Immuntherapie uroonkologischer Tumore Prof. Dr. med. Viktor Grünwald Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Immuntherapie uroonkologischerTumore
Prof. Dr. med. Viktor Grünwald
Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation

DisclosuresCompensated lectures:
BMS, Ipsen, Eisai, Novartis, Pfizer, Roche
Advisory: Bayer, BMS, Cerulean, Ipsen, Eisai, Novartis, Pfizer, Roche
Speaker‘s bureau:
Novartis, Pfizer
Research grants, stock shareholder:
none

Checkpunkt Blockade GU Tumore
Status Ergebnis
Nierenzellkarzinom Phase III positiv
Blasenkarzinom Phase III positiv
Prostatakarzinom Phase III negativ
Hodenkarzinom Basket Studie -
Peniskarzinom Basket Studie -

PD-L1+ als negativer Prädiktor
Das Bild kann zurzeit nicht angezeigt werden.
Gevensleben et al. (2016). CCR, 22(8), 1969–1977. Thompson et al. Proc Natl Acad Sci USA 2004;101:17174–9. Cierna et al. (2016). Annals of Oncology, 27(2), 300–305.
PCA NCC GCT

PD-L1 beim Peniskarzinom
Gut diff.
Moderat diff.
Schlecht diff.
Udager et al. (2016). Annals of Oncology, 27(9), 1706–1712. http://doi.org/10.1093/annonc/mdw216
62% PD-L1+N=37
Assoziation mit fortgeschrittenem Stadium

Inflammatorisches TCC – besseres OS
Bellmunt et al. (2015). Annals of Oncology, mdv009. doi:10.1093/annonc/mdv009
TIMC: tumor infiltrating monocytic cells
12 mo.
23 mo.
PD-L1+ TIMC analysed

PCA: Ipilimumab vs. Placebo
Kantoff et al. (2010). NEJM, 363(5), 411–422.

Mutationsspektrum solide Tumore
MS Lawrence et al. Nature 2013

PD-L1 ist nicht gleich PD-L1
Topalian et al. (2016). Nature Reviews Cancer, 16(5), 275–287. http://doi.org/10.1038/nrc.2016.36
Oncogen drivenPD-L1 expression
Oncogene PD-L1 expression +
Adaptive immunevasion
Immune cells Tumor cellsTumor cells, strong PD-L1+

PD-L1 nur im Kontext beurteilen
H&E PD-L1 TILs (CD3+)
Mansfield et al. (2016). Annals of Oncology, mdw289. http://doi.org/10.1093/annonc/mdw289
NSCLC (primary)
ZNS mets.
N=146 paired lesions, 73 cases. Discrepencies: 14% (tumor), 26% (TILs)

Immuntherapie –kein one-size-fits-all approach
CD8T cellwith
granzyme B
CD8T cell
with PD-L1expression
Immunogenic tumor
microenvironment
Nonimmunogenic tumormicroenvironment
Combination therapieswith agents that create
immunogenic tumormicroenvironment and
immune checkpoint therapy
Durable clinical benef tImmune checkpoint ther apyand durable clinical benef t
CD8T cell
with CD45ROexpression
CD8T cell
CD4T cell
Tumorcell
with PD-L1expression
BA
Sharma & Allison. The future of immune checkpoint therapy. (2015). The future of immune checkpoint therapy. Cancer
Immunology Immunotherapy, 1–7.
hot tumor
single agent
cold tumor
combination

Bevacizumab/Atezolizumab –verbessert T-Zell-Migration
Wallin et al. (2016). Nature Communications, 7, 12624. http://doi.org/10.1038/ncomms12624

IC3 RCC Patient: PR unter ATEZO
Herbst et al. (2014). Nature, 515(7528), 563–567. http://doi.org/10.1038/nature14011

Duale Checkpoint Blockade – die zukünftige Therapie des mRCC?
Hammers et al. ASCO 2015 #4516. Hammers et al. ESMO 2016: 1062P
IPI3 +
NIVO1
IPI1 +
NIVO3
ORR 40% 40%
PD 17% 17%
PFS 6,6 Mo. 9,1 Mo.

Resistenzmechanismen

Erworbene Resistenz (MM)
Zaretsky et al. (2016). NEJM, NEJMoa1604958. http://doi.org/10.1056/NEJMoa1604958
IFNγ-Resistenz
− JAK1/2 mt.
MHC-I Expr.− B2M mt.

Primäre Resistenz: JAK Mutationen
Shin et al. (2016) Cancer Discovery, 1–37. http://doi.org/10.1158/2159-8290.CD-16-1223

Was unterscheidet TKI von IO?

