dental materials 23 ( 2 0 0 7 ) 844–854 available at www.sciencedirect.com journal homepage: www.intl.elsevierhealth.com/journals/dema Review Surface treatments of titanium dental implants for rapid osseointegration L. Le Gu´ ehennec, A. Soueidan, P. Layrolle ∗ , Y. Amouriq Inserm U791, LIOAD, Osteoarticular and Dental Tissue Engineering, Faculty of Dental Surgery, 1 Place Alexis Ricordeau, 44042 Nantes cedex 1, France article info Article history: Received 9 November 2005 Received in revised form 9 June 2006 Accepted 20 June 2006 Keywords: Osseointegration Dental implants Surface roughness Nano-sized topography Biomimetic calcium phosphate coating abstract The osseointegration rate of titanium dental implants is related to their composition and surface roughness. Rough-surfaced implants favor both bone anchoring and biomechanical stability. Osteoconductive calcium phosphate coatings promote bone healing and appo- sition, leading to the rapid biological fixation of implants. The different methods used for increasing surface roughness or applying osteoconductive coatings to titanium dental implants are reviewed. Surface treatments, such as titanium plasma-spraying, grit-blasting, acid-etching, anodization or calcium phosphate coatings, and their corresponding sur- face morphologies and properties are described. Most of these surfaces are commercially available and have proven clinical efficacy (>95% over 5 years). The precise role of surface chemistry and topography on the early events in dental implant osseointegration remain poorly understood. In addition, comparative clinical studies with different implant surfaces are rarely performed. The future of dental implantology should aim to develop surfaces with controlled and standardized topography or chemistry. This approach will be the only way to understand the interactions between proteins, cells and tissues, and implant surfaces. The local release of bone stimulating or resorptive drugs in the peri-implant region may also respond to difficult clinical situations with poor bone quality and quantity. These therapeu- tic strategies should ultimately enhance the osseointegration process of dental implants for their immediate loading and long-term success. © 2006 Academy of Dental Materials. Published by Elsevier Ltd. All rights reserved. Contents 1. Introduction .................................................................................................................. 845 2. Chemical composition of the surface of dental implants .................................................................. 845 3. Surface roughness of dental implants ...................................................................................... 845 3.1. Roughening of implants by titanium plasma-spraying ............................................................. 846 3.2. Roughening of implants by grit-blasting ............................................................................. 846 3.3. Roughening of implants by acid-etching ............................................................................. 847 3.4. Roughening of implants by anodization ............................................................................. 848 ∗ Corresponding author. Tel.: +33 2 4041 2916; fax: +33 2 40 08 37 12. E-mail address: [email protected] (P. Layrolle). 0109-5641/$ – see front matter © 2006 Academy of Dental Materials. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.dental.2006.06.025

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
dental mater ials 2 3 ( 2 0 0 7 ) 844854
avai lab le at www.sc iencedi rec t .com
journa l homepage: www. int l .e lsev ierhea l th .com/ journa ls /dema
Review
Surfa talimpla
L. Le Guehennec, A. Soueidan, P. Layrolle , Y. AmouriqInserm U791, LIOAD, Osteoarticular and Dental Tissue Engineering, Faculty of Dental Surgery,1 Place Alexis Ricordeau, 44042 Nantes cedex 1, France
a r t i c
Article histor
Received 9 N
Received in
Accepted 20
Keywords:
Osseointegr
Dental impl
Surface rou
Nano-sized
Biomimetic
coating
Contents
1. Intro2. Chem3. Surfa
3.1.3.2.3.3.3.4.
CorresponE-mail a
0109-5641/$doi:10.1016/l e i n f o
y:
ovember 2005
revised form 9 June 2006
June 2006
ation
ants
ghness
topography
calcium phosphate
a b s t r a c t
The osseointegration rate of titanium dental implants is related to their composition and
surface roughness. Rough-surfaced implants favor both bone anchoring and biomechanical
stability. Osteoconductive calcium phosphate coatings promote bone healing and appo-
sition, leading to the rapid biological xation of implants. The different methods used
for increasing surface roughness or applying osteoconductive coatings to titanium dental
implants are reviewed. Surface treatments, such as titanium plasma-spraying, grit-blasting,
acid-etching, anodization or calcium phosphate coatings, and their corresponding sur-
face morphologies and properties are described. Most of these surfaces are commercially
available and have proven clinical efcacy (>95% over 5 years). The precise role of surface
chemistry and topography on the early events in dental implant osseointegration remain
poorly understood. In addition, comparative clinical studies with different implant surfaces
are rarely performed. The future of dental implantology should aim to develop surfaceswith
controlled and standardized topography or chemistry. This approach will be the only way to
understand the interactions between proteins, cells and tissues, and implant surfaces. The
local release of bone stimulating or resorptive drugs in the peri-implant region may also
respond to difcult clinical situations with poor bone quality and quantity. These therapeu-
tic strategies should ultimately enhance the osseointegration process of dental implants for
their immediate loading and long-term success.
2006 Academy of Dental Materials. Published by Elsevier Ltd. All rights reserved.
duction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 845ical composition of the surface of dental implants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 845ce roughness of dental implants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 845Roughening of implants by titanium plasma-spraying . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 846Roughening of implants by grit-blasting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 846Roughening of implants by acid-etching. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 847Roughening of implants by anodization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 848
ding author. Tel.: +33 2 4041 2916; fax: +33 2 40 08 37 12.ddress: [email protected] (P. Layrolle). see front matter 2006 Academy of Dental Materials. Published by Elsevier Ltd. All rights reserved.j.dental.2006.06.025ce treatments of titanium dennts for rapid osseointegration
-
dental mater ials 2 3 ( 2 0 0 7 ) 844854 845
4. Osteoconductive calcium phosphate coatings on dental implants. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8495. Future trends in dental implant surfaces . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 849
5.1.5.2.5.3.
6. ConcAcknRefer
1. Int
In the pastdures has imillion denoral implanetry and sulong-term sassociatedfor a succestitanium imDirect boneical for thestages of ostors and paof the impltation. Thetissue capsdoes not enclinical failresponse isan intervenas osseointbe a prereqlong-term stitanium imface compoeters that mosseointegr
This revthat aim toThe physicdiscussed iManufactusurfaces wness. Howefor implant
2. Chdental im
The cheminium impland surfaccritical forimplants aror titaniumious degreeSurface roughness at the nanoscale level. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 849Biomimetic calcium phosphate coatings on titanium dental implants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 850Incorporation of biologically active drugs into titanium dental implants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 850
lusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 851owledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 851ences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 851
roduction
20 years, the number of dental implant proce-ncreased steadily worldwide, reaching about onetal implantations per year. The clinical success ofts is related to their early osseointegration. Geom-rface topography are crucial for the short- anduccess of dental implants. These parameters arewith delicate surgical techniques, a prerequisitesful early clinical outcome [1]. After implantation,plants interact with biological uids and tissues.apposition onto the surface of the titanium is crit-rapid loading of dental implants. After the initialseointegration, both prosthetic biomechanical fac-tient hygiene are crucial for the long-term successants. There are two types of response after implan-rst type involves the formation of a brous softule around the implant. This brous tissue capsulesure proper biomechanical xation and leads to
ure of the dental implant. The second type of bonerelated to direct boneimplant contact without
ing connective tissue layer. This is what is knownegration. This biological xation is considered touisite for implant-supported prostheses and theiruccess. The rate and quality of osseointegration inplants are related to their surface properties. Sur-sition, hydrophilicity and roughness are param-ay play a role in implanttissue interaction and
ation.iew focuses on the different surfaces and methodsaccelerate the osseointegration of dental implants.al and chemical properties of implant surfaces aren relation to their biological and clinical behavior.rers of dental implants have developed a variety ofith different compositions and degrees of rough-ver, there is controversy as to the optimal featuressurfaces regarding osseointegration kinetics.
emical composition of the surface ofplants
cal composition or charges on the surface of tita-ants differ, depending on their bulk compositione treatments. The composition and charges areprotein adsorption and cell attachment. Dentale usually made from commercially pure titaniumalloys. Commercially pure titanium (cpTi) has var-s of purity (graded from 1 to 4). This purity is
characterized by oxygen, carbon and iron content. Most den-tal implants are made from grade 4 cpTi as it is stronger thanother grades. Titanium alloys aremainly composed of Ti6Al4V(grade 5 titanium alloy) with greater yield strength and fatigueproperties than pure titanium [2].
