Impact of anastomotic leak on outcomes after transhiatal esophagectomy Matthew J. Schuchert, MD, Ghulam Abbas, MD, Katie S. Nason, MD, Arjun Pennathur, MD, Omar Awais, MD, Marco Santana, MD, Raphael Pereira, MD, Alicia Oostdyk, BS, James D. Luketich, MD, and Rodney J. Landreneau, MD, Pittsburgh, PA Background. The development of anastomotic leaks and/or strictures can be associated with considerable morbidity and impairment of quality of life. In the current study, we evaluated the outcomes of patients who developed anastomotic complications after esophagectomy to elucidate the impact of these events on morbidity, mortality, and subsequent need for dilation. Methods. We analyzed retrospectively the clinical course of 235 patients who underwent transhiatal esophagectomy for cancer from 2001 to 2009. Patients with confirmed anastomotic leaks were identified and classified with the following scale: class 1: Radiographic leak only, no intervention; class 2: leak requiring opening of the wound, cervical and/or percutaneous drainage; class 3: disruption of anastomosis (10--50% circumference) with perianastomotic abscess requiring video-assisted thoraco- scopic surgery or thoracotomy; and class 4: gastric tip necrosis with anastomotic separation (>50% circumference). Results. Anastomotic leaks were encountered in 30 patients (13%). Anastomotic leaks were associated with greater morbidity (70% vs 47%; P = .02) and stricture formation (57% vs 19%; P = .0001). Mortality was not different. Increasing leak class was associated with an increased need for postoperative anastomotic dilations (P = .016). Conclusion. Anastomotic integrity after esophagectomy has a substantial impact on perioperative course and long-term swallowing. A more formal radiographic and endoscopic leak classification system seems justified. (Surgery 2010;148:831-40.) From the Division of Thoracic and Foregut Surgery, Heart, Lung and Esophageal Surgery Institute, UPMC Health System, Pittsburgh, PA ANASTOMOTIC COMPLICATIONS are encountered fre- quently in the setting of esophagectomy. Leaks and strictures are influenced by multiple factors, including the degree of conduit ischemia, anasto- motic tension, host nutritional parameters, and tissue integrity, as well as anastomotic location (neck versus chest) and technique. 1-3 The develop- ment of anastomotic leaks and/or strictures after esophagectomy are associated with substantial morbidity and impairment of quality of life. 4,5 The reported incidence of anastomotic leaks varies widely in the literature, ranging from 0% to 53%. 6,7 No clear definition of what constitutes a leak and no standardized treatment algorithms have been established. In the current study, our primary objective was to define a leak classification system based on an objective visual (radiographic and endoscopic) assessment of anastomotic integ- rity and the degree of surgical intervention re- quired. We hypothesized that such a classification system would correlate with perioperative course, including duration of stay, morbidity, mortality, and subsequent stricture formation. MATERIALS AND METHODS Patients. Approval for this study was provided by the Institutional Review Board of the University of Pittsburgh, and individual patient consent was waived given the retrospective nature of the anal- ysis. We performed a review of 235 consecutive patients who underwent transhiatal esophagec- tomy for pathologically confirmed cancer at the Presented at the Central Surgical Association 2010 Annual Meeting, March 10–13, 2010, Chicago, Illinois. Accepted for publication July 13, 2010. Reprint requests: Matthew J. Schuchert, MD, Heart, Lung and Esophageal Surgery Institute, Shadyside Medical Building, Suite 715, 5200 Centre Avenue, Pittsburgh, PA 15232. E-mail: [email protected]. 0039-6060/$ - see front matter Ó 2010 Mosby, Inc. All rights reserved. doi:10.1016/j.surg.2010.07.034 SURGERY 831

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PresenteMeeting
Accepte
ReprintEsophag715, 52schuche
0039-60
� 2010
doi:10.1
Impact of anastomotic leak onoutcomes after transhiatalesophagectomyMatthew J. Schuchert, MD, Ghulam Abbas, MD, Katie S. Nason, MD, Arjun Pennathur, MD,Omar Awais, MD, Marco Santana, MD, Raphael Pereira, MD, Alicia Oostdyk, BS,James D. Luketich, MD, and Rodney J. Landreneau, MD, Pittsburgh, PA
Background. The development of anastomotic leaks and/or strictures can be associated with considerablemorbidity and impairment of quality of life. In the current study, we evaluated the outcomes of patientswho developed anastomotic complications after esophagectomy to elucidate the impact of these events onmorbidity, mortality, and subsequent need for dilation.Methods. We analyzed retrospectively the clinical course of 235 patients who underwent transhiatalesophagectomy for cancer from 2001 to 2009. Patients with confirmed anastomotic leaks were identifiedand classified with the following scale: class 1: Radiographic leak only, no intervention; class 2: leakrequiring opening of the wound, cervical and/or percutaneous drainage; class 3: disruption ofanastomosis (10--50% circumference) with perianastomotic abscess requiring video-assisted thoraco-scopic surgery or thoracotomy; and class 4: gastric tip necrosis with anastomotic separation (>50%circumference).Results. Anastomotic leaks were encountered in 30 patients (13%). Anastomotic leaks were associatedwith greater morbidity (70% vs 47%; P = .02) and stricture formation (57% vs 19%; P = .0001).Mortality was not different. Increasing leak class was associated with an increased need for postoperativeanastomotic dilations (P = .016).Conclusion. Anastomotic integrity after esophagectomy has a substantial impact on perioperative courseand long-term swallowing. A more formal radiographic and endoscopic leak classification system seemsjustified. (Surgery 2010;148:831-40.)
From the Division of Thoracic and Foregut Surgery, Heart, Lung and Esophageal Surgery Institute, UPMCHealth System, Pittsburgh, PA
ANASTOMOTIC COMPLICATIONS are encountered fre-quently in the setting of esophagectomy. Leaksand strictures are influenced by multiple factors,including the degree of conduit ischemia, anasto-motic tension, host nutritional parameters, andtissue integrity, as well as anastomotic location(neck versus chest) and technique.1-3 The develop-ment of anastomotic leaks and/or strictures afteresophagectomy are associated with substantialmorbidity and impairment of quality of life.4,5
d at the Central Surgical Association 2010 Annual, March 10–13, 2010, Chicago, Illinois.
d for publication July 13, 2010.
requests: Matthew J. Schuchert, MD, Heart, Lung andeal Surgery Institute, Shadyside Medical Building, Suite00 Centre Avenue, Pittsburgh, PA 15232. E-mail:[email protected].
60/$ - see front matter
Mosby, Inc. All rights reserved.
