Immunological Basis of Vaccination D. Paul Lunn, BVSc, MS, PhD, MRCVS, Dip. ACVIM Author’s Address: Department of Medical Sciences, School of Veterinary Medicine, University of Wisconsin, 2015 Linden Drive West, Madison, Wisconsin 53706. © 2000 AAEP. Introduction Equine veterinarians are faced with new commer- cial vaccines, new efficacy claims, and potential side effects, combined with an increased awareness of the questionable efficacy of established vaccines. These complex issues require of equine veterinari- ans a more comprehensive understanding of vaccine immunology in order to be able to judge this infor- mation. The future promises further change and controversy. The aim of this paper is to provide a review of the basic immunological processes that are critical to an understanding of the process of vaccination. Currently a wide variety of vaccines are available for use in horses but the efficacy of these products varies widely despite the fact that many of these vaccines are similar in design, containing killed or- ganisms or toxoids combined with simple adjuvants. A significant reason for this is that this single type of vaccination strategy will stimulate only one array of immune responses. In the case of infections like tetanus, the inactivated toxoid vaccine generates neutralizing antibodies that are highly successful in providing long-term complete protection. How- ever, in the case of viral infections, such as equine influenza virus, current inactivated virus vaccines fail to induce the complete spectrum of immune re- sponses required for lasting and effective protection. The first step to overcoming the limitations of cur- rent vaccines is understanding what type of immune responses are required to protect against a specific pathogen. Components of the Immune Response Our total immune defenses include both innate re- sponses, such as neutrophils or complement, and adaptive responses, mediated by lymphocytes, which result in immunological memory. Only adaptive responses can be induced by vaccination. The specificity of adaptive responses, mediated by antibodies or by effector cells such as cytotoxic T- lymphocytes (CTLs), is responsible for their capacity to completely protect an animal against a particular pathogen. The principal types of immune effectors, including antibodies and lymphocytes, relevant ac- cessory factors, and examples of infectious agents against which they are most effective are listed in Table 1. There are some over-simplifications; for example, IgG is considered as a single type of im- munoglobulin, while in reality there are different sub-classes of IgG with different functions. To un- derstand how these different types of immune re- sponses are induced it is necessary to have a rudimentary understanding of the biology of lym- phocytes, as it is these cells that govern the adaptive immune responses that we need to generate with vaccines. AAEP PROCEEDINGS / Vol. 46 / 2000 1 IN DEPTH: VACCINATION NOTES Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS Proceedings of the Annual Convention of the AAEP 2000

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Immunological Basis of Vaccination
D. Paul Lunn, BVSc, MS, PhD, MRCVS, Dip. ACVIM
Author’s Address: Department of Medical Sciences, School of Veterinary Medicine, University ofWisconsin, 2015 Linden Drive West, Madison, Wisconsin 53706. © 2000 AAEP.
Introduction
Equine veterinarians are faced with new commer-cial vaccines, new efficacy claims, and potential sideeffects, combined with an increased awareness ofthe questionable efficacy of established vaccines.These complex issues require of equine veterinari-ans a more comprehensive understanding of vaccineimmunology in order to be able to judge this infor-mation. The future promises further change andcontroversy. The aim of this paper is to provide areview of the basic immunological processes thatare critical to an understanding of the process ofvaccination.
Currently a wide variety of vaccines are availablefor use in horses but the efficacy of these productsvaries widely despite the fact that many of thesevaccines are similar in design, containing killed or-ganisms or toxoids combined with simple adjuvants.A significant reason for this is that this single type ofvaccination strategy will stimulate only one array ofimmune responses. In the case of infections liketetanus, the inactivated toxoid vaccine generatesneutralizing antibodies that are highly successful inproviding long-term complete protection. How-ever, in the case of viral infections, such as equineinfluenza virus, current inactivated virus vaccinesfail to induce the complete spectrum of immune re-sponses required for lasting and effective protection.The first step to overcoming the limitations of cur-
rent vaccines is understanding what type of immuneresponses are required to protect against a specificpathogen.
Components of the Immune Response
Our total immune defenses include both innate re-sponses, such as neutrophils or complement, andadaptive responses, mediated by lymphocytes,which result in immunological memory. Onlyadaptive responses can be induced by vaccination.The specificity of adaptive responses, mediated byantibodies or by effector cells such as cytotoxic T-lymphocytes (CTLs), is responsible for their capacityto completely protect an animal against a particularpathogen. The principal types of immune effectors,including antibodies and lymphocytes, relevant ac-cessory factors, and examples of infectious agentsagainst which they are most effective are listed inTable 1. There are some over-simplifications; forexample, IgG is considered as a single type of im-munoglobulin, while in reality there are differentsub-classes of IgG with different functions. To un-derstand how these different types of immune re-sponses are induced it is necessary to have arudimentary understanding of the biology of lym-phocytes, as it is these cells that govern the adaptiveimmune responses that we need to generate withvaccines.
AAEP PROCEEDINGS / Vol. 46 / 2000 1
IN DEPTH: VACCINATION
NOTES
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000

The Lymphocyte FamilyLymphocytes can be divided into different popula-tions with different specialized but coordinatedfunctions, and this family tree is illustrated in Fig-ure 1. The major division within the lymphocytefamily is into T cells and B cells. The critical fea-ture separating these cell populations is that T cellshave on their surface an antigen receptor called theT-cell receptor (TCR) combined with a signalingmolecule called CD3, while B cells express immuno-globulin molecules on their surface and use thesedirectly as antigen receptors. There are two typesof TCR, the ab and the gd TCR, but for our discus-sion of vaccine immunology we are only concernedwith the ab-TCR–expressing T cells. There aremany other critical cell surface molecules, but un-derstanding these is not essential to our discussionof vaccine immunology. Let’s examine the T celland B cell families separately.
