., 2011). Tanzania is not
exceptional to other African countries; it has also been trying initiatives that are
geared towards improving the health service utilization, particularly at the PHC level.
One of the programs that were initiated in Tanzania is the payment for performance
(P4P) scheme that started in Pwani region as a pilot in 2011 with the aim to improve
health service delivery by offering incentive packages to health service providers and
also improvement of some structural components of the health care system
(Chimhutu, Tjomsland, Songstad, Mrisho, & Moland, 2015). The scheme never went
into the full scale because in 2015 Tanzania embarked on the RBF program, among
other things, was to improve service utilization of certain health facility services
upon provision of financial incentives (MoHSW, 2015). Most efforts are usually
driven by financial incentives but have been inadequately evaluated for their
sustainability. Hence, studying the DHFF’s effect on health service utilization is
important as it is a systemic approach to addressing issues which may lead to
improvement of health service delivery and increase health service utilization as
hypothesized by Kapologwe et al. (2019) (Figure 7).
54
Some indicators that MHS utilization are not performing well are: post-natal care
within three to seven days; access to modern family planning methods, fourth
antenatal clinic visits; and attendance at ANCs within 12 weeks of (Samky,
2019)gestation (Borghi et al., 2015; Kanyangarara et al., 2017; Kibusi et al., 2015;
Martin et al., 2019; Saxena et al., 2013).
In another qualitative study, which was done in Dar es Salaam, health providers’
disrespect to pregnant women was the main barriers to their booking and attending
ANC visits (Afulani et al., 2020; Bishanga et al., 2019; Mgata & Maluka, 2019;
Sando et al., 2016).
2.2.6 Conceptual Frameworks Guiding the Study
In 2018/2018, DHFF conceptual framework was developed, just before baseline data
collection that was done in January, 2018 after two consultative meetings with
different stakeholders at different levels (Kapologwe et al., 2019; Samky, 2019). It
contains four dependent variables namely; health utilization of health services, HSR,
governance and accountability and structural quality on maternal health services.
Whereas the independent variables were training on DHFF, Assistant accountant
employment, DHFF coordinator, supportive supervision and facility bank account.
The ToC was adopted and modified from other studies conducted in Kenya in 2010
(Goodman et al., 2010; Opwora et al., 2010) and in Tanzania in 2019 (Kapologwe et
al., 2019).
2.2.7 Theory of Change (ToC)
This is essentially a comprehensive description and illustration of how and why a
desired change is expected to happen in a particular context. In the Tanzanian
context we expected that DHFF would induce change in the series of immediate and
intermediate outcomes, ultimately leading to an improvement of the outcomes of
interest (service utilization, HSR, structural quality and governance and
accountability). The theory was also used to establish a causal link between the
DHFF inputs and the expected outcomes. In this study the causal pathways or change
mechanism that will be brought about by DHFF implementation was studied as has

55
been outlined by MRC guidelines on process evaluation for complex interventions
which suggest studying implementations, mechanism of change and context
moderators (Moore et al., 2014).
The conceptual framework for the ToC on DHFF was used as a reference material
for the implementation of the DHFF in Tanzania and elsewhere. Figure 12 below
shows the anticipated changes that occurred as a result of implementation of DHFF
and helps to open the black box. This ToC was conceptualized in two stakeholder
meetings. The first stakeholder meeting was conducted in July 2017, when
participants spelled out the processes of change they anticipated as a result of DHFF
implementation.
A second stakeholder meeting was conducted in August 2017 followed this, in order
to fine-tune the pathways of DHFF implementation (Figure 12).
Looking at Figure 12, the DHFF components column contains the necessary inputs
required for the implementation of the DHFF initiative in Tanzania. The process
column outlines expected program activities to be implemented and monitored for
level of implementation. Intermediate effects are the immediate results/outcomes
that occur after a successful process of implementation of the DHFF, while the
outcomes are the anticipated ultimate results after eighteen months of DHFF
implementation.

56
Training and raising awareness
about the DHFF and related
financial software (FFARS &
EPICOR)
Greater engagement
of HFGC
Appointment of
assistant accountants
Opening of bank
accounts for Health
facilities
Financial planning and
reporting
Receipt of funds
and proper book
keeping
Appointment of district
DHIFF coordinator and
engagement of CHMT
Increased provider
knowledge of DHFF
Strengthened supportive
supervision and mentorship
Investment in
facility
infrastructure, drugs,
supplies
Improved structural
quality of maternal
health services
Greater provider
autonomy over
resources
Greater health system
responsiveness by
patients/clients
Increased Maternal
services utilization by
communities
Increased provider
practice towards
DHFF
Planning and Budgeting
guidelines of health
facilities
DHFF Components P rocess Intermediate effects Outcome
Training on Governance
and accountability to
HFGCs
Figure 12: Theory of Change of DHFF Implementation in Tanzania
Source: Kapologwe et al., 2019.
In this study the FoI framework was embedded along the ToC for evaluation of the
DHFF initiative implementation in the Tanzanian context (Figure 13).
Fidelity of Implementation of DHFF initiative in Tanzania
Figure 13: Conceptual Framework for Fidelity of Implementation
Source: Kapologwe et al (2019), originally from Carroll et al., 2007).

57
From Figure 13, the most important part of the FoI is the potential moderating factor
of participants’ responsiveness which simply explains how DHFF implementers
responds to the implementation. The participant’s responsiveness was assessed
through indepth interviews of the health service providers and members of the health
facility governing committee with regard to the DHFF initiate implementation (or
their level of acceptability towards DHFF initiative). Participant responsiveness can
be defined as ‘the extent to which participants are engaged by and involved in the
activities and content of the program” (Mihalic, 2002). The content in this study is
defined as knowledge or skills obtained following the training on DHFF and
availability of the operational manuals and guidelines for DHFF implementation. The
three-day training using a cascade approach was conducted to health service
providers and members of HFGC on issues relating to DHFF implementation.
Cascade training was done by having national master trainers who trained the
regional master trainers who in turn trained district councils while financial
management using the software tool called Facility Financial Accounting and Report
System (FFARS).
2.2.8 Governance and Accountability
As discussed earlier, some studies, such as Boex et al. (2015b), sought to determine
the resource allocation and flow to expenditure unit proposed that insufficient
financial resources were reaching service delivery units such as dispensaries. Also
Dutta, (2015) and the World Bank (2015a) argued that health financing, especially
at PPHFPPHF, is challenged with late disbursement of funds associated with
violation of existing guidelines. On the part of accountability, studies prove existence
of unrealistic forecasts and weak internal controls (PWC, 2016; Umarji, 2015 ; Sun
et al., 2017). The WHO estimated about 20 - 40% of health expenditures were
inefficiently allocated and therefore had little to contribute towards peoplaaaae’s
health (Sun et al., 2017).
According to the World Bank (2015a) and Waweru et al. (2013), the functionality of
HFGCs is often poor as their members lack the knowledge of their roles and
responsibilities. Moreover, Kamuzora et al (2013a) showed that despite the

58
significant role of HFGCs in managing and supervising service provision at health
facilities, several hindrances affected their performance such that lack of financial
motivation, insufficient time for making decisions, short duration for consultations,
and lack of feedback from the approving authorities (Kamuzora, Maluka, Ndawi,
Byskov, & Hurtig, 2013b; Mayumana et al., 2017).
In the study by Soto et al (2011) looked into the effects of fiscal decentralization on
health care. The study provided empirical evidence to substantiate the importance of
D-by-D policy implementation; moreover, the study acknowledges that the role of
lower level leadership and governance is of great importance for medical
interventions (Soto, 2011).
A critical review that was conducted in Tanzania in 2017 on the decentralization
revealed that for the viability of CHF as a scheme, there is a need for empowerment
of local institutions and health financing decentralization. While local people are
fully aware of local problems, centrally organized power prevented them from using
their initiative in finding solutions. Findings state that CHMT in collaboration with
Council Health Service Board (CHSB), HFGCs and the people at the grassroots can
make CHF succeed by having a clear power relationship among CHMT, CHSB and
HFGCs, while effectively cooperating in achieving CHF laid down foundation for
other programs to be implemented (Mpambije, 2017).
Ongoing interventions in the study area
Since 2013, Tanzania has been implementing a number of programs geared towards
improving health system performance and MHS. One of the programs is RBF which
was implemented in eight regions of the country in which financing of health system
was guided by the pre-defined qualitative and quantitative indicators (Chimhutu et
al., 2015; Kapologwe et al., 2020; MoHSW, 2014a). Another program which has
been implemented with great success is national development and upgrading of PHC
facilities with essential surgical services (Kapologwe et al., 2020). These initiatives
are similar to DHFF initiative as they use a similar modality to disburse funds to the
PHC facilities. The only difference is RBF have a few selected indicators the
59
majority of which are maternal and child health related whereas DHFF included all
indicators needed in the health care system perfomance.
2.2.9 Research or Knowledge Gap
Empirical and theoretical reviews have shown that many countries face challenges of
health financing decentralization. As a result, there are delays in procurement and
delivery of health services in the public primary health facilities.
The effect of DHFF in the decentralized system on the health system performance
remains unknown in Tanzania and elsewhere (Kapologwe et al., 2019; Opwora et al.,
2009, 2015). Therefore, this research and evaluation study helped to add knowledge
on how these types of initiatives can be implemented. The following are gaps of this
study addressed are:
The first gap addressed was lack of information on the effect of DHFF on HSR,
governance and accountability, structural MHS and service utilization. Moreover, the
second gap addressed was the fidelity of implementation towards DHFF addressing
the challenge how projects or initiatives should be implemented under ideal
condition. Most previous studies were done outside Tanzania in the countries like
Kenya and mainly looked at consequences on service delivery and involvement of
community members and health facility management teams; these studies did not
examine FoI (Waweru, Goodman, Kedenge, Tsofa, & Molyneux, 2016).
Other gaps that exists include:
• Limited real-life knowledge on how initiatives like DHFF produce desired
effects in the health care system. This is a new inititiative in Tanzania.
• Limited understanding on how initiatives like DHFF are implemented in real
life settings. Therefore, after carrying out this study helped to understand how
best practices like the DHFF can be implemented in real life.
• Limited literature on governance and accountability in the health care system.
Therefore, this study helped in obtaining information about governance and
accountability in the health care system in Tanzania particularly in the PHC
facilities.
60
CHAPTER THREE
METHODOLOGY
3.0 Overview
This chapter is comprised of the following subsections: study design, research
approaches, study setting (s), study population, sample size determination and
sampling technique. It also covers data collection methods and tools, data analysis,
validity and reliability and ethical issues. The data for this study were collected
through a geographically represented sample of PPHF across the seven zones of
Tanzania mainland.
This thesis follows an implementation science approach and uses a combination of
methods (i.e., crossectional study design, Focus Group Discussion and Indepth
Interviews, before and after non controlled study) so as to understand the
implementation challenges and note the successes (Peters et al., 2013). Therefore,
triangulation of methods was used to get a better understanding of DHFF initiative
from different perspectives. This is important as the effects of DHFF have been
studied against a complex health systems hence research needs flexible methods and
design to produce sound results (Adam & Savigny, 2012).
3.1 Study Settings
This study was conducted in fourteen (14) councils of seven (7) regions (Mbeya,
Shinyanga, Dodoma, Pwani, Mtwara, Manyara and Katavi) from seven (7)
geographical zones (Figure 14). The reason for selecting seven zones was to seek the
country’s geographical representation. The similar approach has been done in major
Tanzanian health studies (Kapologwe et al., 2019; MoHCDGEC, MoH [Zanzibar],
2016). The forteen regions comprised of 42% of the Tanzanian population. The study
was conducted in 42 PPHF that are in 14 district councils namely: Dodoma City
Council and Bahi District Council in Dodoma Region; Kibaha Town Council and
Kisarawe District Council in Pwani Region; Mtwara Municipal Council and
Nanyumbu District Council in Mtwara Region; Mbeya City Council and Rungwe
City Council in Mbeya Region; Shinyanga Municipal Council and Ushetu District
Council in Shinyaga Region; Babati Town Council and Hanang District Council in
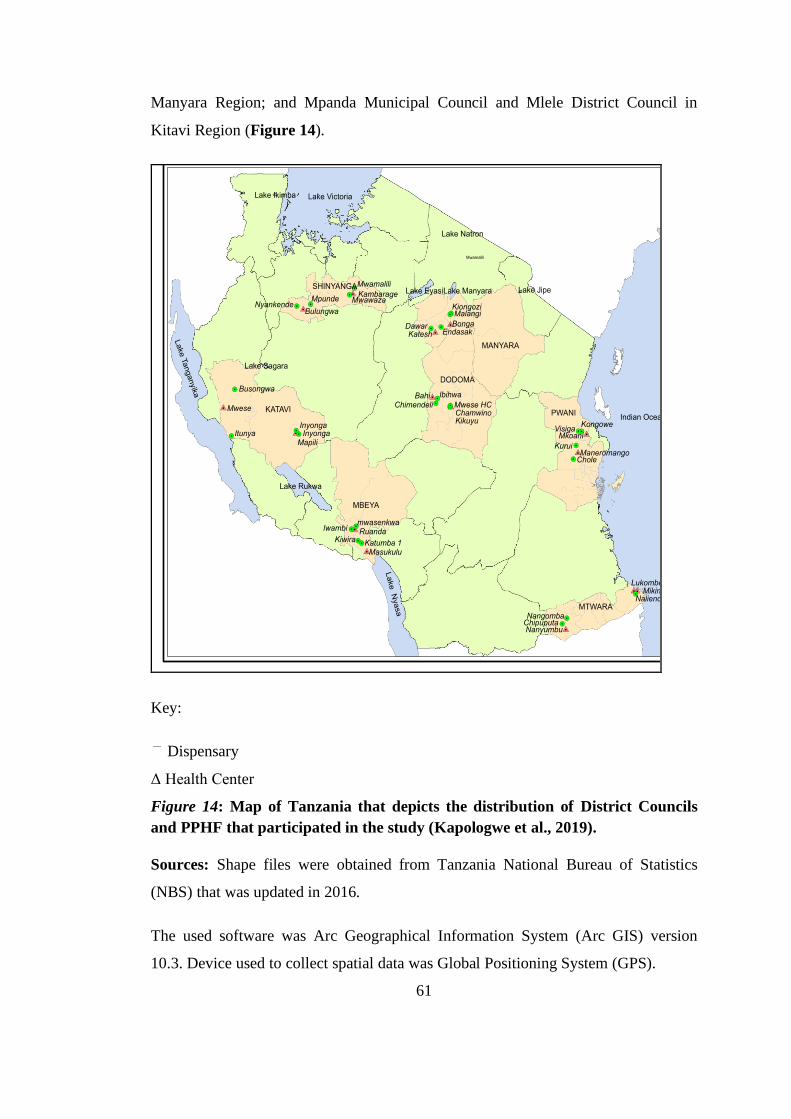
61
Manyara Region; and Mpanda Municipal Council and Mlele District Council in
Kitavi Region (Figure 14).
Key:
Dispensary
Δ Health Center
Figure 14: Map of Tanzania that depicts the distribution of District Councils
and PPHF that participated in the study (Kapologwe et al., 2019).
Sources: Shape files were obtained from Tanzania National Bureau of Statistics
(NBS) that was updated in 2016.
The used software was Arc Geographical Information System (Arc GIS) version
10.3. Device used to collect spatial data was Global Positioning System (GPS).
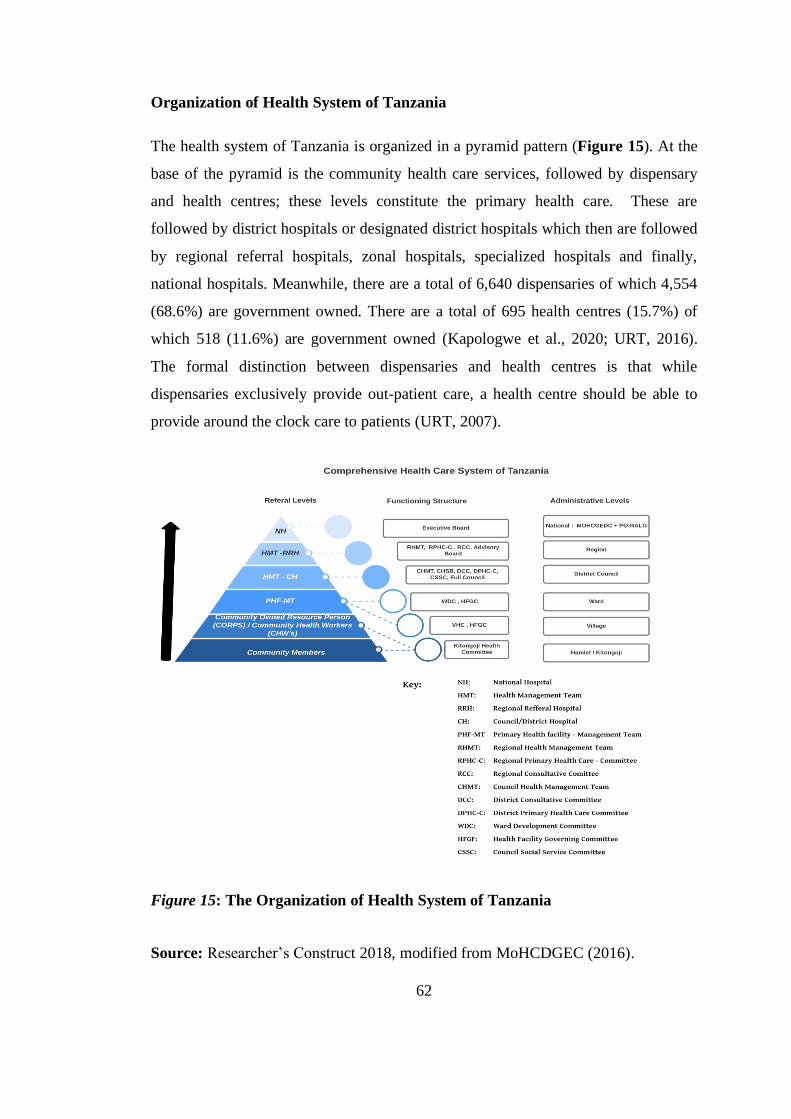
62
Organization of Health System of Tanzania
The health system of Tanzania is organized in a pyramid pattern (Figure 15). At the
base of the pyramid is the community health care services, followed by dispensary
and health centres; these levels constitute the primary health care. These are
followed by district hospitals or designated district hospitals which then are followed
by regional referral hospitals, zonal hospitals, specialized hospitals and finally,
national hospitals. Meanwhile, there are a total of 6,640 dispensaries of which 4,554
(68.6%) are government owned. There are a total of 695 health centres (15.7%) of
which 518 (11.6%) are government owned (Kapologwe et al., 2020; URT, 2016).
The formal distinction between dispensaries and health centres is that while
dispensaries exclusively provide out-patient care, a health centre should be able to
provide around the clock care to patients (URT, 2007).
Figure 15: The Organization of Health System of Tanzania
Source: Researcher’s Construct 2018, modified from MoHCDGEC (2016).

63
3.2 Research Approaches
This research used a mixed method approach employing both qualitative and
quantitative research design. According to Gravetter (2012) and Cresswell (2014),
quantitative approach is for producing quantifiable data that can be analysed using
statistical tests and use of both approaches is aimed at increasing accuracy of
information (Creswell, 2014; Gravetter, 2012). Mixed methods were important
because this study was conducted for the first time in Tanzania and components that
are present in the conceptual frameworks are answered by both qualitative and
quantititave approaches.
3.3 Study Design
This study adopted before and after non-controlled mixed methods (concurrent study
design) employing both qualitative and quantitative with embedded process
evaluation at the midoint of the study. The reason why non-controlled study was
chosen relates to the initiative being implemented nation wide thereby not leaving
any region or district to serve as a control study site.
The pre and post component means that there was one study conducted prior to the
implementation of DHFF initiative and another study was conducted 18 months after
initial implementation of the DHFF initiative, whereas, process evaluation study was
done midway between the baseline and endeline studies. This approach is considered
appropriate for the implementation and evaluation studies (Ary et al., 2010;
Creswell, 2014; Guba, 1981; Peters, Adam, Alonge, Agyepong, & Tran, 2014;
Stuart, Maynard, & Rouncefield, 2017; Wang et al., 2015).
Individual baseline, midline and endline studies employed a cross sectional study
design since the aim was to get a snapshot of the situation and it was less expensive
as compared to other study designs. The baseline study was conducted in February
2018 prior to starting disbursement and use of funds in the primary health facilities,
the midline study in August 2018 (six months after the start of DHFF
implementation) and the endline study was conducted in August 2019. The study
64
units were PPHF, patients exiting facilities, health workers, and members of HFGFs
within their catchment areas.
The baseline and endline studies were used to collect data for the outcome evaluation
study. The midline study was conducted six months (i.e. August 2018) after DHFF
initiative inception and the data obtained was used to appraise the implementation
processes (process evaluation) of the intervention. The study units for process
evaluation were health service providers and members of HFGC.
Outcome Evaluation of Study Components
This was done before and after the implementation of DHFF based on the following
indicators: HSR as perceived by patients attending at the PPHF, structural quality of
MHS, and maternal health service utilization.
Process Evaluation of the Study Components
The process evaluationwas done by measuring the FoI of DHFF initiative at the
midline (Six months after initiation). This approach enabled a consideration of how
the implementation of DHFF initiative was achieved. Moreover, there was an
exploration on how governance and accountability of DHFF initiative were exercised
in the primary health facilities. This was important in opening up the black box
which is usually skipped in most evaluation studies especially those that are health
reform related.
3.4 Target Population
This study population included; health managers, HFGCs chairpersons, patients and
public primary healthcare facilities in the seven regions of Tanzania mainland.
3.5 Study Population
The study population was divided into facilities, in-charges of health facilities,
HFGC members, and exiting patients. Others were members of CHMT from 14
district councils.

65
3.5.1 Inclusion Criteria
A) Patients
1. All exiting outpatients who voluntarily consent from registered PPHF.
2. All exiting outpatients with history of more than 2 times visit at the same
PPHF.
B) Health Care Workers and Members of HFGC
1. All health care workers with more than six months employment in PPHF who
consented. Six months experience implied the experience in budget cycle and
understanding of financial management in PPHF.
2. All HFGC active members within a catchment area with atleast one year
3. HFGCs active members with an experience of more than one year within
PPHF. One year implies experience in the public budget cycle.
3.5.2 Exclusion Criteria
A) Patient
All patients who had less than two visits in the particular health care facility.
B) Health Care Workers and Members of HFGCs.
Health care workers who have worked less than 6 months.
C) Members of HFGC.
HFGCs with members who are not actively involved in the health facilities matters
and those with less than one year of their tenureship.
3.6 Unit of Analysis
The study assessed HSR by examining perceived experience of the exiting patients
after medical consultations in the PPHF. The structural quality of maternal healh
services was assessed by looking into domains of structural elements of PPHF. The
study assessed fidelity of implementation (adherence) of DHFF initiative and level of
content (knowledge) towards DHFF among health care workers working in the
primary health facilities. Further, aspects of governance and accountability were
explored among health workers and HFGC members within their catchment areas.

66
3.7 Sampling Method and Sample Size Estimation
3.7.1 Sampling Methods for Quantitative Data
This study employed a multistage sampling technique for selection of the study units.
The starting point was at the country zones, regions, district and health facilities
(dispensary and health centers). The sampling was predominantly probability
sampling but at some point we also used non probability sampling. The technique is
convenient for studying large and diverse population size (Fawler, 1993;
Molenberghs, 2010). The sampling stages were zones, regions, district councils,
PPHF, health care workers and patients.
First Stage (Zones): All zones were purposively selected from the geographical
zones.
Second Stage (Regions): Randomly selected seven regions out of 26 regions in
mainland Tanzania through table of random numbers. One region from each zone
was selected with each zone having between three and four regions.
Third Stage (District Councils): Two district councils were selected from each
selected region. The sampling frame per region was district councils in the respective
regions. One urban district council was purposefully selected and one rural district
council were randomly selected by using a table of random numbers.
Fourth Stage (Public Primary Health Facilities [PPHF]): The selection of health
facilities employed simple random sampling through use a table of random numbers
from two strata (urban versus rural). Stratification of health facilities based on their
location and homogeneity of the study units (i.e. rural versus urban and health centre
versus dispensary) was done. The sampling frame included the list of PPHF that
obtained from the existing Health Facility Registry (HFR) that is an online platform
used for registration of the public health facilities across the country (www.hfr.go.tz).
At the health centre strata, one health centre was randomly selected and and to the
dispensary strata, two dispensaries were randomly selected by using a table of
random numbers resulting in three facilities in each district council being selected.
This included one health centre and two dispensaries in each district in order to

67
represent urban and rural areas. In this case, 21 (i.e. seven health centres and 14
dispensaries) primary health facilities represented rural areas, and 21 urban facilities
represented urban areas (Figure 16). From each selected public health facilities
service providers were conviniently selected (all those who were present on the day
of an interview) while exiting patients were systematically sampled after medical
consultations based on their gender stratification (Figure 16).

68
Figure 16: Schematic Presentation of Sampling Technique
Random
selection
of Regions
First Stage
One region per
zone
Second
Stage
Stratification of
14 Councils (1-
urban&1 rural
council)
14 Health
centres
28 Dispensaries
Random selection of
both HCs and
Dispensaries by using
a table of random
numbers.
Systematic selection
of patients by their
sex
Systematic selection of 844
exiting patients basing on their
gender on Health System
Responsiveness
14 In-depth interviews to
DMOs, DHFFco, HFi/c and
HFGCs chair.7 FDGs to CHSB
chair, 2 HF i/c, 2 Matrons,
Assistant Accountant and 2
members of HFGCs. 42 Health
Facilities on Structural Quality and Maternal Health Service
utilization
Measuring FOI to 238
participants who were
conveniently selected.
Third
Stage
Stratification
of HFs into
urban and rural
Gender based
stratification
of patients by
their sex
Fourth
Stage

69
3.7.2 Quantitative Sample Size Determination
The study sample size calculation was based on the purpose of this study and the
nature of the population under scrutiny. Thus, referring to Cohen & Crabtree (2008)
sample size of thirty (30) can be considered to be the minimum number of cases if
some form of statistical analysis is to be done (Ary et al., 2010). For this study a total
of 42 PPHF were selected of which 14 were health centres and 28 were dispensaries.
3.7.3 Quantitative Data Collection
The database was developed by using Open Data Kit software (ODK) in which all
the data collected, entered, and then analysed. This study used the mobile data
collection (MDC) approach for quantitative data gathering. Under this approach all
data were collected via mobile phone and uploaded to the central server. Fourteen
(14) research assistants underwent four days of training on mobile data collection
skills and techniques before taking part in the pre-testing of their acquired skills in
health facilities outside the study area. The data collected were sent to the researcher
by using the ODK platform (Figure 17). In Tanzania all primary health facilities
have GPS coordinates. Therefore, all selected study primary facilities had GPS
coordinates and all data enumerators used tablets with GPS sensors to enhance data
integrity.
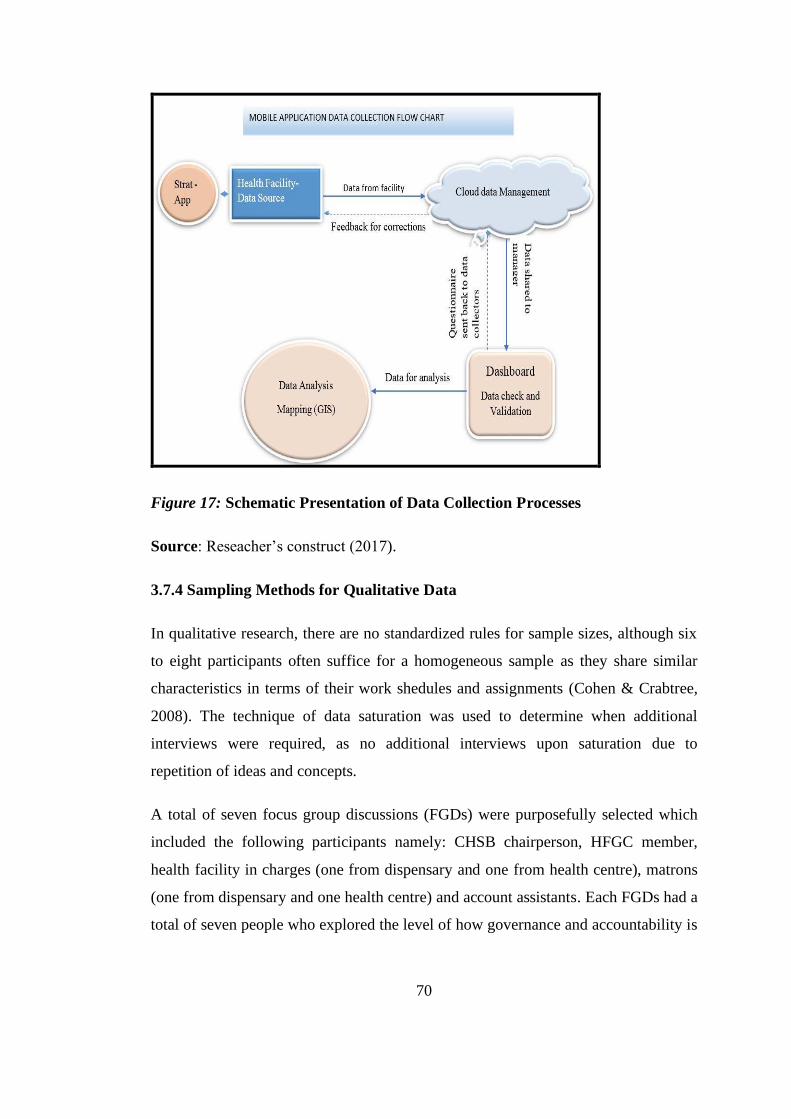
70
Figure 17: Schematic Presentation of Data Collection Processes
Source: Reseacher’s construct (2017).
3.7.4 Sampling Methods for Qualitative Data
In qualitative research, there are no standardized rules for sample sizes, although six
to eight participants often suffice for a homogeneous sample as they share similar
characteristics in terms of their work shedules and assignments (Cohen & Crabtree,
2008). The technique of data saturation was used to determine when additional
interviews were required, as no additional interviews upon saturation due to
repetition of ideas and concepts.
A total of seven focus group discussions (FGDs) were purposefully selected which
included the following participants namely: CHSB chairperson, HFGC member,
health facility in charges (one from dispensary and one from health centre), matrons
(one from dispensary and one health centre) and account assistants. Each FGDs had a
total of seven people who explored the level of how governance and accountability is

71
exercised in relation to DHFF initiative implementation at the PPHF. Interviews
lasted from one to one and half hours.
To understand the participant’s responsiveness towards DHFF initiative
implementation, twenty-eight in-depth interviews were planned to be conducted
however only 14 were conducted after having reached a saturation point with
representatives from the following participant groups: DMO, DHFF coordinator, and
health facility in charge, and HFGC chairperson to explore their responsiveness and
acceptance to the DHFF initiative.
3.7.5 Data Collection Methods and Tools for Qualitative
The principal investigator and research assistants used semi - structured interview
guide to conduct indepth interviews, qualifications of other data enumarators were
degree holders with more than five years of field experience, currently are working at
the University of Dodoma (UDOM) as tutors. Intervew was done by the principal
investigator. Prior to the interview there wa as a pre-test study that was done on how
best to collect qualitative data while ensuring data quality and integrity interview
guide collected qualitative data from the study sites. The qualifications of other data
enumarators were degree holders with more than five years of field experience,
currently are working at the University of Dodoma as tutors. The indepth interviews
were done in three district councils.
Whereas for the FGDs, principal investigator accompanied by two research assistants
with qualitative data collection skills conducted FGDs in seven district councils. The
moderation was done by principal investigator as he has a solid understanding of the
topic under discussion, the research assistants were responsible for taking field notes
and also recording the conversations.
Prior to the FGDs and IDS a pre-test done on how best to collect qualitative data
while ensuring data quality and integrity. The indepth interview guide was comprised
of 21 questions derived from conceptual frameworks (ToC and FoI) and categorised
into areas that measured effects of DHFF initiative (i.e., participants’ responsiveness
towards DHFF implementation and adherence).
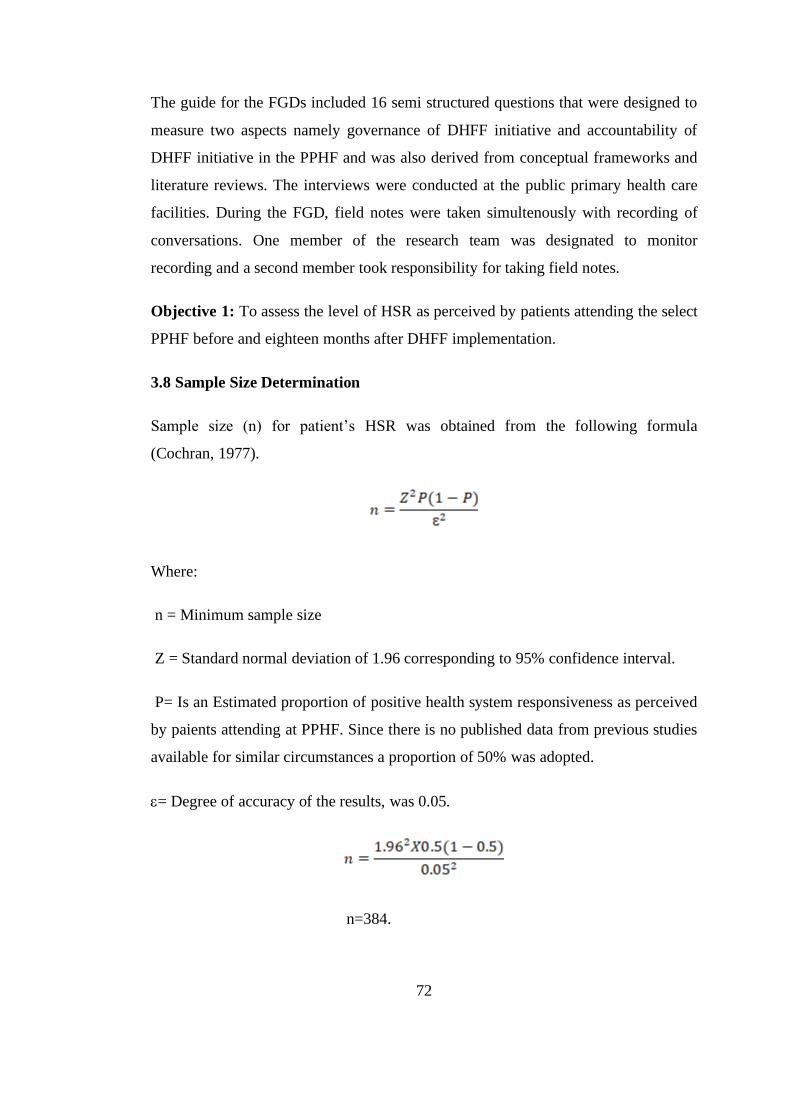
72
The guide for the FGDs included 16 semi structured questions that were designed to
measure two aspects namely governance of DHFF initiative and accountability of
DHFF initiative in the PPHF and was also derived from conceptual frameworks and
literature reviews. The interviews were conducted at the public primary health care
facilities. During the FGD, field notes were taken simultenously with recording of
conversations. One member of the research team was designated to monitor
recording and a second member took responsibility for taking field notes.
Objective 1: To assess the level of HSR as perceived by patients attending the select
PPHF before and eighteen months after DHFF implementation.
3.8 Sample Size Determination
Sample size (n) for patient’s HSR was obtained from the following formula
(Cochran, 1977).
Where:
n = Minimum sample size
Z = Standard normal deviation of 1.96 corresponding to 95% confidence interval.
P= Is an Estimated proportion of positive health system responsiveness as perceived
by paients attending at PPHF. Since there is no published data from previous studies
available for similar circumstances a proportion of 50% was adopted.
= Degree of accuracy of the results, was 0.05.
n=384.

73
The sample size was 384 patients. The 10% of sample size was added (n= 38) to
cover for refusal to participate, making a total of 422 patients.
3.9 Data Collection Tools
A closed-ended Likert scale questionnaire was adopted and modified from the health
systems responsiveness questionnaires used in WHO multi-country studies to study
patients’ experiences during their encounters with the health care system (Appendix
1) (WHO, 2015; Naghavi et al., 2015; Robone, Rice, & Smith, 2011). There were 37
responsiveness questions that were grouped under the seven domains which have
ordinal response categories.
The 37 questions were divided among the seven domains of responsiveness: prompt
to attention (7), respect to dignity (3), clear communication (7), quality of basic
amenities (11), confidentiality (3), access to care (4) and autonomy (2) (Table 3).
The internal consistency of the overall responsiveness scale (37 items) was measured
for Cronbach’s alpha (Nunnally & Bernstein, 1979) which had an average of 0.827
for all eight domains. For each primary health facility, 10 exit interviews were
conducted with the patients who had already received curative health services and
who had made two or more than two visits to the respective facility. In consideration
of gender balance, patients were stratified basing on their gender, the calculated
sample was divided into two (50% male and 50% female patients).
Systematic sampling was used to select exiting patient in which every 3rd exiting
patient was requested to consent to participate in the study, an average of 10 patients
participated per primary health care facility.
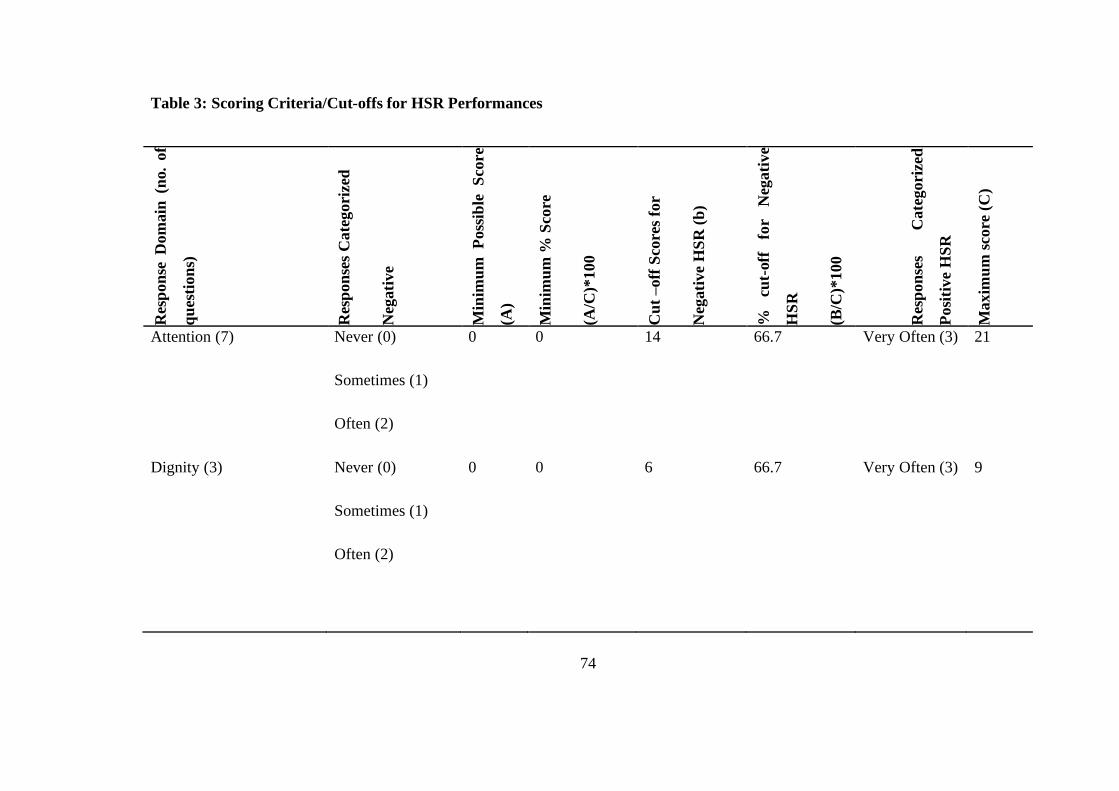
74
Table 3: Scoring Criteria/Cut-offs for HSR Performances
Res
pon
se D
om
ain
(n
o.
of
qu
esti
on
s)
Res
pon
ses
Cate
gori
zed
Neg
ati
ve
Min
imu
m P
oss
ible
S
core
(A)
Min
imu
m %
Sco
re
(A/C
)*100
Cu
t –off
Sco
res
for
Neg
ati
ve
HS
R (
b)
%
cut-
off
fo
r N
egati
ve
HS
R
(B/C
)*100
Res
pon
ses
Cate
gori
zed
Posi
tive
HS
R
Maxim
um
sco
re (
C)
Attention (7) Never (0)
Sometimes (1)
Often (2)
0 0 14 66.7 Very Often (3) 21
Dignity (3) Never (0)
Sometimes (1)
Often (2)
0 0
6 66.7 Very Often (3) 9
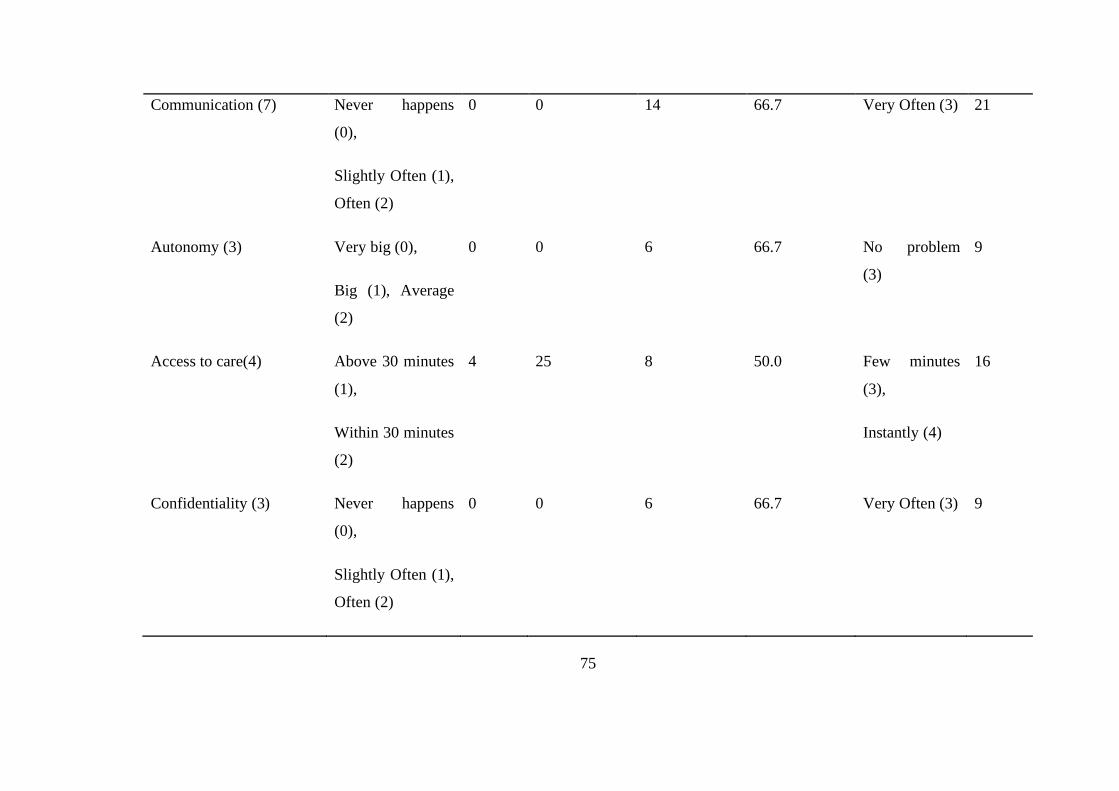
75
Communication (7) Never happens
(0),
Slightly Often (1),
Often (2)
0 0 14 66.7 Very Often (3) 21
Autonomy (3) Very big (0),
Big (1), Average
(2)
0 0 6 66.7 No problem
(3)
9
Access to care(4) Above 30 minutes
(1),
Within 30 minutes
(2)
4 25 8 50.0 Few minutes
(3),
Instantly (4)
16
Confidentiality (3) Never happens
(0),
Slightly Often (1),
Often (2)
0 0 6 66.7 Very Often (3) 9

76
Basic amenities (10) Strongly disagree
(1),
Disagree (2),
Agree (3)
10 25 30 75.0 Strongly
Agree (4)
40
Total Health System
Responsiveness (37)
14 11.2 84 67.2 125

77
Objective 2
To assess the structural quality of MHS, this study adopted tools from the Results
Based Financing (RBF) program (Appendix X) that has been implemented in eight
regions of Tanzania and in more than 48 African countries including Tanzania
(World Bank, 2013). MHS data were collected in 42 selected PPHF in seven regions
of Tanzania mainland.
Data Collection tools: used an adapted and modified observational checklist
adopted from RBF program for data collection. The RBF program is implemented in
eight regions of Tanzania mainland and more than 48 countries of Africa continent.
The checklist on the tool were selected based on the existing challenges particularly
structural quality of MHS in Tanzania. (Mapunda et al., 2016; MoHSW, 2014;
Ojemeni et al., 2017; Wiedenmayer et al., 2015). The checklist was pilot tested and
modified prior to data collection exercise to enhance for rigor and validity of the tool.
Objective 3
Using nine select indicators (Appendix XI), the study assessed the maternal health
service utilization in 42 PPHF. These indicators were extracted from DHIS-2
platform. The following indicators were assessed:
o Institutional/ health facility deliveries.
o Intermittent presumptive treatment for malaria second dose (IPT-2)
o ANC mothers on mebendazole (De-worming).
o Number of women attending the fourth ANC visit.
o Number of HIV infected pregnant women who are receiving antiretroviral
treatment (ART).
o New users of modern family planning methods.
o Proportion of PPHF with availability of all 30-tracer medicines.
o Number of mothers receiving post natal care within three to seven days after
delivery
o Pregnant mothers attending their first ANC before 12 weeks.