016/j.surg.2010.07.034
The reported incidence of anastomotic leaksvaries widely in the literature, ranging from 0% to53%.6,7 No clear definition of what constitutes aleak and no standardized treatment algorithmshave been established. In the current study, ourprimary objective was to define a leak classificationsystem based on an objective visual (radiographicand endoscopic) assessment of anastomotic integ-rity and the degree of surgical intervention re-quired. We hypothesized that such a classificationsystem would correlate with perioperative course,including duration of stay, morbidity, mortality,and subsequent stricture formation.
MATERIALS AND METHODS
Patients. Approval for this study was provided bythe Institutional Review Board of the University ofPittsburgh, and individual patient consent waswaived given the retrospective nature of the anal-ysis. We performed a review of 235 consecutivepatients who underwent transhiatal esophagec-tomy for pathologically confirmed cancer at the
SURGERY 831
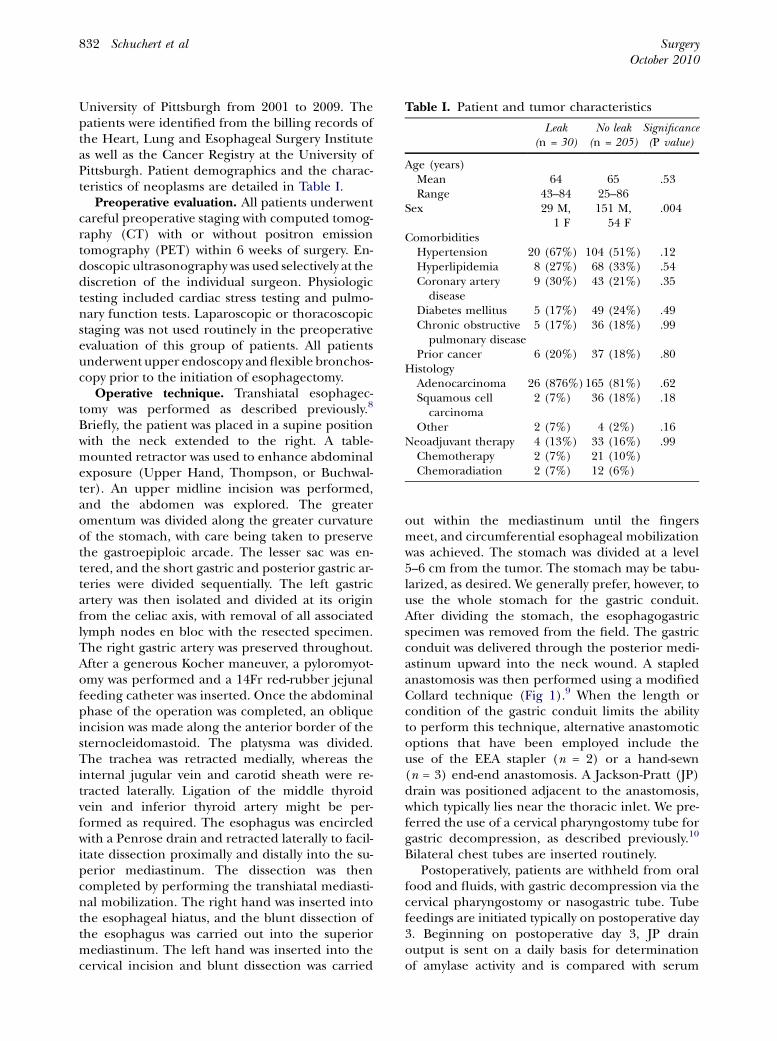
Table I. Patient and tumor characteristics
Leak(n = 30)
No leak(n = 205)
Significance(P value)
Age (years)Mean 64 65 .53Range 43–84 25–86
Sex 29 M,1 F
151 M,54 F
.004
ComorbiditiesHypertension 20 (67%) 104 (51%) .12Hyperlipidemia 8 (27%) 68 (33%) .54Coronary artery
disease9 (30%) 43 (21%) .35
Diabetes mellitus 5 (17%) 49 (24%) .49Chronic obstructive
pulmonary disease5 (17%) 36 (18%) .99
Prior cancer 6 (20%) 37 (18%) .80Histology
Adenocarcinoma 26 (876%)165 (81%) .62Squamous cell
carcinoma2 (7%) 36 (18%) .18
Other 2 (7%) 4 (2%) .16Neoadjuvant therapy 4 (13%) 33 (16%) .99
Chemotherapy 2 (7%) 21 (10%)Chemoradiation 2 (7%) 12 (6%)
SurgeryOctober 2010
832 Schuchert et al
University of Pittsburgh from 2001 to 2009. Thepatients were identified from the billing records ofthe Heart, Lung and Esophageal Surgery Instituteas well as the Cancer Registry at the University ofPittsburgh. Patient demographics and the charac-teristics of neoplasms are detailed in Table I.
Preoperative evaluation. All patients underwentcareful preoperative staging with computed tomog-raphy (CT) with or without positron emissiontomography (PET) within 6 weeks of surgery. En-doscopic ultrasonography was used selectively at thediscretion of the individual surgeon. Physiologictesting included cardiac stress testing and pulmo-nary function tests. Laparoscopic or thoracoscopicstaging was not used routinely in the preoperativeevaluation of this group of patients. All patientsunderwent upper endoscopy and flexible bronchos-copy prior to the initiation of esophagectomy.