T cell FunctionBeyond this initial distinction of T and B lympho-cytes, the T cell family is divided into T-helper cellsthat express the CD4 surface molecule and cytotoxicT lymphocytes (CTLs) that express the CD8 mole-cule. The exact reason why CTLs and T-helpercells express these molecules will become clear later,but let’s consider first the basic features of whatthese cells do and why they are important. Therole of CTLs is the easiest to explain. As theirname suggests, CTLs kill other cells within thebody, and in the case of infectious disease they dothis when cells are infected with a virus or an intra-cellular bacteria (Fig. 2). This specialization is ab-solutely critical to fighting these types of infectionsand CTLs are an essential component of immunedefenses.
Table 1. Effector molecules and cells of the adaptive immune system, accessory factors, and examples of susceptible infectious agents. (From:Lunn DP, McCLure JT. Immunological principles of equine vaccination. In: Colahan PT, Merritt AM, Moore J, Mayhew IG, eds. Equine
Medicine and Surgery 5 ed, St. Louis, MO: Mosby Inc., 1999;183–190)
Effector Accessory Factors Infectious Agents
IgG Complement, neutrophils Bacteria (Streptococcus sp.Clostridial exotoxins), viralneutralization
IgA Alternative complementpathway
Respiratory, enteric and genitalinfections, viral attachment
IgE MAST cells Intestinal parasitesIgM Complement, macrophages Encapsulated bacteriaCTL (CD81) lymphocytes Perforin, lymphotoxin Viruses and intracellular bacteriaTH1 (CD41) lymphocytes Macrophages, B lymphocytes
(IgG sub-isotypes)Intracellular bacteria, viruses, fungi
TH2 (CD41) lymphocytes B lymphocytes (IgA, IgE),MAST cells, Eosinophils
Viruses, parasites
Fig. 1. Major divisions of the lymphocyte family. To the left ofthe diagram different populations of lymphocytes are distin-guished by expression of different cell surface molecules. To theright of the diagram the distinctions are functional.
Fig. 2. Cytotoxic lymphocyte (CTL) killing. This sequenceshows lysis of a virus infected target cell by a CTL. The targetexpresses antigens derived from the virus on its cell surfacebound to MHC I molecules, which are recognized by the CTL,resulting in binding and release of effector proteins that triggercell death. The CTL survives the process and can go on toanother target.
2 2000 / Vol. 46 / AAEP PROCEEDINGS
IN DEPTH: VACCINATION
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000

If the CD81 CTLs are responsible for destroyinginfected target cells, what is the role of the othermajor T lymphocyte subset, the CD41 T-helper lym-phocytes? These lymphocytes, as their name im-plies, “help” other effector cells to fight offpathogens. It is currently believed that two differ-ent subsets of T-helper cells, characterized by theircytokine production profile, may be responsible fordetermining the nature of the immune response toinfectious agents.1 The subsets are the T-helper 1subset (TH1) which stimulates cytotoxic and inflam-matory functions, and the T-helper 2 subset (TH2)which stimulates strong antibody and allergic re-sponses (Fig. 3). These two types of T-helper sub-sets and the cytokines they produce tend to suppresseach other. As a result, in an immune response toa particular pathogen, either the TH1 or the TH2 willpredominate and give rise to either an inflamma-tory/cytotoxic or a humoral immune response.
Therefore, if an appropriate immune response to apathogen is to be produced, vaccination must inducethe appropriate T-helper response. An example ofsuch a circumstance may be Rhodococcus equi infec-tion in foals. Like other intracellular pathogens,such as Salmonella sp, this organism survives byparasitizing macrophages.2 In order to overcomesuch infections, the macrophage requires help frominflammatory TH1 cells that can activate the macro-phage by secretion of cytokines such as IFN-g andGM-CSF. In contrast, a TH2 response may be inef-fective in combating these intracellular organisms,and may actually be counterproductive by suppressingTH1 activity. This may explain the lack of efficacy ofkilled vaccines against intracellular pathogens.
Several factors have been identified which mayinfluence whether a TH1 or TH2 type response willpredominate and these include the type of antigenpresenting cell, dose of antigen, the type of adjuvant,immunization route, and the cytokines present dur-ing antigen presentation. The type of T-helper cell
induced by vaccination will determine whether thevaccine is either helpful or possibly even detrimen-tal, in protecting against disease. Therefore a keyissue in vaccine development is the ability of differ-ent vaccination strategies to stimulate specific T-helper subsets.3
B cell FunctionThe role of the B cell family is the production of acomplex array of antibodies. In the horse all themajor antibody classes have been identified: IgM,IgG, IgA, and IgE. Importantly, the IgG class canbe divided into a number of subclasses, the bestcharacterized and most important of which areIgGa, IgGb, and IgG(T). Each of these classes andsubclasses are specialized for a specific role as indi-cated in Table 1, and discussed in detail below in thecontext of IgA and mucosal immunity. The struc-ture of an antibody molecule is shown for IgA inFigure 4, an antibody which is specialized for activ-ity at mucosal surfaces. The other major immuno-globulins involved in fighting microbial disease areIgM, which is responsible for a rapid initial responseto either infection or vaccination, and IgG, whichincreases after IgM but is produced in largeramounts and with a higher affinity for its antigen.In addition, IgG responses can be very long-lastingand it is IgG that is responsible for recall responseson re-exposure to a pathogen or booster vaccination.
The maturation of B cells, illustrated in Figure 5,provides an example of the process of lymphocyte
Fig. 4. The IgA molecule. This schematic illustrates the majorfeatures of immunoglobulin molecules. While the illustratedIgA molecule is dimeric, with the two Ig units joined by the green“J-chain” and a series of red disulphide bonds, IgG molecules aremonomeric. Each Ig unit consists of two heavy chains and twolight chains. The heavy chains have four subunits and the lightchains two. One end of the Ig unit has a highly variable proteinstructure and is involved in antigen recognition, while the re-mainder of the Ig unit has a constant structure in each Ig classand subclass and determines the functional characteristics of themolecule, such as binding complement, or recognition by macro-phages or neutrophil FC receptors. This specialized dimeric IgAmolecule also has a blue secretory piece that increases its stabil-ity in the harsh mucosal environment.