78
All of the above indicators are present in the health management information system
(HMIS), which is a standard tool for collecting health records across all public health
facilities in Tanzania. The selected indicators are considered to be important in the
safe motherhood initiative (MOHCDGEC, 2016) and also are part of health system
indicators. The HMIS is divided into paper-based tools (MTUHA books) which
consist of 15 registers, tally and summary sheets, and an electronic base referred to
as the District Health Information Software (DHIS-2) (Musau et al., 2011). The
DHIS-2 and health facility HMIS registers were used to assess maternal health
service utilization indicators in the selected 42 PPHFin seven regions of Tanzania
mainland.
Data Collection Tools: After collection of data from the DHIS-2 platform,
compilation was completed on a pre-developed Microsoft Excel™ sheet
(https://hmisportal.moh.go.tz/hmisportal/#/ ).
Objective 4 (Midline)
This objective aimed at measuring the level of FoI towards DHFF initiative. To
achieve this objective, the tool was developed to assess fidelity of implementation
(Appendix XIII A). Reliability test was done, and the tool was found to have a
reliability of 0.812. Six domains with a total of 42 questions were assessed for their
adherence (fidelity): 1) Training on DHFF and FFARS; 2) Coordination of DHFF
activities; 3) Governance and Accountability; 4) Financial management; 5) Planning
and Guidelines; and 6) Supportive Supervision and Mentorship (Appendix 5a). Other
components assessed werecontent (knowledge) and participants’ responsiveness.
Sample size estimation for quantitative data
Sample size (n) for content (Knowledge), and FoI (adherence) of DHFF initiative
was obtained by administering the questionnaire to 238 health care workers who
were conveniently selected on the day of the data collection at 42 PPHF.

79
Sample Size Estimation for Qualitative Data
For the participants’ responsiveness towards DHFF initiative, a total of 14 in-depth
interviews out of 28 planned indepth interviews were conducted to purposefully
selected participants by virtual of their management and leadership roles in the
primary health care system (CHMTs, Health Facility Incharges and HFGC
members). The intent was to get the understanding of participant’s responsiveness
towards DHFF initiative implementation. Initially 17 participants were contacted for
an interview; however, only 14 consented with three declining due to previous
commitments. The saturation level was reached on the 11th participant; however, we
carried out 3 more interviews for a total of 14 interviews. The interviews were
conducted face-to-face and the interviewees were contacted via phone and others on
face-to-face prior to the interview. The interviews were conducted with DMOs,
district DHFF coordinators, primary health facility in charges, and chairs of HFGCs
for each of the seven purposefully selected district councils (Appendix XIV). The
selection of participants based on their implementation roles and position in the
health system. Each nterview lasted between 30 to 60 minutes.
Data Collection Tool to Measure FoI
General information about DHFF initiative implementation, knowledge (content) and
adherence was obtained after administering questionnaires to health service providers
and members of HFGC. The implementation fidelity was measured through
adherence and its sub-categories, which are content (knowledge) and its moderating
factors namely, participant’s responsiveness towards DHFF initiative, training, and
status of HFGC, supportive supervision, assistant accountants, and inclusiveness in
decision making. Moreover, there was assessment of contextual factors.
Fidelity of Implementation (FoI): A total of 40 questions were asked of health
workers to determine whether the health service providers implemented DHFF
initiative as planned. The adherence with DHFF implementation was used to decide
the FoI framework through the cut-off points (high or low).

80
Knowledge (Content): Health care providers were assessed for content by checking
their level of knowledge on DHFF and whether they received training and any
supportive supervision and mentorship. A total of 14 questions for health workers
and five questions for HFGC related to the processes of DHFF were asked. The
questions had weighted points. The mean scores were computed and those who
scored above the mean value (>9.286) were graded as having adequate knowledge
(content) while those scoring below the mean score were categorized as having
inadequate knowledge (content) of DHFF initiative.
Moderating factors: The FoI (adherence) was then assessed for association with
some of the moderating factors, namely participant’s responsiveness, training on
DHFF, supportive supervision, and HFGC existence and presence of assistant
accountants. Levels of fidelity were interpreted as previously reported in the
literature, with ≥ 80% adherence interpreted as ‘high’ fidelity, and <80% as ‘low’
fidelity (Bellg et al., 2004; Borrelli, 2012; Nurjono et al., 2019; Toomey, Mathews,
& Hurley, 2017).
Qualitative Data Analysis
A total of 14 in-depth interviews were audiotaped, transcribed for verbatim, and
anonymized for analysis. Thematic analysis was used to analyse the data of DHFF
implementers leading into thematic analysis. The analysis began with data
familiarization through listening/re-listening to audiotapes as well as reading/re-
reading of transcripts. Three researcher assistants independently coded the material
using NVivo QSR™ version 12 which was used to help to organize the codes, and a
fourth researcher reviewed the coded material, categories, sub-themes and themes to
establish key findings. The Nvivo QSR™ software developed a coding tree by
following all steps from setting up a project in the software then importing files of
interview transcripts, followed by assigning codes to the imported data. These codes
were grouped together to formulate categories, sub - themes and then themes. For
simplification and easiness of readability, processes from formation of codes,
categories, sub-themes and themes were summarized in the Coding Table (Appendix
XI).
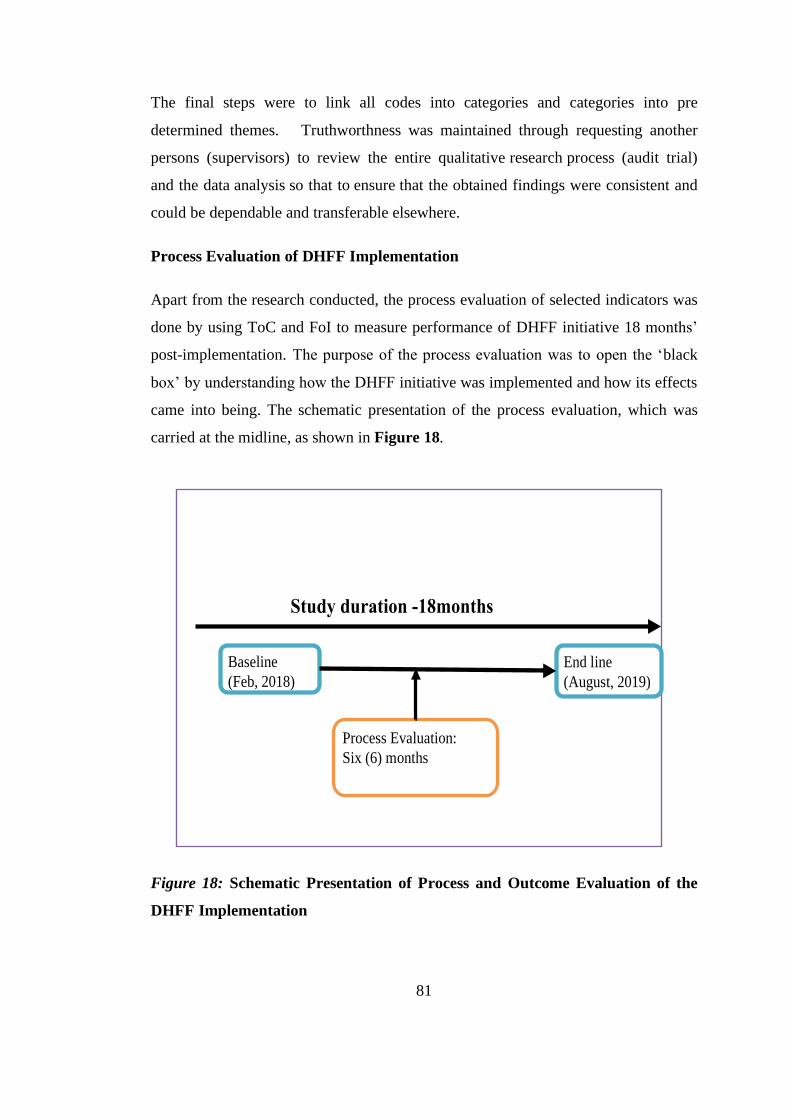
81
The final steps were to link all codes into categories and categories into pre
determined themes. Truthworthness was maintained through requesting another
persons (supervisors) to review the entire qualitative research process (audit trial)
and the data analysis so that to ensure that the obtained findings were consistent and
could be dependable and transferable elsewhere.
Process Evaluation of DHFF Implementation
Apart from the research conducted, the process evaluation of selected indicators was
done by using ToC and FoI to measure performance of DHFF initiative 18 months’
post-implementation. The purpose of the process evaluation was to open the ‘black
box’ by understanding how the DHFF initiative was implemented and how its effects
came into being. The schematic presentation of the process evaluation, which was
carried at the midline, as shown in Figure 18.
Study duration -18months
16/02/20 18
End line
(August, 2019)
Baseline
(Feb, 2018)
Process Evaluation:
Six (6) months
Figure 18: Schematic Presentation of Process and Outcome Evaluation of the
DHFF Implementation
82
The process evaluation undertook an on-going descriptive and mixed methods
assessment of the process of DHFF initiative implementation at the public primary
health facilities, documenting the role and perspectives of key stakeholders at each
stage and at each level of the implementation to understand and open the black box
to better comprehend the ‘how’ (Dunn et al., 2015; Moore et al., 2014). Moreover,
this evaluation intended to examine the degree to which implementation was carried
out by health service providers, if they adhered to design and theory of change and
fidelity of implementation frameworks. Process evaluation data collection was done
at the midline, six months after DHFF launch in the 14 district councils of Tanzania
mainland. A FoI framework with the moderating factors was used to conduct the
process evaluation.
Outcome Evaluation of DHFF Implementation
The outcome evaluation measured the effect of DHFF after 18 months of the DHFF
initiative implementation. It involved data collection at baseline and endline. The
variables assessed were structural quality of MHS and health service utilization. Also
it assessed HSR as perceived by patient’s experience after medical consultations. The
study used the ToC framework with pathways that were hypothesised at the baseline
as stipulated in the Figure 17 and also in the protocol paper (Kapologwe et al.,
2019).
Fidelity of Implementation for DHFF initiative
According to Carroll et al. (2007b), adherence includes knowledge (content),
coverage, frequency and duration, while moderators includes intervention
complexity, facilitation strategies, quality of delivery and participants’
responsiveness. In the current intervention, the adherence was measured against how
health service providers in the PPHF implemented the intervention according to the
context. The context of this intervention includes availability of skilled professionals
(assistant accountants), operational guidelines, and HFGC, along with training and
existence of support systems like Facility Financial Accounting and Reporting
System (FFARS). These factors allowed for effective and efficient implementation of
the DHFF intervention. The degree to which the intervention is implemented defines
83
the degree of FoI. However, moderators of the FoI, such as complexity of the
intervention, strategies kept in place to facilitate it, and participants’ responsiveness
to the initiative (in this case health service providers) influence the overall
performance of the intervention (Carroll et al., 2007).
In measuring coverage, the current intervention focused on the extent of the
availability of assistant accountants in primary health facilities especially the health
centers; availability of operational guidelines and financial management tools and
use of FFARS; health care providers trained on the DHFF initiative process; and
availability and activeness of HFGCs in assuming their roles and responsibilities.
Moreover, the frequency and duration of the DHFF implementation was assessed
based on the adherence to DHFF initiative and reporting of both financial and
technical perfomances.
Not every component of adherence may be mandatory in an implementation as an
intervention can be successful when core or essential components are implemented
(Carroll et al., 2007). The current research was intended to identify the essential
components for successful implementation of DHFF iniative in order to improve the
effectiveness and efficiency of implementation of DHFF iniative.
In the course of implementation of the DHFF initiative, the potential moderators for
successful implementation were assessed. This research adopted the potential
moderators from Carroll et al. (2007b) as indicated in Figure 19. Intervention
complexity was assessed through availability and understanding of operational
guidelines by health service providers as proposed by (Century, Rudnick, &
Freeman, 2010). The evidence shows that detailed guidelines are more easily adopted
and implemented than vague ones. Also there is a higher chance of achieving fidelity
in simple than complex interventions (Carroll et al., 2007; Pérez, Stuyft, Zabala,
Castro, & Lefèvre, 2016).
The GoT has maintained facilitation strategies to ensure there is sufficient
implementation of DHFF in PPHF. These strategies include development and
dissemination of operational guidelines and financial management tools, training of
health service providers, supportive supervision and mentorship, employment of

84
account assistants in health facilities, appointment of DHFF coordinators at council
level, and use of FFARS as a tool for reporting both financial and performance
reports (Kapologwe et al., 2019).
These strategies may potentially moderate the degree of FoI performance; hence, the
more done to help implementation, through monitoring, feedback, and training, the
higher the potential FoI (Carroll et al., 2007). However, of note, the facilitation
strategies do not guarantee better FoI implementation, but rather reflection of
adequacy in quality of delivery. One of the major factors that necessitated this
research study was to establish the potential moderators that escalated the
performance of FoI in the current DHFF intervention.
Finally, participant’s responsiveness as viewed in the context of intervention
relevance to implementers contributes to low or high levels of FoI (Carroll et al.,
2007). The acceptability of the benefits of DHFF to health services providers bares
significant influence on the FoI performance. When health service providers
perceived high benefits from an intervention during their service provision there is
likelihood that adherence to the standards set for implementation will be high.
Therefore, in establishing the level of participants’ responsiveness, the current study
assessed the acceptability of health service providers towards DHFF implementation.
However, this moderator is not only assessed on the individuals receiving the
intervention but also on those responsible such as the DHFF coordinators at council
level. This study was conducted as a part of process evaluation in order to measure
the FoI amongst health service providers and HFGC committee members as a part of
community representation towards DHFF initiative implementation after it started.
Following the midline study on FoI, there were modifications/additions of some
moderating factors that were not in the hypothesis of the FoI framework (Figure 19).
Figure 19 shows that potential moderators are DHFF training, availability, and
functionality of the public financial management tools, participants’ sex, availability
of assistant accountants, inclusiveness in decision making, attitude of health care
workers, enabling environment and location of PPHF are important factors for FoI
towards DHFF initiative.

85
Levels of fidelity were interpreted as previously reported in the literature, with ≥
80% adherence interpreted as ‘high’ fidelity, and < 80% as ‘low’ fidelity (Bellg et
al., 2004; Borrelli, 2012; Nurjono et al., 2019; Toomey et al., 2017).
Figure 19: Modified Conceptual FoI Framework after the Midline Study
(Modified from Original Framework by Kapologwe et al., 2019).
Potential Moderators
• DHFF Training
• Supportive supervision
• Active HFGC
• Availability of operational
guidelines
• Availability and functionality of
PFM tools
• Participants sex
• Availability of account assistant
• Inclusive decision making
• Location of health facility
• Enabling environment
• Planning and Budgeting
• Attitude of Health workers
Adherence
• Context
• Coverage
• Frequency
• Duration
• Dose
Outcome: FoI
towards DHFF
Intervention:
DHFF
86
Objective 5 (End line)
Data collection
Qualitative: To explore how the Governance and Accountability of DHFF were
exercised in the PPHFs, we used an internally created interview guide (Appendix
XII) to conduct FGDs to explore the participants’ insights. The participants were
selected based on their roles and responsibilities in regard to the implementation of
DHFF initative. The seven FDGs were conducted with groups of seven participants
from each region. Each group was composed of the CHSB chairperson, one member
of HFGC, two-health facility in charges (one from dispensary and one health centre),
matrons (one from dispensary and one health center) and account assistants. Each
FGD lasted for an average of one to one and half hours. There was one person who
was designated for recording and another for taking field notes. The FGDs were
conducted by principal investigator accompanied with 2 research assistants with
qualitative data collection skills. The moderator was one of the research assistants
who was conversant with moderation skills and the topic under discussion.
Saturation was reached when there were no new ideas emerging from the discussion
or conversations.
3.10 Pre-testing of Tools
Pre-testing of tools was done in Kongwa – Dodoma region at the selected health
facilities where the study did not take place. This helped in modification of tools by
droping and adding some questions so that to improve data collection tools.
3.11 Data Collection Procedure
The researcher collected data daily with 14 trained research assistants using the
mobile data collection (MDC) system. The interview guide for qualitative data
collection and structured questionnaires were both translated into Kiswahili
language, as it is the national language and widely used (Appendix 1, 2, 3, 4, 5a &
b). The collected data was then sent to the researcher where it was checked and
verified for its relevance to enhance the quality of the collected data and internal
consistency. Some of the data were collected directly from the DHIS-2 platform.

87
Two research assistants accompanied the researcher to all regions for collection of
qualitative data.
3.12 Data analysis
3.12.1 Quantitative data analysis
3.12.1.1 Variables and their measures
3.12.1.1.1 Dependent Variables
i. HSR
ii. Structural quality of MHS
iii. MHS utilization
iv. Implementation fidelity of DHFF initiative
v. Governance and accountability
3.12.1.1.2 Independent Variables
i. Socio-demographic characteristics
ii. Content (knowledge) of DHFF
iii. Participants’ responsiveness of DHFF
iv. Training on DHFF
v. Supportive supervision
vi. Existence of HFGCs
vii. Location of health facilities (urban vs rural)
viii. Staffing level per health facility
ix. Inclusiveness in decision making
x. Enabling environment
The above variables are summarized in Figure 20 below:
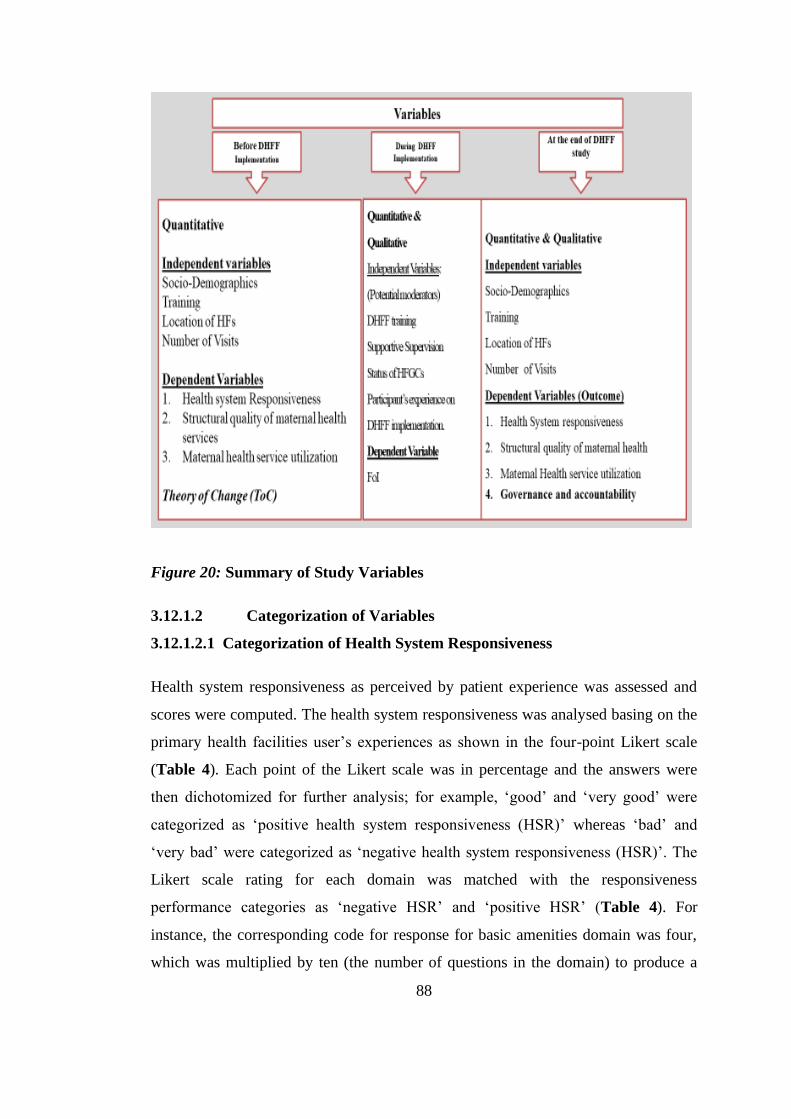
88
Figure 20: Summary of Study Variables
3.12.1.2 Categorization of Variables
3.12.1.2.1 Categorization of Health System Responsiveness
Health system responsiveness as perceived by patient experience was assessed and
scores were computed. The health system responsiveness was analysed basing on the
primary health facilities user’s experiences as shown in the four-point Likert scale
(Table 4). Each point of the Likert scale was in percentage and the answers were
then dichotomized for further analysis; for example, ‘good’ and ‘very good’ were
categorized as ‘positive health system responsiveness (HSR)’ whereas ‘bad’ and
‘very bad’ were categorized as ‘negative health system responsiveness (HSR)’. The
Likert scale rating for each domain was matched with the responsiveness
performance categories as ‘negative HSR’ and ‘positive HSR’ (Table 4). For
instance, the corresponding code for response for basic amenities domain was four,
which was multiplied by ten (the number of questions in the domain) to produce a

89
cut-off score of 40 and yielded a maximum score “positive” for an individual for this
domain (Table 3). One multiplied by 10 (number of questions) and cut off points for
negative HSR was 30 (Table 3). This approach is similar to one that was used in
another study conducted in Ethiopia in 2017 (Yakob & Ncama, 2017).
A total of 37 questions were included to assess health system responsiveness in the
primary health care facilities in Tanzania. The assessement was done by using likert
scale questions. The likert questions had weighted scores that were increasing from
negative to more positive statements and they were converted into numerical values.
The questionnaire had four-point Likert scale question items ranged from zero to
three for five domains (attention, dignity, communication, autonomy and
confidentiality). Zero represented absence of the assessed feature of HSR and three
denoted the highest level of its availability. Any score below three was considered to
be a low score (Negative HSR) and it was hence a cut-off point for the respective
domains (Table 4). On the other hand, one to four points were used for two domains
(access to care and quality of basic amenities) with a score of four indicating the least
performance of the assessed HSR for access to care and 10 for basic amenities
(Table 3). In total, a minimum of HSR score was computed as 14 out of the
maximum score of 125 for all 37 questions (Table 3). Total score for each domain
was computed in percentage by taking the actual score (Column (B) obtained from
each respondent divided by the maximum possible score (Column C) multiplied by
100% (Table 3). Similarly, the overall HSR score was computed by dividing the
overall total cut-off (84) scores over the maximum possible value (125) multiplied by
100%.
The score of the respondents was used to categorize the perception towards HSR into
two major categories [Category I= Positive HSR and Category II= Negative HSR]
(Appendix 1).

90
Table 4: Health Care Responsiveness Performance Criteria and their
Categorization
Domain Number of
questions
Min-max
score(s)
Negative HSR Positive
HSR
Prompt attention 7 0-21 0.0-66.7 66.8-100
Respect for dignity 3 0-9 0.0-66.7 66.8-100
Clear communication 7 0-21 0.0-66.7 66.8-100
Respect of autonomy 3 0-9 0.0-66.7 66.8-100
Access to care 4 4-16 25.0-50.0 50.1-100
Respect for
confidentiality
3 0-9 0.0-66.7 66.8-100
Quality of basic
amenities
10 10-40 25.0-75.0 75.1-100
Overall responsiveness 37 14-125 11.2-67.2 67.3-100
Upon reliability testing, each domain of the health system responsiveness scored a
Cronbach’s alpha of greater than 0.7 (Table 5) indicating the tool was reliable.
Table 5: Reliabilities of each Domain of HSR
Items Number of items Cronbach’s Alpha
Prompt to attention 7 0.892
Respect to dignity 3 0.818
Clear communication 7 0.825
Autonomy 2 0.821
Access to care 4 0.822
Confidentiality 3 0.895
Basic amenities 10 0.817

91
The second step was to conduct the inferential statistics. The basic assumptions for
normality tests were conducted. Visual inspections of histogram Q-Q and box plots
(graphs) were done. Visual inspection of histograms indicated that dependent data
distribution was along the straight line for Q-Q plots for both dispensary and health
centre, whereas symmetry was observed on box plots for both dispensary and health
centre. In addition, skewness and kurtosis z-values and Shapiro-Wilk test for
dependent variables were conducted. Skewness and kurtosis z-values were within the
range of -1.96 to +1.96 for both dispensary and health centre (dispensary =.0599,
.543 and health centre =.245, .543). Shapiro Wilk test showed p ≥ .005 (p= .694 and
.828 for dispensary and health centre, respectively). These findings indicated that
data were approximately reasonably normally distributed. Therefore, parametric tests
for inferential statistics were considered relevant for performance comparisons. A t-
test was used to compare the means of the two groups (before and after).
A multivariable logistic regression analysis model was used to explore the
predictive power of each independent variable on the dependent variables,
specifically demographic information, and perceived responsiveness by the patients.
Multiple regressions were also used to assess the power of predictors for institutional
factors (e.g. staffing level, number of beds) with perceived responsiveness.
3.12.1.2.2 Categorization of Structural Quality of MHS
Using seven domains, the study assessed health facilities’ structural quality of MHS.
The cut-off point that was used was a mean score percentage of 60. This percent has
also been used by Gilson et al (1995) and in the star rating of health facilities in
Tanzania (Gilson, Magomi, & Mkangaa, 1995; Yahya & Mohamed, 2018). Mean
score was computed and those facilities that scored above the mean value were
graded as having high structural quality, while those facilities that scored below the
mean score were categorised as having low structural quality.
Scores of the respondents was used to categorize the respondents’ levels of structural
quality of maternal health services into two major categories [Category I= high
structural quality and Category II= low structural quality].
92
3.12.1.2.3 Categorization of Health Service Utilization
1. Institutional Deliveries
2. Use of IPT2
3. ANC mothers on Mebendazole (De-worming)
4. Number of women attending the fourth ANC visit
5. Number of HIV infected pregnant women receiving ART
6. New users of modern family planning methods
7. Proportion of PPHF with all 30 tracer medicines
8. Number of mothers receiving post-natal care services within three to seven
days
9. Pregnant mothers attending their first ANC below 12 weeks
This study used nine indicators relating to maternal health service utilization to
assess health service utilization at the PPHFs level. Mean score was computed and
those facilities that scored above the mean value were graded as having high health
service utilization, while those facilities that scored below the mean score were
categorised as having low health service utilization.
The scores of the respondents were used to categorize the respondents’ level of
knowledge into two major categories [Category I= high maternal health service
utilization and Category II= low maternal health service utilization].
3.12.1.2.4 Categorization of Fidelity of Implementation (FoI)
Fidelity of implementation was measured by using adherence towards DHFF
initiative. A total of 40 questions for health workers were asked to know whether the
health service providers implemented DHFF initiative. The adherence towards DHFF
implementation was used to decide the FoIframework through the cut-off points
(high or low). Levels of fidelity were interpreted as previously reported in the
literature, with ≥ 80% adherence interpreted as ‘high’ fidelity and <80% as ‘low’
fidelity (Bellg et al., 2004; Borrelli, 2012; Nurjono et al., 2019; Toomey et al., 2017).
The score of the respondents was used to categorize the respondent’s level of FoI
into two major categories [Category I= high FoI and Category II= low FoI].

93
Knowledge (Content): Health care providers were assessed for content by checking
their level of knowledge on DHFF and whether they received training and any
supportive supervision and mentorship. A total of 14 questions for health workers
and five questions for HFGC relating to what is done during DHFF were asked. The
questions had weighted points. The mean score was computed and those who scored
above the mean value of ≥ 9.286 points were graded as having adequate knowledge
while those scoring below < 9.2 points were categorized as having inadequate
knowledge of DHFF. Scores of respondents were categorized into two major groups
of knowledge categories: Category I= adequate content level and Category II=
inadequate content level.
3.13 Data Processing and Statistical Analysis
Data Processing and Quality Control
Data were collected and rechecked for completeness and consistency. Data from the
Open Data Kit (ODK) were extracted by using computer excel file, cleaned, and then
entered into the Statistical Package for Social Science ™ (SPSS) version 25 for
revised coding and analysis (for quantitative data).
3.13.1 Statistical analysis
Statistical analyses in this study used the following approaches: 1) univariate analysis
to describe the sample and distribution of the outcome and explanatory variables; 2)
bivariate analysis (logistic regression analysis) to establish the relationship and
association between variables; and 3) multiple regression analysis to establish
whether the explanatory variables could predict the outcome variables and to control
for confounding variables.
Descriptive statistics were used to generate frequency distribution, and cross
tabulation was used to describe the characteristics of the study participants. The chi
square test (χ2) was used to compare groups (categorical data) and odds ratio (OR)
with 95% confidence interval were computed and used to determine the strength of
association among variables. The statistical significance level was made at p= 0.05
(2-tail) as a cut-off point.
94
Forward stepwise logistic regressions analysis was done to establish whether the
predictor variables were independently associated with outcomes (dependent
variable) of interest. Also, it was done to control/adjust for any confounders. In the
logistic (binary) regression models the association between predictors and outcomes
was measured by odds ratios (ORs) and adjusted odds ratio (AOR) with the 95%
confidence intervals (CIs).
Multiple regression models were used to determine the variables that could predict
the four variables namely HSR, maternal health service utilization, structural quality
of MHS, and FoI. The comparisons within groups (Baseline/Endline) were estimated
using independent t-test for HSR, whereas paired t-test was used for structural
quality of MHS and Wilcoxon ranked signed test was used for maternal health
service utilization.
3.13.2 Governance and Accountability
In alignment with the objective number 7, thematic analysis was used to analyse data
that came from audio-recorded conversations and field notes that were transcribed
into transcripts. After familiarization, the transcripts were then imported into NVivo
QSR™ version 12 where themes and categories were developed.
3.14 Qualitative Data Analysis
For qualitative data, the extracted data from digital recorders were transcribed
verbatim and then thematically analysed using NVivo QSR™ version 12 and similar
codes and categories were grouped to form themes which was then grouped together
for meaningful interpretation and reporting. Quotations were used to support findings
of each theme.
Thematic Analysis
Two independent researchers carried out analyses of data from FGDs and IDIs based
on the original transcripts. The analyses utilized the thematic analysis method (Gale,
Heath, Cameron, Rashid, & Redwood, 2013) and were assisted by NVivo™
software (QSR-international) version 12. This method was selected due to its
95
flexibility and its step-by-step interconnected stages that guide the analytical process.
Previous research (Gale et al., 2013; Smith & Firth, 2011) emphasised the rigor and
transparent nature of this approach as demonstrated by its use of the matrix structure.
The approach is not aligned to any epistemological view point or theoretical
approach so it can be adapted for use in inductive or deductive analysis or a
combination of the two (e.g., using pre-existing theoretical constructs, deductively
then revisiting the theory with inductive aspects and vice versa). In addition, our
research approach was mainly descriptive and aligns itself to the pragmatic paradigm
makes the framework method a suitable approach for analysis (Smith & Firth, 2011).
Analysis followed the following steps: 1) verbatim transcription of audio recordings;
2) familiarization of recordings and field notes with the interview/FGDs; 3) labelling
and coding by underlining the key information; 4) forming categories; 5) formulating
sub-themes and themes; and 6) interpreting the themes. These steps are summarized
in the coding table that shows processes from coding, categories and finally themes
(Appendix XII). Other themes which emerged upon analysis were also incorporated
as part of the findings.
3.15 Integration of Quantitative and Qualitative methods
As this study used a mixed methods approach, it was therefore very important to
integrate findings from the two data sets. As quantitative findings had more weight
than the qualitative findings, we explored the convergence point in the objectives
(number one of the midline study) and the objective number two. Good Reporting of
A Mixed Methods Study (GRAMMS) was used to guide intergration process for
qualitative and quantitative processes (Kaur, Vedel, El Sherif, & Pluye, 2019;
O’Cathain, Murphy, & Nicholl, 2008). We looked if there were any complementarity
of information or any contradictions to each other. Integration allowed us to develop
a composite, holistic, and cross-validated picture of the reality based on results from
both quantitative and qualitative datasets. This process of integration took place after
completion of data analysis and it entailed identifying similarities and differences,
merging the results, and discussing the meaning of the integrated results. Figure 21
provides the integration steps of both.

96
Figure 21: Schematic Presentation of Integration of Mixed Methods
Triangulation Design for Measuring DHFF Fidelity of Implementation (FoI)
3.16 Trustworthiness and Credibility
3.16.1 Credibility: interpretation was achieved through data triangulation (FGDs
and indepth interviews), and supervisors checking repeated interviews. Also,
participation of research assistants’ familiar with the community and culture
potentially minimized threats to the truth-value and contributed to an accurate
presentation of the findings explored within the cultural context. The supervisors
helped in the quotes selection and making sure all protocols observed so that to
enable audit trail/confirmability audit.
Quantitative data
collection
Qualitative data
Collection
Quantitative data
analysis
Qualitative data
analysis
Integration of the Quantitative and
Qualitative Results

97
3.16.2 Dependability: in this study, was achieved through making sure that the
findings were consistent with methods used and repeatable. This was achieved
through cheking findings gathered by principal investigator by another reader
(supervisors) and all procedures were followed accordingly.
3.16.3 Transferability: is the degree to which the results of qualitative research can
be generalized or transferred to other contexts. As for this study, qualitative data
were collected from seven different regional settings making its findings possible to
be used and applied in another context.
3.17 Validity and Reliability
3.17.1 Validity
Validation of instruments was ensured through a researcher by consulting to the
supervisors and other researchers who have used the tools like that before.
3.17.2 Reliability
The pre-test was done in one of the primary health facilities under Dodoma City
Council that was not included in the actual study data collection exercise. The aim of
the pre-test was to identify how long the questions were taking to complete, to
identify the difficulties in questions, and to establish whether the instructions for the
questionnaire were understandable. Findings of this study were used to modify the
tool. Ambiguous questions were clarified and corrected to make the questions easily
understandable to the research participants.

98
Table 6: Data Analysis Plan and Measurement of Variables for Baseline and Endline Study
Specific
objectives
Dependent
variables
Independent variables Measurement Analysis technique
Objective
one
Health system
responsiveness
as perceived by
patient
experiences
Socio-demographic
characteristics
Training on DHFF
1. Supportive
supervision
2. Number of staff
per facility
3. Location of the
health facility
4. Health service
utilization
5. Fidelity of
implementation
The 37 questions were divided among the
seven domains of responsiveness: prompt to
attention (7), respect to dignity (3), clear
communication (7), quality of basic amenities
(11), confidentiality (3), access to care (4)
and autonomy (2). The internal consistency of
the overall responsiveness scale (37 items)
was measured for Cronbach’s alpha
(Nunnally & Bernstein, 1979) and had an
average of 0.827.
The questions in each domain were divided
into four groups:
Ordinal variables range 0 (never) to 3 (very
often) Ordinal variable ranging from 0 (very
big problem) to 3 (no problem)
Ordinal variable ranging from 1 (Waited for
long time) to 4 (serviced instantly) Ordinal
ranging from 1(strongly disagree) to 4
Descriptive statistics;
frequency of scores
distribution and mean &
SD
Cross tabulation for
checking differences of
scores among the
participants.
Independent t test
Regression analysis for
checking associations
among the variables.

99
(strongly agree)
Objective
two
Structural
quality of
maternal health
1. Socio-
demographic
characteristics
2. Training on
DHFF
3. Supportive
supervision
4. Number of staff
per facility
5. Location of the
health facility
7-domain observational checklist.
The domains were: 1) hygiene and sanitation,
2) waste management, 3) maternal audit, 4)
privacy, 5) sterilization equipment, 6)
obstetric emergency medicines, supplies and
equipment, 7) delivery room
Descriptive statistics
(mean, SD)
Cross tabulation to
compare groups’
performances
Paired Sample t Test
Regression analysis for
checking statistical
significances among and
between the participants
Objective
Three
Health Service
Utilization
1. Socio-
demographic
characteristics
2. Training on
DHFF
3. Supportive
supervision
4. Status of HFGCs
5. Number of staff
per facility
6. Location of the
1. Institutional deliveries
2. Consumption of IPT2
3. ANC mothers on Mebendazole
(Deworming)
4. Number of Women attending the 4th
ANC visit
5. Number of HIV infected pregnant
women receiving ARTs
6. New users of modern family planning
Descriptive statistics
(mean, SD)
Cross tabulation to
compare groups’
performances
Wilcoxon signed rank
test analysis for checking
statistical significances
among and between the
participants
100
health facility
methods
7. Proportion of PPHF with all 30 tracer
medicines
8. Number of mothers receiving post
natal care services within 3-7 days
9. Pregnant mothers attending their 1st
ANC below 12 weeks
Paired sample t-test for
comparing means
between the baseline and
end line surveys
Objective
Five
Governance and
accountability
10. FGDs interview guide Thematic analysis

101
Table 7: Objective number 4
Specific Objective Dependent
variable
Independent
variables
Measurement Analysis technique
Measuring fidelity
DHof implementation
for FF
FoI Adherence towards
DHFF
40 items questionnaires for health
service workers
Questions were divided into six
domains: 1) Training on DHFF
and FFARS, 2) coordination of
DHFF affairs, 3) Financial
management, 4) planning and
budgeting, 5) supportive
supervision, and 6) mentorship.
- Descriptive statistics on frequency,
mean & SD
- Cross tabulation to compare
adherence of the participants.
Logistic regression analysis
Participant’s
responsiveness
(acceptability)
towards DHFF
- 21 items semi - structured
interview questions
-Thematic analysis

102
3.18 Ethical Consideration
Ethical approval for this study has been granted by the University of Dodoma
(UDOM) ethical clearance committee and endorsed by National Institute of Medical
Research (NIMR) (Ref. No. NIMR/HQ/R.8a/Vol.IX/2740) (Appendix XVI).
Permission to conduct the study in the respective regions and districts was granted by
the President Office - Regional Administration and Local Government Authority
(PORALG), Regional Administrative Secretariat (RAS) and District Executive
Directors (DEDs). Oral informed consent was undertaken before the administration
of the questionnaires to the study participants (Appendix XV). Participants were able
to withdrawal from the study at any time. Confidentiality was guaranteed for the
participants, and only identification numbers (ID) were used to identify participants,
not names.

103
CHAPTER FOUR
RESULTS
4.0 Introduction
This chapter reports the main findings of the study. The report is arranged into sub-
sections to facilitate easy capture of the main findings in alignment with each
objective of the study.
The first sub-section is descriptive statistics of the study participants. The sub-section
contains the socio-demographic characteristics of health service providers, members
of health facility governance committee, DMOs, District DHFF Coordinators,
Council Health Service Board members and patients.
The second sub-section contains descriptive statistics results for each objective
covering the frequencies and percentages of the response from the study participants.
The third sub-section presents the actual performance/level/status of the objective
results. These includes level of health system responsiveness, level of
implementation fidelity, level of structural quality of maternal health service and
level of maternal health service utilization in PPHF.
The fourth sub-section presents the inferential statistics from each objective. This
part portrays factors attributing to the change in perfomance of the studied objectives
including change in health system responsiveness, structural quality of MHS and
maternal health service utilization before and after implementation of DHFF
initiative in PPHF.
The results are variably presented in the forms of percentages, graphs, figures, and
tables for simple identification/highlighting and ease of understanding of the
employed quantitative data analysis procedures.

104
4.1 Perception of Patients on Health System Responsiveness (HSR) in PPHF
4.1.1 Socio-Demographic Characteristics of Patients in PPHFs
This study included a total sample population of 844 patients who participated in an
exit interviews before (422) and after (422) study respecting HSR study. Of 844
patients (100% response rate) surveyed, 422 were surveyed before and the remaining
patients were surveyed after eighteen months of the study. Table 8 shows the
distribution of socio-demographic characteristics of respondents. The age of patients
ranged between 19 and 88 (mean, 37; SD ± 14) years. Most (36%) of the respondents
were in the age group of between 25 and 35 years; both sexes were equally
represented. Nearly two-thirds had primary education (63%) and 68% resided within
five kilometres of a PPHF. The majority (71%) had visited primary health facilities
more than five times for the past five years (Table 8).
Table 8: Social Demographic Characteristics of the Patients in PPHF (PPHFs)
before and after implementation of Direct Health Facility Financing (DHFF)
(n=844)
Before DHFF (n=422) After DHFF (n=422)
Variable Frequency Percentage Frequency Percentage
Region
Dodoma 62 14.69 59 13.98
Pwani 60 14.22 61 14.45
Mbeya 60 14.22 59 13.98
Katavi 60 14.22 64 15.17
Manyara 58 13.74 63 14.93
Shinyanga 62 14.69 55 13.03
Mtwara 60 14.22 61 14.45

105
Facility type
Dispensary 290 68.72 263 62.32
Health center 132 31.28 159 37.68
Location of the facility
Urban 219 51.90 219 51.90
Rural 203 48.10 203 48.10
Sex
Female 211 50.00 211 50.00
Male 211 50.00 211 50.00
Age group (Mean)(SD)
(Range)
37(14, 15-88)
≤24 80 18.96 81 19.19
25-35 150 35.55 155 36.73
36-44 91 21.56 68 16.11
≥45 101 23.93 118 27.96
Marital status
Married 308 72.99 281 66.59
Cohabiting 28 6.64 36 8.53
Single 65 15.40 75 17.77
Divorced/Separated 12 2.84 14 3.32
Widow/Widowed 9 2.13 16 3.79
Highest level of education
Never went to school 57 13.51 48 11.37
Primary 266 63.03 264 62.56

106
Secondary 69 16.35 79 18.72
Tertiary education 30 7.11 31 7.35
House hold size
(mean)(SD) (range)
5(2, 1-20)
<5 299 70.85 170 40.28
>5 123 29.15 252 59.72
Distance to the health
facility
Within 5 kilometres 284 67.30 288 68.25
5 - 10 kilometres 89 21.09 117 27.73
Above 10 kilometres 49 11.61 17 4.03
Frequency of attending
service delivery on the
same health facility
(Median and IQR)
Twice 51 12.09 30 7.11
Thrice 41 9.72 19 4.50
Four times 33 7.82 34 8.06
Five times 28 6.64 39 9.24
More than five times 269 63.74 300 71.09
4.1.2 Status of Health System Responsiveness (HSR) as perceived by patients in
PPHF (PPHFs) before and after implementation of Direct Health Facility
Financing (DHFF)
The perception of HSR among patients in PPHF was measured by seven domains
namely; prompt to attention, respect to dignity, clear communication, respect of
autonomy, access to care, respect for confidentiality, and quality of basic amenities
107
(Appendix I). These domains were assessed on a four - point likert scale ranging
from zero to three in five domains and one to four points in two domains as
explained in the methodology section (Table 4). The independent t-test was used to
determine significant change in perceived HSR among patients before (422) and after
(422) implementation of DHFF in PPHFs. The descriptive analysis revealed that the
overall mean score of HSR before implementation of DHFF was 62.84, SD and
range were 64.21, 10.05 respectively. Subsequently, upon implementation of DHFF,
the percentage mean score on the perceived HSR was 71.20, SD was 8.05 and range
stood at 48.87 to 99.25. Furthermore, the results portray that the percentage mean
difference among domains experienced a positive shift except for clear
communication and respect for confidentiality. The domain of respect of autonomy
had a higher mean difference (8.86) followed by quality of basic amenities (8.17) and
access to care (6.83) (Table 9). The overall responsiveness showed a significant
change from 62.84 to 71.20 (p<0.0001, 95% CI) percentage mean score upon the
implementation of DHFF.
Almost all regions showed change on HSR upon the implementation of DHFF except
for the Katavi region which showed no shift after the introduction of the DHFF
initiative as seen in Figure 22.

108
Figure 22: Regional pefromance on structural quality of MHS before and after
implementation of Direct Health Facility Financing (n=42).