Operative technique. Transhiatal esophagec-tomy was performed as described previously.8
Briefly, the patient was placed in a supine positionwith the neck extended to the right. A table-mounted retractor was used to enhance abdominalexposure (Upper Hand, Thompson, or Buchwal-ter). An upper midline incision was performed,and the abdomen was explored. The greateromentum was divided along the greater curvatureof the stomach, with care being taken to preservethe gastroepiploic arcade. The lesser sac was en-tered, and the short gastric and posterior gastric ar-teries were divided sequentially. The left gastricartery was then isolated and divided at its originfrom the celiac axis, with removal of all associatedlymph nodes en bloc with the resected specimen.The right gastric artery was preserved throughout.After a generous Kocher maneuver, a pyloromyot-omy was performed and a 14Fr red-rubber jejunalfeeding catheter was inserted. Once the abdominalphase of the operation was completed, an obliqueincision was made along the anterior border of thesternocleidomastoid. The platysma was divided.The trachea was retracted medially, whereas theinternal jugular vein and carotid sheath were re-tracted laterally. Ligation of the middle thyroidvein and inferior thyroid artery might be per-formed as required. The esophagus was encircledwith a Penrose drain and retracted laterally to facil-itate dissection proximally and distally into the su-perior mediastinum. The dissection was thencompleted by performing the transhiatal mediasti-nal mobilization. The right hand was inserted intothe esophageal hiatus, and the blunt dissection ofthe esophagus was carried out into the superiormediastinum. The left hand was inserted into thecervical incision and blunt dissection was carried
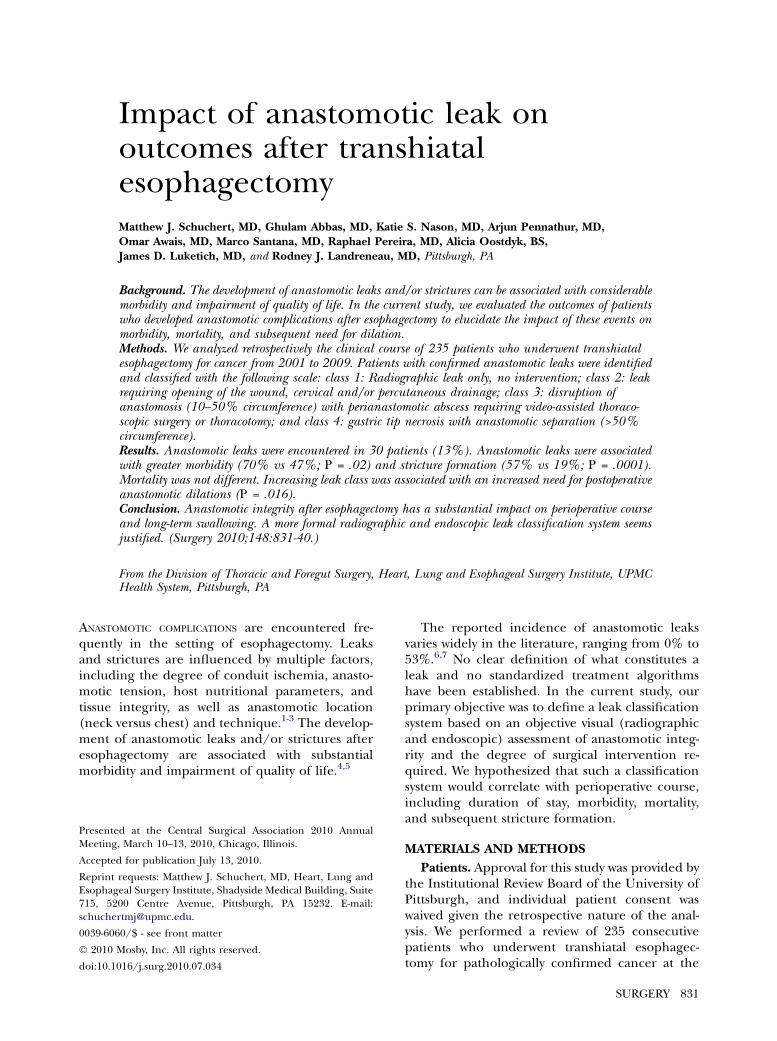
out within the mediastinum until the fingersmeet, and circumferential esophageal mobilizationwas achieved. The stomach was divided at a level5--6 cm from the tumor. The stomach may be tabu-larized, as desired. We generally prefer, however, touse the whole stomach for the gastric conduit.After dividing the stomach, the esophagogastricspecimen was removed from the field. The gastricconduit was delivered through the posterior medi-astinum upward into the neck wound. A stapledanastomosis was then performed using a modifiedCollard technique (Fig 1).9 When the length orcondition of the gastric conduit limits the abilityto perform this technique, alternative anastomoticoptions that have been employed include theuse of the EEA stapler (n = 2) or a hand-sewn(n = 3) end-end anastomosis. A Jackson-Pratt (JP)drain was positioned adjacent to the anastomosis,which typically lies near the thoracic inlet. We pre-ferred the use of a cervical pharyngostomy tube forgastric decompression, as described previously.10
Bilateral chest tubes are inserted routinely.Postoperatively, patients are withheld from oral
food and fluids, with gastric decompression via thecervical pharyngostomy or nasogastric tube. Tubefeedings are initiated typically on postoperative day3. Beginning on postoperative day 3, JP drainoutput is sent on a daily basis for determinationof amylase activity and is compared with serum
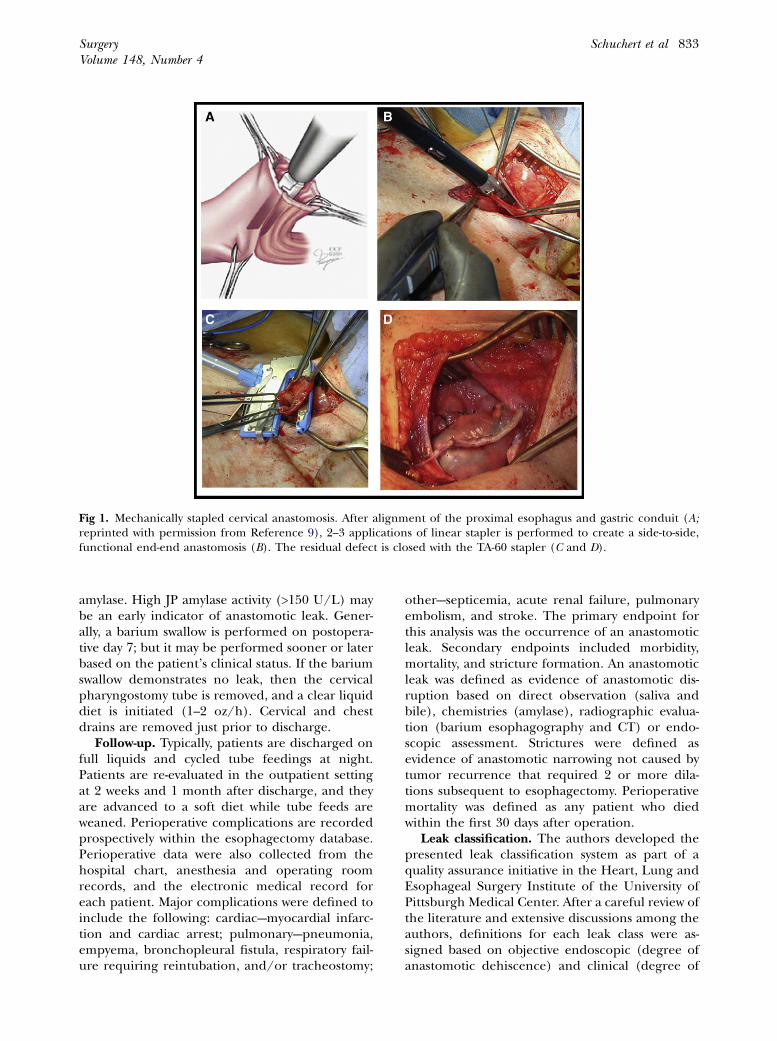
Fig 1. Mechanically stapled cervical anastomosis. After alignment of the proximal esophagus and gastric conduit (A;reprinted with permission from Reference 9), 2--3 applications of linear stapler is performed to create a side-to-side,functional end-end anastomosis (B). The residual defect is closed with the TA-60 stapler (C and D).
