Biological Psychology 99 (2014) 115–124 Contents lists available at ScienceDirect Biological Psychology jo ur nal home p age: www.elsevier.com/locate/biopsycho Impaired upper alpha synchronisation during working memory retention in depression and depression following traumatic brain injury Neil W. Bailey ∗ , Rebecca A. Segrave, Kate E. Hoy, Jerome J. Maller, Paul B. Fitzgerald Monash Alfred Psychiatry Research Centre, The Alfred Hospital and Monash University, Central Clinical School, Melbourne, VIC, Australia a r t i c l e i n f o Article history: Received 3 August 2013 Accepted 21 March 2014 Available online 28 March 2014 Keywords: Traumatic brain injury Major depression Working memory EEG Alpha a b s t r a c t Rates of major depressive disorder (MDD) following traumatic brain injury (TBI) are higher than in the general population. Individuals with depression following traumatic brain injury (TBI-MDD) exhibit working memory (WM) impairments. Electrophysiological evidence has suggested that parieto-occipital upper alpha synchronisation may enhance WM retention by inhibiting irrelevant processes. The current research assessed whether retention period WM parieto-occipital upper alpha activity is disrupted in groups with TBI-only (N = 20), MDD (N = 17), and TBI-MDD (N = 15) compared to healthy controls (N = 31). Behavioural data indicated poorer performance in MDD and TBI-MDD. Parietal-occipital upper alpha was reduced in the MDD and TBI-MDD groups, but was unaffected in TBI-only. These results suggest inhibitory deficits may account for WM impairments in MDD and TBI-MDD, and that for individuals with TBI-MDD it may be the depression rather than the TBI that impairs WM. © 2014 Elsevier B.V. All rights reserved. 1. Introduction Following traumatic brain injury (TBI), rates of major depressive disorder (MDD) are higher than in the general population. Esti- mates suggest rates of 20–45% measured at time points between 3-months and 30-years post-injury, compared with an annual prevalence of between 5% and 10% for the general population (Jorge et al., 1993; Kreutzer, Seel, & Gourley, 2001; Pagulayan, Hoffman, Temkin, Machamer, & Dikmen, 2008; World Health Organisation, 2001). MDD has been shown to have a negative impact on out- comes following TBI, including cognitive outcomes (Rapoport, Kiss, & Feinstein, 2006; Satz et al., 1998). One aspect of cognition frequently impaired in TBI, MDD, and their co-occurrence is working memory (WM) (Burt, Zembar, & Niederehe, 1995; Chuah, Maybery, & Fox, 2004; Jorge et al., 2004). Electroencephalography (EEG) can be used to measure brain activ- ity related to effective WM performance. In particular, an increase in synchronous upper alpha activity (10–12.5 Hz) in the parieto- occipital region is thought to represent inhibition of non-relevant information (Jensen, Gelfand, Kounios, & Lisman, 2002; Klimesch, Sauseng, & Hanslmayr, 2007). Jensen and Mazaheri (2010) propose the mechanism by which the alpha rhythm generates it’s inhibitory ∗ Corresponding author at: Monash Alfred Psychiatry Research Centre, Level 4, 607 St Kilda Road, Melbourne, VIC, 3004, Australia. Tel.: +61 3 9076 8691. E-mail address: [email protected] (N.W. Bailey). action is via disruption of ongoing gamma synchronisation, pre- venting gamma from binding information between areas. This may prevent WM retention from interference by activity in non-WM related regions. Evidence suggests that alpha activity is disrupted following TBI and in individuals with MDD. Following TBI, research has found reduced alpha desynchronisation during motor inhibition (Dockree et al., 2004), reduced resting alpha peak frequency (Angelakis, Lubar, Stathopoulou, & Kounios, 2004), and reduced inter-regional alpha coherence during WM encoding, retention, and retrieval (Kumar, Rao, Chandramouli, & Pillai, 2009). However, no research has directly examined parieto-occipital upper alpha power during WM retention in this population. It has been suggested that alpha alterations post-TBI are related to anxiety and mood rather than the injury itself (Nuwer, Hovda, Schrader, & Vespa, 2005), so we are currently uncertain as to the effect of mild to moderate TBI- alone on WM retention alpha. Research focusing on MDD, however, has examined upper alpha activity specifically during WM. Segrave et al. (2010) measured WM with the Sternberg task (which is con- structed so that information encoding, retention, and recall periods are temporally separate, enabling researchers to isolate each pro- cess), and found increased upper alpha activity in MDD over the left parieto-occipital region during the retention period. Currently, no research has examined WM alpha activity in individuals with TBI-MDD. http://dx.doi.org/10.1016/j.biopsycho.2014.03.008 0301-0511/© 2014 Elsevier B.V. All rights reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Irb
NM
a
ARAA
KTMWEA
1
dm3peT2c&
tNEiioiSt
6
h0
Biological Psychology 99 (2014) 115–124
Contents lists available at ScienceDirect
Biological Psychology
jo ur nal home p age: www.elsev ier .com/ locate /b iopsycho
mpaired upper alpha synchronisation during working memoryetention in depression and depression following traumaticrain injury
eil W. Bailey ∗, Rebecca A. Segrave, Kate E. Hoy, Jerome J. Maller, Paul B. Fitzgeraldonash Alfred Psychiatry Research Centre, The Alfred Hospital and Monash University, Central Clinical School, Melbourne, VIC, Australia
r t i c l e i n f o
rticle history:eceived 3 August 2013ccepted 21 March 2014vailable online 28 March 2014
a b s t r a c t
Rates of major depressive disorder (MDD) following traumatic brain injury (TBI) are higher than inthe general population. Individuals with depression following traumatic brain injury (TBI-MDD) exhibitworking memory (WM) impairments. Electrophysiological evidence has suggested that parieto-occipitalupper alpha synchronisation may enhance WM retention by inhibiting irrelevant processes. The current
eywords:raumatic brain injuryajor depressionorking memory
EGlpha
research assessed whether retention period WM parieto-occipital upper alpha activity is disrupted ingroups with TBI-only (N = 20), MDD (N = 17), and TBI-MDD (N = 15) compared to healthy controls (N = 31).Behavioural data indicated poorer performance in MDD and TBI-MDD. Parietal-occipital upper alpha wasreduced in the MDD and TBI-MDD groups, but was unaffected in TBI-only. These results suggest inhibitorydeficits may account for WM impairments in MDD and TBI-MDD, and that for individuals with TBI-MDDit may be the depression rather than the TBI that impairs WM.
. Introduction
Following traumatic brain injury (TBI), rates of major depressiveisorder (MDD) are higher than in the general population. Esti-ates suggest rates of 20–45% measured at time points between
-months and 30-years post-injury, compared with an annualrevalence of between 5% and 10% for the general population (Jorget al., 1993; Kreutzer, Seel, & Gourley, 2001; Pagulayan, Hoffman,emkin, Machamer, & Dikmen, 2008; World Health Organisation,001). MDD has been shown to have a negative impact on out-omes following TBI, including cognitive outcomes (Rapoport, Kiss,
Feinstein, 2006; Satz et al., 1998).One aspect of cognition frequently impaired in TBI, MDD, and
heir co-occurrence is working memory (WM) (Burt, Zembar, &iederehe, 1995; Chuah, Maybery, & Fox, 2004; Jorge et al., 2004).lectroencephalography (EEG) can be used to measure brain activ-ty related to effective WM performance. In particular, an increasen synchronous upper alpha activity (10–12.5 Hz) in the parieto-ccipital region is thought to represent inhibition of non-relevant
nformation (Jensen, Gelfand, Kounios, & Lisman, 2002; Klimesch,auseng, & Hanslmayr, 2007). Jensen and Mazaheri (2010) proposehe mechanism by which the alpha rhythm generates it’s inhibitory∗ Corresponding author at: Monash Alfred Psychiatry Research Centre, Level 4,07 St Kilda Road, Melbourne, VIC, 3004, Australia. Tel.: +61 3 9076 8691.
