IMPACT OF THERAPEUTIC MILIEU AND UNIT AGGRESSION ON PROGRESSION TO DISCHARGE: CORRELATION OF EMERGENCY EVENTS WITH OUTCOMES FOR PSYCHIATRIC PEERS A Thesis Presented by Student A to The Faculty of the Graduate College of The University of Vermont In Partial Fulfillment of the Requirements for the Degree of Master of Science Specializing in Nursing January 2014

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

IMPACT OF THERAPEUTIC MILIEU AND UNIT AGGRESSION ON PROGRESSION TO DISCHARGE:
CORRELATION OF EMERGENCY EVENTS WITH OUTCOMES FOR PSYCHIATRIC PEERS
A Thesis Presented
by
Student A
to
The Faculty of the Graduate College
of
The University of Vermont
In Partial Fulfillment of the Requirements for the Degree of Master of Science
Specializing in Nursing
January 2014

2
Accepted by the Faculty of the Graduate College, The University of Vermont, in partial fulfillment of the requirements for the degree of Master of Science specializing in Nursing.
Thesis Examination Committee:
________________________________________AdvisorDr. Brenda Hamel-Bissell, Ed.D., PMHCNS
________________________________________Second MemberDr. Jean Coffey, Ph.D., CPNP
________________________________________Thesis DefenseDr. Peter Callas, Ph.D.
________________________________________Interim Dean, Graduate College Cynthia Forehand, Ph.D
September 30th, 2013
2

Abstract
Background: Inpatient psychiatric length-of-stay has decreased in the past 40 years. Previously valued as a therapeutic intervention, the concept of the milieu has been de-emphasized during this period. Studies associate perception of milieu with treatment outcome, but literature is scant on specific independent variables of milieu in psychiatric treatment outcome. Objective: This study investigated the number of emergency events as a proxy for aggression, control and disorder on a psychiatric milieu. These events were analyzed as an independent variable in psychiatric peer outcomes, the dependent variable. Outcomes were measured by length-of-stay, and global-assessment-of-function scores. Methods: This three-year, retrospective, cohort design used data from hospital electronic medical record databases to analyze the independent variables impact on dependent variable outcomes. The study evaluated data from two cohorts on one inpatient unit that experienced a change in patient population after a regional reduction in psychiatric beds, resulting in increased unit emergency events. Correlations, comparison of means, and regression analyses of the independent variables and dependent outcomes from the two cohorts provided data for discussion. Results: The total sample in the study included 778 unique hospital visits. After exclusion criteria were applied, 610 visits were analyzed. Statistical analysis identified significant differences between groups. The latter group was 9% younger (3.76 years), increased male by percentage (49.9% vs. 67.2%), had a patient population with an 11% increased diagnoses of psychosis, 3% increased diagnosis of mania, and a 12% decrease in diagnoses of depression. Additionally, those males who were depressed had 23% lower global-assessment-of-function scores on admission (-4.47 points). Mean number of emergency events experienced by patients in the latter group increased 619% (0.16 to 0.99 events per day). Male patients with psychosis had a 39% increase in length-of-stay (+5.82 days). Length-of-stay was not significantly different for other diagnostic codes. Regression analysis shows that emergency events on the unit were a significant predictor of the variance in length-of-stay for male patients with psychosis. Conclusion: Milieu variables have an impact on psychiatric hospitalizations. Data supports the conclusion that increased unit aggression increases length-of-stay for male patients with psychosis on this unit. Potentially, these findings could impact policy associated with duration of untreated psychosis, enhance education to providers about the differing responses to hospitalization by diagnosis, and affect milieu practices that support coping with hospitalization. This sample provided statistically significant results. Further research should be conducted with diverse inpatient settings to improve generalizability, and to increase statistical power in subgroup analysis.

Dedication
Bret, your support, love, and belief in me has made this journey possible.
Thank you.
4

Acknowledgments
I would like to express my gratitude and appreciation to my advisor, Dr. Brenda
Hamel-Bissell. Your patience, encouragement, and comments have been invaluable.
I would also like to thank my thesis committee member, Dr. Jean Coffey and
defense chair Dr. Peter Callas. Your feedback, guidance, and attention to detail have
helped this thesis have focus and supported conclusions.
Additionally, I wish to thank the Jeffords Institute for Quality and Operational
Effectiveness. Your support with data collection made this research possible.
Finally, I wish to acknowledge the support from my friends, classmates and
instructors. Your patience and support through numerous iterations of this project helped
me to stay focused, continue to work, and to complete this project.
5

Table of Contents
Dedication............................................................................................................................6
Acknowledgments................................................................................................................7
List of Tables........................................................................................................................9
List of Figures......................................................................................................................9
Chapter I.............................................................................................................................10
Theoretical Framework......................................................................................................10
Transactional Model of Stress and Coping....................................................................10
Rationale for Study............................................................................................................10
Hypothesis..........................................................................................................................11
Chapter II ..........................................................................................................................12
Literature Review...............................................................................................................12
Inpatient Patient Profile.................................................................................................12
Emergency Events.............................................................................................................12
Seclusion and Restraint..................................................................................................12
Emergency Events Medication Administration.............................................................12
Predicting Emergency Events........................................................................................13
Evaluation of Outcome of Hospitalization........................................................................13
Global Assessment of Functioning................................................................................13
Length of Stay................................................................................................................13
6

Patient Advocacy: Autonomy........................................................................................14
Nursing Theory: Therapeutic Milieu................................................................................14
Milieu in Context...........................................................................................................14
History............................................................................................................................14
Treatment Modality........................................................................................................15
Aggression on the Unit..................................................................................................15
Summary of Research Findings and Need for Study.........................................................16
.......................................................................................................................................16
Chapter III..........................................................................................................................17
Method...............................................................................................................................17
Study Design.................................................................................................................17
Definitions......................................................................................................................17
Setting............................................................................................................................17
Sample............................................................................................................................17
Data Collection..............................................................................................................17
Ethical Considerations...................................................................................................18
Data Analysis.....................................................................................................................18
Chapter IV ........................................................................................................................18
Results................................................................................................................................18
Data Collection and Sample Selection...........................................................................18
Reliability .....................................................................................................................19
Descriptive Statistics and Comparison of Means..........................................................19
7

Age and Gender.........................................................................................................19
Diagnostic Group ....................................................................................................19
Global Assessment of Function Scores......................................................................20
Length of Stay............................................................................................................20
Total Events per Admission.......................................................................................21
GAF Change per Day.................................................................................................21
Length of Stay per Years of Age................................................................................21
Total Events per Day of Admission...........................................................................21
Correlation and Regression Analysis.............................................................................21
Correlations................................................................................................................21
LOS Regression: Total Sample .................................................................................22
LOS Regression: Groups A and B ............................................................................22
LOS Regression: Diagnosis Code 1 Male Gender ....................................................22
GAF on Discharge Regression Model.......................................................................22
Regression Curve Estimation of Events Predicting LOS..........................................22
Chapter V: .........................................................................................................................22
Discussion..........................................................................................................................23
Milieu Characteristics ...................................................................................................23
Factors Associated with Patient Outcomes....................................................................23
Stress..............................................................................................................................23
Coping............................................................................................................................23
Emotional Reactivity and Psychosis..............................................................................24
Unit Events.....................................................................................................................24
8

Support in Stress Accommodation.................................................................................24
Unit Events Impact on Milieu and Social Support........................................................24
Suggested Explanations for Data Result............................................................................25
Stress Vulnerability........................................................................................................25
Decreased Coping Resources from Peers and Family...................................................25
Decreased Coping Support From Staff..........................................................................25
Implications for Practice....................................................................................................25
Ethical Considerations...............................................................................................25
Policy.........................................................................................................................26
Nursing Education.....................................................................................................26
Limitations.................................................................................................................26
Suggestions for Further Research......................................................................................28
Conclusion.........................................................................................................................28
Appendix T........................................................................................................................38
...........................................................................................................................................38
Appendix U........................................................................................................................39
References..........................................................................................................................40
9
List of Tables
List of Figures
10
Impact of Therapeutic Milieu and Unit Aggression on Progression to Discharge:
Correlation of Emergency Events with Outcomes for Psychiatric Peers
Chapter I
Psychiatric nursing theory postulates a therapeutic milieu as a treatment
intervention for hospitalized psychiatric patients (Peplau, 1989). Conceptualized as a
safe, holding environment for recovery, creation and management of the milieu is
principally a nursing role (Skinner, 1979; Tuck & Keels, 1992). The quality of the
inpatient milieu is subject to variation. Variables affecting milieu include patient
population, unit aggression, staffing, and physical environment (Melle et al.,1996). If
milieu therapy is an intervention that impacts the course of inpatient psychiatric
hospitalizations, then variations in therapeutic milieu would be able to be measured in
changes to patient outcomes.
Extensive nursing literature supports treatment milieu as a factor related to patient
satisfaction (Clarkin, Hurt, & Crilly, 1987; Kirshner & Johnston, 1982; Melle et al., 1996;
Middelboe, Schjødt, Byrsting, & Gjerris, 2008). Among the identified factors positively
associated with patient satisfaction is a highly ordered unit. Such units are predictable, a
“safe house, neutral territory, and a cooling place” (S. P. Thomas, Shattell, & Martin,
2002, p. 101), and facilitate peer relationships that reduce isolation. Negatively
associated with patient satisfaction are the findings that “high levels of aggression and
staff control (e. g. conflicts, use of coercive measures) generally should be avoided”
(Jörgensen, Römma, & Rundmo, 2009, p. 113; Melle et al., 1996).
11
Research completed during the 1980s correlates perceived ward atmosphere as a
variable in treatment outcome for schizophrenic patients (Clarkin et al., 1987). Data from
the 1990’s suggest that “patient’s perception of the ward atmosphere may influence the
rate of improvement from psychotic symptoms and thus may improve short-term
outcomes” (Melle et al., 1996, p. 725).
Additional research in the 1990s associates the impact of nursing therapeutic
alliance on overall improvement at time of discharge. An important measure of treatment
outcome in this research includes hospitalization Length of Stay (LOS) and Global
Assessment Score (GAS) an assessment of functioning (Clarkin et al., 1987; Melle et al.,
1996). There is, however, little current research that correlates therapeutic milieu on
treatment outcomes, LOS and patient improvement (Jörgensen et al., 2009).
Changes in health policy, improvements in medication, and impacts of funding
administrations have affected LOS (Tulloch, Fearon, & David, 2011). Mean LOS “has
fallen sharply over the last 30 years in the US” (Tulloch et al., 2011, p. 155).
Nevertheless, even with the recent reductions in LOS, inpatient services for psychiatric
illnesses represent 16% of US mental health expenditures (Tulloch et al., 2011).
For many patients, “psychiatric admissions may be experienced as stigmatizing
and unpleasant” (Tulloch et al., 2011, p. 155), suggesting that efforts to reduce LOS may
be of benefit. Additional research associating LOS and risk of readmission suggests that
increased LOS is not predictive of risk for readmission (Zhang, Harvey, & Andrew,
2011). Randomized studies associating short versus long hospitalizations show no
significant difference in risk for readmission (Tulloch et al., 2011) suggesting that there is
no inherent benefit in longer LOS. The social impact of cost, the lack of therapeutic
12

benefit, and the unpleasantness of hospitalization justify examination of variables that
may contribute to LOS.
While data do support the correlation of variables of therapeutic milieu, patient
satisfaction and patient outcome, just how this accomplished is argued. A possible
explanation hypothesizes that the ward atmosphere impacts the “attainment of positive
outcomes” (Jörgensen et al., 2009, p. 115). This explanation is suggestive that the milieu
provides the context for the ‘effective’ interventions (pharmacotherapy, for instance)
however, from this perspective, the milieu per-se, is not seen as a therapeutic
intervention.
Other theorists suggest that therapeutic milieu is an intervention in itself, arguing
that “the total environment is thought to have therapeutic potential” (LeCuyer, 1992, p.
108). Such theorists suggest the stress-adaptive components of milieu “containment,
support, structure, involvement, and validation” (Gunderson, 1978; Mahoney, Palyo,
Napier, & Giordano, 2009, p. 424) are essential interventions in the recovery from mental
illness (Jörgensen et al., 2009).
Theoretical Framework
Transactional Model of Stress and Coping
The evolution of psychiatric theory that attempts to explain the causes of mental
illness demonstrate that such diseases are multi-factorial. Biological explanations
occurred as far back as during the days of ancient Greece, and continue to be explored
today. Psychological explanations were first modeled as developmental and relational
13

with the psychodynamic theories of Sigmund Freud (Gay, 2006). Later theorists include
descriptions of maternal attachment, self-efficacy, social learning and other
environmental impacts as factors in mental health (Bandura, 1986; Bifulco, Moran, Ball,
& Bernazzani, 2002; Daniel, 2006).
Contemporary models suggest that a “Diathesis-Stress Model” appreciates a
dynamic that exists between social, psychological, environmental and biologic influences
in mental health (Tusaie & Fitzpatrick, 2013). For example, Hawton and Heerigan
modeled the interplay between psychiatric disorders, psychosocial stressors, hopeless,
and impulsivity to explore concepts related to suicidal behavior (Appendix B: Figure ).
This analysis both explains contributory factors, and identifies opportunities for
interventions to prevent suicidal behaviors (Hawton & van Heeringen, 2009).
In 1984 Richard Lazarus and Susan Folkman proposed a model of stress that
suggests that ones ability to cope with a stressor is a factor in the behavioral response to a
stressor (Lazarus & Folkman, 1984). This model, referred to as the Transactional Model
of Stress and Coping suggests that interventions that promote skill acquisition can
improve coping mechanisms. These interventions, then, positively impact “psychological
well-being and functional status”, states that are associated with “meaning-based
processes” (Glanz, Rimer, & Viswanath, 2008, p. 214). This model (Appendix C: Figure
3) suggests that there are mediating processes and moderating process that contribute to
stress outcomes.
Once an individual has appraised the stressor, and the stress has been moderated
by perception and effort, an outcome occurs. Outcomes can be thought of as representing
an individual’s utilization of skills and understandings to adapt to a change in
14
homeostasis. Such outcomes can impact physical health, psychological health, and social
functioning. As appraisal and moderation are not static assessments, outcomes in
response to stressful encounters vary. This variance could include changes in social
situation, health status, social support, and even include variables such as substance abuse
(Glanz et al., 2008).
Extensive published literature that use the Transactional Model as a theoretical
framework, provide evidence for the health promotion benefits of active coping versus
avoidance coping (Stanton, Revenson, & Tennen, 2007). This suggests that techniques
that facilitate acknowledgement and accommodation of a stressor produce better
outcomes than denial, emotional-based coping, or refusal to engage in adaptive
responses. Much of this discussion is focused on a particular situation. However, as
Glanz suggests, coping strategies “may depend on a person’s dispositional coping style
and perception of support in the environment” (Glanz et al., 2008, p. 219).
Psychiatric nurses can utilize the Transactional Model of Stress and Coping as a
framework to assess and intervene as a patient experiences stress in the milieu. In our
role as nurses, we can support a patient’s cognitive appraisal of a stressor, utilize stress
management techniques, and provide social and environmental support. These
interventions reduce the physiologic and psychological impact of stress. Additionally, by
coaching and supporting our patients as they negotiate stressful situations, we empower
them- promoting a sense of self-confidence, efficacy, and resilience (Psychiatric nursing,
2008). These interventions depend upon the unique therapeutic alliance formed between
nurse and patient. Such an alliance is interpersonal, requiring nursing characteristics
15

such as dependability, accountability, empathy, and therapeutic communication (Peplau,
1989; Townsend, 2011).
Rationale for Study
Research has identified the impact of emergency events on an individual, with
much of the literature finding little therapeutic benefit. (March & Caple, 2012).
However, there has been little research exploring the impact on psychiatric peers who
observe emergency events. As stated by other researchers, investigations into milieu
therapy require identification of milieu variables utilizing correlational designs (Vaglum,
Friis, & Karterud, 1985). This study attempted to research objective measures of
hospitalization outcomes to quantify the effect size of some milieu variables. Using
psychiatric emergency events in a study of outcomes of hospitalization could contribute
to the knowledge base that directs future nursing interventions in the milieu.
Recent events have impacted the percentage of pharmacologically untreated
patients on a small, non-urban, general hospital psychiatric unit. The change has
increased the percentage of patients on this unit that are at risk of harming themselves or
others. This mix has resulted in a milieu with more emergency medication events and
protective seclusions. This patient profile shift has provided a timely opportunity to
examine the impact of unit milieu on treatment outcome of psychiatric peers.
16

Hypothesis
Increased incidence of emergency events in psychiatric hospitals will be
predictive of an increased LOS and decreased global assessment of functioning score
among psychiatric peers.
17

Chapter II
Literature Review
Inpatient Patient Profile
In a longitudinal study of 481 individuals, Centorrino et al. assessed
characteristics of hospitalized patients in 2004 and 2009 in a Boston Massachusetts
psychiatric facility (2010). Data from this study identify 50% of acute inpatient
individuals meeting criteria for major affective disorders (Bipolar I, II or major
depressive disorder), 33.8% met diagnosis of schizoaffective disorders, and 16.2% of
patients met diagnosis for schizophrenia in 2004. The 2009 data was similar: 50.2% of
patients met criteria for major depressive disorder, 38.9% met criteria for schizoaffective
disorders, and 10.8 % of patients met criteria for schizophrenia (Centorrino, Ventriglio,
Vincenti, Talamo, & Baldessarini, 2010).
This data support that acute inpatient hospitalizations may have approximately
50% of patients suffering from thought disorders and 50% with major affective disorders.
Symptomology associated with affective, bipolar illnesses often includes mania,
hypomania, depression, suicidality, and risk of harm to self or others. Symptomology
associated with thought disorders includes hallucinations, delusions, disorganized speech,
or disorganized or catatonic behavior, symptoms that also contribute to risk of harm to
self or others (Diagnostic and statistical manual of mental disorders, 2000).
Primary clinical goals for inpatient hospitalization are patient safety and
stabilization (Sharfstein, 2009). For patients who are at risk of harm to self or others,
18

staff observation, separation from materials with which to do self-harm, opportunities for
assessment and evaluation from psychiatric staff, and administration of medications are
interventions that lead to patient stabilization. Inpatient hospitalization allows for safe
transition from one medication to another medication, monitoring for side effects, and
therapeutic improvement in overall functioning (Sharfstein, 2009). This care is driven by
the best practices in mental health research.
Emergency Events
Emergency events were analyzed as an independent variable in this study. A brief
explanation of rational for use and type of emergency events follows.
If a patient has become destabilized and experiences an exacerbation or
recurrence of previous symptomology, then treatment guidelines recommend scheduled
oral antipsychotic medication as a first line intervention. However, there may be clinical
justification for temporary, rapid tranquilization, and/or the use of intramuscular
preparations of medication during episodes of escalation where there is risk of harm to
self or others, understood to be aggressive behavior. (Lehman & Lieberman, 2004;
Massachusetts General Hospital handbook of general hospital psychiatry, 2010). Such
episodes may be considered a psychiatric emergency, and in addition to the use of
emergency medication, temporary seclusion or restraint may be necessary to promote
safety for patient, staff, and others (Allen & Currier, 2004; Lehman & Lieberman, 2004;
Massachusetts General Hospital handbook of general hospital psychiatry, 2010; Sadock,
Kaplan, & Sadock, 2007).
19