109
Table 9: Two Sample Independent T-test for Perception of Patients towards Health System Responsiveness before and after
implementation of Direct Health facility Financing (DHFF) in PPHF (PPHF) (n=844, p=0.05)
Domain Patients’ perceptions
before DHFF
implementation
(Mean [95% CI])
Patientss
perceptions after
DHFF
implementation
(Mean [95% CI])
Mean
difference
T-value P-value
Respect of autonomy 76.74[74.18, 79.30] 85.60[83.89, 87.30] 8.86 5.67 <.0001
Quality of basic amenities 62.30[61.16, 63.45] 69.07[68.26, 69.88] 8.17 9.51 <.0001
Access to care 48.61[46.63, 50.59] 55.44[53.85, 57.02] 6.83 5.30 <.0001
Respect for dignity 78.95[76.82, 81.07] 82.02[80.28, 83.75] 3.07 2.20 0.0282
Prompt attention 79.40[77.48, 81.32] 81.01[79.47, 82.55] 1.61 1.28 0.2000
Clear communication 74.64[72.31, 76.98] 61.22[59.74, 62.69] 13.43 -9.58 <.0001
Respect for confidentiality 87.64[85.01, 90.26] 85.70[84.05, 87.36] 1.93 -1.22 0.2210
Overall responsiveness 62.84[61.88, 63.80] 71.20[70.42, 71.97] 8.36 13.33 <.0001

110
The descriptive results on the domain of respect for dignity has shown a significant
percentage change of patients who were shown courtesy and affection during service
provision by health care providers. Although clear communication had negative
change (Appendix III).
Furthermore, the current study has revealed that respect of autonomy had a
significant performance change upon the implementation of DHFF initiative
(p<.0001, 95%CI). The indicators in this domain showed that there existed a
potential change on the freedom of choice in health facilities from 47.87% to 72%.
Also, 73% of patients acknowledged the existence of adequate access to physicians
upon the implementation of DHFF as compared to the previous period (67%).
However, more than half (58%) of the patients interviewed in this research indicated
that there was limited freedom to choose services they prefer from physicians
(Appendix V).
Access to care was perceived to have lower change than other domains with
percentage mean difference of 6.83 (p<.0001). Given the overall perception of
patients the indicators have shown the potential improvement from the baseline data
towards end line, since the number of patients awaiting medical consultation
spending more than 30 minutes dropped from 49% to 34.6%. Also, patients in the
waiting roomfor more than 30 minutes decreased from 32% to 18%. However,
patients who spent more than 30 minutes for laboratory services rose from 10% to
18.9% (Appendix VI).
4.1.3 Factors Associated with change in overall perception of patients on Health
System Responsiveness in PPHF before and after implementation of Direct
Health Facility Financing.
In determining factors influenced perception patients towards health system
responsiveness, the cut off points for positive perception and negative perception for
overall health system responsiveness was first determined by assigning minimum
and maximum mean score. Negative perceptions of patients ranged between the
score of 11.2 – 67.2, while the positive perceptions ranged between 67.3 – 100 scores
(Table 4). The reliability was attested by a Cronbach’s alpha greater than 0.8 (Table

111
5). Moreover, there was an introduction of one variable namely time that was
categorized into two groups (i.e., before and after implementation of DHFF). This
variable has been created based on the time of the data collection, whereby those
patients from baseline were coded as 0 (Patients before DHFF) and those patients
from end line were coded as 1 (Patients after DHFF).
Using chi-squire test and binary logistic regression analysis assessed factors
contributing to the performance of HSR in PPHF. The logistic model in cooperated;
time (before and after DHFF introduction) and socio-demographic characteristics of
the patients (Table 10).
The findings showed that implementation of DHFF had almost nine times odds
(AOR = 8.919; CI = 4.953 - 16.060; p< 0.001) towards perception of positive health
system responsiveness among patients compared to before the implementation of this
initiative in the PPHF.
Moreover, household size and type of health facilities had significant association
with perception of patients on HSR but they were not statistically significant upon
adjusting with some other factors through AOR.
Other factors like implementation of RBF initiatives was also significantly associated
with patient’s perception on health system responsiveness (AOR = 5.984; CI = 3.416
- 10.480; p <0.001, nevertheless, renovation of PPHFs independently was not
statistically significant towards HSR.
The results from the multiple regression analysis supported the findings from the
indepenent t-test where before and after implementation of DHFF mean scores of
HSR were compared. Therefore, this denotes that DHFF has a significant effect on
improving HSR as repoted by the patients attending services at primary health
facilities.

112
Table 10: Chi-squire test for factors associated with change in overall
perception of Health System Responsiveness among patients who attended in
the public primary health care facilities before and after DHFF implementation
(n=844, p=0.05).
Variable Overall HSR Chi-square P-value
Negative N
(%)
Positive N
(%)
Time 87.4686 <. 0001
Before DHFF 137(30.90) 285(69.10)
After DHFF 29(6.87) 393(93.13)
Type of Health
Facility
9.4250 0.0021
Dispensary 60(15.19) 335(84.81)
Health center 106(23.61) 343(76.39)
Sex 1.8734 0.1711
Female 83(17.97) 379(82.03)
Male 83(21.73) 299(78.27)
Age 2.2017 0.5316
15-24 33(20.50) 128(79.50)
25-35 58(19.02) 247(80.98)
36-44 37(23.27) 122(76.73)
45+ 38(17.35) 181(82.65)
Marital status 1.2645 0.2608
Married and
cohabitates
123(18.84) 530(81.16)
Single, divorced,
separated, widow
43(22.51) 148(77.49)

113
Variable Overall HSR Chi-square P-value
Negative N
(%)
Positive N
(%)
and widowed
Level of education 2.1755 0.5368
No formal
education
17(16.19) 88(83.81)
Primary education 111(20.94) 419(79.06)
Secondary
education
25(16.89) 123(83.11)
Tertiary education 13(21.31) 48(78.69)
Household size 47.5625 <. 0001
≤5 152(22.62) 520(77.38)
>5 14(8.14) 158(91.86)
Distance to health
facility (km)
2.9501 0.2288
Within 5 120(20.98) 452(79.02)
5 - 10 32(15.53) 174(84.47)
Above 10 14(21.21) 52(78.79)
Health Facility
Visits
6.1990 0.1848
Twice 16(19.75) 65(80.25)
Thrice 16(26.67) 44(73.33)
Four times 17(25.37) 50(74.63)
Five times 17(25.37) 50(74.63)
More than five 100(17.57) 469(82.43)

114
Variable Overall HSR Chi-square P-value
Negative N
(%)
Positive N
(%)
Renovation and
RBF
41.5314 <. 0001
Both 2(9.52) 19(90.48)
Innovation
only
8(17.39) 38(82.61)
RBF only 16(6.64) 225(93.36)
None 140(26.12) 396(73.88)

115
Table 11: Logistic regression model for factors associated with change in overall perception of Health System Responsiveness
before and after implementation of Direct Health Facility Financing in PPHF (p<0.05, 95% CI).
Unadjusted logistic model Adjusted logistic model
Variable OR [95%CI] p-value AOR [95%CI] p-value
Time <. 0001 <. 0001
Before DHFF Reference Reference
After DHFF 6.514[4.243, 10.001] 8.919[4.953, 16.060]
Type of the Health facility 0.0023 0.7712
Dispensary Reference Reference
Health center 0.580[0.408, 0.823] 1.063[0.705, 1.603]
Sex 0.1716
Female Reference
Male 0.789[0.562, 1.108]
Age 0.5334

116
Unadjusted logistic model Adjusted logistic model
Variable OR [95%CI] p-value AOR [95%CI] p-value
<30 Reference
31-44 1.098[0.681, 1.770]
45-64 0.850[0.500, 1.445]
65+ 1.228[0.731, 2.062]
Marital status 0.2614
Married Reference
Single 0.799[0.540, 1.182]
Level of education 0.5389
No formal education Reference
Primary 0.729[0.417, 1.276]
Secondary 0.951[0.484, 1.865]
Tertiary education 0.713[0.320, 1.593]
Household size (Mean)(SD) <.0001 0.3070

117
Unadjusted logistic model Adjusted logistic model
Variable OR [95%CI] p-value AOR [95%CI] p-value
≤5 Reference Reference
>5 3.298[1.855, 5.864] 0.671[0.313, 1.442]
Distance to the health facility (km) 0.2317
Within 5 Reference
5 - 10 1.443[0.941, 2.213]
Above 10 0.986[0.529, 1.840]
Number of Facility visit in the past 0.1898
Twice Reference
Thrice 0.677[0.307, 1.494]
Four times 0.724[0.333, 1.573]
Five times 0.724[0.333, 1.573]
More than five times 1.154[0.641, 2.079]
Renovation and RBF <. 0001 <. 0001

118
Unadjusted logistic model Adjusted logistic model
Variable OR [95%CI] p-value AOR [95%CI] p-value
Both 3.359[0.772, 14.603] 0.1062 4.168[0.902, 19.256] 0.0675
Renovation only 1.679[0.765, 3.687] 0.1964 1.838[0.798, 4.230] 0.1525
RBF only 4.972[2.890, 8.553] <. 0001 5.984[3.416, 10.480] <. 0001
None of them Reference Reference
No other factor could explain the change in reported health system responsiveness except time of the intervention and whether facilities
were implementing RBF and renovation interventions at the time of this study.

119
4.2 Level of Structural Quality of MHS in the PPHF before and after Direct
Health Facility Financing Implementation
4.2.1 Demographic Characteristics of PPHF before and after implementation of
Direct Health Facility Financing
A total of 42 (100%) public primary health facilitates were assessed on structural
quality of MHS. Of all the facilities assessed 14 (33.3%) were health centers,
whereas 28 (66.7%) were dispensaries. The furthest primary health facilities from the
district head office were 140 kms and the nearest 2 kms.
One third of health facilities was located in the rural areas (Table 12). The majority
(60%) of health centers had less than 39 skilled staff and majority (88.89%) of
dispensaries had less than 15 staff (Table 12). Some health facilities experienced
critical shortage of staffs; for instance, five (17.89%) dispensaries had 2 staff only
while another 16 (57.14%) dispensaries had 3 staff.
The average annual deliveries per dispensary before DHFF were 120 while that of
health center was 1,203 after introduction of DHFF initiative. Upon the introduction
of DHFF the average deliveries at dispensary level increased to 230 where as that of
health center plunged to 1,313.
Majority (37.04%) of dispensaries had a catchment population of less than 5,000
people while the majority of health centers (40%) had a catchment population of
more than 30,001.
Of all 42 studied primary health facilities, 25 had piped water, 11 they were using a
rainwater harvesting system, 5 had bore holes and 1 health facility did not have a
reliable water source. Of all the studied health facilities, 14 had ambulances and, of
those ambulances, only 8 were functional.

120
Table 12: Characteristics of the Public Primary Health Facilities before and
after implementation of Direct Health Facility Financing (n=42).
Variable Before DHFF After DHFF
Number
of HFs
Percentage Number of
HFs
Percentage
Region
Dodoma 6 14.29 6 14.29
Pwani 6 14.29 6 14.29
Mbeya 6 14.29 6 14.29
Katavi 6 14.29 6 14.29
Manyara 6 14.29 6 14.29
Shinyanga 6 14.29 6 14.29
Mtwara 6 14.29 6 14.29
Location of health
facility
Urban 21 50.00 21 50.00
Rural 21 50.00 21 50.00
Facility type
Dispensary 28 66.67 28 66.67
Health centre 14 33.33 14 33.33
Catchment population
(Mean) (SD) (Range)
Dispensary
8735(6629, 1723-22039) 8735(6629, 1723-22039)
<5,000 10 37.04 10 37.04
5,000 – 10,000 8 29.63 8 29.63
>10,000 9 33.33 9 33.33

121
Catchment population
(Mean) (SD) (Range)
Health centre
25831(14442, 9105-
52781)
25831(14442, 9105- 52781)
<20,000 6 40.00 6 40.00
20,0000 – 30,000 3 20.00 3 20.00
>30,001 6 40.00 6 40.00
Number of beds (Mean)
(SD) (Range)
Dispensary
5(5,1-20) 6(3,1-16)
<10 26 92.86 24 88.89
≥10 2 7.14 3 11.11
Number of beds (Mean)
(SD) (Range) Health
centre
25(8,13-38) 33(15,12-56)
≤20 5 35.71 4 26.67
>20 9 64.29 11 73.33
Average annual
deliveries
Dispensary
≤50 12 44.44 7 25.93
51 – 100 4 14.81 7 25.93
101 – 150 5 18.52 5 18.52
151 – 200 1 3.70 2 07.41
>200 5 18.52 6 22.23
Health centre
≤150 1 6.67 3 20.00

122
151– 300 2 13.33 4 26.67
301 – 450 1 6.67 1 06.67
451 – 600 3 20.00 1 06.67
>600 8 53.33 6 40.00
Number of staffs (Mean,
SD, Range) Dispensary
6(6,2-34) 6(4,2-18)
0 – 14 26 92.86 24 88.89
≥15 2 7.14 3 11.11
Number of staffs (Mean,
SD, Range) Heath centre
39(33,10-110)
42(35,13-120)
0 – 38 10 71.43 9 60.00
≥39 4 28.57 6 40.00
Availability of
ambulance
Not available 28 66.67 28 66.67
Available 14 33.33 14 33.33
Available & source of
energy in health facility
No Electricity 6 14.29 6 14.29
National Grid 20 47.62 20 47.62
Solar Panels 12 28.57 12 28.57
Generator 2 4.76 2 4.76
Others 2 4.76 2 4.76
Available & source of
water in health facility

123
No sources 1 2.38 1 2.38
Piped Water into Health
Facility
21 50.00 21 50.00
Rainwater Harvesting 11 26.19 11 26.19
Public Tap or Standpipe 4 9.52 4 9.52
Tube Well or Borehole 2 4.76 2 4.76
Others 3 7.14 3 7.14
Status of HFGCs
Dispensary
Active 167 95.98 112 82.35
Inactive 7 4.02 24 17.65
Health center
Active 168 96.55 96 94.12
Inactive 6 3.45 6 5.88
New project introduced/
implemented during
study period
Dispensary 0 0 0 0
Health center 0 0 5 28.57
The descriptive results from the individual domains showed that there were
percentage mean differences existed before and after implementation of DHFF
initiative. There was slight percentage mean change in the structural quality domains
after DHFF implementation compared to when DHFF was not introduced (Table
13).

124
Table 13: Descriptive Results on Change of Structural quality of MHS in
Tanzania before and after DHFF implementation (n= 42).
Domain Before
DHFF
After
DHFF
N % N %
Privacy
All service delivery rooms have doors that
close
36 85.71 41 97.62
All service delivery rooms with screen to
partition the examination area/bed
24 57.14 33 78.57
Windows with curtains or painted or with
frosted glass
28 66.67 35 83.33
Divider (screen/curtain) if the service delivery
room is shared.
24 57.14 34 80.95
Hygiene
Functioning toilet [VIP] latrine which is not
full OR a flushing toilet with work
33 78.57 37 88.10
Toilets clean inside and out with no stagnant
water and no foul smells
18 42.86 35 83.33
Presence of toilet paper or water. In case of
flushing toilet, a dust bin
17 40.48 30 71.43
Hand-washing facilities just outside the toilet
or with basin inside toilet [soap]
13 30.95 23 54.76
No organic waste 30 71.43 38 90.48
No used syringes, needles 19 45.24 37 88.10

125
Domain Before
DHFF
After
DHFF
N % N %
No used bandages or dangerous products on
the ground of the facility that area
6 14.26 37 88.10
Do the burning chamber fenced in and ash pit
available?
6 14.26 20 47.62
Do the placenta pit with slab and cover
available?
6 14.26 33 78.57
Labour ward
Delivery bed functional, clean, adjustable,
with a footstool
23 56.10 39 92.86
One functional gouse neck lamp / light source 17 41.46 24 57.14
One functional new-born weighing scale 36 87.80 40 95.24
One drum with Sterile gauze (with date and
closed)
18 43.90 34 80.95
One drum with cotton wool (with date and
closed),
16 38.10 32 76.19
One Suction machine 16 39.02 36 85.71
Resuscitation kit (Ambu-bag, tubes) 27 65.85 38 90.48
One Mackintosh for each delivery bed 28 68.29 40 95.24
At least 2 sterilized delivery trays 28 68.29 38 90.48
Two Plastic aprons 28 68.29 37 88.10
Two pairs Gumboots/closed shoes 28 68.29 30 71.43
Two Masks 28 68.29 24 57.14
Two Goggles 28 68.29 24 57.14

126
Domain Before
DHFF
After
DHFF
N % N %
At least one full or nearly full box of Clean
(50 pairs)
28 68.29 34 80.95
One full or nearly full Sterile gloves (50 pairs) 28 68.29 32 76.19
Obstetric Care
Sterilized manual removal aspiration kit
available [MVA kits2]
7 50.00 13 86.67
Blood transfusion facilities available [Blood
bank with 5 units different groups
3 21.43 6 40.00
Presence of Vacuum extractor 8 57.14 9 60.00
Presence of Gun let gloves for manual
removal of placenta
8 57.14 10 66.67
Suction machine 13 92.86 15 100.00
Resuscitation kit [Ambubags different sizes,
Sodium bicarbonate, Vit. K]
11 78.57 13 86.67
Three bottles of Ringer lactate, Three bottles
of Normal saline 1000mls
11 78.57 13 86.67
Sets of cannula, Gauge 14 & 18 13 92.86 11 73.33
Giving sets 3 11 78.57 14 93.33
Syringes 2cc, 5cc, 10cc [5,5,5] 10 71.43 15 100.00
Magnesium Sulphate 14 100.00 15 100.00
Nifedipine/Hydralazine 9 64.29 12 80.00
Metronidazole Inj. 8 57.14 11 73.33
Ampicillin inj. OR Gentamycin inj. 9 64.29 13 86.67

127
Domain Before
DHFF
After
DHFF
N % N %
Ceftriaxone inj. 7 50.00 12 80.00
Oxytocin 7 50.00 15 100.00
Sedatives (E.g. diazepam) 11 78.57 13 86.67
Waste management
Labor ward and dressing room 4 9.52 38 90.48
Three buckets, each bucket clearly labeled
with todays date, 1 bucket with chloro
2 4.76 30 71.43
Inclient wards (Including labor ward,
laboratory and immunization/injection room)
8 19.05 38 90.48
At least 1 safety box with sharps not
exceeding ¾ full, and no sharps sitting on
6 14.29 40 95.24
Proper waste segregation using Red, Yellow
and Black/Blue bins with color coded
8 19.05 36 85.71
Liners labeled bin liners ok in lieu of colored 11 26.19 30 71.43
Sterilization
Existence of proper means / methods of
sterilizing instruments: Steam sterilization
36 85.71 39 92.86
SOPs for sterilization displayed on the wall by
the equipment
16 38.10 17 40.48
Each pack has an indicator for control of
sterility (litmus or date of sterilization
15 35.71 21 50.00
Maternal death audit
Select one audited case and check if it is
completely
6 14.29 10 23.81

128
Domain Before
DHFF
After
DHFF
N % N %
Check the selected audited case if it is
correctly filled
6 14.29 9 69.23
Check the selected audited case if it is action
plan in place
6 14.29 8 61.54
Assess if the strategies are in place with
emphasis on ANC clinic
9 32 76.19
Assess if the strategies are in place with
emphasis on labour and delivery
9 21.43 32 76.19
Assess if the strategies are in place with
emphasis on post-natal care
9 21.43 30 71.43
Assess if the strategies are in place with
emphasis on Client/Community factors
9 21.43 30 71.43
4.2.2 Level of Structural Quality of Maternal Health Service in PPHF before
and after implementation of Direct Health Facility Financing.
The level of structural quality of MHS was assessed by using seven domains of
maternal related indicators (Table 14). The overall structural quality was determined
by using mean score percentage of 60 cut-off point adopted from previous studies
(Gilson et al., 1995; Yahya & Mohamed, 2018). The descriptive results portays that
mean, median, and standard deviation before implementation of DHFF were 29.77,
27.20 and 16.40 respectively. Upon the implementation of DHFF mean, median and
standard deviation changed to 44.10, 40.50 and 19.53 correspondingly. The mean
difference before and after implementation of DHFF was 14.33, while change in
median and standard deviation were 17.43 and 18.56 respectively. Normality of data
was tested by using Kolmogorov–Smirnov test and was found to be normally
distributed, therefore the change of structural quality of MHS in PPHF was
determined by using paired t-test.

129
The performance of structural quality of maternal health service from paired T-test
portrayed overall structural quality had a significant change (p<0.001) with mean
difference of 19.39 from the baseline to endline. Moreover, 30.95% of PPHFs scored
above 60% mean score which was a cutoff point for high structural quality of MHS
post-DHFF implementation as compared to 2.38% of PPHFs which scored below
cutoff point pre-DHFF introduction (Figure 23). This significant change was also
observed in the specific domains of structural quality except sterilization of medical
equipment that had no significant change before and after, while availability of
health commodities for obstetric services showed a negative change (Table 14).
The results show that maternal audit had a significantly higher (p<0.001) mean
difference (7.62), followed by the labour ward which had mean difference of 3.55
(p<0.001), hygiene and sanitation and privacy had mean difference of 1.26 (p=0.001)
and 0.74 (p=0.001) respectively (Table 14).
However, the overall change of structural quality of MHS showed that before the
implementation of DHHF only 2.38% (Figure 23) of primary health facilities had
higher structural quality of maternal health service but after eighteen months of
DHFF implementation there were a hike in the number of primary health facilities
with higher structural quality of MHS to 30.95% as shown in Figure 23 below.
.

130
Table 14: Paired T-test Results for Change in Structural Quality of MHS in PPHFs before and after implementation of DHFF
(n=42, p=0.05, CI = 95%).
Domain Mean (95%CI) Mean
deference
T-value P-value
Privacy
Before implementation of DHFF 2.67 [2.29,3.04] 0.74 3.56 0.0010
After implementation of DHFF 3.41 [3.10,3.71]
Hygiene and Sanitation
Before implementation of DHFF 3.83 [3.14,4.53] 1.26 3.60 0.0009
After implementation of DHFF 5.10 [4.59,5.60]
Labour room
Before implementation of DHFF 6.62 [5.51,7.73] 3.55 6.57 <. 0001
After implementation of DHFF 10.17 [9.39,10.94]

131
Domain Mean (95%CI) Mean
deference
T-value P-value
Waste management
Before implementation of DHFF 3.83 [3.14,4.53] 0.86 2.26 0.0290
After implementation of DHFF 4.69 [4.19,5.19]
Availability of Obstetric emergences medicines
Before implementation of DHFF 13.02 [10.84,15.21] -3.76 -2.79 0.0080
After implementation of DHFF 9.26 [5.25,13.27]
Sterilization of medical equipment
Before implementation of DHFF 1.60 [1.32,1.87] 0.24 1.50 0.1423
After implementation of DHFF 1.83 [1.56,2.11]
Maternal death Audit
Before implementation of DHFF 4.64 [2.62,6.66] 7.62 4.51 <. 0001
After implementation of DHFF 12.26 [9.55,14.98]

132
Domain Mean (95%CI) Mean
deference
T-value P-value
Overall Structural quality
Before implementation of DHFF 24.71[20.46,28.95] 19.39 7.10 <.0001
After implementation of DHFF 44.10[38.01,5018]
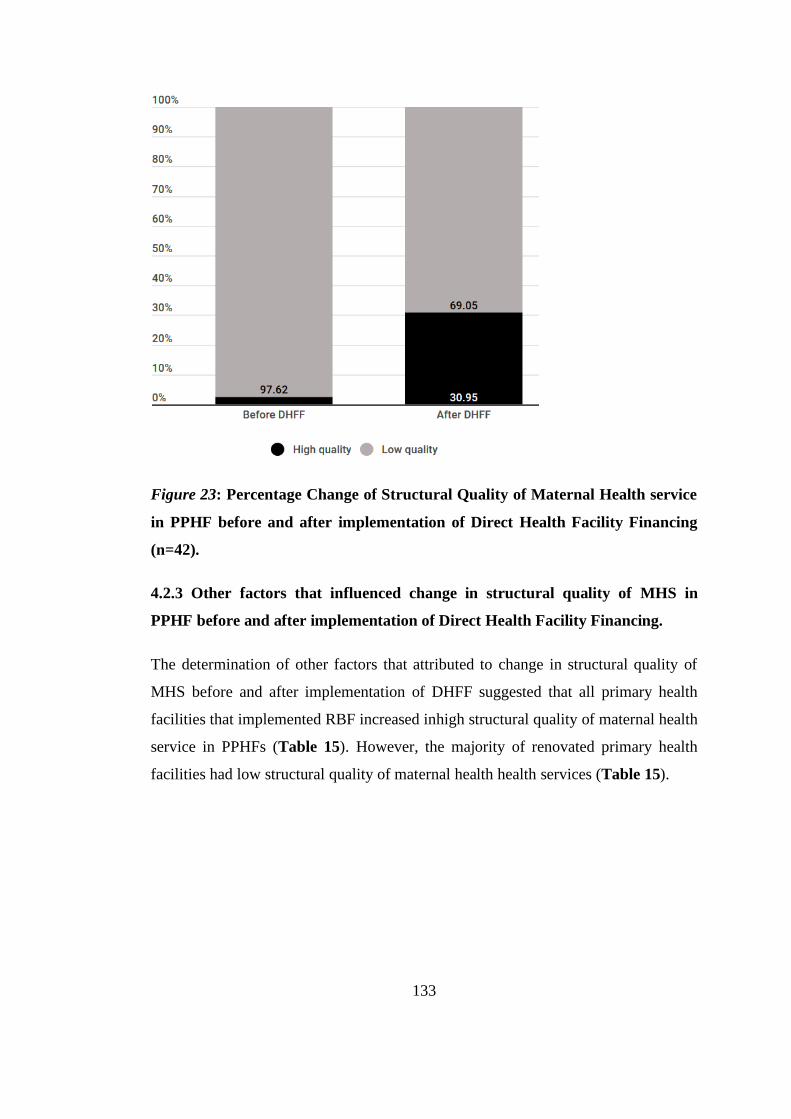
133
Figure 23: Percentage Change of Structural Quality of Maternal Health service
in PPHF before and after implementation of Direct Health Facility Financing
(n=42).
4.2.3 Other factors that influenced change in structural quality of MHS in
PPHF before and after implementation of Direct Health Facility Financing.
The determination of other factors that attributed to change in structural quality of
MHS before and after implementation of DHFF suggested that all primary health
facilities that implemented RBF increased inhigh structural quality of maternal health
service in PPHFs (Table 15). However, the majority of renovated primary health
facilities had low structural quality of maternal health health services (Table 15).

134
Table 15: Fisher’s exact test results for other factors that attributed to change in
overall structural quality of MHS in PPHF before and after implementation of
Direct Health Facility Financing (n= 42).
Variable Low
Structural
quality
High
Structural
quality
P-value
Neither Renovation nor RBF 0.0485*
No 10(66.67) 5(33.33)
Yes 10(37.04) 17(62.96)
RBF 0.0457*
No 20(52.63) 18(47.37)
Yes 0(0.00) 4(100.00)
Renovation 0.0024*
No 10(32.26) 21(67.74)
Yes 10(90.91) 1(9.09)
On the same note the results from cell analysis portrayed that observed cases for
PPHFs without implementation of RBF and Renovation had significant influence on
high structural quality, also all facilities implementing RBF had higher influence on
high structural quality while renovation alonehad no significant influence on
structural quality (Table 16).
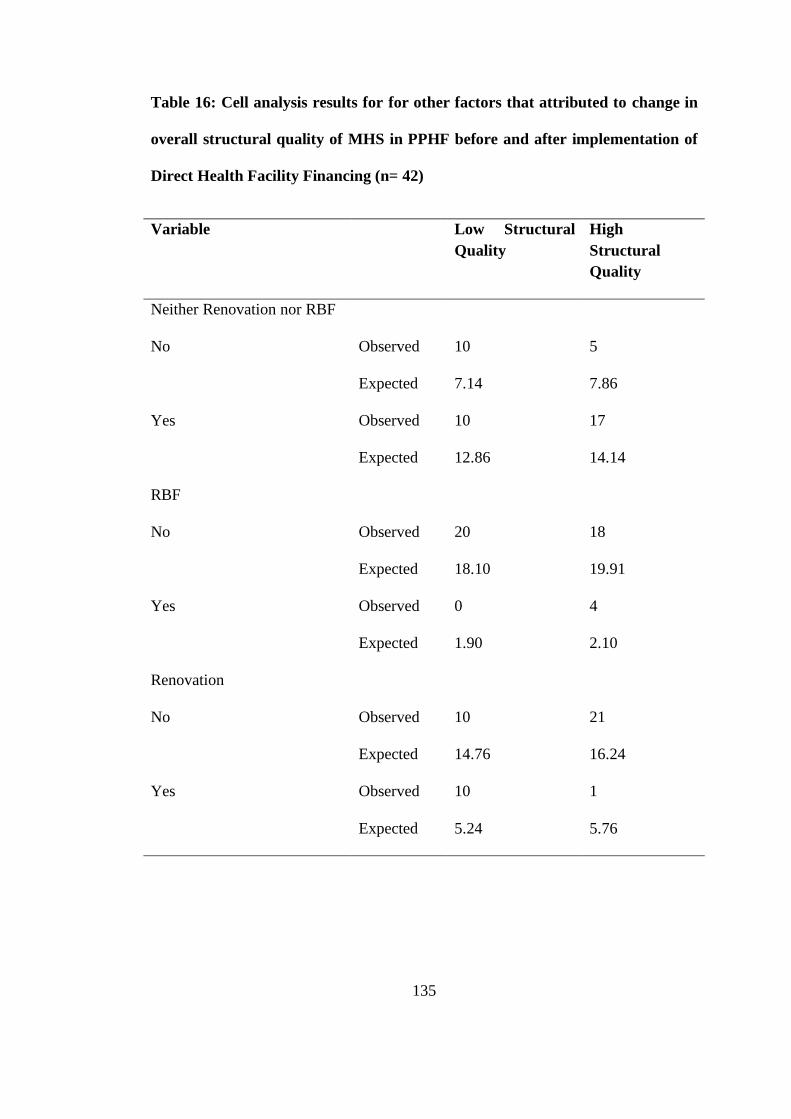
135
Table 16: Cell analysis results for for other factors that attributed to change in
overall structural quality of MHS in PPHF before and after implementation of
Direct Health Facility Financing (n= 42)
Variable Low Structural
Quality
High
Structural
Quality
Neither Renovation nor RBF
No Observed 10 5
Expected 7.14 7.86
Yes Observed 10 17
Expected 12.86 14.14
RBF
No Observed 20 18
Expected 18.10 19.91
Yes Observed 0 4
Expected 1.90 2.10
Renovation
No Observed 10 21
Expected 14.76 16.24
Yes Observed 10 1
Expected 5.24 5.76

136
4.3 Level of maternal health service utilization in PPHF before and after
implementation of Direct Health Facility Financing
In this study, maternal health service utilization was assessed by using selected nine
indicators of health service utilization namely number of institutional deliveries,
number of women attending 4th ANC visits, number of ANC mothers given IPT2,
number of ANC mother initiated mebandazole for deworming, availability of 30
tracer medicines, and use of modern family planning methods.
Also, the study incorporated indicators for number of HIV positive pregnant women
receiving ARVs, number of new users on modern family planning methods and
number of pregnant mothers attending first ANC visit with first 12 weeks of
pregnancy. Moreover, the study covered postnatal services by assessing the number
of mothers receiving postnatal services within three to seven days after delivery.
Furthermore, this study established the status of the availability of all 30-tracer
medicine before and after the implementation of DHFF in PPHFs.
Data for assessing these indicators were extracted from Health Management
Information System (HMIS) using District Health Information Sofware (DHIS2).
The data covered the period of two years namely (January – December) 2017
reflecting the period before the implementation of DHFF and two years later in
(January – December) 2019 after the implementation of DHFF. Moreover, results
from the descriptive analysis shows that mean, median, and standard deviation before
implementation of DHFF were 3652, 1897 and 4476 while after the implementation
of DHFF they changed to 4792, 3089 and 4942 respectively.
The results from the current study showed that, the overall maternal health service
utilization had significant positive mean difference (mean difference = 515; p=0.05),
however, service utilization at the dispensary level had higher significant positive
change as compared to the health center level (Table 17). Moreover, the dispensary
had significant positive mean difference in all nine indicators compared to only three
indicators (i.e., number of women attending four ANC visits, attending first ANC
before 12th week, and HIV positive pregnant women receiving ARV) that were
statistically significant in health centers.

137
The results of this study showed change on the user of modern family planning
methods was higher than other indicators with a mean difference of 262 (p<0.001).
Attendance at the 4th ANC visit and ANC visit within 12 weeks were significantly
positively increased upon the introduction of DHFF with mean difference of 236
(p<0.001) and 140 (p<0.001) respectively.
Further significant change was observed on institutional deliveries, use of IPTp2 and
post-natal services within three to seven days. The proportion of availability of tracer
medicines in PPHFs had a mean difference of 3.64 (p=0.02) pre and post DHFF.
Upon running into the Wilcoxon signed ranged test it was found out that; All
domains of maternal health service utilization were significant after the introduction
of DHFF except for the use of IPT2 (Table 17) and number of HIV infected women
who had significant negative change between the baseline and endline.
4.3.1 Other factors associated with Change of Maternal Health Service
Utilization in PPHF before and after implementation of Direct Health Facility
Financing.
As Table 17 signifies the implementation of DHFF as one of the factors that
attributed to the change in health service utilization at PPHFs, the current study
further explores other factors that attributed to this change. The Poisson regression
analysis was used to determine other factors for the change of maternal health service
utilization in PPHFs since the dependent variable was discrete and assumed
occurrence of events were independent of the outcome, also mean and standard
deviation of overall health service utilization were 1142.52 and 1511.35 respectively
which are close and attained poisson regression model assumptions.
The results from the poisson regression analysis indicated that health centers, rural
health facilities, staffing level, structural quality of MHS and other health program
such that RBF and Renovation of PPHF were significantly associated with change of
maternal health service utilization in primary health facilities (Table 18).

138
Table 17: Wilcoxon signed rank test for Change in Maternal Health Service
Utilization before and after implementation of Direct Health Facility Financing
in PPHF (n=42, p= 0.05).
Indicator Before
DHFF
(2017)
After
DHFF
(2019)
Difference
Mean
Student's
t-test
p-value
Institutional deliveries
Dispensary 170 194 72 4.39 0.0003*
Health center 1203 1701 526 2.55 0.0244
Overall 537 765 249 2.85 0.0074*
Use of IPT2
Dispensary 197 465 271 3.59 0.0016*
Health center 1004 1091 4.92 0.01 0.9885
Overall 492 686 175 1.36 0.1835
Number of ANC mother
initiated on Mebandazole
(De-Worming)
Dispensary 302 428 127 3.56 0.0016*
Health center 974 1172 325 1.64 0.1295
Overall 537 676 191 2.78 0.0085*
Number of Women
attending 4th ANC Visit
Dispensary 137 263 181 4.50 0.0001*
Health center 363 831 573 3.47 0.0046*
Overall 220 452 315 4.62 <
.0001*
Number of HIV positive

139
pregnant on ARVs
Dispensary 17 3 -19 -3.44 0.0262
Health center 39 14 -35 -34.67 0.0061*
Overall 24 7 -24 -24.62 0.0009*
Number of new users on
modern Family Planning
methods
Dispensary 826 1225 595 4.04 0.0005*
Health center 2961 2838 408 1.04 0.3154
Overall 1589 1819 262 3.114 0.0036*
Public health facility with
all 30-tracer medicines
Dispensary 91.23 95.61 4.36 4.31 0.0002*
Health center 92.72 95.13 2.41 0.92 0.3717
Overall 91.77 95.44 3.6439 3.20 0.0027*
Number of mothers
receiving Post Natal
Services within 3-7 days
after delivery
Dispensary 63 119 52 2.69 0.0126*
Health center 591 653 62 1.12 0.2824
Overall 256 310 56 2.39 0.0219*
ANC before 12 weeks of
Gestation
Dispensary 50 145 95 3.54 0.0022*
Health center 202 431 216 3.99 0.0021*

140
Overall 107 246 140 5.04 <.
0001*
Overall Utilization
Dispensary 1657 2386 1149 4.39 0.0002*
Health center 7243 8374 1130 1.76 0.0998
Overall 3652 4794 1143 4.09 0.0002*
Table 18: Poisson Regression Model for other factors associated with change of
maternal health service utilization in Public Primary Health Facilities before
and after implementation of DHFF.
Parameter Estimate Standard
Error
Wald 95%
Confidence
Limits
Wald
Chi-
Square
Pr > ChiSq
Intercept 6.9542 0.0115 6.9316 6.9767 365921 <.0001
Facility type
Health center -0.3256 0.0162 -
0.3572
-
0.2939
405.90 <.0001
Dispensary Ref
Location
Rural 0.1567 0.0108 0.1355 0.1780 209.67 <.0001
Urban Ref
Structural quality
of ,MHS
0.0162 0.0004 0.0155 0.0170 1907.89 <.0001
Renovation and
RBF
Done 0.7092 0.0135 0.6828 0.7356 2768.64 <.0001
Not done Ref

141
4.4 Level of Direct Health Facility Financing (DHFF) Fidelity of
Implementation (FoI) and its potential moderators
The FoI of DHFF was assessed in two categories namely the knowledge of health
care workers to implement the iniative and the adherence of the health care workers
towards the guiding principles for implementation of DHFF in PPHFs.
4.4.1 Socio-Demographic Characteristics of Health Service Providers in
PPHFs
A total of 238 of health service providers participated in the study for fidelity of
implementation. Of 238 health service providers participated, more than two-third
were (70.59%) were male. Most of health service providers were between 31 and 44
years old. In terms of education, half of health service providers were certificate
holders, followed by diploma holders (30.67%) and university degree holders
(8.40%). More than half of the participants had employment experience less than 10
years, while 21% had work experience of between 10 and 20 years. Similarly, 50%
of health service providers were nurses, while clinicians were 11.76% of the sample
and assistant accountants were 3.78%. More than two-thirds of the health service
providers were frontline health service providers, while 4% were health managers
(Table 19).

142
Table 19: Social Demographic characteristics of Health Care Workers (HCWs)
in PPHF implementing DHFF.
End line
Variable Frequency Percentage
Region
Dodoma 43 18.07
Pwani 57 23.95
Mbeya 25 10.50
Katavi 26 10.92
Manyara 26 10.92
Shinyanga 33 13.87
Mtwara 28 11.76
Facility type
Dispensary 102 42.86
Health center 136 57.14
Location of the facility
Urban 124 52.10
Rural 114 47.90
Sex
Female 70 29.41
Male 168 70.59
Age group Mean [SD, Range] 37.9 [10.2,22-59]
≤ 35years 123 51.68
>35 115 48.32
Marital status

143
Married, cohabiting 164 68.91
Single, divorced, separated, widow and
widowed
74 31.09
Highest level of education
Certificate 125 52.52
Diploma 68 28.57
Advanced diploma 5 2.10
University degree 20 8.40
Masters (MMED) 3 1.26
Other 17 7.14
Years of experience (Median, IQR) (8.0, 1-41)
≤ 10 144 60.50
>10 94 39.50
Cadre
Nurse 120 50.42
Clinicians 28 11.76
Assistant Accountant 9 3.78
Medical Attendant 48 20.17
Pharmacist 13 5.46
Laboratory personnel 20 8.40
Position Distribution
Health service provider 180 78.60
Matron/Patron 7 3.06
In charge 3 1.31
Assistant Account 9 3.93
Supporting staffs 30 13.10

144
4.4.2 Knowledge of Health Service Providers on the implementation of Direct
Health Facility Financing in PPHF.
Out of 238 health service providers, 75.63% (180) had adequate knowledge in
relation to DHFF (mean scored >9.286 points) while 24.37% (58) had inadequate
knowledge. The mean score was 9.286 (SD =4.1409; range 0 -16) points indicated
that, on average, health service providers had adequate content on DHFF.
The participant’s awareness was 88.24% however, descriptive results on the
assessment of knowledge had shown that, 95.71% of HSPs acknowledge that DHFF
is different from the previous method of sending money to PPHFs; while 30% can
explain properly what DHFF meant, and 22.86% were trained or oriented about
DHFF prior to its implementation.
Table 20: Descriptive results of knowledge among health care workers in PPHF
during the implementation of Direct Health Facility Financing
Variable Frequency Percentage
Have you ever heard about DHFF program?
No 28 11.76
Yes 210 88.24
Where did you hear about DHFF program?
On the training 22 10.48
From In charge of HF 133 63.33
From other staffs 42 20.00
Somewhere else 13 6.19
What does DHFF Really mean?
Direct submission of funds to the primary Health
Facilities from treasurer.
144 68.75

145
Direct submission of funds from whatever source to
the primary health facilities
107 31.43
Does DHFF differ from the previous disbursement
mechanism?
No 9 4.29
Yes 201 95.71
DHFF must start from the treasurer
No 47 23.38
Yes 154 76.62
DHFF select few funding sources
No 107 53.23
Yes 94 46.77
It should be disbursed on a monthly basis
No 150 74.63
Yes 51 25.37
DHFF does not need presence of HFGC?
No 106 52.74
Yes 95 47.26
Do the health workers abide to financial regulations
when implementing DHFF?
No 9 4.29
Yes 201 95.71
Timely reporting on income and expenditures
No 15 7.46
Yes 186 92.54
Use of receipts whatever the transaction is done
No 22 10.95

146
Yes 179 89.05
Abide to procurement regulations
No 1 0.50
Yes 200 99.50
Preparation of performance report
No 1 0.50
Yes 200 99.50
Where you trained on FFARS and DHFF initiative
No 162 77.14
Yes 48 22.86
Looking into level of FoI and the knowledge of health care workers. It was found out
that of 238 health workers who participated in the study, 75.63% had adequate
knowledge and 27.73% had high FoI towards DHFF (Table 21).
Table 21: Level of FoI among Health Service Providers in PPHFs
Variable Frequency (Percent)
Knowledge
Adequate knowledge (>9.9878049) 180 (75.63)
In adequate knowledge (≤9.9878049) 58(24.37)
Fidelity/ Adherence
High fidelity (≥80%) 66(27.73)
Low fidelity (<80%) 172(72.27)

147
The current research posits that most of the socio- demographic factors analysed
were not associated with knowledge on DHFF, except respecting the location of the
health facilities (Rural) (p=0.004). The results from the logistic regression model
found out that health service providers from PPHFs located in the rural settings were
7.7 times more likely to have DHFF knowledge as compared to their urban
counterparts [AOR 7.7 (2.093,28.356)]. Additionally, inclusive decision-making
process had association with knowledge, but it was not statistically significant
(Table 22).
Table 22: Logistic regression model for factors associated knowledge (p=0.005)
Variable Unadjusted logistic model Adjusted logistic model
OR (95%CI) p-value AOR (95%CI) p-value
Health facility type 0.7274
Dispensary Reference
Health center 1.112[0.613, 2.018]
Facility location 0.0005
Urban Reference Reference 0.0021
Rural 3.137[1.644, 5.987] 7.704[2.093,
28.356]
Sex 0.4957
Female Reference
Male 0.793[0.407, 1.546]
Age (years) 0.1343
≤ 35 Reference

148
Variable Unadjusted logistic model Adjusted logistic model
OR (95%CI) p-value AOR (95%CI) p-value
> 35 0.634[0.349, 1.151]
Marital status 0.7361
Married Reference
Single 1.118[0.585, 2.134]
Level of education 0.2465
Certificate Reference
Diploma 0.788[0.392, 1.584]
Degree and above 0.525[0.247, 1.118]
Inclusive decision-
making process
0.0231 0.0080
No Reference Reference
Yes 3.000[1.162, 7.743] 3.899[1.426,
10.663]
Years of experience
of working at PPHF
0.3403
≤ 10 Reference
>10 0.747[0.411, 1.360]

149
4.4.3 Fidelity of Implementation of DHFF by Health Service Providers
Of 238 health service providers, only 66 (27.73%) reported to have high level of
fidelity on DHFF implementation in their health care facilities (Table 21). The
results of chi-squire for determination of factors associated with FoI revealed that,
cadre of health service providers (p<0.001), position held by the health service
providers (p=0.002) and level of knowledge among health service providers on the
implementation of DHFF (p<0.001) influenced high level of DHFF FoI in PPHFs
(Table 22).
For cadre of health service providers, it was noted that, all assistant account had
higher level of FoI as compared to other cadres such that nurses (28.33%) and
clinicians (21.10%). On the same aspect, all health service providers who were
assigned in managerial task (other staffs) had higher chances of FoI (43.10%)
compared to frontline service providers (22.78%). Moreover, health services
providers with adequate knowledge on DHFF were more likely to possess high level
of FoI compared to those with inadequate knowledge on DHFF (Table 23).
Table 23: Chi-squire test for factors associated with FoI
Variable Level of DHFF Fidelity of
Implementation
Chi-
square
P-value
Low FoI
N (%)
High FoI
N (%)
Health facility type 1.5724 0.2099
Dispensary 78(76.47) 24(23.53)
Health center 94(69.12) 42(30.88)
Facility Location 0.5738 0.4488
Urban 87(70.16) 37(29.84)
Rural 85(74.56) 29(25.44)
Sex 0.0171 0.8959
Female 51(72.86) 19(27.14)
Male 121(72.02) 47(27.98)
Age(years) 0.8116 0.3676
≤ 35years 92(74.80) 31(25.20)

150
> 35 80(69.57) 35(30.43)
Marital status 0.0225 0.8809
Married 119(72.56) 45(27.44)
Single 53(71.62) 21(28.38)
Level of education 0.6356 0.7277
Certificate 93(74.40) 32(25.60)
Diploma 48(70.59) 20(29.41)
Degree and above 31(68.89) 14(31.11)
Cadre 25.8671 <.0001*
Nurses 86(71.67) 34(28.33)
Clinicians 86(78.90) 23(21.10)
Assistant accountant 0(0.00) 9(100.00)
Position in the health
facility
9.0426 0.0026*
Health service provider 139(77.22) 41(22.78)
Other staff 33(56.90) 25(43.10)
Years of experience 0.0004 0.9841
≤ 10 104(72.22) 40(27.78)
>35 68(72.34) 26(27.66)
Knowledge 16.6105 <.0001
Inadequate 54(93.10) 4(6.90)
Adequate 118(65.56) 62(34.44)
Acceptability 0.0014 0.9698
Acceptable 63(72.41) 24(27.59)
Unacceptable 109(72.19) 42(27.81)
The results from the logistic regression model portrays that knowledge on DHFF
implementation among health care workers had higher influence on fidelity of DHFF
implementation.
Health care workers with adequate knowledge were eight times more likely to
implement DHFF with higher FoI compared to HCWs with inadequate knowledge
(AOR = 8.14, CI = 2.755-24.099, p=0.0001) (Table 24). Likewise, health care
workers with managerial positions were three times more likely to implement DHFF
with higher FoI as compared to frontline health service providers (AOR = 3.049, CI
=1.557-5.972, p=0.0012) (Table 24).