Besseres PFS unter TKI
Motzer et al. (2015). NEJM, 150925150201006–11.Choueiri et al. (2016). Lancet Oncol, pp. 1-11.

Bessere Verträglichkeit für IO
McDermottet al. (2016). JCO, 34(8), 833–842. Motzer RJ et al. N Engl J Med, 2015; 373: 1803–13. Choueiri et al. (2016) Lancet Oncology, 17(7), 917–927. http://doi.org/10.1016/S1470-2045(16)30107-3

Immuntherapie: bessere QoL
Cella, D., Grünwald, V., Nathan, P., Doan, J., Dastani, H., Taylor, F., et al. (2016). Lancet Oncology, 17(7), 994–1003. http://doi.org/10.1016/S1470-2045(16)30125-5

Risiken der Immuntherapie: Aggravation der Erkrankung
Champiat et al. (2016). CCR.1741.2016. http://doi.org/10.1158/1078-0432.CCR-16-1741

NIVOSWITCHearly switch to PD-1i
• ccRCC• 1st line TKI for 10-
12 wks.• PR or SD• ECOG: 0-2• MSKCC: all• No intolerance
N=244
Nivolumab 3mg/kgq2Wo.
TKI continuation
R
I°: OS rate at 2 yearsII°: ORR, OS, PFS

SUNNIFORECAST Sunitinib vs. Nivolumab+Ipilimumab as First line Treatment Of Renal cell Cancer of non-
clear cell SubTypes – an international prospective randomized trial
Key Inclusion Criteria
• Metastatic or locally advanced nccRCC: papillary, chromophobe, collecting duct carcinoma (CDC), renal medullary carcinoma (RMC), or translocation tumors and NOS
• Available tumor tissue
• Measurable disease as per RECIST v1.1
• ECOG performance status 0-2
• No prior systemic therapy for RCC
• No active CNS metastases
• No TKI contraindications
Start Date: Q3/2016Estimated Study Completion Date:Number of Sites ~30 (A, D, F, S, P)
PI: Prof. Dr. Lothar Bergmann, FrankfurtCo-Invest.: PD Dr. Peter Goebell, Erlangen
Phase II: N~284 pts.
Strata:
•Histological subtype•MSKCC score: Risk poor vs. other
• Primary Endpoint: Survival rate at 12 mths
• Key Secondary Endpoints:
• Survival rate at 6 and 18 mths
• ORR, TTP, OS, Safety, HR-QoL
• Exploratory Endpoints: biomarker e.g.PD-L1 expression of tumor, PD-1 expression of T cell subtypes etc.
R
1:1Sunitinib
50 mg PO oncedaily for 4 weeks followed
by 2 weeks off, every cycle
Nivolumab 3 mg/kg IV Ipilimumab 1 mg/kg IV
q3wfor 4 doses
then Nivolumab3 mg/kg IV q2w

Ziel der adjuvanten Therapie
− Heilung (i.e. Gesamtüberleben)

Adjuvante TKI-Therapie des NCC
Ravaud et al. (2016). NEJM. http://doi.org/10.1056/NEJMoa1611406Haas et al. (2016). Lancet, 387(10032), 2008–2016. http://doi.org/10.1016/S0140-6736(16)00559-6
S-TRAC ASSUREASSURE

Unverändertes Gesamtüberleben
S-TRAC ASSURE
Ravaud et al. (2016). NEJM. http://doi.org/10.1056/NEJMoa1611406Haas et al. (2016). Lancet, 387(10032), 2008–2016. http://doi.org/10.1016/S0140-6736(16)00559-6

NCC: adjuvante Therapie Start Q1 2017
Hochrisiko: − T2 G4− T3a G3-4− T3b-c/T4− TxN+
N=664
I°: DFS