SurgeryVolume 148, Number 4
Schuchert et al 833
amylase. High JP amylase activity (>150 U/L) maybe an early indicator of anastomotic leak. Gener-ally, a barium swallow is performed on postopera-tive day 7; but it may be performed sooner or laterbased on the patient’s clinical status. If the bariumswallow demonstrates no leak, then the cervicalpharyngostomy tube is removed, and a clear liquiddiet is initiated (1--2 oz/h). Cervical and chestdrains are removed just prior to discharge.
Follow-up. Typically, patients are discharged onfull liquids and cycled tube feedings at night.Patients are re-evaluated in the outpatient settingat 2 weeks and 1 month after discharge, and theyare advanced to a soft diet while tube feeds areweaned. Perioperative complications are recordedprospectively within the esophagectomy database.Perioperative data were also collected from thehospital chart, anesthesia and operating roomrecords, and the electronic medical record foreach patient. Major complications were defined toinclude the following: cardiac---myocardial infarc-tion and cardiac arrest; pulmonary---pneumonia,empyema, bronchopleural fistula, respiratory fail-ure requiring reintubation, and/or tracheostomy;
other---septicemia, acute renal failure, pulmonaryembolism, and stroke. The primary endpoint forthis analysis was the occurrence of an anastomoticleak. Secondary endpoints included morbidity,mortality, and stricture formation. An anastomoticleak was defined as evidence of anastomotic dis-ruption based on direct observation (saliva andbile), chemistries (amylase), radiographic evalua-tion (barium esophagography and CT) or endo-scopic assessment. Strictures were defined asevidence of anastomotic narrowing not caused bytumor recurrence that required 2 or more dila-tions subsequent to esophagectomy. Perioperativemortality was defined as any patient who diedwithin the first 30 days after operation.
Leak classification. The authors developed thepresented leak classification system as part of aquality assurance initiative in the Heart, Lung andEsophageal Surgery Institute of the University ofPittsburgh Medical Center. After a careful review ofthe literature and extensive discussions among theauthors, definitions for each leak class were as-signed based on objective endoscopic (degree ofanastomotic dehiscence) and clinical (degree of
Fig 2. Class 1 leak. (A) Esophagogastroduodenoscopy demonstrates a punctate anastomotic defect (reprinted with per-mission from Reference 11). (B) Barium swallow reveals a small, contained area of extravasation that may communicatewith the JP drain. (C) CT scan shows a small collection of fluid and air outside of the anastomosis. Such leaks can bemanaged successfully by conservative measures, including bowel rest and intravenous antibiotics.
Fig 3. Class 2 leak. (A) Endoscopic evaluation demonstrates a small (<10% of anastomotic circumference) defect (reprin-ted with permission from Reference 12). (B) Esophagram reveals contrast extravasation in the region of the anastomosisnot adequately controlled by previously placed drains. (C) CT confirms the presence of a perianastomotic abscess. Man-agement includes cervical drainage and intravenous antibiotics.
SurgeryOctober 2010
834 Schuchert et al
intervention required) parameters and were ap-proved by the research group overseeing thisproject. The approved classification system wasthen applied retrospectively to the presentedesophagectomy cohort. Patients with confirmedanastomotic leaks were classified with the followingscale (Figs 2--5)11-14: class 1: radiographic leak only,no intervention; class 2: leak (<10% of circumfer-ence) requiring cervical and/or percutaneousdrainage; class 3: disruption of anastomosis (10--50% circumference) with perianastomotic abscessand associated pleural or mediastinal collectionrequiring video-assisted thoracoscopic surgery(VATS) or thoracotomy; and class 4: gastric tipnecrosis with anastomotic separation (>50%circumference).
Statistical analysis. Comparisons of patients withand without anastomotic leak were performed on
the basis of clinical, demographic, and pathologicdata. The Student t test was used to compare thedistributions of continuous data (age, duration ofstay, number of dilations), and the Fisher exacttest was used to compare the frequencies of cate-gorical measures (morbidity, mortality, and stric-ture formation) among groups. All comparisonswere 2-tailed.
RESULTS
Patient and tumor characteristics. Patient andtumor characteristics are summarized in Table I.The mean age for the entire cohort was 65 years.The male:female ratio was 180:55. Adenocarci-noma was the most commonly encountered tumor(81%), followed by squamous cell carcinoma(16%). Neoadjuvant therapy was employed in 37(16%) of patients. No significant differences were
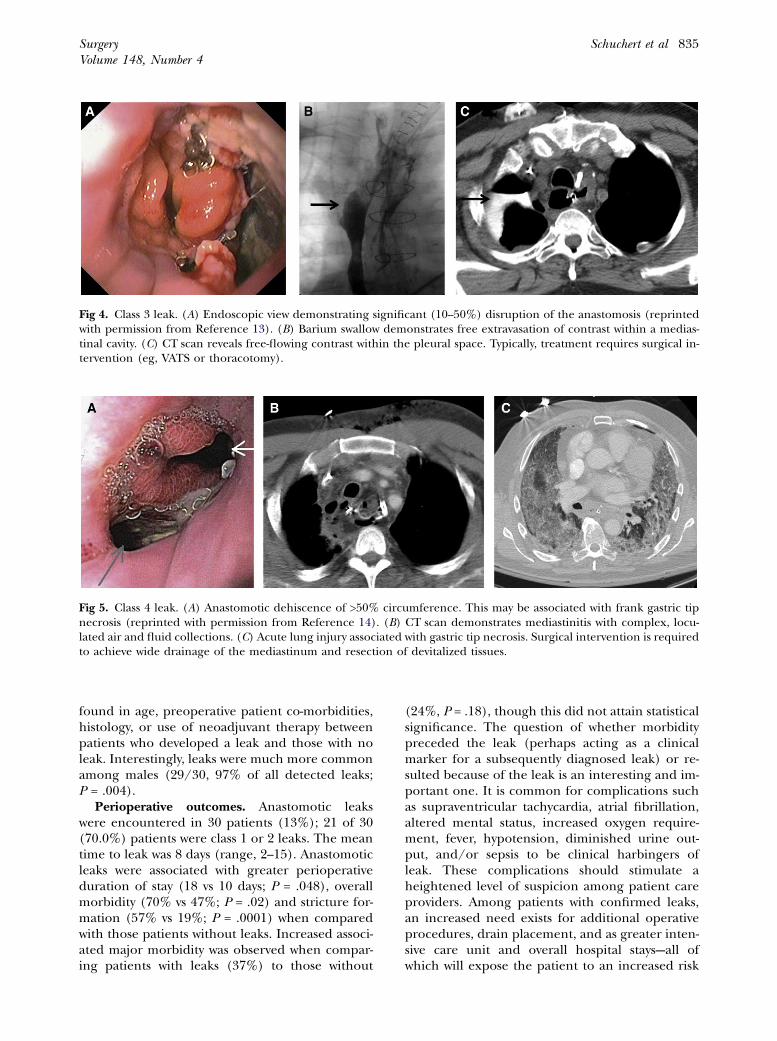
Fig 4. Class 3 leak. (A) Endoscopic view demonstrating significant (10--50%) disruption of the anastomosis (reprintedwith permission from Reference 13). (B) Barium swallow demonstrates free extravasation of contrast within a medias-tinal cavity. (C) CT scan reveals free-flowing contrast within the pleural space. Typically, treatment requires surgical in-tervention (eg, VATS or thoracotomy).