E-mail address: [email protected] (N.W. Bailey).
ttp://dx.doi.org/10.1016/j.biopsycho.2014.03.008301-0511/© 2014 Elsevier B.V. All rights reserved.
© 2014 Elsevier B.V. All rights reserved.
action is via disruption of ongoing gamma synchronisation, pre-venting gamma from binding information between areas. This mayprevent WM retention from interference by activity in non-WMrelated regions.
Evidence suggests that alpha activity is disrupted following TBIand in individuals with MDD. Following TBI, research has foundreduced alpha desynchronisation during motor inhibition (Dockreeet al., 2004), reduced resting alpha peak frequency (Angelakis,Lubar, Stathopoulou, & Kounios, 2004), and reduced inter-regionalalpha coherence during WM encoding, retention, and retrieval(Kumar, Rao, Chandramouli, & Pillai, 2009). However, no researchhas directly examined parieto-occipital upper alpha power duringWM retention in this population. It has been suggested that alphaalterations post-TBI are related to anxiety and mood rather thanthe injury itself (Nuwer, Hovda, Schrader, & Vespa, 2005), so weare currently uncertain as to the effect of mild to moderate TBI-alone on WM retention alpha. Research focusing on MDD, however,has examined upper alpha activity specifically during WM. Segraveet al. (2010) measured WM with the Sternberg task (which is con-structed so that information encoding, retention, and recall periodsare temporally separate, enabling researchers to isolate each pro-cess), and found increased upper alpha activity in MDD over theleft parieto-occipital region during the retention period. Currently,
no research has examined WM alpha activity in individuals withTBI-MDD.
1 l Psychology 99 (2014) 115–124
aipcefaY
2
2
wm(TwAaati
ccso&pImeaTtarnlunwiCofNt
2
OiwwbH(
Table 1Participant details for the TBI and TBI-MDD groups.
Group Age Gender Time sinceinjury (months)
Severity Nature of injury
TBI 54 Male 3 Mild Cycling MVATBI 34 Male 5 Mild Cycling MVATBI 62 Female 250 Moderate MVATBI 30 Male 7 Mild SportTBI 24 Male 8 Moderate MVATBI 27 Female 2 Mild Cycling MVATBI 26 Male 112 Moderate MVATBI 27 Male 3 Mild AssaultTBI 24 Male 3 Moderate Cycling MVATBI 19 Male 2 Mild FallTBI 58 Male 2 Mild MVATBI 51 Male 4 Mild Cycling MVATBI 27 Male 3 Mild Cycling MVATBI 25 Female 4 Mild Cycling MVATBI 17 Male 4 Moderate MVATBI 28 Male 12 Moderate MVATBI 29 Female 5 Mild Cycling MVATBI 17 Female 11 Mild MVATBI 35 Male 26 Moderate MVATBI 49 Male 84 Moderate AssaultTBI-MDD 52 Male 360 Moderate MVATBI-MDD 52 Male 6 Mild FallTBI-MDD 43 Female 156 Mild Cycling MVATBI-MDD 50 Male 34 Moderate FallTBI-MDD 40 Female 42 Mild MVATBI-MDD 46 Female 122 Moderate MVATBI-MDD 40 Male 30 Moderate Cycling MVATBI-MDD 39 Female 20 Moderate SportTBI-MDD 21 Female 2 Mild MVATBI-MDD 25 Female 252 Mild FallTBI-MDD 55 Female 480 Moderate MVATBI-MDD 60 Male 560 Mild SportTBI-MDD 48 Male 14 Moderate Cycling MVATBI-MDD 45 Female 48 Mild MVATBI-MDD 40 Male 300 Mild Cycling MVA
Fb
16 N.W. Bailey et al. / Biologica
The aim of current study was to investigate the impact of TBInd MDD and TBI-MDD on inhibitory (upper alpha) processes dur-ng WM retention. It was hypothesised that both TBI-only and MDDarticipants would show reductions in WM upper alpha activityompared to controls, and that the TBI-MDD group would showven larger reductions. It was also hypothesised that these dif-erences would be more apparent with larger WM loads, as alphactivity is modulated by cognitive load (Gevins, Smith, McEvoy, &u, 1997; Jensen et al., 2002).
. Methods
.1. Participants
Thirty-four healthy controls, 20 MDD, 20 TBI-only, and 15 TBI-MDD participantsere recruited. Data from six participants was excluded; three controls (one showedild depression and two due to equipment faults), and three MDD participants
one did not meet depression severity criteria, and two due to equipment faults).his left 31 control, 17 MDD, 20 TBI-only, and 15 TBI-MDD participants. Participantsere recruited through the Monash Alfred Psychiatry Research Centre database, thelfred Hospital emergency department, and community advertising. The study waspproved by the Ethics Committees of the Alfred Hospital and Monash University,nd all participants gave informed consent. All participants had normal or correctedo normal vision and were between 17 and 65 years of age. A number of participantsn the MDD and TBI-MDD groups were medicated.
Participants in the MDD and TBI-MDD groups had a diagnosis of MDD, andurrent depressive episode was confirmed with the MINI International Neuropsy-hiatric Interview for DSM-IV (Sheehan et al., 1998), as well as a moderate toevere score on the Beck Depression Inventory-II (BDI-II) (>18) (Beck & Steer, 1984)r the Montgomery-Asberg Depression Rating Scale (MADRS) (>19) (Montgomery
Asberg, 1979). With the exception of generalised anxiety disorder, co-morbidsychiatric diagnoses were exclusion criteria for the MDD and TBI-MDD groups.
ndividuals currently using benzodiazapines, mood stabilisers, antipsychotics, orultiple anti-depressants were also excluded. Depression prior to the TBI was an
xclusion criterion for the TBI-MDD group. Injury and depression information wasssessed by a psychiatrist to confirm the MDD was causally related to the TBI. AllBI-only and TBI-MDD participants were tested more than 8 weeks post-injury. Par-icipants with mild to moderate closed head injuries were included in the TBI-onlynd TBI-MDD groups. Injury severity was determined by patient reports and hospitalecords of an initial Glasgow Coma Scale (GCS) score of 9–14, or loss of conscious-ess (LOC)/length of post-traumatic amnesia (PTA) of more than 10 min, and LOC of
ess than 24 h (Kay et al., 1993; Malec et al., 2006; Rao & Lyketsos, 2000). Individ-als with GCS scores of 15 or PTA < 10 min were excluded to ensure uncertainty didot result in inclusion of non-TBI participants, and participants with focal lesionsere excluded to avoid the heterogeneity in neural activity that focal lesions would
ntroduce. Injury details for the TBI and TBI-MDD groups can be viewed in Table 1.ontrols and TBI-only individuals were excluded if they met criteria for currentr prior DSM-IV psychiatric illness. Follow up interviews conducted 6–12 monthsollowing each participant’s testing session confirmed with the MINI Internationaleuropsychiatric Interview for DSM-IV (Sheehan et al., 1998) that no TBI-only par-
icipants developed MDD within this time period.
