doi:10.1016/j.jcmg.2009.11.019 2010;3;555-562 J. Am. Coll. Cardiol. Img. and Simon Ray A. Nienaber, Erlend Eriksen, Kristian Wachtell, John Chambers, Karl Heinz Kuck, Edda Bahlmann, Dana Cramariuc, Eva Gerdts, Christa Gohlke-Baerwolf, Christoph Asymptomatic Aortic Stenosis: A SEAS Substudy Impact of Pressure Recovery on Echocardiographic Assessment of This information is current as of June 26, 2010 http://imaging.onlinejacc.org/cgi/content/full/3/6/555 located on the World Wide Web at: The online version of this article, along with updated information and services, is by Vikranth Gongidi on June 26, 2010 imaging.onlinejacc.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

doi:10.1016/j.jcmg.2009.11.019 2010;3;555-562 J. Am. Coll. Cardiol. Img.
and Simon Ray A. Nienaber, Erlend Eriksen, Kristian Wachtell, John Chambers, Karl Heinz Kuck, Edda Bahlmann, Dana Cramariuc, Eva Gerdts, Christa Gohlke-Baerwolf, Christoph
Asymptomatic Aortic Stenosis: A SEAS SubstudyImpact of Pressure Recovery on Echocardiographic Assessment of
This information is current as of June 26, 2010
http://imaging.onlinejacc.org/cgi/content/full/3/6/555located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by Vikranth Gongidi on June 26, 2010 imaging.onlinejacc.orgDownloaded from

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 3 , N O . 6 , 2 0 1 0
© 2 0 1 0 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 8 X / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . D O I : 1 0 . 1 0 1 6 / j . j c m g . 2 0 0 9 . 1 1 . 0 1 9
O R I G I N A L R E S E A R C H
Impact of Pressure Recovery on EchocardiographicAssessment of Asymptomatic Aortic Stenosis:A SEAS SubstudyEdda Bahlmann, MD,* Dana Cramariuc, MD, PHD,†‡ Eva Gerdts, MD, PHD,†‡Christa Gohlke-Baerwolf, MD,§ Christoph A. Nienaber, MD,� Erlend Eriksen, MD,†Kristian Wachtell, MD, PHD,¶ John Chambers, MD, PHD,# Karl Heinz Kuck, MD,*Simon Ray, MD**
Hamburg, Bad Krozingen, and Rostock, Germany; Bergen, Norway; Copenhagen, Denmark; andLondon, and Manchester, United Kingdom
O B J E C T I V E S The aim of this analysis was to assess the diagnostic importance of pressure recovery
in evaluation of aortic stenosis (AS) severity.
B A C K G R O U N D Although pressure recovery has previously been demonstrated to be particularly
important in assessment of AS severity in groups of patients with moderate AS or small aortic roots, it
has never been evaluated in a large clinical patient cohort.
M E T H O D S Data from 1,563 patients in the SEAS (Simvastatin and Ezetimibe in Aortic Stenosis)
study was used. Inner aortic diameter was measured at annulus, sinus, sinotubular junction, and
supracoronary level. Aortic valve area index (AVAI) was calculated by continuity equation and pressure
recovery and pressure recovery adjusted AVAI (energy loss index [ELI]), by validated equations. Primarily,
sinotubular junction diameter was used to calculate pressure recovery and ELI, but pressure recovery
and ELI calculated at different aortic root levels were compared. Severe AS was identified as AVAI and
ELI �0.6 cm2/m2. Patients were grouped into tertiles of peak transaortic velocity.
R E S U L T S Pressure recovery increased with increasing peak transaortic velocity. Overestimation of AS
severity by unadjusted AVAI was largest in the lowest tertile and if pressure recovery was assessed at the
sinotubular junction. In multivariate analysis, a larger difference between AVAI and ELI was associated with
lower peak transaortic velocity (beta � 0.35) independent of higher left ventricular ejection fraction (beta �
–0.049), male sex (beta � –0.075), younger age (beta � 0.093), and smaller aortic sinus diameter (beta �
0.233) (multiple R2 � 0.18, p � 0.001). Overall, 47.5% of patients classified as having severe AS by AVAI were
reclassified to nonsevere AS when pressure recovery was taken into account.
C O N C L U S I O N S For accurate assessment of AS severity, pressure recovery adjustment of AVAmust be
routinely performed. Estimation of pressure recovery at the sinotubular junction is suggested. (J Am Coll
Cardiol Img 2010;3:555–62) © 2010 by the American College of Cardiology Foundation
From the *Department of Cardiology, Asklepios Clinic St. Georg, Hamburg, Germany; †Institute of Medicine, University ofBergen, Bergen, Norway; ‡Haukeland University Hospital, Bergen, Norway; §Department of Cardiology, Herz-Zentrum BadKrozingen, Bad Krozingen, Germany; �Department of Cardiology, Universitätsklinikum Rostock, Rostock, Germany;¶Department of Cardiology, Rigshospitalet, The Heart Center, Copenhagen, Denmark; #Cardiothoracic Centre, Guy’s and StThomas’ Hospital Trust, London, United Kingdom; and the **Department of Cardiology, University of Manchester, UniversityHospital of South Manchester, Manchester, United Kingdom. The SEAS study was sponsored by MSP Singapore Company,LLC, Singapore, a partnership between Merck & Co., Inc., and the Schering-Plough Corporation. Drs. Gerdts, Gohlke-Baerwolf,Nienaber, Wachtell, Chambers, and Ray were investigators and/or members of the Steering Committees of the SEAS (Simvastatinand Ezetimibe in Aortic Stenosis) study. Drs. Gerdts, Gohlke-Baerwolf, Bahlmann, and Ray have received grant support from Merck& Co., Inc., the sponsor of the SEAS study.
Manuscript received June 12, 2009; revised manuscript received October 30, 2009, accepted November 6, 2009.
by Vikranth Gongidi on June 26, 2010 imaging.onlinejacc.orgDownloaded from
Digtkst
cep(cvtw
eAdt(htprtt
M
SsedaD
r1cmctcddcaSm
1idcCpobcsEomtctH
fAlralbssswwaemofat
A
A
A
A
A
E
J
j
LV � left ventricle
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 3 , N O . 6 , 2 0 1 0
J U N E 2 0 1 0 : 5 5 5 – 6 2
Bahlmann et al.
