Impacts of Antibiotic-Resistant Bacteria September 1995 OTA-H-629 GPO stock #052-003-01446-7

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Impacts of Antibiotic-Resistant Bacteria
September 1995
OTA-H-629
GPO stock #052-003-01446-7
Recommended Citation: U.S. Congress, Office of Technology Assessment,Impacts of Antibiotic-Resistant Bacteria, OTA-H-629 (Washington, DC: U.S.Government Printing Office, September 1995).
iii
Foreword
enicillin, the first antibiotic, and the more than 100 other anti-biotics now available to physicians are the primary weaponsin mankind's battle against bacterial diseases. They revolu-tionized medicine, providing cures for formerly life-threaten-
ing diseases and preventing many previously inevitable deaths frominfected wounds. They still do, but within a short time of each antibi-otic's introduction into medicine, some bacteria became resistant to it,and the antibiotic lost its effectiveness against some diseases. Cur-rently, few bacteria are resistant to all antibiotics, but many more areresistant to all but one or all but a few antibiotics, and the expectationis that resistant bacteria will continue to emerge and spread. The fearis that many bacteria will become resistant to all antibiotics, plunginghumanity back into the conditions that existed in the pre-antibioticage.
OTA's report discusses what is known about the emergence andspread of antibiotic-resistant bacteria and describes research anddevelopment aimed at controlling those organisms. It concludes thatefforts are necessary both to preserve the effectiveness of currentlyavailable antibiotics and to develop new antibiotics. It discusses issuesthat arise in these activities, and it presents options for taking action.
This report was requested by the House Committee on Energy andCommerce in the 103d Congress (now the House Committee on Com-merce). The Senate Committee on Labor and Human Resources in thesame Congress endorsed the request for the study.
OTA was assisted in this study by an advisory panel of scientistsand physicians from academia, industry, and state government chairedby Gail Cassell, Ph.D., of the University of Alabama at Birmingham.OTA gratefully acknowledges the contribution of each advisory panelmember as well as that of many other experts who supplied informa-tion for the report and participated in reviews of the report as it wasprepared. As with all OTA reports, the final responsibility for the con-tent of the assessment rests with OTA.
ROGER C. HERDMANDirector
P
iv
Advisory Panel
Gail Cassell, Ph.D.Professor and ChairmanDepartment of MicrobiologyUniversity of Alabama at
Birmingham/University Station
Birmingham, AL 35294
Anne BolmstromPresidentAB BiodiskPyramidvagon 7S-17136 SolnaSweden
Robert J. Bywater, Ph.D.Director, Anti-Infective
AssessmentSmithKline Beecham Animal
HealthWalton OaksDorking RoadTadworthSurrey KT20 7NTUK
Barry Eisenstein, M.D.Vice President, Lilly Research
LabsLilly Corporate Center, 0434Indianapolis, IN 46285
Prabhavathi B. Fernandes, Ph.D.
Vice President, Drug Discovery
Biomolecular ScreeningBristol-Myers SquibbPO Box 4000Princeton, NJ 08543-4000
Winston Frederick, M.D.Infectious Disease ResearchHoward University Hospital2041 Georgia Ave., NW,
Room 5C-43Washington, DC 20060
Joshua Lederberg, Ph.D.ProfessorThe Rockefeller UniversityNew York, NY 10021-6399
Stephen Lerner, M.D.Professor of MedicineWayne State University School
of MedicineHarper Hospital/Division of
Infectious Diseases3990 John RDetroit, MI 48201
Stuart Levy, M.D.Professor of Medicine and of
Molecular Biology and Microbiology
Tufts University Medical School
136 Harrison Ave.Boston, MA 02111-1800
Robert C. Moellering, Jr., M.D.
Physician-In-Chief and Chairman
New England Deaconess Hospital
Department of Medicine/Room 6A
110 Francis StreetBoston, MA 02215-5553
Barbara Murray, M.D.Professor of Medicine and of
Microbiology and Molecular Genetics
Infectious DiseasesUniversity of Texas Medical
School at Houston6431 FanninHouston, TX 77030
v
Tom O'Brien, M.D.Medical DirectorMicrobiology LaboratoryBrigham and Women's
Hospital75 Francis StreetBoston, MA 02115
Lone Simonsen, Ph.D.926 Waverly Way, Apt. AAtlanta, GA 30307
Harry Taber, Ph.D.Acting Director, Division of
Infectious DiseasesNY State Department of
HealthWadsworth CenterDavid Axelrod InstitutePO Box 22002Albany, NY 12201-2002
Alexander Tomasz, Ph.D.Professor and Head/Laboratory
of MicrobiologyThe Rockefeller University1230 York Ave., Box 152New York, NY 10021-6399
Richard Wenzel, M.D., M.Sc.Associate ChairmanDepartment of Internal
MedicineThe University of IowaIowa City, IA 52242
Craig Townsend, Ph.D.Chairman, Department of
ChemistryThe Johns Hopkins UniversityCharles and 34th StreetsBaltimore, MD 21218
Michael Zasloff, M.D., Ph.D.President, Magainin Research
Institute5110 Campus DrivePlymouth Meeting, PA 19462
vi
Project Staff
Clyde J. BehneyAssistant Director, OTA
Sean TunisHealth Program Director
ADMINISTRATIVE STAFF
Charlotte BrownWord Processing Specialist
Monica FinchWord Processing Specialist
Louise StaleyOffice Administrator
Carolyn SwannPC Specialist
PRIMARY STAFF
Michael GoughProject Director
Elise BerlinerCongressional Fellow
Dwayne L. SmithResearch Assistant
Jacqueline T. KellerResearch Analyst
CONTRIBUTING STAFF
Beth HadleySenior Analyst
CONTRACTORS
Michael J. BennettWashington, DC
Mitchell BurkenPhiladelphia V.A. Hospital
Julian DaviesThe University of British
Columbia
Susan FeinmanPotomac, Maryland
David FrankelThe Lancet
Sandra HandwergerRockefeller University
Kathie E. HannaChurchton, Maryland
Judith HellersteinNorthwestern University
James H. JorgensenUniversity of Texas
Karen KaunitzJacksonville Baptist Medical
Center
Calvin KuninOhio State University
David H. PersingMayo Clinic Rochester
David RelmanStanford University
Barbara RosenkrantzHarvard University
Lee SabathUniversity of Minnesota
vii
Contents
1 Summary, Conclusions, Issues and Options 1Summary 1Origins of the Antibiotic Era 2Survey of Antibiotic Resistance 3Costs of Antibiotic-Resistant Bacterial Diseases6Reducing the Impacts of Antibiotic-Resistant Bacteria8Conclusions 18Issues and Options for Prolonging Effectiveness of
Antibiotics 19Issues and Options for Encouraging Development
of New Antibiotics 28
2 Introduction 33The Discovery of Antibiotics 36Confronting Antibiotic Resistance 45References 46
3 Antibiotic Use and Resistance in the Community 49Introduction 49Populations Susceptible to Antibiotic-Resistant
Bacteria 53Factors in the Emergence of Bacterial Diseases57Changes in Disease Patterns59Surveillance of Antibiotic-Resistant Bacteria61Conclusions 63References 65
4 Antibiotic Use in Hospitals 69Infections Acquired in the Hospital 69The Rise of Antibiotic-Resistant Infections in
Hospitals 71The Uses of Antibiotics in Hospitals73Legal Aspects of Antibiotic Use 75Controlling the Emergence and Spread of Antibiotic
Resistance in Hospitals76
viii
Hospital Accreditation and Infection Control Regulations Under Medicare 80
Costs of Controlling the Emergence and Spread of Antibiotic-Resistant Bacteria 93
Conclusions 96References 96
5 Antibiotic Development 101Designing New Antibiotics 101Antibiotics in Current Clinical Use 104Antibiotics That Inhibit or Block DNA Replication or
Protein Synthesis 109Development of New Antibiotics From Old110New Research Tools 113Antibiotics From New Sources 113Getting New Antibiotics to Market 118Patents 120Pricing of Drugs Developed in Part by Federal
Research 121Conclusions 121References 122
6 New Technologies for Infection Diagnosis and Control 127Diagnostic Methods 127Vaccines 142Stimulating the Immune System146Targeted Delivery of Antibiotics 146Reducing Infections by Modifying Devices147Old Therapies 150Summary 151References 151
ix
7 Antibiotics in Animal Husbandry 155Antibiotic Use in Food Production 158Antibiotic-Resistant Bacteria in Humans159Controversy About Antibiotic Use in Raising
Livestock 162Controversy Over Fluoroquinolones in Food
Production 164References 165
Appendix A: Coverage of Antibiotic Resistance in the Popular Literature, 1950 to 1994 167
Appendix B: Glossary 173
Appendix C: Acknowledgments 181
| 1
1
Summary,Conclusions,
Issues andOptions
SUMMARYs more and more bacteria become resis-tant to the effects of antibiotics and asthe flow of new antibiotics into medicalpractice slows, it is clear that the pro-
nouncement of the Surgeon General of theUnited States nearly a quarter century ago that itwas time to “close the book on infectious dis-eases” was premature.1 Indeed, the popular pressand some experts worry that we are headedtoward an era of infectious diseases akin to theone that existed before antibiotics were intro-duced over a half-century ago.
This Office of Technology Assessment (OTA)report is a response to congressional requests(see box 1-1) for a description of the threat posedby antibiotic-resistant bacteria to our society.This report explores the biological bases for thedevelopment of bacterial resistance to antibiot-ics, describes new antibiotics that are in researchand development, and outlines a number of strat-egies to control the proliferation of antibiotic-resistant bacteria.
1 Citations to the literature are not included in this summary. Complete citations are included in other chapters.
❚ Impacts of Antibiotic-Resistant Bacteria:■ Difficult-to-treat infections: Many strains of
bacteria are resistant to one or more of the 100antibiotics now in use. Physicians may have totry a number of different antibiotics until oneproves effective.
■ Untreatable infections: Some strains of bacte-ria are resistant to all available antibiotics.Currently, infections caused by these bacteriaare fairly uncommon, but they are rapidlyincreasing. Additionally, other bacteria areresistant to all but one antibiotic, and they areexpected to become resistant to all antibiotics.
■ Antibiotic use increases the spread of antibi-otic-resistant bacteria: Antibiotic use creates“selective pressure” that promotes the spreadof resistant bacteria. Susceptible bacteria arekilled or inhibited, and resistant bacteria sur-vive and multiply. As bacteria become resis-tant to increasing numbers of antibiotics, theremaining effective antibiotics are used moreoften—increasing the selection pressure forbacteria to become resistant to them.
A
2 | Impacts of Antibiotic-Resistant Bacteria
■ Costs: OTA estimates the in-hospital costs ofhospital-acquired (nosocomial) infectionscaused by six common kinds of antibiotic-resistant bacteria to be a minimum of $1.3 bil-lion. The estimate ignores the costs of infec-tions caused by other kinds of antibiotic-resistant bacteria, costs of lost work days, andcosts for post-hospital care. If these factorswere considered, the total cost to societywould be at least several billion dollars peryear. Further, these costs can be expected toincrease rapidly as the numbers of antibiotic-resistant bacteria increase.
■ Antibiotic-resistant bacteria spread inter-nationally: Antibiotic-resistant bacteria arefound all over the world and are spread amongcountries as people and goods are transportedinternationally.
❚ Controlling Antibiotic-Resistant Bacteria■ Prolong the effectiveness of currently avail-
able antibiotics through three primaryactivities:1) Prudent use of antibiotics: Studies indicate
that many antibiotics are overused or usedinappropriately. Physicians who prescribeantibiotics in the hospital or in their officepractices often face difficult choices indeciding whether to prescribe an antibioticand which one to prescribe. Surveillancesystems to track the emergence and spreadof disease-causing bacteria are essential.New technologies that quickly and accu-
rately identify bacteria will improve use ofantibiotics.
2) Vaccines: Vaccines prevent infections andreduce the need for antibiotics. Effectivevaccines against bacteria will reduce theuse of antibiotics.
3) Infection control: Effective infection con-trol efforts range from simple proceduressuch as diligence in hand-washing to newmaterials for use in medical devices thatimpede the growth of bacteria.
■ Develop new antibiotics: New antibiotics arenecessary to treat bacteria that are resistant tocurrently available antibiotics. Pharmaceu-tical companies are currently searching fornew antibiotics by screening biological com-pounds for antibacterial activity and by use ofnew techniques to design molecules that areactive against specific biochemical pathwaysin bacteria.
ORIGINS OF THE ANTIBIOTIC ERAA century ago, physicians had few effectivemedicines to treat infectious diseases. Plenty ofmedicines existed, but most had no effect exceptto offer the relief associated with narcotics andalcohol. Physicians prescribed elixirs, nostrums,and potions for all sorts of illnesses. Systematicexamination of their effectiveness, which beganin the 1890s, showed that few had worth. Withfew effective treatments, the physician’s role waslimited to informing the patient and family aboutthe expected course of the disease and keepingthe patient comfortable, clean, and nourished
BOX 1-1: Origins of This OTA Study
In 1994, two Committees of Congress asked OTA to prepare a report that describes the incidence ofinfections with antibiotic-resistant bacteria in hospitals and in the community and any information aboutthe costs of such infections. Moreover, the request asked how surveillance of antibiotic-resistant bacteriacan be improved and for descriptions of the relationships between virulence and antibiotic resistance inbacteria, the state of the search for new antibiotics, and the success or lack of success in efforts to con-trol the ongoing spread of antibiotic-resistant bacteria. In addition, OTA was asked to discuss issues thatarise in attempts to control the impacts of antibiotic-resistant bacteria and to present options for actionsby Congress and other organizations.

Chapter 1 Summary, Conclusions, Issues and Options | 3
while waiting for the body’s immune system toovercome the infection, if it could.
In 1928, the English microbiologist AlexanderFleming discovered that a common mold (Peni-cillium) produced a substance—penicillin—thatkilled bacteria. This became the foundation of anew era in treatment of infectious diseases.About a decade later, a British research and engi-neering team led by H.W. Florey developedmethods for the large-scale production of peni-cillin. Penicillin became known as the “wonderdrug,” and diseases that were once life-threaten-ing became manageable.
Over time, however, bacteria demonstratedtheir ability to “fight back.” In 1945, shortly afterpenicillin’s debut into hospitals, scientists iso-lated Staphylococcus aureus strains that wereresistant to the drug, and by the 1950s, suchstrains were a common cause of disease in hospi-tals where penicillin had been heavily used. Thesemi-synthetic penicillin methicillin was tempo-rarily effective against hospital strains of Staph.aureus, but only one year after methicillin’sintroduction in 1960, a study reported strainsresistant to it. By 1991, more than 40 percent ofStaph. aureus strains in some large hospitalswere methicillin-resistant, and some of thosestrains were resistant to all antibiotics exceptvancomycin.
Vancomycin-resistant Enterococcus (VRE)are strains of Enterococcus resistant to the antibi-otic vancomycin. Some strains of VRE are resis-tant to all Food and Drug Administration (FDA)-approved antibiotics.2 In 1994, 15 percent of theenterococcus infections in intensive care units(ICUs) were resistant to vancomycin, as werealmost 10 percent of the enterococcal strainsacquired outside the ICUs.
Today, antibiotics remain effective againstmost bacterial diseases, but some antibiotics areno longer effective against infectious diseasesthat they defeated only a few years ago. More-over, the spread of methicillin-resistant Staphylo-
2 A drug now in the final stage of clinical trials may work against some strains of VRE, and it is available under an FDA emergency-useprogram, upon request to the manufacturer (Rhone-Poulenc Rorer, 1995).
coccus aureus (MRSA) and VRE and theexpectation that other bacteria will develop resis-tance to all or almost all antibiotics warn that wemay be entering a post-antibiotic era.
SURVEY OF ANTIBIOTIC RESISTANCE
❚ The Microbial BattlefieldThe ongoing survival contest between microor-ganisms and antibiotics dates back millions ofyears. Bacteria live in the soil and other placeswhere they compete with other bacteria andmicroorganisms for nutrients. Over time, somemicroorganisms, such as the Penicillium mold,have evolved the biochemical machinery to pro-duce antibiotics, such as penicillin, that inhibitgrowth of or kill bacteria. This eliminates com-petitors for nutrients.
“Antibiotic-resistant bacteria” are strains ofbacteria that were once susceptible to an antibi-otic but have since acquired resistance after theintroduction of antibiotics into medical practice.Antibiotic resistance operates through one offour general mechanisms. The resistant bacte-rium: 1) does not absorb the antibiotic, or 2)expels it, or 3) degrades it, or 4) has altered theusual molecular target for the antibiotic so thatthe drug has no effect.
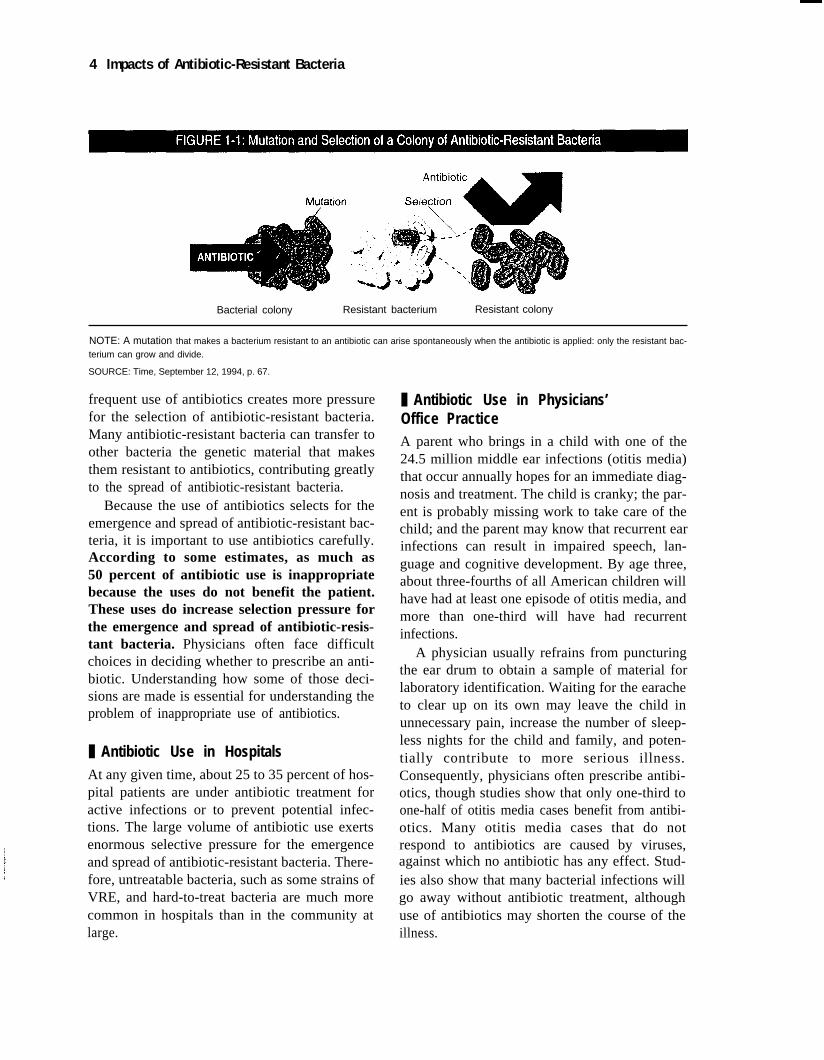
Resistance results from mutations that arisespontaneously in bacteria. Mutation is a rareevent—occurring once in a few million or a fewhundred million bacteria, for instance—but theprobability of a mutation occurring during aninfection is the product of mutation and the num-ber of bacteria, and millions of bacteria can bepresent in an infection. If a mutation for resis-tance to an antibiotic does occur, and if the per-son is being treated with that antibiotic, theantibiotic will kill off or inhibit the non-resistantor “susceptible” bacteria (see figure 1-1), leavingthe antibiotic-resistant bacteria to multiply andflourish. This is the process of “selection.” More
4 Impacts of Antibiotic-Resistant Bacteria
Bacterial colony Resistant bacterium Resistant colony
NOTE: A mutation that makes a bacterium resistant to an antibiotic can arise spontaneously when the antibiotic is applied: only the resistant bac-
terium can grow and divide.
SOURCE: Time, September 12, 1994, p. 67.
frequent use of antibiotics creates more pressurefor the selection of antibiotic-resistant bacteria.Many antibiotic-resistant bacteria can transfer toother bacteria the genetic material that makesthem resistant to antibiotics, contributing greatlyto the spread of antibiotic-resistant bacteria.
Because the use of antibiotics selects for theemergence and spread of antibiotic-resistant bac-teria, it is important to use antibiotics carefully.According to some estimates, as much as50 percent of antibiotic use is inappropriatebecause the uses do not benefit the patient.These uses do increase selection pressure forthe emergence and spread of antibiotic-resis-tant bacteria. Physicians often face difficultchoices in deciding whether to prescribe an anti-biotic. Understanding how some of those deci-sions are made is essential for understanding theproblem of inappropriate use of antibiotics.
❚ Antibiotic Use in HospitalsAt any given time, about 25 to 35 percent of hos-pital patients are under antibiotic treatment foractive infections or to prevent potential infec-tions. The large volume of antibiotic use exertsenormous selective pressure for the emergenceand spread of antibiotic-resistant bacteria. There-fore, untreatable bacteria, such as some strains ofVRE, and hard-to-treat bacteria are much morecommon in hospitals than in the community atlarge.
❚ Antibiotic Use in Physicians’Office PracticeA parent who brings in a child with one of the24.5 million middle ear infections (otitis media)that occur annually hopes for an immediate diag-nosis and treatment. The child is cranky; the par-ent is probably missing work to take care of thechild; and the parent may know that recurrent earinfections can result in impaired speech, lan-guage and cognitive development. By age three,about three-fourths of all American children willhave had at least one episode of otitis media, andmore than one-third will have had recurrentinfections.
A physician usually refrains from puncturingthe ear drum to obtain a sample of material forlaboratory identification. Waiting for the earacheto clear up on its own may leave the child inunnecessary pain, increase the number of sleep-less nights for the child and family, and poten-tially contribute to more serious illness.Consequently, physicians often prescribe antibi-otics, though studies show that only one-third toone-half of otitis media cases benefit from antibi-otics. Many otitis media cases that do notrespond to antibiotics are caused by viruses,against which no antibiotic has any effect. Stud-ies also show that many bacterial infections willgo away without antibiotic treatment, althoughuse of antibiotics may shorten the course of theillness.

Chapter 1 Summary, Conclusions, Issues and Options | 5
Faced with the uncertainties of diagnosis andthe certainty that at least some of their patientswill benefit from antibiotics, most physicianswill prescribe an antibiotic, generally amoxicil-lin, because it is usually effective against allthree of the common bacterial causes of otitismedia. Even so, amoxicillin will be ineffectiveagainst 10 to 15 percent of infections caused bythe three common bacterial agents of otitis mediabecause the bacteria will be resistant. Anotherantibiotic may have to be prescribed in thosecases.
Experience of treatment failures with amox-icillin may encourage the physician to routinelyprescribe antibiotics other than amoxicillin.Antibiotic prescription patterns are also influ-enced by patient expectation or demand (seebox 3-1 in chapter 3 for misperceptions aboutantibiotic use) and promotion by pharmaceuticalcompanies.
❚ Antibiotic Resistance in the CommunityEveryone is at risk for infections caused by anti-biotic-resistant bacteria, but some populationsare at particularly high risk. Those communitiesrange from the poor, who often live in crowdedconditions with less than optimal hygiene andmedical care, to middle-class children in daycarecenters, who are at high risk for otitis media andother infectious diseases. Other populations athigher risk are people in institutions such as hos-pitals, nursing homes, prisons and military instal-lations. People with diseases or conditions thatsuppress the immune system are also at increasedrisk. However, once antibiotic-resistant bacteriaemerge in these populations, they can be spreadwidely to other groups.
Factors in the Emergence of Antibiotic-Resistant BacteriaSome of the bacteria acquired in the communityare antibiotic-resistant and have been carried intothe community by people returning from hospi-tals where antibiotic-resistant bacteria are morecommon. Some arrive by other means. Moderntransportation has fostered global accessibility
and allows humans and their microbes to travelmore quickly than ever before. For example, epi-demiologists have tracked the spread of a multi-ple-resistant strain of Streptococcus pneumoniaefrom Spain to Iceland. Other factors that contrib-ute to the emergence and spread of antibiotic-resistant bacteria, as well as the spread of otherbacteria in the community are improper foodpreparation practices both in homes and com-mercial establishments, inadequate water treat-ment and inspection, and poor sanitation andhygiene.
Prevalence of Antibiotic-Resistant Bacterial Diseases in the CommunityNo one knows how common antibiotic-resistantbacteria are in the community. The United Stateshas no surveillance system to track antibiotic-resistant bacteria over wide areas, and ourknowledge of community patterns is restricted toa few studies in specific geographic areas and toinformation about antibiotic resistance in gonor-rhea and tuberculosis. Both are “notifiable dis-eases,” and cases of these diseases are to bereported to the Centers for Disease Control andPrevention (CDC). Even so, information aboutthe antibiotic susceptibility or resistance of thosebacteria is often not obtained or reported.
GonorrheaPenicillin-resistant strains of Neisseria gonor-rhoeae are now found in at least 17 countries.Between 1988 and 1991, CDC documented a50 percent increase in the proportion of penicil-lin- or tetracycline-resistant N. gonorrhoeae.This finding led CDC to discourage the use ofpenicillin or tetracycline as first-line treatmentfor the disease. Gonorrhea is an example ofwidespread resistance forcing the use of newer,more expensive antibiotics as primary treatment.In welcome contrast, Treponema pallidum, thecause of syphilis, remains universally susceptibleto penicillin.
TuberculosisPublic health measures and the use of antibioticsreduced the number of tuberculosis (TB) cases

6 | Impacts of Antibiotic-Resistant Bacteria
from 135,000 in 1947 to 22,000 in 1985 andfueled the expectation that the disease would beconquered. By 1992, however, the number ofcases had resurged to 30,000.
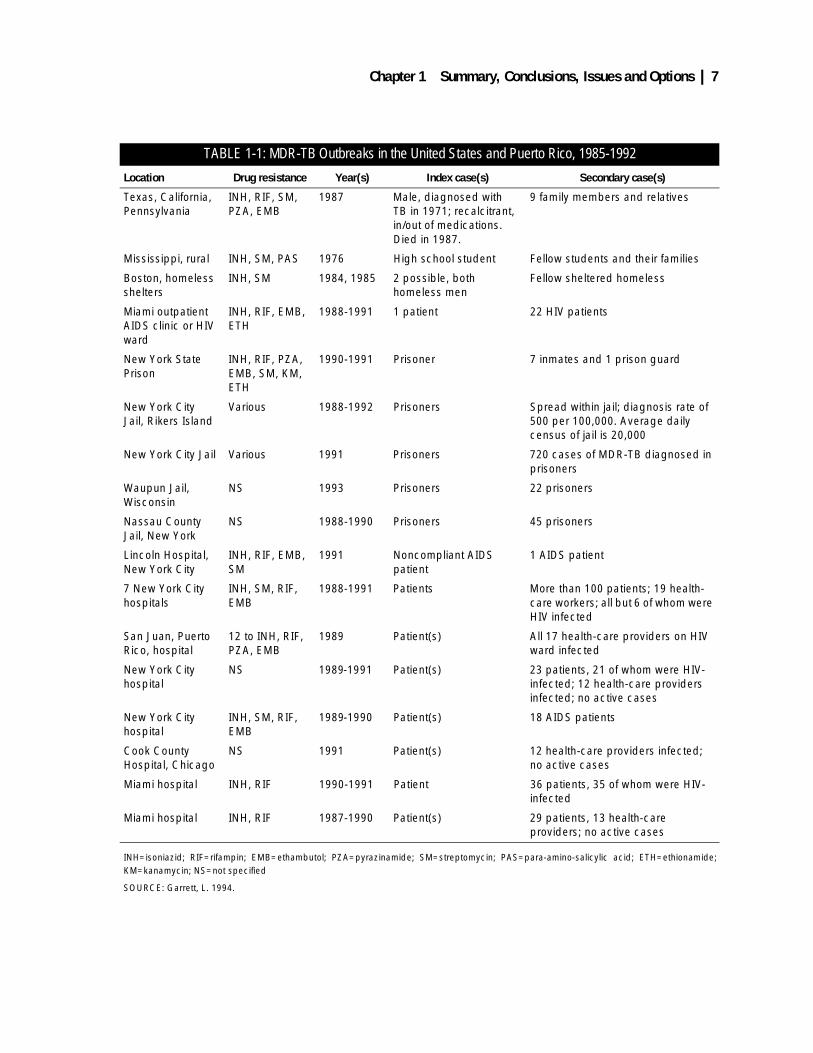
Drug-resistant strains of TB present a majorchallenge to health officials. In 1991, in NewYork City, 14 percent of all newly diagnosed TBcases were resistant to one or more antibioticsused for primary treatment, and 60 percent of therelapse cases in the first 12 weeks of the yearwere multiply drug resistant (MDR). Thesestrains spread from impoverished homeless pop-ulations of New York City to their health careproviders, jail guards, fellow patients inside hos-pitals, and other parts of the country. Table 1-1illustrates the MDR-TB outbreaks in the UnitedStates and Puerto Rico from 1985 to 1992.
❚ Antibiotic Use in Animal HusbandryProbably no other issue about antibiotic-resistantbacteria elicits more emotion than questionsabout the impact of the use of antibiotics in ani-mal husbandry on the appearance of antibiotic-resistant bacteria in humans (see chapter 7).
About half, by weight, of the antibiotics usedin the United States are used in the production offood animals, such as swine, cattle, and poultry,and the most used antibiotics are “old” ones, pen-icillin and the tetracyclines. Almost 90 percent ofthe agricultural use is for prophylaxis or growthpromotion, rather than for treatment of sickanimals.
Long-term use of antibiotics such as penicillinand tetracyclines decreases the time necessary toraise an animal to marketable weight or reducesthe amount of feed necessary to reach suchweights. Perhaps because those uses are equatedonly with economic gain, the strongest criticismshave usually been addressed at such long-termuses.
There is no question that agricultural uses ofantibiotics select for antibiotic-resistant bacteriajust as do medical uses. For instance, some anti-biotic-resistant Salmonella cases have beentraced back to meat from animals fed antibiotics.Questions arise about the quantitative public
health importance of antibiotic-resistant bacteriafrom agriculture. No differences in the preva-lence of antibiotic-resistant bacteria were foundbetween groups of people who ate meat andgroups who did not eat meat. Indeed, there was aslightly increased frequency of multiply resistantbacteria in the vegetarians. These results are con-sistent with the conclusion that meat is not theonly source of antibiotic-resistant bacteria, butthey do not show that meat is unimportant nor dothey pinpoint the other sources of antibiotic-resistant bacteria in the diet.
Over the last two decades, the FDA, theNational Academy of Sciences, OTA, and offi-cial boards and committees overseas have exam-ined the evidence for the contribution thatagricultural uses of antibiotics make to humandiseases or to the prevalence of antibiotic-resis-tant bacteria. None was able to pinpoint data thatshow the extent of the problem, and all havepointed to the great difficulties in studying thisissue.
COSTS OF ANTIBIOTIC-RESISTANT BACTERIAL DISEASESBecause of the costs involved in controlling andmonitoring the spread of antibiotic-resistant bac-teria, it would be useful to know how muchwould be saved by reducing the impacts of anti-biotic-resistant bacteria. Calculation of the costsimposed by antibiotic-resistant bacteria caninclude such factors as the direct cost of time in ahospital, the costs of extra physicians’ visitswhen antibiotics are ineffective, the extra hospi-talizations due to community-acquired resistantinfections, and the costs of newer antibiotics toreplace antibiotics to which bacteria havebecome resistant. Other costs include lost workdays and deaths, if they occur. Only one suchstudy has been published, and it included theestimate that the cost of antibiotic-resistant bac-teria nationwide was between $100 million and$30 billion annually, with different valuesattached to the cost of a life accounting for mostof the wide range of the estimate. A medical
Chapter 1 Summary, Conclusions, Issues and Options | 7
TABLE 1-1: MDR-TB Outbreaks in the United States and Puerto Rico, 1985-1992
Location Drug resistance Year(s) Index case(s) Secondary case(s)
Texas, California, Pennsylvania
INH, RIF, SM, PZA, EMB
1987 Male, diagnosed with TB in 1971; recalcitrant, in/out of medications. Died in 1987.
9 family members and relatives
Mississippi, rural INH, SM, PAS 1976 High school student Fellow students and their families
Boston, homeless shelters
INH, SM 1984, 1985 2 possible, both homeless men
Fellow sheltered homeless
Miami outpatient AIDS clinic or HIV ward
INH, RIF, EMB, ETH
1988-1991 1 patient 22 HIV patients
New York State Prison
INH, RIF, PZA, EMB, SM, KM, ETH
1990-1991 Prisoner 7 inmates and 1 prison guard
New York City Jail, Rikers Island
Various 1988-1992 Prisoners Spread within jail; diagnosis rate of 500 per 100,000. Average daily census of jail is 20,000
New York City Jail Various 1991 Prisoners 720 cases of MDR-TB diagnosed in prisoners
Waupun Jail, Wisconsin
NS 1993 Prisoners 22 prisoners
Nassau County Jail, New York
NS 1988-1990 Prisoners 45 prisoners
Lincoln Hospital, New York City
INH, RIF, EMB, SM
1991 Noncompliant AIDS patient
1 AIDS patient
7 New York City hospitals
INH, SM, RIF, EMB
1988-1991 Patients More than 100 patients; 19 health-care workers; all but 6 of whom were HIV infected
San Juan, Puerto Rico, hospital
12 to INH, RIF, PZA, EMB
1989 Patient(s) All 17 health-care providers on HIV ward infected
New York City hospital
NS 1989-1991 Patient(s) 23 patients, 21 of whom were HIV- infected; 12 health-care providers infected; no active cases
New York City hospital
INH, SM, RIF, EMB
1989-1990 Patient(s) 18 AIDS patients
Cook County Hospital, Chicago
NS 1991 Patient(s) 12 health-care providers infected; no active cases
Miami hospital INH, RIF 1990-1991 Patient 36 patients, 35 of whom were HIV- infected
Miami hospital INH, RIF 1987-1990 Patient(s) 29 patients, 13 health-care providers; no active cases
INH=isoniazid; RIF=rifampin; EMB=ethambutol; PZA=pyrazinamide; SM=streptomycin; PAS=para-amino-salicylic acid; ETH=ethionamide;KM=kanamycin; NS=not specified
SOURCE: Garrett, L. 1994.

8 | Impacts of Antibiotic-Resistant Bacteria
society subsequently estimated the costs of suchdiseases at $4 billion.
In this report, OTA calculates the direct hospi-tal costs from five classes of nosocomial infec-tions associated with only six different strains ofantibiotic-resistant bacteria and concluded thatthe minimum nationwide hospital costs of thoseinfections was $1.3 billion in 1992 dollars. Add-ing other infections associated with other bacte-ria and other costs in addition to direct hospitalcosts would increase the total to several billiondollars. This number can be expected to increaseas the numbers of antibiotic-resistant bacteriaincrease.
REDUCING THE IMPACTS OF ANTIBIOTIC-RESISTANT BACTERIAThe impacts of antibiotic-resistant bacteria canbe reduced by preserving the effectiveness ofcurrent antibiotics through infection control, vac-cination and prudent use of antibiotics, and bydeveloping new antibiotics specifically to treatinfections caused by antibiotic-resistant bacteria.
❚ Preserving the Effectiveness of Current AntibioticsReducing infection rates, which will reduce thedemands for antibiotics, will reduce the pressuresfor selection of antibiotic-resistant bacteria.
SurveillanceSurveillance systems are necessary to track pat-terns of antibiotic resistance. At the local level,physicians can use the information to chooseappropriate antibiotics. At the national level,pharmaceutical companies can use the informa-tion to plan new drug development.
Many hospitals have surveillance systems totrack the spread of disease-causing organisms,including antibiotic-resistant bacteria, and to pro-vide information to physicians about the use andeffectiveness of antibiotics. These systems havesaved hospitals money; for example, a system inthe LDS Hospital in Salt Lake City, Utah, moni-tored the use of prophylactic antibiotics beforesurgery. This system reduced unnecessary antibi-
otic use and saved $42 per patient, resulting in aprojected cost savings to the hospital of $89,000per year.
At the state level, the New Jersey Departmentof Health collects data about antibiotic-resistantbacteria from microbiology laboratories in eachof the 95 acute care general hospitals licensed bythe Department. Since its inception in 1991, allNew Jersey hospitals have submitted monthlyreports to the Department of Health, which col-lects and analyzes the data and makes it availableto all participating hospitals and to the public.The surveillance system has been used to studymany questions about antibiotic-resistant bacte-ria including: patient risk factors for VRE bacter-emia, the role of antibiotic usage in VREbacteremia, the effectiveness of infection controlpractices in preventing nosocomial transmissionof VRE, and VRE susceptibility to the experi-mental drug quinupristin/dalfopristin. The sys-tem’s operation requires about a day’s work byone person each month in the State Departmentof Health.
SCOPE, Surveillance and Control of Patho-gens of Epidemiological Importance, is anational effort established by the University ofIowa and Lederle Laboratories (now Wyeth-Ayrst Lederle Laboratories) in 1995. The pro-gram expects to collect reports of all nosocomialbloodstream infections in 48 hospitals nation-wide as well as samples of the organisms isolatedfrom the infected patients. The reports will pro-vide information about the spread of antibiotic-resistant bacteria in the hospitals.
There are also other industry-funded surveil-lance systems. A number of academic and com-mercial laboratories conduct surveillance undercontract to pharmaceutical companies, but theyare not necessarily designed to obtain informa-tion most useful for public health purposes.
The CDC-run National Nosocomial InfectionSurveillance (NNIS) is the single nationwide sur-veillance system that produces information aboutantibiotic-resistant bacteria. While it is limited toreports on nosocomial infections from about 200hospitals, it is the source for most of the data inthis report about MRSA, VRE, and other drug-

Chapter 1 Summary, Conclusions, Issues and Options | 9
resistant bacterial infections. NNIS publishesresults infrequently and at long intervals after thedata are collected. NNIS, in whatever form itcontinues, should be urged to publish in a timelyfashion so that data can be used more efficiently.
CDC is in the early stages of establishingnationwide surveillance of drug-resistant S.pneumoniae (DRSP), which will cover infectionswhether or not they occur in a hospital. Success-ful establishment and operation of that systemcould provide a model for surveillance of allantibiotic-resistant bacteria, but the full systemwould require additional funding. As an earlystep in setting up the DRSP system, and atCDC’s request, the Council of State and Territo-rial Epidemiologists has recommended DRSP forinclusion on the list of notifiable diseases, andfour states now report it. The CDC initiatedDRSP in 20 laboratories in New Jersey in April1995, and if funds are available, CDC expectsthat most of the nearly 2,000 hospital and com-mercial laboratories that now have computerizedrecord keeping will be on the system by 1998. Aslaboratories add computer capabilities, the CDCwill encourage them to enlist in the system,expecting that all of the nearly 5,000 laboratoriesin the country will eventually participate. If theDRSP system works, CDC envisions expandingit to include other antibiotic-resistant bacteria.
WHONET, an established surveillanceproject, is a computer-based system that is spon-sored by the World Health Organization. It tracksthe resistance patterns of bacteria in clinicalmicrobiology laboratories in hospitals worldwideand provides the participating hospitals withmethods to follow the spread of antibiotic-resis-tant bacteria and to examine the efficacy of localinfection control procedures. WHONET wasestablished by two people, and it is maintainedsingle-handedly by Dr. Thomas O’Brien of theBrigham and Women’s Hospital, Boston, MA.
Even with its limited resources, WHONEThas about 100 participating hospitals, and someof those hospitals report information from largeareas, up to the size of countries. It is a primarysource of data about antibiotic-resistant bacteriaaround the world, and it provides a method to
track the flow of bacteria from country to coun-try. It also provides scientists in the participatinghospitals a powerful tool to analyze the spread ofantibiotic-resistant bacteria in their own hospi-tals.
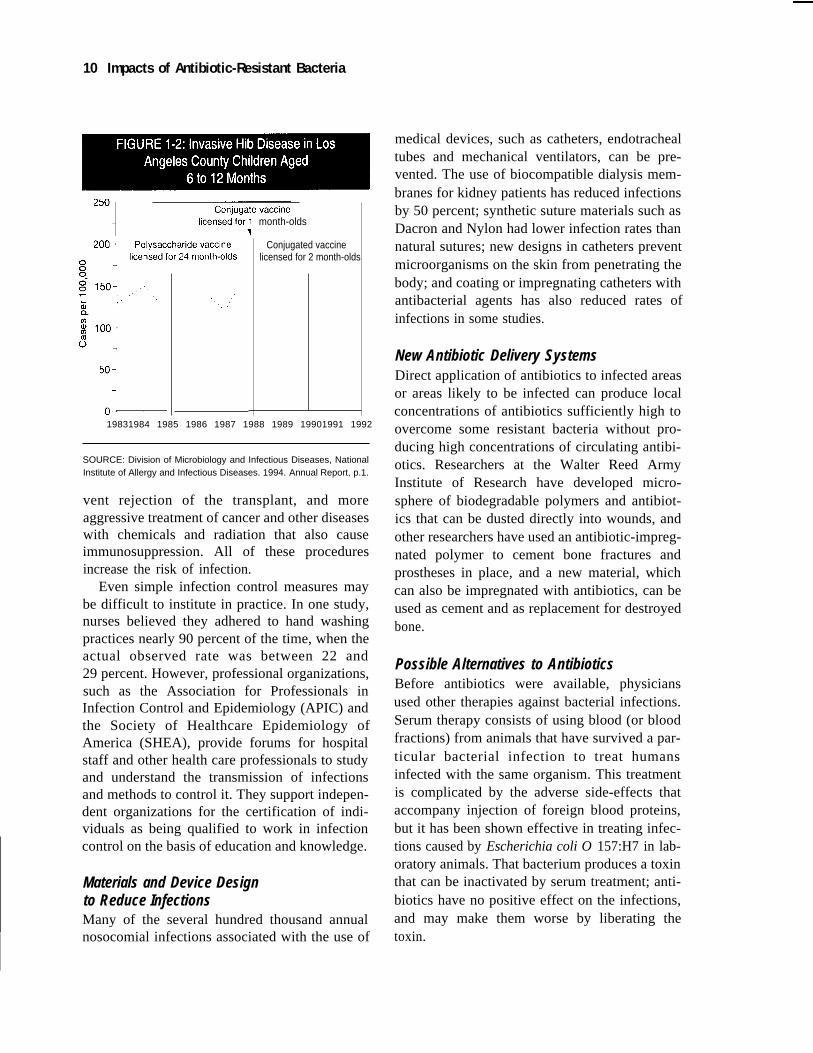
VaccinesVaccines now protect millions of people frombacterial and viral diseases, and as shown in fig-ure 1-2, successful vaccines can have a rapid,profound effect on bacterial disease rates. Vac-cines that are successful against pathogenic bac-teria will protect against both antibiotic-sensitiveand antibiotic-resistant strains and reduce theneed for antibiotics and the selection pressure forthe emergence of resistance. While the rate ofintroduction of new vaccines has been slow inyears past, new developments in molecular biol-ogy research may increase the rate in the nearfuture.
The policies surrounding vaccine develop-ment in the United States are not a focus of thisOTA report, but the Federal National VaccineProgram is often described as faltering andresearch as underfunded.
Infection ControlInfection control measures are a crucial elementin preserving the effectiveness of current antibi-otics. A 1976 CDC study showed that hospitalswith intensive infection control and surveillanceprograms could reduce the approximately twomillion infections acquired in hospitals per yearby 32 percent. The report identified handwash-ing, improved hygiene, and patient isolation assuccessful infection control efforts.
Despite whatever infection control methodswere put in place, the number of bloodstreaminfections increased by 70 percent in large teach-ing hospitals and 279 percent in small non-teach-ing hospitals during the 1980s. These increases,in part, reflect the increased life-saving capacityof modern medicine that includes increased sur-gery rates with attendant catheterizations andother invasive procedures, organ and tissue trans-plants that require immunosuppression to pre-
10 Impacts of Antibiotic-Resistant Bacteria
month-olds
Conjugated vaccinelicensed for 2 month-olds
19831984 1985 1986 1987 1988 1989 19901991 1992
SOURCE: Division of Microbiology and Infectious Diseases, NationalInstitute of Allergy and Infectious Diseases. 1994. Annual Report, p.1.
vent rejection of the transplant, and moreaggressive treatment of cancer and other diseaseswith chemicals and radiation that also causeimmunosuppression. All of these proceduresincrease the risk of infection.
Even simple infection control measures maybe difficult to institute in practice. In one study,nurses believed they adhered to hand washingpractices nearly 90 percent of the time, when theactual observed rate was between 22 and29 percent. However, professional organizations,such as the Association for Professionals inInfection Control and Epidemiology (APIC) andthe Society of Healthcare Epidemiology ofAmerica (SHEA), provide forums for hospitalstaff and other health care professionals to studyand understand the transmission of infectionsand methods to control it. They support indepen-dent organizations for the certification of indi-viduals as being qualified to work in infectioncontrol on the basis of education and knowledge.
Materials and Device Designto Reduce InfectionsMany of the several hundred thousand annualnosocomial infections associated with the use of
medical devices, such as catheters, endotrachealtubes and mechanical ventilators, can be pre-vented. The use of biocompatible dialysis mem-branes for kidney patients has reduced infectionsby 50 percent; synthetic suture materials such asDacron and Nylon had lower infection rates thannatural sutures; new designs in catheters preventmicroorganisms on the skin from penetrating thebody; and coating or impregnating catheters withantibacterial agents has also reduced rates ofinfections in some studies.
New Antibiotic Delivery SystemsDirect application of antibiotics to infected areasor areas likely to be infected can produce localconcentrations of antibiotics sufficiently high toovercome some resistant bacteria without pro-ducing high concentrations of circulating antibi-otics. Researchers at the Walter Reed ArmyInstitute of Research have developed micro-sphere of biodegradable polymers and antibiot-ics that can be dusted directly into wounds, andother researchers have used an antibiotic-impreg-nated polymer to cement bone fractures andprostheses in place, and a new material, whichcan also be impregnated with antibiotics, can beused as cement and as replacement for destroyedbone.
Possible Alternatives to AntibioticsBefore antibiotics were available, physiciansused other therapies against bacterial infections.Serum therapy consists of using blood (or bloodfractions) from animals that have survived a par-ticular bacterial infection to treat humansinfected with the same organism. This treatmentis complicated by the adverse side-effects thataccompany injection of foreign blood proteins,but it has been shown effective in treating infec-tions caused by Escherichia coli O 157:H7 in lab-oratory animals. That bacterium produces a toxinthat can be inactivated by serum treatment; anti-biotics have no positive effect on the infections,and may make them worse by liberating thetoxin.

Chapter 1 Summary, Conclusions, Issues and Options | 11
“Phage” or “bacteriophage” are viruses thatinfect and kill bacteria. Physicians used them totreat human infections in the years between theWorld Wars, and they were the research projectof the physician in Arrowsmith. Some scientistsbelieve study of their possible use in a post-anti-biotic era may be justified.
While both phage and serum therapy aresometimes suggested as alternatives to antibiot-ics, the rapid disappearance of both therapiesafter the introduction of antibiotics points to theirless-than-successful past. These old therapies arenot likely to receive serious consideration unlesseffective antibiotics disappear.
Optimizing Antibiotic UseA comparison of prescription records to verifiedcauses of disease shows that antibiotics are oftenprescribed for viral infections, for which theyhave no value, and for self-limited infections thatwould have cleared up whether or not an antibi-otic had been prescribed. Of course, the prescrip-tions are often, necessarily, written in advance orin the absence of the laboratory testing requiredto verify causes. While these cases offer evi-dence of inappropriate use of antibiotics, manyof them are, at least partially, understandable.Clearly inappropriate, however, is the admin-istration of prophylactic antibiotics at timesgreater than two hours before or after sur-gery; antibiotics administered at these timesare ineffective for preventing surgical woundinfections. Reducing inappropriate uses shouldretard the development of antibiotic resistance,and over the years, academicians and scientistshave urged better education of physicians aboutantibiotic use and resistance.
A new educational initiative being planned bya number of pharmaceutical companies, theAmerican Society for Microbiology, and CDCwill produce educational materials encouragingmore appropriate use of antibiotics. Other orga-nizations are making similar efforts. Evaluationof the success of those efforts could pinpoint theitems in the educational package that make themost difference. OTA’s 1994 report IdentifyingHealth Technologies That Work describes the
features of successful programs designed toinfluence physician behavior.
Past educational efforts have had limitedeffect, partially because not all cases of “over-use” are as clearly defined as the case of inappro-priately prescribing prophylactic antibiotics. Forexample, different interpretations are possible ofthe wisdom of giving a prophylactic dose of anti-biotics to the President after his exposure to alow risk of contracting an infection (see box 1-2). Another example is one type of ear infection(otitis media with effusion). The Agency forHealth Care Policy and Research recently wrotea guideline to clarify treatments for otitis media(not necessarily to promote prudent use of antibi-otics) and concluded that:
Meta-analysis for Guideline developmentshowed a 14 percent increase in the probabilitythat otitis media with effusion would resolvewhen antibiotic therapy was given versus notreatment....When this small improvement inresolution of otitis media with effusion isweighed against the side effects and cost ofantibiotic therapy, antibiotic therapy may not bepreferable to observation in management of oti-tis media with effusion in the otherwise healthyyoung child....
A physician who elected not to prescribe anantibiotic, foregoing the 14 percent increasedprobability that the condition “would resolve,”might be liable for legal action. Such potential lia-bility might encourage physicians to prescribeantibiotics even when they may not be indicated.The above guidelines do not instruct physicians toconsider the spread of antibiotic resistance in thedecision to prescribe antibiotics, only the cost andrisk vs. benefit of the antibiotic to the patient.
Some hospitals control drug use by establish-ing formularies, listings of approved drugs forvarious medical indications. Some Denver, Colo-rado, area hospitals combined their formularieswith a computerized antibiotic order form thatrequires physicians to enter the suspected causeof infection. The system saved the hospitalsmoney, and allowed officials there to change theformularies when susceptibility tests revealed anew pattern of antibiotic resistance.

12 | Impacts of Antibiotic-Resistant Bacteria
Managed care plans are beginning to employPharmacy Benefit Managers (PBMs) to monitorpharmacy use. PBMs analyze pharmacy use datato control costs and they may be helpful in set-ting guidelines for appropriate antibiotic use.
The LDS hospital in Salt Lake City, Utah,developed a computerized antibiotic monitoringsystem, which is part of a larger computerizedpatient record system that automatically collectssurveillance data and generates profiles of antibi-otic resistance in the hospital’s bacteria. Clini-cians enter the results of susceptibility tests intothe computer which checks to be certain that anyprescribed antibiotic will work and generates analert when an antibiotic is inappropriate. Anotherpart of the hospital’s system is a computerizedantibiotic consultant, which uses surveillancedata along with information about the site ofinfection and patient allergies to determine thebest choice of empiric antibiotic therapy. As
judged by a panel of infectious disease experts,this computer consultant “chose” the appropriateantibiotic 94 percent of the time, as compared toa 77-percent rate for the physicians. These sys-tems require up-front costs with no guaranteethat the costs will be recouped. Thus, convincinghospital administrators to invest in such a systemin financially strapped times appears difficult,despite the advantages such a system could bringto a hospital.
Diagnostic TechnologiesSore throats, as well as ear aches, are often men-tioned in connection with the overuse of antibiot-ics. When a physician sees a patient with a sorethroat, the physician asks about the patient’ssymptoms, examines the patient’s throat, notesthe inflammation, and may swab the throat topick up any organisms that are there. If the physi-cian is like more than 40 percent of all primary
BOX 1-2: The President's Doctor's Dilemma
On June 13, 1995, President Clinton took antibiotics to prevent a possible case of meningitis aftershaking hands with a college student who was diagnosed with the disease (Washington Post, June 14,1995, page A6).
Meningitis is often caused by Hemophilius influenzae type b (Hib), Neisseria meningitidis, or Strepro-coccus pneumoniae. A standard textbook (Mandell, Douglas and Bennett's Principles and Practices ofInfectious Disease, 4th Edition, pages 856–857) describes considerations for deciding when prophylacticantibiotics are necessary after contact with a patient with meningitis. For meningitis caused by Hib, thetextbook states that prophylaxis is indicated for household contacts, and possible for day care contacts,“...in day care centers that resemble households where children have prolonged contact.” For meningitiscaused by N. meningitidis, the textbook states that “Chemoprophylaxis is recommended for close con-tacts of the index case, defined as household contacts or close contacts in a closed community such asa military barracks or boarding school, and medical personnel performing mouth-to-mouth resuscitation.”For meningitis caused by S. pneumoniae, the textbook states that in one outbreak in a day care center,chemoprophylaxis “...did not prevent new acquisition of this organism by three children and one familymember. Further studies are needed before chemoprophylaxis is recommended for contacts ofpatients....”
Prescribing a dose of antibiotics for the President after he shook hands with someone with meningitisis an example of individual vs. public health considerations in the use of antibiotics. Shaking hands is apretty minor contact; far less intense than those for which the textbook recommended prophylaxis. How-ever, even the insignificant chance that the President was infected was considered worth one dose ofantibiotics. This illustrates a dilemma about appropriate antibiotic use. The President had the benefit ofthe antibiotic preventing a very small risk. The use of the antibiotic might increase the spread of antibiotic-resistant bacteria. Millions of such cases, justified on similar individual bases, would add together toincrease the risk of spread of antibiotic resistance.

Chapter 1 Summary, Conclusions, Issues and Options | 13
care physicians, he will begin antibiotic treat-ment without any more information. This ispartly because of the time necessary for a labora-tory to identify the bacteria associated with anillness.
Chapter 6 describes methods currently used toidentify bacteria and to determine their antibioticsusceptibility. Methods to determine susceptibil-ity rely on putting the bacteria into culture media,where the bacteria will grow, and also puttingthem into culture media with known concentra-tions of antibiotics. Laboratory personnel thendetermine which antibiotics and which concen-trations of antibiotics inhibit the growth of or killthe bacteria.
More rapid methods for making diagnosismight improve the physician’s decisions aboutprescribing antibiotics, but only if the resultshave high reliability. “Quick strep” tests for sorethroats produce results in 20 minutes. If the testresult is positive, 95 percent of the time the resultis accurate and strep is present. If the test doesnot indicate strep, there’s a 20–30 percent chancethat strep was present, but the test missed it.Guidelines recommend a follow-up culture forall negative “quick strep” tests. The result is thatthe “quick strep” test probably affects practiceonly marginally. All patients with a positive“quick strep” test will surely get an antibiotic,and many with a negative test will get antibioticsas well (at least until the results of a standard cul-ture assay are available). This result differs littlefrom what would likely happen in the absence ofthe test. The test provides an advance in the rightdirection, but further advances are necessary.
A strep test that employs DNA methodsreportedly produces results sufficiently accurateso that they do not have to be verified by stan-dard tests. However, the test is so involved thatits use will probably be restricted to large prac-tices or hospitals. Moreover, it produces resultsin a few hours, not in a few minutes. Even if thistest proves to be as good as it appears and it isadopted where there are large numbers ofpatients, it will not produce results during thecourse of an office visit. The physician may electto give the patient a prescription with instruc-
tions to call the office in a few hours to learn thetest results before the prescription is filled (ordiscarded). Of course, the patient might have theprescription filled regardless and save it foranother time. The impact of any test will dependa great deal on the interactions between physi-cian and patient until the results are so rapid thatthey are complete before the patient leaves theoffice.
Faster tests may have a marked impact in thediagnosis of tuberculosis so that patients can betreated before they pass the infectious disease toothers. Isolation of the slowly growing Mycobac-terium causing tuberculosis requires three toeight weeks, and susceptibility testing by tradi-tional methods can add 20 days to six weeks.New diagnostic tests based on identifying myco-bacterial DNA are being developed to allow phy-sicians to identify Mycobacteria in the sputum ofpatients within a few hours to a few days.
New diagnostic technologies raise some newissues. For instance, the DNA test for tuberculo-sis might be so sensitive that it can detect theDNA of Mycobacteria already killed or inhibitedby previous treatment. To act entirely on the testresult might result in treatments that are unneces-sary.
Tests which directly measure the presence ofan antibiotic-resistance gene in bacteria alsobring a new set of considerations. A gene forresistance that is detectable by the new testsmight not be “expressed,” and its detection mightnot accurately predict whether the bacteria willbe resistant or susceptible. Or a resistance genemay have undergone a mutation that does notaffect its function, but alters it so that a genetictest might not register the presence of the antibi-otic-resistant gene. All these issues are antici-pated in designing genetic tests and bringingthem to clinical practice.
Practice GuidelinesPractice guidelines are medical protocols that areintended to assist practitioners in making clinicaldecisions. For example, the Agency for HealthCare Policy and Research (AHCPR), a federalagency empowered to establish practice guide-

14 | Impacts of Antibiotic-Resistant Bacteria
lines, encourages health care providers to adoptits guidelines to improve patient care, patientoutcomes, and quality of life. Practice guidelinesthat are written to balance patient benefits andpublic health effects and that provide specificdirection about antibiotic use might reduce over-use. Nationwide data cannot capture the local-ized nature of antibiotic-resistant bacteria, but anonline computer system linking health care prac-titioners in a geographic area could provide thatinformation. Such a system would allow healthcare practitioners to consult with specialists indetermining the best way to comply with thepractice guidelines and would also allow healthcare practitioners to enter the specifics of theircases.
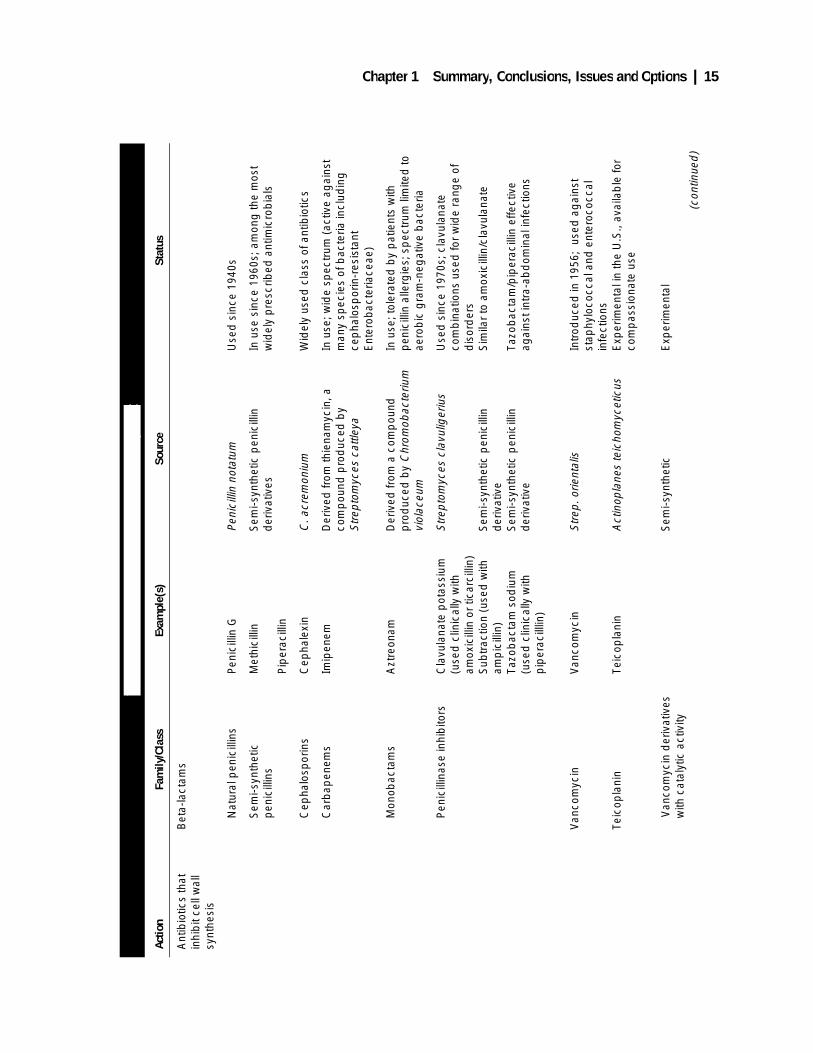
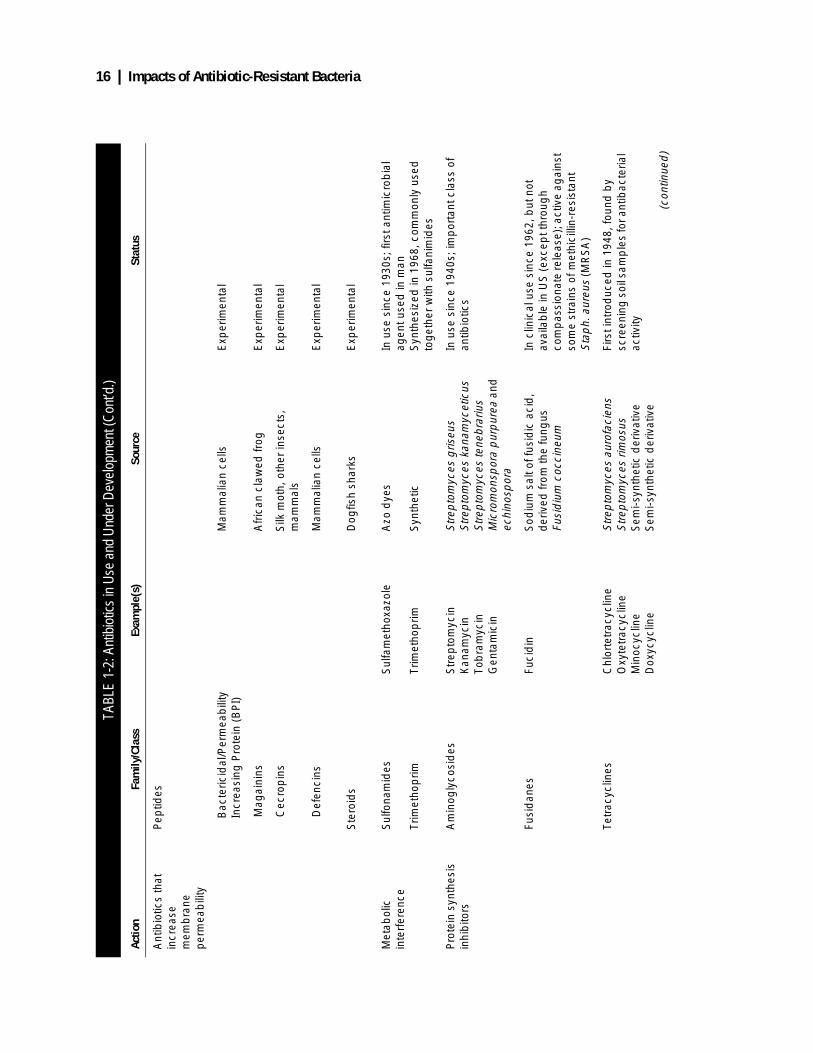
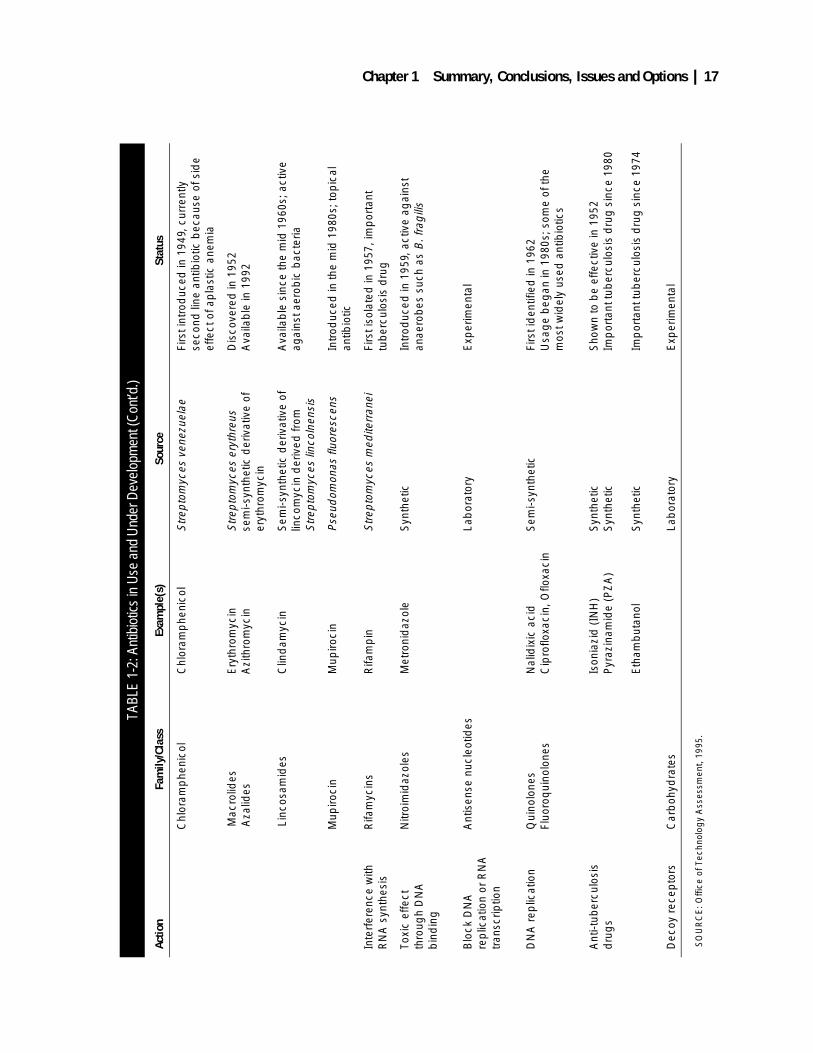
❚ Designing New AntibioticsIn the arms race with resistant bacteria, drugmanufacturers have research programs to isolateor synthesize new antibiotics or to develop deriv-atives of old ones that have greater antibacterialactivity, fewer side effects, or that can be admin-istered orally rather than requiring injections.Researchers are continuing to search throughsamples of soils and other materials rich in moldsand bacteria, which have yielded many of theexisting antibiotics, and they have widened thesearch to include carbohydrates, proteins, andsteroids from many biological sources. Compa-nies are investigating the use of modern chemicaltechniques to design new molecules for specificpurposes. While the payoff from any line ofresearch remains uncertain, many small, newcompanies as well as the older, established phar-maceutical companies are sufficiently confidentof producing useful products that they are invest-ing in antibiotic research (see chapter 5). Table1-2 lists some currently used and in-developmentantibiotics.
New antibiotics can be divided between thosethat are improvements on already-existing drugs,which depend on known mechanisms of action,and those drugs that have new mechanisms ofaction. None of the nine antibiotics approved by
FDA in 1992 and 1993 had a new mechanism ofaction, and no antibiotic was approved in 1994.
Antibiotics that depend on “old” mechanismsof action can be very useful (and profitable). Forinstance, cefaclor, a third-generation cepha-losporin, accounted for 15 percent of a majorpharmaceutical company’s sales when its patentexpired in 1992. It remains a clinically usefuldrug, and the company expects to retain a majorpart of the market for cephalosporins even afterthe expiration of patent protection. In general,however, antibiotics with new mechanisms ofaction might be expected to be more successfulas therapies against certain antibiotic-resistantbacteria because no similar antibiotics exertedpressure for the selection of resistance to them inthe past. Many of the substances currently beingexamined as potential antibiotics have novelmechanisms of action, and some may not fosterthe development of resistance (see chapter 5).
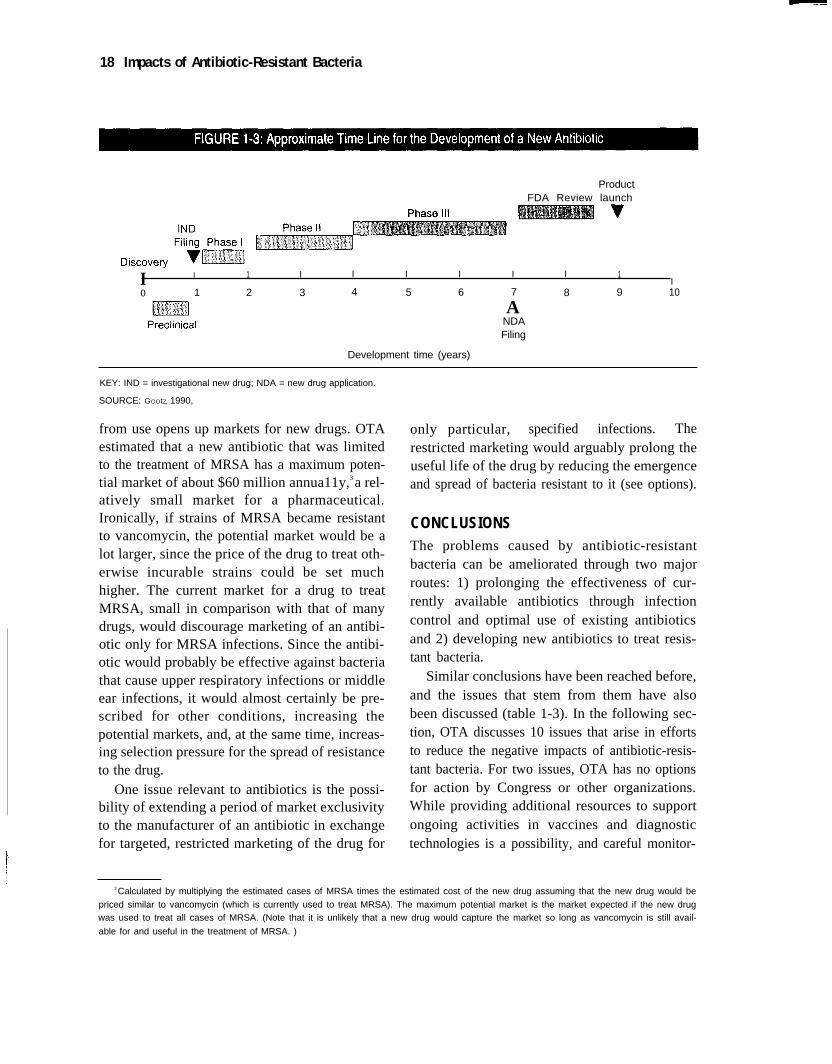
The isolation or synthesis of a chemical withantibiotic activity starts a long process of evalua-tion in the microbiology lab, laboratory animals,and ultimately, in humans. At the end of thosetests, FDA reviews the results and considersapproving it as a new drug (see figure 1-3). Theentire process between discovery and finalapproval takes years; frequently a potential drugfails a critical test—for instance, it is found tohave toxic side effects—and is discarded. Therisks of toxicity may be re-evaluated against thebenefits of an antibiotic, however, if the antibi-otic proves useful against a disease with few orno other treatments.
Pharmaceutical firms are largely responsiblefor antibiotic research and development, but thefederal government supports a small researchprogram aimed at antibiotic-resistant bacteria atthe National Institute of Allergy and InfectiousDiseases. In 1994, the institute spent about$13 million on that program, and about the sameamount in 1995.
Antibiotic Resistance and MarketsAntibiotic resistance both limits and creates newmarkets. Although drugs may lose their efficacyand market life because of resistance, their slide
Chapter 1 Summary, Conclusions, Issues and Options | 15
TABL
E 1-
2: A
ntib
iotic
s in
Use
and
Und
er D
evel
opm
ent
Actio
nFa
mily
/Cla
ssEx
ampl
e(s)
Sour
ceSt
atus
Ant
ibio
tics
that
in
hib
it ce
ll w
all
synt
hesi
s
Bet
a-la
ctam
s
Nat
ural
pen
icill
ins
Pen
icill
in G
Peni
cilli
n no
tatu
mU
sed
sin
ce 1
940s
Sem
i-syn
thet
ic
pen
icill
ins
Met
hici
llin
Pip
erac
illin
Sem
i-syn
thet
ic p
enic
illin
d
eriv
ativ
esIn
use
sin
ce 1
960s
; am
ong
the
mos
t w
idel
y p
resc
ribed
ant
imic
rob
ials
Cep
halo
spor
ins
Cep
hale
xin
C. a
crem
oniu
mW
idel
y us
ed c
lass
of a
ntib
iotic
s
Car
bap
enem
sIm
ipen
emD
eriv
ed fr
om th
iena
myc
in, a
co
mp
ound
pro
duc
ed b
y S
trep
tom
yces
cat
tleya
In u
se; w
ide
spec
trum
(ac
tive
agai
nst
man
y sp
ecie
s of
bac
teria
incl
udin
g
cep
halo
spor
in-r
esis
tant
E
nter
obac
teria
ceae
)
Mon
obac
tam
sA
ztre
onam
Der
ived
from
a c
omp
ound
p
rod
uced
by
Chr
omob
acte
rium
vi
olac
eum
In u
se; t
oler
ated
by
pat
ient
s w
ith
pen
icill
in a
llerg
ies;
sp
ectr
um li
mite
d to
ae
rob
ic g
ram
-neg
ativ
e b
acte
ria
Pen
icill
inas
e in
hib
itors
Cla
vula
nate
pot
assi
um
(use
d c
linic
ally
with
am
oxic
illin
or
ticar
cilli
n)S
ubtr
actio
n (u
sed
with
am
pic
illin
)Ta
zob
acta
m s
odiu
m
(use
d c
linic
ally
with
p
iper
acill
lin)
Str
epto
myc
es c
lavu
liger
ius
Sem
i-syn
thet
ic p
enic
illin
d
eriv
ativ
eS
emi-s
ynth
etic
pen
icill
in
der
ivat
ive
Use
d s
ince
197
0s; c
lavu
lana
te
com
bin
atio
ns u
sed
for
wid
e ra
nge
of
dis
ord
ers
Sim
ilar
to a
mox
icill
in/c
lavu
lana
te
Tazo
bac
tam
/pip
erac
illin
effe
ctiv
e ag
ains
t int
ra-a
bd
omin
al in
fect
ions
Van
com
ycin
Teic
opla
nin
Van
com
ycin
Teic
opla
nin
Str
ep. o
rient
alis
Act
inop
lane
s te
icho
myc
etic
us
Intr
oduc
ed in
195
6; u
sed
ag
ains
t st
aphy
loco
ccal
and
ent
eroc
occa
l in
fect
ions
Exp
erim
enta
l in
the
U.S
., av
aila
ble
for
com
pas
sion
ate
use
V
anco
myc
in d
eriv
ativ
esw
ith c
atal
ytic
act
ivity
Sem
i-syn
thet
icE
xper
imen
tal
(con
tinue
d)
16 | Impacts of Antibiotic-Resistant Bacteria
TABL
E 1-
2: A
ntib
iotic
s in
Use
and
Und
er D
evel
opm
ent (
Con
t’d.)
Actio
nFa
mily
/Cla
ssEx
ampl
e(s)
Sour
ceSt
atus
Ant
ibio
tics
that
in
crea
se
mem
bra
ne
per
mea
bili
ty
Pep
tides
Bac
teric
idal
/Per
mea
bili
tyIn
crea
sing
Pro
tein
(B
PI)
Mam
mal
ian
cells
Exp
erim
enta
l
M
agai
nins
Afr
ican
cla
wed
frog
Exp
erim
enta
l
C
ecro
pin
sS
ilk m
oth,
oth
er in
sect
s,
mam
mal
sE
xper
imen
tal
D
efen
cins
Mam
mal
ian
cells
Exp
erim
enta
l
Ste
roid
sD
ogfis
h sh
arks
Exp
erim
enta
l
Met
abol
ic
inte
rfer
ence
Sul
fona
mid
es
Trim
etho
prim
Sul
fam
etho
xazo
le
Trim
etho
prim
Azo
dye
s
Syn
thet
ic
In u
se s
ince
193
0s; f
irst a
ntim
icro
bia
l ag
ent u
sed
in m
anS
ynth
esiz
ed in
196
8, c
omm
only
use
d
tog
ethe
r w
ith s
ulfa
nim
ides
Pro
tein
syn
thes
is
inhi
bito
rsA
min
ogly
cosi
des
Str
epto
myc
inK
anam
ycin
Tob
ram
ycin
Gen
tam
icin
Str
epto
myc
es g
riseu
sS
trep
tom
yces
kan
amyc
etic
usS
trep
tom
yces
tene
bra
rius
Mic
rom
onsp
ora
pur
pur
ea a
nd
echi
nosp
ora
In u
se s
ince
194
0s; i
mp
orta
nt c
lass
of
antib
iotic
s
Fusi
dan
esFu
cid
inS
odiu
m s
alt o
f fus
idic
aci
d,
der
ived
from
the
fung
us
Fusi
diu
m c
occi
neum
In c
linic
al u
se s
ince
196
2, b
ut n
ot
avai
lab
le in
US
(ex
cep
t thr
oug
h co
mp
assi
onat
e re
leas
e); a
ctiv
e ag
ains
t so
me
stra
ins
of m
ethi
cilli
n-re
sist
ant
Sta
ph.
aur
eus
(MR
SA
)
Tetr
acyc
lines
Chl
orte
trac
yclin
eO
xyte
trac
yclin
eM
inoc
yclin
eD
oxyc
yclin
e
Str
epto
myc
es a
urof
acie
ns
Str
epto
myc
es r
imos
usS
emi-s
ynth
etic
der
ivat
ive
Sem
i-syn
thet
ic d
eriv
ativ
e
Firs
t int
rod
uced
in 1
948,
foun
d b
y sc
reen
ing
soi
l sam
ple
s fo
r ant
ibac
teria
l ac
tivity
(con
tinue
d)
Chapter 1 Summary, Conclusions, Issues and Options | 17
TABL
E 1-
2: A
ntib
iotic
s in
Use
and
Und
er D
evel
opm
ent (
Con
t’d.)
Actio
nFa
mily
/Cla
ssEx
ampl
e(s)
Sour
ceSt
atus
Chl
oram
phe
nico
lC
hlor
amp
heni
col
Str
epto
myc
es v
enez
uela
eFi
rst i
ntro
duc
ed in
194
9, c
urre
ntly
se
cond
line
ant
ibio
tic b
ecau
se o
f sid
e ef
fect
of a
pla
stic
ane
mia
Mac
rolid
es A
zalid
esE
ryth
rom
ycin
Azi
thro
myc
in
Str
epto
myc
es e
ryth
reus
sem
i-syn
thet
ic d
eriv
ativ
e of
er
ythr
omyc
in
Dis
cove
red
in 1
952
Ava
ilab
le in
199
2
Lin
cosa
mid
esC
lind
amyc
inS
emi-s
ynth
etic
der
ivat
ive
of
linco
myc
in d
eriv
ed fr
om
Str
epto
myc
es li
ncol
nens
is
Ava
ilab
le s
ince
the
mid
196
0s; a
ctiv
e ag
ains
t aer
obic
bac
teria
Mup
iroci
nM
upiro
cin
Pse
udom
onas
fluo
resc
ens
Intr
oduc
ed in
the
mid
198
0s; t
opic
al
antib
iotic
Inte
rfer
ence
with
R
NA
syn
thes
isR
ifam
ycin
sR
ifam
pin
Str
epto
myc
es m
edite
rran
eiFi
rst i
sola
ted
in 1
957,
imp
orta
nt
tub
ercu
losi
s d
rug
Toxi
c ef
fect
th
roug
h D
NA
b
ind
ing
Nitr
oim
idaz
oles
Met
roni
daz
ole
Syn
thet
icIn
trod
uced
in 1
959,
act
ive
agai
nst
anae
rob
es s
uch
as B
. fra
gili
s
Blo
ck D
NA
re
plic
atio
n or
RN
A
tran
scrip
tion
Ant
isen
se n
ucle
otid
esLa
bor
ator
yE
xper
imen
tal
DN
A r
eplic
atio
nQ
uino
lone
sFl
uoro
qui
nolo
nes
Nal
idix
ic a
cid
Cip
roflo
xaci
n, O
floxa
cin
Sem
i-syn
thet
icFi
rst i
den
tifie
d in
196
2U
sag
e b
egan
in 1
980s
; som
e of
the
mos
t wid
ely
used
ant
ibio
tics
Ant
i-tub
ercu
losi
s d
rug
sIs
onia
zid
(IN
H)
Pyr
azin
amid
e (P
ZA
)
Eth
amb
utan
ol
Syn
thet
icS
ynth
etic
Syn
thet
ic
Sho
wn
to b
e ef
fect
ive
in 1
952
Imp
orta
nt tu
ber
culo
sis
dru
g s
ince
198
0
Imp
orta
nt tu
ber
culo
sis
dru
g s
ince
197
4
Dec
oy r
ecep
tors
Car
boh
ydra
tes
Lab
orat
ory
Exp
erim
enta
l
SO
UR
CE
: Offi
ce o
f Tec
hnol
ogy
Ass
essm
ent,
1995
.
18 Impacts of Antibiotic-Resistant Bacteria
ProductFDA Review launch
I I 1 I I I I I I 1I
o 1 2 3 4 5 6 7 8 9 10
Development time (years)
ANDAFiling
KEY: IND = investigational new drug; NDA = new drug application.
SOURCE: GOOtZ, 1990,
from use opens up markets for new drugs. OTAestimated that a new antibiotic that was limitedto the treatment of MRSA has a maximum poten-tial market of about $60 million annua11y,3 a rel-atively small market for a pharmaceutical.Ironically, if strains of MRSA became resistantto vancomycin, the potential market would be alot larger, since the price of the drug to treat oth-erwise incurable strains could be set muchhigher. The current market for a drug to treatMRSA, small in comparison with that of manydrugs, would discourage marketing of an antibi-otic only for MRSA infections. Since the antibi-otic would probably be effective against bacteriathat cause upper respiratory infections or middleear infections, it would almost certainly be pre-scribed for other conditions, increasing thepotential markets, and, at the same time, increas-ing selection pressure for the spread of resistanceto the drug.
One issue relevant to antibiotics is the possi-bility of extending a period of market exclusivityto the manufacturer of an antibiotic in exchangefor targeted, restricted marketing of the drug for
only particular, specified infections. Therestricted marketing would arguably prolong theuseful life of the drug by reducing the emergenceand spread of bacteria resistant to it (see options).
CONCLUSIONSThe problems caused by antibiotic-resistantbacteria can be ameliorated through two majorroutes: 1) prolonging the effectiveness of cur-rently available antibiotics through infectioncontrol and optimal use of existing antibioticsand 2) developing new antibiotics to treat resis-tant bacteria.
Similar conclusions have been reached before,and the issues that stem from them have alsobeen discussed (table 1-3). In the following sec-tion, OTA discusses 10 issues that arise in effortsto reduce the negative impacts of antibiotic-resis-tant bacteria. For two issues, OTA has no optionsfor action by Congress or other organizations.While providing additional resources to supportongoing activities in vaccines and diagnostictechnologies is a possibility, and careful monitor-
3 Calculated by multiplying the estimated cases of MRSA times the estimated cost of the new drug assuming that the new drug would be
priced similar to vancomycin (which is currently used to treat MRSA). The maximum potential market is the market expected if the new drugwas used to treat all cases of MRSA. (Note that it is unlikely that a new drug would capture the market so long as vancomycin is still avail-
able for and useful in the treatment of MRSA. )
I

Chapter 1 Summary, Conclusions, Issues and Options | 19
ing and oversight of federal programs and theirprogress are important, no options for such incre-mental changes are presented. For the remainingissues, OTA proposes one or more options. Someof these options would involve greater researchsupport by the federal government, and OTAunderlines the reasons for such support and, insome cases, why it is expected to bring savingsin costs. Box 1-3 contains an outline of the issuesand options. All of these efforts will have to besustained, as the quote in box 1-4 underlines.
ISSUES AND OPTIONS FOR PROLONGING EFFECTIVENESS OF ANTIBIOTICS
❚ Issue A: SurveillanceIf officials decide to design a nationwide surveil-lance system, they must resolve many issuesbefore its implementation. Often, Congress or anexecutive branch agency turns to a commissionor panel to make recommendations, and any suchgroup could be instructed to consider the follow-ing questions in the design of a national surveil-lance system.
TABLE 1-3: Publications/Articles on Antibiotic-Resistant BacteriaThe problem of antibiotic-resistant bacteria has existed for years, and many articles and publications have discussed issues surrounding the dilemma. The following is a sample listing of some of them. A full bibliography follows.
Year Author Issue
1959 Finland, et al. Antibiotic use and resistance
1973 Kunin, et al. Problem and solution of antibiotic usage
1979 Buckwold, et al. Antimicrobial misuse
1985 Burke and Levy Worldwide antibiotic resistance
1992 Cohen Epidemiology of drug resistance
1992 Institute of Medicine Emerging infections
1992 Levy The antibiotic paradox
1992 Neu The crisis in antibiotic resistance
1994 Murray Can antibiotic resistance be controlled?
1994 Tomasz Multiple-antibiotic-resistant pathogenic bacteria
1995 CISET Emerging and re-emerging infectious diseases
SOURCES:Finland, M., et al., “Occurrence of Serious Bacterial Infections Since Introduction of Antibacterial Agents,” Journal of the American Medical Asso-ciation, 170:2188–2197, 1959.Kunin, C.M., Tupasi, T., and Craig, W.A., “Use of Antibiotics: A Brief Exposition of the Problem and Some Tentative Solutions,” Annals of InternalMedicine 79:555–560, 1973.Buckwold, F.J. and Ronald, A.R., “Antimicrobial Misuse—Effects and Suggestions for Control,” Journal of Antimicrobial Chemotherapy 5:129–135, 1979.Burke, J.P. and Levy, S.B., “Summary Report on Worldwide Antibiotic Resistance: International Task Forces on Antibiotic Use,” Reviews of Infec-tious Diseases 7:560–564, 1985.Cohen, M.L., “Epidemiology of Drug Resistance: Implications for a Post-Antimicrobial Era,” Science 257:1050–1055, 1992.Institute of Medicine, Emerging Infections: Microbial Threats to Health in the United States, J. Lederberg, R.E. Shope, S.C.J. Oaks (Eds.), 1992.Levy, S.B., “The Antibiotic Paradox: How Miracle Drugs Are Destroying the Miracle,” 1992.Neu, H.C., “The Crisis in Antibiotic Resistance,” Science 257:1064–1073, 1992.Murray, B.E., “Can Antibiotic Resistance Be Controlled?” New England Journal of Medicine 330:1229–1230, 1994.Tomasz, A., “Multiple-Antibiotic-Resistant Pathogenic Bacteria—A Report on the Rockefeller University Workshop,” New England Journal of Med-icine 330:1247–1251, 1994.Executive Office of the President, National Science and Technology Council, Committee on International Science, Engineering, and TechnologyWorking Group, Emerging and re-emerging infectious diseases: global microbial threats in the 1990s. (Washington, DC: 1995).
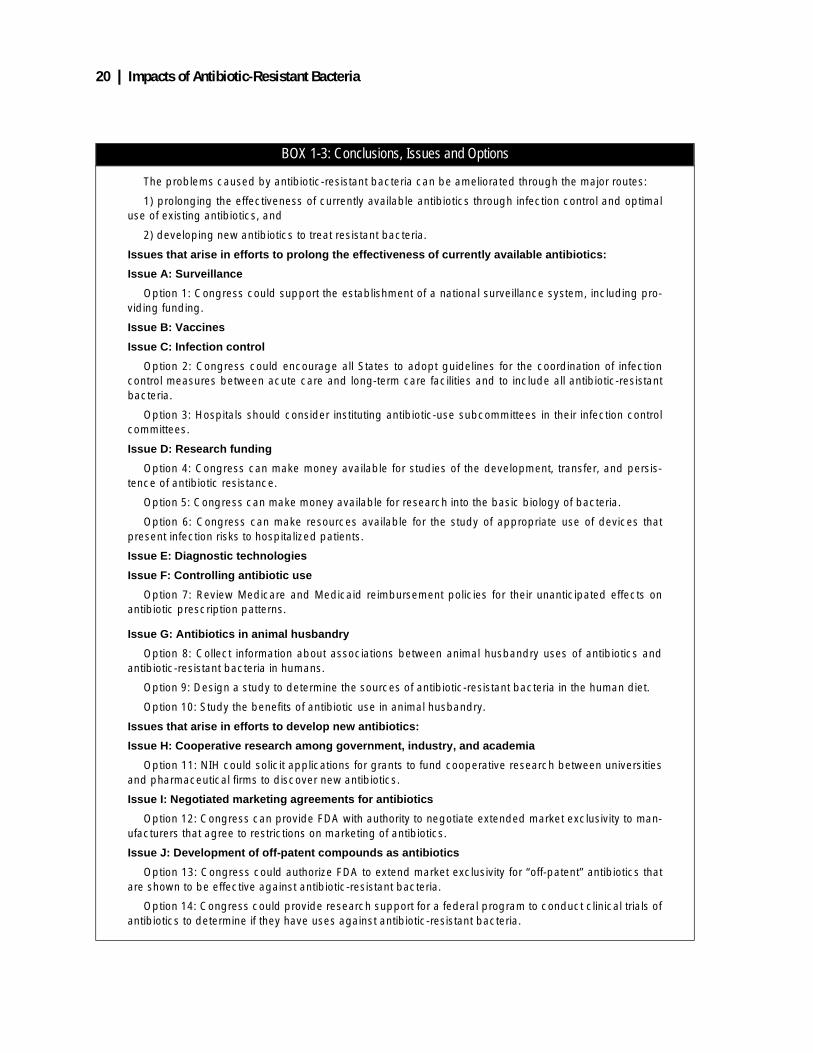
20 | Impacts of Antibiotic-Resistant Bacteria
BOX 1-3: Conclusions, Issues and Options
The problems caused by antibiotic-resistant bacteria can be ameliorated through the major routes:
1) prolonging the effectiveness of currently available antibiotics through infection control and optimaluse of existing antibiotics, and
2) developing new antibiotics to treat resistant bacteria.
Issues that arise in efforts to prolong the effectiveness of currently available antibiotics:
Issue A: Surveillance
Option 1: Congress could support the establishment of a national surveillance system, including pro-viding funding.
Issue B: Vaccines
Issue C: Infection control
Option 2: Congress could encourage all States to adopt guidelines for the coordination of infectioncontrol measures between acute care and long-term care facilities and to include all antibiotic-resistantbacteria.
Option 3: Hospitals should consider instituting antibiotic-use subcommittees in their infection controlcommittees.
Issue D: Research funding
Option 4: Congress can make money available for studies of the development, transfer, and persis-tence of antibiotic resistance.
Option 5: Congress can make money available for research into the basic biology of bacteria.
Option 6: Congress can make resources available for the study of appropriate use of devices thatpresent infection risks to hospitalized patients.
Issue E: Diagnostic technologies
Issue F: Controlling antibiotic use
Option 7: Review Medicare and Medicaid reimbursement policies for their unanticipated effects onantibiotic prescription patterns.
Issue G: Antibiotics in animal husbandry
Option 8: Collect information about associations between animal husbandry uses of antibiotics andantibiotic-resistant bacteria in humans.
Option 9: Design a study to determine the sources of antibiotic-resistant bacteria in the human diet.
Option 10: Study the benefits of antibiotic use in animal husbandry.
Issues that arise in efforts to develop new antibiotics:
Issue H: Cooperative research among government, industry, and academia
Option 11: NIH could solicit applications for grants to fund cooperative research between universitiesand pharmaceutical firms to discover new antibiotics.
Issue I: Negotiated marketing agreements for antibiotics
Option 12: Congress can provide FDA with authority to negotiate extended market exclusivity to man-ufacturers that agree to restrictions on marketing of antibiotics.
Issue J: Development of off-patent compounds as antibiotics
Option 13: Congress could authorize FDA to extend market exclusivity for “off-patent” antibiotics thatare shown to be effective against antibiotic-resistant bacteria.
Option 14: Congress could provide research support for a federal program to conduct clinical trials ofantibiotics to determine if they have uses against antibiotic-resistant bacteria.