151
Table 24: Logistic regression results for factors associated with FoI in PPHF
before and after implementation of DHFF (n=234).
Variable Unadjusted logistic model Adjusted logistic model
OR (95%CI) p-
value
AOR (95%CI) p-
value
Position of HCWs
in the health
facility
0.0031 0.0012
Health service
provider
Reference Reference
Other staff 2.568[1.374- 4.801] 3.049[1.557-5.972]
Knowledge 0.0003 0.0001
Inadequate
knowledge
Reference Reference
Adequate
knowledge
7.093[2.455- 20.496] 8.148[2.755-
24.099]
4.5 The association between Fidelity of Implementation (FoI) and overall
Structural quality of maternal health service in PPHF.
Looking into the association between changes of structural quality by FoI it was
found out that, there were positive structural changes among facilities with high FoI
as compared to those with low FoI.
Upon running in the logistic regression model to look for changes on structural
quality by FoI it was found out that, facility with high FoI were almost twice high in
structural quality of MHS compared with low FoI facilities (AOR=1.821, CI = 0.994
- 3.334, p= 0.00523) (Table 25).

152
Table 25: Association between Changes of Structural Quality by Fidelity of
Implementation
Variable Overall Structural Quality of MHS Chi-
square
P-value
Low Structural
Quality (%)
High Structural
Quality (%)
FoI 3.8199 0.0506
Low fidelity 76(44.19) 96(55.81)
High fidelity 20(30.30) 46(69.70)
Table 26: Logistic regression results for association between FOI and overall
structural quality of HS and in PPHFs before and after implementation of
DHFF (n= 42).
Variable Unadjusted Overal Change of Structural
Quality
OR (95% CI) P-value
Fidelity of Implementation 0.00523
Low fidelity Reference
High fidelity 1.821[0.994,3.334]

153
4.6 The association between Fidelity of Implementation (FoI) and overall
Maternal health service utilization in PPHF before and after implementation
of Direct Health Facility Financing.
Looking into the association between changes of maternal health service utilization
by FoI it was found out that, there was high maternal health service utilization among
facilities with low FoI as compared to those with high FoI (Table 27).
Table 27: Association between overall changes of health service utilization and
Fidelity of Implementation of Direct Health facility financing in PPHFs.
Variable Utilization Chi-square P-value
Low maternal
health service
utilization (%)
High maternal
health service
utilization (%)
FoI 16.3856 <. 0001
Low fidelity 16(9.30) 156(90.70)
High fidelity 20(30.30) 46(69.70)
The results of logistic regression analysis on the association between FoI and
utilization of maternal health service portrayed that, where there was existence of
high FoI of DHFF among health service providers, there was less utilization of MHS
(OR = 0.236, CI = 0.113 - 0.492, p<0.001) compared to high FoI health facilities
(Table 28).

154
Table 28: Logistic regression results for the association between FoI and overall
maternal health service utilization in PPHFs before and after implementation of
DHFF.
Variable Unadjusted OR for overall change of
maternal health service utilization
OR (95% CI) P-value
Fidelity of Implementation 0.0001
Low fidelity Reference
High fidelity 0.236[0.113,0.492]
4.6.1 Health Care Providers’ experience towards Direct Health Facility
Financing
Participants’ responsiveness towards DHFF was explored through 14 in-depth
interviews with key informants including DMOs, District DHFF coordinator, Health
Facility in charges and Chair of HFGCs. A total of three themes and eight sub –
thematic areas were obtained after thematic analysis.
A total of fourteen people from three district councils participated in 14 in-depth
interviews with the following socio-demographic characteristics (Table 29).

155
Table 29: Socio-demographic Characteristics of Interviewees
DMOs DDHFF Co In-Charges HFGC
Total
Interviewed
3 3 4 4
Age ≤ 35 2 1 2 2
>35 1 2 2 2
Gender
Male
2
1
1
2
Female 1 2 3 2
4.6.2 Thematic Findings for Qualitative Research
Table 30: Results from Indepth interviews by thematic and sub thematic areas
Theme Sub – themes
Health Care Providers’
experience toward DHFF
implementation
Training
Knowledge
Coordination
Health Care Providers’
Responsiveness towards
DHFF implementation
Attitude
Panctuality
- Issues
- Availability
- Utilization/Provision
Enabling Environment - Capacity building for DHFF implementers
- Adherence to the Public Financial management
protocols
- Motivation of DHFF implementers

156
Thematic Area Number 1: Health Care Providers’ experience towards DHFF
4.6.2.1 Training on DHFF, FFARS, Planning and Budgeting
Exploring whether participants had training on DHFF and FFARS it was revealed
that, majority attended the training, the challenge; however, they also had to
subsequently train others at their health facilities.
“Capacity building through training was another thing which
was implemented before the start of the program and therefore
one of the staff had to attend a special training on how this
program operates and shared the feedback with rest of the
workers at the facility”. (IDIs – DDHFF Co).
It was also revealed that, the approach that was used for the training was cascading,
as it was echoed by one of the participants who said:
“Training has only been provided to the health facility
in-charge and not to all healthcare providers and this
brings difficulties when discussing various issues related
to DHFF as most of the staffs seem to be not aware on most
of the issues”. (IDIs – Health Facility in Charge).
Other participants acknowledeged a training they have had on Planning and
Budgeting, as it was testified by a participant who said:
“Having knowledge and skills on planning and budgeting offers
a great opportunity to have a realistic budget that reflects
the community needs”. (IDIs – Health Facility in Charge).

157
4.6.2.2 Knowledge (Content) on DHFF initative
Assessment of knowledge of health service providers in relation to the DHFF
inititative, it was found out that, majority of health facility incharges were
knowledgable.
“This is a program which involves sending fund directly
to the health facilities as opposed to the old way which
involved sending money to the health facilities via district
medical officer”. (IDI in Charge-Health Facility).
Another testimonial was given by another participant who said:
“This program requires involvement of HFGC before you
commit any transaction and also whatever decision is made must
be participator”.
He added by saying:
“This is one of the financial decentralization approaches that
are geared towards improving the quality of health services
at the primary health care level”. (IDI – Health Facility in charge).
4.6.2.3 Coordination of DHFF activities
Exploring the coordination of DHFF activities it was found that the majority of
health service providers were aware of the of the coordination issues around DHFF
implementation. This was testified by one of the participants who said: -
“Once the fund is sent to the facilities, they have to acknowledge
the receipt of the fund by revealing the exact amount sent to

158
them. The next step is that I will ask them to submit their plan
before they start spending the money. Therefore, I can monitor
the fund through their plan; no money can be authorized
without submitting the action plan. The action plan also helps
to trace if what is planned to be spent on is what is in the budget?”
Then he paused, and started giving an example by saying:
“For instance, if you receive five million, you have to submit an
action plan for verification showing how you are going to spend
the money and if it happens to be not in the annual budget, we don’t
approve it. So for an activity to be approved, it has to be passed
through all he recommended steps and once it is implemented,one
has to submit a receipt and a report. So I do monitor the program
through all these mentioned steps”. (IDI – DDHFF Co).
Whereas the other participant testified by saying that:
“Before submitting their budgets, we usually go and meet the
health facilities guardians to discuss the identified challenges
and advise them the best process of planning and budgeting”.
He then added by saying;“This goes hand in hand with conducting supportive
supervision and mentorship so that to ensure if they have adhered to he guidelines
and protocols”. (IDI – DMO).

159
Thematic Area Number 2: Health Care Providers’ Responsivenes towards
DHFF implementation
4.6.2.4 Attitude of Health care providers towards DHFF
Looking at the attitude of the health service providers towards DHFF
implementation. They admitted to having had a good experience with the outcomes
of DHFF.
“This is one of the best programs I have ever seen, almost everyone
loves it at the Health Facility”. (IDI HFGC Chairperson).
Another participant appreciated the feeling of belongingness and ownership:
“This program makes us feel we are part of the system as we
can make decisions on our own and things happens right away
and things gives us impetus to thrive more”. (IDI Health Facility in
Charge).
4.6.2.5 Timeliness in addressing issues due to DHFF presence
Respondents admitted that there has been timely response to the issues they raise
with regards to the DHFF due to its web in nature.
“To me DHFF is the best because it has made the process
of planning easy as compared to the previous system. The web
based has helped us to work with the specific health facility
as compared to the old stand-alone plan Rep that forced us
to manually prepare the action plan for each individual facility”.
(IDI– DMO).

160
Then added by saying that:
“The old stand-alone plan Rep involved a lot of paper works and
books preparation as compared to the current system where one
can anytime access the system online, wherever someone is, and
for each specific facility. To me this program is the best even in
the preparation of quarterly reports, I can trace the performance
of any facility online by looking at their reports and their status.
So this is the best program”. (IDI– DMO).
4.6.2.6 Timely availability of health service provider’s benefits, tools and other
resources
Majority of health care workers acknowledged that, the introduction of DHFF initive
has brough some relief in terms of getting their benefits, working tools and other
resources as echoed by some of them who said:
“Nowdays we are getting our uniform allowances timely and also
we have all ledgers that are helping us to keep inventory of all
what is needed in our facilities”. (IDI - Health Facility in Charge).
Other participants testified that there is constant supply of medicines since
introduction of DHFF by saying that:
‘Since the introduction of DHFF initiative we have been having
constant supply of essential medicines and people are no longer
complaining about medicine shortage”. (IDI – HFGC Chairperson).
4.6.2.7 Timely fund utilization and service provision
Majority of respondents echoed on the importance of having DHFF initiative being
implemented as it helps to improve services provision close to their locality.
“What I can say is that this program has brought healthcare

161
services close to the health facilities as compared to the previous
years. In the previous years, planning was done by the heath facility
workers but the fund was retained by the DMO’s office, so after
planning each facility had to apply for the fund from the DMO’s
office”. (IDI-1; In charge of Health Facility).
The other participant also echoed this in the following statement:
“During previous arrangement very few people were deciding how
much to give us and when to give us that caused a lot of delays and
also hampered service provision of our health facility”. (IDI – HFGC
Chairperson).
4.6.2.8 Capacity of health service providers on management of DHFF initiative
Exploring the capacity on management of DHFF initiative it was found out that, the
lower level health facilities had adequate capacity for the management of DHFF.
“Yes, there were some challenges as we were worried if the lower
level could manage to implement the program and if they could
manage to timely utilize the whole fund but we thank God that it
was well perceived and its implementation is well execute”.
(IDIs–DDHFF Coordinator).
Other participant spoke on the importance of having knowledge and skills for
leading:
“Leadership skills are important for successful DHFF

162
implementation, we at the district level we cannot teach them
everything”.(IDIs – DMO).
4.6.2.9 Timeleness in disbursement of funds
The majority of participants indicated that the DHFF initiative has solved the issue of
fund disbursement delays as compared to the previous arrangement, which was
reflected in the following comment:
“Nowdays we receive funds timely as compared to previous time,
however, the challenge is you may find out that sometimes funds
have gone to our facilities without our knowledge”. (IDI –DMO).
Another participant echoed the same:
“We really love this arrangement; it is up to us to make most of this
System”. (IDI – HFGC Chairperson).
4.6.2.10 Improvement in working environment
Many participantsshared that:
“In the meantime, we can conduct minor renovations and also take
tea or coffee during working hours centrally to previous
arrangement were we have to ask everything from the DMO’s
office”. (IDI – In Charge).
Another participant also echod this experience by saying:
“Nowdays our facility undergoes minor renovations now and then
and makes facilities attractive to patients and make the health care
workers happy”. (IDI –HFGC Chairperson).
4.7 Thematic Number 1: Governance
A total of 49 people participated in seven FGDs which composed of seven people
whose socio-Demographic characteristics are as follows: - Council Health Service
Board, Health Facility Governing Committee, two matrons (one from Dispensary
and one from Health centre), two Health facility in charges (one from Health Centre
and One from Dispensary) and Assistant accountants (Table 30).

163
The themes and sub themes obtained from FGDs were the ones from the theoretical
frameworks and also the others emerged as per discussion. The transcripts for the
indepth interview and FGDs are found in Appendix 9.
Table 31: Characteristics of Interviewees
CHSB HFGC In Charges Matrons Assistant
Accountants
Total
Interviewed
7 7 14 14 7
Age ≤ 35 1 2 4 4 6
> 35 6 4 10 10 1
Gender
Male
6
2
12
1
3
Female 1 4 2 13 4
4.7.1 Governance of DHFF
Participants in the FGDs pointed out to their roles in the DHFF initiative and pointed
out that their roles are mainly to supervise and also to endose various decisions at the
primary health care facilities, as pointed out by one of participants of the FGDs.
“Our role is to authorize the allocated fund towards the main
objectives of the health facility. Dispensary has some priorities that
are shared to us for the review”. (FGD 1).
Moreover, they highlighted the challenges they face in implementing the DHFF
initiative processes that include the following: -
“A challenge is that, FFARS system involves a series of processes
and hence time consuming”.(FGD 2).

164
4.7.2 Funds Management
Participants expressed the importance of having funds management knowledge and
skills so that to enable smooth implementation of DHFF initiative. One of the
participants echoed by saying that:
“We were taught on financial management, however there is a
need to be also tought on bookkeeping”. (FGD 4).
The other participants expressed importance of participatory monitoring,
and endorsement of all transactions by all key player. One of the
participants said:
“All members should always participate in decision making
regarding endorsement of funds, its use and also expenditure
report”. (FGD 7).
4.7.3 Capacity of Health Facility Governing Committee (HFGC) Members
Majority of participants echoed on the importance of capacitating the HFGC
members on their roles and reponsibilities in relation to the implementation of DHFF
initiative. One of the partipants in the discussion said:
“We have been just inspecting medicines and supplies that are
brought at the facility and we do not have much skills on the
financial management, and budgeting”. (FGD 6).
Other participant expressed the importance of using mobile technology in helping the
HFGC to discharge their duties accordingly.
“Nowdays it is important to be flexible so that to build the
capacity of the HFGC so that they can discharge their duties
accordingly, itis not feasible to call for a meeting of HFGC
members throughout the country”. (FGD 5).
4.7.4 Planning and Budgeting
In this aspect the participants explained their involvement in the process and also
spelled out their roles and responsibilities. For example, one of the FGD participants
said:

165
“They have to prepare their own budget then share it with us for
verification so see if they have followed the rules and guidelines”. (FGD 3).
Other participants acknowledged the importance of having a well-prepared budget
and plan for successful implementation of DHFF initiative, one of the participants
said:
“For successful implementation of DHFF initiative we as
implementers we must be conversant with planning and
budgeting skills so that we can have realist budgets for
improvement of community health”. (FGD 4).
4.8 Thematic Area Number 2: Accountability
In this theme the particpants responded to the issues around transparency and
community involvement, supportive supervision and mentorship.
4.8.1 Transparency and Community Involvement
For this thematic area, participants were able to explain how they were engaged in
various discusions around transparency and also their participation in the decision-
making processes.
“All issues discussed and agreed through various committee
meetingsre posted on the notes board for community
consumption”. (FGD 4).
The other participant echoed similar sentiments with slight difference. She said: -
“There are other issues we must get a go ahead from the general
village assembly where we have representatives from different
hamlets”. (FGD 6).

166
4.8.2 Financial and performance report review and approval
The financial management and performance report also surfaced in the FGDs
regarding DHFF implementation.
One of the participants said:“With introduction of FFARS it has simplified how to
manage finances and how to report our perfomances”. (FGD 7).
4.8.3 Oversight
The issue of the oversight was also discussed in FGD as in important component for
effective implementation of DHFF initiative.
In one of the FDG one participants echoed on the importance by saying that:
“The oversight to the public primary health facilities has
resulted into the change of so many things regarding DHFF
implementation”. (FGD 6).
4.9 Thematic Number 3: Supportive Supervision and Mentorship
With regard to supportive supervision and mentorship of DHFF initiative related
activity, it was found out that the quality of supportive supervision was in question,
as facilities didn't receive regular supportive supervision and mentorship as testified
in the group discussion. One participant echoed on the importance of supportive
supervision and mentorship by saying: -
“Our main role is to do supervision and to regularly visit the
system (FFARS) to see if there are issues not moving smoothly
as the system provides a clear picture on what is being
implemented and what is not being implemented. E.g. if the
received fund is just sitting in the account without being
utilized, that signifies that things are not being attended and

167
we have to find the responsible person for more clarification
and insist him/her to move things forward”. (FGD 5).
Other participant testsfies that they do not regullary receive supportive supervision
and mentorship. While participatory approches decision-making was aconsidered as
one of the key prerequisites in having successful and impactiful supportive
supervision as echoed by one of the focus group discussions:
“After submitting their action plans, we do organize a two or
three days joint meeting (depending on the work load) to
review the action plans by agreeing together which should
be included and which should not. Sometimes one can include
a certain challenge in the action plan but after a joint
discussion and deep analysis you can find it as not a challenge”.
He continued by saying that:
“After getting the consensus, the next step is to enter the action
plan into the system after this it has to go through several steps
like assessment and securitization. After being approved, they
have to be given some copies of the budget and they have to
give feedback to the committee and their colleagues at the
health facility”. (FGD 6).
Other participants, stressed that through supportive supervision CHMT offers clarity
to the circulars and guidelines to the primary health facilities, as testified by one of
the participants:

168
“Our role is to ensure that guidelines, standard operating procedures
and circulars are availed to all facilities in the district council and
also to offer clarity whenever is needed”. (FGD 7).
4.9.1 Regular monitoring of primary health facilities, Consistency provision of
guidance (mentorship)
This was stressed by majority of participants as they felt it was a new initiative that
needed guidance. This was testified by one of the participants who said:
“Being supervised by people who knows very well DHFF
initiative helps us to implement the initiative”. (FGD 6).
4.9.2 Clarification/ interpretation of policies, strategies and operational
guidelines.
This was echoed by some participants, that operational guidelines are important for
DHFF implementation. This was testified by one of the participants who said: -
“To have a unified performance throughout the region we
need to have a standardized operational guideline”. (FGD 4).
4.9.3 Integration of Quantitative and Qualitative Results
The integrated results provide a holistic picture of the DHFF initiative
implementation processes and the effects of DHFF on the health system performance
of the PPHF. The intergration used Good Reporting of A Mixed Methods Study
(GRAMMS) to guide intergration process for qualitative and quantintative results
(Kaur et al., 2019; O’Cathain et al., 2008).
4.9.3.1 Framework for Integration
In order to achieve intergration, this study used a side-by-side comparison approach
(Creswell & Plano Clark, 2011), quantitative and qualitative results were compared

169
according to the main topics of the study in order to describe the similarities and
difference presented by the two strands.
4.9.3.2 Interpretation of the Integrated Results
Both quantitative and qualitative results indicated differences in the level of
knowledge of health care providers towards DHFF initiative. The majority
participants were aware of the DHFF initiative; however, about 76% had adequate
knowledge on DHFF. During FGDs very few participants articulated well what was
the DHFF initiative all about. There was also a general lack of understanding of
DHFF knowledge, specifically the disbursement modality from Ministry of Finance
and Planning to thePPHF.
The quantitative and qualitative findings indicated the variation of implementation of
fidelity towards DHFF among health care workers who were residing in rural areas
versus those who were residing in the urban areas.
The results on implementation fidelity from both strands of data indicate that there
were variations of implementation fidelity across the facilities in implementing the
DHFF initiative.

170
CHAPTER FIVE
DISCUSSION
5.0 Introduction
This chapter discusses results from the research on the DHFF’s effects onHSR,
governance and accountablity, health services utilization, and structural quality of
maternal health services. The other results that were discussed and measured were
FoI towards DHFF initiative in PPHF. Qualitative results on participant’s responses
towards DHFF implementation and how Governance and Accountability were
exercised in the PPHF were also discussed. The discussed results are compared to the
studies done inside and outside Tanzania.
The discussed findings from this study were obtained from four study sample units,
namely, patients exiting facilities after their medical consultations, PPHF, health
managers, health service providers and members of HFGCs from seven select
regions across all zones of the Tanzanian mainland.
Globally, governments have been trying to implement new health sector reforms and
policies that are geared towards improving the health system performance of
respective countries (Berman & Bitran, 2011b; OECD, 2017; Roberts et al., 2002).
Reforms in various components of the health sectors are necessary and need to be
sustainable to be responsive to the changing demands and evolution of health
systems.
5.1 Health System’s Responsiveness
Responsiveness of health services as perceived by patients has emerged as a strong
aspect of measuring the legitimate expectations of populations for the non-health
aspects of health care systems. In Tanzania, there has been little or no evidence from
studies conducted on HSR that measures the non-health aspects of the system;
however, there are many studies conducted to measure patient satisfaction
(Binyaruka et al., 2015; Juma & Manongi, 2009; Khamis & Njau, 2014; Mwansisya
& Mwansisya, 2015). However, the results from this study present mixed findings in
comparison to other studies (Bazzaz et al., 2015; Ebrahimipour et al., 2013; Gupt,

171
Kaur, Kamraj, & Murthy, 2016; Liabsuetrakul, Petmanee, Sanguanchua, &
Oumudee, 2012; Mohammadi & Koorosh, 2014; Yakob & Ncama, 2017).
In the current study, domains of access to care, respect to dignity and clear
communication were rated as the three most important domains of HSR given their
high-performance rate. The overall performance was positive since more than half
(55.9%) of the patients/clients were satisfied with HSR at PPHFs, illustrating a
beneficial DHFF initiative effect. These results are similar to the study conducted by
Mohammadi & Koorosh (2014) in Iran with inpatient clients at Zanjan University
Hospital who reported that responsiveness satisfaction level was 58.4% .
In a study conducted in Thailand (Liabsuetrakul et al. ,2012) that sought to discover
the reasons women chose to deliver in a hospital, the authors found that respect to
dignity, clear communication, and autonomy had higher scores than other domains.
Likewise, for this current study, both women and men showed high scores with
respect to these same three measures. This can also be substantiated by the Tanzania
Demographic Health Survey of 2015/16 that showed an upward increase in the
institutional deliveries across all primary health facilities in Tanzania (MoHCDGEC,
MoH [Zanzibar], 2016). This has been demonstrated by an increase in deliveries in
institutions that proxycally show that there is an increase in satisfaction with respect
to dignity and communication as this was one of the complaints in the previous
studies as pointed out by Bishanga et al. (2019) in the study about respective
maternity care (Bishanga et al., 2019).
In contrast, studies conducted in Iran and Ethiopia (Mohammadi & Koorosh, 2014;
Yakob & Ncama, 2017) found that that the domain of respect to dignity was low.
However, similar studies had higher percentage scores on the domain of clear
communication. The reasons for the differences could be due to the fact that a study
that was conducted in Iran (who?) was done amongst inpatients while the study in
Ethiopia by Yakob & Ncama (2017) was done solely with people living among HIV
and AIDS enrolled in the ART programme. This study design therefore denied the
opportunity to study other clients or patients who were not enrolled in care and
treatment programmes for people living with HIV and AIDS. However, the current

172
study incorporated opinions from clients in different health departments and units in
primary health care facilities, including people living with HIV and AIDS while
making sure that both genders were equally represented.
This study reports a significance increase in positive health system responsiveness
from 62.84% at the baseline to 71.20% at the endline, this shows that the DHFF
initiative have had some effects on HSR. There were confounding effects from
programs like RBF in the facilities where DHFF initiative has been implemented,
showing some effect on increasing positive HSR this could be due to the fact that the
RBF program uses a similar implementation approaches and indicators to the DHFF
initiative, hence having a multiplier effect on the outcomes of interest.
5.2 Structural Quality of MHS
The quality of health services can be measured through different approaches and the
toolkit for its measurement is replete with components of structure, process, and
outcome. These components were introduced by Donabedian and have been used and
tested by many other scholars (Donabedian, 1973; Gunawardena, Bishwajit, & Yaya,
2018; Yahya & Mohamed, 2018). However, this study looked into the structural
quality of PPHF especially on MHS delivery. Some of the structural quality were
grouped into seven domains of maternal health related services and staffing level. In
this study the majority of health facilities had high structural quality, a finding that
was similar to previous studies done in five African countries (Kruk et al., 2016;
Langer et al., 2014). In the current study high structural quality was associated with
an increase in maternal health service utilization, but this finding was contrary to that
of the Ethiopian demographic health survey. In that context, one study showed that
infrastructure improvement was not enough to attract mothers to deliver at the health
facilities (Central Statistical Agency [Ethiopia] & ICF International, 2012). Poor
quality of health services has been always associated with poor maternal health
outcomes, as shown in the study that was done in resources limited countries (Van
Den Broek & Graham, 2009). In this study 60% of health centers had less than 39
required health providers while 89% had less than 15 required health providers,
which could have an effect on the structural quality of services rendered to the

173
people. In this study, there was significance difference between baseline and endline
studies; however, health centers were five times more likely to offer structural
quality as compared to dispensaries. This could be due to fact that health centers are
more equipped and better staffed than the dispensaries. It could be due to some
diagnostic services that are offered at the health centers like X – ray and ultra Sound
services that cannot be offered at the dispensary level, thereby making the health
center a superior point of care than the dispensaries. In this study, structural quality
of MHS was found to be an important determinant of the health system
responsiveness as facilities with high structural quality has three times the odds to
have positive HSR as compared to those facilities with low structural quality. This
might reflect how high structural quality facilities tend to have adequate staffing
levels with adequate availability of essential commodities and good infrastructure,
thereby attracting people to access services.
5.3 Maternal Health Service Utilization
Health service utilization can be considered as a proxy indicator for the improvement
of quality of services in sub-Saharan Africa, especially in relation to access to MHS
(Alam et al., 2015; Kanyangarara et al., 2017). Generally, in this study, there was
significant increase in maternal service utilization between the before and after
studies. This finding is in line with other studies that have been conducted during the
Tanzania Service Provision Assessment (TSPA) and Service Availability and
Readiness Assessment (SARA) both of which revealed similar findings (MoHSW,
2015b; Tanzania Ministry of Health and Social Welfare, 2013). However, the only
difference that exists is a sharp increase in the maternal health service utilization just
eighteen months after DHFF introduction, which is reasonably interpreted that there
is an effect due to DHFF implementation on maternal health service utilization.
Additionally, it is important to note that, prior to the DHFF introduction, there have
been other government initiatives that might have contributed to the increase in the
maternal health service utilization especially among women who visit primary health
care facilities. This finding is similar to the study conducted in Tanzania by
Kanyangarara et al. (2017) that revealed the same findings (Kanyangarara et al.,
2017).

174
Dispensaries had positive significant mean differences in all nine indicators as
compared to the health centers with only three (i.e., ANC visits, ANC attendance
before 12th week of gestation, and number of positive pregnant women who receive
ARVs. This achievement may reflect that MHS can be easily accessed at the
dispensary level, hence women finding no reason whatsoever to go to the health
centers for the said services while they are available at the dispensary level. In this
study, use of family planning, intermittent presumptive treatment for malaria and
other 30 tracer medicines were found to have significant difference between baseline
and endline studies. The DHFF initiative has brought more resources to the primary
health facilities; hence, they have more autonomy to decide in a timely manner on
how to order essential health commodities even before the stockout as some studies
from World Bank Fiduciary System Assessment and Boex, et al. (2015) showed that
there has been misappropriation of funds and less autonomy when funds were
disbursed through the district head office (Boex et al., 2015b; The World Bank,
2015).
In this study, facilities with high structural quality had 41 times the likelihood to
have high maternal health service utilization than those with low structural quality.
This might reflect that many women or other clients are more attracted to use high
quality services as shown in previous studies done in sub–Saharan Africa
(Kanyangarara et al., 2017; Kruk et al., 2016).
5.4 FoI towards DHFF initiative
In this study, of all health service providers studied, about 76% had adequate
knowledge (adequate content) on DHFF initiative implementation although 88.2%)
of them were aware of the existence of DHFF initiative. This might relate to the
training which was conducted with the health service providers which employed a
cascade approach that might have compromised the quality of training and impacted
its implementation due to the dilution effect; hence, about 26% did not report
adequate knowledge. In some facilities there were no DHFF guidelines that would
have helped them to acquire more knowledge on the DHFF initiative. Surprisingly,
health service providers, who were working in the rural primary health facilities, had
over 7 times more knowledge compared to their counterparts in urban settings, which

175
may reflect that those working in the rural settings have adequate time to learn more
about DHFF initiative, as there are fewer programs to be implemented than required
in urban settings. Another reason could be those who are working in the urban
settings have higher workloads yielding inadequate time to focus on best
implementation of the DHFF initiative.
Of all health services providers in the current study, approximately 28% were found
to have high fidelity to DHFF implementation. This is a lower level of FoI than
would have been anticipated as they received training on DHFF prior to the
implementation and had started to implement the initiative six months after its
introduction. This could be due to assistant accountants being in the health centers
only and providing assistance to satellite dispensaries, leading to potential burnout
and low FoI towards DHFF initiative. Also it could be due to shortage of human
resources for health. However, many studies around the global take note of
difficulties experienced and the challenges faced by the achievement of high fidelity
by new innovations or programmes (Durlak & DuPre, 2008). Durlak & Dupre (2008)
suggested that getting the higher FoI (85%) has been achieved in some contexts due
to early monitoring of the programme coupled with constant feedback to the
responsible people and the programme’s need to be sustained (Durlak & DuPre,
2008; Hasson, 2010). In this study, it was observed that, the training was done by
using a cascade approach that might have resulted to some health service providers to
fail to comprehend what they have been taught from their coallegues due to lack on
facilitation skills and hence failed to implement according to the description as
shown in the theory of change frameworks (Kapologwe et al., 2019). The other
reason could be some of the health facilitity which were assessed did not had
guidelines and in some facilities they did not engage the HFGCs in the decision
making process and implementation of the initiative due to various reasons including
expirely of HFGC tenureship is three years and some of members been pre occupied
by other duties when they are needed. HFGC are instrumental in admninistrative and
financial decisions at the primary health facility level as DHFF initiative depends on
the interface meetings between health facility management and the community
representatives, therefore any weak or partial involvement may have a negative
176
effect on DHFF initiative. The existing relationship has been well elaborated by
authors from Tanzania (Kessy, 2014; Maluka, 2017; Maluka et al., 2018).
In this study, high FoI was strongly associated with the adequate knowledge of the
participants and position held by health care worker in the health facility. This was
similar to the studies conducted by Nurjono et al (2019) in which findings portrayed
a similar picture (Nurjono et al., 2019). Supprisingly, Health care workers experience
of more than ten years was not associated with high FoI, which was also the case for
the study which was done in Dodoma –Tanzania on the improved community health
fund (iCHF) implementation in which it was found out that the implementers
responded well on the call to shift to the new designed CHF hence high FoI (Kalolo
et al., 2015a). In this study, health care workers holding managerial position had
three times high FoI of DHFF initiative as compared other front-line health service
providers. This is due to the fact that, health service providers with managerial
positions were trained on the implementation of DHFF initiative and they are
responsible to account for financial resources being used at the health facilities.
Moreover, it could be due to fact that their roles at the managerial positions do not
involve management of patients hence they have adequate time to concentrate with
DHFF issues as compared to the frontline workers.
In this study, it was found out that, facilities with high structural quality of MHS
were strongly associated with high FoI. This might be due to the fact that health
service providers at the facilities with low structural quality compensated their
performances with the high FoI towards DHFF initiative due to low turn up of
patients or clients hence giving them an opportunity to implement DHFF as per
design.
In this study, facilities with high maternal health service utilization were associated
with low FoI. This might be due to fact that, facilities with high FoI towards DHFF
initiative were much concentrating towards realization of better performance on
DHFF initiative implementation than service delivery. This was expressed by some
health care workers that; DHFF initiative has brought some additional tasks hence
increase in the workload as they had also to carry out some financial management
tasks.

177
5.5 Health Care Providers’ responsiveness towards implementation of Direct
Health Facility Financing in PPHF.
During the in-depth interviews, participants clearly outlined that there were some
improvements attributable to the DHFF initiative, while concomitantly addressing
previous challenges including timely disbursement of funds and health services
utilization. This was also the case for the evaluation study that was conducted in
Kenya (Goodman et al., 2010; Waweru, Goodman, et al., 2016; Waweru, Molyneux,
et al., 2016).
Participants showed that they had adequate knowledge on the DHFF initiative and
had received the training needed to help them implement the DHFF initiative. This
was acknowledged despite the shortcomings of the cascade approach used to foster
training.
Exploring attitude of participants towards DHFF implementation, it showed that,
majority said they had a good feeling and experience and also showed positive
attitude towards DHFF initiative implementation. Meaning that, they were ready to
implement the initiative without any problem as they see its importance to their
health systems. This might be due to the fact that the introduction of the DHFF
initiative has been able to address number of challenges they have experienced
before like late disbursement of funds and also having low control over their finances
but also it could be the mandatory nature of the initiative that gave no other option of
implementers apart from implementing it. In this study, it was revealed that the
health facility’s capacity on management of DHFF initiative was good due to
existence of account assistants in some facilities and FFARS that eased the process
of management and reporting of fund use. This was different from the study done in
Kenya and Rwanda in which health facilities were found not to have adequate
capacity to manage funds and the program as whole (Kemri Welcome Trust, 2013;
Tsofa et al., 2017).

178
5.6 Governance and Accountability on DHFF implementation
5.6.1 Governance
In this study, governance was assessed through FGDs that were carried out to
explore governance through a number of pre-determined themes that looked on the
functionality of the existing governance structures like the HFGC. Upon discussion,
the sense of autonomy and ownership of financial affairs at the PPHF was one of
positive hope and potential, as reflected in the quotation “Our role is to authorise the
allocated funds towards achieving the main objective of the facility”.
This role was seen as being able to expedite various activities without any challenges
or interference from the district level. This finding was echoed in a Kenyan study on
facility governing committees (Waweru, Molyneux, et al., 2016). However, in this
study, health service providers complained of being overwhelmed by many tasks due
to the introduction of DHFF and FFARS to manage finances in the primary health
facilities, contributing additional tasks without additional staff. this might due to fact
that this is considered as an addition task to their routine duties especially in the
facilities that had no assistant accountants.
In this study, planning and budgeting emerged as a key governance function as all
members of team were fully engaged from the beginning which built a sense of
ownership in their respective health facilities from the planning to implementation.
This finding was similar to a study conducted in Kenya which after introduction of
direct facility financing saw uniting of members of the community and health
facilities to fully participate in the planning and budgeting for the welfare of their
facilities (Goodman et al., 2010; Waweru, Molyneux, et al., 2016). This finding was
also the case for the study which was done among European countries that looked
into the governance functions of the primary health care facilities in which. among
other things the issue of planning, budgeting,, and financing, found to be of
importance to flourish by using a health system thinking approach (Espinosa-
gonzález, Delaney, Marti, & Darzi, 2019). The governance structures tend to play a
pivotal role in implementation through appropriate planning and budgeting at the
primary health care level (Kessy, 2014; Mpambije, 2017).

179
5.6.2 Accountability
In the current study, three major sub-thematic areas of accountability were studied
namely transparency and community, financial and performance report review and
approval, supportive supervision and mentorship. All sub themes had a significant
degree of dimension across study area and participants.
The first dimension of transparency and community involvement assessed issues
related to reporting mechanisms, inclusive decision-making processes, endorsement
procedures, and availability of income and expenditure reports. These were aligned
for adherence of external accountability frameworks in PPHFs. The FGD with
members of HFGC revealed that there existed a potential increase in trust,
confidence, and functionality of HFGCs especially in making decision over financial
use and endorsement of funds. This result signifies that the ToC for DHFF
(Kapologwe et al., 2019) stressed the importance of HFGC in the process of making
DHFF effective. A similar study that was conducted in Kenya (Goodman, Opwora,
Kabare, & Molyneux, 2011) revealed functionality of HFGC increased upon the
introduction of direct facility financing due to increased financial autonomy in the
facilities. Moreover, on the aspects of reporting mechanism, the current study
revealed adherence to means in which the community were informed of the decision-
making processes through community meetings and other modes of communication.
Study by Maluka (Maluka & Bukagile (2016) reported on the functionality of
HFGCs stating that community meetings were used to provide feedback on the
performance of health facilities. Both the current and Maluka & Bukagile (2016)
studies identified challenges that affect performance of HFGCs, including inadequate
knowledge of their roles and responsibilities, inadequate training to improve their
skills, and knowledge especially with the introduction of new indicatives like DHFF,
lack of motivation, and low interaction or linkage among the HFGC members and
other instruments of accountability at the community level.
On the second thematic area of financial and performance report review and approval
an important need for the interface meetings between the members of HFGC and
health facility management teams was identified to build consensus on expenditures
180
and performance. This is similar to study done in Kenya which revealed the same
experience for successful implementation of any initiative (Goodman et al., 2011).
The third dimension of accountability in the current study was supportive supervision
and mentorship. The ToC proposed by (Kapologwe et al., 2019) and other
stakeholders to measure the performance of DHFF initiative in PPHFs acknowledged
the use of supportive supervision and mentorship as an important input to ensure
adherence to guidelines during implementation of DHFF initiative. Supportive
supervision was assessed in the current study among health managers at the council
level and at health facility level revealing irregularities in the implementation of this
important component. The in-depth interview conducted with district DHFF
coordinators revealed the existence of document and system review that was
undertaken at the council headquarters upon the submission of health facility
comprehensive plan and fund request. All of these strategies are essential for the
oversight function of CHMT; however, the quality aligned in the supportive
supervision and mentorship is compromised by this practice. According to DHFF
operational standard operating procedures (URT, 2016), members of CHMT under
the DHFF coordinator are responsible to ensure quality planning and effective
implementation of the plans.
The assessment conducted at the council level assured the plans and budgets
submitted by primary health facilities address all the priorities as per health facility
planning and budgeting guidelines (URT, 2016). Moreover, the current practice
addressed the proposed benefits of supportive supervision and mentorship by other
studies (Mboya et al., 2016; Olafsdottir et al., 2014) which affirms that the quality of
implementation of programs and their effectiveness are assured through supportive
supervisions and mentorship and at all levels.
In the current study, in-depth interviews with health managers at the health facility
level revealed the existence of weakness in supportive supervision and mentorship as
these activities are not done in a timely manner due to lack of capacity to conduct
support supervision in the area of DHFF and financial resources constraints in some
council. Also, in councils with proper supportive supervision and mentorship, there
181
were good financial management practices compared to others. These findings
resonate with those reported in studies conducted in Kenya, Tanzania, and Pakistan
(Bossert & Mitchell, 2011; Kamuzora et al., 2013b; Kessy, 2014). However, the
difference between the current study and the previous studies is that, this has been
done under improved financial decentralization environment where health facilities
have been given the mandate to plan and use their own resources.
5.6.3 Theoretical reviews
In this study, two related models that helped to understand health system
performance and reforms are reviewed. These theories were summarized in the six
steps namely: Problem identification, as per this study, the main identified problem
was delays in timely disbursement of funds and misappropriation of funds that led to
poor health service delivery at the primary health facilities and lowered the level of
autonomy amongst frontline workers and governance structures like HFGC of the
primary health care facilities. It was clearly seen upon introduction of DHFF
initiative it has clearly solved the problem of delays in the disbursement of funds that
was witnessed before the introduction of DHFF initiative in 2017/2018. The other
one is problem diagnosis. This study had all control knobs that were used are in the
areas of: financing, payment, organization, regulation and behaviours or persuasion
(Roberts et al., 2002), which thus qualified this effort as a major country’s health
financing reform. Looking into each of the items in the control knobs: -
The financing knob determines what resources were available to run the health care
system. As for this study were funds from health basket fund, national health
insurance funds and improved community health fund (iCHF).
The payment knob determines resources that were available to providers. As for this
study payment was made by the Ministry of Finance and Planning (MoFP) directly to
the primary health facilities via exchequer without going through District’s head
office.
The organization knob determines the kinds of provider organizations that exist and
their internal structures that shape how these organizations perform. In this study, the
182
organizational structures that are responsible for implementation of DHFF are
CHMT, CHSB, Health Facility Management Teams (HFMT) and HFGC.
The regulation knob imposes constraints on desired behaviors to allow the health
system to perform. In this study, the regulations for financial disbursement were
under the Ministry of Finance and Planning who are also mandated with
implementation of Budget Acts.
Finally, the efforts to change behavior knob influences how individuals respond to
health sector organizations, which, in turn, shapes the opportunities that
organizations confront (Roberts et al., 2002).
Another important step was policy development. Under this step we diagnosed health
problems through the control knobs using this information to inform policies and
guidelines used to guide its implementation. As for this study, there was a policy
meeting that took place in December 2016 in which among other things they decided
an introduction of DHFF as a strategy to improve quality of health care services at
the primary health facility level. Political will and commitment were evident during
the introduction of DHFF initiative in Tanzania through a series of meetings from
both technical (technical working group and annual joint technical review meeting)
and political levels (annual joint policy meeting and discussion with social services
parliamentary committee). Both series of meetings aimed at ensuring that there was
political decisions and commitments to the introduction of the DHFF (MOHCDGEC,
2016). Evaluation of the implemented reform. In this study, the baseline and endline
cross-sectional studies were conducted to evaluate the effect of the DHFF on selected
health system areas. Then a midline study was done to evaluate processes and also
the FoI of DHFF in order to get a better understanding on how the initiative evolved
over a period of time (Kapologwe et al., 2019).
5.6.4 Conceptual frameworks
In this study, ToC was used as one of the conceptual frameworks to evaluate the
implementation of DHFF initiative in Tanzania. There were some modifications
needed, which was hypothesised at the baseline study by adding other variables that
were found to be of great importance to the endline study (Kapologwe et al., 2019).

183
Some variables included leadership training on implementation of the DHFF
initiative to all relevant stakeholders as there were variation in performance of
initiative among different primary health facilities, which some participants pointed
out might have been due to leadership capability factor (e.g. the issue of inclusive
decision making by engaging the members of the community structures). The
importance of strong leadership in the implementation of new programs or initiative
has been also pointed out by authors from Tanzania (Kamuzora et al., 2013a; S.
Maluka et al., 2018; Mgata & Maluka, 2019).
In the FoI framework, there were couple of variables that emerged during a midline
study that were not included in the original proposed framework as moderating
factors by Kapologwe et al (2019), that found to be of great effect in the
implementation of the DHFF initiative (Kapologwe et al., 2019). Some of variables
were functioning financial management tools like cashbooks, ledgers and software
like FFARS this was also one of the things that was observed in the study that was
done in Kenya that availability of financial management tools was important in the
implementation of direct facility financing in Kenya (Goodman et al., 2010;
Waweru, Molyneux, et al., 2016). This modification of variables from the original
concept was also something that was experienced by other authors who conducted
some other studies in Tanzania to look into FoI of programs like improved
community health fund (Kalolo et al., 2015b).
Therefore, combination of the above study objectives and conceptual framework was
important for the better understanding of the study variables.
184
CHAPTER SIX
CONCLUSION, RECOMMENDATIONS AND SUGGESTION FOR
FURTHER RESEARCH
6.1 Conclusion
The findings from this study revealed a significant increase in HSR after the
introduction of the DHFF initiative in Tanzania, meaning that the initiative have had
an effect on the health system performance in the country. Moreover, there has been
a significance change in the structural quality of MHS and maternal health service
utilization since the introduction of the DHFF initiative. It is noteworthy that
programmes such as Results Based Financing (RBF) and ongoing construction of the
primary health facilities across the country have had some effect on the health system
performance although these two variables were controlled for their potential
confounding effects in this study.
Furthermore, findings from this study revealed that governance of DHFF initiative
needs a collaborative effort from both the supply side (i.e., health service providers)
and the demand side (i.e., community side through the HFGC). Therefore,
understanding the governance structures by those who are responsible with
implementation of the DHFF initiative is of great importance as it determines the
success and ultimate sustainability of the initiative.
The study findings also revealed that internal accountability among health managers
presented mixed opinions since some of the participants admitted that there is
existence of strong accountability while others felt a weak accountability mechanism
was in place. This variability in results calls for decision makers and health managers
at the ministerial level to critically assess the DHFF initiative in order to create a
sense of ownership at the implementation level, rather than concentrating on a few
staff members who possess managerial positions having the control. It is important to
invest on ensuring that DHFF guidelines are available and achievable, and that there
is adequate training on DHFF and FFARS as health service providers described these
are potentially enhancing accountability mechanisms.