Pressure Recovery in Asymptomatic AS
556
ownstream pressure recovery in the aortaaffects transvalvular pressure gradientmeasurement and estimation of aortic
valve area (AVA) by continuity equationn patients with aortic stenosis (AS) (1). Conver-ence of flow through the stenotic aortic valve tohe vena contracta converts potential energy toinetic energy with a resulting reduction in pres-ure at the vena contracta (2– 4). As streamlineshen diverge and slow again distal to the vena
See page 563
ontracta, there is reconversion of some kineticnergy to potential energy with recovery of a pro-ortion of the pressure lost from the left ventricularLV) outflow tract to the vena contracta (5). Be-ause Doppler-based methods detect peak flowelocity that occurs at the vena contracta, theransvalvular pressure drop estimated by Dopplerill be greater than that calculated from simulta-
neous invasive pressure measurements inthe LV outflow tract and in the aortic rootdistal to the vena contracta. The implica-tion of pressure recovery is that AVAcalculated by Doppler-based methods un-derestimates valve area calculated bycatheter-based methods where aortic pres-sure is routinely measured in the aorticroot several centimeters distal to the aorticvalve (1,6–8). To overcome these limita-tions, Garcia et al. (9) derived an equationto calculate the pressure recovery adjusted
ffective valve area, named energy loss index (ELI).lthough pressure recovery has previously beenemonstrated to be particularly important in pa-ients with moderate AS and small aortic roots1,8,10), it has never been evaluated in a large,omogeneous cohort, and so its diagnostic impor-ance has not been assessed. Thus, the aim of theresent study was to evaluate the impact of pressureecovery on assessment of AS severity in asymp-omatic patients recruited in the SEAS (Simvasta-in and Ezetimibe in Aortic Stenosis) study (11).
E T H O D S
tudy population. The present substudy was pro-pectively planned within the SEAS study thatnrolled 1,873 patients with asymptomatic AS,efined by echocardiography at local study centerss aortic valve thickening and peak transaortic
ex
oppler velocity �2.5 and �4.0 m/s. Patients were t
by Vikranimaging.onlinejacc.orgDownloaded from
andomized from January 2001 to February 2004 in73 European study centers to �4-year placebo-ontrolled combined treatment with ezetimibe 10g/day and simvastatin 40 mg/day. Patients with
oronary heart disease, heart failure, diabetes, his-ory of stroke or peripheral vascular disease, clini-ally significant mitral valve disease, severe or pre-ominant aortic regurgitation, rheumatic valvularisease, aortic valve prosthesis, or renal insuffi-iency, and patients already on lipid-lowering ther-py were not included in the SEAS study. TheEAS study protocol, design, and patient recruit-ent was recently published (11).The present study population comprises the
,563 (83.4%) of the total 1,873 patients recruitedn the SEAS study, in whom AVA and aorticiameter at the sinotubular junction (junctional)ould be measured on the baseline echocardiogram.ompared with the 311 ineligible patients, theresent study population did not differ in age, sex,r body mass index. The SEAS study was approvedy regional ethics committees in all participatingountries. All patients gave written informed con-ent to participate in the SEAS study.chocardiography. Baseline echocardiograms werebtained using echocardiographs with second har-onic imaging and following a standardized pro-
ocol in all participating hospitals (12). All echo-ardiograms were sent for expert interpretation athe SEAS echocardiography core laboratory at
aukeland University Hospital, Bergen, Norway.Quantitative echocardiography was performed
ollowing the joint European Association andmerican Society of Echocardiography guide-
ines (13). End-diastolic diameter of the aorticoot was measured at annulus, sinus, junctional,nd supracoronary (1 cm distal to junction) aorticevel in 2-dimensional parasternal long-axis viewy an inner-edge-to-inner-edge method. LVtroke volume and ejection fraction were mea-ured by biplane Simpson method (13). LVtroke volume �22 ml/m2.04 was defined as low,hich corresponds to the previous cutoff of 35 mlhen correcting for body surface area (13). Sub-
ortic and transaortic blood velocities and gradi-nts were derived from velocity time integrals,easured by pulsed-wave Doppler in the LV
utflow tract and by continuous-wave Dopplerrom different windows by imaging and nonim-ging transducers, respectively. The highestransaortic velocity was used for tracing of the
B B R E V I A T I O N S
N D A C R O N YM S
S � aortic stenosis
VA � aortic valve area
VAI � aortic valve area ind
LI � energy loss index
unctional � sinotubular
unction
ime-velocity integral. The effective AVA was
th Gongidi on June 26, 2010
cvswAvcp[S
�aSv(mavwpdmatiefifpsjAt�b
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 3 , N O . 6 , 2 0 1 0
J U N E 2 0 1 0 : 5 5 5 – 6 2
Bahlmann et al.
Pressure Recovery in Asymptomatic AS
557
alculated using the continuity equation with theelocity time integrals and indexed for bodyurface area (AVAI). Pressure recovery (mm Hg)as calculated as 4v2 � 2AVA/Aa[1 – (AVA/a)], where v is the maximum Doppler transval-
ular velocity (1,6), AVA is calculated by theontinuity equation, Aa is the aortic area, andressure recovery adjusted AVAI (i.e., the ELIcm2/m2] as: AVA � Aa/(Aa – AVA)/m2) (1,9).evere AS was defined conventionally as AVAI
Table 1. Characteristics of the Total Study Population
Variable n � 1,563
Age, yrs 67 � 10
Women, n (%) 607 (39)
Systolic blood pressure, mm Hg 144 � 20
Diastolic blood pressure, mm Hg 82 � 10
Heart rate, beats/min 66 � 12
History of hypertension, n (%) 803 (51)
Height, cm 170 � 9
Weight, kg 78 � 15
Body surface area, m2 1.89 � 0.20
Body mass index, kg/m2 26.9 � 4.4
All p � NS between tertiles of peak transaortic velocity.