Fig 5. Class 4 leak. (A) Anastomotic dehiscence of >50% circumference. This may be associated with frank gastric tipnecrosis (reprinted with permission from Reference 14). (B) CT scan demonstrates mediastinitis with complex, locu-lated air and fluid collections. (C) Acute lung injury associated with gastric tip necrosis. Surgical intervention is requiredto achieve wide drainage of the mediastinum and resection of devitalized tissues.
SurgeryVolume 148, Number 4
Schuchert et al 835
found in age, preoperative patient co-morbidities,histology, or use of neoadjuvant therapy betweenpatients who developed a leak and those with noleak. Interestingly, leaks were much more commonamong males (29/30, 97% of all detected leaks;P = .004).
Perioperative outcomes. Anastomotic leakswere encountered in 30 patients (13%); 21 of 30(70.0%) patients were class 1 or 2 leaks. The meantime to leak was 8 days (range, 2--15). Anastomoticleaks were associated with greater perioperativeduration of stay (18 vs 10 days; P = .048), overallmorbidity (70% vs 47%; P = .02) and stricture for-mation (57% vs 19%; P = .0001) when comparedwith those patients without leaks. Increased associ-ated major morbidity was observed when compar-ing patients with leaks (37%) to those without
(24%, P = .18), though this did not attain statisticalsignificance. The question of whether morbiditypreceded the leak (perhaps acting as a clinicalmarker for a subsequently diagnosed leak) or re-sulted because of the leak is an interesting and im-portant one. It is common for complications suchas supraventricular tachycardia, atrial fibrillation,altered mental status, increased oxygen require-ment, fever, hypotension, diminished urine out-put, and/or sepsis to be clinical harbingers ofleak. These complications should stimulate aheightened level of suspicion among patient careproviders. Among patients with confirmed leaks,an increased need exists for additional operativeprocedures, drain placement, and as greater inten-sive care unit and overall hospital stays---all ofwhich will expose the patient to an increased risk
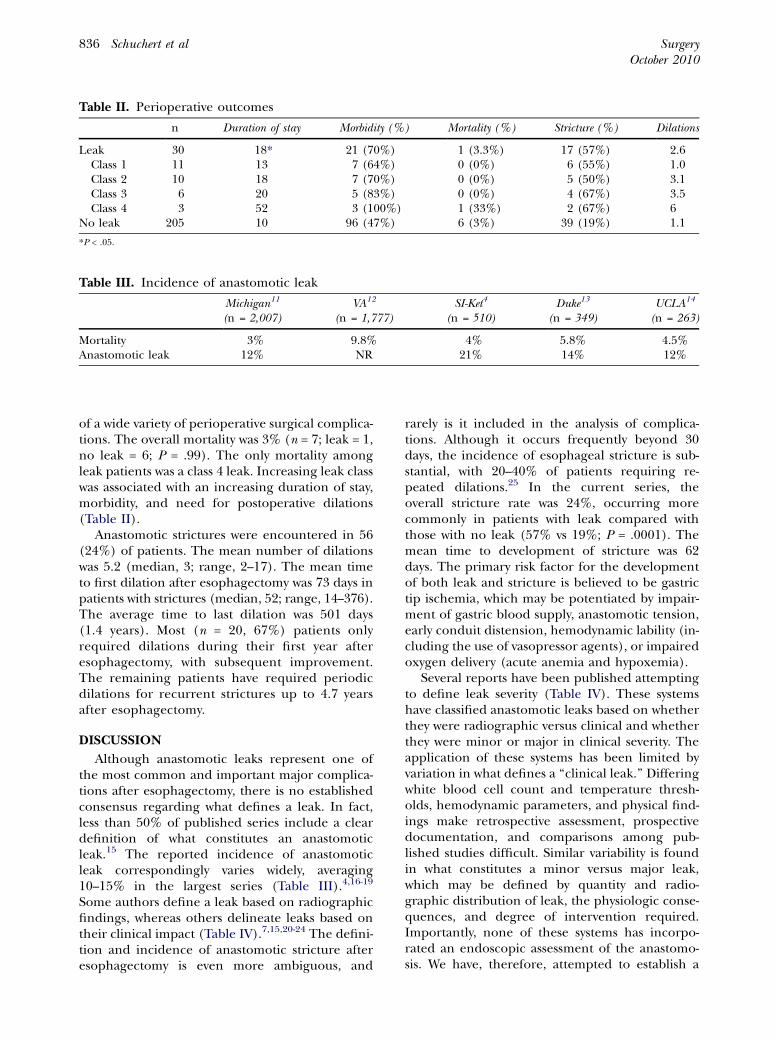
Table II. Perioperative outcomes
n Duration of stay Morbidity (%) Mortality (%) Stricture (%) Dilations
Leak 30 18* 21 (70%) 1 (3.3%) 17 (57%) 2.6Class 1 11 13 7 (64%) 0 (0%) 6 (55%) 1.0Class 2 10 18 7 (70%) 0 (0%) 5 (50%) 3.1Class 3 6 20 5 (83%) 0 (0%) 4 (67%) 3.5Class 4 3 52 3 (100%) 1 (33%) 2 (67%) 6
No leak 205 10 96 (47%) 6 (3%) 39 (19%) 1.1
*P < .05.