Chapter 1 Summary, Conclusions, Issues and Options | 21
■ Which antibiotics and organisms will beincluded in the system? There are more than100 different antibiotics and many possibleorganisms, and it will be impossible to main-tain surveillance of all “drug-bug” combina-tions. Some regional adjustments might beconsidered because of geographical variationsin antibiotic usage.
■ How many hospitals and laboratories willparticipate in the system? Will all participate,or will a representative sample of hospitalsand laboratories comprise the network?
■ What kinds of laboratory-determined data willbe incorporated into the system? This will be amajor issue in any surveillance system forantibiotic-resistant bacteria because of thevariety of techniques already available and themajor changes in diagnostic technologies thatare now underway.
■ How will the system assure the quality of testresults? Would the surveillance system collectraw data as WHONET does? Or insist on useof standard guidelines to interpret the data?Who would develop the guidelines? Howwould results from genotypic tests, whichdirectly measure the presence of a gene forresistance, be compared to phenotypic tests,which measure the ability of the bacteria tosurvive in the presence of an antibiotic?
■ Who will have access to the system? Willaccess be restricted to the medical community,or would others, such as pharmaceutical com-
panies and private computer owners, be able togain entry to the system?
■ Would banking of samples be part of the sys-tem? Some small, currently operating systemscollect and bank some bacterial samples toallow rechecking of identification. Wouldpharmaceutical companies be provided accessto banked samples to test new antibiotics?
■ Will hospitals link pharmacy records, patientdata, and laboratory information? This link-age would be ideal, because it would allowresearchers to correlate data about the effect ofantibiotic usage and resistance directly and tocorrelate clinical outcomes with test data.
■ Should the system be extended internation-ally? Antibiotic-resistant bacteria travel fromcountry to country, posing an internationalproblem. Therefore, it may be in the best inter-est of the U.S. to include other countries in asurveillance system. How would this be done?
■ What role would surveillance system person-nel take in training of hospital personnel touse the results of the surveillance system? Thesuccess of the system will depend on the usethat is made of its results, and system person-nel may have to devote some time to makesure the results are well used.
The cost of the system will have to be consid-ered. The more complex the system, the more itwill cost. However, some successful surveillancesystems, such as WHONET and the New JerseyState System, have been built on very small bud-
BOX 1-4: The Myth of Sisyphus and Antibiotics
“The search for and development of new drugs by the pharmaceutical industry will go a long waytoward conquering the growing microbial resistances to available antibiotics. But there is much more tobe done than merely generating new antibiotics—the pace of which cannot keep up with the microbialresistance responses....
“The history of antibiotics reminded our student Raul Borbolla of the Greek myth of Sisyphus, the kingof Corinth who, as punishment for his hubris, was condemned by the gods to push a boulder up a moun-tain, only to have the boulder roll to the bottom, from which Sisyphus had to start pushing again. Againthe boulder would roll to the bottom, and the cycle was repeated into perpetuity. The rational and con-trolled use of antibiotics may prevent medicine from facing Sisyphus's fate.”
SOURCE: C.F. Amabile-Cuevas, M. Cardenas-Garcia and M. Ludgar (1995), American Scientist 83:320–329.

22 | Impacts of Antibiotic-Resistant Bacteria
gets. The CDC estimates that bringing theirDRSP system to each state would require start-up costs of about $200,000 for each state, for atotal of $10 million and annual operating costsbetween $2.5 and $5 million. If a surveillancesystem prevents even 1 percent of infectionscaused by antibiotic-resistant bacteria (whichOTA estimates cost a minimum of $1.3 billionper year in 1992 dollars), the system would payfor itself.
An alternative to surveillance systems is aprogram to investigate outbreaks of infectiousdiseases as they are reported. A difficulty withthe alternative is that in the absence of a surveil-lance system, not all cases will be reported tohealth officials. According to CDC, 27 illnessescaused by E. coli O157:H7 were confirmed inNew Jersey in June 1994, compared to five casesin the same period in 1993. This “pseudo-out-break,” as CDC called it, resulted from betterreporting as a result of institution of a surveil-lance system that required laboratory testing ofsome clinical laboratory samples for the E. coli.It illustrates that many opportunities to interveneand disrupt transmission of infectious diseasescan be missed without a surveillance system.
Congress could support the establish-ment of a national surveillance system, including pro-viding funding.
A surveillance system is essential for under-standing the spread of antibiotic-resistant bacte-ria and planning interventions so as to preservethe efficacy of currently available antibiotics.Because of these public health considerations,and the likelihood that a surveillance systemwould decrease medical costs, including costs toMedicare, Congress could consider funding anationwide surveillance system.
The features of current, limited systems can beincorporated and combined to produce a systemof desired size, complexity, and cost. It may beadvantageous to begin with a less complex sys-tem (such as some of the operating systemsdescribed in this report), and then add more fea-tures. Any system must have a strong advisory
group that includes diagnostic laboratory andcomputer experts, clinicians, hospital administra-tors, pharmaceutical company researchers, aca-demic scientists, and federal and state regulatoryand health officials. The advisors could work toassure that the surveillance system collects anddisseminates the information in the forms for itsbest use.
❚ Issue B: VaccinesThe biotechnology revolution is expected to pro-duce many new potential vaccines. This wouldbe a welcome change from the slow rates of dis-covery and development of recent years, and itwill benefit from and may, indeed, require newmechanisms for vaccine testing, development,and approval. If this effort is successful, effectivevaccines would reduce the need for some antibi-otics and would, therefore, help control antibioticresistance.
The private sector conducts much of the cur-rent vaccine research, but current federal policiesrestrict the income from vaccines sales, and thatmay inhibit research activities. To provide low-income Americans with vaccines, the federalgovernment now purchases up to 80 percent ofall vaccines at a fixed, low price. GAO, however,reports that the price of vaccines for children haslittle effect on vaccination rates, largely becausepoor children are entitled to free vaccine. AsCongress considers the Vaccines for Childrenprogram, it can be expected that vaccine manu-facturers will argue that the price cap andreduced profits have created an adverse effect onnew vaccine development. Determining theimpact of the price cap on research could be anobjective of the congressional inquiries.
GAO describes efforts that have fallen short inreaching various federal goals for immunizationrates. Although Medicare pays for the adminis-tration of pneumococcal vaccine to the elderly,73 percent of them have never received it. Thatand other observations made by GAO indicatethat there is much to be done to increase vaccina-tion rates, and the reports make somesuggestions.
OPTION

Chapter 1 Summary, Conclusions, Issues and Options | 23
Encouragement of adult vaccination deservesspecial consideration in light of changes aroundthe world. Currently, diphtheria is epidemic inEastern Europe, and as many as 50 percent ofUnited States adults over 30 are susceptible tothat disease because they have not had immuni-zation booster shots. Since 1988, the few con-firmed cases of diphtheria in the United Stateshave been related to importation of disease fromother countries, illuminating the internationalnature of the spread of infectious diseases, whichcan include those caused by antibiotic-resistantbacteria.
❚ Issue C: Infection ControlSeveral new medical techniques and devices aredesigned to reduce infections, and private organi-zations, such as insurance companies and hospi-tals, have a financial incentive to instituteeffective infection control procedures that cansave money, reduce hospitalization rates, andhelp control antibiotic-resistant bacteria. Thegovernment, acting as an insurer through Medi-care and Medicaid, may also have an interest infunding research to develop new techniques andmethods and to apply them.
Some devices and techniques that reduceinfection rates are available, and their adoptionhas been demonstrated to reduce in-hospital timeand costs. Most importantly, the patients bene-fited from fewer hospitalizations. Nevertheless,adoption of such improvements may hinge onevents as distant as Medicare reimbursementprocedures. Medicare reimburses dialysis centersand hospitals separately, and there is no financialincentive for dialysis centers to invest in thesenew technologies.
The Joint Commission for the Accreditationof Health Care Organizations (JCAHO) is begin-ning to collect data on infection control fromhospitals on a voluntary basis, with about 400hospitals now participating. Analysis of thesedata may be a very useful tool in understandingthe differences between successful and not-so-successful infection control in hospitals. Thisprogram provides limited information; it is not
mandatory and it collects no data on antibioticresistance. Nevertheless, it provides informationfor research efforts, and it can be expanded.
With recent changes in the health care system,hospitals discharge many patients more quicklythan in the past, and many patients are moved tolong-term care facilities. Some of these patients,when discharged to the long-term facilities, haveactive infections or are at high risk for infectionbecause of indwelling invasive devices such ascatheters or intravenous lines or because they areon dialysis. Further, the large concentrations ofantibiotics used in these facilities (like the largeconcentrations used in hospitals) selects for theemergence and spread of antibiotic-resistant bac-teria, as is demonstrated by the high prevalenceof MRSA in nursing homes. Patients infectedwith antibiotic-resistant bacteria in nursinghomes frequently return to the hospital, wherethe antibiotic-resistant bacteria can spreadfurther.
Congress could encourage all states toadopt guidelines for the coordination of infection con-trol measures between acute care and long-term carefacilities and to extend guidelines to include all antibi-otic-resistant bacteria.
Many state health departments have recog-nized the problems of transfer of MRSA betweenhospitals and long-term care facilities and havepublished extensive guidelines for coordinationof the admission, discharge and transfer ofMRSA-colonized patients between two facilities.Wider adoption of these procedures shouldreduce the transmission of infections caused byantibiotic-resistant bacteria (and other bacteria)while simultaneously lowering costs and opti-mizing patient care.
Hospitals should consider institutingantibiotic-use subcommittees in the infection controlcommittees.
Every hospital has an infection control com-mittee. Assigning a subcommittee responsibilityfor monitoring antibiotic use and relating that useto the spread of antibiotic-resistant bacteria
OPTION
OPTION
24 | Impacts of Antibiotic-Resistant Bacteria
would focus attention on these problems andbring them to the attention of hospital staff.
❚ Issue D: Research FundingThe current federal belt-tightening era has pro-duced a reluctance to commit new sums ofmoney to research, which may make it necessaryto transfer money from other research areas tosupport research related to antibiotic-resistantbacteria. Such decisions are difficult, but withoutadditional research support, the country may fallfurther behind in trying to counter antibiotic-resistant bacteria. One consequence of increasedsupport of such research will be the training ofscientists and physicians in skills necessary toteach others the newest methods in research andin the application of research findings.
Congress can make money available forstudies of the development, transfer, and persistenceof antibiotic resistance.
Scientists understand the basic principles ofthe emergence and spread of antibiotic resistanceand of the genetic transfer of resistance betweenbacteria, but they do not have enough details topredict how the patterns of use of antibiotics willaffect the prevalence of resistance genes. Forexample, restricting the use of an antibiotic oftenleads to a decrease in the prevalence of antibioticresistance. That would appear to pave the wayfor reintroducing the antibiotic, but it is uncertainwhat will happen when the antibiotic is reintro-duced because the time course for the reappear-ance of resistance is unknown.
Congress can make money available forresearch into the basic biology of bacteria.
The molecular organization and function andthe biochemistry of bacteria differ from those ofanimal and human cells, and pharmaceuticalcompanies have exploited those differences indeveloping antibiotics. Basic research directed atbetter understanding of bacterial biochemistrymay reveal new targets for antibiotics; in anycase, it will produce information that will be use-
ful in understanding bacterial growth and patho-genesis.
The amounts of federal money spent on non-AIDS research have not increased in parallelwith the increasing inroads being made by antibi-otic-resistant bacteria. For instance, the federalgovernment gave CDC a $6.7 million increase inits non-AIDS budget specifically to combatemerging infectious diseases. However, onlyabout 10 to 15 percent of that money will be usedfor antibiotic resistance, and it is unclear howmuch of that amount will be used for research.Relatively small increases, a few million dollarsin the total federal budget directed at antibiotic-resistant bacteria, could produce a markedincrease in the amount of research being done.
Congress can make resources avail-able for the study of appropriate use of devices thatpresent infection risks to hospitalized patients.
Many nosocomial infections result from theuse of invasive devices such as catheters andmechanical ventilators, often routinely used inintensive care units. There is little research aboutwhen such devices improve outcomes. Suchresearch will probably not be funded by manu-facturers that benefit from the sales of equip-ment. Learning about the risks and benefits ofthese devices may depend on government fund-ing. This information would guide decisionsabout when to use these devices, probably reduc-ing their use (and associated costs) and reducinginfection rates.
❚ Issue E: Diagnostic TechnologiesThe most powerful weapon in the arsenaldirected at antibiotic-resistant bacteria are tech-niques for the rapid and accurate identification ofbacteria and determination of their susceptibilityto antibiotics. New techniques are necessary.When available, they will provide the most cer-tain information for appropriate antibiotic use.
The lack of rapid in-office methods to screenfor and to identify bacteria and to characterizetheir antibiotic-resistance patterns probably rein-forces physicians’ tendency to prescribe broad-
OPTION
OPTION
OPTION

Chapter 1 Summary, Conclusions, Issues and Options | 25
spectrum antibiotics for presumed bacterialinfections. As quicker tests become available,some of which are likely to be quite simple toperform and present few problems in interpreta-tion, more conflicts are expected between theprovisions of the Clinical Laboratory Improve-ment Act (CLIA) and physicians’ desires to usethe new tests. CLIA requires that physicians reg-ister their offices and fulfill (largely record-keep-ing) requirements in order to carry out laboratorytests. One solution to the conflict is to excusephysicians’ offices from CLIA, and legislationhas been introduced to exempt clinical laborato-ries in physicians’ offices from having to complywith CLIA regulations.
Another way to improve the use of diagnostictests in physician offices would be encourage-ment of manufacturers to develop test kits tomeet the performance specifications for productsin the “waived” category of tests under CLIA.This would preserve the positive effects ofCLIA. For example, CLIA has had a positiveeffect on the way tests are manufactured: manycurrently waived tests contain built-in controls tocomply with CLIA. These controls make it easierfor the person performing the test to determinewhether it has been performed correctly. CDC,which determines the categorization of testsunder CLIA, has already taken steps in this direc-tion by sending a letter to manufacturers toinform them of the possibility of including theirtests in the waived category and outlining therequirements for tests in this category. Groupssuch as the American Medical Association coulddetermine which tests are most useful for physi-cian offices and work together with the manufac-turers and CLIA administrators to provide testssuitable for the waived category.
With no action taken at all, potential conflictsbetween physicians’ desires to carry out in-officetests and CLIA will diminish. Over the next fewyears, group practices that develop sufficient testvolumes to require comprehensive laboratorieswill seek CLIA approval as a matter of course.Smaller offices, however, will persist in ruralareas, and CLIA may be more of an issue inthose locations.
The term “service labs” is generally used torefer to laboratories in hospitals or to commerciallaboratories that identify and characterize bacte-ria and other infectious organisms. In a draftreport about a new surveillance system for anti-biotic-resistant S. pneumoniae (see option 1),CDC states that laboratories may not be using themost up-to-date standards. CDC suggests that theNational Committee for Clinical LaboratoryStandards (NCCLS) guidelines could be pub-lished in the Morbidity and Mortality WeeklyReport (MMWR) and as letters to clinical labora-tory journals to inform both physicians and labo-ratories about appropriate standards. This seemsa reasonable step. Since CDC publishes MMWR,it should be able to disseminate the guidelinesthrough that publication.
New diagnostic technologies, such as thosebased on DNA identification, have advanced rap-idly, but regulatory procedures have not keptabreast of the new technologies. This slow pacehas resulted in conflicting signals about the useof the tests, which can be illustrated by the caseof tuberculosis diagnostic tests. The public healthbenefits of rapid and specific diagnostic testsinclude reducing the transmission of tuberculosisthrough optimal use of the few beds reserved fortuberculosis patients and the better treatment ofinfected individuals, reducing unnecessary use ofantibiotics and the resulting selection for resis-tant bacteria. Many hospitals in areas with hightuberculosis rates currently rely on DNA diag-nostic tests for these applications.
Despite the great advantage in speed and thecurrent use of such tests, CDC and the FDA haveadvised that physicians should use conventionalmethods until DNA techniques are betterdefined. Even so, conventional tests are not with-out problems. Culture tests for tuberculosis aredifficult to perform accurately and obtainingreproducible results is difficult. Also, differenttesting laboratories have produced conflictingresults in measuring susceptibility to the tubercu-losis drug pyrazinamide, demonstrating that con-ventional tests are not without problems.
Even in the absence of a CDC approval of thenew DNA-based tests, some private insurers will

26 | Impacts of Antibiotic-Resistant Bacteria
pay for them. However, tuberculosis is a diseasethat disproportionately affects poor people, andMedicare and Medicaid coverage of these proce-dures would improve those people’s access tothese methods. Such coverage would result inhealth benefits of prompt treatment and reducedtransmission of tuberculosis to health care work-ers and the community.
To date, the FDA has not approved a kit fortuberculosis testing. However, some service lab-oratories perform tests using devices of their ownmaking or devices that are licensed for researchbut not clinical applications. There are, however,no guidelines for proficiency testing of laborato-ries. The adoption of guidelines for ensuring pro-ficiency testing of laboratories performing newtests should be a priority of government organi-zations such as CDC. In this way, access to andquality of new diagnostic technologies can bemaximized.
Service labs are likely to face these difficultiesfor many tests. Some bacteria are so rare that notest kits will ever be made to identify them; themarket is too small. But microbiology servicelabs will devise their own tests, and those testswill raise many of the same issues as the issuesraised by new tuberculosis tests.
❚ Issue F: Controlling Antibiotic UseNumerous organizations, including state and fed-eral agencies, insurance companies, and healthprofessional associations, have developed prac-tice guidelines that address a range of clinicalconditions. Practice guidelines might influencethe use of antibiotics.
For example, a physician considering whetheror not to prescribe an antibiotic may decide to doso because of a possible malpractice action if heor she does not and the patient fails to improve.The physician might want to rely on a practiceguideline as an authority for the decision he orshe made, but it might not be sufficient defensein a malpractice suit. Currently, the use of prac-tice guidelines in medical malpractice litigationis a complicated and controversial issue. More-over, guidelines may actually have the effect of
encouraging the use of antibiotics because aguideline which admits any benefit of the use ofantibiotics for a specific illness may be used asevidence against a physician who chose not toprescribe antibiotics.
Hospitals use formularies to restrict the num-ber of antibiotics available and that can requireapproval by an infectious disease specialist foruse of some antibiotics. A 1994 review of theserestrictive measures documented reducedexpenses for antimicrobial acquisition andadministration, reduced adverse drug reactions ina limited number of cases, and improved appro-priateness of drug choice. It also found disadvan-tages, including difficulties of implementation inthe community hospital setting, inconveniencefor the prescribing physician, and increasedadministrative costs. Antibiotic control programswere associated with a decrease in antibioticresistance in a few hospitals, but disappointingly,the resistance increased “abruptly when controlor monitoring was relaxed or removed.” Thisphenomenon suggests that permanent control ormonitoring is necessary for prolonged decreasesin antibiotic resistance.
Change of at least one federal policy mightreduce the use of vancomycin, the antibiotic oflast resort in some infections.
Review Medicare and Medicaid reim-bursement policies for their unanticipated effects onantibiotic prescription patterns.
Medicare generally does not pay for intrave-nous medications in the home but does pay formedications that require the use of an infusionpump. This policy has caused some physicians toprescribe vancomycin, which requires the use ofan infusion pump and therefore is covered underthis policy, rather than other antibiotics that arenot covered. This policy runs counter to CDC’srecommended judicious use of vancomycin.Should Medicare change this policy, it may alsoinfluence private insurers to consider unantici-pated effects on antibiotic prescription patterns,and there may be other examples of policies hav-ing such undesirable effects on antibiotic use.
OPTION

Chapter 1 Summary, Conclusions, Issues and Options | 27
❚ Issue G: Antibiotics in Animal HusbandryThe overriding uncertainty about agriculturaluses of antibiotics is their contribution to antibi-otic-resistant bacteria and to complications in thetreatment of human diseases. Years of expertreview testify to the difficulty of coming to anygenerally accepted conclusions about theeffects of long-term, low-level feeding of anti-biotics to food animals and the appearance ofantibiotic-resistant bacteria in humans (seechapter 7), and it is unreasonable to expectthat another review of existing data wouldprovide resolution. The following three options,if adopted, would provide for the collection ofnew information. Importantly, however, carefulanalysis needs to precede any study because it isquite possible that no study can produce informa-tion sufficiently definitive to justify the expenseof the study, and that analysis would have toinvolve agricultural interests, pharmaceuticalcompanies, farmers, farmers organizations, pub-lic health officials, environmental organizations,organic food processors, and scientists from allthose organizations as well as universities andthe government. All have a stake in any studyabout antibiotic use in animal husbandry.
Collect information about associationsbetween animal husbandry uses of antibiotics andantibiotic-resistant bacteria in humans.
Any serious study of the risks from animalhusbandry uses of antibiotics will require theexpertise of epidemiologists, and many of thosescientists are at the CDC. Congress could pro-vide money to CDC to convene a group of scien-tists to examine the prospects of designing astudy about the transfer of antibiotic-resistantbacteria from animals to humans. The scientists,representing all the interests involved in thisissue, would be required to estimate the cost andtime necessary for the study and the size of theimpact that they can detect. For instance, wouldit be possible to design a study to answer thequestion: “Does agricultural use of antibiotics
contribute 2 (or 5, or 10) percent of the antibi-otic-resistant bacteria in humans?”
One possible outcome of the scientists’ delib-erations would be the conclusion that the studycould not provide any certain information. FDA,in making comments on an earlier draft of thisreport, said it is convinced that such a study can-not be done, and OTA’s 1993 assessmentResearching Health Risks discusses the difficul-ties of investigations of environmental healthrisks; some of those are applicable here. A deci-sion that the study would not answer the ques-tions could be accompanied with advice aboutwhat new techniques might alter the decision inthe future.
If this study were undertaken, a study of genetransfer from bacteria from food animals to bac-teria important to human health could be builtinto it.
Design a study to determine thesources of antibiotic-resistant bacteria in the humandiet.
A study to investigate the sources of antibi-otic-resistant bacteria need not be so demanding.It could be designed to collect a sample of mar-keted foods, isolate bacteria from the foods, andcharacterize their antibiotic resistance. The char-acterization could be done at the molecular levelto determine the source of the bacteria.
The successful completion of this study wouldbe informative about the levels and perhapssources of antibiotic-resistant bacteria in com-mon foods. That information might lead to inter-ventions in some food handling processes toreduce bacterial contamination, and it might leadto consumers’ being more careful in food prepa-ration. On the other hand, since it is well-knownthat food poisoning is a risk and people take pre-cautions against it, the information about transferof antibiotic-resistant bacteria might have no orfew effects on behavior.
OPTION
OPTION

28 | Impacts of Antibiotic-Resistant Bacteria
Study the benefits of antibiotic use inanimal husbandry.
Reviews of the information about healthimpacts of antibiotic use in animal husbandryoften point to possible risks. Statements aboutrisk are often countered by claims that the bene-fits of continued use of antibiotics for growthpromotion outweigh the risk, and farmers’ con-tinued use of subtherapeutic doses is offered asevidence for those benefits.
An analysis of written information couldprobably determine the costs of the antibiotics infeeds. It might also be possible to determine thebenefits of their use from the literature. Morelikely, however, some feeding experimentswould be necessary to make quantitative deter-mination of the benefits as measured byincreased yields. This information about benefitscould be considered in efforts to sort out thecosts and benefits of subtherapeutic doses ofantibiotics.
ISSUES AND OPTIONS FOR ENCOURAGING DEVELOPMENT OF NEW ANTIBIOTICSUntil recently, new antibiotics had been devel-oped at such a rate that no bacteria were resistantto all of them. Today, this is no longer true.
Manufacturers develop antibiotics in anticipa-tion of markets and profits. In the 1980s, themarket was saturated with more than 100 antibi-otics, which reduced the profit to be expectedfrom yet another entry in a crowded field.Although research and development expendi-tures in pharmaceutical companies greatlyincreased in the 1980s, the percentage ofresearch and development devoted to anti-infec-tives decreased. Because of the long times neces-sary for discovery, testing, and development ofnew drugs, the decisions in the 1980s account inpart for the shortage of new antibiotics in the1990s. Reports of pharmaceutical companies hir-ing new senior-level scientists for antibioticresearch and the interest of many biotechnology
companies in antibiotics indicate that they nowsee opportunities in antibiotic development (seebox 1-5), but consolidations and purchases ofpharmaceutical firms have also reduced the num-ber and size of research departments and thenumber of industry-employed scientists devotedto antibiotics.
Because of the importance of drugs to publichealth, Congress has provided assistance andincentives to pharmaceutical companies, includ-ing tax credits for research, increased patent lifeto compensate for the years of patent protectionlost to regulatory delays, a commitment to morerapid review of new drug applications at theFDA, and active technology transfer of drugsdeveloped in whole or in part by government sci-entists. These tax, patent and research and devel-opment policies are discussed in chapter 5 of thisreport, and in detail in the 1993 OTA reportPharmaceutical R&D: Costs, Risks andRewards. Here OTA considers four optionsdirected specially at antibiotics.
❚ Issue H: Cooperative Research Among Government, Industry, and AcademiaThe National Cancer Institute (NCI) has fundedthe National Cooperative Drug Discovery Pro-gram since 1983. The program solicits applica-tions from consortia of university researchersand pharmaceutical companies to search for newanti-cancer drugs. The awards are limited to thesupport of pre-clinical research. Generally, theprincipal investigator is from a university withco-principal investigators from industry. Whilethe research can take different directions, it gen-erally involves university researchers doing basicresearch, and industry scientists developingmethods for widespread application of theresearch methods. Through the end of 1994, NCIhad invested about $100 million in this program,and several compounds discovered in the pro-gram-sponsored research have entered clinicaltrials.
OPTION

Chapter 1 Summary, Conclusions, Issues and Options | 29
NIH could solicit applications for grantsto fund cooperative research between universitiesand pharmaceutical firms to discover new antibiotics.
The National Institute of Allergy and Infec-tious Diseases (NIAID) could develop a similarprogram for antibiotics. Such an effort wouldhave the advantages of forging relationshipsbetween university and industry researchers,increasing the speed of dispersion of “academic”ideas to industry, and producing a community ofuniversity-industry research groups that couldspeed up drug discovery. Moreover, such jointresearch activities would quickly deliver promis-ing substances to pharmaceutical company scien-tists who could evaluate them against criteria forpharmaceuticals: penetrability, toxicity, specific-ity, and bioavailability.
There are disadvantages as well. It is unlikelythat additional money will be provided to NIAIDin the near future, and in FY 93, NIAID spentabout $10 million on research directed at antibi-otic resistance, which is about the average annual
amount spent by NCI on its Cooperative DrugDiscovery Program. To set up an expensive anti-biotic discovery program would require divertingfunds from other research programs. This maynot be the optimal use of limited governmentfunding for research, especially in light of basicresearch needs for which industry support isunlikely (see Issue D).
❚ Issue I: Negotiated Marketing Agreements for AntibioticsA pharmaceutical company that discovers anddevelops an antibiotic that is effective againstparticularly troublesome antibiotic-resistant bac-teria as well as against many other bacteria mightbe willing to restrict its marketing to use againstthe antibiotic-resistant bacteria in exchange forlonger market exclusivity. The trade-off, simplyput, is that 10 years of a protected market mightgenerate as much profit as five years of higher,less-restricted sales that resulted in faster devel-opment of antibiotic resistance.
BOX 1-5: Industry-Funded Cooperative Research
“The Action TB Initiative is an international 5-year programme of collaborative research sponsored byGlaxo. The ultimate objective from Glaxo’s point of view is to discover ways to produce new anti-tubercu-losis medicines and vaccines....
“In the UK, an ambitious research programme is being pursued under the initiative at centers in Lon-don and Birmingham, and scientists at Glaxo are conducting their own research in collaboration. In SouthAfrica, the Medical Research Council is coordinating research programmes at various institutes through-out the country. At the London School of Hygiene and Tropical Medicine, a wide-ranging programme wasinitiated in July, 1993....
“Apart from the scientific progress achieved already, tangible benefits for the London School haveincluded laboratory renovations and the appointment of new staff. The three project supervisors in Lon-don each have their counterpart at Glaxo, and the scientist-to-scientist collaborations are deemed valu-able. At this juncture skeptics might reasonably ask ‘what’s in this for the company?’. Clearly short-termgoals have been eschewed, but as a public relations exercise the initiative is unquestionably a success.Moreover, Glaxo has by this means secured an impressive array of medical research expertise tosharpen its competitive edge. Although not all academic researchers would feel comfortable with suchan arrangement, as an example of an effective partnership between the pharmaceutical industry andacademic health sciences it has much to offer.”
SOURCE: Lancet (May 13, 1995)
OPTION

30 | Impacts of Antibiotic-Resistant Bacteria
Congress can provide FDA with author-ity to negotiate extended market exclusivity to manu-facturers that agree to restrictions on marketing ofantibiotics.
Usually, a drug enjoys an exclusive marketuntil its patent protection expires. The exclusiv-ity means that generic compounds that are identi-cal to it cannot be marketed. Congress hasgranted FDA the authority to extend the length ofexclusivity under certain conditions when a man-ufacturer shows that its product is safe and effec-tive against a new indication. Congress couldextend the same authority to FDA to negotiateagreements for extended exclusivity in exchangefor restricting marketing to uses against particu-lar antibiotic-resistant bacteria or against dis-eases likely to be complicated by antibiotic-resistant bacteria.
The advantage of such an action could belonger effective usefulness of the antibiotics.Moreover, FDA authority to negotiate sucharrangements would leave pharmaceutical com-panies free to consider different marketing strate-gies and to choose the most beneficial one interms of profits, public relations, or other factors.
Extended exclusivity would not precludeanother company’s efforts to develop antibioticsfor similar conditions. If the other company pro-duced a comparable or better drug, the companywith the extended exclusivity might see itspotential profits disappear.
Physicians commonly prescribe drugs “off-label” for indications other than those approvedby the FDA and that could weaken the restrictedmarketing program. On the other hand, exclusiv-ity extensions could include provisions to allowFDA to be certain that companies with suchagreements not sponsor research or research dis-semination activities that would promote suchoff-label uses.
An examination of how such a system mighthave affected the sales of, and the developmentof resistance to, antibiotics that are no longer ofclinical use because of resistance would informany congressional decision about this option.While pharmaceutical companies might be will-ing to fund the analysis, public funding might benecessary for a credible study and results.
❚ Issue J: Development of Off-Patent Compounds as AntibioticsMany chemical compounds were discovered andpatented but never developed as pharmaceuticalsfor various reasons. For instance, a substancewith antibiotic activity might not have beenbrought to market because it was no better thanmarketed antibiotics against susceptible bacteriaor because it was somewhat more toxic than mar-keted antibiotics. In screening materials for anti-biotic activity against antibiotic-resistantbacteria, companies often re-discover such oldcompounds. Although they might appear promis-ing because of activity against antibiotic-resis-tant bacteria, no company will do the researchand development necessary to bring them to mar-ket because patent protection is or soon will begone.
As an example, fusidic acid is an antibioticthat was never brought to market in the UnitedStates but that has been used in other countries,including Canada, for years. It is used in thetreatment of MRSA in other countries, but itsmanufacturer perceives that the return on invest-ment would be too low to warrant pursuing clini-cal trials for use against MRSA in this country. Alicensing agreement with a United States firmfaces a similar obstacle; if the trials were suc-cessful, any other company could manufactureand sell the off-patent substance, greatly reduc-ing the opportunities for the foreign-UnitedStates company venture to recoup its losses andmake a profit.
Congress could authorize FDA toextend market exclusivity for “off-patent” antibioticsthat are shown to be effective against antibiotic-resis-tant bacteria.
Such legislation might result in pharmaceuti-cal companies’ ferreting out effective antibioticsfrom the thousands that have been patented, butit would leave FDA with the difficult problem ofdeciding when the advantages of an antibioticjustified the granting of exclusivity. Marketexclusivity is one privilege granted under theorphan drug law, and it is possible that antibiot-
OPTION
OPTION

Chapter 1 Summary, Conclusions, Issues and Options | 31
ics that are effective against antibiotic-resistantbacteria would meet the requirements of anorphan drug.
Congress could establish a federal pro-gram to conduct clinical trials of antibiotics to deter-mine if they have uses against antibiotic-resistantbacteria.
An antibiotic that is off-patent and manufac-tured generically could be reported to be activeagainst infections caused by antibiotic-resistantbacteria. No company, however, would be inter-
ested in paying for the clinical trials necessary todemonstrate that the drug is useful because itcould not expect to reap sufficient profit fromsales of a generic drug.
A federal program could be established toconduct such trials. The advantage would be theidentification of useful antibiotics. The disadvan-tage would be the shouldering of clinical trialcosts, traditionally the responsibility of pharma-ceutical companies, by the government. More-over, it is possible that such a program, as anyresearch program, might have no successes.
OPTION

| 33
2Introduction
any of the organisms living around,on, and in human beings are too smallto be seen without a microscope.They include viruses, bacteria, fungi,
and protozoa (figure 2-1).Viruses are short lengths of genetic mate-
rial—deoxyribonucleic acid (DNA) or ribonu-cleic acid (RNA)—enclosed in a protein coat. Sosmall that they have no room for the structuresand processes for the biochemistry of their repli-cation, viruses are obligate internal parasites.They must invade cells—human, animal, plant,or bacterial, depending on the virus—take overthe cells’ genetic apparatus, and direct the bio-chemistry of the cell to produce viral nucleic acidand protein and package them into new viruses.
Bacteria, the single-celled organisms that arethe subject of this report, carry the structures andfunctions necessary for their replication in theircytoplasm. They generally are about one thou-sandth of a millimeter wide and nearly 500 timessmaller than the average animal cell (Watson etal., 1986.). Bacteria are classified as prokary-otes because, unlike eukaryotes, such as fungi,
protozoa, plants and animals, they have no inter-nal membrane (the nuclear envelope) separatingtheir genetic material from other components ofthe cell (figure 2-2). Bacteria differ from eukary-otes in having some molecular structures andbiochemical processes that are absent fromeukaryotes or that differ in significant ways fromthose of eukaryotes. Most antibiotics1 work byinterfering with a structure or process that ispresent in bacterial and not in other cells. Thisselectivity accounts for the rarity of serious side-effects associated with most antibiotics; thedrugs find no good targets in human (or othereukaryotic cells) and cause few effects there.Figure 2-3 illustrates the differential effects ofpenicillin on animal cells, which do not have cellwalls, and bacteria, which do, and a photo showsthe destruction of a bacterial cell by penicillin.Antibiotics have no effect on viral infections;viruses use the molecular structures and func-tions of the infected cells and viral-infected cellsoffer no targets for antibiotics.
Fungi and protozoa are eukaryotes. Antibiot-ics have no effect on most of these microorgan-
1 OTA uses the term “antibiotics” to refer to substances that kill or inhibit the growth of bacteria. It is sometimes used to refer to sub-stances that kill or inhibit organisms other than bacteria, but it is used here only to refer to substances with antibacterial activity.
M
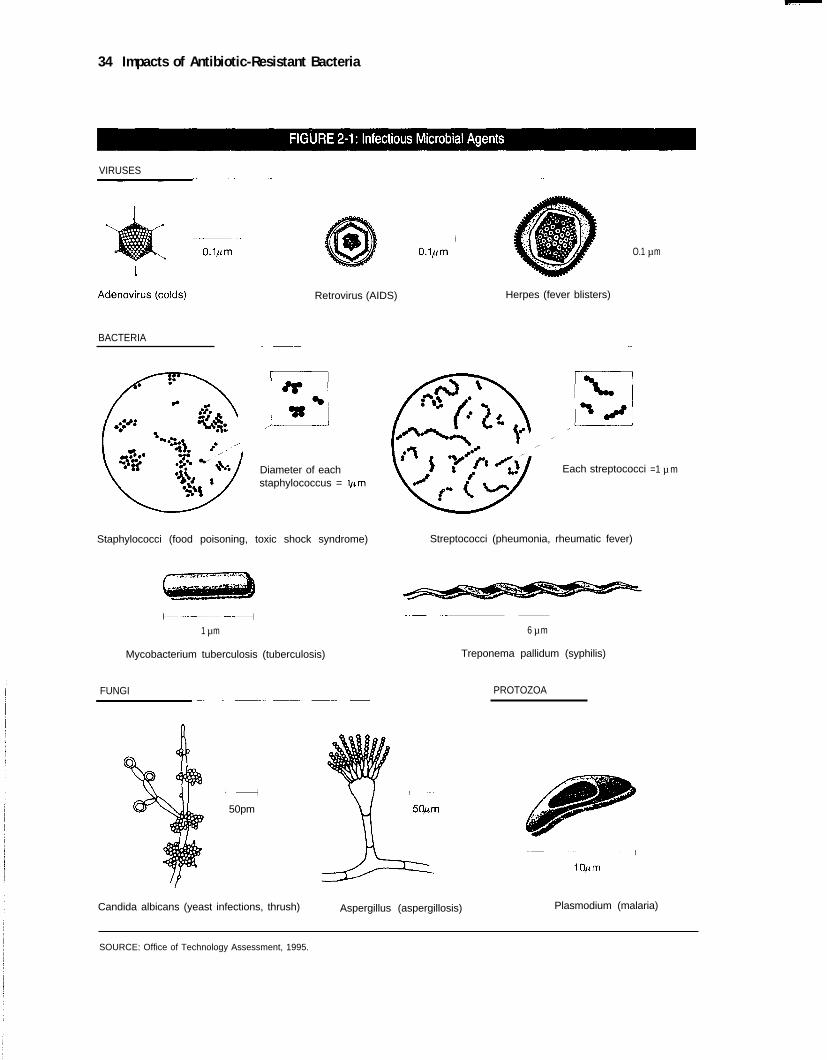
34 Impacts of Antibiotic-Resistant Bacteria
VIRUSES
BACTERIA
Retrovirus (AIDS)
Diameter of eachstaphylococcus =
Staphylococci (food poisoning, toxic shock syndrome)
1 µ m
Mycobacterium tuberculosis (tuberculosis)
FUNGI
Herpes (fever blisters)
O.1 µ m
Each streptococci
Streptococci (pheumonia, rheumatic fever)
6 µ m
Treponema pallidum (syphilis)
PROTOZOA
50pm
=1 µ m
Candida albicans (yeast infections, thrush) Aspergillus (aspergillosis) Plasmodium (malaria)
SOURCE: Office of Technology Assessment, 1995.
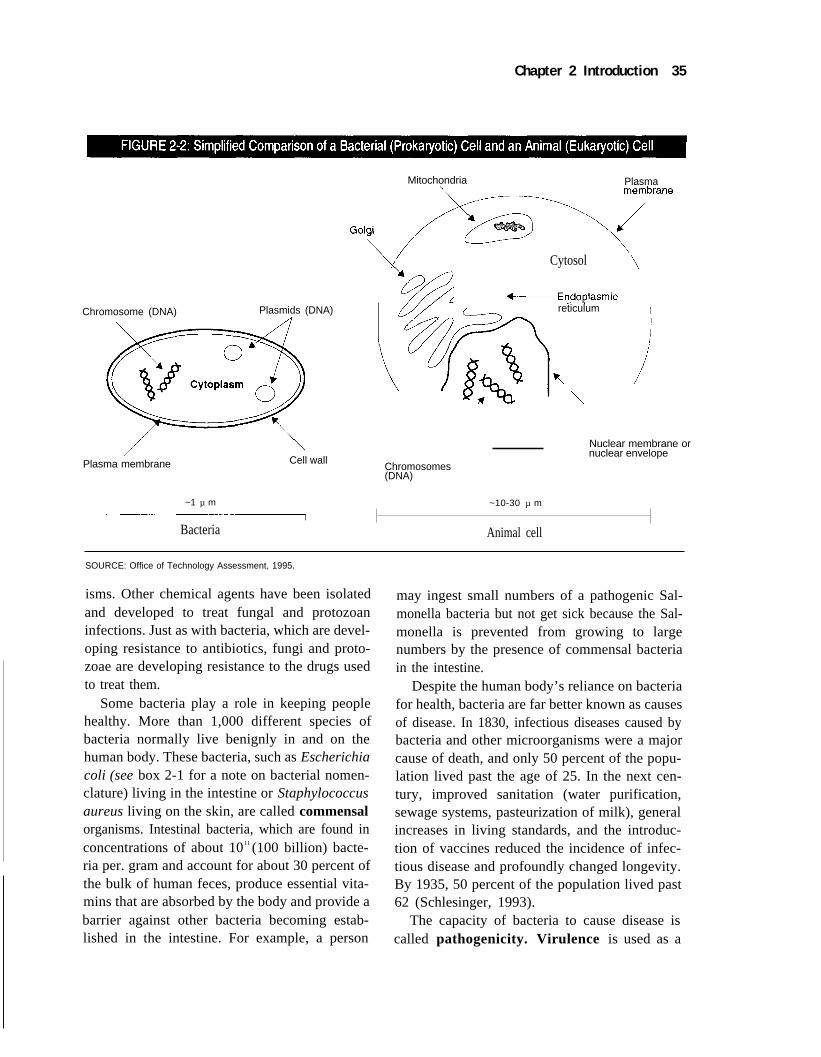
Chapter 2 Introduction 35
Mitochondria Plasma
Cytosol
Chromosome (DNA) Plasmids (DNA) reticulum
Nuclear membrane or
Cell wallnuclear envelope
Plasma membrane Chromosomes(DNA)
~1 µ m ~10-30 µ m
Bacteria Animal cell
SOURCE: Office of Technology Assessment, 1995.
isms. Other chemical agents have been isolatedand developed to treat fungal and protozoaninfections. Just as with bacteria, which are devel-oping resistance to antibiotics, fungi and proto-zoae are developing resistance to the drugs usedto treat them.
Some bacteria play a role in keeping peoplehealthy. More than 1,000 different species ofbacteria normally live benignly in and on thehuman body. These bacteria, such as Escherichiacoli (see box 2-1 for a note on bacterial nomen-clature) living in the intestine or Staphylococcusaureus living on the skin, are called commensalorganisms. Intestinal bacteria, which are found inconcentrations of about 1011 (100 billion) bacte-ria per. gram and account for about 30 percent ofthe bulk of human feces, produce essential vita-mins that are absorbed by the body and provide abarrier against other bacteria becoming estab-lished in the intestine. For example, a person
may ingest small numbers of a pathogenic Sal-monella bacteria but not get sick because the Sal-monella is prevented from growing to largenumbers by the presence of commensal bacteriain the intestine.
Despite the human body’s reliance on bacteriafor health, bacteria are far better known as causesof disease. In 1830, infectious diseases caused bybacteria and other microorganisms were a majorcause of death, and only 50 percent of the popu-lation lived past the age of 25. In the next cen-tury, improved sanitation (water purification,sewage systems, pasteurization of milk), generalincreases in living standards, and the introduc-tion of vaccines reduced the incidence of infec-tious disease and profoundly changed longevity.By 1935, 50 percent of the population lived past62 (Schlesinger, 1993).
The capacity of bacteria to cause disease iscalled pathogenicity. Virulence is used as a
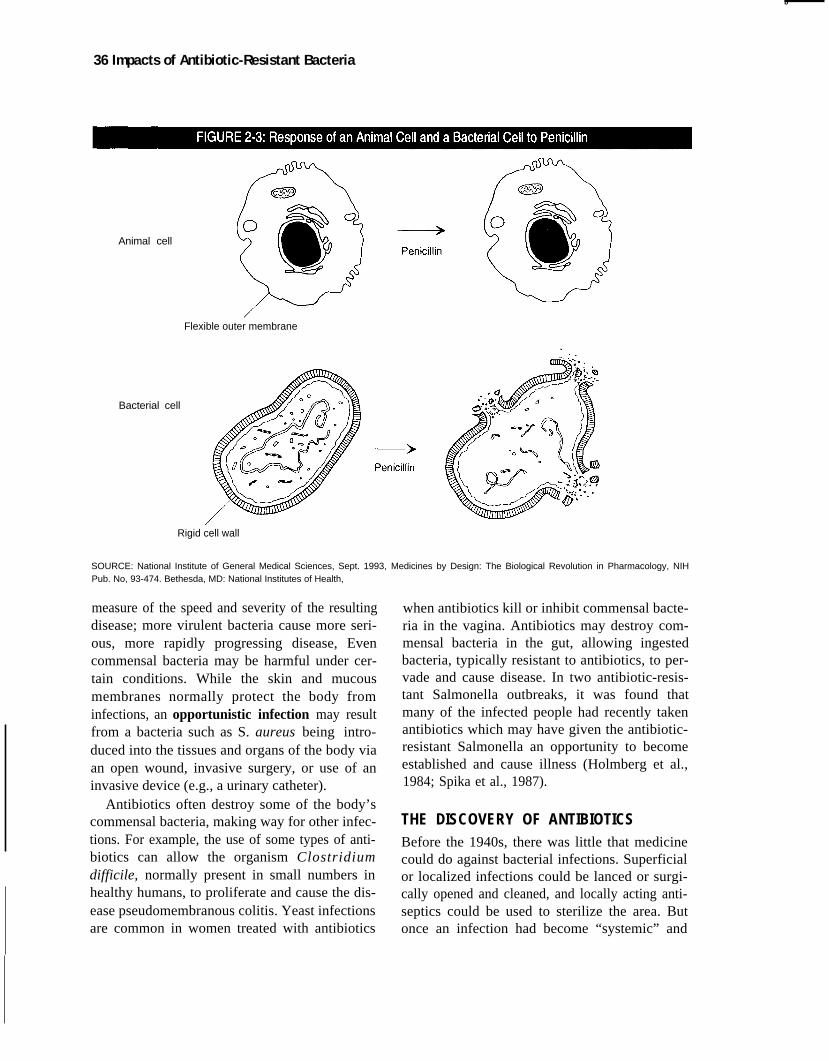
b
36 Impacts of Antibiotic-Resistant Bacteria
Animal cell
Bacterial cell
Flexible outer membrane
Rigid cell wall
SOURCE: National Institute of General Medical Sciences, Sept. 1993, Medicines by Design: The Biological Revolution in Pharmacology, NIHPub. No, 93-474. Bethesda, MD: National Institutes of Health,
measure of the speed and severity of the resultingdisease; more virulent bacteria cause more seri-ous, more rapidly progressing disease, Evencommensal bacteria may be harmful under cer-tain conditions. While the skin and mucousmembranes normally protect the body frominfections, an opportunistic infection may resultfrom a bacteria such as S. aureus being intro-duced into the tissues and organs of the body viaan open wound, invasive surgery, or use of aninvasive device (e.g., a urinary catheter).
Antibiotics often destroy some of the body’scommensal bacteria, making way for other infec-tions. For example, the use of some types of anti-biotics can allow the organism Clostridiumdifficile, normally present in small numbers inhealthy humans, to proliferate and cause the dis-ease pseudomembranous colitis. Yeast infectionsare common in women treated with antibiotics
when antibiotics kill or inhibit commensal bacte-ria in the vagina. Antibiotics may destroy com-mensal bacteria in the gut, allowing ingestedbacteria, typically resistant to antibiotics, to per-vade and cause disease. In two antibiotic-resis-tant Salmonella outbreaks, it was found thatmany of the infected people had recently takenantibiotics which may have given the antibiotic-resistant Salmonella an opportunity to becomeestablished and cause illness (Holmberg et al.,1984; Spika et al., 1987).
THE DISCOVERY OF ANTIBIOTICSBefore the 1940s, there was little that medicinecould do against bacterial infections. Superficialor localized infections could be lanced or surgi-cally opened and cleaned, and locally acting anti-septics could be used to sterilize the area. Butonce an infection had become “systemic” and
Chapter 2 Introduction 37
Penicillin-treated bacteria cell bursting at three different places.
Photo courtesy of National Institute of General Medical Sci-
ences, National Institutes of Health, Bethesda, MD.
was in the blood stream, little could be done. InWorld War I, once an infection from even aminor wound developed into dreaded “gas gan-grene” (an infection caused by Clostridium bac-teria related to the bacteria that cause botulism),there was no treatment except amputation of thewounded limb and prayer that the infection hadnot reached the soldier’s vital organs. Peoplelived in dread that they or their relatives woulddevelop a bacterial pneumonia and die or that abacterial endocarditis (infection of the heartvalves) would doom a child.
In 1906, chemist Paul Ehrlich provided thefirst weapon for combating bacterial infectionwhen he discovered that the chemical compoundsalvarsan was effective against syphilis. In 1936,Gerhard Dogmagk discovered that Prontosil, asynthetic dye, had antibacterial activity. Theactive chemical component of Prontosil, sulfanil-amide, was the first of the sulfonamide (or“sulfa”) drugs, and sulfa drugs are still usedwidely today.
In 1928, Alexander Fleming, an Englishmicrobiologist, discovered that a common mold(Penicillium) produced a substance that killedbacteria. Dr. Fleming returned from a weekend
Bacteria and bacterial diseases are our daily companions. There are bacteria literally everywhere in the envi-
ronment, and a few cause human diseases. Just as in sports where a scorecard is necessary to know the play-
ers, some knowledge of bacteria will help the reader, Humans—from the smallest children learning to talk to the
astronomer studying craters on other planets—identify and name things So it is with microbiologists who study
bacteria and biologists who study other forms of life. Everyone recognizes different mammals—humans, dogs,
cats, rats, mice, etc.—and recognizes their unique and salient features if not their scientific names—Homo sapi-
ens, Canis familiaris, Felis catus, Rattus rattus, Mus muscus. Such easy familiarity is not possible with organ-
isms that cannot be seen, and everyone has to rely on scientists’ identification and nomenclature to talk about
bacteria.
OTA associates bacteria with specific disease states, whenever possible, and uses standard scientific
nomenclature. For example, the cause of cholera is Vibrio cholerae, where “Vibrio” is the name of a bacterial
genus and “cholerae” is the name of a species. After the first use of such a name, the generic name is usually
abbreviated, as in V. cholerae. When both generic and specific names are used, the words are italicized. When
reference is made to a genus, such as “Enterococcus, ” the name is capitalized but not italicized, The terms “dif-
ferent bacteria” or “several bacteria” refer to ill-defined collections of different genera. “Strains” refers to further
divisions among a species; in particular, there are antibiotic-sensitive strains and antibiotic-resistant strains.
I
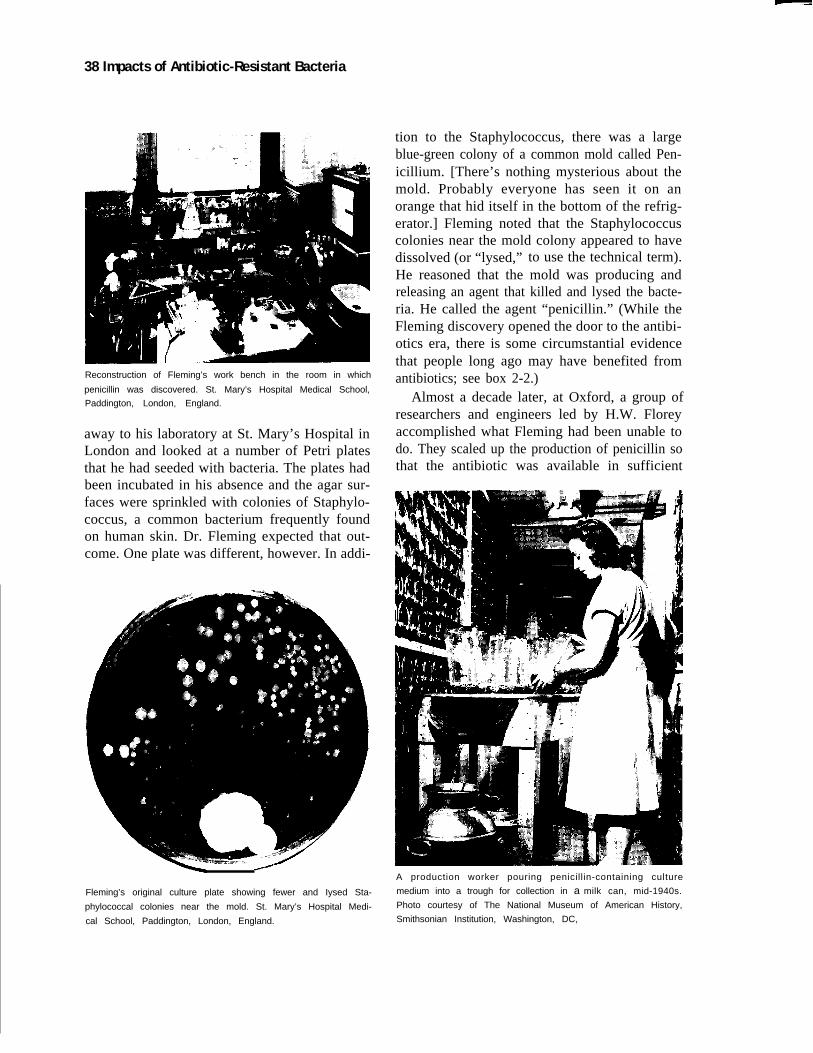
38 Impacts of Antibiotic-Resistant Bacteria
Reconstruction of Fleming’s work bench in the room in which
penicillin was discovered. St. Mary’s Hospital Medical School,
Paddington, London, England.
away to his laboratory at St. Mary’s Hospital inLondon and looked at a number of Petri platesthat he had seeded with bacteria. The plates hadbeen incubated in his absence and the agar sur-faces were sprinkled with colonies of Staphylo-coccus, a common bacterium frequently foundon human skin. Dr. Fleming expected that out-come. One plate was different, however. In addi-
Fleming’s original culture plate showing fewer and Iysed Sta-
phylococcal colonies near the mold. St. Mary’s Hospital Medi-
cal School, Paddington, London, England.
tion to the Staphylococcus, there was a largeblue-green colony of a common mold called Pen-icillium. [There’s nothing mysterious about themold. Probably everyone has seen it on anorange that hid itself in the bottom of the refrig-erator.] Fleming noted that the Staphylococcuscolonies near the mold colony appeared to havedissolved (or “lysed,” to use the technical term).He reasoned that the mold was producing andreleasing an agent that killed and lysed the bacte-ria. He called the agent “penicillin.” (While theFleming discovery opened the door to the antibi-otics era, there is some circumstantial evidencethat people long ago may have benefited fromantibiotics; see box 2-2.)
Almost a decade later, at Oxford, a group ofresearchers and engineers led by H.W. Floreyaccomplished what Fleming had been unable todo. They scaled up the production of penicillin sothat the antibiotic was available in sufficient
A production worker pouring penicillin-containing culture
medium into a trough for collection in a milk can, mid-1940s.
Photo courtesy of The National Museum of American History,
Smithsonian Institution, Washington, DC,

Chapter 2 Introduction | 39
quantities to be released to the Armed Forces totreat wounded servicemen as well as those withdiseases. Early production methods includedgrowing hundreds of cultures of Penicillium inglass bottles (sometimes milk bottles were used),collecting the culture broth, and purifying, con-centrating, and packaging the penicillin for ship-ment. The collection of the penicillin-containingculture medium could be done with devices assimple as a metal trough and a milk can. Cur-rently, the growth (fermentation) of the organ-isms that produce penicillin and other antibioticsis done in automated factories and with muchhigher efficiencies than were possible in the1940s.
By 1944, penicillin supplies were largeenough that some of the antibiotic was releasedfor civilian use, and the first antibiotic that couldbe ingested or injected without toxic side effectsentered medical practice. The cover of this reportis a reproduction of a 1944 advertisement forpenicillin. Penicillin was not made a prescriptiondrug until the 1950s, and, for about a decade, itwas available directly to the public (Levy 1992,p. 9).
Other “wonder drugs” followed penicillin, andmany dreaded infectious diseases became treat-able; people were saved from death and fromprolonged periods of disability. Tuberculosissanatoriums closed because antibiotics were suf-ficient treatment; people with burns over largeareas of their bodies, who would have died inearlier years, survived; childhood meningitis(infections of membranes around the brain or
spinal cord), formerly a death sentence, wastreatable; prolonged, dangerous, and only-some-times-effective treatments for syphilis and gon-orrhea were replaced by injection or ingestion ofan antibiotic. According to Schlessinger (1993),the use of antibiotics, along with nutrition andhealth education, increased the median lifespanby eight years, from 62 to 70 years, between1935 and 1955. (There has been little change inmedian lifespan since 1955.)
❚ The Limits of AntibioticsAntibiotics can fail to cure an illness because thebacteria are intrinsically resistant toward thedrugs or because they acquire resistance. Resis-tance is a property of bacteria that confers thecapacity to inactivate or exclude antibiotics or amechanism that blocks the inhibitory or killingeffects of antibiotics. Acquired resistance, here-after simply “resistance,” which is characterizedby changes in bacteria such that organisms thatwere formerly treatable with an antibioticbecome untreatable, is the focus of this report.
Most bacterial infections can be successfullytreated with one antibiotic or another, but theemergence of resistance to older antibiotics, suchas penicillin, leads physicians to prescribe newerantibiotics as the first choice in treating manydiseases. The use of the newer antibioticincreases selective pressure for the emergenceand spread of bacteria resistant to it, and themore an antibiotic is used, the greater the chancethat resistance to it will emerge and spread.
BOX 2-2: Antibiotic Use by Ancient Civilizations?
Perhaps unknowingly, earlier civilizations may have benefited from antibiotics. Bassett, Keith, Armelagos, etal. (1980) found evidence for the antibiotic tetracycline in the bones of Nubians who had been buried between350 and 550 A.D. Streptomycetes, the bacteria from which many antibiotics are derived, are common in theNubian Sudanese desert, and it is to be expected that the bacteria would have been picked up when the Nubi-ans harvested grain for bread and beer. Conditions in grain storage bins would have favored the growth of theStreptomycetes, which could have been the source of the antibiotic. Drawing upon other information, Bassett etal. state that infectious disease rates were low among this population of Nubians. Regardless of the details, thisevidence indicates that humans have interacted with antibiotics from well before 1928.
SOURCE: E.J. Bassett, M.S. Keith, G.J. Armelagos, et al. 1980. “Tetracycline-labeled bone from ancient Sudanese Nubia.” Science209:1532-1534.
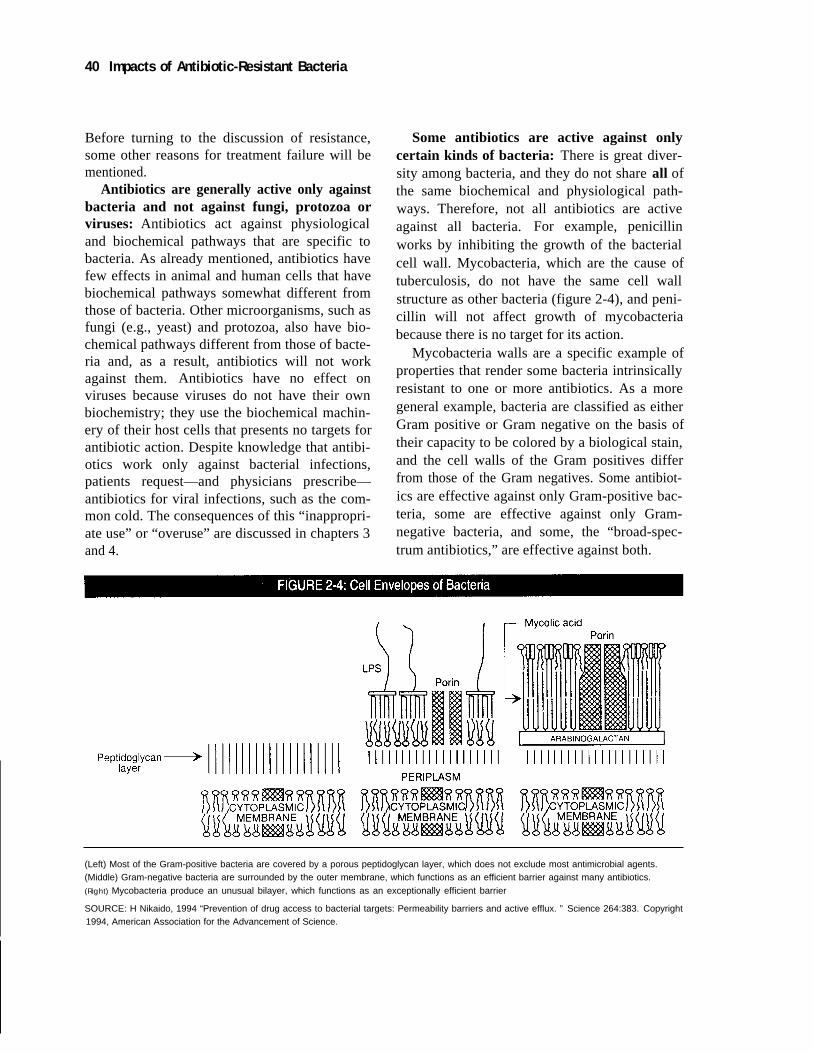
40 Impacts of Antibiotic-Resistant Bacteria
Before turning to the discussion of resistance,some other reasons for treatment failure will bementioned.
Antibiotics are generally active only againstbacteria and not against fungi, protozoa orviruses: Antibiotics act against physiologicaland biochemical pathways that are specific tobacteria. As already mentioned, antibiotics havefew effects in animal and human cells that havebiochemical pathways somewhat different fromthose of bacteria. Other microorganisms, such asfungi (e.g., yeast) and protozoa, also have bio-chemical pathways different from those of bacte-ria and, as a result, antibiotics will not workagainst them. Antibiotics have no effect onviruses because viruses do not have their ownbiochemistry; they use the biochemical machin-ery of their host cells that presents no targets forantibiotic action. Despite knowledge that antibi-otics work only against bacterial infections,patients request—and physicians prescribe—antibiotics for viral infections, such as the com-mon cold. The consequences of this “inappropri-ate use” or “overuse” are discussed in chapters 3and 4.
Some antibiotics are active against onlycertain kinds of bacteria: There is great diver-sity among bacteria, and they do not share all ofthe same biochemical and physiological path-ways. Therefore, not all antibiotics are activeagainst all bacteria. For example, penicillinworks by inhibiting the growth of the bacterialcell wall. Mycobacteria, which are the cause oftuberculosis, do not have the same cell wallstructure as other bacteria (figure 2-4), and peni-cillin will not affect growth of mycobacteriabecause there is no target for its action.
Mycobacteria walls are a specific example ofproperties that render some bacteria intrinsicallyresistant to one or more antibiotics. As a moregeneral example, bacteria are classified as eitherGram positive or Gram negative on the basis oftheir capacity to be colored by a biological stain,and the cell walls of the Gram positives differfrom those of the Gram negatives. Some antibiot-ics are effective against only Gram-positive bac-teria, some are effective against only Gram-negative bacteria, and some, the “broad-spec-trum antibiotics,” are effective against both.
(Left) Most of the Gram-positive bacteria are covered by a porous peptidoglycan layer, which does not exclude most antimicrobial agents.(Middle) Gram-negative bacteria are surrounded by the outer membrane, which functions as an efficient barrier against many antibiotics.
(Right) Mycobacteria produce an unusual bilayer, which functions as an exceptionally efficient barrier
SOURCE: H Nikaido, 1994 “Prevention of drug access to bacterial targets: Permeability barriers and active efflux. ” Science 264:383. Copyright1994, American Association for the Advancement of Science.

Chapter 2 Introduction | 41
Some bacteria are virulent and can killquickly: A virulent strain of group A streptococ-cus causes a disease called toxic shock-like syn-drome (TSLS) which killed Muppeteer JimHenson. Because this strain and other virulentbacteria can “fell otherwise healthy peoplewithin hours of the onset of symptoms” (Wright,1990), antibiotics have to be administered veryearly in order to defeat the infection.
Some bacteria grow in biofilms that cannotbe easily penetrated by antibiotics: Biofilmsare multilayer bacterial populations embedded ina film that is attached to some surface. Someexamples of bacteria growing in biofilms are theplaque that causes tooth decay, films ofPseudomonas aeruginosa that infect lung tissueespecially in cystic fibrosis patients, and filmsthat grow on the surfaces of medical devicessuch as catheters (see chapter 6). Antibioticsoften cannot penetrate biofilms; therefore, eventhough the antibiotic may be effective against thestrain of the bacteria in the laboratory, the antibi-otic may be ineffective against the infection.
❚ Mechanisms for the Emergence and Spread of ResistanceWhen a new antibiotic is introduced, many bac-teria are susceptible to it. Hughes and Datta(1983) demonstrated that bacteria preservedfrom 1917-1954 (the “pre-antibiotic” era) hadlittle if any antibiotic resistance except intrinsicresistance. However, since the dawn of the anti-biotic age, acquired resistance to every knownantibiotic has been observed in one or more bac-terial strains. This resistance sometimes arises inan individual patient during the course of treat-ment, but more often people are infected byresistant bacteria that are acquired from the com-munity or the hospital environment.
MutationsAntibiotic resistance arises through processesthat involve mutations and selection. Mutationsoccur spontaneously in bacterial DNA that mod-ify or eliminate a target for an antibiotic’s action,or that cause changes in the bacteria surface so
that the antibiotic is not taken up, or that causethe production of an enzyme that inactivates theantibiotic, or that cause the antibiotic to beexcreted from the bacterial cell. These mutationshappen in the absence of any exposure to antibi-otics, but the presence of an antibiotic favors thegrowth of the bacteria that contain a mutation forresistance, or in the usual jargon, the antibiotic“selects for” the mutant bacteria. Weiner (1995at pp. 257-262) discusses the origins of muta-tions to antibiotic resistance and the selection ofthose mutations in an evolutionary context.
Mutations are of three general kinds. Pointmutations are “single letter” mistakes that occa-sionally occur in copying the DNA code, andthey can cause a small change in an enzyme orstructural protein. The other two kinds of muta-tions, insertions and deletions, generally havemore far-reaching effects; they can completelyeliminate an enzyme activity or destroy a struc-tural protein. Mutations are passed on to futuregenerations of bacteria, and the number of resis-tant bacteria can increase very rapidly. Under themost favorable conditions, some bacteria canduplicate every 20 minutes.
As shown on figure 2-2, bacterial DNA ispresent on “chromosomes” and “plasmids.”Chromosomes usually contain all the genes nec-essary for the life of the bacteria, and some genesthat confer resistance to antibiotics are found onthe chromosome. Plasmids, smaller pieces ofDNA that replicate separately from the chromo-some, can also be present. They can and often docarry genes for antibiotic resistance, and, as dis-cussed below, they can be transferred from bac-terium to bacterium.
Chromosomal mutationsGenes for resistance to fluoroquinolone antibiot-ics (e.g., ciprofloxacin and ofloxacin) are knownto occur, so far, only on chromosomes and not onplasmids. Single courses of therapy with fluoro-quinolones may produce only low levels of resis-tance, but multiple mutations selected byrepeated exposure to increasing doses of fluoro-quinolones can confer high levels of resistance(Hooper and Wolfson, 1991). Even though muta-
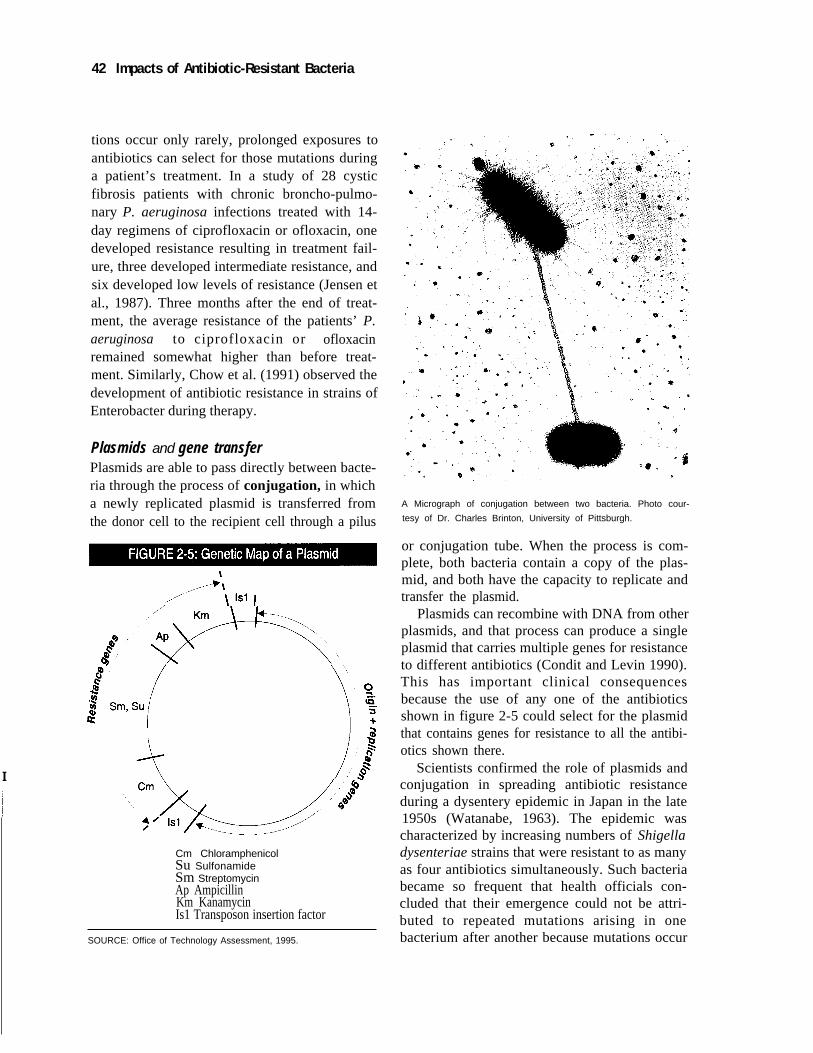
42 Impacts of Antibiotic-Resistant Bacteria
I
tions occur only rarely, prolonged exposures toantibiotics can select for those mutations duringa patient’s treatment. In a study of 28 cysticfibrosis patients with chronic broncho-pulmo-nary P. aeruginosa infections treated with 14-day regimens of ciprofloxacin or ofloxacin, onedeveloped resistance resulting in treatment fail-ure, three developed intermediate resistance, andsix developed low levels of resistance (Jensen etal., 1987). Three months after the end of treat-ment, the average resistance of the patients’ P.aeruginosa to ciprofloxacin or ofloxacinremained somewhat higher than before treat-ment. Similarly, Chow et al. (1991) observed thedevelopment of antibiotic resistance in strains ofEnterobacter during therapy.
Plasmids and gene transferPlasmids are able to pass directly between bacte-ria through the process of conjugation, in whicha newly replicated plasmid is transferred fromthe donor cell to the recipient cell through a pilus
Cm ChloramphenicolSu SulfonamideSm StreptomycinAp AmpicillinKm KanamycinIs1 Transposon insertion factor
SOURCE: Office of Technology Assessment, 1995.
A Micrograph of conjugation between two bacteria. Photo cour-
tesy of Dr. Charles Brinton, University of Pittsburgh.
or conjugation tube. When the process is com-plete, both bacteria contain a copy of the plas-mid, and both have the capacity to replicate andtransfer the plasmid.
Plasmids can recombine with DNA from otherplasmids, and that process can produce a singleplasmid that carries multiple genes for resistanceto different antibiotics (Condit and Levin 1990).This has important clinical consequencesbecause the use of any one of the antibioticsshown in figure 2-5 could select for the plasmidthat contains genes for resistance to all the antibi-otics shown there.
Scientists confirmed the role of plasmids andconjugation in spreading antibiotic resistanceduring a dysentery epidemic in Japan in the late1950s (Watanabe, 1963). The epidemic wascharacterized by increasing numbers of Shigelladysenteriae strains that were resistant to as manyas four antibiotics simultaneously. Such bacteriabecame so frequent that health officials con-cluded that their emergence could not be attri-buted to repeated mutations arising in onebacterium after another because mutations occur

Chapter 2 Introduction | 43
too rarely. Scientists showed that conjugationaltransfer of multiple-resistant plasmids accountedfor the epidemic and established plasmids asmajor agents in the spread of antibiotic-resistantgenes.
Hughes and Datta (1983), who examined pre-served bacterial strains from the pre-antibioticera, showed that plasmids were present in manyof the bacteria and that 24 percent of the plas-mids were able to be transferred by conjugationbetween bacteria. However, very few of the pre-served bacteria were resistant to antibiotics andthose few were resistant to only one antibiotic.This indicates that multi-resistance plasmidsmust have been created in the decades followingthe discovery of penicillin, when the use of anti-biotics became extensive. Importantly, however,the pre-existing transferable plasmids in bacteriabecame the vehicle for transfer of multiple anti-biotic-resistant genes.
Resistance genes can also travel on trans-posons, small pieces of DNA that can transfer todifferent sites on bacterial chromosomes andplasmids in the same bacterial cell or in differentbacterial cells. Hall and coworkers (Hall andStokes, 1993) have been studying the structure ofsome transposons called integrons that carryantibiotic-resistance genes. The integrons arelike freight trains: sequences of DNA necessaryfor the functioning of the integrons at the frontand the back are like the engine and the caboose,and any number of “cassettes” of resistancegenes, like the cars of the train, can be carriedbetween them. Different cassettes can insert intointegrons, and this facilitates the acquisition ofresistance genes by bacteria. Collis and Hall(1995) have also found that the expression of theintegrons depends on their position in the cas-sette: resistance coded by genes close to the frontof the train is stronger than resistance from genesnear the back of the train. This helps explain thevariability in the levels of resistance between dif-ferent strains of bacteria.
The origin of the resistance genes that can betransferred between bacteria on plasmids andtransposons is unknown, but some, at least,
might have originated as a self-protective mecha-nism in antibiotic-producing organisms. Forexample, some strains of streptomyces that pro-duce aminoglycosides (streptomycin is an ami-noglycoside) also produce aminoglycoside-modifying enzymes (Benveniste and Davies,1973).
Genes can be transferred between differentspecies of bacteria. In a 1979 outbreak in a Ken-tucky hospital (Tauxe, Holmberg, and Cohen,1989), 31 patients and personnel became infectedwith a strain of Staph. aureus that was resistantto methicillin, penicillin, gentamicin, erythromy-cin, clindamycin and tetracycline. Bacteria iso-lated from all of those affected contained thesame resistance plasmid. Plasmids of a similarsize were also found in the common skin com-mensal organism Staph. epidermis from theaffected patients. Analysis of the plasmids bymolecular techniques suggested that the sameplasmid had been transferred between Staph.aureus and Staph. epidermis.
In another study that demonstrated inter-spe-cies transfer, Tauxe, Cavanagh, and Cohen(1989) examined multiple-antibiotic-resistant E.coli and Shigella flexneri that were isolated froma hospitalized patient. Their analysis indicatedthat the resistant genes had been transferred fromthe E. coli to the S. flexneri and that the antibi-otic-resistant S. flexneri had then become thecause of a small outbreak of infections in thecommunity. These examples show that resistancegenes can be transferred between different bacte-rial species and demonstrate a pathway for wide-spread distribution of antibiotic-resistant genes.
There are two other mechanisms for genetransfer in addition to conjugation: transductionand transformation . In transduction, genes aretransferred by bacterial viruses (called “bacte-riophages” or “phages”). In transformation,pieces of DNA in the bacteria’s environment aretaken into the bacteria and incorporated into thebacterial chromosome. Hemophilus influenzaetakes up DNA from its surroundings, andrecently reported data indicate that transforma-tion may play an important role in the survival ofthose bacteria (box 2-3).