Table 2. Echocardiographic Findings in the Total Study Populat
Variables<2.79 m/(Tertile #1
Annular diameter, cm 2.18 � 0.2
Sinus diameter, cm 3.05 � 0.4
Junctional diameter, cm 2.79 � 0.4
Supracoronary diameter, cm 3.07 � 0.4
LV end-diastolic diameter, cm 5.04 � 0.6
Septal wall thickness, cm 1.12 � 0.2
Posterior wall thickness, cm 0.87 � 0.1
LV mass, g 187 � 67*
LV mass index, g/m2 98 � 31*
Stroke volume, ml/m2.04 22 � 5
Ejection fraction, % 66 � 7
Peak transaortic velocity, m/s 2.49 � 0.2
Peak transaortic gradient, mm Hg 25 � 4*†
Mean transaortic gradient, mm Hg 14 � 3*†
AVA, cm2 1.51 � 0.5
AVAI, cm2/m2 0.80 � 0.2
Pressure recovery, mm Hg 4 � 1*†
Pressure recovery/peak transaortic gradient, % 17 � 4*†
ELI, cm2/m2 1.14 � 0.5
AVAI – ELI, cm �0.35 � 0.3
AVAI – ELI, % �39 � 34*
Pressure recovery/peak transaortic gradientratio �20%, n (%)
(131) 25.5*
*p � 0.001 versus Tertile #3; †p � 0.001 versus Tertile #2.
AVA � aortic valve area; AVAI � aortic valve area index; ELI � energy loss index;imaging.onlinDownloaded from
0.6 cm2/m2 and adjusted for pressure recoverys ELI �0.6 cm2/m2 (14 –16).tatistical analysis. The study population was di-ided into tertiles of peak transaortic velocityGroup #1: �2.79 m/s; Group #2: 2.79 to 3.33/s; Group #3: �3.33 m/s). Continuous vari-
bles are presented as mean � SD and categoricalariables as percentages. Comparisons of groupsere performed by analysis of variance and Sidakost hoc test. Pressure recovery and ELI atifferent aortic levels were compared by para-etric statistics. Univariate correlations were
ssessed by Pearson correlation coefficients. Mul-ivariate linear regression analysis was used todentify independent covariates of pressure recov-ry. Results are given as standardized beta coef-cients for individual variables and as multiple R2
or the model. To demonstrate the association ofressure recovery with aortic root dimension, thetudy population was also divided into tertiles ofunctional aortic diameter. Interaction betweenVAI and pressure recovery in predicting AS was
ested in a logistic regression model. A p value0.05 was considered statistically significant in
oth univariate and multivariate analyses.
and When Divided Into Tertiles of Peak Transaortic Jet Velocity
2.79–3.33 m/s(Tertile #2)
>3.33 m/s(Tertile #3) Total
2.19 � 0.24 2.20 � 0.28 2.19 � 0.26
3.10 � 0.45 3.10 � 0.45 3.08 � 0.44
2.82 � 0.43 2.84 � 0.45 2.82 � 0.43
3.14 � 0.49 3.13 � 0.48 3.11 � 0.47
5.03 � 0.63 5.07 � 0.62 5.05 � 0.63
1.15 � 0.27* 1.21 � 0.29 1.16 � 0.28
0.88 � 0.18* 0.92 � 0.19 0.89 � 0.19
191 � 63* 207 � 69 195 � 67
100 � 29* 108 � 32 102 � 31
23 � 7 25 � 9 24 � 8
66 � 7 67 � 7 66 � 7
3.04 � 0.16* 3.71 � 0.29 3.08 � 0.54
37 � 4* 55 � 9 39 � 14
21 � 3* 32 � 6 23 � 9
1.25 � 0.40* 1.06 � 0.35 1.27 � 0.46
0.66 � 0.20* 0.56 � 0.18 0.67 � 0.23
6 � 2* 8 � 2 6 � 2
15 � 4* 14 � 4 16 � 4
0.86 � 0.35* 0.69 � 0.26 0.89 � 0.45
�0.20 � 0.17* �0.13 � 0.10 �0.23 � 0.26
�28 � 16* �22 � 11 �30 � 24
(85) 15.7* (47) 9.2 (263) 16.8
ion
s)
7
3
0
4
4
6*
9*
1*†
0*†
4*†
6*†
8*†
†
†
LV � left ventricle.
by Vikranth Gongidi on June 26, 2010 ejacc.org
R
AaipmdsPima
m0pbohppc1(ipasavtlal(p
sgsgva
EtspFeTtsaEve�s�at
A4tic stenosis
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 3 , N O . 6 , 2 0 1 0
J U N E 2 0 1 0 : 5 5 5 – 6 2
Bahlmann et al.