Fig. 3. T-helper lymphocyte subsets. The TH1 and TH2 lym-phocyte subsets provide help for macrophage activation and hu-moral immunity, respectively. This is mediated by production ofcytokines which have a regulatory effect on each other.
AAEP PROCEEDINGS / Vol. 46 / 2000 3
IN DEPTH: VACCINATION
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000

development. There are two key processes that oc-cur here. The first is a rearrangement of the germline DNA of the B cell in order to determine theexact structure of the immunoglobulin molecule an-tigen binding site it will later express on its surfaceor secrete. This process is mirrored in T cells whenthey determine the antigen binding specificity of theTCR they will subsequently express. This is a crit-ical step in all lymphocyte development as it is re-sponsible for the ability of the immune system torecognize a vast array of foreign antigens. Inter-estingly, a failure in this process, due to mutation inan enzyme gene, is responsible for the failure of Band T cell development that we see in Arabiansevere combined immunodeficiency foals (SCID).A second key step in B cell development is the pro-cess of deciding what type of immunoglobulin classto produce. All B cells start out making IgM andIgD, but later make a final commitment to one spe-cific class or subclass of immunoglobulin. This de-cision depends on a number of factors, but cytokinesreleased by TH1 or TH2 cells play a critical role inthis decision.
Protective and Non-protective Immunity to InfluenzaVirus
At this stage we have explained the major compo-nents of the adaptive immune response and it is agood time to put these in some context. The exam-ple we will use is the immune response to equineinfluenza virus, after either infection or vaccination.
We will focus on the antibody response to this patho-gen, as this is probably a critical component of pro-tective immunity to influenza. Until recently onlykilled vaccines were commercially available forequine influenza, but in young horses in particularthey gave short-lasting protection at best.5 In con-trast, equine influenza virus infection leaves horsesprotected for at least 6–12 months.6 To work outwhy vaccinal immunity compared so poorly withinfection-acquired immunity, Dr. Kay Nelson per-formed an experiment to study local and circulatingantibody responses and protection resulting from aconventional commercial vaccination or natural in-fluenza virus infection.7 It was found that 3months after administration of two doses of a con-ventional vaccine, ponies were left unprotectedwhen subjected to a challenge infection. In con-trast, 3 months after being given an initial influenzavirus infection, ponies were completely immune to arepeat challenge infection. The key local and se-rum antibody responses to infection or vaccinationare shown in Figure 6. A critical difference be-tween infection and vaccination was that infectioninduced high levels of IgA in nasal mucosal secre-tions whereas vaccination induced no IgA antibod-ies. In addition there were marked differences inthe isotypes of IgG induced by infection compared tovaccination, with natural infection inducing IgGaand IgGb responses and conventional vaccines in-ducing IgG(T) responses. It is interesting to notethat in the horse the IgGa and IgGb sub-isotypes arecapable of mediating important anti-viral activitiessuch as complement fixation and antibody-depen-dent cellular cytotoxicity, while IgG(T) responsescan actually inhibit complement fixation and arebetter adapted to neutralizing toxins such as thoseproduced by the Clostridia sp.8,9
Fig. 6. Immune response to influenza virus. Equine immuno-globulin responses in two groups of four influenza naı̈ve ponies toeither influenza virus infection or conventional inactivated vac-cine administration. The graphs show the mean nasal mucosalIgA response to a viral infection (administered on Day 0), or theIgG subclass responses to infection or a series of two vaccinations(second dose on Day 0).
Fig. 5. Maturation of B lymphocytes. Different stages of Blymphocyte development can be recognized by expression of im-munoglobulin molecules. This maturation requires a series ofgene rearrangements in order to select the genes which willencode the antigen binding part of the immunoglobulin molecule(variable region), and subsequently to select the genes that de-termine the class or subclass of the antibody molecule. Initially,immature B cells express IgM (the majority of peripheral blood Bcells), but after antigen exposure the B cell becomes activated andmay express any of the immunoglobulin classes or subclasses.This decision depends in large part on cytokine signals fromT-helper cells. Finally, activated B cells either mature intoshort-lived antibody secreting plasma cells, or become long-livedmemory B cells.
4 2000 / Vol. 46 / AAEP PROCEEDINGS
IN DEPTH: VACCINATION
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000
Not all killed equine influenza vaccines perform aspoorly as did the one used in this study, but thisexample highlights that vaccines must induce theright kind of immune responses, and in the rightplaces. Now that we understand the components ofthe immune response, there is one more basic im-munological concept that must be grasped, and thatis how the immune system sees an invading patho-gen. This process is called antigen presentation.