44 | Impacts of Antibiotic-Resistant Bacteria
❚ International Spread of Antibiotic ResistanceAntibiotic-resistance genes move with travelersfrom one country to another, making antibioticresistance an international problem. O’Brien etal. (1985) document the intercontinental spreadof an antibiotic-resistant gene on a plasmid, andSoares et al. (1992) reported the introduction ofstrains of multiple-resistant Streptococcus pneu-moniae from Spain to Iceland in the late 1980s.These examples illustrate that antibiotic use andbacterial resistance patterns all over the worldwill have an impact on the United States andindicate the importance of international coopera-
tion in dealing with the antibiotic-resistanceproblem.
❚ Persistence of Antibiotic Resistance Genes in the Absence of AntibioticsThe extent to which antibiotic resistance can becontrolled by limiting the use of antibiotics maybe answered by studying the molecular mecha-nisms of transposon and plasmid replication andthe behavior of populations of bacteria. Antibi-otic use selects for bacteria that carry antibiotic-resistance genes, but the resistant bacteria mightbe less efficient or use more energy because theycarry “excess baggage” of altered or extra genes.
BOX 2-3: The Complete DNA Sequence of Haemophilus influenzae
Using a variety of newly discovered methods, scientists have been working to sequence the DNA ofseveral different organisms, from humans to mice to bacteria. These sequences, when complete, locateevery “base“ or “nucleotide,“ the chemical units that carry the genetic code in an organism’s genome.
H.O. Smith and J.C. Venter led a group of scientists who completely mapped the DNA sequence ofHaemophilus influenzae Rd (Fleischmann et al., 1995). Their success marked the first complete DNAsequence for any free-living organism, and Venter has announced that sequences for two other bacteriaare nearly completed (Nowak, 1995).
The speed at which these sequences can be completed opens up a new era in understanding howbacterial DNA directs the activity of bacterial metabolism, and, in particular, it will enable scientists tounderstand the genes that are involved in virulence. For instance, H. influenzae Rb is a non-pathogenic“laboratory strain“ which is closely related to the human pathogen H. influenzae b. By comparing theDNA sequences from the Rb and b strains of H. influenzae, Fleischmann and colleagues (1995) wereable to demonstrate that eight genes that code for proteins necessary for the b strain to adhere to hostcells were missing from the Rb strain. This suggests that the Rb strains may not be pathogenic, at least inpart, because they cannot attach firmly to host cells.
H. influenzae can take up DNA from its environment and recombine the taken-up DNA into its ownDNA through the process called transformation. Smith et al. (1995) found that certain DNA sequencesoccur at 1,465 different locations on the H. influenzae DNA and that these sequences cause the bacteriato preferentially take up and incorporate DNA from its own species.
This feature enhances the capacity of H. influenzae to take up DNA from other H. influenzae that havedied. Why it would be desirable to take up DNA from bacteria that have been killed is unclear; presum-ably, the bacteria that die were less fit for their environment. However, the fact that the bacteria have somany recognition sequences suggests that the sequences, which increase opportunities for recombina-tion between the DNA of the dead bacteria and the surviving bacteria, are of survival advantage to thebacteria.
SOURCES: R.D. Fleischmann, M.D. Adams, O. White, O., et al. 1995. “ Whole-genome random sequencing and assembly of Hae-mophilus influenzae Rd.” Science 269:496-512; Nowak, R. 1995. “Bacterial genome sequence bagged.” Science 269:468-470;H.O. Smith, J.-F. Tomb, B.A. Dougherty, et al. 1995. “Frequency and distribution of DNA uptake signal sequences in the Haemo-philus influenzae Rd genome.” Science 269:538-540.

Chapter 2 Introduction | 45
Such genes can make the difference between sur-vival and death in the presence of an antibiotic,but their maintenance in an antibiotic-free envi-ronment might put bacteria that bear them at acompetitive disadvantage with bacteria that donot carry such genes.
Simonsen (1991) discusses the fate of plas-mids in the absence of selection pressure fromantibiotics. The “excess baggage” theory predictsthat easing the selective pressure by decreasingthe use of antibiotics would lead to a decrease inthe carriage of antibiotic-resistance genes bybacteria. But Bouma and Lenski (1988) showedthat this may not always be the case. Theyinserted a plasmid that carried a tetracycline-resistance gene into a strain of E. coli. The E.coli carrying the plasmid grew poorly as com-pared to E. coli without it (the plasmid is “excessbaggage”). Of course, in the presence of tetracy-cline, the bacteria that did not have the plasmidwould not grow. As expected, after 500 genera-tions of growth in tetracycline, all bacteria con-tained the plasmid. Moreover, even in theabsence of tetracycline, the plasmid-bearing bac-teria now grew better than the bacteria withoutthe plasmid. The bacteria had somehow adaptedin those 500 generations to become more effi-cient while retaining the plasmid.
This result leads to the suggestion that evolu-tion can produce plasmid-carrying bacteria thatare not at significant disadvantage in competitionwith other bacteria in antibiotic-free environ-ments. It can also be interpreted to indicate thatplasmid-carrying bacteria will not be eliminatedby eliminating antibiotics.
On the other hand, there are many examples inwhich controlling the use of antibiotics leads to adecrease in the frequency of bacteria carryingantibiotic-resistance genes. This may reflect thatantibiotic-susceptible bacteria (those without“excess baggage”) usually outgrow antibiotic-resistant bacteria so that the resistant bacteriabecome a smaller and smaller proportion of thetotal population. However, this process may bevery slow, and the resistance does not decrease tozero. The observation that the antibiotic-resistantbacteria do not disappear (drop to zero) may be
consistent with the results of Bouma and Lenski,because bacteria may adapt so that carrying plas-mids containing resistance genes provides anadvantage, even in the absence of the antibiotic.
CONFRONTING ANTIBIOTIC RESISTANCECurrently, half a century after the introduction of“wonder drugs,” scientists, physicians and thepublic fear the re-emergence of infectious dis-eases caused by antibiotic-resistant bacteria.Krause (1992) observed
[M]icrobes are not idle bystanders, waiting fornew opportunities offered by human mobility,ignorance or neglect. Microbes possess remark-able genetic versatility that enables them todevelop new pathogenic vigor, to escape popu-lation immunity by acquiring new antigens, andto develop antibiotic resistance.
Scientists who contributed to the biologicalresearch that produced antibiotics warn that soci-ety has unwisely tolerated the risk that was evi-dent in reports of the proliferation of geneticalterations in bacteria that spread antibiotic resis-tance:
The stunning success of the pharmaceuticalindustry in the United States, Japan, the UnitedKingdom, France and Germany in creating newantibiotics over the past three decades hascaused society and the scientific community tobecome complacent about the potential of bac-terial resistance... [D]espite all these antibiotics,a person could die in a hospital in New York,San Francisco, Paris, Barcelona, Tokyo, or Sin-gapore as a result of a resistant bacterial infec-tion (Neu, 1992).
There are many questions surrounding antibi-otic resistance. Is it possible that alternative strat-egies of scientific research and antibioticdevelopment could have prevented this out-come? Have antibiotics been improperly pre-scribed or inappropriately requested by patients?If evidence was available from the start that dis-ease-carrying bacteria could become resistant toantibiotics, what postponed the crisis for 50years? Although the Institute of Medicine identi-fied antibiotic-resistant microorganisms as onlyone of six factors contributing to the rising risk
46 | Impacts of Antibiotic-Resistant Bacteria
of morbidity and mortality from infection, itwarned that antibiotic resistance “may be agreater threat to the public than the emergence ofa new disease” (IOM, 1992).
The following chapters discuss what is knownabout antibiotic resistance and address theimportant questions of what can be done now tohelp slow the emergence and spread of antibi-otic-resistant bacteria, to preserve the capacity totreat bacterial infectious diseases with availableantibiotics, and to develop new antibiotics.
REFERENCESBenveniste, R., and J. Davies. 1973. Aminogly-
coside antibiotic-inactivating enzymes inactinomycetes similar to those present inclinical isolates of antibiotic-resistant bacte-ria. Proceedings of the National Academy ofScience, U.S.A. 70(8):2276–2280.
Bouma J.E., and R.E. Lenski. 1988. Evolution ofa bacteria/plasmid association. Nature 335:351–352.
Chow J.W., M.J. Fine, D.M. Shlaes, et al. 1991.Enterobacter bacteremia: clinical featuresand emergence of antibiotic resistance dur-ing therapy. Annals of Internal Medicine115:585–590.
Collis, C.M., and R.M. Hall. 1995. Expression ofantibiotic resistance genes in the integratedcassettes of integrons. Antimicrobial Agentsand Chemotherapy 39:155–162.
Condit, R., and B.R. Levin. 1990. The evolutionof plasmids carrying multiple resistancegenes: the role of segregation, transposition,and homologous recombination. The Ameri-can Naturalist 135:573–596.
Fleischmann, R.D., M.D. Adams, O. White, et al.1995. Whole-genome random sequencingand assembly of Haemophilus influenzaeRd. Science 269:496–512.
Hall, R.M., and H.W. Stokes. Integrons: novelDNA elements which capture genes by site-specific recombination. Genetica 90:115–132.
Holmberg, S.D., J.D. Wells, and M.L. Cohen.1984. Animal-to-man transmission of anti-microbial-resistant Salmonella: investiga-tions of U.S. outbreaks, 1971–1983. Science225:833–835.
Hooper, D.C., and J.S. Wolfson. 1991. Fluoro-quinolone antimicrobial agents. NewEngland Journal of Medicine 324:384–394.
Hughes, V.M., and N. Datta. 1983. Conjugativeplasmids in bacteria of the “pre-antibiotic”era. Nature 302:725–726.
Institute of Medicine. 1992. Emerging Infections.Microbial Threats to Health in the UnitedStates. Washington D.C. National AcademyPress.
Jensen, T., S.S. Pedersen, C.H. Nielsen, et al.1987. The efficacy and safety of ciprofloxa-cin and ofloxacin in chronic Pseudomonasaeruginosa infection in cystic fibrosis. Jour-nal of Antimicrobial Chemotherapy 20:585–594.
Krause, R.M. 1992. The origin of plagues: oldand new. Science 257:1073–1082.
Levy, S. 1992. The Antibiotic Paradox. NewYork, NY. Plenum Press.
Neu, H.C. 1992. The crisis in antibiotic resis-tance. Science 257:1064–1073.
O'Brien, T.F., M. Del Pilar Pla, K.H. Mayer, etal. 1985. Intercontinental spread of a newantibiotic resistance gene on an epidemicplasmid. Science 230:87–88.
Schlessinger, D. 1993. Biological basis forantibacterial action. In: M. Schaechter, G.Medoff and B.I. Eisenstein (eds.) Mecha-nisms of Microbial Disease: Second EditionBaltimore, MD. Williams and Wilkins, pp.77–89.
Simonsen, L. 1991. The existence conditions forbacterial plasmids: theory and reality.Microbial Ecology 22:187–205.
Smith, H.O., J.-F. Tomb, B.A. Dougherty, et al.1995. Frequency and distribution of DNAuptake signal sequences in the Haemophilusinfluenzae Rd genome. Science 269:538–540.

Chapter 2 Introduction | 47
Soares, S., K.G. Dristinsson, J.M. Musser, et al.1992. Evidence for the introduction of amultiresistant clone of serotype 6B Strepto-coccus pneumoniae from Spain to Iceland inthe late 1980s. Journal of Infectious Dis-eases 168:158–163.
Spika, J.S., S.H. Waterman, G.W. Soo Hoo, et al.1987. Chloramphenicol-resistant Salmonellanewport traced through hamburger to dairyfarms. New England Journal of Medicine316:565–570.
Tauxe, R.V., T.R. Cavanagh, and M.L. Cohen.1989. Interspecies gene transfer in vivo pro-ducing an outbreak of multiple resistantshigellosis. The Journal of Infectious Dis-eases 160:1066–1070.
Tauxe, R.V., S.D. Holmberg, and M.L. Cohen.1989. The epidemiology of gene transfer in
the environment. In: S.B. Levy and R.V.Miller (eds.) Gene Transfer in the Environ-ment. New York, NY. McGraw-Hill Pub-lishing Company, pp. 377–403.
Watanabe, T. 1963. Infective heredity of multi-drug resistance in bacteria. BacteriologicalReviews 27:87–115.
Watson, J.D., N.H. Hopkins, J.W. Roberts, et al.1986. Molecular Biology of the Gene:Fourth Edition Vol. 1: General Principles.Menlo Park, CA. Benjamin/Cummings Pub-lishing Co., p 123.
Weiner, J. 1995. The Beak of the Finch: A Storyof Evolution in Our Time. New York, NY.Alfred A. Knopf.
Wright, K. 1990. Bad news bacteria. Science249:22–24.
| 49
3
AntibioticUse and
Resistance inthe Community
he introduction of antibiotics nearly ahalf century ago controlled many life-threatening diseases, reduced the tolls ofdeath and illness, and increased the life
expectancy of Americans (Schlessinger, 1993).However, treatment with antibiotics can selectfor resistant bacteria that are not killed by thedrugs, and those bacteria flourish and spread inenvironments where antibiotics are present (seechapter 2). As a result, bacterial resistance toantibiotics accompanied the use of the “wonderdrugs,” and some antibiotics lost their effective-ness in treating certain bacterial diseases. Antibi-otic-resistant bacteria complicate treatment ofillnesses ranging from ear infections to pneumo-nia and tuberculosis (TB). Patients infected withthese organisms are more likely to require hospi-talization, have a longer hospital stay, and die(McCaig and Hughes, 1995). Antibiotic-resistantbacteria are more common in hospitals, whereantibiotic concentrations are high (see chapter 4),but they are also present in the community.
This chapter describes antibiotic use and resis-tance in the community, which in this report
refers to those persons not in hospitals or nursinghomes. The first section of this chapter discussesnon-hospital use of antibiotics with an emphasison physicians’ office practice. The second sec-tion describes the populations that are most sus-ceptible to antibiotic-resistant bacteria, thediseases to which they are most vulnerable, fac-tors in the emergence of antibiotic-resistant bac-teria, and changes in disease patterns related to orcomplicated by antibiotic-resistant bacteria. Italso discusses the paucity of information aboutthe prevalence of antibiotic-resistant bacteria aswell as some surveillance systems used to obtaininformation about other infectious organisms.
INTRODUCTIONA mother takes her 2-year-old son to the doctor’soffice for a middle ear infection, also known asotitis media.1 This visit is one of nine such visitsover the past year. About every four to six weeksher son’s physician switched antibiotics becausethe drugs had stopped working. She has had sim-ilar problems with her 4-year-old son, who has
1 Otitis media is a bacterial disease that is prevalent in young children and more common in those in day care. Children in day-care are anat-risk population that are susceptible to all infectious diseases, some of which are caused or worsened by antibiotic-resistant bacteria. Thisissue is discussed further later in this chapter.
T

50 | Impacts of Antibiotic-Resistant Bacteria
had about six ear infections during the same timeperiod. This scenario is becoming more prevalentwith increasing resistance to antibiotics. From1975 to 1990, the annual visit rate to office-basedphysicians for otitis media more than doubled;for children under 15 years of age, the rateincreased almost 150 percent (Schappert, 1992).Ninety percent of all American children willhave had at least one ear infection before age six,and the national cost of treating them is $3.5 bil-lion each year (Williams, 1994).
One of the causative agents in these recurringinfections is Streptococcus pneumoniae (“pneu-mococcus”), which is a leading cause of illnessand death in the United States, causing an esti-mated 7 million cases of otitis media; 50,000cases of bacteremia; and 3,000 cases of meningi-tis annually. Scientists at the Centers for DiseaseControl and Prevention (CDC) and otherresearchers have documented increasingly com-mon resistance to penicillin in S. pneumoniae.From 1979 through 1987, 0.02 percent of S.pneumoniae isolated from invasive infectionswere resistant to penicillin. By 1992, that per-centage had jumped 60-fold to 1.3 percent.Resistance is much higher in some communities,where at least 30 percent of isolates are eitherintermediately or highly resistant to penicillin(Jernigan et al., 1995). Among the states, thehighest documented penicillin resistance ratewas 26 percent in Alaska, with rates in otherparts of the country ranging from 1 to 16 percent(Tan et al., 1993).
Like antibiotic-resistant bacteria in general,penicillin-resistant S. pneumoniae are an interna-tional problem. They emerged in Australia andSouth Africa in the 1960s and 1970s. By the late1980s, 40 percent of community-acquired and 95percent of hospital-acquired S. pneumoniaeinfections in South Africa were penicillin-resis-tant. The strains spread rapidly and had beenidentified in Southeast Asia, other parts ofAfrica, and Europe in the 1980s. Hungary hadthe highest resistance rate in Europe in the late1980s: up to 69 percent of S. pneumoniae iso-lated from children were resistant. In other coun-tries, such as Spain and Romania, penicillin-
resistance rates ranged between 22 and 44 per-cent (Klugman, 1990; Tan et al., 1993).
By the 1990s, some S. pneumoniae strains hadbecome resistant to all penicillin-type drugs, aswell as the aminoglycoside-type antibiotics,chloramphenicol, and erythromycin, leavingphysicians with few treatment options, and caus-ing epidemiologists to worry about when resis-tance to vancomycin—one of the last antibioticsavailable to treat some multidrug resistant organ-isms such as Staph. aureus—would emerge(Levine et al. 1991).
❚ Antibiotic Use and ResistanceAny use of antibiotics, whether “appropriate” or“inappropriate,” can contribute to the emergenceand spread of antibiotic-resistant bacteria.Appropriate uses are those that benefit thepatient, by treating a bacterial infection, and therisks of increasing the spread of antibiotic-resis-tant bacteria are offset by those benefits. Inap-propriate uses are those that do not benefit thepatient, but that increase the use of antibioticsand the risk of encouraging the spread of antibi-otic-resistant bacteria. The term “overuse” iscommonly used in reference to inappropriate use.
Numerous studies have shown a direct rela-tionship between use of antibiotics and the spreadof antibiotic-resistant bacteria (McGowan, 1983;Mouton et al., 1990; Moller, 1989; Ringertz andKronvall, 1987; and Sogaard et al., 1974). Studiesalso indicate that reducing use of antibiotics maylower the frequency of antibiotic-resistant bac-teria (Ballow and Schentag, 1992; McGowan,1983). The focus in reducing antibiotic use hasbeen on reducing inappropriate uses.
Resistant microbes would have emerged evenif antimicrobial drugs were always used for theproper indication and at the proper dose andduration. However, the selective pressure wouldnot have been as great, the pace of developmentof resistance would have been slower, and theextent of the problem in terms of the number ofpeople involved would have been less. Onceresistant strains are selected, they can infect otherindividuals and spread within a community or

Chapter 3 Antibiotic Use and Resistance in the Community | 51
institution. They can also transfer the geneticinformation for resistance to other bacteria.While the natural history of the spread of antibi-otic-resistant genes is not known with certaintyand probably varies depending on the bacteria inwhich the mutation arose, the process can bedescribed in a general way. Mutations occur andbacteria that bear them are selected by exposureto antibiotics. The frequency of the mutationsmay remain constant and low for many years andthen spurt upwards, most likely as a result of thetransfer of resistant genes among bacteria and theincreased selection by antibiotic usage.
❚ Factors in Prescribing AntibioticsThe most common infectious conditions seen inoffice practice are diseases of the respiratory sys-tem, nervous or sense organs (mostly otitis mediain children), skin and subcutaneous tissue, andgenitourinary system. In sum, these conditionsaccount for more than 80 percent of office visitsin which antimicrobial drugs are prescribed.Antibiotics are not only used to treat infectionsbut to prevent them. Physicians prescribe antibi-otics prophylactically to protect people who havebeen exposed to individuals with infectious dis-eases and to prevent commensal organisms—those bacteria that are naturally found in thedigestive system or on the skin—from spreadingas a result of disease or injury from their usualresidence to normally sterile parts, the blood, tis-sues, and organs of the body. For example, peni-cillin may be administered prophylactically topatients who have damaged heart valves to pre-vent bacterial infections in the bloodstream andheart when they undergo dental or minor surgicalprocedures in dental or medical offices. (In-hos-pital prophylaxis is discussed in chapter 4.)
Many respiratory and ear infections are causedby viruses. Antibiotics have no effect on viruses,and there is no clinical evidence that antibioticswill prevent secondary or superimposed bacterialinfections in a patient with a viral infection. Anti-biotics prescribed for viral infections are wastedand are examples of inappropriate use and over-use. Moreover, some bacterial diseases will clear
up in the same time with or without antibiotics.For instance, despite their widespread use forearaches, antibiotics do not always convey a ben-efit: about 20 percent of middle ear infections arecaused by viruses. Perhaps one-third of them arecaused by bacteria that cause self-limiting infec-tions that will “go away” without treatment(Klein, 1994), although antibiotics may helpthem go away faster.
Physicians can obtain information about thecauses of middle ear infections only by obtainingfluid samples from behind the patient’s eardrum.Those samples are then sent to laboratorieswhere the possible infecting organisms are cul-tured, identified, and classified as either suscepti-ble or resistant to antibiotics (see chapter 6).These activities take several days, and ofteninvolve an invasive procedure, such as punctur-ing the eardrum to obtain a sample, which mostphysicians and patients want to avoid. The physi-cian seeing a patient is not likely to wait severaldays for laboratory results before prescribing anantibiotic, and the patient is almost certainly notgoing to want to wait. Generally, the physicianknows that there may be several types of bacteriathat may be causing the infection. Therefore, heor she will usually prescribe a broad-spectrumantibiotic that will work against any of the sev-eral bacteria most likely to be causing the infec-tion.
However, it would be preferable to treatpatients with a narrow-spectrum antibiotic tar-geted at the specific cause of infection and savebroad-spectrum antibiotics for the treatment ofbacteria resistant to other antibiotics. But empirictreatment is the standard of care and, in someinfections, the only possible course of action.Even so, some prescriptions are written with nomore information than the patient’s complaint orin response to the patient’s request (see box 3-1).
Improvements in diagnostic technologies thatwould enable the rapid identification of bacteriaand their patterns of antibiotic-susceptibility andresistance would reduce the need for empirictherapy. However, rapid technologies that wouldproduce useful diagnostic results during thecourse of an office visit are not on the immediate

52 | Impacts of Antibiotic-Resistant Bacteria
horizon. Moreover, to produce significantchanges in antibiotic usage, the use of new tech-nologies would probably have to be accompa-nied by changes in physicians’ and patients’attitudes and expectations (see chapter 6).
Forces other than those created by the techni-cal challenges of diagnosis influence and indeedpromote the use of antibiotics. Antibiotics aresometimes referred to as the “drugs of fear”(Kunin et al., 1973) because they can be used tomitigate the physicians’ fear of failing to providepatients with the very best care. Patients’ fears ofthe unknown and expectations for rapid cure arefostered by exaggerated stories in the newsmedia of dread diseases and new miracle cures.Pharmaceutical advertisements and sales repre-sentatives encourage “empiric, broad-spectrumcoverage,” perhaps glossing over the need for afull diagnostic assessment (Kim and Gallis,
1989; DiNubile, 1990). In addition, the physicianmay work for a health plan that prefers payingfor antibiotics over paying for a test that mayrequire another office visit.
Fundamentally, the risks, benefits, and costsof antibiotic treatment are not spread equally.The patient can expect to benefit from treatmentwith an antibiotic; there are few side effects fromthe antibiotics used in office practice, and out-of-pocket costs are likely to be relatively low. In thecase where the antibiotic is not effective, and thepatient recovers regardless, he or she has bornethe very low risk of side effects and any out-of-pocket costs. The significant risks and costs ofantibiotic use, including overuse, are borne bysociety as a whole. The contribution to antibioticresistance from one person taking antibiotics isnot that significant. Therefore, it might seem to aphysician treating a specific patient that it is bet-
BOX 3-1: Misperceptions About Antibiotic Usage
An OTA staff member went to the doctor because of a persistent sore throat. The physician asked,“Want some antibiotics?” There was no physical examination, and the physician did not take a throat cul-ture.
OTA staff understand the proper use of surveys and how they should be conducted to obtain data thatare representative of the population. However, there are times when informal, non-scientific surveys canprovide a snapshot of ideas and attitudes on a particular subject. The “Want some antibiotics?” eventprompted a survey of all OTA staff by electronic mail to find out their attitudes toward antibiotic use. Ofthe nearly 200 OTA employees and contractors onsite, 95 responded. Here are some of the results:Within the past year, 59 percent of respondents or their family members had used antibiotics, with themost common conditions being ear infections, sinusitis, and upper respiratory infections. About half ofthe respondents, at one time or another, had requested antibiotics from their doctor, and 30 percent ofthe respondents indicated that a physician had offered them an antibiotic without an examination.
Most of those responding apparently understood the importance of taking all of their own prescribedantibiotics; 56 percent of the respondents indicated that they always completed their full course of pre-scribed antibiotics. One person reported that he did not complete his full course of antibiotics for an ear
infection and stored the remainder of the prescription in his medicine cabinet because he felt better. Helater had to reach into the cabinet for those same antibiotics because the ear infection got worse. Thisrespondent’s attitude toward “left-over” or “unused” antibiotics was common. Thirty-seven percentreplied that they had later taken unfinished antibiotics that were stored in their medicine cabinets, and 10percent said that they had taken antibiotics that someone else had stored in the medicine cabinet. Takingmedicine prescribed for other persons is not only illegal, but it can have serious side effects.
Finally, most of the respondents were aware that antibiotics only work for bacterial infections and notcolds, which are caused by viruses. But there were a few exceptions. Fifteen percent indicated they hadtaken antibiotics for a cold.

Chapter 3 Antibiotic Use and Resistance in the Community | 53
ter to prescribe a broad-spectrum antibiotic, forexample, than to wait for test results or for theinfection to possibly clear on its own. However,collectively, these prescribing habits contributeto the spread of antibiotic-resistant bacteria. Nev-ertheless, the request for this study and the cur-rent attention given to antibiotic-resistantbacteria point to society’s need to collectivelyalter the uses of antibiotics to preserve the effi-cacy of these drugs.
❚ Trends in Antibiotic UseA 1995 study of antibiotic use shows no changein the number of prescriptions for antibiotics, butindicates that older antibiotics, such as thepenicillins, are being used less frequently infavor of the newer, more expensive drugs, suchas cephalosporins (McCaig and Hughes, 1995).Currently, the most-used drugs are the new andexpensive macrolides (azithromycin and clari-thromycin), the fluoroquinolones (ciprofloxacin,ofloxacin, and others), and newer cephalosporins(cefuroxime, ceflacor, and cefixime) (Kunin,1995).
Ciprofloxacin provides an example of theenthusiastic use of a new antibiotic among com-munity and hospital physicians. Its low toxicityand broad-spectrum activity make it the primarychoice for treating a wide range of conditions.Two years after its introduction in 1987, ciprof-loxacin became the fourth most commonly pre-scribed antimicrobial at total sales value of $248million (Frieden, 1990). This use may have con-tributed to the emergence of ciprofloxacin-resis-tant strains of MRSA (methicillin-resistantStaph. aureus), which is a common cause of seri-ous infections in hospitals (see chapter 4)
POPULATIONS SUSCEPTIBLE TO ANTIBIOTIC-RESISTANT BACTERIAAntibiotic-resistant bacteria pose a threat to thepopulation as a whole but are more likely tocause illness in populations at greater overall riskof contracting infectious diseases. The followingsection examines those susceptible populations,the factors that contribute to their vulnerability,
and the infectious agents to which they are mostsusceptible.
❚ The PoorThe poor and those who do not have adequateaccess to sanitary living conditions or properhealth care are particularly susceptible to infec-tious diseases. In underdeveloped countries mostof the poor live in overcrowded urban areas, havepoor hygiene, use unsanitary water, and havepoor nutrition and inadequate waste disposal.Half of the city dwellers of developing countries,who are not classified as homeless, live in shan-tytowns and slums that, among other things, lacksafe drinking water. Forty percent of them arewithout public sanitation or sewage facilities anda third live in areas in which there are no garbageor solid waste collection services (Garrett, 1994).As well illustrated by Levy (1992) and others,antibiotic-resistant bacteria that arise in foreigncountries migrate to the United States when resi-dents of foreign lands visit or immigrate here andwhen American citizens visit other countries andreturn with illnesses.
Even in this country, where sanitary standardsare much better, other deplorable conditionsexist. Many urban areas are laced with inade-quate housing. Drug addiction, alcoholism,homelessness, incarcerations, and general eco-nomic impoverishment is a way of life for someinner-city residents, many of whom are ethnicminorities. These factors provide a ripe breedingground for disease-causing organisms and thevectors that carry and spread them throughoutthe population.
❚ People Without Adequate Health CareApproximately 37 million Americans do nothave medical insurance, and most of them are theworking poor and their dependents (Hammond,1994). Because this population generally cannotafford health care, many of their medical condi-tions go undiagnosed, or they may delay treat-ment because they have to choose betweenmeeting basic living expenses and living with anillness that they think is not severe or life-threat-

54 | Impacts of Antibiotic-Resistant Bacteria
ening. Those who are poor, uninsured, and with-out a regular physician delay seeking medicalcare 40 to 80 percent more often than otherpatients; most think their problems are not seri-ous. Overall, patients who are poor or uninsuredare 12 times more likely than other patients todelay seeking health care because of cost (Weiss-man et al., 1991).
A 1992 OTA study confirmed this phenome-non. The report analyzed American studies onthe relationships between having health insur-ance and individual health outcomes and foundthat, all other being essentially equal, uninsuredpeople were up to three times more likely thanprivately insured individuals to experience lowerhealth care utilization, potentially inadequatehealth care, and adverse health outcomes (OTA,1992). These delays can worsen medical condi-tions and allow contagious diseases, like TB, tospread. Hospital stays of patients who reporteddelays in seeking medical care are 9 percentlonger than hospital stays of other patients(Weissman et al., 1991). Once hospitalized, thepatient may be at higher risk of a nosocomialinfection (hospital-acquired infections) becausethe delay in treatment has lowered the body’snatural resistance.
Lack of adequate medical care may have con-tributed to an outbreak of multiply resistantpneumococcal infections in Oklahoma in 1989 to1990. Among the hardest hit were infants, theelderly, and the state’s poor African Americanpopulation, whose overall rate of disease was 60percent higher than in whites. Overall, more than15 percent of the patients who developed thepneumonia died (Haglund et al., 1993).
❚ The IncarceratedDuring the 1980s, the United States’ “War onDrugs” produced a 126 percent increase in drug-related arrests (Skolnick, 1992). Most federaland state prisons were not equipped to handlethis sudden onslaught of prisoners, many ofwhom came from disadvantaged backgroundsand did not have a history of adequate preventivehealth care (Anderson, 1990). Almost one-third
of the newly admitted inmates in New York Statereported having been homeless just before incar-ceration, and the majority of inmates had histo-ries of substance abuse (OTA, 1993). Theseindividuals are at high risk for infections, espe-cially for TB and pneumococcal diseases,because both are diseases spread by airbornetransmission and can move easily through badlyventilated, overcrowded areas (Anderson, 1990;Hoge et al., 1994).
Additionally, the inmate population is tran-sient and provides a constant flow of people andtheir infectious organisms between the prisonand the community. As many as half the inmatesdetained in a large New York City correctionalcomplex, for example, are released within thefirst 48 hours after admission (Chisolm, 1988).Of the 15,000 to 20,000 or more inmates on anygiven day at Riker’s Island, a correctional facilityin New York City, half are discharged within aweek (Navarro, 1993; Bellin et al., 1993).Although the National Commission on Correc-tional Health Care recommends that medicalscreening or a review of the medical screening ofa prisoner’s health be performed on or before the14th day after initial booking, many prisoners arenot screened or treated for asymptomatic com-municable diseases. In Los Angeles County, forexample, the average stay is less than 14 days.Even when screening is performed, the resultsmay not be available until after the inmate hasbeen released. Subsequently, those at risk maynot be located and treated (Cohen et al., 1992).
The lack of adequate screening can result indire consequences, not only for the inmates butto the community in which they are released, aswell as for the workers at correctional facilities.From 1990 to 1992, 11 outbreaks of multiple-drug-resistant TB occurred in correctional facili-ties in 8 states, killing 13 inmates and one correc-tional officer. An outbreak in an Arkansas Stateprison spread to the community when a releasedinmate infected his wife and two children, one ofwhom died of probable tuberculous meningitis.Also, a news reporter covering the problems ofovercrowding in urban jails became infectedwith TB after working on a story about a New
Chapter 3 Antibiotic Use and Resistance in the Community | 55
York City jail (Skolnick, 1992). Because of over-crowding, the lack of adequate screening, and thetransient populations, TB has emerged in epi-demic proportions in the nation’s prisons. In1988, the new case rate of active TB infection inthe United States was 13.7 per 100,000, while theaverage rate was 75 per 100,000 among inmatesof state and federal prisons. Some correctionalfacilities had higher rates. In 1991, Riker’s Islandin New York City had an active infection rate of400 to 500 per 100,000 (Skolnick, 1992).
Prison overcrowding can also be a factor inthe spread of pneumococcal disease amonginmates. After two Houston, Texas, inmates diedfrom pneumococcal sepsis on the same day,health officials uncovered an epidemic of pneu-mococcal disease, a rare occurrence in the era ofantibiotics. The jail, which had been designed tohouse 3,500 persons, was accommodating 6,700residents at the time of the outbreak. Over a four-week period, 46 inmates developed acute pneu-monia or invasive pneumococcal disease.Besides overcrowded conditions, investigatorsalso discovered that inmate susceptibility andinadequate ventilation for the number of inmatesin the building were cofactors responsible for theoutbreak. Although none of the strains of S.pneumoniae were resistant, the re-emergence ofpneumococcal disease, coupled with sharpincreases in the number of strains that are multi-ple-drug-resistant raises questions about the needfor isolation wards in prisons and the vaccinationof institutionalized persons at risk for pneumo-coccal disease (Hoge, et al., 1994).
❚ The HomelessFinding an accurate estimate of the homelesspopulation is elusive. The estimates range from192,000 to 3 million people. Regardless of thetrue number, the homeless are at greater risk forimmune suppression because of poor nutrition,inadequate rest, and concurrent medical illness(Paul, 1993). Homeless shelters and shelters forbattered women provide ideal conditions fortransmission of infectious diseases, especiallyTB: large numbers of people in close quarters,
poor ventilation, the presence of undiagnosed oruntreated infectious cases, and prolonged expo-sure during lengthy stays, particularly in wintermonths. Several outbreaks of drug-resistant TBhave emerged among the homeless in southTexas, New York, and Boston. Resistance ratesin some of those areas were as high as 57 percent(Morris and McAllister, 1992; Pablos-Mendes etal., 1990; Barry et al., 1986; Gross and Rosen-berg, 1987.)
❚ Military PersonnelMilitary personnel in wartime field conditionslive in close quarters, experience rudimentaryfood and water sanitation services, and have fewopportunities to exercise good personal hygiene.Even peacetime training is characterized bycrowding and confined quarters, which favortransmission of infectious diseases.
Historically, respiratory diseases are a com-mon and serious problem in the military. As farback as 1500, historians recorded apparent strep-tococcal pneumonia epidemics. Recently, theU.S. military has experienced an increase instreptococcal-related disease. Outbreaks of S.pyogenes pharyngitis, acute rheumatic fever, andcases of streptococcal-induced toxic shock-likesyndrome have caused concern among militaryhealth officials. Respiratory disease caused bythe bacterium S. pneumoniae has also emerged asa problem. During the winter of 1989-1990, 124Marine trainees developed pneumococcal pneu-monia. Despite the Navy’s administration ofthousands of doses of pneumococcal vaccine andpenicillin G to the troops, this Marine populationcontinued to have the highest rates of pneumoniahospitalization in the Navy. In late 1991 andearly 1992, a pneumonia outbreak on two U.S.Navy ships located in Italian waters afflicted 25of the more than 1,700 crew members over afour-month period and killed two of them (Grayet al., 1994). These recent outbreaks, coupledwith the emergence of drug-resistant strains ofstreptococci, could present increasing difficultiesfor military health officials and impede the mili-tary’s performance.

56 | Impacts of Antibiotic-Resistant Bacteria
❚ Children in Daycare FacilitiesAn upsurge of women in the paid work force andthe increasing number of single-parent familiescontribute to the increased use of daycare facili-ties. About 90 percent of families with preschoolchildren use full- or part-time child daycare ser-vices (Thacker et al., 1992). As children spendmore time in daycare, the risk for some infec-tious diseases has increased. Close physical con-tact, inadequate hygiene, and lack of toilettraining facilitate the transmission of infectiousagents within childcare settings. These agents arespread by the fecal-oral route, contact with skin,excretions, or bodily fluids, or transmission byaerosols or respiratory droplets. The two mostcommon ailments for children in daycare areacute upper-respiratory tract illnesses and otitismedia. By age two, children attending daycarehave approximately seven or eight episodes ofacute respiratory illness per year, which is 1.6times greater than among children not attendingdaycare facilities (Thacker et al., 1992). Interpre-tation of these data is complicated because not allinfections recognized in children in daycare areacquired in the daycare environment; some areacquired elsewhere but first recognized in thedaycare facility (Sterne et al., 1986).
Many cases of drug-resistant bacteria havebeen reported in the daycare setting. One studyshowed that 57 percent of the children attendinga particular daycare center were colonized withtrimethoprim-resistant Escherichia coli, whileanother study detailed the hospitalization of twoinfants from the same daycare center in Texas,who had contracted sepsis and meningitis due toa multiple-resistant strain of S. pneumoniae (For-nasini et al., 1992; Rauch et al., 1990).
❚ The ElderlyAlthough the elderly, those aged 65 and older,are a relatively small proportion of the popula-tion, their numbers are increasing. By the year2025, the elderly will comprise a little more than10 percent of the population (USBC, 1994).Almost all of the nation’s nursing home popula-tion and a substantial part of the hospital popula-
tion are elderly. Because of their diminishingimmune systems, the presence of underlying dis-eases, and the use of invasive medical devices,the elderly are more susceptible to infectiousorganisms, including antibiotic-resistant bacteria(OTA, 1987). Hospitalized elderly patients aretwo to five times more likely to develop nosoco-mial infections than hospitalized youngerpatients. These infections are often fatal, in partbecause they are frequently caused by agents thatare resistant to antibiotics. The elderly are sus-ceptible to endocarditis, pneumonia, bacteremia,and bacterial meningitis, which is caused by S.pneumoniae in more than half the cases world-wide (Madhavan, 1994). (See chapter 4 for infor-mation about in-hospital disease, which isgenerally applicable to diseases in nursinghomes.)
❚ The ImmunosuppressedImmunosuppression, which is a result of a low-ered immune system response, can be caused bya number of factors, including the following con-ditions:
■ Prematurity (neonates);■ Inherited diseases;■ Malnutrition;■ Pregnancy;■ Concurrent infections;■ Severe trauma and burns;■ Infection with the human immunodeficiency
virus (HIV);■ Malignancy;■ Radiation treatment;■ Immunosuppressive medications for trans-
plantation, cancer chemotherapy, or treatmentfor autoimmune disease;
■ Aging.
Immunosuppression can result in opportunis-tic infections in an individual who otherwisewould have been able to fight illness. Theseinfections are caused by typically non-threaten-ing organisms that take advantage of a person’sweakened state. Although opportunistic infec-tions have received a great deal of attention over

Chapter 3 Antibiotic Use and Resistance in the Community | 57
the past decade with the onset of the HIV pan-demic, they are not new. It is well known that thevery young and the elderly are at the greatestdanger of succumbing to disease. Also, newmedical treatments and invasive technologieshave created additional openings for opportunis-tic pathogens (IOM, 1992). Therefore, drug-resistant bacterial infections can exacerbatehealth problems for the already immunocompro-mised.
FACTORS IN THE EMERGENCE OF BACTERIAL DISEASES
❚ Global AccessibilityTravel involves the movement of people andmicrobes from one region to another and hasalways been a factor in the emergence of infec-tious disease. Whether new diseases emergedepends on the novelty of the microbe beingintroduced, its transmissibility, and the existenceof an environment suitable for maintaining thedisease and its agent. Therefore it is important todistinguish between transient introductions oracquisitions of new diseases, which occur fre-quently, and the establishment and propagationof a new pathogen, which occurs rarely (IOM,1992).
For example, travelers from industrializednations to developing countries may unknow-ingly transport virulent pathogens on their return.One traveler who smuggled South Americancrabs back to the United States was the origin ofa cholera outbreak, and other infected travelershave brought the same disease to the UnitedStates from South America (Levine and Levine,1995).
❚ Improper Food Preparation PracticesFoodborne pathogens account for up to 7 millioncases of foodborne illnesses yearly and in 1992caused more than 9,000 deaths, most of whichwere associated with meat and poultry productscontaminated by pathogenic micro-organisms(Cassell, 1995). Moreover, these estimates maybe low because the surveillance systems for such
diseases are passive, meaning they are based onvoluntary reporting by state and local healthdepartments.
Foods contaminated with pathogenic microor-ganisms can lead to infection and illness in twomajor ways. The first is by direct consumption ofthe contaminated food under conditions thatallow the survival of the pathogen or its toxin,such as when a meat or poultry product is con-sumed raw or undercooked, or when productsthat are pre-cooked during processing are recon-taminated before consumption (AMA, 1993).
For example, in 1982 a virulent bacterialstrain, E. coli O157:H7, caused serious hemor-rhages of the colon, bowel, and kidneys in 47people in Oregon and Michigan (Riley et al.,1983). Nine years later an outbreak of E. coli inMassachusetts produced serious illness in 27people, 10 of whom required hospitalization.Health officials traced the disease to batches ofapple cider, which were made from apples ontrees that were fertilized with livestock manure(Besser et al., 1993). In Washington State in Jan-uary 1993, an E. coli outbreak caused severe ill-ness in 144 people, many of whom ateundercooked hamburgers prepared by Jack-in-the-Box fast-food restaurants. A majority of theseriously ill were young children, who had toundergo kidney dialysis for weeks. Althoughmedia reports indicated that the outbreak killedfour children, health officials could only link oneof those deaths to the hamburger from the restau-rant chain (Garrett, 1994).
The second method by which contaminatedfoods can cause illness is through cross-contami-nation in the kitchen or other food-handlingareas. Salmonella bacteria, which can contami-nate eggs, meat, and poultry, can cause severebut rarely fatal symptoms and are transmittedthrough improper food handling (Maurice,1994). For example, when raw chicken or beefwith a Salmonella-contaminated exterior con-taminates a cutting board, countertop, kitchenutensil, or a person’s hands, the bacteria can thencome in contact with other foods, some of whichare consumed raw, such as salad. Symptoms ofSalmonella food poisoning are nausea and vom-

58 | Impacts of Antibiotic-Resistant Bacteria
iting, followed by abdominal cramps and diar-rhea, which last about three or four days,accompanied by fever in about half of the indi-viduals infected. The most common source ofSalmonella is food; only about 10 percent oftransmissions are from person to person, and insome of those instances the ultimate source ofthe infecting organism was food (Cohen andTauxe, 1986). Salmonella outbreaks have beenreported in nursing homes and hospitals, particu-larly pediatric wards and nurseries, and on airlineflights (Villarino et al., 1992; Hatakka andAsplund, 1993; Tauxe et al., 1987).
In addition to causing foodborne illness, manySalmonella are resistant to multiple antibioticsand are capable of transferring that resistance(Snydman and Gorbach, 1982; Lee et al., 1994).In 1983, the Minnesota State Department ofHealth discovered an antibiotic-resistant strain ofSalmonella newport that caused six persons to behospitalized for more than a week. Officialstraced the outbreak to beef that had been fed lowlevels of antibiotics. All the bacterial strainsfound in the infected persons were resistant topenicillin, ampicillin, carbenicillin, and tetracy-cline (Garrett, 1994; Holmberg et al., 1984).
❚ Sanitation and HygieneImproved public sanitation and personal hygienepractices have dramatically reduced the inci-dence of certain infectious diseases, especially indeveloped countries. The U.S. experience withcholera is an example of the success of suchefforts. Between 1830 and 1896, the nation’smajor cities’ populations swelled and producedcrowded slums and fetid water and sewage “sys-tems.” These conditions caused a widespreaddeath toll. In 1832, cholera killed thousands ofNew York City residents and during a three-month epidemic in 1849 claimed 10 percent ofthe population of St. Louis, Missouri. Reformwas soon to follow. New York City officials,outraged by municipal filth, financed the con-struction of the Croton Aqueduct, which broughtclean drinking water to the city for the first time.Eventually, the squalid slums were slowly
upgraded, and subsequent outbreaks of the dis-ease claimed fewer lives (Garrett, 1994). In con-trast, in January 1991, cholera reached epidemiclevels in South America for the first time inalmost a century, demonstrating the health con-sequences of disruptions in sanitation. Vibriocholerae, the bacterium that causes cholera,probably was introduced into the harbor at Lima,Peru, through the dumping of bilge water by aship arriving from the Far East. Once in thewater, the bacteria contaminated the fish andshellfish, which were then consumed by humans.
After causing these initial seafood-relatedcases in humans, the organisms probably werespread by fecal contamination of the water sup-ply, which may have been inadequately chlori-nated (IOM, 1992). In Latin America theepidemic raged well into 1994, and officials atthe World Health Organization see no end insight. As of 1995, Latin American governmentshave spent more than $200 billion for emergencyrepairs of water, sanitation, and sewage systems,according to the Pan American Health Organiza-tion. One of the substrains of the bacterium car-ried genes for resistance to the antibioticsampicillin, trimethoprim, and sulfamethoxazole.
Clean water supplies and their protection fromhuman and other wastes are fundamental publichealth principles in the United States. Wheregood sanitary practices are followed, many dis-eases that were once epidemic are successfullycontrolled. The same may be said for personalhygiene. Hand washing is effective in preventingthe spread of many infectious agents. In addition,safe food-handling practices, including properstorage, cleaning, and preparation, have resultedin fewer cases of bacterial food poisonings. Also,the pasteurization of milk, which was institutedto prevent the transmission of bovine TB tohumans, has been equally effective against otherdiseases such as brucellosis and salmonellosis(IOM, 1992).
The emergence of antibiotic-resistant bacteria,which makes bacterial disease more difficult totreat, increases the importance of sanitation andhygiene to prevent occurrences of these diseases.

Chapter 3 Antibiotic Use and Resistance in the Community | 59
Proper sanitation breaks the route of transmis-sion, thereby bettering public health.
❚ Inadequate Water Treatment and Inspection and Failing InfrastructureAlthough the U.S. Environmental ProtectionAgency recommends that each state evaluate allcomponents of its public water systems, most ofthem do not, according to a 1994 GeneralAccounting Office report. The report found that45 states did not perform the recommended eval-uations, primarily because responsible stateagencies lack sufficient funds for inspection andverification once problems are corrected (GAO,1994).
In Missouri in the winter of 1989, a drug-resis-tant strain of E. coli in the drinking water supplykilled two persons and hospitalized 32. Thestrain, which was resistant to sulfisoxazole, tetra-cycline, and streptomycin, was the first, and stilllargest, waterborne outbreak of E. coli and thefirst due to a multiple-resistant organism. The E.coli outbreak probably resulted from sewagecontamination of the water distribution system.The bacteria survived and spread into the watersystem because there was no hyperchlorinationto kill them (Swerdlow et al., 1993).
About two-thirds of the water systems in theUnited States are not disinfected, and many ofthem are in disrepair. The existence of antibiotic-resistant bacteria increases the risks from watersystems that do not adequately control bacterialcontamination, and outbreaks such as the one inMissouri may become more common. It isentirely possible that other waterborne outbreakshave involved antibiotic-resistant bacteriabecause there is no surveillance system fromwhich to obtain accurate information.
CHANGES IN DISEASE PATTERNS
❚ Sexually Transmitted DiseasesTransmission patterns of sexually transmitteddiseases have changed a great deal in the last 20years. In the 1980s, scientists initially recognizedHIV as a sexually transmitted disease, and inves-
tigators discovered sexually transmitted etiolo-gies for such diverse medical conditions asinfertility, ectopic pregnancy, other adverse out-comes of pregnancy, anogenital cancers, andprotocolitis—an inflammation extending fromthe rectum to the colon.
Also, syphilis re-emerged. Following WorldWar II, the widespread availability of penicillinled to a 95 percent reduction of infectious syphi-lis in the United States. But after 1956, when theinfection rate was four cases per 100,000, theincidence rose sharply to a 40-year peak of 20cases per 100,000 in 1990. During this timeperiod the target population for the diseaseshifted. From about 1960 to 1980, the diseasetargeted homosexual men, but during the lastdecade, the disease has had its greatest impactamong minority heterosexuals as a result of thesex-for-crack cocaine epidemic. However, theincidence among minority heterosexuals involvedin the trade is declining (Morse, 1995). The caus-ative organism for syphilis, Treponema palli-dum, remains completely sensitive to penicillin,and the re-emergence of this disease is not cou-pled with decreased treatment efficiency.
In contrast to syphilis, treatment of gonorrhea,which is caused by the bacterium Neisseria gon-orrhoeae, has been complicated by rapid andrepeated emergence of new types of antimicro-bial resistance. Between 1988 and 1991, CDCdocumented a 50 percent increase in the propor-tion of resistant “gonococcal” isolates, most ofthem being resistant to penicillin or tetracycline(Wasserheit, 1995). As a result, CDC discour-aged the use of the two drugs as first-line thera-pies against the organisms (Schwarcz et al.,1990). The origins of antibiotic-resistant gono-coccus are unknown, but the organism has spreadrapidly. In 1976, CDC found two cases of gonor-rhea caused by organisms that produced anenzyme that destroyed penicillin. By the follow-ing year, health officials identified a strain calledpenicillinase-producing N. gonorrhoeae (PPNG)in 17 countries. In the United States most of thecases were in New York City, with three cases in1977 involving resistance to penicillin, ampicil-lin, and spectinomycin. By 1981, treatment of

60 | Impacts of Antibiotic-Resistant Bacteria
gonorrhea had become far more complicatedbecause of resistance to antibiotics (Garrett,1994). The major impact of antibiotic resistanceon gonorrhea is the cost of treatment. A non-resistant case of gonorrhea costs less than a dol-lar, but a resistant case may increase treatmentanywhere between 12 and 15 times that amount(Morse, 1995).
❚ TuberculosisOnce thought to be conquered, tuberculosis(TB)an airborne disease that is spread throughthe air when a person with active infectioncoughs, sneezes, or speaks, expelling contami-nated droplets from the lungshas re-emergedas a public health threat, with drug-resistantstrains greatly complicating treatment. In 1947,when antibiotic therapy for TB was still consid-ered a novel treatment and disease preventiontechnique, nearly 135,000 cases of the diseasewere reported in the United States. By 1985 theuses of streptomycin, rifampin, isoniazid, andother antibiotics, coupled with an aggressivepublic health effort to identify and treat TBcases, had brought the nation’s caseload down toa little more than 22,000. By 1992, however,there were nearly 30,000 newly reported cases(OTA, 1993).
Well before the actual numbers of TB casesbegan to swell, the demographics of the diseaseshifted. Between 1961 and 1969 more than 80percent of all active TB cases in the UnitedStates were among people over 62 years of age,and the majority of them were elderly individualsof European descent who had carried the Myco-bacterium tuberculosis microbes in their bodiesfor decades, only falling ill as their agingimmune systems failed to keep the bacteria incheck. Most of these people were readily treatedwithout hospitalization through basic long-termantibiotic therapy. Between 1975 and 1984 thenumbers of active TB cases reported among theelderly declined sharply. By 1984, only 29 per-cent of TB patients were over 62 years of age. Inthe non-white population, less than one out ofevery five active TB cases that year involved
someone over 62, and fully 20 percent werebetween the ages of 25 and 34. During thatdecade, white male cases dropped 41 percent,and white female cases fell 39 percent. While TBwas declining across the board, its downturnamong non-whites was slower; only 25 percentfor males and 26 percent for females.
The warning signs were clear. Between 1980and 1986 five different surveys documented arelationship between rising homelessness and thesurge of TB in young adult populations, and by1984 new resistant strains of drug-resistant TBwere spreading among the urban indigent. By1986, nearly half of all active TB cases reportedin the United States were among non-whites,most of them African Americans. More specifi-cally, TB now occurs disproportionately amongindividuals who lack stable housing, abuse alco-hol or intravenous drugs, become incarcerated,are employed as migrant farm workers, and who,for various reasons, are exposed to people whodo not adhere to treatment guidelines (OTA,1993).
Geographically, the disease shifted from ruralareas to scattered urban areas such as New YorkCity and Miami. CDC noted the shift in 1986,which coincided with the first upward trend inTB cases reported in the United States since1953. Agency officials believe that the impairedimmune systems associated with HIV infectionmay be largely responsible for the increase in TBin New York City and Florida. However, otherfactors also can contribute to the spread of TB. Arecent case in Minnesota prompted health offi-cials there to theorize that heavy alcohol con-sumption may play a role in the weakening of theimmune system, permitting initial infections toprogress to active TB (Boodman, 1995).
In the mid-1980s, budget cuts in New YorkCity forced a three-fold reduction in the numberof TB clinics and disbanded public health clinics.During that same period, federal and state offi-cials slashed TB control and surveillance bud-gets. For example, budget cuts eliminated NewYork City’s surveillance system for multiple-drug resistant TB (MDR-TB) in 1986. Inade-quate treatment and the lack of surveillance led

Chapter 3 Antibiotic Use and Resistance in the Community | 61
to the increase in the number of MDR-TB cases.Frieden et al. (1995) analyzed TB surveillancedata and discovered that drug resistance amongpatients who had never been treated increasedfrom 10 percent in 1983 to 23 percent in 1991.Nearly 25 percent of patients with TB in NewYork City had multiple drug-resistant strains,and the proportion of new patients with MDR-TB had more than doubled from 1984 to 1991(Freiden et al., 1995). From 1985 to 1992, publichealth officials documented outbreaks of MDR-TB in more than a dozen hospitals, homelessshelters, prisons, and other areas in the UnitedStates and Puerto Rico. Those cases are illus-trated in table 3-1 (Garrett, 1994).
By the time politicians realized the scope ofthis re-emergence, TB, and especially MDR-TB,was draining already tight budgets and hadbecome a public health crisis. When all the costsof the 1989-1994 MDR-TB epidemic weretotaled, health officials had spent more than $1billion to tackle the resistant bacteria (Garrett,1994). Only after this crisis were federal dollarsallocated and a modified surveillance system forMDR-TB reinstated (Berkelman et al., 1994). Asa result of the revised surveillance system, alongwith directly observed therapy (in which health-care workers observe patients as they take eachdose of medicine), New York City reported a 19percent decline in all TB cases and a 44 percentdecline in the MDR-TB cases from 1991-1992 to1993-1994 (Freiden et al., 1995). Despite therecent successes, New York City has not con-trolled TB. The case rate there is still more thanfour times the national rate, and there are morepatients in the city with MDR-TB than in the restof the United States combined. However, NewYork City’s experience shows that TB can becurtailed despite the prevalence of drug-resistantstrains and immunosuppressed populations.
SURVEILLANCE OF ANTIBIOTIC-RESISTANT BACTERIADiseases are transmitted in the community, andsome of those diseases are caused by antibiotic-resistant bacteria. How commonly that occurs is
unknown. Almost all of the information aboutantibiotic-resistant diseases in the communitycomes from episodic reports, and it is unknownhow many go unreported or unnoticed. Someexceptions are TB, syphilis, and gonorrhea, all ofwhich are notifiable diseases, which means thatCDC obtains and combines records from thestates to provide national data on those infec-tions. Public health officials at state healthdepartments, CDC, and the Council of State andTerritorial Epidemiologists recommend annualadditions and deletions to the national notifiabledisease list, which is published in CDC’s Mor-bidity and Mortality Weekly Report. Generally,diseases are added to the list as new pathogensemerge and are deleted as their incidencedeclines. However, health officials in each stateultimately decide which diseases they will reporton the nationally notifiable list. Table 3-2 showsa listing of nationally reportable diseases. Of the50 diseases notifiable to CDC, 31 are bacterialand are therefore subject to antibiotic resistance.
Drug-resistant S. pneumoniae (DRSP) wasadded to the list of reportable diseases in 1995 asa result of a CDC-convened working group thatidentified methods for prevention and control ofthe bacterium. The working group, consisting ofpublic health practitioners, clinical laboratoryprofessionals, health-care providers, and repre-sentatives of professional societies, establishedDRSP, which is associated with many illnesses,as a nationally reportable condition. Currently,only a few states have made DRSP a reportablecondition on a national level. If more statesreported DRSP nationally, the system not onlywould provide better surveillance informationbut could serve as a model for surveillance ofother antibiotic-resistant bacteria.
More surveillance information about the prev-alence of drug-resistant microbes such as S.pneumoniae, for example, would enable physi-cians to prescribe antibiotics more effectively,thereby possibly reducing resistance, the addedcosts associated with treating an antibiotic-resis-tant disease, and in some cases death. Had thesurveillance program for MDR-TB in New YorkCity not been eliminated, perhaps more money
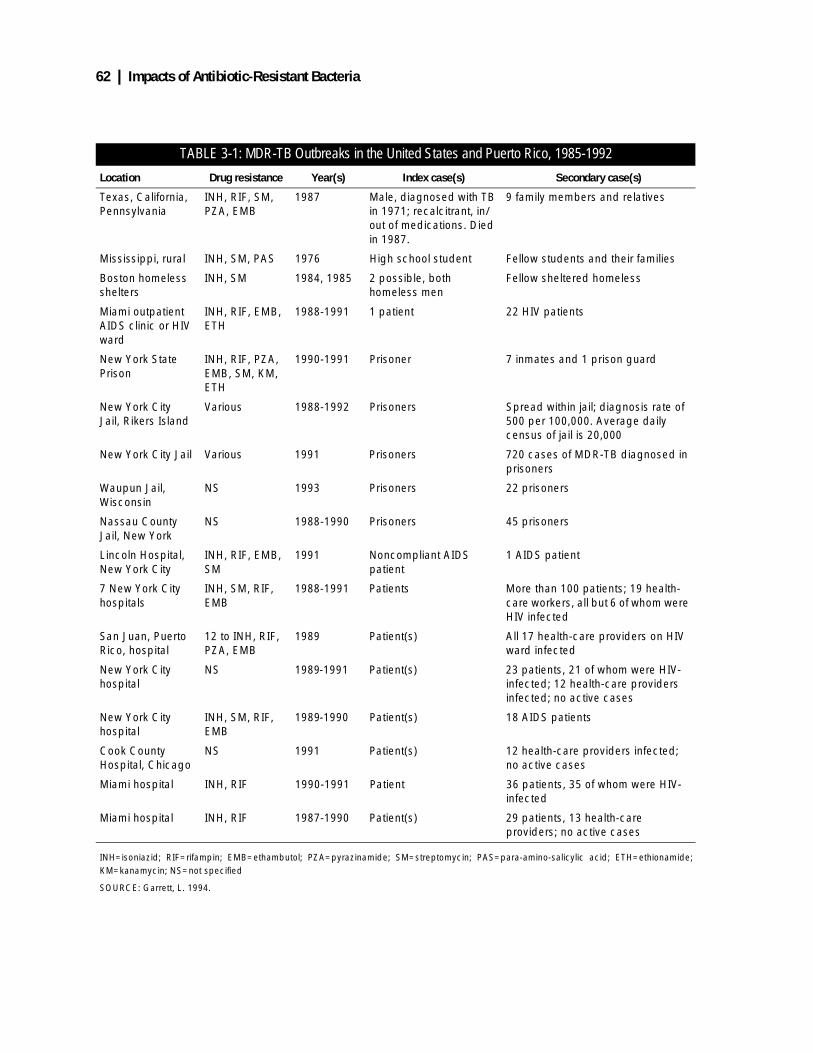
62 | Impacts of Antibiotic-Resistant Bacteria
TABLE 3-1: MDR-TB Outbreaks in the United States and Puerto Rico, 1985-1992
Location Drug resistance Year(s) Index case(s) Secondary case(s)
Texas, California, Pennsylvania
INH, RIF, SM, PZA, EMB
1987 Male, diagnosed with TB in 1971; recalcitrant, in/out of medications. Died in 1987.
9 family members and relatives
Mississippi, rural INH, SM, PAS 1976 High school student Fellow students and their families
Boston homeless shelters
INH, SM 1984, 1985 2 possible, both homeless men
Fellow sheltered homeless
Miami outpatient AIDS clinic or HIV ward
INH, RIF, EMB, ETH
1988-1991 1 patient 22 HIV patients
New York State Prison
INH, RIF, PZA, EMB, SM, KM, ETH
1990-1991 Prisoner 7 inmates and 1 prison guard
New York City Jail, Rikers Island
Various 1988-1992 Prisoners Spread within jail; diagnosis rate of 500 per 100,000. Average daily census of jail is 20,000
New York City Jail Various 1991 Prisoners 720 cases of MDR-TB diagnosed in prisoners
Waupun Jail, Wisconsin
NS 1993 Prisoners 22 prisoners
Nassau County Jail, New York
NS 1988-1990 Prisoners 45 prisoners
Lincoln Hospital, New York City
INH, RIF, EMB, SM
1991 Noncompliant AIDS patient
1 AIDS patient
7 New York City hospitals
INH, SM, RIF, EMB
1988-1991 Patients More than 100 patients; 19 health-care workers, all but 6 of whom were HIV infected
San Juan, Puerto Rico, hospital
12 to INH, RIF, PZA, EMB
1989 Patient(s) All 17 health-care providers on HIV ward infected
New York City hospital
NS 1989-1991 Patient(s) 23 patients, 21 of whom were HIV- infected; 12 health-care providers infected; no active cases
New York City hospital
INH, SM, RIF, EMB
1989-1990 Patient(s) 18 AIDS patients
Cook County Hospital, Chicago
NS 1991 Patient(s) 12 health-care providers infected; no active cases
Miami hospital INH, RIF 1990-1991 Patient 36 patients, 35 of whom were HIV- infected
Miami hospital INH, RIF 1987-1990 Patient(s) 29 patients, 13 health-care providers; no active cases
INH=isoniazid; RIF=rifampin; EMB=ethambutol; PZA=pyrazinamide; SM=streptomycin; PAS=para-amino-salicylic acid; ETH=ethionamide;KM=kanamycin; NS=not specified
SOURCE: Garrett, L. 1994.

Chapter 3 Antibiotic Use and Resistance in the Community | 63
could have been saved in treatment, and moreimportantly, more deaths could have been pre-vented. However, since its reinstatement, theNew York City TB surveillance system, alongwith directly observed therapy, as mentionedpreviously, has resulted in dramatic decreases inthe number of TB and MDR-TB cases. Experi-ences in Washington State and Nevada in 1993also demonstrate the usefulness of surveillancesystems. Washington requires that hospitalsreport cases of illness caused by E. coli O157:H7to the state health department. After health offi-cials learned of a few cases, they determined thatthe bacteria were coming from fast-food ham-burgers and recalled more than 250,000 ham-burgers. This action ended the outbreak. Cases ofE. coli infection derived from the same sourcehad occurred earlier in Nevada, but without asurveillance system officials in that state wereunaware of them until after the Washingtonhealth officials had detected their cases.
Nevada’s outbreak caused 58 cases of bloodydiarrhea and acute kidney failure. None had beenreported to the health department because physi-cians and laboratories were not testing for thatparticular pathogen.
CONCLUSIONSAntibiotics have produced a great paradox. Aftertheir introduction into medical practice nearly 50years ago, the drugs controlled many life-threat-ening diseases, reduced death and illness, andincreased the life expectancy of Americans.Since then, the use of antibiotics, including inap-propriate uses that have little benefit to thepatients, has fostered antibiotic resistance andcaused many antibiotics to lose their effective-ness against some bacterial diseases. As a result,some illnesses that were once easily treatablenow pose problems for patients and physicians.One solution is the development of new drugsagainst antibiotic-resistant strains. However,
TABLE 3-2: Infectious Diseases Classified as Notifiable at the National Level (United States, 1994)
AIDSAmebiasis*AnthraxAseptic meningitisBotulismBrucellosisChancroid*CholeraCongenital rubella syndromeDiphtheriaDRSP**EncephalitisEscherichia coli O157:H7*GonorrheaGranuloma inguinaleHaemophilus influenzae
Hepatitis AHepatitis BHepatitis, non-A, non-BHepatitis, unspecifiedLegionellosisLeprosy (Hansen disease)LeptospirosisLyme diseaseLymphogranuloma venereum*MalariaMeaslesMeningococcal infectionMumpsPertussisPlaguePoliomyelitisPsittacosis
Rabies, animalRabies, humanRheumatic fever*Rocky Mountain Spotted fever (Typhus fever, tickborne)RubellaSalmonellosis*ShigellosisSyphilisSyphilis, congenitalTetanusToxic shock syndromeTrichinosisTBTularemiaTyphoid fever
Varicella (chicken pox) +*Yellow fever*
* Reports of these diseases are not printed weekly in Table I or Table II of the Morbidity and Mortality Weekly Report.** Drug-resistant Streptococcus pneumoniae was added in 1995.+ Although varicella is not officially a nationally notifiable disease, the Council of State and Territorial Epidemiologists encourages reporting casesof varicella to CDC.
SOURCE: Centers for Disease Control and Prevention. 1994. Morbidity and Mortality Weekly Report 43 (43):801.
NOTE: Boldface indicates bacterial diseases.

64 | Impacts of Antibiotic-Resistant Bacteria
strains resistant to the new antibiotics are likelyto develop eventually. Therefore, a more long-term solution includes the more prudent use ofantibiotics that are currently available.
Outbreaks of illnesses and diseases caused byantibiotic-resistant bacteria are increasing. Howcommon these outbreaks are is unknown becauseof inadequate surveillance. Almost all of theinformation about antibiotic-resistant illnessesand diseases is episodic, and it is unknown howmany go unreported or unnoticed. Surveillance isthe essential element for health officials to iden-tify, isolate, and control these outbreaks. Theimportance of a surveillance system was demon-strated in the E. coli outbreak in WashingtonState and Nevada in 1993. Health officials inWashington traced the outbreak’s origin toundercooked hamburger from a fast-food chain.The finding led to the recall of more than250,000 hamburgers and the end of the outbreak.In contrast, an outbreak from the same sourcehad occurred earlier in Nevada and caused 58cases of bloody diarrhea and acute kidney fail-ure. Because of inadequate surveillance, theNevada health officials did not identify theircases until after the Washington State casesoccurred. Although these cases were not antibi-otic-resistant, they serve as an example of how
surveillance could track cases that are. In thoseinstances, time is essential to prevent the spreadof antibiotic-resistant illnesses that are generallyharder to treat.
Although all persons are susceptible to ill-nesses related to antibiotic-resistant bacteria,some are more than others. The poor, peoplewithout adequate health care, the incarcerated,the homeless, military personnel, children indaycare facilities, the elderly, and the immuno-suppressed are more susceptible to these ill-nesses than the general population. However,because most of the general public comes in con-tact with members of these vulnerable popula-tions daily, the general public is at risk becausethe diseases or illnesses can spread from personto person. Because of the potential of widespreadillnesses caused by resistant bacteria, better useof current antibiotics and more adequate surveil-lance systems would help control antibiotic resis-tance and reduce its effects on the generalpopulation.
Therefore, it is crucial that the scientific andmedical communities, the pharmaceutical indus-try, and the general public cooperate to find solu-tions that will slow the pace of antibioticresistance and lessen the impact of illness onpublic health.
Chapter 3 Antibiotic Use and Resistance in the Community | 65
REFERENCESAmerican Medical Association, Council on Sci-
entific Affairs. 1993. Food Safety Archivesof Family Medicine 2:210-214.
Anderson, G.M. Feb. 10, 1990. Sick behind bars:health care in prison. America 134:124-126.
Ballow, C.H., and Schentag, J.J. 1992. Trends inantibiotic utilization and bacterial resistance(Report of the National NosocomialResistance Surveillance Group). DiagnosticMicrobiology and Infectious Diseases 15:37S-42S.
Barry, M., Wall, C., Shirley, L., et al., 1986. TBscreening in Boston’s homeless shelters.Public Health Reports 101(5):487-494.
Bellin, E.Y., Fletcher, D.D., and Safyer, S.M.1993. Association of tuberculosis infectionwith increased time in or admission to theNew York City jail system. Journal of theAmerican Medical Association 269(17):2228-2231.
Berkelman, R.L., Bryan, R.T., Osterholm, M.T.,et al., 1994. Infectious disease surveillance:A crumbling foundation. Science 264:368-370.
Besser, R.E., Lett, S.M., Weber, J.T., et al., 1993.An outbreak of diarrhea and hemolyticuremic syndrome from Escherichia coliO157:H7 in fresh-pressed apple cider. Jour-nal of the American Medical Association269(17):2217-2220.
Boodman, S.G. August 15, 1995. 45 Infectedwith TB by homeless man. Washington Post,Health section, p.11.
Breiman, R.F., Butler, J.C., Tenover, F.C., et al.,1994. Emergence of drug-resistant pneumo-coccal infections in the United States. Jour-nal of the American Medical Association271(23):1831-1835.
Cassell, G. June 22, 1995. Department of Micro-biology, University of Alabama at Birming-ham. Personal communication.
Chisolm, S.A. 1988. Infection control in correc-tional facilities: A new challenge. AmericanJournal of Infection Control 16:107-113.
Cohen, D., Scribner, R., Clark, J., Cory, D. 1992.The potential role of custody facilities incontrolling sexually transmitted diseases.American Journal of Public Health 82(4):552-556.
Cohen, M.L., and R.V. Tauxe. 1986. Drug-resis-tant salmonella in the United States: An epi-demiologic perspective. Science 234:964-969.
DiNubile, M.J. 1990. Antibiotics: The antipyret-ics of choice. American Journal of Medicine89:787-788.
Fornasini, M., Reves, R., Murray, B., et al.,1992. Trimethoprim-resistant Escherichiacoli in households of children attending daycare centers. Journal of Infectious Diseases166(2):326-330.
Frieden, T.R., Fujiwara, P.I., Washko, R.M.,Hamburg, M.A. 1995. Tuberculosis in NewYork City—turning the tide. The NewEngland Journal of Medicine 333(4):229-233.
Frieden, T.R., and R.J. Mangi. 1990. Inappropri-ate use of oral ciprofloxacin. Journal of theAmerican Medical Association 264(11):1438-1440.
Garrett, L. 1994. The Coming Plague: NewlyEmerging Diseases in a World Out of Bal-ance (New York, NY: Farrar, Straus, andGiroux).
Gray, G.C., Mitchell, B.S., Tueller, J.E., et al.,1994. Pneumonia hospitalizations in theU.S. Navy and Marine Corps: Rates and riskfactors for 6,522 admissions, 1981-1991.American Journal of Epidemiology 139(8):793-802.
Gross, T.P., and M.L. Rosenberg. 1987. Sheltersfor battered women and their children: anunder-recognized source of communicabledisease transmission. American Journal ofPublic Health 77(9):1198-1201.
Haglund, L.A., Istre, G.R., Pickett, D.A., et al.,1993. Invasive pneumococcal disease incentral Oklahoma: Emergence of high-levelpenicillin resistance and multiple antibioticresistance. Journal of Infectious Diseases168(6):1532-1536.
66 | Impacts of Antibiotic-Resistant Bacteria
Hammond, A. (ed.) 1994. The 1994 InformationPlease Environmental Almanac (New York,NY: Houghton Mifflin Co.).
Hatakka, M., and K. Asplund. 1993. The occur-rence of salmonella in airline meals. ActaVeterinaria Scandinavica 34(4):391-396.
Hoge, C.W., Reichler, M.R., Dominguez, E.A.,et al., 1994. An epidemic of pneumococcaldisease in an overcrowded, inadequatelyventilated jail. The New England Journal ofMedicine 331(10):643-648.
Holmberg, S.D., Osterholm, M.T., Senger, K.A.,Cohen, M.L. 1984. Drug-resistant salmo-nella from animals fed antimicrobials. TheNew England Journal of Medicine 311(10):617-622.
Institute of Medicine. 1992. Emerging In-fections: Microbial Threats to Health in theUnited States, J. Lederberg, R.E. Shope, andS.C.J. Oaks (eds.) (Washington, DC:National Academy Press).
Jernigan, D.B., Cetron, M.S., Breiman, R.F., etal., April 18, 1995. Centers for Disease Con-trol and Prevention, Atlanta, GA. A nationalstrategy for the surveillance, appliedresearch, prevention, and control of drug-resistant Streptococcus pneumoniae (unpub-lished document).
Kim, J.H., and H.A. Gallis. 1989. Observationson spiraling empiricism: Its causes, allure,and perils, with particular reference to anti-biotic therapy. American Journal of Medi-cine 87:201-206.
Klein, J.O. 1994. Otitis externa, otitis media,mastoiditis. In G.L. Mandell, J.E. Bennett,and R. Dolin (eds.) Mandell, Douglas andBennett’s Principles and Practice of Infec-tious Diseases (New York: Churchill Liv-ingstone).
Klugman, K.P. 1990. Pneumococcal resistance toantibiotics. Clinical Microbiology Reviews.3:171-196.
Kunin, C.M., Tupasi, C., Craig, W.A. 1973. Useof antibiotics: A brief exposition of the prob-lem and some tentative solutions. Annals ofInternal Medicine 79:555-560.
Kunin, C.M. 1995. Relationships between antibi-otic use and the emergence and persistanceof antibiotic resistance (unpublished paper).
Lee, L.A., Puhr, N.D., Maloney, E.K., et al.,1994. Increase in antimicrobial-resistant sal-monella infections in the United States,1989-1990. The Journal of Infectious Dis-eases 170:128-134.
Levine, D.P., Fromm, B.S., and Reddy, B.R.1991. Slow response to vancomycin or van-comycin plus rifampin in methicillin-resis-tant Staphylococcus aureus endocarditis.Annals of Internal Medicine, 115:674-680.
Levine, M. and O. Levine. 1995. Changes inhuman ecology and behavior in relation tothe emergence of diarrheal diseases, includ-ing cholera. In B. Roizman (ed.) InfectiousDiseases in an Age of Change (Washington,DC: National Academy Press).
Levy, S.B. 1992. The antibiotic paradox: Howmiracle drugs are destroying the miracle(New York: Plenum Press).
Madhavan, T. 1994. Infections in the elderly:Current concepts in management. Compre-hensive Therapy 20(8):465-470.
Maurice, J. 1994. The rise and rise of food poi-soning. New Scientist 144(1956):28-33.
McCaig, L.F. and J.M. Hughes. 1995. Trends inantimicrobial drug prescribing amongoffice-based physicians in the United States.Journal of the American Medical Associa-tion 273(3):214-219.
McGowan, J.E.J. 1983. Antimicrobial resistancein hospital organisms and its relation to anti-biotic use. Reviews of Infectious Diseases5(6):1033-1048.
Moller, J.K. 1989. Antimicrobial usage andmicrobial resistance in a university hospitalduring a seven-year period. Journal of Anti-microbial Chemotherapy 24:983-992.
Morris, J. and C. McAllister. 1992. Homelessindividuals and drug-resistant tuberculosis inSouth Texas. Chest 102(3):802-804.
Morse, S. August 15, 1995. Centers for DiseaseControl and Prevention, National Center forInfectious Diseases, Atlanta, GA. personalcommunication.
Chapter 3 Antibiotic Use and Resistance in the Community | 67
Mouton, R.P., Herman, J., Simoons-Smit, A.M.,et al., 1990. Correlations between consump-tion of antibiotics and methicillin resistancein coagulase negative staphylococci. Journalof Antimicrobial Chemotherapy 26:573-583.
Navarro, M. May 5, 1993. Report links timespent in jail to risk of tuberculosis. New YorkTimes, p. B5.
Pablos-Mendes, A., Raviglione, M., Battan, R.,et al., 1990. Drug-resistant TB among thehomeless in N.Y.C. N.Y. State Journal ofMedicine 90(7):351-355.
Paul, E.A., Lebowitz, S.M., Moore, R.E., et al.,1993. Nemesis revisited: Tuberculosis infec-tion in a New York City men’s shelter.American Journal of Public Health 83(12):1743-1745.
Rauch, A., O’Ryan, M., Van, R., Pickering, L.1990. Invasive disease due to multiply resis-tant Streptococcus pneumoniae in a Hous-ton, Texas, day care center. AmericanJournal of Diseases in Children 144(8):923-927.
Riley, L.W., Remis, R.S., Helgerson, S.D., et al.,1983. Hemorrhagic colitis associated with arare Escherichia coli serotype. New EnglandJournal of Medicine 308:681-685.
Ringertz, S. and G. Kronvall. 1987. Increaseduse of erythromycin causes resistancein Haemophilus influenzae. ScandinavianJournal of Infectious Diseases 19:247-256.
Schappert, S.M. Sept. 1992. Office visits for oti-tis media: United States, 1975-90. AdvanceData From Vital and Health Statistics of theNational Center for Health Statistics, No.214 (PHS) 88-1250 (Hyattsville, MD).
Schlessinger, D. 1993. Biological basis for anti-bacterial action. In M. Schaechter, G. Med-off, and B.I. Eisenstein (eds.) Mechanisms ofMicrobial Disease (Baltimore, MD: Will-iams and Wilkins).
Schwarcz, S.K., Zenilman, J.M., Schnell, D., etal., 1990. National surveillance of antimicro-bial resistance in Neisseria gonorrhoeae.Journal of the American Medical Associa-tion 264(11):1413-1417.
Skolnick, A.A. 1992. Some experts suggest theNation’s ‘war on drugs’ is helping. Journalof the American Medical Association 268(22):3177-3178.
Snydman, D. and S. Gorbach. 1982. Salmonello-sis: Nontyphoidal. In A. Evans and H. Feld-man (eds.) Bacterial Infections of Humans(New York, NY: Plenum Medical BookCo.).
Sogaard, H., Zimmerman-Nielsen, C., andSibioni, K. 1974. Antibiotic resistant gram-negative bacilli in a urological ward. Journalof Infectious Diseases 130:646.
Sterne, G.G., Hinman, A., and Schmid, S. 1986.Potential health benefits of child day careattendance. Reviews of Infectious Diseases8(4):660-662.
Swerdlow, D.L., Woodruff, B.A., Brady, R.C., etal., 1993. A waterborne outbreak in Missouriof Escherichia coli O157:H7 associated withbloody diarrhea and death. Annals of Inter-nal Medicine 117(10):812-819.
Tan, T., Mason, Jr., E., and Kaplan, S. 1993.Penicillin-resistant systemic pneumococcalinfections in children: A retrospective case-control study. Pediatrics 92(6):761-767.
Tauxe, R.V., Tormey, M.P., Mascola, L., et al.,1987. Salmonellosis outbreak on transatlan-tic flights; foodborne illness on aircraft:1947-1984. American Journal of Epidemiol-ogy 125(1):150-157.
Thacker, S.B., Addiss, D.G., Goodman, R.A.,Holloway, B. 1992. Infectious diseases andinjuries in child day care. Journal of theAmerican Medical Association 268(13):1720-1726.
U.S. Congress, General Accounting Office, 1994.Drinking water: Stronger efforts essentialfor small communities to comply with stan-dards. RCED-94-40 (Washington, DC: U.S.Government Printing Office).
U.S. Congress, Office of Technology Assess-ment. July 1987. Life-Sustaining Tech-nologies and the Elderly. OTA-BA-306(Washington, DC: U.S. Government Print-ing Office).