Radiologisches Assessment
De Velasco et al. (2016). Cancer Immunology Research, 4(1), 12–17.
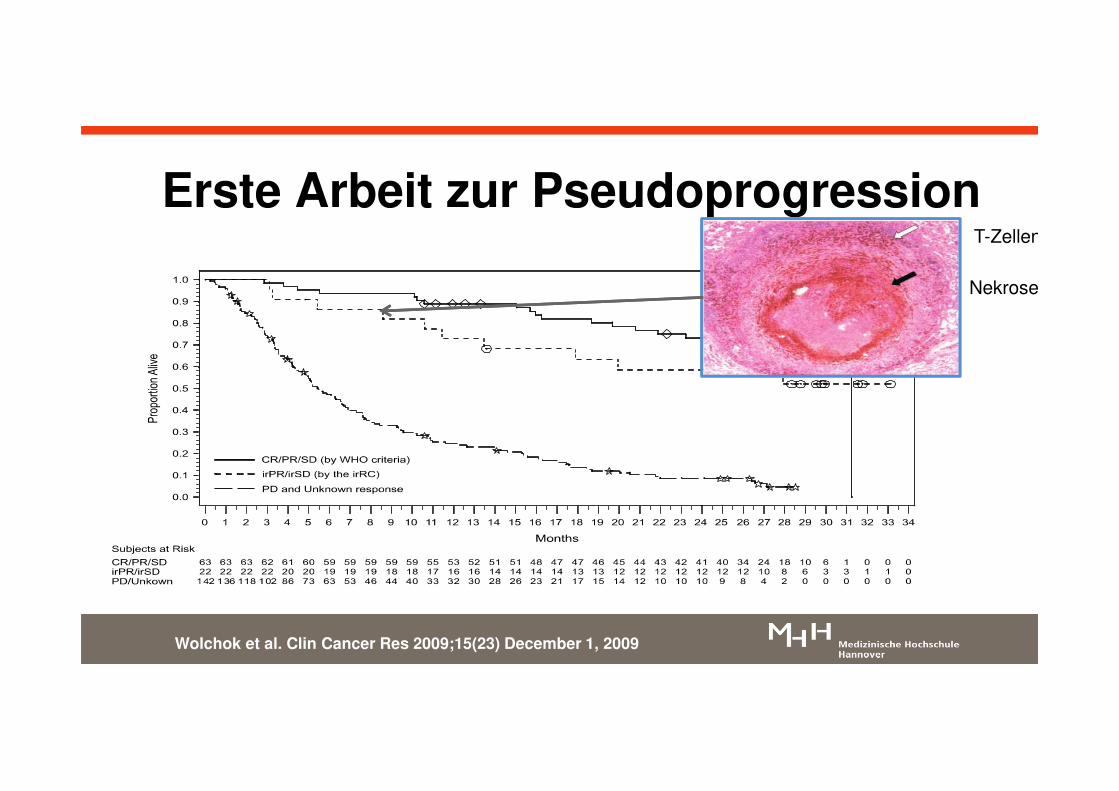
Erste Arbeit zur PseudoprogressionT-Zellen
Nekrose
Wolchok et al. Clin Cancer Res 2009;15(23) December 1, 2009

Urothelkarzinom

Systemtherapie des TCC
1st Linie- Cisplatin/Gemcitabine
- (DD-MVAC)
2nd Linie- Vinflunine
- Taxane- (Ifosfamide)
1st Linie: frail- Carboplatin/Gemcitabine
- Gemcitabine- Taxane
Bellmunt et al. ESMO Guidelines Working Group. (2014, September). Annals of Oncology. http://doi.org/10.1093/annonc/mdu223

Chemotherapie beim TCC
Bellmunt et al. (2012). JCO, 30(10), 1107–1113. Bellmunt et al. (2009). JCO, 27(27), 4454–4461. http://doi.org/10.1200/JCO.2008.20.5534
ORR: 44%OS: 12,7 Mo.PFS: 7,6 Mo.
Erstlinie Zweitlinie
ORR: 9%PFS: 3 Mo.