Pressure Recovery in Asymptomatic AS
558
E S U L T S
ortic dimension. Clinical and hemodynamic char-cteristics for the total study population are shownn Table 1. Age, sex, systolic and diastolic bloodressure, height, weight, body surface area, bodyass index, heart rate, and history of hypertension
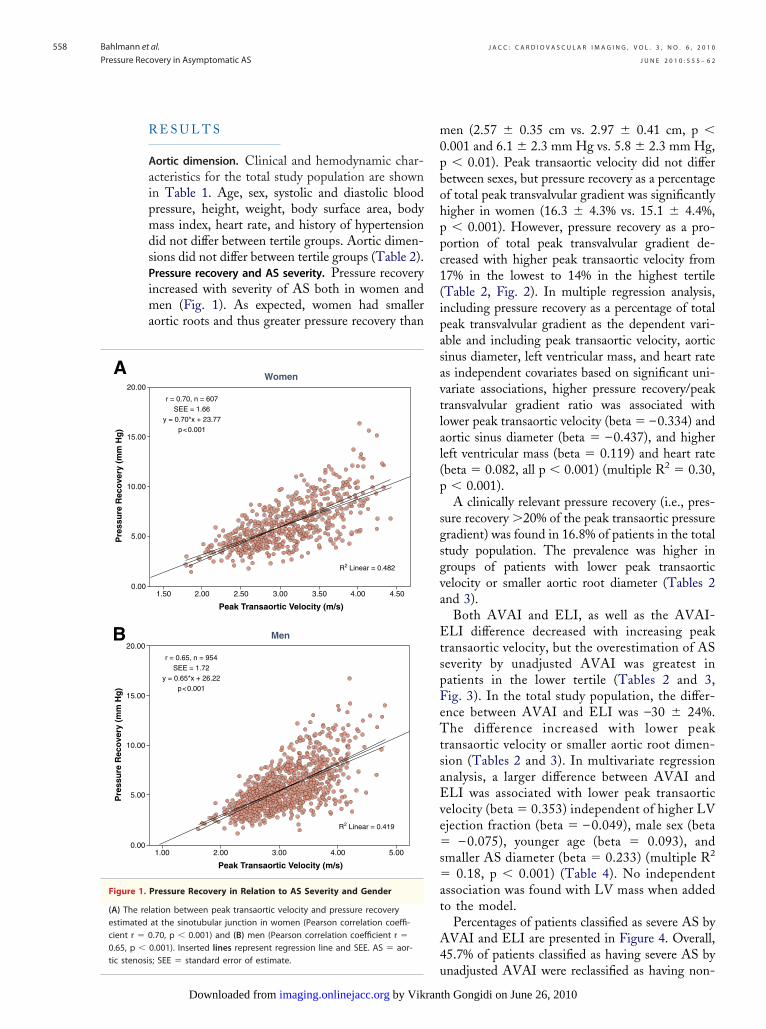
id not differ between tertile groups. Aortic dimen-ions did not differ between tertile groups (Table 2).ressure recovery and AS severity. Pressure recoveryncreased with severity of AS both in women and
en (Fig. 1). As expected, women had smallerortic roots and thus greater pressure recovery than
1.50 2.00 3.502.50 3.00 4.00 4.50
Peak Transaortic Velocity (m/s)
Women
r = 0.70, n = 607SEE = 1.66
y = 0.70*x + 23.77p<0.001
R2 Linear = 0.482
1.00 2.00 3.00 4.00 5.00
Peak Transaortic Velocity (m/s)
Men
r = 0.65, n = 954SEE = 1.72
y = 0.65*x + 26.22p<0.001
R2 Linear = 0.419
Pressure Recovery in Relation to AS Severity and Gender
ation between peak transaortic velocity and pressure recoveryat the sinotubular junction in women (Pearson correlation coeffi-.70, p � 0.001) and (B) men (Pearson correlation coefficient r �
0.001). Inserted lines represent regression line and SEE. AS � aor-
u; SEE � standard error of estimate.
by Vikranimaging.onlinejacc.orgDownloaded from
en (2.57 � 0.35 cm vs. 2.97 � 0.41 cm, p �.001 and 6.1 � 2.3 mm Hg vs. 5.8 � 2.3 mm Hg,� 0.01). Peak transaortic velocity did not differ
etween sexes, but pressure recovery as a percentagef total peak transvalvular gradient was significantlyigher in women (16.3 � 4.3% vs. 15.1 � 4.4%,� 0.001). However, pressure recovery as a pro-
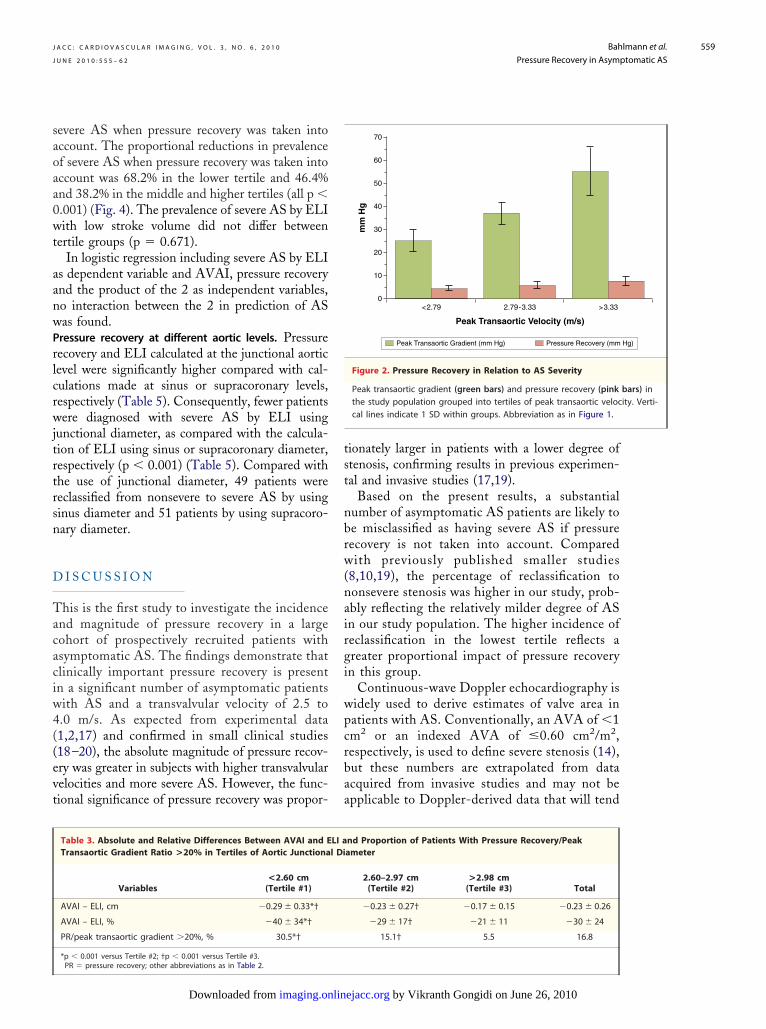
ortion of total peak transvalvular gradient de-reased with higher peak transaortic velocity from7% in the lowest to 14% in the highest tertileTable 2, Fig. 2). In multiple regression analysis,ncluding pressure recovery as a percentage of totaleak transvalvular gradient as the dependent vari-ble and including peak transaortic velocity, aorticinus diameter, left ventricular mass, and heart rates independent covariates based on significant uni-ariate associations, higher pressure recovery/peakransvalvular gradient ratio was associated withower peak transaortic velocity (beta � –0.334) andortic sinus diameter (beta � –0.437), and highereft ventricular mass (beta � 0.119) and heart ratebeta � 0.082, all p � 0.001) (multiple R2 � 0.30,� 0.001).A clinically relevant pressure recovery (i.e., pres-
ure recovery �20% of the peak transaortic pressureradient) was found in 16.8% of patients in the totaltudy population. The prevalence was higher inroups of patients with lower peak transaorticelocity or smaller aortic root diameter (Tables 2nd 3).