Seclusion and Restraint
The use of seclusion and restraint to care for psychiatric patients has evolved
from the 18th to the 21st Century. Earlier mental health approaches utilized complete
restriction of the mentally ill, treatment that is non-therapeutic and inhumane. Current
hospitalization practices prefer social therapies over restriction or seclusion (March &
Caple, 2012). The concept of “least restrictive practices” identifies multiple interventions
that can be used before seclusion or restraint is initiated. Such least restrictive alternatives
could include redirection, relocation, PRN medication administration, supportive
listening, management of pain, and use of therapeutic distraction. All such measures are
intended to de-escalate, assess, and provide therapeutic interventions for patient safety
and well-being (Bower, McCullough, & Timmons, 2003; Lewis, Taylor, & Parks, 2009;
March & Caple, 2012).
The use of inpatient seclusion varies from institution to institution. Possible
explanations for this variation include “philosophy of the institution; the attitude of the
staff; the impact of community pressure; and the ward milieu” (Bower et al., 2003, p. 4).
Used as an intervention to protect patient and staff from dangerous behavior, seclusion
may be a preferable, if undesirable intervention that may replace the need for
tranquilizing medication.
Data consistently suggest that use of seclusion may be best predicted by staff and
unit factors rather than by level of agitation or violence in the patient population. These
analyses also suggest that seclusion may be considered useful to ‘manage workload when
too many agitated patients are admitted at the same time” (Bower et al., 2003, p. 5). An
additional finding perhaps counterintuitive, is that incidents of seclusion may increase
20
when staff ratios go up (Bower et al., 2003). This apparent contradiction may be
understood as an interaction between the increased stimulation on milieu produced by
higher density of people and disturbed patients. Another explanation for this phenomenon
could include the staff culture created with higher staffing ratios that may differ from low
patient to staff ratios (Phillips & Nasr, 1983).
Restraint of a patient may include either manual or mechanical means to prevent
body movement, possibly resulting in the forced ingestion or injection of medication, and
may also include the verbal threat of force (Bower et al., 2003). For patients who are
involuntarily committed and are medication noncompliant, such restraint events may be
the only time these patients receive medication.
Understood to be a failure of therapeutic redirection and de-escalation, seclusion
and restraint are a last resort interventions on an inpatient psychiatric hospital (March &
Caple, 2012). Use of such measures is understood to have little therapeutic value.
Emergency Events Medication Administration
Psychiatric emergencies that may justify the clinical use of involuntary
medication may include occasions when a patient is violent, assaultive, experiencing a
massive panic attack, or when experiencing adverse effects from psychotropic
medication. During such emergencies, psychiatric staff including doctors, nurses, and
technicians are trained first to use supportive listening, assurance of safety, and
redirection. These psychotherapeutic interventions occur while removing objects of
harm or persons of harm from the environment (Sadock et al., 2007).
21
If these interventions fail to reduce risk of harm to self or other, then
pharmacotherapy is justified. This use of medication is not intended as part of a
comprehensive, scheduled plan for clinical improvement, rather, it is intended to produce
tranquilization, sedation, and to reduce disturbances associated with a psychotic or manic
process (Sadock et al., 2007). Medications used in psychiatric emergencies generally
include benzodiazepines, antihistamines and/or antipsychotics. These medications may be
given orally, intramuscularly, or intravenously. For patients who are conscious and can
respond to questioning, oral medications are offered first if judged clinically safe
(Wilson, Pepper, Currier, Holloman Jr, & Feifel, 2012).
In a 2012 clinical practice guideline outlining the best practices for treatment of
agitation, five considerations are included in the algorithm for medication. Abbreviated
here, they include: 1. The use of medication as a restraint should be discouraged; 2. Non-
pharmacologic approaches should be attempted first; 3. Medication should be used to
calm patients not to produce sleep; 4. Patients should be included in selection of
medication; 5; Oral medications are preferred over intramuscular preparations (Wilson et
al., 2012).
Long term use, or overdose of antipsychotics is associated with potential changes
in heart rhythm, may induce extra-pyramidal side effects (EPS), or induce neuroleptic
malignant syndrome (NMS), all of which can be life-threatening complications.
It is important to note that even short duration use of emergency medications can
have adverse risks and outcomes to patients. Benzodiazepine administration can
potentiate central nervous system depression, especially if there are unknown other
substances that the patient has in his or her system (Massachusetts General Hospital
22

handbook of general hospital psychiatry, 2010; Sadock et al., 2007; Stahl, 2008; Villari et
al., 2008). The use of emergency medications is associated with cumulative risks from
recent drug use, intolerance to medications, or unknown adverse reactions that a patient
may express. The goal of use of emergency medication is short-term stabilization,
assessment, and integration in the inpatient environment where further evaluation
continues.
Ideally, patients cooperate with the prescribed treatment plan for administration of
medication and psychotherapy. Combined, social and cognitive therapeutic approaches,
administration of medications, monitoring of side effects, and coordination of transferred
care to the outpatient environment, constitute hospital-based treatment (Massachusetts
General Hospital handbook of general hospital psychiatry, 2010).
Predicting Emergency Events
Attempts to dependably predict which patients may require seclusion or restraint
using demographic data have failed. The only demographic data that correlated is age,
with a negative correlation. There is, however, some data that are suggestive that female
gender, involuntary admission, and hospitalization between 30 and 365 days is associated
with increased use of seclusion (Bower et al., 2003). Multiple studies have correlated
diagnostic features with incidence of seclusion and restraint. These studies find
“psychosis, personality and character disorders, manic symptoms, abnormal ECGs, and
mental retardation were associated with higher seclusion and restraint use” (Bower et al.,
2003, p. 5).
23

Precipitating factors may include staff perceptions that such interventions are
necessary to prevent violent, harmful, and unruly behavior. Patient characteristics
associated with increased frequency of seclusion, including involuntary commitment, are
un-medicated or medication non-compliant patients and patient populations higher in
diagnoses of psychoses (Phillips & Nasr, 1983).
In studies attempting to predict staff perceptions and organizational settings that
contribute to the use of seclusion and restraint, some correlations have been found. In
their 2011 study, De Benedictus et al. evaluated hospital setting type, gender of provider,
scales of perceived aggression, group environment characteristics, violence management
training, and perception of staff safety in a multi-variant regression analysis of predictors
for seclusion and restraint. Inpatient aggression is distinct from inpatient agitation, and
includes an assessment that there is risk of harm to the patient him/herself, or to another
person. Patients may be agitated, but not aggressive, and patients may show no signs of
agitation, but become aggressive, or there may be a combination of agitation and
aggression. Their data give findings to suggest that “greater expression of anger and
aggression among staff members and perception of a higher level of physical aggression
against the self among patients were significant independent predictors of greater use of
seclusion and restraint” (De Benedictis et al., 2011, p. 488). Additional trends show
significant association between the perception of staff safety and use of such events. This
study is suggestive that variability in the therapeutic milieu not only impacts the patient’s
perception, but is also associated with behavior of staff.
24

Evaluation of Outcome of Hospitalization
After a course of inpatient hospitalization, evaluation of the outcome of treatment
can be assessed in a few ways. Multiple studies correlate cost, psychiatric diagnosis, and
LOS (Stensland, Watson, & Grazier, 2012; Tulloch et al., 2011; Zhang et al., 2011).
These categorical and continuous variables can be used in treatment planning, evaluation
of programming, and preparation for budgets.
Outcomes that measure patient variables include assessment of patient
satisfaction of the hospital experience, utilization of hospital-based recommendations
(such as compliance with outpatient provider appointments), and mean change in
functioning pre-and post admission (Aas, 2010; Appleby, Desai, Luchins, Gibbons, &
Hedeker, 1993; Jörgensen et al., 2009; Middelboe et al., 2008; Startup, Jackson, &
Bendix, 2002).
As will be shown in review of the literature, studies that objectively measure
effect size of unit setting variables are scant. Appreciation of these objective findings is
necessary to guide further research into milieu variables that impact patient satisfaction
and patient outcome. Having been validated as reliable measures of outcome, LOS and
GAF were used as the objective dependent variables for purposes of this study.
Global Assessment of Functioning
Recorded on Axis V in the Diagnostic and Statistical Manual (DSM-III, DSM-IV-
TR), the Global Assessment of Functioning (GAF) (Appendix A: Figure 1) is a brief
rating scale to evaluate a patient’s psychological, social, and occupational functioning
(American Psychiatric Association & American Psychiatric Association, 1987, 2000;
25
Startup et al., 2002) . This scale places a patient’s hypothetical level of functioning on a
combined continuum rated from 0 to 100. The scale is divided into 10 increments that
define 10-point intervals. Early researchers considered the simplicity and unit
dimensionality to be major advantages of the GAF (Goldman, Skodol, & Lave, 1992;
Jones, Thornicroft, Coffey, & Dunn, 1995; Skodol, Link, Shrout, & Horwath, 1988).
Data from these researchers found a high inter-rater reliability of R =.76. These findings
confirmed earlier studies concluding that mental health professionals require brief
training to use the scale reliably (Startup et al., 2002).
Jones and colleagues investigated the validity and reliability of the GAF for
patients with schizophrenia in a research setting. This research also shows the GAF to be
a “reliable, quick measure of disturbance in functioning, which can be readily used by
multidisciplinary raters, without the need for extensive training” (Jones et al., 1995, p.
659).
However, when the GAF was tested in the clinical setting of a psychiatric
hospital, the GAF was found to have poor reliability when assessing patients with
depression. The study found a Pearson’s correlation coefficient of 0.26 (P ≤ 0.001) for
this population. A partial explanation for this discrepancy in reliability is that this
population of depressed patients often present with more somatic symptoms. Such
symptomology may not be associated with social functioning, but is associated with
overall score (Grootenboer et al., 2012).
With diverse findings based on research setting, primary Axis I diagnosis, and
physical symptomology, it is suggestive that perhaps the GAF should be used within
patient populations rather than between (Aas, 2010; Grootenboer et al., 2012). This
26

scale may be useful to measure the relative change in a given patient when evaluated by
the same staff over time. However as a measure used to compare different patients in
different environments by different staff, the GAF may not be useful as an absolute
assessment of functioning.
In the context of this study, GAF is assessed on admission and on discharge. In
the typical short course of stay, patients at this hospital setting are assigned one attending
physician and one psychiatric resident for the duration of hospitalization. While there is
some turnover in psychiatric resident population each year, the cohort of psychiatric
residents is relatively stable..
As an example of how GAF measures are used to assess outcome, in a McLean
Hospital study, mean change in admission to discharge GAF score was evaluated both in
2004 and 2009. For patients diagnosed with major affective disorders, schizoaffective
disorder, and schizophrenia, the mean improvement in GAF score was 43.0 ± 14.6 (SD).
The 2009 data for the same patient population, show a mean improvement in GAF of
42.2 ±14.4 (SD) (Centorrino et al., 2010). Thus study suggests that over time, and in the
same environment, mean scores and standard deviation are stable.
Length of Stay
Defined as the period of time from admission to discharge, psychiatric inpatient
LOS has steadily decreased in the last 30 years in the United States. In their 1998 article,
Lieberman et al. state that “the past decade has seen dramatic changes in the role played
by psychiatric hospitals in the care of patients. Patients who would remain hospitalized
for weeks, months, or even years are now treated mostly or entirely in outpatient settings.
27

LOS are measured in days” (Lieberman, Wiitala, Elliott, McCormick, & Goyette, 1998,
p. 905).
In a 1993 study, Appleby and colleagues report that “the median public hospital
stay [for mental illness] dropped by almost half between 1970 and 1980 to 28 days in
1986” (Appleby et al., 1993, p. 72) . Data from their 1993 study found that 1,500
patients with severe mental illness (schizophrenia) had a mean inpatient LOS of 17 days
(Appleby et al., 1993).
Examining variables associated with LOS in 106 Level 1 Hospitals and 42 Level
2 County Mental Health Facilities, Lee, Rothbard and Noll found a further decrease in
mean inpatient LOS to 10.0 days for persons with serious mental illness (2012). This
data confirm studies that find average LOS of psychiatric hospitalizations declined from
12.1 days to 9.6 days between 1988 and 1994. For patients with serious mental health
disorders, similar declines are observed between 1995 and 2002 with a decrease from
12.8 days to 9.7 days (Lee, Rothbard, & Noll, 2012; Mechanic, McAlpine, & Olfson,
1998).
In their 2012 study, Stensland et al. attempted to estimate costs associated with
inpatient psychiatric care (2012). Utilizing databases from 418 community-based
hospitals, they calculated mean days of hospitalization by diagnosis. Their published
findings of inpatient, psychiatric stays paid by Medicare found mean LOS for
schizophrenia at 11.1 days, bipolar disorder 9.4 days, depression 8.4 days, drug abuse
disorder 5.2 days and alcohol use disorder 6.2 days (Stensland et al., 2012).
Primary motivating factors for the reductions in hospitalization LOS were (and
are) financial. LOS is affected by payer type, state and national budgets for care. In their
28

1993 study, Bezold et al., found mean LOS for their patient population was 11.78 days.
The most important correlation predicting LOS was method of payment. This study
found that shorter LOS were associated with managed care and both private pay and
government pay patients had longer hospitalizations (Bezold, MacDowell, & Kunkel,
1996; Blader, 2011).
Socio-demographic and clinical diagnosis have not been supported by research to
be significant predictors of LOS range, accounting for only 3% of the variation. Beyond
restrictions by payer, significant associations with LOS can be attributed to hospital
characteristics. However, there have been very few studies that use statistical models to
assess hospital characteristics (Lee et al., 2012).
During the period of time that LOS has decreased, clinical goals of hospitalization
have changed as well. Previous lengthy hospitalizations were associated with “ego-
enhancing aspects”, a therapeutic goal that is not expected or assessed in shorter course
treatment (Lieberman et al., 1998, p. 905). Current goals for hospitalization are patient
safety and stabilization, initiation and adjustment of medications, opportunities to clarify
diagnosis, and ultimately, swift transitioning of the patient to outpatient providers
(Lieberman et al., 1998; Massachusetts General Hospital handbook of general hospital
psychiatry, 2010). Shorter stays are not associated with increased rates of readmission,
however there is uncertainty about the level of functioning at discharge, whether patients
are discharged as ‘well’ as they had been with longer stays (Lieberman et al., 1998;
Zhang et al., 2011).
29
Patient Advocacy: Autonomy
Published by the American Nurses Association, the Code of Ethics for Nurses
outlines legal, ethical, and social considerations to protect the rights of individuals in
their healthcare interactions. Provision 1 of the Code directs nurses to practice with
“compassion, respect for the inherent dignity, worth, and uniqueness of every individual”
(American Nurses’ Association, 2001, p. 3). This provision highlights the patient’s right
to self-determination. Also known as autonomy, this is the basis of non-paternal, patient
centered, patient informed, and patient consent to treatment. As a society we have
determined that “patients have the moral and legal right to determine what will be done
with their own person” (American Nurses’ Association, 2001, p. 4).
A caveat to patient autonomy occurs in an appreciation that patients are members
of a community, the framework of utilitarian ethics in health care (Fry, 2002). The
definition of community can include living with psychiatric peers, staff and family on an
inpatient hospital unit. Patient autonomy is weighed by nurses, and other health
providers, when patient actions limit the “rights, health, and welfare of others” in the
context of impingement on the rights of the community (American Nurses’ Association,
2001, p. 4).
Nurses understand that the involuntary administration of medications is a serious
departure from our code, a code that is focused on patient autonomy. The involuntary
administration of treatments, restraints, seclusion, or other protective mechanisms are
ethically justified only when there are no less restrictive means available that would
protect the safety and rights of others and the safety and rights of the patient (American
30

College of Emergency Physicians, 2012; American Nurses’ Association, 2001; Bower et
al., 2003; Fry, 2002).
It is worth noting that extensive literature documents the negative impact on
hospital staff when any action is taken that impinges on patient autonomy. Literature
supports the moral distress, professional burnout, shame, and in some cases guilt that
nurses feel as a result of involuntary administration of medication (Bower et al., 2003; De
Benedictis et al., 2011).
Policies that protect patient autonomy require a judicial review process before the
administration of involuntary court ordered medications for scheduled therapeutic
treatment. This judicial process creates a period of time when patients are involuntarily
committed to hospital care, but do not receive psychotropic medications that will reduce
the risks of harm to self and others.
Evidenced based practices suggest that early treatment of thought disorders results
in improved outcome (Lehman & Lieberman, 2004). For patients who are involuntarily
committed to a hospital due to risk of harm to himself or others, and whose risk is not
related to a substance which will clear the system (Dawe, Geppert, Occhipinti, &
Kingswell, 2011), psychotropic medication will be required for stabilization and safety.
Additional considerations are the data that suggests that for many patients, a period of
protracted hallucinatory, delusionary, paranoid, or manic illness is traumatic, and is in
itself harmful to the patient’s well-being (Jackson et al., 2009).
Balancing these considerations of patient autonomy, patient legal rights, the
process of patient observation to assess for substance-induced causes of psychosis,
contribute to a patient milieu that has a mixture of pharmacologically treated and
31

untreated individuals. Managing this patient mix requires nurses to utilize frameworks of
patient care, appreciation of their role in managing patient stress and coping, and assuring
that the milieu is a safe environment (Bower et al., 2003; Lazarus & Folkman, 1984;
Mahoney et al., 2009).
Nursing Theory: Therapeutic Milieu
Milieu in Context
In psychiatric mental health nursing, the therapeutic environment is referred to as
the therapeutic milieu. From the French word meaning “middle”, in the context of
inpatient hospitalization “milieu” refers to the surroundings or environment. The
therapeutic milieu has it’s origins in the psychoanalytic tradition: In the 1930s,
psychiatrists would instruct staff in the management of inpatient behaviors in an attempt
to address patients intra-psychic conflict (Delaney, 1997).
Emerging from the less humane treatment of the mentally ill in the 1930s and 40s,
Peplau’s theory of Interpersonal Relations contributed humane, patient-centered care into
the milieu. In the United States during the 1960s, 70s, and 80s, Milieu Therapy, an
interpersonal dynamic construct, was the rationale for nurse-patient relationships. This
evolving theme of patient-centered care informed the process of nurse-patient
interactions. In this revision of role interaction, nurses began to identify the milieu itself
as a primary intervention: “the patient’s illness is in his relationships with people; his
recovery must be achieved through relationships with people” (Holmes, 1966, p. 4).
32