The surface chemical composition of titanium implantsalso affects the hydrophilicity of the surface. Highlyhydrophilic surfaces seem more desirable than hydropho-bic ones in view of their interactions with biological uids,cells and tissues [3,4]. Contact angle measurements give val-ues ranging from 0 (hydrophilic) to 140 (hydrophobic) fortitanium implant surfaces [3,5,6]. In a recent animal study,Buser et al. [3] found that a hydrophilic SLA surface gavehigher bone-to-implant contact than regular SLA. Neverthe-less, previous in vivo studies performed by Albrektsson andco-workers [7,8] failed to demonstrate higher osseointegrationusing hydrophilic surfaced dental implants.
3. Surface roughness of dental implants
There are numerous reports that demonstrate that the surfaceroughness of titanium implants affects the rate of osseointe-gration and biomechanical xation [9,10]. Surface roughnesscan be divided into three levels depending on the scale of thefeatures: macro-, micro- and nano-sized topologies.
The macro level is dened for topographical features asbeing in the range ofmillimetres to tens ofmicrons. This scaleis directly related to implant geometry, with threaded screwand macroporous surface treatments giving surface rough-ness of more than 10m. Numerous reports have shown thatboth the early xation and long-term mechanical stability ofthe prosthesis can be improved by a high roughness prolecompared to smooth surfaces [1113]. The high roughnessresulted in mechanical interlocking between the implant sur-face and bone ongrowth. However, a major risk with highsurface roughness may be an increase in peri-implantitis aswell as an increase in ionic leakage [14]. A moderate rough-ness of 12m may limit these two parameters [15].
The microtopographic prole of dental implants is denedfor surface roughness as being in the range of 110m. Thisrange of roughness maximizes the interlocking betweenmineralized bone and the surface of the implant [10,13]. Atheoretical approach suggested that the ideal surface shouldbe covered with hemispherical pits approximately 1.5m indepth and 4m in diameter [16].
The main clinical indication for using an implant witha rough surface is the poor quality or volume of the hostbone. In these unfavorable clinical situations, early and high
-
846 dental mater ials 2 3 ( 2 0 0 7 ) 844854
Table 1 Surface properties of titanium dental implants
Type of implant Surface roughness (m) Contact angle () References
cpTi Ra=0.220.01a 55.44.1 [5,107]Ti6Al4V Ra=0.230.01a 56.32.7 [5,107]TPS Ra=7.012.09 n.d. [5]SLA Sa=1.150.05 138.34.2 [3]Modied SLA Sa=1.160.04 0 [3]Plasma-sprayed HA coating Ra=1.060.21 57.43.2 [6,108]Biomimetic CaP coating Ra=1.830.64 13.40.17 This work
a Machined and polished surfaces.
bone-to-implant contact would be benecial for allowing highlevels of loading. In the cases of insufcient bone quantity oranatomical limitations, short designed implants with a roughsurface have demonstrated superior clinical outcomes thansmooth susurface rouimplant coother typesdemonstrafaces havewith smootoration hathe superio
Surfacerole in thecells and thducible surto producesurface nanleading toapposition
Variousa rough sunium dentaplasma-sprand anodiz
3.1. Rouplasma-spr
A titaniumproducingsists in injhigh tempe
the surface of the implants where they condense and fusetogether, forming a lm about 30m thick. The thicknessmust reach 4050m to be uniform. The resulting TPS coat-ing has an average roughness of around 7m,which increases
rfacedimeboninip
surfarageomets [2eouphagen reprodce ofic cic aen uA aned b, theinferyapasusrouthan.
Ro
er apblas
Fig. 1 SEMrfaces [17,18]. Numerous studies have shown thatghness in this range resulted in greater bone-to-ntact and higher resistance to torque removal thanof surface topography [10,13]. These reports have
ted that titanium implants with roughened sur-greater contact with bone than titanium implantsher surfaces [9,10]. However, the Cochrane collab-s not found any clinical evidence demonstratingrity of any particular implant surface [19].proles in the nanometer range play an importantadsorption of proteins, adhesion of osteoblasticus the rate of osseointegration [20]. However, repro-face roughness in the nanometer range is difcultwith chemical treatments. In addition, the optimalo topography for selective adsorption of proteins
the adhesion of osteoblastic cells and rapid boneis unknown.methods have been developed in order to createrface and improve the osseointegration of tita-l implants (Table 1). These methods use titaniumaying, blastingwith ceramic particles, acid-etchingation.
ghening of implants by titaniumaying
plasma-spraying (TPS) method has been used forrough implant surfaces (Fig. 1). This method con-ecting titanium powders into a plasma torch atrature. The titanium particles are projected on to
the suthree-at theusingma TPSan avehave simplanendossmacroalso bebe thea soursystemsystemnot being SLobservmodelto behydroxconseneratelyrather[11,26]
3.2.
Anothsists inmicrographs of a titanium plasma-sprayed (TPS) surface (Courarea of the implant. It has been shown that thisnsional topography increased the tensile strengthe/implant interface [11]. In this pre-clinical studyigs, the bone/implant interface formed faster withce than with smooth surface implants presentingroughness of 0.2m.However, particles of titaniumtimes been found in the bone adjacent to these1]. The presence of metallic wear particles froms implants in the liver, spleen, small aggregates ofes and even in the para-aortic lymph nodes haveported [21].Metal ions released from implantsmayuct of dissolution, fretting and wear, and may beconcern due to their potentially harmful local andarcinogenic effects [22,23]. However, the local anddverse effects of the release of titanium ions haveniversally recognized. In a clinical study compar-d TPS implant surfaces, no clinical difference wasetween these two surfaces [24]. In a pre-clinicalpercentage of bone/implant contact was found
ior for the TPS surface than for plasma-sprayedtite-coated implants [25]. Nowadays, there is aon the clinical advantages of implanting mod-gh surfaced implants (in the micrometric range)
using rough plasma-sprayed implant surfaces
ughening of implants by grit-blasting
proach for roughening the titanium surface con-ting the implants with hard ceramic particles. Thetesy of Cam Implants BV, The Netherlands).