185
The findings of this study revealed that FoI towards the DHFF initiative was very
low despite majority of health service providers found to have adequate knowledge.
This finding calls for revision of training methodology used and exploration of
motivators and facilitators necessary to deliver the DHFF initiative as per design.
6.2 Recommendations
Based on the current research findings, discussions and conclusion, this study
generates the following recommendations:
6.2.1 Recommendation to Policy makers
From this study it was clear that the DHFF initiative have had an effect on the
structural quality of MHS in the PPHF in Tanzania, despite confounding effects from
existing programs like RBF and ongoing renovation and construction of primary
health care facilities, both of which they were controlled during study and analysis
period. Structural quality assessment should be part of routine data to be obtained
from registers (MTUHA Books) that are present at the PPHF, which should be
incorporated into management information system like the District Health
Management Information System – 2 (DHIS-2). This should go hand in hand with
development of the
From this study we learned of different sources of funds at the primary health facility
level like National Health Insurance Fund (NHIF), Community Health Fund (CHF),
User Fees (UF), Basket Fund (BF), and Council Own Source (COS). However, all
these funds have different resource allocation and use formulae hence confusing the
health managers and health service providers on expenditure patterns. There is a
need for a harmonization of these resources.
Tanzania has embarked into streghthening its Community Health System (CHS) by
formalizing the Community Own Resource Persons (CORPs) cadre commonly
known as Community Health Workers (CHWs). However, one of the identified
challenges has been lack of unified modality that is used for payment of CORPs.
This study calls for all CORPS to be paid their incentives or allowances through
PPHF which serves as a conduit for DHFF approach hence enhancing accountability

186
to both parties. This is important in the sense that CORPS are represented in the
HFGC.
In this study we used Open Data Kit (ODK) software enabling us to access real time
data with instant analysis. The tablets with GPS sensors were used for data collection
at all 42 primary health care facilities. We highly recommend this data collection
system to allow managers at all levels to have access to date to inform timely data-
driven decisions resulting responsive interventions. Furthermore, ODK offers an
opportunity for cost reduction as it reduces the burdensome of the current system
with about 15 registers for data collection from patients or clients.
6.2.2 Recommendation to Policy Implementers
The DHFF initiative in an important approach in making sure that the health system
responds to the legitimate requirements of the people who visit primary health
facilities. It is therefore important that all seven domains that were used to assess
HSR should always be carried out in the specified period of time to ensure that
delivery of services to meet the expectations of the clients. Therefore, we highly
recommend HSR surveys through exit interviews should be carried out in all primary
health facilities on a monthly or quarterly basis to offer feedback to the managers at
the respective facilities and also at district and regional on areas where they can be
improved. The tool used can also be integrated into the already existing health
management system like DHIS-2 that can simplify its analysis at different levels.
It was clear that the DHFF had an effect on the maternal health service utilization
with an increase in the number of women accessing the MHS after introduction of
the DHFF initiative. However, this calls for a study that will look into the socio-
demographics and social determinants of health that will help to understand various
factors that are responsible for an increase in maternal health service utilization. We
highly recommend that local data use on maternal health service utilization should be
given a priority as it will help health managers to be informed on what should be
improved in order to increase maternal health service utilization.

187
In this study, accountability in the PPHFs was an integral part of successful
implementation of DHFF initiative. Therefore, it is the role of the government and
stakeholders to ensure that, there is capacity development of health managers at
PPHFs and council level in order to ensure effective and efficient use of public
funds. This should be compared to the service delivered at the PPHF which satisfy
the requirements of the members of the community.
This study also calls for enhancing the governance and accountability functions like
supportive supervision and mentorship from CHMT to the primary health facilities
so that to improve and also to address all challenges that are experienced in the
course of DHFF implementation by both health service providers and HFGC which
are comprised of the community representatives.
The accountability can be appreciated by following the financial memorandum and
budget acts to ensured timely disbursement of funds and utilization by the primary
health facilities. Therefore, this study calls for Ministry of Finance and Planning,
who is the main funder, MoHCDGEC, PO-RALG and other stakeholders to comply
with all regulations governing public fund allocation and disbursement for efficiency
and effectiveness of primary health care system performance.
This study also recommends that all the stakeholders from both Government and
Non-State Actors (NSA) should comply with the DHFF initiative. There were some
NSA who used a direct to project fund approach as their disbursement modality
therefore by passing the DHFF initiative and posing a challenge in the accountability
of funds that are disbursed outside of the DHFF arrangement.
In addition, this is an opportune time to digitize all primary health care, reaching
beyond the FFARS health centre level software, in order to remove the dispensary
level reliance on financial service support including assistant accountants from the
health centres.
From this study it was learned that Guidelines for implementation of DHFF initiative
was not yet developed by the responsible ministries instead PPHF are using Circulars
and FFARS guidelines to implement the initiative. This study calls for responsible

188
ministries to develop and disseminate guidelines for DHFF implementation so that to
improve FoI.
6.2.3 Recommendations to the DHFF Initiative
From this study, it was clear that for successful implementation of the DHFF
initiative there is need to have strong and resilient governance structures from
national level to the community level. Despite successes observed in the governance
there is a need to capacitate all players in the implementation of DHFF initiative with
some leadership skills to enable them to discharge their duties accordingly. We
therefore strongly recommend for leadership and management training to all people
who are responsible for DHFF implementation.
From this study it was clear that the DHFF initiative has been rolled out the country
despite an observed level of FoI which was low among the majority of health care
providers. This flag calls for revision of training program and materials that were
used during training coupled with changing the approach of training from cascade to
another approach that will not dilute the content of the training.
Moreover, this study recommends that all financial management tools should be
availed to all primary health facilities so that to enable them to conduct proper book
keeping in line with the Government’s financial regulations and memorandum.
All health facilities need to have assistant accountants as those facilities who have
full time assistant accountants out performed dispensaries which relied on satellite
services from health centers.
From this study it was learnt that, there were long procurement processes for
commodities and supplies to be used at the PPHF as they had to seek for
endorsement of procurement of even small needed items. This was partly due to lack
of Guidelines and Circulars with threshold that allows frontline teams to procure
essentials at their locality instead of travelling long distance to seek for procurement
approval. I therefore, recommend that there should be a set threshold for
procurement of essentials at the PPHF that gives allowance for petty or micro
189
procurement and for the commodities that exceeds threshold should be forwarded to
District Head Office for approval and endorsement by District Tender Board.
6.3 Strengths of the Study
o This study used standards and validated tools to measure health system
responsiveness and structural quality of MHS (World Bank, 2013; Valentine
et al., 2003; Van Der Kooy et al., 2014).
o It used 9 indicators for assessing the Maternal Health Service utilization that
are in the One Plan II and III which are guiding documents for maternal and
child health in Tanzania and these information can be obtained from the
DHIS-2 (MOHCDGEC, 2016).
o This is both implementation research study and an evaluation study
o This study is supported by two theoretical reviews: the health system
performance model and the health system reform model. DHFF
implementation and two conceptual frameworks were also used to inform it
i.e., theory of change (ToC) and FoI.
o A range of the various stakeholders who are involved in the DHFF
implementation participated in this study, such as health managers (DMOs
and DHFF Coordinators), health service providers, patients/clients, and
members of the community (CHSB chairpersons and HFGC members).
o This study employed a mixed method approach, using both quantitative and
qualitative approaches.
6.4 Limitations of the Study
o The main limitation to this study is that it used a before and after design that
is non-controlled, because DHFF initiative has been implemented as a part of
national wide initiative; hence, there is no control group. In this case a case -
control study design would have been appropriate; however, it cannot be
done now as DHFF has been started already. Such a method may have been
possible by comparing Tanzania with neighboring countries, but such a study
would have resulted in high cost implications. In order to address some of the
challenges that might have emerged as a result of data contamination during

190
study period, there were some strategies which were put in place. First, the
project established a surveillance system with special arrangements to track
any events, projects, programmes, or any support in the study areas. That
helped in understanding if there were any contributions from other
interventions. Secondly, there was triangulation of data in order to
authenticate the collected information.
o The other limitation is that, at both baseline and endline, the study used a
cross-sectional survey that just offers the snapshot of opinions at that
moment, and such a survey makes it difficult to establish a causal effect
pathway.
o The other limitation is that, is on the objective to assess the maternal health
service utilization in which we relied on utilization data that are not enough
as other social demographic factors such as education level and social quintile
level were not studied.
6.5 Suggestions for Further Research
Further studies should address the existing gaps raised due to study limitations and
areas where the current study failed to address. The following are potential areas for
the future studies to be undertaken:
DHFF implementation is a lasting program that has undertaken an approach within
structures of the government; therefore, the results from the current study can be
improved with a long period study like prospective cohort study that will help to
establish behaviour change and health system improvement overtime.
The current study was conducted in some regions where other programs like RBF
were implemented along with the ongoing construction or renovation of primary
health facilities across the country. Despite the fact that we successfully managed to
control for confounders, we recommend that other interventional studies should be
undertaken to compare between other programme implementing regions and non-
programme implementing regions to get a clear picture of the performance.

191
The current study was a before and after, therefore we recommend another inter-
country study to be conducted Tanzania and any neighbouring country that is yet to
implement DHFF initiative as it will take care all the noted limitations from before
and after studies.
The findings from this study showed a majority of health service providers had low
FoI towards the DHFF initiative. This finding calls for another study to look for level
of motivation among health service providers and their governing structures like
CHSB and also HFGC.
The other area is implementation research to offer practical evidence-based solutions.

192
REFERENCES
Abel-smith, B., & Rawal, P. (1992). Can the poor afford “free” health services? a
case study of Tanzania. Health Policy and Planning, 7(4), 329–341.
https://doi.org/10.1093/heapol/7.4.329
Adam, T., & Savigny, D. De. (2012). Systems thinking for strengthening health
systems in LMICs : need for a paradigm shift, 2006–2008.
https://doi.org/10.1093/heapol/czs084
Addicott, R. (2011). Social enterprise in health care, 1–28.
Afulani, P. A., Buback, L., McNally, B., Mbuyita, S., Mwanyika-Sando, M., & Peca,
E. (2020). A rapid review of available evidence to inform indicators for routine
monitoring and evaluation of respectful maternity care. Global Health Science
and Practice, 8(1), 125–135. https://doi.org/10.9745/GHSP-D-19-00323
Akowuah, J. A., Agyei-Baffour, P., & Awunyo-Vitor, D. (2018). Determinants of
antenatal healthcare utilisation by pregnant women in third trimester in peri-
urban Ghana. Journal of Tropical Medicine, 2018(2000).
https://doi.org/10.1155/2018/1673517
Alam, N., Hajizadeh, M., Dumont, A., & Fournier, P. (2015). Inequalities in
maternal health care utilization in sub-saharan African countries: A multiyear
and multi-country analysis. PLoS ONE, 10(4), 1–16.
https://doi.org/10.1371/journal.pone.0120922
Andrew, C. (1995). Health sector reform: key issues in less developed countries.
Journal of International Development, 7(3), 329–347.
https://doi.org/10.1002/jid.3380070303
Ary, D., Jacobs, L., Sorenson, C., Razavieh, A., Jacobs, C., C, S., & Razavier, A.
(2010). Introduction to Research in Education.
Asian Development Bank. (2016). Rural Primary Health Services Delivery Project
(RRP PNG 41509), 1–4.
193
Ayala, G. X., & Elder, J. P. (2011). Qualitative methods to ensure acceptability of
behavioral and social interventions to the target population. Journal of Public
Health Dentistry, 71(SUPPL. 1), 1–17. https://doi.org/10.1111/j.1752-
7325.2011.00241.x
Basinga, P., Gertler, P. J., Binagwaho, A., Soucat, A. L., Sturdy, J., & Vermeersch,
C. M. (2011). Effect on maternal and child health services in Rwanda of
payment to primary health-care providers for performance: An impact
evaluation. The Lancet, 377(9775), 1421–1428. https://doi.org/10.1016/S0140-
6736(11)60177-3
Bazzaz, M. M., Reza, M., Taghvaee, E., Salehi, M., Bakhtiari, M., & Shaye, Z. A.
(2015). Health System ’ s Responsiveness of Inpatients : Hospitals of Iran.
Global Journal of Health Science, 7(7), 106–113.
https://doi.org/10.5539/gjhs.v7n7p106
Bellg, A. J., Borrelli, B., Resnick, B., Hecht, J., Minicucci, D. S., Ory, M., …
Czajkowski, S. (2004). Enhancing Treatment Fidelity in Health Behavior
Change Studies : Best Practices and Recommendations From the NIH Behavior
Change Consortium. Health Psychology, 23(5), 443–451.
https://doi.org/10.1037/0278-6133.23.5.443
Berman, P., & Bitran, R. (2011). Health Systems Analysis for Better Health System
Strengthening. Washington, DC 20433.
Binyaruka, P., Patouillard, E., Powell-Jackson, T., Greco, G., Maestad, O., & Borghi,
J. (2015). Effect of paying for performance on utilisation, quality, and user costs
of health services in Tanzania: A controlled before and after study. PLoS ONE,
10(8), 1–16. https://doi.org/10.1371/journal.pone.0135013
Bishanga, D. R., Massenga, J., Mwanamsangu, A. H., Kim, Y. M., Eorge, J.,
Kapologwe, N. A., … Stekelenburg, J. (2019). Women’s experience of facility-
based childbirth care and receipt of an early postnatal check for herself and her
newborn in Northwestern Tanzania. International Journal of Environmental
Research and Public Health, 16(3). https://doi.org/10.3390/ijerph16030481

194
Boex, J. (2013). PEFA Performance Measurement Framework at Sub National
Government Level – definitions and typology.
Boex, J., Fuller, L., & Malik, A. (2015). Decentralized Local Health Services in
Tanzania Are Health Resources Reaching Primary Health Facilities , or Are
They Getting. Urban Institute, (April).
https://doi.org/10.13140/RG.2.1.4208.5288
Borghi, J., Ramsey, K., Kuwawenaruwa, A., Baraka, J., Patouillard, E., Bellows, B.,
… Manzi, F. (2015). Protocol for the evaluation of a free health insurance card
scheme for poor pregnant women in Mbeya region in Tanzania: A controlled-
before and after study. BMC Health Services Research, 15(1), 15–17.
https://doi.org/10.1186/s12913-015-0905-1
Borrelli, B. P. (2012). The Assessment, Monitoring, and Enhancement of Treatment
Fidelity In Public Health Clinical Trials, 71, 1–21.
https://doi.org/10.1111/j.1752-7325.2011.00233.x.The
Bossert, T. J., & Mitchell, A. D. (2011). Health sector decentralization and local
decision-making : Decision space , institutional capacities and accountability in
Pakistan. Social Science & Medicine, 72(1), 39–48.
https://doi.org/10.1016/j.socscimed.2010.10.019
Braveman, P., & Gottlieb, L. (2014). The social determinants of health: It’s time to
consider the causes of the causes. Public Health Reports, 129(SUPPL. 2), 19–
31. https://doi.org/10.1177/00333549141291s206
Brousselle, A., & Champagne, F. (2011). Program theory evaluation: Logic analysis.
Evaluation and Program Planning, 34(1), 69–78.
https://doi.org/10.1016/j.evalprogplan.2010.04.001
Brunelli, B. (2007). Structural Adjustment Programs and the Delivery of Health Care
in the Third World. Pell Scholars & Senior Theses, 16, 1–29.
Carroll, C., Patterson, M., Wood, S., Booth, A., Rick, J., & Balain, S. (2007). A
195
conceptual framework for implementation fidelity. Implementation Science, 9,
1–9. https://doi.org/10.1186/1748-5908-2-40
Central Statistical Agency [Ethiopia], & ICF International. (2012). Ethiopia
Demographic and Health Survey 2011, 1–452.
Century, J., Rudnick, M., & Freeman, C. (2010). A Framework for Measuring
Fidelity of Implementation : A Foundation for Shared Language and
Accumulation of Knowledge, 199–218.
https://doi.org/10.1177/1098214010366173
Chakraborty, N., Islam, M. A., Chowdhury, R. I., Bari, W., & Akhter, H. H. (2003).
Determinants of the use of maternal health services in rural Bangladesh. Health
Promotion International, 18(4), 327–337.
https://doi.org/10.1093/heapro/dag414
Chang, R., Zangle, K. C., & Hunter, J. (n.d.). Social enterprise opportunities in the
healthcare sector.
Chimhutu, V., Tjomsland, M., Songstad, N. G., Mrisho, M., & Moland, K. M.
(2015). Introducing payment for performance in the health sector of Tanzania-
the policy process. Globalization and Health, 1–10.
https://doi.org/10.1186/s12992-015-0125-9
Cohen, D. J., & Crabtree, B. F. (2008). Research in Health Care : Controversies and
Recommendations. Annals Of Family Medicine, 6(4), 331–339.
https://doi.org/10.1370/afm.818.INTRODUCTION
Compaoré, R., Yameogo, M. W. E., Millogo, T., Tougri, H., & Kouanda, S. (2017).
Evaluation of the implementation fidelity of the seasonal malaria
chemoprevention intervention in Kaya health district, Burkina Faso. PLoS ONE,
12(11), 1–18. https://doi.org/10.1371/journal.pone.0187460
Creswell, J. W. (2014). Research Design: Quantitative, Qualitative and Mixed
methods Approaches (4th Edition).
196
Darby, C., Valentine, N., Murray, C. J., & de Silva, A. (2001). World Health
Organization (WHO) : Strategy on Measuring Responsiveness.
Donabedian. (1973). Evaluating the Quality of Medical Care. New England Journal
of Medicine, 288(25), 1352–1353.
https://doi.org/10.1056/NEJM197306212882509
Donnell, C., (2015). Defining , Conceptualizing , and Measuring Fidelity of
Implementation and Its Relationship to Outcomes in K – 12 Curriculum
Intervention Research, (June). https://doi.org/10.3102/0034654307313793
Dunn, S., Sprague, A. E., Grimshaw, J. M., Graham, I. D., Taljaard, M., Fell, D., …
Walker, M. (2015). A mixed methods evaluation of the maternal-newborn
dashboard in Ontario: dashboard attributes, contextual factors, and facilitators
and barriers to use: a study protocol. Implementation Science, 11(1), 59.
https://doi.org/10.1186/s13012-016-0427-1
Durlak, J. A., & DuPre, E. P. (2008). Implementation matters: A review of research
on the influence of implementation on program outcomes and the factors
affecting implementation. American Journal of Community Psychology, 41(3–
4), 327–350. https://doi.org/10.1007/s10464-008-9165-0
Dusenbury, L, Brannigan, R., Falco, F., & Hansen, W. B. (2003). A review of
research on fidelity of implementation: implications for drug abuse prevention
in school settings. Health Education Research, 18(May), 237–256.
https://doi.org/org/10.1093/her/18.2.237
Dusenbury, Linda, Brannigan, R., Falco, M., & Hansen, W. B. (2003). A review of
research on fidelity of implementation : implications for drug abuse prevention
in school settings. Health Education Research, 18(2), 237–256.
Dutta, A. (2015). Prospects for Sustainable Health Financing in Tanzania: Baseline
Report. Health Policy Project , Futures Group: Washington , (February), 1–40.
Ebrahimipour, H., Najjar, A. V., Jahani, A. K., Pourtaleb, A., Javadi, M., Rezazadeh,

197
A., … Shirdel, A. (2013). Health System Responsiveness : A Case Study of
General Hospitals in Iran. International Journal of Health Policy and
Management, 1(1), 85–90. https://doi.org/10.15171/ijhpm.2013.13
Espinosa-gonzález, A. B., Delaney, B. C., Marti, J., & Darzi, A. (2019). The impact
of governance in primary health care delivery : a systems thinking approach
with a European panel, 8, 1–16.
Fawler, A. (1993). Non-governmental organizations as agents of democratization:
An African perspective.
Fjeldstad, O. H. (2001). Fiscal decentralisation in Tanzania: For better or for worse?
Working Paper - Chr. Michelsen Institute, (10), 1–15.
Frederick J Gravetter, L.-A. B. F. (2012). Research Methods for Behavioral Sciences
(5th Editio).
Frieden, T. R. (2014). Six components necessary for effective public health program
implementation. American Journal of Public Health, 104(1), 17–22.
https://doi.org/10.2105/AJPH.2013.301608
Frumence, G., Nyamhanga, T., Mwangu, M., & Hurtig, A. K. (2013). Challenges to
the implementation of health sector decentralization in Tanzania: Experiences
from kongwa district council. Global Health Action, 6(1), 1–11.
https://doi.org/10.3402/gha.v6i0.20983
Gale, N. K., Heath, G., Cameron, E., Rashid, S., & Redwood, S. (2013). Using the
framework method for the analysis of qualitative data in multi-disciplinary
health research. BMC Medical Research Methodology, 13(1), 1.
https://doi.org/10.1186/1471-2288-13-117
Gary, P. et al. (1990). The New England Journal of Medicine Downloaded from
nejm.org on April 1, 2015. For personal use only. No other uses without
permission. Copyright © 1990 Massachusetts Medical Society. All rights
reserved. The New English Journal of Medicine, 323(16), 1120–1123.

198
Gilson, L., Magomi, M., & Mkangaa, E. (1995). The structural quality of Tanzanian
primary health facilities. Bulletin of the World Health Organization, 73(1), 105–
114.
Gilson, L., & Mills, A. (n.d.). Health sector reforms in sub-Saharan Africa: lessons of
the last 10 years. Health Policy (Amsterdam, Netherlands), 32(1–3), 215–243.
Goodman, C., Opwora, A., Kabare, M., & Molyneux, S. (2011). Health facility
committees and facility management - exploring the nature and depth of their
roles in Coast Province , Kenya. BMC Health Services Research, 11(1), 229.
https://doi.org/10.1186/1472-6963-11-229
Goodman, C., Waweru, E., Kedenge, S., Tsofa, B., & Molyneux, S. (2010). Funding
Kenyan health centres : experiences of implementing direct facility financing
and local budget management, 3.
Grittner, A. M. (2013). Results-based Financing Evidence from performance-based
financing in the health sector.
Guba, E. (1981). Criteria for assessing the trustworthiness of naturalistic inquiries.
Educational Communication & Technology, 29(2), 75–91.
https://doi.org/10.1007/BF02766777
Gunawardena, N., Bishwajit, G., & Yaya, S. (2018). Facility-Based Maternal Death
in Western Africa: A Systematic Review . Frontiers in Public Health .
Gupt, A., Kaur, P., Kamraj, P., & Murthy, B. N. (2016). Out of pocket expenditure
for hospitalization among below poverty line households in district Solan,
Himachal Pradesh, India, 2013. PLoS ONE, 11(2), 1–11.
https://doi.org/10.1371/journal.pone.0149824
Harachi, T. (1999). Opening the Black Box : Using Process Evaluation Measures to
Assess Implementation and Theory Building Opening the Black Box : Using
Process Evaluation, (1999). https://doi.org/10.1023/A
Harachi, T. W., Abbott, R. D., Catalano, R. F., Haggerty, K. P., & Fleming, C. B.
199
(1999). Opening the Black Box: Using Process Evaluation Measures to Assess
Implementation and Theory Building. American Journal of Community
Psychology, 27(5), 711–731. https://doi.org/10.1023/A:1022194005511
Hasson, H. (2010). Systematic evaluation of implementation fidelity of complex
interventions in health and social care, 1–9.
Hsiao, W. (2000). Inside the Black Box of Health Systems. Bulleting of the World
Health Organization.
Hulleman, C. S., & Cordray, D. S. (2009). Moving From the Lab to the Field : The
Role of Fidelity and Achieved Relative Intervention Strength. Journal of
Research on Educational Effectiveness, 2(November 2014), 37–41.
https://doi.org/10.1080/19345740802539325
Innocent Semali, D. D. S. & M. T. (2005). Health Sector Reform And
Decentralization In Tanzania : The Case Of The Expanded Programme On
Immunization At District Level. Journal of Health & Population in Developing
Countries.
International Budget Partnership. (2018). Open Budget Survey 2017 Partners.
Washington, DC 20002.
International Health System Group- Havard School of Public Health. (2000). A
Decade of Health Sector Reform: What Have We Learned? DDM Project, 2.
James Macinko, Barbara Starfield, T. E. (2009). The Impact of Primary Healthcare
on Population Health in Low- and, 32(2), 150–171.
Juma, D., & Manongi, R. (2009). Users’ perceptions of outpatient quality of care in
Kilosa District Hospital in central Tanzania. Tanzan J Health Res, 11(4), 196–
204.
Kalolo, A., Radermacher, R., Stoermer, M., Meshack, M., & De Allegri, M. (2015).
Factors affecting adoption, implementation fidelity, and sustainability of the
Redesigned Community Health Fund in Tanzania: A mixed methods protocol

200
for process evaluation in the Dodoma region. Global Health Action, 8(January
2018). https://doi.org/10.3402/gha.v8.29648
Kamuzora, P., & Gilson, L. (2007). Factors influencing implementation of the
Community Health Fund in Tanzania. Health Policy and Planning, 22(2), 95–
102. https://doi.org/10.1093/heapol/czm001
Kamuzora, P., Maluka, S., Ndawi, B., Byskov, J., & Hurtig, A. K. (2013). Promoting
community participation in priority setting in district health systems:
experiences from Mbarali district, Tanzania. Global Health Action, 6, 22669.
https://doi.org/10.3402/gha.v6i0.22669
Kanyangarara, M., Munos, M. K., & Walker, N. (2017). Quality of antenatal care
service provision in health facilities across sub-Saharan Africa: Evidence from
nationally representative health facility assessments. Journal of Global Health,
7(2). https://doi.org/10.7189/jogh.07.021101
Kapologwe, N.A,et al., (2020). Development and upgrading of public primary
healthcare facilities with essential surgical services infrastructure : a strategy
towards achieving Universal Health Coverage in Tanzania. BMC Health
Services Research.
Kapologwe N.A, J. S., & Msuya, S. E. (2011). Perceived barriers and attitudes of
health care providers towards Provider-Initiated HIV Testing and Counseling in
Mbeya region, southern highland zone of Tanzania. The Pan African Medical
Journal, 8, 17. https://doi.org/10.4314/pamj.v8i1.71070
Kapologwe,N.A (2011). Provider-initiated HIV testing and counseling in Mbeya
City, south-western Tanzania: knowledge and practice of health care providers.
Tanzania Journal of Health Research, Vol 13, No(ISSN: 0856-6496;), 4.
Kapologwe,N.A, Kagaruki, G. B., Kalolo, A., Ally, M., Shao, A., Meshack, M., …
Hoffman, A. (2017). Barriers and facilitators to enrollment and re-enrollment
into the community health funds/Tiba Kwa Kadi (CHF/TIKA) in Tanzania: a
cross-sectional inquiry on the effects of socio-demographic factors and social
201
marketing strategies. BMC Health Services Research, 17(1), 308.
https://doi.org/10.1186/s12913-017-2250-z
Kapologwe, N. A., Kalolo, A., Kibusi, S. M., Chaula, Z., Nswila, A., Teuscher, T.,
… Borghi, J. (2019). Understanding the implementation of Direct Health
Facility Financing and its effect on health system performance in Tanzania: a
non-controlled before and after mixed method study protocol. BMC Health
Services Research, 1–13. https://doi.org/https://doi.org/10.1186/s12961-018-
0400-3
Kapologwe, N. A., Kibusi, S. M., Borghi, J., Gwajima, D. O., & Kalolo, A. (2020).
Assessing health system responsiveness in primary health care facilities in
Tanzania. BMC Health Services Research, 20(1), 104.
https://doi.org/10.1186/s12913-020-4961-9
Kaur, N., Vedel, I., El Sherif, R., & Pluye, P. (2019). Practical mixed methods
strategies used to integrate qualitative and quantitative methods in community-
based primary health care research. Family Practice, 36(5), 666–671.
https://doi.org/10.1093/fampra/cmz010
Keith, R. E., Hopp, F. P., Subramanian, U., Wiitala, W., & Lowery, J. C. (2010).
Fidelity of implementation : development and testing of a measure.
Implementation Science, 5(99), 1–11.
Kemri Welcome Trust. (2013). Direct funding of health facilities Findings from an
evaluation of the Health Sector Services Fund in Kenya.
Kessy, F. L. (2014). Improving Health Services through Community Participation in
Health Governance Structures in Tanzania. Journal of Rural and Community
Development.
Khaleghian, P. (2004). Decentralization and public services: The case of
immunization. Social Science and Medicine, 59(1), 163–183.
https://doi.org/10.1016/j.socscimed.2003.10.013

202
Khamis, K., & Njau, B. (2014). Patients’ level of satisfaction on quality of health
care at Mwananyamala hospital in Dar es Salaam, Tanzania. BMC Health
Services Research, 14(1), 1–8. https://doi.org/10.1186/1472-6963-14-400
Kibusi, S. M., Kimunai, E., & Hines, C. S. (2015). Predictors for uptake of
intermittent preventive treatment of malaria in pregnancy (IPTp) in Tanzania.
BMC Public Health, 15(1), 1–8. https://doi.org/10.1186/s12889-015-1905-0
Kinney, M. V., Kerber, K. J., Black, R. E., Cohen, B., Nkrumah, F., Coovadia, H., …
Lawn, J. E. (2010). Sub-Saharan Africa’s mothers, newborns, and children:
Where and why do they die? PLoS Medicine, 7(6), 1–9.
https://doi.org/10.1371/journal.pmed.1000294
Kolehmainen-Aitken, R. L. (2004). Decentralization’s impact on the health
workforce: Perspectives of managers, workers and national leaders. Human
Resources for Health, 2, 1–11. https://doi.org/10.1186/1478-4491-2-5
Komba, A. A. (2012). Strategies for enhancing equity in financing primary education
in Tanzania, 3(June), 495–501.
Kress, D. H., Su, Y., Wang, H., Kress, D. H., Su, Y., & Wang, H. (2016).
Assessment of Primary Health Care System Performance in Nigeria : Using the
Primary Health Care Performance Indicator Conceptual Framework Assessment
of Primary Health Care System Performance in Nigeria : Using the Primary
Health Care Performance Indicato, 8604.
https://doi.org/10.1080/23288604.2016.1234861
Kruk, M. E., Leslie, H. H., Verguet, S., Mbaruku, G. M., Adanu, R. M. K., &
Langer, A. (2016). Quality of basic maternal care functions in health facilities of
five African countries: an analysis of national health system surveys. The
Lancet Global Health, 4(11), e845–e855. https://doi.org/10.1016/S2214-
109X(16)30180-2
Kutzin, J. (2013). Financement des soins de santé pour une couverture santé
universelle et résultats du système de santé: Concepts et implications politiques.
203
Bulletin of the World Health Organization, 91(8), 602–611.
https://doi.org/10.2471/BLT.12.113985
Langer, A., Salam, R. A., Lassi, Z. S., Link, C., Austin, A., Langer, A., … Bhutta, Z.
A. (2014). Approaches to improve the quality of maternal and newborn health
care : an overview of the evidence The Harvard community has made this article
openly available . Please share how this access benefits you . Your story matters
. Approaches to improve the q. Reproductive Health, 11(Suppl 2), S1.
https://doi.org/10.1186/1742-4755-11-S2-S1
Liabsuetrakul, T., Petmanee, P., Sanguanchua, S., & Oumudee, N. (2012). Health
system responsiveness for delivery care in Southern Thailand. International
Journal for Quality in Health Care, 24(2), 169–175.
Liaropoulos, L., & Goranitis, I. (2015). Health care financing and the sustainability
of health systems. International Journal for Equity in Health, 14(1), 5–8.
https://doi.org/10.1186/s12939-015-0208-5
Lindeman, S. (2014). “Until We Live Like They Live in Europe”: A Multilevel
Framework for Community Empowerment in Subsistence Markets. Journal of
Macromarketing, 34(2), 171–185. https://doi.org/10.1177/0276146713514753
Mainz, J. (2003). Defining and classifying clinical indicators for quality
improvement. International Journal for Quality in Health Care, 15(6), 523–
530. https://doi.org/10.1093/intqhc/mzg081
Maluka, S. (2017). Comprehensive case study from United Republic of Tanzania
PRIMARY HEALTH CARE SYSTEMS (PRIMASYS).
Maluka, S., Chitama, D., Dungumaro, E., Masawe, C., Rao, K., & Shroff, Z. (2018).
Contracting-out primary health care services in Tanzania towards UHC : how
policy processes and context influence policy design and implementation.
International Journal for Equity in Health, 17(118), 1–13.
https://doi.org/10.1186/s12939-018-0835-8

204
Maluka, S. O., & Bukagile, G. (2016). Community participation in the decentralised
district health systems in Tanzania : why do some health committees perform
better than others ?, (June 2015), 86–104.
Mapunda, O. E., Msuya, S. E., A. Kapologwe, N., John, B., Damian, D. J., &
Mahande, M. J. (2016). Assessment of Maternal Mortality and its Associated
Causes at Shinyanga Regional Hospital in Tanzania. Women’s Health Bulletin,
Inpress(Inpress). https://doi.org/10.17795/whb-38976
Martin, V., Msuya, S. E., Kapologwe, N., Damian, D. J., John, B., & Mahande, M. J.
(2019). Prevalence and Determinants of Modern Contraceptive Methods Use
among Women of Reproductive Age (15 - 49 Years) in Rural Setting: A Case of
Kishapu District, Shinyanga Region. Advances in Sexual Medicine, 09(04), 53–
66. https://doi.org/10.4236/asm.2019.94005
Massoi, L., & Norman, A. S. (2009). Decentralisation by devolution in Tanzania:
Reflections on community involvement in the planning process in Kizota Ward
in Dodoma. Journal of Public Administration and Policy Research, 1(7), 133–
140.
Mayumana, I., Borghi, J., Anselmi, L., Mamdani, M., & Lange, S. (2017). Effects of
Payment for Performance on accountability mechanisms : Evidence from Pwani
, Tanzania. Social Science & Medicine, 179, 61–73.
https://doi.org/10.1016/j.socscimed.2017.02.022
Mboya, D., Mshana, C., Kessy, F., Alba, S., Lengeler, C., Renggli, S., … Schulze, A.
(2016). Embedding systematic quality assessments in supportive supervision at
primary healthcare level : application of an electronic Tool to Improve Quality
of Healthcare in Tanzania. BMC Health Services Research, 1–15.
https://doi.org/10.1186/s12913-016-1809-4
Mgata, S., & Maluka, S. O. (2019). Factors for late initiation of antenatal care in Dar
es Salaam, Tanzania: A qualitative study. BMC Pregnancy and Childbirth,
19(1), 415. https://doi.org/10.1186/s12884-019-2576-0

205
MoHCDGEC., PORALG., (2017). Direct Health Facility Financing Guide.
Dodoma.
Mmari, V., Stephen, K., Lilian, M., & Osaki, K. (2019). The Implementation Fidelity
of Competency Based Curriculum for Nursing and Midwifery Programme in
Tanzania: A protocol for a Mixed Methods. Nursing & Primary Care, 3(2).
https://doi.org/10.33425/2639-9474.1101
Mohammadi, A., & Koorosh, K. (2014). Responsiveness in the Healthcare Settings :
A Survey of Inpatients. International Journal of Hospital Research, 3(3), 123–
132.
MoHCDGEC, MoH [Zanzibar], (2016). Tanzania Demographic and Health Survey
and Malaria Indicator Survey 2015-2016. Tanzania Demographic and Health
Survey and Malaria Indicator Survey (TDHS-MIS) 2015-16. Dar es Salaam,
Tanzania, and Rockville, Maryland, USA.
MoHCDGEC. (2015). Availability , Utilisation and Quality of Emergency Obstetric
and New-born Care ( EmONC ) Services in Tanzania Mainland.
MOHCDGEC. (2016). The National Road Map Strategic Plan to Improve
Reproductive, Maternal, Newborn, Child and Adolescent Health in Tanzania
(2016 - 2020) (One Plan II), (June), 142.
MoHSW. (2011a). The Tanzania Quality Improvement Framework in Health Care
(2011 - 2016).
MoHSW. (2011b). Comprehensive Council Health Planning Guidelines, (July), 1–
393.
MoHSW. (2014). RESULT BASED FINANCING (RBF) OPERATIONAL
MANUAL.
MoHSW. (2015). Tanzania Health Sector Strategic Plan 2015 -2020 (HSSP IV),
2020(July), 53.
206
MOHSW. (2009). National Guidelines for Improving Quality of Care, Support, and
Protection for Most Vulnerable Children in Tanzania. Ministry of Health and
Social Welfare, (September).
Molenberghs, G. (2010). Sampling Techniques Master in Statistics , Universiteit
Hasselt Master in Quantitative Methods , Katholieke Universiteit Brussel
Contents.
Moore, G., Audrey, S., Barker, M., & Bond, L. (2014). Process evaluation of
complex interventions. UK Medical Research Council (MRC) Guidance
Prepared, 19–45; 64–75.
https://doi.org/http://www.populationhealthsciences.org/MRC-PHSRN-Process-
evaluation-guidance-final-2-.pdf
Mowbray, C. T., Holter, M. C., Gregory, B., & Bybee, D. (2003). Fidelity Criteria :
Development , Measurement , and Validation. American Journal of Evaluation,
24(3), 315–340.
Mpambije, C. J. (2017). Decentralisation of Health Systems and the Fate of
Community Health Fund in Tanzania : Critical Review of High and Low
Performing Districts, 5(2), 136–144.
https://doi.org/10.11648/j.sjph.20170502.21
Murray, C. J., & Frenk, J. (2000). A framework for assessing the performance of
health systems. Bulletin of the World Health Organization, 78(6), 717–731.
https://doi.org/10.1590/S0042-96862000000600004
Musau, S., Chee, G., Patsika, R., Malangalila, E., Chitama, D., Van Praag, E., &
Schettler, G. (2011). Tanzania Health System Assessment 2010, (January), 1–
101.
Musgrove, P., Creese, A., Preker, A., Baeza, C., Anell, A., & Prentice, T. (2000).
Health Systems: Improving Perfomance. World Health Organization, 78(1), 1–
215. https://doi.org/10.1146/annurev.ecolsys.35.021103.105711
207
Mwansisya, T. E., & Mwansisya, G. C. M. (2015). Reliability and Validity of Patient
Satisfaction Questionnaire for Community Pharmacies in Dodoma Municipality
, Tanzania, 2(6), 163–170.
Naghavi, M., Wang, H., Lozano, R., Davis, A., Liang, X., Zhou, M., … Temesgen,
A. M. (2015). Global, regional, and national age-sex specific all-cause and
cause-specific mortality for 240 causes of death, 1990-2013: A systematic
analysis for the Global Burden of Disease Study 2013. The Lancet, 385(9963),
117–171. https://doi.org/10.1016/S0140-6736(14)61682-2
Nielsen, K., & Randall, R. (2013). Opening the black box : Presenting a model for
evaluating organizational-level interventions, 0643(January).
https://doi.org/10.1080/1359432X.2012.690556
NIMR. (2010). Evidence-informed Policy Making in the United Republic of
Tanzania : Setting REACH-Policy Initiative Priorities for Evidence-Informed
Policy Making in the United Republic of Tanzania : Setting REACH-Policy
Initiative Priorities for 2008-2010. Reeport, (September 2008).
Njeru, M. K., Blystad, A., Nyamongo, I. K., & Fylkesnes, K. (2009). A critical
assessment of the WHO responsiveness tool : lessons from voluntary HIV
testing and counselling services in Kenya. BMC Health Services Research, 11,
1–11. https://doi.org/10.1186/1472-6963-9-243
Nunnally, J. C., & Bernstein, I. H. (1979). Psychometric theory. PsycCRITIQUES.
https://doi.org/10.1037/018882
Nurjono, M., Shrestha, P., Yi, I., Ang, H., Shiraz, F., Yoong, J. S., … Vrijhoef, M.
(2019). Implementation fidelity of a strategy to integrate service delivery :
learnings from a transitional care program for individuals with complex needs in
Singapore. BMC Health Services Research, 19(177), 1–14.
https://doi.org/https://doi.org/10.1186/s12913-019-3980-x (2019)
O’Cathain, A., Murphy, E., & Nicholl, J. (2008). The quality of mixed methods
studies in health services research. Journal of Health Services Research and
208
Policy, 13(2), 92–98. https://doi.org/10.1258/jhsrp.2007.007074
Odd-Helge Fjeldstad, L. K. and E. N. (2010). Planning in Local Government
Authorities in Tanzania: Bottom-up Meets Top-down. Repoa Brief, (18).
OECD. (2017). Statistics by region: Africa. Development Aid at a Glance.
Ojemeni, M. T., Niles, P., Mfaume, S., Kapologwe, N. A., Deng, L., Stafford, R., …
Squires, A. (2017). A case study on building capacity to improve clinical
mentoring and maternal child health in rural Tanzania: the path to
implementation. BMC Nursing, 16(1), 57. https://doi.org/10.1186/s12912-017-
0252-0
Olafsdottir, A. E., Mayumana, I., Mashasi, I., Njau, I., Mamdani, M., Patouillard, E.,
… Borghi, J. (2014). Pay for performance : an analysis of the context of
implementation in a pilot project in Tanzania, 1–9.
Opwora, A., Kabare, M., Molyneux, S., & Goodman, C. (2009). The Implementation
and Effects of Direct Facility Funding in Kenya’s Health Centres and
Dispensaries, (April), 1–28.
Opwora, A., Kabare, M., Molyneux, S., & Goodman, C. (2010). Direct facility
funding as a response to user fee reduction: Implementation and perceived
impact among Kenyan health centres and dispensaries. Health Policy and
Planning, 25(5), 406–418. https://doi.org/10.1093/heapol/czq009
Opwora, A., Waweru, E., Toda, M., Noor, A., Edwards, T., Fegan, G., … Goodman,
C. (2015). Implementation of patient charges at primary care facilities in Kenya:
Implications of low adherence to user fee policy for users and facility revenue.
Health Policy and Planning, 30(4), 508–517.
https://doi.org/10.1093/heapol/czu026
Panda, B., & Thakur, H. P. (2016). Decentralization and health system performance
– a focused review of dimensions , difficulties , and derivatives in. BMC Health
Services Research, 16(Suppl 6), 1–14. https://doi.org/10.1186/s12913-016-
209
1784-9
Pérez, D., Stuyft, P. Van Der, Zabala, C., Castro, M., & Lefèvre, P. (2016). A
modified theoretical framework to assess implementation fidelity of adaptive
public health interventions. Implementation Science, 11(91), 1–11.
https://doi.org/10.1186/s13012-016-0457-8
Peters, D.H., Tran, N. T., & Adam, T. (2013). Implementation Research in Health: a
practical guide. Alliance for Health Policy and Systems Research, World Health
Organization. A Practical Guide, 66. https://doi.org/ISBN 978 92 4 150621 2
Peters, David H., Adam, T., Alonge, O., Agyepong, I. A., & Tran, N. (2014).
Republished research: Implementation research: What it is and how to do it.
British Journal of Sports Medicine, 48(8), 731–736.
https://doi.org/10.1136/bmj.f6753
PWC. (2016). Sub-national (Local Government) PEFA Assessment in Tanzania
Final Consolidated Report, (July).
Raine, R., Fitzpatrick, R., Barratt, H., Bevan, G., Black, N., Boaden, R., …
Zwarenstein, M. (2016). Challenges, solutions and future directions in the
evaluation of service innovations in health care and public health. Health
Services and Delivery Research, 4(16), 1–136.
https://doi.org/10.3310/hsdr04160
Ramsey, K., Hingora, A., Kante, M., Jackson, E., Exavery, A., Pemba, S., …
Phillips, J. F. (2013). The Tanzania Connect Project: A cluster-randomized trial
of the child survival impact of adding paid community health workers to an
existing facility-focused health system. BMC Health Services Research,
13(SUPPL.2), S6. https://doi.org/10.1186/1472-6963-13-S2-S6
Renggli, S. (2017). Promoting Universal Health Coverage in Tanzania : Towards
Improved Health Service Quality and Financial Protection.
Rifkin, S. B. (2018). Alma Ata after 40 years: Primary Health Care and Health for
210
All-from consensus to complexity. BMJ Global Health, 3, 1–7.
https://doi.org/10.1136/bmjgh-2018-001188
Roberts, M. J., Reich, M. R., Hsiao, W., & Berman, P. (2002). Getting Health
Reform Right (First). Oxford University Press.
Robone, S., Rice, N., & Smith, P. C. (2011). Health Systems’ Responsiveness and Its
Characteristics: A cross-Country Comparative Analysis. Health Services
Research, 46(6 PART 2), 2079–2100. https://doi.org/10.1111/j.1475-
6773.2011.01291.x
Rogers, P. J. (2008). Using programme theory to evaluate complicated and complex
aspects of interventions. Evaluation, 14(1), 29–48.
https://doi.org/10.1177/1356389007084674
ROURKE, A. J. (1957). Evaluating the quality of medical care. Hospital Progress,
38(9), 72–73. https://doi.org/10.2307/3348969
Saltman, R. B., Bankauskaite, V., & Vrangbaek, K. (2007). Decentralization in
Health Care. European Observatory on Health Systems and Policies Series, 9–
21. https://doi.org/126,00 Euro
Samky, H. (2019). The Influence of Direct Health Facility Financing on Perceived
Health System Responsiveness , Health Service Satisfaction and Accountability
Compliance Among Public Primary Health Facilities in Central Zone of
Tanzania . Master of Science in Public Health.
Sando, D., Ratcliffe, H., McDonald, K., Spiegelman, D., Lyatuu, G., Mwanyika-
Sando, M., Langer, A. (2016). The prevalence of disrespect and abuse during
facility-based childbirth in urban Tanzania. BMC Pregnancy and Childbirth,
16(1), 1–10. https://doi.org/10.1186/s12884-016-1019-4
Savedoff, W. D. (2011). Governance in the Health Sector: A Strategy for Measuring
Determinants and Performance. Corporate Governance, 1(May), 780–0810.
https://doi.org/doi:10.1596/1813-9450-5655