Antigen Presentation
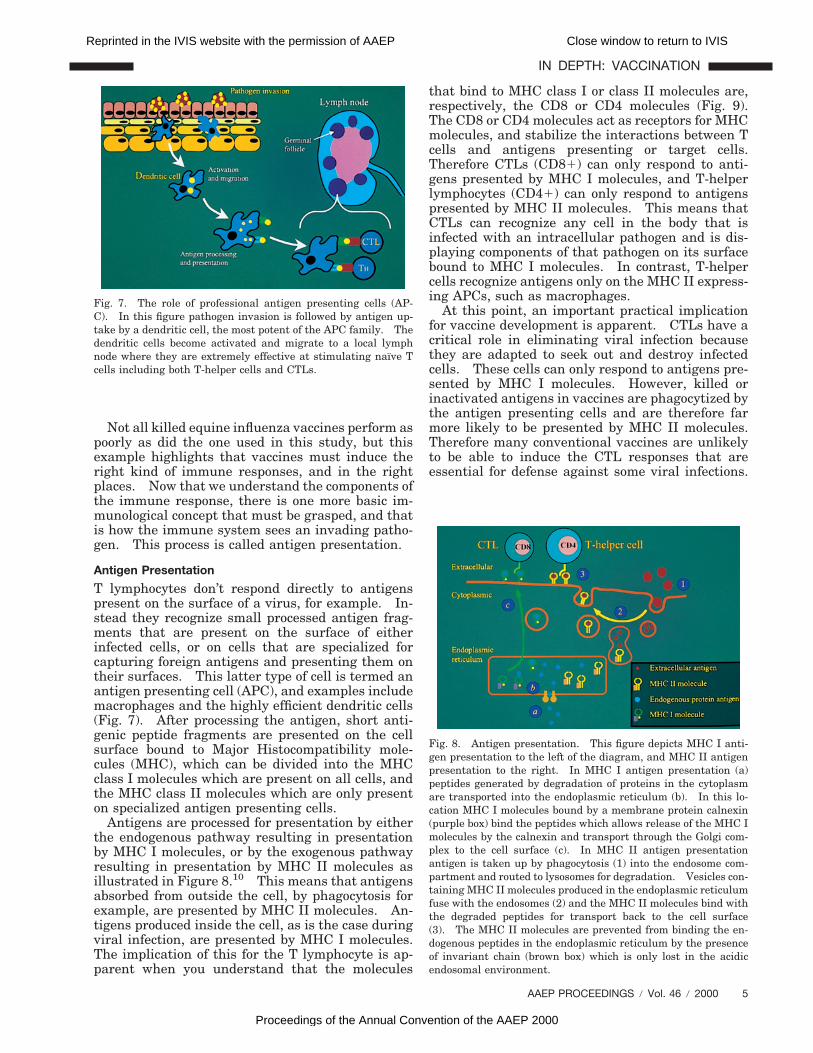
T lymphocytes don’t respond directly to antigenspresent on the surface of a virus, for example. In-stead they recognize small processed antigen frag-ments that are present on the surface of eitherinfected cells, or on cells that are specialized forcapturing foreign antigens and presenting them ontheir surfaces. This latter type of cell is termed anantigen presenting cell (APC), and examples includemacrophages and the highly efficient dendritic cells(Fig. 7). After processing the antigen, short anti-genic peptide fragments are presented on the cellsurface bound to Major Histocompatibility mole-cules (MHC), which can be divided into the MHCclass I molecules which are present on all cells, andthe MHC class II molecules which are only presenton specialized antigen presenting cells.
Antigens are processed for presentation by eitherthe endogenous pathway resulting in presentationby MHC I molecules, or by the exogenous pathwayresulting in presentation by MHC II molecules asillustrated in Figure 8.10 This means that antigensabsorbed from outside the cell, by phagocytosis forexample, are presented by MHC II molecules. An-tigens produced inside the cell, as is the case duringviral infection, are presented by MHC I molecules.The implication of this for the T lymphocyte is ap-parent when you understand that the molecules
that bind to MHC class I or class II molecules are,respectively, the CD8 or CD4 molecules (Fig. 9).The CD8 or CD4 molecules act as receptors for MHCmolecules, and stabilize the interactions between Tcells and antigens presenting or target cells.Therefore CTLs (CD81) can only respond to anti-gens presented by MHC I molecules, and T-helperlymphocytes (CD41) can only respond to antigenspresented by MHC II molecules. This means thatCTLs can recognize any cell in the body that isinfected with an intracellular pathogen and is dis-playing components of that pathogen on its surfacebound to MHC I molecules. In contrast, T-helpercells recognize antigens only on the MHC II express-ing APCs, such as macrophages.
At this point, an important practical implicationfor vaccine development is apparent. CTLs have acritical role in eliminating viral infection becausethey are adapted to seek out and destroy infectedcells. These cells can only respond to antigens pre-sented by MHC I molecules. However, killed orinactivated antigens in vaccines are phagocytized bythe antigen presenting cells and are therefore farmore likely to be presented by MHC II molecules.Therefore many conventional vaccines are unlikelyto be able to induce the CTL responses that areessential for defense against some viral infections.
Fig. 8. Antigen presentation. This figure depicts MHC I anti-gen presentation to the left of the diagram, and MHC II antigenpresentation to the right. In MHC I antigen presentation (a)peptides generated by degradation of proteins in the cytoplasmare transported into the endoplasmic reticulum (b). In this lo-cation MHC I molecules bound by a membrane protein calnexin(purple box) bind the peptides which allows release of the MHC Imolecules by the calnexin and transport through the Golgi com-plex to the cell surface (c). In MHC II antigen presentationantigen is taken up by phagocytosis (1) into the endosome com-partment and routed to lysosomes for degradation. Vesicles con-taining MHC II molecules produced in the endoplasmic reticulumfuse with the endosomes (2) and the MHC II molecules bind withthe degraded peptides for transport back to the cell surface(3). The MHC II molecules are prevented from binding the en-dogenous peptides in the endoplasmic reticulum by the presenceof invariant chain (brown box) which is only lost in the acidicendosomal environment.
Fig. 7. The role of professional antigen presenting cells (AP-C). In this figure pathogen invasion is followed by antigen up-take by a dendritic cell, the most potent of the APC family. Thedendritic cells become activated and migrate to a local lymphnode where they are extremely effective at stimulating naı̈ve Tcells including both T-helper cells and CTLs.
AAEP PROCEEDINGS / Vol. 46 / 2000 5
IN DEPTH: VACCINATION
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000

In addition, in the case of T-helper cells, severalfactors involved in antigen presentation can influ-ence whether a TH1 or TH2 response is induced.It is apparent, therefore, that appropriate and effi-cient antigen presentation is an essential require-ment for any vaccine.
Mucosal Immunity
The components of the mucosal immune system areno different from the immune system in the rest ofthe body, but this “compartment” of the immunesystem is so important that it deserves special con-sideration. In the equine influenza study abovethere was a strong mucosal IgA response followinginfection, and there is excellent evidence that thistype of immunity is critical for protection from manypathogens that invade mucosal surfaces. The mu-cosal surfaces of the gastrointestinal, respiratory,and genitourinary tracts are continuously exposedto foreign antigens, including potentially infectiousbacteria and viruses. The adaptive mucosal im-mune responses that have evolved to protect thebody against these challenges have distinct and spe-cialized characteristics.11 The principal immuno-globulin produced by the mucosal immune system issecretory IgA, which is the most abundant immuno-globulin class in the body. Specialized antigen up-take cells in the Peyer’s Patches of the intestinaltract or nasopharyngeal lymphoid tissues, termedmicrofold or M cells, transport antigens to underly-ing mucosal associated lymphoid tissues or MALT(Fig. 10).12,13 In the MALT antigen processing andpresentation takes place, resulting in immunoglob-ulin class-switching and activation of antigen-spe-cific IgA-positive B cells.13 T-helper cells arecritical to this process.14 After homing of these
IgA-B cells to effector sites such as the lamina pro-pria of the gut and respiratory tract, second signalsfrom antigen presentation cells and from T-helpercells result in further differentiation into IgA pro-ducing plasma cells.