-
dental mater ials 2 3 ( 2 0 0 7 ) 844854 847
Fig. 2 SEM micrographs of a TiO blasted surface (Courtesy of Astratech TiOblastTM, France).
ceramic particles are projected through a nozzle at high veloc-ity by means of compressed air. Depending on the size of theceramic paduced on tichemicallyosseointegrparticles hacalcium ph
Aluminaand producetry of theoften embeeven after ution. Alumifrom the titbeen releasferedwith tchemical hthe excelleical environ
Titaniumtal implantof 25m prange on dblasted surmicroimplament for bimplants inexperimenniumgrit-bhigh clinicaup to 10 yea
studies gave highermarginal bone levels and survival rates forTiO2 grit-blasted implants than formachined turned implants
.nnerrit-blof bchanh titancrecompeselantir biird pts inableyapaonsres
surfabonred temoed weved
Rou
g withertchinangi
Fig. 3 rticles, different surface roughnesses can be pro-tanium implants. The blasting material should bestable, biocompatible and should not hamper theation of the titanium implants. Various ceramicve been used, such as alumina, titanium oxide andosphate particles.(Al2O3) is frequently used as a blasting material
es surface roughness varying with the granulom-blasting media. However, the blasting material isdded into the implant surface and residue remainsltrasonic cleaning, acid passivation and steriliza-na is insoluble in acid and is thus hard to removeanium surface. In some cases, these particles haveed into the surrounding tissues and have inter-he osseointegration of the implants.Moreover, thiseterogeneity of the implant surface may decreasent corrosion resistance of titanium in a physiolog-ment [27].oxide is also used for blasting titanium den-
s. Titanium oxide particles with an average sizeroduce a moderately rough surface in the 12mental implants. An example of a titanium oxide-face is shown in Fig. 2. An experimental study usingnts in humans has shown a signicant improve-one-to-implant contact (BIC) for the TiO2 blastedcomparison with machined surfaces [28]. Other
tal studies conrmed the increase in BIC for tita-lasted surfaces [12,29]. Other studies have reportedl success rates for titanium grit-blasted implants,rs after implantation [30,31]. Comparative clinical
[32,33]We
that gvaluesbiomesmootforce iwhile[34]. Thtal impnot the
A thconsisresorbhydroxbeen cals areniumhighercompahave dobservis achi
3.3.
Etchinis anotAcid-esizes rSEM micrographs of an SLA surface on a titanium dental implaberg et al. [13] demonstrated with a rabbit modelasting with TiO2 or Al2O3 particles gave similaroneimplant contact, but drastically increased theical xation of the implants when compared tonium. These studies have shown that the torqueased with the surface roughness of the implantsarable values in bone apposition were observedstudies corroborate that roughening titanium den-s increases their mechanical xation to bone butological xation.ossibility for roughening titanium dental implantsusing a biocompatible, osteoconductive and
blasting material. Calcium phosphates such astite, beta-tricalciumphosphate andmixtures have
idered useful blasting materials. These materi-orbable, leading to a clean, textured, pure tita-ce. Experimental studies have demonstrated ae-to-implant contact with these surfaces wheno machined surfaces [35,36]. Experimental studiesnstrated a bone-to-implant contact similar to thatith other blasting surfaces when osseointegration[37].
ghening of implants by acid-etching
h strong acids such as HCl, H2SO4, HNO3 and HFmethod for roughening titanium dental implants.g produces micro pits on titanium surfaces withng from 0.5 to 2m in diameter [38,39]. Acid-nt (Courtesy of Straumann AG, Switzerland).
-
848 dental mater ials 2 3 ( 2 0 0 7 ) 844854
etching has been shown to greatly enhance osseointegra-tion [40]. Immersion of titanium implants for several min-utes in a mixture of concentrated HCl and H2SO4 heatedabove 100 C (dual acid-etching) is employed to produce amicrorough surface (Fig. 3). This type of surface promotesrapid osseointegration while maintaining long-term suc-cess over 3 years [41]. It has been found that dual acid-etched surfaces enhance the osteoconductive process throughthe attachment of brin and osteogenic cells, resulting inbone formation directly on the surface of the implant [42].In the peri-implant area, woven bone with thin trabecu-lae projecting into the implants, has been described [43].These studies hypothesized that implants treated by dualacid-etching have a specic topography able to attach tothe brin scaffold, to promote the adhesion of osteogeniccells, and thus to promote bone apposition [44,45]. Severalexperimental studies have reported higher bone-to-implantcontact ansurfaces coRecently, ato increastemperaturporous surTPS surfacity of therin adhesiance for texperimenface greatlystandard sa[3].
Anotherimplants inoride ions,has amicrotreatmentand uoridof dental imical surfacein compariimplants alsignicantl[50,51]. Thifurther impimplant su
Nevertheless, chemical treatments might reduce themechanical properties of titanium. For instance, acid-etchingcan lead to hydrogen embrittlement of the titanium, creatingmicro cracks on its surface that could reduce the fatigue resis-tance of the implants [53]. Indeed, experimental studies havereported the absorption of hydrogen by titanium in a biologi-cal environment. This hydrogen embrittlement of titanium isalso associated with the formation of a brittle hybrid phase,leading to a reduction in the ductility of the titanium. Thisphenomenon is related to the occurrence of fracture mecha-nisms in dental implants [53].
3.4. Roughening of implants by anodization
Micro- or nano-porous surfaces may also be produced bypotentiostatic or galvanostatic anodization of titanium instrong acids (H2SO4, H3PO4, HNO3, HF) at high current density
m2)hickeWheidend tlayero-poes my ofrath
s cuectrodizeespophom. A hed tsurfaropocking [55
aniummagen foxideto otummality
Fig. 4 SEM uoOsseoSpeed less bone resorption with dual acid-etchedmpared to machined or TPS surfaces [9,46,47].
cid-etching methods have been improved in ordere cell adhesion and bone neoformation. Highe acid-etching produces a homogeneous micro-face with higher bone-to-implant contact thanes in experimental studies [48,49]. The wettabil-surface has also been proposed to promote b-on. This brin adhesion provides contact guid-he osteoblasts migrating along the surface. Antal study has demonstrated that a hydrophilic sur-improved the bone/implant contact compared tond-blasted and acid-etched implants in minipigs
approach involves treating titanium dentaluoride solutions. Titanium is very reactive to u-
forming soluble TiF4 species. The surface producedrough topography as shown in Fig. 4. This chemicalof the titanium created both a surface roughnesse incorporation favorable to the osseointegrationplants [50,51]. It has been shown that this chem-treatment enhanced osteoblastic differentiation
son with control samples [52]. Fluoridated roughsowithstood greater push-out forces and showed ay higher torque removal than the control implantss chemical treatment may have the potential torove implant anchorage in bone by rendering therface bioactive.
(200A/is to tnium.the oxlines aoxideor nanproductallinitcess issuch aand el
Anobone rtomor[59,60]anodizniumbeen pinterlobondinthe tittion ofhas benium opared
In sthe qu
micrographs of treatment of titanium dental implants in adTM, France).or potential (100V). The result of the anodizationn the oxide layer to more than 1000nm on tita-n strong acids are used in an electrolyte solution,layer will be dissolved along current convectionhickened in other regions. The dissolution of thealong the current convection lines creates micro-res on the titanium surface [5457]. Anodizationodications in the microstructure and the crys-
the titanium oxide layer [58]. The anodization pro-er complex and depends on various parameters
rrent density, concentration of acids, compositionlyte temperature.d surfaces result in a strong reinforcement of thense with higher values for biomechanical and his-etric tests in comparison to machined surfacesigher clinical success rate was observed for the
itanium implants in comparison with turned tita-ces of similar shapes [61]. Two mechanisms havesed to explain this osseointegration: mechanicalg through bone growth in pores, and biochemical,62]. Modications to the chemical composition ofoxide layer have been tested with the incorpora-
nesium, calcium, sulfur or phosphorus [63,64]. Itund that incorporating magnesium into the tita-layer leads to a higher removal torque value com-
her ions [55].ary, surface roughness plays a major role in bothand rate of osseointegration of titanium dental
ride solution surface (Courtesy of Astratech
-
dental mater ials 2 3 ( 2 0 0 7 ) 844854 849
implants. Highly roughened implants such as TPS or grit-blasted have been shown to favor mechanical anchorageand primary xation to bone. Topographies in the nanome-ter range have been used to promote protein adsorption,osteoblastic cell adhesion and the rate of bone tissue healingin the peri-implant region.