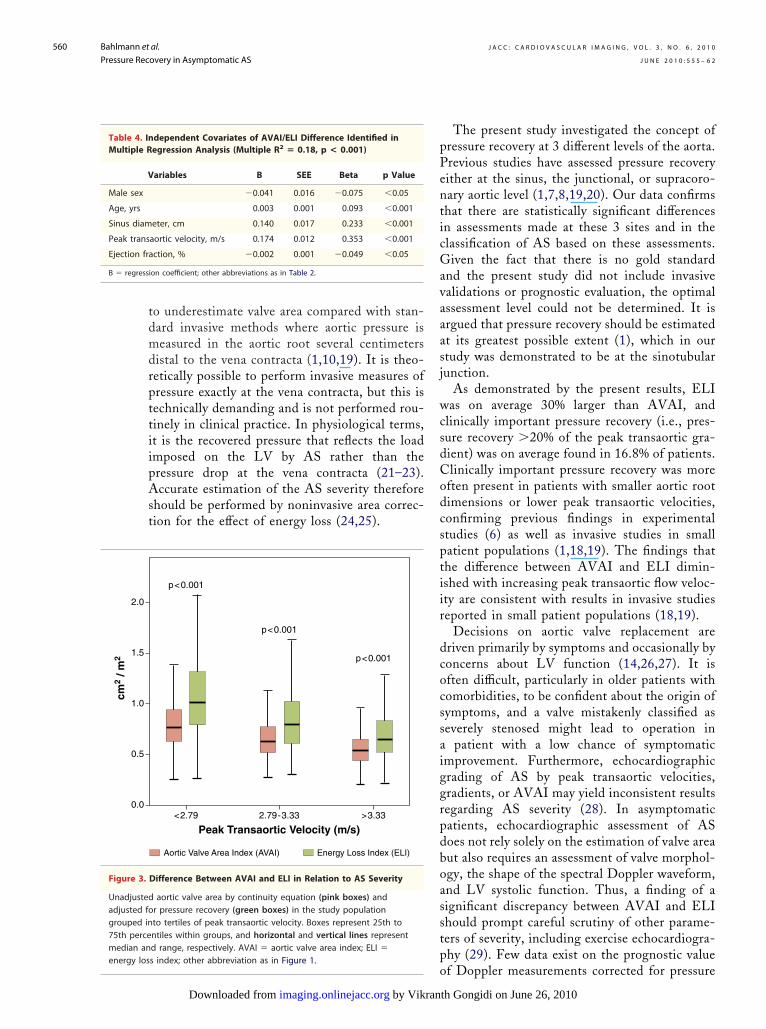
Both AVAI and ELI, as well as the AVAI-LI difference decreased with increasing peak
ransaortic velocity, but the overestimation of ASeverity by unadjusted AVAI was greatest inatients in the lower tertile (Tables 2 and 3,ig. 3). In the total study population, the differ-nce between AVAI and ELI was –30 � 24%.he difference increased with lower peak
ransaortic velocity or smaller aortic root dimen-ion (Tables 2 and 3). In multivariate regressionnalysis, a larger difference between AVAI andLI was associated with lower peak transaortic
elocity (beta � 0.353) independent of higher LVjection fraction (beta � – 0.049), male sex (beta
– 0.075), younger age (beta � 0.093), andmaller AS diameter (beta � 0.233) (multiple R2
0.18, p � 0.001) (Table 4). No independentssociation was found with LV mass when addedo the model.
Percentages of patients classified as severe AS byVAI and ELI are presented in Figure 4. Overall,5.7% of patients classified as having severe AS by
0.00
5.00
10.00
15.00
20.00
Pre
ssu
re R
eco
very
(m
m H
g)
0.00
5.00
10.00
15.00
20.00
Pre
ssu
re R
eco
very
(m
m H
g)
A
B
Figure 1.
(A) The relestimatedcient r � 00.65, p �
nadjusted AVAI were reclassified as having non-
th Gongidi on June 26, 2010
saoaa0wt
aanwPrlcrwjtrtrsn
D
Tacaciw4((evt
tst
nbrw(nairgi
wpcrbaa
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 3 , N O . 6 , 2 0 1 0
J U N E 2 0 1 0 : 5 5 5 – 6 2
Bahlmann et al.
Pressure Recovery in Asymptomatic AS
559
evere AS when pressure recovery was taken intoccount. The proportional reductions in prevalencef severe AS when pressure recovery was taken intoccount was 68.2% in the lower tertile and 46.4%nd 38.2% in the middle and higher tertiles (all p �.001) (Fig. 4). The prevalence of severe AS by ELIith low stroke volume did not differ between
ertile groups (p � 0.671).In logistic regression including severe AS by ELI
s dependent variable and AVAI, pressure recoverynd the product of the 2 as independent variables,o interaction between the 2 in prediction of ASas found.ressure recovery at different aortic levels. Pressureecovery and ELI calculated at the junctional aorticevel were significantly higher compared with cal-ulations made at sinus or supracoronary levels,espectively (Table 5). Consequently, fewer patientsere diagnosed with severe AS by ELI using
unctional diameter, as compared with the calcula-ion of ELI using sinus or supracoronary diameter,espectively (p � 0.001) (Table 5). Compared withhe use of junctional diameter, 49 patients wereeclassified from nonsevere to severe AS by usinginus diameter and 51 patients by using supracoro-ary diameter.
I S C U S S I O N
his is the first study to investigate the incidencend magnitude of pressure recovery in a largeohort of prospectively recruited patients withsymptomatic AS. The findings demonstrate thatlinically important pressure recovery is presentn a significant number of asymptomatic patientsith AS and a transvalvular velocity of 2.5 to.0 m/s. As expected from experimental data1,2,17) and confirmed in small clinical studies18–20), the absolute magnitude of pressure recov-ry was greater in subjects with higher transvalvularelocities and more severe AS. However, the func-ional significance of pressure recovery was propor-
Table 3. Absolute and Relative Differences Between AVAI and ETransaortic Gradient Ratio >20% in Tertiles of Aortic Junctiona
Variables<2.60 cm(Tertile #1)
AVAI – ELI, cm �0.29 � 0.33*†
AVAI – ELI, % �40 � 34*†
PR/peak transaortic gradient �20%, % 30.5*†
*p � 0.001 versus Tertile #2; †p � 0.001 versus Tertile #3.