Secretory IgA protects the body from bacteria andviruses principally by immune exclusion, i.e., by phys-ically preventing attachment to mucosal surfaces.11,15
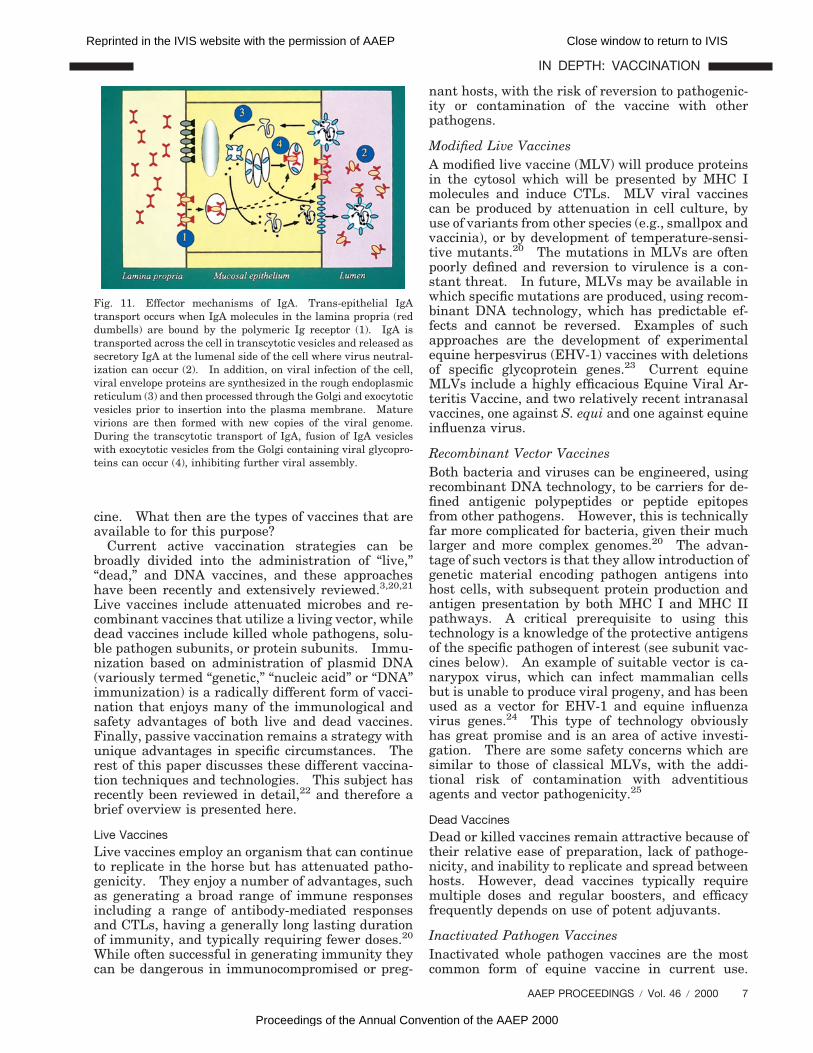
After release of secretory IgA by plasma cells intothe interstitium, it is transported across the epithe-lial cell and released at the luminal surface (Fig. 11).During its transit through the epithelial cell it iseven possible that IgA can neutralize intracellularinfections.16 Overall the mucosal immune systemcan function as an independent immunological or-gan, equipped with specialized tools to deal with theparticular antigenic challenges faced by mucosalsurfaces. For many diseases, including influenzavirus17 and Streptococcus equi18,19 infection, a mu-cosal immune response may be the most effectivetype of immune protection.
Effective Vaccination
We have reviewed many of the key functional ele-ments of the adaptive immune response, and someof the regulatory processes that control them. Inparticular, we have identified three types of T lym-phocytes that mediate immunity: the CTL whichcan destroy virus infected cells; the TH1 lymphocyteswhich can provide pro-inflammatory signals to acti-vate cell mediated immunity (e.g., macrophage acti-vation); and the TH2 lymphocyte which can driveantibody production. Appropriately stimulatingthese regulatory and effector T lymphocyte re-sponses is an essential function of an effective vac-
Fig. 9. The role of T cell CD4 and CD8 molecules. T cells usetheir T-cell receptors to recognize processed antigen presented incombination with either MHC I or MHC II molecules. T cellsexclusively express either CD4 (T-helper cells) or CD8 (CTLs),and the CD4 molecule is required for interaction with MHC IImolecules, while CD8 is required for MHC I interaction. As aresult T-helper cells recognized antigens presented by MHC IIand CTLs only recognize antigens presented by MHC I molecules.
Fig. 10. Mucosal immunity. In this simplified overview of themucosal immune system a virus (1) first encounters an M cell(purple cell) overlying an aggregate of lymphocytes in mucosalassociated lymphoid tissues (2). This results in production ofboth IgG and IgA antibody responses and circulation of primedantigen specific B lymphocytes in the blood system (3). These Blymphocytes can travel to other mucosal surfaces where on re-exposure to antigen (4) they can secrete IgA which can be trans-ported across the mucosal epithelium to neutralize virus. The IgG,in contrast, is restricted to the circulation and lamina propria.
6 2000 / Vol. 46 / AAEP PROCEEDINGS
IN DEPTH: VACCINATION
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000
cine. What then are the types of vaccines that areavailable to for this purpose?