4. Osteoconductive calcium phosphatecoatings on dental implants
Metal implants have been coated with layers of calciumphosphates mainly composed of hydroxyapatite. Followingimplantation, the release of calcium phosphate into the peri-implant region increases the saturation of body uids andprecipitates a biological apatite onto the surface of the implant[65,66]. Thinous proteiment and gimplant is tThe biologifaster withIt is well-reto better clititanium imdue to a supmethodshaspraying, sdepositionplasma-sprdental imp
Plasma-(HA) ceramtemperaturwhere theyPlasma-sprranging froto obtain mthemetalliblasting, w
The plassuch as ththe substrain the comphosphatehave been
tricalcium phosphates (- and -TCP), tetracalcium phos-phate, calcium oxide and amorphous calcium phosphate(ACP) [7375]. Plasma-sprayed HA coatings are usually com-posed of large crystalline HA particles embedded into a highlysoluble amorphous calcium phosphate phase. Moreover, theplasma-spraying technique is not very effective for coatingtiny dental implants with a complex shape.
Plasma-sprayed HA-coated dental implants have also beenassociated with clinical problems [6,7679]. One of the majorconcernswith plasma-sprayed coatings is the possible delam-ination of the coating from the surface of the titanium implantand failure at the implant-coating interface despite the factthat the coating is well-attached to the bone tissue. The dis-crepancy in dissolution between the various phases thatmakeup the coating has led to delamination, particle release andthus the clinical failure of implants [7679]. Coating delamina-
s bema-sts [6ally w
all odHAatededicmetates wts co
Fu
trateort ats. Te routiongs fobiolthe
Sur
emisthess, s
Fig. 5 SEM tingNetherlands layer of biological apatite might contain endoge-ns and serve as amatrix for osteogenic cell attach-rowth [67]. The bone healing process around theherefore enhanced by this biological apatite layer.cal xation of titanium implants to bone tissue isa calcium phosphate coating than without [68,69].cognized that calciumphosphate coatings have lednical success rates in the long-term than uncoatedplants [68,70]. These long-term success rates areerior initial rate of osseointegration [70]. Differentve beendeveloped to coatmetal implants: plasma-putter-deposition, solgel coating, electrophoreticor biomimetic precipitation. However, only theaying coating method has been used for titaniumlants in clinical practice.spraying is a technique in which hydroxyapatiteic particles are injected into a plasma torch at highe and projected on to the surface of the titaniumcondense and fuse together, forming a lm (Fig. 5).ayed coatings can be deposited with a thicknessm a few micrometers to a few millimeters. In orderechanical retention of the coating, the surface of
c implantmust be roughened, e.g. bymeans of grit-hen using this method.ma-spraying method has disadvantages, however,e porosity of the coating and residual stress atte/coating interface, as well as drastic changesposition and crystallinity of the initial calciumpowder [71,72]. Several calcium phosphate phasesobserved in plasma-sprayed HA coatings such as
tion haof plasimplanespecibone.
ForsprayeHA-coorthoptice, avival raimplan
5.
A few sthe shimplansurfacadsorpcoatintion ofcess in
5.1.
The chrole inerthele
micrographs of a plasma-sprayed hydroxyapatite (HA) coas).en reported in dental situations where the efcacypraying is not optimal due to the size of the dental]. Loosening of the coating has also been reported,hen the implants have been inserted into dense
f the above reasons, the clinical use of plasma--coated dental implants is limited. Plasma-sprayedprostheses are nevertheless highly successful ins. Despite their negative reputation in dental prac--analytic review did not show that long-term sur-ere inferior for plasma-sprayed HA-coated dentalmpared to other types of dental implant [78].
ture trends in dental implant surfaces
gies should be considered in order to improve bothnd long-term osseointegration of titanium dentalhese future trends concern the modications ofghness at thenanoscale level for promotingproteinand cell adhesion, biomimetic calcium phosphater enhancing osteoconduction and the incorpora-ogical drugs for accelerating the bone healing pro-peri-implant area.
face roughness at the nanoscale level
try and roughness of implant surfaces play amajorbiological events that follow implantation. Nev-urfaces are often developed using an empirical
surface (Courtesy of Cam Implants BV, The
-
850 dental mater ials 2 3 ( 2 0 0 7 ) 844854
alciu
approach wfaces currerange of thexact biolothe absencraphy at thand depth,standardizetions betwesurfaces mimplants.
Only aroughnessin a reprodprocessinglithographystudies [80osteoblastitures but ndirectly enment of thmayalso gitive attachselective atof initial he
5.2. Biotitanium de
In order toings (see Smethod insIn this biomphate apatlated body(Fig. 6). In oaqueous so
The rstphosphateinum anodconductedto the formconverted itrochemicabuffered ating directly
le peof coshory [86sec
of caSBFnd gt at. Inanceplanm hleatif cala t
he che htitaano, stanicaurfaitioniumlciumeenphyntina-sprts cogatee deeticFig. 6 SEM micrographs of a biomimetic c
ith in vitro and in vivo tests. Most of the sur-ntly available have random topographywith awideicknesses, from nanometers to millimeters. Thegical role of these features is unknown because ofe of standardized surfaces with repetitive topog-e nano-sized level (e.g. pits with xed diameterslanes with controlled proles). Such controlled ord surfaces might help to understand the interac-en specic proteins and cells. These standardizedight also promote early bone apposition on the
few studies have reported modications to theas well as the chemistry at the nanometer scaleucible manner. Most of these attempts have usedmethods from the electronic industry such asand surface laser-pitting. In vitro experimental
82] have demonstrated that the attachment ofc cells was enhanced on submicron scale struc-ot on smooth surfaces. Well-developed lopodiatered nanometer-sized pores for the initial attach-e osteoblastic cells. These nanometer structuresve the cells positive guidance bymeansof the selec-ment of osteoblasts to the implant surface. Thistachment processmight result in the improvementaling around dental implants.
mimetic calcium phosphate coatings onntal implants
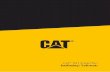
avoid the drawbacks of plasma-sprayed HA coat-ection 4), scientists have developed a new coatingpired by the natural process of biomineralization.imetic method, the precipitation of calcium phos-
ite crystals onto the titanium surface from simu-
possibkindsis veryefcac
Thetationsion ination aimplanditionsto enhthe imtitaniuas nuctions oto formstep, t[89]. Ton theing of nmatrixmechanium sIn addof calcoctacaIt has buble inlike deplasmimplaninvestiies havbiomimuids (SBF) formed a coating at room temperaturerder to accelerate the deposition of coatings fromlutions, several methods have been developed.method involves the electrodeposition of calciumby using a current, a titanium cathode and a plat-e [83,84]. This electrochemical method is usuallyin acidic calcium phosphate solutions and leadsation of brushite coatings which are subsequentlynto apatite by hydrothermal processing. The elec-l deposition performed in simulated body uidneutral pH can produce a carbonated apatite coat-on the titanium surfaces [85]. This method makes
titanium imtitanium dbeen compmodels.