.2. Procedure
Participants completed two 2.5 h long experimental sessions within two weeks.ne session consisted of the demographic, TBI history and depression sever-
ty assessments. The other session involved the EEG recording. All rating scales
ere administered by a single trained researcher. Pre-morbid IQ was estimatedith the Weschler Test of Adult Reading (WTAR) (Wechsler, 2001), which haseen validated as a measure of pre-morbid IQ post-TBI (Green et al., 2008).andedness was measured using the Edinburgh Handedness Inventory (EHI)
Oldfield, 1971).
ig. 1. (Previous page) Task design and stimuli timing for the Sternberg task. All letteretween containing either five or seven letters. Responses were only classified as correct
MVA = motor vehicle accident.
2.3. Task and stimuli
Participants performed a modified Sternberg task while EEG activity wasrecorded. Stimuli were presented via Neuroscan STIM2 software (Compumedics,Melbourne Australia). Memory sets contained five or seven pseudo-randomlyselected consonants (presented simultaneously, selected from a set of fifteen – B,C, D, F, H, J, K, L, N, R, S, T, Y, W, and Z). In the five letter condition + symbols weredisplayed at each end so that both conditions presented an equal visual angle. Thenumber of letters in each trial was determined by a pseudo-random sequence sothat no more than three of each condition occurred consecutively. Trials beganwith a fixation cross (517 ms) followed by a blank screen (500 ms). The memoryset was presented for 3017 ms, followed by a retention period of 3017 ms, afterwhich a probe letter was presented for 2017 ms. Participants were instructed torespond with a yes or no button press (with their right hand) to indicate whetherthe probe had been in the preceding memory set, and to do their best to performaccurately. Each trial ended with a brief visual mask (133 ms), followed by a blankscreen (1867 ms) before the onset of the fixation cross for the following trial (Fig. 1).The probe had a 50% probability of being present in the memory set. The position ofthe probe in the memory set was pseudo-randomly allocated so it was not located
in the same position consecutively. No letter was presented as the probe consecu-tively and no more than three consecutive probe present or absent trials occurredin a row. The sequence was the same for each participant. Participants performeds in the memory set were presented simultaneously, and the memory set varied if made during the probe presentation.

l Psyc
se
2
aMClEa
od±atfiEclptwsbspbrowtbm
2
2
bcg
tgfwMgwoacec
2
tBwfpu1piWStmao(aAs
N.W. Bailey et al. / Biologica
ix blocks of twenty trials per block. Accuracy and reaction times were recorded forach participant.
.4. Electrophysiological recording and analysis
A Neuroscan 64 electrode EEG Quick cap with Ag/AgCl electrodes recorded EEGctivity via a Synamps 2 amplifier onto Neuroscan Acquire software (Compumedics,elbourne Australia). Electrodes were referenced online to a point between Cz and
pz. Eye movements were recorded with vertical and horizontal EOG electrodesocated above and below the left eye and adjacent to the outer canthus of each eye.lectrode impedances were kept below 5 k�. The EEG was digitised at 500 Hz, with
bandpass of 0.1–100 Hz (24 dB/octave roll-off).Scan 4.3 (Compumedics, Melbourne Australia) was used to analyse EEG data
ffline. Eye movements were corrected for using the eye correction algorithmesigned by Croft and Barry (2000). Epochs containing amplitudes that exceeded75 �v were rejected. EEG recordings were re-referenced offline to a common aver-ge. Only trials with correct responses were analysed. Responses occurring laterhan 2017 ms after probe onset were considered incorrect. Trials were epochedrom the beginning of the fixation cross to the offset of the end of trial blank screenn order to calculate event related desynchronisation/synchronisation (ERD/ERS).RD/ERS is the percentage change in power within a specific frequency band whenomparing a test interval to a designated reference interval. It is calculated as fol-ows: ERD/ERS% = (R − A)/R × 100. A refers to the active test period, R to the referenceeriod. This calculation provides negative values when power increases in the activeest period compared to the reference period (i.e. neural synchronisation). ERD/ERS%as calculated for event related spectral power (induced and evoked) zero phase-
hift filtered while computing signal envelope around 11.25 Hz with a 1.25 Hz halfandwidth (48 dB/octave roll-off). This calculation equals the average magnitudequared activity in the frequency band of interest (Andrew, 1999). The referenceeriod was defined as power in the middle 300 ms window of the blank pauseetween the fixation cross and memory set. The active test period was during theetention period, defined from 250 ms after the memory set offset until the probenset. Mean ERD/ERS% was calculated for the active period for each participant. Theindow for the test period was selected because previous research indicates con-
rols show maximal alpha enhancement during this period (Jensen et al., 2002), andecause grand averages of participant responses in the current study also showedaximal upper alpha enhancement across this whole period.
.5. Statistical analysis
.5.1. Demographic and behavioural analysesOne way analysis of variance (ANOVA) compared BDI and MADRS scores
etween the groups, as well as demographic data. Independent samples t-testsompared GCS, LOC, PTA, and time since injury between the TBI-only and TBI-MDDroups.
A three way mixed ANOVA compared percentage correct for number of let-ers (five or seven) and whether the probe was present or absent, and betweenroups (control, TBI-only, MDD, TBI-MDD). A three way mixed ANOVA was per-ormed for participant reaction times for number of letters (five or seven) andhether the probe was present or absent, and between groups (control, TBI-only,DD, TBI-MDD). Although years of education differed between groups, between
roup comparisons were not conducted with ANCOVA, as this test is not validhen variation in a covariate is found between groups (Miller & Chapman, 2001). In
rder to assess the impact of years of education on WM performance, two separatenalysis of multiple linear regression were conducted with accuracy pooled acrossonditions and reaction times pooled across conditions as the dependent factor forach, and inserting independent factors of MADRS scores, upper alpha pooled acrossonditions and electrodes, and years of education in a stepwise fashion.