Such a perspective reflects the social causes of mental health illness, prevalent at that
time (Mahoney et al., 2009).
Social process literature published in the 1960s and 1970s identify the hospital
staff as contributors to the milieu experience. Staff-generated treatment environments
were understood as an expression of attitudes about patient’s autonomy, respect, and
benevolence. “The resulting concept of ward atmosphere created by staff attitude was the
foundation of 20 years of milieu research” (Delaney, 1997; Sugden, 1985, p. 21). This
research attempted to identify both the relevance, and the contribution of ward
atmosphere to patient outcomes.
However, “20 years of milieu research attempting to substantiate a relationship
between positive patient outcomes and particular ward atmospheres” were unable to
establish a clear relationship (Delaney, 1997, p. 21; Kirshner & Johnston, 1982). This
lack of correlation was not due to a lack of patient benefit from the therapeutic milieu,
rather it was a function of an inability to operationalize the milieu construct (Ellsworth &
Maroney, 1972; Kirshner & Johnston, 1982; Melle et al., 1996) . Identified as a practice
issue in their 1985 review of milieu studies, Norwegian researchers concluded that “our
knowledge in this field of research has not yet reached the level were experimental
investigations using ward comparison design can give us meaningful results. It is
necessary to identify more specifically milieu variables which are correlated to the course
of functional psychosis by use of correlational designs” (Vaglum et al., 1985, p. 350).
33
History
Reviewing the published literature of the times, one can see prevalent concepts of
mental health treatment and responses from providers in the evolving definition of
Therapeutic Milieu:
1950s: “ The idea of a therapeutic community as a form of social therapy in
psychiatry emerged… With the notion that the structure of the environment was a
therapeutic element of treatment” (Mahoney et al., 2009, p. 423).
1960s: The therapeutic milieu aims were described as “ to control or set limits on
the main kinds of pathological behavior (destructiveness, disorganization,
deviancy, dysphoria and dependency) and promote the development of basic
psychosocial skills” (Abroms, 1969, p. 560).
1970s: “A scientific structuring of the environment in order to effect behavioral
changes and to improve the psychological health and functioning of the
individual” (Skinner, 1979; Townsend, 2009, p. 196)
1980s: An environment to learn “new, more constructive ways for solving
problems” (Jack, 1989, p. 69).
1990s: “The purpose of a therapeutic milieu is to provide inpatients with a “stable
and coherent social organization” (Mahoney et al., 2009, p. 424; Tuck & Keels,
1992, p. 54).
2000s: “The development of an environment where the purpose is to contribute
to the patient’s recovery” (Skorpen, Anderssen, Øye, & Bjelland, 2009, p. 410)
34

In these definitions, one can observe the influence of social thinking, behaviorism,
solutions focus, cognitive training, and finally to a treatment goal of ‘stabilization and
discharge’ to the outpatient environment. In part, this emerging definition was a reaction
to the realities of inpatient treatment: “Increasingly, people with acute and severe mental
illness are admitted for short periods of intense treatment and are discharged quickly to
community-based care” (Thibeault, Trudeau, d’ Entremont, & Brown, 2010, p. 216).
This reduction in LOS reduced the clinical relevance of milieu, with a focus
placed increasingly on the administration of medications to achieve therapeutic goals
(Massachusetts General Hospital handbook of general hospital psychiatry, 2010;
Skorpen et al., 2009; Tusaie & Fitzpatrick, 2013). Reflecting the shift to short-term
hospitalization, Echternacht suggests a reframing of milieu interventions proposing that
the psychiatric nurse provide “on the spot therapeutic interventions designed to enhance
socialization competency and interpersonal relationship awareness” (Echternacht, 2001,
p. 40). This shift in focus deemphasizes the role of an enduring “nurse-patient”
relationship, and instead focuses on the role of any nurse to intervene with any patient,
providing brief redirection, reassurance and support.
Current focus on the therapeutic milieu suggests its “lack of relevance” (Mahoney
et al., 2009, p. 423) in the hospital treatment of mental illness. This is in contrast to other
initiatives in patient care where rooms are refurbished, noise is addressed, and patient
comfort is considered a therapeutic good. This highlights a recurring theme in the
discussion of milieu: “There are two general views of the relationship between
environment and outcome. The first one claims that an appropriate treatment environment
is a prerequisite for therapeutic outcome. The second possibility is that the treatment
35

environment is therapeutic in itself and leads to an improved outcome” (Eklund &
Hansson, 1997; Jörgensen et al., 2009).
If we accept the first definition, that milieu is just a ‘container’ in which we
provide therapeutic interventions, then such a container need only be good-enough.
There would be no benefit to improving milieu beyond its capacity to provide actual care.
However, if we accept the second definition, that milieu is an intervention itself, and then
we should be able to see variability in outcome when milieu is just ‘good enough’ or
when it is optimized.
Treatment Modality
The American Nurses Association credentials and set standards of practice for
psychiatric-mental health nurses. Standard 5C: Milieu Therapy, states that “The
psychiatric-mental health registered nurse provides, structures, and maintains a safe and
therapeutic environment in collaboration with patients, families, and other healthcare
clinicians”(American Psychiatric Nurses Association, International Society of
Psychiatric-Mental Health Nurses, & American Nurses Association, 2007, p. 39).
Measurement criteria for this standard includes patient orientation, protection of patients
rights, patient assessment, participating in activities that promote personal growth,
utilizing lease restrictive measures, supporting and validating the patient’s experience of
their illness, and seeking to prevent complications of their illness (American Psychiatric
Nurses Association et al., 2007).
These measurement criteria are difficult to operationalize. But, importantly,
research has shown that patient satisfaction has been shown to be a valid indicator of
36
quality of treatment and that quality impacts outcome (Druss, Rosenheck, & Stolar,
1999). Early attempts to quantify the milieu experience resulted in the production of
various scales. The Ward Atmosphere Scale (WAS) was used in the 1970s and 1980s in
milieu research. It is a subjective measure of perceived atmosphere from both patients
and staff; it is not a measure of objective findings on the unit. As such, analysis from
these studies can help identify patient outcomes that are associated with their perception
of the hospitalization experience.
Using this instrument as a measure of patient satisfaction, post-hospitalization
outcomes correlated with variables in WAS scores. In particular, hospital outcomes
were positively correlated to the perceived level of order and organization and were
negatively correlated to levels of anger and aggression (Friis, 1984; Vaglum et al., 1985).
This may be explained in the results of a quasi-experimental study, that demonstrated that
levels of aggression on the ward were observed to increase when the amount of
individual care and support by staff was reduced (Vaglum & Bøe, 1981). This
correlation may be related to decreased ability of nursing staff to provide support while
they are engaged in managing aggression of psychiatric peers.
Additional findings of milieu perception as a factor in treatment outcome
includes; Increased number of patients results in unfavorable milieu perception; Low
order and organization, low support, and high anger and aggression decreased perception
of favorable milieu; Increased percentage of psychotic patients on the milieu is negatively
associated with favorable milieu; Increased mean age is positively associated with milieu
favorability ratings; And, finally frequent staff turnover is negatively associated with
patient outcomes (Vaglum et al., 1985).
37

Such investigations provided data supporting the conclusion that patients prefer
ordered environments. Data also support the conclusion that patient satisfaction is
negatively associated with high levels of aggression and the resulting need for staff
control, and that patient satisfaction is associated with outcomes (Friis, 1984; Jörgensen
et al., 2009; Middelboe et al., 2008; Moos, Shelton, & Petty, 1973). Melle, who studied
psychiatric units that implemented a program resulting in decreased unit aggression and
increased unit order, produced additional support for an ordered milieu. Outcomes from
this research show that patients LOS was reduced, and symptom reduction was
maintained. This data suggest that more ordered units may be more effective in
delivering optimum treatment (Jörgensen et al., 2009; Melle et al., 1996).
However, with the shift to shorter LOS, increased focus on safety and
stabilization, and difficulties in operationalizing milieu treatment, few recent studies have
attempted to evaluate psychiatric patient outcomes as a function of milieu. A decade
ago, a literature review of milieu found that “in the past five years, research and
professional articles about the therapeutic milieu and milieu therapy concepts have been
almost nonexistent" (Echternacht, 2001, p. 43). This trend continues today. Absent from
current discussion of milieu is current investigation on the continuing role of hospital
environment on treatment outcome.
To date, milieu therapy has not been operationalized, nor has it been standardized
(Mahoney et al., 2009). With milieu atmosphere a function of nursing style, assessment
of milieu ‘in toto’ has been inconclusive. With data that associated perception of anger,
aggression and disorder related to outcome, it is reasonable to continue the investigation
38

of the environmental impact on psychiatric patients by examining specific, objective,
independent variables.
Aggression on the Unit
Associated with decreased patient satisfaction, increased LOS, and poor patient
outcomes, data that identify anger, aggression, and unit disorder are suggestive of an
objective measure correlating milieu quality and patient outcome (Friis, 1984; Jörgensen
et al., 2009; Melle et al., 1996; Vaglum & Bøe, 1981). To manage unit safety, staff may
implement emergency interventions that reduce unit disorder; such interventions are
recorded in patient charts. While it may be difficult to gather data on the subjective
experience of unit aggression, objective data on use of seclusion, restraint, and
emergency medication administration may be useful as a proxy.
The use of chemical restraint or emergency medication is intended to control
behavior. When medications are administered as part of an ongoing, scheduled regimen,
they are used for therapeutic purposes. However, in the event of behavioral escalation,
patient agitation, patient aggression, after evaluation by a physician, a one-time order for
medication can be prescribed. Often considered an ‘least restrictive alternative”,
chemical restraint may be part of a therapeutic approach to avoid the use of seclusion or
restraint (Currier & Allen, 2000; O’Sullivan, Fava, Agustin, Baer, & Rosenbaum, 2007).
Intended to be used as an intervention of last resort, data suggest that violence is
the major reason for patient seclusion in psychiatric hospitals (Lewis et al., 2009). This
therapeutic removal from milieu is judged necessary to protect a patient, peers, staff or
39

visitors to the unit from violent or risky behavior (Bower et al., 2003; March & Caple,
2012).
Patient characteristics associated with increased likelihood of seclusion include
patients referred from state psychiatric hospitals, younger age, involuntary commitment,
or LOS between 30 and 365 days. Diagnostic associations with increased likelihood of
seclusion include psychosis, personality disorders, mania, substance abuse, and mental
retardation (Bower et al., 2003; Cornaggia, Beghi, Pavone, & Barale, 2011; Norton,
2004).
Knowledge about the effectiveness of seclusion is inconclusive. There are limited
data suggesting that seclusion reduces incidence of violence on units, or that it results in
therapeutic improvement of patients secluded. Few nurses surveyed find that seclusion
or restraint has a positive impact on patients. Interestingly, data are suggestive that the
impact of seclusion on non-secluded psychiatric peers, is negative as well (Bower et al.,
2003; Lewis et al., 2009).
Factors associated with successful management of aggressiveness include nurse
staffing ratios, a setting with ample space for patients and nurse training, in other words,
“a good ward climate” (Cornaggia et al., 2011, p. 18). Models of therapeutic response to
aggression suggest that patient-centered, ‘authentic engagement’ with patients result in
patient de-escalation without the risks and consequences of emergency events.
Research has produced “evidence which seems to identify the patient’s perceived
levels of anger and aggression, order and organization, support, and practical orientation
as crucial factors which are related to the post hospital outcome of short and intermediate
treatment” (Vaglum et al., 1985, p. 359). As a proxy for therapeutic milieu, researchers
40
can use the negative findings of patient dissatisfaction with unit aggression and disorder,
and the positive findings of therapeutic use of nursing staff that reduce unit aggression to
be measurable by number of emergency events.
Summary of Research Findings and Need for Study
As described in the discussion of the history of inpatient psychiatric care, with the
introduction of psychotropic medications, a move to patient deinstitutionalization, the
reduction in number of psychiatric hospitals, increased proportion of psychotic patients,
and decreased LOS, “ the environment of the acute inpatient psychiatric ward is
significantly different from that of the 1960s and the 1970s” (Norton, 2004, p. 280).
Originally conceptualized as a therapeutic intervention, the hospital milieu has been
deemphasized in recent years. Research on the impact of milieu is scant: “There are only
a few published studies on milieu therapeutic practices since the early studies conducted
in the 1950s, 1960s, and 1970s” (Skorpen et al., 2009, p. 410). With focuses on the
impact of medication, impact of cost, there has been “little systematic work that has been
reported about what actually goes on in the standard acute psychiatric ward” (Norton,
2004, p. 279). This suggests that objective data of milieu variables that impact treatment
are needed.
With this lack of research, data are limited to guide our construction of an
optimal therapeutic milieu. A description of milieu characteristics can be gained from
research about patient satisfaction which may be useful to identify independent variables
in patient outcome. Through various researchers, data have been collected identifying a
milieu satisfying to patients as one that is “characterized by a combination of a high level
41

of order and organization, practical orientation, and support and a low level of anger and
aggression” (Vaglum et al., 1985, p. 360). However, subjective data of satisfaction does
not quantitatively describe the activities, setting variables, or events that occur in the
milieu. Such data reflect an understanding that patients prefer certain environments, not
how these preferred environmental variables interact.
While researchers can appreciate these characteristics, objective ways to identify
them as independent variables needs to be explored. To build on existing data, milieu
therapy research should “study the relationships among five types of variables: Setting
variables, treatment variables, human interaction, perceived milieu variables, and
treatment outcome variables” (Vaglum et al., 1985, p. 350). This data is needed, but
without data to support the impact of independent variables on dependent variables,
researchers do not know precisely which interventions to study to optimize patient
outcome. As stated by Delaney “without an explicit explanation of the critical processes
of milieu therapy, it has been impossible to build a body of research that supports milieu
therapy as an intervention technique with clear outcomes” (1997, p. 23).
Research has identified the impact of seclusion on an individual. There seems to
be little therapeutic benefit from seclusion, and significant increased risk of harm to both
staff and patient from emergency events (March & Caple, 2012). However, there has
been little focus on the impact of psychiatric peers who are on units with high incidents
of aggression, anger, and use of emergency interventions. Recognizing that “the
patient’s apprehension of the milieu is an important intervening variable between setting
variables and behavioral variables” (Vaglum et al., 1985, p. 350), research can be
42

expanded that identifies negative perceptions of aggressive and disordered units, and
evaluates the outcomes of psychiatric peers who experience such misapprehension.
As stated by previous researchers, investigations into milieu therapy require
identification of milieu variables utilizing correlational designs (Vaglum et al., 1985).
Operationalizing psychiatric care along data from correlational designs allows us to
evaluate nursing interventions as measured by patient outcomes (Delaney, 1997). As
previous data suggest LOS and GAF change are valid objective tools to assess the
dependent variable of inpatient psychiatric hospitalization outcome. Unit emergency
events are a proxy for a disordered unit high on scales of aggression, the independent
variable. Thus, the explicit need for this study is: To objectively quantify the
independent milieu variables that impact treatment outcome.
43

Chapter III
Method
Study Design
This is a retrospective cohort study examining treatment outcomes of two
psychiatric patient populations: Those admitted to one hospital eighteen months before or
eighteen months after August 29, 2011.
Definitions
Therapeutic Milieu: Using Skorpen’s definition of the milieu as “the
development of an environment where the purpose is to contribute to the patient’s
recovery” (2009, p. 410)
Emergency Event: Unusual events, that are not part of a treatment plan, when
interventions are used to protect individuals from harm to self or others. For this
study, emergency events include the number of uses of seclusion, restraint or
administration of emergency medications on the unit per day.
Length of Stay: The duration in days of time from admission to time of discharge
from the inpatient hospital environment.
Global Assessment of Functioning: The Global Assessment of Functioning
(GAF) is a scale used by clinicians to numerically described judgment and
functioning at the time of interview. Numerical values are assigned. When a
44

range is listed (i.e. 11-20), then the lower value will be used to measure mean
change.
Setting
On August 29, 2011 a flood occurred in a small New England state. This flood
permanently destroyed the existing State Hospital (SH). Patients currently in treatment at
the SH were moved on August 29 to other psychiatric facilities in the state (Goodnough,
2011). Previous to the closure of the SH, patients who were acute, aggressive, or
medication non-compliant would be treated at the SH. After the closure, such patients
received care in other regional inpatient psychiatric facilities. These alternate facilities
were not designed for patients requiring specific care for acute psychiatric need
(Goodnough, 2011). The setting for this study is one such hospital.
No significant changes were made to the hospital environment after the flood
event. There were no significant changes in psychiatric staff, psychiatric residents, or
registered nurses. There was however, a short-term change in staff-to-patient ratio.
Mental health technicians and registered nurses from SH were on the unit for
approximately seven months after relocation. This did result in a short-term increase in
staff-to-patient ratio which returned to pre-SH closure after seven months. During this
temporary increase, both state employees and hospital employees worked together.
The data were collected from a locked 16-bed inpatient psychiatric ward in
Burlington, Vermont. In addition to 14 patient rooms, this unit has a locked seclusion
room and a locked restraint room. The patient milieu includes a circular hallway, a small
computer room, a kitchen area, an activities room, and an enclosed porch.
45

This short-term, acute psychiatric ward serves patients in northern Vermont and
parts of New York State. The region contains approximately 160,000 inhabitants. The
hospital is affiliated with the University of Vermont. Attending physicians and psychiatric
residents provide psychiatric services. Additionally, the unit serves educational purposes
for both nursing students and medical students (Fletcher Allen, 2013).
Staffing on the unit varies. Typically, registered nurses are staffed at a 1:3 ratio,
and mental health technicians are staffed at a 1:6 ratio. This ratio may change during
periods of increased acuity on the unit. This staffing ratio changed post August 2011
with an increase in staff on the unit per shift with SH staff.
Sample
The study sample includes all inpatient hospitalizations on this locked unit during
the time period of March 2010-March 2013. The sample includes adults over the age of
18 who were either voluntarily or involuntarily hospitalized. The study sample includes
a total of 778 patients.
Exclusion criteria for outcome analysis of the dependent variables, includes
patients hospitalized for one day, patients whose LOS was more than three times the
Interquartile Range (IQR) over the 75th percentile of the calculated LOS, and patients
who were not discharged to home care. This exclusion is to acknowledge that one day of
treatment is not sufficient and may represent discharges against medical advice, to other
units, or to other providers. Additionally, patients who are non-compliant have extended
stays, thus resulting in data non-representative of treatment. This limits the results
46

generalizability to those whose stays are two days or longer and less than three times the
IQR over the 75th percentile of LOS.
However, seclusions and restraints, emergency medication administrations, and
other markers of therapeutic milieu of such patients with longer stays are included as
independent variables for milieu aggression and disorder. After exclusion criteria were
applied, 610 patients were included in the study.
The patients were then divided into two separate cohorts. All patients in the
sample discharged prior to August 29, 2011 were included in Group A. The remaining
subjects in the sample who were discharged after that date were included in Group B.
Data Collection
Consent for this study was sought and approved by the Fletcher Allen Health
Care (FAHC) Nursing Research Council, and the University of Vermont (UVM)
Institutional Review Board (CHRBS). Data were acquired from PRISM, the electronic
medical records database at FAHC. The hospital electronic medical records provided
patient’s gender, date of birth, date of admission, date of discharge, admission GAF,
discharge GAF, disposition at discharge, and discharge primary diagnosis.
For purposes of this study, the Jeffords Institute of Quality Measurement staff,
accessed data from PRISM the hospital electronic medical record, and then delivered the
data to researcher. Demographic data, GAF scores (Axis V from psychiatric diagnosis),
discharge diagnoses (Axis I from psychiatric diagnosis) and emergency events are
independent variables and were mined from the patient record by the researcher. All data
was de-identified and assigned a record number for the study. The dependent variables
47

are the patient outcomes assessed by LOS and change in GAF from admission to
discharge, also mined from patient record. This data was collected and recorded in an
Excel spreadsheet.
In the case that specific information is not available de-identified, then, such
identity-coded-data had the identity separated from the data producing a de-identified
master list. The study then used this separate de-identified master list. The original
master list with identities was kept separately in locked cabinets and with secret password
access, and was destroyed in a secure fashion after the list was no longer needed to
produce the de-identified list.
Ethical Considerations
The UVM institutional review board (CHRBS) and the FAHC Nursing Research
Collaboration (NRC) received and approved the study in advance. This is a study of
group characteristics, and not of individual behaviors or outcomes. Patient confidentiality
was assured and there were no issues with autonomy, or protected patient information.
Data Analysis
The collected data were first assessed for exclusion criteria and outliers.
Descriptive analysis provided demographic and diagnosis characteristics of the sample
population. The analysis of the independent variables for each cohort produced number,
percentage, and when applicable mean and standard deviation of groups. The dependent
variables also appear in this descriptive analysis, and quantify LOS and GAF mean and
standard deviation calculations.
48