5.3. Inctitanium de
The surfacbone-stimuto enhancethe transfom phosphate coating.
rfect control of the thickness of the deposit on allmplicated surfaces. The time required for coatingt and the process presents high reproducibility and,87].ond method is based on the biomimetic precipi-lcium phosphate on titanium surfaces by immer-. This method involves the heterogeneous nucle-rowth of bone-like crystals on the surface of thephysiological temperatures and under pH con-general, two subsequent steps have been usedthe heterogeneous nucleation of the CaP. First,ts are treated with an alkaline in order to formydroxyl groups on the titanium surface, to serveng points [88]. Others have used high concentra-cium and phosphate in an increasing pH solutionhin layer on the titanium surface. In the secondoating develops under crystal growth conditionseterogeneous nucleation and growth of the CaPnium surface is initiated by the chemical bond--sized clusters, forming an interfacial unstructuredbilized by the presence ofmagnesium ions [90]. Thel stability of the CaP coating requires a rough tita-ce to ensure themechanical stability of the coating., this physiological method broadens the varietyphosphate phases that can be deposited, such asphosphate or bone-like carbonate apatite [88,91].
shown that such biomimetic coatings aremore sol-siological uids and resorbable by osteoclastic cellsmaterials than high temperature coatings such asayed HA [91,92]. The osseointegration of titaniumatedwith biomimetic calciumphosphate has beend in pre-clinical comparative models. These stud-monstrated a higher bone-to-implant contact forcalcium phosphate coatings than for uncoated
plants [69,93]. However, the osseointegration of
ental implants coated biomimetically has not yetared with other surface treatments in pre-clinical
orporation of biologically active drugs intontal implants
e of titanium dental implants may be coated withlating agents such as growth factors in orderthe bone healing process locally. Members of
rming growth factor (TGF-) superfamily, and
-
dental mater ials 2 3 ( 2 0 0 7 ) 844854 851
in particular bone morphogenetic proteins (BMPs), TGF-1,platelet-derived growth factor (PDGF) and insulin-like growthfactors (IGFdates for thbeen incorpfrom a varis that theand not inadjunction[100]. Thisinserting pprotein. Innot be desi
The sumoleculesporation onates, mighsupport, e.recently thimplants inregion [101limited tostudies havbut only a[102,103]. OHA-coateddronate dearea [1041tained releasurface. Dufor calciumsorptive druthe biomimever, the iddeterminedsity is biph
6. Co
There aredental impcal efcacythese surfaand in vivousing diffeThe exactearly eventpoorly undies with diffuture of dfaces withistry. Thiscell and tisrelease ofimplant regwith poor bgies shouldof dental imsuccess.
Acknowledgements
uthofor, Rue
sseoSlandsmascoscar c
en
lbreksseonsurn mateineerioduserochrhem004;8haoochrespoateragnorope004;1iavaimonvaluareatm003;2arlsslasmmplaennre-trschaeochroneith atudy998;4ennistomach pmplausernueitaniuiniaotfrejortind mabbitennistomcrewurfacecket al. A-1 and 2) are some of the most promising candi-is purpose. Experimental data, inwhich BMPs haveorated into dental implants, have been obtained
iety of methodologies [9499]. The limiting factoractive product has to be released progressivelya single burst. Another possibility may be the
of a plasmid containing the gene coding for a BMPpossibility is limited due to the poor efcacy oflasmids into the cells and the expression of theaddition, overproduction of BMPs by cells mightrable after the bone healing process.rface of implants could also be loaded withcontrolling the bone remodeling process. Incor-f bone antiresorptive drugs, such as biphospho-t be very relevant in clinical cases lacking boneg. resorbed alveolar ridges. It has been shownat a biphosphonate incorporated on to titaniumcreased bone density locally in the peri-implant]. The effect of the antiresorptive drug seems to bethe vicinity of the implant. Experimental in vivoe demonstrated the absence of negative effectsslight increase in dental implant osseointegrationther experimental studies using plasma-sprayeddental implants immersed in pamidronate or zole-monstrated a signicant increase in bone contact06]. The main problem lies in the grafting and sus-se of antiresorptive drugs on the titanium implante to the high chemical afnity of biphosphonatesphosphate surfaces, incorporation of the antire-g on to dental implants could be achieved by usingetic coating method at room temperatures. How-eal dose of antiresorptive drug will have to bebecause the increase in peri-implant bone den-
osphonate concentration-dependent [106].
nclusion
a number of surfaces commercially available forlants. Most of these surfaces have proven clini-(>95% over 5 years). However, the development ofceshas beenempirical, requiringnumerous in vitrotests. Most of these tests were not standardized,
rent surfaces, cell populations or animal models.role of surface chemistry and topography on thes of the osseointegration of dental implants remainerstood. Furthermore, comparative clinical stud-ferent implant surfaces are rarely performed. Theental implantology should aim at developing sur-controlled and standardized topography or chem-approach is the only way to understand protein,sue interactions with implant surfaces. The localbone-stimulating or resorptive drugs in the peri-ionmay also respond to difcult clinical situationsone quality and quantity. These therapeutic strate-ultimately enhance the osseointegration processplants for their immediate loading and long-term
The aland)Zenecaand ONetherHA plathe Migramm
r e f e r
[1] AOei
[2] SP
[3] BCc2
[4] ZCrM
[5] Bp2
[6] GRet2
[7] CpI
[8] Wpi
[9] CBws1
[10] WheI
[11] BItm
[12] GHar
[13] WHss
[14] Bers acknowledge Straumann AG (Bern, Switzer-providing the SLA samples, Astra Tech (Astrail-Malmaison, France) for providing theTiOblastTM
peedTM samples. Cam Implants BV (Leiden, Thes) is also acknowledged for providing the TPS and-sprayed samples. We also thank Paul Pilet fromopy Centre for SEM pictures and Kirsty Snaith fororrections of the manuscript.