.5.2. EEG analysesAnalyses were pooled across both probe present and absent trials (the reten-
ion period precedes the probe presentation so is not influenced by the probe).ecause the ERS/ERD data were non-normally distributed, logarithmic transformsere used to normalise the distribution of upper alpha activity. Logarithmic trans-
orms cannot be performed on negative values, so to enable the transforms theolarity of each value was reversed. Because some of the participants had positivepper alpha ERD/ERS values, reversing their polarity generated negative values, so00 was added to each data point to ensure all values were positive. This transformreserves the essential relationships between data points. Upper alpha compar-
sons focused on PO7, PO8, O1 and O2 electrodes, as previous research indicatesM retention period upper alpha is maximal at these electrodes (Jensen et al., 2002;
egrave et al., 2010), and topographical analyses of the current data indicated reten-ion period upper alpha power was maximal at these four electrodes. A four way
ixed ANOVA compared upper alpha ERD/ERS within subjects for side (right–O2nd PO8, left O1 and PO7), parietal-occipital (parietal occipital – PO8 and PO7, and
ccipital – O1 and O2), memory set size (five or seven letters) and between groupscontrol, TBI-only, MDD, TBI-MDD). In order to explore the potential impact ofntidepressant medication data was reanalysed excluding medicated participants.four way mixed ANOVA was conducted comparing upper alpha ERD/ERS withinubjects for side (right – O2 and PO8, left O1 and PO7), parietal-occipital (parietal
hology 99 (2014) 115–124 117
occipital – PO8 and PO7, and occipital – O1 and O2), memory set size (five or sevenletters) and between groups, with medication free MDD and TBI-MDD participantscombined into one group (control, TBI-only, medication free MDD and TBI-MDD).The medication free MDD and TBI-MDD participants were combined into one groupto ensure this comparison would have sufficient statistical power. Similarly, in orderto test whether the results were consistent across genders, the ANOVA was repeatedseparately for males and females, again with the MDD and TBI-MDD group combinedto enhance statistical power, and the TBI-only group excluded from the analysis (theTBI-only group showed no differences in the initial analysis, and had low numbersfollowing a gender split). Four way mixed ANOVAs were conducted for each gen-der comparing upper alpha ERD/ERS within subjects for side (right – O2 and PO8,left O1 and PO7), parietal-occipital (parietal occipital–PO8 and PO7, and occipital –O1 and O2), memory set size (five or seven letters) and between groups (combinedMDD and TBI-MDD group, controls). To control for multiple comparisons, post hocTukey tests were performed when omnibus ANOVAs were significant. In the interestof brevity, only interactions involving group were explored. All sphericity viola-tions were corrected for using the Greenhouse–Geisser correction (Greenhouse &Geisser, 1959). Pearson’s correlations were conducted (separately for each groupthat showed significant differences in upper alpha) between upper alpha ERD/ERS(pooled across electrodes/memory sets to reduce the number of multiple compar-isons) and reaction time and accuracy (pooled across memory sets/probe present orabsent conditions). Because groups differed in years of education, analysis of multi-ple linear regression was used inserting independent factors of MADRS scores andyears of education in a stepwise fashion, with log transformed upper alpha activitypooled across memory loads and electrodes as the dependent factor. Similarly timesince injury, injury severity, years of education and MADRS scores were examinedwithin the TBI groups with a multiple linear regression inserting independent fac-tors in a stepwise fashion, with log transformed upper alpha activity pooled acrossmemory loads and electrodes as the dependent factor.
3. Results
3.1. Demographics, depression, and TBI severity
Table 2 displays the means and standard deviations for demo-graphic data and clinical measures. Groups did not significantlydiffer in age, handedness or estimated pre-morbid IQ (all F’s < 2.05,all p’s > 0.10). Significant differences were found for years of educa-tion (F(3,78) = 2.96, p < 0.05). Post hoc Tukey showed the TBI-MDDgroup had fewer years than the control group (p < 0.05). The TBI-only and TBI-MDD groups did not significantly differ in brain injuryseverity as measured by length of PTA, GCS, and duration of LOC (allt’s < 1.50, all p’s > 0.10). The TBI-MDD group had significantly longertime since injury than the TBI-only group (t(30) = 2.78, p < 0.05).Groups significantly differed in BDI-II (F(3,78) = 223.29, p < 0.01)and MADRS scores (F(3,78) = 86.95, p < 0.01). As expected, for bothmeasures the MDD and TBI-MDD scored significantly higher thanthe control and TBI-only groups (both p’s < 0.01). The TBI-only andcontrol groups did not differ in depression severity, nor did theMDD and TBI-MDD groups (all p’s > 0.10).
3.2. Sternberg behavioural data
Behavioural data is summarised in Fig. 2. There was a signifi-cant difference in accuracy across the memory load conditions, withhigher accuracy for lower memory load conditions (F(1,79) = 49.84,p < 0.01, partial �2 = 0.39). There was also a significant differ-ence in accuracy between groups (F(3,79) = 3.91, p < 0.05, partial�2 = 0.13). Post hoc Tukey tests showed the control and TBI-onlygroup were more accurate than the MDD group (control moreaccurate than MDD – Cohen’s d = 0.70, TBI-only more accuratethan MDD – Cohen’s d = 0.95, both p < 0.05). No other betweengroup differences were detected for accuracy (all p’s > 0.10). Nodifferences were detected between probe present and absent con-ditions (F(1,79) = 1.73, p < 0.05), and no interactions were present(all p’s > 0.10). Multiple linear regression indicated that MADRS
score significantly predicted accuracy pooled across conditions( = −0.37, t(79) = −3.56, p < 0.01), but years of education didnot ( = 0.06, t(79) = 0.58, p > 0.10), nor did pooled alpha activity( = −0.05, t(79) = 0.48, p > 0.10).
118 N.W. Bailey et al. / Biological Psychology 99 (2014) 115–124
Table 2Demographics, depression rating scores, head injury severity measures, and medications for each group (means with SD in parentheses).
Controls TBI-only MDD TBI-MDD
N 31 20 17 15Gender (F/M) 18/13 5/15 9/8 8/7Age (years) 38.48 (13.67) 33.15 (13.83) 38.47 (12.18) 43.73 (10.44)Years of formal educationa 17.87 (3.26) 16.98 (3.41) 15.71 (3.58) 14.87 (3.67)WTAR pre-morbid IQ 111.59 (3.28) 107.47 (5.66) 107.31 (7.78) 109.69 (5.94)MADRSb 1.73 (1.70) 2.45 (2.42) 26.47 (4.47) 16.47 (7.75)BDIb 2.45 (2.97) 3.30 (3.53) 24.41 (10.01) 29.36 (9.75)Handedness (R/L/mixed) 26/2/3 16/1/3 16/1 12/3EHI 80.97 (44.52) 75.54 (48.32) 86.29 (43.66) 66.64 (64.11)GCS 13.00 (1.41) 13.67 (0.58)LOC (h) 1.28 (2.88) 1.49 (3.29)PTA (h) 7.68 (12.02) 10.62 (13.59)Time since injury (months)a 22.89 (59.66) 176.77 (197.68)Severity (mild/moderate) 12/8 8/7MedicationsNone 7 7SNRI 4 3SSRI 5 3Tricyclic 1 2Comorbid Anxiety (Yes/no) 9/8 5/10
contri
the c
fdtcdpstgnNartPttp(
3
fi(gOp(plcTvdlpwtd
alpha ( = −0.34, t(79) = −3.17, p < 0.01), but years of education didnot ( = 0.13, t(79) = 1.23, p > 0.10). Within the TBI groups multi-ple linear regression indicated that MADRS score predicted logtransformed pooled upper alpha power ( = −0.35, t(33) = −2.11,
Table 3Mean and standard deviation log transformed upper alpha ERD for control, MDD,TBI-only and TBI-MDD participants.