ANOVA tests were performed using LOS as the predictor. These tests assess
relative contribution on the variance of LOS outcome contributed by number of
emergency events, by Axis I diagnosis, by gender, age and GAF on admission. These
two-way ANOVA tests were done separately on each cohort. These tests were then
repeated with cohort as a factor in the model to measure effect size of cohort
characteristics.
Multiple linear regressions were performed on each cohort and then retested with
cohort as a factor in the model. This analysis establishes the relationship of emergency
events to LOS in each cohort, and assessed the relative contribution on the dependent
variables outcomes from each independent variable. As before, these regressions were
performed and included cohort as a variable. This analysis allows researchers to explore
alternate explanations that contribute to the dependent variables.
To assess significance of the difference in dependent variables in both cohorts, a
comparison of means was done. This comparison includes a two-sample t-test for
equality of means (See Table 5, Appendix F). This analysis assesses whether there are
any statistically significant differences in LOS change between cohorts.
For all tests of significance p <0.05 was be used. Data analysis were done using
IBM SPSS 21 Statistics software.
49

Chapter IV
Results
Data Collection and Sample Selection
Approval to conduct the study was received from the University of Vermont
Institutional Review Board and from the Nursing Research Council at the studied
hospital. The Jeffords Institute of Quality Measurement was then granted access to the
mirror site of the hospital’s electronic medical records. Two data sets were then retrieved.
The first set included unique codes for patient visits, gender, date of birth, date of
admission, date of discharge, disposition at discharge, and primary diagnosis code at time
of discharge. This data set did not include GAF scores, data that was later obtained
during a chart review by researcher. The second data set, included number of emergency
events by date for the study period.
The original sample included 778 unique patient visits. All patient visits with LOS
of one day (n=53, Group A n=36, Group B n= 17) were removed from data analysis.
The remaining data set of 725 visits included 446 admissions in Group A, and 279
admissions in Group B with LOS of two days or longer.
Chart reviews were then conducted of these remaining patient visits to obtain
GAF scores on admission and discharge. These scores were found in two different
patient documents. The majority of these scores were found in the Discharge Summary
Report, the remaining scores were found in the Initial Psychiatric Evaluation. Thirty
patient visits had incomplete GAF Scores. Group A had 21 (5% of Group A sample), and
50

Group B had 9 (3% of Group B sample) incomplete scores and were eliminated from the
data set. The remaining data set had 695 visits, with Group A having 425 remaining
visits, and Group B having 270 remaining visits. These scores were entered into the
database containing patient visit data.
Initial data analysis includes the generation of scatterplots. The LOS scatterplots
showed significant outliers, and the histogram had a long right-hand tail. To exclude
extreme outliers of LOS, patient visits longer than three times the Inter-quartile Range
(IQR=16) over 75% percentile (22 days) were excluded (Polit, 2012); a total of 22 visits
longer than 66 days. Nine of these visits (2% of Group A), were in Group A, and 13 of
these visits (5.05% of Group B) were in Group B. The remaining data set included 673
visits, with the Group A sample including 416 visits, and the remaining Group B sample
including 257 visits.
To further exclude outliers from the study sample, only patients with a discharge
disposition “Home Care” where included. This eliminated patients transferred to other
units in the hospital, patients transferred to other hospitals or psychiatric facilities, and
patients who left against medical advice. A total of 63 such records were found, and
included 35 visits (9% of Group A sample) from Group A, and 28 visits (12% of Group B
sample) from Group B.
The remaining sample of 610 visits included all patients with complete GAF
scores, LOS >= 2 days, LOS <= 66 days, and disposition to Home Care. Group A
includes 381 visits, and Group B includes 229 visits.
Using Microsoft Excel SUMIFS function, If/Then, commands were written to pull
emergency event data from the second data set. Data included number of administrations
51

of emergency medications, four point restraints, manual restraints, and seclusion events.
Total numbers of events were entered in each visit data group. Total events were summed
creating a separate data set of Total Emergency Events. These combined and limited data
sets comprised the working data for statistical analysis.
Reliability
Descriptive statistics include minimum, maximum, range, mean and standard
deviation. Data analysis includes t-test of means, and multiple linear regressions.
Significance is reported at p<0.05. However, when relevant to discussion, scores
significant at p<0.10 will be included and noted for this marginal level of significance.
Descriptive Statistics and Comparison of Means
Age and Gender
Gender, as reported in the data set, is either listed as male or female. It does not
distinguish transgendered patients identified gender orientation when it may differ from
biological gender. As such gender is analyzed as a bivariate variable.
The total sample (see ) with N=610, had a mean age at admission of 40.23 years
(SD 14.14 years). The total sample included 344 males (56.4%) and 266 females
(43.6%) with mean ages at admission of 38.83 years (SD 14.68 years) for males and
42.05 years (SD 13.85 years) for females.
Group A (see ) with N=381, had a mean age at admission of 41.65 years (SD
14.37 years). The total sample included 190 males (49.87%) and 191 females (50.13%)
with mean ages at admission of 40.68 years (SD 14.61 years) for males and 42.61 years
(SD 14.10 years) for females.
52

Group B (see Table 2) with N=229, had a mean age at admission of 37.88 years
(SD 14.17 years). The total sample included 154 males (67.25%) and 75 females
(32.75%) with mean ages at admission of 36.55 years (SD 14.48 years) for males and
40.63 years (SD 13.19 years) for females.
Mean age between total sample of Groups A and B are significantly different (see
Table 2) with Group B 3.76 years younger than Group A. The t-test score between
Groups A and B is 3.160 with a 2-tailed significance of 0.002. However, within
Diagnostic Code groups, age is not statistically different (see Appendix I: Table 8,
Appendix J: Table 9, Appendix K: Table 10).
Significant mean age differences between Groups A and B are limited to males.
Mean age of males in Group A was 40.68 years (SD 14.61) and Group B 36.55 years (SD
14.48). Mean age of females in Group A was 42.61 years (SD 14.10) and Group B 40.36
years (SD 13.19).
53

Table
Testing independent samples for significance, Male age between Group A and B
is significantly different with a t score of 2.622 (2-tailed sig. 0.009). Female age between
Group A and B was not significant with a t score of 1.05 (2-tailed sig. 0.282) (see
Appendix G: Table 6).
Diagnostic Group
Previous data suggest that course of illness and varying responses to therapy
affect length of stay by diagnostic group (Huntley, Cho, Christman, & Csernansky, 1998;
54
Sadock et al., 2007; Tulloch et al., 2011). All received data included an International
Classification of Disease Ninth Revision (ICD-9) principle diagnosis code at time of
discharge. To improve validity of impact of milieu on length of stay, patient visits were
divided into six Diagnostic Codes (DC) based on ICD-9 discharge diagnosis:
Diagnostic Code 1: Psychotic Disorders. Includes non-substance induced
psychosis, psychosis NOS, hebephrenia, catatonia, schizophrenia, and
schizoaffective disorders.
Diagnostic Code 2: Bipolar Disorders. Includes both manic and depressed most
recent episodes, bipolar disorder NOS, and bipolar disorder with psychotic
features.
Diagnostic Code 3: Major Depressive Disorders. Includes both single, recurrent,
with psychotic features, and adjustment disorder with depressed mood.
Diagnostic Code 4: Anxiety Disorders. Includes anxiety state NOS, post-
traumatic stress disorder, and adjustment reactions with anxious features.
Diagnostic Code 5: Substance Induced Disorders. Includes alcohol induced
mental disorders, drug induced psychotic disorder, drug induced mood disorder,
and drug induced delirium.
Diagnostic Code 6: Other. Includes ante-partum and post-partum mood
disorders, Alzheimer’s disease, dementia, and conduct disorders.
The majority of the samples were either in DC 1, 2, or 3. In the total sample,
theses codes represent 87.87% of the data. In Group A, they represent 86.88% of the
data. In Group B they represent 89.52% of the data. The remaining data are distributed
55

between DCs 4, 5, and 6. This data accounts for 12.13% of the data in the total sample,
13.12% of the data in Group A, and 10.48% of the data in Group B (see Appendix L:
Table 11). Due to the small, and disproportionate distribution of patients visits to these
latter DCs, discussion on milieu impact does not refer to DC Groups 4, 5, or 6.
DC 1 includes 203 (33.44%) of the visits in the total sample. This code includes
111 (29.13%) of visits in Group A, and 93 (40.61%) of visits in Group B. As a proportion
of the studied sample, this code is the largest sample, and is larger in Group B.
DC 2 includes 160 (26.23%) of the visits in the total sample. This code includes
95 (24.93%) of visits in Group A, and 65 (28.38%) of visits in Group B. As a proportion
of the studied sample, this code is larger in Group B.
DC 3 includes 172 (28.20 %) of the visits in the total sample. This code includes
127 (32.81%) of visits in Group A, and 47 (20.52%) of visits in Group B. As a
proportion of the studied sample, this code is smaller in Group B.
Gender is distributed differently between Groups A and B in the DCs. DC 1 has a
male/female ratio of 45.9%/54.1% in Group A and 69.9%/30.1% in Group B. DC 2 has a
male/female ratio of 54.7%/45.3% in Group A and 66.2%/33.8% in Group B. DC 3 has a
male/female ratio of 45.6%/54.4% in Group A and 61.7%/38.3% in Group B. Group A
has fewer males than Group B as a proportion on the study sample (see Table 2).
Global Assessment of Function Scores
Global Assessment of Function (GAF) scores were retrieved from the electronic
medical records (EMR) for all patient visits. Two data points were entered into the
database: GAF scores on admission and GAF on discharge. Incomplete GAF scores,
56

(i.e. incomplete scores on admission and/or on discharge) were eliminated from the data
set. GAF scores on admission were often entered into the EMR as a range, (i.e. GAF on
admission: 11-20, 21-30). Few GAF scores on discharge were entered as a range. GAF
scores on admission are often ranges as the EMR provides range selections with drop-
down menus while completing the evaluation database. However, on discharge, the
provider must enter a unique number, as no selections are available from drop-down
menus for the discharge document.
Table
57

For consistency in data entry, the lowest score was chosen when a range value was
entered. As a result, GAF scores cluster around 11 and 21 on admission. GAF scores on
discharge are more often discrete numbers. A separate data set was created to calculate
the difference between admission and discharge. This data set was labeled “GAF
Change”.
Mean GAF scores on admission for the total sample were 17.38 (SD 7.72). Mean
GAF on discharge were 48.36 (SD 9.04). The resulting mean GAF Change was 30.98
(SD 11.70). Scores for males and females were similar in the total sample (see Appendix
D: Table 3).
Group A and Group B differed on GAF scores. Mean GAF scores on admission
for the Group A were 18.10 (SD 7.25). Mean GAF on discharge were 48.13 (SD 8.99).
The resulting mean GAF Change was 30.03 (SD 12.01). Mean GAF scores on admission
for the Group B were 16.17 (SD 7.23). Mean GAF on discharge were 48.73 (SD 9.12).
The resulting GAF Change was 32.57 (SD 10.99) (see Appendix D: Table 3).
Comparing means, t-tests confirmed statistically significant differences between
Group A and Group B on GAF scores. GAF on Admission had a t-test of 3.090, with a 2-
tailed significance of 0.002. GAF on Discharge was not significant with a t-test of
-0.791, with a 2-tailed significance of 0.430. As a result, GAF Change was significant
with a t-test of -2.664, with a 2-tailed significance of 0.008 (see Appendix F: Table 5).
Within Diagnostic Codes, significantly different GAF scores between Group A
and B occurred for males in DC 3. GAF on Admission in Group A for males was 19.26
(SD 7.59), Group B scores were 14.79 (SD 4.72). T-test scores on this sample were
58

significant with a t-value of 3.354 with a 2-tailed significance of 0.001 (see Appendix K:
Table 10).
This data shows that overall, Group A patients entered the hospital with a
statistically higher GAF on admission than Group B. Additionally, Group A DC 3 males
entered the hospital with a statistically higher GAF on admission than Group B DC 3
males.
However, data suggest that there was no significant difference on discharge GAF
between Groups or Diagnostic Codes. This means that patients were discharged equally
well in both Groups. As a result, no further statistical analysis was conducted to evaluate
associations with GAF on Discharge.
Length of Stay
Mean LOS scores for the total sample were 14.45 (SD 12.27). Mean LOS scores
for the total sample of males were 14.43 (SD 11.70). Mean LOS scores for the total
sample of females were 14.47 (SD 12.98) (see Appendix D: Table 3).
Group A and Group B differed on LOS scores. Mean LOS score for Group A was
13.09 (SD 11.23). Mean LOS score for Group B was 16.00 (SD 12.23). Mean LOS score
for males in Group A was 12.57 (SD 10.33) and LOS score for Group B was 16.39 (SD
12.16). Mean LOS score for females in Group A was 13.61 (SD 12.07) and LOS score
for Group B was 15.20 (SD 12.43) (see Appendix D: Table 3).
Comparing means, t-tests confirmed statistically significant differences between
LOS for Group A and Group B with a t-test of -2.753, and a 2-tailed significance of 0.006
(see Appendix F: Table 5).
59

Within DCs, LOS was significantly different for males in DC 1. Group A mean
LOS was 14.92 (SD 11.32), Group B mean for males was 20.74 (SD 12.95). Comparing
means, t-value was -2.578 with a 2-tailed significance of 0.011 (see Appendix I: Table 8).
Total Events per Admission
Events were reviewed before statistical analysis. Data was provided with a tally
of total daily emergency medication administrations, four-point restraints, manual
restraints, and seclusion events. The EMR for this hospital requires separate entries for
each type of emergency event, even when they occur to the same patient at the same time.
For instance, manual escort to seclusion, placement in seclusion, manual restraint for
emergency medication administration and then the administration of emergency
medications would score as two manual restraints, one seclusion, and one emergency
medication event; totaling four events. However, as these events all occurred in the
context of one patient interaction that may have lasted less than five minutes, they are not
useful to consider in analysis as separate independent variables. Instead, totaling events
for a combined daily value provides for statistical power of number of emergency events.
For this analysis, Total Events per Admission (TEPA) were used for as a proxy for unit
aggression.
Mean TEPA scores for the total sample were 7.38 (SD 13.81). Mean TEPA scores
for the total sample of males were 8.46 (SD 14.80). Mean TEPA scores for the total
sample of females were 5.99 (SD 12.29) (see Appendix D: Table 3).
Group A and Group B differed on TEPA per admission scores. Mean TEPA score
for Group A was 2.24 (SD 4.44). Mean TEPA score for Group B was 15.93 (SD 18.94).
60

Mean TEPA score for males in Group A was 2.08 (SD 4.01) and TEPA score for Group B
was 16.32 (SD 18.94). Mean TEPA score for females in Group A was 2.40 (SD 4.84) and
TEPA score for Group B was 15.13 (SD 19.06) (see Appendix D: Table 3).
Comparing means, t-tests confirmed statistically significant differences between
TEPA for Group A and Group B with a t-test of -10.756, and a 2-tailed significance of
<0.001. Within DCs, TEPA was significantly different for both genders in DCs 1, 2, and 3
(see Appendix I, J, K: Table 8, 9, 10).
GAF Change per Day
To assess the impact of varying LOS and changes to GAF, a calculation produced
a data line of GAF change per day of admission (GAF/Day). Mean GAF/Day scores for
the total sample were 4.09 (SD 3.96). Mean GAF/Day scores for the total sample of
males were 3.95 (SD 3.77). Mean GAF/Day scores for the total sample of females were
4.29 (SD 4.19) (see Appendix D: Table 3). Between Group A and B t-tests did not
produce significant values. The t value was 1.157 with a 2-tailed significance of 0.248
(see Appendix F: Table 5).
Length of Stay per Years of Age
Age was statistically significant between groups, but in was not significant in any
DC. LOS was significantly different between Groups A and B, and in select DCs (DC 1
males), but not in all DC. To evaluate the relationship between LOS and age, a
calculation produced a data line of LOS/Age in Years (LOS/Age). This data provides the
mean number of days of hospitalization per the patient’s years of age at admission and
reflects differences in LOS by age in years.
61

Mean LOS/Age scores for the total sample were 0.40 (SD 0.38). Mean LOS/Age
scores for the total sample of males were 0.42 (SD 0.39). Mean LOS/Age scores for the
total sample of females were 0.37 (SD 0.37) (see Appendix D: Table 3).
Group A and Group B differed on LOS/Age per admission scores. Mean
LOS/Age score for Group A was 0.34 (SD 0.31). Mean LOS/Age score for Group B was
0.49 (SD 0.45). Mean LOS/Age score for males in Group A was 0.33 (SD 0.28) and
LOS/Age score for Group B was 0.52 (SD 0.47). Mean LOS/Age score for females in
Group A was 0.35 (SD 0.34) and LOS/Age score for Group B was 0.41 (SD 0.38) (see
Appendix D: Table 3).
Comparing means, t-tests confirmed statistically significant differences between
LOS/Age for Group A and Group B with a t-test of -4.295, and a 2-tailed significance of
<0.001. Within DCs, LOS/Age was significantly different for DC 1 males with a t-value
of -2.885 and a 2-tailed significance of 0.005 (see Appendix F: Table 5).
Total Events per Day of Admission
A calculation was required to assess if the increased TEPA had a statistical
relationship to the increased LOS. TEPA produces number of events, and LOS indicates
duration, however, a calculation was needed to assess number of events per day of
admission. The calculation of TEPA/LOS produced significant differences between
groups.
Mean TEPA/LOS scores for the total sample were 0.47 (SD 0.80). Mean
TEPA/LOS scores for the total sample of males were 0.54 (SD 0.89). Mean TEPA/LOS
scores for the total sample of females were 0.38 (SD 0.66) (see Appendix D: Table 3).
62

Group A and Group B differed on TEPA/LOS per admission scores. Mean
TEPA/LOS score for Group A was 0.16 (SD 0.30). Mean TEPA/LOS score for Group B
was 0.99 (SD 1.06). Mean TEPA/LOS score for males in Group A was 0.15 (SD 0.29)
and TEPA/LOS score for males in Group B was 1.02 (SD 1.11). Mean TEPA/LOS score
for females in Group A was 0.17 (SD 0.31) and TEPA/LOS score for Group B was 0.91
(SD 0.96) (see Appendix D: Table 3).
Comparing means, t-tests confirmed statistically significant differences between
TEPA/LOS for Group A and Group B with a t-test of -11.519, and a 2-tailed significance
of <0.001. Within DCs, TEPA/LOS was significantly different for DCs 1, 2, and 3 and
for both genders (see Appendix I, J, K: Table 8, 9, 10).
Correlation and Regression Analysis
Correlations
Data analysis showed significant correlations between LOS, GAF on Discharge,
TEPA and age (see Appendix E: Table 4). However, as previous data show increased
LOS in Group B and increased TEPA in Group B, positive correlations are expected
between LOS and number of emergency events experienced (see Appendix F: Table 5).
As a result, correlation analysis of this data show what descriptive statistical analysis
reveals and is not useful for establishing relationships. To further explore contribution to
variance in outcomes, linear regression was used.
63