Langzeitüberleben unter CTX
PCG1
n=312GC1
n=314GC2
n=203MVAC2
n=202MVAC3
n=129DD-MVAC3
n=134
PFS (mo.) 7.6 8.3 7.7 8.3 8.2 9.1
2y-PFS rate - - 14% 18% 12 25
5y-PFS rate - - 10% 11% - -
OS (mo.) 15.8 12.7 14 15.2 14.1 15.5
2y-OS rate - - 25% 31% 25 35
5y-OS rate 17%* 16%* 13% 15% 10%§ 14%§
1Bellmunt et al. (2012). JCO, 30(10), 1107-11132van der Maase et al. (2005). JCO, 23(21), 4602–4608.3Sternberg et al. (2001). JCO, 19(10), 2638–2646.
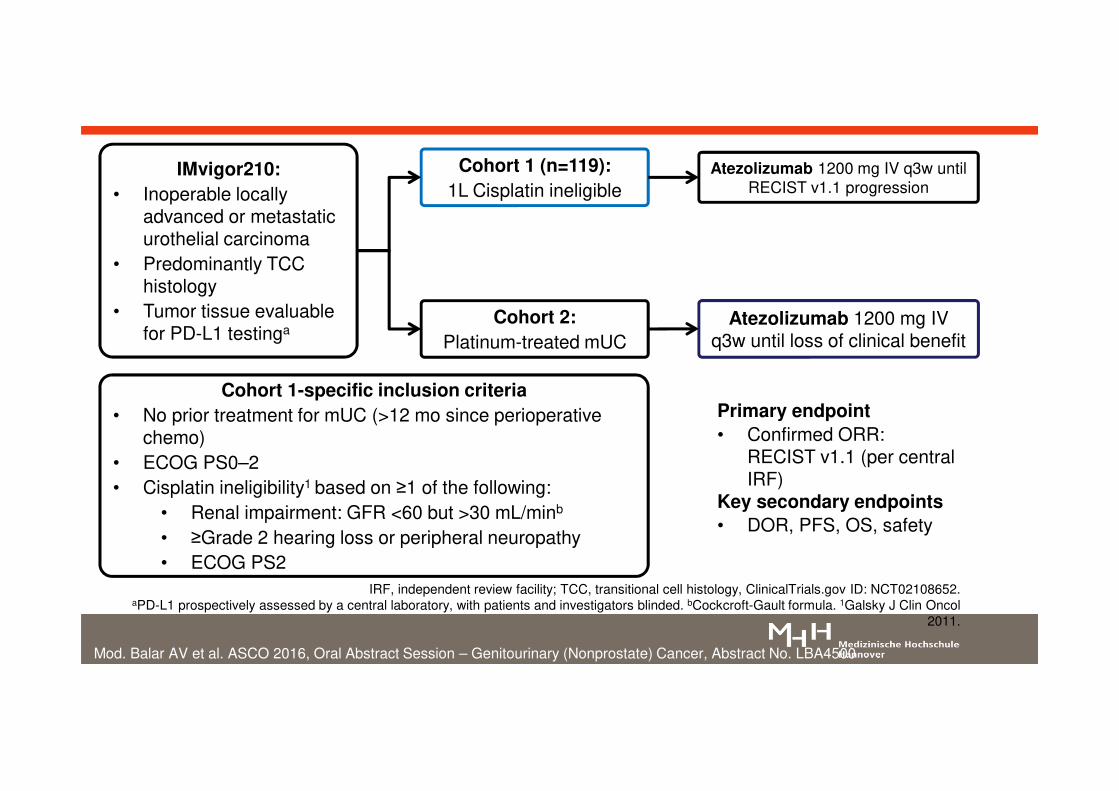
IMvigor210:
• Inoperable locally advanced or metastatic urothelial carcinoma
• Predominantly TCC histology
• Tumor tissue evaluable for PD-L1 testinga
Cohort 2:
Platinum-treated mUC
Cohort 1 (n=119):
1L Cisplatin ineligible
Atezolizumab 1200 mg IV q3w until loss of clinical benefit
Atezolizumab 1200 mg IV q3w until RECIST v1.1 progression
Cohort 1-specific inclusion criteria
• No prior treatment for mUC (>12 mo since perioperative chemo)
• ECOG PS0–2• Cisplatin ineligibility1 based on ≥1 of the following:
• Renal impairment: GFR <60 but >30 mL/minb
• ≥Grade 2 hearing loss or peripheral neuropathy• ECOG PS2
Primary endpoint
• Confirmed ORR: RECIST v1.1 (per central IRF)
Key secondary endpoints
• DOR, PFS, OS, safety
Mod. Balar AV et al. ASCO 2016, Oral Abstract Session – Genitourinary (Nonprostate) Cancer, Abstract No. LBA4500
IRF, independent review facility; TCC, transitional cell histology, ClinicalTrials.gov ID: NCT02108652.aPD-L1 prospectively assessed by a central laboratory, with patients and investigators blinded. bCockcroft-Gault formula. 1Galsky J Clin Oncol
2011.

1st Linie TCC: Atezolizumab(Platin-ungeeignet)
Bellmunt et al. ESMO 2016, 782PD
57%

TCC, transitional cell carcinoma. aPatients and investigators blinded to PD-L1 ICH status. Trial Identifier: NCT02108652.1Balar ASCO 2016 [abstract LBA4500].
2Rosenberg ASCO 2016 [abstract 104].)
• Locally advanced or metastatic urothelial carcinoma
• Predominantly TCC histology
• Tumor tissue for PD-L1 testinga
Cohort 1 presented earlier this morning1
Atezolizumab 1200 mg IV q3w until loss of benefit
Cohort 1 (n=119)1L Cisplatin ineligible
Cohort 2 (n=310)Platinum-treated mUC
Cohort 2-specific inclusion criteria
• Progression during/following Platinum (no restrictions on # prior lines of therapy)
• ECOG PS 0–1• CrCl ≥30mL/min
Median follow-up: 17.5 months
(range, 0.2 to 21.1+ mo)
Co-primary endpoints:• ORR (confirmed) per RECIST v1.1 by central review• ORR per immune-modified RECIST by investigatorKey secondary endpoints• DOR, PFS, OS, safetyKey exploratory endpoints• Biomarkers (To be presented by Rosenberg et al.,
Abstract #1042)