Controls TBI-only MDDa TBI-MDDa Total
Seven lettersPO8 2.46 (0.34) 2.40 (0.26) 2.26 (0.29) 2.22 (0.28) 2.36 (0.31)PO7 2.28 (0.28) 2.24 (0.25) 2.11 (0.23) 2.08 (0.12) 2.20 (0.25)O2 2.41 (0.32) 2.37 (0.23) 2.18 (0.26) 2.21 (0.25) 2.31 (0.29)O1 2.34 (0.30) 2.29 (0.26) 2.14 (0.23) 2.16 (0.14) 2.26 (0.27)
Five lettersPO8 2.41 (0.32) 2.38 (0.28) 2.25 (0.28) 2.23 (0.20) 2.34 (0.28)PO7 2.28 (0.27) 2.20 (0.24) 2.12 (0.23) 0.11) 2.18 (0.25)O2 2.37 (0.31) 2.34 (0.24) 2.19 (0.28) 2.20 (0.23) 2.29 (0.28)
a TBI-MDD group showed significantly fewer years of education than the healthynjury than the TBI-only group (p < 0.05).
b Both the TBI-MDD and MDD groups showed higher BDI and MADRS scores than
Reaction time comparisons also revealed a significant differenceor memory load, with faster reaction times in the five letter con-ition (F(1,79) = 125.68, p < 0.01, partial �2 = 0.61). Faster reactionimes were also shown for the probe present compared to absentondition (F(1,79) = 26.87, p < 0.01, partial �2 = 0.25). Significantifferences were again detected between groups (F(3,79) = 5.18,
= 0.01, partial �2 = 0.16). Post hoc between group comparisonshowed the MDD group had significantly slower reaction timeshan the control group (Cohen’s d = 0.98, p < 0.01) and TBI-onlyroup (Cohen’s d = 0.85, p < 0.05), and the TBI-MDD group was sig-ificantly slower than the control group (Cohen’s d = 0.85, p < 0.05).o other between group differences were significant (all p’s > 0.10),nd no interactions were present (all p’s > 0.10). Multiple linearegression indicated that MADRS score significantly predicted reac-ion time pooled across conditions ( = 0.36, t(79) = 3.49, p < 0.01).ooled alpha activity also explained a significant proportion ofhe variation in reaction time pooled across conditions ( = −0.22,(79) = −2.04, p < 0.05). Years of education did not significantlyredict the variation in reaction time pooled across conditions
= −0.18, t(79) = −1.76, p > 0.05).
.3. Upper alpha ERD/ERS activity
The average distribution of upper alpha activity during a trialor each group can be viewed in Figs. 3 and 4. All groups showedncreased ERS at PO7, PO8, O1 and O2 during the retention periodFigs. 5 and 6). A significant effect of laterality was observed, withreater upper alpha activity at the right parieto-occipital (PO8,2) electrodes than the left (PO7, O1) (F(1,79) = 28.55, p < 0.01,artial �2 = 0.27). A significant effect of group was also shownF(3,79) = 3.91, p < 0.05, partial �2 = 0.13). Post hoc Tukey com-arisons indicated that the MDD and TBI-MDD groups exhibited
ess upper alpha activity than the control group (control groupompared to MDD – Cohen’s d = 0.70, control group compared toBI-MDD – Cohen’s d = 1.01, both p < 0.05). These differences can beiewed in Table 3 and Fig. 7. No significant effect of WM load wasetected (F(1,79) = 1.67, p > 0.10). A significant interaction between
aterality and parietal/occipital region was shown (F(1,79) = 44.24,
< 0.01, partial �2 = 0.36). Visual inspection of the data suggests thisas due to less lateralised upper alpha in the occipital electrodeshan the parieto-occipital electrodes (Figs. 3 and 4). The interactionid not involve group, so was not explored with further statistical
ol group (p < 0.05). The TBI-MDD group also showed significantly longer time since
ontrol and TBI-only groups (all p < 0.01).
analysis. No other interactions were present (all p’s > 0.10). Whenmedicated participants were excluded, a significant effect of groupwas still shown (F(2,60) = 5.89, p < 0.01, partial �2 = 0.16). Post hocTukey comparisons indicated that the combined unmedicated MDDand TBI-MDD group showed less upper alpha activity than both thecontrol group (Cohen’s d = 0.98, p < 0.01) and the TBI-only group(Cohen’s d = 0.98, p < 0.05). When group comparisons were madein each gender separately, significant reductions in upper alphaactivity were still found in the combined MDD and TBI-MDD groupcompared to the control group (females: F(1,33) = 5.74, p < 0.05,partial �2 = 0.15, males: F(1,26) = 4.74, p < 0.05, partial �2 = 0.15).
Within the control group a negative relationship was foundbetween pooled upper alpha and pooled reaction time (r = −0.49,p < 0.01). No relationship was found between pooled upper alphaand pooled accuracy (r = 0.08, p > 0.10). Within the MDD and TBI-MDD groups no relationship was found between pooled upperalpha and pooled reaction time (r = 0.10, p > 0.10 and r = −0.13,p > 0.10 respectively), nor was a relationship found between pooledupper alpha and pooled accuracy (r = −0.01, p > 0.10 and r = 0.25,p > 0.10 respectively). Multiple linear regression indicated thatMADRS score significantly predicted log transformed pooled upper
O1 2.34 (0.31) 2.26 (0.25) 2.16 (0.28) 2.11 (0.14) 2.24 (0.27)
a TBI-MDD and MDD < controls (p < 0.05). Data was log transformed. To enable logtransform, the polarity of data was reversed 100 was added to each value so that allvalues were positive.

N.W. Bailey et al. / Biological Psychology 99 (2014) 115–124 119
F or eacc e wasd
ppn
4
TrdwiuNd
r1o
ig. 2. (Previous page) Mean percent accuracy (top) and reaction times (bottom) fonditions showed significantly greater accuracy and faster reaction times, and therifferences are show with asterisks *p < 0.05, **p < 0.01.
< 0.05), but time since injury did not ( = 0.12, t(33) = 0.64, > 0.10), nor did injury severity ( = −0.25, t(33) = −1.56, p > 0.10),or did years of education ( = 0.27, t(33) = 1.63, p > 0.10).
. Discussion
The aim of this study was to determine the relative impact ofBI and MDD on inhibitory (upper alpha) processes during WMetention. We found that individuals with MDD and TBI-MDD showelayed WM reaction times compared to controls, and individualsith MDD alone showed accuracy impairments. We also found that
ndividuals with MDD and TBI-MDD showed less elevated posteriorpper alpha activity while information is being retained in WM.o WM impairments or reductions in upper alpha activity wereetected in the TBI-only group.
Our behavioural results align with previous studies which haveeported WM impairments in MDD and TBI-MDD (Burt et al.,995; Jorge et al., 2004). In addition to the WM impairments,ur study showed that individuals with MDD and TBI-MDD do
h condition in the Sternberg task (error bars reflect standard error). The five letter faster reaction times in the probe present conditions (all p’s < 0.01). Between group
not exhibit the same magnitude of upper alpha synchronisationduring the retention phase of WM as healthy controls. As upperalpha activity is thought to reflect inhibition, this finding mayreflect an impairment in inhibitory processes in individuals withMDD and TBI-MDD (Klimesch et al., 2007). This reduced upperalpha activity may suggest a mechanism for cognitive impair-ments in MDD and TBI-MDD. It is possible that reduced upperalpha activity in these groups may result in difficulty inhibitingnegative ruminations, which may impact upon WM performance(Gohier et al., 2009; Lau, Christensen, Hawley, Gemar, & Segal,2007). In support of this idea, we observed that MADRS scorepredicted upper alpha reductions. We also observed that reac-tion times were related to upper alpha activity in the controlgroup, and upper alpha predicted reaction times independent ofMADRS score, suggesting there is a relationship between upper
alpha and cognitive performance. No relationships were foundbetween upper alpha and accuracy, perhaps because the accu-racy data lacked the variation to show statistical sensitivity withcorrelation.