LOS Regression: Total Sample
Linear regressions were used to predict contribution of the independent variables
to the dependent variable, LOS. Significant data includes the R square, F- Score,
unstandardized Beta coefficient, t score, with significance at the p = 0.050 level.
Group, Age, GAF on Admission, Total Events and Gender were used to predict
LOS on the total sample. The resulting model calculated an R Square of 0.330 for the
model. Analysis of Variance (ANOVA) predictions for this model calculated an F-score
of 59.406 (sig. <0.001). Independent variables that were significant predictors of LOS
included Group, GAF on admission, Total Events and Age. Gender was not significant as
a variable predicting LOS in the total sample (see Appendix M: Table 12).
LOS Regression: Groups A and B
Age, GAF on Admission, Total Events and Gender were used to predict LOS for
Groups A and B. The resulting model calculated R Square of 0.334 for Group A and
0.473 for Group B. ANOVA predictions for this model calculated an F-score of 47.175
(sig. <0.001) for Group A and 50.183 (sig. <0.001) for Group B (see Appendix N: Table
13).
Beta coefficients for Group A were significant for GAF on admission at -0.183
(sig. 0.004), Total Events with a Beta of 1.360 (sig. <0.001), and Age with a beta of
0.176 (sig. <0.001). Beta coefficients for Group B were significant for GAF on
admission at -0.227 (sig. 0.009), and Total Events with a beta of 0.452 (see Appendix N:
Table 13).
64

LOS Regression: Diagnosis Code 1 Male Gender
Using previous DCs significant t-test scores of LOS as a guide for significance,
regression for DC 1 males were used to compare Groups A and B. Independent variables
for this model were GAF on Admission, Total Events, and Age, with LOS as the
dependent variable.
Data from Group A, DC 1, Males produced an R square value of 0.371, with an F-
score of 9.222 (sig. <0.001). Significant coefficients for this model were Total Events
with a Beta of 1.429 (sig. <0.001) (see Appendix O: Table 14).
Data from Group B, DC 1, Males produced an R square value of 0.473, with an F-
score of 18.254 (sig. <0.001). Significant coefficients for this model were GAF on
admission with a Beta of –0.423 (sig. 0.045), Total Events 0.438 (sig. <0.001) and Age
0.174 (sig. 0.031) (see Appendix P: Table 15).
To further assess significance, regressions were done on this sample excluding
LOS outliers. The sample included males in DC 1 with a LOS less than or equal to 1.5
times the IQR over the 75% percentile or 46 days.
Data from Group A, DC 1, Males (LOS ,<=46 days) produced an R square value
of 0.284, with an F-score of 6.096 (sig. 0.001). Significant coefficients for this model
were Total Events with a Beta of 1.175 (sig. <0.001) (see Appendix Q: Table 16).
Data from Group B, DC 1, males produced an R square value of 0.384, with an F-
score of 11.859 (sig. <0.001). Significant coefficients for this model were Total Events
with a Beta of 0.358 (sig. <0.001). Age was very close to significant with a Beta of 0.142
(sig. 0.064) (see Appendix R: Table 17).
65

GAF on Discharge Regression Model
Regression models predicting GAF on Discharge with the independent variables
of Total Events, Gender, Age, and LOS produced analysis with very low R-Square
values. This was true for both Groups A and B for DC 1, 2 and 3. None of the models
were statistically significant. This data suggest that GAF on discharge is not dependent
on any unit variables; rather it is a clinical criterion for discharge, not subject to milieu
characteristics (see Appendix S: Table 18).
Regression Curve Estimation of Events Predicting LOS
To further assess the impact of emergency events on LOS, regression curve
analyses were performed on each diagnostic group. These analysis show that the models
that best predict the variance of LOS from number of emergency events are non-linear
(see Appendix U: Table 20).
Additionally, these analyses produce regression line equations with varying ‘x
multipliers’. The quadratic regression curve estimation equation for DX Code 1 was:
Y=9.42+0.84*x+-6.96E-3*x*x, for DX Code 2 was: Y= 9.42+0.32*x+1.41E-3*x*x, and
for DX Code 3 was: Y=7.28+0.25*x+2.4E-3*x*x. This analysis quantifies the differential
impact of emergency events by diagnostic code with patients with psychosis have the
largest ‘x multiplier’ (0.84x) in the regression curve estimation.
This analysis show that patients with psychosis have increased LOS variance
predicted by number of emergency events as compared to patients with bipolar disorder
or with major depressive disorder and that the cumulative impact is non-linear.
66

Chapter V:
Discussion
Milieu Characteristics
Providing patients with acute psychiatric needs with specialized care at the SH
both assured their safety, and resulted in regional hospital milieus that were less acute.
The closure of the State Hospital (SH) resulted in a redistribution of acute psychiatric
patients to regional hospitals. Such patients, prior to the closure of the SH, may have
initially been admitted to regional hospitals, and were then transferred to the SH due to
medication noncompliance or aggressiveness on the unit.
Data collected for this study document the change in milieu from pre-SH to post-
SH closure. Referred to as Group A (pre-SH closure) and Group B (post-SH closure),
these groups differed in age at admission, length of stay, GAF on admission, gender, and
primary diagnosis. Additionally, the Group A milieu had significantly fewer total
emergency events per admission then did the Group B milieu (see Appendix G: Table 6).
In an attempt to evaluate the impact of emergency events on psychiatric peers,
data selection attempted to remove outcome analysis of patients from the sample that
may have previously been transferred to SH. Applying this rationale, all patients
discharged to other healthcare facilities, other hospitals, or who left AMA were excluded
from both groups. Additionally, extreme length of stay hospitalizations (LOS> 66 days),
representing patients who were non-medication compliant, were excluded from both
groups for outcome analysis.
67

However, emergency events were not associated with any patient identifying
data. As such, all emergency events occurring on the unit were included in analysis
regardless of whether the patient involved in emergency events had been excluded from
the outcome analysis.
As reported previously in the results section, the Group B sample included a 41%
increase in the percentage of DC 1 patients, a 12% increase in DC 2 patients, and a 36%
decrease in DC 3 patients. This suggests that the Group B sample included significantly
more patients with psychosis and mania. Additionally, there were significantly fewer
patients with a depressive disorder. An associated finding was a statistically significant
difference in GAF on admission between Group A and Group B. The mean decrease in
GAF scores was significant only for males in DC 3. All other DCs were not statistically
different between Group A and Group B.
An additional change in the Group B sample was the distribution of male to
female patients: The Group A sample included approximately 50% male and 50%
females. The Group B sample was 67% male and 33% female. Another characteristic of
the sample was an overall statistically significant difference in male age with males 4.13
years younger in Group B.
Group B patients, overall, had a significantly longer length of stay. However,
this increased length of stay was statistically significant only for males DC 1, with a
mean increase of 5.82 days or a 39% longer admission.
For all patients in Group B, an increase in total emergency events was recorded.
Mean total events increased from approximately 2.25 per admission in Group A, to
approximately 15.93 per admission in Group B. This represents more than a sevenfold
68

increase in emergency events on the unit that would have been experienced/observed by
the patients per admission.
To summarize the differences between Group A and Group B, the Group B
sample was younger, more male, had more patients with psychosis and mania and less
with depression, those males who were depressed had lower GAF on admission, male
patients with psychosis had increased length of stay, and all patients experienced more
emergency events per admission.
Factors Associated with Patient Outcomes
Reviews of previous work suggest that diagnosis does predict LOS, with patients
with psychotic disorders having increased LOS, but may be moderated by social support
and behavioral manifestations during hospitalization. (Tulloch et al., 2011; Zhang et al.,
2011). Data from our sample confirm that Group A LOS varied by DC with DC 1 LOS
longer than others. Group B LOS, was significantly longer only for DC 1 with an
increase of 4.35 days or 28% increased LOS. More notably, the increase in LOS for
Group B DC 1 males was 5.82 days or 39%, while the increase in LOS for Group B DC 2
males was less at 28% (see Appendix I: Table 8). Small sample size may contribute to
the non-significant results of increased LOS for females in these respective DCs (DC 1
Female N= 28, DC 2 Females N = 22).
GAF on admission was only significantly different for DC 3 males. Data suggest
that Group B DC 1 patients did not enter the hospital less well then their Group A
counterparts (as measured by GAF). Previous studies have associated a patient diagnosis
of psychosis, being of female gender and admission into a larger hospital size with
69

increased in LOS (Tulloch et al., 2011). Female gender and hospital size do not explain
the variance in LOS of Group B DC 1 males.
Possible explanations for the increase in LOS for DC males with an increase in
total events may include the interpretation of stressors, stress management style, and
impact on social support associated with the increased total emergency events
experienced by Group B.
Previous data suggesting that predictors of LOS in mental health admissions
include a diagnosis of a psychotic disorder, being of female gender, and admission into a
larger hospital (Tulloch et al., 2011), may give evidence to a common factor associated
with LOS, that is, coping style associated with stress accommodation.
Stress
Largely understood to be relative, stressors in the environment are appraised by
individuals in the here-and-now. This evaluation weighs the stressor in the context of the
potential impact to do harm, threaten, or make a challenge, balanced by the resources at
hand to meet the threat or to reduce harm. This evaluation is considered an appraisal
and occurs multiple times during the experience of a stressor: Initially to evaluate risk,
and then secondarily to assess impact of coping tools on the continuing stressor (Glanz et
al., 2008). This appraisal is a function of biological, psychological, environmental, and
social factors. These factors participate in the appraisal process, i.e, ‘What is the risk?’.
Additionally, these factors contribute to the assessment of coping resources, i.e. ‘How can
I solve this?’. As such, a key element of the appraisal is evaluative, a process that
70

requires intact mechanisms that attend to the stressor, and the ability to use cognition to
arrive at a solution.
However, the psychological and physiological impact of stress is to activate the
hypothalamus-pituitary-adrenal (HPA) axis, produce changes in attention (either
increased or decreased), decrease working memory, increase subjective anxiety, trigger a
recall of previous trauma, promote habitual response, and decrease both judgment and
capacity to make decisions (Horan & Blanchard, 2003; Staal, 2004). These changes
decrease one’s capacity to have alternatives to respond to stress. Individuals have unique
and variable techniques to respond to stress, and are thought to develop and use various
coping tools.
Coping
Defined as the “constantly changing cognitive and behavioral efforts to manage
specific external or internal demands” (Matud, 2004, p. 1403), coping styles vary, and are
associated with certain personal characteristics.
Data suggest that men more often use coping styles that are focused on solutions
to problems, and women more often use coping styles that assist in management of
emotional responses to stress (Matud, 2004). This data suggest that solutions-based
coping may attend more to risk and outcomes associated with the stressor, and emotional
based coping maintains attention on the subjective feelings associated with the stressor.
Data evaluating the impact of stress on gender suggest that women experience more
stress then do men, but does not associate this stress with coping style (Matud, 2004).
71

Dependent on physical and mental health, social support, and resources in the
environment, individuals often use a variety of coping styles at different times to
optimize response to a stressor. However, when health is less robust, social support is
lacking, or when the environment does not support coping solutions, responses to
stressors suggest less effective coping and greater subjective distress (Horan &
Blanchard, 2003; Matud, 2004; Ossman & Mahmoud, 2012; M. S. Ritsner & Lysaker,
2011).
Emotional Reactivity and Psychosis
Although not considered an emotional disorder, patients with schizophrenia are
highly responsive to emotionally laden stimuli. Neurobiological hypotheses for psychotic
symptomology suggest that increased responsiveness to dopamine is partially responsible
for psychotic symptoms (Sadock et al., 2007). This correlates to findings that increased
psychological stress results in increased secretion of dopamine (Soliman et al., 2007).
Observed milieu aggression, and the increased presence staff to address emergency
events, may provide a significant psychological stress to patients with psychosis. This
would result in increased dopamine secretion, resulting in increased symptomology.
Patients with schizophrenia have increased emotional responses to normal daily
stress, resulting in “increased negative mood and decreased positive mood” (Horan &
Blanchard, 2003, p. 272). Increased negative mood is associated with activation of the
HPA axis mediating the response to stress, decreasing the capacity for solution based
stress coping. Daily life stressors, associated with decreased tolerance to stress in
psychotic individuals, is associated with increased levels of psychotic experience (Collip
72

et al., 2013). Social stressors, in particular, are associated with increased psychotic
symptomology (Docherty et al., 2009).
Diathesis-stress models are used to explain expression and management of
psychotic symptoms (Lincoln, Peter, Schäfer, & Moritz, 2008) and serve as a proposed
mechanism explaining the process of stressors causing increased symptoms (Horan &
Blanchard, 2003; Ventura, Nuechterlein, Subotnik, Green, & Gitlin, 2004). This suggests
that variance in coping strategies to psychological and social stressors may impact
susceptibility to stress (Horan & Blanchard, 2003).
Data support that patients with schizophrenia use emotional based coping
mechanisms more frequently than they use solution based coping strategies. (M. S.
Ritsner & Lysaker, 2011). This implies that coping is focused on managing the response
to stressors rather than appraising the stressor and seeking a solution that manages the
stressful situation itself. Further, this data suggest that this patient population uses
emotional based coping predictably over time, with little evidence of variability in coping
strategy employed (M. Ritsner et al., 2003).
Studies suggest that emotional coping strategies are less adaptive (as opposed to
task oriented problem solving) and may result in increased somatic complaints and more
psychological distress (Matud, 2004). Additionally, emotional based coping in this patient
population is associated with increased dysphoria, emotional distress, and overall
decreased quality of life (M. S. Ritsner & Lysaker, 2011).
Further data suggest that paranoia is a mediating response to anxiety and results in
ineffective coping in patients with psychosis (Lincoln et al., 2008). For this patient
population, increased psychological and social stress, with resulting increased anxiety
73

and paranoia, is also associated with increases in delusional thinking (Lincoln et al.,
2008), further contributing to anxiety and the need for coping mechanisms. However,
cause and effect is not clear in the pathway of stress and psychotic symptomology, and
further studies need to explore moderating influences.
Of interest to this study, data suggest that individuals with non-affective psychosis
are more vulnerable to the effects of stressors than those with bipolar affective disorder or
major depressive disorders (Myin-Germeys et al., 2003). The decreased resilience to
stress tolerance is hypothesized to be associated with psychotic symptoms and recurrence
of psychotic symptoms associated with stress (Myin-Germeys et al., 2003). This
hypothesis is supported by data that suggest that psychotic relapse is associated with
increased emotional response to stressors (Docherty et al., 2009).
Unit Events
Emergency events (defined as events during hospitalization that that pose
imminent risk of harm to self or other and require immediate interventions by staff) are
often preceded by patient escalation and agitation occurring in the milieu. As such,
psychiatric peers will often be in close proximity to an escalating patient, and may feel
that their environment is less safe.
For patients with psychosis, increased negative symptoms are associated with
decreased ability to redirect attention from stressful stimuli. Such patients may continue
engagement with stressful thoughts and attention when presented with stressful stimuli
(Strauss, Llerena, & Gold, 2011). Maintaining a focus on stressful environmental stimuli
may require an additional cognitive burden, and decrease the capacity to respond to
74

“positive cues” available in the patients surroundings (Strauss et al., 2011, p. 223).
Coupled with an emotional coping style, the inability to redirect oneself from attention on
stressful stimuli may contribute to a prolonged period of stress following the witnessing
of an emergency event in the milieu.
Support in Stress Accommodation
Data strongly support that social support is a factor in coping and LOS for
patients with schizophrenia. Increased access to social support is negatively correlated
with LOS, is associated with decreased psychotic symptomology, improved capacity to
problem solve, and impacts quality of life (M. Ritsner et al., 2003).
When unit emergency events occur, social support can assist in an appraisal of
the threat, assist in problem solving solutions, and redirect attention from a focus on the
stressful event. This type of social support may be more focused on problem-based
coping, producing less emotional distress than emotional based coping (Collip et al.,
2013; Docherty et al., 2009; Horan & Blanchard, 2003; M. Ritsner et al., 2003; Strauss et
al., 2011). In this way, social support is a mediator of coping. (Glanz et al., 2008).
Three broad types of social support are understood to be of benefit to mental health
patients: Peer support, family and friend support, and professional support.
Peer (or mutual) support is characterized by support from people with serious
mental illness who offer themselves to those that are “not as far along in their own
recovery process” (Davidson, Chinman, Sells, & Rowe, 2005, p. 444). This type of
support is found to play a significant role in recovery from mental health disorders
(Pistrang, Barker, & Humphreys, 2008; Repper & Carter, 2011). Associated with
75

decreased neurotic distress, medication usage, improved well-being for those that
participate regularly in peer groups, giving and receiving support are associated with
improved outcomes (Pistrang et al., 2008, p. 114) Operationalized to provide empathy,
role modeling, expert advise and stress tolerance, this type of support may be considered
as a type of mental health care in it’s own right (Davidson et al., 2005, p. 443).
Ongoing support from family and friends (or social support) is similarly
associated with recovery from mental illness. This type of support provides emotional
support, provides support to self-esteem, provides practical support in living, and
provides a context for quality of life.
Evidence of the value of social support is data that show that social isolation
predicts poor outcomes for those recovering from schizophrenia. (Evert, Harvey,
Herrman, & Trauer, 2003). Among the factors important in this support include
“opportunities for social interactions”, which are casual and frequent (Harvey, Jeffreys,
McNaught, Blizard, & King, 2007, p. 352).
Professional support includes all those that are trained in providing care. This
support may be pastoral, occupational, and medical, psychological, and nursing to name a
few. On the inpatient unit, staff may provide one-to-one interactions, participate in
groups, lead groups, manage the milieu, or be involved in assessment and interventions.
The overall focus of nursing in milieu management is a “ focus on the mental health
continuum and emphasizes wellness and adaptation in the community and within a social
and cultural context” (Psychiatric nursing, 2008, p. 987). The unique perspective of
psychiatric nursing of the milieu is derived from a recognition that “a supportive and
76
therapeutic milieu is an integral part of healing and restoration of mental health”
(Psychiatric nursing, 2008, p. 988).
Unit Events Impact on Milieu and Social Support
Units high in aggression or agitation may have a negative impact on an milieu
atmosphere. This may decrease opportunities for social interaction with peers, friends
and family and staff. The milieu may not be a relaxed or safe environment, peers may be
struggling with their own reactivity to observed agitation or aggression, and family may
not feel comfortable visiting a unit that may not feel safe. Additionally, staff that is
managing patient escalation may be ‘on alert’, may not be able to be calming, supportive
presence for patients that are struggling to form a coping response to a
social/environmental stressor. Data suggest that just as emergency events are stressful for
patients, they are stressful for staff as well (Bower et al., 2003). This may result in staff
having increased vigilance, may be more circulating in the unit and less available for
relaxed conversation, and may manage the milieu by directing patients to their own
rooms for safety.
Overall, a more acute milieu may have an impact on the coping resources
available to patients. This may result in increased stress, increased symptomology, with a
resulting impact on treatment outcome.
77