211
Schaap, R., Bessems, K., Otten, R., Kremers, S., & van Nassau, F. (2018).
Measuring implementation fidelity of school-based obesity prevention
programmes: A systematic review. International Journal of Behavioral
Nutrition and Physical Activity, 15(1), 1–14. https://doi.org/10.1186/s12966-
018-0709-x
Sharon Mihalic. (2002). The importance of implementation fidelity, (57), 1–16.
O’donnell, D., Donnelly, S., Davies, C., Fattori, F., & Kroll, T. (2020). “What
Bothers Me Most Is the Disparity between the Choices that People Have or
Don’t Have”: A Qualitative Study on the Health Systems Responsiveness to
Implementing the Assisted Decision-Making (Capacity) Act in Ireland.
International Journal of Environmental Research and Public Health, 17(9).
https://doi.org/10.3390/ijerph17093294
Shewade, H. D., & Aggarwal, A. K. (2012). Health sector reforms: Concepts, market
based reforms and health inequity in India. Educational Research, 3(2), 118–
125.
Shoo, R. S., Mboera, L. E. G., Ndeki, S., & Munishi, G. (2017). Stagnating maternal
mortality in Tanzania: What went wrong and what can be done. Tanzania
Journal of Health Research, 19(2), 1–12. https://doi.org/10.4314/thrb.v19i2.6
Smith & Firth, (2011). Qualitative data analysis: application of the framework
approach, 18, 52–62.
Smith, P. C. (2002). Measuring health system performance. European Journal of
Health Economics, 3(3), 145–148. https://doi.org/10.1007/s10198-002-0138-1
Smith, P. C., & Busse, R. (2008). Health policy and performance measurement.
Performance Measurement for Health System Improvement Experiences,
Challenges and Prospects.
Smith, P. C., Rice, N., Robone, S., & Smith, P. C. (2008). The measurement and
comparison of health system responsiveness. Health, Econometrics and Data

212
Group (HEDG), 08/05(March).
Stains, M., & Vickrey, T. (2017). Fidelity of Implementation : An Overlooked Yet
Critical Construct to Establish Effectiveness of Evidence-Based Instructional
Practices. American Society for Cell Biology, 1–11.
https://doi.org/10.1187/cbe.16-03-0113
Stuart, K., Maynard, L., & Rouncefield, C. (2017). Types of Evaluation. Evaluation
Practice for Projects with Young People: A Guide to Creative Research, 59–78.
https://doi.org/10.4135/9781473917811.n5
Sun, D., Ahn, H., Lievens, T., & Zeng, W. (2017). Evaluation of the performance of
national health systems in 2004-2011 : An analysis of 173 countries, 1–13.
https://doi.org/10.1371/journal.pone.0173346
Ministry of Health and Social Welfare. (2013). Tanzania Service Availability and
Readiness Assessment (SARA). World Health Organisation (WHO), (July).
Tashobya, C., da Silveira, V., Ssengooba, F., Nabyonga-Orem, J., Macq, J., & Criel,
B. (2014). Health systems performance assessment in low-income countries:
learning from international experiences. Globalization and Health, 10(1), 5.
https://doi.org/10.1186/1744-8603-10-5
The United Republic of Tanzania. (2016). Annual Health Sector Perfomance Profile
2014/2015. Dar es Salaam.
The World Bank. (2005). Financing health in low-income countries. Health
Financing Revisited, 209–248.
The World Bank. (2013). Results-Based Financing for Health. African Health
Forum, 3–6.
The World Bank. (2015). Fiduciary Systems Assessment Tanzania – Strengthening
Primary Health Care Services for Results, (March).
Tomson, G., & Biermann, O. (2015). Health Policy Reform in Low-Income and

213
Lower Middle-Income Countries in Southeast Asia BT - The Palgrave
International Handbook of Healthcare Policy and Governance. In E. Kuhlmann,
R. H. Blank, I. L. Bourgeault, & C. Wendt (Eds.) (pp. 171–187). London:
Palgrave Macmillan UK. https://doi.org/10.1057/9781137384935_11
Toomey, E., Matthews, J., & Hurley, D. A. (2017). Using mixed methods to assess
fidelity of delivery and its influencing factors in a complex self-management
intervention for people with osteoarthritis and low back pain. BMJ Global
Health, 7(e015452), 1–14. https://doi.org/10.1136/bmjopen-2016-015452
Tsofa, B., Goodman, C., Gilson, L., & Molyneux, S. (2017). Devolution and its
effects on health workforce and commodities management - early
implementation experiences in Kilifi County, Kenya. International Journal for
Equity in Health, 16(1), 169. https://doi.org/10.1186/s12939-017-0663-2
Umarji, M. (2015). Informative Note PEFA | Public Expenditure and Financial
Accountability Assessment Methodology Maputo , February 2015.
UN. (2015). Sustainable development goals - United Nations.
URT. (1999). Vision and Priorities to Achieve Middle Income Status by 2025
Contents from Ministry of Finance & Planning 1–35.
URT. (2007). Primary Health Services Development Programme - MMAM: 2007-
2017, 1–130.
Valentine, N., de Silva, A., Kawabata, K., Darby, C., Murray, C., Evans, D., & et al.
(2003). Health system responsiveness: concepts, domains, and
operationalization. Health System Responsiveness: Debate, Methods and
Empericism, (January 2003), 573–596.
Van Den Broek, N. R., & Graham, W. J. (2009). Quality of care for maternal and
newborn health: The neglected agenda. BJOG: An International Journal of
Obstetrics and Gynaecology, 116(SUPPL. 1), 18–21.
https://doi.org/10.1111/j.1471-0528.2009.02333.x
214
Van Der Kooy, J., Valentine, N. B., Birnie, E., Vujkovic, M., De Graaf, J. P.,
Denktaş, S., … Bonsel, G. J. (2014). Validity of a questionnaire measuring the
world health organization concept of health system responsiveness with respect
to perinatal services in the Dutch obstetric care system. BMC Health Services
Research, 14(1). https://doi.org/10.1186/s12913-014-0622-1
Vesel, L., Manu, A., Lohela, T. J., Gabrysch, S., Okyere, E., Ten Asbroek, A. H. A.,
… Kirkwood, B. R. (2013). Quality of newborn care: A health facility
assessment in rural Ghana using survey, vignette and surveillance data. BMJ
Open, 3(5), 1–11. https://doi.org/10.1136/bmjopen-2012-002326
Victoria, E., (2011). Fiscal Decentralisation and Infant Mortality Rates: The
Colombian Case
Waiswa, P., Manzi, F., Mbaruku, G., Rowe, A. K., Marx, M., Tomson, G., …
Hanson, C. (2017). Effects of the EQUIP quasi-experimental study testing a
collaborative quality improvement approach for maternal and newborn health
care in Tanzania and Uganda. Implementation Science, 12(1), 89.
https://doi.org/10.1186/s13012-017-0604-x
Walraven, G. (2019). The 2018 Astana Declaration on primary health care, is it
useful? Journal of Global Health, 9(1). https://doi.org/10.7189/jogh.09.010313
Wang, M., Fang, H., Bishwajit, G., Xiang, Y., Fu, H., & Feng, Z. (2015). Evaluation
of rural primary health care in Western China: A cross-sectional study.
International Journal of Environmental Research and Public Health, 12(11),
13843–13860. https://doi.org/10.3390/ijerph121113843
Waweru, E., Goodman, C., Kedenge, S., Tsofa, B., & Molyneux, S. (2016). Tracking
implementation and (un)intended consequences: A process evaluation of an
innovative peripheral health facility financing mechanism in Kenya. Health
Policy and Planning, 31(2), 137–147. https://doi.org/10.1093/heapol/czv030
Waweru, E., Molyneux, S., Goodman, C., & Tsofa, B. (2016). Direct funding of
health facilities: Findings from an evaluation of the Health Sector Services Fund

215
in Kenya. Resilient & Responsive Health System, 2010–2013.
Waweru, E., Opwora, A., Toda, M., Fegan, G., Edwards, T., & Goodman, C. (2013).
Are Health Facility Management Committees in Kenya ready to implement
financial management tasks : findings from a nationally representative survey,
1–14.
Westaway, M. S., Rheeder, P., Van Zyl, D. G., & Seager, J. R. (2003). Interpersonal
and organizational dimensions of patient satisfaction: the moderating effects of
health status. International Journal for Quality in Health Care : Journal of the
International Society for Quality in Health Care, 15(4), 337–344.
WHO, OECD, WB. (2018). Delivering quality health services.
WHO, UNICEF, UNFPA, World Bank Group, U. N. P. D. (2019). Trends in
maternal mortality: 2000 to 2017: estimates. Geneva.
WHO. (2013). Arguing for Universal Health Coverage. World Health Organization,
39.
WHO. (2016). The sustainable development goals report 2016. The Sustainable
Development Goals Report 2016.
https://doi.org/10.29171/azu_acku_pamphlet_k3240_s878_2016
Stansfield, S. K., Walsh, J., Prata, N., Evans, T., Organization, W. H., … Low-Beer,
D. (2012). Monitoring and evaluation of health systems strengthening: An
operational framework. Health (San Francisco), 2nd Editio(November), 1–19.
https://doi.org/10.3402/gha.v6i0.20001
WHO, & WORLDBANK. (2012). Trends in Maternal Mortality : 1990 to 2010.
Organization, 32(5), 1–55. https://doi.org/ISBN 978 92 4 150363 1
Wiedenmayer, K. A., Kapologwe, N.A, Charles, J., Chilunda, F., & Mapunjo, S.
(2015). The reality of task shifting in medicines management- a case study from
Tanzania. Journal of Pharmaceutical Policy and Practice, 8(1).
https://doi.org/10.1186/s40545-015-0032-8
216
Wiedenmayer, K., Mbwasi, R., Mfuko, W., Mpuya, E., Charles, J., Chilunda, F., …
Kapologwe, N. (2019). Jazia prime vendor system- A public-private partnership
to improve medicine availability in Tanzania: From pilot to scale. Journal of
Pharmaceutical Policy and Practice, 12(1), 1–10.
https://doi.org/10.1186/s40545-019-0163-4
World Health Organization. (2017). Developing a national health financing strategy:
A reference guide.
Yahya, T., & Mohamed, M. (2018). Raising a mirror to quality of care in Tanzania:
the five-star assessment. The Lancet Global Health, 6(11), e1155–e1157.
https://doi.org/10.1016/S2214-109X(18)30348-6
Yakob, B., & Ncama, B. P. (2017). Measuring health system responsiveness at
facility level in Ethiopia : performance , correlates and implications. BMC
Health Services Research, 17(263), 1–12. https://doi.org/10.1186/s12913-017-
2224-1
217
PUBLICATIONS
Publication Paper 1: Understanding the implementation of direct health facility
financing and its effect on health system performance in Tanzania

218
Publication Paper 2: Assessing health system responsiveness in primary health
care facilities in Tanzania

219
APPENDICES
Appendix I: A descriptive results of Health System Responsiveness as perceived
by patients in PPHF before and after implementation of DHFF
Domain Time Responsiveness
% Score, Mean
[95% CI]
Min–Max
% score
Negative
N (%)
Positive
N (%)
Prompt
attention
Base line 79.40[77.48,
81.32]
0.00- 100.00 135(31.99) 287(68.01)
End line 81.01[79.47,
82.55]
28.57-100.00 142(33.65) 280 (66.35)
All 80.21[78.98,
81.44]
0.00-100.00 277
(32.82)
567(67.18)
Respect for
dignity
Base line 78.95[76.82,
81.07]
0.00- 100.00 166(39.34) 256(60.66)
End line 82.02[80.28,
83.75]
22.22-100.00 151(35.78) 271(64.22)
All 80.48[79.11,
81.86]
0.00- 100.00 317(37.56) 527(62.44)
Clear
communicatio
n
Base line 74.64[72.31,
76.98]
0.00- 100.00 204(48.34) 218(51.66)
End line 61.22[59.74,
62.69]
28.57-100.00 300(71.09) 122(28.91)
All 67.93[66.48, 0.00- 100.00 504(59.72) 340(40.28)

220
69.38]
Respect of
autonomy
Base line 76.74[74.18,
79.30]
0.00- 100.00 168(39.81) 254(60.19)
End line 85.60[83.89,
87.30]
22.22-100.00 84(19.91) 338(80.09)
All 81.17[79.60,
82.73]
0.00- 100.00 252(29.86) 592(70.14)
Access to care Base line 48.61[46.63,
50.59]
14.29-100.00 280(66.35) 142(33.65)
End line 55.44[53.85,
57.02]
25.00-100.00 213(50.47) 209(49.53)
All 52.02[50.74,
53.31]
14.29-100.00 493(58.41) 351(41.59)
Respect for
confidentiality
Base line 87.64[85.01,
90.26]
0.00- 100.00 82(19.43) 340 (80.57)
End line 85.70[84.05,
87.36]
33.33-100.00 141(33.41) 281(66.59)
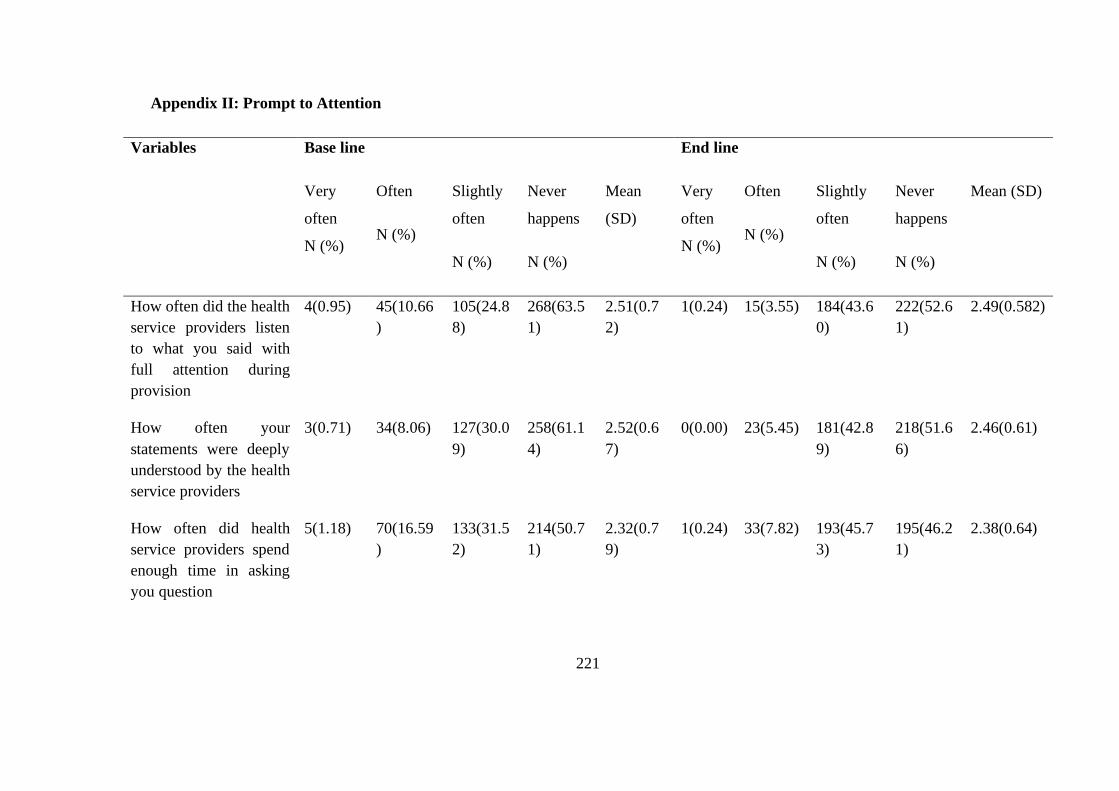
221
Appendix II: Prompt to Attention
Variables Base line End line
Very
often
N (%)
Often
N (%)
Slightly
often
N (%)
Never
happens
N (%)
Mean
(SD)
Very
often
N (%)
Often
N (%)
Slightly
often
N (%)
Never
happens
N (%)
Mean (SD)
How often did the health
service providers listen
to what you said with
full attention during
provision
4(0.95) 45(10.66
)
105(24.8
8)
268(63.5
1)
2.51(0.7
2)
1(0.24) 15(3.55) 184(43.6
0)
222(52.6
1)
2.49(0.582)
How often your
statements were deeply
understood by the health
service providers
3(0.71) 34(8.06) 127(30.0
9)
258(61.1
4)
2.52(0.6
7)
0(0.00) 23(5.45) 181(42.8
9)
218(51.6
6)
2.46(0.61)
How often did health
service providers spend
enough time in asking
you question
5(1.18) 70(16.59
)
133(31.5
2)
214(50.7
1)
2.32(0.7
9)
1(0.24) 33(7.82) 193(45.7
3)
195(46.2
1)
2.38(0.64)

222
How often the health
service providers were
accurately and actively
in following up your
treatment process
14(3.32) 71(16.82
)
160(37.9
1)
177(41.9
4)
2.18(0.8
3)
5(1.18) 56(13.27
)
171(40.5
2)
190(45.0
2)
2.29(0.74)
Are the clients with
similar needs treated
equally in this health
facility?
4(0.95) 10(2.37) 161(38.1
5)
247(58.5
3)
2.54(0.5
9)
1(0.24) 10(2.37) 177(41.9
4)
234(55.4
5)
2.53(0.56)
Are Clients with
unequal needs treated
equally in the health
units?
3(0.71) 22(5.21) 172(40.7
6)
225(53.3
2)
2.47(0.6
3)
2(0.47) 21(4.98) 189(44.7
9)
210(49.7
6)
2.43(0.61)
Has the health facility
always met your
expectations?
1(0.24) 26(6.16) 180(42.6
5)
215(50.9
5)
2.44(0.6
2)
1(0.24) 25(5.92) 189(44.7
9)
207(49.0
5)
2.41(0.61)
Attention 0(0.00) 12(2.84) 204(48.3
4)
206(48.8
2)
2.46(0.5
5)
0(0.00) 9(2.13) 209(49.5
3)
204(48.3
4)
2.46(0.54)

223
Appendix III: Respect to Dignity
Variables Base line End line
Very
often
N (%)
Often
N (%)
Slightly
often
N (%)
Never
happens
N (%)
Mean
(SD)
Very
often
N (%)
Often
N (%)
Slightly
often
N (%)
Never
happens
N (%)
Mean
(SD)
How often did the health
service providers show
courtesy and affection
towards you during
service provision
7(1.66
)
46(10.90
)
118(27.96) 251(59.4
8)
2.45(0.7
5)
2(0.47
)
48(11.37
)
150(35.5
5)
222(52.61
)
2.40(0.71)
How often did the health
care workers paid
attention specifically into
your need
7(1.66
)
64(15.17
)
153(36.26) 198(46.9
2)
2.28(0.7
8)
0(0.00
)
12(2.84) 181(42.8
9)
229(54.27
)
2.51(0.55)
How often is respect
shown for the client’s
desire for privacy during
treatment
1(0.24
)
29(6.87) 158(37.44) 234(55.4
5)
2.48(0.6
3)
2(0.47
)
29(6.87) 162(38.3
9)
229(54.27
)
2.46(0.64)
Dignity 0(0.00
)
23(5.45) 193(45.73) 206(48.8
2)
2.43(0.6
0)
0(0.00
)
18(4.27) 187(44.3
1)
217(51.42
)
2.47(0.58)

224
Appendix IV: Clear Communication
Variables Base line End line
Very
often
N (%)
Often
N (%)
Slightly
oftenN
(%)
Never
happensN
(%)
Mean
(SD)
Very
often
N (%)
OftenN
(%)
Slightly
often
N (%)
Never
happens
N (%)
Mean (SD)
How often did health
care workers explain
things in a way you
could understand?
5(1.18) 56(13.27
)
150(35.5
5)
211(50.00
)
2.34(0.7
5)
0(0.00
)
28(6.64
)
166
(39.34)
228
(54.03)
2.47 (0.62)
How often health care
workers explain things
and issues related to
your health in detail
for you?
22(5.21
)
71(16.82
)
157(37.2
0)
172(40.76
)
2.14(0.8
8)
5(1.18
)
36(8.53
)
168
(39.81)
213
(50.47)
2.40 (0.69)
How would you rate your experience about how well you were treated as human during interaction with
Not
Satisfie
d
N (%)
Satisfied
N (%)
Very
Satisfied
N (%)
Highly
Satisfied
N (%)
Mean(S
D)
Not
Satisfie
d
N (%)
Satisfied
N (%)
Very
Satisfied
N (%)
Highly
Satisfie
d
N (%)
Mean(SD)
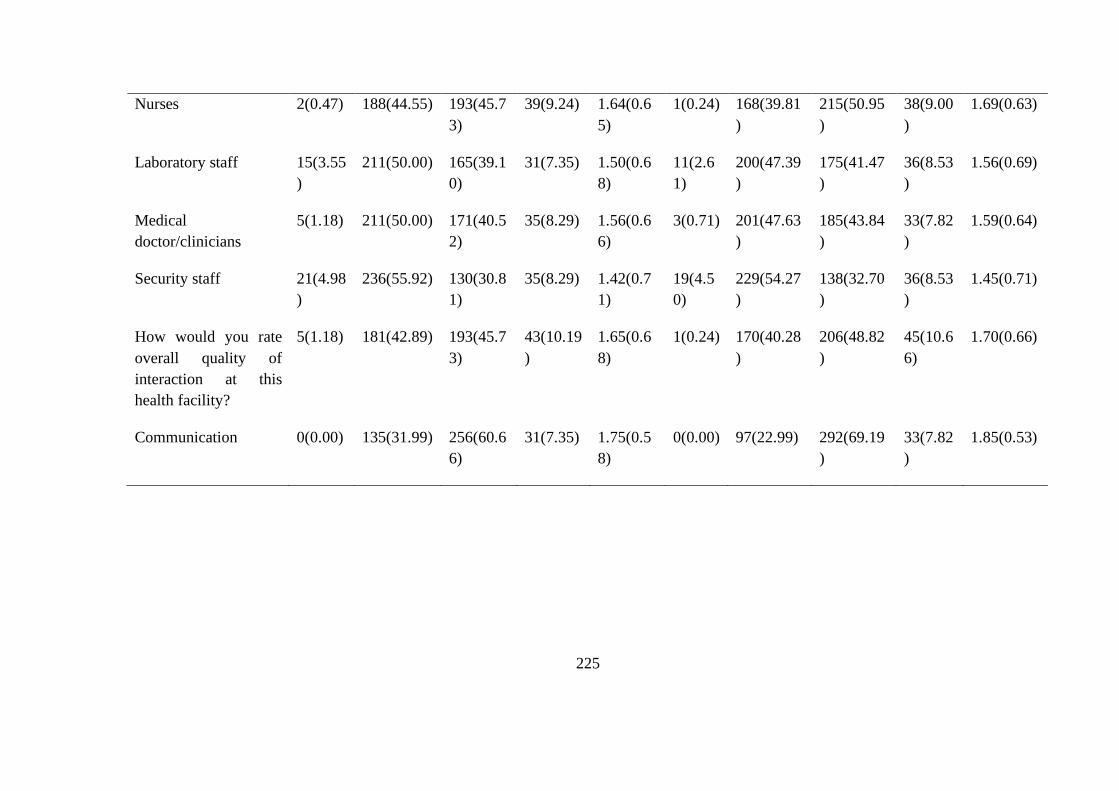
225
Nurses 2(0.47) 188(44.55) 193(45.7
3)
39(9.24) 1.64(0.6
5)
1(0.24) 168(39.81
)
215(50.95
)
38(9.00
)
1.69(0.63)
Laboratory staff 15(3.55
)
211(50.00) 165(39.1
0)
31(7.35) 1.50(0.6
8)
11(2.6
1)
200(47.39
)
175(41.47
)
36(8.53
)
1.56(0.69)
Medical
doctor/clinicians
5(1.18) 211(50.00) 171(40.5
2)
35(8.29) 1.56(0.6
6)
3(0.71) 201(47.63
)
185(43.84
)
33(7.82
)
1.59(0.64)
Security staff 21(4.98
)
236(55.92) 130(30.8
1)
35(8.29) 1.42(0.7
1)
19(4.5
0)
229(54.27
)
138(32.70
)
36(8.53
)
1.45(0.71)
How would you rate
overall quality of
interaction at this
health facility?
5(1.18) 181(42.89) 193(45.7
3)
43(10.19
)
1.65(0.6
8)
1(0.24) 170(40.28
)
206(48.82
)
45(10.6
6)
1.70(0.66)
Communication 0(0.00) 135(31.99) 256(60.6
6)
31(7.35) 1.75(0.5
8)
0(0.00) 97(22.99) 292(69.19
)
33(7.82
)
1.85(0.53)

226
Appendix V: Respect to Autonomy
Variables Baseline Endline
Very
often
N (%)
Often
N (%)
Slightly
often
N (%)
Never
happens
N (%)
Mean
(SD)
Very
often
N (%)
Often
N (%)
Slightly
often
N (%)
Never
happens
N (%)
Mean
(SD)
How big a problem if any
was it to get an
appointment with the
health care workers
38(9.00
)
24(5.69)
76(18.01
)
284(67.3
0)
2.44(0.9
5)
6(1.42) 39(9.24) 67(15.88
)
310(73.4
6)
2.61(0.71)
How big a problem (if
any) was it to use other
health facility other than
the on
36(8.53
)
59(13.98
)
125(29.6
2)
202(47.8
7)
2.17(0.9
7)
4(0.95) 29(6.87) 84(19.91
)
305(72.2
7)
2.64(0.65)
Do you feel that physicians
provide you with choices
and options on the service
5(1.18) 44(10.43
)
127(30.0
9)
246(58.2
9)
2.45(0.73)
Autonomy 12(2.84
)
42(9.95) 114(27.0
1)
254(60.1
9)
2.45(0.7
9)
0(0.00) 26(6.16) 126(29.8
6)
270(63.9
8)
2.58(0.61)

227
Appendix VI: Access to Care
Variables Base line End line
Above
30min
N (%)
Up to
30min N
(%)
Few
minutes
N (%)
Serviced
instantly
N (%)
Mean
(SD)
Above
30min
N (%)
Up to
30min N
(%)
Few
minutes
N (%)
Instantl
y
N (%)
Mean
(SD)
How long did you
have to wait to get
medical consultation
from service
provider?
207(49.05
)
115(27.2
5)
87(20.62
)
13(3.08) 1.78(0.8
8)
146(34.6
0)
182(43.1
3)
74(17.54
)
20(4.74
)
1.92(0.8
4)
How long did you
have to stay in the
waiting room?
136(32.23
)
127(30.0
9)
135(31.9
9)
24(5.69) 2.11(0.9
3)
78(18.48
)
201(47.6
3)
105(24.8
8)
38(9.00
)
2.24(0.8
6)
How long did you
have to stay at the
pharmacy or
34(8.06) 130(30.8
1)
132(31.2
8)
126(29.8
6)
1.83(0.9
5)
45(10.66
)
153(36.2
6)
191(45.2
6)
33(7.82
)
2.50(0.7
9)

228
dispensing area?
How long did you
have to stay waiting
for laboratory
services and results?
43(10.19) 110(26.0
7)
122(28.9
1)
147(34.8
3)
1.88(1.0
0)
80(18.96
)
202(47.8
7)
116(27.4
9)
24(5.69
)
2.20(0.8
1)
Access to care? 126(29.86
)
154(36.4
9)
121(28.6
7)
21(4.98) 2.09(0.8
8)
42(9.95) 212(50.2
4)
145(34.3
6)
23(5.45
)
2.35(0.7
3)
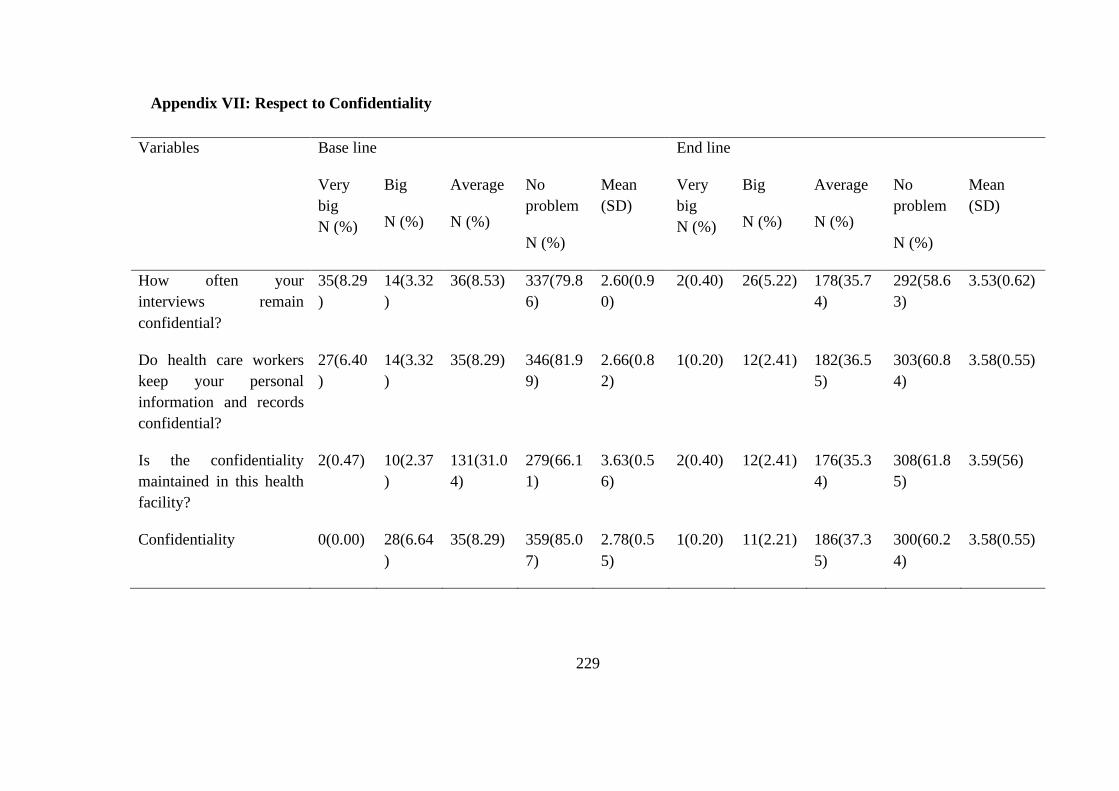
229
Appendix VII: Respect to Confidentiality
Variables Base line End line
Very
big
N (%)
Big
N (%)
Average
N (%)
No
problem
N (%)
Mean
(SD)
Very
big
N (%)
Big
N (%)
Average
N (%)
No
problem
N (%)
Mean
(SD)
How often your
interviews remain
confidential?
35(8.29
)
14(3.32
)
36(8.53) 337(79.8
6)
2.60(0.9
0)
2(0.40) 26(5.22) 178(35.7
4)
292(58.6
3)
3.53(0.62)
Do health care workers
keep your personal
information and records
confidential?
27(6.40
)
14(3.32
)
35(8.29) 346(81.9
9)
2.66(0.8
2)
1(0.20) 12(2.41) 182(36.5
5)
303(60.8
4)
3.58(0.55)
Is the confidentiality
maintained in this health
facility?
2(0.47) 10(2.37
)
131(31.0
4)
279(66.1
1)
3.63(0.5
6)
2(0.40) 12(2.41) 176(35.3
4)
308(61.8
5)
3.59(56)
Confidentiality 0(0.00) 28(6.64
)
35(8.29) 359(85.0
7)
2.78(0.5
5)
1(0.20) 11(2.21) 186(37.3
5)
300(60.2
4)
3.58(0.55)

230
Appendix VIII: Basic Amenities
Variables Base line End line
Strongly
disagree
N (%)
Disagree
N (%)
Agree
N (%)
Strongly
agree N
(%)
Mean
(SD)
Strongly
disagree
N (%)
Disagree
N (%)
Agree
N (%)
Strongl
y agree
N (%)
Mean
(SD)
This health
facility has
enough buildings
for service
delivery
121(28.67
)
219(51.9
0)
70(16.59
)
12(2.84) 1.94(0.7
5)
99(19.88
)
164(32.9
3)
198(39.7
6)
37(7.43
)
2.35(0.88)
This facility has
enough
staff to service
clients
126(29.86
)
222(52.6
1)
63(14.93
)
11(2.61) 1.90(0.7
4)
115(23.0
9)
178(35.7
4)
184(36.9
5)
21(4.22
)
2.22(0.85)
I agree with the
quality of
direction aids of
18(4.27) 97(22.99
)
261(61.8
5)
46(10.90
)
2.79(0.6
8)
13(2.61) 89(17.87
)
375(75.3
0)
21(4.22
)
2.81(0.54)

231
Variables Base line End line
Strongly
disagree
N (%)
Disagree
N (%)
Agree
N (%)
Strongly
agree N
(%)
Mean
(SD)
Strongly
disagree
N (%)
Disagree
N (%)
Agree
N (%)
Strongl
y agree
N (%)
Mean
(SD)
this facility
I agree with the
cleanliness of this
surroundings
23(5.45) 114(27.0
1)
245(58.0
6)
40(9.48) 2.72(0.7
1)
7(1.41) 67(13.45
)
385(77.3
1)
39(7.83
)
2.92(0.51)
I agree with the
waiting
environment of
this facility
(waiting seats)
32(7.58) 126(29.8
6)
216(51.1
8)
48(11.37
)
2.66(0.7
8)
5(1.00) 79(15.86
)
376(75.5
0)
38(7.63
)
2.90(0.51)
Are you
convenient with
the safety of
service delivery
13(3.08) 65(15.40
)
278(65.8
8)
66(15.64
)
2.94(0.6
6)
4(0.80) 27(5.42) 427(85.7
4)
40(8.03
)
3.01(0.41)

232
Variables Base line End line
Strongly
disagree
N (%)
Disagree
N (%)
Agree
N (%)
Strongly
agree N
(%)
Mean
(SD)
Strongly
disagree
N (%)
Disagree
N (%)
Agree
N (%)
Strongl
y agree
N (%)
Mean
(SD)
environment in
this facility
Is there access to
clean water in this
health care
facility?
57(13.51) 55(13.03
)
289(68.4
8)
21(4.98) 2.65(0.7
7)
59(11.85
)
71(14.26
)
339(68.0
7)
29(5.82
)
2.68(0.76)
Do the cleanliness
of the toilets in
the health facility
maintained?
12(2.84) 58(13.74
)
329(77.9
6)
23(5.45) 2.86(0.5
4)
29(5.82) 98(19.68
)
333(66.8
7)
38(7.63
)
2.76(0.67)
Are there
facilities for
people with
28(6.64) 84(19.91
)
283(67.0
6)
27(6.40) 2.73(0.6
8)
32(6.43) 152(30.5
2)
292(58.6
3)
22(4.42
)
2.61(0.67)

233
Variables Base line End line
Strongly
disagree
N (%)
Disagree
N (%)
Agree
N (%)
Strongly
agree N
(%)
Mean
(SD)
Strongly
disagree
N (%)
Disagree
N (%)
Agree
N (%)
Strongl
y agree
N (%)
Mean
(SD)
disabilities in the
health care?
Is the smell in this
health care
facility pleasant?
2(0.47) 34(8.06) 361(85.5
5)
25(5.92) 2.97(0.4
0)
2(0.40) 37(7.43) 424(85.1
4)
35(7.03
)
2.99(0.40)
Amenities 0(0.00) 105(24.8
8)
316(74.8
8)
1(0.24) 2.75(0.4
4)
1(0.20) 91(18.27
)
392(78.7
1)
14(2.81
)
2.84(0.44)
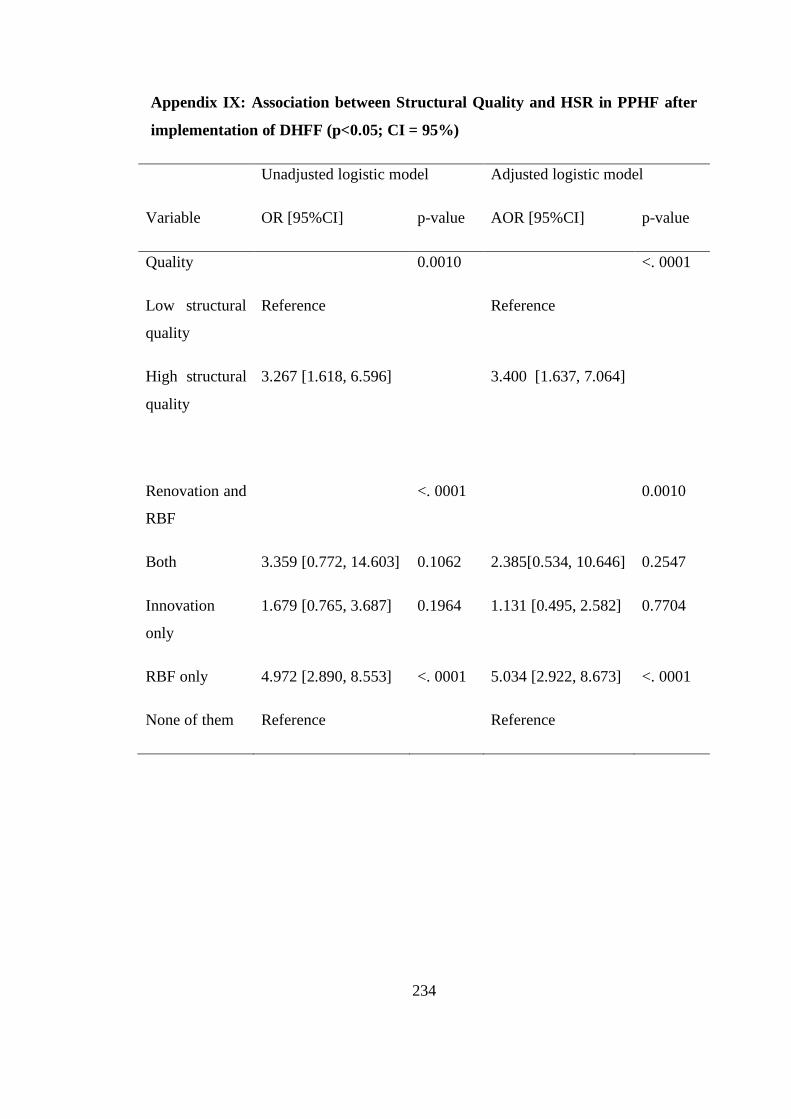
234
Appendix IX: Association between Structural Quality and HSR in PPHF after
implementation of DHFF (p<0.05; CI = 95%)
Unadjusted logistic model Adjusted logistic model
Variable OR [95%CI] p-value AOR [95%CI] p-value
Quality 0.0010 <. 0001
Low structural
quality
Reference Reference
High structural
quality
3.267 [1.618, 6.596] 3.400 [1.637, 7.064]
Renovation and
RBF
<. 0001 0.0010
Both 3.359 [0.772, 14.603] 0.1062 2.385[0.534, 10.646] 0.2547
Innovation
only
1.679 [0.765, 3.687] 0.1964 1.131 [0.495, 2.582] 0.7704
RBF only 4.972 [2.890, 8.553] <. 0001 5.034 [2.922, 8.673] <. 0001
None of them Reference Reference

235
Appendix X: Table of Random Numbers

236
Appendix XI: Coding Table for In-depth Interviews
Coding framework including progression from Codes and Categories to Themes for
Health Service Providers responsiveness towards DHFF initiative implementation.
Themes Sub themes Categories Codes
Health Care
Providers’
experience toward
DHFF
implementation
Training 1. Training on
planning and
budgeting
• Cascade training,
• Proper documentation and book
keeping,
• Budget and planning
preparation and execution.
• Use of assistant accountants,
• Use of funds as per plan and
budget allocated,
• Preparation of financial reports
by using,
• Monitoring proper use of funds,
• Adherence to implementation
guidelines and financial
memorandums.
2. Training on use
of FFARS
• FFARS for reporting financial
expenditures and also fund receipt
notification,
• Procurement of health commodities
and supplies guidelines,

237
• Timely disbursement,
• Real time financial reports
1. Knowledge
(content) on
DHFF
initiative
Level of
understanding about
DHFF concepts
• Decision making space,
• Disbursement modality,
• Autonomy,
• Quality improvement of health
services and financial reports
1. Coordination of
DHFF initiative
activities
Implementation
arrangement of
DHFF activities
• Communication and
collaboration,
• Supportive supervision and
mentorship schedule/matrix,
• Timely submission of reports,
• Adherence to the budget and
planning cycle.
Oversight • Mentorship and Supportive
supervision,
• Council health service board
endorsement of budget.
• Consultations

238
Health Worker’s
Responsiveness
towards DHFF
implementation
Attitude Attitude towards
DHFF
implementation
• Positive perceptions,
• Feelings
• Readiness for change,
• Autonomy,
• Team work
Punctuality Timeliness in
addressing issues
• Complaint management system,
• Participatory approach,
• Local decision making and
solutions
1. Timely
availability of
health service
providers’
benefits, tools
and other
resources
• Disbursement according to
schedule,
• Motivation
• Guidelines
• Financial management tools
• Incentives,
• Procurement of commodities
and supplies,
• Lead time

239
Timeliness in fund
utilization and
service provision
• Local decision making,
• Budget and planning,
• Patient satisfaction,
• Increase number of patients,
• Increase workload
Enabling
environment for
DHFF
implementation
Capacity building for
DHFF implementers
Capacity of health
service providers on
management of
DHFF
• Management,
• Leadership and stewardship
skills,
• Knowledge,
• Tools
Adherence to the
Public Financial
management protocols
Timeliness in
disbursement of
funds using available
institutions
• Adherence to schedules,
• Financial auditing,
• Financial management
Motivation of DHFF
implementers
Improvement of
working environment
• Renovation of Health Facility
and Offices,
• Allowances,

240
Appendix XII: Coding table for Focus Group Discussion
Coding Table including progression from Codes and Categories to Themes for
Governance and Accountability of DHFF initiative.
Themes Sub –themes Categories Codes
Governance
Funds
Management
Adherence to
financial protocols
• Proper documentation of
financial statements,
• Book keeping,
• Endorsement of transactions
by all responsible people,
• Use of funds as per plan and
budget allocated,
• Preparation of financial
reports by using,
• Monitoring proper use of
funds,
• Timely receipts of funds.
Capacity of
Health Facility
Governing
Committee
(HFGC) Members
Capabilities of
HFGCs
• Appropriateness,
• Feasibility,
• Correctness on budget
interpretation and supervise its
implementation,
• Participation in facility meetings
and budgeting,

241
Themes Sub –themes Categories Codes
• Training on DHFF initiative,
• Magnitude of the health problem
at the community level.
Planning and
Budgeting
Comprehensive
primary health
facilities
• Budget and planning
preparation and execution.
• Use of assistant accountants,
• Use of funds as per plan and
budget allocated,
• Preparation of financial reports
by using
Accountability Transparency and
Community
involvement
Openness • Participatory decision
making,
• Effective communication and
collaboration,
• Posting reports in health
facility billboards,
• Frequent of assessment,
• Matching resources to
patient’s need,
• Organization and timely care,
• Giving progress reports at the
village general assembly and

242
Themes Sub –themes Categories Codes
other meetings.
Financial and
performance
report review and
approval
Compliance to
reporting
• Authorization of use of funds,
• Use of funds as per financial
memorandums,
• Accountability and compliance
reports
Oversight Supportive
supervision
• Supportive supervision,
• Mentorship,
• Council health service board,
• Endorsement of budget.
Supportive
Supervision and
mentorship
Regular
monitoring of
primary health
facilities,
Consistency
provision of
guidance
(mentorship)
Monitoring • Adherence to DHFF
protocol,
• Proper financial management
arrangement,
• Schedule of support,
• Frequency of visits,
• Regular visits,
• Enforcement of directives
and guidance to DHFF
243
Themes Sub –themes Categories Codes
implementation,
• Adherence to guidelines.
6 Clarification/
interpretatio
n of policies,
strategies
and
operational
guidelines
Policy interpretation • Policies and strategies
implementation assessment,
• Guidelines availability,
• Standard Operating
Procedures (SOPs),
• Enforcement of public
financial regulations and
laws,
• Compliance to circulars and
directives
244
Appendix XIII: Objective number One: Health System Responsiveness as
perceived by the end users of PPHF
Serial No. [__|__|__|__]
Namba ya kumbukumbu
Name of the Region: _____________________________________
Jina la Mkoa;
Name of the District Council: ______________________________
Jina la Wilaya:
Ward _____________________________Village/Street _______________
Kata ______________________________ Kijiji/ Mtaa________________
Name of the Health Facility: _______________________________
Jina la kituo:
Type of Health Facility: 01= Dispensary [ ] 02= Health center [ ]
Aina ya kituo: 01 = Zahanati [ ] 02 = Kituo cha afya [ ]
Please put the appropriate number of a response in the given box
Tafadhali weka namba ya jibu sahihi kwenye chumba ulichopewa

245
SN
Na.
Questions
Maswali
Responses
Majibu
Code Code
SECTION A: DEMOGRAPHIC INFORMATION
KIPENGELE A: TAARIFA ZA AWALI ZA MDODOSWAJI.
1. (a)Sex
Jinsia
1.Male
Mwanaume
2.Female
Mwanamke
1
0
[ ]
(b)How old are you?
Una umri gani?
1. ----------------
2. Marital status
Hali ya ndoa
1.Married
Nina ndoa
2.Cohabiting
Tunaishi pamoja
3.Single
Sina ndoa
4.Divorced/Separated
Mtalaka
5.Widow/widowed
Mjane / Mgane
01
02
03
04
05
[ ]
246
3. Highest level of
education
Kiwango cha elimu
1.Primary
Msingi
2.Secondary
Sekondari
3.Certificate
Astashahada
4.Diploma
Stashahada
5.Advanced diploma
Astashahada ya juu
6.University degree
Shahada
7.Masters
Shahada ya uzamili
8. Others
Nyingine
1
2
3
4
5
6
7
8
[ ]
4. What is the size of your
family?
Familia yako inawatu
wangapi?
--------------

247
5. What is the number of
visits you have had to
this facility before?
Umewahi kupata
huduma mara ngapi
katika kituo hiki?
----------------
[ ]
6. How much
distance would
you have to
undertake in
order to reach
health care?
Unatembea umbali gani
kuifikia huduma ya
afya?
----------------------

248
Prompt to Attention (7)
Umakini
Very
often (3)
Mara zote
Often (2)
Mara kwa
mara
Slightly
Often (1)
Mara
chache
Never
happens
(0)
Haijawa
hi
kutokea
1. How often did the health
service providers listen to
what you said with full
attention during provision?
Nimara ngapi watoa huduma wa
afya wamekusikiliza kwa
umakini wakati wa kupata
huduma?
2. How often your statements
were deeply understood by
the health service providers?
Nimara ngapi maeezo yako
yameeleweka vyema kwa watoa
huduma wa afya wa kituo hiki?
3. How often did health service
providers spend enough time
in asking you questions?
Mara ngapi mtoa huduma
ametumia muda wa kutosha
kukuuliza maswali juu ya ugojwa
wako?
4. How often the health service

249
providers were accurately and
actively in following up your
treatment process?
Ni kwa kiwango gani watoa
huduma wa afya wamekuwa
makini katika kufuatilia matibabu
yako ndani ya kituo cha kutoa
huduma?
5. The patients with similar
needs are treated equally in
the health units?
Wagonjwa wenye mahitaji sawa
huhudumiwa kwa usawa katika
idara za kituo cha huduma za
afya?
6. Patients with unequal needs
are treated equally in the
health units?
Wagonjwa wenye mahitaji tofauti
huhudumiwa kwa usawa katika
kituo cha huduma za afya?
7. The health facility has always
met my expectations
Kituo hiki cha afya hutimiza
mahitaji yangu kila wakati
Respect to Dignity (3)
Utu
250
1. How often did the health service
providers show courtesy and affection
towards you during service provision?
Ni mara ngapi watoa huduma wa
afya wameonyesha heshima na
upendo kwako wakati wa kupata
huduma?
2. How often did the health care workers
paid attention specifically into your
needs and characteristics?
Ni mara ngapi mtoa huduma
amekuwa makini hasa kwa
mahitaji yako na hali yako?
3. How often is respect shown for the
patient’s desire for privacy during
treatment and examination?
Ni mara ngapi heshima hutolewa kwa
wateja wanapokuwa wanapata huduma
za uchunguzi na matibabu?
Clear Communication (7)
Mawasiliano bayana
1. How often did health care workers
explain things in a way you could
understand?
Ni mara ngapi watoa huduma wameeleza
vyema mambo yanayokuhusu katika njia
unayoielewa?