120 N.W. Bailey et al. / Biological Psyc
Fig. 3. The average upper alpha ERD/ERS distribution for each group in selectedelectrodes during the 5 letter memory condition.
Fe
ae(awtuttattht
ig. 4. The average upper alpha ERD/ERS distribution for each group in selectedlectrodes during the 7 letter memory condition.
Further research is required to confirm that reduced upper alphactivity leads to WM impairments in MDD and TBI-MDD, how-ver, as the current study did not control for motivational factorsaside from instructing all participants to ‘do their best to performccurately’). Motivation may be reduced in MDD and TBI-MDD,hich may have resulted in reduced upper alpha activity during
he retention period. However, a number of lines of evidence leads to believe the reductions in upper alpha are not due to motiva-ional factors. The first is that impairments in accuracy and reactionime in the MDD and TBI-MDD groups were small – between 5nd 10%. Secondly, TBI-MDD group did not differ from the con-
rol group in accuracy. If the upper alpha differences were dueo lower motivation on the part of the TBI-MDD group, we wouldave expected lower memory performance in that group. Thirdly,he within group pattern and magnitude of differences betweenhology 99 (2014) 115–124
conditions (for probe present/absent and memory load) was thesame across all groups. If the MDD and TBI-MDD groups wereless motivated, their responses would be expected to vary lessbetween conditions (as their focus on task performance decreased,the advantages of 5 letter memory loads compared to seven let-ter memory loads also decrease). In particular, lower motivationwould be expected to have resulted in a higher proportion of falsenegatives in the MDD groups. Less motivated participants wouldhave shown reduced attention to (and as such reduced encodingof) the memory set, and as a result, recognise the probe as havingbeen present the memory set less often (committing more falsenegatives than false positives) (Burt et al., 1995).
The results of the current study are also in contrast to thosereported by Segrave et al. (2010), who found increased upper alphain the left hemisphere during WM retention in MDD compared tocontrols. There are a number of differences between the two stud-ies that may explain the contradiction. Segrave et al. (2010) testedonly female participants, while the current study tested both gen-ders. However, comparisons separated by gender in the currentstudy still indicated that female MDD and TBI-MDD participantsshowed reduced upper alpha activity. Segrave et al. (2010) alsoused an eight letter memory set, while the current study comparedfive and seven letter memory sets. It is possible that the effect ofMDD on upper alpha activity is reversed when WM demands areincreased (although it seems unlikely that increasing the WM loadby one digit would reverse the between group differences). Lastly,Segrave et al. (2010) based their analysis on EEG activity withinindividualised upper alpha bands (i.e. the upper alpha bandwidthwas calculated for each participant based on their unique spectralcharacteristics), whereas the current study examined upper alphaactivity within a fixed 10–12.5 Hz upper alpha range for all partic-ipants. However, it seems unlikely that examining individualisedupper alpha rather than a fixed band for all participants wouldsubstantially influence the current results, as previous research hasindicated very little difference between ERD/ERS% when comparingfixed and individualised upper alpha bands (Segrave et al., 2011).
Regardless of the contrast with previous research, both theMDD and TBI-MDD groups showed WM impairments and reduc-tions in upper alpha activity. The TBI-only group, however, showedno significant differences. If the TBI was responsible for the WMimpairments and disrupted upper alpha activity found in the TBI-MDD group, we would expect the TBI-only group to also showdisruptions. Especially considering the TBI-only group had less timesince injury than the TBI-MDD group, so less time for potentialrecovery mechanisms to reverse changes. These findings suggestthat MDD may be the causal factor in upper alpha activity reduc-tions and WM impairments found in TBI-MDD, rather than the TBI.However, this conclusion is tentative, as causation may operatein the reverse direction. Despite the lack of significant differencesbetween TBI groups in the available injury information, individualswho developed TBI-MDD may have suffered injuries which directlyaffected upper alpha activity and WM. These injury related impair-ments may have later caused the onset of depression. Individuals inthe TBI-only group may not have suffered injuries that affected WMand upper alpha activity, and as a result did not develop depression.If the causation operates in this direction, then WM related upperalpha impairments soon after a TBI may be predict the developmentof TBI-MDD.
The conclusion that the MDD is the feature that causes upperalpha reductions in TBI-MDD is also tentative because it may bethat TBI does cause upper alpha reductions, but the current sam-ple size was insufficient to show significance. In that case, TBI and
MDD may sum to cause the upper alpha reductions in the TBI-MDDgroup. Indeed, the lack of differences between the TBI-only and con-trol groups is in disagreement with some previous research, whichhas found resting alpha alterations, WM performance impairments,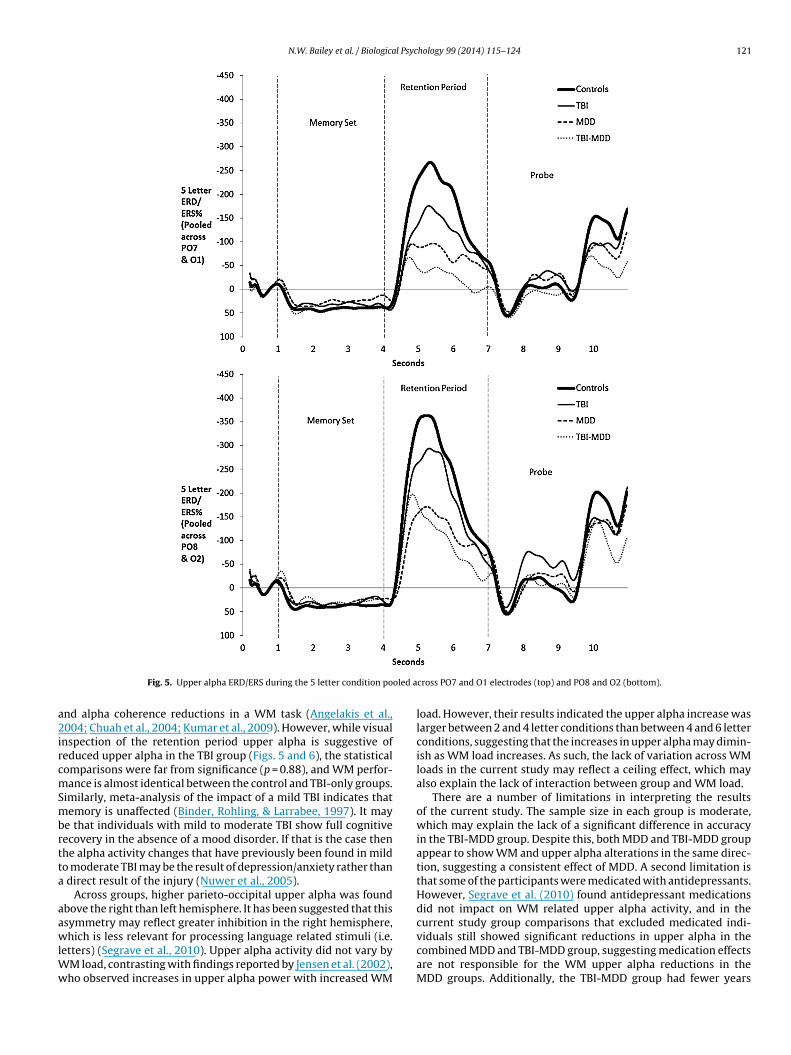
N.W. Bailey et al. / Biological Psychology 99 (2014) 115–124 121
oled a
a2ircmSmbrtta
aawlWw
Fig. 5. Upper alpha ERD/ERS during the 5 letter condition po
nd alpha coherence reductions in a WM task (Angelakis et al.,004; Chuah et al., 2004; Kumar et al., 2009). However, while visual
nspection of the retention period upper alpha is suggestive ofeduced upper alpha in the TBI group (Figs. 5 and 6), the statisticalomparisons were far from significance (p = 0.88), and WM perfor-ance is almost identical between the control and TBI-only groups.