Table III. Incidence of anastomotic leak
Michigan11
(n = 2,007)VA12
(n = 1,777)SI-Ket4
(n = 510)Duke13
(n = 349)UCLA14
(n = 263)
Mortality 3% 9.8% 4% 5.8% 4.5%Anastomotic leak 12% NR 21% 14% 12%
SurgeryOctober 2010
836 Schuchert et al
of a wide variety of perioperative surgical complica-tions. The overall mortality was 3% (n = 7; leak = 1,no leak = 6; P = .99). The only mortality amongleak patients was a class 4 leak. Increasing leak classwas associated with an increasing duration of stay,morbidity, and need for postoperative dilations(Table II).
Anastomotic strictures were encountered in 56(24%) of patients. The mean number of dilationswas 5.2 (median, 3; range, 2--17). The mean timeto first dilation after esophagectomy was 73 days inpatients with strictures (median, 52; range, 14--376).The average time to last dilation was 501 days(1.4 years). Most (n = 20, 67%) patients onlyrequired dilations during their first year afteresophagectomy, with subsequent improvement.The remaining patients have required periodicdilations for recurrent strictures up to 4.7 yearsafter esophagectomy.
DISCUSSION
Although anastomotic leaks represent one ofthe most common and important major complica-tions after esophagectomy, there is no establishedconsensus regarding what defines a leak. In fact,less than 50% of published series include a cleardefinition of what constitutes an anastomoticleak.15 The reported incidence of anastomoticleak correspondingly varies widely, averaging10--15% in the largest series (Table III).4,16-19
Some authors define a leak based on radiographicfindings, whereas others delineate leaks based ontheir clinical impact (Table IV).7,15,20-24 The defini-tion and incidence of anastomotic stricture afteresophagectomy is even more ambiguous, and
rarely is it included in the analysis of complica-tions. Although it occurs frequently beyond 30days, the incidence of esophageal stricture is sub-stantial, with 20--40% of patients requiring re-peated dilations.25 In the current series, theoverall stricture rate was 24%, occurring morecommonly in patients with leak compared withthose with no leak (57% vs 19%; P = .0001). Themean time to development of stricture was 62days. The primary risk factor for the developmentof both leak and stricture is believed to be gastrictip ischemia, which may be potentiated by impair-ment of gastric blood supply, anastomotic tension,early conduit distension, hemodynamic lability (in-cluding the use of vasopressor agents), or impairedoxygen delivery (acute anemia and hypoxemia).
Several reports have been published attemptingto define leak severity (Table IV). These systemshave classified anastomotic leaks based on whetherthey were radiographic versus clinical and whetherthey were minor or major in clinical severity. Theapplication of these systems has been limited byvariation in what defines a ‘‘clinical leak.’’ Differingwhite blood cell count and temperature thresh-olds, hemodynamic parameters, and physical find-ings make retrospective assessment, prospectivedocumentation, and comparisons among pub-lished studies difficult. Similar variability is foundin what constitutes a minor versus major leak,which may be defined by quantity and radio-graphic distribution of leak, the physiologic conse-quences, and degree of intervention required.Importantly, none of these systems has incorpo-rated an endoscopic assessment of the anastomo-sis. We have, therefore, attempted to establish a

Table IV. Previously published leak classifications10
Reference Grade Definition
Csendes et al20 Type 1—subclinical Local leak without dissemination of contrast into bodycavities or drains
Type 2---clinical Great dissemination or fistula involving body cavities ordrains
Bardini et al7 Radiologic/minor Asymptomatic; radiographic evidence onlyClinical/moderate Fever, leukocytosis, local inflammationSerious Early leak with severe disruption of the anastomosisNecrosis Total disruption resulting from inadequate blood supply
Deshmane et al21 Small, asymptomatic Radiographic evidence onlyLarge, clinical Perianastomotic collection manifested clinically
Isozaki et al22 Major Leakage limited to a small area around anastomotic siteMinor Extensive leakage within body cavity or drain
Nambirajan et al23 Incidental Small radiographic leak; asymptomaticMinor Saliva in chest drain, but clinically wellMajor Mediastinitis, abscess, empyema, major disruption
Bruce et al15 Radiologic Small radiographic leak; asymptomatic—no change inmanagement
Clinical minor Leakage through wound or drain—inflammation,leukocytosis
Clinical major Severe disruption of anastomosis—change in clinicalmanagement
Lerut et al24 Radiologic Small radiographic leak; asymptomatic—no change inmanagement
Clinical minor Leakage through wound/drain (inflammation,leukocytosis)—drain, abx
Clinical major Major disruption, sepsis—CT/surgical interventionConduit necrosis Endoscopic confirmation—surgical intervention
SurgeryVolume 148, Number 4
Schuchert et al 837
classification based on discrete, objective endo-scopic (degree of anastomotic dehiscence), andclinical (degree of intervention required) parame-ters. In the current series, anastomotic leaks wereencountered in 13% of patients. When applyingthe classification system to these patients, we foundthat increasing leak class was associated with in-creasing duration of stay, morbidity, and numberof dilations required secondary to anastomoticstricture (Table II). It is likely that a fraction ofsmall, subclinical leaks will not be detected by bar-ium esophagography, endoscopy, drain outputs, orhospital course. These patients might be expectedhave a clinical course similar to the class 1 leak cat-egory. It is, therefore, possible that we are underes-timating, to a degree, the number of true class1 leaks given their minimal clinical manifestationsand/or impact on management.
The clinical impact of anastomotic leaks peri-operatively can range from trivial to severe, and itis associated with substantial increases in durationof stay and patient morbidity (Table II). The pa-tient care team must maintain a high level of vigi-lance in the postoperative period to recognize andmanage anastomotic leaks promptly and their
associated complications. With coordinated andaggressive surgical and intensive care unit care,the vast majority of patients can be salvaged, evenin the setting of major (class 3 or 4) leaks. It isimportant to recognize that the implications ofanastomotic leakage extend far beyond the pa-tient’s initial hospitalization. The development ofanastomotic strictures (57% among patients withleaks in this series) that required multiple dilations(mean, 5.2; range, 2--17) can have a long-term im-pact on patient swallowing and quality of life. In ad-dition, anastomotic complications increase overallconvalescence time that might extend beyond theinitial hospital stay and might delay or negate thecandidacy of patients for adjuvant chemotherapy.
Limitations of the current study include theretrospective nature of the analysis, which willintroduce the possibility of surgical, and selectionbias. The small sample size in this analysis limitsthe ability to discriminate differences in morbidity,mortality, and need for dilation among the indi-vidual classes. Another limitation of this study isthat the current analysis is restricted to patientswho underwent transhiatal esophagectomy. Thissystem will need to undergo subsequent evaluation

SurgeryOctober 2010
838 Schuchert et al
in the context of different esophagectomy ap-proaches (eg, Ivor Lewis, 3 hole, left thoracoab-dominal---whether minimally invasive or open).This classification system will also need to bevalidated using an independent data set and willbe best applied during prospective data collection.