PR � pressure recovery; other abbreviations as in Table 2.imaging.onlinDownloaded from
ionately larger in patients with a lower degree oftenosis, confirming results in previous experimen-al and invasive studies (17,19).
Based on the present results, a substantialumber of asymptomatic AS patients are likely toe misclassified as having severe AS if pressureecovery is not taken into account. Comparedith previously published smaller studies
8,10,19), the percentage of reclassification toonsevere stenosis was higher in our study, prob-bly reflecting the relatively milder degree of ASn our study population. The higher incidence ofeclassification in the lowest tertile reflects areater proportional impact of pressure recoveryn this group.
Continuous-wave Doppler echocardiography isidely used to derive estimates of valve area inatients with AS. Conventionally, an AVA of �1m2 or an indexed AVA of �0.60 cm2/m2,espectively, is used to define severe stenosis (14),ut these numbers are extrapolated from datacquired from invasive studies and may not bepplicable to Doppler-derived data that will tend
Pressure Recovery (mmPeak Transaortic Gradient (mm Hg)
mm
Hg
Peak Transaortic Velocity (m/s)
10
20
30
40
50
60
70
0<2.79 2.79-3.33 >3.33
Figure 2. Pressure Recovery in Relation to AS Severity
Peak transaortic gradient (green bars) and pressure recovery (pinkthe study population grouped into tertiles of peak transaortic veloccal lines indicate 1 SD within groups. Abbreviation as in Figure 1.
nd Proportion of Patients With Pressure Recovery/Peakameter
2.60–2.97 cm(Tertile #2)
>2.98 cm(Tertile #3) Total
�0.23 � 0.27† �0.17 � 0.15 �0.23 � 0.26
�29 � 17† �21 � 11 �30 � 24
15.1† 5.5 16.8
Hg)
bars) inity. Verti-
LI al Di
by Vikranth Gongidi on June 26, 2010 ejacc.org
tdmdrpttiipAst
pPenticGavaaasj
wcsdCodcsptiir
dcocssaiggrpdboasstpenergy los
B � regressi
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 3 , N O . 6 , 2 0 1 0
J U N E 2 0 1 0 : 5 5 5 – 6 2
Bahlmann et al.
Pressure Recovery in Asymptomatic AS
560
o underestimate valve area compared with stan-ard invasive methods where aortic pressure iseasured in the aortic root several centimeters
istal to the vena contracta (1,10,19). It is theo-etically possible to perform invasive measures ofressure exactly at the vena contracta, but this isechnically demanding and is not performed rou-inely in clinical practice. In physiological terms,t is the recovered pressure that reflects the loadmposed on the LV by AS rather than theressure drop at the vena contracta (21–23).ccurate estimation of the AS severity therefore
hould be performed by noninvasive area correc-ion for the effect of energy loss (24,25).
Energy Loss Index (ELI)Aortic Valve Area Index (AVAI)
Peak Transaortic Velocity (m/s)<2.79 2.79-3.33 >3.33
p<0.001
p<0.001
p<0.001
Difference Between AVAI and ELI in Relation to AS Severity
aortic valve area by continuity equation (pink boxes) andr pressure recovery (green boxes) in the study populationto tertiles of peak transaortic velocity. Boxes represent 25th tontiles within groups, and horizontal and vertical lines representd range, respectively. AVAI � aortic valve area index; ELI �
dependent Covariates of AVAI/ELI Difference Identified inegression Analysis (Multiple R2 � 0.18, p < 0.001)
ariables B SEE Beta p Value
�0.041 0.016 �0.075 �0.05
0.003 0.001 0.093 �0.001
eter, cm 0.140 0.017 0.233 �0.001
aortic velocity, m/s 0.174 0.012 0.353 �0.001
ction, % �0.002 0.001 �0.049 �0.05
on coefficient; other abbreviations as in Table 2.
os index; other abbreviation as in Figure 1.
by Vikranimaging.onlinejacc.orgDownloaded from
The present study investigated the concept ofressure recovery at 3 different levels of the aorta.revious studies have assessed pressure recoveryither at the sinus, the junctional, or supracoro-ary aortic level (1,7,8,19,20). Our data confirmshat there are statistically significant differencesn assessments made at these 3 sites and in thelassification of AS based on these assessments.iven the fact that there is no gold standard
nd the present study did not include invasivealidations or prognostic evaluation, the optimalssessment level could not be determined. It isrgued that pressure recovery should be estimatedt its greatest possible extent (1), which in ourtudy was demonstrated to be at the sinotubularunction.
As demonstrated by the present results, ELIas on average 30% larger than AVAI, and
linically important pressure recovery (i.e., pres-ure recovery �20% of the peak transaortic gra-ient) was on average found in 16.8% of patients.linically important pressure recovery was moreften present in patients with smaller aortic rootimensions or lower peak transaortic velocities,onfirming previous findings in experimentaltudies (6) as well as invasive studies in smallatient populations (1,18,19). The findings thathe difference between AVAI and ELI dimin-shed with increasing peak transaortic flow veloc-ty are consistent with results in invasive studieseported in small patient populations (18,19).
Decisions on aortic valve replacement areriven primarily by symptoms and occasionally byoncerns about LV function (14,26,27). It isften difficult, particularly in older patients withomorbidities, to be confident about the origin ofymptoms, and a valve mistakenly classified aseverely stenosed might lead to operation in
patient with a low chance of symptomaticmprovement. Furthermore, echocardiographicrading of AS by peak transaortic velocities,radients, or AVAI may yield inconsistent resultsegarding AS severity (28). In asymptomaticatients, echocardiographic assessment of ASoes not rely solely on the estimation of valve areaut also requires an assessment of valve morphol-gy, the shape of the spectral Doppler waveform,nd LV systolic function. Thus, a finding of aignificant discrepancy between AVAI and ELIhould prompt careful scrutiny of other parame-ers of severity, including exercise echocardiogra-hy (29). Few data exist on the prognostic value
cm2
/ m2
2.0
0.0
0.5
1.0
1.5
Figure 3.