imilarly, meta-analysis of the impact of a mild TBI indicates thatemory is unaffected (Binder, Rohling, & Larrabee, 1997). It may
e that individuals with mild to moderate TBI show full cognitiveecovery in the absence of a mood disorder. If that is the case thenhe alpha activity changes that have previously been found in mildo moderate TBI may be the result of depression/anxiety rather than
direct result of the injury (Nuwer et al., 2005).Across groups, higher parieto-occipital upper alpha was found
bove the right than left hemisphere. It has been suggested that thissymmetry may reflect greater inhibition in the right hemisphere,
hich is less relevant for processing language related stimuli (i.e.etters) (Segrave et al., 2010). Upper alpha activity did not vary byM load, contrasting with findings reported by Jensen et al. (2002),ho observed increases in upper alpha power with increased WM
cross PO7 and O1 electrodes (top) and PO8 and O2 (bottom).
load. However, their results indicated the upper alpha increase waslarger between 2 and 4 letter conditions than between 4 and 6 letterconditions, suggesting that the increases in upper alpha may dimin-ish as WM load increases. As such, the lack of variation across WMloads in the current study may reflect a ceiling effect, which mayalso explain the lack of interaction between group and WM load.
There are a number of limitations in interpreting the resultsof the current study. The sample size in each group is moderate,which may explain the lack of a significant difference in accuracyin the TBI-MDD group. Despite this, both MDD and TBI-MDD groupappear to show WM and upper alpha alterations in the same direc-tion, suggesting a consistent effect of MDD. A second limitation isthat some of the participants were medicated with antidepressants.However, Segrave et al. (2010) found antidepressant medicationsdid not impact on WM related upper alpha activity, and in thecurrent study group comparisons that excluded medicated indi-
viduals still showed significant reductions in upper alpha in thecombined MDD and TBI-MDD group, suggesting medication effectsare not responsible for the WM upper alpha reductions in theMDD groups. Additionally, the TBI-MDD group had fewer years
122 N.W. Bailey et al. / Biological Psychology 99 (2014) 115–124
oled a
owcwtb1dTsttttuottc
Fig. 6. Upper alpha ERD/ERS during the 7 letter condition po
f education compared to healthy controls. However, educationas not predictive of upper alpha, reaction time, or accuracy when
ontrolling for other factors. Gender is another potential confound,ith a higher proportion of males in the TBI-only group compared
o other groups. If alpha is differentially modulated by gender as haseen suggested (Corsi-Cabrera, Ramos, Guevara, Arce, & Gutierrez,993), the gender ratio for this group may have masked potentialifferences between the TBI-only group and controls. Finally, theBI-only group had less time between their injury and the testingession than the TBI-MDD group. Although regression indicatedhat MADRS scores were predictive of upper alpha activity whileime since injury was not, the results do not rule out the possibilityhat these individuals may suffer a delayed onset MDD followinghe TBI, which would affect upper alpha activity in these individ-als. As such, a prospective study is required before TBI can be ruled
ut as a factor in WM upper alpha changes. Additionally, becausehe TBI-only group does not show significant differences comparedo the TBI-MDD group, we cannot be certain that it is the MDDausing the upper alpha and WM changes in the TBI-MDD group,cross PO7 and O1 electrodes (top) and PO8 and O2 (bottom).
rather than an additive effect of TBI and MDD. However, three linesof evidence suggest that this is not the case. Firstly, examinationof Figs. 2 and 7 suggests that the TBI-only group showed similarbehavioural and alpha results to controls. Secondly, the TBI-onlygroup showed significantly more upper alpha than the combinedunmedicated MDD and TBI-MDD groups. And thirdly, regressionindicated that while MADRS scores were a predicting factor ofaltered upper alpha activity, TBI severity was not. If mild to mod-erate TBIs did influence upper alpha activity, we would expect alinear relationship between severity and upper alpha. As such, itseems likely that MDD is responsible for the upper alpha and WMchanges in TBI-MDD, rather than the TBI.
In sum, this study indicates that individuals with MDD and TBI-MDD have impaired upper alpha activity in the parieto-occipitalarea during WM retention. This may result in impaired inhibition of
non-relevant information, causing interference with task-relevantinformation held in WM. This interpretation of the current dataprovides a physiological explanation for WM impairments in indi-viduals with TBI-MDD. The findings also suggest that WM retention
N.W. Bailey et al. / Biological Psychology 99 (2014) 115–124 123
cross e
pag
D
MC
A
tvos(FF
R
A
A
B
B
B
C
C
C
Fig. 7. Mean log transformed upper alpha ERD/ERS for each group pooled a
eriod upper alpha activity may be unaffected by mild to moder-te TBI-only. As such, the WM impairments found in the TBI-MDDroup may be due to depression rather than to TBI.
isclosure statement
PBF has received equipment for research from Medtronic ltd,agventure A/S and Brainsway Ltd. and funding for research from
ervel Neurotech. NWB, RAS, KEH, JJM have no conflicts to declare.
cknowledgments
Funding for this study was provided by Monash University andhe Victorian Neurotrauma Initiative. Equipment funding was pro-ided in part by the Neurosciences Victoria Clinical Neurobiologyf Psychiatry Platform. PBF is supported by a Practitioner Fellow-hip grant from the National Health and Medical Research CouncilNHMRC). RAS and KEH are supported by Post Doctoral Trainingellowships from NHMRC. JJM is supported by an NHMRC CDFellowship.
eferences
ndrew, C. (1999). Quantification of event-related coherence (ERCoh). In G. Pfurts-celler, & F. H. Lopes de Silver (Eds.), Handbook of Electroencephalography andClinical Neurophysiology, Event Related Desynchronisation (vol. 6) (pp. 119–137).Amsterdam: Elsevier.
ngelakis, E., Lubar, J. F., Stathopoulou, S., & Kounios, J. (2004). Peak alpha frequency:An electroencephalographic measure of cognitive preparedness. Clinical Neuro-physiology, 115, 887–897.
eck, A. T., & Steer, R. A. (1984). Internal consistencies of the original and revisedBeck Depression Inventory. Journal of Clinical Psychology, 40(6), 1365–1367.
inder, L. M., Rohling, M. L., & Larrabee, G. J. (1997). A review of mild head trauma.Part I: Meta-analytic review of neuropsychological studies. Journal of Clinical andExperimental Neuropsychology, 19, 421–431.
urt, D. B., Zembar, M. J., & Niederehe, G. (1995). Depression and memoryimpairment: A meta-analysis of the association, its pattern, and specificity. Psy-chological Bulletin, 117(2), 285–305.
huah, Y. M. L., Maybery, M. T., & Fox, A. M. (2004). The long-term effects of mildhead injury on short-term memory for visual form, spatial location, and theirconjunction in well-functioning university students. Brain and Cognition, 56,304–312.
orsi-Cabrera, M., Ramos, J., Guevara, M. A., Arce, C., & Gutierrez, S. (1993). Gender
differences in the EEG during cognitive activity. International Journal of Neuro-science, 72, 257–264.roft, R. J., & Barry, R. J. (2000). EOG correction of blinks with saccade coefficients:A test and revision of the aligned-artefact average solution. Clinical Neuro-physiology, 111(3), 444–451.
lectrodes and memory loads. Error bars represent standard error. *p < 0.05.