68 | Impacts of Antibiotic-Resistant Bacteria
U.S. Congress, Office of Technology Assess-ment. Sept. 1992. Does Health InsuranceMake a Difference? OTA-BP-H-89 (Wash-ington, DC: U.S. Government PrintingOffice).
U.S. Congress, Office of Technology Assess-ment. Sept. 1993. The Continuing Challengeof Tuberculosis. OTA-H-574 (Washington,DC: U.S. Government Printing Office).
U.S. Department of Commerce, U.S. Bureau ofCensus. 1994. Statistical Abstract of theUnited States (Washington, DC: U.S. Gov-ernment Printing Office).
Villarino, M., Vugia, D., Bean, N., et al., 1992.Foodborne disease prevention in health carefacilities. In J. Bennett and P. Brachman(eds.) Hospital Infections (Boston, MA: Lit-tle, Brown and Company).
Wasserheit, J. 1995. Effect of human ecologyand behavior on sexually transmitted dis-eases, including HIV infection. In B. Roiz-man (ed.) Infectious Diseases in an Age ofChange (Washington, DC: National Acad-emy Press).
Weissman, J.S., Stern, R., Fielding, S.L., Epstein,A.M. 1991. Delayed access to health care:Risk factors, reasons, and consequences.Annals of Internal Medicine 114 (4):325-331.
Whitnack, E. 1993. Streptococci. In M. Schaechter,G. Medoff, and B. Eisenstein (eds.) Mecha-nisms of Microbial Disease (Baltimore, MD:Williams and Wilkins).
Williams, R.D. Dec. 1994. Protecting little pitch-ers. FDA Consumer 10-14.
| 69
4
AntibioticUse in
Hospitals
t any given time, 25 to 35 percent ofhospitalized patients are receiving sys-temic antibiotics (Eickhoff, 1991) totreat active infections or to prevent
potential infections. The heavy use of antibioticsin the hospital exerts enormous selective pres-sure for the emergence and spread of antibiotic-resistant bacteria. Consequently, many of the twomillion bacterial infections acquired in the hospi-tal are antibiotic-resistant, and a few are resistantto every antibiotic currently approved for use.Some hospitals have reduced infections fromantibiotic-resistant bacteria through a combina-tion of infection control procedures that preventthe spread of the resistant organisms and throughmonitoring and control of antibiotic use.
This chapter 1) describes antibiotic use in hos-pitals and its contribution to the rise of antibiotic-resistant nosocomial infections, 2) discusses cur-rent efforts to control antibiotic-resistant infec-tions, 3) explores medical and financial factorsthat make such efforts difficult to implement inhospitals, and 4) discusses some possible solu-tions.
INFECTIONS ACQUIRED IN THE HOSPITALThe Centers for Disease Control and Prevention(CDC) estimates that 1 out of 20 patients(2 million per year) acquire infections in the hos-pital (Haley et al., 1985).1 Nosocomial infectionscost $4.5 billion a year (1992 dollars) in terms ofextra treatment and days of hospitalization,directly cause 19,000 deaths, and contribute to58,000 deaths annually (table 4-1). The 19,000deaths per year directly caused by nosocomialinfections makes them the 11th leading cause ofdeath in the U.S. population (Martone et al.,1992).
Recent data from the National NosocomialInfections Surveillance (NNIS) system show thatnosocomial infections are increasing (figure 4-1).The number of blood stream infections increased279 percent in small non-teaching hospitals, 196percent in large non-teaching hospitals, by 124percent in small teaching hospitals, and by 70percent in large teaching hospitals during the1980s. It might be discouraging that the rates ofblood stream infections have been increasing
1 Based on data from CDC’s 1976 Study on the Efficacy of Nosocomial Infection Control (SENIC). This number is still widely quoted inrecent reports (see, for example, IOM, 1992).
A
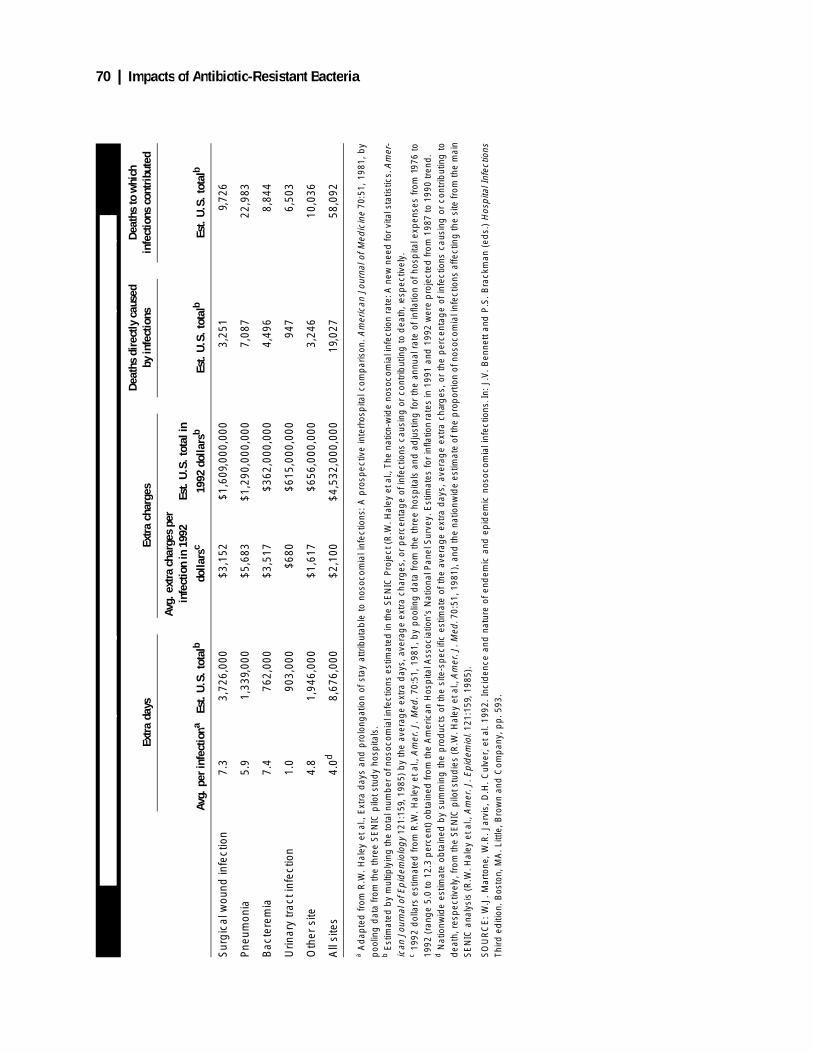
70 | Impacts of Antibiotic-Resistant Bacteria
TABL
E 4-
1: E
stim
ated
Ext
ra D
ays,
Ext
ra C
harg
es, a
nd D
eath
s At
tribu
tabl
e to
Nos
ocom
ial I
nfec
tions
Ann
ually
in U
.S. H
ospi
tals
Extra
day
sEx
tra c
harg
esDe
aths
dir
ectly
cau
sed
by in
fect
ions
Deat
hs to
whi
ch
infe
ctio
ns c
ontr
ibut
ed
Avg.
per
infe
ctio
naEs
t. U
.S. t
otal
b
Avg.
ext
ra c
harg
es p
er
infe
ctio
n in
199
2 do
llars
cEs
t. U
.S. t
otal
in
1992
dol
lars
bEs
t. U
.S. t
otal
bEs
t. U
.S. t
otal
b
Sur
gic
al w
ound
infe
ctio
n7.
33,
726,
000
$3,1
52$1
,609
,000
,000
3,25
19,
726
Pne
umon
ia5.
91,
339,
000
$5,6
83$1
,290
,000
,000
7,08
722
,983
Bac
tere
mia
7.4
762,
000
$3,5
17$3
62,0
00,0
004,
496
8,84
4
Urin
ary
trac
t inf
ectio
n1.
090
3,00
0$6
80$6
15,0
00,0
0094
76,
503
Oth
er s
ite4.
81,
946,
000
$1,6
17$6
56,0
00,0
003,
246
10,0
36
All
site
s4.
0d8,
676,
000
$2,1
00$4
,532
,000
,000
19,0
2758
,092
a Ad
apte
d fr
om R
.W. H
aley
et
al.,
Ext
ra d
ays
and
pro
long
atio
n of
sta
y at
trib
utab
le t
o no
soco
mia
l inf
ectio
ns:
A p
rosp
ectiv
e in
terh
osp
ital c
omp
aris
on. A
mer
ican
Jou
rnal
of M
edic
ine
70:5
1, 1
981,
by
poo
ling
dat
a fr
om th
e th
ree
SE
NIC
pilo
t stu
dy
hosp
itals
.b E
stim
ated
by
mul
tiply
ing
the
tota
l num
ber
of n
osoc
omia
l inf
ectio
ns e
stim
ated
in th
e S
EN
IC P
roje
ct (R
.W. H
aley
et a
l., T
he n
ation
-wid
e no
soco
mia
l inf
ectio
n ra
te: A
new
nee
d fo
r vita
l sta
tistic
s. A
mer
-ic
an J
ourn
al o
f Ep
idem
iolo
gy
121:
159,
198
5) b
y th
e av
erag
e ex
tra
day
s, a
vera
ge
extr
a ch
arg
es, o
r p
erce
ntag
e of
infe
ctio
ns c
ausi
ng o
r co
ntrib
utin
g to
dea
th, r
esp
ectiv
ely.
c 19
92 d
olla
rs e
stim
ated
from
R.W
. Hal
ey e
t al.,
Am
er. J
. Med
. 70:
51,
1981
, by
poo
ling
dat
a fr
om th
e th
ree
hosp
itals
and
ad
just
ing
for
the
annu
al r
ate
of in
flatio
n of
hos
pita
l exp
ense
s fr
om 1
976
to19
92 (
rang
e 5.
0 to
12.
3p
erce
nt)
obta
ined
from
the
Am
eric
an H
osp
ital A
ssoc
iatio
n’s
Nat
iona
l Pan
el S
urve
y. E
stim
ates
for
infla
tion
rate
s in
199
1 an
d 1
992
wer
e p
roje
cted
from
198
7 to
199
0 tr
end
.d N
atio
nwid
e es
timat
e ob
tain
ed b
y su
mm
ing
the
pro
duc
ts o
f the
site
-sp
ecifi
c es
timat
e of
the
aver
age
extr
a d
ays,
ave
rag
e ex
tra
char
ges
, or
the
per
cent
age
of in
fect
ions
cau
sing
or
cont
ribut
ing
tod
eath
, res
pec
tivel
y, fr
om th
e S
EN
IC p
ilot s
tud
ies
(R.W
. Hal
ey e
t al.,
Am
er. J
. Med
. 70:
51, 1
981)
, and
the
natio
nwid
e es
timat
e of
the
pro
por
tion
of n
osoc
omia
l inf
ectio
ns a
ffect
ing
the
site
from
the
mai
nS
EN
IC a
naly
sis
(R.W
. Hal
ey e
t al.,
Am
er. J
. Ep
idem
iol.
121:
159,
198
5).
SO
UR
CE
: W
.J. M
arto
ne,
W.R
. Ja
rvis
, D
.H.
Cul
ver,
et
al. 1
992.
Inc
iden
ce a
nd n
atur
e of
end
emic
and
ep
idem
ic n
osoc
omia
l inf
ectio
ns. I
n: J
.V.
Ben
nett
and
P.S
. B
rack
man
(ed
s.)
Hos
pita
l Inf
ectio
nsTh
ird e
diti
on. B
osto
n, M
A. L
ittle
, Bro
wn
and
Com
pan
y, p
p.5
93.
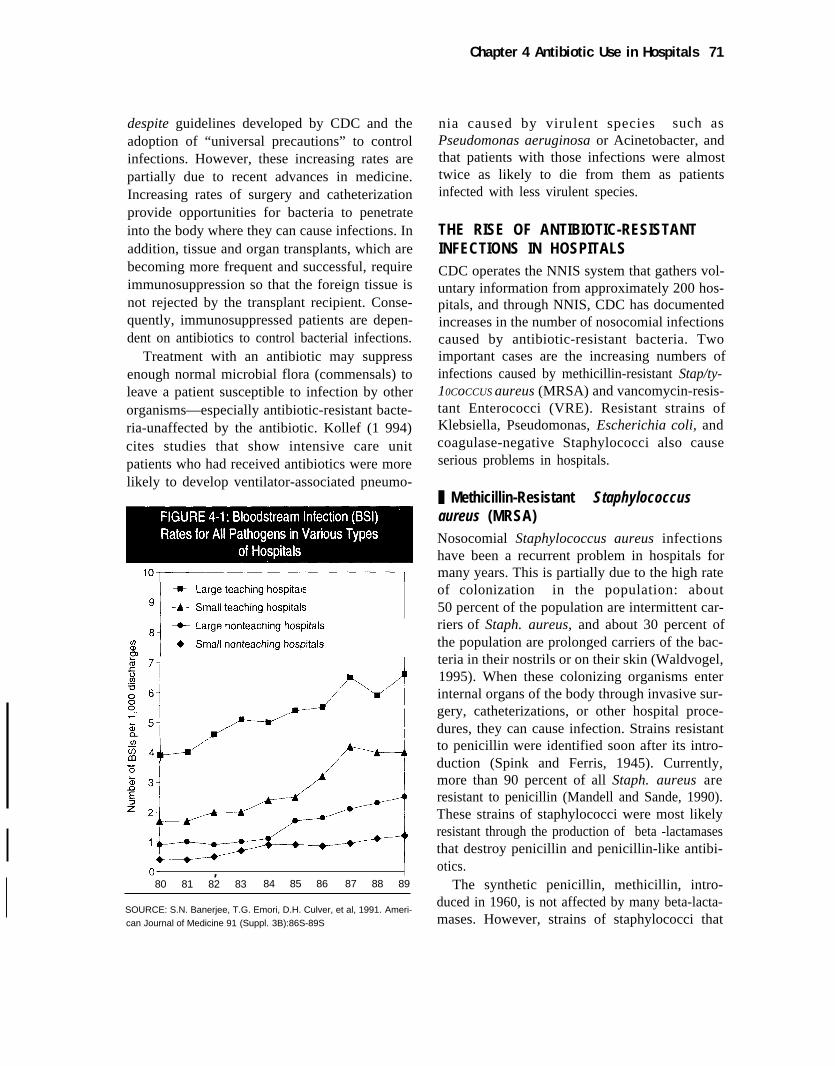
Chapter 4 Antibiotic Use in Hospitals 71
despite guidelines developed by CDC and theadoption of “universal precautions” to controlinfections. However, these increasing rates arepartially due to recent advances in medicine.Increasing rates of surgery and catheterizationprovide opportunities for bacteria to penetrateinto the body where they can cause infections. Inaddition, tissue and organ transplants, which arebecoming more frequent and successful, requireimmunosuppression so that the foreign tissue isnot rejected by the transplant recipient. Conse-quently, immunosuppressed patients are depen-dent on antibiotics to control bacterial infections.
Treatment with an antibiotic may suppressenough normal microbial flora (commensals) toleave a patient susceptible to infection by otherorganisms—especially antibiotic-resistant bacte-ria-unaffected by the antibiotic. Kollef (1 994)cites studies that show intensive care unitpatients who had received antibiotics were morelikely to develop ventilator-associated pneumo-
,80 81 82 83 84 85 86 87 88 89
SOURCE: S.N. Banerjee, T.G. Emori, D.H. Culver, et al, 1991. Ameri-
can Journal of Medicine 91 (Suppl. 3B):86S-89S
nia caused by virulent species such asPseudomonas aeruginosa or Acinetobacter, andthat patients with those infections were almosttwice as likely to die from them as patientsinfected with less virulent species.
THE RISE OF ANTIBIOTIC-RESISTANTINFECTIONS IN HOSPITALSCDC operates the NNIS system that gathers vol-untary information from approximately 200 hos-pitals, and through NNIS, CDC has documentedincreases in the number of nosocomial infectionscaused by antibiotic-resistant bacteria. Twoimportant cases are the increasing numbers ofinfections caused by methicillin-resistant Stap/ty-10CoCCUS aureus (MRSA) and vancomycin-resis-tant Enterococci (VRE). Resistant strains ofKlebsiella, Pseudomonas, Escherichia coli, andcoagulase-negative Staphylococci also causeserious problems in hospitals.
❚ Methicillin-Resistant Staphylococcusaureus (MRSA)Nosocomial Staphylococcus aureus infectionshave been a recurrent problem in hospitals formany years. This is partially due to the high rateof colonization in the population: about50 percent of the population are intermittent car-riers of Staph. aureus, and about 30 percent ofthe population are prolonged carriers of the bac-teria in their nostrils or on their skin (Waldvogel,1995). When these colonizing organisms enterinternal organs of the body through invasive sur-gery, catheterizations, or other hospital proce-dures, they can cause infection. Strains resistantto penicillin were identified soon after its intro-duction (Spink and Ferris, 1945). Currently,more than 90 percent of all Staph. aureus areresistant to penicillin (Mandell and Sande, 1990).These strains of staphylococci were most likelyresistant through the production of beta -lactamasesthat destroy penicillin and penicillin-like antibi-otics.
The synthetic penicillin, methicillin, intro-duced in 1960, is not affected by many beta-lacta-mases. However, strains of staphylococci that
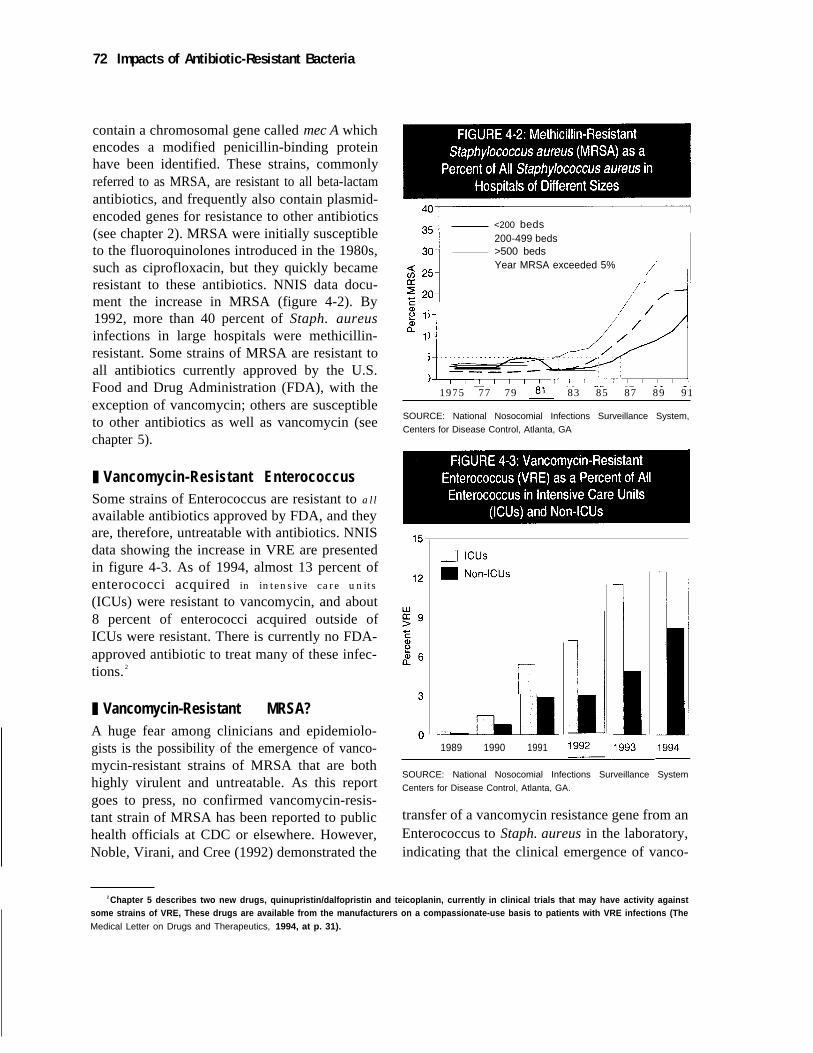
72 Impacts of Antibiotic-Resistant Bacteria
contain a chromosomal gene called mec A whichencodes a modified penicillin-binding proteinhave been identified. These strains, commonlyreferred to as MRSA, are resistant to all beta-lactamantibiotics, and frequently also contain plasmid-encoded genes for resistance to other antibiotics(see chapter 2). MRSA were initially susceptibleto the fluoroquinolones introduced in the 1980s,such as ciprofloxacin, but they quickly becameresistant to these antibiotics. NNIS data docu-ment the increase in MRSA (figure 4-2). By1992, more than 40 percent of Staph. aureusinfections in large hospitals were methicillin-resistant. Some strains of MRSA are resistant toall antibiotics currently approved by the U.S.Food and Drug Administration (FDA), with theexception of vancomycin; others are susceptibleto other antibiotics as well as vancomycin (seechapter 5).
❚ Vancomycin-Resistant EnterococcusSome strains of Enterococcus are resistant to all
available antibiotics approved by FDA, and theyare, therefore, untreatable with antibiotics. NNISdata showing the increase in VRE are presentedin figure 4-3. As of 1994, almost 13 percent ofenterococci acquired in intensive care units
(ICUs) were resistant to vancomycin, and about8 percent of enterococci acquired outside ofICUs were resistant. There is currently no FDA-approved antibiotic to treat many of these infec-tions. 2
❚ Vancomycin-Resistant MRSA?A huge fear among clinicians and epidemiolo-gists is the possibility of the emergence of vanco-mycin-resistant strains of MRSA that are bothhighly virulent and untreatable. As this reportgoes to press, no confirmed vancomycin-resis-tant strain of MRSA has been reported to publichealth officials at CDC or elsewhere. However,Noble, Virani, and Cree (1992) demonstrated the
<200 beds200-499 beds>500 bedsYear MRSA exceeded 5%
1975 77 79 83 85 87 89 91
SOURCE: National Nosocomial Infections Surveillance System,
Centers for Disease Control, Atlanta, GA
1989 1990 1991
SOURCE: National Nosocomial Infections Surveillance System
Centers for Disease Control, Atlanta, GA.
transfer of a vancomycin resistance gene from anEnterococcus to Staph. aureus in the laboratory,indicating that the clinical emergence of vanco-
2 Chapter 5 describes two new drugs, quinupristin/dalfopristin and teicoplanin, currently in clinical trials that may have activity againstsome strains of VRE, These drugs are available from the manufacturers on a compassionate-use basis to patients with VRE infections (TheMedical Letter on Drugs and Therapeutics, 1994, at p. 31).
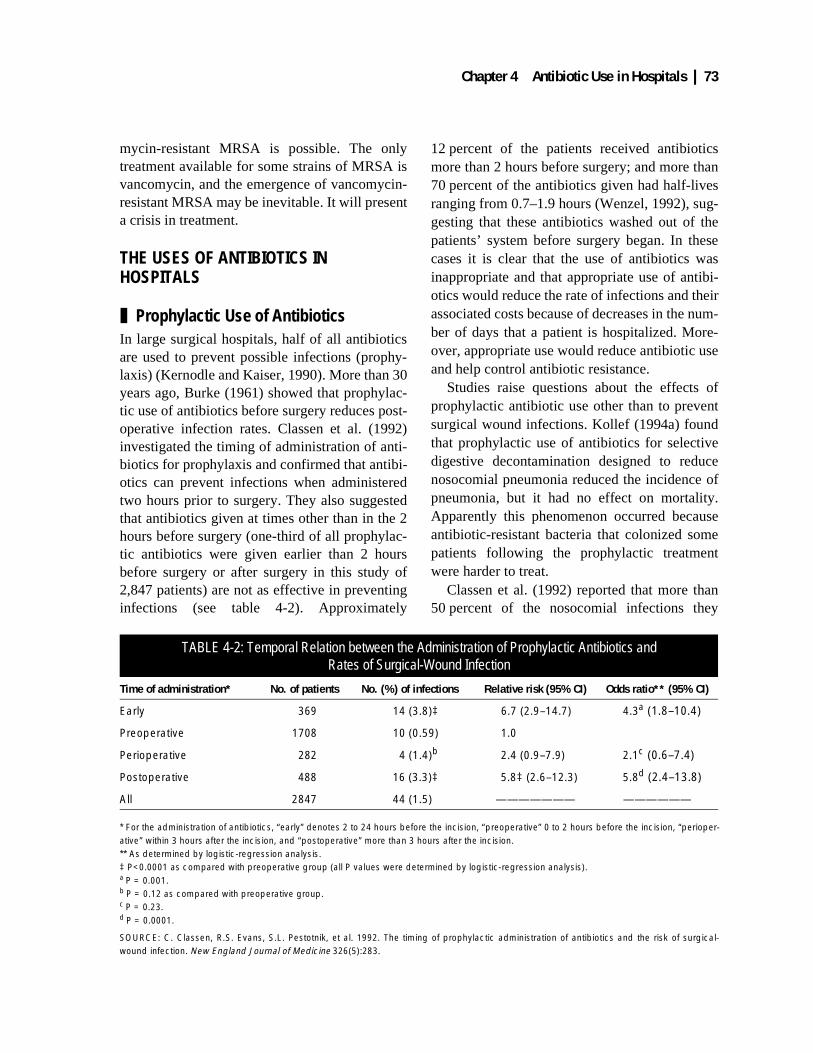
Chapter 4 Antibiotic Use in Hospitals | 73
mycin-resistant MRSA is possible. The onlytreatment available for some strains of MRSA isvancomycin, and the emergence of vancomycin-resistant MRSA may be inevitable. It will presenta crisis in treatment.
THE USES OF ANTIBIOTICS IN HOSPITALS
❚ Prophylactic Use of AntibioticsIn large surgical hospitals, half of all antibioticsare used to prevent possible infections (prophy-laxis) (Kernodle and Kaiser, 1990). More than 30years ago, Burke (1961) showed that prophylac-tic use of antibiotics before surgery reduces post-operative infection rates. Classen et al. (1992)investigated the timing of administration of anti-biotics for prophylaxis and confirmed that antibi-otics can prevent infections when administeredtwo hours prior to surgery. They also suggestedthat antibiotics given at times other than in the 2hours before surgery (one-third of all prophylac-tic antibiotics were given earlier than 2 hoursbefore surgery or after surgery in this study of2,847 patients) are not as effective in preventinginfections (see table 4-2). Approximately
12 percent of the patients received antibioticsmore than 2 hours before surgery; and more than70 percent of the antibiotics given had half-livesranging from 0.7–1.9 hours (Wenzel, 1992), sug-gesting that these antibiotics washed out of thepatients’ system before surgery began. In thesecases it is clear that the use of antibiotics wasinappropriate and that appropriate use of antibi-otics would reduce the rate of infections and theirassociated costs because of decreases in the num-ber of days that a patient is hospitalized. More-over, appropriate use would reduce antibiotic useand help control antibiotic resistance.
Studies raise questions about the effects ofprophylactic antibiotic use other than to preventsurgical wound infections. Kollef (1994a) foundthat prophylactic use of antibiotics for selectivedigestive decontamination designed to reducenosocomial pneumonia reduced the incidence ofpneumonia, but it had no effect on mortality.Apparently this phenomenon occurred becauseantibiotic-resistant bacteria that colonized somepatients following the prophylactic treatmentwere harder to treat.
Classen et al. (1992) reported that more than50 percent of the nosocomial infections they
TABLE 4-2: Temporal Relation between the Administration of Prophylactic Antibiotics and Rates of Surgical-Wound Infection
Time of administration* No. of patients No. (%) of infections Relative risk (95% CI) Odds ratio** (95% CI)
Early 369 14 (3.8)‡ 6.7 (2.9–14.7) 4.3a (1.8–10.4)
Preoperative 1708 10 (0.59) 1.0
Perioperative 282 4 (1.4)b 2.4 (0.9–7.9) 2.1c (0.6–7.4)
Postoperative 488 16 (3.3)‡ 5.8‡ (2.6–12.3) 5.8d (2.4–13.8)
All 2847 44 (1.5) ——————— ——————
* For the administration of antibiotics, “early” denotes 2 to 24 hours before the incision, “preoperative” 0 to 2 hours before the incision, “perioper-ative” within 3 hours after the incision, and “postoperative” more than 3 hours after the incision.** As determined by logistic-regression analysis.‡ P<0.0001 as compared with preoperative group (all P values were determined by logistic-regression analysis).a P = 0.001.b P = 0.12 as compared with preoperative group.c P = 0.23.d P = 0.0001.
SOURCE: C. Classen, R.S. Evans, S.L. Pestotnik, et al. 1992. The timing of prophylactic administration of antibiotics and the risk of surgical-wound infection. New England Journal of Medicine 326(5):283.

74 | Impacts of Antibiotic-Resistant Bacteria
studied were caused by organisms resistant to theantibiotic used. In these cases the infections mayhave been caused because the resistant organ-isms were able to multiply when the susceptiblenormal bacterial flora of the patients was inhib-ited by the prophylactic antibiotics. Siegel et al.(1980) reported an especially tragic example ofprophylactic use gone awry based on examina-tion of the results of giving a single dose of peni-cillin to ward off streptococcal infections insome 9,000 newborns. Although penicillin-sensi-tive infections were reduced by the prophylactictreatment, infections with penicillin-resistantbacteria were more frequent in the babies whoreceived the antibiotic, and mortality was higherfrom the resistant infections (15 of 35) than fromthe sensitive infections (3 of 27). Overall, thedeath rate from streptococcus infections was3 times higher in the babies that received penicil-lin (1.2/1,000 vs. 0.43/1,000 live births).
❚ Antibiotic Use to Treat Active InfectionsThe remainder of antibiotic use in hospitals is fortreatment of active infections. It takes at leasttwo days to identify the bacteria causing aninfection and to determine its antibiotic suscepti-bility (see chapter 6). Therefore, the physicianoften has to make an empirical judgment aboutthe identity of the bacteria and prescribe an anti-biotic before the laboratory test results are avail-able. If a patient is very sick, the physician willoften use multiple antibiotics. If the patient isimproving when the laboratory tests arrive, thephysician might ignore the results of the tests andcontinue the patient on the empiric antibiotics. Itis difficult to determine inappropriate antibioticuse and how to improve use in such cases.
The appearance of unexpected resistant organ-isms in one patient may influence a physician toroutinely prescribe newer or broader spectrumantibiotics. A letter to the editor of the NewEngland Journal of Medicine (Lonks et al.,1995) illustrates a case where a patient sufferedbecause he was infected with an unlikely resis-tant strain. Physicians knew that no highly resis-tant strains of pneumococci had been reported inProvidence, Rhode Island; only 2.3 percent of
isolates obtained in hospitals in 1990 and 1991showed intermediate-level resistance to penicil-lin, and none was highly resistant. An otherwisehealthy 33-year-old man, who lived a little morethan 30 miles from the city, was treated in thehospital for a Streptococcus pneumoniae infec-tion. Assuming that the strain was not ceftriax-one-resistant, doctors treated the patient withdexamethasone and ceftriaxone for the first fourdays. After initial improvement, encephalitisdeveloped, and doctors switched drugs to vanco-mycin and rifampin based on antibiotic-suscepti-bility test results that showed the infecting strainswere resistant to penicillin and ceftriaxone. Thepatient’s condition eventually improved and hewas sent home. Based on this experience, theauthors concluded that “all patients with the pre-sumptive diagnosis of pneumococcal meningitisshould receive high-dose ceftriaxone (or cefo-taxime) plus vancomycin, with or withoutrifampin, until the isolate is proved to be suscep-tible to penicillin or ceftriaxone” [emphasisadded]. It may be true that following this advicewill prevent a few adverse outcomes such asthose described in the letter to the journal. How-ever, if similar reasoning is applied in manycases, the widespread use of antibiotics such asvancomycin will increase the risk for the emer-gence of antibiotic-resistant organisms.
In a study of the reasoning strategies used byphysicians in empiric antibiotic selection, Yu etal. (1991) found that unexpected organismsappeared in 3.8 percent of all blood cultures. Inthese cases, antibiotics had been prescribedwhich were not the antibiotics of choice based onlogical reasoning, but which did cover the unex-pected organisms. The authors comment that“[t]hese memorable situations may have a dis-proportionate influence in these physicians’future selection of antibiotic therapy.” They fur-ther conclude that “our disturbing and unex-pected finding is that reflex prescription ofbroad-spectrum antibiotic therapy that is so oftendecried by academicians may have a rationalbasis” and that “educational efforts that empha-size narrow, rather than broad-spectrum prescrib-ing may be inadequate to change physicianprescribing habits.”

Chapter 4 Antibiotic Use in Hospitals | 75
LEGAL ASPECTS OF ANTIBIOTIC USEMalpractice concerns might provide an addi-tional incentive to prescribe antibiotics. Accord-ing to data published by St. Paul Fire and MarineInsurance Company, a large nationwide malprac-tice insurer, a significant number of claims arerelated to infection-related illnesses and antibi-otic use (St. Paul Fire and Marine Insurance Co.,1995). It is reasonable to speculate that fear of
malpractice litigation may contribute to prescrip-tion of overly broad spectrum antibiotics or ofantibiotics in cases where the chance of a bacte-rial infection is small. Box 4-1 contains excerptsfrom a commentary in the medical journal Lan-cet discussing the medical and legal controversyover the use of prophylactic antibiotics to pre-vent neonatal bacterial sepsis caused by Group Bstreptococcus.
BOX 4-1: Group B Streptococcus: The Controversy
Group B streptococcus (GBS) is the leading cause of neonatal bacterial sepsis in the United States,infecting about 12,000 newborns annually. Some newborns infected with GBS may die or have perma-nent neurological damage from meningitis. In 1992, both the American Academy of Pediatrics (AAP) andthe American College of Obstetricians and Gynecologists (ACOG) issued protocols regarding thescreening of pregnant women to detect and treat carriers of GBS in an effort to prevent neonatal GBSsepsis.
AAP called for universal prenatal GBS screening for all pregnant women at 26–28 weeks’ gestation.Because certain population groups are more likely to carry GBS, ACOG advocated for optional screeningtargeted to certain populations where the incidence of neonatal GBS infection is inordinately high, suchas populations where sexually transmitted diseases are common.
Inasmuch as GBS is part of the normal gut flora of some women and may or may not become a patho-gen during pregnancy, both AAP and ACOG recommended intrapartum (during delivery) antibiotic treat-ment only to women with positive cultures who have additional high-risk factors such as preterm labor orpremature rupture of the membranes before 37 weeks’ gestation, fever in labor, multiple births, rupture ofmembranes for more than 18 hours at any gestational age, or a previous affected child.
The AAP and ACOG protocols leave a number of issues unresolved that expose obstetricians, familypractitioners, and nurse midwives to considerable medicolegal liability. Screening for GBS during preg-nancy does not provide certainty as to whether or not intrapartum antibiotic treatment is warranted. Astudy found that in women who were culture-positive at 28 weeks’ gestation, 30 to 50 percent were cul-ture-negative at the time of delivery; in women who were culture-negative at 28 weeks, 8 to 15 percentwere culture-positive at the time of delivery. Consequently, some women will be treated unnecessarilyand some who need treatment will be ignored.
Moreover, if only certain groups are targeted for screening in keeping with ACOG’s protocol, canexcluded groups hold health care professionals responsible if their newborn babies developed undetec-ted GBS sepsis? Further, would the withholding of treatment in a pregnant woman with a positive culturewho has no additional risk factors absolve a health care professional from medicolegal liability if that babywere affected?
The best approach to the management of GBS sepsis would be a rapid screening test during labor todetermine whether antibiotic therapy is warranted, but the poor sensitivity of such tests currently rendersthem clinically useless. Until these tests are improved, health care professionals will most likely err on theside of caution and prescribe antibiotics even in extremely low-risk cases.
SOURCE: C.V. Towers, 1995, Lancet 346:197–198.

76 | Impacts of Antibiotic-Resistant Bacteria
The following review of some malpracticesuits exemplifies the dramatic consequences thatcan occur due to undertreating with antibiotics.In Hellwig v. Potluri (Case No. WL 285712,Ohio Court of Appeals 7th Circuit, 1991), thedefendant emergency room physician was heldliable for failing to prescribe antibiotics for theplaintiff who had stepped on a rusty nail at hishome. The plaintiff developed osteomyelitiswhich forced him to “wear an appliance in hisshoe and have an altered gait for the rest of hislife.” In Toler v. United States of America aplaintiff claimed that failure of a VeteransAdministration (VA) hospital to administer anadequate course of antibiotics resulted in sepsisand death. In Griffith v. West Suburban Hospital(Case No. 86L-23904, Cook County, Illinois Cir-cuit Court, 1993), a jury returned a $3.5-millionverdict for failure to diagnose and timely treat aGroup B Strep infection. In this case, a patientshowed signs of respiratory distress shortly afterbirth, and although he was moved to an intensivecare crib, antibiotics were not administered.Seven hours later, after being transferred toanother hospital which then administered antibi-otics, the patient died.
The medical and financial consequences offailing to prescribe prophylactic antibiotics forendocarditis can be considerable. In 1993, a den-tist was held liable in Orbay v. Castellanos (CaseNo. 91-36124, Dade County Circuit Court,Miami, Florida, 1993) for failing to prescribeprophylactic antibiotics prior to tooth extraction.Soon after the tooth extraction, the plaintiff wasdiagnosed with bacterial endocarditis and under-went open heart valve replacement surgery. Thedefendant was held liable for failure to prescribeprophylactic antibiotics and failure to obtain afull medical history or medical clearance for apatient at risk of developing bacterial endocardi-tis. The jury awarded the plaintiff $1.24 million,which was reduced to $964,000 to reflect thedecision that the plaintiff was 20 percent com-paratively negligent for failure to take appropri-ate care of himself. However, a standard medicaltextbook comments:
The issue of professional liability in the pro-phylaxis of endocarditis often has led to allega-tions of negligence and malpractice suits. . . . [Itis hard] to prove that the failure of a physicianor dentist to administer antibiotics was thedirect cause of a patient acquiring endocarditis.If a strict demonstration of proximate causewere always required, it is doubtful that anyclaim based on the failure to administer prophy-laxis could succeed, but juries are sometimescapricious in deciding liability in malpracticecases. . . (Mandell et al., 1990).
The “capricious” nature of the juries mightbias physicians in favor of prescribing antibiot-ics, even when the risk of endocarditis (or otherdisease) is very minimal.
CONTROLLING THE EMERGENCE AND SPREAD OF ANTIBIOTIC RESISTANCE IN HOSPITALSPart of the difficulty in controlling antibioticresistance in hospitals is incomplete understand-ing of all the factors that contribute to the emer-gence and spread of antibiotic resistance ingeneral. Most hospital personnel would agreethat infection control is critical, but there aremany disagreements about the benefits vs. costof various infection control procedures. Few, ifany, scientists disagree that the use of antibioticsis related to the emergence and spread of antibi-otic resistance. Nevertheless, there are manycontroversies about how to implement programsto control the use of antibiotics.
❚ Infection Control in HospitalsIn 1847, Ignac Semmelweis noticed that the rateof childbed fever in new mothers was muchhigher when the babies were delivered by obste-tricians and medical students than by midwivesand midwifery students. Semmelweis surmisedthat the high rate was due to the transmission ofinfectious particles from cadavers by the obste-tricians and medical students and instituted themeasure of handwashing in a chlorine solution.This measure greatly decreased the incidence ofchildbed fever (reviewed by Sanford, 1992).

Chapter 4 Antibiotic Use in Hospitals | 77
In hospitals today, infection control proce-dures are considered absolutely essential. In1976, CDC conducted a comprehensive Study onthe Efficacy of Nosocomial Infection Control(SENIC) that measured the extent and effective-ness of infection control procedures in U.S. hos-pitals. The SENIC study included a survey of allhospitals in the United States and detailed inter-views with representative hospitals. Twentyyears later, the study remains the most compre-hensive survey of the effectiveness of infectioncontrol procedures.3 The study concluded thathospitals with intensive infection surveillanceand control programs were able to reduce the rateof nosocomial infections by 32 percent (Haley etal., 1985). Yet the study found that only about0.2 percent of U.S. hospitals had programs thateffectively controlled all four of the major typesof infections: surgical wound infection, urinarytract infection, primary bloodstream infection,and lower respiratory tract infection.
❚ Infection Control ActivitiesThe SENIC study concluded that a successfulinfection control program required leadership bya trained infection control physician, an infectioncontrol nurse for every 250 beds, organizedinfection surveillance efforts, and a system forreporting infection rates to practicing surgeons.
Handwashing and Other PrecautionsSimple infection control procedures, such ashandwashing and wearing gloves, reduce thespread of infections in hospitals, lowering theneed for antibiotics and thereby reducing selec-tive pressure for the spread of antibiotic-resistantbacteria. Health care workers have a large incen-tive to follow procedures such as universal pre-cautions4 because they were designed to protectthem from infection from organisms such as the
3 SENIC data have the serious shortcoming that they were collected before implementation of current infection control procedures suchas universal precautions, which were instituted beginning in 1985 largely because of the fear of transmission of the human immunodeficiencyvirus (HIV).
4 Universal precautions include requirements that gloves be worn when handling bodily fluids, that needles and other sharp objects bedisposed of in special containers to help prevent needle-stick accidents, and that health care workers with open or infected wounds haverestricted contact with patients or patient care equipment (Garner, 1993).
human immunodeficiency virus (HIV). How-ever, in the hospital setting health care workerswho respond to a life-threatening emergencyoften do not have time to put on gloves and fol-low proper infection control procedures. Willy etal. (1990) found that health care workers’ per-ception of their own risk and potential spread ofinfections to patients is surprisingly low. In ananonymous nationwide survey of health careworkers who might have frequent exposure toblood and other bodily fluids, only 55 percent ofthose responding reported routinely practicinguniversal precautions.
Human nature seems to prevent the full imple-mentation of one of the simplest, yet most effec-tive infection control method: handwashing.Handwashing is a proven method for reducingnosocomial infections, but the practice is notstrictly followed. Handwashing compliance ratesof less than 50 percent were observed in twostudies of intensive care units (Simmons et al.,1990; Doebbeling et al., 1992). Goldmann andLarson (1992) make the following commentsabout the lack of compliance with handwashing:
Experts in infection control coax, cajole,threaten, and plead, but still their colleaguesneglect to wash their hands.... Education andpersuasion do not generally lead to sustainedimprovement in handwashing. Physicians havebeen particularly refractory. Innovativeapproaches are needed desperately, but fewhave emerged.... There is so little confidence inhand-washing habits that hospital isolation poli-cies now assume noncompliance.... [Originalreferences not included].
Simmons et al. (1990) revealed one clue tohandwashing noncompliance: nurses who werequestioned about their handwashing practicesbelieved they were washing their hands nearly

78 | Impacts of Antibiotic-Resistant Bacteria
90 percent of the time, when actual rates werebetween 22 and 29 percent.
Research into the seemingly simple questionof which soap to use for washing hands may beuseful in helping to prevent infections. Severalstudies have shown that a 7- to 10-second hand-wash with a non-antibacterial soap increased thetransmission of bacteria due to the shedding ofbacteria-laden skin cells, but that handwashingwith antiseptic soaps reduces the rates of nosoco-mial infections (Martin, 1994). Rotter (1988)compared the efficacy of different antiseptics forwashing hands and found that antiseptics con-taining isopropanol alcohol were significantlybetter at reducing skin bacteria than liquid soap.
Applying Infection Control Procedures to Control Antibiotic-Resistant Bacteria: Some Case StudiesBox 4-2 describes the successful countrywidecontrol of MRSA in Denmark. The followingcase studies describe attempts to apply infectioncontrol procedures to control MRSA in nursinghomes and hospitals in the United States.
Case 1: Successful control in a (mostly chronic care) VA medical center (Murray-Leisure et al., 1990)The Lebanon, Pennsylvania, Medical Center isan 884-bed facility which successfully controlledan epidemic of MRSA patients during 1988–1989 within six months of instituting aggressiveinterventions. These interventions included con-fining known active MRSA carriers and MRSA-infected patients to one nursing unit, screeningpatients transferred into the facility for MRSA,using gown and glove isolation and treating bothcolonized and actively infected patients with top-ical and enteral antibiotics.
Case 2: Unsuccessful control in a VA medical center (Strausbaugh et al., 1992)The Portland, Oregon, VA Medical Center Nurs-ing Home Care Unit (NHCU) is a 120-bed facil-ity that attempted to control MRSA primarilythrough administration of the antibioticsrifampin, trimethoprim-sulfamethoxazole, and
clindamycin, used either alone or in differentcombinations, to asymptomatic carriers ofMRSA. Other measures included restrictingMRSA-infected or colonized patients to a smallcluster of rooms, glove use to prevent the spreadof any body fluids, and frequent environmentalsurface decontamination. The majority of MRSApatients in this facility remained either colonizedor became recolonized during a 30-day follow-up period after treatment. Furthermore, a mostdisturbing byproduct of the Portland VA studywas the emergence of resistance to rifampin aftertherapy.
Case 3: Coordination of infection control practices between a hospital and nursing homes to manage MRSA (Jewell, 1994)The Christ Hospital and Medical Center, OakLawn, Illinois, is an 823-bed teaching hospitalthat serves many patients who live in regionalnursing homes. Before 1991, nursing homesoften required three successive test results show-ing the patient was not carrying MRSA beforethey would accept a patient from the hospital.This led to extended stays in the hospital forpatients who were colonized with MRSA, butotherwise did not need to be in the hospital. Aquality improvement team including clinicians,hospital administrators, and nursing home repre-sentatives adopted guidelines that allowed colo-nized patients to be returned to the nursinghomes. When these new guidelines wereadopted, the hospital did not see any change inthe number of patients infected or colonized withMRSA. It did see an average decrease of over10 days in the length of stay in the hospital, areduction in the readmission rate of patients col-onized with MRSA from 8.7 to 2.7 percent in1992, and total cost savings of over $1.9 million.
These case studies illustrate the complexitiesin determining which infection control practicesare the most likely to help control antibiotic-resistant bacteria such as MRSA. In the firstcase, a combination of isolation of patients colo-nized or infected with MRSA and antibiotic ther-apy seemed to control MRSA, but in the secondcase similar procedures failed to produce posi-
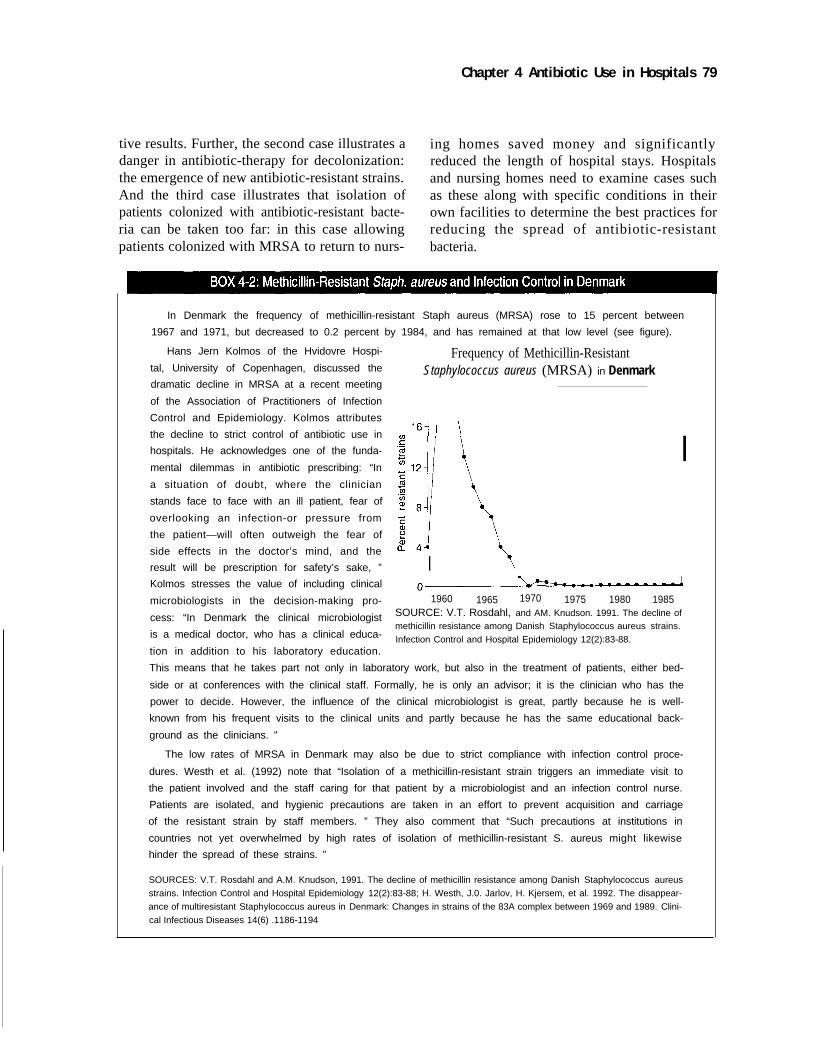
Chapter 4 Antibiotic Use in Hospitals 79
tive results. Further, the second case illustrates a ing homes saved money and significantlydanger in antibiotic-therapy for decolonization: reduced the length of hospital stays. Hospitalsthe emergence of new antibiotic-resistant strains. and nursing homes need to examine cases suchAnd the third case illustrates that isolation of as these along with specific conditions in theirpatients colonized with antibiotic-resistant bacte- own facilities to determine the best practices forria can be taken too far: in this case allowing reducing the spread of antibiotic-resistantpatients colonized with MRSA to return to nurs- bacteria.
In Denmark the frequency of methicillin-resistant Staph aureus (MRSA) rose to 15 percent between
1967 and 1971, but decreased to 0.2 percent by 1984, and has remained at that low level (see figure).
Hans Jern Kolmos of the Hvidovre Hospi-
tal, University of Copenhagen, discussed the
dramatic decline in MRSA at a recent meeting
of the Association of Practitioners of Infection
Control and Epidemiology. Kolmos attributes
the decline to strict control of antibiotic use in
hospitals. He acknowledges one of the funda-
mental dilemmas in antibiotic prescribing: “In
a situation of doubt, where the clinician
stands face to face with an ill patient, fear of
overlooking an infection-or pressure from
the patient—will often outweigh the fear of
side effects in the doctor’s mind, and the
result will be prescription for safety’s sake, ”
Kolmos stresses the value of including clinical
microbiologists in the decision-making pro-
cess: “In Denmark the clinical microbiologist
is a medical doctor, who has a clinical educa-
tion in addition to his laboratory education.
Frequency of Methicillin-ResistantStaphylococcus aureus (MRSA) in Denmark
I
I
1960 1965 1970 1975 1980 1985SOURCE: V.T. Rosdahl, and AM. Knudson. 1991. The decline ofmethicillin resistance among Danish Staphylococcus aureus strains.
Infection Control and Hospital Epidemiology 12(2):83-88.
This means that he takes part not only in laboratory work, but also in the treatment of patients, either bed-
side or at conferences with the clinical staff. Formally, he is only an advisor; it is the clinician who has the
power to decide. However, the influence of the clinical microbiologist is great, partly because he is well-
known from his frequent visits to the clinical units and partly because he has the same educational back-
ground as the clinicians. ”
The low rates of MRSA in Denmark may also be due to strict compliance with infection control proce-
dures. Westh et al. (1992) note that “Isolation of a methicillin-resistant strain triggers an immediate visit to
the patient involved and the staff caring for that patient by a microbiologist and an infection control nurse.
Patients are isolated, and hygienic precautions are taken in an effort to prevent acquisition and carriage
of the resistant strain by staff members. ” They also comment that “Such precautions at institutions in
countries not yet overwhelmed by high rates of isolation of methicillin-resistant S. aureus might likewise
hinder the spread of these strains. ”
SOURCES: V.T. Rosdahl and A.M. Knudson, 1991. The decline of methicillin resistance among Danish Staphylococcus aureus
strains. Infection Control and Hospital Epidemiology 12(2):83-88; H. Westh, J.0. Jarlov, H. Kjersem, et al. 1992. The disappear-
ance of multiresistant Staphylococcus aureus in Denmark: Changes in strains of the 83A complex between 1969 and 1989. Clini-
cal Infectious Diseases 14(6) .1186-1194

80 | Impacts of Antibiotic-Resistant Bacteria
HOSPITAL ACCREDITATION AND INFECTION CONTROL REGULATIONS UNDER MEDICARECurrent hospital accreditation and Medicare reg-ulations recognize that each hospital must ana-lyze conditions in its own facility to determinethe best methods of infection control.
Loeb and O’Leary of The Joint Commissionon Accreditation of Healthcare Organizations(JCAHO) explain that
The Joint Commission historically has usedcompliance with contemporary standards as itsbasic measure of health care quality in theaccreditation process. In recent years, however,there has been growing interest in monitoringand evaluating the actual results of care. . .
JCAHO has recently developed a system forperformance measurement called the IndicatorMeasurement System (IMSystem). Beginning in1996, the system will include several measure-ments related to antibiotic use and infection con-trol: timing of administration of prophylacticantibiotics, surveillance and prevention of surgi-cal site infection, surveillance and prevention ofventilator-associated pneumonia, and surveil-lance and prevention of primary blood streaminfections. JCAHO has recognized “. . . thealready tremendous information burdens on mostorganizations” and therefore has designed
“. . . the IMSystem to be parsimonious, thatis, to collect only those data elements that areneeded and to use all the elements that are col-lected. Whenever possible, the IMSystem usesdata elements likely to be already collected byhealth care organizations” (IMSystem GeneralInformation, JCAHO).
Participation in this system, which is volun-tary, has great potential to help hospitals identifyspecific problems in infection control.
Medicare regulations state that as a conditionof participation in Medicare, hospitals must havea quality assurance program in which “nosoco-mial infections and medication therapy must beevaluated” (42 CFR 482.21a2). Further, “theremust be an active program for the prevention,control, and investigation of infectious and com-
municable diseases” (42 CFR 482.42). This pro-gram includes the designation of an infectioncontrol officer who “must develop a system foridentifying, reporting, investigating, and control-ling infections and communicable diseases ofpatients and personnel” (42 CFR 482.42a1) and“must maintain a log of incidents related toinfections and communicable diseases” (42 CFR482.42a2).
In the past, regulations for accreditation andMedicare participation were more specificallyworded, and specifically acknowledged the prob-lems of antibiotic resistance: for example, hospi-tals had to have “measures which control theindiscriminate use of preventive antibiotics in theabsence of infection, and the use of antibiotics inthe presence of infection is based on necessarycultures and sensitivity tests” (42 CFR405.1022c6 as of Oct. 1, 1983). However, basedon past experiences such as those described inthis chapter, specific regulations such as thesemay not be applicable to every facility.
❚ Surveillance of Antibiotic-Resistant BacteriaThere is no national system for reporting thepresence and pattern of antibiotic-resistant bacte-ria, leaving physicians and scientists in the darkabout the prevalence of those organisms in dif-ferent geographical areas. Although many in-hospital, small-scale surveillance systems,designed to track the spread of disease-causingorganisms, including antibiotic-resistant bacte-ria, provide information to physicians aboutwhich antibiotics remain effective, there is nostandard format for the collection and dissemina-tion of data. Antibiotic prescriptions and micro-biology test results are often recorded onseparate slips of paper, making correlation of thetwo sets of data almost impossible. However, theincreasing use of computer technology and theInternet provides increased opportunities forstandardized record keeping in hospitals andeasy database collection and access.
At the state level, the New Jersey StateDepartment of Health started collecting dataabout antibiotic-resistant bacteria in 1991. The

Chapter 4 Antibiotic Use in Hospitals | 81
system includes the 95 acute-care hospitalslicensed by the State of New Jersey and uses datathat are already routinely collected in hospitallaboratories. All hospitals make monthly reportsto the State Department of Health, which, in turn,disseminates its compilation of information toanyone on request. This system’s tracking ofvancomycin-resistant Enterococcus (VRE)spurred collaborative efforts involving privateand public sector and academic organizations toevaluate risk factors for the disease, treatmentoptions, effectiveness of infection-control proce-dures, and the in-vitro susceptibility of VRE toantimicrobial agents during the planning of clini-cal trials (MMWR, 1995). The system is inex-pensive to operate and simple to maintain.
SCOPE, Surveillance and Control of Patho-gens of Epidemiological Importance, is anational effort established by the University ofIowa and Lederle Laboratories (now Wyeth-Ayerst Lederle Laboratories) in 1995. The pro-gram expects to collect reports of all nosocomialbloodstream infections in 48 hospitals nation-wide as well as samples of the organisms isolatedfrom the infected patients. The reports will pro-vide information about the spread of antibiotic-resistant bacteria in the participating hospitals.The bacterial samples will be banked at the Uni-versity of Iowa, and the accuracy of bacterialidentification and antibiotic resistance determi-nations will be verified for representative sam-ples. For a fee, the University will test newantibiotics from any company against bacteria inits collection. The first hospital entered the pro-gram on April 1, 1995, and 40 had entered byJune 30.
There are also other industry-funded surveil-lance systems. A number of academic and com-mercial laboratories conduct surveillance undercontract to pharmaceutical companies, but theyare not necessarily designed to obtain informa-tion most useful for public health purposes.Instead, and understandably, they collect infor-mation about the efficacy of producers’ products.
The National Nosocomial Infection Survey(NNIS), which is run by CDC, is the singlenationwide surveillance system that produces
information about antibiotic-resistant bacteria.While it is limited to reports on nosocomialinfections, it is the source for most of the data inthis OTA report about MRSA, VRE, and otherdrug-resistant bacterial infections.
CDC is in the early stages of establishingnationwide surveillance of drug-resistant Strep-tococcus pneumoniae (DRSP), which will coverinfections whether or not they occur in a hospital.The system requires that participating laborato-ries test all S. pneumoniae isolated from bloodand cerebrospinal fluid for antibiotic susceptibil-ity by using standard testing methods, and thatall test results be reported to the state healthdepartments. The CDC initiated this system in 20laboratories in New Jersey in April 1995, and iffunds are available, the organization expects thatmost of the nearly 2,000 hospital and commerciallaboratories that now have computerized recordkeeping will be in the system by 1998. As labo-ratories add computer capabilities, CDC willencourage them to enlist in the system, and itexpects that all of the nearly 5,000 laboratories inthe country will participate. If the DRSP systemworks, CDC envisions expanding it to includeother antibiotic-resistant bacteria. As an earlystep in setting up the DRSP system, and atCDC’s request, the Council of State and Territo-rial Epidemiologists has recommended DRSP forinclusion on the list of notifiable diseases, andfour states now report it.
WHONET, a surveillance project of theWorld Health Organization, was established andoperated by two scientists, and it functions on ashoestring budget. The system collects informa-tion about resistance patterns in bacteria fromabout 100 hospitals all over the world, makes thedata available to researchers, and provides muchof the available information about the interna-tional flow of antibiotic-resistant bacteria.
One of WHONET’s great strengths is that ithas demonstrated that laboratories around theworld can produce data that can be interpretedand incorporated into a system that providesresults that are comparable from country to coun-try. To do this, the network collects laboratorydata, not interpretations of the data. While rulesfor interpreting susceptibility test results differ

82 | Impacts of Antibiotic-Resistant Bacteria
among various countries, WHONET can makeinternational comparisons based on the raw data.
Participating institutions also gain fromWHONET. The network provides laboratorieswith a computer program, which can be taught inabout six hours, and, where necessary, a com-puter. The software of WHONET, set up to iden-tify unusual patterns of resistance, allows theinfection control practitioner at the hospital totrace the spread of individual strains of bacteriaand use that information to modify infection con-trol procedures.
WHONET is inexpensive, it requires littlesupervision, and it obtains raw data, the data ofmost value to researchers (see chapter 6). It hasbeen successful in obtaining information fromdeveloping countries as well as developed ones,
and it provides an example of the feasibility ofcollecting and reporting antibiotic-resistanceinformation for little money.
❚ Controlling the Use of AntibioticsMuch evidence links the use of antibiotics to theemergence and spread of antibiotic resistance.Table 4-3 summarizes some studies which dem-onstrate relationships between increased use ofantibiotics and prevalence of resistance in hospi-tal organisms. There are also many exampleswhere the prevalence of resistance in hospitalorganisms decreased when the use of antibioticswas decreased (table 4-4). McGowan (1994)recently asked the question: “Do intensive hospi-tal antibiotic control programs prevent the spreadof antibiotic resistance?” and concluded that
TABLE 4-3: Some Studies Demonstrating a Temporal Relationship Between Increased Usage of Antimicrobial Agents and Increased Prevalence of Resistant Hospital Organisms
Year Reference Setting for use of antimicrobials Organism(s) Antimicrobial(s) used
1953 1 General use Staphylococcus aureus Erythromycin
S. aureus Penicillin
S. aureus Chlortetracycline
1956 2 Burn ward S. aureus Chloramphenicol
S. aureus Chlortetracycline
1967 3 Surgical prophylaxis S. aureus Neomycin cream
1971 4 Burn ward Pseudomonas aeruginosa Gentamicin
1978 5 Surgical prophylaxis P. aeruginosa Gentamicin
Serratia Gentamicin
1979 6 Postoperative use Serratia Gentamicin
1. M.H. Lepper, B. Moulton, H.F. Dowling, et al. 1953. Epidemiology of erythromycin-resistant staphylococci in a hospital population—effect onthe therapeutic activity of erythromycin. In: H. Welch and F. Martí-Ibáñez (eds.) Antibiotics annual 1953–1954. New York, NY. Medical Encyclope-dia, pp. 308–313.2. C.D. Gibson, Jr., and W.C. Thompson, Jr. 1956. The response of burning wound staphylococci to alternating programs of antibiotic therapy. In:H. Welch and F. Martí-Ibáñez (eds.) Antibiotics annual 1955–1956. New York, NY. Medical Encyclopedia, pp. 32–34.3. P.M. Rountree, M.A. Beard, J. Loewenthal, et al. 1967. Staphylococcal sepsis in a new surgical ward. British Medical Journal 1:132–137.4. J.A. Shulman, P.M. Terry, and C.E. Hough. 1971. Colonization with gentamicin-resistant Pseudomonas aeruginosa, pyocine type 5, in a burnunit. Journal of Infectious Disease 124(suppl):S18–23.5. N.J. Roberts, Jr., and R.G. Douglas, Jr. 1978. Gentamicin use and Pseudomonas and Serratia resistance: effect of a surgical prophylaxis reg-imen. Antimicrobial Agents and Chemotherapy 13:214–220.6. V.L. Yu, C.A. Oakes, K.J. Axnick, et al. 1979. Patient factors contributing to the emergence of gentamicin-resistant Serratia marcescens. Amer-ican Journal of Medicine 66:468–472.
SOURCE: J.E. McGowan, Jr. 1983. Antimicrobial resistance in hospital organisms and its relation to antibiotic use. Reviews of Infectious Dis-eases 5(6):1033–1048.
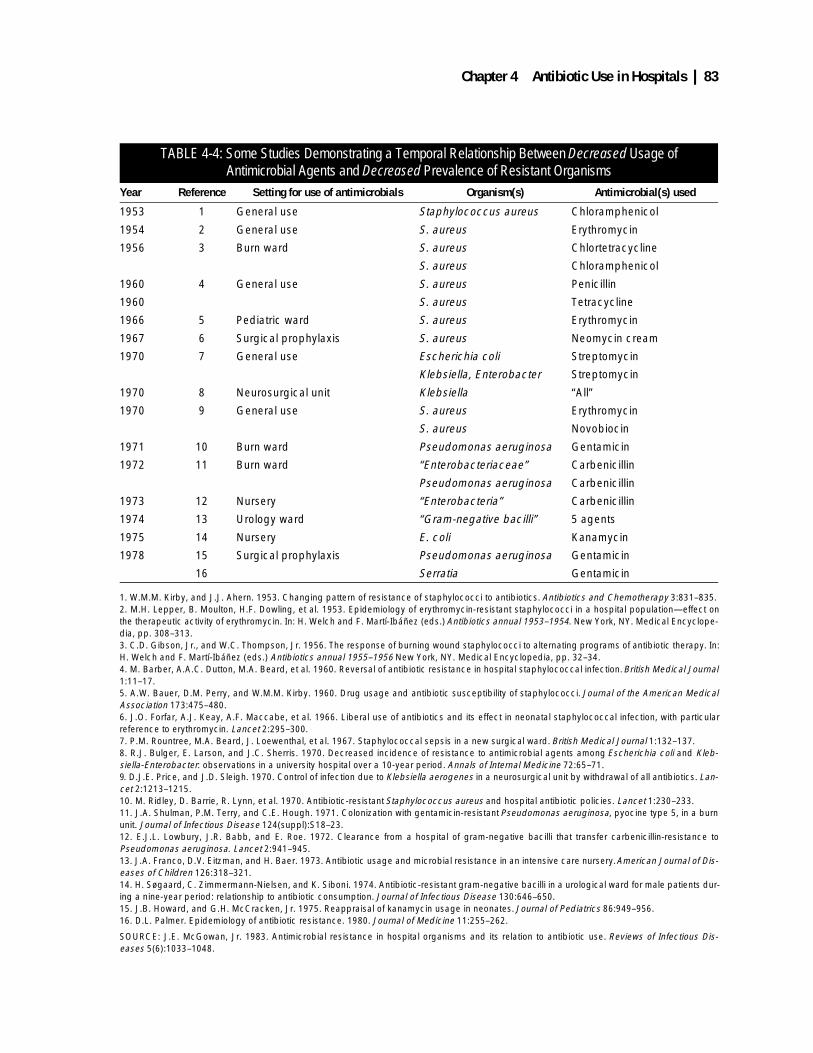
Chapter 4 Antibiotic Use in Hospitals | 83
TABLE 4-4: Some Studies Demonstrating a Temporal Relationship Between Decreased Usage of Antimicrobial Agents and Decreased Prevalence of Resistant Organisms
Year Reference Setting for use of antimicrobials Organism(s) Antimicrobial(s) used
1953 1 General use Staphylococcus aureus Chloramphenicol
1954 2 General use S. aureus Erythromycin
1956 3 Burn ward S. aureus Chlortetracycline
S. aureus Chloramphenicol
1960 4 General use S. aureus Penicillin
1960 S. aureus Tetracycline
1966 5 Pediatric ward S. aureus Erythromycin
1967 6 Surgical prophylaxis S. aureus Neomycin cream
1970 7 General use Escherichia coli Streptomycin
Klebsiella, Enterobacter Streptomycin
1970 8 Neurosurgical unit Klebsiella “All”
1970 9 General use S. aureus Erythromycin
S. aureus Novobiocin
1971 10 Burn ward Pseudomonas aeruginosa Gentamicin
1972 11 Burn ward “Enterobacteriaceae” Carbenicillin
Pseudomonas aeruginosa Carbenicillin
1973 12 Nursery “Enterobacteria” Carbenicillin
1974 13 Urology ward “Gram-negative bacilli” 5 agents
1975 14 Nursery E. coli Kanamycin
1978 15 Surgical prophylaxis Pseudomonas aeruginosa Gentamicin
16 Serratia Gentamicin
1. W.M.M. Kirby, and J.J. Ahern. 1953. Changing pattern of resistance of staphylococci to antibiotics. Antibiotics and Chemotherapy 3:831–835.2. M.H. Lepper, B. Moulton, H.F. Dowling, et al. 1953. Epidemiology of erythromycin-resistant staphylococci in a hospital population—effect onthe therapeutic activity of erythromycin. In: H. Welch and F. Martí-Ibáñez (eds.) Antibiotics annual 1953–1954. New York, NY. Medical Encyclope-dia, pp. 308–313.3. C.D. Gibson, Jr., and W.C. Thompson, Jr. 1956. The response of burning wound staphylococci to alternating programs of antibiotic therapy. In:H. Welch and F. Martí-Ibáñez (eds.) Antibiotics annual 1955–1956 New York, NY. Medical Encyclopedia, pp. 32–34.4. M. Barber, A.A.C. Dutton, M.A. Beard, et al. 1960. Reversal of antibiotic resistance in hospital staphylococcal infection. British Medical Journal1:11–17.5. A.W. Bauer, D.M. Perry, and W.M.M. Kirby. 1960. Drug usage and antibiotic susceptibility of staphylococci. Journal of the American MedicalAssociation 173:475–480.6. J.O. Forfar, A.J. Keay, A.F. Maccabe, et al. 1966. Liberal use of antibiotics and its effect in neonatal staphylococcal infection, with particularreference to erythromycin. Lancet 2:295–300.7. P.M. Rountree, M.A. Beard, J. Loewenthal, et al. 1967. Staphylococcal sepsis in a new surgical ward. British Medical Journal 1:132–137.8. R.J. Bulger, E. Larson, and J.C. Sherris. 1970. Decreased incidence of resistance to antimicrobial agents among Escherichia coli and Kleb-siella-Enterobacter: observations in a university hospital over a 10-year period. Annals of Internal Medicine 72:65–71.9. D.J.E. Price, and J.D. Sleigh. 1970. Control of infection due to Klebsiella aerogenes in a neurosurgical unit by withdrawal of all antibiotics. Lan-cet 2:1213–1215.10. M. Ridley, D. Barrie, R. Lynn, et al. 1970. Antibiotic-resistant Staphylococcus aureus and hospital antibiotic policies. Lancet 1:230–233.11. J.A. Shulman, P.M. Terry, and C.E. Hough. 1971. Colonization with gentamicin-resistant Pseudomonas aeruginosa, pyocine type 5, in a burnunit. Journal of Infectious Disease 124(suppl):S18–23.12. E.J.L. Lowbury, J.R. Babb, and E. Roe. 1972. Clearance from a hospital of gram-negative bacilli that transfer carbenicillin-resistance toPseudomonas aeruginosa. Lancet 2:941–945.13. J.A. Franco, D.V. Eitzman, and H. Baer. 1973. Antibiotic usage and microbial resistance in an intensive care nursery. American Journal of Dis-eases of Children 126:318–321.14. H. Søgaard, C. Zimmermann-Nielsen, and K. Siboni. 1974. Antibiotic-resistant gram-negative bacilli in a urological ward for male patients dur-ing a nine-year period: relationship to antibiotic consumption. Journal of Infectious Disease 130:646–650.15. J.B. Howard, and G.H. McCracken, Jr. 1975. Reappraisal of kanamycin usage in neonates. Journal of Pediatrics 86:949–956.16. D.L. Palmer. Epidemiology of antibiotic resistance. 1980. Journal of Medicine 11:255–262.
SOURCE: J.E. McGowan, Jr. 1983. Antimicrobial resistance in hospital organisms and its relation to antibiotic use. Reviews of Infectious Dis-eases 5(6):1033–1048.

84 | Impacts of Antibiotic-Resistant Bacteria
. . . in a few institutions there has been anincrease in susceptibility to antimicrobials fol-lowing intensive control or monitoring . . . in afew hospitals, intensive antibiotic control forselected drug-organisms pairs was associatedwith a high prevalence of susceptibility, and theproportion susceptible fell abruptly when con-trol or monitoring was relaxed or removed.
This latter finding indicates that the decreasein resistance may not be stable: reintroduction ofthe antibiotic can cause the resistance to immedi-ately return.
There are also counterexamples where antibi-otic control programs do not increase susceptibil-ity. In one example, resistance patterns inEnterobacter cloacae but not Pseudomonasaeruginosa were related to ceftazidime use in 18different hospitals in different geographical loca-tions (Ballow and Schentag, 1992). Silber et al.found that “facilities with restriction programswere as likely as those without to have had a caseof VRE bacteremia.” In Denmark the use ofmethicillin increased substantially in the 1970swhile the prevalence of MRSA decreased sub-stantially. The decrease in MRSA was correlatedwith a decrease in the use of tetracycline andstreptomycin (Rosendal et al., 1977). This mightbe explained by the use of tetracycline and strep-tomycin selecting for bacteria with multi-resis-tant plasmids (see chapter 2) also containinggenes for resistance to methicillin. Takentogether, these examples indicate that it is notsimple to determine the specific relationshipbetween antibiotic use and antibiotic resistance.
CDC recently began a systematic study of therelationship between antibiotic use and antibioticresistance. In the initial phase of the I-CARE(Intensive Care Antimicrobial Resistance Epide-miology) project, eight pilot hospitals monitoredthe use of antibiotics and the numbers of antibi-
otic-resistant bacteria. The results for MRSA(shown in figure 4-4) indicate that some hospi-tals use large amounts of methicillin and havehigh frequencies of resistant organisms(hospital B), while others use very little methicil-lin, but still have high frequencies of resistantorganisms (hospital E).
One possible explanation for this is suggestedby the Klebsiella results in figure 4-5: hospital Emay be receiving many patients from anotherhospital (or nursing home) that uses a lot ofmethicillin. Hospital H is interesting in that it hasone of the lowest rates of MRSA and the highestuse of methicillin of any of the eight pilot hospi-tals. This result might be related to a recent resultfrom a French 15-year study (Loulergue et al.,1994) that showed the prevalence of MRSA wasunrelated to cloxacillin (a semisynthetic penicil-lin derivative closely related to methicillin) useon some wards of a hospital where none of thestaff was a carrier of MRSA. This study indi-cated that carriage of MRSA by hospital staff isone risk factor for patients becoming infectedwith MRSA. The data from I-CARE correlate theemergence and spread of antibiotic resistancewith different causes in different hospitals.Moreover, the pilot study demonstrates how use-ful a system such as I-CARE can be in compar-ing an individual hospital to national trends andusing that comparison to design antibiotic useand infection control procedures specifically tai-lored to the problems in the individual hospi-tal.Antibiotics are widely used by physicians incommunity practice as well as by physicians inthe hospitals. In one study (table 4-5), about halfof the cardiac surgery patients colonized withcefazolin-resistant strains of bacteria were colo-nized upon admission to the hospital.5 There-fore, some antibiotic-resistant strains arise in thecommunity, indicating that antibiotic use must be
5 Cefazolin is commonly administered to cardiac patients as prophylaxis to prevent infections during the surgery. The risk of developinga Staph. aureus infection after cardiac surgery has been estimated as 15-44 percent (Mandell, Bennet, Dolin, page 2747). Colonization of thepatient or attending staff with cefazolin-resistant strains would be a significant risk factor for surgical infections when cefazolin is used forprophylaxis.