Suggested Explanations for Data Result
Stress Vulnerability
Increased unit events caused an increase in stress with a resulting need for
increased utilization of coping strategies. DC 1 patients are more likely to use emotional
based coping strategies that are associated with increased duration of attention on
stressor, increased dysphoria, increased somatic complaint and increased psychotic
symptomology. Additionally, increased events may produce a physiologic response that
exacerbates presenting symptoms. This may result in increased LOS for this population,
as the therapeutic environment itself was a cause for symptom expression, thus delaying
clinical improvement. As previously mentioned, stress vulnerability is a unique feature
of this DC and would explain why the increased total events in Group B did not result in
significantly increased LOS for DC 2 or 3.
Decreased Coping Resources from Peers and Family
Psychiatric peers support each other as they interpret the milieu. With decreased
percentage of non-psychotic peers in Group B DC 3, (<36%), and an increase in manic,
and psychotic peers, there was a reduced milieu resource for support and cognitive
appraisal of stressors. Data analysis of Group B DC 3 patients showed lower GAF on
admission. This may have contributed to a milieu with less well peers, thus contributing
less support to peers during stressful events. Additionally, during periods of unit
escalation, it is possible that friends and family made shorter visits, or reduced visit
frequency altogether.
78

For Group B DC 1 male patients, increased total events during admission
required increased need of appraisal support and redirection of attention from unit
stressors. Lack of such support may have increased symptomology and resulting LOS.
Decreased Coping Support From Staff
Data strongly support that unit emergency events have a stress impact on staff. As
a result, the staff experience of increased unit aggression may have reduced their capacity
to be ‘calming resource’. This may also have served to decrease access to an appraisal
and redirection resource for Group B DC 1 male, thus increasing LOS.
Implications for Practice
Unit milieu variables, especially unit aggression that result in emergency events,
have clinical implications for patients with psychotic disorders. This exposure may
increase LOS, or otherwise complicate course of treatment. This study suggests that
patient profile, including the number of patients on the unit that are aggressive and the
relative mix of mental health diagnosis, have an impact on psychiatric peers. The
contribution to psychiatric peers outcomes may be moderated by coping demands in
response to stress and moderate coping resources during hospitalization.
More importantly, this data supports the conclusion that the neurobiological
source of symptoms must be a critical factor in milieu selection for patient placement.
While a unit characterized by frequent emergency events may have little impact on one
diagnostic group, the same milieu is, in fact, harmful to other diagnostic groups. This data
has implications for practice ethics, health policy, and nursing education.
79

Ethical Considerations
Implicit in the professional ethics and scope of practice for nurses is a mandate to
preserve the dignity, rights, and autonomy of our patients. Professionalism requires us to
advocate for patient protection and best outcomes at both institutional and policy levels.
If data support that number of emergency events increases LOS for psychotic
male patients, then as health care providers, we have a responsibility to our patients to
reduce exposure to a critical number of emergency events. However, as emergency
events on the unit may be associated with patients exercising their right to refuse
medications, milieu management may include restricting the number of very acute
patients on the unit in order to facilitate best outcome for peers. This solution would
result in displaced acute patients having lengthy stays in emergency departments or other
non-therapeutic environments when beds are not available.
An alternative approach has equally difficult implications, and that is to limit the
duration of untreated psychosis on inpatient units. Our professional mandate to avoid
maleficence could be construed to mean that complicity with non-medication adherence
exposes psychotic patients to the negative effects of untreated psychosis, the traumatic
exacerbation of hallucinations, and the trauma of unnecessary emergency events.
Balancing patient autonomy, rights to refuse medication, beneficence and non-
maleficence require a comprehensive assessment of resources and rights.
Demands for distributive justice impact decisions of resource allocation: If LOS
is increased for psychiatric peers exposed to increased number of emergency events, then
we are increasing costs of treatment, decreasing number of beds available to treat other
80

patients, and overall, depriving the health care system of resources. Thus, individual
autonomy has an impact on others that require access to health care resources.
If increased aggression results in poorer outcomes for peers, policies at the
institutional, state, and national level should address the shared resource of therapeutic
milieu as a “public good”. As such, individuals must be provided best access to this
resource for mental health recovery. Prolonged delay of therapeutic initiation must be
balanced with appreciation for impact on those seeking medical care. Distributive justice
demands “allocation of resources and the collective, rather than the individual rights of
society”(Psychiatric nursing, 2008, p. 202) as a guiding principle.
At the least, this data support increased communication between providers,
payers, policy makers, and patients. This could include proactive agreements between
patients and providers to clarify treatment options for future need. If the increased events
are associated with medically untreated patients, then perhaps drafting a psychiatric
advance directive at time of discharge could assist in more timely administration of future
medications if readmission occurs, thus reducing emergency events, and sparing
resources.
Other suggestions for practice include the creation of units that can segregate
patients who frequently escalate, provide additional space for movement, or manage
other unit structural issues to maximize opportunities for peers to not experience the
stress associated with unit escalation. Units need to implement strategies, resources,
milieu management to reduce number of emergency events on Inpatient Psychiatric
Units. This suggests changes to health care policy at the state and local level.
81
Policy
Examining the variables of therapeutic milieu, data from this study support
previous work associating unit satisfaction with outcome. Data presented suggest that the
milieu variable of aggression and emergency events have an impact on patient outcomes,
advancing the knowledge gap in milieu variables argued for by Vaglum et al (1985).
This study provides support to a quantifiable milieu impact of emergency events on LOS
for psychotic males. From a nursing practice perspective, patient advocacy suggests that
our milieu management should focus on decreasing exposure to, and supportive recovery
from milieu agitation associated with emergency events.
As suggested earlier, the impact of unit aggression by non-medicated patients on
the course of symptoms for patients with psychosis could inform patient rights, advocacy
and health policy. The patient’s right to refuse treatment, and to then contribute to a non-
therapeutic milieu, could lead to policy discussions that either expedite patient
competency hearings and resulting court-ordered administration of medications, or
require that patients who do choose to not accept medications and are significant
contributors to unit aggression be placed in units specifically designed for their care.
Such units would minimize contact with patient populations that are vulnerable to
negative impact from unit aggression.
Stakeholders at the policy level include the patients, families, health care
providers, insurers, community at large, and related interest groups. Current discussion
between these groups focuses on balancing the risk-benefit evaluation associated with
psychotropic medications, community resources, and concerns about safety. This
discussion is significantly informed by an appreciation of the adverse effects associated
82

with psychiatric medication administration, and incremental improvements in mental
health associated with these medications: Patients with psychotic disorders do not have
complete recovery of illness, nor are they “cured” by treatment. Rather, the longitudinal
course of untreated schizophrenia, for example, is a progressive neurologic decline,
balanced with the protective effects of medication that reduce neurologic decline, but
often provide significant adverse effects. Policy decisions require sensitivity to the
patients right to choose quality of life, and the communities right to distribute resources
and ensure safety.
Decreases in access to inpatient beds fro psychiatric hospitalization must
contribute to the stakeholder conversation on policy for medication administration.
Increased unit aggression (associated with medically untreated patients) results in poorer
outcomes for peers. Therefore, policies at the institutional, state, and national level
should address shared resource of therapeutic milieu as a “public good”, and individuals
must be provided best access to this resource for mental health recovery. Prolonged
delay of therapeutic initiation must be balanced with appreciation for impact on those
seeking medical care.
Nursing Education
This study refutes the perspective of the milieu as irrelevant, as an non-
therapeutic intervention (Mahoney et al., 2009). This data suggest that the milieu can be
harmful to psychiatric outcomes. If that is the case, then the milieu can also be
therapeutic, thus affirming the milieu role as an intervention during psychiatric
hospitalization.
83
Evidence from this study informs curriculum change in nursing education. If a
significant contribution to LOS outcome of patients with psychosis is attributable to
challenges with stress and coping, then the milieu as a therapeutic intervention would
include adaptive support from nursing staff. Nursing education must focus the use of
stress and coping assessments, interventions, and evaluations, reflecting patient diagnosis
as a variable in outcome.
Staff support measures includes the recognition of the special coping needs of
psychotic patients, and provide additional coping support, redirection, and family support
during times of unit aggression to this population. This provides additional coping
resources when other attempts to reduce exposure to stressors have not been sufficient.
Specific implications to nursing education include assessments and interventions
to support psychiatric peers as they adapt to milieu stressors. Supportive interventions
may include peer support/unit mix for optimal recovery, active inclusion of family and
friend support with special environments or accommodations, and interdisciplinary
approaches to stress accommodation.
Implications for nursing research support the need to develop a relative coping
tool and relative coping theory for psychotic patients. This tool would utilize a
quantifiable algorithm of PRN medications administered for anxiety and pain, sleep
records, socialization with others, attendance to self-care, appetite, restlessness/agitation,
change in psychotic symptomology, tolerance for communication and changes to vital
signs to create a relative coping value. Such a tool could assist staff in quantifying the
changes in stress-burden of patients on an acute unit, and support interdisciplinary
interventions.
84

Current nursing models and theoretical frameworks that explain stress and coping
utilize cognitive approaches as a variable in stress appraisal and accommodation. These
models do not specifically address the challenges to cognitively compromised psychotic
individuals, nor do they address source of stressors when they appear as part of a
psychotic symptomology. Nursing theory could benefit from an approach that leads to
interventions with an appreciation for psychotic symptomology stressors within a stress
and coping model.
In addition to providing support during periods of stress for patients, nursing
education must stress practice principles that reduce unit aggression and emergency
events before they occur. This education would include focused education to understand
the cycles of patient escalation and primary prevention that would reinforce the necessity
of interdisciplinary collaboration; both of which are found to be crucial elements in
reducing emergency events in psychiatric facilities (American Psychiatric Association,
American Psychiatric Nurses Association, & National Association of Psychiatric Health
Systems, 2003)
Data from this study have implications for nursing care of psychiatric patients
experiencing unit aggression and milieu stress. Addressing policies that reduce unit
aggression, improving awareness of the negative impact to peers, utilization of supportive
coping therapies, and improved assessment of milieu coping may have significant
benefits to psychiatric outcomes. Improved LOS outcomes for psychotic patients would
decrease exposure to the risks associated with hospitalization, would increase access to
hospital resources for other patients, and would decrease obstacles to patients seeking
care.
85

Limitations
This retrospective study evaluated the impact of emergency events occurring on
an inpatient psychiatric unit on the outcomes of psychiatric peers. The goal of this study
is not to establish cause and effect, as measuring outcomes after an intentional exposure
to a harmful milieu variable would require a randomized controlled study; this would be
unethical. While this study does support a relationship between events and LOS
outcomes, several limitations restrict this study, and the specific LOS results are not
generalizable to other units. Such limitations to generalizability include variability in
health care policy, staff training, unit facilities, and unit size. However, this study does
support the conclusion that unit emergency events are a stressor which negatively impacts
the course of recovery for male patients with psychosis. As such, this data are
generalizable to psychotic males experiencing emergency events during an inpatient
admission.
This retrospective, naturalistic sample of the total population during study period
limited the researcher to the number of available admissions and time constraints
associated with the data set. This sample size is too small to suggest outcomes for other
diagnostic populations, as small sample size may have reduced statistical significance for
outcomes in DC 2 and 3 and for female gender: These groups did show increased LOS,
but were not statistically significant.
GAF on admission is recorded as a range, rather than as a discrete number value.
This may have masked actual GAF on admission between populations. The most
common admission GAF score for DC 1 patients was 11-20. It may have been the case
that Group A patients had a mean GAF on admission closer to 20, and Group B patients
86

had a mean GAF on admission closer to 11. This would have partially explained the
increased LOS, but this cannot be explored with the present data.
An additional limitation was the decision in this study design to not exclude
patients that were directly involved in emergency events from the outcome analysis. Data
support that emergency events are associated with increased LOS for patients involved in
emergency events. A goal of this study was to study the LOS impact on peers that are in
the milieu when emergency events occur. One could argue that only non-participatory
patients would measure the true effect of an agitated milieu on LOS outcome. However,
research does show that emergency events on a unit is a contributor to unit disorder and a
predictor of future emergency events (S. D. M. Thomas et al., 2009). This could further
the argument that the stress caused by emergency events impacts stress and coping
mechanisms and causes additional individuals to participate in emergency events. To
exclude this population would skew the data to assess only those that have effective stress
and coping mechanisms. With a goal of evaluating impact of emergency events on
psychiatric peers, inclusion of all patients in milieu must be part of the outcome analysis,
regardless of effectiveness of coping with milieu stressors.
Staffing variables are not included in this study. This unit experienced a change
in designated staff to patient ratios, increased utilization of mental health technicians, and
staff were provided both with direct experience and in-service education that could have
had an impact on LOS outcomes and unit aggression and management. While it is most
likely that improved management of aggressive patients occurred in Group B, thus
potentially decreasing LOS, this variable was not controlled and would be difficult to
quantify.
87

This unit was in a teaching hospital, and no inclusion of staff experience, presence
of students, annual cycle of resident rotation were included. However, previous
researcher have identified that LOS is not affected by teaching hospital status (Tulloch et
al., 2011).
LOS has been associated with source of payment. No accounting for this variable
was included in the outcome analysis. Additionally, mental health policy has impacts on
patient’s rights, LOS, access, and payment sources. Current change to health care policy
and treatment of mental illness may make future comparison difficult, and limit studies to
retrospective analysis. Changes to patient advocacy and state policy were not included in
this analysis and may have impacts on admission and discharge plans.
88

Suggestions for Further Research
While this data is supportive of an association between psychiatric outcomes
measured by LOS and unit emergency events, using additional retrospective studies could
further explore this association. If the hypothesis, that stress is a mediator in LOS of
mental health patients is true, then future research that correlates biological and treatment
based markers of stress with emergency events could further our understanding.
Retrospective studies that investigate the relationship with vital signs, somatic
complaints of pain, validated stress assessment tools, and frequency of PRN anxiolytics
and pain medications, correlated with date and times of emergency events could provide
objective data for stress tolerance and coping demands.
Data that evaluates attendance at group sessions, number of family visitors,
number of patients in milieu and number of phone calls by patients, could help to identify
access and utilization of coping resources. A secondary source of coping resources could
include objective assessments of time staff has to participate in patient interactions; this
variable may be affected by unit characteristics.
Additionally, studies could explore the relationship to diagnosis category as a
percentage of unit populations as a variable in LOS. Data from this study is supportive
that DC distribution is a variable, perhaps impacting coping during stressful events.
These studies should include multi-site evaluations, and strive to maximize
number of subjects. This study did show differences in outcomes for other DC codes and
for female gender, however statistical significance was not achieved due to lack of power
of study size. Previous data analysis suggest that LOS studies should have patient
89

samples of over 3,000 subjects, a sample size not available for this study (Tulloch et al.,
2011).
An alternative approach to study could include data that compare variables before
and after a unit introduces new coping support programs. Such programs could include
nurse led daily stress and coping groups, access to quite spaces, segregation of disruptive
peers, and designated family meeting rooms when milieu does not impact quality of
social support.
Conclusion
Using a naturalistic sample in a milieu that experienced dramatic change provided
an opportunity to retrospectively explore milieu variables associated with LOS and GAF.
The hypothesis that emergency events would be predictive of LOS and GAF was
supported by this study. LOS was significantly increased for a subset of the population,
and this unit had a change in GAF on admission during periods of increased unit
emergency events. These data samples were limited by constraints of size and period of
time available for study. This small sample, did however, suggest that an objective
relationship exists on the LOS for male patients with psychosis when exposed to
increased unit stress, a relationship previously explored based on subjective data (Melle
et al., 1996; Røssberg, Melle, Opjordsmoen, & Friis, 2006). Further study must be done
to explore this correlation, appreciate it’s magnitude, and understand who is vulnerable to
impacts of this type of stress.
Potentially, this data could inform change in treatment parameters for mental
health patients, based on individual diagnosis. This data supports the conclusion that
90
individual patient diagnosis be a factor in milieu selection, as milieu variables impact
LOS. This consideration of unit selection would be based on the individual patient’s risk
for impaired coping, resulting in increased symptom expression.
This data could have significant impact on health care policy, tolerance of
duration of untreated psychosis, development of milieu structure and patient composition,
and of patient bed assignment. In the short term, this study is suggestive that health care
providers initiate programs to assist in stress and coping of peers that observe milieu
emergency events, and provide supportive redirection from a focus on stressors, cognitive
reappraisal of stressors, and problem based coping strategies to psychotic males on
inpatient units.
91

Appendix A
Figure : Global Assessment of Functioning Scale
Global Assessment of Functioning Scale: American Psychiatric Association, & American Psychiatric Association. (2000). Diagnostic and statistical manual of mental
92

disorders: DSM-IV-TR (4th ed., text revision.) pg. 34. Washington, DC: American Psychiatric Association.
Appendix B
Figure : Stress Diathesis Model of Suicide
Stress Diathesis Model of Suicide: Hawton, K., & Van Heeringen, K. (2009). Suicide. Lancet, 373, pg. 1375.
93
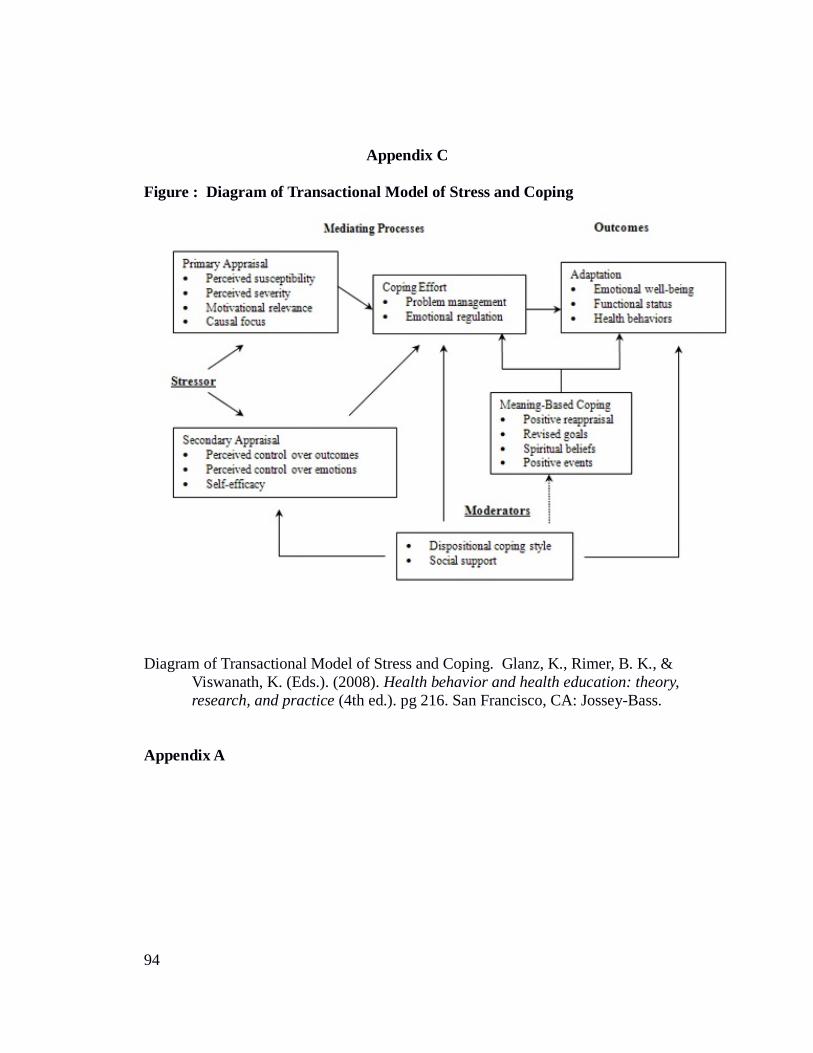
Appendix C
Figure : Diagram of Transactional Model of Stress and Coping
Diagram of Transactional Model of Stress and Coping. Glanz, K., Rimer, B. K., & Viswanath, K. (Eds.). (2008). Health behavior and health education: theory, research, and practice (4th ed.). pg 216. San Francisco, CA: Jossey-Bass.
Appendix A
94