Unadjustedadjusted fogrouped in75th percemedian an
Table 4. InMultiple R
V
Male sex
Age, yrs
Sinus diam
Peak trans
Ejection fra
f Doppler measurements corrected for pressure
th Gongidi on June 26, 2010

rEimaAaSpfimetdicida
pAtAtp
porr
C
Tcaa
RAL
bre
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 3 , N O . 6 , 2 0 1 0
J U N E 2 0 1 0 : 5 5 5 – 6 2
Bahlmann et al.
Pressure Recovery in Asymptomatic AS
561
ecovery. Results by Garcia et al. (9) showed thatLI was superior to unadjusted AVAI in predict-
ng adverse clinical outcomes in patients withoderate to severe AS. Whether AVAI or ELI isbetter predictor of outcome in asymptomaticS patients needs to be clarified in further
nalyses.tudy limitations. Routine catheterization was noterformed in this study, and so we cannot con-rm our estimates of pressure recovery by invasiveeasurements. However, in clinical practice,
chocardiography is often the sole method usedo assess the severity of AS. Current recommen-ations reserve transvalvular catheterization only
n those instances where there is significant doubtoncerning the true severity of stenosis. However,t should also be kept in mind that it is technicallyifficult to measure invasive pressure recoveryccurately during routine cardiac catheterization.
Ultimately, proving the value of calculatingressure recovery and pressure recovery adjustedVA, known as ELI, will require the demonstra-
ion of energy loss as a better prognosticator thanVA in predicting clinical outcome. However,
he present study is the first to demonstrate the
Re-classified from Severe AS
Non-severe AS Both by AVA
Severe AS Both by AVAI and
Peak Trans
0%
20%
40%
60%
80%
100%
<2.79
14.3%
6.6%
79.1%
23.5%
Figure 4. Reclassification From Severe to Nonsevere AS by Pres
Percentage of patients classified as having severe AS by both unadadjusted valve area increased (pink bars), while percentage of patiedecreased with increasing peak transaortic velocity. Percentage of p(yellow bars) increased with increasing peak transaortic velocity. Ab
revalence, correlates, and clinical relevance of D
imaging.onlinDownloaded from
ressure recovery and ELI in a large populationf AS patients. It demonstrates that pressureecovery adjustment of AVA frequently leads toeclassification of AS severity.
O N C L U S I O N S
he severity of AS is frequently overestimated iforrection for pressure recovery is not performed. Forccurate assessment of AS severity, pressure recoverydjustment of AVA must be routinely performed.
eprint requests and correspondence: Dr. Edda Bahlmann,sklepios Clinic St. Georg, II. Med. Clinic (Cardiology),ohmühlenstrasse 5, 20099 Hamburg, Germany. E-mail:
AVAI to Non-severe AS by ELI
d ELI
I
rtic Velocity (m/s)
.3%
56.2%
25.9%
41.8%
32.2%
9-3.33 >3.33
Recovery Adjustment
d aortic valve area by continuity equation and pressure recoveryhaving nonsevere AS by both ELI and AVAI (green bars)nts reclassified from severe AS by AVAI to nonsevere AS by ELIviations as in Figures 1, 2, and 3.
Table 5. Estimation of Pressure Recovery and ELI at Different Lthe Aorta
Variables Sinus Junctional Supra
Aortic diameter, cm 3.08 � 0.44*† 2.82 � 0.42† 3.11
Pressure recovery, mm Hg 5.14 � 1.97* 5.88 � 2.27† 5.07
ELI, cm2/m2 0.84 � 0.38* 0.89 � 0.45† 0.84
Severe AS, % 19.7* 17.2† 2
*p � 0.001 versus junctional level; †p � 0.001 versus supracoronary level.AS � aortic stenosis; other abbreviations as in Table 2.
by
I an
EL
ao
20
2.7
sure
justentsatie
evels of
coronary
� 0.47
� 1.98
� 0.38
0.0
by Vikranth Gongidi on June 26, 2010 ejacc.org

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 3 , N O . 6 , 2 0 1 0
J U N E 2 0 1 0 : 5 5 5 – 6 2
Bahlmann et al.
Pressure Recovery in Asymptomatic AS
562
R
1
1
2
2
2
2
2
2
2
2
2
2
Kly
E F E R E N C E S
1. Baumgartner H, Stefanelli T, Nied-erberger J, Schima H, Maurer G.“Overestimation” of catheter gra-dients by Doppler ultrasound inpatients with aortic stenosis: a pre-dictable manifestation of pressurerecovery. J Am Coll Cardiol 1999;33:1655– 61.
2. Clark C. The fluid mechanics of aorticstenosis—I. Theory and steady flowexperiments. J Biomech 1976;9:521–8.
3. Clark C. The fluid mechanics of aorticstenosis—II. Unsteady flow experi-ments. J Biomech 1976;9:567–73.
4. Clark C. Relation between pressuredifference across the aortic valve andleft ventricular outflow. CardiovascRes 1978;12:276–87.
5. Levine RA, Jimoh A, Cape EG.Pressure recovery distal to a stenosis:potential cause of gradient “overes-timation” by Doppler echocardiog-raphy. J Am Coll Cardiol 1989;13:706 –15.
6. Niederberger J, Schima H, MaurerG, Baumgartner H. Importance ofpressure recovery for the assessmentof aortic stenosis by Doppler ultra-sound. Role of aortic size, aorticvalve area and direction of the ste-notic jet in vitro. Circulation 1996;94:1934 – 40.
7. Garcia D, Dumesnil J, Durand LG,Kadem L, Pibarot P. Discrepanciesbetween catheter and Doppler esti-mates of valve effective orifice area canbe predicted from the pressure recov-ery phenomenon. J Am Coll Cardiol2003;41:435–42.
8. Kume T, Okura H, Kawamoto T, etal. Clinical implication of energy losscoefficient in patients with severe aor-tic stenosis diagnosed by Dopplerechocardiography. Circ J 2008;72:1265–9.
9. Garcia D, Pibarot P, Dumesnil JG,Sakr F, Durand LG. Assessment ofaortic valve stenosis severity: a newindex based on the energy loss con-cept. Circulation 2000;101:765–71.