c e s
tsson T, Branemark PI, Hansson HA, Lindstrom J.integrated titanium implants. Requirements foring a long-lasting, direct bone-to-implant anchoragen. Acta Orthop Scand 1981;52(2):15570.mann S. Titanium-the material of choice?ontology 2000 1998;17:721.D, Broggini N, Wieland M, Schenk RK, Denzer AJ,an DL, et al. Enhanced bone apposition to aically modied SLA titanium surface. J Dent Res3:52933.G, Schwartz Z, Wieland M, Rupp F, Geis-Gerstorfer J,an DL, et al. High surface energy enhances cellnse to titanium substrate microstructure. J BiomedRes A 2005;74:4958.A, Di Bello C. Surface treatments and roughnessrties of Ti-based biomaterials. J Mater Sci Mater Med5:93549.resi G, Fini M, Cigada A, Chiesa R, Rondelli G,dini L, et al. Mechanical and histomorphometrictions of titanium implants with different surfaceents inserted in sheep cortical bone. Biomaterials4:158394.on L, Albrektsson T, Berman C. Bone response toa-cleaned titanium implants. Int J Oral Maxillofacnts 1989;4:199204.erberg A, Bolind P, Albrektsson T. Glow dischargeeated implants combined with temporary bonemia. Swed Dent J 1991;15:95101.an DL, Schenk RK, Lussi A, Higginbottom FL, Buser D.response to unloaded and loaded titanium implantssandblasted and acid-etched surface: a histometricin the canine mandible. J Biomed Mater Res0:111.erberg A, Hallgren C, Johansson C, Danelli S. Aorphometric evaluation of screw-shaped implantsrepared with two surface roughnesses. Clin Oralnts Res 1998;9:119.D, Schenk R, Steinemann S, Fiorellini J, Fox C, Stich H.nce of surface characteristics on bone integration ofm implants. A histomorphometric study inture pigs. J Biomed Mater Res 1991;25:889902.dsen K, Wennerberg A, Johansson C, Skovgaard LT,ng-Hansen E. Anchorage of TiO2-blasted, HA-coated,achined implants: an experimental study withs. J Biomed Mater Res 1995;29:122331.erberg A, Albrektsson T, Albrektsson B, Krol JJ.orphometric and removal torque study of
-shaped titanium implants with three differente topographies. Clin Oral Implant Res 1996;6:2430.r W, Becker BE, Ricci A, Bahat O, Rosenberg E, Rose LF,prospective multicenter clinical trial comparing
-
852 dental mater ials 2 3 ( 2 0 0 7 ) 844854
one- and two-stage titanium screw-shaped xtures withone-sImpla
[15] Albrekimpla2005;7
[16] Hanssroughbone-Biome
[17] Testomultifour-y2001;1
[18] ConneD. Guplasmimpla
[19] EsposIntervdenta2005;2
[20] BrettRough2004;3
[21] UrbanPeochspleenknee
[22] Brownpretre2000;2
[23] MartiTinitiuoroimpla
[24] Roccuof sanprospImpla
[25] Taba JDB, Pawith din dog
[26] Ong JLplasmimpla
[27] ApariCorroblastefor de2003;2
[28] IvanoA. HisblasteClin O
[29] RasmdesignstabilImpla
[30] Gotfrexedmach2001;1
[31] Rasmof titaRelat
[32] van SI. A pr
screw-shaped self-tapping pure titanium implant systems.lin Ostranrondrospear. Cbronvaluopogodeovaeistombtainlacedaxiliateliatelater
abbituelll. Evaurfacarticassaielaf comompingeeanf ostcale-ong
urfacater995;2ho Snsertiomaark Jith t000;1risi Pone-urfaceriodavierosthrisi Pnd bontaeriodrisi Pith m
n hum003;2ochraylorimesSLA)mplaovaeajiwsseoeriodogs.apalajiwynamlacedtage plasma-sprayed solid-screw xtures. Clinnt Dent Relat Res 2000;2:15965.tsson T, Wennerberg A. The impact of oralntspast and future, 19662042. J Can Dent Assoc1:327.on S, Norton M. The relation between surfaceness and interfacial shear strength foranchored implants. A mathematical model. Jch 1999;32:82936.ri T, Wiseman L, Woolfe S, Porter S. A prospectivecenter clinical study of the Osseotite implant:ear interim report. Int J Oral Maxillofac Implants6:193200.r K, Sabatini R, Mealey B, Takacks V, Mills M, Cochran
ided bone regeneration around titaniuma-sprayed, acid-etched and hydroxyapatite-coatednts in the canine model. J Periodontol 2003;74:65868.ito M, Coulthard P, Thomsen P, Worthington HV.entions for replacing missing teeth: different types ofl implants. Cochrane Database Syst Rev5:CD003815.PM, Harle J, Salih V, Mihoc R, Olsen I, Jones FH, et al.ness response genes in osteoblasts. Bone5:12433.RM, Jacobs JJ, Tomlinson MJ, Gavrilovic J, Black J,M. Dissemination of wear particles to the liver,and abdominal lymph nodes of patients with hip or
replacement. J Bone Jt Surg Am 2000;82:45777.e M, Gregson PJ. Effect of mechanical surfaceatment on metal ions release. Biomaterials1:38592.ni D, Fini M, De Pasquale V, Bacchelli B, Gamberini M,A, et al. Detachment of titanium andhydroxyapatite particles in unloaded endosseousnts. Biomaterials 2003;24:130916.zzo M, Bunino M, Prioglio F, Bianchi SD. Early loadingdblasted and acid-etched (SLA) implants: aective split-mouth comparative study. Clin Oralnts Res 2001;12:5728.unior M, Novaes Junior AB, Souza SL, Grisi MF, Paliotordini LC. Radiographic evaluation of dental implantsifferent surface treatments: an experimental studys. Implant Dent 2003;12:2528., Carnes DL, Bessho K. Evaluation of titaniuma-sprayed and plasma-sprayed hydroxyapatitents in vivo. Biomaterials 2004;25:46016.cio C, Gil FJ, Fonseca C, Barbosa M, Planell JA.sion behavior of commercially pure titanium shotd with different materials and size of shot particlesntal implant applications. Biomaterials4:26373.ff CJ, Hallgren C, Widmark G, Sennerby L, Wennerbergtologic evaluation of the bone integration of TiO(2)d and turned titanium microimplants in humans.ral Implants Res 2001;12:12834.usson L, Kahnberg KE, Tan A. Effects of implantand surface on bone regeneration and implant
ity: an experimental study in the dog mandible. Clinnt Dent Relat Res 2001;3:28.dsen K, Karlsson U. A prospective 5-year study ofpartial prostheses supported by implants withined and TiO2-blasted surface. J Prosthodont0:27.usson L, Roos J, Bystedt H. A 10-year follow-up studynium dioxide-blasted implants. Clin Implant DentRes 2005;7:3642.teenberghe D, De Mars G, Quirynen M, Jacobs R, Naertospective split-mouth comparative study of two
C[33] A
Gpy
[34] AEtm
[35] NHopM
[36] PPmr
[37] Masp
[38] MWoc
[39] ZJos
[40] Wsm1
[41] CiB
[42] Pw2
[43] TBsP
[44] DP
[45] TacP
[46] Twi2
[47] CTt(i
[48] NKopd
[49] PKdpral Implants Res 2000;11:2029.d P, Engquist B, Dahlgren S, Engquist E, Feldmann H,ahl K. Astra Tech and Branemark System implants: aective 5-year comparative study. Results after onelin Implant Dent Relat Res 1999;1:1726.A, Hopfensperger M, Thompson J, Cooper L.