Appendix D
Table
95

Appendix E
Table
96

Appendix F
Table
97

Appendix G
Table
98

Appendix H
Table
99

100

Appendix I
Table
101
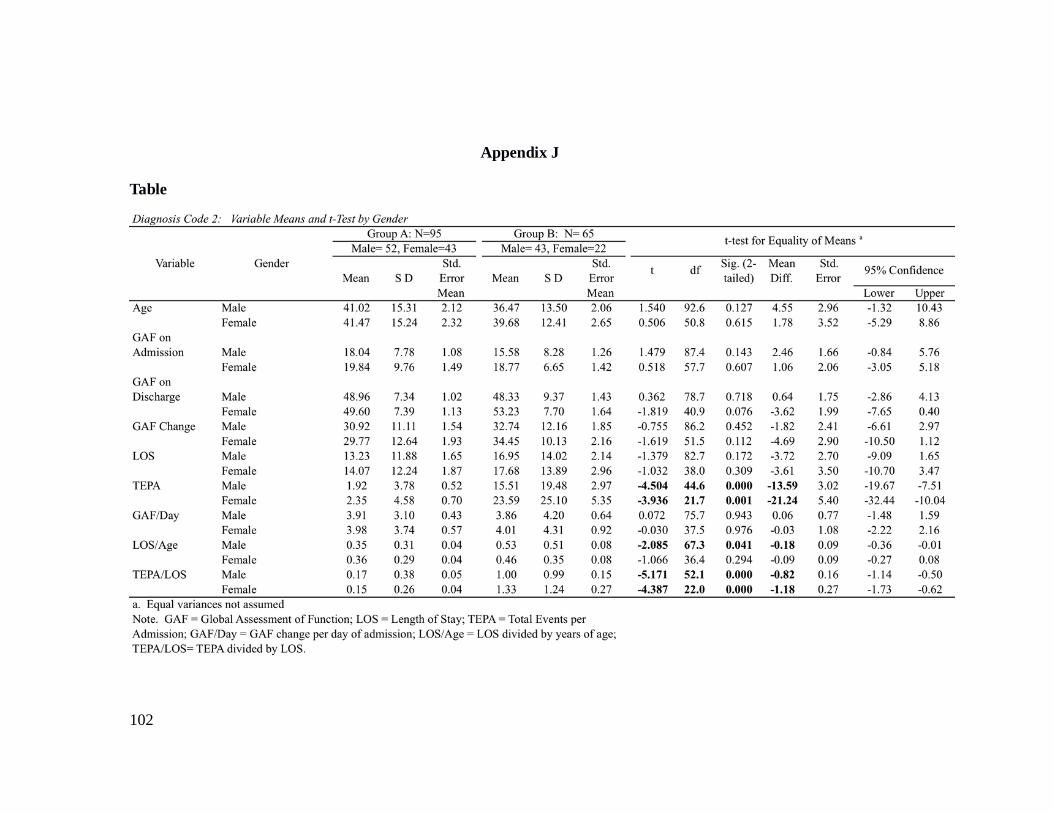
Appendix J
Table
102

Appendix K
Table
103

104

Appendix L
Table
105

Appendix M
Table
106

Appendix N
Table
107

Appendix O
Table
108
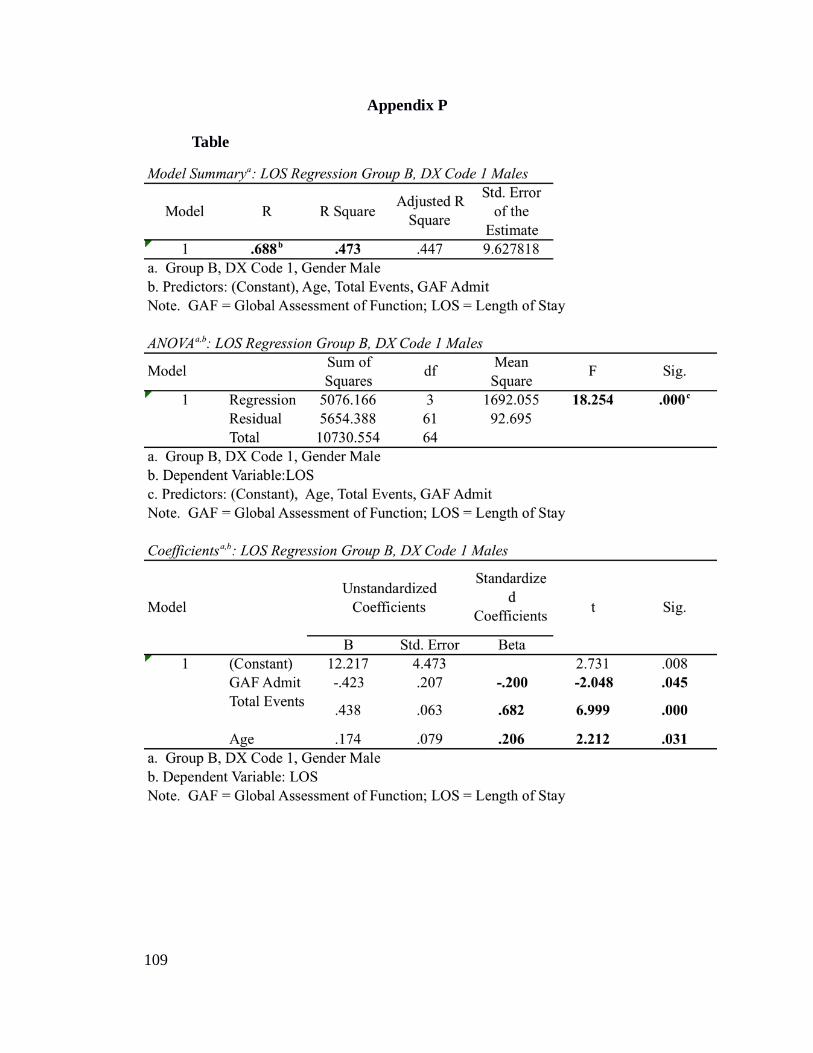
Appendix P
Table
109

Appendix Q
Table
110
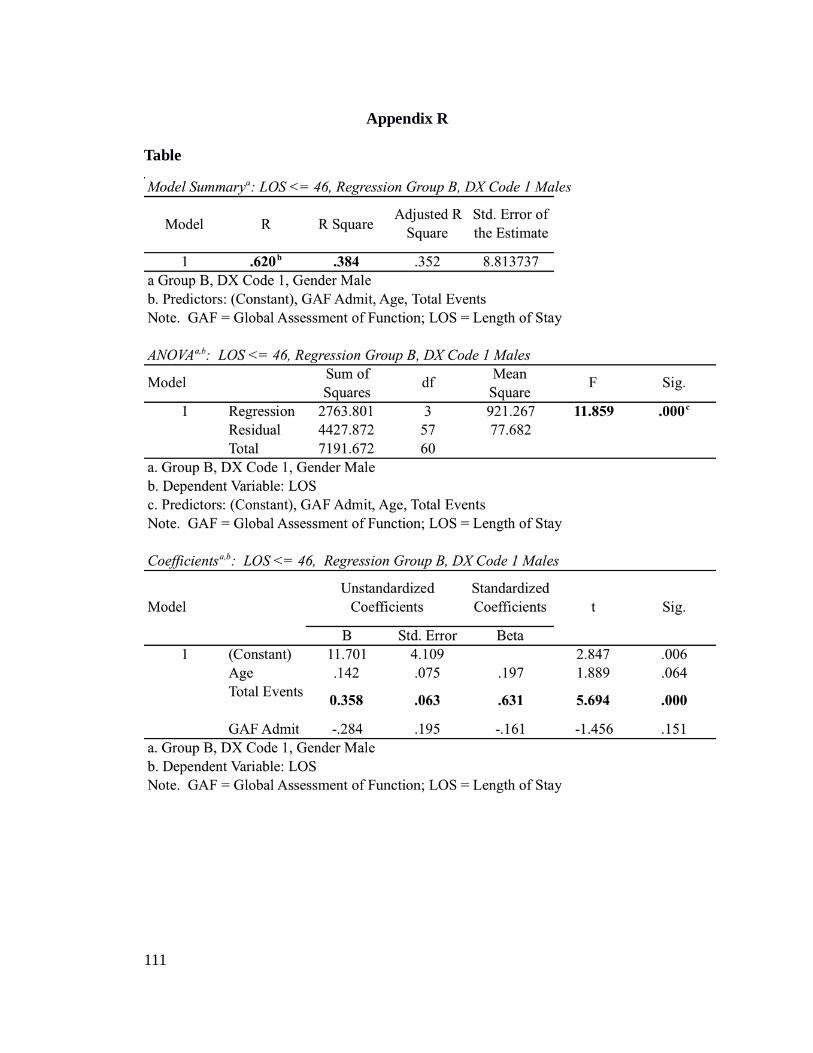
Appendix R
Table
111
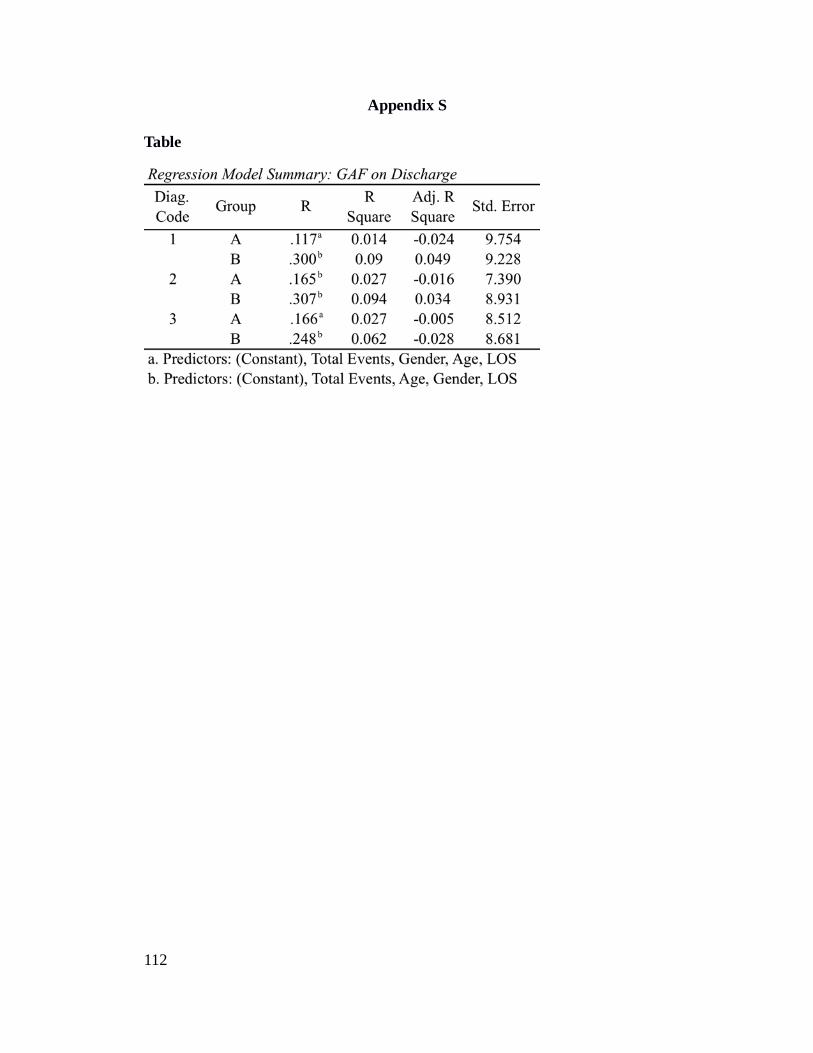
Appendix S
Table
112

Appendix T
Table
113
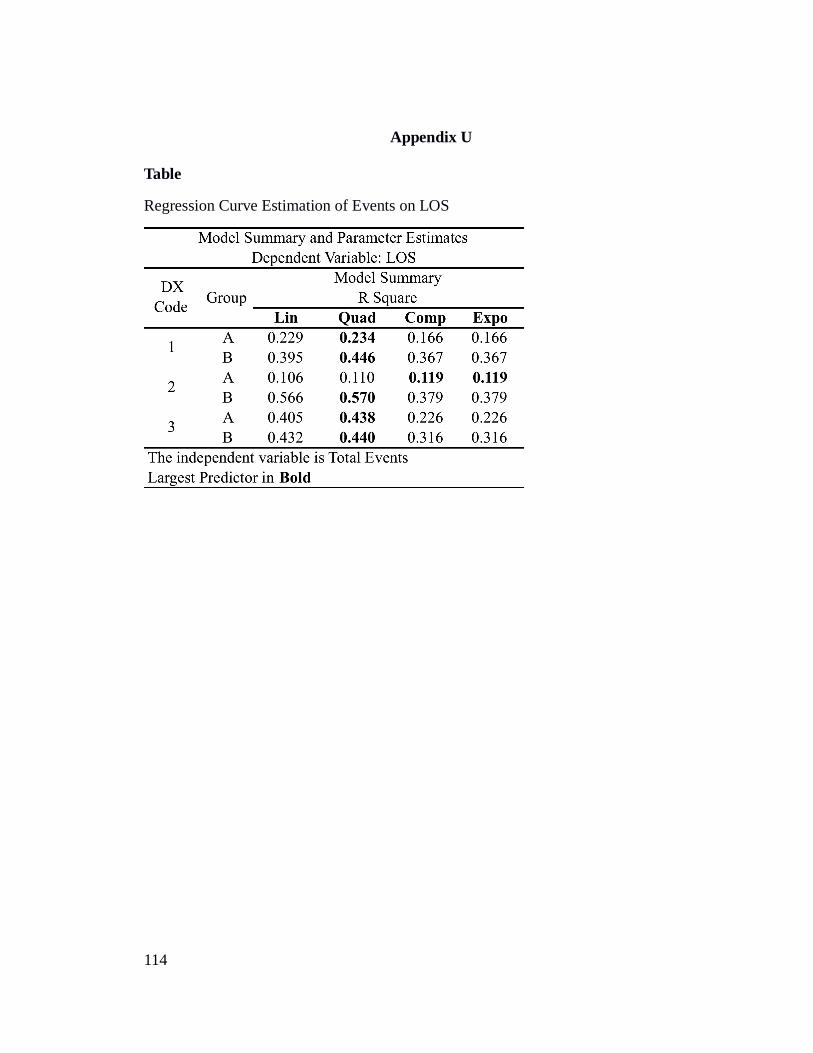
Appendix U
Table
Regression Curve Estimation of Events on LOS
114

References
Aas, I. M. (2010). Review Global Assessment of Functioning (GAF): Properties and
frontier of current knowledge. doi:10.1186/1744-859X-9-20
Abroms, G. M. (1969). Defining Milieu Therapy. Archives of General Psychiatry, 21(5),
553. doi:10.1001/archpsyc.1969.01740230041006
Allen, M. H., & Currier, G. W. (2004). Use of restraints and pharmacotherapy in
academic psychiatric emergency services. General Hospital Psychiatry, 26(1),
42–49. doi:10.1016/j.genhosppsych.2003.08.002
American College of Emergency Physicians. (2012). The ethics of Health Care Reform:
Issues in emergency medicine - An information paper.
http://rstream.umassp.edu:8080/ramgen/amherst/COMHLTH/CARY/ethicsPH_1.
rmvb. Retrieved July 1, 2012, from http://www.acep.org/Content.aspx?id=80871
American Nurses’ Association. (2001). Code of ethics for nurses with interpretive
statements. Washington, D.C: American Nurses Association.
American Psychiatric Association, & American Psychiatric Association. (1987).
Diagnostic and statistical manual of mental disorders: DSM-III-R (3rd ed., rev.).
Washington, DC: American Psychiatric Association.
American Psychiatric Association, & American Psychiatric Association. (2000).
Diagnostic and statistical manual of mental disorders: DSM-IV-TR (4th ed., text
revision.). Washington, DC: American Psychiatric Association.
American Psychiatric Association, American Psychiatric Nurses Association, & National
Association of Psychiatric Health Systems. (2003). Learning from each other:
115

Success stories and ideas for reducing restraint/seclusion in behavioral health.
American Psychiatric Association.
American Psychiatric Nurses Association, International Society of Psychiatric-Mental
Health Nurses, & American Nurses Association. (2007). Psychiatric-mental
health nursing: Scope and standards of practice. Silver Spring, MD: American
Nurses Association.
Appleby, L., Desai, P. N., Luchins, D. J., Gibbons, R. D., & Hedeker, D. R. (1993).
Length of stay and recidivism in schizophrenia: A study of public psychiatric
hospital patients. American Journal of Psychiatry, 150, 72–72.
Bandura, A. (1986). The explanatory and predictive scope of self efficacy theory. Journal
of Social and Clinical Psychology, 4(3), 359–373.
Bezold, H., MacDowell, M., & Kunkel, R. (1996). Predicting psychiatric length of stay.
Administration and Policy in Mental Health, 23(5), 407–423.
Bifulco, A., Moran, P. M., Ball, C., & Bernazzani, O. (2002). Adult attachment style. I:
Its relationship to clinical depression. Social psychiatry and psychiatric
epidemiology, 37(2), 50–59.
Blader, J. C. (2011). Acute Inpatient Care for Psychiatric Disorders in the United States,
1996 Through 2007. Archives of General Psychiatry, 68(12), 1276.
doi:10.1001/archgenpsychiatry.2011.84
Bower, F. L., McCullough, C. S., & Timmons, M. E. (2003). A synthesis of what we
know about the use of physical restraints and seclusion with patients in
psychiatric and acute care settings: 2003 update. The online journal of knowledge
synthesis for nursing, 10, 1.
116