Chapter 4 Antibiotic Use in Hospitals | 85
controlled by community physicians as well asby hospital physicians in order for hospital-basedprograms to be fully effective. (For more infor-mation about antibiotic-resistant bacteria andantibiotic use in the community, see chapter 3.
❚ Improving Antibiotic Use
Antibiograms To guide physicians in the use of antibiotics,many hospitals provide “antibiograms” thatdescribe the susceptibility of commonly encoun-tered bacteria to various antibiotics. As shown intable 4-6, the vast majority of causes of bacterialinfections in both inpatients and outpatientsremain sensitive to the modern antibiotics. Onthe other hand, many Staph. aureus, coagulase-negative Staphylococci, and S. pneumoniae areresistant to many commonly used antibiotics, andsome Enterococcus are resistant to all antibiotics.
FormulariesThe use of all drugs in hospitals is increas-
ingly controlled by hospital formularies, whichwere set up to control the costs of drugs. The for-mularies may have the added benefit of helpingto control the use of antibiotics and the antibioticresistance problem. In Denver, Colorado, areahospitals (North, 1993), a formulary is combinedwith a computerized antibiotic order form. Thissystem restricts some antibiotics to approvedindications, and use of others requires approvalby specialists in infectious disease. This systemhas saved the hospitals money, and allowed themto easily change the formulary when susceptibil-ity testing indicated a problem of increased resis-tance to a specific antibiotic ) .
Physician EducationPhysician education is crucial to avoid mistakesmade by inadequate knowledge of antibiotic
FIGURE 4-4a: Percent of Staphylococcus Aureus Resistant to Methicillin
SOURCE: National Nosocomial Infections Surveillance System, Centers for Disease Control, Atlanta, GA.
FIGURE 4-4b: Grams of Methicillin Used per 1,000 Patient Days
SOURCE: National Nosocomial Infections Surveillance System, Centers for Disease Control, Atlanta, GA.
FIGURE 4-4c: Percent of Staphylococcus aureus Resistant to Methicillin/Methicillin Use
SOURCE: National Nosocomial Infections Surveillance System, Centers for Disease Control, Atlanta, GA.
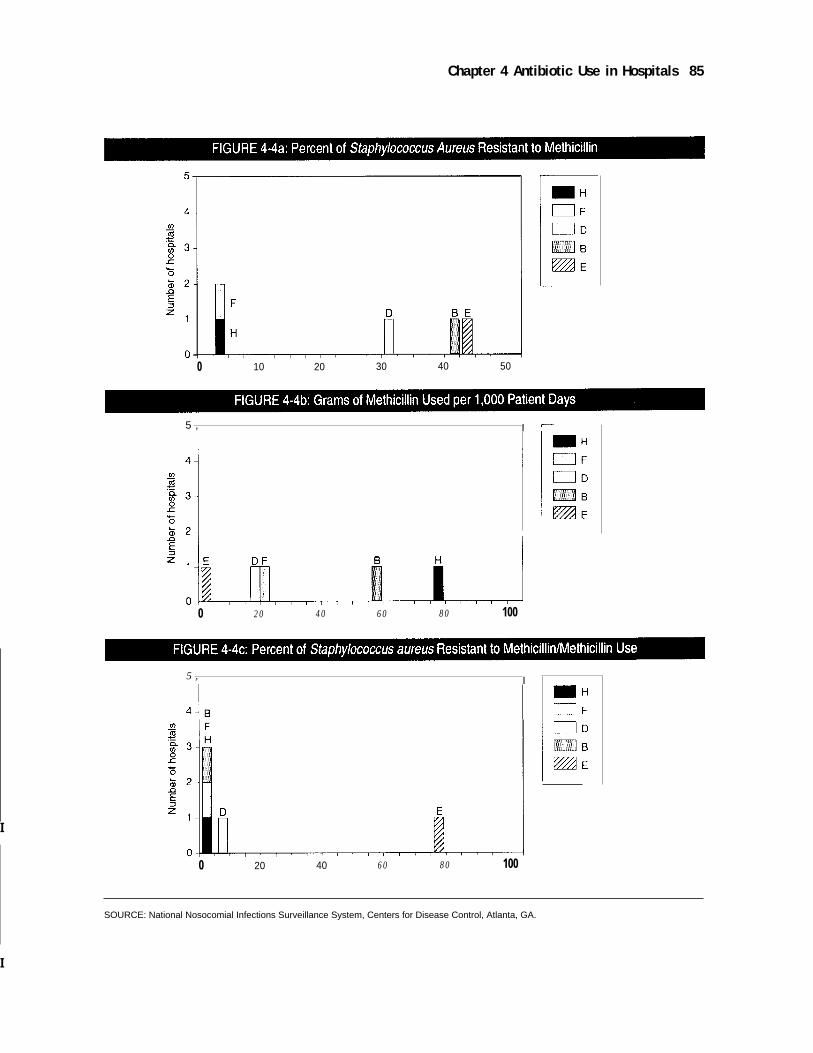
Chapter 4 Antibiotic Use in Hospitals 85
I
0 10 20 30 40 50
5 , I
0 20 40 60 80 100
5 , I
0 20 40 60 80 100
SOURCE: National Nosocomial Infections Surveillance System, Centers for Disease Control, Atlanta, GA.
I
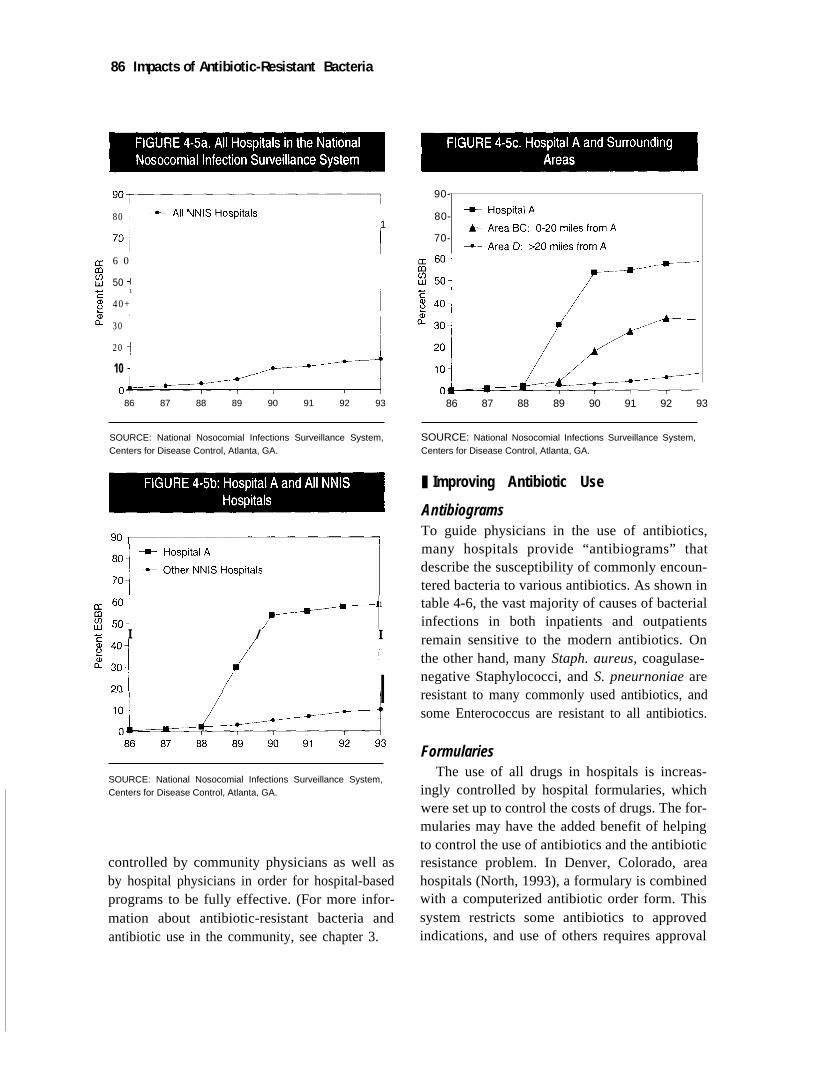
86 Impacts of Antibiotic-Resistant Bacteria
I
801
6 0
501
40+
30
20
10
86 87 88 89 90 91 92 93
SOURCE: National Nosocomial Infections Surveillance System,Centers for Disease Control, Atlanta, GA.
1
I / I
I
SOURCE: National Nosocomial Infections Surveillance System,Centers for Disease Control, Atlanta, GA.
controlled by community physicians as well asby hospital physicians in order for hospital-basedprograms to be fully effective. (For more infor-mation about antibiotic-resistant bacteria andantibiotic use in the community, see chapter 3.
90-
80-
70-
86 87 88 89 90 91 92 93
SOURCE: National Nosocomial Infections Surveillance System,Centers for Disease Control, Atlanta, GA.
❚ Improving Antibiotic Use
AntibiogramsTo guide physicians in the use of antibiotics,many hospitals provide “antibiograms” thatdescribe the susceptibility of commonly encoun-tered bacteria to various antibiotics. As shown intable 4-6, the vast majority of causes of bacterialinfections in both inpatients and outpatientsremain sensitive to the modern antibiotics. Onthe other hand, many Staph. aureus, coagulase-negative Staphylococci, and S. pneurnoniae areresistant to many commonly used antibiotics, andsome Enterococcus are resistant to all antibiotics.
FormulariesThe use of all drugs in hospitals is increas-
ingly controlled by hospital formularies, whichwere set up to control the costs of drugs. The for-mularies may have the added benefit of helpingto control the use of antibiotics and the antibioticresistance problem. In Denver, Colorado, areahospitals (North, 1993), a formulary is combinedwith a computerized antibiotic order form. Thissystem restricts some antibiotics to approvedindications, and use of others requires approval
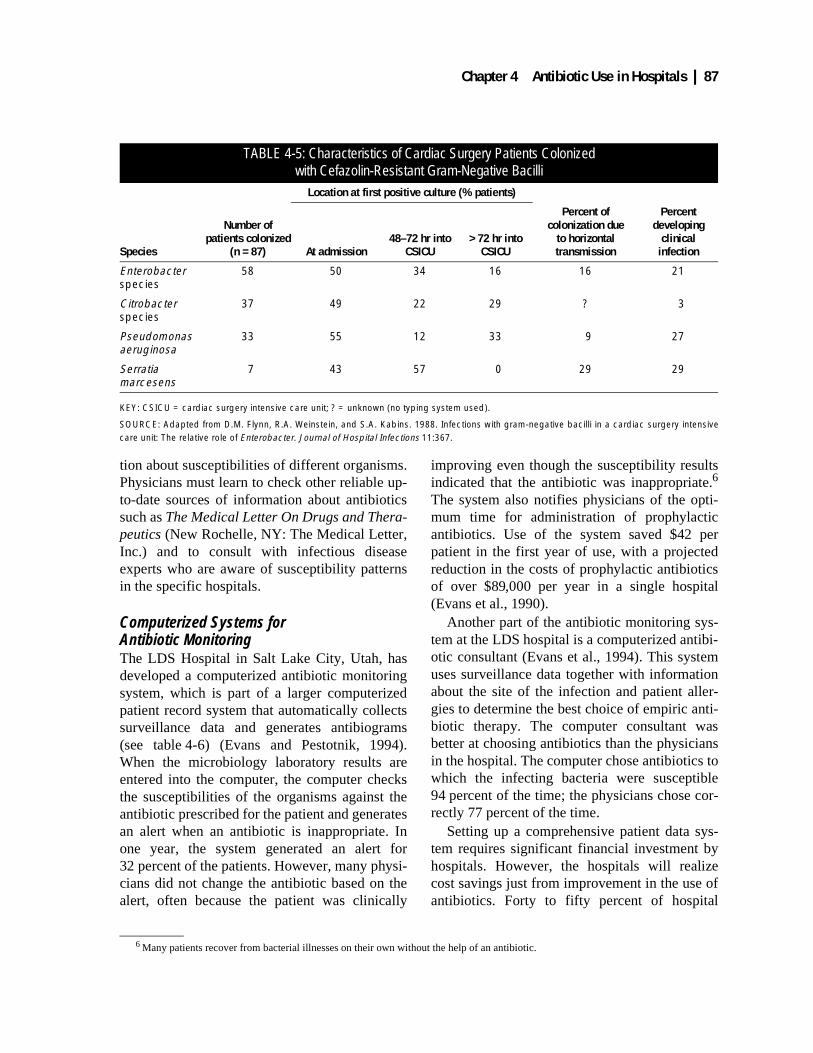
Chapter 4 Antibiotic Use in Hospitals | 87
tion about susceptibilities of different organisms.Physicians must learn to check other reliable up-to-date sources of information about antibioticssuch as The Medical Letter On Drugs and Thera-peutics (New Rochelle, NY: The Medical Letter,Inc.) and to consult with infectious diseaseexperts who are aware of susceptibility patternsin the specific hospitals.
Computerized Systems for Antibiotic MonitoringThe LDS Hospital in Salt Lake City, Utah, hasdeveloped a computerized antibiotic monitoringsystem, which is part of a larger computerizedpatient record system that automatically collectssurveillance data and generates antibiograms(see table 4-6) (Evans and Pestotnik, 1994).When the microbiology laboratory results areentered into the computer, the computer checksthe susceptibilities of the organisms against theantibiotic prescribed for the patient and generatesan alert when an antibiotic is inappropriate. Inone year, the system generated an alert for32 percent of the patients. However, many physi-cians did not change the antibiotic based on thealert, often because the patient was clinically
improving even though the susceptibility resultsindicated that the antibiotic was inappropriate.6
The system also notifies physicians of the opti-mum time for administration of prophylacticantibiotics. Use of the system saved $42 perpatient in the first year of use, with a projectedreduction in the costs of prophylactic antibioticsof over $89,000 per year in a single hospital(Evans et al., 1990).
Another part of the antibiotic monitoring sys-tem at the LDS hospital is a computerized antibi-otic consultant (Evans et al., 1994). This systemuses surveillance data together with informationabout the site of the infection and patient aller-gies to determine the best choice of empiric anti-biotic therapy. The computer consultant wasbetter at choosing antibiotics than the physiciansin the hospital. The computer chose antibiotics towhich the infecting bacteria were susceptible94 percent of the time; the physicians chose cor-rectly 77 percent of the time.
Setting up a comprehensive patient data sys-tem requires significant financial investment byhospitals. However, the hospitals will realizecost savings just from improvement in the use ofantibiotics. Forty to fifty percent of hospital
6 Many patients recover from bacterial illnesses on their own without the help of an antibiotic.
TABLE 4-5: Characteristics of Cardiac Surgery Patients Colonizedwith Cefazolin-Resistant Gram-Negative Bacilli
Location at first positive culture (% patients)
Species
Number of patients colonized
(n = 87) At admission48–72 hr into
CSICU> 72 hr into
CSICU
Percent of colonization due
to horizontal transmission
Percent developing
clinicalinfection
Enterobacter species
58 50 34 16 16 21
Citrobacter species
37 49 22 29 ? 3
Pseudomonas aeruginosa
33 55 12 33 9 27
Serratia marcesens
7 43 57 0 29 29
KEY: CSICU = cardiac surgery intensive care unit; ? = unknown (no typing system used).
SOURCE: Adapted from D.M. Flynn, R.A. Weinstein, and S.A. Kabins. 1988. Infections with gram-negative bacilli in a cardiac surgery intensivecare unit: The relative role of Enterobacter. Journal of Hospital Infections 11:367.
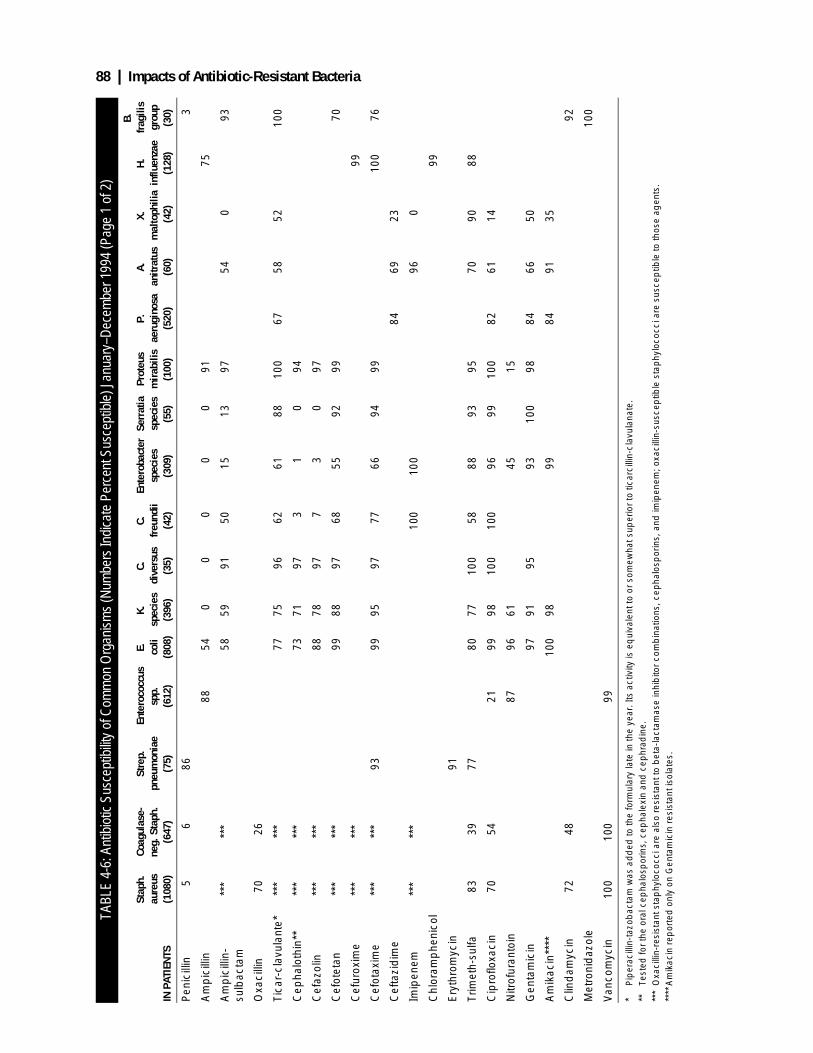
88 | Impacts of Antibiotic-Resistant Bacteria
TABL
E 4-
6: A
ntib
iotic
Sus
cept
ibilit
y of
Com
mon
Org
anis
ms
(Num
bers
Indi
cate
Per
cent
Sus
cept
ible
) Jan
uary
–Dec
embe
r 199
4 (P
age
1 of
2)
IN P
ATIE
NTS
Stap
h.
aure
us(1
080)
Coag
ulas
e-ne
g. S
taph
. (6
47)
Stre
p.
pneu
mon
iae
(75)
Ente
roco
ccus
sp
p.(6
12)
E. coli
(808
)
K.
spec
ies
(396
)
C.
dive
rsus
(3
5)
C.fr
eund
ii (4
2)
Ente
roba
cter
spec
ies
(309
)
Serr
atia
sp
ecie
s (5
5)
Prot
eus
mir
abili
s (1
00)
P.
aeru
gino
sa
(520
)
A.
anitr
atus
(6
0)
X.
mal
toph
ilia
(42)
H.
influ
enza
e (1
28)
B.
frag
ilis
grou
p (3
0)
Pen
icill
in5
686
3
Am
pic
illin
8854
00
00
091
75
Am
pic
illin
-su
lbac
tam
***
***
5859
9150
1513
9754
093
Oxa
cilli
n70
26
Tica
r-cl
avul
ante
***
***
*77
7596
6261
8810
067
5852
100
Cep
halo
thin
****
***
*73
7197
31
094
Cef
azol
in**
***
*88
7897
73
097
Cef
otet
an**
***
*99
8897
6855
9299
70
Cef
urox
ime
***
***
99
Cef
otax
ime
***
***
9399
9597
7766
9499
100
76
Cef
tazi
dim
e84
6923
Imip
enem
***
***
100
100
960
Chl
oram
phe
nico
l99
Ery
thro
myc
in91
Trim
eth-
sulfa
8339
7780
7710
058
8893
9570
9088
Cip
roflo
xaci
n70
5421
9998
100
100
9699
100
8261
14
Nitr
ofur
anto
in87
9661
4515
Gen
tam
icin
9791
9593
100
9884
6650
Am
ikac
in**
**10
098
9984
9135
Clin
dam
ycin
7248
92
Met
roni
daz
ole
100
Van
com
ycin
100
100
99
* P
iper
acill
in-t
azob
acta
m w
as a
dd
ed to
the
form
ular
y la
te in
the
year
. Its
act
ivity
is e
qui
vale
nt to
or
som
ewha
t sup
erio
r to
tica
rcill
in-c
lavu
lana
te.
**Te
sted
for
the
oral
cep
halo
spor
ins,
cep
hale
xin
and
cep
hrad
ine.
***
Oxa
cilli
n-re
sist
ant s
tap
hylo
cocc
i are
als
o re
sist
ant t
o b
eta-
lact
amas
e in
hib
itor
com
bin
atio
ns, c
epha
losp
orin
s, a
nd im
ipen
em; o
xaci
llin-
susc
eptib
le s
tap
hylo
cocc
i are
sus
cep
tible
to th
ose
agen
ts.
****
Am
ikac
in r
epor
ted
onl
y on
Gen
tam
icin
res
ista
nt is
olat
es.
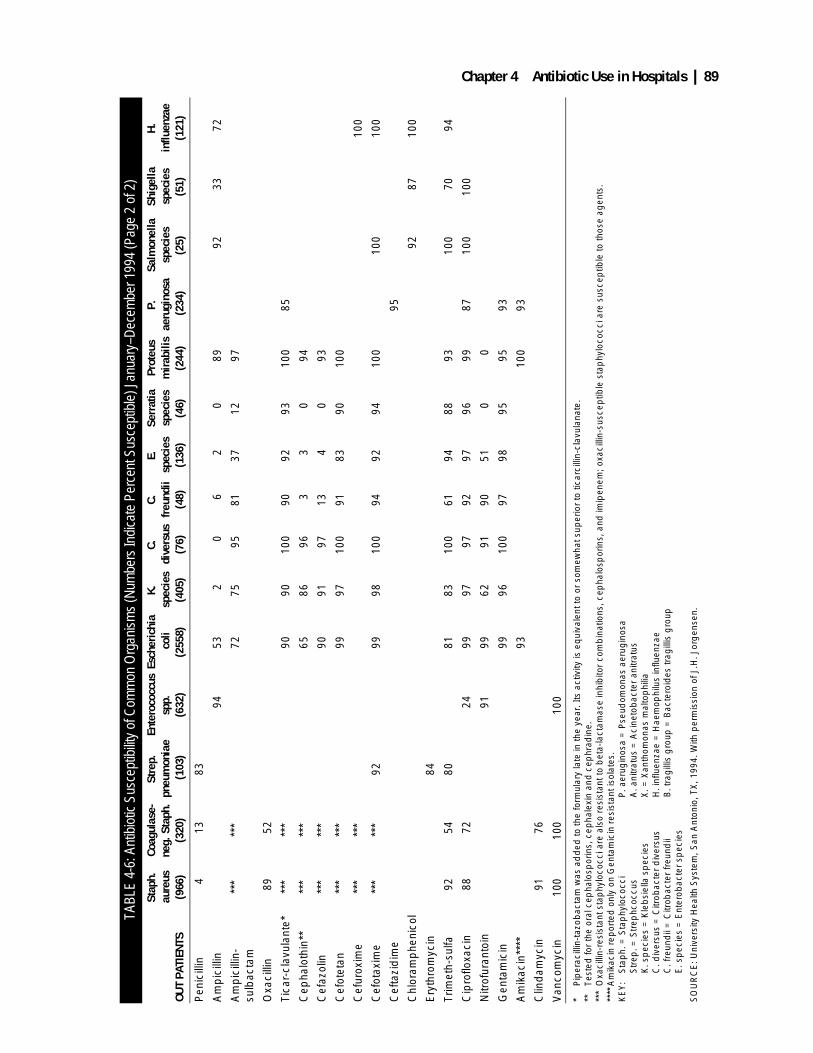
Chapter 4 Antibiotic Use in Hospitals | 89
TABL
E 4-
6: A
ntib
iotic
Sus
cept
ibilit
y of
Com
mon
Org
anis
ms
(Num
bers
Indi
cate
Per
cent
Sus
cept
ible
) Jan
uary
–Dec
embe
r 199
4 (P
age
2 of
2)
OUT
PATI
ENTS
Stap
h.
aure
us(9
66)
Coag
ulas
e-ne
g. S
taph
. (3
20)
Stre
p.
pneu
mon
iae
(103
)
Ente
roco
ccus
sp
p.(6
32)
Esch
eric
hia
col
i(2
558)
K.
spec
ies
(405
)
C.
dive
rsus
(7
6)
C.
freu
ndii
(48)
E.
spec
ies
(136
)
Serr
atia
sp
ecie
s (4
6)
Prot
eus
mira
bilis
(2
44)
P.
aeru
gino
sa (2
34)
Salm
onel
la
spec
ies
(25)
Shig
ella
sp
ecie
s(5
1)
H.
influ
enza
e (1
21)
Pen
icill
in4
1383
Am
pic
illin
9453
20
62
089
9233
72
Am
pic
illin
-su
lbac
tam
***
***
7275
9581
3712
97
Oxa
cilli
n89
52
Tica
r-cl
avul
ante
***
***
*90
9010
090
9293
100
85
Cep
halo
thin
****
***
*65
8696
33
094
Cef
azol
in**
***
*90
9197
134
093
Cef
otet
an**
***
*99
9710
091
8390
100
Cef
urox
ime
***
***
100
Cef
otax
ime
***
***
9299
9810
094
9294
100
100
100
Cef
tazi
dim
e95
Chl
oram
phe
nico
l92
8710
0
Ery
thro
myc
in84
Trim
eth-
sulfa
9254
8081
8310
061
9488
9310
070
94
Cip
roflo
xaci
n88
7224
9997
9792
9796
9987
100
100
Nitr
ofur
anto
in91
9962
9190
510
0
Gen
tam
icin
9996
100
9798
9595
93
Am
ikac
in**
**93
100
93
Clin
dam
ycin
9176
Van
com
ycin
100
100
100
* P
iper
acill
in-t
azob
acta
m w
as a
dd
ed to
the
form
ular
y la
te in
the
year
. Its
act
ivity
is e
qui
vale
nt to
or
som
ewha
t sup
erio
r to
tica
rcill
in-c
lavu
lana
te.
**
Test
ed fo
r th
e or
al c
epha
losp
orin
s, c
epha
lexi
n an
d c
ephr
adin
e.**
*O
xaci
llin-
resi
stan
t sta
phy
loco
cci a
re a
lso
resi
stan
t to
bet
a-la
ctam
ase
inhi
bito
r co
mb
inat
ions
, cep
halo
spor
ins,
and
imip
enem
; oxa
cilli
n-su
scep
tible
sta
phy
loco
cci a
re s
usce
ptib
le to
thos
e ag
ents
.**
**A
mik
acin
rep
orte
d o
nly
on G
enta
mic
in r
esis
tant
isol
ates
.K
EY
:S
tap
h. =
Sta
phy
loco
cci
P. a
erug
inos
a =
Pse
udom
onas
aer
ugin
osa
Str
ep. =
Str
ephc
occu
s A
. ani
trat
us =
Aci
neto
bac
ter
anitr
atus
K. s
pec
ies
= K
leb
siel
la s
pec
ies
X. =
Xan
thom
onas
mal
top
hilia
C. d
iver
sus
= C
itrob
acte
r d
iver
sus
H. i
nflu
enza
e =
Hae
mop
hilu
s in
fluen
zae
C. f
reun
dii
= C
itrob
acte
r fr
eund
ii B
. tra
gill
is g
roup
= B
acte
roid
es tr
agill
is g
roup
E. s
pec
ies
= E
nter
obac
ter
spec
ies
SO
UR
CE
: Uni
vers
ity H
ealth
Sys
tem
, San
Ant
onio
, TX
, 199
4. W
ith p
erm
issi
on o
f J.H
. Jor
gen
sen.

90 | Impacts of Antibiotic-Resistant Bacteria
BOX 4-3: “Food-Borne” Outbreak of Expensive Antibiotic Usein Community Teaching Hospital
To the Editor—Drug utilization review assures cost-effective use of medications in hospitals. Wepresent an example of drug utilization review that began with the identification of an “index case” of acostly therapeutic decision. Subsequent investigation lead to the identification of a prescribing outbreakas well as its probable source.
Report of a Case—A 32-year-old man had been on a camping trip and noted an insect bite at the topmargin of his sock. The next day he noted redness and swelling at the site of the bite. The third day hewas febrile and the redness began to spread. On the fourth day, red streaks extended 15 cm above thesite of injury. He felt ill and came to the emergency department. His examination demonstrated a temper-ature of 39.4°C, sickly appearance, and a tender cellulitis of his lower leg. Blood pressure was normaland he did not have a truncal rash. Therapy with a new, expensive, broad-spectrum antibiotic was initi-ated. When asked about his antibiotic choice, the admitting intern noted at morning report that he hadplanned on giving penicillin or nafcillin, but had been overruled by the supervising resident who insistedon a “more modern choice for a severely ill patient.”
Comment—Following discussion of this case, we evaluated the use of the new antibiotic in our hospi-tal. We found that use had transiently increased following its addition to our formulary in February 1994,then abruptly increased in June and July. After conducting interviews with our house officers, it wasrevealed that an extravagant dinner party had been held for incoming and current house staff the thirdweek of June. The sponsor of this dinner was the manufacturer of the antibiotic. The increase in use ofthis agent bore a striking temporal association with this dinner. Furthermore, the prescribing resident hadattended the dinner and directed the admitting intern to use the drug instead of nafcillin.
The prescribed antibiotic exhibits a broad spectrum of activity, including β-lactamase-producingstrains of staphylococci, Haemophilus influenzae, anaerobes, and facultative gram-negative rods. Theagent would be expected to be effective in most settings where nafcillin might be used. Although thisagent is not contraindicated in treating uncomplicated cellulitis, it is much more expensive ($183.20 perday) than other effective drugs such as nafcillin ($84 per day). In this single case, the daily excess cost oftherapy would approximate $100. The relationship between pharmaceutical marketing maneuvers andprescribing is controversial. Previous ecological studies have found an association between educational“enticements” and hospital formulary additions and prescribing trends. However, we are not aware of adetailed case description where a more expensive therapeutic choice was made when less expensivetherapeutic alternatives were indicated. We do not know if the resident’s attendance at the dinner causedhis therapeutic choice. However, the striking epidemiological association between resident attendance atthis drug company-sponsored event and the subsequent changes in hospital-wide prescribing practicesshould prompt training programs to be wary of such outside sources of medical education.
SOURCE: Quoted from R.I. Shore and W.L. Greene, letter to the editor, Journal of the American Medical Association273(24):1908. Copyright 1995, American Medical Association.

Chapter 4 Antibiotic Use in Hospitals | 91
FIGURE 4-6: An Antibiotic Advertisement from a Medical Journal
SOURCE: A major pharmaceutical company.

92 | Impacts of Antibiotic-Resistant Bacteria
pharmacy budgets are for antibiotics, and one-fourth of that in some hospitals is for vancomy-cin alone (Modern Healthcare, 1994). Eliminat-ing unnecessary use of antibiotics will decreasetotal pharmacy expenditures. Treating infectionswith appropriate antibiotics and administeringprophylactic antibiotics with appropriate timingwill also increase the quality of patient care anddecrease the number of days spent in the hospi-tal. (OTA’s report Bringing Health Care Online:The Role of Information Technologies, Septem-ber 1995, discusses costs and benefits of comput-erized patient record systems.)
Practice GuidelinesPractice guidelines, or practice protocols, aremedical guidelines that “encompass a broadrange of strategies designed to assist practitio-ners in the clinical decision-making process”(Shanz, 1993). More specifically, they are “stan-dardized specifications for care developed by aformal process that incorporates the best scien-tific evidence of effectiveness with expert opin-ion” (Leape, 1990). These guidelines are set byexperts from specific areas of the medical profes-sion to advise about recommended standards ofcare. For example, the goal of practice guidelinesestablished by the Agency for Health Care Policyand Research, a federal agency empowered toestablish practice guidelines, is to encouragephysicians and other health care providers tochange their practice behavior, thus improvingpatient care, patient outcomes, and quality of life(AHCPR, 1994).
Practice guidelines on infection control or theprudent use of antibiotics might be helpful incontrolling antibiotic resistance. For example,practice guidelines might specify that older anti-biotics such as amoxicillin be tried for commu-nity-acquired infections before newer, broaderspectrum antibiotics are used. Under managedcare, insurers may adopt guidelines such as thesebecause they will save money as older antibioticsare generally much less expensive than newerantibiotics.
Practice guidelines may also be of use in med-ical malpractice litigation. A major difficulty in
medical malpractice cases is establishing theappropriate standard of care before “layperson”decision-makers on juries. Practice guidelineshave the potential to reduce such difficulties. Byestablishing an unbiased standard of care, prac-tice guidelines should “significantly reduce themost vexing problem in malpractice litigation:the battle of the experts” (West, 1994). In theory,a physician could rely on the practice guidelineas the appropriate standard of care without hav-ing to worry whether a judge or jury, in a medi-cal malpractice case, would consider the careadministered appropriate. The only remainingissues to be determined in medical negligence lit-igation would be whether the practice guideline“is relevant to the case at hand, and whether it isappropriate to use the [guideline] to establish thestandard of care” (West, 1994).
On the other hand, practice guidelines whichsuggest any benefit from the use of antibioticsmay be used as evidence against the physician inthe case of a bad outcome. For example, a guide-line on the treatment of otitis media with effusionpublished by the Agency for Health Care Policyand Research concludes:
Meta-analysis for Guideline developmentshowed a 14 percent increase in the probabilitythat otitis media with effusion would resolvewhen antibiotic therapy was given versus notreatment. . . . When this small improvement inresolution of otitis media with effusion isweighed against the side effects and cost ofantibiotic therapy, antibiotic therapy may not bepreferable to observation in management of oti-tis media with effusion in the otherwise healthyyoung child. . . . To assist in making choices formanagement of otitis media with effusion,health care providers need to inform parentsfully as to the side effects and costs of antibiotictherapy, as well as the benefits and harms ofother options for care (AHCPR, 1994).
A physician who elects not to prescribe anantibiotic, foregoing the 14-percent increasedprobability that the condition “would resolve,”might be held legally liable for any negative out-come. Such potential liability might encouragephysicians to prescribe antibiotics even when

Chapter 4 Antibiotic Use in Hospitals | 93
they may not be necessary. Further, the aboveguidelines do not instruct physicians to considerthe spread of antibiotic resistance in the decisionto prescribe antibiotics. If practice guidelines aregoing to have an effect on promoting prudentantibiotic use, they have to acknowledge that thebenefit to a few patients from routine use ofnewer and broader spectrum antibiotics may beoutweighed by the public health benefitsexpected from reducing the prevalence of antibi-otic-resistant bacteria.
One concern of practice guidelines relevant toantibiotic use is that national standards of con-duct do not adequately reflect the localizedaspect of antibiotic-resistant bacteria outbreaks.The National Health Lawyers Associationaddressed this concern in its 1995 ColloquiumReport on Legal Issues Related to Clinical Prac-tice Guidelines, which conceded that “[s]omelocal adaptation of national guidelines is proba-bly inevitable and may be useful, because evenwell-developed guidelines may have gaps andmay not foresee significant local objectives orconstraints” (National Health Lawyers Associa-tion Colloquy, 1995). One solution may be theuse of an online computer system that allowshealth care practitioners in a particular geo-graphic area to consult with each other and localexperts concerning appropriate local adaptationsto practice guidelines (Meyers, 1995). Such asystem would also allow health care practitionersto disseminate the specifics of their cases, as wellas establish a record of compliance with the prac-tice guidelines in the event of future litigation(Meyers, 1995).
COSTS OF CONTROLLING THE EMERGENCE AND SPREAD OF ANTIBIOTIC-RESISTANT BACTERIAHospitals cannot charge costs of infection con-trol procedures and the monitoring of antibiotic-resistant bacteria directly to insurance compa-nies. As a result, although these proceduresimprove the quality of patient care, hospitals’efforts to minimize costs may retard spending onthem. Haley et al. (1987) commented that hospi-
tals might not be placing enough emphasis oninfection control because “the direction and mag-nitude of the financial incentive to prevent noso-comial infections are not clear to many hospitaladministrators.” They analyzed the financialincentives for hospitals to prevent nosocomialinfections under the prospective payment systemand concluded that
Assuming an average nosocomial infectionrate of 5.7 percent, one would expect. . . a hos-pital with 10,000 admissions annually to haveapproximately 570 nosocomial infections peryear in the absence of an effective infectioncontrol program. If the average 1985 marginalcost of providing extra care for a nosocomialinfection were approximately $1800, the totalcost of treating these infections would amountto approximately $1 million per year, not count-ing physicians’ fees or medicolegal losses. . . .From the nationwide SENIC project evaluation,we know that at least 32 percent of the infec-tions can be prevented, thus indicating that aneffective infection control program could pro-duce a gross financial savings of approximately$305,000 per year. . . nearly five times the costsof the program.
A computerized antibiotic monitoring system,such as that of the LDS Hospital, reduces costsboth by controlling the use of antibiotics andreducing the length of hospital stays, but the LDSsystem has been in development for 20 years, itis based on obsolete computer technology, and itis not exportable. Developing a system on cur-rent computer technology will take a significantinvestment in research and development. Givenall the costs involved in control and monitoring,it would be useful to calculate the total cost tohospitals of antibiotic resistance to judgewhether infection control procedures and moni-toring of antibiotic-resistant bacteria will have afinancial payoff.
Many different factors can be considered in acalculation of the cost of antibiotic-resistant bac-teria: the direct cost of time in the hospital, thecosts of extra physician visits when antibioticsare ineffective, the extra hospitalizations due tocommunity-acquired resistant infections, and thecosts of newer antibiotics to replace antibiotics

94 | Impacts of Antibiotic-Resistant Bacteria
such as penicillin to which organisms havebecome resistant. To those must be added theindirect costs to patients from lost days of work,increased illness, and, at worst, death. It is diffi-cult to estimate the costs of all of these factors.
Phelps (1989) made such an estimate and con-cluded that antibiotic-resistant bacteria cost thenation between $0.1 billion and $30 billion annu-ally. Use of different values for the value of a lifeaccounted for almost all of the 300-fold range inthe estimate. The National Foundation for Infec-tious Disease (1990) estimated that the costs ofnosocomial infections caused by antibiotic-resis-tant bacteria could be as high as $4 billion annu-ally, and CDC has estimated the costs of allnosocomial infections at $4.5 billion per year, anestimate that includes costs from both antibiotic-resistant and susceptible infections.
Here, OTA estimates the effects of antibiotic-resistant bacteria on the costs of some hospital-izations. The national costs of five classes ofnosocomial infections—surgical wound infec-tions, pneumonia, bacteremias, urinary tractinfections, and others—are taken from the resultsof the SENIC project (see table 4-1). Those costsare shown on the first data line in table 4-7 (forinstance, the cost of all surgical wound infectionsis $1.6 billion annually). The calculation of thecosts of each of the infections caused by each ofsix different antibiotic-resistant bacteria is illus-trated by the example of MRSA-associated sur-gical wound infections. Staph. aureus isassociated with 19 percent of all surgical woundinfections, and 15 percent of all Staph. aureus isMRSA. Therefore, the hospital cost of MRSA-associated surgical wound infections is$50 million [$1.6 billion × 0.19 × 0.15 =$50 million]. Repeating this process for the fivekinds of infections and the six different antibi-otic-resistant bacteria produces an annual total of$661 million (1992) for hospital costs.
Using the estimate of Holmberg, Solomon andBlake (1987) that antibiotic resistance doublesthe cost of nosocomial infections, the minimumextra cost of antibiotic-resistant bacteria in hos-pitals is $661 million annually (1992 dollars) andthe minimum total cost of antibiotic-resistant
bacteria in hospitals is $1.3 billion annually(1992 dollars). The actual hospital costs arebound to be much higher as this calculation con-siders only six species of bacteria, and in somecases considers strains of bacteria that are resis-tant to only one antibiotic and not other strains ofthe same bacteria that are resistant to other anti-biotics. Further, the trends in antibiotic resistanceindicate that the number of antibiotic-resistantinfections is likely to be increasing rapidly.Finally, the OTA estimate considers only onefactor among many that increase the costs ofantibiotic-resistant bacteria; it ignores costs ofother infections, costs of days of work lost, andpost-hospital care, and other major costs. Forthese reasons, the OTA estimate of $1.3 billionmust be considered a minimum estimate .
CONCLUSIONSTwenty-five to 35 percent of all hospitalizedpatients receive antibiotics, which producesenormous pressure for the selection of antibiotic-resistant bacteria. The result of that pressure isincreasing frequencies of antibiotic-resistant bac-teria in hospitals: Some strains of vancomycin-resistant Enterococcus are now resistant to allFDA-approved antibiotics, and some strains ofStaphylococcus aureus, a common cause ofnosocomial infections, are resistant to all antibi-otics except vancomycin. Many experts fear theemergence and spread of Staph. aureus strainsresistant to all antibiotics, including vancomycin,which would pose a major health care crisis.
Two avenues are open to reduce the spread ofantibiotic-resistant bacteria. One is infection con-trol to reduce the rate of hospital infections, andthe other is the reduction in the use of antibioticsto reduce selection pressures. While infectioncontrol programs have worked well in someinstitutions, similar programs have produced nopositive results elsewhere. The mixed resultsindicate that more research into what makes sys-tems work and why is needed to guide infectioncontrol efforts. Formularies, lists of drugs thatare available for use in a hospital, were estab-lished to control drug costs, but they can be tied
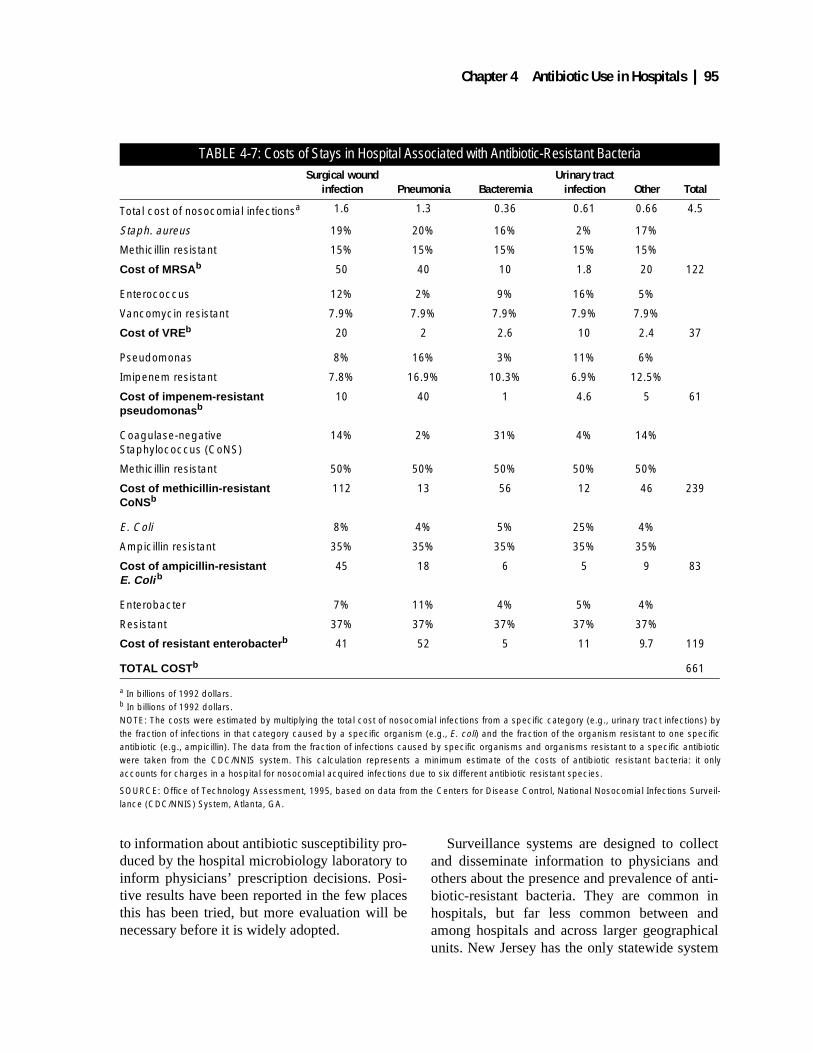
Chapter 4 Antibiotic Use in Hospitals | 95
to information about antibiotic susceptibility pro-duced by the hospital microbiology laboratory toinform physicians’ prescription decisions. Posi-tive results have been reported in the few placesthis has been tried, but more evaluation will benecessary before it is widely adopted.
Surveillance systems are designed to collectand disseminate information to physicians andothers about the presence and prevalence of anti-biotic-resistant bacteria. They are common inhospitals, but far less common between andamong hospitals and across larger geographicalunits. New Jersey has the only statewide system
TABLE 4-7: Costs of Stays in Hospital Associated with Antibiotic-Resistant BacteriaSurgical wound
infection Pneumonia BacteremiaUrinary tract
infection Other Total
Total cost of nosocomial infectionsa 1.6 1.3 0.36 0.61 0.66 4.5
Staph. aureus 19% 20% 16% 2% 17%
Methicillin resistant 15% 15% 15% 15% 15%
Cost of MRSA b 50 40 10 1.8 20 122
Enterococcus 12% 2% 9% 16% 5%
Vancomycin resistant 7.9% 7.9% 7.9% 7.9% 7.9%
Cost of VRE b 20 2 2.6 10 2.4 37
Pseudomonas 8% 16% 3% 11% 6%
Imipenem resistant 7.8% 16.9% 10.3% 6.9% 12.5%
Cost of impenem-resistant pseudomonas b
10 40 1 4.6 5 61
Coagulase-negative Staphylococcus (CoNS)
14% 2% 31% 4% 14%
Methicillin resistant 50% 50% 50% 50% 50%
Cost of methicillin-resistant CoNSb
112 13 56 12 46 239
E. Coli 8% 4% 5% 25% 4%
Ampicillin resistant 35% 35% 35% 35% 35%
Cost of ampicillin-resistant E. Coli b
45 18 6 5 9 83
Enterobacter 7% 11% 4% 5% 4%
Resistant 37% 37% 37% 37% 37%
Cost of resistant enterobacter b 41 52 5 11 9.7 119
TOTAL COSTb 661
a In billions of 1992 dollars.b In billions of 1992 dollars.NOTE: The costs were estimated by multiplying the total cost of nosocomial infections from a specific category (e.g., urinary tract infections) bythe fraction of infections in that category caused by a specific organism (e.g., E. coli) and the fraction of the organism resistant to one specificantibiotic (e.g., ampicillin). The data from the fraction of infections caused by specific organisms and organisms resistant to a specific antibioticwere taken from the CDC/NNIS system. This calculation represents a minimum estimate of the costs of antibiotic resistant bacteria: it onlyaccounts for charges in a hospital for nosocomial acquired infections due to six different antibiotic resistant species.
SOURCE: Office of Technology Assessment, 1995, based on data from the Centers for Disease Control, National Nosocomial Infections Surveil-lance (CDC/NNIS) System, Atlanta, GA.

96 | Impacts of Antibiotic-Resistant Bacteria
in the country, and CDC is only now establishinga nationwide system for one kind of antibiotic-resistant bacterium. In addition, a number of pri-vately supported surveillance systems collectdata for pharmaceutical companies, but, under-standably, those systems collect information fortheir clients rather than for general public healthinformation. On the international level, WHO-NET collects data from over 100 institutionsaround the world. Chapter 1 discusses some fea-tures that could be built into a national surveil-lance system directed at antibiotic-resistantbacteria and offers an option for its implementa-tion.
One estimate of the total costs associated withantibiotic-resistant bacteria had a range of$100 million to $30 billion annually, with mostof the 300-fold range in cost coming from vary-ing estimates of the value of a human life, andanother estimate said that the costs could be up to$4 billion annually. OTA estimates the minimalextra hospital costs associated with five kinds ofnosocomial infections caused by antibiotic-resis-tant bacteria to be $1.3 billion per year. The totalcosts would certainly be certainly higher whenhospital costs of other antibiotic-resistant bacte-rial infections and non-hospital costs are consid-ered.
REFERENCESBallow, C.H., and J.J. Schentag. 1992. Trends in
antibiotic utilization and bacterial resistance.Report of the National Nosocomial Resis-tance Surveillance Group. DiagnosticMicrobiology and Infectious Disease15(Suppl. 2):37S–42S.
Burke, J.F. 1961. The effective period of preven-tive antibiotic action in experimental inci-sions and dermal lesions. Surgery 50:161–168.
Classen, D.C., R.S. Evans, S.L. Pestotnik, et al.1992. The timing of prophylactic adminis-tration of antibiotics and the risk of surgical-wound infection. New England Journal ofMedicine 326(5): 281–286.
Doebbeling, B.N., G.L. Stanley, C.T. Sheetz, etal. 1992. Comparative efficacy of alternativehand-washing agents in reducing nosoco-mial infections in intensive care units. NewEngland Journal of Medicine 327(2): 88–93.
Eickoff, T.C. 1992. Antibiotics and nosocomialinfections. In: J.V. Bennett, and P.S. Brach-man (eds.). Hospital Infections Third Edi-tion. Boston, MA. Little, Brown andCompany.
Evans, R.S., and S.L. Pestotnik. 1993. Applica-tions of medical informatics in antibiotictherapy. In: J.A. Poupard, L.R. Walsh, andB. Kelger (eds.) Antimicrobial SusceptibilityTesting: Critical Issues for the 90s. NewYork, NY. Plenum Press, pp. 87–96.
Evans, R.S., S.L. Pestotnik, J.P. Burke, et al.1990. Reducing the duration of prophylacticantibiotic use through computer monitoringof surgical patients. DICP, The Annals ofPharmacotherapy 24:351–354.
Evans, R.S., D.C. Classen, S.L. Pestotnik, et al.1994. Improving empiric antibiotic selectionusing computer decision support. Archivesof Internal Medicine 154(8):878–884.
Garner, J.S. 1993. The CDC hospital infectioncontrol practices advisory committee. Amer-ican Journal of Infection Control 21(3):160–162.
Goldmann, D. and E. Larson. 1992. Hand-wash-ing and nosocomial infections [editorialcomment]. New England Journal of Medi-cine 327(2): 120–122.
Haley, R.W. 1991. Measuring the costs of noso-comial infections: Methods for estimatingeconomic burden on the hospital. AmericanJournal of Medicine 91 (Suppl. 3B):32S–38S.
Haley, R.W. 1992. Cost-benefit analysis ofinfection control programs. In: J.V. Bennettand P.S. Brachman (eds.) Hospital Infec-tions Third Edition, Boston, MA. Little,Brown and Company, pp. 507–532.
Haley, R.W., J.W. White, D.H. Culver, et al.1987. The financial incentive for hospitals toprevent nosocomial infections under the pro-spective payment system. An empirical
Chapter 4 Antibiotic Use in Hospitals | 97
determination from a nationally representa-tive sample. Journal of the American Medi-cal Association 257(12):1611–1614.
Haley, R.W., D.H. Culver, J.W. White, et al.1985. The nationwide nosocomial infectionrate: a new need for vital statistics. AmericanJournal of Epidemiology 121(2):159–167.
Holmberg, S.D., S.L. Solomon, and P.A. Blake.1987. Health and economic impacts of anti-microbial resistance. Reviews of InfectiousDiseases 9(6):1065–1078.
Institute of Medicine. 1992. Microbial Threats toHealth in the United States. WashingtonD.C., National Academy Press.
Joint Commission on Accreditation of Health-care Organizations. Feb. 1995. IMSystemGeneral Information. Oak Terrace, IL, p. 15.
Jewell, M. 1994. Cost-containment using anoutcome-based best practice model for themanagement of MRSA. Journal of Chemo-therapy VI(Suppl. 2):35–39.
Kernodle, D.S., and A.B. Kaiser. 1990. In: Man-dell, G.L., J.E. Bennett, and R. Dolin (eds.)Mandell, Douglas and Bennett’s Principlesand Practice of Infectious Diseases. NewYork, NY. Churchill Livingstone, Inc.
Kollef, M.H. 1994. Antibiotic use and antibioticresistance in the intensive care unit: Are wecuring or creating disease? Heart and Lung23:363–367.
Kollef, M.H. 1994. The role of selective diges-tive tract decontamination on mortality andrespiratory tract infections: A meta-analy-sis. Chest 105:1101–1108.
Leape, L.L. 1990. Practice guidelines and stan-dards: an overview. 16 Quality Review Bul-letin, pp. 42–49.
Loeb, J.M., D.S. O’Leary. 1995. A call for col-laboration in performance measurement.(From the Joint Commission on Accredita-tion of Healthcare Organizations). Journalof the American Medical Association273(18):1405.
Lonks, J.R., Durkin, M.R., Meyerhoff, A.N., etal. 1995. Meningitis due to ceftriaxone-resis-tant Streptococcus pneumoniae. NewEngland Journal of Medicine 332:893–894.
Loulergue, J., A. Audurier, J.M. DeLarbre, et al.1994. Changes in microbial ecology and useof cloxacillin. Journal of Hospital Infection27(4):275–283.
Mandell, G.L., J.E. Bennett, and R. Dolin. 1990.Mandell, Douglas and Bennett’s Principlesand Practice of Infectious Diseases. NewYork, NY. Churchill Livingstone, Inc.
Mandell, G.L., and M.A. Sande. 1990. Antimi-crobial agents: penicillins, cephalosporins,and other beta-lactam antibiotics. In: A.GGilman, T.W. Rall, A.S. Nies, et al. (eds.)Goodman and Gilman’s The Pharmacologi-cal Basis of Therapeutics, Eighth Edition.New York, NY. Pergamon Press, pp. 1065–1097.
Martin, M.A. 1994. Methicillin-resistant Staphy-lococcus aureus: the persistent resistantnosocomial pathogen. Current Clinical Top-ics in Infectious Diseases 14:170–91.
Martone, W.J., W.R. Jarvis, D.H. Culver, et al.1992. Incidence and nature of endemic andepidemic nosocomial infections. In: J.V.Bennett, and P.S. Brachman (eds.) HospitalInfections Third Edition. Boston, MA. Little,Brown and Company, pp. 577–596.
McGowan, Jr., J.F. 1994. Do intensive hospitalantibiotic control programs prevent thespread of antibiotic resistance? InfectionControl and Hospital Epidemiology15(7):478–483.
Meyers, K., Chief of Infectious Diseases andHospital Epidemiologist, Baptist MedicalCenter. Feb. 21, 1995. Personal communica-tion.
Murray-Leisure, K.A., Geib, S., Graceley, D. etal. 1990. Control of epidemic methicillin-resistant Staphylococcus aureus. InfectionControl and Hospital Epidemiology11(7):343–350.
National Foundation for Infectious Disease.1990. Press release at Interscience Confer-ence on Antimicrobial Agents and Chemo-therapy. Reported in D. North. 1993.
National Health Lawyers Association Colloquy.1995. Legal Issues Related to Clinical Prac-tice Guidelines. vol. 47.
98 | Impacts of Antibiotic-Resistant Bacteria
Noble, W.C., Z. Virani, and R.G. Cree. 1992.Co-transfer of vancomycin and other resis-tance genes from Enterococcus faecalisNCTC 12201 to Staphylococcus aureus.FEMS-Microbiol-Lett. 72(2): 195–198.
North, D. 1993. Controlling the Costs of Antibi-otic Resistance. Clinical Therapeutics15(Suppl. A):3–11.
Phelps, C.E. 1989. Bug/drug resistance. Some-times less is more. Medical Care 27:194–203.
Rosdahl, V.T., and A.M. Knudson. 1991. Thedecline of methicillin resistance among Dan-ish Staphylococcus aureus strains. InfectionControl and Hospital Epidemiology12(2):83–88.
Rosendal, K., O. Jessen, M.W. Bentzon, et al.1977. Antibiotic policy and spread of Sta-phylococcus Aureus strains in Danish hospi-tals, 1969–1974. Acta Pathologica etMicrobiologica. Scandinavica (Sect. B)85:143–152.
Rotter, M. 1988. Are models useful for testinghand antiseptics? Journal of Hospital Infec-tions 11 (Suppl. A):236–243.
Sanford, J.P. 1992. Forward. In: J.V. Bennett,and P.S. Brachman (eds.) Hospital Infec-tions Third Edition. Boston, MA. Little,Brown and Company.
Scott, L. June 13, 1994. Restraint on use of anti-biotics urged. Modern Healthcare, p. 47.
Shanz, S.J. Fall 1993. The emerging status ofpractice parameters. 7 Medical Staff Counsel31.
Siegel, J.D., G.H. McCracken Jr., N. Threlkeld,et al. 1980. Single-dose penicillin prophy-laxis against neonatal group B streptococcalinfections. A controlled trial in 18,738 new-born infants. New England Journal of Medi-cine 303:769–775.
Silber, J.L., S.M. Paul, G. Crane, et al. 1994.Influence of hospital antibiotic policy andusage on the incidence of vancomycin-resis-tant enterococcal (VRE) bacteremia.Abstract. Infection Control and HospitalEpidemiology 15(4):32.
Simmons, B., J. Bryant, K. Neiman, et al. 1990.The Role of Handwashing in Prevention ofEndemic Intensive Care Unit Infections.Infection Control and Hospital Epidemiol-ogy 11(11):589–594.
Spink, W.W., and V. Ferris. 1945. Quantitativeaction of penicillin inhibitor from penicillin-resistant strains of staphylococci. Science102:221.
St. Paul Fire & Marine Insurance Co. 1995. 1994Annual report to policyholders, pp. 4–5.
Strausbaugh, L.J., C. Jacobson, D.L. Sewell, etal. 1992. Antimicrobial therapy for methicil-lin-resistant Staphylococcus aureus coloni-zation in residents and staff of a veteransaffairs nursing home care unit. InfectionControl and Hospital Epidemiology13(3):151–159.
The Medical Letter on Drugs and Therapeutics.1994. Handbook of Antimicrobial Therapy.New Rochelle, NY. The Medical Letter, Inc.
U.S. Congress, Office of Technology Assess-ment. September 1995. Bringing HealthCare Online: The Role of Information Tech-nologies, Washington, DC. U.S. Govern-ment Printing Office.
U.S. Department of Public Health, Public HealthService, Agency for Health Care Policy andResearch. July 1994. Clinical PracticeGuideline Number 12: Otitis Media withEffusion in Young Children. AHCPR Pub.No. 94-0622. Rockville, MD.
U.S. Department of Public Health, Public HealthService, Centers for Disease Control. 1995.Morbidity and Mortality Weekly Report44:27.
Waldvogel, F.A. 1995. Staphylococcus aureus(including toxic shock syndrome). In: G.L.Mandell, J.E. Bennett, and R. Dolin (eds.)Mandel, Douglas and Bennett’s Principlesand Practice of Infectious Diseases Fourthedition. New York, NY. Churchill Living-stone, Inc., p. 1757.
Wenzel, R.P. 1992. Preoperative antibiotic pro-phylaxis. New England Journal of Medicine326(5):337–339.

Chapter 4 Antibiotic Use in Hospitals | 99
Westh, H., J.O. Jarlov, H. Kjersem, et al. 1992.The disappearance of multiresistant Staphy-lococcus aureus in Denmark: changes instrains of the 83A complex between 1969and 1989. Clinical Infectious Diseases14(6):1186–1194.
Willy, M.E., G.L. Dhillon, N.L. Loewen, et al.1990. Adverse exposures and universal pre-cautions practices among a group of highly
exposed health professionals. Infection Con-trol and Hospital Epidemiology 11(7):351–356.
Yu, V.L., G.P. Stoehr, R.C. Starling, et al.. 1991.Empiric antibiotic selection by physicians:evaluation of reasoning strategies. Ameri-can Journal of the Medical Sciences301:165–172.
| 101
5Antibiotic
Development
he fact that U.S. Food and Drug Admin-istration (FDA) approved no new antibi-otics in 1994 has led to fear that there areno new ideas for antibiotics or that there
are insufficient financial incentives for new anti-biotic development. Even the information that 13new antibiotics are currently awaiting FDAapproval, and that two-thirds of the 53 antibioticsdeveloped by drug companies since 1960received FDA approval after 1980 (ModernHealthcare, 1994) must be tempered by addi-tional information. The 13 antibiotics awaitingapproval are not “new” in terms of new mecha-nisms of action. They are derivatives or newapplications or formulations of antibioticsalready on the market.
As shown in figure 5-1 (and discussed below)several years elapse between the discovery of achemical with antibiotic activity and its reachingthe market. The scarcity or abundance of newantibiotics is dependent on many factors, some ofwhich are described in this chapter, but some ofthe decisions necessary for the appearance ofnew antibiotics in 1995 were made years ago.
This chapter reviews general considerations inthe development of new antibiotics and describessome antibiotics that are now in use and howresearchers are attempting to modify them to
extend their usefulness. It also discusses thesearch for new antibiotics using new chemicaland molecular biology knowledge and tech-niques as well as the search for new antibiotics inbiological materials not formerly examined. Italso reviews briefly some aspects of drug devel-opment and approval (those issues are covered ingreater depth in OTA’s 1993 report Pharmaceu-tical R&D: Risks, Costs, and Rewards).
DESIGNING NEW ANTIBIOTICSDevelopment of almost any drug is a matter ofscience and serendipity, and antibiotics are nodifferent. Traditional methods, like screening ofsoil and biological samples—“panning” for com-pounds—have been partly replaced by computer-ized modeling, recombinant DNA technologies,new methods of chemical synthesis, and otheradvances (Levy 1992, p. 39). Nevertheless, look-ing for antibiotic activity in biological materialsas exotic as frogs and the silk glands of moths isa part of current research.
No matter how chemicals with antibioticproperties are derived, they must still be evalu-ated in the microbiology laboratory, laboratoryanimals, and ultimately, humans. “Preclinicalstudies” are tests for efficacy and toxicity in lab-oratory animals, and “phases I, II, and III” are
T
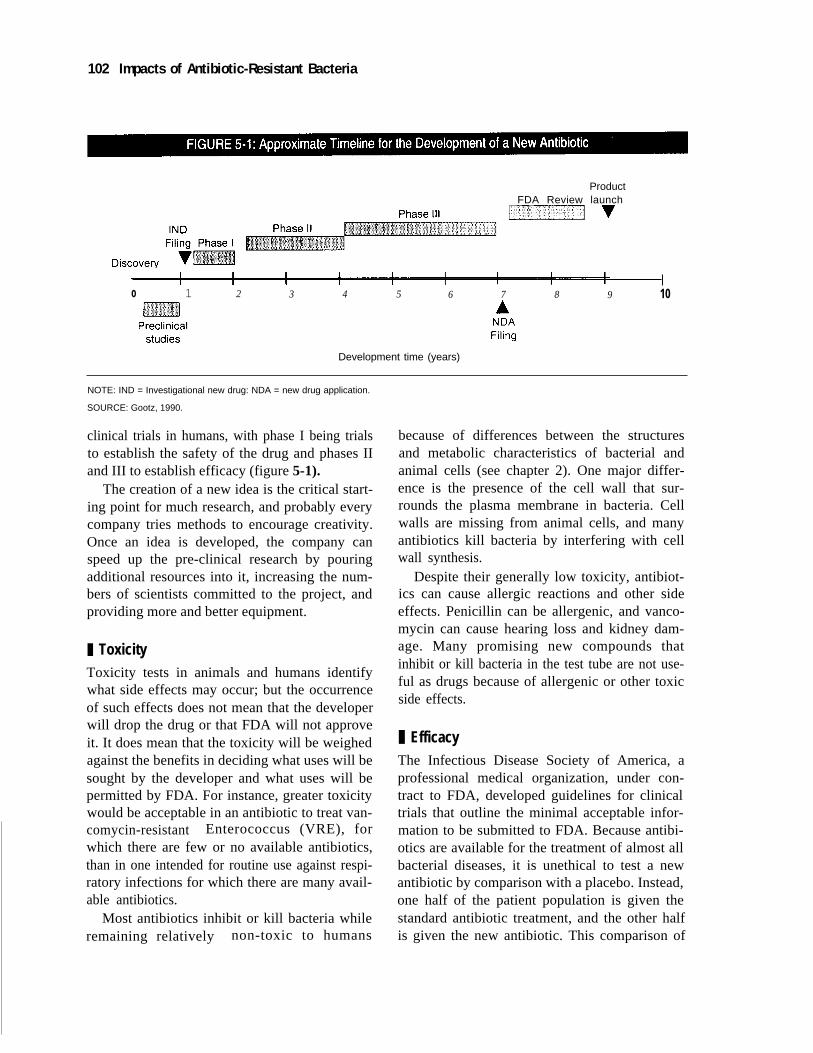
102 Impacts of Antibiotic-Resistant Bacteria
ProductFDA Review launch
o 1 2 3 4 5 6 7 8 9 10
Development time (years)
NOTE: IND = Investigational new drug: NDA = new drug application.
SOURCE: Gootz, 1990.
clinical trials in humans, with phase I being trialsto establish the safety of the drug and phases IIand III to establish efficacy (figure 5-1).
The creation of a new idea is the critical start-ing point for much research, and probably everycompany tries methods to encourage creativity.Once an idea is developed, the company canspeed up the pre-clinical research by pouringadditional resources into it, increasing the num-bers of scientists committed to the project, andproviding more and better equipment.
❚ ToxicityToxicity tests in animals and humans identifywhat side effects may occur; but the occurrenceof such effects does not mean that the developerwill drop the drug or that FDA will not approveit. It does mean that the toxicity will be weighedagainst the benefits in deciding what uses will besought by the developer and what uses will bepermitted by FDA. For instance, greater toxicitywould be acceptable in an antibiotic to treat van-comycin-resistant Enterococcus (VRE), forwhich there are few or no available antibiotics,than in one intended for routine use against respi-ratory infections for which there are many avail-able antibiotics.
Most antibiotics inhibit or kill bacteria whileremaining relatively non-toxic to humans
because of differences between the structuresand metabolic characteristics of bacterial andanimal cells (see chapter 2). One major differ-ence is the presence of the cell wall that sur-rounds the plasma membrane in bacteria. Cellwalls are missing from animal cells, and manyantibiotics kill bacteria by interfering with cellwall synthesis.
Despite their generally low toxicity, antibiot-ics can cause allergic reactions and other sideeffects. Penicillin can be allergenic, and vanco-mycin can cause hearing loss and kidney dam-age. Many promising new compounds thatinhibit or kill bacteria in the test tube are not use-ful as drugs because of allergenic or other toxicside effects.
❚ EfficacyThe Infectious Disease Society of America, aprofessional medical organization, under con-tract to FDA, developed guidelines for clinicaltrials that outline the minimal acceptable infor-mation to be submitted to FDA. Because antibi-otics are available for the treatment of almost allbacterial diseases, it is unethical to test a newantibiotic by comparison with a placebo. Instead,one half of the patient population is given thestandard antibiotic treatment, and the other halfis given the new antibiotic. This comparison of

Chapter 5 Antibiotic Development | 103
efficacies necessarily requires more patients thanif the antibiotic were evaluated against no treat-ment or a placebo. If the new antibiotic is equalto or more effective in treating the disease thanthe standard treatment, FDA will approve its use.Even if it is not quite so effective, FDA willapprove the new antibiotic if it has lower toxicitythan the standard to which it is compared.
FDA will consider the results of foreign trialswhen the makeup of the test population in theforeign country approximates the U.S. popula-tion, the distribution of antibiotic-resistant bacte-ria in the foreign country is about the same as inthe United States, and the disease is caused bythe same bacteria in the other country and in theUnited States. The Office of Technology Assess-ment (OTA) did not investigate how often, ifever, FDA has decided not to consider a foreigntrial, but there appears to be some room for dis-agreement between a manufacturer and FDAabout how closely the foreign conditionsapproach those in the United States. On the otherhand, an FDA official stated that multi-nationalcompanies have done one trial in a Europeancountry and one in the United States, combinedthe results, and obtained approval for the newdrug in both countries, and that FDA will makeapproval decisions based solely on foreign stud-ies (FDA, 1995).
The time necessary for FDA review hasdecreased in the last few years. In the early1990s, FDA took an average of 25 months to acton a New Drug Application (NDA). Through“The Prescription Drug User Fee Act of 1992(P.L. 102-571),” Congress increased funds forFDA to staff and run the review process. Thatlaw requires that each manufacturer pay anannual fee based on the number of the com-pany’s drugs that are in use and the number of itsmanufacturing plants. In addition, manufactur-ers may pay a fee at the time of submission of anNDA. These fees are used to hire additionalreviewers at FDA to speed up the review process,not to speed up the review of the particular NDA.Since the Act’s implementation, the average timefor FDA drug approval in 1994 had dropped to19 months.
The time line on figure 5-1 is an approxima-tion; some drugs move more quickly through thetrials, and some move more slowly. More fre-quently, a drug fails some critical test and mustbe abandoned. Such hurdles have always beenpresent. Scaling-up production of a drug from thesmall quantities needed for initial testing to thelarge quantities needed for phase III clinical test-ing and manufacture can also be significant hur-dles in getting a new drug to market (box 5-1).
FDA regulations allow for an acceleratedreview process when a candidate drug is a possi-ble treatment for a life-threatening disease (suchas an antibiotic for use against VRE). FDA offi-cials can meet with the drug sponsors at the endof the phase I trial and design a phase II trial thatwill be sufficient to make a decision aboutapproval of the drug. Moreover, drugs that areentered into accelerated review go to the “headof the line” at all stages of the review process.
A company seeking approval to market anantibiotic for use against diseases caused byantibiotic-resistant bacteria must demonstrateefficacy against particular bacteria-disease com-binations. For instance, an antibiotic effective
BOX 5-1: Quantities of Drugs Needed at Different Stages of Development
0.01 g-10 g: Discovery (performs initial bench-level discovery, creation, or isolation of the newentity).
10 g-100 g: Chemical process research (iden-tifies possible ways to make the entity on a largerscale).
1,000 g-100,000 g: Chemical process develop-ment (a collaboration between research anddevelopment programs (R&D) and manufacturing;scales up manufacture for toxicology and clinicalresearch; makes the process useful for manufac-turing).
100,000 g-1,000,000 g: Manufacture (scalesup once again to make the entity in commercialamounts).
SOURCE: Bristol-Meyers Squibb, 1995.

104 | Impacts of Antibiotic-Resistant Bacteria
against VRE in laboratory tests would have to beshown effective against VRE-caused endocardi-tis to be marketed for that use, and it would alsohave to be shown effective against VRE-causedbacteremia to be marketed for use against thatindication. This raises problems because thenumber of such diseases is relatively small, mak-ing it difficult to obtain as many cases for a clini-cal trial as are commonly required. According toa U.S. FDA official, however, the agency couldadjust the number of cases required for the trialof an antibiotic for use against particular diseasescaused by particular antibiotic-resistant bacteria.
ANTIBIOTICS IN CURRENT CLINICAL USETable 5-1 is a listing of the actions of antibiotics,a sampling of antibiotics that display thoseactions, and the development or use status of theantibiotics. Currently, research and developmentefforts are in place that seek to improve currentlyused antibiotics.
❚ Sulfonamides1
The sulfonamides are synthetic, not of naturalorigin, and are properly called “antimicrobials”and not antibiotics. They are included herebecause they were the first antibacterial drugsthat were not overtly toxic to humans, and theirchemical modifications foreshadowed much ofthe work to improve natural antibiotics.
In 1936, a year after German researchersreported that Prontosil (the first sulfonamide)cured bacterial diseases, British researchers setout to improve upon its usefulness (Colebrookand Kenny, 1936). The British researchers’ planswere based on the results of studies by Frenchinvestigators, who noted that the antibacterialeffects of compounds like Prontosil were lostwhen some parts of the chemical were removed,but that removal of other substituents had noeffect on antibacterial properties in mice. Theyconcluded that a metabolic product, para-aminobenzenesulfonamide, was responsible for
1 NOTE: An OTA mention of products and companies does not imply any endorsement, and products andcompanies are included only as examples.
the activity of Prontosil, and that the full struc-ture of the parent compound was not necessaryfor bacterial killing. The involvement ofresearchers from three different countries in thisresearch points to the international flavor of anti-biotic research from its very beginning.
The British researchers tested a dozen sulfona-mide analogues for antibiotic activity, but, prac-tically, their most important discovery was thatpara-aminobenzenesulfonamide was well toler-ated when injected subcutaneously and that itcould be given orally. Prontosil, on the otherhand, was biologically active only when given byinjection (Buttle et al., 1936; Mandell and Sande,1990). This finding was another harbinger ofresearch directions with antibiotics; low toxicityand ease of administration increased the accept-ability of an antibiotic and reduced the medicalcare costs associated with it.
If bacteria were passive when faced with anti-bacterials, the sulfonamides would haveremained potent therapy. Bacteria are not pas-sive. Through mutation and selection, theybecome resistant to antibiotics. This sets up thestruggle between antibiotic developers and bac-teria—the biological war.
Sulfonamides inhibit one step in the bacterialsynthesis of folic acid. Humans and other mam-mals do not synthesize folic acid; they obtain itfrom food. Hence, sulfonamides have no effecton mammalian cells. When, by the early 1960s,many bacteria had developed resistance to thesulfonamides, researchers postulated that theantimicrobial action of sulfonamides might beaugmented by the co-administration of trimetho-prim, which blocks another step in folic acid syn-thesis (Bushby and Hitchings, 1968). Blockingtwo sequential enzymes on the bacterial biosyn-thetic pathway of a vital nutrient (such as folicacid) was expected to act synergistically. Thereasoning proved correct, and bacteria resistantto sulfonamide were inhibited by the sulfona-mide/trimethoprim formulation. The preparationis still used widely.
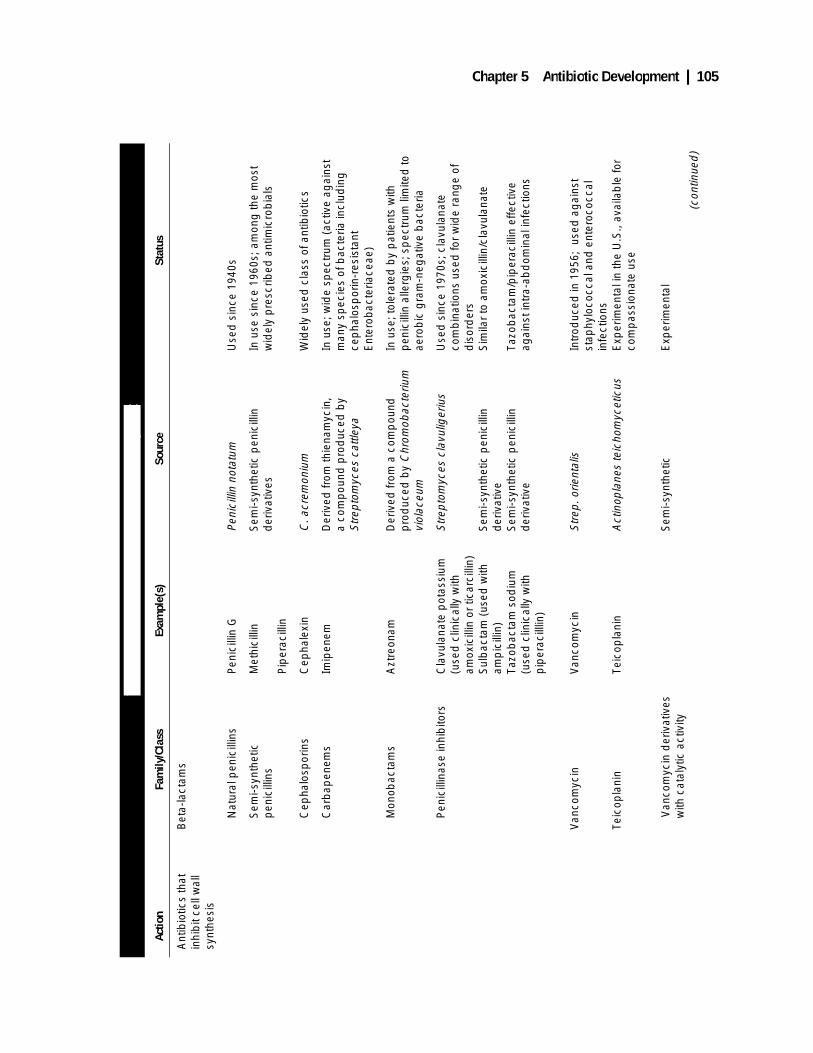
Chapter 5 Antibiotic Development | 105
TABL
E 5-
1: A
ntib
iotic
s in
Use
and
Und
er D
evel
opm
ent
Actio
nFa
mily
/Cla
ssEx
ampl
e(s)
Sour
ceSt
atus
Ant
ibio
tics
that
in
hib
it ce
ll w
all
synt
hesi
s
Bet
a-la
ctam
s
Nat
ural
pen
icill
ins
Pen
icill
in G
Peni
cilli
n no
tatu
mU
sed
sin
ce 1
940s
Sem
i-syn
thet
ic
pen
icill
ins
Met
hici
llin
Pip
erac
illin
Sem
i-syn
thet
ic p
enic
illin
d
eriv
ativ
esIn
use
sin
ce 1
960s
; am
ong
the
mos
t w
idel
y p
resc
ribed
ant
imic
rob
ials
Cep
halo
spor
ins
Cep
hale
xin
C. a
crem
oniu
mW
idel
y us
ed c
lass
of a
ntib
iotic
s
Car
bap
enem
sIm
ipen
emD
eriv
ed fr
om th
iena
myc
in,
a co
mp
ound
pro
duc
ed b
y S
trep
tom
yces
cat
tleya
In u
se; w
ide
spec
trum
(ac
tive
agai
nst
man
y sp
ecie
s of
bac
teria
incl
udin
g
cep
halo
spor
in-r
esis
tant
E
nter
obac
teria
ceae
)
Mon
obac
tam
sA
ztre
onam
Der
ived
from
a c
omp
ound
p
rod
uced
by
Chr
omob
acte
rium
vi
olac
eum
In u
se; t
oler
ated
by
pat
ient
s w
ith
pen
icill
in a
llerg
ies;
sp
ectr
um li
mite
d to
ae
rob
ic g
ram
-neg
ativ
e b
acte
ria
Pen
icill
inas
e in
hib
itors
Cla
vula
nate
pot
assi
um
(use
d c
linic
ally
with
am
oxic
illin
or
ticar
cilli
n)S
ulb
acta
m (
used
with
am
pic
illin
)Ta
zob
acta
m s
odiu
m
(use
d c
linic
ally
with
p
iper
acill
lin)
Str
epto
myc
es c
lavu
liger
ius
Sem
i-syn
thet
ic p
enic
illin
d
eriv
ativ
eS
emi-s
ynth
etic
pen
icill
in
der
ivat
ive
Use
d s
ince
197
0s; c
lavu
lana
te
com
bin
atio
ns u
sed
for
wid
e ra
nge
of
dis
ord
ers
Sim
ilar
to a
mox
icill
in/c
lavu
lana
te
Tazo
bac
tam
/pip
erac
illin
effe
ctiv
e ag
ains
t int
ra-a
bd
omin
al in
fect
ions
Van
com
ycin
Teic
opla
nin
Van
com
ycin
Teic
opla
nin
Str
ep. o
rient
alis
Act
inop
lane
s te
icho
myc
etic
us
Intr
oduc
ed in
195
6; u
sed
ag
ains
t st
aphy
loco
ccal
and
ent
eroc
occa
l in
fect
ions
Exp
erim
enta
l in
the
U.S
., av
aila
ble
for
com
pas
sion
ate
use
V
anco
myc
in d
eriv
ativ
esw
ith c
atal
ytic
act
ivity
Sem
i-syn
thet
icE
xper
imen
tal
(con
tinue
d)
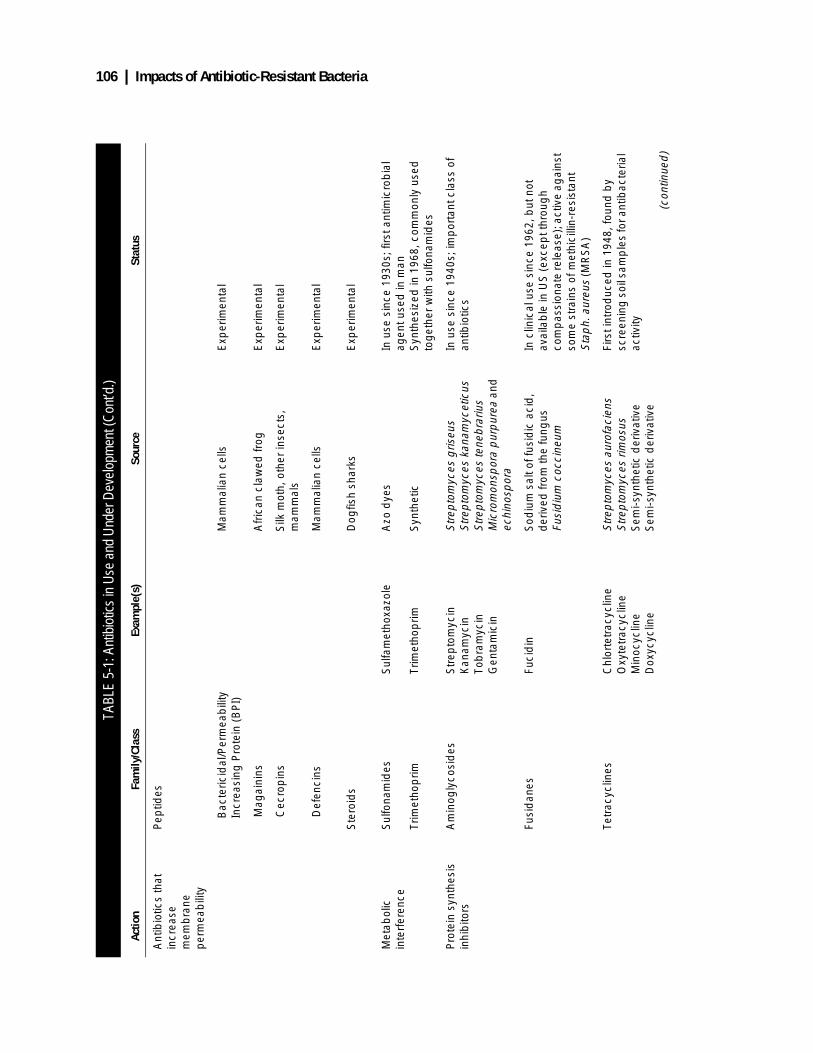
106 | Impacts of Antibiotic-Resistant Bacteria
TABL
E 5-
1: A
ntib
iotic
s in
Use
and
Und
er D
evel
opm
ent (
Con
t’d.)
Actio
nFa
mily
/Cla
ssEx
ampl
e(s)
Sour
ceSt
atus
Ant
ibio
tics
that
in
crea
se
mem
bra
ne
per
mea
bili
ty
Pep
tides
Bac
teric
idal
/Per
mea
bili
tyIn
crea
sing
Pro
tein
(B
PI)
Mam
mal
ian
cells
Exp
erim
enta
l
M
agai
nins
Afr
ican
cla
wed
frog
Exp
erim
enta
l
C
ecro
pin
sS
ilk m
oth,
oth
er in
sect
s,
mam
mal
sE
xper
imen
tal
D
efen
cins
Mam
mal
ian
cells
Exp
erim
enta
l
Ste
roid
sD
ogfis
h sh
arks
Exp
erim
enta
l
Met
abol
ic
inte
rfer
ence
Sul
fona
mid
es
Trim
etho
prim
Sul
fam
etho
xazo
le
Trim
etho
prim
Azo
dye
s
Syn
thet
ic
In u
se s
ince
193
0s; f
irst a
ntim
icro
bia
l ag
ent u
sed
in m
anS
ynth
esiz
ed in
196
8, c
omm
only
use
d
tog
ethe
r w
ith s
ulfo
nam
ides
Pro
tein
syn
thes
is
inhi
bito
rsA
min
ogly
cosi
des
Str
epto
myc
inK
anam
ycin
Tob
ram
ycin
Gen
tam
icin
Str
epto
myc
es g
riseu
sS
trep
tom
yces
kan
amyc
etic
usS
trep
tom
yces
tene
bra
rius
Mic
rom
onsp
ora
pur
pur
ea a
nd
echi
nosp
ora
In u
se s
ince
194
0s; i
mp
orta
nt c
lass
of
antib
iotic
s
Fusi
dan
esFu
cid
inS
odiu
m s
alt o
f fus
idic
aci
d,
der
ived
from
the
fung
us
Fusi
diu
m c
occi
neum
In c
linic
al u
se s
ince
196
2, b
ut n
ot
avai
lab
le in
US
(ex
cep
t thr
oug
h co
mp
assi
onat
e re
leas
e); a
ctiv
e ag
ains
t so
me
stra
ins
of m
ethi
cilli
n-re
sist
ant
Sta
ph.
aur
eus
(MR
SA
)
Tetr
acyc
lines
Chl
orte
trac
yclin
eO
xyte
trac
yclin
eM
inoc
yclin
eD
oxyc
yclin
e
Str
epto
myc
es a
urof
acie
ns
Str
epto
myc
es r
imos
usS
emi-s
ynth
etic
der
ivat
ive
Sem
i-syn
thet
ic d
eriv
ativ
e
Firs
t int
rod
uced
in 1
948,
foun
d b
y sc
reen
ing
soi
l sam
ple
s fo
r ant
ibac
teria
l ac
tivity
(con
tinue
d)
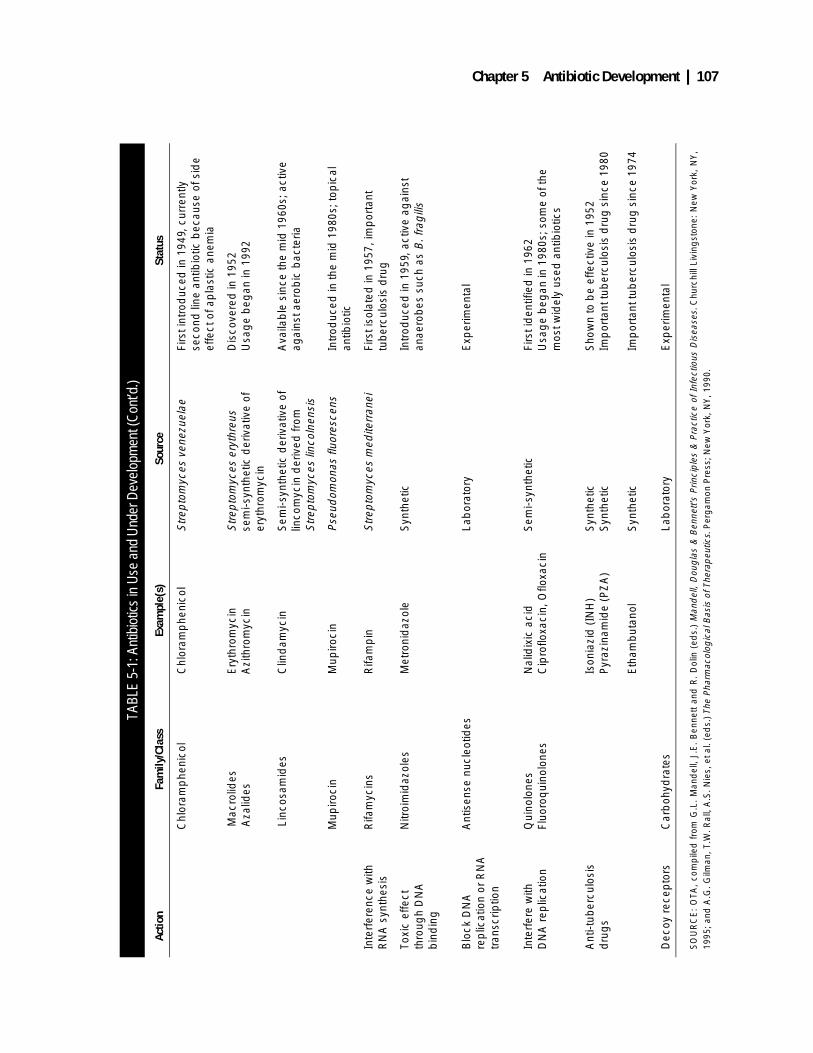
Chapter 5 Antibiotic Development | 107
TABL
E 5-
1: A
ntib
iotic
s in
Use
and
Und
er D
evel
opm
ent (
Con
t’d.)
Actio
nFa
mily
/Cla
ssEx
ampl
e(s)
Sour
ceSt
atus
Chl
oram
phe
nico
lC
hlor
amp
heni
col
Str
epto
myc
es v
enez
uela
eFi
rst i
ntro
duc
ed in
194
9, c
urre
ntly
se
cond
line
ant
ibio
tic b
ecau
se o
f sid
e ef
fect
of a
pla
stic
ane
mia
Mac
rolid
es A
zalid
esE
ryth
rom
ycin
Azi
thro
myc
in
Str
epto
myc
es e
ryth
reus
sem
i-syn
thet
ic d
eriv
ativ
e of
er
ythr
omyc
in
Dis
cove
red
in 1
952
Usa
ge
beg
an in
199
2
Lin
cosa
mid
esC
lind
amyc
inS
emi-s
ynth
etic
der
ivat
ive
of
linco
myc
in d
eriv
ed fr
om
Str
epto
myc
es li
ncol
nens
is
Ava
ilab
le s
ince
the
mid
196
0s; a
ctiv
e ag
ains
t aer
obic
bac
teria
Mup
iroci
nM
upiro
cin
Pse
udom
onas
fluo
resc
ens
Intr
oduc
ed in
the
mid
198
0s; t
opic
al
antib
iotic
Inte
rfer
ence
with
R
NA
syn
thes
isR
ifam
ycin
sR
ifam
pin
Str
epto
myc
es m
edite
rran
eiFi
rst i
sola
ted
in 1
957,
imp
orta
nt
tub
ercu
losi
s d
rug
Toxi
c ef
fect
th
roug
h D
NA
b
ind
ing
Nitr
oim
idaz
oles
Met
roni
daz
ole
Syn
thet
icIn
trod
uced
in 1
959,
act
ive
agai
nst
anae
rob
es s
uch
as B
. fra
gili
s
Blo
ck D
NA
re
plic
atio
n or
RN
A
tran
scrip
tion
Ant
isen
se n
ucle
otid
esLa
bor
ator
yE
xper
imen
tal
Inte
rfer
e w
ith
DN
A r
eplic
atio
nQ
uino
lone
sFl
uoro
qui
nolo
nes
Nal
idix
ic a
cid
Cip
roflo
xaci
n, O
floxa
cin
Sem
i-syn
thet
icFi
rst i
den
tifie
d in
196
2U
sag
e b
egan
in 1
980s
; som
e of
the
mos
t wid
ely
used
ant
ibio
tics
Ant
i-tub
ercu
losi
s d
rug
sIs
onia
zid
(IN
H)
Pyr
azin
amid
e (P
ZA
)
Eth
amb
utan
ol
Syn
thet
icS
ynth
etic
Syn
thet
ic
Sho
wn
to b
e ef
fect
ive
in 1
952
Imp
orta
nt tu
ber
culo
sis
dru
g s
ince
198
0
Imp
orta
nt tu
ber
culo
sis
dru
g s
ince
197
4
Dec
oy r
ecep
tors
Car
boh
ydra
tes
Lab
orat
ory
Exp
erim
enta
l
SO
UR
CE
: O
TA,
com
pile
d f
rom
G.L
. M
and
ell,
J.E
. B
enne
tt an
d R
. D
olin
(ed
s.)
Man
del
l, D
oug
las
& B
enne
tt’s
Prin
cip
les
& P
ract
ice
of I
nfec
tious
Dis
ease
s. C
hurc
hill
Livi
ngst
one:
New
Yor
k, N
Y,
1995
; and
A.G
. Gilm
an, T
.W. R
all,
A.S
. Nie
s, e
t al.
(ed
s.) T
he P
harm
acol
ogic
al B
asis
of T
hera
peu
tics.
Per
gam
on P
ress
; New
Yor
k, N
Y, 1
990.