ation of a predictive model for implant surfaceraphy effects on early osseointegration in the rat tibial. J Prosth Dent 2001;85:406.s A, Souza S, de Oliveira P, Souza A.orphometric analysis of the bone-implant contacted with 4 different implant surface treatmentsside by side in the dog mandible. Int J Oral
lofac Implants 2002;17:37783.li M, Scarano A, Paolantonio M, Iezzi G, Petrone G,li A. Bone response to machined and resorbable blastial titanium implants: an experimental study ins. J Oral Implantol 2002;28:28.er WD, Gross U, Fritz T, Voigt C, Fischer P, Berger G, etluation of the interface between bone and titaniumes being blasted by aluminium oxide or bioceramicles. Clin Oral Implants Res 2003;3:34956.ro C, Rotolo F, De Riccardis F, Milella E, Napoli A,nd M, et al. Comparative investigation of the surfacemercial titanium dental implants. Part 1: chemical
osition. J Mater Sci Mater Med 2002;13:53548.r O, Anselme K, Denzer A, Habersetzer P, Wieland M,ls J, et al. Time-dependent morphology and adhesioneoblastic cells on titanium model surfaces featuringresolved topography. Biomaterials 2004;25:2695711.M, Eulenberger J, Schenk R, Hunziker E. Effect ofe topology on the osseointegration of implantials in trabecular bone. J Biomed Mater Res9:156775.A, Park KT. The removal torque of titanium screwed in rabbit tibia treated by dual acid etching.terials 2003;24:36117.Y, Davies JE. Red blood cell and platelet interactionsitanium implant surfaces. Clin Oral Implants Res1:5309., Lazzara R, Rebaudi A, Rao W, Testori T, Porter SS.implant contact on machined and dual acid-etchedes after 2 months of healing in the human maxilla. Jontol 2003;74:94556.s JE. Mechanisms of endosseous integration. Int Jodont 1998;11:391401., Lazzara R, Rao W, Rebaudi A. Bone-implant contactone quality: evaluation of expected and actual bonect on machined and osseotite implant surfaces. Int Jontics Restorative Dent 2002;22:53545., Marcato C, Todisco M. Bone-to-implant appositionachined and MTX microtextured implant surfacesan sinus grafts. Int J Periodontics Restorative Dent
3:42737.an DL, Buser D, ten Bruggenkate CM, Weingart D,TM, Bernard JP, et al. The use of reduced healingon ITI implants with a sandblasted and acid-etchedsurface: early results from clinical trials on ITI SLAnts. Clin Oral Implants Res 2002;13:14453.s Jr AB, Papalexiou V, Grisi MF, Souza SS, Taba Jr M,ara JK. Inuence of implant microstructure on theintegration of immediate implants placed inontally infected sites. A histomorphometric study inClin Oral Implants Res 2004;15:3443.exiou V, Novaes Jr AB, Grisi MF, Souza SS, Taba Jr M,ara JK. Inuence of implant microstructure on theics of bone healing around immediate implantsinto periodontally infected sites. A confocal laser
-
dental mater ials 2 3 ( 2 0 0 7 ) 844854 853
scanning microscopic study. Clin Oral Implants Res2004;1
[50] EllinguoridMed 1
[51] EllingImprouoridImpla
[52] CoopeFluoriboneendos
[53] YokoyK. Frain den
[54] Sul YTAlbrekthe bo
[55] Sul YTAlbrekimplachemstruct
[56] XiropaMD, Wphosp(TiUni2005;1
[57] HuangWikes(TiUniRes 20
[58] Sul YTand qanodi
[59] Sul YTT. ResimplaOral Im
[60] RocciBranein theclinica
[61] Jungnimplatitaniuimplawith eOral Im
[62] SchupLundgimplamicroand edenta
[63] Sul YTscrewrabbit
[64] Sul YTcalciueffectImpla
[65] de Grocoatin1998;2
[66] Daculart ofMater
[67] Davies JE. Understanding peri-implant endosseous healing.Dentorrieasuon-Heriodarrer, LayoatinemureursK. Inharaaxililiaggnterfmplaadinalciun ine Grydromplaim YommabstreGerautisA cohee
itaniuylind996;1hangorphith v999;5ee J,mpla000;5insleydroemovral Imnselroovrowtigereost Aurfacsteobhu X, Kernubmells Tangeposurfac003;2angf bioiomaang
harahosp004;8an Sitaniuuid.5:4453.sen JE. Pre-treatment of titanium implants withe improves their retention in bone. J Mater Sci Mater995;6:74958.sen JE, Johansson CB, Wennerberg A, Holmen A.ved retention and bone-to-implant contact withe-modied titanium implants. Int J Oral Maxillofacnts 2004;19:65966.r LF, Takabe J, Guo J, Abron A, Holmen A, Ellingsen JE.de modication effects on osteoblast behavior andformation at TiO(2) grit-blasted c.p. titaniumseous implants. Biomaterials 2006;27:92636.ama K, Ichikawa T, Murakami H, Miyamoto Y, Asaokacture mechanisms of retrieved titanium screw threadtal implants. Biomaterials 2002;23:245965., Johansson CB, Jeong Y, Roser K, Wennerberg A,tsson T. Oxidized implants and their inuence onne response. J Mater Sci Mater Med 2001;12:102531., Johansson C, Wennerberg A, Cho LR, Chang BS,tsson T. Optimum surface properties of oxidizednts for reinforcement of osseointegration: surfaceistry, oxide thickness, porosity, roughness, and crystalure. Int J Oral Maxillofac Implants 2005;20:34959.idis AV, Qahash M, Lim WH, Shanaman RH, Rohrerikesjo UM, et al. Bone-implant contact at calciumhate-coated and porous titanium oxidete)-modied oral implants. Clin Oral Implants Res6:5329.YH, Xiropaidis AV, Sorensen RG, Albandar JM, Hall J,
jo UM. Bone formation at titanium porous oxidete) oral implants in type IV bone. Clin Oral Implants05;16:10511., Johansson CB, Roser K, Albrektsson T. Qualitativeuantitative observations of bone tissue reactions tosed implants. Biomaterials 2002;23:180917., Johansson CB, Jeong Y, Wennerberg A, Albrektssononance frequency and removal torque analysis ofnts with turned and anodized surface oxides. Clinplants Res 2002;13:2529.
A, Martignoni M, Gottlow J. Immediate loading ofmark System TiUnite and machined-surface implantsposterior mandible: a randomized open-endedl trial. Clin Implant Dent Relat Res 2003;5:S5763.er M, Lundqvist P, Lundgren S. Oxidized titaniumnts (Nobel Biocare TiUnite) compared with turnedm implants (Nobel Biocare mark III) with respect tont failure in a group of consecutive patients treatedarly functional loading and two-stage protocol. Clinplants Res 2005;16:30812.
bach P, Glauser R, Rocci A, Martignoni M, Sennerby L,ren A, et al. The human bone-oxidized titaniumnt interface: a light microscopic, scanning electronscopic, back-scatter scanning electron microscopic,nergy-dispersive X-ray study of clinically retrievedl implants. Clin Implant Dent Relat Res 2005;7:S3643., Johansson CB, Albrektsson T. Oxidized titaniums coated with calcium ions and their performance inbone. Int J Oral Maxillofac Implants 2002;17:62534., Byon ES, Jeong Y. Biomechanical measurements ofm-incorporated oxidized implants in rabbit bone:of calcium surface chemistry of a novel implant. Clinnt Dent Relat Res 2004;6:10110.ot K, Wolke JG, Jansen JA. Calcium phosphategs for medical implants. Proc Inst Mech Eng12:13747.si G, Laboux O, Malard O, Weiss P. Current state of thebiphasic calcium phosphate bioceramics. J Mater SciMed 2003;14:195200.
J[68] M
mnP
[69] BKcf
[70] GMcM
[71] Fii
[72] Rco
[73] DhI
[74] Kc[
[75] LBH
[76] Wtc1
[77] Cmw1
[78] Li2
[79] ThrO
[80] Agg
[81] BIso
[82] ZJsC
[83] Wds2
[84] YoB
[85] Wcp2
[86] BtEduc 2003;67:93249.s HF, Ochi S, Spray JR, Olson JW. Periodontal-typerements associated with hydroxyapatite-coated andA-coated implants: uncovering to 36 months. Annontol 2000;5:5667.e F, van der Valk CM, Meijer G, Dalmeijer RA, de Grootrolle P. Osteointegration of biomimetic apatiteg applied onto dense and porous metal implants ins of goats. J Biomed Mater Res 2003;67:65565.NC, Jeffcoat RL, McGlumphy EA, Reddy MS, Jeffcoatuence of implant geometry and surfacecteristics on progressive osseointegration. Int J Orallofac Implants 2002;17:8115.i MJ, Coombs NA, Pilliar RM. Characterization of theace in the plasma-sprayed HA coating/Ti-Al6-4Vnt system. J Biomed Mater Res 1991;25:121130.S, Ducheyne P. Plasma spraying induced changes ofm phosphate ceramic characteristics and the effectvitro stability. Mater Med 1992;3:3342.oot K, Wolke JCG, Jansen JA. State of the art:xylapatite coatings for dental implants. J Oralnt 1994;20:2324., LeGeros J, LeGeros RZ. Characterization ofercial HA-coated implants. J Dent Res 1994;73:137act no. 287].os RZ, LeGeros JP, Kim Y, Kijkowska R, Zheng R,ta C, et al. Calcium phosphates in plasma-sprayedatings. Ceram Trans 1995;48:17389.ler S. Eight-year clinical retrospective study ofm plasma-sprayed and hydroxyapatite-coateder implants. Int J Oral Maxillofac Implants1:34050.YL, Lew D, Park JB, Keller JC. Biomechanical andometric analysis of hydroxyapatite-coated implantsarying cristallinity. J Oral Maxillofac Surg7:1096108.Rouhfar L, Beirne O. Survival of hydroxypatite-coatednts: a meta-analytic review. J Oral Maxillofac Surg8:13729 [discussion 137980].y D, Watson C, Russell J. A comparison ofxyapatite coated implant retained xed andable mandibular prostheses over 4 to 6 years. Clinplant Res 2001;12:15966.