Centorrino, F., Ventriglio, A., Vincenti, A., Talamo, A., & Baldessarini, R. J. (2010).
Changes in medication practices for hospitalized psychiatric patients: 2009 versus
2004. Human Psychopharmacology: Clinical and Experimental, 25(2), 179–186.
doi:10.1002/hup.1095
Clarkin, J., Hurt, S., & Crilly, J. (1987). Therapeutic alliance and hospital treatment
outcome. Hospital and Community Psychiatry, 38(8), 871–875.
Collip, D., Wigman, J. T. W., Myin-Germeys, I., Jacobs, N., Derom, C., Thiery, E., …
van Os, J. (2013). From Epidemiology to Daily Life: Linking Daily Life Stress
Reactivity to Persistence of Psychotic Experiences in a Longitudinal General
Population Study. PLoS ONE, 8(4), e62688. doi:10.1371/journal.pone.0062688
Cornaggia, C. M., Beghi, M., Pavone, F., & Barale, F. (2011). Aggression in psychiatry
wards: a systematic review. Psychiatry research, 189(1), 10–20.
Currier, G. W., & Allen, M. H. (2000). Emergency psychiatry: Physical and chemical
restraint in the psychiatric emergency service. Psychiatric Services, 51(6), 717–
719.
Daniel, S. I. F. (2006). Adult attachment patterns and individual psychotherapy: A review.
Clinical Psychology Review, 26(8), 968–984. doi:10.1016/j.cpr.2006.02.001
Davidson, L., Chinman, M., Sells, D., & Rowe, M. (2005). Peer support among adults
with serious mental illness: A report from the field. Schizophrenia Bulletin, 32(3),
443–450. doi:10.1093/schbul/sbj043
Dawe, S., Geppert, L., Occhipinti, S., & Kingswell, W. (2011). A comparison of the
symptoms and short-term clinical course in inpatients with substance-induced
117

psychosis and primary psychosis. Journal of Substance Abuse Treatment, 40(1),
95–101. doi:10.1016/j.jsat.2010.08.002
De Benedictis, L., Dumais, A., Sieu, N., Mailhot, M. P., Létourneau, G., Tran, M. A. M.,
… Côté, G. (2011). Staff perceptions and organizational factors as predictors of
seclusion and restraint on psychiatric wards. Psychiatric Services, 62(5), 484–
491.
Delaney, K. R. (1997). Milieu therapy: A therapeutic loophole. Perspectives in
psychiatric care, 33(2), 19–28.
Diagnostic and statistical manual of mental disorders. (2000) (Fourth Edition, Text
Revision.). Washington, DC: American Psychiatric Association.
Docherty, N. M., St-Hilaire, A., Aakre, J. M., Seghers, J. P., McCleery, A., & Divilbiss,
M. (2009). Anxiety Interacts With Expressed Emotion Criticism in the Prediction
of Psychotic Symptom Exacerbation. Schizophrenia Bulletin, 37(3), 611–618.
doi:10.1093/schbul/sbp123
Druss, B. G., Rosenheck, R. A., & Stolar, M. (1999). Patient satisfaction and
administrative measures as indicators of the quality of mental health care.
Psychiatric Services, 50(8), 1053–1058.
Echternacht, M. (2001). Fluid group: Concept and clinical application in the therapeutic
milieu. Journal of the American Psychiatric Nurses Association, 7(2), 39–44.
doi:10.1067/mpn.2001.115760
Eklund, M., & Hansson, L. (1997). Relationships between characteristics of the ward
atmosphere and treatment outcome in a psychiatric day-care unit based on
occupational therapy. Acta Psychiatrica Scandinavica, 95(4), 329–335.
118
Ellsworth, R., & Maroney, R. (1972). Characteristics of psychiatric programs and their
effects on patients’ adjustment. Journal of Consulting and Clinical Psychology,
39(3), 436–447. doi:10.1037/h0034028
Evert, H., Harvey, C., Herrman, H., & Trauer, T. (2003). The relationship between social
networks and occupational and self-care functioning in people with psychosis.
Social Psychiatry and Psychiatric Epidemiology, 38(4), 180–188.
doi:10.1007/s00127-003-0617-4
Fletcher Allen. (2013). About Fletcher Allen Health Care. Fletcher Allen Health Care.
Retrieved from http://www.fletcherallen.org/about/
Friis, S. (1984). The ward atmosphere: A crucial dimension of inpatient settings:
Measurement, clinical relevance and some influencing factors: An empirical
study. Oslo, Norway: University of Oslo.
Fry, S. T. (2002). Ethics in nursing practice: a guide to ethical decision making (2nd ed.).
Osney Mead, Oxford ; Malden, MA: Blackwell Science.
Gay, P. (2006). Freud : a life for our time . New York: Norton.
Glanz, K., Rimer, B. K., & Viswanath, K. (Eds.). (2008). Health behavior and health
education: theory, research, and practice (4th ed.). San Francisco, CA: Jossey-
Bass.
Goldman, H., Skodol, A., & Lave, T. (1992). Revising Axis V for DSM-III: A review of
measures of social functioning. American Journal of Psychiatry, 149(9), 1148–
1156.
Goodnough, A. (2011, November 4). Storm has Vermont scrambling to find beds for
mentally ill. New York Times. Retrieved from
119

http://www.nytimes.com/2011/11/05/health/shortage-of-beds-after-irene-shut-a-
vermont-mental-hospital.html?pagewanted=all&_r=0
Grootenboer, E. M. V., Giltay, E. J., van der Lem, R., van Veen, T., van der Wee, N. J. A.,
& Zitman, F. G. (2012). Reliability and validity of the Global Assessment of
Functioning Scale in clinical outpatients with depressive disorders. Journal of
Evaluation in Clinical Practice, 18(2), 502–507. doi:10.1111/j.1365-
2753.2010.01614.x
Gunderson, J. (1978). Defining the therapeutic processes in psychiatric milieus.
Psychiatry (Edgmont), 41(4), 327–35.
Harvey, C. A., Jeffreys, S. E., McNaught, A. S., Blizard, R. A., & King, M. B. (2007).
The Camden Schizophrenia Surveys III: Five-Year Outcome of a Sample of
Individuals From a Prevalence Survey and the Importance of Social
Relationships. International Journal of Social Psychiatry, 53(4), 340–356.
doi:10.1177/0020764006074529
Hawton, K., & van Heeringen, K. (2009). Suicide. Lancet, 373, 1372–81.
Holmes, M. (1966). Psychiatric nursing in the therapeutic community. In M. Holmes &
J. Werner (Eds.), Psychiatric nursing in a therapeutic community (pp. 3–25). New
York: Macmillian.
Horan, W. P., & Blanchard, J. J. (2003). Emotional responses to psychosocial stress in
schizophrenia: The role of individual differences in affective traits and coping.
Schizophrenia Research, 60(2-3), 271–283. doi:10.1016/S0920-9964(02)00227-X
Huntley, D., Cho, D. W., Christman, J., & Csernansky, J. (1998). Prediciting length of
stay in an acute psychiatric hospital. Psychiatric Services, 49(8).
120

Jack, L. (1989). Use of milieu as a problem-solving strategy in addiction treatment.
Nursing Clinic of North America, 24(1), 69–80.
Jackson, C., Trower, P., Reid, I., Smith, J., Hall, M., Townend, M., … others. (2009).
Improving psychological adjustment following a first episode of psychosis: A
randomized controlled trial of cognitive therapy to reduce post psychotic trauma
symptoms. Behaviour research and therapy, 47(6), 454–462.
Jones, S. H., Thornicroft, G., Coffey, M., & Dunn, G. (1995). A brief mental health
outcome scale-reliability and validity of the Global Assessment of Functioning
(GAF). The British Journal of Psychiatry, 166(5), 654–659.
doi:10.1192/bjp.166.5.654
Jörgensen, K. N., Römma, V., & Rundmo, T. (2009). Associations between ward
atmosphere, patient satisfaction and outcome. Journal of Psychiatric and Mental
Health Nursing, 16(2), 113–120.
Kirshner, L., & Johnston, L. (1982). Current Status of milieu psychiatry. General
Hospital Psychiatry, 4(1), 75–80.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer
Pub. Co.
LeCuyer, E. (1992). Milieu therapy for short stay units: A transformed practice theory.
Archives of Psychiatric Nursing, VI(2), 108–116.
Lee, S., Rothbard, A. B., & Noll, E. L. (2012). Length of inpatient stay of persons with
serious mental illness: Effects of hospital and regional characteristics. Psychiatric
Services, 63(9), 889–895.
121

Lehman, A., & Lieberman, J. (Eds.). (2004). Practice guidelines for the treatment of
patients with schizophrenia. American Psychiatric Association. Retrieved from
http://psychiatryonline.org.ezproxy.uvm.edu/data/Books/prac/Schizophrenia2e_In
activated_04-16-09.pdf
Lewis, M., Taylor, K., & Parks, J. (2009). Crisis prevention management: A program to
reduce the use of seclusion and restraint in an inpatient mental health setting.
Issues in Mental Health Nursing, 30(3), 159–164.
doi:10.1080/01612840802694171
Lieberman, P. B., Wiitala, S. A., Elliott, B., McCormick, S., & Goyette, S. B. (1998).
Decreasing length of stay: are there effects on outcomes of psychiatric
hospitalization? American Journal of Psychiatry, 155(7), 905–909.
Lincoln, T. M., Peter, N., Schäfer, M., & Moritz, S. (2008). Impact of stress on paranoia:
an experimental investigation of moderators and mediators. Psychological
Medicine, 39(07), 1129. doi:10.1017/S0033291708004613
Mahoney, J. S., Palyo, N., Napier, G., & Giordano, J. (2009). The therapeutic milieu
reconceptualized for the 21st-century. Archives of Psychiatric Nursing, 23(6),
423–429. doi:10.1016/j.apnu.2009.03.002
March, P., & Caple, C. (2012, July 6). Restraint and seclusion: Minimizing use in
psychiatric facilities. Cinahl Information Systems. Retrieved from
http://search.ebscohost.com.ezproxy.uvm.edu/login.aspx?
direct=true&db=nrc&AN=5000000245&site=nrc-live
Massachusetts General Hospital handbook of general hospital psychiatry. (2010) (6th
ed.). Philadelphia: Saunders/Elsevier.
122

Matud, M. P. (2004). Gender differences in stress and coping styles. Personality and
Individual Differences, 37(7), 1401–1415. doi:10.1016/j.paid.2004.01.010
Mechanic, D., McAlpine, D., & Olfson, M. (1998). Changing patterns psychiatric
inpatient care in the United States, 1988-1994. Archives of General Psychiatry,
55(9), 786–791.
Melle, I., Friis, S., Hauff, E., Kristian Island, T., Lorentzen, S., & Vaglum, P. (1996). The
importance of ward atmosphere in inpatient treatment of schizophrenia on short-
term units. Psychiatric Services, 47(7), 721–6.
Middelboe, T., Schjødt, T., Byrsting, K., & Gjerris, A. (2008). Ward atmosphere in acute
psychiatric in-patient care: Patients’ perceptions, ideals and satisfaction. Acta
Psychiatrica Scandinavica, 103(3), 212–219.
Moos, R., Shelton, R., & Petty, C. (1973). Perceived ward climate and treatment
outcome. Journal of Abnormal Psychology, 82(2), 291.
Myin-Germeys, I., Peeters, F., Havermans, R., Nicolson, N. A., DeVries, M. W.,
Delespaul, P., & Van Os, J. (2003). Emotional reactivity to daily life stress in
psychosis and affective disorder: an experience sampling study. Acta Psychiatrica
Scandinavica, 107(2), 124–131.
Norton, K. (2004). Re-thinking acute psychiatric inpatient care. International Journal of
Social Psychiatry, 50(3), 274–284. doi:10.1177/0020764004043146
O’Sullivan, R. L., Fava, M., Agustin, C., Baer, L., & Rosenbaum, J. F. (2007). Sensitivity
of the six-item Hamilton Depression Rating Scale. Acta Psychiatrica
Scandinavica, 95(5), 379–384.
123
Ossman, L. H., & Mahmoud, N. M. (2012). Social Support and Length of Hospital Stay
among Schizophrenic Patients. World Applied Sciences Journal, 19(5), 625–633.
Peplau, H. E. (1989). Interpersonal theory in nursing practice: selected works of
Hildegard E. Peplau. New York: Springer Pub. Co.
Phillips, P., & Nasr, S. (1983). Seclusion and restraint and prediction of violence.
American Journal of Psychiatry, (2), 229–232.
Pistrang, N., Barker, C., & Humphreys, K. (2008). Mutual help groups for mental health
problems: A review of effectiveness studies. American Journal of Community
Psychology, 42(1-2), 110–121. doi:10.1007/s10464-008-9181-0
Polit, D. F. (2012). Nursing research: generating and assessing evidence for nursing
practice (Ninth Edition.). Philadelphia: Wolters Kluwer Health/Lippincott
Williams & Wilkins.
Psychiatric nursing: Biological & behavioral concepts. (2008) (2nd ed.). Clifton Park,
NY: Thomson Delmar Learning.
Repper, J., & Carter, T. (2011). A review of the literature on peer support in mental health
services. Journal of Mental Health, 20(4), 392–411.
doi:10.3109/09638237.2011.583947
Ritsner, M., Ben-Avi, I., Ponizovsky, A., Timinsky, I., Bistrov, E., & Modai, I. (2003).
Quality of life and coping with schizophrenia symptoms. Quality of Life
Research, 12(1), 1–9.
Ritsner, M. S., & Lysaker, P. H. (2011). Coping with schizophrenia: Measuring coping
styles, patterns and temporal types. In M. S. Ritsner (Ed.), Handbook of
Schizophrenia Spectrum Disorders, Volume III (pp. 149–171). Dordrecht:
124
Springer Netherlands. Retrieved from
http://www.springerlink.com/index/10.1007/978-94-007-0834-1_8
Røssberg, J. I., Melle, I., Opjordsmoen, S., & Friis, S. (2006). Patient satisfaction and
treatment environment: A 20-year follow-up study from an acute psychiatric
ward. Nordic Journal of Psychiatry, 60(2), 176–180.
doi:10.1080/08039480600583894
Sadock, B. J., Kaplan, H. I., & Sadock, V. A. (2007). Kaplan & Sadock’s synopsis of
psychiatry : Behavioral sciences/clinical psychiatry. Philadelphia: Wolter
Kluwer/Lippincott Williams & Wilkins.
Sharfstein, S. S. (2009). Goals of inpatient treatment for psychiatric disorders. Annual
Review of Medicine, 60(1), 393–403. doi:10.1146/annurev.med.60.042607.080257
Skinner, K. (1979). The therapeutic milieu: making it work. Journal of psychiatric
nursing and mental health services, 17(8), 38–44.
Skodol, A., Link, B., Shrout, P., & Horwath, E. (1988). The revision of Axis V in DSM-
III-R: Should symptoms have been included? American Journal of Psychiatry,
145(7), 825–829.
Skorpen, A., Anderssen, N., Øye, C., & Bjelland, A. K. (2009). Treatment regimes in a
psychiatric hospital and apparent contradictions: Report from field work in a lock-
up ward illustrated with a constructed case. International Journal of Mental
Health Nursing, 18(6), 409–416. doi:10.1111/j.1447-0349.2009.00630.x
Soliman, A., O’Driscoll, G. A., Pruessner, J., Holahan, A.-L. V., Boileau, I., Gagnon, D.,
& Dagher, A. (2007). Stress-induced dopamine release in humans at risk of
125

psychosis: A [11C] Raclopride PET Study. Neuropsychopharmacology, 33(8),
2033–2041.
Staal, M. A. (2004). Stress, cognition, and human performance: A literature review and
conceptual framework. NASA technical memorandum, 212824. Retrieved from
http://human-factors.arc.nasa.gov/flightcognition/Publications/IH_054_Staal.pdf
Stahl, S. M. (2008). Stahl’s essential psychopharmacology : Neuroscientific basis and
practical applications. Cambridge: Cambridge University Press.
Stanton, A. L., Revenson, T. A., & Tennen, H. (2007). Health psychology: Psychological
adjustment to chronic disease. Annual Review of Psychology, 58(1), 565–592.
doi:10.1146/annurev.psych.58.110405.085615
Startup, M., Jackson, M. C., & Bendix, S. (2002). The concurrent validity of the Global
Assessment of Functioning (GAF). British Journal of Clinical Psychology, 41(4),
417–422.
Stensland, M., Watson, P. R., & Grazier, K. L. (2012). An examination of costs, charges,
and payments for inpatient psychiatric treatment in community hospitals.
Psychiatric Services, 63(7), 666–671. doi:10.11 76/appi.ps.201100402
Strauss, G. P., Llerena, K., & Gold, J. M. (2011). Attentional disengagement from
emotional stimuli in schizophrenia. Schizophrenia Research, 131(1-3), 219–223.
doi:10.1016/j.schres.2011.06.001
Sugden, J. (1985). The psychiatric treatment setting: Some general considerations. In A.
Altschul (Ed.), Recent advances in psychiatric nursing (pp. 3–18). Edinburgh,
Scotland: Churchill Livingston.
126

Thibeault, C. A., Trudeau, K., d’ Entremont, M., & Brown, T. (2010). Understanding the
milieu experiences of patients on an acute inpatient psychiatric unit. Archives of
Psychiatric Nursing, 24(4), 216–226. doi:10.1016/j.apnu.2009.07.002
Thomas, S. D. M., Daffern, M., Martin, T., Ogloff, J. R. P., Thomson, L. D. G., &
Ferguson, M. (2009). Factors associated with seclusion in a statewide forensic
psychiatric service in Australia over a 2-year period. International Journal of
Mental Health Nursing, 18(1), 2–9. doi:10.1111/j.1447-0349.2008.00567.x
Thomas, S. P., Shattell, M., & Martin, T. (2002). What’s therapeutic about the therapeutic
milieu? Archives of Psychiatric Nursing, 16(3), 99–107.
doi:10.1053/apnu.2002.32945
Townsend, M. C. (2009). Psychiatric mental health nursing: concepts of care in
evidence-based practice (6th ed.). Philadelphia: F.A. Davis.
Townsend, M. C. (2011). Nursing diagnoses in psychiatric nursing: Care plans and
psychotropic medications (8th ed.). Philadelphia, PA: F.A. Davis Co.
Tuck, I., & Keels, M. C. (1992). Milieu therapy: A review of development of this concept
and its implications for Psychiatric Nursing. Issues in Mental Health Nursing,
13(1), 51–58. doi:10.3109/01612849209006885
Tulloch, A. D., Fearon, P., & David, A. S. (2011). Length of stay of general psychiatric
inpatients in the United States: Systematic review. Administration and Policy in
Mental Health and Mental Health Services Research, 38(3), 155–168.
doi:10.1007/s10488-010-0310-3
Tusaie, K. R., & Fitzpatrick, J. J. (2013). Advanced practice psychiatric nursing
integrating psychotherapy, psychopharmacology, and complementary and
127

alternative approaches. New York, NY: Springer Pub. Co. Retrieved from
http://site.ebrary.com/lib/byuprovo/docDetail.action?docID=10603010
Vaglum, P., & Bøe, L. (1981). What was helpful and what was harmful? Patients evaluate
the progress of recovery in a therapeutic community. Journal of the Oslo city
hospitals, 31(4-6), 55–58.
Vaglum, P., Friis, S., & Karterud, S. (1985). Why are the results of milieu therapy for
schizophrenic patients contradictory? An analysis based on four empirical studies.
The Yale Journal of Biology and Medicine, 58(4), 349.
Ventura, J., Nuechterlein, K. H., Subotnik, K. L., Green, M. F., & Gitlin, M. J. (2004).
Self-efficacy and neurocognition may be related to coping responses in recent-
onset schizophrenia. Schizophrenia Research, 69(2-3), 343–352.
doi:10.1016/j.schres.2003.09.002
Villari, V., Rocca, P., Fonzo, V., Montemagni, C., Pandullo, P., & Bogetto, F. (2008). Oral
risperidone, olanzapine and quetiapine versus haloperidol in psychotic agitation.
Progress in Neuro-Psychopharmacology and Biological Psychiatry, 32(2), 405–
413. doi:10.1016/j.pnpbp.2007.09.007
Wilson, M. P., Pepper, D., Currier, G. W., Holloman Jr, G. H., & Feifel, D. (2012). The
psychopharmacology of agitation: consensus statement of the American
Association for Emergency Psychiatry Project BETA Psychopharmacology
Workgroup. Western Journal of Emergency Medicine, 13(1), 26.
Zhang, J., Harvey, C., & Andrew, C. (2011). Factors associated with length of stay and
the risk of readmission in an acute psychiatric inpatient facility: a retrospective
128

study. Australian and New Zealand Journal of Psychiatry, 45(7), 578–585.
doi:10.3109/00048674.2011.585452
129
Related Documents