Current active vaccination strategies can bebroadly divided into the administration of “live,”“dead,” and DNA vaccines, and these approacheshave been recently and extensively reviewed.3,20,21
Live vaccines include attenuated microbes and re-combinant vaccines that utilize a living vector, whiledead vaccines include killed whole pathogens, solu-ble pathogen subunits, or protein subunits. Immu-nization based on administration of plasmid DNA(variously termed “genetic,” “nucleic acid” or “DNA”immunization) is a radically different form of vacci-nation that enjoys many of the immunological andsafety advantages of both live and dead vaccines.Finally, passive vaccination remains a strategy withunique advantages in specific circumstances. Therest of this paper discusses these different vaccina-tion techniques and technologies. This subject hasrecently been reviewed in detail,22 and therefore abrief overview is presented here.
Live VaccinesLive vaccines employ an organism that can continueto replicate in the horse but has attenuated patho-genicity. They enjoy a number of advantages, suchas generating a broad range of immune responsesincluding a range of antibody-mediated responsesand CTLs, having a generally long lasting durationof immunity, and typically requiring fewer doses.20
While often successful in generating immunity theycan be dangerous in immunocompromised or preg-
nant hosts, with the risk of reversion to pathogenic-ity or contamination of the vaccine with otherpathogens.
Modified Live VaccinesA modified live vaccine (MLV) will produce proteinsin the cytosol which will be presented by MHC Imolecules and induce CTLs. MLV viral vaccinescan be produced by attenuation in cell culture, byuse of variants from other species (e.g., smallpox andvaccinia), or by development of temperature-sensi-tive mutants.20 The mutations in MLVs are oftenpoorly defined and reversion to virulence is a con-stant threat. In future, MLVs may be available inwhich specific mutations are produced, using recom-binant DNA technology, which has predictable ef-fects and cannot be reversed. Examples of suchapproaches are the development of experimentalequine herpesvirus (EHV-1) vaccines with deletionsof specific glycoprotein genes.23 Current equineMLVs include a highly efficacious Equine Viral Ar-teritis Vaccine, and two relatively recent intranasalvaccines, one against S. equi and one against equineinfluenza virus.
Recombinant Vector VaccinesBoth bacteria and viruses can be engineered, usingrecombinant DNA technology, to be carriers for de-fined antigenic polypeptides or peptide epitopesfrom other pathogens. However, this is technicallyfar more complicated for bacteria, given their muchlarger and more complex genomes.20 The advan-tage of such vectors is that they allow introduction ofgenetic material encoding pathogen antigens intohost cells, with subsequent protein production andantigen presentation by both MHC I and MHC IIpathways. A critical prerequisite to using thistechnology is a knowledge of the protective antigensof the specific pathogen of interest (see subunit vac-cines below). An example of suitable vector is ca-narypox virus, which can infect mammalian cellsbut is unable to produce viral progeny, and has beenused as a vector for EHV-1 and equine influenzavirus genes.24 This type of technology obviouslyhas great promise and is an area of active investi-gation. There are some safety concerns which aresimilar to those of classical MLVs, with the addi-tional risk of contamination with adventitiousagents and vector pathogenicity.25
Dead VaccinesDead or killed vaccines remain attractive because oftheir relative ease of preparation, lack of pathoge-nicity, and inability to replicate and spread betweenhosts. However, dead vaccines typically requiremultiple doses and regular boosters, and efficacyfrequently depends on use of potent adjuvants.
Inactivated Pathogen VaccinesInactivated whole pathogen vaccines are the mostcommon form of equine vaccine in current use.
Fig. 11. Effector mechanisms of IgA. Trans-epithelial IgAtransport occurs when IgA molecules in the lamina propria (reddumbells) are bound by the polymeric Ig receptor (1). IgA istransported across the cell in transcytotic vesicles and released assecretory IgA at the lumenal side of the cell where virus neutral-ization can occur (2). In addition, on viral infection of the cell,viral envelope proteins are synthesized in the rough endoplasmicreticulum (3) and then processed through the Golgi and exocytoticvesicles prior to insertion into the plasma membrane. Maturevirions are then formed with new copies of the viral genome.During the transcytotic transport of IgA, fusion of IgA vesicleswith exocytotic vesicles from the Golgi containing viral glycopro-teins can occur (4), inhibiting further viral assembly.
AAEP PROCEEDINGS / Vol. 46 / 2000 7
IN DEPTH: VACCINATION
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000

Inactivation is achieved with agents such as thi-mersol or phenol in the case of bacteria, and formalinor beta-proprionolactone for viruses. Historicallysuch vaccines have frequently proven highly immu-nogenic, although their limitations in protectinghorses from respiratory pathogens represent an on-going and serious problem.5,7,26 Quality control inthe production of such vaccines can overcome someof these limitations,27 but development and use ofeffective adjuvants represents the most importanttool for overcoming their limitations (see below).28,29
Protein VaccinesProtein vaccines include naturally produced compo-nents of pathogens, such as the M-protein vaccinefor S. equi which is non-pathogenic and may pro-mote fewer injection site reactions than whole bac-terial products. The most commonly used proteinvaccine in horses is tetanus toxoid, which is pre-pared by formalin inactivation of tetanus toxin andincorporation with an alum adjuvant.
Recombinant Subunit VaccinesThe explosion of knowledge in the field of recombi-nant DNA technology has led to the identification,and in some instances, synthetic production of manyof the specific antigens that are important for im-munity to pathogens. Such vaccines can includerecombinant polypeptides, or peptide-based vac-cines containing a single antigenic epitope. Unfor-tunately these purified proteins may be poorlyimmunogenic by themselves, and particularly so inthe case of peptide vaccines, and cannot overcomethe barriers that prevent MHC I presentation with-out the use of appropriate adjuvants.