0. Spevack D, Almuti K, Ostfeld R,Bello R, Gordon G. Routine adjust-ment of Doppler echocardiographi-cally derived aortic valve area using apreviously derived equation to accountfor the effect of pressure recovery.J Am Soc Echocardiogr 2008;21:34–7.
1. Rossebo AB, Pedersen TR, Allen C,et al. Design and baseline characteris-
imaging.onlinDownloaded from
tics of the Simvastatin and Ezetimibein Aortic Stenosis (SEAS) study.Am J Cardiol 2007;99:970–3.
12. Cramariuc D, Rieck A, Staal E, et al.Factors influencing left ventricularstructure and stress-corrected systolicfunction in men and women withasymptomatic aortic valve stenosis (aSEAS substudy). Am J Cardiol 2008;101:510–5.
13. Lang RM, Bierig M, Devereux RB, etal., on behalf of the American Societyof Echocardiography’s Nomenclatureand Standards Committee, TaskForce on Chamber Quantification,American College of CardiologyEchocardiography Committee, Amer-ican Heart Association, EuropeanAssociation of Echocardiography,European Society of Cardiology. Rec-ommendations for chamber quantifi-cation. Eur J Echocardiogr 2006;7:79–108.
14. Bonow RO, Blase A, Carabello BA, etal., on behalf of the American Collegeof Cardiology/American Heart Asso-ciation Task Force on Practice Guide-lines. 2008 focused update incorpo-rated into the ACC/AHA 2006guidelines for the management of pa-tients with valvular heart disease: areport of the American College ofCardiology/American Heart Associa-tion Task Force on Practice Guide-lines (Writing Committee to Revisethe 1998 Guidelines for the Manage-ment of Patients with Valvular HeartDisease): endorsed by the Society ofCardiovascular Anesthesiologists, So-ciety for Cardiovascular Angiographyand Interventions and Society of Tho-racic Surgeons. J Am Coll Cardiol2008;52:e1–142.
15. Rahimtoola SH. Perspective on valvu-lar heart disease: an update. J Am CollCardiol 1989;14:1–23.
16. Dumesnil JG, Pibarot P, Akins C.New approaches to quantifying aorticstenosis severity. Curr Cardiol Rep2008;10:91–7.
17. Volker W, Reul H, Stelzer T,Schmidt A, Karsch KR. Pressurerecovery in aortic stenosis: an invitro study in a pulsatile flow model.J Am Coll Cardiol 1992;20:1585–93.
18. Laskey WK, Kussmaul WG. Pressurerecovery in aortic valve stenosis. Cir-culation 1994;89:116–21.
19. Schoebel WA, Voelker W, HaaseKK, Karsch KR. Extent, determi-
nants and clinical importance ofpressure recovery in patients with jby Vikranth Gongidi on June 2ejacc.org
aortic valve stenosis. Eur Heart J1999;20:1355– 63.
0. Gjertson P, Caidahl K, Svensson G,Wallentin I, Bech-Hanssen O. Im-portant pressure recovery in patientswith aortic stenosis and high Dopplergradients. Am J Cardiol 2001;88:139–44.
1. Khan SS. Assessment of prostheticvalve hemodynamics by Doppler: les-sons from in vitro studies of the St.Jude valve. J Heart Valve Dis 1993;2:183–93.
2. Snell RE, Luchsinger PC. Determi-nation of the external work and powerof the left ventricle in intact man. AmHeart J 1965;69:529–37.
3. Heinrich RS, Fontaine AA, GrimesRY, et al. Experimental analysis offluid mechanical energy losses in aor-tic valve stenosis: importance of pres-sure recovery. Ann Biomed Eng 1996;24:685–94.
4. Clark C. Energy losses in flowthrough stenosed valves. J Biomech1976;12:737–46.
5. Heinrich RS, Marcus RH, EnsleyAE, Gibson DE, Yoganathan AP.Valve orifice area alone is an insuf-ficient index of aortic stenosis se-verity: effects of the proximal anddistal geometry on transaortic energyloss. J Heart Valve Dis 1999;8:509 –15.
6. Otto CM. Valvular aortic stenosis.Disease severity and timing of inter-vention. J Am Coll Cardiol 2006;47:2141–51.
7. Rosenhek R, Binder T, Porenta G, etal. Predictors of outcome in severe,asymptomatic aortic stenosis. N EnglJ Med 2000;343:611–7.
8. Minners J, Allgeier M, Gohlke-Baerwolf C, Kienzle RP, NeumannFJ, Jander N. Inconsistencies of echo-cardiographic criteria for the gradingof aortic valve stenosis. Eur Heart J2008;29:1043–8.
9. Vahanian A, Baumgartner H, Bax J, etal. Guidelines on the management ofvalvular heart disease. The task force onthe management of valvular heart dis-ease of the European Society of Cardi-ology. Eur Heart J 2007;28:230–68.
ey Words: aortic stenosis yeft ventricle y aortic valve area
energy loss y sinotubular
unction.6, 2010
doi:10.1016/j.jcmg.2009.11.019 2010;3;555-562 J. Am. Coll. Cardiol. Img.
and Simon Ray A. Nienaber, Erlend Eriksen, Kristian Wachtell, John Chambers, Karl Heinz Kuck, Edda Bahlmann, Dana Cramariuc, Eva Gerdts, Christa Gohlke-Baerwolf, Christoph
Asymptomatic Aortic Stenosis: A SEAS SubstudyImpact of Pressure Recovery on Echocardiographic Assessment of
This information is current as of June 26, 2010
& ServicesUpdated Information
http://imaging.onlinejacc.org/cgi/content/full/3/6/555including high-resolution figures, can be found at:
References
http://imaging.onlinejacc.org/cgi/content/full/3/6/555#BIBLfree at: This article cites 29 articles, 15 of which you can access for
Citations
icleshttp://imaging.onlinejacc.org/cgi/content/full/3/6/555#otherartThis article has been cited by 1 HighWire-hosted articles:
Rights & Permissions
http://imaging.onlinejacc.org/misc/permissions.dtltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://imaging.onlinejacc.org/misc/reprints.dtl
Information about ordering reprints can be found online:
by Vikranth Gongidi on June 26, 2010 imaging.onlinejacc.orgDownloaded from
Related Documents