In conclusion, anastomotic integrity afteresophagectomy has a significant impact on peri-operative course and long-term swallowing func-tion. Even class 1 and class 2 leaks can beassociated with important morbidity. The severityof anastomotic leaks after esophagectomy seems tocorrelate with postoperative morbidity. For severeleaks (classes 3 and 4), an aggressive surgicalapproach to resect devitalized tissue and establishwide drainage remains the hallmark of care andwill salvage most patients. We anticipate that thisclassification will provide a simple and objectivemeans of describing leak severity that will allowcomparisons among different esophagectomy ap-proaches, anastomotic techniques, and studies.
The authors acknowledge the important contributionof Peg Reamer and Judy Forster in clinical trial enroll-ment. We also to recognize Lorraine Ickes of the Tho-racic Surgery Tumor Registry for her assistance indatabase management and analysis. We thank KimberlyBurke, Lauren Matteo, Patricia Williams, Diane Sabilla,and Maria Haffely for their assistance in organizing andanalyzing hospital charts and in providing timely up-dates regarding patient follow-up.
REFERENCES
1. Dewar L, Gelfand G, Finley RJ, Evans K, Inculet R, NelemsB. Factors affecting cervical anastomotic leak and strictureformation following esophagogastrectomy and gastric tubeinterposition. Am J Surg 1992;163:484-9.
2. Mitchell JD. Anastomotic leak after esophagectomy. ThorSurg Clin 2006;16:1-9.
3. Rindani R, Martin CJ, Cox MR. Transhiatal versus Ivor Lewisesophagectomy: is there a difference? ANZ J Surg 1999;69:187-94.
4. Rizk NP, Bach PB, Schrag D, Bains MS, Turnbull AD, Kar-peh M, et al. The impact of complications on outcomes af-ter resection for esophageal and gastroesophageal junctioncarcinoma. J Am Coll Surg 2004;198:42-50.
5. Donington JS. Functional conduit disorders after esopha-gectomy. Thor Surg Clin 2006;16:53-62.
6. Mathisen DJ, Grillo HC, Wilkins EW Jr, Moncure AC, Hilgen-berg AD. Transthoracic esophagectomy: a safe approach to car-cinoma of the esophagus. Ann Thorac Surg 1988;45:137-43.
7. Bardini R, Asolati M, Ruol A, Bonavina L, Baseggio S, Perac-chia A. Anastomosis. World J Surg 1994;18:373-8.
8. Santos RS, Raftopoulos Y, Singh D, DeHoyos A, FernandoHC, Keenan RJ, et al. Utility of total mechanical stapled cer-vical esophagogastric anastomosis after esophagectomy: acomparison to conventional anastomotic techniques. Sur-gery 2004;136:917-25.
9. Ercan S, Rice TW, Murthy SC, Rybicki LA, Blackstone EH.Does esophagogastric anastomotic technique influence
the outcome of patients with esophageal cancer? J ThoracCardiovasc Surg 2005;29:623-31.
10. Schuchert MJ, Pettiford BL, Landreneau JP, Waxman J, KilicA, Santos RS, et al. Transcervical gastric tube drainage facil-itates patient mobility and reduces the risk of pulmonarycomplications after esophagectomy. J Gastrointest Surg2008;12:1479-84.
11. Nardella JE, Van Raemdonck D, Piessevaux H, Deprez P,Droissart R, Staudt JP, et al. Gastro-tracheal fistula--unusualand life threatening complication after esophagectomy forcancer: a case report. J Cardiothorac Surg 2009;4:69.
12. Scharf JG, Ramadori G, Becker H, Muller A. Implantationof a colorectal stent as a therapeutic approach in the treat-ment of esophageal leakage. BMC Gastroenterol 2007;7:10.
13. Schubert D, Pross M, Nestler G, Ptok H, Scheidbach H,Fahlke J, et al. [Endoscopic treatment of mediastinal anas-tomotic leaks]. Zentralbl Chir 2006;131:369-75.
14. Nguyen NT, Mailey BA, Hinojosa MW, Chang K. Natural or-ifice management of anastomotic leaks after minimally inva-sive esophagogastrectomy. Surg Innov 2008;15:249-52.
15. Bruce J, Krukowski ZH, Al-Khairy G, Russell EM, Park KGM.Systematic review of the definition and measurement ofanastomotic leak after gastrointestinal surgery. Br J Surg2001;88:1157-68.
16. Orringer MB, Marshall B, Chang AC, Lee J, Pickens A, LauCL. Two thousand transhiatal esophagectomies: changingtrends, lessons learned. Ann Surg 2007;246:363-74.
17. Bailey SH, Bull DA, Harpole DH, Rentz JJ, Neumayer LA,Pappas TN, et al. Outcomes after esophagectomy: a ten-year prospective cohort. Ann Thorac Surg 2003;75:217-22.
18. Atkins BZ, Shah AS, Hutcheson KA, Mangum JH, PappasTN, Harpole DH Jr, et al. Reducing hospital morbidityand mortality following esophagectomy. Ann Thorac Surg2004;78:1170-6.
19. Portale G, Hagen JA, Peters JH, Chan LS, DeMeester SR,Gandamihardja TA, et al. Modern 5-year survival of resecta-ble esophageal adenocarcinoma: single-institution experi-ence with 263 patients. J Am Coll Surg 2006;202:588-96.
20. Csendes A, Diaz JC, Burdiles P, Braghetto I, Maluenda F,Nava O, et al. Classification and treatment of anastomoticleakage after extended total gastrectomy in gastric carci-noma. Hepatogastroenterol 1990;37(Suppl 2):174-7.
21. Deshmane VH, Shinde SR. The cervical esophagogastricanastomotic leak. Dis Esoph 1994;7:42-6.
22. Isozaki H, Okajima K. How to reduce surgical complicationsafter extended gastric surgery. Dis Surg 1994;11:78-85.
23. Nambirajan L, Rintala RJ, Losty PD, Carty H, Lloyd DA.The value of early post-operative oesophagography follow-ing repair of oesophageal atresia. Pediatr Surg Int 1998;13:76-8.
24. Lerut T, Coosemans W, Decker G, De Leyn P, Nafteaux P,Van Remdonck D. Anastomotic complications after esopha-gectomy. Dig Surg 2002;19:92-8.