AdjuvantsComprehensive explanations of the many types ofadjuvants is beyond the scope of this paper; how-ever, several excellent reviews have been pub-lished,3,4,30,31 including one review of vaccineadjuvants in use in veterinary products.32 The suc-cess of killed vaccines frequently depends on theadjuvant system used, as adjuvants can determinethe form of immune response that will be stimulatedthrough stimulating either the TH1 or TH2 regula-tory lymphocyte subsets. Current adjuvants, suchas alum, tend to stimulate TH2 responses whileFreund’s Complete Adjuvant (FCA) is an example ofan adjuvant that stimulates TH1 responses. How-ever, although FCA can induce TH1 responses, itcannot be used in commercial vaccines due to its sideeffects. Another critical function of adjuvants is togain access to the cellular compartments that allowfor MHC I presentation and CTL induction. One ofthe most promising adjuvants for this purpose is theImmune Stimulating Complex (ISCOM). ISCOMadjuvants have been associated with greatly in-creased antigen-specific antibody responses, and awide range of T cell responses including the induc-tion of cytotoxic T-lymphocytes.33 There is already
evidence of the efficacy of influenza virus ISCOMvaccines in horses.28,34,35 An important componentof ISCOMs is Quil A, a component of a plant sapo-nin. Quil A is also found in several current equinevaccines, often in combination with alum, and whilenot as potent as an ISCOM, its inclusion does aug-ment adjuvanticity.
One particular type of adjuvant deserving specialmention are the mucosal adjuvants. Mucosal im-munity has a critical role in resistance to wide vari-ety of pathogens such as equine influenza virus7 andS. equi.36 Generating mucosal IgA responses withkilled vaccines is challenging, and the only effectivemucosal adjuvants are the bacterial exdotoxins ofenteric bacterial pathogens such as cholera toxin(CT) or the labile toxin of E. coli.37 This adjuvanteffect may depend on several known actions of CT,including enhancement of antigen presentation, pro-motion of B lymphocyte isotype differentiation, stim-ulation of CD41 T-helper lymphocytes, andinduction of local and systemic memory responses.A disadvantage of using CT is that it can producecholera diarrhea in humans,11 although it is welltolerated in other species. Recently, encouragingresults have been reported in horses vaccinated in-tranasally with inactivated equine influenza viruscombined with cholera toxin B subunit.38
DNA Vaccines
DNA vaccination results in the in vivo synthesis ofantigenic proteins in a manner identical to that oc-curring in natural infection.25 This endogenousproduction results in presentation of antigens byMHC I and presentation to CD81 T cytotoxic lym-phocytes, and uptake and presentation of solubleproteins by MHC II to CD41 T-helper lymphocytes.As a result DNA vaccination has been shown toinduce both potent CTL and antibody responses.Investigations of the use of DNA vaccines in horsesare at an early stage, but it has already been dem-onstrated that they are effective at protecting horsesfrom influenza virus infection and induce appropri-ate antibody isotype responses,39,40 and there is pro-visional evidence of their potential for EHV-1vaccination.41,42
Passive Vaccination
Passive vaccination is accomplished by administer-ing preformed antibodies either as a plasma trans-fusion or in a concentrated form, as in commerciallyavailable tetanus antitoxin. This strategy can behighly effective in diseases for which there is noavailable form of active vaccination (e.g., R. equi) orin high-risk situations when there is inadequatetime for protection to be generated by active vacci-nation. Generally passive vaccination should beavoided when possible due to the risk of transmis-sion of infection in serum-derived products. Aprime example of this is the association with acutehepatic necrosis with a previous administration oftetanus antitoxin.43
8 2000 / Vol. 46 / AAEP PROCEEDINGS
IN DEPTH: VACCINATION
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000
Summary
Understanding the basics of T cell and immunoglob-ulin function, antigen presentation, and mucosal im-munity makes the immunological reasons behindvaccine success or failure far easier to grasp andbetter equips us to evaluate new and old products.As new and innovative vaccines reach the market-place, this knowledge will have increasing value forequine veterinarians as we try to distinguish factfrom fiction.
References1. Mosmann TR, Sad S. The expanding universe of T-cell
subsets: Th1, Th2 and more. Immunol Today 1996;17:138 –146.
2. Prescott JF. Rhodococcus equi: an animal and human patho-gen. Clin Microbiol Rev 1991;4:20–34.
3. Rabinovich NR, McInnes P, Klein DL, et al. Vaccine tech-nologies: view to the future. Science 1994;265:1401–1404.
4. Audibert FM, Lise LD. Adjuvants: current status, clinicalperspectives and future prospects. Trends Pharmacol Sci1993;14:174–178.
5. Mumford JA. Progress in the control of equine influenza.In: Proceedings. Equine Infect Dis VI 1992;207–217.
6. Hannant D, Mumford JA, Jessett DM. Duration of circulat-ing antibody and immunity following infection with equineinfluenza virus. Vet Rec 1988;122:125–128.
7. Nelson KM, Schram BR, McGregor MW, et al. Local andsystemic isotype-specific antibody responses to equine influ-enza virus infection versus conventional vaccination. Vac-cine 1998;16:1306–1313.
8. Montgomery PC. Molecular aspects of equine antibodies.In: Proceedings. Equine Infect Dis III 1973;341–363.
9. McGuire TC, Crawford TB, Henson JB. The isolation, char-acterisation and functional properties of equine immunoglob-ulin classes and subclasses. In: Proceedings. EquineInfect Dis III 1973;364–381.
10. Braciale TJ, Braciale VL. Antigen presentation: structur-al themes and functional variations. Immunol Today 1991;12:124–129.
11. Holmgren J, Czerkinsky C, Lycke N, et al. Strategies for theinduction of immune responses as mucosal surfaces makinguse of cholera toxin B subunit as immunogen, carrier, andadjuvant. Am J Trop Med Hyg 1994;50:42–54.
12. Ramsay AJ, Kohonen-Corish M. Interleukin-5 expressed bya recombinant virus vector enhances specific mucosal IgAresponsess in vivo. Eur J Immunol 1993;23:3141–3145.
13. McGhee JR, Kiyono H. Mucosal immunity to vaccines:current concepts for vaccine development and immune re-sponse analysis. Adv Exp Med Biol 1992;327:3–12.