108 | Impacts of Antibiotic-Resistant Bacteria
❚ Penicillins and Clavulanic AcidPenicillin was the first true antibiotic. Its actioninvolves binding to penicillin-binding proteinswhich are enzymes necessary for the synthesis ofthe bacterial cell wall, inhibiting those enzymes,which leads to the death of the cell, and uncover-ing or activating other enzymes that cause thebacterial cell to burst. Shortly after penicillin’sintroduction, resistant micro-organisms began toappear. By the mid-1940s, the enzyme penicilli-nase or β-lactamase, which degrades penicillinso that it has no effect on bacteria, had been iso-lated from a bacterium that was not specificallyidentified, and soon after, scientists found it waspresent in other bacteria such as Staphylococcusaureus. As early as 1948, 50 percent of S. aureusin hospitals were resistant to penicillin, rising to80 percent in 1957 (Gootz, 1990).
Semi-synthetic PenicillinsSemi-synthetic penicillins—methicillin, nafcil-lin, and cloxacillin—are the product of searchesfor penicillins that could escape the action ofpenicillinase. They were made possible by thelarge-scale production of a part of the penicillinmolecule, called 6-aminopenicillanic acid, towhich chemists could add different chemicalsubstitutions. These penicillins resist the degrad-ing action of penicillinases, and they foundimmediate application in treating some penicillin-resistant bacteria. The extremely low toxicity ofpenicillin has fueled efforts to continue develop-ment of this antibiotic.
Penicillinase InhibitorsMolds of the genus Streptomyces produce chem-ical compounds that “suicidally” tie up penicilli-nases. When administered with penicillins, theinhibitors bind the penicillinases, leaving theunbound penicillin free to kill bacteria (Readingand Cole, 1977). By the early 1970s, olivanicacid, produced by Streptomyces olivaceus, hadproved a successful penicillinase inhibitor, and it
was used with ampicillin and amoxicillin intreating S. aureus and Klebsiella pneumonia,both Gram-positive bacteria, but it was unable topenetrate the Gram-negative bacterial cell wall.2
Clavulanic acid, from Streptomyces clavuligerus,proved more effective than the olivanic acids,and it extended the spectrum of penicillinaseactivity to Gram-negative bacteria. Amoxicillin/clavulanic acid is the mainstay of treatment forotitis media in children caused by Hemophilusinfluenzae and Branhamella catarrhalis.
The success of the penicillin/clavulanic acidcombination suggested that semi-synthetic peni-cillins—while promising as single-agent ther-apy—might not be the only solution to theproblem of antibiotic resistance. More impor-tantly, perhaps, the notion of identifying andattacking a specific bacterial target responsiblefor resistance (in this case, penicillinases)became a principle of antibiotic research.
❚ Other Beta-Lactam AntibioticsThe cephalosporins (see figure 5-2) share a simi-lar chemical structure (the beta-lactam ring) andsimilar mechanisms of action (inhibition of syn-thesis of the bacterial cell wall) with penicillin.Cephalosporin antibiotics were first isolatedfrom the organism Cephalosporium acremo-nium in 1948 from the sea near a sewer outlet offthe Sardinian coast (reviewed in Mandell andSande, 1990). Chemists have modified the struc-ture of the antibiotics and produced semisyn-thetic antibiotics with increased antimicrobialactivity. The resulting so-called “third genera-tion” cephalosporins, including ceftriaxone andceftazidime, are widely used. Imipenem, yetanother β-lactam antibiotic, is a chemical deriva-tive of a compound first isolated from the organ-ism Streptomyces catleya; it is the broadest-spectrum antibiotic commercially available (seeEmori and Gaynes, 1993).
2 Some bacteria take up a stain, called the Gram stain, and some do not. The difference depends on the structure of the cell wall in the twokinds of bacteria, and the permeability of the two kinds of bacteria differ as a result of the difference in the cell walls.
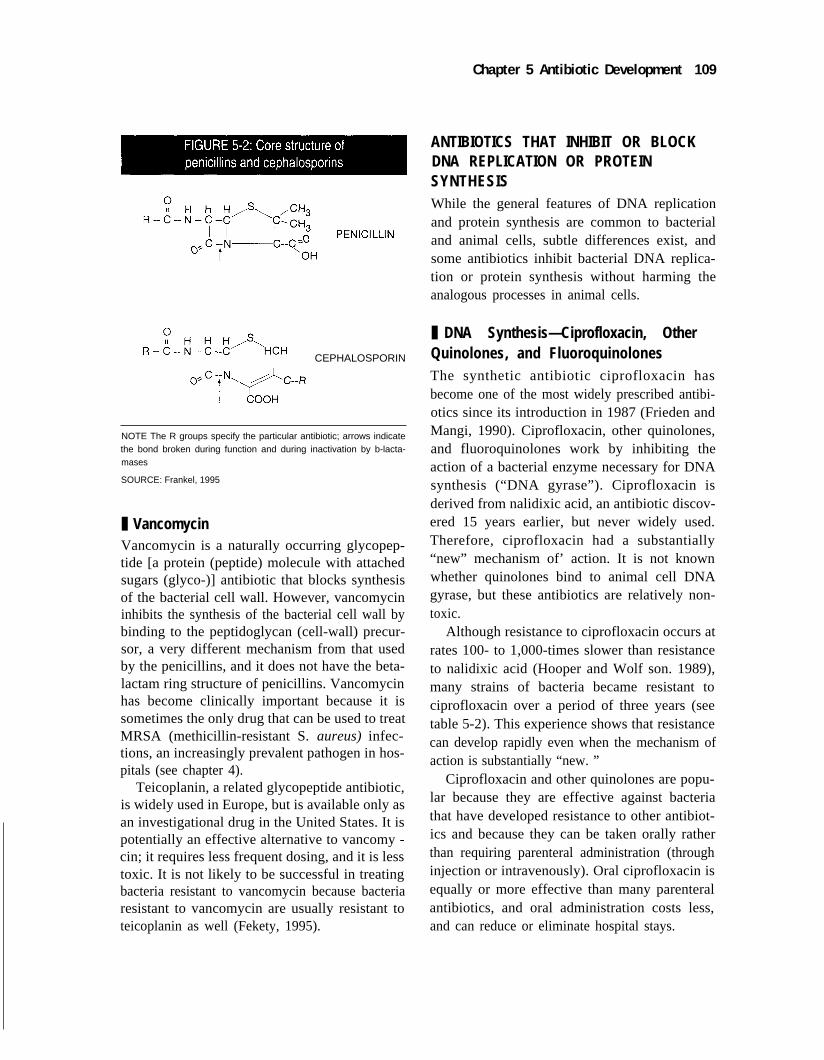
Chapter 5 Antibiotic Development 109
I
CEPHALOSPORIN
NOTE The R groups specify the particular antibiotic; arrows indicatethe bond broken during function and during inactivation by b-lacta-mases
SOURCE: Frankel, 1995
❚ VancomycinVancomycin is a naturally occurring glycopep-tide [a protein (peptide) molecule with attachedsugars (glyco-)] antibiotic that blocks synthesisof the bacterial cell wall. However, vancomycininhibits the synthesis of the bacterial cell wall bybinding to the peptidoglycan (cell-wall) precur-sor, a very different mechanism from that usedby the penicillins, and it does not have the beta-lactam ring structure of penicillins. Vancomycinhas become clinically important because it issometimes the only drug that can be used to treatMRSA (methicillin-resistant S. aureus) infec-tions, an increasingly prevalent pathogen in hos-pitals (see chapter 4).
Teicoplanin, a related glycopeptide antibiotic,is widely used in Europe, but is available only asan investigational drug in the United States. It ispotentially an effective alternative to vancomy -cin; it requires less frequent dosing, and it is lesstoxic. It is not likely to be successful in treatingbacteria resistant to vancomycin because bacteriaresistant to vancomycin are usually resistant toteicoplanin as well (Fekety, 1995).
ANTIBIOTICS THAT INHIBIT OR BLOCKDNA REPLICATION OR PROTEINSYNTHESISWhile the general features of DNA replicationand protein synthesis are common to bacterialand animal cells, subtle differences exist, andsome antibiotics inhibit bacterial DNA replica-tion or protein synthesis without harming theanalogous processes in animal cells.
❚ DNA Synthesis—Ciprofloxacin, OtherQuinolones, and FluoroquinolonesThe synthetic antibiotic ciprofloxacin hasbecome one of the most widely prescribed antibi-otics since its introduction in 1987 (Frieden andMangi, 1990). Ciprofloxacin, other quinolones,and fluoroquinolones work by inhibiting theaction of a bacterial enzyme necessary for DNAsynthesis (“DNA gyrase”). Ciprofloxacin isderived from nalidixic acid, an antibiotic discov-ered 15 years earlier, but never widely used.Therefore, ciprofloxacin had a substantially“new” mechanism of’ action. It is not knownwhether quinolones bind to animal cell DNAgyrase, but these antibiotics are relatively non-toxic.
Although resistance to ciprofloxacin occurs atrates 100- to 1,000-times slower than resistanceto nalidixic acid (Hooper and Wolf son. 1989),many strains of bacteria became resistant tociprofloxacin over a period of three years (seetable 5-2). This experience shows that resistancecan develop rapidly even when the mechanism ofaction is substantially “new. ”
Ciprofloxacin and other quinolones are popu-lar because they are effective against bacteriathat have developed resistance to other antibiot-ics and because they can be taken orally ratherthan requiring parenteral administration (throughinjection or intravenously). Oral ciprofloxacin isequally or more effective than many parenteralantibiotics, and oral administration costs less,and can reduce or eliminate hospital stays.
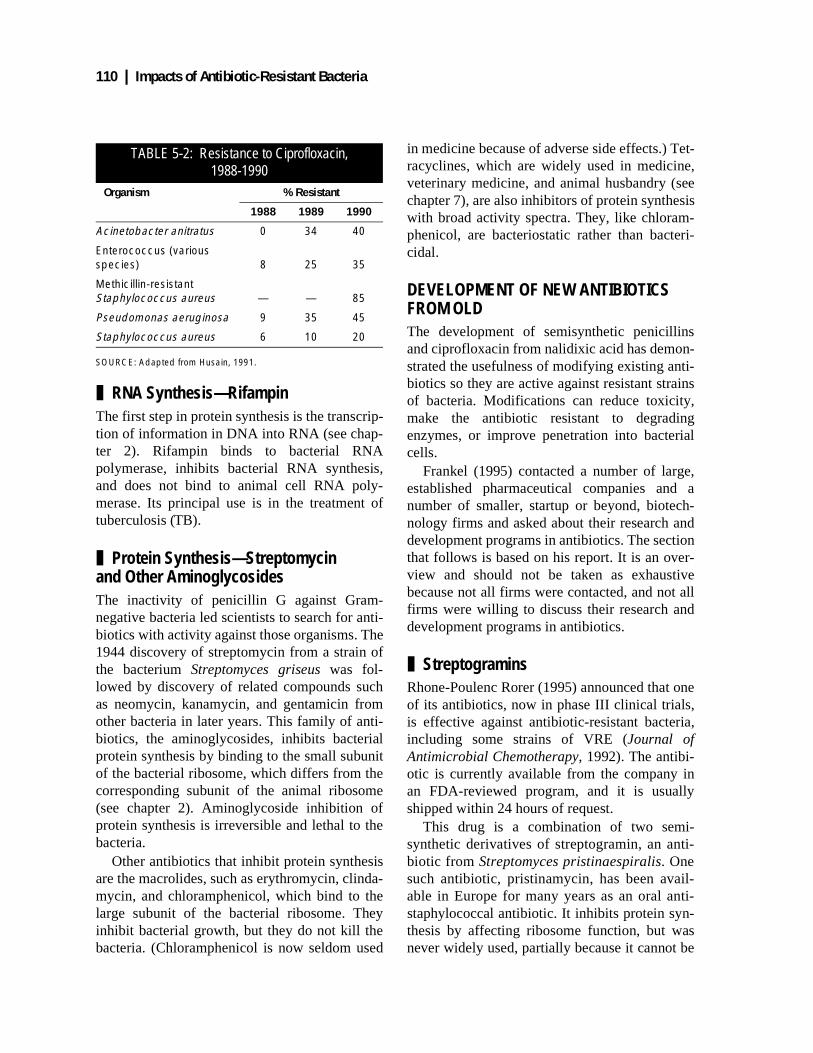
110 | Impacts of Antibiotic-Resistant Bacteria
❚ RNA Synthesis—RifampinThe first step in protein synthesis is the transcrip-tion of information in DNA into RNA (see chap-ter 2). Rifampin binds to bacterial RNApolymerase, inhibits bacterial RNA synthesis,and does not bind to animal cell RNA poly-merase. Its principal use is in the treatment oftuberculosis (TB).
❚ Protein Synthesis—Streptomycin and Other AminoglycosidesThe inactivity of penicillin G against Gram-negative bacteria led scientists to search for anti-biotics with activity against those organisms. The1944 discovery of streptomycin from a strain ofthe bacterium Streptomyces griseus was fol-lowed by discovery of related compounds suchas neomycin, kanamycin, and gentamicin fromother bacteria in later years. This family of anti-biotics, the aminoglycosides, inhibits bacterialprotein synthesis by binding to the small subunitof the bacterial ribosome, which differs from thecorresponding subunit of the animal ribosome(see chapter 2). Aminoglycoside inhibition ofprotein synthesis is irreversible and lethal to thebacteria.
Other antibiotics that inhibit protein synthesisare the macrolides, such as erythromycin, clinda-mycin, and chloramphenicol, which bind to thelarge subunit of the bacterial ribosome. Theyinhibit bacterial growth, but they do not kill thebacteria. (Chloramphenicol is now seldom used
in medicine because of adverse side effects.) Tet-racyclines, which are widely used in medicine,veterinary medicine, and animal husbandry (seechapter 7), are also inhibitors of protein synthesiswith broad activity spectra. They, like chloram-phenicol, are bacteriostatic rather than bacteri-cidal.
DEVELOPMENT OF NEW ANTIBIOTICS FROM OLDThe development of semisynthetic penicillinsand ciprofloxacin from nalidixic acid has demon-strated the usefulness of modifying existing anti-biotics so they are active against resistant strainsof bacteria. Modifications can reduce toxicity,make the antibiotic resistant to degradingenzymes, or improve penetration into bacterialcells.
Frankel (1995) contacted a number of large,established pharmaceutical companies and anumber of smaller, startup or beyond, biotech-nology firms and asked about their research anddevelopment programs in antibiotics. The sectionthat follows is based on his report. It is an over-view and should not be taken as exhaustivebecause not all firms were contacted, and not allfirms were willing to discuss their research anddevelopment programs in antibiotics.
❚ StreptograminsRhone-Poulenc Rorer (1995) announced that oneof its antibiotics, now in phase III clinical trials,is effective against antibiotic-resistant bacteria,including some strains of VRE (Journal ofAntimicrobial Chemotherapy, 1992). The antibi-otic is currently available from the company inan FDA-reviewed program, and it is usuallyshipped within 24 hours of request.
This drug is a combination of two semi-synthetic derivatives of streptogramin, an anti-biotic from Streptomyces pristinaespiralis. Onesuch antibiotic, pristinamycin, has been avail-able in Europe for many years as an oral anti-staphylococcal antibiotic. It inhibits protein syn-thesis by affecting ribosome function, but wasnever widely used, partially because it cannot be
TABLE 5-2: Resistance to Ciprofloxacin, 1988-1990
Organism % Resistant
1988 1989 1990
Acinetobacter anitratus 0 34 40
Enterococcus (various species) 8 25 35
Methicillin-resistant Staphylococcus aureus — — 85
Pseudomonas aeruginosa 9 35 45
Staphylococcus aureus 6 10 20
SOURCE: Adapted from Husain, 1991.

Chapter 5 Antibiotic Development | 111
made in an injectable form due to low water sol-ubility. The new derivatives of pristinamycin—quinupristin/dalfopristin (used in combina-tion)—are injectable.
❚ Tetracycline AnalogsThe first clinically useful tetracycline, chlortetra-cycline, was introduced in 1948. It was isolatedfrom the micro-organism Streptomyces aurofa-ciens and was discovered after screening samplesof Missouri farm soil (Levy, 1981). Followingthis discovery, other researchers identified moretetracyclines by further screening of soil micro-organisms or by synthesis in laboratories. Aswith the penicillins, manipulation of the tetracy-cline molecule has brought different spectrumsand properties of antibiotic activity. While all ofthe tetracyclines now used in the United Statesare generally considered broad-spectrum agents,bacterial resistance to this family of agents iswidespread.
“Active efflux,” which transports tetracyclinesout of the bacteria, is a major mechanism of bac-terial resistance. Since its description (Levy,1981), it has also been shown to be a mechanismof resistance to several other antibiotics includ-ing chloramphenicol, fluoroquinolones, erythro-mycin, and ß-lactams (Nikaido, 1994), and it ispresent in both Gram-positive and Gram-negative bacteria. Nikaido (1994) reviews evi-dence about permeability barriers to antibioticentry into bacteria and active efflux, which canbestow resistance to many antibiotics, and statesthat, “It will be a major challenge for the pharma-ceutical industry to produce compounds that areable to overcome mechanisms of this type.”
Such research is underway. Nelson et al.(1993) tested 30 tetracycline analogues and iden-tified two chemical substitutions that blockactive efflux. Subsequently, Nelson et al. (1994)determined the part of the tetracycline moleculethat is essential for its antibacterial activity andwhich substitutions inhibit efflux. This informa-tion may increase the usefulness of tetracycline,an old antibiotic.
Minocycline, the last tetracycline to reach themarket, was introduced in the 1970s, and it wasthe starting point for researchers who tookanother look at the tetracyclines in the late 1980s.This new tetracycline research program, a multi-disciplinary effort by chemists, molecular bio-logists, biochemists and microbiologists, hasproduced the semisynthetic glycylcyclineantibiotics. These are active against both Gram-positive and Gram-negative bacteria and evaderesistance mediated by six of the known mecha-nisms of tetracycline resistance. Researchers arecontinuing to modify the glycylcyclines to opti-mize their antibacterial properties (Bergeron etal., 1994; Sum, Lee, Peterson et al., 1994), andhave recently introduced modifications that maylead to the production of “later-generation” gly-cylcyclines (Sum, Lee, and Tally, 1994). Whenand whether they will reach clinical applicationis unknown.
❚ Dual-Action Cephalosporins One approach to evading bacterial resistance tocephalosporins or quinolones is to chemicallycouple the two to produce conjugates that have adual mechanism of action (hence the name“dual-action” cephalosporins), reflecting theactions of both the ß-lactam, cephalosporin, andquinolone components.
The first of these conjugates, as reported byGeorgopapdakau et al. (1989), was found to actinitially as a cephalosporin by binding to appro-priate penicillin-binding proteins, and then toinhibit DNA replication, as would be expectedfrom the quinolone function. Some conjugatesappeared to act primarily as cephalosporins,while others acted primarily as quinolones(Georgopapdakau and Bertasso, 1993). Thepharmaceutical company that sponsored Georgo-papdakau’s work is no longer supportingresearch in dual-action cephalosporins, but suchresearch is reportedly continuing in at least oneother company.

112 | Impacts of Antibiotic-Resistant Bacteria
❚ Vancomycin ResearchVancomycin is the antibiotic of last resort insome specific situations, and it is a popular one,accounting for a quarter of the budget for antibi-otics in some hospitals. The appearance of somestrains of VRE that are resistant to all antibiotics3
leaves physicians with no currently approvedantibiotic treatment for infections caused bythose organisms. Intravenous vancomycin isthe first choice for the antibiotic treatment ofMRSA, and the probably inevitable appearanceof vancomycin-resistant MRSA will leave physi-cians with no marketed antibiotic effectiveagainst that serious nosocomial infection.
Currently, however, some strains of MRSAare reportedly susceptible to other antibiotics:Novobiocin, which is available only in oral form,is active against many strains of MRSA. Minocy-cline (a tetracycline) has been used in successfultreatment of a few cases of endocarditis causedby MRSA. Most isolates of MRSA are suscepti-ble to fusicid acid. Used in combination withother antibiotics, fusicid acid has been part ofsuccessful therapy for a variety of MRSA-causeddiseases, but the role of fusicid acid is notentirely clear. Emergence of resistance to all ofthese antibiotics has been reported, and it is espe-cially a problem with fusicid acid. The problemswith resistance have lead to the recommendationthat alternatives to vancomycin be used in com-bination—such as rifampin with fusicid acid—totreat MRSA (Mulligan, Murray-Leisure, Ribneret al., 1993). While these alternatives to vanco-mycin exist, they are less than the first choice fortreatment of MRSA.
Like penicillin and other antibiotics before it,vancomycin is a starting compound in efforts toproduce new and more effective antibiotics.
Semisynthetic VancomycinEli Lilly and Company (1995) has prepared asemisynthetic vancomycin (LY333328) specifi-
3 Not all vancomycin-resistant enterococcus are resistant to all antibiotics. Enterococcus faecalis remains susceptible to ampicillin, as dosome strains of E. faecium.
cally for use against vancomycin-resistant organ-isms. The drug has demonstrated activity againstVRE in animal tests and against MRSA andpenicillin-resistant Strep. pneumoniae in in vitrotests. According to a company spokesperson,more animal tests of safety and efficacy arerequired, and, if they are successful, human trialsmay begin in 1996. This new compound is theproduct of research centered on development ofantibiotics for use against vancomycin-resistantorganisms.
Catalytic AntibioticsShi and Griffin (1993) discovered that vancomy-cin has a catalytic (chemical-degrading action)activity, and they are chemically altering vanco-mycin to develop a molecule that will not onlybind to the cell-wall precursor and inhibit cell-wall synthesis, the normal activity of vancomy-cin, but destroy the precursor as well. If this isachieved, it should increase the potency of van-comycin; the catalytic antibiotic should be ableto move to another cell-wall precursor afterdestroying the first, and so on. Griffin (1994) isalso seeking to alter the vancomycin molecule sothat it regains its binding affinity to the altered cell-wall precursors that are present in vancomycin-resistant bacteria. Once affinity is restored, theantibiotic can bind to the cell wall precursor,inhibit the synthesis of the wall, and kill the bac-teria. If researchers develop the catalytic functionso that it destroys the cell-wall precursor, thatactivity could be added.
❚ The MacrolidesThe macrolide antibiotics inhibit protein synthe-sis. Erythromycin, the most commonly usedmember of the class, is effective against a broadrange of Gram-positive and Gram-negative bac-teria, and is available for oral, intravenous, andtopical uses. While resistance has been noted inthe United States, it is more common in other

Chapter 5 Antibiotic Development | 113
countries, and the level of resistance appearsrelated to the level of use (Steigbigel, 1995).
Azithromycin, a closely related molecule, isnow being marketed with advertised advantagesin being effective against more strains of bacteriathan erythromycin, but it is being marketed onthe basis of other positive attributes as well.Because it persists in human white blood cellsfor a few days (rather than a few hours as withsome other antibiotics), two tablets of azithromy-cin on the first day of treatment and one tablet aday for four more days is sufficient for mostapplications (Pfizer, Inc., 1993). The conve-nience of this schedule is contrasted with thosefor other antibiotics that require three or fourdaily doses for up to 10 days. According to stud-ies referenced in the advertising literature(Pfizer, Inc., 1993), compliance is better, thereare fewer side effects, and patient costs arelower. This example illuminates some of thefactors, including convenience and cost, as wellas effectiveness, that go into marketing ofantibiotics.
NEW RESEARCH TOOLSNew techniques in chemistry and molecular biol-ogy have immediate application to research anddevelopment of antibiotics. Box 5-2 discussessome of those techniques.
ANTIBIOTICS FROM NEW SOURCESIn addition to using new laboratory tools,antibiotic researchers are also exploring new bio-logical sources for antibiotic activities. Unlikethe traditional searches that have looked at prod-ucts from micro-organisms, some current onesare looking at materials from humans and otheranimals.
❚ CarbohydratesCarbohydrates called oligosaccharides [“oligo-”a few, “saccharides” sugars] (OS), are ubiquitouson the surface of mammalian cells, and bacteriaand viruses adhere to host cell OS as the first stepin the process of recognition, adhesion, andinfection (Rosenstein et al., 1988). Individual OS
are structurally specific for different organisms,and microbial adherence has been referred to as a“lock and key” phenomenon, in which only cer-tain keys (microbial proteins, called “lectins” or“adhesions”) “fit” into specific locks (host-cellOS receptors).
Until recently, the complexity of OS structureand the resulting inability to synthesize sufficientOS at reasonable cost hindered OS drug design.The simplest OS—a disaccharide that is com-posed of only two sugars—can take any of 20different forms. The problem increases with size;there are 35,560 possible ways to arrange foursugars into tetrasaccharides. In comparison, fouramino acids can create only 24 distinct tetrapep-tides (Hughes, 1994). These complexities con-tributed to the formerly high costs that ranged upto $2 million per gram of OS. New techniqueshave lowered the cost of some OS by 10,000times to $200 per gram, and OS drug design hasaccelerated (George, 1994; Glaser, 1994) withapplications in treating bacterial diseases, includ-ing ulcers.
The bacteria Helicobacter pylori causes gas-tric and duodenal ulcers, and the usual treatmenteradicates it and prevents the reappearance ofulcers with a success rate of 70 to above 90 per-cent. Resistance of H. pylori to antibiotics usedin the usual therapy is a factor in lower treatmentsuccess rates.
Neose Pharmaceuticals (Roth, 1995) has per-fected the synthesis of the OS to which H. pyloribinds, and animal studies have shown thatadministration of the OS competes with the H.pylori binding sites in the digestive tract, causingthe H. pylori to release from those sites with thebacteria then being eliminated from the body.The OS is identical to an OS found in mothers’milk, and it has extremely low toxicity in animaltests. Phase I clinical trials for toxicity wereunderway in March 1995.
Up to 80 percent of all hospital-acquired bac-terial pneumonias are caused by one of six bacte-rial species. According to Roth (1995), all six ofthose bacterial species bind to the same OS,which opens the possibility of treating thoseinfections with a soluble form of the OS. Another

114 | Impacts of Antibiotic-Resistant Bacteria
BOX 5-2: Some New Methods for Research in Antibiotics
Structure-Based Drug Design
Traditionally, that is, for 50 or so years, scientists have discovered new antibiotics by screening thou-sands of natural, synthetic, or semi-synthetic compounds for antimicrobial properties, analyzing the struc-tures of active ones, and modifying active compounds for greater utility. Scientists have discovered manyantibiotics serendipitously, usually an expensive and time-consuming process and always an unpredict-able one, and many have been discovered and tested in laboratories and in humans long beforeresearchers understood their mechanism of action.
Structure-based drug design (SBDD), on the other hand, begins with an understanding—or physicalmodel—of the drug mechanism, especially the ligand:receptor interaction (Kuntz, 1992). This interactionoccurs at the “active site” where the “ligand,” in this case the antibiotic, binds to some structure, the“receptor” (or “target”) in the bacteria. SBDD employs newer research tools, such as X-ray crystallogra-phy, nuclear magnetic resonance spectroscopy, and supercomputer combinatorial chemistry to designnew compounds that will bind more tightly to the active site (Knox, 1993; Fan et al., 1994; Balbes et al.,1994; Boyd and Milosevich, 1993).
Targeted Replacement of Segments of Antibiotic Proteins
The bacterium Bacillus subtilis produces an antibiotic called surfactin. Stachelhaus, Schneider, andMarahiel (1995) isolated the DNA segments that code for surfactin from B. subtilis, and DNA segmentsfrom another bacterium, Bacillis brevis, and from the fungus, Penicillium chrysogenum. Using recombi-nant DNA techniques, they constructed hybrid B. subtilis-B. brevis and hybrid B. subtilis-P. chrysogenumDNA molecules that they reinserted into B. subtilis. Hybrid DNAs of the first kind coded for recombinantproteins in which some segments of the protein came from B. subtilis and some from B. brevis hybrids ofthe second kind resulted in the production of proteins with some segments from B. subtilis and othersfrom P. chrysogenum.
This experiment demonstrates a method to construct hybrid molecules, and it may have an applica-tion to the development of new antibiotics. Because the DNA segments can come from unrelated organ-isms, or even from chemical synthesis, the structure of the recombinant DNA, and the resulting protein,can be specified. Better understanding of ligand:receptor interactions may provide the information for theconstruction of recombinant DNA molecules that will code for new antibiotics.
“Unnatural” natural products
The bacterium Streptomyces coelicolor produces the antibiotics tetracyclines and erythomycin, whichare members of a class of compounds called polyketides. Scientists have discovered more than 10,000polyketides, including many useful drugs, but the percentage of medically useful compounds in the totalnumber of discovered natural polyketides has decreased in recent years (Lipkin, 1995). McDaniel et al.,(1995) have categorized the enzymes involved in the synthesis of polyketides and constructed plasmidsthat contain genes for those enzymes. When expressed in S. coelicolor, the genes on the plasmidsresulted in the synthesis of new polyketides.
Based on their understanding of the activities of the enzymes, McDaniel et al., (1995) devised rules forthe bioengineered synthesis of polyketides, and they suggested that chemists will be able to generatebioengineered (unnatural) products that will be as diverse as the thousands of polyketides already seenin nature. The expectation is that medically useful compounds will be generated.
(continued)

Chapter 5 Antibiotic Development | 115
OS designed to lower the risk of infant infectionsis modeled after naturally occurring OS found inmothers’ milk (Neose Pharmaceuticals, 1994).
Microbial resistance to OS is predicted to besmall because two independent genetic eventswould have to take place. First, the bacteriumwould have to mutate so that it would no longerbind to the OS; that would also make it non-infective because it could not bind to OS on cellsurfaces. Only a second mutation that produced a
mechanism to bind to another molecule on thesurface of the stomach cell could restore bacte-rial infectivity.
❚ Antibiotic PeptidesAmong the most widely studied of the “new”antibiotics are peptide antibiotics. Within thislarge group of molecules are bactericidal/perme-ability increasing proteins (BPI), magainins, andcecropins.4 Their common antimicrobial activity
4 These agents are included here to be illustrative; this list is not inclusive. J.E. Gabay provides a short description of these and some otherantimicrobial peptides as well as a useful reference list in “Vbigitous and natural antibiotics,” Science 264:373–374, 1994.
In vivo Expression Technology
Traditional research has sought microbial virulence factors by culturing and growing microbes in thelaboratory and then examining the products of bacterial growth that are present in the culture broth. Well-known examples of such products are diphtheria and cholera toxins which were used for vaccine devel-opment.
Mekalanos and his colleagues (Mahan, Slauch, and Mekalanos, 1993) acted on the idea that bacteriaare “Trojan Horses,” hiding their virulence factors and toxins until specific host signals cause them to bereleased. Such genes would cause the production of proteins that could be the targets for antibiotics orantigens for the production of vaccines. Mahan et al., (1993) call the technology to explore such hiddenbacterial strategies “in vivo expression technology” (IVET), which has been heralded as “revolutionary”(Barinaga, 1993).
IVET may be applied to the problem of antibiotic resistance in at least two ways. First, it can identifynew antimicrobial targets. Nearly half of the Salmonella genes detected with IVET were previouslyunknown. The products of these genes are potential targets for new antibiotic design. Second, IVET mayguide production of new vaccines, as previously unknown products of IVET-identified genes give vaccine
developers new immunogens against which humans can be inoculated.
Antibiotics Targeted Against a Bacterial Regulatory System
In bacteria, some RNA synthesis depends on a two-step regulatory system. The first component is asensor protein in the bacterial membrane that can detect a signal in the environment, say, a sugar orother nutrient of use to the bacterium. In response, the sensor chemically adds a phosphate to itself andto another protein, the transducer. The phosphorylated transducer then activates RNA synthesis fromspecific sites on the DNA, and the RNA is used to direct synthesis of enzymes necessary to transport thenutrient into the bacterial cell, for its metabolism, or for some other aspect of biochemistry associated withthe nutrient.
Virulence genes, as detected by IVET or other methods, are probably regulated by a two-componentsystem, with the sensor detecting some chemical in the host animal or host cell. A substance that inter-feres with the regulatory system might be a useful antibiotic, and such substances have been described.The two-component regulatory system does not exist in mammalian cells, making toxic side effects fromsuch antibiotics unlikely (Salyers and Whitt, 1994).
BOX 5-2: Some New Methods for Research in Antibiotics (Cont’d.)

116 | Impacts of Antibiotic-Resistant Bacteria
results from increasing bacterial permeability,and in this regard they are similar to the topicalpeptide antibiotic polymyxin B, produced by thebacterium Bacillus polymyxa. Scientists, how-ever, know few specifics about their mechanismsof action (Gabay, 1994). New technologies thatallow researchers to synthesize and screen “com-binatorial libraries” consisting of tens of millionsof natural and synthetic peptides (Blondelle etal., 1994) have increased the capacity to makeand test candidate peptide antibiotics.
Bactericidal/Permeability Increasing PeptideWeiss et al. (1978) reported isolation of a bacte-ricidal protein from human and rabbit cells thatappeared to cause an “almost immediate” break-down of the bacterial permeability barrier to theentry of the antibiotic actinomycin D. While BPIwas bactericidal to several strains of E. coli andSalmonella typhimurium, both Gram-negatives,it had no effect on Gram-positive bacteria or theyeast Candida.
Using molecular biology techniques, scientistsproduced a fragment of the BPI molecule (calledrBPI-23) that increased bactericidal activity,including activity against penicillin-resistant strainsof Streptococcus pneumoniae (Lambert, 1994),and enhanced the efficacy of co-administeredantibiotics (Meszaros et al., 1994). Human sub-ject testing has recently begun with another frag-ment (rBPI-23). When administered along withlow doses of endotoxin, a toxin produced byGram-negative bacteria, rBPI-23 blunted theadverse effects of the endotoxin, was well toler-ated by the volunteers, and was not immunogenic(von der Mohlen, 1994).
MagaininsScience, like all human pursuits, has its ownfolklore, and the discovery of the magaininspassed immediately into the legends of science.In the late 1970s, a researcher at the NationalInstitutes of Health was studying RNA expres-sion in the African clawed frog, Xenopus laevis.He noted that the frogs never developed post-operative inflammation or wound infections–
even though surgical procedures were performedunder non-sterile conditions–and he wondered if“there might be a ‘sterilizing’ activity in theskin.” Zasloff (1987) isolated two closely relatedpeptides with broad-spectrum bactericidal activ-ity that were also active against some single-celled parasite species. He named the two pep-tides “magainin 1" and “magainin 2" (Hebrewfor “shield”).
The magainins are short peptides that insertinto the bacterial cell membrane and open upchannels that lead to the death of the bacteria.Thousands of magainin analogues have beensynthesized with the goal of increasing antimi-crobial activity (Cuervo et al., 1988). One magai-nin, MSI-78, is now in phase III trials, which areexpected to be completed in mid-1996. If thatschedule is kept, Magainin Pharmaceuticalsexpects to file an NDA at the end of that year forthe sale of MSI-78 as a topical antibiotic (Magai-nin Pharmaceuticals, 1994); however, an earliertrial of this magainin against impetigo wassuspended because of disappointing results.Other magainins are undergoing toxicity tests inanimals in expectation that they will find appli-cation as systemic antibiotics.
CecropinsCecropins are peptides from the North Americansilk moth, Hyalophora cecropia. They are simi-lar in size to the magainins, and like the magain-ins, they increase bacterial permeability.Researchers have chemically combined cecropinwith another natural peptide antibiotic, mellitin,derived from bee venom. The resulting productdemonstrated activity against S. aureus and Pla-modium falciparum (Blondelle and Houghten,1992). More recently, a recombinant cecropin/mellitin hybrid was shown to be bactericidalagainst Pseudomonas aeruginosa. Other antimi-crobial cecropins and cecropin-like moleculeshave been recently isolated from the hemolymphof the silk worm Bombyx mori, the male repro-ductive tract of the fruitfly Drosophila melano-gaster, and from the intestines of pigs.

Chapter 5 Antibiotic Development | 117
DefensinsDefensins are broad-spectrum antimicrobial pep-tides isolated from mammalian cells, includingepithelial cells lining the human small intestine(Blondelle and Houghten, 1992). Although simi-lar in size to magainins and cecropins, defensinsdiffer in chemical structure. The isolation of arelated group of molecules isolated from cow air-ways, called “ß-defensins,” has added to the the-ory that defensins form a natural, primarymucosal defense against microbial pathogensand are therefore potentially powerful new anti-microbial agents (Taylor, 1993).
❚ Lactoferrin, a Substance with Antibiotic Properties from Human MilkLactoferrin, the second most abundant protein inhuman milk, is bacteriostatic in vitro and in tis-sue culture tests against a variety of bacteria,including MRSA. Three different mechanismscontribute to the bacteriostatic activity of lacto-ferrin: It binds iron, thereby depriving bacteria ofthat essential element, it increases bacterialpermeability, and it activates immunologicaldefenses. Ward et al., (1995) recently described amethod to produce human lactoferrin in the labo-ratory, and the product has the same antibioticproperties as the human protein. Pre-clinicalstudies are now under way with the laboratory-produced chemical (Ward et al., 1995; Wyatt,1995).
Human milk has antibacterial properties, andsome of those properties reside in lactoferrin.Lactoferrin is also found in other external secre-tions—tears, nasal secretions, saliva, and genitalsecretions—all of which have antibacterial prop-erties. Those secretions have been around formillions of years and they are still effectiveagainst bacteria. Development of lactoferrin, orother substances with antibiotic activity fromhumans, as antibiotics might provide therapiesthat will not elicit resistance.
Like all the protein antibiotics, lactoferrin pre-sents administration difficulties because theycannot be absorbed from the digestive tract,thereby eliminating oral uses. They can be used
topically, as polymyxin B, and they may find useagainst enteric infections and pulmonary infec-tions, where they might be administered by aspi-ration.
❚ Steroid AntibioticsThe discoverer of magainins also wondered overthe rarity of infections in fetal dogfish sharks(Squalus acanthis), despite the fact that mothersharks flush their fallopian tubes regularly withseawater to remove fetal wastes. Moreover, henoted that the sharks rarely became infected aftersurgery. Using the same methodology as the oneused for magainins, he and co-workers success-fully isolated squalamine from shark stomach,liver, gall bladder, spleen, testes, gills, and intes-tine. Squalamine is a steroid compound, closely-related to cholesterol (Moore et al., 1993) andhas antimicrobial activity against both Gram-positive and Gram-negative bacteria as well asfungi and protozoa. Testing of squalamine is nowat the pre-clinical stage.
❚ “Anti-Sense” NucleotidesOne of the more frequently proclaimed “magicbullets” against drug-resistant bacteria is “anti-sense” molecules (Stein and Cheng, 1993) thatbind to critical DNA or RNA segments in thebacterial cell and disrupt their functioning. Avariety of new technologies, many developed forapplication in the federally funded HumanGenome Project, allow for simpler and morerapid DNA sequencing and have made investiga-tions of anti-sense therapy feasible.
Like many new therapies, the oligionucle-otides (ON), the segments of DNA and RNAmolecules that would be used as anti-sense mole-cules, present many challenging problems. Newtechnologies need to be developed for the bulksynthesis of ON and to transport ON through thebody and inside bacterial cells, and methods mayhave to be developed to deliver the ONs to theircomplementary DNA or RNA target (Rahman etal., 1991). “Oligonucleotide-like” molecules willbe required to circumvent the instability andrapid degradation of ON in the body, and some

118 | Impacts of Antibiotic-Resistant Bacteria
such molecules have been synthesized andshown to have improved stability.
GETTING NEW ANTIBIOTICS TO MARKETThis chapter reviews some ideas for new antibi-otics, and any of those ideas will require signifi-cant investments to support the research anddevelopment necessary to bring it through clini-cal trials and to market. In 1993, OTA (1993)comprehensively reviewed the return on invest-ments in pharmaceutical research and develop-ment. This section contains a brief review ofsome of the issues related to pharmaceuticaldevelopments specifically focused on antibiotics.
Antibiotics are used for short periods of time,and representatives of some pharmaceuticalcompanies claim that greater profit is to be madein developing drugs for chronic illnesses such asheart disease and arthritis, for which drugs maybe necessary every day for years at a time. Thecounter-argument to that contention is that a life-saving drug with no alternative, even if used onlyrarely, can command a high price. Resistancelimits the market life of antibiotics: As they losesome of their efficacy, they become less profit-able. At the same time, antibiotic resistanceopens up new markets.
Participants at OTA advisory panel meetingssaid that major pharmaceutical companies arenot likely to mount a research and developmenteffort for potential annual markets of less than$100 million. They also stated that some smallercompanies, generally lumped under the rubric of“biotech firms,” could do very well on a marketof $20 to $30 million a year.
Some antibiotics, however, have generatedmajor markets. As shown in box 5-3, a singleantibiotic can account for 15 percent of a majormanufacturer’s sales. Such a percentage is proba-bly unusual, but it indicates that an antibiotic canbe a major source of revenue.
A new antibiotic that overcomes resistancehas a ready market. There are approximately19,000 VRE cases yearly. If an antibiotic effec-tive against VRE were developed, OTA assumesthe company that marketed it could charge a highprice because no other antibiotic is available forthat use, but OTA did not try to estimate thatprice. There are about 60,000 MRSA cases annu-ally, and some proportion of those are treatableonly with vancomycin. For illustrative purposes,OTA assumes that all 60,000 cases are nowtreated with vancomycin, that the antibiotic costs$100 per day, and that the treatment requires 10days. That market is then $60 million annually(60,000 cases per year × $100 per day × 10 daysof treatment per case), and the new antibioticwould be competing for that market with vanco-mycin.
A major company might not be interested inthis market; it is well below $100 million peryear. But the new antibiotic could probably beused for many other infections, and the marketcould be much larger, with, most likely, earlieremergence and spread of resistance than if theantibiotic were restricted to use against MRSA.
Whatever the size of market for an antibiotic,it is expected to erode with the development ofantibiotic-resistant bacteria. Control of the emer-gence and spread of resistance would result in alonger market life and greater sales and profits.However, the major way known to slow downresistance is to minimize the use of the antibiotic,which would have an adverse effect on sales andprofits, at least in the short run. To return to thehypothetical example of an antibiotic to treatMRSA, restricting the use of the drug would pro-long its effectiveness before resistance devel-oped. That restriction would also reduce salescompared to those expected if there were unre-stricted use against all respiratory infections, forexample. This tradeoff is discussed further in thefollowing section.

Chapter 5 Antibiotic Development | 119
BOX 5-3: Patent Protection and Post-Patent Hurdles for Competitors(News media clips)
“Generic Erosion for Ceclor?
“When Lilly’s Ceclor (cefaclor) comes off patent in the U.S. in 1992, unit sales of the antibiotic, whichaccount for roughly 15 percent of the company’s total sales, could be eroded by 70 to 80 percent bygeneric competition in the first 18 months, according to Kidder, Peabody analyst James Flynn.
“This erosion will take place despite the fact that Lilly holds process patents for Ceclor which expirebetween 1994 and 2006, and plans to introduce a sustained-release formulation, Ceclor AF, the analystpredicts.
“Recent legal action in Japan, where Lilly has filed suit against 10 companies for alleged infringementof its cefaclor patent, suggest that the company intends to defend its patents vigorously.... However, Mr.Flynn argues that Lilly’s process patents will not be recognized in a number of countries (e.g., Italy) whichare likely to be used as manufacturing sites for generic companies planning to import formulations ofcefaclor on expiration of the product patent.
“Barr and Biocraft, which have valid cephalosporin manufacturing facilities in the U.S., may also try to‘skirt’ Lilly’s process patents, Mr. Flynn says. Such a strategy would give these companies a ‘meaningfulcost advantage’ over importing firms, he adds.
“Ceclor AF is unlikely to be introduced in the United States much before the cefaclor product patentexpires, Mr. Flynn says. A preferred dosing regimen is the only benefit he is aware Ceclor AF would haveover generic competition. The analyst notes that Lilly’s keftabs formulation of Keflex (cefalexin) gainedless than 15 percent of Keflex’ sales after the 1987 product patent expired.”
SOURCE: “Generic Erosion for Ceclor,” Scrip World Pharmaceutical News 1594:25, 1991.
“Ceclor Market Dominance Will Continue Past Dec. 1992 Patent Expiration, Lilly Contends: Process Protection Thru 1994
“Lilly’s dominant position in the oral antibiotic market will survive the expiration of the U.S. patent onCeclor in December 1992, the company maintained at a meeting with financial analysts in New York onFeb. 28. Based on a process protection for cefaclor and a pending NDA application for the follow-upcompound loracarbef, Lilly is forcefully declaring its intention to hold its place in the oral antibiotic field....
“Asked to comment on the impact of the upcoming patent expiration on Ceclor sales, Lilly Pharmaceu-tical President Gene Step said the relevant questions should be what will be Lilly’s overall position in theoral antibiotic market and what is the likelihood of generic versions of cefaclor reaching the market.
“‘You really have to [ask] what is our participation in the oral antibiotic market and to what extent willthat be affected’ by generic cefaclor or ‘by other products that we may or may not be selling’ in the future,Step said.
“Lilly is emphasizing the de facto protection of a difficult production process and a patent position ona late-stage intermediate... Step declared that when all factors are considered Ceclor should ‘remain aviable product for Eli Lilly beyond expiration of the patent.’
“As the company often has been pointing out recently, Step told the Feb. 28 meeting that Ceclor hasyet to face generic competition outside the U.S., even in markets where there is no patent protection.‘While we cannot know what the actions of everybody else in the world will be,’ Step said, ‘it is very inter-esting to observe that while there isn’t patent coverage in a large part of the world for Ceclor, there isn’tany generic Ceclor.’
(continued)

120 | Impacts of Antibiotic-Resistant Bacteria
PATENTSPatents provide the primary protection for apharmaceutical company’s investment inresearch, development, marketing, and produc-tion costs. The 1991 OTA report, Biotechnologyin a Global Economy, described the patent pro-cess for pharmaceuticals:
Drug companies usually secure patent pro-tection early in drug development, before thedrug enters the regulatory process. Regulatoryapproval for new drugs takes, on average, 7 to10 years to complete. This translates into a 7- to10-year reduction in [the usual 17-year] patentprotection for pharmaceutical products whenthey reach the market, leaving such productswith, on average, 9 years of protected life.....
[T]he Drug Price Competition and Patent TermRestoration Act of 1984... restores part of thepatent life lost due to lengthy regulatoryapproval. The act allows extension of the patentterm for up to 5 years, but it does not allowextension beyond 14 years for effective patentlife. The actual extension granted is equal to thetotal time taken by the Food and Drug Adminis-tration (FDA) to review the New Drug Applica-
tion, plus one-half of the clinical testing time. Inaddition, the act promotes generic competitionby providing FDA with an Abbreviated NewDrug Application (ANDA) process. This pro-cess facilitates the approval of generic drugs byeliminating the need for costly clinical studies.An ANDA does require the sponsoring com-pany to demonstrate its generic’s bioequiva-lence to the pioneer drug. This is much lesscostly and time-consuming than complete clini-cal trials and facilitates the market entrance ofgeneric drugs.
The GATT (General Agreement on Tariffsand Trade) legislation changed patent terms from17 years from issuance to 20 years from filing(OTA, 1991, discusses the nuances of theseterms), and in March 1995, the U.S. Patent andTrademark Office (PTO) announced a prelimi-nary policy statement that extensions would beadded to the new 20-year patent term. In June1995, however, PTO reversed its position andpresented manufacturers a choice between add-ing any extension they had to the 17-year term oraccepting the 20-year term under GATT. Manu-facturers are expected to challenge this decisionin court.
“Lilly Research Labs President Mel Perelman explained the process protection during question-and-answer. ‘The Ceclor synthetic route is so long and so complex’ that it will be difficult to duplicate, Perel-man said....
“A producer of cefaclor can take a number of different routes to get to the intermediate, Perelmanexplained, ‘but they can’t go through it without violating our patent. So an ethical or legal end-run seemsextremely improbable.’ The patent on the intermediate runs until December 1994. Step further pointed outthat establishing a cefaclor manufacturing process ‘will require very considerable capital investment...wehaven’t seen that yet’....”
SOURCE: Ceclor market: Quoted from “Ceclor Market Dominance Will Continue Past Dec. 1992 Patent Expiration, Lilly Contends:Process Protection Thru 1994, Lorabid NDA Filed as Backup,” FDC Reports: Prescription and OTC Pharmaceuticals, March 4,1991. p. 15.
“Ivax Corp. faces lawsuit from Eli Lilly”
In 1995, Eli Lilly sued Ivax Corporation, a pharmaceutical company that announced that it hadreceived FDA approval to manufacture cefaclor capsules, a generic version of Lilly’s Ceclor. Lilly claimedthat Ivax’s supplier of a raw material used a process that infringes on Lilly’s process patents.
SOURCE: Ft. Lauderdale, FL Sun-Sentinel. 1995. April 29, 1995. p. 8B.
BOX 5-3: Patent Protection and Post-Patent Hurdles for Competitors(News media clips) (Cont’d.)

Chapter 5 Antibiotic Development | 121
Members of the OTA advisory panel dis-cussed the pluses and minuses of a negotiatedagreement between a manufacturer and the PTOto extend the patent life of an antibiotic inexchange for restrictions on its use. Again, con-sider the example of an antibiotic effectiveagainst MRSA. Could PTO, FDA, and the manu-facturer work out an agreement so that the antibi-otic was marketed only for use against MRSA?Such an agreement would have a positive impacton the emergence of resistance, but it wouldpresent supervision or enforcement problems toassure that the restrictions were followed. Itwould also present problems for the manufac-turer in estimating its returns from unrestrictedsales over a few years—until resistance becomescommon—as compared to restricted sales overmore years. How soon resistance would arise inboth cases is difficult to estimate, as are thechances of another company developing a com-parable or better drug.
Many compounds are patented but neverbrought to market. If, subsequently, it was dis-covered that such a compound was useful againstantibiotic-resistant bacteria, probably no firmwould be interested in conducting the tests andtrials necessary to bring it to market. Withoutpatent protection, the firm that paid for the testsand trials would be unable to recover its costs.Fusidic acid, an antibiotic that has been used inDenmark and other countries since 1962 (Man-dell and Sande, 1995), provides a real-life exam-ple of such a drug. Fusidic acid is active againstat least some strains of MRSA, and it is usedagainst those bacteria in other countries. It hasnever been marketed in the United States,although it can be made available under compas-sionate use procedures to physicians in this coun-try. Because it is off-patent, the company thatdeveloped and sells it elsewhere is not willing tofund clinical trials that would be necessary toobtain FDA approval for its being marketed foruse against MRSA here.
Patent protection of the chemical substance isnot the only method by which companies canmaintain their markets. OTA (1993, p. 82-87)describes how complicated and expensive pro-
duction methods and facilities can be a majorhurdle for competitors, especially when themethods and facilities are protected with processpatents. For example, in 1995, Ivax Corporationannounced it had received FDA approval to man-ufacture a generic version of a cephalosporin onwhich the patent had expired in 1992. Eli Lillysued Ivax, claiming that Ivax’s supplier of a rawmaterial used a process that infringed uponLilly’s process patents (Fort Lauderdale Sun-Sentinel, 1995).
PRICING OF DRUGS DEVELOPED IN PART BY FEDERAL RESEARCHThe Federal Technology Transfer Act of 1986(P.L. 99-502) authorized the establishment ofCRADAs (Cooperative Research and Develop-ment Agreements) between federal intramurallaboratories and private industry to bring inven-tions and discoveries in federal laboratories tomarket. In exchange, the private industries wouldreceive the profit from sales of the developedproducts. In 1989, Congress directed theNational Institutes of Health (NIH) to require“reasonable pricing” of any drugs that weredeveloped in cooperation between its laborato-ries and industry. Industry objected to the restric-tions on pricing, and, in April 1995, NIHrelinquished its right to require reasonable pric-ing.
This change is expected to have little affect onantibiotics. While the federal government con-ducts research on antiviral and antifungal agents,it has supported little research on antibacterials,leaving that research to the pharmaceutical firms,and none of the six products that had been devel-oped as of April 1995 through CRADAs was adrug (Health News Daily, 1995).
CONCLUSIONSAntibiotic research and development, as almostall drug research and development in the UnitedStates, is carried out and sponsored by pharma-ceutical companies. Recent years have seen theintroduction of few new antibiotics into the mar-

122 | Impacts of Antibiotic-Resistant Bacteria
ket, which may reflect a diminished researcheffort in antibiotics five, 10, and more years ago.
Currently, there is a great deal of activity inlooking for substances with antibiotic propertiesin biological sources that have not been exploitedin the past and in applying new molecular bio-logic and chemical techniques to the synthesis ofantibiotics and to understanding their mecha-nisms of action. On the positive side, some of thecompounds being considered as possible antibi-otics have mechanisms of action different fromthose of currently used antibiotics, and theyshould be especially useful against bacteria nowresistant to many or all currently available antibi-otics. Despite that promise, there is great uncer-tainty about if and when there will be a pay-offfrom the research efforts, and few experts expectcommercial availability of any antibiotics withnew mechanisms of activity in this century. Theuncertainty about availability of new antibioticsunderlines the importance of efforts to reduce theemergence and spread of bacteria resistant tonow-used antibiotics.
The emergence of antibiotic-resistant bacteriaproduces new market opportunities, and it can beexpected that pharmaceutical firms will be inter-ested in developing products for it. Some expertsargue, however, that the profits to be expectedfrom an antibiotic are smaller than those fromother drugs and that pharmaceutical firms willfocus their efforts on other, more profitabledrugs. On the other side of that argument, anantibiotic that is effective against an infectionresistant to all other antibiotics could probably besold at a very high price.
REFERENCESBalbes, L.M., S.W. Mascarella, and D.B. Boyd.
1994. A perspective of modern methods incomputer-aided drug design. ComprehensiveReviews Chemistry 5:337-379.
Barinaga, M. 1993. New technique offers a win-down on bacteria’s secret weapons. Science259:595.
Bergeron, J., L. Wondrack, M. Ammirate, et al.1994. Glycycyclines evade both ribosomal
and efflux tetracycline resistance mecha-nisms. Presented at First International Con-ference on Antibiotic Resistance: Impact onDiscovery. Englewood, CO. Sept. 1994.
Blondelle, S.E., and R.A. Houghten. 1992.Progress in antimicrobial peptides. AnnualReports in Medicinal Chemistry 27:159-168.
Blondelle, S.E., E. Takahashi, P.A. Weber, et al.1994. Identification of antimicrobial pep-tides by using combinatorial libraries madeup of unnatural amino acids. AntimicrobialAgents and Chemotherapy 38:2280-2286.
Boyd, D.B. and S.A.F. Milosevich. 1993. Super-computing and drug discovery research.Perspectives Drug Discovery and Design1:345-348.
Bristol-Meyers Squibb. 1995. The “Hand-Offs”at Bristol-Myers Squibb. BiotechnologyIndustry Advertising Supplement. Science267:1692.
Bushby, S.R.M., and G. H. Hitchings. 1968. Tri-methoprim, a sulfonamide potentiator. Brit-ish Journal of Pharmacology andChemotherapy 33:72-90.
Buttle, G.A.H., W.E. Gray, and D. Stephenson.1936. Protection of mice against streptococ-cal and other infections by p-aminobenzene-sulphonamide and related substances.Lancet i:1286-1290.
Colebrook, L., and M. Kenny. 1936. Treatmentof human puerperal infections, and of exper-imental infections in mice with prontosil.Lancet i:1279-1286.
Cuervo, J.H, B. Rodriguez, and R.A. Houghten.1988. The magainins: sequence factors rele-vant to increased antimicrobial activity anddecreased hemolytic activity. PeptideResearch 1:81-86.
Eli Lilly and Company. 1995. Lilly announcesdevelopment of a compound to address anti-biotic resistance. Press release, March 28.
Emori, T.G. and R.Y. Gaynes. 1993. An over-view of nosocomial infections, including therole of the microbiology laboratory. ClinicalMicrobiology Reviews 6:428-442.
Fan, C., P.C. Moews, C.T. Walsh, et al.1994. Vancomycin resistance: Structure
Chapter 5 Antibiotic Development | 123
of D-alanine:D-alanine ligase at 2.3 ang-strom resolution. Science 266:439-443.
Fekety, R. 1995. Vancomycin and teicoplanin.In: G.L. Mandell, J.E. Bennett, and R. Dolin(eds.) Mandell, Douglas and Bennett’s Prin-ciples and Practice of Infectious Diseases.Churchill Livingstone: New York, NY. pp346-354.
Fort Lauderdale (FL) Sun-Sentinel. 1995. IvaxCorp. faces lawsuit from Eli Lilly. April 29.p. 8B.
Frankel, D.H. 1995. Designing New Antibiotics.Contractor report to the Office of Technol-ogy Assessment. Photocopied typescript.January.
Frieden, T.R. and R.J. Mangi, 1990. Inappropri-ate use of oral ciprofloxacin. Journal Ameri-can Medical Association 264:1438-1440.
Gabay, J.E. 1994. Ubiquitous natural antibiotics.Science 264:373-374.
George, J. 1994. Biopharmaceutical companyraises $10M. Philadelphia Business Journal13:1,27.
Georgopapdakau, N.H., A. Bertasso, K.K. Chan,et al. 1989. Mode of action of the dual-actioncephalosporin Ro-23–9424. AntimicrobialAgents and Chemotherapy 33:1067-1071.
Georgopapdakau, N.H., and A. Bertasso. 1993.Mechanisms of action of cephalosporin 3’-quinolone esters, carbamates, and tertiaryamines in Escherichia coli. AntimicrobialAgents and Chemotherapy 37:559-565.
Glaser, V. 1994. Carbohydrate biotechnologyenters the domain of rational drug design.Genetic Engineering News, July, p. 6,7,11.
Gootz, T.D. 1990. Discovery and developmentof new antimicrobial agents. Clinical Micro-biology Reviews 3:13-32.
Griffin, J.H. 1994. Research summary. Depart-ment of Chemistry, Stanford University,Palo Alto, CA (data on file).
Health News Daily. 1995. NIH removes “reason-able price” clause from standard CRADAagreement. April 12, p. 2-3.
Hooper, D.C. and J.S. Wolfson. 1989. Bacterialresistance to the quinolone antimicrobial
agents. American Journal Medicine 87(suppl 6C):17S-23S.
Hughes, S. 1994. Carbohydrate researcha newsource of therapeutics. Scriptorium Apr., pp.28-31.
Husain, R.A. 1991. Disturbing susceptibility pat-tern for ciprofloxacin. American JournalPublic Health 48:1892.
Journal of Antimicrobial Chemotherapy. 1992.RP 59500: a semi-synthetic injectable strep-togramin antibiotic. Supplement A to Vol-ume 30, July.
Knox, J.R. 1993. Crystallography of penicillin-binding enzymes. In: Bentley, P.H. and R.Ponsford (eds.) Recent Advances in theChemistry of Anti-infective Agents. RoyalSociety of Chemistry: Cambridge, England.pp. 37-49.
Kuntz, I.D. 1992. Structure-based strategies fordrug design and discovery. Science257:1078-1082.
Lambert, L. 1994. rBPI-21 kills both gram-positive and gram-negative bacteria. Paperpresented at 34th Interscience Conference onAntimicrobial Agents and Chemotherapy.Orlando, FL. Oct. 4-7.
Levy, S.B. 1981. The tetracyclines: microbialsensitivity and resistance. In: G.G. Grassi,and L.D. Sabath (eds.) New Trends in Anti-biotics: Research and Therapy. Elsevier/North Holland Biomedical Press: New York,NY. pp. 27-44.
Levy, S.B. 1992. The Antibiotic Paradox. Ple-num Press: New York.
Lipkin, R. 1995. New “design rules” yield noveldrugs. New Scientist 147:374.
Magainin Pharmaceuticals, Inc. Plymouth Meet-ing, PA. 1994. (data on file).
Mahan, M.J., J.M. Slauch, J.J. Mekalanos. 1993.Selection of bacterial virulence genes thatare specifically induced in host tissues. Sci-ence 259:686-688.
Mandell, G.L., and M.A. Sande. 1990. Antimi-crobial agents (continued). In: A.G. Gilman,T.W. Rall, A.S. Nies, et al. (eds.) The Phar-macological Basis of Therapeutics. Perga-mon Press: New York, NY. pp.1047-1065.
124 | Impacts of Antibiotic-Resistant Bacteria
McDaniel, R., S. Ebert-Khosla, D.A. Hopwood,and C. Khosla. 1995. Rational design of aro-matic polyketide natural products by recom-binant assembly of enzymatic subunits.Nature 375:549-554.
Meszaros, K., S. Aberle, K. Lin, and J.B. Parent.1994. Recombinant fragment of bactericidal/permeability increasing protein (rBPI-21)and complement activation by Lipid A andrough bacteria. Paper presented at 34thInterscience Conference on AntimicrobialAgents and Chemotherapy. Orlando, FL.Oct. 4-7.
Modern Healthcare. 1994. Restraint on use ofantibiotics urged. June 13, p. 47.
Moore, K.S., S. Wehrlii, H. Roder, et al. 1993.Squalamine: an aminosterol antibiotic fromthe shark. Proceeding of the National Acad-emy of Science 90:1354-1358.
Mulligan, M.E., K.A. Murray-Leisure, B.S. Rib-ner, et al. 1993. Methicillin-resistant Staphy-lococcus aureus: A consensus review of themicrobiology, pathogenesis, and epidemiol-ogy with implications for prevention andmanagement. American Journal Medicine94:313-328.
Nelson, M.L., B.H. Park, J.S. Andrews, et al.,1993. Inhibition of the tetracycline effluxantiport protein by 13-thio-substituted 5-hydroxy-6-deoxtetracyclines. Journal ofMedicinal Chemistry 36:370-377.
Nelson, M.L., B.H. Park, and S.B. Levy. 1994.Molecular requirements for the inhibition ofthe tetracycline antiport protein and theeffect of potent inhibitors on the growth oftetracycline-resistant bacteria. JournalMedicinal Chemistry 37:1355-1361.
Neose Pharmaceuticals, Inc. Horsham, PA. 1994.(data on file).
Nikaido, H. 1994. Prevention of drug access tobacterial targets: permeability barriers andactive efflux. Science 264:382-388.
Pfizer, Inc. 1993. Advertising folder for azithro-mycin antibiotic. Pfizer U.S. Pharmaceu-tials Group, New York, NY.
Rahman, M.A., J. Summerton, E. Foster, et al.1991. Antibacterial activity and inhibition ofprotein synthesis in Escherichia coli by anti-sense DNA analogs. Antisense Research andDevelopment 1:319-327.
Reading, C., and M. Cole. 1977. Clavulanic acid:a ß-lactamase inhibiting ß-lactam fromStreptomyces clavuligerus. AntimicrobialAgents and Chemotherapy 11:852-857.
Rhone-Poulenc Rorer. 1995. 1994 SummaryReport: Building for the Future. Report tostockholders. Rhone-Poulenc Rorer, Colle-geville, PA.
Rosenstein, I.J., T. Mizouchi, E.F. Hounsell, etal. 1988. New type of adhesive specificityrevealed by oligosaccharide probes inEscherichia coli from patients with urinarytract infections. Lancet ii:1327-1330.
Roth, S. 1995. Neose Pharmaceutical, Horsham,PA. Personal communication.
Roth, S., and D. Zopf. 1994. Oligosaccharidepharmaceuticals. In: D.B. Weiner, and W.V.Williams (eds.) Biological Approaches toRational Drug Design. CRC Press: BocaRaton, FL. p. 137-147.
Salyers, A.A. and D.D. Whitt. 1994. BacterialPathogenesis. ASM Press: Washington, DC.p. 63-72.
Schaechter, M., G. Medoff, and B.I. Eisenstein(eds). 1993. Mechanisms of Microbial Dis-ease (Second Editon). Williams andWilkins: Baltimore, MD.
Shi, Z., and J.D. Griffin. 1993. Catalysis of car-bamate hydrolysis by vancomycin and semi-synthetic derivatives. Journal of theAmerican Chemical Society 115:6482-6486.
Stachelhaus, T., A. Schneider, and M.A.Marahiel. 1995. Rational design of peptideantibiotics by targeted replacement of bacte-rial and fungal domains. Science 269:69-72.
Steigbigel, N.H. 1995. Macrolides and clindamy-cin. In: G.L. Mandell, J.E. Bennett, and R.Dolin (eds.) Mandell, Douglas and Bennett’sPrinciples and Practice of Infectious Dis-eases. Churchill Livingstone: New York,NY. p. 334-346.

Chapter 5 Antibiotic Development | 125
Stein, C.A., and Y.C. Cheng, Y-C. 1993.Antisense oligonucleotides as therapeuticagents–is the bullet really magic? Science261:1004-1011.
Sum, P-E., V.J. Lee, P.T. Petersen, et al. 1994.Novel glycylcycline derivatives: the design,synthesis and structure-activity relationshipof 7-(substituted)-9(substituted glycylamid)-6dimethyl-6 deoxytetracyclines. Paper pre-sented at 34th Interscience Conference onAntimicrobial Agents and Chemotherapy.Orlando, Fl., October 4-7.
Sum, P.E., V.J. Lee, and F.P. Tally. 1994. Syn-thesis of novel tetracycline derivatives withsubstitution at the C-8 position. TetrahedronLetters 35:1835-1836.
Taylor, R. 1993. Drugs “R” us: finding new anti-biotics at the endogenous pharmacy. Journalof NIH Research 5:59-63.
U.S. Congress, Office of Technology Assess-ment. 1991. Biotechnology in a GlobalEconomy. (OTA-H-494). U.S. GovernmentPrinting Office: Washington, DC.
U.S. Congress, OTA (Office of TechnologyAssessment). 1993. Pharmaceutical R&D:Costs, Risks and Rewards. (OTA-H-522).U.S. Government Printing Office: Washing-ton, DC.
U.S. Department of Health and Human Services,Food and Drug Administration. 1995. Com-ments to OTA on earlier draft of this report.June 16.
von der Mohlen, M. 1994. Effects of rBPI-23 onendotoxin-induced cytokine release and leu-kocyte changes in human volunteers. Pre-sented at 34th Interscience Conference onAntimicrobial Agents and Chemotherapy.Orlando, FL, Oct. 4-7.
Ward, P.P., C.S. Piddington, G.A. Cunningham,et al. 1995. A system for production of com-mercial quantities of human lactoferrin: Abroad spectrum natural antibiotic. Bio/Tech-nology 13:498-503.
Wyatt, R.D., Agennix Inc., Houston, TX. 1995.Personal communication. July 13.
Weiss, J., P. Elsbach, I. Olsson, et al. 1978. Puri-fication and characterization of a potent bac-tericidal and membrane active protein fromthe granules of human polymorphonuclearleukocytes. Journal of Biological Chemistry253:2664-2672.
Zasloff, M. 1987. Magainins, a class of antimi-crobial peptides from Xenopus skin: isola-tion, characterization of two active forms,and partial cDNA sequence of a precursor.Proceeding of the National Academy of Sci-ence 84:5449-5453.
| 127
6
NewTechnologiesfor Infection
Diagnosis andControl
hree major options exist for the controlof bacterial diseases: 1) disrupt or halttransfer of bacteria from person to per-son and from the environment to people,
2) treat cases of disease with antibiotics, and3) prevent disease through vaccination. Thischapter describes diagnostic methods that guidethe selection and use of antibiotics, the use ofvaccines, methods for delivery of high concen-trations of antibiotics to areas of localized infec-tions, devices and materials designed to reducethe transfer of bacteria in the hospital, and sometreatment methods used before the antibiotic age.
The cartoon, which is adapted from one thatoriginally appeared in Science, is a humorouslook at the serious problem posed by bacteriaresistant to all available antibiotics. Some bacte-ria are expected to develop resistance to any anti-biotic introduced into medical practice.Therefore, continued improvement in infectiondiagnosis and control is necessary to optimizethe use of antibiotics and slow the spread ofresistant bacteria.
DIAGNOSTIC METHODSIn the future, science may develop a smalldevice, such as the “tricorder” used in the TVseries Star Trek, that physicians can pass over the
body of a sick person to identify the cause of adisease. Such methods are far in the future, andcurrent techniques used to identify bacteria andsusceptibility patterns are “traditional methods”that have been developed over the last century.Newer methods that involve techniques frommolecular biology and modern instrumenta-tion—not immediately at the level of Star Trek—promise to make identification and characteriza-tion faster and more certain.
❚ Traditional Methods for the Identification of BacteriaSome experts estimate that there may be a mil-lion different bacteria and that scientists haveidentified only one percent (10,000 species) ofthat total. Of those 10,000, only a fraction havebeen associated with human diseases.
When seeing a patient, a physician will askquestions, make observations, and perform teststo determine which bacteria are likely to be asso-ciated with an illness and to choose an antibiotictreatment. The physician may swab the throat inthe case of a sore throat or obtain a sample ofurine in the case of a urinary tract infection. Thecollected material on the swab or the urine can bestained with diagnostic dyes, such as the Gramstain (see chapter 2), and examined under a
T
128 Impacts of Antibiotic-Resistant Bacteria
Copyright @ 1995 Sidney Harris. Reprinted with permission,
microscope. Distinctive shapes and stainingproperties facilitate reliable preliminary rapididentification of the bacteria causing infection.
Collected samples may contain such low num-bers of bacteria as to make finding them underthe microscope difficult. The staining propertiesand shapes of the bacteria may not be unique andtherefore not identifiable. The sample may con-tain a mixture of bacteria, as is common in faecalsamples. To identify the bacteria in those cases,the physician sends a biological sample of somekind—a volume of blood or pus or other exudate,a scraping or swab from the throat or otherorifice, a sample of urine or feces—to a micro-biology laboratory.
In the laboratory, the sample is transferred toculture media specifically designed to encourage
the growth of certain pathogenic bacteria and toprevent the growth of others such as commensalbacteria that may be present in samples fromboth healthy and sick individuals. The bacteriathat are able to grow form visible colonies onagar-based media in a Petri dish or grow in brothso that the broth becomes turbid, as apple ciderdoes when yeast grow in it. In both the collectionand handling of the sample, health care personnelmust be careful to avoid contamination with thebacteria that grow literally everywhere, on thepatient’s and physician’s skin, on the surfaces offurniture and unsterilized devices in the examin-ing room, and on apparatus in the diagnostic lab-oratory.
Microbiologists can sometimes look at andsmell the colonies or liquid cultures and, based

Chapter 6 New Technologies for lnfection Diagnosis and Control 129
on their knowledge and experience, identify thebacteria in the sample. They may be able to dis-miss some bacteria from further consideration byrecognizing them as contaminants. Iterative testswith more selective media and biochemical testsmay be used for more specific identification.
Culturing and identification take time. Theshigella that might be present in a fecal sample,or the Escherichia coli that frequently cause uri-nary tract infections, grow quickly, forming col-onies in 24 hours or so, and a laboratory wouldprobably identify them in one or two days. Myco-bacterium tuberculosis grows far more slowly,and six weeks may pass before traditional meth-ods can be used to identify it.
Identifying the bacteria is often critical forchoosing the most appropriate antibiotic therapybecause some antibiotics work better against cer-tain bacteria. But identification does not provideinformation about whether the bacteria are resis-tant to the antibiotic or susceptible to it. “Suscep-tibility tests” are used to determine that.
Traditional Susceptibility TestsInformation about antibiotic-resistance/suscepti-bility is developed by testing the bacteria isolatedfrom the infection against six to 12 different anti-biotics, or more if necessary. The results fromthese tests may support the use of the antibioticthat was empirically selected by the physician,indicate that other antibiotics would work aswell, or show that the disease-causing bacteriaare resistant to the antibiotic empirically chosen.
Jorgensen (1995) describes four methods thatare currently used to determine the antibioticsusceptibility or resistance of bacteria: 1) diskdiffusion tests, 2) broth dilution tests, 3) agardilution tests, and 4) agar gradient methods.
Disk diffusion testsDisk diffusion tests measure the size of a cleararea of no bacterial growth around a sterile paperdisk containing antibiotic. The size of this area,called the “zone of inhibition,” can be measuredand reported directly, or the measurement can becompared to criteria established by the NationalCommittee for Clinical Laboratory Standards
Photo of a disk diffusion (Kirby-Bauer) susceptibility test plate.
Courtesy of James H. Jorgensen, University of Texas Health
Science Center, San Antonio, TX, 7995.
(NCCLS) to classify the bacteria as susceptible,intermediate or resistant (S, I, or R). These testsare well standardized for certain bacteria andmay be highly reproducible. However, disk testsare influenced by many laboratory variables thatcan limit accuracy unless tightly controlled.
O’Brien (1994), who initiated and runs WHO-NET, the World Health Organization-sponsoredsurveillance system for antibiotic-resistant bacte-ria, emphasizes the importance of requiring labo-ratories to report raw data about the size of thezones of inhibition (figures 6-1 and 6-2) to sur-veillance organizations. While laboratories inEurope and North America are consistent in theirmeasurement and reporting of the diameters ofzones of inhibition around antibiotic disks, theyinterpret the meaning of the measurements dif-ferently (figure 6-l). Therefore, data reported aszones of inhibition rather than as interpretationsare necessary to make any valid internationalcomparisons about the prevalence of antibiotic-resistant bacteria.
Broth dilution testsDilution tests measure the concentration of anti-biotic that is necessary to prevent the growth ofbacteria. In these tests, known amounts of bacte-ria are deposited into small test tubes containing
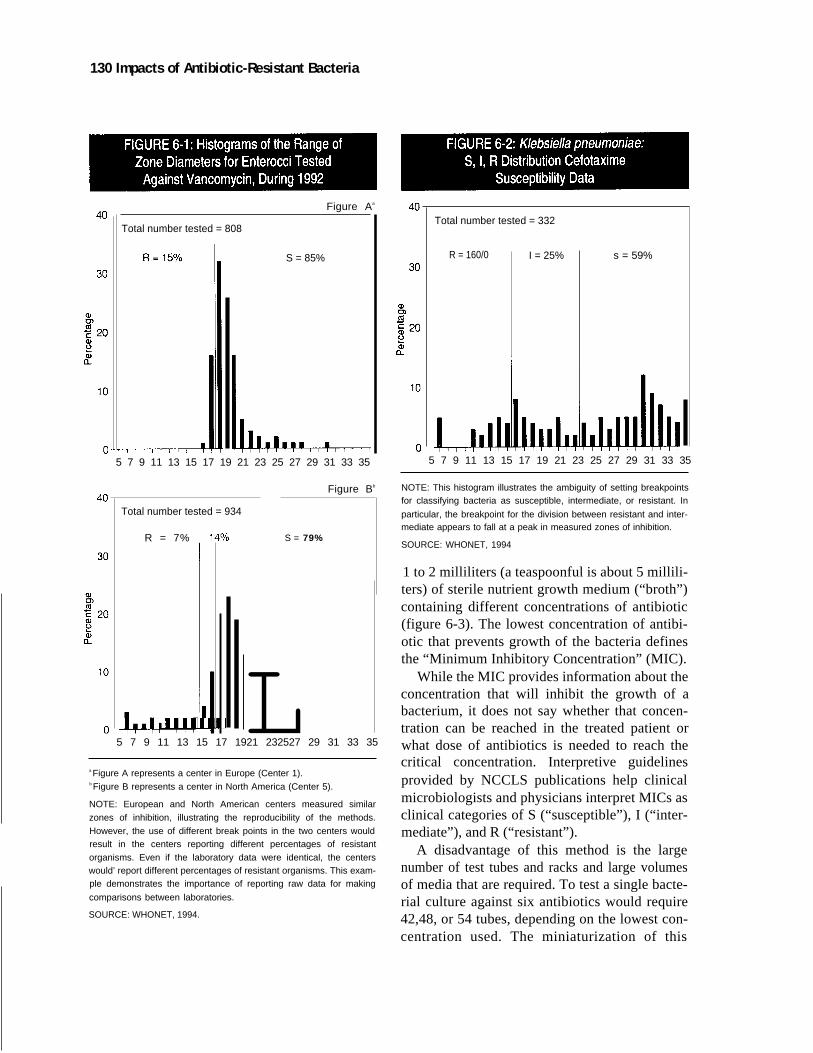
130 Impacts of Antibiotic-Resistant Bacteria
Figure Aa
Total number tested = 808
S = 85%
5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35
Total number tested = 934
R = 7%
Figure Bb
S = 79%
L5 7 9 11 13 15 17 1921 232527 29 31 33 35
a Figure A represents a center in Europe (Center 1).b Figure B represents a center in North America (Center 5).
NOTE: European and North American centers measured similar
zones of inhibition, illustrating the reproducibility of the methods.
However, the use of different break points in the two centers wouldresult in the centers reporting different percentages of resistant
organisms. Even if the laboratory data were identical, the centerswould’ report different percentages of resistant organisms. This exam-ple demonstrates the importance of reporting raw data for making
comparisons between laboratories.
SOURCE: WHONET, 1994.
Total number tested = 332
R = 160/0 I = 25% s = 59%
5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35
NOTE: This histogram illustrates the ambiguity of setting breakpointsfor classifying bacteria as susceptible, intermediate, or resistant. In
particular, the breakpoint for the division between resistant and inter-mediate appears to fall at a peak in measured zones of inhibition.
SOURCE: WHONET, 1994
1 to 2 milliliters (a teaspoonful is about 5 millili-ters) of sterile nutrient growth medium (“broth”)containing different concentrations of antibiotic(figure 6-3). The lowest concentration of antibi-otic that prevents growth of the bacteria definesthe “Minimum Inhibitory Concentration” (MIC).
While the MIC provides information about theconcentration that will inhibit the growth of abacterium, it does not say whether that concen-tration can be reached in the treated patient orwhat dose of antibiotics is needed to reach thecritical concentration. Interpretive guidelinesprovided by NCCLS publications help clinicalmicrobiologists and physicians interpret MICs asclinical categories of S (“susceptible”), I (“inter-mediate”), and R (“resistant”).
A disadvantage of this method is the largenumber of test tubes and racks and large volumesof media that are required. To test a single bacte-rial culture against six antibiotics would require42,48, or 54 tubes, depending on the lowest con-centration used. The miniaturization of this

Chapter 6 New Technologies for lnfection Diagnosis and Control 131
II
2 4 8 16 32
Concentration of antibiotic A(zero time)
Concentration of antibiotic B
o 2 4 8 16 32
Concentration of antibiotic A
2
Concentration of antibiotic B(zero time)
NOTE: In both A and B, a small measured volume of bacterial culture is added to each test tube at time zero, Following incubation (the time ofIncubation depends on the growth characteristics of the bacteria), the test tubes in which bacteria were able to grow are turbid (the first three
tubes in A and all tubes in B). The absence of growth in the last three tubes that contain antibiotic A indicates that the bacteria are killed or inhib-ited by concentrations of A equal to 8 units or more, Growth in all tubes that contain antibiotic B indicates that the bacteria are resistant to all
tested concentrations of antibiotic B
SOURCE: Office of Technology Assessment, 1995.
method with microdilution trays solved thatproblem. The broth micro dilution test is cur-rently the most popular antibiotic sensitivity testin the U.S. (table 6-I; the test using test tubes iscalled the “broth macro dilution test”). The smallsize of the wells and the small volumes, about0.1 milliliter (about a drop from an eye-dropper),require that some viewing device be used todetermine which of the wells in the test plate areclear and which are turbid. There are a number ofcommercial devices that make that determina-tion, and some plot out the MICs from the tests.
To hold down costs and reduce the spaceneeded for incubation of test cultures, many lab-oratories do not use the entire series of dilutions
Photo of a broth microdilution susceptibility test tray with dispos-
able inoculator.
Courtesy of James H. Jorgensen, University of Texas Health
Science Center, Sari Antonio, TX, 7995,
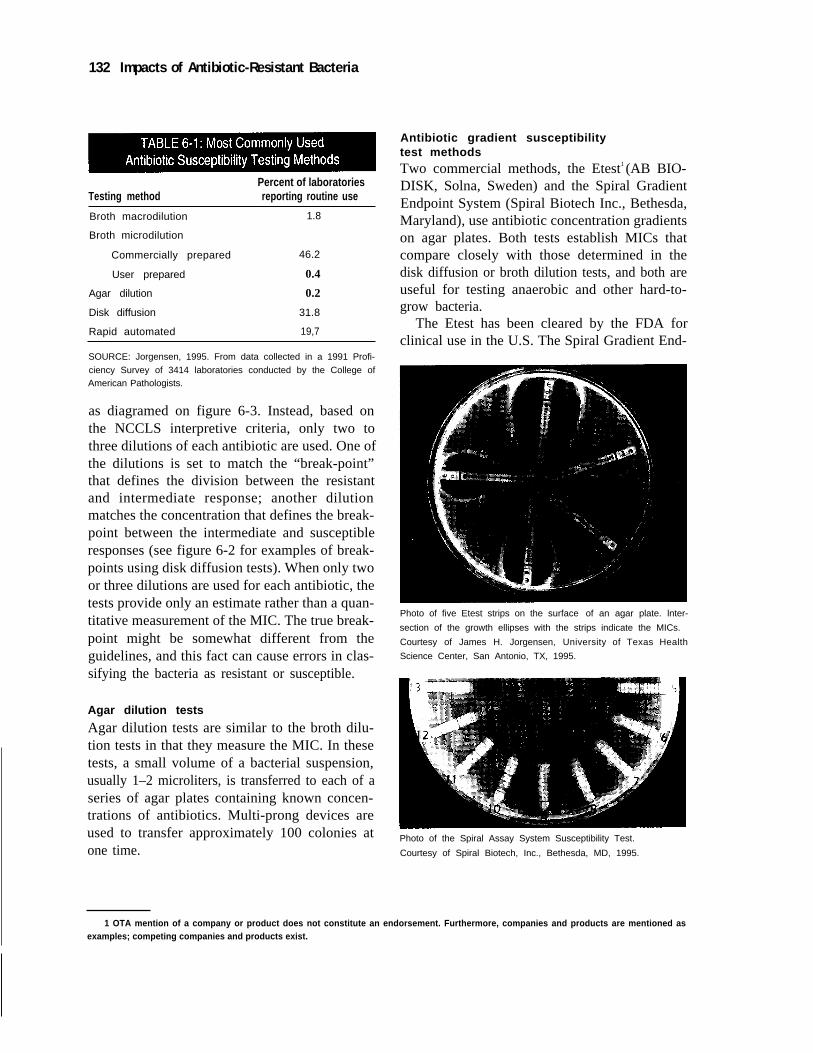
132 Impacts of Antibiotic-Resistant Bacteria
Percent of laboratoriesTesting method reporting routine use
Broth macrodilution 1.8
Broth microdilution
Commercially prepared 46.2
User prepared 0.4
Agar dilution 0.2
Disk diffusion 31.8
Rapid automated 19,7
SOURCE: Jorgensen, 1995. From data collected in a 1991 Profi-
ciency Survey of 3414 laboratories conducted by the College ofAmerican Pathologists.
as diagramed on figure 6-3. Instead, based onthe NCCLS interpretive criteria, only two tothree dilutions of each antibiotic are used. One ofthe dilutions is set to match the “break-point”that defines the division between the resistantand intermediate response; another dilutionmatches the concentration that defines the break-point between the intermediate and susceptibleresponses (see figure 6-2 for examples of break-points using disk diffusion tests). When only twoor three dilutions are used for each antibiotic, thetests provide only an estimate rather than a quan-titative measurement of the MIC. The true break-point might be somewhat different from theguidelines, and this fact can cause errors in clas-sifying the bacteria as resistant or susceptible.
Agar dilution tests
Agar dilution tests are similar to the broth dilu-tion tests in that they measure the MIC. In thesetests, a small volume of a bacterial suspension,usually 1–2 microliters, is transferred to each of aseries of agar plates containing known concen-trations of antibiotics. Multi-prong devices areused to transfer approximately 100 colonies atone time.
Antibiotic gradient susceptibilitytest methodsTwo commercial methods, the Etest1 (AB BIO-DISK, Solna, Sweden) and the Spiral GradientEndpoint System (Spiral Biotech Inc., Bethesda,Maryland), use antibiotic concentration gradientson agar plates. Both tests establish MICs thatcompare closely with those determined in thedisk diffusion or broth dilution tests, and both areuseful for testing anaerobic and other hard-to-grow bacteria.
The Etest has been cleared by the FDA forclinical use in the U.S. The Spiral Gradient End-
Photo of five Etest strips on the surface of an agar plate. lnter-
section of the growth ellipses with the strips indicate the MICs.
Courtesy of James H. Jorgensen, University of Texas Health
Science Center, San Antonio, TX, 1995.
Photo of the Spiral Assay System Susceptibility Test.
Courtesy of Spiral Biotech, Inc., Bethesda, MD, 1995.
1 OTA mention of a company or product does not constitute an endorsement. Furthermore, companies and products are mentioned asexamples; competing companies and products exist.