me K, Bigerelle M, Noel B, Iost A, Hardouin P. Effect ofed titanium substratum on human osteoblastic cellh. J Biomed Mater Res 2002;60:52940.lle M, Anselme K, Noel B, Ruderman I, Hardouin P,. Improvement in the morphology of Ti-basedes: a new process to increase in vitro humanlast response. Biomaterials 2002;23:156377., Chen J, Scheideler L, Altebaeumer T, Geis-GerstorferD. Cellular reactions of osteoblasts to micron- and
icron-scale porous structures of titanium surfaces.issues Organs 2004;178:1322.X, Yan W, Hayakawa S, Tsuru K, Osaka A. Apatiteition on thermally and anodically oxidized titaniumes in a simulated body uid. Biomaterials4:46317.B, Uchida M, Kim HM, Zhang X, Kokubo T. Preparationactive titanium metal via anodic oxidation treatment.terials 2004;25:100310.J, de Boer J, de Groot K. Preparation andcterization of electrodeposited calciumhate/chitosan coating on Ti6Al4V plates. J Dent Res3:296301., Maruno S. Deposition of calcium phosphate onm by electrochemical process in simulated body
Jpn J Appl Phys 1993;32:157780.
-
854 dental mater ials 2 3 ( 2 0 0 7 ) 844854
[87] Sena LA, Andrade MC, Rossi AM, Soares GA. Hydroxyapatitedeposition by electrophoresis on titanium sheets withdifferent surface nishing. J Biomed Mater Res 2002;60:17.
[88] Kokubo T, Kushitani H, Abe Y, Yamamuro T. Apatite coatingon various substrates in simulated body uids. Bioceramics1989;2:23542.
[89] Habibovic P, Barre`re F, van Blitterswijk CA, de Groot K,Layrolle P. Biomimetic hydroxyapatite coating on metalimplants. J Am Ceram Soc 2002;85:51722.
[90] Barrere F, Snel M, Van Blitterswijk C, de Groot K, Layrolle P.Nano-scale study of the nucleation and growth of calciumphosphate coating on titanium implants. Biomaterials2004;25:290110.
[91] Barrere F, van der Valk CM, Dalmeijer RA, van BlitterswijkCA, de Groot K, Layrolle P. In vitro and in vivo degradationof biomimetic octacalcium phosphate and carbonateapatite coatings on titanium implants. J Biomed Mater Res2003;64:37887.
[92] Leeuwenburgh S, Layrolle P, Barre`re F, de Bruijn J,Schoonman J, van Blitterswijk CA, et al. Osteoclasticresorption of biomimetic calcium phosphate coatings invitro. J Biomed Mater Res 2001;56:20815.
[93] Habibovic P, Li J, van der Valk CM, Meijer G, Layrolle P, vanBlitterswijk CA, et al. Biological performance of uncoatedand octacalcium phosphate-coated Ti6Al4V. Biomaterials2005;26:2336.
[94] Bessho K, Carnes DL, Cavin R, Chen HY, Ong JL. BMPstimulation of bone response adjacent to titaniumimplants in vivo. Clin Oral Implants Res 1999;10:2128
[95] WikesRhBMridgeClin Im
[96] TatakUM. Phumadose-
[97] StenpC, Albgrowtimpla
experimental study in dogs. Clin Oral Implants Res2003;14:21925.
[98] Boyne P, Jones SD. Demonstration of the osseoinductiveeffect of bone morphogenetic protein within endosseousdental implants. Implant Dent 2004;13:1804.
[99] Liu Y, de Groot K, Hunziker EB. BMP-2 liberated frombiomimetic implant coatings induces and sustains directossication in an ectopic rat model. Bone 2005;36:74557.
[100] Huang YC, Simmons C, Kaigler D, Rice KG, Mooney DJ. Boneregeneration in a rat cranial defect with delivery ofPEI-condensed plasmid DNA encoding for bonemorphogenetic protein-4 (BMP-4). Gene Ther2005;12:41826.
[101] Josse S, Faucheux C, Soueidan A, Grimandi G, Massiot D,A1onso B, et al. Chemically modied calcium phosphatesas novel materials for bisphosphonate delivery. Adv Mater2004;16:14237.
[102] Meraw SJ, Reeve CM. Qualitative analysis of peripheralperi-implant bone and inuence of alendronate sodium onearly bone regeneration. J Periodontol 1999;70:122833.
[103] Meraw SJ, Reeve CM, Wollan PC. Use of alendronate inperi-implant defect regeneration. J Periodontol1999;70:1518.
[104] Yoshinari M, Oda Y, Ueki H, Yokose S. Immobilization ofbisphosphonates on surface modied titanium.Biomaterials 2001;22:70915.
[105] Kajiwara H, Yamaza T, Yoshinari M, Goto T, Iyama S, AtsutaI, et al. The bisphosphonate pamidronate on the surface oftitanium stimulates bone formation around tibial implantsn rateteralciuoledoneabburfacentaiointerrazantoydroA/Ca.jo UM, Sorensen RG, Kinoshita A, Wozney JM.P-2/alphaBSM induces signicant vertical alveolaraugmentation and dental implant osseointegration.plant Dent Relat Res 2002;4:17482.
is DN, Koh A, Jin L, Wozney JM, Rohrer MD, Wikesjoeri-implant bone regeneration using recombinantn bone morphogenetic protein-2 in a canine model: aresponse study. J Periodontal Res 2002;37:93100.ort VF, Roos-Jansaker AM, Renvert S, Kuboki Y, Irwinrektsson T, et al. Failure to induce supracrestal boneh between and around partially inserted titaniumnts using bone morphogenetic protein (BMP): an
i[106] P
CzB
[107] MSdB
[108] FShHs. Biomaterials 2005;26:5817.B, Pioletti DP, Laib S, Bujoli B, Pilet P, Janvier P, et al.m phosphate drug delivery system: inuence of localronate release on bone implant osteointegration.2005;36:5260.oux F, Ponsonnet L, Morrier JJ, Jaffrezic N, Barsotti O.e free energy and bacterial retention to saliva-coatedl implant materialsan in vitro study. Colloids Surf Berfaces 2004;39:199205.MP, Monteiro FJ, Serro AP, Saramago B, Gibson IR,
s JD. Effect of chemical composition onphobicity and zeta potential of plasma sprayedO-P2O5 glass coatings. Biomaterials 2001;22:310512.
Surface treatments of titanium dental implants for rapid osseointegrationIntroductionChemical composition of the surface of dental implantsSurface roughness of dental implantsRoughening of implants by titanium plasma-sprayingRoughening of implants by grit-blastingRoughening of implants by acid-etchingRoughening of implants by anodization
Osteoconductive calcium phosphate coatings on dental implantsFuture trends in dental implant surfacesSurface roughness at the nanoscale levelBiomimetic calcium phosphate coatings on titanium dental implantsIncorporation of biologically active drugs into titanium dental implants
ConclusionAcknowledgementsReferences
Related Documents