251
2. How often health care workers explain
things and issues related to your health in
detail for you?
Ni kwa kiwango gani watoa huduma wa
afya hueleza hali yako ya afya kiundani
kwako?
3. How would you rate your experience
about how well you were treated as
human during interaction with the
following service providers?
Toa kiwango cha ubora wa huduma kwa
mujibu wa uzoefu wako wa kupata
huduma katika kituo hiki cha afya
1. Nurses / Muuguzi
2. Laboratory staff/ Mtaalamu wa
maabara
3. Medical doctors/clinicians/
Madaktari na matabibu
4. Security staff / Walinzi
5. How would you rate overall
quality of interaction at this
health facility?
Toa mtazamo wako wa jumla wa
jinsi ulivyo pata huduma katika
kituo hiki

252
Autonomy (3)
Uhuru wa kufanya mahamuzi
No
problem
(3)
Hakuna
tatizo
Average
(2)
Wastani
Big (1)
Kubwa
Very big
(0)
Kubwa
sana
1. How big a problem if any was it to get
an appointment with the health care
worker of your choice?
Ni kwa kiwango gani ulipata
tatizo (kama lipo) la kupata fursa
ya kukutana na mtuo huduma wa
afya uliyemhitaji?
2. How big a problem if any was it to use
other health facility other than the one
you usually went to?
Nikwa kiwango gani ulipata
tatizo (kama lipo) kutumia kituo
kingine cha huduma ya afya zaidi
ya kile ambacho huenda kila
wakati?
3. I feel that my physicians have
provided me choices and options
Nahisi daktari amenipatia chaguo la
huduma
Access to Care (4)
Upatikanaji wa huduma
Waited
for long
time
(above
Average (up
to 30min)
Waited for
few
minutes
Serviced
instantly

253
30min)
(1)
Nilisubiri
muda
mrefu
(zaidi ya
dakika 30)
(2)
Wastani
(mpaka
dakika 30)
(3)
Kusubiri
kwa
dakika
chache
(4)
Nilipata
huduma
mara
moja
1. How long did you have to wait to get
medical consultation from service
provider?
Ulitumia muda gani kusubiri
huduma ya afya?
2. How long did you have to stay in the
waiting room?
Ulisubiri muda gani katika
chumba cha kusibiri kumuona
mtoa huduma wa afya?
3. How long did you have to stay at the
pharmacy or dispensing area?
Ulisubiri kwa muda gani katika eneo la
kuchukua dawa la kituo?
4. How long did you have to stay waiting
for laboratory services and results?
Ulisubiri muda gani kupata huduma na
majibu ya maabara?
Confidentiality (3)

254
Usiri
1. How often interviews remained
confidential?
Kwa kiwango gani mahojiano
yamekuwa ya usiri?
2. Health care workers keep your
personal information and records
confidential?
Watoa huduma ya afya huweka
taarifa zako binafsi kwa siri?
3. Is the confidentiality maintained in
this health facility?
Usiri unazingatiwa katika kituo hiki?
Basic Amenities
Mahitaji muhimu
Strongly
agree
(4)
Nakubali
kabisa
Agree
(3)
Nakubali
Disagree
(2)
Sikubali
Strongly
disagree
(1)
Sikubali
kabisa
1.I agree that this facility have enough
buildings for service delivery
Nakubali kuwa kituo kina
majengo ya kutosha ya kutoa
huduma
2.I agree that this facility have enough
staffs to service patients
Nakubali kuwa hiki kituo kina

255
watoa huduma wa kutosha kutoa
huduma kwa wagonjwa
3.I agree with the quality of direction
aids of this facility
Nakubaliana na ubora wa
vielelezo na miongozo iliyo
kwenye kituo hiki.
4.I agree with the cleanliness of this
surroundings
Nakubaliana na hali ya usafi wa
hiki kituo
5.I agree with the waiting environment of
this facility (waiting seats)
Nakubaliana na mazingira ya
kusubiria huduma ya kituo hiki
(ikiwa ni pamoja na viti)
6. Are you convenient with the safety of
service delivery environment in this
facility?
Je unaridhishwa na mazingira ya
usalama ya utoaji huduma wa
hiki kituo?
6. Access to clean water at health
care units
Upatikanaji wa maji katika vitengo vyote
vya kituo cha huduma ya afya
7. Cleanness of the toilets in the

256
health care units
Usafi wa vyoo unazingatiwa kila wakati
katika kituo cha huduma za afya.
9.Facilities for people with disabilities in
the health care units
Kituo kina mazingira ya watu wenye
ulemavu katika vitengo vyote
10.Are the bed sheet of this facility clean
Mashuka ya vitanda katika kituo ni
masafi
11. The smell in the health care units is
not disquieting
Kituo cha huduma za afya hakina harufu
mbaya

257
Appendix XIV: Objective number two: Structural Quality of MHS in the PPHF
Lengo Namba 1 (tathmini ya matokeo): Viashiria vya muundo wa ubora wa huduma za afya ya uzazi.
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
1 PRIVACY
FARAGHA
Privacy in Individual treatment /service
delivery rooms have full privacy during
service provision
Faragha wakati wa kumtibu mgonjwa/
vyumba vya kutolea huduma vina
faragha ya kutosha
• All service delivery rooms with
doors that close
Vyumba vyote vya kutoa huduma vina
milango inayofunga/yenye vitasa
• All service delivery rooms with
Privacy Assured in
rooms and all
criteria met = 4
Faragha niya
uhakika katika
vyumba vyote na
vigezo vyote
vimezingatiwa =4
Service room with
4
258
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
screen to partition the
examination area/bed
Vyumba vyoote vya kutolea huduma
vina pazia la kuzuia eneo la kutolea
huduma/kitanda
• Windows with curtains or painted
or with frosted glass
Madirisha yenye mapazia au yenye rangi
au kioo usichoweza ona ndani
• Divider (screen/curtain) if the
service delivery room is shared.
Kitenganishi (kioo/pazia) kama chumba
cha huduma kinatumiwa na mtu zaidi ya
all criteria =
Number of rooms
fulfilling all criteria
X 4/Number of
available rooms
Privacy not
assured=0
Vyumba vya
huduma vyenye
vigezo/sifa zote =
Idadi ya vyumba
vinavyo kidhi
vigezo vyote X
4/vyumba vilivyopo.

259
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
mmoja. Faragha
haijasibitishwa =0
2 HYGIENE AND
SANITATION
AFYA NA
USAFI WA
MAZINGIRA
2a) Presence of clean and functioning
disinfected toilet/s for patients, staffs and
physically challenged people:
Upatikanaji wa vyoo safi na salama kwa
wagonjwa, watumishi na walemavu wa
viungo;
1) Functioning toilet [VIP latrine which
is not full OR a flushing toilet with
working or improvised flushing system],
Choo kinachofanya kazi (choo bora cha
shimo ambacho hakijajaa au choo cha
maji ambacho mfumo wa kusafisha choo
All element
available for all
toilets = 4
Vipengele vyote
katika vyo
vinapatikana = 4
Element missing for
one or all toilets =
Deduct 1 Point per
missing element
Kipengele kimoja
kikosekana kwa vyo

260
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
unafanya kazi)
2) Toilets clean inside and out with no
stagnant water and no foul smells],
Choo safi nje na ndani ambacho hakina
maji yaliyotwama wala harufu mbaya.
3) Presence of toilet paper or water. And
in case of flushing toilet, a dust bin.
Upatikanaji wa karatasi laini au maji. Na
kama choo cha mfumo wa maji basi
kuwa na chombo cha taka.
4) Hand-washing facilities just outside
the toilet or with basin inside toilet [soap
and source of water]
vyote au kimoja =
toa alama 1 kwa kila
kipengele
kilichokosekana
7
261
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
Chombo cha kunawia mikono nje ya
choo au sinki la ndani (sabuni na maji)
2b. No organic waste, used syringes,
needles, used bandages or dangerous
products on the ground of the facility
that are easily accessible to the public
(including waste pit area) and grounds
surrounding the HF entirely cleared of
weeds and stagnant water drained
Kusiwe na taka ngumu, mabomba ya
sindanoyaliyotumika au vitu vya hatari
kwenye kumbi, vyumba au mahali
pengine kokote kwenye maeneo ambayo
hufikiwa na watu (ikiwemo sehemu ya
kutupa taka) na eneo la kuzunguka kituo
Yes = 1
Ndio = 1
If present = 0/1
Kama vipo =0/1
262
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
linatakiwa liwe safi na halina maji yaliyo
tuwama.
2c. Presence of: Functioning incinerator,
fenced in and ash pit.
If no incinerator, it must have waste pit
with evidence of use by burn and bury
but also fenced in.
Presence of placenta pit with slab and
cover Kuwapo kwa tanuru la kuchomea
taka linalofanya kazi na lililozungushiwa
uzio na lina sehemu ya kutupa majivu.
Endapo kituo hakina tanuru la kuchomea
taka ni lazima kituo kiwe na shimo la
kuchomea taka na kuzifukia
Functioning
incinerator=2
Tanuru linalofanya
kazi au shimo la
taka
lililozungushiwa
uzio = 1
If it is Placenta pit in
use meeting all
criteria = 1
Kama kunashimo la
kutupa kondo na

263
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
lililozungushiwa uzio.
Kuwepo na shimo la kutupa kondo la
nyuma lenye mfuniko.
lina vipengele vyote
= 1
If not available =0
Kama hakuna = 0
3 LABOUR WARD
WODI YA
KUJIFUNGULIA
Delivery room with essential equipment
and supplies for quality service delivery:
Chumba cha kujifungufungulia chenye
vifaa tiba vyote muhimu kwa utoaji wa
huduma bora ya afya.
A. Delivery bed functional, Clean,
Adjustable, with a footstool,
Kitanda cha kujifungulia kinafanya kazi,
kisafi, kurekebishika na chenye ngazi ya
All delivery bed
meeting all criteria =
1
Vitanda vyote vya
kujifungulia
vimekidhi vigezo
vyote = 1
If not
264
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
kupandia na kisicho na kutu. all=1/#beds*bed
meeting criteria
Kama sio vyote =
1/idadi ya
vitanda*vitanda
vyenye vigezo vyote
If none meets
criteria=0
Kama hakuna
kinacho kidhi vigezo
=0
14
B.1) One Functional gouse neck lamp /
light source, 2) one Functional newborn
weighing scale, 3) One Drum with
All elements
Available element =

265
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
Sterile gauze (with date and closed) and,
4) One drum with cotton wool (with date
and closed), 5) One Suction machine, 6)
Resuscitation kit (Ambu-bag, tubes), 7)
One Mackintosh (plastic mattress cover
or disposable) for each delivery bed
1)Taa 1 maalumu / tochi 1 inayofanya
kazi (chanzo cha mwanga)
2)Mzani 1 wa kumpima motto mchanga
unaofanya kazi 3) Dramu moja lenye
vifaa tasikama vile shashi 4)Dramu 1
lenye pamba
5) Mashine moja ya kutolea mchojozo
kwa mototo 6)Kifaa cha kumpa hewa
7
Missing element =
Deduct 1 point per
missing element
Uwepo wa
vipengele vyote =7
Kukosekana kwa
kipengele kimoja toa
maksi 1

266
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
motto 7)Mpira 1 wa kufunika kitanda
kwenye kitanda cha kujifungulia.
B) At least 2 sterilized delivery trays (1
kidney dish or gallipot, 2 scissors, 2
clamp forceps, 1 stitching forceps, 1
dissecting forceps, 1 sponge holding
forceps per tray, 2 needles with suture, 1
umbilical cord clamp)
Angalau trei 2 za kuzalishia ambazo
zimetasiswa kila trei ndani liwe na
(kibeseni kimoja chenye umbo la
figo/kikombe, mikasi 2, foseps 2 za
kubania kitovu, foseps moja ya
kushikilia nyuzi, foseps moja ya
kushikilia shashi/pamba na sindano 2 za
All elements
Available element
=3
If one is not
available = 0 Vigezo
vyote vimetimia = 3
Kama hata kimoja
hakuna =0/3
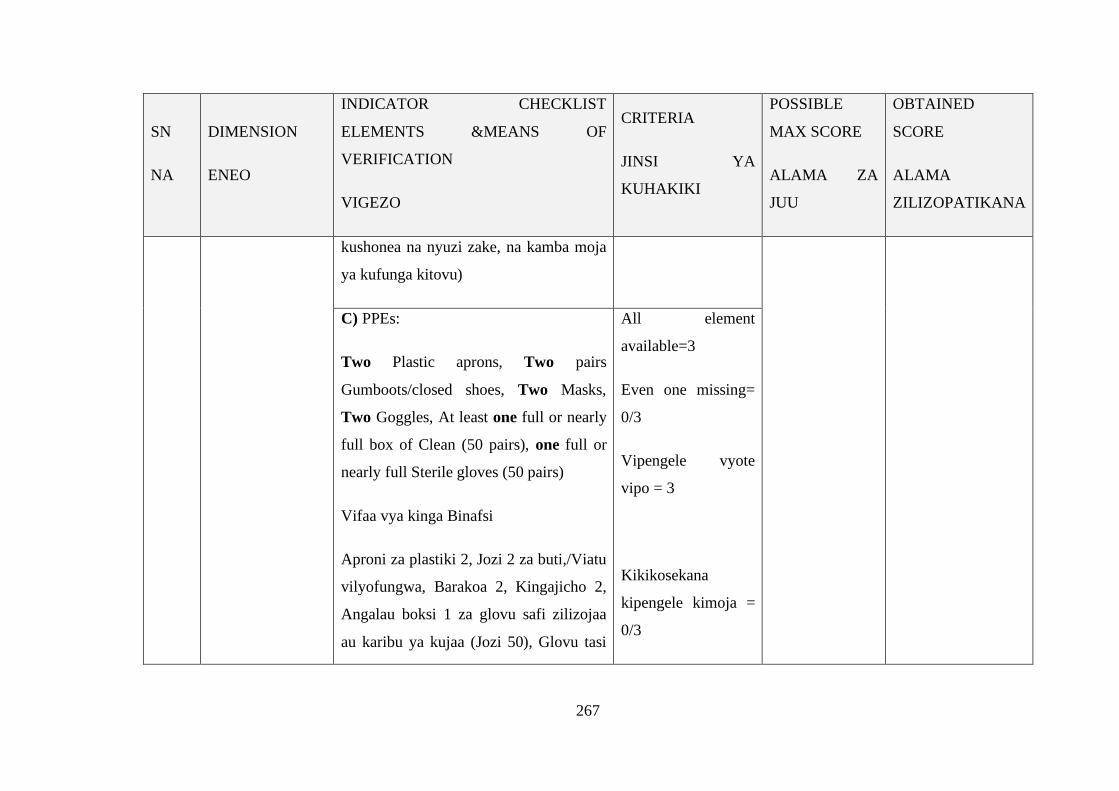
267
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
kushonea na nyuzi zake, na kamba moja
ya kufunga kitovu)
C) PPEs:
Two Plastic aprons, Two pairs
Gumboots/closed shoes, Two Masks,
Two Goggles, At least one full or nearly
full box of Clean (50 pairs), one full or
nearly full Sterile gloves (50 pairs)
Vifaa vya kinga Binafsi
Aproni za plastiki 2, Jozi 2 za buti,/Viatu
vilyofungwa, Barakoa 2, Kingajicho 2,
Angalau boksi 1 za glovu safi zilizojaa
au karibu ya kujaa (Jozi 50), Glovu tasi
All element
available=3
Even one missing=
0/3
Vipengele vyote
vipo = 3
Kikikosekana
kipengele kimoja =
0/3
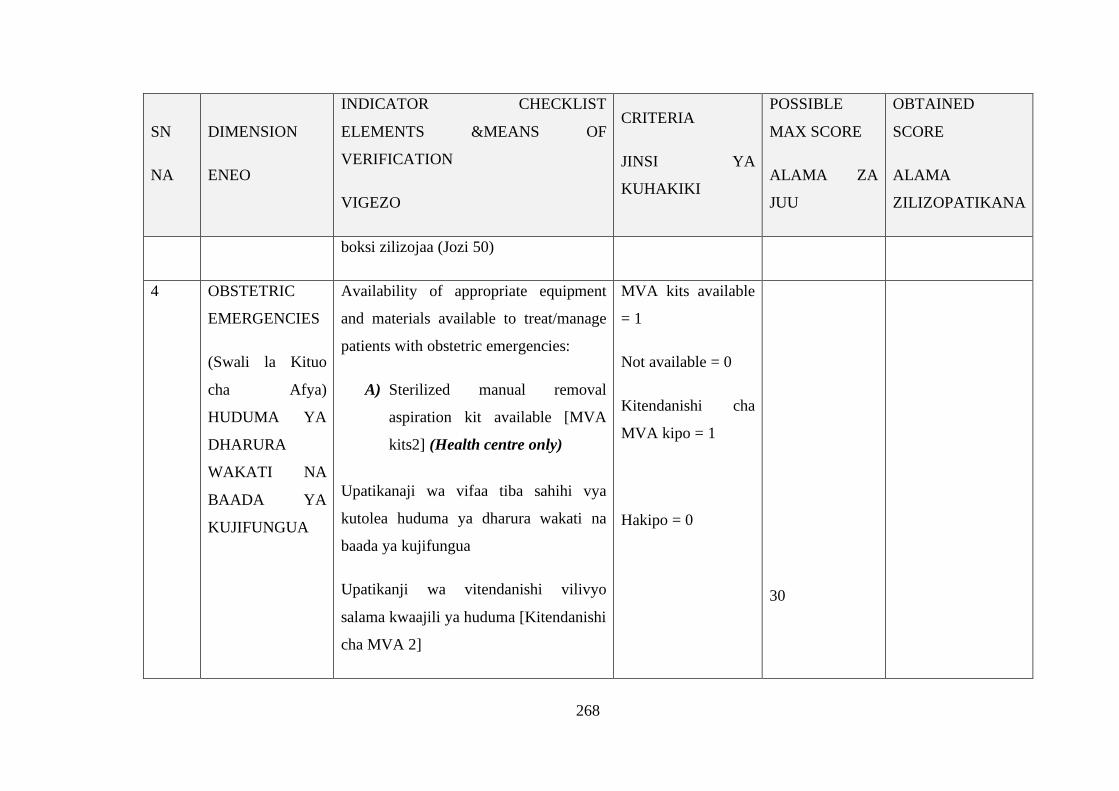
268
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
boksi zilizojaa (Jozi 50)
4 OBSTETRIC
EMERGENCIES
(Swali la Kituo
cha Afya)
HUDUMA YA
DHARURA
WAKATI NA
BAADA YA
KUJIFUNGUA
Availability of appropriate equipment
and materials available to treat/manage
patients with obstetric emergencies:
A) Sterilized manual removal
aspiration kit available [MVA
kits2] (Health centre only)
Upatikanaji wa vifaa tiba sahihi vya
kutolea huduma ya dharura wakati na
baada ya kujifungua
Upatikanji wa vitendanishi vilivyo
salama kwaajili ya huduma [Kitendanishi
cha MVA 2]
MVA kits available
= 1
Not available = 0
Kitendanishi cha
MVA kipo = 1
Hakipo = 0
30

269
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
B) Blood transfusion facilities
available [Blood bank with 5
units different groups preferably
O-group of blood available]
(health centre only)
Upatikanaji wa huduma ya kuongezewa
damu [benki ya damu yenye uniti 5 za
aina tofauti za makundi ya damu
ikiwemo aina ya kundi O]
All O-groups
available=5
O groups
missing=0/5
All other groups
available=5
All other groups
missing=0/5
Uwepo wa uniti zote
5 kuwa aina ya
kundi O/ makundi
yote (A.B,AB, & O)
= 5

270
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
Kuwepo kwa
makundi yote ya
damu bila kundi “O”
= 0
C) Presence of: -
1) Vacuum extractor, (Health centre
only)
2) Gun let gloves for manual removal of
placenta
1)Uwepo wa chombo cha kuvutia motto,
2)Glovu ndefu za kutolea kondo la
nyuma
2 elements available
= 4
One missing =
deduct 2
Uwepo wa
vipengele vyote 2=
4
Kipengele kimoja
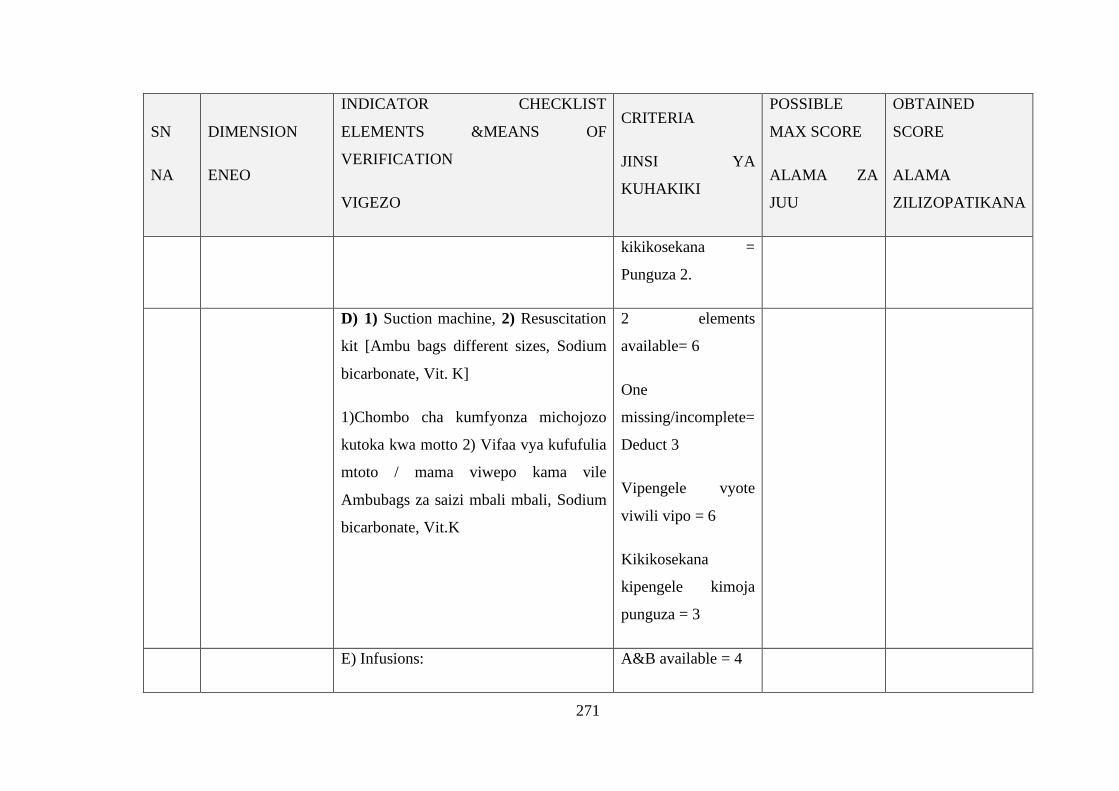
271
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
kikikosekana =
Punguza 2.
D) 1) Suction machine, 2) Resuscitation
kit [Ambu bags different sizes, Sodium
bicarbonate, Vit. K]
1)Chombo cha kumfyonza michojozo
kutoka kwa motto 2) Vifaa vya kufufulia
mtoto / mama viwepo kama vile
Ambubags za saizi mbali mbali, Sodium
bicarbonate, Vit.K
2 elements
available= 6
One
missing/incomplete=
Deduct 3
Vipengele vyote
viwili vipo = 6
Kikikosekana
kipengele kimoja
punguza = 3
E) Infusions: A&B available = 4

272
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
1) Three bottles of Ringer lactate, three
bottles of normal saline 1000mls, 2) Sets
of canula, Gauge 14 & 18
Kuwepo kwa maji ya dripu;
A)Chupa 3 za Ringer lactate, Chupa 3 za
Normal saline 1000mls,
B)Seti ya Kanula ya saizi 14 & 18
A/B missing =
Deduct 2
A&B vikiwepo = 4
A/B ikikosekana =
punguza 2.
Infusions (cont.):
3) Giving sets 3, 4) Syringes 2ml, 5ml,
10ml [5,5,5]
Dripu (endelea)
C)Seti 3 za kuweka dripu, D) Mabomba
C & D available = 2
C/D missing /
incomplete = Deduct
1
C&D vikiwepo = 4
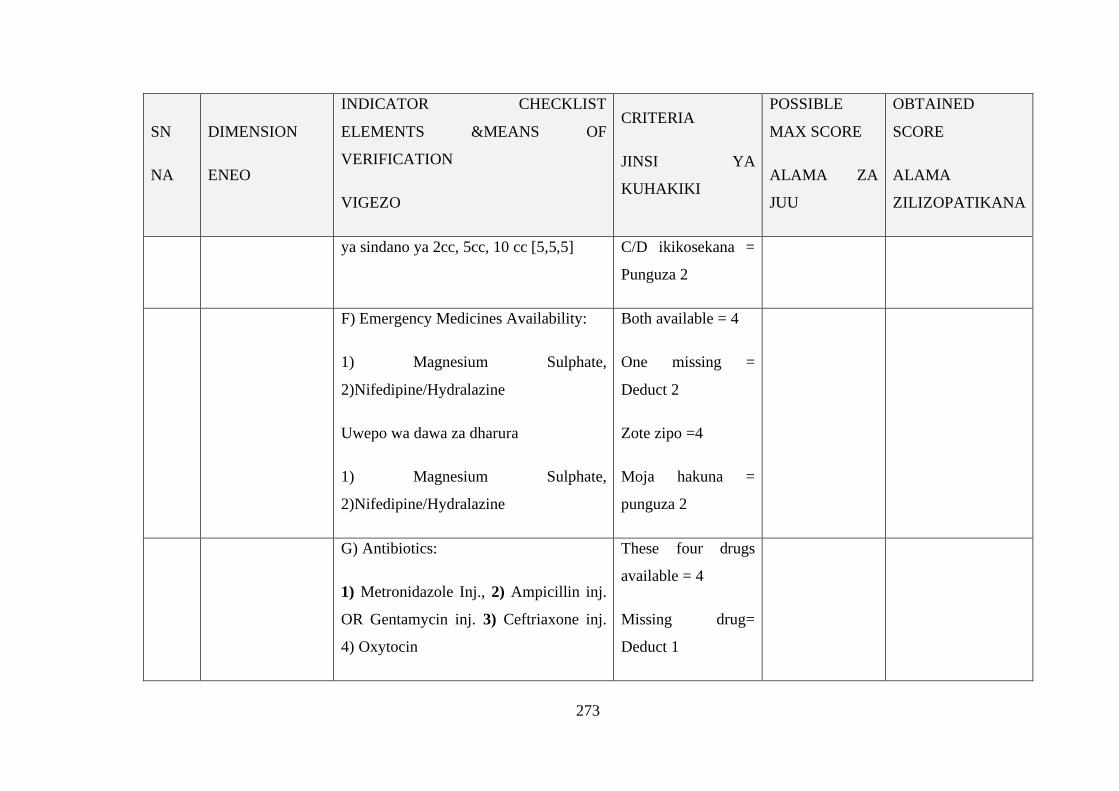
273
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
ya sindano ya 2cc, 5cc, 10 cc [5,5,5] C/D ikikosekana =
Punguza 2
F) Emergency Medicines Availability:
1) Magnesium Sulphate,
2)Nifedipine/Hydralazine
Uwepo wa dawa za dharura
1) Magnesium Sulphate,
2)Nifedipine/Hydralazine
Both available = 4
One missing =
Deduct 2
Zote zipo =4
Moja hakuna =
punguza 2
G) Antibiotics:
1) Metronidazole Inj., 2) Ampicillin inj.
OR Gentamycin inj. 3) Ceftriaxone inj.
4) Oxytocin
These four drugs
available = 4
Missing drug=
Deduct 1
274
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
Viua vijisumu: (rejea sampuli 4 za dawa
tajwa juu)
Dawa 4 zikiwepo =
4
Ikikosekana dawa =
punguza 1
H) Sedatives:
(E.g. diazepam)
“Sedatives” Mfano : Diazepam
Sedative Available =
1
Not available = 0/1
Ikiwepo = 1
Hakuna = 0/1

275
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
5 WASTE
MANAGEMENT
UTUPAJI
SAHIHI WA
TAKA
Waste management done as per standard
guidelines in clinical procedures rooms:
Availability of:
4.1)Labor ward and dressing room:
Three buckets, each bucket clearly
labeled with today’s date, 1 bucket with
chlorine 0.5%, 1 with soapy water and 1
with clean water;
Utupaji taka unafanyika kwa kuzingatia
miongozo ya vyumba vya tiba:
Uwepo wa:
Kwenye wodi ya kujifungulia na chumba
cha upasuaji: Ndoo tatu kila ndoo
3 buckets available
= 1
Not available or not
meeting criteria =
0/1
Ndoo 3 zipo = 1
Hazipo au
hazijakidhi vigezo
=0/1
6
276
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
iwekwe alama ya tarehe ya leo, ndoo
moja klorini 0.5%, 1 maji ya sabuni na 1
maji safi.
2)Inpatient wards (Including labor ward,
laboratory and immunization/Injection
room):
At least 1 safety box with sharps not
exceeding ¾ full, and no sharps sitting
on top of the box
Wodi ya kulaza wagonjwa (ikiwemo
wodi ya wazazi, maabara na sehemu ya
Available and
criteria met=2
If partial= 0/2
Uwepo wa vigezo
vyote = 2
Kama

277
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
kutolea Chanjo/ sindano): Angalau boksi
salama moja la vifaa vyenye ncha kali
ambalo linatakiwa lisijae kufikia ¾,
kusiwe na taka zinazoonekana nje ya
kasha.
havijakamilika = 0/2
3) In labor ward, laboratory and minor
theatre:
Proper waste segregation using Red,
Yellow and Black/Blue bins with color
coded bin liners – labeled bin liners ok in
lieu of colored
Kwenye wodi ya kujifungulia, maabara
Waste segregation
meeting criteria and
in all relevant
rooms= 3
If partial= 0/3
Utenganishaji wa

278
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
ma chumba cha upasuaji
Utenganishaji wa taka ufanyike kwa
kutumia vifaa vyenye rangi nyekundu,
njano na nyeusi/ bluu navyo viwe na
mifuko laini yenye rangi nyekundu,
njano na bluu kulingana na vifaa vyake.
Taka unafuata
vigezo katika
vyumba vyote = 3
Kama haijakamilika
= 0/3
6 STERILIZATION
UTASISHAJI
WA VIFAA
Availability of proper sterilization of
instruments:
1. Existence of proper means / methods
of sterilizing instruments:
Steam sterilization (Autoclave) or Dry
heat sterilization or Chemical
Each element
fulfilling the criteria
= 1
Criteria not met =
3

279
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
sterilization
2. SOPs for sterilization displayed on the
wall by the equipment
3. Each pack has an indicator for control
of sterility (litmus or date of
sterilization)
Upatikanaji wa mbinu/njia zinazofaa za
kutasisha vifaa:
• Kutasisha kwa kutumia mvuke (
Autoclave) au Joto kali au
kemikali
• Hatua za utasishaji
zilizobandikwa ukutani kwa vifaa
0/1
Kila kipengele
kinachokidhi
vigezo=1
Vigezo
havijafikiwa=0/1

280
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
maalumu
• Kila kifurushi iwe na kifaa
kinachoonyesha namna ya
kutambua kuwa vifaa ni tasi
(tarehe)
7 MATERNAL
DEATH AUDITS
UHAKIKI WA
VIFO VYA
UZAZI
Proportion of maternal deaths in HFs that
are completely and appropriately audited
and action plan in place:
A) Select one audited case and check if
they were; 1) Completely, 2) Correctly
filled and 3) Action plan in place.
B) Chagua bila mpangilio vifo 3
vilivyotokea na angalia kama 1)Fomu
zimejazwa kote 2)Fomu zimejazwa kwa
A case with 3
criteria = 10
Even one criteria
missing = 0/10
Kifo kinachokidhi
vipengele vyote 3 =
10
Kifo kisichokidhi

281
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
usahihi 3) Mpango mkakati upo. hata kipengele 1 =
0/10
B) In cases where the facility has no
maternal deaths, staff should hold
meetings and discuss strategies should be
in place to ensure that the community do
not experience deaths in the next quarter
Assess if the strategies are in place with
emphasis on
• ANC clinic
If meeting minutes
and well-structured
with 4 strategies
available = 15
Even if one Strategy
not discussed = 0
/15
Uwepo wa
muhtasari wa kikao
unaogusa mikakati

282
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
• Labour and delivery
• Post-natal care
• Patient/Community factors
C) Katika vituo ambavyo hakuna vifo,
watumishi wa vituo waitishe mikutano
na wananchi kujadili mikakati ya
kuondoa vifo vitokanavyo na uzazi ili
jamii isipate vifo katika robo inayofuata.
Hakiki kama mikakati iliyopo ina weka
msisitizo kwenye
• Kliniki ya mama na mtoto
yote 4 = 15
Kama mkakati hata
mmoja
haujajadiliwa =0/15

283
SN
NA
DIMENSION
ENEO
INDICATOR CHECKLIST
ELEMENTS &MEANS OF
VERIFICATION
VIGEZO
CRITERIA
JINSI YA
KUHAKIKI
POSSIBLE
MAX SCORE
ALAMA ZA
JUU
OBTAINED
SCORE
ALAMA
ZILIZOPATIKANA
• Huduma ya kujifungua
• Huduma baada ya kujifungua
• Mgonjwa/ sababu za kijamii

284
Appendix XV: Objective number three: Maternal Health Service Utilization in
the PPHF
Health Facility Name:
Jina la Kituo:
Assessed Quarter: ……… Year: ……….
Robo iliyotathminiwa: Mwaka ….
District:
Wilaya :
Region:
Mkoa:
Phone No:
Namba ya simu:
Fax:
Nukushi:
P.O Box:
S.L.P
Status: Public: Missionary: Private: Partner:
Hali : Serikali Misheni: Binafsi Mbia:
Catchment Population:
Idadi ya walengwa :
Number of beds:
Idadi ya vitanda:
Name of In-charge:
Jina la Mfawidhi:
Phone No:
Namba ya simu:
P.O. Box:
S.L.P:
E-mail:
Barua pepe:

285
NO Service
category
Indicator Type of
Indicator
Description/
definition of
indicator
Source of
data
1. Staffing Number of
staff in this
facility
Service
availability
Number of staffs in
that facility in a
given period of time
Health
Facility
profile.
2. Staffing
cadre
Number of
staff in this
facility per
cadre
Service
availability
Number of staffs in
that facility per
cadre in a given
period of time
Health
facility
profile
3. Outpatient Number of
new
outpatient
consultations
Service
Utilization
Number of new
cases or patients
(New diagnosis)
attending and
receiving outpatient
services during the
quarter
HMIS –
OPD
Register
Book 5
4. RCHS Number of
first antenatal
visits, with
gestation age
<12 weeks.
Service
Utilization
Number of women
starting ANC before
12 weeks of
gestation age at the
health facility.
HMIS –
ANC
Register
book 6
5. RCHS Number of
pregnant
women
attending
ANC at least
4 times
Service
Utilization
The number of
pregnant women
receiving fourth
ANC consultation
with a health
professional at the
HMIS –
Register
book 6

286
during
pregnancy.
facility or through
outreach by facility
staff at the
particular quarter.
6. Reproductive
and Child
Health
Number of
pregnant
women
receiving 2+
doses of
treatment
presumptive
treatment of
malaria
Service
availability
Number of pregnant
women receiving 2+
doses of SP during
pregnancy at that
particular quarter.
HMIS –
ANC
Register
book 6
7. Reproductive
and Child
Health
Number of
HIV infected
pregnant
women
receiving
ARVs for
PMTCT
Service
availability
Number of HIV
infected pregnant
women receiving
ARVs Prophylaxis
for PMTCT at
health in that
particular quarter
HMIS –
ANC
Register
book 6/
ART
Register
8. Reproductive
and Child
health
Number of
institutional
deliveries
Service
Utilization
Number of
deliveries
conducted at the
health facility and
attended by a health
professional (MD,
Midwife, RN, EN,
CO, CA) during the
period of that
HMIS
Book 12

287
quarter.
9. Reproductive
and Child
health
Number of
new users on
modern
Family
Planning
methods
Service
availability
Number of newly
accepting
contraception by
pills, injection,
implant, IUCD, at
the facility or
through outreach
and CBD within the
particular quarter.
HMIS-
Family
Planning
Register
book 8
10. Reproductive
and Child
health
Number of
pregnant
mothers
receiving
Mebendazole
for de-
worming
Service
availability
Number of pregnant
women given
mebendazole in the
evaluated quarter at
the health facility
during pregnancy
(20 weeks and
above)
ANC
Register
Book 6
11. Reproductive
and Child
health
Number of
postnatal
mothers
receiving
Post Natal
Care services
within 3-7
days after
delivery
Service
utilization
Number of women
receiving post natal
care at the facility
within seven day
after delivery
HMIS –
Post Natal
Register
Book 13
12. HIV/AIDS Number of
clients
Service
utilization
Number of
patients/clients
ART
Register

288
initiated by
heath care
provider to
counsel and
Test for HIV
(PITC)
attended at the
health facility and
initiated by the
health provider to
test for HIV

289
Appendix XVI: Objective Number Four: To explore Governance and
Accountability on DHHF in PPHFs
Focus Group Discussion Guide (FGD):
A: INTRODUCE MODERATORS, AND RECORD KEEPERS
Introduce yourself and the note takers, and send the Sign-In Sheet with a few quick
Demographic questions (age, gender, number of years in the HF) around to the group
while you are introducing the focus group.
Review the following:
Who we are and what we’re trying to do
What will be done with this information
Why we asked you to participate
B: INTRODUCE TOPIC OF RESEARCH
Thank you for taking the time to participate in a focus group. This discussion is part
of the evaluation of the implementation processes of the DHFF program in …….
region. We want to understand how you are accountable and Governance processes
of this program intervention.
You are a group of people 18 years and older working in this district. We would like
to hear about your experiences with DHFF program particularly on the way you
govern and your accountability towards DHFF.
Please keep in mind that there are no “right” or “wrong” answers to any of the
questions I will ask. The purpose is to stimulate conversation and hear the opinions
of everyone in the room. I hope you will be comfortable speaking honestly and
sharing your ideas with us.