25. Rice TW. Anastomotic stricture complicating esophagec-tomy. Thor Surg Clin 2006;16:63-73.
DISCUSSION
Dr Louis Bernhardt (Madison, WI): I have a couple ofquestions, and some of these you answered on the slides.You used the drain, and I see that it was a soft drainrather than a somewhat harder Jackson-Pratt or BlakeDrain, harder drain. So, when you did drain, did youpull the drain at any particular time and was this in rela-tion to when you began to feed the patient? You have astandardized approach for the surgeons in your group.

SurgeryVolume 148, Number 4
Schuchert et al 839
Did you happen to use the so-called ‘‘camera bag’’ tohelp pull up the stomach so that the vascular supply ofthe stomach was not impaired? Did you do a pyloromyot-omy or a pyloroplasty as an emptying procedure to pre-vent gastric stasis and prevent delayed emptying? Thismight be a contribution to postoperative vomiting withintragastric pressure.
Dr Matthew Schuchert (Pittsburgh, PA): Thank youDr Bernhardt. I appreciate those insightful comments. Iagree wholeheartedly that we do not have an accurateassessment of the cause of leaks, based on the availabledata. We feel strongly that the number one contributorwas likely due to ischemia. Anything that might impairthe blood supply to the gastric tip could lead to anasto-motic failure. The second thing that we feel is parti-cularly important is avoiding gastric distensionpost-operatively. Early gastric distension will exacerbateany impairment in vascular supply. Those would be theprincipal etiologies of concern, but we agree that wecannot discern any clear cause on a case by case basiswith the data that’s available. With regard to your secondquestion, we do use a Jackson-Pratt drain and cervicalesophagostomy tube for cervical drainage. The JP drainand cervical esophagostomy tube are left in place untilthe barium swallow on postoperative day 7. If the swal-low is negative, clear liquids are initiated, and the cervi-cal esophagostomy drain is pulled. The JP drain istypically pulled the following day, and the patient is pre-pared for discharge. The third question relates to theuse of a camera bag to protect the conduit as we advancethe gastric tube from the abdomen to the neck. We doemploy this technique. I do feel that this will help to pro-tect the gastroepiploic arcade as the gastric conduit isdelivered to the neck. Other technical aspects thatmay contribute to the preservation of blood flow tothe gastric tip include a generous Kocher maneuver(which will help to minimize tension on the gastric con-duit), as well as the use of the whole stomach withoutsignificant gastric tubularization. Lastly, as part of ourstandardized approach, we typically perform a pyloro-myotomy to enhance gastric emptying.
Dr P. Marco Fisichella (Maywood, IL): I have 2 ques-tions and some general comments. First, you aimed tocorrelate the grading of anastomotic leaks to the clinicaloutcomes of patients undergoing transhiatal esophagec-tomy for cancer. By clinical outcomes you meant lengthof stay, morbidity, mortality, stricture, and dilatations.However, you showed only that the more severe the com-plication, the higher the length of stay and morbidity, al-though this association was not statistically significant,maybe because of the small number of leaks you encoun-tered in each class. Although the duration of hospitalstay is a useful and less arbitrary parameter of the severityof a complication within a single center, I have found nodefinition of morbidity in your study. Can you pleaseclarify what kind of morbidity did you take into account?Did you take into account a morbidity caused by the leakor a morbidity in a patient who had a leak and not nec-essarily caused by it?
Secondly, among those 250 patients who did not havea leak, you reported 6 deaths and 39 strictures, eachtreated, on average, with one dilatation, just as those 11patients in class 1 who did have a leak. Do you think it ispossible that some leaks went unnoticed? Finally, I amwondering if you are planning to test this classificationalso in patients who underwent transthoracic or mini-mally invasive esophagectomy in order to have only1 classification for esophageal leaks regardless of thesurgical technique used.
Dr Matthew Schuchert (Pittsburgh, PA): The datapresented on morbidity takes into account all other com-plications besides the anastomotic leaks. When compar-ing leak and no leak, leak-associated morbidity includesany complication, whether minor or major. When con-sidering the occurrence of any complication, a statisti-cally significant difference is noted. We found nostatistically significant difference in either major or mi-nor complications, however, when analyzed separately.There may be an important clinical difference, though,in major complications. Nearly 40% of patients in theanastomotic leak group had major complications,whereas only 23.9% of the no-leak group had major com-plications. But again, this did not attain statistical signif-icance. The most common major complications that wesaw among leaks were respiratory failure and pneumo-nia. The most common minor complication was atrial fi-brillation. It is unclear from the available data whethercomplications on a case-by-case basis were actuallycaused by the leak, or whether they arose from an inde-pendent inciting cause. The second question relates toClass I leaks. It certainly is possible that a fraction of pa-tients classified as no leak may have had a subclinicalleak not detected by barium swallow or clinical evalua-tion. We may be, therefore, be underestimating to a de-gree the overall rate of Class I leaks.
We do hope to use this leak classification system inpatients undergoing a transthoracic approach. Ourgroup has now performed over 1,000 minimally-invasiveesophagectomies, including the 3-hole and Ivor Lewisvariations. We are currently adopting this method ofclassification to these patients. That particular databaseis nearing completion, and we intend to break down thenumbers to see if similar trends emerge. It will beimportant to validate the findings of the current studywith these different approaches, and utilizing indepen-dent data sets from around the country.
Dr Margo Shoup (Maywood, IL): I think this is a greatfirst start to trying to come up with a classification forleaks, like we do in pancreas. The next step would be,now what do you do with that? What is the step thatyou do to treat those patients? My question is a littlebit different. Maybe you haven’t looked at it. But I no-ticed only 16% of your patients had neoadjuvant ther-apy. What are your criteria for giving neoadjuvanttherapy? At our institution, anybody who is T-3 or greateror N-1 or greater gets neoadjuvant, and that’s most ofthe patients. I understand there’s no study that showsthere’s a survival benefit from that. But I’m just curious,

SurgeryOctober 2010
840 Schuchert et al
of those who had neoadjuvant versus those that didn’t, isthere any difference in leak or the severity of leak?
Dr Matthew Schuchert (Pittsburgh, PA): The next stepwill be to validate this classification system with indepen-dent data sets. It is too early at present to speculatewhether this classification can be systematically appliedto guide therapeutic decision-making in a prospectivefashion. Certainly, however, this system provides an
objective measure of leak severity which can be comparedbetween studies. The use of neoadjuvant therapy at ourinstitution varies somewhat from surgeon to surgeon.Generally speaking, however, neoadjuvant therapy is em-ployed in bulky T3 or N1 tumors based upon thoroughpreoperative staging. We did not see a difference in ourleak or complication rates when comparing those patientsthat received neoadjuvant therapy with those that did not.
Related Documents