14. McIntyre TM, Kehry MR, Snapper CM. Novel in vitromodel for high-rate IgA class switching. J Immunol 1995;154:3156–3161.
15. Wolff JA, Ludtke JJ, Acsadi G, et al. Long-term persistenceof plasmid DNA and foreign gene expression in mouse mus-cle. Hum Mol Genet 1992;1:363–369.
16. Mazanec MB, Nedrud JG, Kaetzel CS, et al. A three-tieredview of the role of IgA in mucosal defense. Immunol Today1993;14:430–435.
17. Renegar KB, Small PAJ. Passive transfer of local immunityto influenza virus infection by IgA antibody. J Immunol1991;146:1972–1978.
18. Galan JE, Timoney JF, Lengemann FW. Passive transfer ofmucosal antibody to Streptococcus equi in the foal. InfectImmun 1986;54:202–206.
19. Wallace FJ, Emery JD, Cripps AW, et al. An assessment ofmucosal immunisation in protection against Streptococcusequi (Strangles) infections in horses. Vet Immunol Immu-nopathol 1995;48:139–154.
20. Ellis RW. New technologies for making vaccines. In:Plotkin SA, Orenstein WA, eds. Vaccines. 3rd ed. Phila-delphia: W.B. Saunders Company, 1999;881–901.
21. Ertl HCJ, Xiang Z. Novel vaccine approaches. J Immunol1996;156:3579–3582.
22. Lunn DP, Townsend HGG. Equine vaccination. Veteri-nary Clinics of North America. Equine Pract 2000;16:199–226.
23. Matsumura T, Kondo T, Sugita S, et al. An equine herpesvirustype 1 recombinant with a deletion in the gE and gI genes isavirulent in young horses. Virology 1998;242:68–79.
24. Audonnet JC, Mumford JA, Jessett D, et al. Safety andefficacy of a canarypox-EHV recombinant vaccine in horses.In: Proceedings. Equine Infect Dis VIII 1999;418–419.
25. Hassett DE, Whitton JL. DNA immunization. Trends Mi-crobiol 1996;8:307–312.
26. Townsend HGG, Morley PS, Newton JR. Measuring serumantibody as a method of predicting infection and disease inhorses during outbreaks of influenza. In: Equine Infec-tious Diseases VIII Wernery U, Wade JA, Mumford JA,Kaaden O-R, eds. R&W Publications, Newmarket, 1999;33–37.
27. Mumford JA. The equine influenza surveillance program.Adv Vet Med Veterinary Vaccines and Diagnostics 1999;41:379–387.
28. Mumford JA, Jessett D, Dunleavy U, et al. Antigenicity andimmunogenicity of experimental equine influenza ISCOMvaccines. Vaccine 1994;12:857–863.
29. Mumford JA, Wilson H, Hannant D, et al. Antigenicity andimmunogenicity of equine influenza vaccines containing aCarbomer adjuvant. Epidemiol Infec 1994;112:421–437.
30. Gupta RK, Relyveld EH, Lindblad EB, et al. Adjuvants—abalance between toxicity and adjuvanticity. Vaccine 1993;11:293–306.
31. Allison AC, Byars NE. Immunological adjuvants and theirmode of action. Biotechnol 1992;20:431–449.
32. Macy DW. Vaccine adjuvants. Semin Vet Med Surg(Small Anim) 1997;12:206–211.
33. Morein B, Villacres-Eriksson M, Ekstrom J, et al. ISCOM:a delivery system for neonates and for mucosal administra-tion. Adv Vet Med Veterinary Vaccines and Diagnostics1999;41:405–413.
34. Mumford JA, Jessett DM, Rollinson EA, et al. Duration ofprotective efficacy of equine influenza immunostimulatingcomplex/tetanus vaccines. Vet Rec 1994;134:158–162.
35. Sundquist B, Lovgren K, Morein B. Influenza virus ISCOMs:antibody response in animals. Vaccine 1988;6:49–53.
36. Sheoran AS, Sponseller BT, Holmes MA, et al. Serum andmucosal antibody isotype responses to M-like protein (SeM)of Streptococcus equi in convalescent and vaccinated horses.Vet Immunol Immunopathol 1997;59:239–251.
37. Foss DL, Murtaugh MP. Role of macrophage cytokines inmucosal adjuvanticity. Adv Vet Med Veterinary Vaccinesand Diagnostics 1999;41:83–104.
38. Hannant D, Easeman R, Mumford JA. Equine mucosal im-mune system: intranasal vaccination with inactivatedequine influenza virus protects from infection. In: Proc-eedings. Equine Infect Dis VIII 1999;50–56.
39. Lunn DP, Olsen CW, Soboll G, McGregor MW, Macklin MD,McCabe DE, Swain WF. Development of practical DNA vac-cination strategies for use in horses. In: Equine InfectiousDiseases VIII. Wernery U, Wade JA, Mumford JA, KaadenO-R, eds. R&W Publications, Newmarket. 1999;38–43.
40. Lunn DP, Soboll G, Schram BR, et al. Antibody responses toDNA vaccination of horses using the influenza virus hemag-glutinin gene. Vaccine 1999;17:2245–2258.
41. Walker C, Ruitenberg K, Wellington J, et al. Genetic immuni-zation with equine herpesvirus-1 glycoprotein D. In: Proc-eedings. First Internat Vet Vaccines Diag Conf 1997;93.
42. Ruitenberg K, Walker C, Wellington J, et al. Vaccine poten-tial of DNA immunisation against equine herpesvirus-1. In:Proceedings. Equine Infect Dis VIII 1999;420–421.
43. Savage CJ. Diseases of the liver. In: Moore J, ed.Equine Medicine and Surgery. 5th ed. St. Louis, MO:Mosby Inc 1999;816–833.
AAEP PROCEEDINGS / Vol. 46 / 2000 9
IN DEPTH: VACCINATION
Reprinted in the IVIS website with the permission of AAEP Close window to return to IVIS
Proceedings of the Annual Convention of the AAEP 2000
Related Documents