Chapter 6 New Technologies for lnfection Diagnosis and Control 133
point System has not yet been cleared by theFDA for clinical use.
These tests may have a special advantage forresistance surveillance because they have a con-t inuous concentration gradient and are able to
show subtle changes in susceptibi l i ty, and the
wide concentration gradients of these tests cover
the MIC ranges of susceptibility of a wide vari-ety of pathogens and allow both low-level andhigh-level resistance to be detected. The Etest isreportedly easy to use in most laboratory settingsand requires no complicated procedures.
Modifications of Traditional Methods ToShorten Times Necessary To Obtain ResultsThe four methods discussed require at least over-night incubation to obtain results. That time canbe shortened to four to 10 hours for certain anti-biotics and organisms by using optical devices(sometimes coupled with fluorescent indicators)more sensitive than the human eye to detectgrowth in microdilution tubes. Two commer-cially available automated systems can produceresults in four to 10 hours.
The AutoSCAN Walk/Away (Dade Micro-scan, USA, Miami, Florida) uses standardmicrodilution trays that are inoculated in thestandard way and placed in an automated incuba-tor that uses a fluorometer to detect the presenceor absence of growth at different antibiotic con-centrations. The Vitek System (bioMerieuxVitek, Hazelwood, Missouri) was developed byNASA to diagnose urinary tract infections inastronauts in space in the 1970s. It uses credit-card size reagent cards, each of which has 30 tinywells for the testing of different antibiotic con-centrations, and the assays can be completed inthree to 10 hours. While both systems providerapid results, each requires backup cultures andother tests in case of power or mechanical fail-ures.
In some cases, the automated machines canfail to detect resistance. To deal with this prob-lem, manufacturers of both of these instrumentshave developed computer software that reviewsthe results to identify those that may be false.Some of these systems can also identify unex-
Photo of bioMerieux Vitek susceptibility testing reagent card. It
was originally developed by NASA to diagnose urinary tract
infections in astronauts in space and had to be very small.
Courtesy of James H. Jorgensen, University of Texas Health
Science Center, San Antonio, TX, 1995.
pected resistance patterns and offer suggestionsfor antibiotic treatment (Jorgensen, 1993). Com-puter analysis of the test results can also belinked to the hospital pharmacy’s computer toalert the pharmacy personnel when the wrongantibiotic therapy is being used. As discussed inchapter 4, computer networks such as this canimprove patient care and reduce costs.
Summary of the Test MethodsTable 6-1 shows the reported frequency of use ofthe various test methods in a survey of Americanlaboratories, and table 6-2 provides informationabout the relative costs of the most commonlyused methods. None of the methods differs verymuch in labor costs. Based on the costs of equip-ment and supplies, the disk diffusion method isthe least costly. O’Brien (1994) argues that it canalso be the most informative under most condi-tions because the sizes of the zones of inhibition(see photograph) provide raw data that have notbeen subject to interpretation, and zone of inhibi-tion information is more quantitative than brothdilution tests that are sometimes based on onlyone or two dilutions.
Will Faster Tests Make a Difference?A test result that shows that bacteria are resistantto the empirically chosen antibiotic will certainlycause the physician to substitute another antibi-
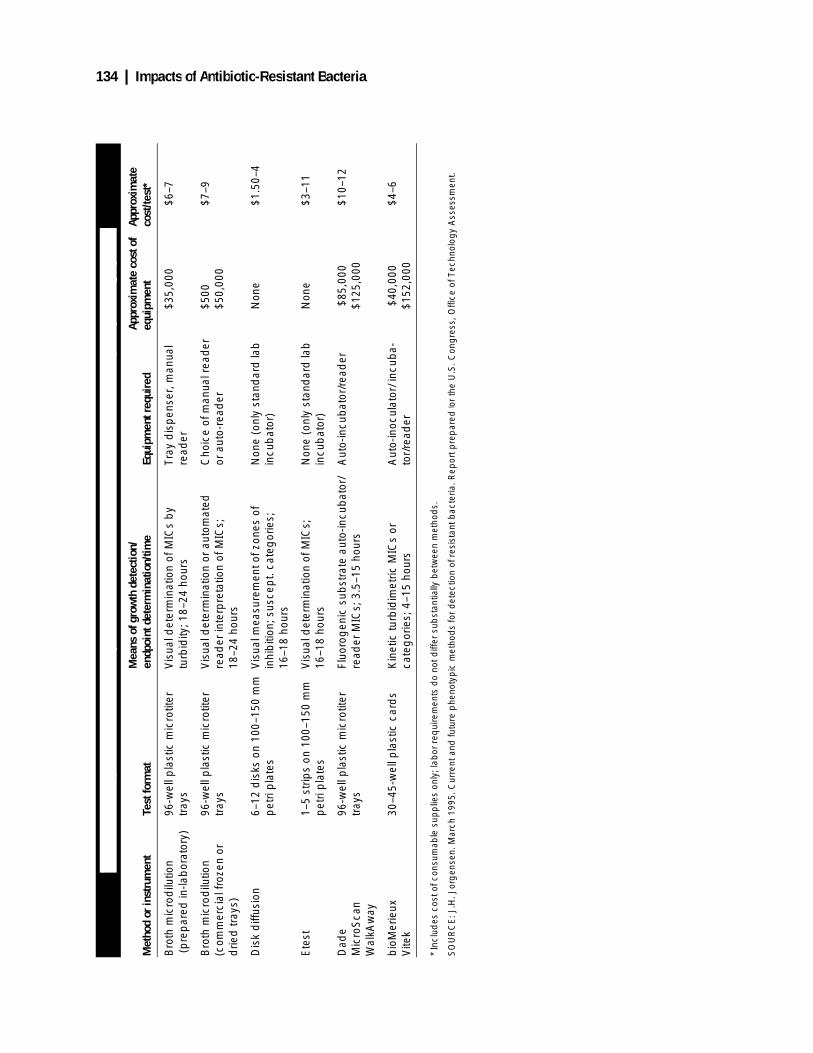
134 | Impacts of Antibiotic-Resistant Bacteria
TABL
E 6-
2: P
rinci
pal F
eatu
res
of P
rese
ntly
Ava
ilabl
e M
anua
l and
Aut
omat
ed A
ntim
icro
bial
Sus
cept
ibilit
y Te
stin
g Sy
stem
s
Met
hod
or in
stru
men
tTe
st fo
rmat
Mea
ns o
f gro
wth
det
ectio
n/
endp
oint
det
erm
inat
ion/
time
Equi
pmen
t req
uire
dAp
prox
imat
e co
st o
f eq
uipm
ent
Appr
oxim
ate
cost
/test
*
Bro
th m
icro
dilu
tion
(p
rep
ared
in-la
bor
ator
y)96
-wel
l pla
stic
mic
rotit
er
tray
sV
isua
l det
erm
inat
ion
of M
ICs
by
turb
idity
; 18–
24 h
ours
Tray
dis
pen
ser,
man
ual
read
er
$35,
000
$6–7
Bro
th m
icro
dilu
tion
(com
mer
cial
froz
en o
r d
ried
tray
s)
96-w
ell p
last
ic m
icro
titer
tr
ays
Vis
ual d
eter
min
atio
n or
aut
omat
ed
read
er in
terp
reta
tion
of M
ICs;
18
–24
hour
s
Cho
ice
of m
anua
l rea
der
or
aut
o-re
ader
$500
$50,
000
$7–9
Dis
k d
iffus
ion
6–12
dis
ks o
n 10
0–15
0 m
m
pet
ri p
late
sV
isua
l mea
sure
men
t of z
ones
of
inhi
biti
on; s
usce
pt.
cate
gor
ies;
16
–18
hour
s
Non
e (o
nly
stan
dar
d la
b
incu
bat
or)
Non
e$1
.50–
4
Ete
st1–
5 st
rips
on 1
00–1
50 m
m
pet
ri p
late
sV
isua
l det
erm
inat
ion
of M
ICs;
16
–18
hour
sN
one
(onl
y st
and
ard
lab
in
cub
ator
)N
one
$3–1
1
Dad
eM
icro
Sca
nW
alkA
way
96-w
ell p
last
ic m
icro
titer
tr
ays
Fluo
rog
enic
sub
stra
te a
uto-
incu
bat
or/
read
er M
ICs;
3.5
–15
hour
sA
uto-
incu
bat
or/r
ead
er $
85,0
00$1
25,0
00$1
0–12
bio
Mer
ieux
Vite
k30
–45-
wel
l pla
stic
car
ds
Kin
etic
turb
idim
etric
MIC
s or
ca
teg
orie
s; 4
–15
hour
sA
uto-
inoc
ulat
or/ i
ncub
a-to
r/re
ader
$40
,000
$152
,000
$4–6
* In
clud
es c
ost o
f con
sum
able
sup
plie
s on
ly; l
abor
req
uire
men
ts d
o no
t diff
er s
ubst
antia
lly b
etw
een
met
hod
s.
SO
UR
CE
: J.H
. Jor
gen
sen.
Mar
ch 1
995.
Cur
rent
and
futu
re p
heno
typ
ic m
etho
ds
for
det
ectio
n of
res
ista
nt b
acte
ria. R
epor
t pre
par
ed fo
r th
e U
.S. C
ong
ress
, Offi
ce o
f Tec
hnol
ogy
Ass
essm
ent.

Chapter 6 New Technologies for Infection Diagnosis and Control | 135
otic if the patient is not improving. Sometimes,however, the patient improves despite the pres-ence of apparently resistant bacteria. This canoccur because the patient’s immune system issuccessfully controlling the bacteria, or becausethe antibiotic reached a higher concentration inthe patient’s body than in the laboratory test, sothat the bacteria were killed or inhibited.
Up to 40 percent of antibiotic therapy wasinappropriate as judged by a comparison of phy-sicians’ prescriptions to an analysis of the labora-tory results for bacterial identification andantibiotic susceptibility tests (see, for example,Jorgensen and Matsen, 1987). While olderreports in the literature (see Edwards, Levin,Balogtas, et al., 1973) indicated that physicianspay little attention to microbiology test results,more recent publications (Doern, Scott, andRashad, 1982; Weinstein, Murphy, Reller, et al.,1983; Jorgensen and Matsen, 1987) indicate thatsome physicians do modify their prescriptionsupon receiving additional laboratory informa-tion. In particular, rapid susceptibility tests,which can be completed in four to 10 hours,resulted in more appropriate therapy, and Doern,Vautour, Gaudet, et al. (1994) found that rapidtests resulted in fewer additional laboratory tests,fewer invasive procedures, shortened time inintensive care, and reduced mortality.
Physicians typically receive the results of anti-biotic susceptibility tests on the morning of thesecond or third day after specimens are submit-ted to the laboratory. The faster methods producethe results more quickly, but unless the physi-cians and nursing staff are prepared to use theinformation at the earlier time, it will not be con-sidered until the next morning. In this case, tech-nological improvements can only be useful ifaccompanied by changes in habits.
Jorgensen (1995) discusses another obstacle tothe use of rapid methods. Laboratory managersoften confirm the results of the faster methodswith backup tests using the older, slower meth-ods. However, this requires performing the testsmore than once and therefore increases costs.Trade-offs must be made among the objectives
of speeding up the process, ensuring accuracy byperforming backup tests, and saving money.
❚ New Technologies for Identifying Bacteria
Antigen TestsAntigen tests use antibodies to recognize specificmolecules on or in bacterial or other cells. Forinstance, the home pregnancy test detects anti-gens that are produced only during pregnancy.
There are many versions of antigen tests todetect the presence of strep A bacteria in sorethroats, but the usefulness of these tests is limitedby low sensitivity. Traditional cultures are stillrecommended when tests are negative. Antigentests are also available to detect Clostridium difi-cile in patients with diarrhea and to determine thebacterial cause of meningitis.
Methicillin-resistant Staphylococcus aureus(MRSA) presents identification problemsbecause it and all other S. aureus grow slowly.Further, its identification is usually accomplishedby a specific test for protein antigens on its sur-face, and these tests failed to identify between 1and 25 percent of S. aureus. Kuusela, Hilden,Savolainen, et al. (1994) discovered another pro-tein on the surface of S. aureus and developed atest for it that detects both methicillin-susceptibleS. aureus and MRSA.
Tests which Directly Measure the Presence of a Bacterial or Antibiotic Resistance GeneTests which directly measure the presence of abacterial gene (discussion of tests for antibioticresistance genes follows) are fundamentally dif-ferent from the traditional tests, which measure aproperty of an organism such as its ability togrow in the presence of a certain concentration ofantibiotic. The new gene tests bring with them anew set of considerations: A bacterium mightcontain a gene for resistance, but not “express” itunder the conditions of the traditional diagnostictests, or a resistance gene may have undergone amutation that does not affect its function but thatmakes its presence undetectable, or the genes ofdead bacteria may be detected with DNA tests.

136 | Impacts of Antibiotic-Resistant Bacteria
For example, samples from a patient who isbeing successfully treated with anti-TB drugsoften test positive in DNA tests, but negative inculture-based tests that rely on growing theorganism. These are problems that must be con-sidered in designing new genetic tests and usingthem in clinical practice.
One huge advantage of tests that measure thepresence of a bacterial gene is that they arequick; many tests take only a few hours or less.Another advantage is that they generally havemuch higher sensitivity than the antigen andother enzymatic tests described above, althoughin some cases the sensitivity is not as high as thatof traditional culture methods. The speed com-bined with the sensitivity is very useful. How-ever, some tests require culturing, i.e., thegrowing of bacteria from the clinical samples,before the genetic test can be performed. Theculturing requirement adds time to the process.To date there exists no test so rapid that it willconfirm bacterial identification and susceptibilitybefore a patient leaves a physician’s office. Thedevelopment of faster and more susceptiblegenetically based tests for bacteria started in theearly 1980s, but most are still not available forroutine use. Nevertheless, some of these tests,such as those that are able to diagnose tuberculo-sis in a few hours instead of a few weeks, repre-sent a significant technological advancement thathas improved clinical practice.
DNA probe assaysSingle-stranded fragments of DNA or RNA thatare complementary to a target DNA or RNAsequence will form a double-stranded molecule,known as a “stable hybrid,” under certain reac-tion conditions. Diagnostic fragments, or probes,which will bind to target DNAs or RNAs, arelabeled with enzymes or dyes so that the bindingof the probe to the target can be detected.
At the present time, several commercial DNAprobe tests in clinical use are manufactured byGen-Probe, Inc. (San Diego, California), Gene-Trak (Framingham, Massachusetts), Ortho Diag-nostic Systems (Raritan, New Jersey), andothers. Some of these tests are designed to con-
firm the identification of cultivated colonies,such as tests for M. tuberculosis, M. avium (animportant pathogen in patients with AIDS), andNeisseria gonorrheae (the agent of gonorrhea).Other tests can be used for the direct detection ofbacteria in clinical samples, such as Neisseria,Chlamydia trachomatis (an agent of urethritis,cervicitis, and pelvic inflammatory disease) andS. pyogenes (a cause of suppurative tonsillitis or“strep throat”). These are organisms that for themost part are difficult or slow to cultivate andidentify in the laboratory. The tests requireapproximately two to four hours to complete andcost the patient approximately $20–40 per test.
One important disadvantage of probe-basedmethods to date has been their low sensitivitycompared to culture-based methods. Probeassays for M. pneumoniae (an agent of atypicalor “walking” pneumonia) and Legionella pneu-mophilia (the agent of Legionnaire’s Disease)are no longer much used, primarily because ofthis problem. New technologies in development,which provide the ability to amplify probe orprobe-linked signals after binding to the target,may help increase the sensitivity of these tests.
One promising probe-based test that doeshave adequate sensitivity is a rapid direct DNAprobe test from Gen-Probe that can identifyGroup A Streptococcus directly from throatswabs. In comparative studies, test results agreedclosely with those from older and slower tests(see, for example, Rippin, et al., 1994; Heiter andBourbeau, 1993), unlike the quick antigen streptests described above. However, Heiter andBourbeau conclude that because this test requiresseveral instruments not routinely found in doc-tors’ offices and because it still requires twohours, the test will not be useful for point-of-caretesting in doctors’ offices or emergency roomclinics.
Target amplification methodsOne of the most promising approaches forincreasing the sensitivity of probe-based DNAtests is to amplify the target DNA sequencethrough such methods as polymerase chain reac-tion (PCR), which can rapidly generate millions

Chapter 6 New Technologies for Infection Diagnosis and Control | 137
of copies of bacterial or resistance gene DNA orRNA sequences. PCR requires identifying andsynthesizing short sequences complementary tothe target gene that act as “primers” for the syn-thesis of the DNA. It is relatively easy to synthe-size millions of these short sequences, but itwould be difficult to synthesize larger pieces ofDNA. Starting with as little as one strand ofDNA from the sample, PCR uses enzymes toelongate the “primers” into full copies of theDNA. PCR can generate millions of copies of aparticular DNA in hours.
Species-specific PCR detection assays havebeen developed for at least 50 different bacterialpathogens, and specific sequences are availablefrom a much larger number of species, for whichPCR primers can be designed. However, only afew standardized kits for performing these testson specific bacterial species are commerciallyavailable in the U.S. Among those kits that eitherhave been cleared, or are nearing clearance, bythe Food and Drug Administration are PCRassays for C. trachomatis, N. gonorrheae, and M.tuberculosis. Even without a commercially avail-able standardized kit, the tests can still be set upindividually by service labs. However, there areseveral disadvantages to performing these testswithout using a standard kit. First, most of theseassays do not perform as well in detecting bacte-ria in clinical samples as they do in purified cul-tures; suboptimal sample preparation proceduresand reaction conditions are probably to blame.Second, unless physical, chemical, or enzymaticprecautions are in place, PCR and other targetamplification methods are easily jeopardized bycontaminating nucleic acid, either from prioramplification reactions or from positive clinicalsamples. Third, there is dramatic interlaboratoryvariability in the test results for the same groupof clinical samples. Many of these problems maybe solved by the availability of standardizedcommercial kits.
After the nucleic acid is isolated and amplifiedby a technique such as PCR, the nucleic acid canbe sequenced to identify the organism. Auto-mated sequencers marketed by Applied Biosys-tems can determine 48 independent DNA
sequences of 400–500 nucleotides in length inapproximately 8 hours, and speed and sequencelength capabilities are continually beingimproved. Automated sequencing systemsrequire an initial investment of approximately$55,000 (Molecular Dynamics) to $125,000(Applied Biosystems, including sequence analy-sis software). It is estimated that identification ofa single bacterial isolate with an automated pro-cedure will cost approximately $75.
Another way to identify the organism is tobind the nucleic acid to probes that recognizespecific sequences. Currently, sequences pre-pared from specific reference strains of bacteriaare used. New strategies are expected to use ran-dom sequences of nucleic acid bound in orderlyarrays on micro-scale photolithographic siliconchips, and the nucleic acid can be identified bydetermining which probes bind to it. Because ofthe microscopic scale of these tests, the boundnucleic acid must be detected with a laser confo-cal microscope. This approach has already beenshown to be useful for the detection of singlebase pair mutations in the human immunodefi-ciency virus. This technology offers significantpotential for rapid sequence determination ofspecific gene targets and for the detection ofspecific identifying signature sequences or anti-biotic-resistance-associated sequences. First-generation chip-based sequencing systems maybe available for research by 1996.
Using rapid DNA tests to diagnose tuberculosisDiagnosing tuberculosis is difficult because ithas many different clinical manifestations. More-over, many physicians were not trained to recog-nize tuberculosis because its prevalence wasdecreasing until about 10 years ago. The recentresurgence of this disease is a huge problem,both in the United States and around the world,and rapid diagnosis is critical so that patients canbe treated before they pass this highly infectiousdisease to others. Quick determination of the sus-ceptibility of the infecting organism is alsobecoming increasingly important because many

138 | Impacts of Antibiotic-Resistant Bacteria
drugs are inactive against some of the multi-resistant strains of tuberculosis.
The tuberculin skin test is often used as thefirst diagnostic indication that a person has beeninfected with tuberculosis. A positive tuberculinskin test does not mean that the person has activedisease, only that the person has been exposed totuberculosis. Haas and Des Prez (1995) reviewstudies of the interpretation of positive tuberculinskin tests in nursing homes which show that3.8 percent of men who were tuberculin-positiveon admission to nursing homes subsequentlydeveloped active disease, and that 11.6 percentof men who became positive while in the nursinghome later developed the disease. The percent-age developing active disease could be reducedto 0.2–0.3 percent with the prophylactic use ofthe antibiotic INH. However, the level of hepatictoxicity from INH was 3–4 percent, and therewere other side effects. Deciding when to pre-scribe antibiotics for a patient with a positiveskin test but no other symptoms is very compli-cated because the toxicity of the drug must beweighed against the probability that the patientwill develop tuberculosis. The same consider-ations apply to new diagnostic tests based on thedetection of the DNA of M. tuberculosis.
Isolating the mycobacteria causing tuberculo-sis requires from three to eight weeks, and sus-ceptibility testing by agar dilution methodsrequires another three to six weeks. Highly vari-able results have been observed between two dif-ferent clinical laboratories using culture methods(Hewlett, Horn, and Alfalla, 1995). The identifi-cation and susceptibility testing of drug-resistantTB can be significantly hastened by using theBACTEC radiometric method, but the timerequired is still 20 days or more. Recent data onthe Etest for susceptibility testing of mycobacte-ria suggest that MIC values can be obtained infive to 10 days, a significant improvement overcurrent methods (Wanger and Mills, 1995).
With PCR and probe-based DNA tests, physi-cians will have the ability to identify mycobacte-ria in the sputum of patients within a few hoursto a few days. All tests that are currently clearedby the FDA require some culturing of the clinical
sample, but newer tests in development willallow identification of mycobacteria directlyfrom clinical samples. These tests are used inmany other countries, including much of Europe.Some laboratories are promoting clinical use ofPCR tests in the U.S. Macher and Goosby (1995)document a difficulty in interpretation of PCRtests in the absence of other clinical signs oftuberculosis. On the basis of two (out of three)positive PCR tests, the patient received antituber-culosis chemotherapy and was placed in isola-tion. Later, six cultures turned out to be negativefor tuberculosis, and the patient was taken offdrugs for active tuberculosis and placed on INHalone for preventive therapy. This case studyindicates that the DNA probe tests might be toosensitive: they might detect non-viable mycobac-teria from a previous exposure. This result iscomparable to a positive tuberculin skin test,which, as discussed above, indicates past expo-sure to mycobacteria but does not necessarilysignify active tuberculosis.
❚ New Technologies for Detecting Antibiotic ResistanceThe increasing prevalence of antibiotic-resistantbacteria is leading manufacturers to develop testsspecifically to identify resistant strains. In gen-eral, these tests are designed to produce results ina few hours. Discrepancies may arise betweenthe results of old and new methods. The oldermethods directly measure whether an organismexpresses resistance and can grow in the pres-ence of an antibiotic. Some of the newer methodsindicate whether an organism has a gene encod-ing for resistance. However, the organism maynot “express” this resistance even if it has thegene. In some cases, it is unknown whether thepresence of the gene or the expression of thegene under laboratory conditions is the moreimportant predictor of clinical outcome.
Enzymatic TestsEnzymatic tests can directly measure the pres-ence of an enzyme that confers antibiotic resis-tance, such as β-lactamases that inactivate

Chapter 6 New Technologies for Infection Diagnosis and Control | 139
penicillins and other β-lactam antibiotics and theenzyme that inactivates chloramphenicol. Thedetection of the β-lactamases requires only a fewminutes (Stratton and Cooksey, 1990), but it islimited to only a few bacterial species. More-over, it does not detect penicillin resistancecaused by other mechanisms, such as the produc-tion of modified penicillin binding proteins. Thetest for the chloramphenicol inactivating enzymerequires one to two hours and can be used todetect the most common form of chlorampheni-col resistance, but it has decreasing utilitybecause of the declining use of this antibiotic.
Tests Based on Indicator Dyes or Light-Producing EnzymesSome tests add indicator dyes to a bacterial cul-ture and then detect the presence of living organ-isms by a color change in the indicator dye. Anexample is the Crystal MRSA Rapid ID test fromBeckton Dickinson. This test, which can detectMRSA in four hours in cultured bacteria, uses anindicator dye that can be observed under an ultra-violet light source in the absence of oxygen. Inthis test, three samples of bacteria are incubatedwith the indicator dye. In addition, one of thesamples is incubated with oxacillin (a semi-syn-thetic penicillin similar to methicillin) and one ofthe samples is incubated with vancomycin. If thebacteria survive, they will use the oxygen in thesamples and the dye changes color. If the samplecontains MRSA, the organism will survive in thepresence of oxacillin but not in the presence ofvancomycin. If the organism is susceptible tooxacillin, it will not survive either antibiotic. Thetest, which costs about five dollars, does notrequire expensive instrumentation. Kohner, Kol-bert, Geha, et al. (1994) found that this system isan effective rapid screening method for MRSAbut has poor performance for coagulase-negativeStaphylococci, which often present a greaterdiagnostic dilemma.
A more complicated test for multiresistanttuberculosis is currently in very early develop-ment (Jacobs, Barletta, Udani, et al., 1993). Inthis test, the gene for the light-producing enzymefrom fireflies was cloned into a virus that infectsM. tuberculosis. The virus is added to a sampleof sputum from the patient. The virus will infectany mycobacteria that are present. If the virusinfects living mycobacteria, the viral DNA isactivated, and the firefly enzyme will cause theculture to give off light. When antibiotics areadded to the test, only resistant mycobacteria willsupport viral growth; susceptible ones will not,and susceptible cultures will not light up. Thussusceptibility can be determined. Research iscurrently underway to determine if this test canmeasure as few as 100 live M. tuberculosis bac-teria, and would therefore work directly onpatient samples in a few hours (Jacobs, NIHGrant R01AI27235). However, this sensitivitymay be difficult or impossible to achieve becauseof background signals in the sample.2
DNA-Based Methods for Testing Antibiotic ResistanceCurrent susceptibility patterns suggest thatrifampin resistance in M. tuberculosis can beused as a predictive marker of multidrug resis-tance. In general, surveillance indicates thatresistance to rifampin correlates well with resis-tance to three or more antituberculosis drugs.Furthermore, virtually all of the highly resistantmycobacterial strains (resistant to greater thanfive drugs) are rifampin-resistant. However, thismay change in the future if M. tuberculosisundergoes further genetic mutation.
PCR tests are in development to detectrifampin resistance in M. tuberculosis caused bythe rpoB gene. The use of the signaturesequences in the rpoB gene assumes that thereare not significant numbers of rifampin-resistantM. tuberculosis strains in the community withother, uncharacterized rpoB mutations in thegene.
2 All samples “glow in the dark”—some background signals are detected. This test will only achieve high sensitivity if the signal from thefirefly enzyme is significantly larger than the background signal.

140 | Impacts of Antibiotic-Resistant Bacteria
MRSAs are currently identified by using thetraditional tests discussed in the first part of thischapter. The performance of these tests may bevariable. Factors such as the inoculum size, incu-bation time and temperature, pH of the medium,salt concentration of the medium, and prior expo-sure to β-lactam antibiotics all influence theexpression of resistance. To complicate mattersfurther, only some bacteria in a culture mayexpress methicillin resistance, even if all havethe gene. Taking into account these factors, theNational Committee for Clinical LaboratoryStandards (NCCLS) has recommended guide-lines to optimize the detection of resistance.However, occasional organisms have been iso-lated that are difficult to characterize by thesemethods. The results produced by various meth-ods of disk diffusion and those from agar dilutionmethods are often not consistent. In addition, it isdifficult to separate organisms that are highlyresistant due to overproduction of β-lactamasefrom organisms that have the mecA gene encod-ing for an altered penicillin binding protein.Organisms resistant due to the mecA gene oftenrequire vancomycin therapy, while organismsresistant due to overproduction of β-lactamasemight actually respond better to treatment withβ-lactam antibiotic/β-lactamase inhibitor combi-nations than vancomycin.
PCR and DNA-probe techniques have nowbeen developed to identify the mecA gene. Ingeneral, the studies to date show a high degree ofcorrelation between traditional and DNA-basedtests and allow accurate classification of highlyresistant and borderline resistant strains.
Guidelines for interpretation of the mecAdetection result will need to be formallyaddressed as more laboratories begin to use thisand other genetic methods. Proposals have beenmade to regard mecA-positive organisms (bothcoagulase-negative staphylococci and S. aureus)as intrinsically resistant to all antibiotics exceptvancomycin and to report immediately all mecA-positive results, which can be available wellbefore results from traditional methods. Thereare situations where the mecA-positive organismdoes not express resistance clinically and may
respond to β-lactam therapy. It is important todocument these cases carefully to avoid unneces-sary use or overuse of vancomycin. Neverthe-less, all mecA-positive organisms may be highlyresistant if the organism expresses the mecAgene. This may lead to treatment failures if β-lac-tam antibiotics are chosen.
Surveillance and DNA-based diagnosticsSurveillance of genetic mutations in bacteria willbe essential in the use of new DNA diagnostics,which measure the presence of specific geneticsequences. Mutations might alter thesesequences, or new genes conferring resistancemay spread. For example, widespread surveil-lance efforts are necessary to insure that signa-ture sequences represent the majority ofmutations in the rpoB gene that confer rifampinresistance in M. tuberculosis.
❚ Regulation of Diagnostic TestsThe Clinical Laboratory Improvement Amend-ments (CLIA ’88) were passed by Congress toregulate the quality of diagnostic testing. Regula-tions under CLIA, which became effective inSeptember of 1992, require all clinical laborato-ries that perform certain diagnostic tests to regis-ter with the federal government and performquality control tests and document quality assur-ance. However, certain tests are “waived” underCLIA; this means that the test can be performedin any physician’s office, whether or not theoffice is registered under CLIA. Other tests, gen-erally the more complex ones, can be performedonly in offices that comply with the CLIA regu-lations for laboratories.
The CLIA regulations may be a disincentiveto performing tests. Complying with themincreases the cost of testing and may delayresults. For example, physicians may choose notto register their offices under CLIA and willtherefore be compelled to send out numeroustests that they formerly performed. This mayresult in the performance of fewer diagnostictests, which could contribute to the overuse ofantibiotics. A physician might decide that it is

Chapter 6 New Technologies for Infection Diagnosis and Control | 141
easier and more cost-effective to prescribe anti-biotics for all sore throats rather than performthroat cultures. However, this negative potentialconsequence of the CLIA regulations must beweighed against whatever positive effects theyhave had on the quality and consistency of test-ing that is done in the clinical laboratories thatmeet CLIA standards.
❚ Getting New Tests to MarketThe worst outcome for a sensitivity test is toindicate that bacteria are susceptible to an antibi-otic when the antibiotic has no effect against thatstrain. Such an error, which can result in apatient’s death, is called a “very major error” intesting. The second worst outcome is to reportthat bacteria are resistant to an antibiotic that isin fact effective against them. That error, whichcould result in treatment with a more toxic, moreexpensive antibiotic than necessary, is termed a“major error” (Jorgensen 1995).
It is impossible to design and perform teststhat are completely error free. The manufactur-ers, the FDA, health care providers, and the pub-lic have to decide what levels of errors areacceptable. Often, new tests are compared with a“gold standard”—an older test that has beenproved to be reliable. However, the “gold stan-dard” is also not completely error free. Thereforeit is sometimes difficult to interpret differencesbetween a new test and a “gold standard.” Forexample, culturing M. tuberculosis is consideredthe “gold standard” for the diagnosis of tubercu-losis. However, Abe, et al. (1993) found thatsome patient samples were positive for M. tuber-culosis by DNA-based techniques but negativewhen cultured; these patients had clinical signsof tuberculosis, including characteristic radio-graphs, clinical manifestations of the diseaseand/or clinical response to antituberculosis che-motherapy.
Two FDA centers are involved in approvingtest methods for antibiotic susceptibility. TheFDA Center for Drug Evaluation and Researchcertifies that disks are available for each antibi-otic on the market in the United States, and it
assures the potency of the disks and that criteriafor interpretation of the disk assays are availablewhen an antibiotic goes on the market. The FDACenter for Devices and Radiological Health hasresponsibility for determining the safety andeffectiveness of other devices and materials,including computer software, for susceptibilitytesting.
A new diagnostic device can be reviewed byFDA under two different procedures. A device ormethod that employs principles similar to thoseused by products already on the market and thatrequires an incubation period of 16 hours ormore is reviewed under the “510(k) clearance”process. The performance of the new device ormethod is compared to the performance of theproduct already marketed to determine whetherthe two are “substantially equivalent.” If theyare, the new device or method is cleared for mar-keting without undergoing the more extensiveprocedures, known as “pre-market approval.”The 510(k) process is also used when a manufac-turer wants to add a new antibiotic to the batteryof antibiotics already included in a test kit.
New diagnostic tests that are not “substan-tially equivalent” to any product on the marketmust submit an application for “pre-marketapproval” (PMA) to the FDA. Because theapproval process under the PMA review is sub-stantially more difficult, manufacturers have adisincentive to develop novel products.
Any device that requires less than 16 hours’incubation is required to undergo the pre-marketapproval process, which takes longer and is sub-stantially more difficult to complete than the510(k) clearance process. Jorgensen (1995)claims that there is no clear justification for the16-hour incubation period serving as the cutoffbetween a 510(k) review and a PMA reviewbecause there is no indication that more rapiddevices are inherently less accurate than others.The difference in the time required to obtain a510(k) clearance, as opposed to a pre-marketapproval, is a matter of contention. According toJorgensen (1995), the requirements for a 510(k)clearance have grown since 1990, and they arenow approaching those required for a PMA. On

142 | Impacts of Antibiotic-Resistant Bacteria
the other hand, FDA (1995) asserts that therehave been marked improvements in the process-ing of 510(k) applications.
VACCINESPerhaps the ultimate weapon against antibiotic-resistant bacteria is the development of vaccinesand pre-emptive immunization. In concept, vac-cines are simple. When a person receives aninoculation of a preparation of killed or attenu-ated (“weakened”) disease-causing bacteria orvirus, a component of such an agent, or a relatedorganism that does not cause disease, the inocu-lated person’s immune system will respond andproduce antibodies to antigens on the injectedmaterials. The immune system has a “memory.”As a result, if the person is subsequently infectedby the organism for which the vaccine was pre-pared, he or she will produce antibodies that caninactivate the agent and remove it from the body.“Natural immunity” is produced in a similarway; once a person has had a disease, theimmune system recognizes the organism thatcaused it and eliminates it from the body.
In practice, preparation of the specific mate-rial for the inoculation—the antigen—can be dif-ficult. Preparing it so that the production ofantibody is stimulated without objectionable tox-icity, either at the time of inoculation or later,may not be simple.
The success of Haemophilus influenzaetype B (Hib) vaccines, which were introduced in1988, demonstrates that antibacterial vaccinescan be quite successful. Countering that greatsuccess is the more than 75 years’ experiencewith an antituberculosis vaccine.
❚ Hib Vaccines, a Success StoryBefore the introduction of vaccines against it,Hib (Haemophilus influenzae type B) was theleading cause of invasive bacterial disease inchildren under five years of age, and it causedabout 20,000 cases of meningitis and another3,000 to 5,000 cases of invasive Hib diseaseannually. The mortality rate was 3 to 5 percent;moreover, up to 20 percent of the survivors of
meningitis suffered hearing loss or mental retar-dation, and resistance to ampicillin was increas-ing (Adams, Deaver, Cochi, et al. 1993).
In 1993, five years after the introduction ofHib vaccines, a number of researchers publishedreports about the incidence of Hib diseases inchildren up to five years old. Those vaccinatedwith Hib vaccine generally had disease rates 80to 90 percent below the rates seen in unvacci-nated children (Wenger 1994). The rates of Hibmeningitis began to fall in 1989, after the intro-duction of the vaccine, and they continued to fallthrough 1991 (the last year for which data wereavailable). In contrast, the rates of meningitisfrom Neisseria meningitidis and Streptococcuspneumonia remained unchanged, ruling out ageneral decline in meningitis as the explanationfor the Hib results. An unexpected result of theHib vaccination program was a reduction in thenumber of children who carry Hib in their upperairways. That, in turn, reduced the number ofchildren who could infect others, and the rates ofHib disease have fallen in both vaccinated andunvaccinated children.
A polysaccharide (a polymer of sugar mole-cules that is unique to the Hib bacteria) vaccinelicensed in 1985 had no effect on the occurrenceof invasive Hib disease in Los Angeles County(see figure 6-4) and, in fact, it was of little valuein disease prevention. Three years later, a conju-gate vaccine, prepared by chemically joining thepolysaccharide to a protein that was known tostimulate antibody production, was licensed.This vaccine was very successful. Even when useof this vaccine was restricted to children olderthan 18 months (from 1988 through 1990), therewas a drop in the Hib invasive disease rate inyounger children. Vaccination of the older chil-dren had reduced infections of the younger ones,due to reduced transmission of the bacteria.Licensing of a vaccine for 2-month-old childrenin 1990 led to great reductions in the disease inLos Angeles County by 1992.
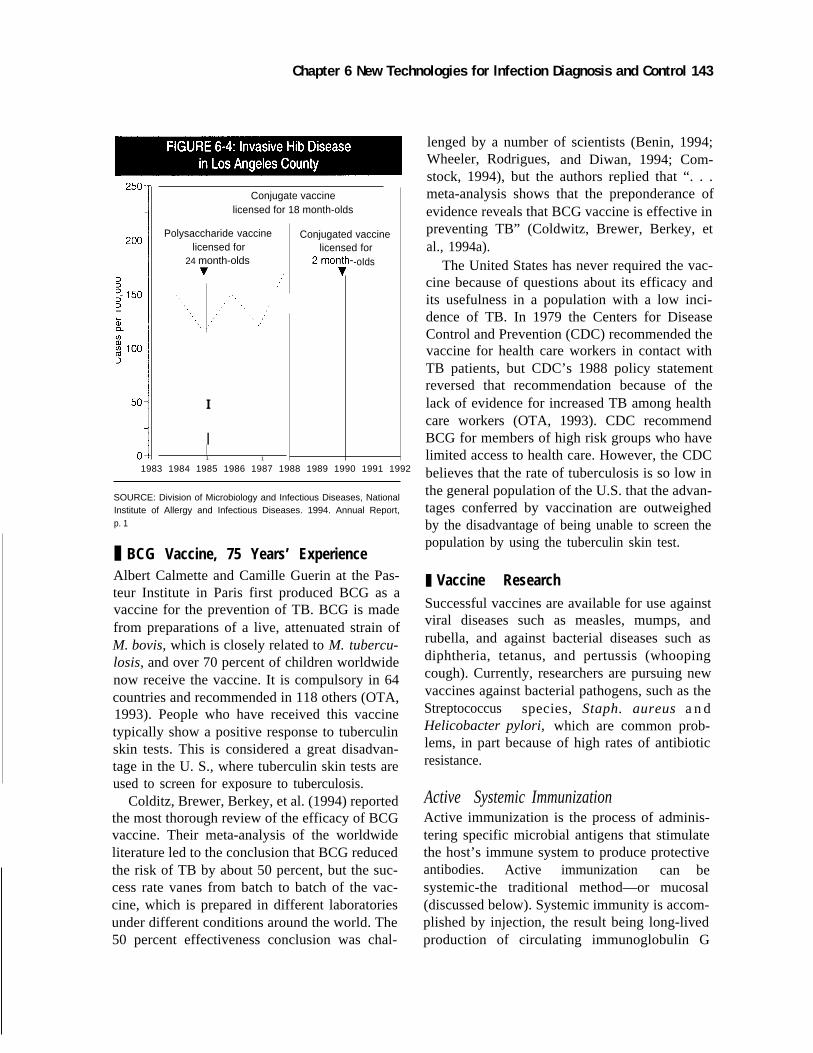
Chapter 6 New Technologies for lnfection Diagnosis and Control 143
Conjugate vaccinelicensed for 18 month-olds
Polysaccharide vaccinelicensed for
24 month-olds
I
I1 1
Conjugated vaccinelicensed for
-oIds
1983 1984 1985 1986 1987 1988 1989 1990 1991 1992
SOURCE: Division of Microbiology and Infectious Diseases, NationalInstitute of Allergy and Infectious Diseases. 1994. Annual Report,p. 1
❚ BCG Vaccine, 75 Years’ ExperienceAlbert Calmette and Camille Guerin at the Pas-teur Institute in Paris first produced BCG as avaccine for the prevention of TB. BCG is madefrom preparations of a live, attenuated strain ofM. bovis, which is closely related to M. tubercu-losis, and over 70 percent of children worldwidenow receive the vaccine. It is compulsory in 64countries and recommended in 118 others (OTA,1993). People who have received this vaccinetypically show a positive response to tuberculinskin tests. This is considered a great disadvan-tage in the U. S., where tuberculin skin tests areused to screen for exposure to tuberculosis.
Colditz, Brewer, Berkey, et al. (1994) reportedthe most thorough review of the efficacy of BCGvaccine. Their meta-analysis of the worldwideliterature led to the conclusion that BCG reducedthe risk of TB by about 50 percent, but the suc-cess rate vanes from batch to batch of the vac-cine, which is prepared in different laboratoriesunder different conditions around the world. The50 percent effectiveness conclusion was chal-
lenged by a number of scientists (Benin, 1994;Wheeler, Rodrigues, and Diwan, 1994; Com-stock, 1994), but the authors replied that “. . .meta-analysis shows that the preponderance ofevidence reveals that BCG vaccine is effective inpreventing TB” (Coldwitz, Brewer, Berkey, etal., 1994a).
The United States has never required the vac-cine because of questions about its efficacy andits usefulness in a population with a low inci-dence of TB. In 1979 the Centers for DiseaseControl and Prevention (CDC) recommended thevaccine for health care workers in contact withTB patients, but CDC’s 1988 policy statementreversed that recommendation because of thelack of evidence for increased TB among healthcare workers (OTA, 1993). CDC recommendBCG for members of high risk groups who havelimited access to health care. However, the CDCbelieves that the rate of tuberculosis is so low inthe general population of the U.S. that the advan-tages conferred by vaccination are outweighedby the disadvantage of being unable to screen thepopulation by using the tuberculin skin test.
❚ Vaccine ResearchSuccessful vaccines are available for use againstviral diseases such as measles, mumps, andrubella, and against bacterial diseases such asdiphtheria, tetanus, and pertussis (whoopingcough). Currently, researchers are pursuing newvaccines against bacterial pathogens, such as theStreptococcus species, Staph. aureus a n dHelicobacter pylori, which are common prob-lems, in part because of high rates of antibioticresistance.
Active Systemic ImmunizationActive immunization is the process of adminis-tering specific microbial antigens that stimulatethe host’s immune system to produce protectiveantibodies. Active immunization can besystemic-the traditional method—or mucosal(discussed below). Systemic immunity is accom-plished by injection, the result being long-livedproduction of circulating immunoglobulin G

144 | Impacts of Antibiotic-Resistant Bacteria
(IgG) antibodies. For bacterial vaccines, polysac-charides from the outside capsule of the bacteriaare generally employed, but as was seen with theHib vaccines (Wenger, 1994), capsular polysac-charides alone do not always stimulate sufficientantibody production. To raise sufficient levels ofantibodies, the polysaccharides may have to beconjugated with “carrier proteins,” potent immu-nogens that provoke an immune system responseto the entire complex (i.e., to polysaccharideantigen and protein carrier). The combination ofpolysaccharide and protein is called a “conjugatevaccine.” Finding the proper carrier is one of themore difficult aspects of vaccine development,but four different proteins—all of bacterial ori-gin—work well in Hib vaccines.
Streptococcus pneumoniae vaccinesVaccine development is further complicatedbecause different strains of the same bacteriahave different polysaccharide antigens. Forinstance, Streptococcus pneumoniae has 84 dis-tinct capsular polysaccharides. A vaccine thatcontains 23 different polysaccharides providesprotection against 90 percent of invasive pneu-mococcal strains (Siber, 1994). That vaccine is75 percent effective when administered to immu-nocompetent adults, and its wider use might pre-vent half of the 80,000 annual pneumococcalpneumonia deaths among older people (MedicalWorld News, 1993). It is not, however, reliablein children under two years of age. For the vacci-nation of children, several companies are devel-oping conjugated vaccines against thepolysaccharides of the seven strains of pneumo-coccus that most commonly infect children, andthese are currently undergoing human trials. Inaddition, researchers are investigating the possi-bility of using a polysaccharide that is commonto all pneumococcus conjugated to one or moreof several proteins that are common to all pneu-mococcus as vaccines, but there is no definitiveevidence for their usefulness (Siber 1994).
Vaccines against otitis mediaS. pneumonia is one of several bacteria that causeotitis media. That illness is so notorious that phy-
sicians who surveyed parents about their willing-ness to have their children immunized against thedisease titled their report “The Surprisingly HighAcceptability of Low-Efficacy Vaccines for Oti-tis Media...” (Wischnack, Jacobson, Poland, etal., 1995). Although no such vaccine is now inuse, the interviewers asked about five hypotheti-cal vaccines that had different efficiencies in dis-ease prevention, and side effects that rangedfrom the temporary discomfort of a “shot” in allchildren to a few days of flu-like symptoms in upto half of vaccinated children. About half of the601 interviewed parents would accept any vac-cine if it would prevent three or more infectionsin the next six months. Parents were less accept-ing of vaccines with lower efficiencies and worseside effects. The authors of the study concludethat parents, even of children who have not hadotitis media, are willing to accept some discom-fort in their children to obtain protection againstthe disease and that parents’ willingness isgreater than the medical establishment’s orFDA’s.
A biotech firm, MicroCarb (Bethesda, Mary-land), has licensed one vaccine against Haemo-philus influenza, another cause of otitis media, toPasteur Merieux Serums et Vaccines S.A. If thisvaccine proves successful, it will be of valueagainst both antibiotic susceptible and resistantH. influenza, which are increasingly common.
Staphylococcus aureus vaccinesVaccines against Staph. aureus, which is oftenantibiotic resistant, would be helpful to patientsat high risk for infection with this organism,including renal dialysis patients, or patientsreceiving prosthetic devices like hips or vasculargrafts, which act as sites for infection (Univax,1994). Researchers are pursuing vaccines madeof capsular polysaccharide types 5 and 8, whichwould encompass 90 percent of Staphylococcussystemic infections. Recent research has shownthat high levels of biologically active antibodiesagainst Staph. aureus types 5 and 8 can be stimu-lated in human subjects when the antigens arecombined with a protein from P. aeruginosa as

Chapter 6 New Technologies for Infection Diagnosis and Control | 145
the carrier (Fatton, et al., 1990; Fatton, et al.,1993).
Active Mucosal ImmunizationThe second approach to active immunization isto stimulate the immune defenses of the mucosallinings of the gastrointestinal, respiratory andurogenital tracts, the nasal passages, and theinner ear. These mucosal linings produce immu-noglobulin A (IgA). IgA diminishes microbialvirulence by preventing microbial adherence tohost cells. It also coats the surface of the antigen,making an antigen/IgA complex that stimulateswhite blood cells to recognize, engulf, anddestroy any pathogen expressing that antigen.Mucosal lymphocytes also trigger production ofcirculating IgG antibodies. Current targets formucosal immunity include Helicobacter pylori,Clostridium difficile, Shigella flexneri, Campylo-bacter strains, and certain strains of Escherichiacoli.
Mucosal vaccines are immunogenic only ifthey reach specific immune response tissuesbeyond the stomach, which requires their surviv-ing passage through stomach acid and enzymes.Some researchers are testing synthetic polymersto protect their vaccines. Another strategy is touse liposomes, lipid-containing vesicles madefrom the same natural materials that composemammalian cell membranes.
Helicobacter pylori vaccinesThe discovery by Marchetti, Arico, Burroni, etal. (1995) that bacteria isolated from humanswith ulcers could infect mice and cause diseaseprocesses that mimic those seen in humans hasspurred progress toward a vaccine against H.pylori, the causative organism. Those researchersfound that mice were protected from infectionafter administration of disrupted H. pylori bacte-ria. This finding, characterized as “of extremepractical importance” (Tompkins and Falkow1995) may lead to a vaccine to protect the50 percent of the world’s population that are cur-rently infected by H. pylori. While H. pylori ismost often associated with gastritis and ulcers in
the United States, elsewhere in the world it isalso a common cause of stomach cancers.
Campylobacter vaccinesCampylobacter strains have recently emerged asone of the common causes of diarrhea and maycause 2.5 million cases annually in the UnitedStates. Treatment is increasingly complicated byantibiotic resistance. In 1994, the U.S. Navysigned a Cooperative Research and DevelopmentAgreement (CRADA) with MicroCarb Inc. forclinical trials of a vaccine against Campylo-bacter.
Passive immunizationPassive immunization involves administeringantibodies directed against specific pathogens toindividuals who have not developed such anti-bodies on their own but who are at risk for infec-tion. This may be due to lack of prior exposure tothe pathogen, or due to immunosuppression,which renders the individual’s immune systemunable to produce antibodies. The antibodies arepurified from the blood of healthy donors whoseantibody levels are raised by active immuniza-tion. The most common example of passiveimmunization is the administration of HepatitisB virus-specific gamma-globulin to travelers.Researchers are currently focusing efforts todevelop antibodies against Staph. aureus and P.aeruginosa, both of which are often antibioticresistant, as well as against other bacteria.
Passive immunization does not always work.Low birthweight babies are at high risk of noso-comial infections because of long hospitaliza-tions and immature immune systems. Injectionsof pooled human antibodies (“immune globu-lin”) into very low birthweight babies did notreduce the incidence of nosocomial infectionscompared to the incidence in very low birth-weight babies who did not receive the immuneglobulin (Fanaroff, Korones, Wright, et al.,1994). This failure does not invalidate the idea ofpassive immunization, even in low birthweightbabies, but it underlines the importance of trialsof the efficacy of interventions before they areintroduced widely into practice.
146 | Impacts of Antibiotic-Resistant Bacteria
Vaccine SummaryVaccines are not high-profit items. UNICEF esti-mates that the entire global vaccine market isabout $3 billion, which can be compared to the$3.5 billion market for a single ulcer drug. Whilevaccine development against bacteria that havehigh frequencies of antibiotic-resistant strains,such as Staph. aureus or S. pneumonia, wouldreduce infections by those bacteria, few vaccineswill be developed for bacteria solely because ofthe problems raised by antibiotic resistance.Instead, the general problems raised by the bacte-ria may lead to development of a vaccine thatwill protect against both antibiotic susceptibleand resistant strains.
STIMULATING THE IMMUNE SYSTEMGranulocyte colony-stimulating factor (G-CSF)is a growth factor that stimulates the proliferationof neutrophil cells, important components of theimmune system. Crawford, Ozer, Stoller, et al.(1991) have shown that the administration of G-CSF to cancer patients on chemotherapy led to a51 percent reduction in culture-confirmed infec-tions, a 47 percent reduction in the mean numberof days of antibiotic use, and a 45 percent reduc-tion in the mean number of days of hospitaliza-tion. G-CSF in the form of filgrastim (Amgen,Thousand Oaks, California) has been approvedby the FDA and is clinically available.
TARGETED DELIVERY OF ANTIBIOTICSSome sites of infection or potential infection arelocalized, such as wounds or the area around ajoint replacement. Delivery of antibiotics directlyto those sites may stop the growth of susceptiblebacteria, and if the concentration can be raisedhigh enough, it may even stop the growth ofmany resistant bacteria. Direct delivery of antibi-otics in this way has the additional advantage ofproducing only very low levels of circulatingantibiotics, thus reducing pressure for the selec-tion of resistant bacteria elsewhere in the body.
❚ MicroencapsulationEntry into the body, whether surgical or trau-matic, opens pathways for infection. Surgicalpatients who develop wound infections spent, onaverage, 14.3 days longer in the hospital thanuninfected matched controls (Maderazo, Judson,and Pasternak, 1988), at an increased cost of$36,000 to $45,000 per patient (Cohen, 1994;Daly, Eliopoulos, Reiszner, et al., 1988).Twenty-four percent of United States servicemenwho sustained open fracture wounds in Panamaduring Operation “Just Cause” developed woundinfections (Jacob, Erpelding, and Murphy, 1992),and 48 percent of wounded United States sol-diers in the Persian Gulf conflict who sustainedopen fractures developed postoperative infec-tions (Travis and Cosio, 1993). Gustilo, Men-doza, and Williams (1984) report similarinfection rates in civilians with severe open frac-tures of the tibia. Many of these infections occurin patients who receive very large doses of sys-temic antibiotics.
Researchers at the Walter Reed Army Instituteof Research (WRAIR) have developed a novelbiodegradable local antibiotic delivery systemthat promises to decrease infections in wounds.They encapsulate an antibiotic in a copolymer ofpoly (DL-lactide-coglycolide) to produce micro-spheres 50 to 250 micrometers (µm) in diameter.Dusted into wounds after surgery, these micro-spheres provide an initial burst of the antibioticwithin the first few hours and prolonged drugrelease over a period of up to 21 days. After 2 to3 months, the microspheres completely degrade.As of March 1995, the WRAIR researchers hadconstructed microspheres containing ampicillin,cefazolin, cefamandole, and tobramycin.
Cefazolin-containing microspheres were usedto treat wounds in rats that had been intentionallyinfected with cefazolin-resistant MRSA, andthey were as effective as free cefazolin powder ineliminating MRSA. Systemic administration ofcefazolin, on the other hand, had no effect on theMRSA infections. In a similar experimentinvolving ampicillin-resistant MRSA, micro-spheres containing ampicillin were more effec-

Chapter 6 New Technologies for Infection Diagnosis and Control | 147
tive than free ampicillin powder, and systemicampicillin had no effect.
The United States Army, which developedthis technique (Setterstrom, Tice, and Myers,1994; Jacob, Setterstrom, Bach, et al., 1991;Jacob, Cierny, Fallon, et al., 1993), has a patentpending on it. Further development will requireprivate funding to take the research from the pre-clinical stage to trials in humans.
❚ Antibiotic-Impregnated CementBone infections and infections of joint prosthesesare hard to treat with systemic antibiotics, par-tially because limited blood flow to the skeletaltissues does not allow high concentrations of thedrug to reach the area of infection. An antibiotic-impregnated polymer, poly (methyl-methacry-late) (PMMA), has been used to cement bonefractures and prostheses in place, and has shownclinical success, but its usefulness is limited bythe toxicity of the material and shrinkage whichleaves marginal mechanical support for theremaining bone. Yu, et al. (1992) describedhydroxyapatite (HAP) cement, which has thesame chemical composition as bone mineral.This material can be molded to fill the space leftby the absence of bone, and Yu, et al. demon-strated that antibiotics impregnated in this mate-rial are slowly released. They concluded that thismaterial is very promising for preventing infec-tions in bone fractures and in joining prostheses,and they propose future in vivo experiments.
❚ Biological Substances to Facilitate the Entry of Antibiotics into BacteriaOne mechanism of resistance involves bacterialcell walls in excluding antibiotics from the bacte-rial cell. Research is underway on biological sub-stances that allow antibiotics to penetrate intosuch bacteria. For example, because iron is insol-uble but necessary for bacterial metabolism, bac-teria synthesize and excrete compounds that canbind iron ions, called “siderophores.” Thesecompounds scavenge iron outside the cell, andthe cell then transports the iron-siderophore com-pound back inside the cell. Inside the cell, the
iron-siderophore complex is metabolized by thebacteria, releasing iron for bacterial use. Sidero-phores may be modified to carry antibiotics intothe bacteria. These may be especially useful inthe treatment of Gram-negative bacterial infec-tions. Although the outer cell membrane chan-nels (“porins”) of Gram-negative bacteria are toosmall to accommodate many antibiotics, sidero-phores enter the cell via a non-porin route, andresearchers reason that antibiotics attached tosiderophores might be “dragged” inside.
Over 200 siderophore molecular structures areknown. Often, only portions of the siderophoresare required to penetrate the cell. One goal ofcurrent research is to optimize synthetic sidero-phores in order to make their transport intobacterial cells more efficient. Synthetic sidero-phores, when conjugated with beta-lactam antibi-otics or erythromycin, can carry the antibioticacross bacterial cell membranes with high effi-ciency. These antibiotics kill bacteria whendelivered inside the cell in this manner (Miller,1989; McKee, Sharma, and Miller, 1991).Siderophores are also being explored for theirpotential to transport vancomycins. Althoughsiderophore/antibiotic conjugates have thus farbeen used only as antibacterials, researchers arecurrently attempting to apply the same methodol-ogy to antifungal/siderophore conjugates.
REDUCING INFECTIONS BY MODIFYING DEVICESSeveral hundred thousand cases of hospitalacquired infection per year are related to the useof medical devices such as catheters, endotra-cheal tubes and mechanical ventilators (IOM,1992). These devices provide extra opportunitiesfor bacteria to enter the body. Experience withdialysis, the filtering of the blood of patients withkidney disease, indicates that changing thedesign and materials of medical devices can min-imize infections.
❚ Infections in Dialysis PatientsIn 1991, there were approximately 120,000patients on maintenance dialysis (Favero, Alter,

148 | Impacts of Antibiotic-Resistant Bacteria
and Bland, 1992) with 45,000 new patientsadded per year. Infections are the cause of deathin 15 to 30 percent of dialysis patients.
The technique called hemodialysis is used totreat approximately 85 percent of dialysispatients. Simulating the function normally per-formed by the kidney, it filters the patient’sblood through a membrane which separates outunwanted components and adds needed compo-nents. Cupraphane membranes, the most com-monly used filtration membrane in hemodialysis,are made from cotton fibers dissolved in anammonia solution of cupric oxide. Recently,membranes made of synthetic polymers such aspolysulfone (PS), polymethylmethacrylate(PMMA) and polyacrylonitirile (PAN) havebeen developed. A recent review of the proper-ties of hemodialysis membrane (Hakim, 1993)describes how the interaction of blood with cot-ton fiber membranes such as Cupraphane pro-duces a decrease in the immune functions in theblood, leaving the patient more susceptible toinfection. The membranes made of syntheticpolymers do not seem to decrease the immunefunctions in the blood. Retrospective studiesshowed that replacing a Cupraphane membranewith a polysulfone membrane eliminated50 percent of the infections.
Another 15 percent of patients are on perito-neal dialysis. In this technique, fluid is pumpedinto the patient’s abdomen, allowing exchange ofblood components through the peritoneal liningof the abdomen. A recent review (Diaz-Buxo,1993) shows that the incidence of peritonitis(peritoneal infection) was twice as high whenolder CAPD (continuous ambulatory peritonealdialysis) machines were used than when newdialysis machines of different design, such asCCPD (continuous cyclic peritoneal dialysis)machines and Y-set connections for CAPD, wereused. This may be because the order of flow isreversed in CCPD and Y-set CAPD compared toother forms of CAPD, so that the connections(and contaminating bacteria) are washed outbefore fluid is pumped into the body. Diaz-Buxocomments that CAPD machines are more com-mon than CCPD machines, partially because of
the lower cost of the machine itself. When thetotal costs of the two systems were calculated,including the cost of the machine and the cost ofhospitalization for peritoneal infections, the totalcosts were the same (King, et al., 1992).
Analyzing the costs of dialysis for kidneypatients is especially interesting because dialysispatients have been covered by Medicare since1973 regardless of their age. Medicare pays a setamount per patient for dialysis and pays sepa-rately for any hospitalization necessitated bycomplications. Under this system, physicianshave a financial incentive to use the least expen-sive equipment. However, it would be beneficialto the patients, and probably cheaper for Medi-care, to use the more expensive equipment andprevent infections that may require hospitaliza-tion. Outpatient costs, primarily dialysis,accounted for 33 percent of total costs comparedwith 44 percent of total costs attributable to hos-pitalizations (Smits, 1995). (The remainder of thecosts were for physician services, skilled nursingcare, and home health care.) This demonstratesthat investing in new technologies that preventinfections and hospitalizations can be cost-effec-tive. These investments would also reduce antibi-otic resistance by preventing infections and thusreducing the use of antibiotics.
❚ Infections from Sutures and CathetersImprovements in the materials used for othermedical devices such as sutures and catheterscould also greatly reduce the rate of infection. Inparticular, sutures made of synthetic materialssuch as dacron and nylon have lower infectionrates compared to natural sutures such as cotton,silk and catgut, and monofilament sutures havelower infection rates compared to polyfilamentsutures.
Studies of the colonization of medical devicesby coagulase-negative staphylococci (Chris-tensen, Baldassarri, and Simpson, 1994) providessome insight into why some suture materials areassociated with infections more than others. Theprocess of colonization of non-biological sur-faces by coagulase-negative staphylococci is
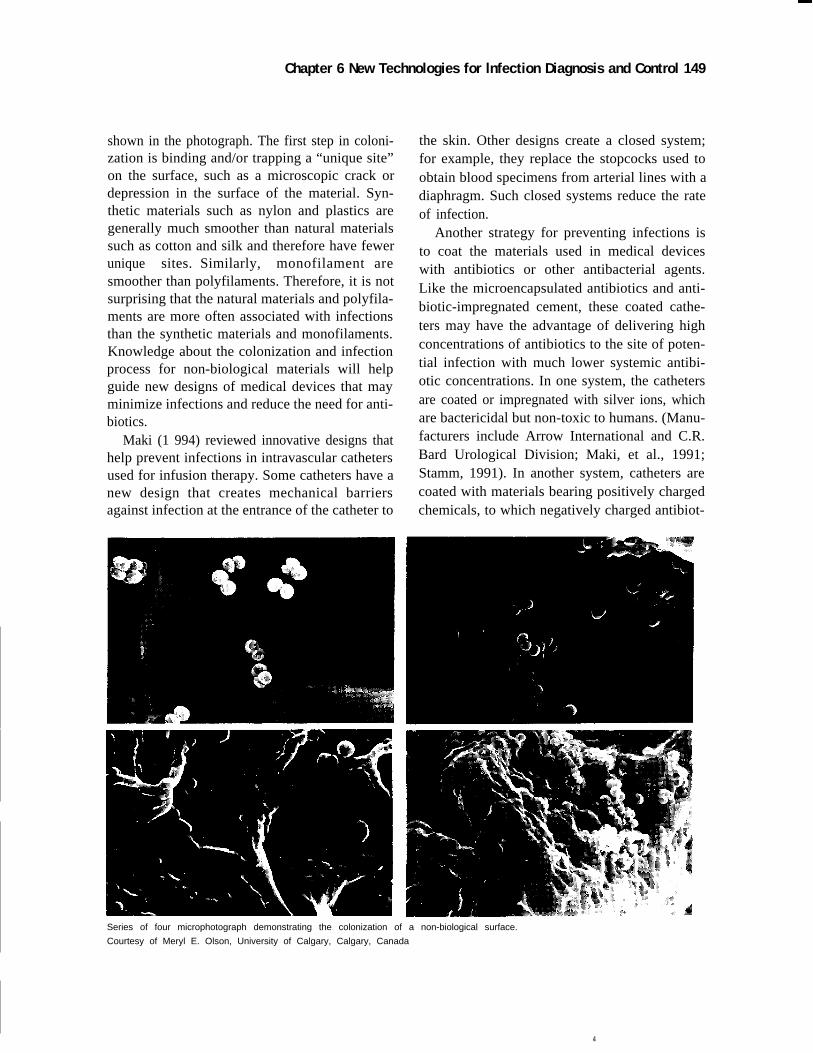
Chapter 6 New Technologies for lnfection Diagnosis and Control 149
shown in the photograph. The first step in coloni-zation is binding and/or trapping a “unique site”on the surface, such as a microscopic crack ordepression in the surface of the material. Syn-thetic materials such as nylon and plastics aregenerally much smoother than natural materialssuch as cotton and silk and therefore have fewerunique sites. Similarly, monofilament aresmoother than polyfilaments. Therefore, it is notsurprising that the natural materials and polyfila-ments are more often associated with infectionsthan the synthetic materials and monofilaments.Knowledge about the colonization and infectionprocess for non-biological materials will helpguide new designs of medical devices that mayminimize infections and reduce the need for anti-biotics.
Maki (1 994) reviewed innovative designs thathelp prevent infections in intravascular cathetersused for infusion therapy. Some catheters have anew design that creates mechanical barriersagainst infection at the entrance of the catheter to
the skin. Other designs create a closed system;for example, they replace the stopcocks used toobtain blood specimens from arterial lines with adiaphragm. Such closed systems reduce the rateof infection.
Another strategy for preventing infections isto coat the materials used in medical deviceswith antibiotics or other antibacterial agents.Like the microencapsulated antibiotics and anti-biotic-impregnated cement, these coated cathe-ters may have the advantage of delivering highconcentrations of antibiotics to the site of poten-tial infection with much lower systemic antibi-otic concentrations. In one system, the cathetersare coated or impregnated with silver ions, whichare bactericidal but non-toxic to humans. (Manu-facturers include Arrow International and C.R.Bard Urological Division; Maki, et al., 1991;Stamm, 1991). In another system, catheters arecoated with materials bearing positively chargedchemicals, to which negatively charged antibiot-
Series of four microphotograph demonstrating the colonization of a non-biological surface.
Courtesy of Meryl E. Olson, University of Calgary, Calgary, Canada
4

150 | Impacts of Antibiotic-Resistant Bacteria
ics are bound (Cook Bio-Guard AB coated cathe-ters, Cook Critical Care). A trial with thesecatheters coated with cefazolin showed a seven-fold decrease in the infection rate (Kamal,Pfaller, Rempe, et al., 1991). Further, a reductionin the infection rate was seen even if the cathe-ters were changed only once every seven days(compared to once every four days for standardcatheters; Kamal, Divishek, Adams, et al., 1994).The longer life of the coated catheter compen-sates for its higher cost (about $4.50 more percatheter).
OLD THERAPIESIn the pre-antibiotic era, scientists and physicianstried different methods to treat bacterial infec-tions. Two of those methods, “phage therapy”and “serum therapy,” are now mentioned as pos-sible treatments in a post-antibiotic era.
❚ Phage TherapyWhile most people may not recognize the term“phage therapy,” many people read about it inArrowsmith. The hero of that novel tried to treatbacterial infections by the use of viruses thatwould specifically attack the bacteria, and in reallife, many physicians tried the same method inthe early part of this century. Because virusesthat infect bacteria are called “bacteriophages”(literally, eaters of bacteria) or “phages” forshort, the treatment is called “phage therapy.”Phage therapy has remained outside the main-stream of medicine because of doubts about itsefficacy and the success of antibiotics.
Phages recognize specific binding sites on thebacteria. Therefore, phages that infect E. coligenerally do not infect other bacteria, and, infact, sometimes will only recognize a singlestrain of bacteria. This specificity offers thepromise of being able to prepare phages to attackparticular bacteria.
Levin and Bull (1995) and Levin, DeRouin,Moore, et al. (1995) review the literature aboutphage therapy. They focus on some recent exper-iments with systems that involve mice infectedwith E. coli and argue that phage therapy is
worth renewed investigation. While they do notthink that it will replace antibiotics, they believethat it may have some future use in treating anti-biotic-resistant bacteria. They also argue that thetime to develop alternatives to antibiotic therapyis now, when antibiotics remain effective againstmost diseases.
❚ Serum TherapyTextbooks of medicine and of microbiology pub-lished before 1940 are filled with instructions forserum therapy. In some respects similar to pas-sive immunization, serum therapy involves tak-ing blood serum from horses or rabbits that havesurvived an intentional bacterial infection andinjecting it into a patient suffering from an infec-tion by the same organism.
Serum is still used in the treatment of somediseases that involve bacterial toxins; in particu-lar, tetanus and botulism are treated with horseserum. Serum for the treatment of botulism iskept at several major airports around the country,ready for shipment to hospitals that diagnose therare disease. (According to the CDC [1979],there were about 10 outbreaks of botulism,involving about 2.5 people per outbreak, eachyear in the period 1899 through 1977.) For otherinfections, serum therapy was replaced as antibi-otics became available. A patient’s possible ana-phylactic response to chemical substances in theanimal serum is the chief danger.
Serum therapy may have application in treat-ing Escherichia coli O157:H7, which becamefamous as the cause of more than 500 cases ofdisease and perhaps four deaths in people whoate under-cooked fast-food hamburgers in thePacific Northwest in early 1993. The usual treat-ment for the disease does not include antibiotics(Salyers and Whitt, 1994). Antibiotics have notbeen shown to shorten the course of the diseaseor to reduce the occurrence of kidney complica-tion. Further, antibiotic treatment may cause thebacteria to increase the production of the bacte-rial toxin that causes the disease. The cause ofdisease in E. coli O157:H7 infections is a toxinthat resembles the Shigella toxin that causes dys-

Chapter 6 New Technologies for Infection Diagnosis and Control | 151
entery. That toxin has been isolated and purified.Antibodies generated against the toxin havepotential in treating E. coli O157:H7-caused dis-eases, but the market for such a drug is small,and no trials are in progress.
SUMMARYThis chapter reviews some new technologies thatwill help health care providers use antibioticsmore effectively. Diagnostic technologies helpthe clinician identify the specific bacteria caus-ing the infection and its susceptibility to antibiot-ics. This information is critical for choosing themost appropriate antibiotic. New technologies,such as DNA identification of antibiotic resis-tance genes, have the potential to provide thisinformation more quickly than is possible withtraditional diagnostic tests, which require grow-ing the bacteria in cultures. These new diagnostictechnologies have already proven useful in diag-nosing tuberculosis. Many companies are rapidlydeveloping additional tests for TB and other bac-teria. There are unresolved issues with respect tothe accuracy, sensitivity, and reproducibility ofthese tests. These issues may not be resolveduntil the tests have received FDA review and arewidely used in clinical settings. This chapter dis-cusses some of these issues.
Preventing infections is another way to slowthe increase of antibiotic-resistant bacteriabecause prevention will reduce the total use ofantibiotics. Methods of preventing infectioninclude vaccines and changes in the design andcomposition of medical devices to prevent thegrowth of bacteria. The recent introduction of avaccine against Hemophilus influenza B resultedin a dramatic reduction in the incidence of child-hood diseases caused by this bacteria. A numberof other vaccines are under development, includ-ing those for Staphylococcus aureus, as well asbetter vaccines for Streptococcus pneumoniae.Indwelling devices and sutures are often ports ofentry for bacteria into the body, and improveddevices and materials have been shown to reduceinfection rates. Further research and applicationcould produce further reductions.
REFERENCESAbe, C., K. Hirano, M. Wada, et al. 1993. Detec-
tion of Mycobacterium tuberculosis in clini-cal specimens by polymerase chain reactionand Gen-Probe Amplified MycobacteriumTuberculosis Direct Test. Journal of ClinicalMicrobiology 31:3270–3274.
Adams, W.G., K.A. Deaver, S.L. Cochi, et al.1993. Decline of childhood Haemophilusinfluenzae type b (Hib) disease in the Hibvaccine era. Journal of the American Medi-cal Association 269:221–226.
American Medical News. March 27, 1995. Chi-cago, IL. American Medical Association.
Bellin, E. 1994. Letter to the Editor. Journal ofthe American Medical Association 272: 765.
Christensen, G.D., L. Baldassarri, and W.A.Simpson. 1994. Colonization of medicaldevices by coagulase-negative staphylo-cocci. In: A.L. Bisno and F.A. Waldvogel(eds.) Infections Associated with IndwellingMedical Devices. Washington, DC. ASMPress.
Cohen, M.L. 1994. Antibiotic resistance: Prog-nosis for public health. Trends in Microbiol-ogy 2:422–425.
Coldwitz, G.A., T.F. Brewer, C.S. Berkey, et al.1994. Efficacy of BCG vaccine in the pre-vention of tuberculosis: Meta-analysis of thepublished literature. Journal of the AmericanMedical Association 271:698–702.
Coldwitz, G.A., T.F. Brewer, C.S. Berkey, et al.1994a. Letter to the Editor. Journal of theAmerican Medical Association 272:766.
Comstock, G. 1994. Letter to the Editor. Journalof the American Medical Association272:766.
Crawford, J., H. Ozer, R. Stoller, et al. 1991.Reduction by granulocyte colony-stimulat-ing factor of fever and neutropenia inducedby chemotherapy in patients with small-celllung cancer. New England Journal of Medi-cine 325:164–170.
Daly, J.S., G.M. Eliopoulos, E. Reiszner, et al.1988. Activity and mechanism of action ofDuP105 and DuP721, new oxazolidononecompounds. Journal Antimicrobial Chemo-therapy 21:721–730.
152 | Impacts of Antibiotic-Resistant Bacteria
Diaz-Buxo, J.A. 1993. Differences betweenCAPD and CCPD: Implications for therapy.Seminars in Dialysis 6:312–315.
Doern, G.V., D.R. Scott, and A.L. Rashad. 1982.Clinical impact of rapid antimicrobial sus-ceptibility testing of blood culture isolates.Antimicrobial Agents and Chemotherapy21:1023–1024.
Doern, G.V., R. Vautour, M. Gaudet, et al. 1994.Clinical impact of rapid in-vitro susceptibil-ity testing and bacterial identification. Jour-nal of Clinical Microbiology 32:1757–1762.
Edwards, L.D., S. Levin, R. Balogtas, et al. 1973.Ordering patterns and utilization of bacterio-logic identification. Archives of InternalMedicine 132:678–682.
Fanaroff, A.A., S.B. Korones, L.L. Wright, et al.1994. A controlled trial of intravenousimmune globulin to reduce nosocomialinfections in very-low-birth-weight infants.New England Journal of Medicine330:1107–1113.
Fatton, A., R. Schneerson, S.C. Szu, et al. 1990.Synthesis and immunologic properties inmice of vaccine composed of Staphylococ-cus aureus type 5 and type 8 capsularpolysaccharides conjugated to Pseudomonasaeruginosa exotoxin A. Infection and Immu-nity 58:2367–2374.
Fatton, A., J. Shiloach, D. Bryla, et al. Compara-tive immunogenicity of conjugates com-posed of the Staphylococcus aureus type 8capsular polysaccharide bound to carrierproteins by adipic acid dihydrazide or N-succinimidyl-3(2-pyridyldithio) propionate.Infection and Immunity 60:584–589.
Favero, M.S., M.J. Alter, and L.A. Bland. 1992.Dialysis-associated infections and their con-trol. In: J.V. Bennett, and P.S. Brachman(eds.) Hospital Infections Third Edition.Boston, MA. Little, Brown and Company.
Gustilo, R.B., R.M. Mendoza, and D.N. Will-iams. 1984. Problems in the management oftype III (severe) open fractures: A new clas-sification of type III open fractures. Journalof Trauma 24:742–746.
Haas, D.W., and R.M. Des Prez. 1995. Mycobac-terium tuberculosis. In: G.L. Mandell, J.E.
Bennett, and R. Dolin (eds.) Mandel, Dou-glas and Bennett’s Principles and Practiceof Infectious Diseases Fourth edition. NewYork, NY. Churchill Livingstone, Inc.
Hakin, R.M. 1993. Clinical implications ofhemodialysis membrane biocompatibility.Kidney International 44:484–494.
Hewlette, D. Jr., D.L. Horn, and C. Alfalla. 1995.Drug-resistant tuberculosis: Inconsistentresults of pyrazinamide susceptibility test-ing. Journal of the American Medical Asso-ciation 273:916–917.
Heiter, B.J., and B.P. Bourbeau. 1993. Compari-son of the Gen-Probe Group A Streptococ-cus Direct Test with culture and rapidstreptococcal antigen detection assay fordiagnosis of streptococcal pharyngitis. Jour-nal of Clinical Microbiology 31(8):2070–2073.
Institute of Medicine. 1992. Emerging InfectiousDiseases. Washington, DC. National Acad-emy Press.
Jacob, E., G. Cierny, M.T. Fallon, et al. 1993.Evaluation of biodegradable cefazolinsodium microspheres for the prevention ofinfections in rabbits with experimental openttibial fractures stabilized with internal fixa-tion. Journal of Orthopedic Research11:404–411.
Jacob, E., J.M. Erpelding, and K.P. Murphy.1992. A retrospective analysis of open frac-tures sustained by U.S. military personnelduring Operation Just Cause. Military Medi-cine 157:552–556.
Jacob, E., J.A. Setterstrom, D.E. Bach, et al.1991. Evaluation of biodegradable ampicil-lin anhydrate microcapsules for local treat-ment of experimental staphylococcalosteromyelitis. Clinical Orthopedics267:237–244.
Jacobs, W.R., Jr., R.G. Barletta, R. Udani, et al.1993. Rapid assessment of drug susceptibili-ties of Mycobacterium tuberculosis bymeans of luciferase reporter phages. Science260:819–822)
Jorgensen, J.H. 1993. Recent developments inautomated and rapid susceptibility testingmethods. In: R.C. Spencer, E.P. Wright, and
Chapter 6 New Technologies for Infection Diagnosis and Control | 153
S.W.B. Newson (eds.) Rapid Methods andAutomation in Microbiology and Immunol-ogy. Andover, England. Intercept Ltd.
Jorgensen, J.H. 1995. Current and Future Pheno-typic Methods for Detection of ResistantBacteria. Contract report to the Office ofTechnology Assessment. Photocopied type-script.
Jorgensen, J.H., and J.M. Matsen. 1987. Physi-cian acceptance and application of rapidmicrobiology instrument test results. In: J.H.Jorgensen (ed.) Automation in ClinicalMicrobiology. Boca Raton, FL. CRC Press,Inc.
Kamal, G., D. Divishek, J. Adams, et al. 1994.Reduced intravascular catheter infection byroutine use of antibiotic bonded catheters(abstract). Critical Care Medicine 22:A115.
Kamal, G.D., M.A. Pfaller, L.E. Rempe, et al.1991. Reduced intravascular catheter infec-tion by antibiotic bonding: A prospective,randomized, controlled trial. Journal of theAmerican Medical Association 265:2364–2368.
King, L.K., J.C. Kingswood, P. Sharpstone.1992. Comparison of the efficacy, cost, andcomplication rate of APD and CAPD aslong-term outpatient treatments for renalfailure. In: R. Khanna, K.D. Nolph, B.F.Prowant, et al. (eds.) Advances in PeritonealDialysis. Vol. 8. Toronto, Canada. pp. 123–126.
Kohner, P., C. Kolbert, D. Geha, et al. 1994.Evaluation of the BBL Crystal MRSA IDSystem for the detection of methicillin resis-tance in Staphylococci. Abstract presented atthe 93rd General Meeting, American Societyfor Microbiology, Las Vegas, Nevada.
Kuusela, P., P. Hilden, K. Savolainen, et al.1994. Rapid detection of methicillin-resis-tant Staphylococcus aureus strains not iden-tified by slide agglutination tests. Journal ofClinical Microbiology 32:143–147.
Levin, B.R. and J.J. Bull. 1995. Phage therapyrevisited: The population biology of a bacte-rial infection and its treatment with bacte-riophage and antibiotics. AmericanNaturalist. Submitted.
Levin, B.R., T. DeRouin, N. Moore, and J.J.Bull. 1995. Phage therapy revisited II: Anexperimental study of the population dynam-ics of a bacterial infection and its controlwith antibiotics and bacteriophage. Microbi-ology. Submitted.
Macher, A. and E. Goosby. 1995. PCR and themisdiagnosis of active tuberculosis. Letter.New England Journal of Medicine332(2):128–129.
Maderazo, E.G., S. Judson, and H. Pasternak.1988. Late infections of total joint prosthe-sis. Clinical Orthopedics 229:131–142.
Maki, D.G. 1994. Infections caused by intravas-cular devices used for infusion therapy:pathogenesis, prevention, and management.In: A.L. Bisno and F.A. Waldvogel (eds.)Infections Associated with Indwelling Medi-cal Devices. Washington, DC. ASM Press.
Marchetti, M., B. Arico, D. Burroni, et al. 1995.Development of a mouse model of Helico-bacter pylori infection that mimics humandisease. Science 267:1655–1658.
McKee, J.A., S.K. Sharma, and M.J. Miller.1991. Iron transport mediated drug deliverysystems: Synthesis and antibacterial activityof spermidine- and lysine-based sidero-phore-β lactam conjugates. BioconjugateChemistry 2:281–291.
Miller, M.J. 1989. Synthesis and therapeuticpotential of hydroxamic acid based sidero-phores and analogues. Chemical Reviews89:1563–1579.
Medical World News. 1995. CDC says many eld-erly skipping pneumovax. Medical WorldNews 34(6):11.
O’Brien, T. 1994. Remarks at U.S. Food andDrug Administration, Part 15 Hearing: Sur-veillance Systems for Antibacterial Resis-tance. Rockville, MD, November 9, 1994.
Rippin, K., C. Carlyn, J. Goldfard, et al. 1994.Rapid direct DNA probe testing of throatswabs for group A Streptocccus (GrAS)from pediatric patients. Abstract D1.Abstracts of the 34th Interscience Confer-ence on Antimicrobial Agents and Chemo-therapy. Washington, DC. American Societyfor Microbiology.
154 | Impacts of Antibiotic-Resistant Bacteria
Salyers, A.A. and D.D. Whitt. 1994. BacterialPathogenesis: A Molecular Approach.Washington, DC. ASM Press.
Setterstrom, J.A., T.R. Tice, and W.E. Myers.1984. Development of encapsulated antibi-otics for topical administration to wound. In:J.M. Anderson, and S.W. Kim (eds.) 1984.Recent Advances in Drug Delivery Systems.New York, NY. Plenum Press, pp. 185–198.
Siber, G.R. 1994. Pneumococcal disease: pros-pects for a new generation of vaccines. Sci-ence 265:1385–1387.
Smits, H. 1995. Testimony presented before theSubcommittee on Health, Committee onWays and Means, United States House ofRepresentatives, on the Medicare End StageRenal Disease (Kidney Failure) Program,April 3.
Stamm, W.E. 1991. Catheter-associated urinarytract infections: epidemiology, pathogenesis,and prevention. American Journal of Medi-cine 91(3B):65S–71S.
Stratton, C.W., and R.C. Cooksey. 1990. Suscep-tibility tests: special tests. In: A. Balows,W.J. Hausler, K.L. Herrmann, et al. Manualof Clinical Microbiology, 5th Edition. Wash-ington, DC. American Society of Microbiol-ogy.
Tompkins, L.S., and S. Falkow. 1995. The newpath to preventing ulcers. Science267:1621–1622.
Travis, M.T., and M.Q. Cosio. 1993. A retro-spective review of orthopedic patientsreturning from Operation Desert Shield andDesert Storm to an Army medical center.Military Medicine 158:348–351.
Trenholme, G.M., R.L. Kaplan, P.H. Karahusis,et al. 1989. Clinical impact of rapid identifi-cation and susceptibility testing of bacterialblood culture isolates. Journal of ClinicalMicrobiology 27:1342–1345.
Univax Biologics, Inc. Rockville, MD. 1994.Personal communication to D. Frankle. Dataon file.
U.S. Congress, Office of Technology Assess-ment. 1993. The Continuing Challenge ofTuberculosis. U.S. Government PrintingOffice: Washington, DC.
U.S. Department of Health and Human Services,Food and Drug Administration. 1995. Com-ments on second draft of this OTA report.Memorandum from Associate Commis-sioner for Legislative Affairs, U.S. Food andDrug Administration to Office of Technol-ogy Assessment. June 16.
U.S. Department of Health, Education, and Wel-fare, Center for Disease Control. 1979. Botu-lism in the United States, 1899–1977.Handbook for Epidemiologists, Clinicians,and Laboratory Workers. Washington, DC.
Wanger A. and Mills K. 1995. E-Test for Sus-ceptibility Testing of Mycobacterium tuber-culosis to first line antituberculosis agents.Poster U-67. American Society for Microbi-ology 95th General Meeting. WashingtonDC.
Weinstein, M.P., J.R. Murphy, L.B. Reller, et al.1983. The clinical significance of positiveblood cultures: A comprehensive analysis of500 episodes of bacteremia and fungemia inadults. II. Clinical observations, with specialreferences to factors influencing prognosis.Reviews of Infectious Disease 5:54–70.
Wenger, J.D. 1994. Mini review: Impact of Hae-mophilus influenzae type B vaccines on theepidemiology of bacterial meningitis. Infec-tious Agents and Disease 2:324–332.
Wheeler, J.G., L.C. Rodrigues, and V. Diwan.1994. Letter to the Editor. Journal of theAmerican Medical Association 272:765–766.
Wischnack, L.L., R.M. Jacobson, G.A. Poland,et al. 1995. The surprisingly high acceptabil-ity of low-efficacy vaccines for otitis media:A survey of parents using hypothetical sce-narios. Pediatrics 95:350–354.
Yu et al. 1992. Self-setting hydroxyapatitecement: a novel skeletal drug-delivery sys-tem for antibiotics. Journal PharmaceuticalSciences 81:529–531.
| 155
7
Antibiotics inAnimal
Husbandry
hat effect does the use of antibioticsin food production have on theoccurrence of antibiotic-resistantbacteria? Everyone concerned with
that question agrees about a few things: Abouthalf of the antibiotics (by weight) used in theUnited States are used in the production of foodanimals, much smaller amounts are used to con-trol bacterial diseases in plants and in fish farm-ing, and some proportion of the bacteria that arepresent in and on food may survive cooking orother preparation in the food eaten by humans.Beyond such small areas of agreement, there iswidespread disagreement, or so it would seem. Infact, the real questions about the transfer of anti-biotic-resistant bacteria from foods to humansare how often does it happen and what are itsconsequences, rather than does it happen at all.
The chairman of a National Research Council(NRC) advisory panel that looked at the questionneatly posed a scenario for the risks from use ofantibiotics in farm animals:
...a beef producer feeds tetracycline in lowdoses to his calves to encourage rapid weightgain; nonpathogenic Escherichia coli in the gutsof the calves acquire antibiotic resistance.Somewhere along the chain from feedlot todinner table, the E. coli may come into close
association with some salmonella, and the sal-monella may acquire resistance to antibiotics byplasmid transfer. The meat eater becomesinfected, develops Salmonella septicemia anddies while his physicians are treating him withan inadequate antibiotic (Stallones, 1982).
The scenario is clearly stated, but how oftendoes it occur? That question could be answeredby identifying people who harbor antibiotic-resistant bacteria and linking those bacteria tomeat that was derived from antibiotic-treatedanimals. That has proved impossible to do; thereare many possible sources for bacteria, each onewould have to be eliminated, and it is difficult totrace the origins of “meat” as it arrives at abutcher shop or supermarket. “[S]ome studiescan be conceived but cannot be delivered” (Stal-lones, 1982).
In the absence of definitive information, dis-agreements about the significance of antibioticuse in agriculture on the emergence of antibiotic-resistant human pathogens have fostered severalreviews and analyses of the data about animal tohuman transfer of antibiotic-resistant bacteria.Congress requested an Office of TechnologyAssessment (OTA) study, Drugs in LivestockFeed, that reviewed risks and benefits of antibi-otic (and other drug) use in agriculture including
W

156 | Impacts of Antibiotic-Resistant Bacteria
the risks of increasing the prevalence of antibi-otic-resistant bacteria in humans (OTA 1979).OTA did not reach a hard and fast conclusionabout the magnitude of the risk. Instead, it putthat risk in context by comparing it to the risk ofantibiotic resistance developing as a result ofantibiotic use in medicine, and concluded that therisk exists, but that it is less than the risk fromuses of antibiotics in humans:
The risk from resistant plasmids of animalorigin is not quantifiable....The majority ofresistance in human bacterial populations isprobably caused by widespread use of antibac-terials in humans (some of which are unneces-sary), but the enormous pool of R-plasmids thatnow exist in animals, together with the abilityof an R-plasmid to be promiscuously trans-ferred among bacterial species, must beregarded as a threat to the therapeutic value ofantibacterials in the treatment of both humanand animal diseases. (U.S. Congress, Office ofTechnology Assessment 1979, p. 7)
A year later, an NRC committee (1980)reached a similar conclusion, and painted a bleakpicture about the possibility of learning more:
After reviewing the evidence, the committeeconcluded that the postulations concerning thehazards to human health that might result fromthe addition of subtherapeutic antimicrobials tofoods have been neither proven nor disproven.The lack of data linking human illness with sub-therapeutic levels of antimicrobials must not beequated with proof that the proposed hazards donot exist. The research necessary to establishand measure a definite risk has not been con-ducted, and, indeed may not be possible.
In contrast to the report’s conclusion that sug-gests the possibility of a link between uses ofantibiotics in animals and human health, thechairman of the NRC committee, in a later publi-cation, downplayed any risk: “If the decisionwere mine, the hog farmers could use all the anti-biotic drugs they wish to make the pigs grow.The risk to humans looks to me to be vanishinglysmall” (Stallones, 1982). Not everyone sharedthat opinion, and studies and reviews have con-tinued to the present time.
Almost a decade later, the Institute of Medi-cine (IOM) issued a report that dealt with therisks from subtherapeutic use of two commonantibiotics—penicillin and two kinds of tetracy-clines (oxytetracycline and chlortetracycline)—in animal feeds (IOM, 1989). Its authors furthernarrowed the focus of the report to the risks ofantibiotic-resistant Salmonella from animalsources causing human deaths. The authors cal-culated that,
“The likeliest estimate of excess deaths attribut-able to subtherapeutic uses of penicillin and/orthe tetracylines...is in the range of 6 per year.”
The committee also considered the difficultiesthat might arise in treating antibiotic-resistantSalmonella infections in humans and calculatedthat,
“The likeliest estimate of deaths...arisingbecause of ‘increased difficulty of disease treat-ment’ is 20 per year.”
At the same time, the committee acknowledgedthat it
“was unable to find a substantial body of directevidence that established the existence of a def-inite human health hazard in the use of subther-apeutic concentrations of penicillin and thetetracyclines in animal feeds.”
The controversy over the health effects ofantibiotic use in animal husbandy has spawnedseveral expert committee reviews that have clari-fied the issue somewhat (see table 7-1 for a list-ing of review bodies other than the threementioned above). There is no doubt that riskexists. There is also no doubt that direct evi-dence, in the form of studies that show a directconnection between agricultural use of antibiot-ics and human illness or death, is sparse anddifficult to obtain. Moreover, if the IOM com-mittee’s estimate of the number of deaths causedby antibiotic-resistant Salmonella of agriculturalorigin is in the right range, determining what pro-portion of the 40,000 cases of reported Salmo-nella infection each year is related to agriculturaluse of antibiotics is probably impossible.
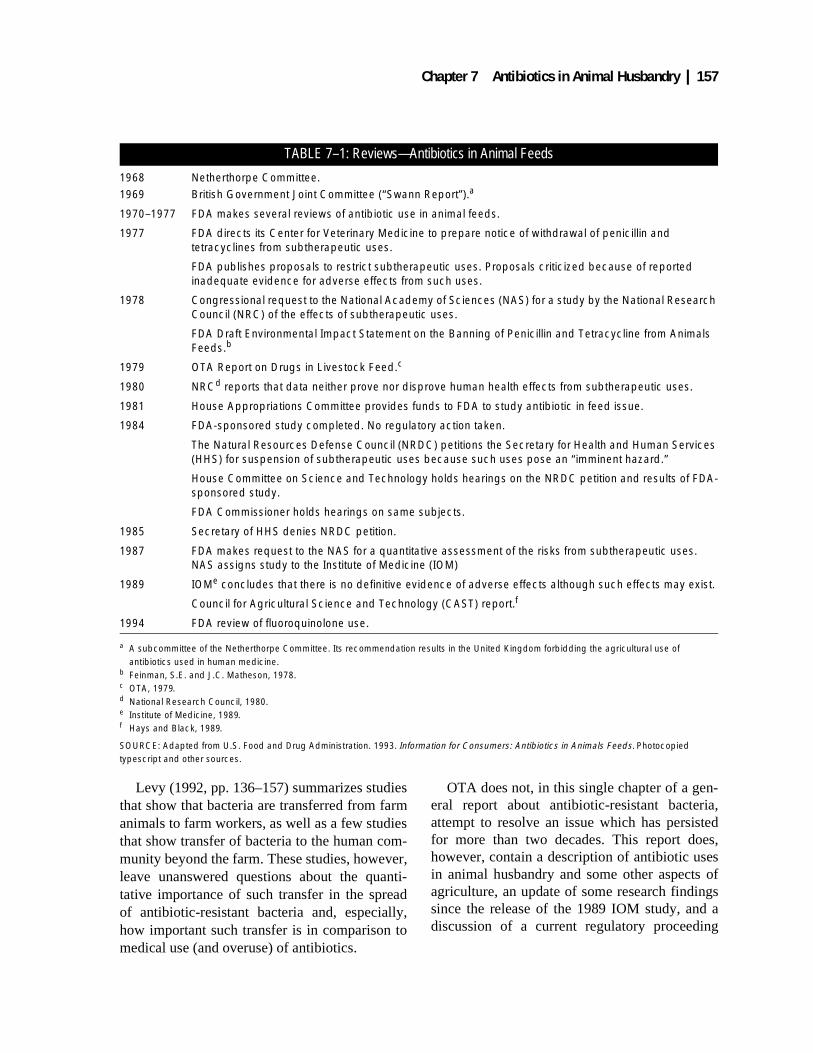
Chapter 7 Antibiotics in Animal Husbandry | 157
Levy (1992, pp. 136–157) summarizes studiesthat show that bacteria are transferred from farmanimals to farm workers, as well as a few studiesthat show transfer of bacteria to the human com-munity beyond the farm. These studies, however,leave unanswered questions about the quanti-tative importance of such transfer in the spreadof antibiotic-resistant bacteria and, especially,how important such transfer is in comparison tomedical use (and overuse) of antibiotics.
OTA does not, in this single chapter of a gen-eral report about antibiotic-resistant bacteria,attempt to resolve an issue which has persistedfor more than two decades. This report does,however, contain a description of antibiotic usesin animal husbandry and some other aspects ofagriculture, an update of some research findingssince the release of the 1989 IOM study, and adiscussion of a current regulatory proceeding
TABLE 7–1: Reviews—Antibiotics in Animal Feeds
1968 Netherthorpe Committee.1969 British Government Joint Committee (“Swann Report”).a
1970–1977 FDA makes several reviews of antibiotic use in animal feeds.
1977 FDA directs its Center for Veterinary Medicine to prepare notice of withdrawal of penicillin and tetracyclines from subtherapeutic uses.
FDA publishes proposals to restrict subtherapeutic uses. Proposals criticized because of reported inadequate evidence for adverse effects from such uses.
1978 Congressional request to the National Academy of Sciences (NAS) for a study by the National Research Council (NRC) of the effects of subtherapeutic uses.
FDA Draft Environmental Impact Statement on the Banning of Penicillin and Tetracycline from Animals Feeds.b
1979 OTA Report on Drugs in Livestock Feed.c
1980 NRCd reports that data neither prove nor disprove human health effects from subtherapeutic uses.
1981 House Appropriations Committee provides funds to FDA to study antibiotic in feed issue.
1984 FDA-sponsored study completed. No regulatory action taken.
The Natural Resources Defense Council (NRDC) petitions the Secretary for Health and Human Services (HHS) for suspension of subtherapeutic uses because such uses pose an “imminent hazard.”
House Committee on Science and Technology holds hearings on the NRDC petition and results of FDA-sponsored study.
FDA Commissioner holds hearings on same subjects.
1985 Secretary of HHS denies NRDC petition.
1987 FDA makes request to the NAS for a quantitative assessment of the risks from subtherapeutic uses. NAS assigns study to the Institute of Medicine (IOM)
1989 IOMe concludes that there is no definitive evidence of adverse effects although such effects may exist.
Council for Agricultural Science and Technology (CAST) report.f
1994 FDA review of fluoroquinolone use.
a A subcommittee of the Netherthorpe Committee. Its recommendation results in the United Kingdom forbidding the agricultural use of antibiotics used in human medicine.
b Feinman, S.E. and J.C. Matheson, 1978.c OTA, 1979. d National Research Council, 1980.e Institute of Medicine, 1989.f Hays and Black, 1989.
SOURCE: Adapted from U.S. Food and Drug Administration. 1993. Information for Consumers: Antibiotics in Animals Feeds. Photocopied typescript and other sources.