290
C: SECURE INFORMED CONSENT
Please note that this session will be recorded (or [name] will be taking notes during
the focus group) to ensure we adequately capture your ideas during the conversation.
However, the comments from the focus group will remain confidential and your
name will not be attached to any comments you make.
Do you have any questions before we begin?
Finally, tell participants that if they don’t wish/no longer wish to participate in the
study for any reason, they may withdraw at any time. Encourage them to ask any
questions they have.
Do you agree to participate?
NOTE WHETHER RESPONDENTS AGREE TO INTERVIEW.
[ ] AGREES TO Participate
[ ] DO NOT AGREE TO participate
Please record the number of people who do not agree.
TO BE COMPLETED BY INTERVIEWER
I CERTIFY THAT I HAVE READ THE ABOVE CONSENT PROCEDURE TO
THE GROUP. SIGNED:
______________________________________________________
1. In your opinion, what is the main purpose of the DHFF program?
2. What changes has DHFF program brought to your facility? (Please probe the
following)
a. Medicines supply management
b. Equipment
c. Staffing
d. Staff (Motivation), relationship among yourselves
e. Renovation and Rehabilitation
291
f. Relationship with your supervisors
3. Does each and every one of you know the role and responsibilities in relation to
the DHFF program? How about others at your HF level? Explain
4. How DHFF program has enhanced Governance at the Health Facility Level?
Please probe: Participatory decision Making (Participation in HF planning and
Budgeting), How CHMT participate in monitoring of DHFF programs, how do
you participate in HF’s planning and budgeting
5. How do you collaborate with other actors outside your sector in the
Implementation of DHFF program? How is the collaboration with schools, civil
society organizations or other (outside the formal health sector)? Do you think
these collaborations emanated from DHFF program introduction?
6. Can you explain the policy or a strategy that guides implementation of DHFF
program in your working areas? Are the policy and strategies supportive to the
DHFF program implementation? Probe: What should be done?
7. How administrative structures are organized and contribute to the enforcement of
DHFF policy? How do you connect with your superiors? Probe: What should be
done?
8. How do you decide resources use at your health facility? How have you been
involved on the use of these funds? Probe: How do you respond to different
financial allocation formula? Probe (User fees (OOP), RBF, Health Basket Fund,
iCHF, NHIF and Receipt in Kind).
9. What have been your strategies to ensure there is effective implementation of
DHFF program? Probe: How do you deal with issues relating to the
implementation of DHFF?
10. How DHFF program has enhanced accountability at the Health Facility Level?
11. Are you able to make choices and decisions without any interference from other
bodies or structures? Probe: Have you received any capacity building to enable
you to execute DHFF tasks?
12. How is HFGC engaged in decision making at the Health Facility? Have you
received any capacity building to enable you to execute DHFF tasks?
292
13. How is Community involved to realize the achievement of DHFF? How
Community benefit from DHFF program implementation? (Probe: what changes
have you observed? What led to these changes?)
14. Have you ever evaluated your implementation status of DHFF program at your
facility level? If yes, how did you evaluate?
15. Are there any other factors beyond the facility that contribute or affect DHFF
implementation here? Probes: cultural issues, policies.
16. What modifications do you think should be done to improve the quality of
implementation of the DHFF program?
Thanks for your time

293
Appendix XVII: Objective Number Five (Quantitative): Level of Fidelity of
Implementation and its potential moderators
Serial No. [__|__|__|__]
Name of the Region: _____________________________________
Jina la Mkoa
Name of the District Council: ______________________________
Jina la Wilaya [_____________]
Name of the Health Facility: _______________________________
Jina la kituo cha kutolea huduma
Type of Health Facility: 01= Dispensary/Zahanati [ ] 02= Health center/ Kituo
cha Afya [ ]
Aina ya Kituo [________]
Please put the appropriate number of a response in the given box.
Tafadhali jaza namba yenye jibu/majibu sahihi
PART 1: HEALTH SERVICE PROVIDERS
Sehemu ya kwanza:watoa Huduma
SN Questions/Maswali Responses /Majibu Code Code
SECTION A: DEMOGRAPHIC
INFORMATION
1. (a)Sex/Jinsi 1.Male/Mwanaume
2.Female/ Mwanamke
01
02
[ ]
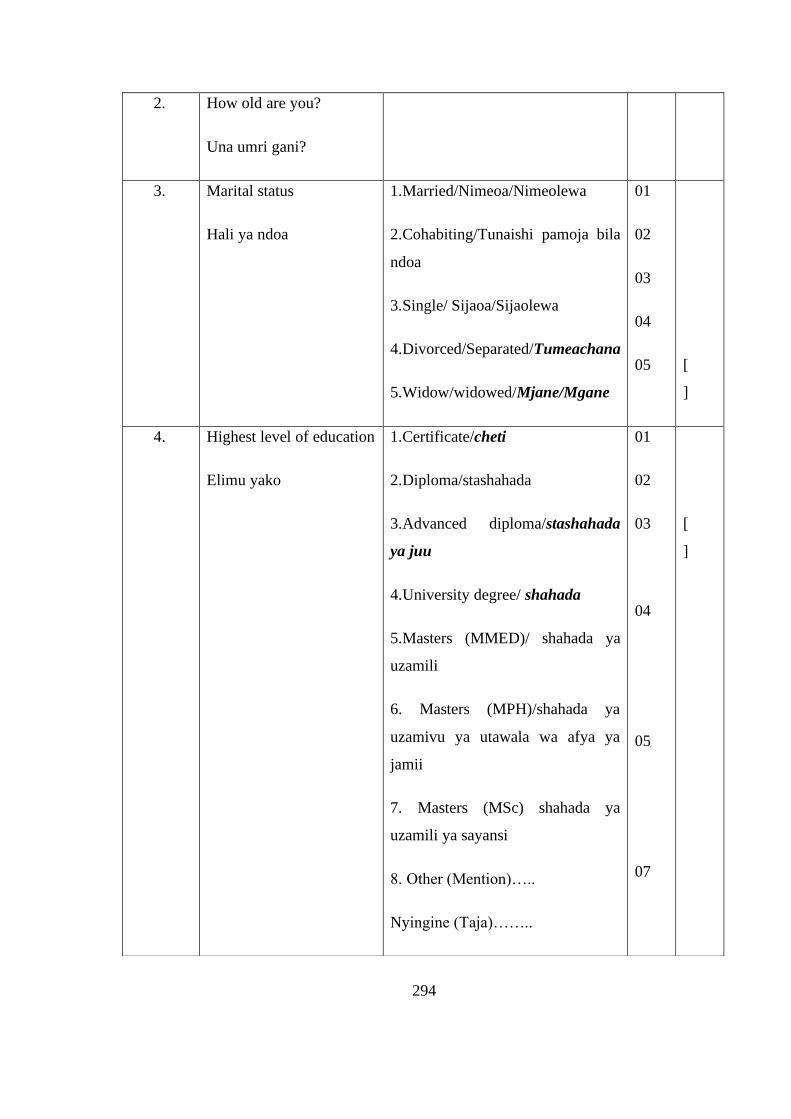
294
2. How old are you?
Una umri gani?
3. Marital status
Hali ya ndoa
1.Married/Nimeoa/Nimeolewa
2.Cohabiting/Tunaishi pamoja bila
ndoa
3.Single/ Sijaoa/Sijaolewa
4.Divorced/Separated/Tumeachana
5.Widow/widowed/Mjane/Mgane
01
02
03
04
05
[
]
4. Highest level of education
Elimu yako
1.Certificate/cheti
2.Diploma/stashahada
3.Advanced diploma/stashahada
ya juu
4.University degree/ shahada
5.Masters (MMED)/ shahada ya
uzamili
6. Masters (MPH)/shahada ya
uzamivu ya utawala wa afya ya
jamii
7. Masters (MSc) shahada ya
uzamili ya sayansi
8. Other (Mention)…..
Nyingine (Taja)……..
01
02
03
04
05
07
[
]

295
08
5. What is your cadre?
Taalum uliyosomea
1.Enrolled Nurse
Nesi mwenye cheti
2.Registered Nurse
Nesi mwenye astashahda
3.Nurse Officer
Nesi mwenye shahada
4.Assistant Clinical Officer
Tabibu msaidizi
5.Clinical Officer
Tabibu
6.Assistant Medical Officer
Msaidizi wa Daktari
7.Medical Officer/Dental Officer
Daktari
8.Medical specialist (MMED)
Daktari bingwa
9.Assistant Accountant
Mhasibu Msaidizi
10. Health Facility Governance
01
02
03
04
05
06
07
08
09
[
]

296
Committee Chair/ Member
Mwenyekiti wa Kamati ya
Usimamizi wa Kituo.
10
6. How long have you been
working in your current
job/position? [Clinician]/
[nurse] (record number of
years or term served)
Je! umefanya kazi kwa
muda gani?
[
]
7. What is your position at
this health facility?
Unacheo gani katika kituo
chako cha kazi?
1. Health service provider
2. Matron
3. In charge
4. Assistant Account
5. HFGC Chair/ Member.
6. Other
(Mention)___________
01
02
03
04
05
06
[
]
Knowledge Assesssment
8. Have you ever heard
about DHFF program?
Umeawhi kusikia kuhusu
mpango wa kupeleka
fedha moja kwa moja
katika kituo cha kutolea
1. No / Hapana
2. Yes / Ndio
01
02
[
]

297
huduma (DHFF)?
9. Where did you heard
about DHFF program?
Uliskia kuhusu mpango
huu wapi?
1. On the training
Kwenye mafunzo
2. From In charge of HF
Kwa mfawidhi wa Kituo
3. From other staffs.
Kutoka kwa watumishi wengine.
4. Somewhere else
(mention)……………..
Mahali pengine (Taja)……..
01
02
03
04
10. What minimum
requirements do you have
for the implementation of
DHFF at facilities?
(multiple selection)
Assess the performanc of
the given variable, if the
facility missed one of
them then its lack
minimum requirements.
Je, Ni mahitaji gani ya
msingi mliyo nayo kwa
ajili ya utekelzaji wa
mpango wa kupeleka
fedha moja kwa moja
1. Health facility accounts
Akaunti ya wa kituo
2. At least one skilled personnel
Angalau mtaalam mmoja
3. Active HFGC
Kuwepo kwa kamati ya usimamizi
wa kituo inayofanya kazi.
4. Others (mention)________
Nyingine (taja)….
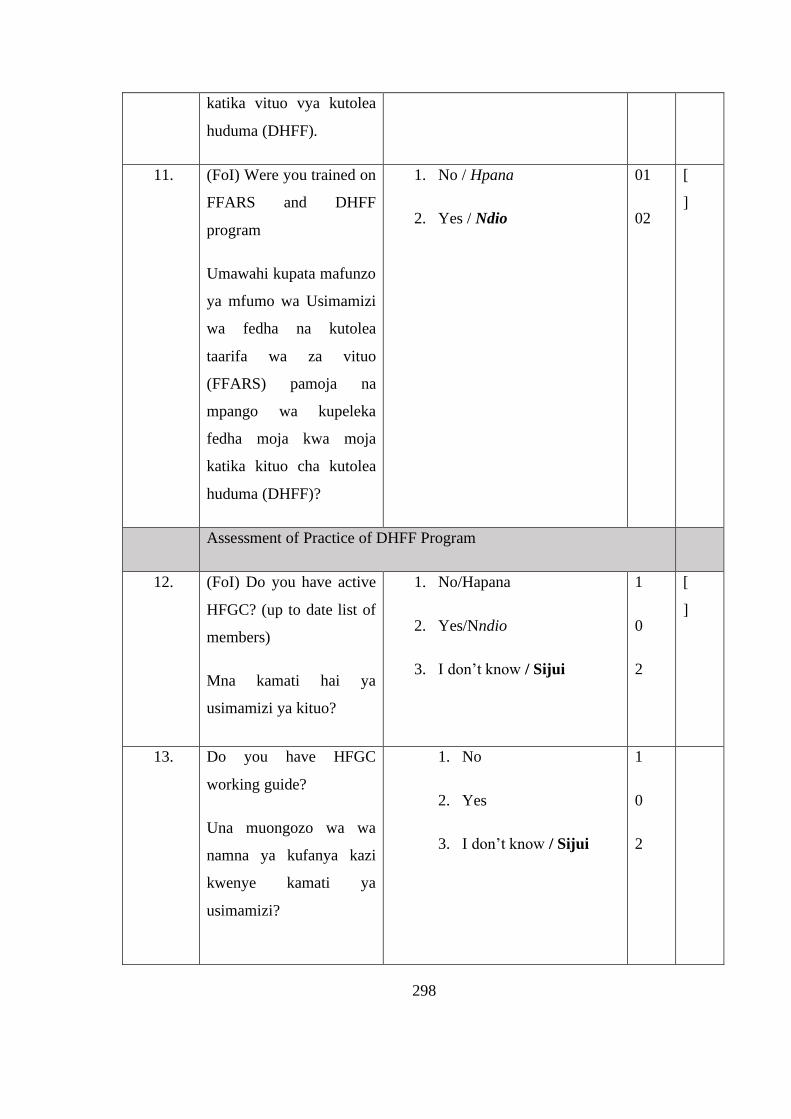
298
katika vituo vya kutolea
huduma (DHFF).
11. (FoI) Were you trained on
FFARS and DHFF
program
Umawahi kupata mafunzo
ya mfumo wa Usimamizi
wa fedha na kutolea
taarifa wa za vituo
(FFARS) pamoja na
mpango wa kupeleka
fedha moja kwa moja
katika kituo cha kutolea
huduma (DHFF)?
1. No / Hpana
2. Yes / Ndio
01
02
[
]
Assessment of Practice of DHFF Program
12. (FoI) Do you have active
HFGC? (up to date list of
members)
Mna kamati hai ya
usimamizi ya kituo?
1. No/Hapana
2. Yes/Nndio
3. I don’t know / Sijui
1
0
2
[
]
13. Do you have HFGC
working guide?
Una muongozo wa wa
namna ya kufanya kazi
kwenye kamati ya
usimamizi?
1. No
2. Yes
3. I don’t know / Sijui
1
0
2
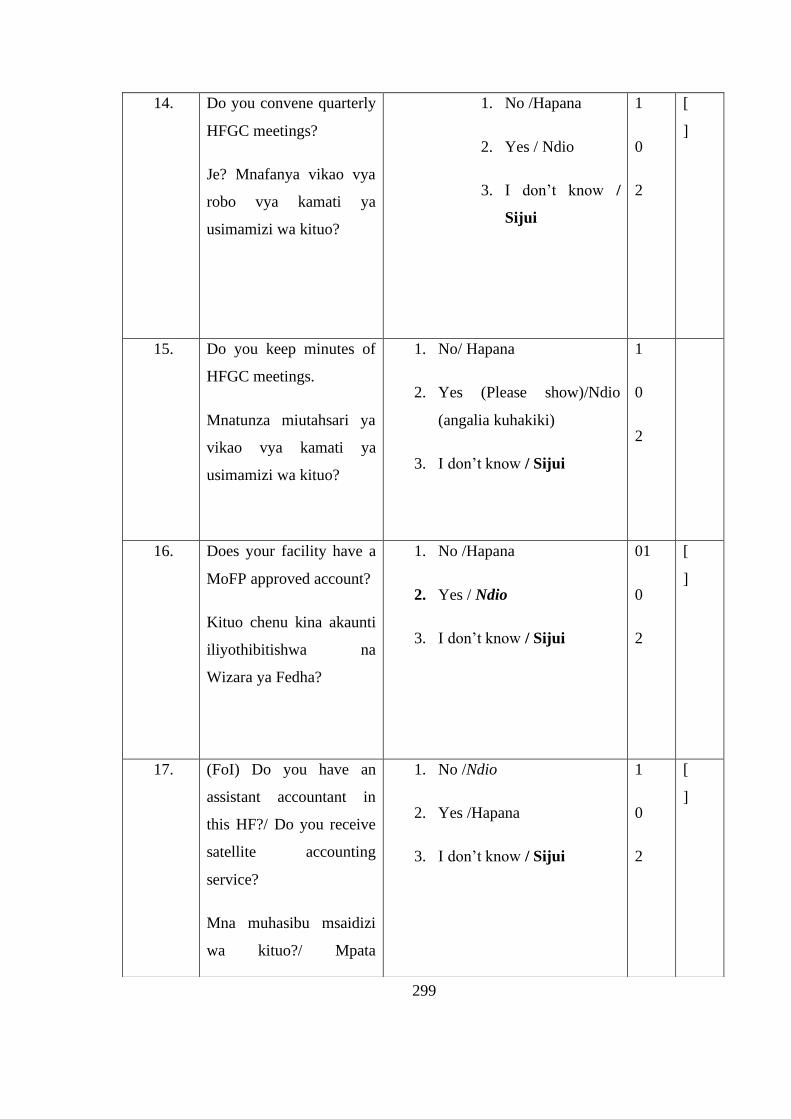
299
14. Do you convene quarterly
HFGC meetings?
Je? Mnafanya vikao vya
robo vya kamati ya
usimamizi wa kituo?
1. No /Hapana
2. Yes / Ndio
3. I don’t know /
Sijui
1
0
2
[
]
15. Do you keep minutes of
HFGC meetings.
Mnatunza miutahsari ya
vikao vya kamati ya
usimamizi wa kituo?
1. No/ Hapana
2. Yes (Please show)/Ndio
(angalia kuhakiki)
3. I don’t know / Sijui
1
0
2
16. Does your facility have a
MoFP approved account?
Kituo chenu kina akaunti
iliyothibitishwa na
Wizara ya Fedha?
1. No /Hapana
2. Yes / Ndio
3. I don’t know / Sijui
01
0
2
[
]
17. (FoI) Do you have an
assistant accountant in
this HF?/ Do you receive
satellite accounting
service?
Mna muhasibu msaidizi
wa kituo?/ Mpata
1. No /Ndio
2. Yes /Hapana
3. I don’t know / Sijui
1
0
2
[
]
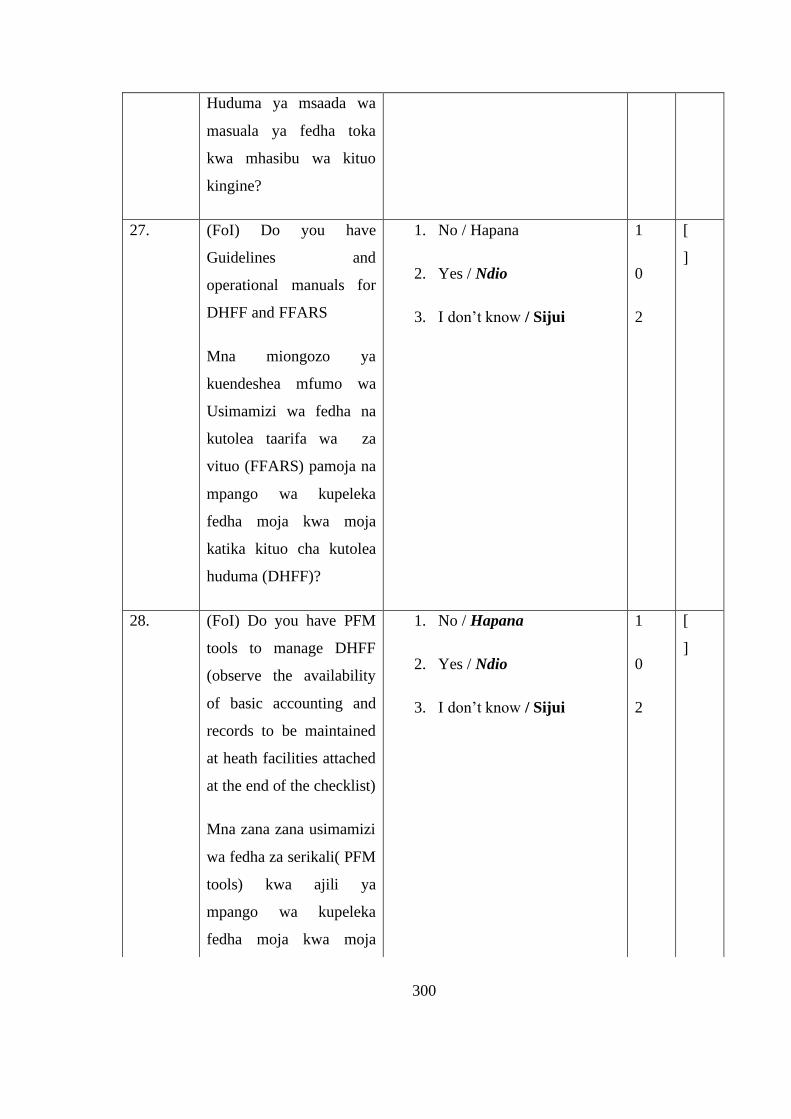
300
Huduma ya msaada wa
masuala ya fedha toka
kwa mhasibu wa kituo
kingine?
27. (FoI) Do you have
Guidelines and
operational manuals for
DHFF and FFARS
Mna miongozo ya
kuendeshea mfumo wa
Usimamizi wa fedha na
kutolea taarifa wa za
vituo (FFARS) pamoja na
mpango wa kupeleka
fedha moja kwa moja
katika kituo cha kutolea
huduma (DHFF)?
1. No / Hapana
2. Yes / Ndio
3. I don’t know / Sijui
1
0
2
[
]
28. (FoI) Do you have PFM
tools to manage DHFF
(observe the availability
of basic accounting and
records to be maintained
at heath facilities attached
at the end of the checklist)
Mna zana zana usimamizi
wa fedha za serikali( PFM
tools) kwa ajili ya
mpango wa kupeleka
fedha moja kwa moja
1. No / Hapana
2. Yes / Ndio
3. I don’t know / Sijui
1
0
2
[
]
301
katika kituo cha kutolea
huduma (DHFF)?
`Angalia kama zipo`
29.
HCWs
only.
How many times do you
convene HF Management
meetings and then give
various response options
per quarter?
Ni mara ngapi mnakaa
vikao vya Menejimenti ya
kituo kwa robo mwaka?
[
]
30.
HCWs
only.
What are the dates of the
last two HF Management
meetings you have
conducted?
Taja, tarehe za vikao
viwili vya mwisho vya
Menejimenti ya Kituo.
31. Do you have a HF Quality
Improvement Plan (QIP)?
Mna mpango wa uboshaji
wa huduma?
1. No /Hapana
2. Yes / Ndio
3. I don’t know / Sijui
1
0
2
[
]
32.HFGC
only.
Do you endorse a Quality
Improvement Plan (QIP)
for your health facility?
1. No /Hapana
2. I don’t know
1
0
[
]

302
Je, huwa unaidhinisha
mpango wa uboreshaji wa
huduma wa kituo?
sijui
3. Yes / Ndio
0.5
33. Do you have Annual
Health Facility Plan
Guideline?
Je, Mnamuongozo wa
kuandaa mpango kazi wa
kituo?
1. No/Hapana
2. I don’t Know/ Sijui
3. Yes/ Ndio
34. Do you have annual HFP?
Mna mpango wa kituo wa
mwaka?
1. No /Hapana
2. Yes / Ndio
01
02
[
]
35. Budget ceilings are
received on time (before
November)
Taarifa za ukomo wa
bajeti hupatikana kwa
wakati
1. No /Hapana
2. Yes / Ndio
3. I don’t know / Sijui
1
0
2
[
]
36. Head teacher from a
school near by facility
take part in the planning
team.
Mwalimu Mkuu au
Mwalimu mwingine
1. No /Hapana
2. Yes / Ndio
3. I don’t know / Sijui
1
0
2
[
]
303
hushiriki katika zoezi la
uandaaji wa mpango wa
Kituo.
37. Always Planning is
coordinated by
representative from
CHMT and Technical.
Mchakato wa uandaaji wa
mpango wa kiuo
huratibiwa na Mjumbe
kutoka CHM na Kamati
ya Ufundi au Mratibu wa
Kanda.
1. No /Hapana
2. Yes / Ndio
01
02
[
]
38. Member from
Village/Ward
Development Committee
if not a member of HFGC
take part in the planning
team of the health facility.
Mjumbe kutoka kamati ya
kijiji/ kata kama sio
miongoni mwa wajumbe
wa kamati ya usimamizi
wa kituo hushiriki katika
mchakato wa kuandaa
mpango wa kituo.
1. No /Hapana
2. Yes / Ndio
01
02
[
]
39. Have you received funds 1. No /Hapana 1 [
304
for DHFF program(if the
answer is no skip
questions 40, 42,43,45,46,
,47,48 and 49,)
Mmeshapata fedha za
mpango wa kupeleka
fedha moja kwa moja
katika kituo cha kutolea
huduma (DHFF)?
(Kama hapana neda swali
la 40,42,43,45,46,47,48
na 49)
2. Yes / Ndio
3. I don’t know / Sijui
0
2
]
40 When did you receive
money for this quarter?
Mlipokea lini fedha ya
robo hii ya mwaka?
1. Before 14th of first month of the
following quarter.
Kabla ya tarehe 14 ya mwezi wa
kwanza wa robo ya mwaka
iliyofuata.
2. On 14th of first month of the
following quarter.
Manamo tarehe 14 ya mwezi wa
kwanza wa robo ya mwaka
iliyofuata.
3. After 14th of first month of the
following quarter.
Baada ya tarehe 14 ya mwezi wa
kwanza wa robo ya mwaka
01
02
03
04
[
]
305
iliyofuata.
4. Not yet received/ Bado
hatujapata.
41 If No Why?
Kama hapana kwa nini?
1. We are yet to receive
funding
Bado hatujaingiziwa fedha
2. We are yet to be trained
Bado hatujapata mafunzo
3. We are not aware at all
Hatuelewi
01
02
03
42. What are the challenges
you are facing in the
course of implementing
DHFF? (Request for
Qualitative semi
structured interview
guide)
Je! kuna changamoto gani
mnapata wakati wa
utekelezaji wa mpango
wa kupeleka fedha moja
kwa moja katika kituo cha
kutolea huduma (DHFF)
1. Inadequate financial
management skills.
Uwezo mdogo wa usimamizi wa
fedha
2. Inadequate transparent
among team.
Kukosekana kwa uwazi
3. Inadequate supportive
supervision.
Usimamizi shirikishi usi wa
kuridhisha
4. Inadequate health service
providers.
[
]

306
Upungufu wa watoa huduma
5. Unsupportive relationship
with HFGC.
6. Poor coordination from
district level.
7. Inadequate availability of
working tools.
8. Inadequate availability of
accounting services.
9. Program complexity.
10. Political interfearance.
11. No challenges.
12. Other (Mention)
Mengineyo (taja)
43. In case of any challenges
in the course of
implementing the
program, where do you
report first?
1. DMO
2. District DHFF coordinator
3. Others……(mention)
44. What has been helpful to
you in achieving DHFF
goals in this Health
Facility?
Unadhani kitu gani
kimewezesha nyinyi
1. Supportive supervision
Usimamizi shirikishai
2. Provision of working tools
Kuongeza vitendea kazi

307
kufanikiwa kutekeleza
mpango huu wa DHFF
katika kituo hiki?
3. Employment of other staff
Kuajiri watumishi
4. Others (mention)________
(Mengine taja)
45. When did you receive
your last supportive
supervision from CHMT?
Ni lini ulifanyika
usimamizi shirikishi wa
timu ya uisimamizi wa
Afya ya Wilaya (CHMT)?
1. Last Quarter
Robo iliyopita
2. This quarter
Robo hii
3. Not yet (skip question 46)
Bado haujafanyika
01
02
03
[
]
46. During the supportive
supervision did you
discuss issues of DHFF
implementation?
Katika kipindi cha
ukaguzi mlijadili masuala
ya DHFF?
1. No
2. Yes
47. Have you received any
feedback on the previous
supportive supervision?
Umewahi kupata
mrejesho wa usimamizi
shirikishi wa timu ya
uisimamizi wa Afya ya
1. No /Hapana
2. Yes / Ndio
01
02
[
]

308
Wilaya (CHMT)?
48. Who is making decision
of your routine Health
Facility activities?
Nani anafanya maamuzi
ya mpango wa kituo
chenu?
1. Matron
2. In charge
3. Any one
4. All of us through meetings.
5. Other (mention)________
01
02
03
04
05
[
]
49. (FoI) Do you play an
active role (in charge) /
get involved (health care
workers)/ endorse
(HFGC) (in) DHFF
program implementation
decision making?
Je unashiriki kikamilifu
(mfawidhi wa kituo) /
unashirikishwa kikamilifu
(wahudumu wa kituo)
katika maamuzi ya
utekelezaji wa mpango
wa kupeleka fedha moja
kwa moja katika kituo cha
kutolea huduma (DHFF)
1. No /Hapana
2. Yes / Ndio
01
02
[
]
50. What are the sources of
your Health facility fund?
(Multiple selection)
Vyanzo vya fedha za
1. Health Basket Fund
2. Results Based Financing
01
02
[
]
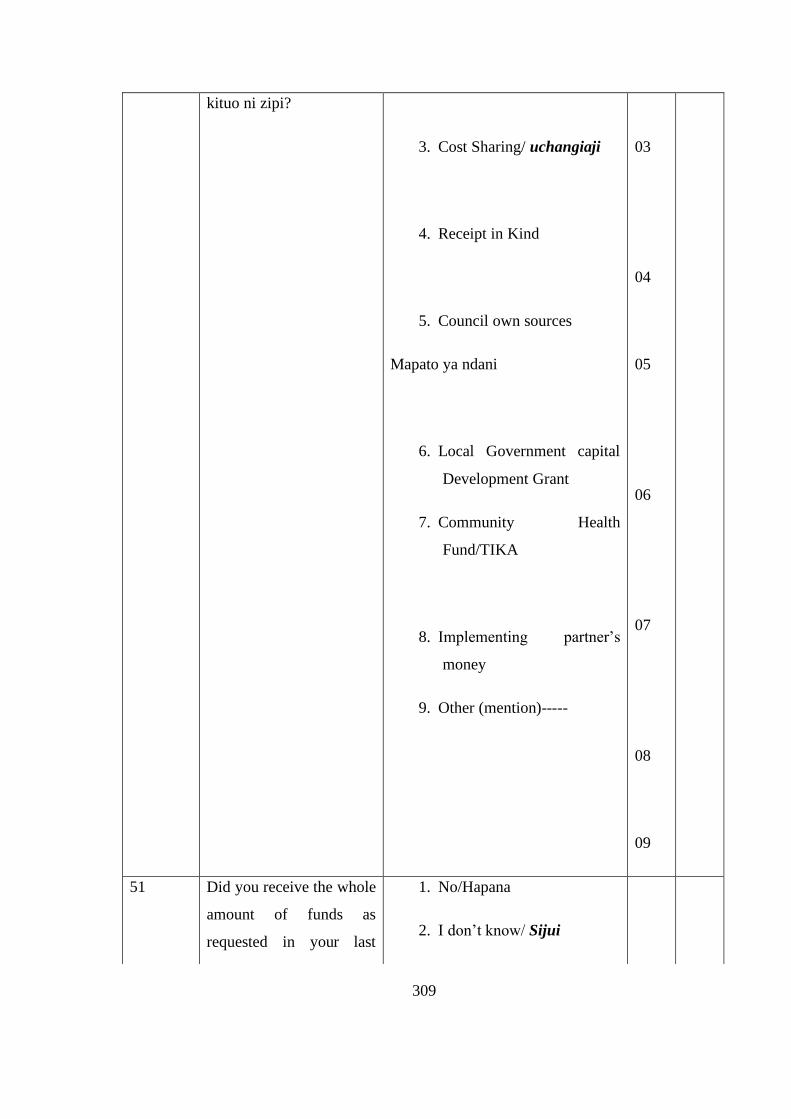
309
kituo ni zipi?
3. Cost Sharing/ uchangiaji
4. Receipt in Kind
5. Council own sources
Mapato ya ndani
6. Local Government capital
Development Grant
7. Community Health
Fund/TIKA
8. Implementing partner’s
money
9. Other (mention)-----
03
04
05
06
07
08
09
51 Did you receive the whole
amount of funds as
requested in your last
1. No/Hapana
2. I don’t know/ Sijui
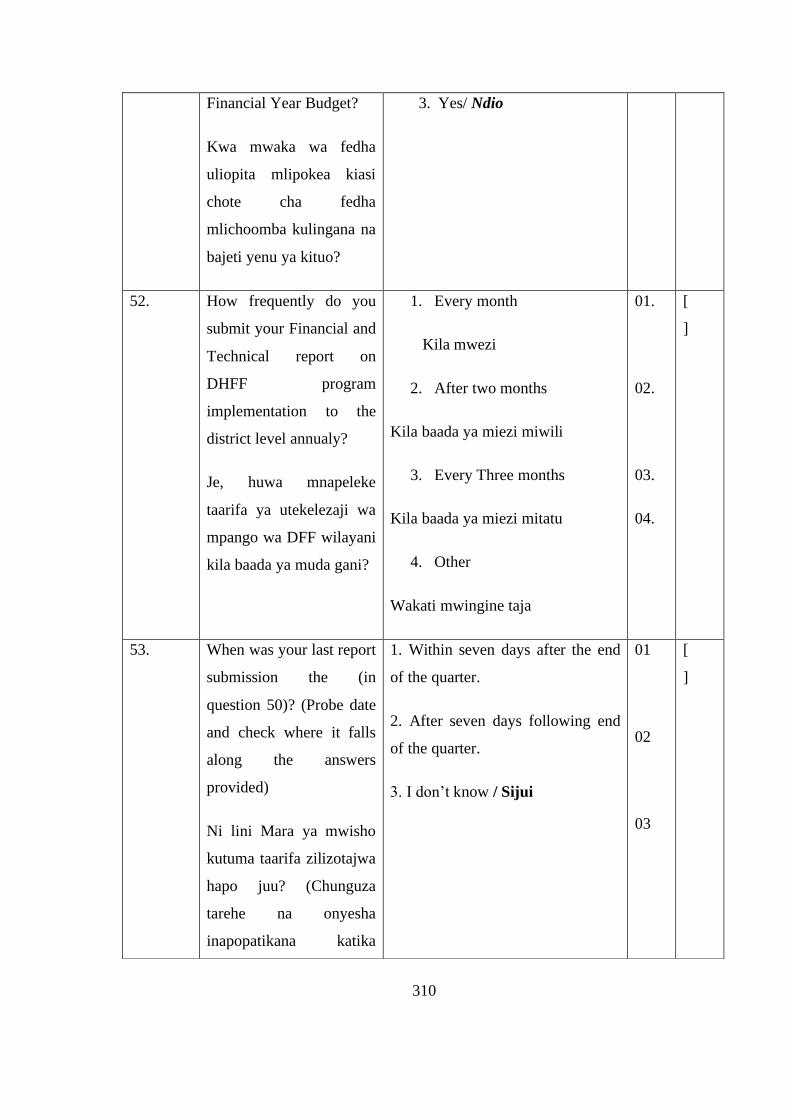
310
Financial Year Budget?
Kwa mwaka wa fedha
uliopita mlipokea kiasi
chote cha fedha
mlichoomba kulingana na
bajeti yenu ya kituo?
3. Yes/ Ndio
52. How frequently do you
submit your Financial and
Technical report on
DHFF program
implementation to the
district level annualy?
Je, huwa mnapeleke
taarifa ya utekelezaji wa
mpango wa DFF wilayani
kila baada ya muda gani?
1. Every month
Kila mwezi
2. After two months
Kila baada ya miezi miwili
3. Every Three months
Kila baada ya miezi mitatu
4. Other
Wakati mwingine taja
01.
02.
03.
04.
[
]
53. When was your last report
submission the (in
question 50)? (Probe date
and check where it falls
along the answers
provided)
Ni lini Mara ya mwisho
kutuma taarifa zilizotajwa
hapo juu? (Chunguza
tarehe na onyesha
inapopatikana katika
1. Within seven days after the end
of the quarter.
2. After seven days following end
of the quarter.
3. I don’t know / Sijui
01
02
03
[
]

311
majibu yaliyotolewa).
54. Do you know Village
Health Committee? (If the
answer is no skip
questions 56 – 57)
Unaifahamu kamati ya
afya ya kijiji?
1. No / Hapana
2. Yes / Ndio
01
02
[
]
55. If Yes, are you a member
of that committee?
Kama ndio wewe ni
mjumbe wa kamati hiyo?
1. No / Hapana
2. Yes / Ndio
01
02
[
]
56. Have you ever attended in
their meetings?
Umewahimkuhudhuria
vikao hivyo?
1. No / Hapana
2. Yes / Ndio
01
02
[
]
57. Do you work with Village
Health Committee?
Unafanya kazi na kamati
ya afya ya kijiji?
1. No / Hapana
2. Yes / Ndio
01
02
[
]
58. What other programs
apart form DHFF are
implemented in this
facility? (List them)
Ni programu gani
nyingine za uboresha
huduma za afya

312
zinatekelezwa kwenye
kituo hiki? (Taja)
Reccomendations for Improving Program Implementation
59 Which approach/ways/
means will you prefer to
be used in submitting
your reports?
Ni njia gani ungependelea
kutumia wakati wa
kutuma taarifa?
1. Monthly submission as
DHIS2
Kila mwezi kama kwenye
mfumo wa DHIS2
2. Weekly through text messages
via mobile phones
Kwa ujumbe wa simu kila
wiki
3. On quarterly basis like any
other reports for technical and
financial
Kwa kila robo
4. Other (mention)
Nyingine (taja)….
01
02
03
04
[
]
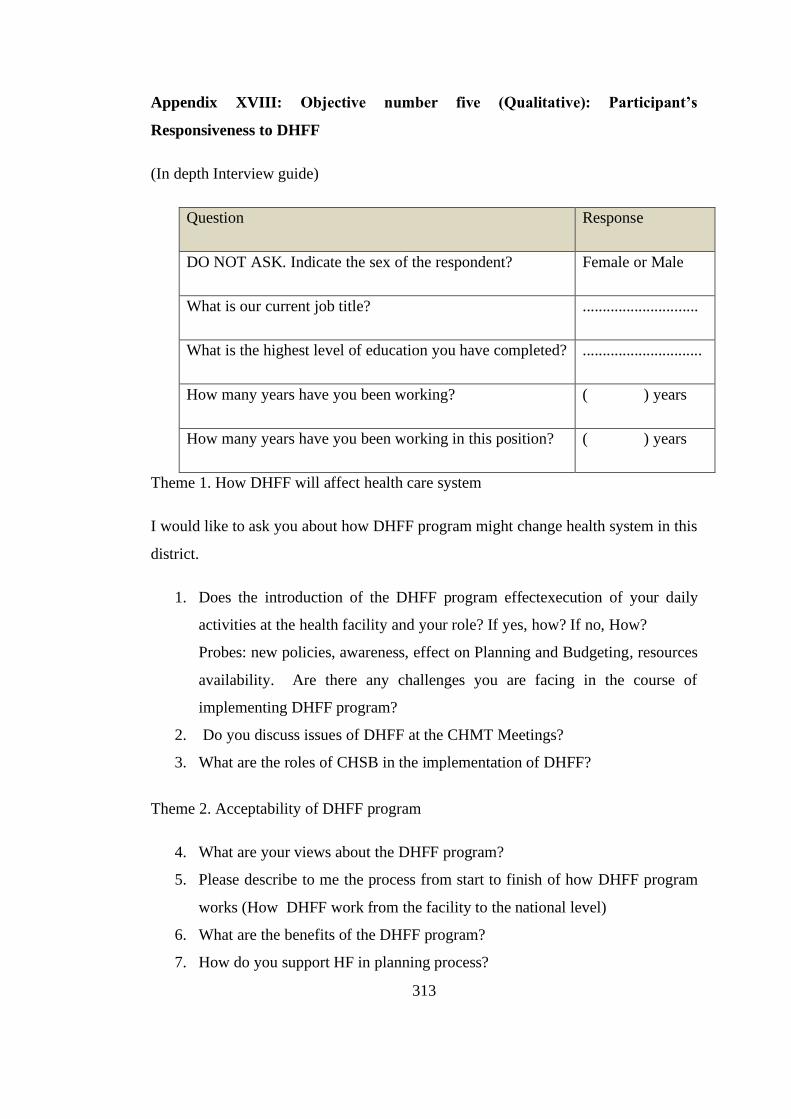
313
Appendix XVIII: Objective number five (Qualitative): Participant’s
Responsiveness to DHFF
(In depth Interview guide)
Question Response
DO NOT ASK. Indicate the sex of the respondent? Female or Male
What is our current job title? .............................
What is the highest level of education you have completed? ..............................
How many years have you been working? ( ) years
How many years have you been working in this position? ( ) years
Theme 1. How DHFF will affect health care system
I would like to ask you about how DHFF program might change health system in this
district.
1. Does the introduction of the DHFF program effectexecution of your daily
activities at the health facility and your role? If yes, how? If no, How?
Probes: new policies, awareness, effect on Planning and Budgeting, resources
availability. Are there any challenges you are facing in the course of
implementing DHFF program?
2. Do you discuss issues of DHFF at the CHMT Meetings?
3. What are the roles of CHSB in the implementation of DHFF?
Theme 2. Acceptability of DHFF program
4. What are your views about the DHFF program?
5. Please describe to me the process from start to finish of how DHFF program
works (How DHFF work from the facility to the national level)
6. What are the benefits of the DHFF program?
7. How do you support HF in planning process?

314
8. How do health service providers respond to the available DHFF guideline?
9. How do you track the performance of the DHFF program in your Health
Facilities?
10. How RHMT support you in the implementation of DHFF program? (Probe
for frequency?)
11. Which steps did you undertake during introduction of DHFF program in
district? Probe measures undertaken (They must include; Meeting with
HFGC, HF providers meeting, Meeting with Ward/Village council)
12. What are the benefits associated with implementation of DHFF in your
district?
13. Which approach will you prefer the HF to submit DHFF implementation
reports?
14. Do budget ceilings reveled before November of every year/ If Yes/No, do
you feel of any other month to be suitable for ceilings submission and why?
15. How did you handle the transaction of disbursement of funds from the
previous practice to the DHFF program implementations?
16. What are your accountability options to ensure that DHFF program is
implemented as per design/expectations?
17. What do you think should be done to make DHFF program successful (probe
reasons)
18. Imagine that you are the Minister of Heath Community Development,
Gender, Elderly and Children instilled to decide whether or not to continue
with the implementation of DHFF program. What would you do?
• If says to continue, ask if they would change anything
• If says to stop, ask why
19. Can you tell me something about the Village Health Committee? Probe more
on the composition, function and their mandate.
20. How do you support them?
21. Is there anyone else who you think it would it be important for me to speak to
about the program?
Thanks for your time!
315
Appendix XIX: Consent Form
CONSENT FORM
Hello, my name is NTULI A. KAPOLOGWE, I am from University of Dodoma
(UDOM) (Dodoma), as part of my PhD program in Public Health; I am conducting a
research on EFFECT OF DIRECT HEALTH FACILITY FINANCING (DHFF) ON
THE PERFORMANCE OF HEALTH SYSTEMS IN THE PPHF IN TANZANIA.
The results of this study will give insight of DHFF program as well as help the
government in planning the other program.
You are kindly requested to participate in this study by giving your views, opinion
and experiences so as to fulfil our goal. I would like to request you to answer these
questions as truthfully as you can. You will be required to answer the questions from
the questionnaires. The administration of questionnaire/Interview will take about 15-
20 minutes.
All the information which you are going to give will remain confidential and limited
to only members of research team, and they will be used in nothing more than for the
purpose explained above. Codes will be used and no identification will be made for
you.
Your participation is voluntarily. You may decide to refuse or not participate in this
study without giving any reasons. However, your input through participation is
highly valued and will be appreciated.
I have read and understood the request. Under my own will, without force or any
promises, I would like to participate in this study for the purpose explained.
Interviewee signature…….. Interviewer ignature……………….Date……………..
Witness signature ……………………….. Date……………………
“I am sorry; I am not willing to participate”
316
HATI YA KUKUBALI KUSHIRIKI
Habari, Jina langu naitwa NTULI A. KAPOLOGWE. Nipo katika chuo Kikuu Cha
Dodoma (UDOM), ikiwa kama sehemu ya kukamilisha masomo yangu ya shahada
ya Uzamivu ya Afya ya Jamii (PhD in Public Health), ninafanya utafiti juu ya
Manufaa ya Upelekaji wa Fedha Moja kwa Moja Katika Vituo vya Kutolea
Huduma (DHFF) katika utendaji wa Mifumo ya utoaji wa huduma za Afya
ngazi ya Msingi nchini Tanzania.
Matokeo ya utafiti huu yataiwezesha Serikali kusimamiza vyema mpango huu
pamoja na Mipango mingine.
Mazungumzo yetu yatachukuwa kama dakika kumi na tano mpaka ishirini hivi
kukamilika, zitatumika namba na sio jina wala hakutakuwa na kitu kingine chochote
cha kukutambua ushiriki wako. Taarifa utakazozitoa zitakuwa ni siri na zitatumika
kwa ajili ya utafiti tu na si kwa kitu kingine chochote.
Kushiriki kwako katika utafiti huu ni hiari, unaweza kuamua kukataa au kutoshiriki
katika utafiti huu. Hata hivyo ni mategemeo yangu kuwa utashiriki kikamilifu katika
utafiti huu kwani maoni yako ni muhimu sana.
“Nimesoma na nimeelewa ombi lako, kwa hiari yangu, bila ya nguvu wala ahadi
zozote nakubali kushiriki katika utafiti huu”.
Sahihi ya mshiriki………………. Sahihi ya muulizaji....................
Tarehe ........................................... Tarehe ............................
Sahihi ya shahidi ...........................
“Samahani, sipo tayari kushiriki

317
Appendix XX: Ethical Clearance Forms

318
319
Related Documents