Gesamtüberleben: Atezolizumab
Loriot et al. ESMO 2016: 783P
IC0/1 n=210
IC2/3n=100
Alle Pts.N=310
OS; Mo.(95% CI)
6,7(5,4-8,0)
11,9(9,0-NE)
7,9 (6,7-9,3)
12-Mo. OS 31% 50% 37%

All treated patients
No. at RiskAll treated patients
PD-L1 <1%PD-L1 ≥1%
PD-L1 ≥1%
Median OS, Months (95% CI)a
All treated 8.74 (6.05–NR)
PD-L1 <1% 5.95 (4.30–8.08)
PD-L1 ≥1% 11.30 (8.74–NR)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 3 6 9 12 15
Overa
ll S
urv
ival (P
rob
ab
ilit
y)
Months
PD-L1 <1%
aSimilar results were seen using the 5% PD-L1 tumor expression cutoff; NR, not reached
265 198 148 63 5 0143 101 69 26 2 0122 97 79 37 3 0
Galsky et al. ESMO 2016: LBA31
27% mit Vinflunin
22% mit BSC ca. 40%
Nivolumab (Platin-vorbehandelt)

Checkpunkt Blockade beim TCC
ATEZO1 ATEZO2 NIVO3 NIVO4 PEMBRO5 AVELU6
N 119 310 78 270 100 129
Linie CDDPungeeignet
≥2. ≥2. ≥2. CDDPungeeignet
≥2. oderCDDP ungeeignet
CR (%) 7 7 6 2 6 3
PR (%) 17 16 18 17 18 14
OS (mo.) 14.8 7.9 9.7 8.7 - -
1Balar et al. ASCO 2016 #4500. 2Dreicer et al.ASCO 2016 #4515. 3Sharma et al. ASCO 2016 #4501. 4Galsky et al. ESMO 2016 LBA31. 5Balar et al. ESMO 2016 LBA32. 6Patel ESMO 2016: 2534




SAUL Studie
Testsubstanz: Atezolizumab
Einschlusskriterien:
• Lokal fortgeschrittenes (T4, jedes N oder jedes T, N 2-3) oder metastasiertes Urothelkarzinom (M1, Stage IV) oder nicht-urotheliales Karzinom
• Zweitlinienchemotherapie geeignet

TCC: wenig aktivierende Mutationen
TCGA network. (2014). Comprehensive molecular characterization of urothelial bladdercarcinoma. Nature, 507(7492), 315–322. doi:10.1038/nature12965

Neue Ansätze zur molekularen Rx
TCGA network. (2014). Comprehensive molecular characterization of urothelialbladder carcinoma. Nature, 507(7492), 315–322. doi:10.1038/nature12965

Molekulare Therapiestudien
Substanz Inhibition Phase Mol. Stratum*
offen Ident
BEZ235 PI3K/mTOR II + - NCT01856101
Buparlisib PI3K II NR (+) NCT01551030
Dovitinib VEGFR/FGFR II + - NCT01732107
BGJ398 FGFR I/II + + NCT01004224
Nintedanib VEGFR/FGFR II + - NCT02278978
BAY1163877 FGFR I/II + + NCT01976741
LY3076226 FGFR3 mAb I + + NCT02529553
B-701 FGFR3 mAb II + + NCT02401542
Palbociclib CDK4/6 II + + NCT02334527
*Stratifizierung nach Mutation, Amplifikation, Überexpression, Aktivierung und/oder Wildtyp
www.clinicaltrials.gov

FGFR Inhibition
Testsubstanz: Erdafitinib (pan FGFR Inhibitor)
Einschlusskriterien:
• metastasiertes oder inoperables Urothelzellkarzinom (cT4b, N+ oder M+)
• progrediente Erkrankung
• FGFR mutiert

Zusammenfassung
• Adjuvante Therapie – noch kein Standard beim NCC
• Erstlinie: neuer Standard in 2017 möglich
• Zweitlinie: Nivolumab, Cabozantinib & Lenvatinib/Everolimus sind Optionen mit OS-Vorteil
• Keine Rationale in der Therapieauswahl
• PD-L1 ist kein optimaler prädiktiver Marker
• Kombinationen und Therapieoptimierung sind aktuelle Studienkonzepte
Related Documents