158 | Impacts of Antibiotic-Resistant Bacteria
about approving of fluoroquinolone antibioticsfor use in food animals.
ANTIBIOTIC USE IN FOOD PRODUCTIONEveryone, whether a city dweller or farmer,knows about antibiotic uses in medicine. Doctorsprescribe antibiotics to treat diseases, in advanceof certain surgical procedures to prevent infec-tion, and, sometimes, as prophylaxis during den-tal procedures to prevent infections in peoplewith heart valve abnormalities. In all these casesthe administration of the antibiotic is overseen bya physician.
Paralleling physicians’ practice in humans,veterinarians use antibiotics to treat infectiousdiseases in food (and companion) animals.1 Butfrom there on, things are different on the farm.There are differences in medical and veterinariandiagnostic laboratories, and veterinarian diagnos-tic laboratories reportedly do not meet the samestandards for accuracy and reliability as do medi-cal laboratories (Walker, 1994). Currently, how-ever, practices are changing in veterinarylaboratories, and the National Commission forClinical Laboratory Standards has recently pub-lished the first guideline document for detectingantibiotic sensitivity in animal pathogens. Lackof laboratory quality assurance is not, however,the major difference between uses of antibioticsin animals and humans.
The major difference is that about 90 percentof all the antibiotics used in food animals is usedin subtherapeutic doses and not for the treatmentof sick animals. For instance, in 1985, veterinari-ans used about 1 million kilograms (about 2.2million pounds or 1,100 tons) of antibiotics totreat diseases in cattle, swine, and poultry. Dur-ing the same year, farmers fed about 5 millionkilograms of antibiotics to cattle, swine, andpoultry for “disease prevention,” and another 2million kilograms for “growth promotion” (table7-2). The estimated total of all antibiotics used in
1 “In fact, it has been said that the definition of a physician is a veterinarian with a limited knowledge that restricts his practice to a singlespecies.” (Walker, R. 1994. Remarks at U.S. Food and Drug Administration, Part 15 Hearing: Surveillance Systems for Antibacterial Resis-tance, Rockville Civic Center, Rockville, MD, November 10.)
cattle, swine, and poultry in that year was 8 mil-lion kilograms, or 18 million pounds.
“Disease prevention” describes prophylacticactions taken to stave off the spread of a disease.If a poultry producer notices that a few chickensare ill and he suspects that the illness is causedby bacteria, he could add antibiotics to the feedor water in an effort to stop the spread of the dis-ease. These decisions can be made by the poultryproducer acting alone without any involvementof a veterinarian.
“Growth promotion” is a little-understoodeffect from feeding low levels of antibiotics, gen-erally at a rate of 200 grams or less of antibioticin each ton of feed. How such levels of antibiot-ics affect growth is not clear; they may ward offundetectable but consequential, minor infections,or they may have other effects.
Both disease prevention and growth promo-tion are long-term uses, and the U.S. Food andDrug Administration (FDA) uses 14 days as thethreshold for long-term use. When a companyrequests approval for longer-than-14-day use,FDA requires the company to demonstrate thatsuch use will not increase the shedding of Salmo-nella (through feces) that might infect humansand that it will not increase the number of antibi-otic-resistant bacteria that contaminate carcasses.FDA (1995) has stated that submissions ofrequests for approval of long-term uses of antibi-otics are decreasing, being replaced, in part, byrequests for approval of somatotropins and othergrowth-promoting substances. More specifically,R.H. Teske of FDA (1995) has stated that, “It isnot likely that FDA will see applications forlong-term use of antibiotics that have therapeuticuses.”
There is so much overlap between prophylac-tic uses and doses and growth-promotion usesand doses that the division between the twoapplications that is shown in table 7-2 must beregarded as uncertain. Furthermore, the estimates
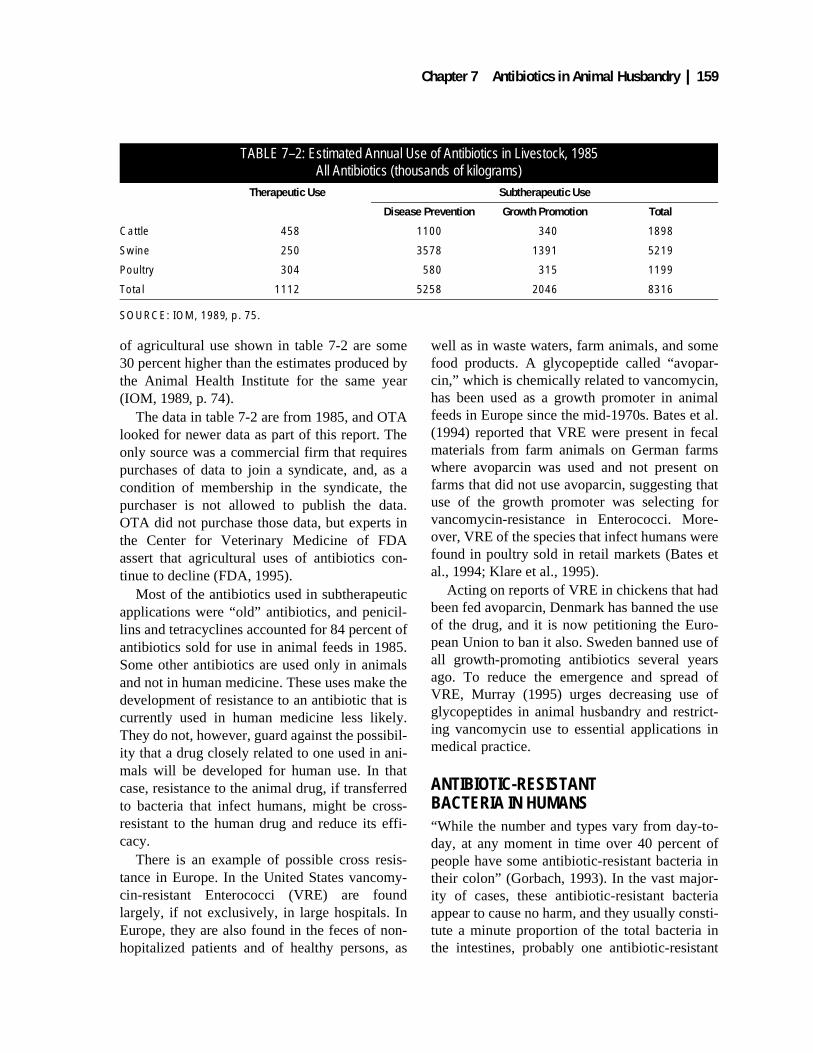
Chapter 7 Antibiotics in Animal Husbandry | 159
of agricultural use shown in table 7-2 are some30 percent higher than the estimates produced bythe Animal Health Institute for the same year(IOM, 1989, p. 74).
The data in table 7-2 are from 1985, and OTAlooked for newer data as part of this report. Theonly source was a commercial firm that requirespurchases of data to join a syndicate, and, as acondition of membership in the syndicate, thepurchaser is not allowed to publish the data.OTA did not purchase those data, but experts inthe Center for Veterinary Medicine of FDAassert that agricultural uses of antibiotics con-tinue to decline (FDA, 1995).
Most of the antibiotics used in subtherapeuticapplications were “old” antibiotics, and penicil-lins and tetracyclines accounted for 84 percent ofantibiotics sold for use in animal feeds in 1985.Some other antibiotics are used only in animalsand not in human medicine. These uses make thedevelopment of resistance to an antibiotic that iscurrently used in human medicine less likely.They do not, however, guard against the possibil-ity that a drug closely related to one used in ani-mals will be developed for human use. In thatcase, resistance to the animal drug, if transferredto bacteria that infect humans, might be cross-resistant to the human drug and reduce its effi-cacy.
There is an example of possible cross resis-tance in Europe. In the United States vancomy-cin-resistant Enterococci (VRE) are foundlargely, if not exclusively, in large hospitals. InEurope, they are also found in the feces of non-hopitalized patients and of healthy persons, as
well as in waste waters, farm animals, and somefood products. A glycopeptide called “avopar-cin,” which is chemically related to vancomycin,has been used as a growth promoter in animalfeeds in Europe since the mid-1970s. Bates et al.(1994) reported that VRE were present in fecalmaterials from farm animals on German farmswhere avoparcin was used and not present onfarms that did not use avoparcin, suggesting thatuse of the growth promoter was selecting forvancomycin-resistance in Enterococci. More-over, VRE of the species that infect humans werefound in poultry sold in retail markets (Bates etal., 1994; Klare et al., 1995).
Acting on reports of VRE in chickens that hadbeen fed avoparcin, Denmark has banned the useof the drug, and it is now petitioning the Euro-pean Union to ban it also. Sweden banned use ofall growth-promoting antibiotics several yearsago. To reduce the emergence and spread ofVRE, Murray (1995) urges decreasing use ofglycopeptides in animal husbandry and restrict-ing vancomycin use to essential applications inmedical practice.
ANTIBIOTIC-RESISTANT BACTERIA IN HUMANS“While the number and types vary from day-to-day, at any moment in time over 40 percent ofpeople have some antibiotic-resistant bacteria intheir colon” (Gorbach, 1993). In the vast major-ity of cases, these antibiotic-resistant bacteriaappear to cause no harm, and they usually consti-tute a minute proportion of the total bacteria inthe intestines, probably one antibiotic-resistant
TABLE 7–2: Estimated Annual Use of Antibiotics in Livestock, 1985All Antibiotics (thousands of kilograms)
Therapeutic Use Subtherapeutic Use
Disease Prevention Growth Promotion Total
Cattle 458 1100 340 1898
Swine 250 3578 1391 5219
Poultry 304 580 315 1199
Total 1112 5258 2046 8316
SOURCE: IOM, 1989, p. 75.
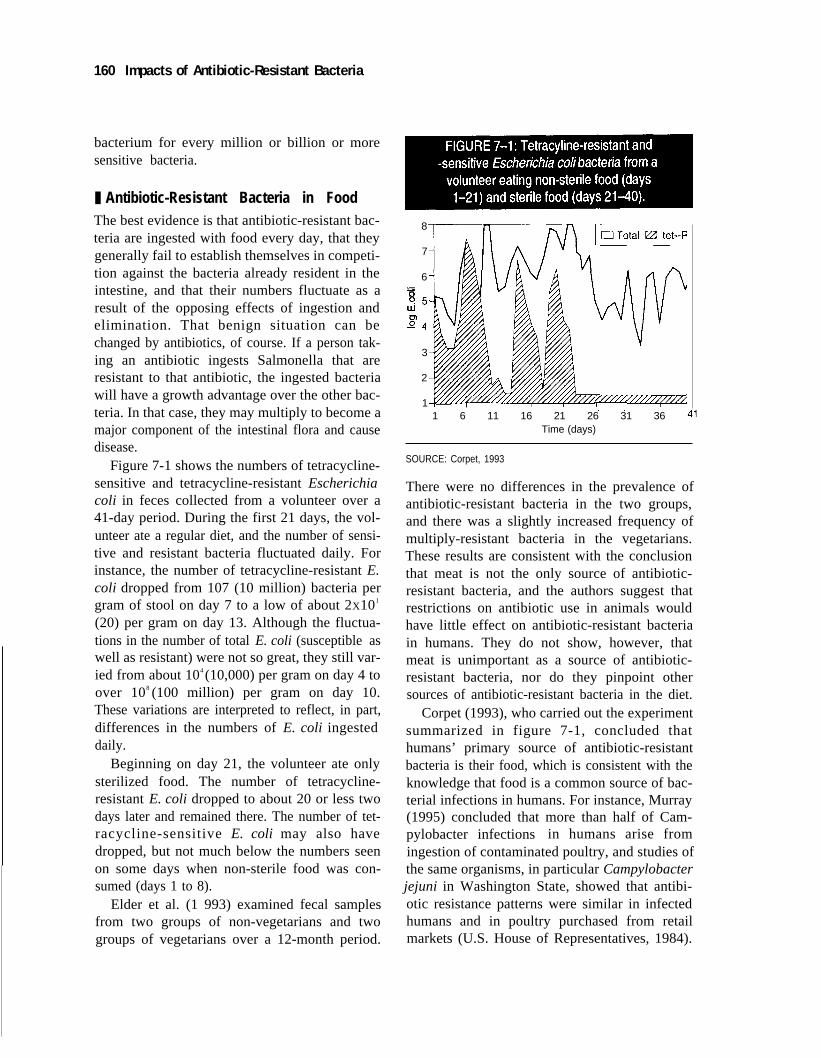
160 Impacts of Antibiotic-Resistant Bacteria
bacterium for every million or billion or moresensitive bacteria.
❚ Antibiotic-Resistant Bacteria in FoodThe best evidence is that antibiotic-resistant bac-teria are ingested with food every day, that theygenerally fail to establish themselves in competi-tion against the bacteria already resident in theintestine, and that their numbers fluctuate as aresult of the opposing effects of ingestion andelimination. That benign situation can bechanged by antibiotics, of course. If a person tak-ing an antibiotic ingests Salmonella that areresistant to that antibiotic, the ingested bacteriawill have a growth advantage over the other bac-teria. In that case, they may multiply to become amajor component of the intestinal flora and causedisease.
Figure 7-1 shows the numbers of tetracycline-sensitive and tetracycline-resistant Escherichiacoli in feces collected from a volunteer over a41-day period. During the first 21 days, the vol-unteer ate a regular diet, and the number of sensi-tive and resistant bacteria fluctuated daily. Forinstance, the number of tetracycline-resistant E.coli dropped from 107 (10 million) bacteria pergram of stool on day 7 to a low of about 2X101
(20) per gram on day 13. Although the fluctua-tions in the number of total E. coli (susceptible aswell as resistant) were not so great, they still var-ied from about 104 (10,000) per gram on day 4 toover 108 (100 million) per gram on day 10.These variations are interpreted to reflect, in part,differences in the numbers of E. coli ingesteddaily.
Beginning on day 21, the volunteer ate onlysterilized food. The number of tetracycline-resistant E. coli dropped to about 20 or less twodays later and remained there. The number of tet-racycline-sensitive E. coli may also havedropped, but not much below the numbers seenon some days when non-sterile food was con-sumed (days 1 to 8).
Elder et al. (1 993) examined fecal samplesfrom two groups of non-vegetarians and twogroups of vegetarians over a 12-month period.
8
7
6.0
3
2
11 6 11 16 21 26 31 36
Time (days)
SOURCE: Corpet, 1993
There were no differences in the prevalence ofantibiotic-resistant bacteria in the two groups,and there was a slightly increased frequency ofmultiply-resistant bacteria in the vegetarians.These results are consistent with the conclusionthat meat is not the only source of antibiotic-resistant bacteria, and the authors suggest thatrestrictions on antibiotic use in animals wouldhave little effect on antibiotic-resistant bacteriain humans. They do not show, however, thatmeat is unimportant as a source of antibiotic-resistant bacteria, nor do they pinpoint othersources of antibiotic-resistant bacteria in the diet.
Corpet (1993), who carried out the experimentsummarized in figure 7-1, concluded thathumans’ primary source of antibiotic-resistantbacteria is their food, which is consistent with theknowledge that food is a common source of bac-terial infections in humans. For instance, Murray(1995) concluded that more than half of Cam-pylobacter infections in humans arise fromingestion of contaminated poultry, and studies ofthe same organisms, in particular Campylobacterjejuni in Washington State, showed that antibi-otic resistance patterns were similar in infectedhumans and in poultry purchased from retailmarkets (U.S. House of Representatives, 1984).

Chapter 7 Antibiotics in Animal Husbandry | 161
It is important in this context that both antibiotic-sensitive and antibiotic-resistant C. jejuni causedhuman disease, underlining the importance ofother factors in whether or not ingested bacteriawill cause illness.
Virulent, antibiotic-resistant Salmonellacaused an outbreak of lethal diseases in cattle inEngland that infected as many as 500 humansand might have contributed to the deaths of 6individuals (Anderson, 1968). [The closing downof one farm which was in the business of buyingand reselling calves apparently stopped that epi-demic (Bywater, 1995).] Furthermore, there is nodoubt that farmers and others who are aroundand care for antibiotic-treated livestock canbecome carriers of bacteria with the same kindsof antibiotic-resistant bacteria as are found in theanimals (Levy, 1978, 1983, 1992 and Levy et al.,1976).
Antibiotic-resistant bacteria in food areingested by humans along with other bacteria,and antibiotic-resistant bacteria can be passedfrom animals to humans. Questions remain abouthow often these transmissions cause disease inhuman beings or promote the flow of geneticinformation for antibiotic resistance from bacte-ria of animal origin to bacteria that can causehuman disease.
❚ Antibiotic Residues in FoodFDA, in approving uses of an antibiotic in foodanimals, specifies a “withdrawal period” follow-ing the administration of the antibiotic to allowtime for the antibiotic “residue” concentration tofall to a level that is of no concern to the agency.When the withdrawal period is observed, and theresidue level falls appropriately, the concentra-tion of antibiotics in meat, according to FDA,should have no effect on the bacterial flora inhumans. Any meat that has a higher concentra-tion violates the law.
If, however, residue concentrations were highenough, they could have the same effect onhumans as ingesting antibiotics directly. Corpet(1993) summarizes a number of experiments thatindicate that the concentrations of antibiotics in
meats may rarely be sufficient to have an effecton human bacterial flora. He emphasizes, how-ever, that those effects are less important tohuman health than the ingestion of antibiotic-resistant bacteria.
A number of papers printed in two specialissues of journals about veterinary microbiologyreached similar conclusions: Veterinary andHuman Toxicology 35 (supplement 1), 1993, andVeterinary Microbiology 35 (no. 3,4), 1993.Kidd (1994), in a report prepared for the Fédéra-tion Européenne de la Santé Animale, comes to asimilar conclusion, but cautions that the lack ofevidence for any effect of antibiotics in meatmay reflect an absence of investigations of thepossibility. While there may remain some linger-ing suspicions that antibiotic residues in meatscan affect the micro-organisms in human beings,the remainder of this chapter will focus on therisks of antibiotic-resistant bacteria from foodthat was treated with antibiotics.
Antibiotics on Plants and VegetablesLevy (1992, p. 159–167) estimates that 40,000 to50,000 pounds of antibiotics are used on fruittrees in the United States each year. While thatamount is small in comparison to the 18 millionpounds of antibiotics used in animals, some of itis sprayed onto fruit trees and other crops,spreading it into the environment, and some of itcould be ingested by humans when they consumefruits and vegetables. Oxytetracycline and strep-tomycin are used to treat various “rots,” “molds,”and “spots” on fruits and vegetables, and some ofthe plant pathogens that cause those diseaseshave developed resistance to the antibiotics.Levy (1992, pp. 163–165) points to the possibil-ity that the bacteria that infect plants serve as areservoir for antibiotic-resistant genes that can betransferred to other bacteria that infect humans,but this possibility has not been researched.
Antibiotics in FishCommercial fish farming is a fast-growing enter-prise, and oxytetracycline, a sulfa drug, and aderivative of trimethoprim are used to control

162 | Impacts of Antibiotic-Resistant Bacteria
diseases. FDA requires that the antibiotics bewithdrawn from the fish for a specified numberof days before the fish are sold to reduce trans-mission of antibiotics to humans, but bacteria canbe carried along with the fish when they go tomarket.
Catfish, raised in ponds, are the primary com-mercially farmed fish in the United States. Troutare raised in enclosed raceways, and somesalmon are raised in ocean netpens in PugetSound, Washington, and off the Maine coast.
Farmed fish, when treated with antibiotics, arefed medicated feeds. Thus, antibiotics enter theenvironment either in fish feces or uneaten food.In catfish farming, antibiotics in feces or fooddrop to the bottom of the pond and are subject tobiological binding or degradation in the sedi-ment. When catfish ponds are drained, the sedi-ment is generally placed on the pond levee,restricting movement of the antibiotics into thegeneral environment.
These U.S. practices differ from those else-where. In Norway, antibiotics are sometimessprayed onto the surface of bodies of water andthe antibiotic can then spread throughout thewater and possibly cause disturbances in the eco-system. In that country, quinolones, as well asoxytetracycline, are used to treat diseases infarm-grown fish, and Ervik et al. (1994) showedthat detectable residues of antibiotics in the fleshof wild fish and mussels in sprayed water bodieswere more common than in fish and musselstaken from waters not known to be treated withantibiotics. The frequency of antibiotic-resistantbacteria in fish and mussels near the fish farmswas also higher, but the frequency of such bacte-ria was not zero, even in fish and mussels fromuntreated waters. This study demonstrates thatantibiotics can move through the aquatic envi-ronment and affect the flora of wild fish. Itsimplications for human health are unknown, andnot generally applicable to the United States. Inparticular, no quinolones are approved for use inaquaculture in the United States, and, accordingto the Animal Health Institute (1995), no suchuse is contemplated.
CONTROVERSY ABOUT ANTIBIOTIC USE IN RAISING LIVESTOCKThere is little controversy about the desirabilityof using antibiotics to treat sick animals. Morecontroversy arises about the subtherapeutic usesin prophylaxis and growth promotion, and thepossible diversion of antibiotics licensed only fortherapeutic purposes to other uses. Whatever thereason for the use of the antibiotic, treatment ofanimals can result in contamination of meat byantibiotic-resistant bacteria. Three things canhappen as a result. The first is that antibiotic-resistant pathogenic bacteria might be transferredto humans. The second is that antibiotic-resis-tance genes, although present in non-pathogenicbacteria in the animal, may be transferred topathogenic organisms in humans. The third isthat antibiotic-resistant bacteria that do not nor-mally infect humans will be ingested by peopleon antibiotic therapy, that the therapy will havealtered the human flora, and that the alterationwill favor the growth of bacteria that pose a riskto human health.
Any of these effects is a risk to human health.Why would anyone subject himself or herself,his or her family, and his or her customers to arisk? Clearly, if there were no apparent gain fromusing subtherapeutic doses of antibiotics in ani-mals, no one would do it. The manufacturers ofantibiotics gain, of course, because such usesincrease their sales. But farmers would not beexpected to buy the antibiotics if they did notprofit from them.
Discussions about subtherapeutic uses havebeen dominated by concerns about risks, but thefact that the uses continue and are sanctioned bythe federal government is convincing evidence ofthe received benefits. Whatever the risks may be,any decision about subtherapeutic uses willinvolve considerations of both risks and benefits,and continued focus on efforts to better pin downestimates of risks to the exclusion of benefitsmay have little effect on the decisions. In anycase, as can be seen from the earlier reviews ofthis issue, determining actual risk is not simple.

Chapter 7 Antibiotics in Animal Husbandry | 163
❚ How Well Do Subtherapeutic Doses Work?A measure of the success of subtherapeutic usesof antibiotics in increasing meat productionwould be provided by information about theamounts of antibiotics that meat producers buyover time. From the limited information avail-able it appears that success varies from animal toanimal and from time to time. As discussedbelow, a major chicken producer uses the samekinds and amounts of subtherapeutic antibioticsas were used years ago, and large-scale pork pro-ducers are reducing their use. In addition, small“niche” markets have been developed for meatsfrom drug-free animals, and some producers donot use antibiotics in order to participate in thesemarkets.
While OTA has not carried out any originalresearch or analysis on this issue, it appears thatanswers to the question of how well subtherapeu-tic antibiotics work to promote growth dependson the particulars of the application. Unsatisfyingas it may be, the answer appears to be, “Itdepends.”
Chickens—Constant Use and Constant BenefitsChickens are archetypal food animals (see box7-1). Because of selection for faster growingchickens and attention to animal husbandry,farmers can now produce a 6-pound chicken in56 days. Thirty years ago, a chicken of the sameage weighed two pounds.
Viral infections, against which antibioticshave no effect, are a far greater threat to chickensthan are bacterial infections, and they are con-trolled by hygiene, vaccination, and isolation ofchickens from possible human and animalsources of contamination (Dekich, 1994). A few“old” antibiotics, including tetracyclines, areavailable for treating bacterial infections, butsuch actions are uncommon. A large east coastproducer treated less than 2 percent of its 7,500flocks in 1994.
Two antibiotics—virginamycin and bamber-micin—are used to promote growth in chickens.
Neither is used in human medicine. The dose forgrowth promotion has remained constant at 1 to2 grams per ton of feed for 10 years, and theincreased growth rate has remained constant.According to a chicken-producing company, thecompany would discontinue growth promotionuse if it did not contribute to profits.
Pigs—Decreasing Use with Increasing Concentration of ProductionThe number of pork producers is decreasing andthe number of pigs sold by each producer isincreasing (National Pork Producers Council,1994), and antibiotic use appears to decreasewith increasing size of pork production opera-tions (Sundberg, 1994). The reasons for the trendare not well known, but better hygiene isbelieved to account for part of the decrease insubtherapeutic antibiotic use. More generally,larger operations mean that the producer’sincome is more dependent on pork production,rather than being drawn from several products,say, corn and pigs, and management probablybecomes more focused on the animals.
The National Pork Producers Council has pro-duced a Quality Assurance Program (NationalPork Producers Council, 1994) that includesguidelines for the use of all drugs, including anti-biotics. Those guidelines are intended to preventthe appearance of levels of drugs that exceed fed-eral limits in finished meat products. Accordingto the pork producers council, the percentage of
BOX 7–1: Chickens in the United States
The chicken—not the sparrow, pigeon, or star-ling—is the most common bird on the planet. TheUnited States produces 7 billion chickens annu-ally, or about 29 chickens for every one of the 240million Americans.
About 20,000 farm families contract with large
chicken producers and packers, and the averagefarm has two chicken houses. Each house pro-duces all of the chicken consumed by 15,000Americans annually. Production has doubledsince 1978, and increases 4 to 5 percent annually.

164 | Impacts of Antibiotic-Resistant Bacteria
violations for all drug residues in pork droppedfrom 10 percent in the mid-1980s to less than 1percent in 1994.
Trends in Some Other Sectors of Meat ProductionDuring the early 1980s, sales of tetracyclines andpenicillin for use in animal feeds slowly declinedfrom 2.9 million kilograms of tetracyclines in1980 to 2.4 million in 1985 and from 400,000kilograms of penicillin in 1980 to 300,000 in1984 (IOM, 1989, chap. IV). No more recentdata are readily available.
Levy (1992, p. 142) states that tetracyclineswere added to animal feeds for growth promo-tion at levels of 5 to 10 parts per million in the1950s (roughly 5 to 10 grams of antibiotic perton of feed). Currently, concentrations of 50 to200 parts per million are commonly used. Thehigher rates of use have not substantiallyincreased production costs because the cost ofantibiotics on a weight basis has decreased overthe same period. Because of the slim profit mar-gin in meat production, decreased growth promo-tion effects, coupled with increased costs, couldlead to a reduction in subtherapeutic uses of anti-biotics as the costs of the drugs approach orexceed the benefits from faster growth.
❚ Summary of Comments on Subtherapeutic Uses of AntibioticsLevy (1992, p. 156) suggests that several factorsare reducing the agricultural uses of antibiotics:increased concerns about drugs of all kinds infood; greater appreciation of the threat of antibi-otic-resistant bacteria and the contribution thatagricultural use of antibiotics may make to it;better animal husbandry that reduces the need forantibiotics; and legislative and regulatory initia-tives. Indeed, FDA experts report that they seefew applications for the subtherapeutic uses ofnew antibiotics (FDA, 1995). While Levy’simpressions may be accurate, and decreases insuch uses were reported over a decade ago, thephasing out of subtherapeutic uses would not
necessarily end the controversy about antibioticuse in animals.
CONTROVERSY OVER FLUOROQUINO-LONES IN FOOD PRODUCTIONJust as physicians need new antibiotics to treathuman diseases, veterinarians see needs for theuse of new antibiotics in their practices. FDA hasapproved the use of one fluoroquinolone in thetreatment of diseases in companion animals, andseveral manufacturers have requested approvalsfor the use of fluoroquinolones in the treatmentof diseases in food animals. Fluoroquinolone usein animals has been more widespread in Europe,and resistance to the drugs has been reported inbacteria isolated from treated animals.
Because of the importance of fluoroquinolo-nes in medicine, the American Society forMicrobiology, the Infectious Diseases Society ofAmerica, and officials of the Centers for DiseaseControl and Prevention have advised FDA torestrict the use of fluoroquinolones in foodanimals. In particular, the Infectious DiseasesSociety requested that no formulations of fluoro-quinolones in animal feeds be allowed. Thatrequest, if honored, would allow veterinarians totreat individual animals, but prevent treatment ofherds or flocks. It is opposed by some veterinari-ans who maintain that using the antibiotic in feedis necessary to treat animals.
FDA has received no applications for thelong-term use of fluoroquinolones in agricultureand does not expect to (FDA Veterinarian,1994), but it held public hearings in May 1994on possible therapeutic uses. At that meetingFDA announced that it was considering a newpolicy that would restrict approval of new antibi-otics to prescription uses in disease treatment andprevention. The consensus of the advisory panelconvened for that study was that the benefits ofrestricted short-term therapeutic use of fluoro-quinolones in food animals outweighed thepotential human health risk due to resistantorganisms, but that strict controls on usage andimproved surveillance were warranted (FDA1995a).

Chapter 7 Antibiotics in Animal Husbandry | 165
As therapeutic agents, fluoroquinolones couldbe used to prevent disease in herds or flocks thatare known to contain infected animals. Such pre-ventive use requires formulations of antibioticsthat can be incorporated into water or feed, lead-ing to concern that those formulations will findwidespread use in growth promotion, exertingheavy selection pressure for the emergence offluoroquinolone-resistant bacteria. There is a his-torical base for this concern. Chloramphenicol(CAP) was licensed for therapeutic use in live-stock but never for subtherapeutic uses. Never-theless, veterinarian and husbandry expertspublished articles that gave details about the useof CAP for growth promotion. As sales soaredfor such unapproved use, FDA intervened andbanned the marketing of oral solutions of CAPthat were convenient for treating farm animals.Unlike most antibiotics, CAP causes severe ane-mias and other diseases of the blood in somehumans, increasing concern that any residualCAP in meat might directly harm humans.
At the May 1994 meeting, FDA consideredopinions from private organizations and profes-sional societies and other federal agencies thatranged from urging that the fluoroquinolones becompletely restricted from agricultural use toarguments that they were necessary for the careof animals and that the risk of resistance fromagricultural use paled beside the risk from medi-cal uses. Currently (July 1995) FDA is preparingits policy statement for agricultural uses of fluo-roquinolones.
In November 1994, FDA held another meet-ing about the possible use of surveillance sys-tems to keep track of the emergence ofantibiotic-resistant bacteria, including the emer-gence of fluoroquinolone-resistant bacteria inanimals if agricultural uses of those drugs arepermitted. FDA is also drafting a statement onsurveillance that will consider the questionsraised by antibiotic resistance.
REFERENCESAnderson, E.S. 1968. The ecology of transfer-
able drug resistance in the enterobacteria.Annual Review of Microbiology 22:131.
Animal Health Institute. 1995. Personal commu-nication; letter comments on earlier draft ofthis report. 30 May.
Bates, J., J.Z. Jordens, and D.T. Griffiths. 1994.Farm animals as a putative reservoir for van-comycin-resistant enterococcal infection inman. Journal of Antibiotics and Chemother-apy 34:507–516.
Bywater, R.J., SmithKline Beecham AnimalHealth, Surrey, United Kingdom. 1995. Per-sonal communication; telephone conversa-tion with M. Gough, OTA. April 20.
Corpet, D.E. 1993. An evaluation of methods toassess the effect of antimicrobial residues onthe human gut flora. Veterinary Microbiol-ogy 35:199–212.
Dekich, M., Purdue Farms, Salisbury, Maryland.1994. Remarks at U.S. Food and DrugAdministration “Part 15 Hearing: Surveil-lance Systems for Antibacterial Resis-tance.” Rockville Civic Center, Rockville,MD. November 9.
Elder, H.A., I. Roy, S. Lehman, et al. 1993.Human studies to measure the effect of anti-biotic residues. Veterinary and Human Toxi-cology 35 (Supplement 1):31–36.
Ervik, A., B. Thorsen, V. Eriksen, et al. 1994.Impact of administering antibacterial agentson wild fish and blue mussels Mytilus edulisin the vicinity of fish farms. Diseases ofAquatic Organisms 18:45–51.
Feinman, S.E. and J.C. Matheson. 1978. DraftEnvironmental Impact Statement. Subthera-peutic Antibacterial Agents in Animal Feeds.U.S. Food and Drug Administration: Rock-ville, MD.
FDA Veterinarian. 1994. Advisory committeesdiscuss fluoroquinolones. July/Augustissue, pp. 2–5.
Gorbach, S.L. 1993. Perturbation of intestinalmicroflora. Veterinary and Human Toxicol-ogy 35 (Supplement 1):15–23.
166 | Impacts of Antibiotic-Resistant Bacteria
Hays, V.W. and C.A. Black. 1989. Antibiotics forAnimals: The Antibiotic Resistance Issue.Comments from CAST: 1989-92. Council forAgricultural Science and Technology:Ames, IA.
Institute of Medicine. 1989. Human Health Riskswith the Subtherapeutic Use of Penicillin orTetracyclines in Animal Feed. NationalAcademy Press: Washington, DC.
Kidd, A.R.M. 1994. The Potential Risk of Effectsof Antimicrobial Residues on HumanGastro-intestinal Microflora. FédérationEuropéenne de la Santé Animale: Brussels,Belgium.
Klare, I., H. Heier, H. Claus, R. Reissbrodt, andW. Witte. 1995. vanA mediated high levelglycopeptide resistance in Streptococcusfaecium from animal husbandry. FEMSMicrobiology Letters 125:165–172.
Levy, S.B. 1978. Emergence of antibiotic-resis-tant bacteria in the intestinal flora of farminhabitants. Journal of Infectious Diseases137:688–690.
Levy, S.B. 1983. Antibiotic-resistant bacteria infood of man and animals. In Woodbine, M.(ed.) Antimicrobials and Agriculture. Butter-worth: London, pp. 43–61.
Levy, S.B. 1992. The Antibiotic Paradox. Ple-num Press: New York.
Levy, S.B., G.G. Fitzgerald, and A.B. Macone.1976. Changes in intestinal flora of farmpersonnel after introductions of tetracy-clines-supplemented feed on a farm. NewEngland Journal of Medicine 295:583–588.
Murray, B.E. 1995. Editorial response: What canwe do about vancomycin-resistant entero-cocci? Clinical Infectious Diseases20:1134–1136.
National Pork Producers Council. 1994. PorkFacts. National Pork Producers Council:Des Moines, IA.
National Research Council. 1980. The Effects onHuman Health of Subtherapeutic Use ofAntimicrobials in Animal Feeds. NationalAcademy Press: Washington, DC.
Stallones, R.A. 1982. Epidemiology and publicpolicy: Pro- and anti-biotic. American Jour-nal of Epidemiology 115:485–491.
Sundberg, P., National Pork Producers Council,Des Moines, IA. 1994. Remarks at U.S.Food and Drug Administration “Part 15Hearing: Surveillance Systems for Antibac-terial Resistance.” Rockville Civic Center,Rockville, MD. November 9.
Teske, R.H., Center for Veterinary Medicine,U.S. Food and Drug Administration. 1995.Personal communication. Telephone conver-sation with M. Gough, OTA. April 21.
U.S. Congress, Office of Technology Assess-ment. 1979. Drugs in Livestock Feed. Wash-ington, DC: U.S. Government PrintingOffice. [OTA-F-91.]
U.S. Food and Drug Administration. 1995. Com-ments on earlier draft of this OTA report.Memorandum from Lois Adams, U.S. Foodand Drug Administration, to M. Gough,OTA. April 10.
U.S. Food and Drug Administration. 1995a.Comments on second draft of this OTAreport. Memorandum from Associate Com-missioner for Legislative Affairs, U.S. Foodand Drug Administration to Office of Tech-nology Assessment. June 16.
U.S. House of Representatives, Committee onScience and Technology, Subcommittee onInvestigations and Oversight. 1984. Hearing:Contract with Seattle. U.S. GovernmentPrinting Office: Washington, DC.
Walker, R., Michigan State University. 1994.Remarks at Food and Drug Administration“Part 15 Hearing: Surveillance Systems forAntibacterial Resistance.” Rockville CivicCenter, Rockville, MD. November 10.
| 167
A
Appendix A:Coverage of Antibiotic
Resistance in thePopular Literature,
1950 to 1994
he substance and tone of articles aboutantibiotic resistance in the popular litera-ture have changed over time (Rosen-krantz, 1995).1 In the 1950s sobering
cautions about the dangers of antibiotic overuseaccompanied announcements from medical andscientific experts celebrating reduced mortalityfrom specific diseases. The articles were recastby the mid 1980s. The public was faced withnew warnings that bacteria are “winning therace” because they are “smarter” than men.These conclusions are illuminated through thedecade-by-decade analysis that follows.
❚ 1950 to 1959In the late 1940s and early 1950s scientific andpopular periodicals were generally enthusiasticabout the benefits that antibiotics would providefor human health and well-being through bettermedicine, agriculture, and even home gardening.Public interest can partly be gauged by the rangeof journals and articles. The Saturday EveningPost, as well as Science, published articles onstreptomycin and tuberculosis; Reader’s Digest
1 Rosenkrantz, B.G. 1995. Historical Review: Responses to Antibiotic Resistance. Contract Report to the Office of Technology Assess-ment. Photocopied transcript.
(June 1955) excerpted an article, “Bringing theAntibiotics Up To Date,” by Paul DeKruif, apopular science writer and author of TheMicrobe Hunters. But there were also manywarnings against false confidence in the continu-ing usefulness of antibiotics.
Literature is this decade included feature arti-cles about the problems of resistance. The NewYork Times (May 2, 1953) quoted Sir AlexanderFleming, who discounted reports that germs werebecoming penicillin resistant and suggested thatindiscriminate use led to patient sensitivity.Howard Florey, the English scientist who devel-oped methods for producing penicillin, wasquoted in Newsweek (Oct. 20, 1958) explainingthat Staphylococcus aureus itself is not resistant;only certain strains that develop in hospitals pro-duce an enzyme called penicillinase that destroyspenicillin.
A reporter covering a U.S. Public Health Ser-vice conference on hospital infections wrote that“ . . . every week in the year at least one hospitalin the cleanest country on earth is threatenedwith an outbreak of serious ‘staph’ infections”(Newsweek, Sept. 29, 1958). In the same year,
T

168 | Impacts of Antibiotic-Resistant Bacteria
the U.S. Surgeon General announced that over-reliance on antibiotics had led to inroads by the“golden staph” [Staph. aureus]. The publiclearned that these germs could be found every-where. The recommended response for controlwas hospital hygiene and asepsis, not more anti-biotics (Time, Mar. 24, 1958).
The popular press pondered the cause of thisgrowing problem. Was it the unjustified or unsci-entific use of antibiotics, or were medical practi-tioners taking a “shotgun” approach to therapy?An unnamed surgeon reflected that in his fieldpenicillin was used casually, “like water.” Anarticle in Science News Letter (1953) was titled“Fear Man-made Epidemics.” Scientists werecited explaining that antibiotics should not beused prophylactically in attempts to ward offinfection.
At the same time, scientists informed the pub-lic about research on the causes of bacterial resis-tance. Time (Mar. 24, 1958; Nov. 17, 1958)reported that microbiologists were divided aboutwhether Staphylococcus develops resistance toantibiotics or whether antibiotics eliminate sus-ceptible Staphylococci, leaving behind the mostvirulent strains. Although antibiotics might havefalsely raised expectations, by the end of thedecade most of the popular press did not questionthe authority of scientists or the capability of sci-ence and medicine to continue to make progressin fighting disease.
❚ 1960 to 1969During the 1960s new questions surfaced aboutthe responsibility of government in ensuring thesafety and efficacy of pharmaceuticals, andincreasing concern about the dangers of bacterialresistance furthered public interest in the devel-opment of new antibiotics. In this decade theU.S. Food and Drug Administration (FDA)became more visible to the public; first throughSenator Estes Kefauver’s hearings on the drugindustry, but even more so when the tragedy ofthalidomide was narrowly averted in the UnitedStates.
For the more informed reader, Science(May 26, 1967) explained how “R factors” (nowcalled plasmids) mediated resistance, and News-week (Aug. 22, 1966) introduced scientific lan-guage to explain that “resistant bacteria can passtheir R factors along to bacteria of other strains,”emphasizing the specific dangers posed bymutant Escherichia coli from cattle fed antibi-otic-laced feed. Perhaps to appear evenhanded,the same article implied that an editorial in theNew England Journal of Medicine warning aboutthe dangers of indiscriminate antibiotic usemight be overdramatic. Good Housekeeping(August 1961; January 1964) warned that antibi-otics were never to be used casually for minorailments. In the early 1960s, the New York Timespublished reports of a steady increase in antibi-otic-resistant hospital infections (Mar. 12, 1961;Feb. 25, 1962; Sept. 28, 1962).
Despite the introduction of new antibiotics,and the promise of more yet to be identified, thepopular press cautioned that specific criteriashould be used to determine which drugs areeffective in treating each disease. The scienceeditor and editorial board of the New York Times(Sept. 9, 12, 14, 1966; Nov. 21, 23, 1969) pro-duced a series on the transmission of antibioticresistance among bacteria. Resistance wasdescribed as a widespread peril that could bespread by “mating” among different bacteria.
In 1967 the New York Times reported that, incomparison to Great Britain, the United Stateswas slow to control use of antibiotics in agricul-ture, a lapse that could exacerbate resistance(New York Times, June 11, 1967). Newspaperscovered the tensions in the debate among inter-ested parties, including: recommendations gener-ated by FDA and the National Research Councilof the National Academy of Sciences regardinglimiting antibiotics in animal feed; skepticismregistered by pharmaceutical firms about the sig-nificance of antibiotic resistance; and warningsby the meat industry about potential priceincreases should antibiotic protection of herds beprohibited (New York Times, Sept. 22, 1966;June 11, 1967).

Appendix A: Coverage of Antibiotic Resistance in the Popular Literature, 1950 to 1994 | 169
❚ 1970 to 1979In the 1970s the periodical press turned sympa-thetically to physicians for their perspectives onthe conflicting benefits and dangers of antibiot-ics. McCalls’ (October 1976) regular physiciancolumnist Dr. William Nolen authored “Antibi-otics: What They Will and Won’t Cure,” andfocused on the therapeutic limitations of antibiot-ics, but he did not raise the complications of anti-biotic resistance. Other periodicals focused onthe fundamentals of bacterial genetics. News-week (June 19, 1978), in its regular coverage ofmedical news, directed attention to hospital“mini-epidemics” and the new medical specialty,infection control, that brought doctors, nurses,technicians and epidemiologists to the scene.Attention to antibiotic resistance was also morefrequent in articles on agriculture, and in thesereports both pharmaceutical and agriculturalinterests were identified as enemies of regula-tion.
Accounts of bacterial resistance available tothe general reader varied, sometimes framed indramatic language that emphasized the emer-gence of “super bugs” like the “Andromedastrain,” and at other times presenting detailedreports of scientific meetings (New York Times,Oct. 15, 18, 1970; Feb. 6, 1972; Mar. 3, 1975).Concerns about the consequences of indiscrimi-nate use of antibiotics were reflected in a SenateHealth Subcommittee finding “that drug compa-nies over-promote antibiotics to physicians andphysicians overprescribe them, especially forcolds and other viral infections that antibioticscan’t counter” (Science News, May 27, 1972).Information on the basic mechanics of “Trans-missible Multiple Drug Resistance” (Science,May 19, 1972) became increasingly sophisti-cated in Science, Scientific American, and Sci-ence News. Good Housekeeping (March 1975)reported that the American Medical Associationhad discovered that resistant organisms, oncelargely confined to hospitals, were now alsofound in the community.
Reflecting a general frustration, the New YorkTimes (July 16, 1971) reported on a 25-year sur-
vey of health care that found despite “spectacularscientific advances. . .many diseases that shouldno longer exist, such as TB, still do.” Data fromthe CDC reported pneumonia and gonorrhearesistance to antibiotics. A CDC research teamestimated that 22 percent of antibiotic use in thehospital was unnecessary and led to “superinfec-tion” (New York Times, Jan. 28, 1976; Nov. 10,1976).
The FDA proposed policies (congruent withBritain and other European countries) to limitantibiotics in animal feed and reported that ani-mals consumed more than 40 percent of the anti-biotics produced. In a replay of an article that hadappeared in the late 1960s, Time (Sept. 10, 1979)reported that the FDA-proposed limits wereopposed “by a coalition of pharmaceutical manu-facturers and farming interests.” Congress agreed“to stay any action pending further studies.”
❚ 1980 to 1994Reports of emergent and re-emergent diseaseshave often implicated antibiotic resistance.Tuberculosis, once slated for virtual eradicationin the United States by the early 21st century,proved impossible to eliminate, and its persis-tence was linked to premature budget cuts in thenation’s public health efforts. But the blame forthe re-emergence of tuberculosis was spreadbroadly. New cases of tuberculosis were oftenassociated with homeless populations or withimmigrants from areas of the world where thedisease was endemic (New York Times, July 26,1980, June 18, 1985); reportedly, attempts tocontrol tuberculosis were exacerbated bypatients’ failure to comply with extended treat-ment, which could lead to multi-drug-resistantdisease.
In the 1980s epidemiologic and comparativeinternational perspectives on antibiotic resistancebecame prominent for the first time. In 1981 doc-tors in medical teaching centers called for inter-national controls “to halt ‘indiscriminate’ use ofantibiotics” (New York Times, Aug. 6, 1981).Broader concern was reflected in reports fromprominent spokespersons for the international

170 | Impacts of Antibiotic-Resistant Bacteria
scientific and medical communities, as well as inreports of the dangers to Americans from multi-ple-drug-resistant organisms imported as a resultof increased world travel, and via immigrants(often illegal) from developing countries.
Some diseases once treated by antibioticswere reportedly now out of control. CDC reportson the rise of antibiotic-resistant gonorrhea,streptococci, and hemophilus infections broughtthe danger closer to home when they were con-nected to children’s ear infections and to theoverwhelming (not antibiotic-resistant) infectionthat killed the Muppets creator, Jim Henson(New York Times, Feb. 23, 1989; May 8, 18,1990; Jan. 28, 1992). The emphasis and tone ofreporting on antibiotic-resistant bacteria shifted,markedly influenced by accounts of how infec-tious disease strikes back in the war between pes-tilence and people (Time, Sept. 12, 1994).
Time reported that the rising tide of antibioticresistance affected “nearly every disease organ-ism known to medicine”; the “microbe’s extraor-dinary ability to adapt” was “a fact of life.” Themagazine reported that adaptation was “writteninto evolution,” but few anxieties were relievedby reassurances that microorganisms were only“trying to. . . survive and reproduce, just as weare” (Time, Sept. 12, 1994).
Readers of popular magazines were chal-lenged by articles such as “Are you overdosingon antibiotics?” (Redbook, December 1991).There was mounting tension between warningsof dangers from “the ghost of scourges from thepast” (U.S. News and World Report, Oct. 26,1992) and reports of FDA approvals of new anti-biotics. As in the 19th century, doctors cautionedthat “A Hospital is No Place for a Sick Person ToBe” (Discover, October 1985), and patientsfeared that “Hospitals May Be BreedingGrounds” (USA Today, February 1991), as evi-dence mounted that “Hospitals Can Make YouSick” (World Press Review, August 1988).
Scientists and physicians were quoted in des-perate moments as they drew dire conclusionsfor the future. A feature article, “The End ofAntibiotics,” quoted one physician’s explanationthat “microorganisms are winning” because
“they are so much older than we are . . . andwiser” (Newsweek, Mar. 28, 1994). With no newantibiotics ready for introduction and evidence ofthe existence of “smart bugs” that carry informa-tion in resistance genes, attention to misuse ofantibiotics in medicine and agriculture competedfor blame with human populations which werelikened to hothouses for breeding of germs.Some reports downplayed professional account-ability, shifting responsibility to social changesthat included the spread of AIDS, the rise inhomelessness, the proliferation of child care cen-ters, the influx of immigrants, increases in inter-national travel, and the disturbance ofecosystems in both economic development andrecreation (U.S. News and World Report, Oct.26, 1992).
A change of tone and target appeared in the1980s. Partly as a consequence of lessons inimmunology that accompanied publicity onAIDS, but also because bacterial genetics hadbecome a growth industry, reports of new evi-dence on antibiotic resistance used adaptations ofeveryday language and diagrams to explain resis-tance genes to the public. Bacteria acquired iden-tities of their own. They were pictured orperceived as willful beings governing their ownmutations and transferring resistance genes toother bacteria in conscious efforts to outwithumans and their antibiotics. Journalists quotedscientists describing “bugs” with a crafty intelli-gence capable of becoming relentless demons.
❚ Comments on the Popular LiteraturePenicillin marked the beginning of a new era formost Americans and a majority of people aroundthe world. However, from its very beginning thetriumph of antibiotics was accompanied by fearthat resistance might reverse the advantagesgained over infections. Anxiety was expressed asconcern that ordinary germs would take revenge,that miracle drugs were a two-edged sword,eliminating some bacteria and favoring others.
Over time the early warnings transformed intoforecasts of apocalypse. Penicillin had not ban-ished hospital infections as had once been

Appendix A: Coverage of Antibiotic Resistance in the Popular Literature, 1950 to 1994 | 171
dreamed; instead, first “staph” and then otherorganisms became resistant. Unexpected diseaseand death spread among patients despite theefforts of infectious disease experts. Scientistsdiscovered that bacterial resistance to antibioticswas transmitted among disease-bearing organ-isms in ways that were unimaginable before theavailability of the tools of molecular biology.Scientists collaborated with journalists to instructthe public in the new language of resistancegenes, and the American public read about unex-pected outbreaks of untreatable mysterious infec-tions in the 1960s and 1970s. But the 1980sappeared more dangerous yet. AIDS laid thegroundwork for new fears, and fatal multiple-drug-resistant tuberculosis and streptococcalpneumonia put medical news and the terms“emergent” and “re-emergent” disease on thefront page of newspapers and on bestseller lists.
According to Rosenkrantz (1995), the emer-gence or control of antibiotic resistance wasposed first as a contest between knowledge andignorance, then between control and irresponsi-bility, and ultimately between good and evil. The1990s saw the stream of scientific and medicalinformation merge with fears about social disor-der and political corruption. The bearers of thenew threat were often immigrants from Asia,Africa, and South America, where AIDS, tuber-culosis, and other infectious diseases were preva-lent and where antibiotics were unavailable orimproperly used. The homeless, who failed tocomply with treatment plans, were blamed forthe spread of antibiotic-resistant tuberculosis.
Child-care centers and hospitals were singled outas places that spawn antibiotic resistance. Butblame was not restricted to the powerless. Phar-maceutical firms and agribusiness were alsoincriminated on the basis of alleged irresponsi-bility and greed. Attributing the spread of antibi-otic resistance to victims of disease as well as torepresentatives of corporate power accentuatedpublic anxiety and seemingly placed control out-side the realm of science. Meanwhile, it appearsthat fear of antibiotic-resistant disease has noteroded public demand for antibiotics. The plac-ing of blame on the most vulnerable and the mostpowerful may have compromised the impetus forcontrolling patients’ inappropriate requests forantibiotic prophylaxis and therapy.
The problems with antibiotic-resistant bacteriaare not new to this decade or even to this genera-tion. Such bacteria were identified soon after thefirst use of antibiotics, and the technical and pop-ular press has reported on them and the problemswith which they are associated. Over the last50 years, warnings have been voiced about inap-propriate antibiotic use—too frequentlydemanded by patients, too heavily prescribed byphysicians, too heavily used in agriculture, andtoo often used when they have no effect. Thevariety of possible explanations for the emer-gence of this public health problem highlightsthe complexity of the issues and also provides anumber of approaches to control the problem,which are discussed elsewhere in this OTAreport.
| 173
BAppendix B:
Glossary
Active Efflux: a major mechanism of bacterialresistance in which an antibiotic is pumpedout of the bacterial cell.
Active Immunization: the process of adminis-tering specific microbial antigens that stimu-late the host’s immune system to produceprotective antibodies, “vaccination.”
Agar Dilution Test: one of four diagnosticmethods currently used to determine theantibiotic susceptibility or resistance of bac-teria. See also agar gradient test, broth dilu-tion test, and disk diffusion test.
Agar Gradient Test: one of four diagnosticmethods currently used to determine theantibiotic susceptibility or resistance of bac-teria. See also agar dilution test, broth dilu-tion test, and disk diffusion test.
Aminoglycosides: a family of bactericidal anti-biotics that block bacterial protein synthesisby binding to the small subunit of the bacte-rial ribosome; examples are streptomycin,kanamycin, neomycin, gentamicin, amika-cin, and tobramycin.
Amoxicillin: a broad-spectrum β-lactam antibi-otic drug.
Antibacterial: a drug that kills or inhibits thegrowth of bacteria.
Antibiogram: a guide produced by a microbiol-ogy laboratory for physicians’ use that pro-files the susceptibility of commonlyencountered bacteria to various antibiotics.
Antibiotics: a class of substances that can kill orinhibit the growth of some groups of micro-organisms. Used in this report to refer tochemicals active against bacteria. Examplesare penicillin, tetracycline, erythromycin,and cephalosporins. Originally antibioticswere derived from natural sources, e.g., pen-icillin from molds, but many currently usedantibiotics are semi-synthetic and modifiedwith additions of man-made chemical com-ponents. See antimicrobials.
Antibiotic Resistance: a property of bacteriathat confers the capacity to inactivate orexclude antibiotics or a mechanism thatblocks the inhibitory or killing effects ofantibiotics.
Antibiotic Susceptibility: the opposite of resis-tance and applies to bacteria that are killedor inhibited by an antibiotic. Susceptibilityto a particular antibiotic does not mean thatthe bacteria are susceptible to all antibiotics.
Antigen: a chemical structure on or in a cell thatis recognized by the immune system. The
174 | Impacts of Antibiotic-Resistant Bacteria
immune system produces antibodies thatreact with the antigens.
Antigen Test: a diagnostic method for detectingthe presence of a specific chemical structure.As used here, it is a test for detecting thepresence of specific bacteria.
Antimicrobials: a class of substances that candestroy or inhibit the growth of bacteria;examples are sulfonamides. See antibiotics.
Anti-Sense: DNA is a helical molecule with twostrands. One strand, the “sense” strand, isused in the synthesis of RNA and protein;the other strand, the “anti-sense” strand,serves a structural purpose in DNA but notin RNA synthesis.
Anti-Sense Oligonucleotide: a length of theanti-sense strand of DNA prepared to bindspecifically to a target stretch of DNA.
Bacteremia: a pathologic state characterized bythe presence of bacteria in the blood.
Bacteria: microscopic, single-celled organismsthat have some biochemical and structuralfeatures different from animal and plantcells.
Bactericidal: a term for agents that kill bacteria.Bacteriophage: see phage.Bacteriostatic: a term for agents that inhibit bac-
terial growth.Beta-Lactam Antibiotics: the most widely used
class of antibiotics which includes penicil-lins, cephalosporins including ceftriaxoneand ceftazidime, carbapenems, monobac-tams, and imipenem. β-lactam antibiotics actby inhibiting the synthesis of peptidogly-can—the major component of a bacterial cellwall.
Beta-Lactamase: an enzyme produced by somebacteria that degrades beta-lactam antibiot-ics. See penicillinase.
Breakpoint: a concentration of antibiotic thatmarks the division either between the resis-tant and intermediate response or betweenthe intermediate and susceptible responseusing antibiotic susceptibility tests.
Broad-Spectrum Antibiotic: an antibioticeffective against a large number of bacterialspecies; generally describes antibiotics
effective against both Gram-positive andGram-negative bacteria.
Broth: a sterile nutrient growth medium used togrow bacteria.
Broth Dilution Test: one of four diagnosticmethods currently used to determine theantibiotic susceptibility or resistance of bac-teria. See also agar dilution test, agar gradi-ent test, and disk diffusion test.
Broth Microdilution Test: a miniaturized ver-sion of the broth dilution test that uses a testplate with small-sized wells that hold a smallvolume (about 0.1 milliliters) of broth.
Cecropin: a peptide from the North Americansilk moth Hyalophora cecropia thatincreases bacterial permeability and cancause bacterial death.
Cell Culture: propagation of cells in a labora-tory environment.
Chromosome: used in this report to refer to thecircular DNA that contains the genes for thefunctioning of a bacterium.
Clinical Trial: used in this report to refer toresearch to establish the safety and efficacyof a drug such as an antibiotic.
Colonization: capacity of a bacterium to remainat a particular site and multiply there.
Commensals: bacteria that live on the skin, inbody orifices, or the intestines, and do notusually cause disease, and may be beneficialto the host organism.
Conjugation: the process by which DNA istransferred from one bacterium to anotherthat involves cell-to-cell contact.
Defensin: a peptide from mammalian cellsincluding epithelial cells lining the humansmall intestine that increases bacterial per-meability and can cause bacterial death.
Deletion Mutation: a mutation that results inloss of a length of DNA from the chromo-some.
Disk Diffusion Test: one of four diagnosticmethods currently used to determine theantibiotic susceptibility or resistance of bac-teria. See also agar dilution test, agar gradi-ent test, and broth dilution test.

Appendix B: Glossary | 175
DNA (deoxyribonucleic acid): the substance ofheredity; a nucleic acid that is found in thecell nucleus that carries the genetic informa-tion necessary for all cellular functions.
DNA Probe Assay: a new diagnostic method foridentifying the presence of bacteria by usingfragments of DNA or RNA (probes) thatbind to target bacterial or resistance geneDNA or RNA sequences.
Efficacy: used in this report to refer to the proba-bility of benefit to individuals in a definedpopulation from a medical technologyapplied for a given medical problem underdefined conditions of use.
Empiric Therapy: used in this report to describeantibiotic treatment based on signs andsymptoms of disease and in absence ofknowledge of the causative agent of infec-tion.
Enterococcus: bacteria normally found in theintestinal tract and genitourinary tract. Somestrains are pathogenic and a few are resistantto all available antibiotics, including vanco-mycin.
Enzymatic Test: a diagnostic method of testingfor antibiotic resistance that directly mea-sures the presence of an enzyme that confersresistance in a bacterium.
Escherichia coli: a commensal bacterium thatlives in the intestine, a workhorse of biotech-nology, and sometimes a cause of opportu-nistic infections.
Eukaryote: a cell or organism with membrane-bound, structurally discrete nuclei, and well-developed cell organelles. Eukaryotesinclude all plants, animals, and fungi. Com-pare prokaryote.
Expression: functioning of a gene, generallymeasured by the amount of gene product(usually a protein or nucleic acid) made bythe cell. See gene expression.
Flora: the populations of commensal bacterianormally present in the intestine, body ori-fices, and on the skin.
Fluorometer: an optical device more sensitivethan the human eye to detect the presence or
absence of growth of bacteria in microdilu-tion tubes. See broth microdilution test.
Formularies: a listing of approved drugs forvarious medical indications originally cre-ated as a cost-controlling measure, but usedmore recently to guide use of antibioticsbased on information about resistance pat-terns.
Fungus: member of a class of relatively primi-tive organisms; includes mushrooms, yeasts,rusts, molds, and smuts.
Gene: a unit of heredity; a segment of the DNAmolecule that carries the directions for thestructure of a given protein.
Gene Expression: activity of a gene measuredby the amount of gene product (usually aprotein or nucleic acid) made by the cell.
Genetic Recombination: the process by whichseparate lengths of DNA from differentsources are chemically joined to producenew genetic combinations.
Glycopeptides: compounds made up of aminoacids and sugars that may have antibacterialactivity; vancomycin and teichoplanin areglycopeptide antibiotics.
Gram’s Stain: a bacteriological stain used todetermine a major division between bacterialspecies; the reaction depends on the com-plexity of the cell wall. Bacteria that retainthe gram stain (blue) are Gram-positive; bac-teria that lose the gram stain but stain with acounterstain (red) are Gram-negative.
Haemophilus influenzae: a commensal bacte-rium commonly found in the upper respira-tory tract capable of causing infections suchas otitis media, sinusitis, conjunctivitis,bronchopneumonia and type b meningitis.
Immunosuppression: inhibition or suppressionof the normal immune response, as a resultof giving drugs to prevent transplant rejec-tion, of irradiation or chemotherapy, or ofsome infections as in AIDS.
Incidence: the frequency of new occurrences ofdisease within a defined time interval. Inci-dence rate is the number of new cases of aspecified disease divided by the number of
176 | Impacts of Antibiotic-Resistant Bacteria
people in a population over a specifiedperiod of time, usually one year.
Infection: successful colonization on a site ofthe body by a microorganism capable ofcausing damage to the body.
Insertion Mutation: a mutation that adds alength of DNA to an existing DNA mole-cule.
Integron: DNA segment that can carry multipleantibiotic resistance genes and that can insertin plasmid and chromosomal locations.
Intermediate Resistance: In some cases, resis-tance to an antibiotic emerges in incrementalsteps, so some bacteria have “intermediate”resistance and can survive and grow in lowconcentrations but not higher concentrationsof an antibiotic.
Invasive: of a bacterium, (1) capable of penetrat-ing the host’s defenses; (2) capable of enter-ing host cells or passing through mucosalsurfaces and spreading in the body.
In-vitro Tests: techniques that use cells, tissues,or explants grown in a nutritive mediumrather than using living animals or humansubjects.
In-vivo Expression Technology (IVET): tech-niques that identify bacterial genes that areexpressed only when the bacteria are in thehost.
Isolate: to establish a pure culture of a microor-ganism.
Lactoferrin: the second most abundant proteinin human milk; found to have antibacterialactivity.
Macrolides: a family of bacteriostatic antibioticsthat inhibit protein synthesis by binding tothe large subunit of the bacterial ribosome;include erythromycin, clindamycin, chlor-amphenicol (rarely used because of adverseside effects), and the new drugs clarithromy-cin and azithromycin.
Magainins: short peptides, taken from the skincells of frogs, that increase bacterial perme-ability by inserting into the bacterial cellmembrane that can lead to death of the bac-terial cells.
MDR-TB: multi-drug-resistant tuberculosis.
Methicillin-Resistant Staphylococcus aureus(MRSA): strictly speaking, a bacterial strainresistant to methicillin. In practice, MRSAsare generally resistant to many antibioticsand some are resistant to all but vancomycin.
Microorganism: minute, microscopic or submi-croscopic living organisms; includes bacte-ria, fungi, and protozoa. Viruses are oftenincluded in this category, but they are inca-pable of growth and reproduction outside ofhost cells, and some experts insist theyshould not be classified as organisms.
Minimum Inhibitory Concentration (MIC):the lowest concentration of antibiotic thatprevents growth of a bacterium.
MRSA: See methicillin-resistant Staphyloccusaureus.
Multiple Resistance or Multiple Drug Resis-tance: applies to bacteria that are resistant tomore than one antibiotic.
Mutation: a genetic change; can occur eitherrandomly or at an accelerated rate throughexposure to radiation or certain chemicals(mutagens); may lead to a change in thestructure of the protein coded by the mutatedgene.
Mycobacteria: bacteria that have cell wall struc-tures different from other bacteria. Myco-bacterium tuberculosis is the cause oftuberculosis.
Narrow-Spectrum Antibiotic: an antibioticeffective against a limited number of micro-organisms; often applied to an antibioticactive against either Gram-positive or Gram-negative bacteria.
Natural Selection: process by which ancestralspecies of animals and plants evolve intonew species.
Nosocomial Infection: infection acquired duringhospitalization that is neither present norincubating at the time of hospital admissionunless related to prior hospitalization andthat may become clinically manifest afterdischarge from the hospital.
Notifiable Disease: a disease that physicians arerequired to report to State health depart-ments.
Appendix B: Glossary | 177
Oligosaccharides: (“oligo,” a few; “saccha-rides,” sugars). Specific oligosaccharides arepresent on the surfaces of cells in differentorgans and tissues.
Opportunistic Infection: an infection caused byan organism that does not usually troublepeople, such as a commensal bacterium.
Oxacillin: a semi-synthetic penicillin similar tomethicillin.
Parasite: an organism living in or on an organ-ism of another species (its host), obtainingpart or all of its subsistence from it withoutrendering any service in return.
Pathogen: an organism that is capable of caus-ing disease.
Pathogenicity: capacity to cause disease.Penicillin: the first true antibiotic.Penicillinase: an enzyme which degrades peni-
cillin so that it has no effect on bacteria. Seebeta-lactamase.
Peptides: small protein molecules. Most of inter-est in this report are peptides from bacteriaand from human, frog, shark, rabbit, andmoth cells that have been shown to inhibitthe growth of or kill some bacteria bybreaking down their permeability barriers tothe entry of antibiotics. See magainins,cecropin, and defensin.
Peptidoglycan: a complex polymer of sugarsand amino acids that form the major compo-nent of the bacterial cell wall.
Phage: a virus that infects bacteria.Phage Therapy: the use of viruses that attack
bacteria to treat disease; an “old” and cur-rently unused therapy.
Plasmid: a circular piece of DNA not associatedwith the chromosome found in the cyto-plasm and capable of replicating and segre-gating independently. Many plasmids can bespread through bacterial populations by con-jugation, and many of the antibiotic-resis-tance genes of clinical significance arecarried by plasmids.
Point Mutation: a “single letter” mutation con-sisting of an alteration in a single nucleotidein DNA.
Polymerase Chain Reaction (PCR): a labora-tory procedure that produces millions ofcopies of DNA from one or a few molecules.
Preclinical Test: animal studies of drugs beforethey are tested in human beings.
Prevalence: refers to the total number of cases(new as well as previous cases) of a diseaseduring a designated time period.
Prokaryote: an organism lacking cell organellesand whose DNA is not enclosed within amembrane-bound, structurally discretenucleus. Bacteria and blue-green algae areprokaryotes. (Some experts consider “blue-green algae” to be better classified as “blue-green bacteria.”) Compare eukaryote.
Prophylactic Antibiotic Therapy: the adminis-tration of antibiotics before evidence ofinfection and intended to ward off disease.
Protozoa: single-celled animals with membrane-bound organelles.
Quinolones: a class of purely synthetic antibiot-ics that inhibit the replication of bacterialDNA; includes ciprofloxacin and fluoro-quinoline.
Resistance: see antibiotic resistance.Rifampin: an antibiotic that blocks transcription,
e.g. synthesis of RNA; its principal use is intreatment of tuberculosis.
Selective Pressure: used in this report to refer tothe selection of antibiotic-resistant bacteriathrough the use of antibiotics. Susceptiblebacteria are killed or inhibited, and resistantones are selected.
Self-Limiting: of an infection, one that proceedsto a point and no further.
Semi-Synthetic Antibiotics: antibiotics derivedin part from natural products produced by anorganism and in part from synthetic compo-nents. Examples are methicillin, nafcillinand cloxacillin.
Sepsis: a state characterized by the presence ofpathogenic microorganisms and their prod-ucts into the bloodstream.
Serum Therapy: the use of fractions of bloodfrom infected animals to treat human dis-ease; an “old” therapy with limited use. Cur-
178 | Impacts of Antibiotic-Resistant Bacteria
rently used for the treatment of tetanus andbotulism (and snakebites).
Service Laboratory: a commercial microbiol-ogy laboratory to which physicians sendclinical specimens for analysis.
Squalamine: a steroid compound, closelyrelated to cholesterol, with antibacterialactivity. Testing of squalamine is at the pre-clinical stage.
Staphylococcus aureus: Normally commensalbacteria on the skin that can cause nosoco-mial infections when they penetrate intobody tissues and organs as a result ofwounds and surgery. See MRSA.
Steroids: natural compounds; the best known ischolesterol. Some steroids isolated from var-ious organs of sharks have been shown tohave antibacterial characteristics.
Streptococcus pneumoniae or “Pneumococ-cus” bacteria: the most common cause ofbacterial infection in the United States.
Streptogramin: a new antibiotic, now in phaseIII clinical trials, effective against some anti-biotic-resistant bacteria, including somestrains of VRE.
Structure-Based Drug Design: a method ofantibiotic research that focuses on an under-standing of the ligand:receptor interactionthat occurs at the “active site” where the“ligand,” in this case the antibiotic, binds tosome structure, the “receptor” in the bacte-ria. Research tools such as X-ray crystallog-raphy, nuclear magnetic resonancespectroscopy, and supercomputer combina-torial chemistry are used to design new com-pounds that will bind more tightly to the“active site.”
Sulfa Drugs: a group of synthetic chemicals thatinhibit bacterial growth and metabolism. Seesulfonamide.
Sulfonamide: the first antibacterial drug thatwas not overly toxic to humans. It is a syn-thetic, antimicrobial (rather than antibiotic)drug.
Surveillance Systems: used in this report torefer to data collection and record keeping totrack the emergence and spread of disease-
causing organisms such as antibiotic-resis-tant bacteria.
Susceptibility Test: any of a large number oftests used to determine if bacteria are sus-ceptible or resistant to an antibiotic.
Systemic: pertaining to or affecting the body as awhole; frequently applied to bloodstreaminfections.
Target Amplification Method: methods toincrease the number of target DNAsequences through such methods as poly-merase chain reaction (PCR). See poly-merase chain reaction.
Tetracyclines: a family of broad-spectrum anti-biotics used in the therapy of infectionscaused by Gram-positive and Gram-negativebacteria.
Toxicity: the quality of being poisonous. Refer-ring to antibiotics, the degree to which theyproduce unwanted, adverse effects.
Transcription: synthesis of RNA from a DNAtemplate.
Transduction: transfer of bacterial genes fromone bacterium to another by a bacterial virus(called a phage).
Transformation: uptake by a bacterium of DNAfrom a ruptured cell and incorporation ofgenes from the DNA into the bacterial chro-mosome.
Transposons: small, mobile DNA sequencesthat can move around chromosomes andplasmids. Often they carry genes specifyingantibiotic resistance.
Treponema pallidum: bacteria that cause syphi-lis.
Trimethoprim: an antibiotic administered incombination with a sulfonamide in the treat-ment of urinary tract infections.
Vaccine: a preparation of living, attenuated, orkilled bacteria or viruses, fractions thereof,or synthesized antigens identical or similarto those found in the disease-causing organ-isms, that is administered to raise immunityto a particular microorganism.
Vancomycin: a widely used glycopeptide antibi-otic, particularly important for treatment ofinfections caused by strains of Staphylococ-

Appendix B: Glossary | 179
cus aureus some of which are resistant to allother antibiotics.
Vancomycin-Resistant Enterococcus (VRE): abacterial strain. Some VREs are resistant toall commercially available antibiotics.
Virulence: a measure of the degree and severityof pathogenicity of a disease-causing organ-ism.
Virus: submicroscopic pieces of genetic material(RNA or DNA) enclosed in a protein coatthat cause infectious disease. Viruses areobligate parasites that can reproduce only inliving cells.
Zone of Inhibition: area of no bacterial growtharound a disk containing antibiotic; used tomeasure the antibiotic susceptibility or resis-tance of bacteria. See disk diffusion test.
| 181
CAppendix C:
Acknowledgments
OTA wishes to thank the Impacts of Antibiotic-Resistant Bacteria advisory panel and the fol-lowing individuals and organizations for theircontributions of materials and advice to thisOTA report. In addition, several unnamed indi-viduals at the Food and Drug Administrationcontributed to the review of drafts of this report.
Lois AdamsFood and Drug Administration
Association of Practitioners of Infection Control and Epidemiology
Washington, DC
Karen BushLederle Laboratories
Jose Diaz BuxoMetrolina Nephrology Associates, P.A.
Marty CetronThe Centers for Disease Control and Prevention
Mitchell CohenThe Centers for Disease Control and Prevention
N. Cary EnglebergUniversity of Michigan Medical School
Victor EspositoMicrocarb, Inc.
Scott EvansLatter-Day Saints Hospital
Gerard FergersonNew York University
Robert GaynesThe Centers for Disease Control and Prevention
Donald GoldmanChildren’s Hospital, Boston
Gregory J. GoschBio-Rad Laboratories
John H. GriffinStanford University
Richard GustafsonLawrenceville, NJ
182 | Impacts of Antibiotic-Resistant Bacteria
George HabelFood and Drug Administration
Raymond M. HakimVanderbilt University Medical Center
David HooperMassachusetts General Hospital
Tom IsettBecton Dickinson Microbiology Systems
Daniel KacianGen-Probe Inc.
Gagan KamalUniversity of Iowa Hospital
Gordon KempAnimal Health Institute
Bruce KreterRhone-Poulenc Rorer
Elliot JacobsWalter Reed Army Medical Center
Richard LenskiUniversity of Michigan
Bruce R. LevinEmory University
Robert LinnabaryUniversity of Tennessee
William MaiseLederle Laboratories
Tom McDanielsWashington, DC
John E. McGowan, Jr.The Centers for Disease Control and Prevention
George MillerSchering-Plough Research Laboratory
National Pork Producers CouncilDes Moines, IA
Michael O’ConnellMiles Inc.
Brian O’MalleyU.S. House of Representatives
Sindy PaulNew Jersey Department of Health
Elaine PowerOffice of Technology Assessment
Issam RaadM.D. Anderson Cancer Center
Linda RayfordOffice of Technology Assessment
Eric RobinsonMcNeil Pharmaceutical
Susan RoseDepartment of Energy
Daniel SahmWashington University Medical Center
David R. ScottKaiser Permanente
Jean A. SetterstromWalter Reed Army Medical Center
Rodney SobinOffice of Technology Assessment
P. Frederick SparlingUniversity of North Carolina School of Medicine
Morton SwarzMassachusetts General Hospital
Robert V. TauxeThe Centers for Disease Control and Prevention
Appendix C: Acknowledgments | 183
Fred TenoverThe Centers for Disease Control and Prevention
Martin TerryAnimal Health Institute
Steve TeutschThe Centers for Disease Control and Prevention
Judith WagnerOffice of Technology Assessment
Robert A. WeinsteinCook County Hospital
Thomas WhiteRoche Molecular Systems
Maureen WirthMiddle Village, NY
Leah WolfeCleveland Heights, OH
Related Documents