Dockree, P. M., Kelly, S. P., Roche, R. A. P., Hogan, M. J., Reilly, R. B., & Robertson, I. H.(2004). Behavioural and physiological impairments of sustained attention aftertraumatic brain injury. Cognitive Brain Research, 20, 403–414.
Gevins, A., Smith, M. E., McEvoy, L., & Yu, D. (1997). High-resolution EEG mappingof cortical activation related to working memory: Effects of task difficulty, typeof processing, and practice. Cerebral Cortex, 7, 374–385.
Gohier, B., Ferracci, L., Surguladze, S. A., Lawrence, E. C., El Hage, W., Kefi, M. Z.,et al. (2009). Cognitive inhibition and working memory in unipolar depression.Journal of Affective Disorders, 116, 100–105.
Green, R. E. A., Melo, B., Christensen, B., Ngo, L. A., Monette, G., & Bradbury, C.(2008). Measuring premorbid IQ in traumatic brain injury: An examination ofthe validity of the Wechsler Test of Adult Reading (WTAR). Journal of Clinical andExperimental Neuropsychology, 30(2), 163–172.
Greenhouse, S. W., & Geisser, S. (1959). On methods in the analysis of profile data.Psychometrika, 24(2), 95–112.
Jensen, O., Gelfand, J., Kounios, J., & Lisman, J. E. (2002). Oscillations in the alpha band(9–12 Hz) increase with memory load during retention in a short-term memorytask. Cerebral Cortex, 12, 882–887.
Jensen, O., & Mazaheri, A. (2010). Shaping functional architecture by oscillatory alphaactivity: Gating by inhibition. Frontiers in Human Neuroscience, 4, 1–8.
Jorge, R. E., Robinson, R. G., Arndt, S., Starkstein, S. E., Forrester, A. W., & Geisler, F.(1993). Depression following traumatic brain injury: A 1 year longitudinal study.Journal of Affective Disorders, 27, 233–243.
Jorge, R. E., Robinson, R. G., Moser, D., Tateno, A., Crespo-Facorro, B., & Arndt, S.(2004). Major depression following traumatic brain injury. Archives of GeneralPsychiatry, 61, 42–50.
Kay, T., Harrington, D. E., Adams, R., Anderson, T., Berrol, S., & Cicerone, K. J. M. (1993).Definition of mild traumatic brain injury. Journal of Head Trauma Rehabilitation,8(3), 86–87.
Klimesch, W., Sauseng, P., & Hanslmayr, S. (2007). EEG alpha oscillations: Theinhibition-timing hypothesis. Brain Research Reviews, 53, 63–88.
Kreutzer, J. S., Seel, R. T., & Gourley, E. (2001). The prevalence and symptom ratesof depression after traumatic brain injury: A comprehensive examination. BrainInjury, 15(7), 563–576.
Kumar, S., Rao, S., Chandramouli, B. A., & Pillai, S. V. (2009). Reduction of func-tional brain connectivity in mild traumatic brain injury during working memory.Journal of Neurotrauma, 26(5), 665–675.
Lau, M. A., Christensen, B., Hawley, L. L., Gemar, M. S., & Segal, Z. V. (2007). Inhibitorydeficits for negative information in persons with major depressive disorder.Psychological Medicine, 37, 1249–1259.
Malec, J. F., Brown, A. W., Leibson, C. L., Flaada, J. T., Mandrekar, J. N., Diehl, N. N.,et al. (2006). The Mayo classification system for traumatic brain injury severity.Journal of Neurotrauma, 24, 1417–1424.
Miller, G. A., & Chapman, J. P. (2001). Misunderstanding analysis of covariance.Journal of Abnormal Psychology, 110(1), 40–48.
Montgomery, S. A., & Asberg, M. A. (1979). A new depression scale designed to besensitive to change. British Journal of Psychiatry, 134, 382–389.
Nuwer, M. R., Hovda, D., Schrader, L. M., & Vespa, P. M. (2005). Routine andquantitative EEG in mild traumatic brain injury. Clinical Neurophysiology, 116,2001–2025.
Oldfield, R. C. (1971). The assessment and analysis of handedness: The Edinburgh
Inventory. Neuropsychologia, 9(1), 97–113.Pagulayan, K. F., Hoffman, J. M., Temkin, N. R., Machamer, J. E., & Dikmen, S. S. (2008).Functional limitations and depression after traumatic brain injury: Examinationof the temporal relationship. Archives of Physical & Medical Rehabilitation, 89,1887–1892.

1 l Psyc
R
R
S
S
24 N.W. Bailey et al. / Biologica
ao, V., & Lyketsos, C. (2000). Neuropsychiatric sequalae of traumatic brain injury.Psychosomatics, 41, 95–103.
apoport, M. J., Kiss, A., & Feinstein, A. (2006). The impact of major depression on out-come following mild-to-moderate traumatic brain injury in older adults. Journalof Affective Disorders, 92, 273–276.
atz, P., Forney, D. L., Zaucha, K., Asarnow, R. R., Light, R., McCleary, C., et al. (1998).
Depression, cognition, and functional correlates of recovery outcome after trau-matic brain injury. Brain Injury, 12(7), 537–553.egrave, R. A., Cooper, N. R., Thomson, R. H., Croft, R. J., Sheppard, D. M., & Fitzger-ald, P. B. (2011). Individualized alpha activity and frontal asymmetry in majordepression. Clinical EEG and Neuroscience, 42, 45–52.
hology 99 (2014) 115–124
Segrave, R. A., Thomson, R. H., Cooper, N. R., Croft, R. J., Sheppard, D. M., & Fitzgerald,P. B. (2010). Upper alpha activity during working memory processing reflectsabnormal inhibition in major depression. Journal of Affective Disorders, 127,191–198.
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E.,et al. (1998). The mini-international neuropsychiatric interview (M.I.N.I.): The
development and validation of a structured diagnostic psychiatric interview forDSM-IV and ICD-10. Journal of Clinical Psychiatry, 59, 22–33.Wechsler, D. (2001). Wechsler test of adult reading (WTAR). San Antonio: TX.World Health Organisation. (2001). World health report 2001 mental health: New
understanding, new hope. Geneva, Switzerland.
Related Documents