Elsevier ELSEVIER 0264-410X(95)00132-8 Vaccine, Vol. 14, No. 3, pp. 237-243, 1996 Copyright 0 1996 Elsevier Science Ltd. All rights reserved Printed in Great Britain 0264-41 OX/96 515+0.00 Immunogenicity, safety and protective efficacy of one dose of the rhesus rotavirus vaccine and serotype 1 and 2 human-rhesus rotavirus reassortants in children from Lima, Peru Claudio F. Lanata*§, Robert E. Black*?, Jorge Florest, Francisco Laze*, Betzabe Butron”, Albert0 Linares*, Ana Huapaya*, Gladis Ventura*, Ana Gil* and Albert Z. Kapikianl In a four cell trial, a single IO4 plaque-forming unit dose of rhesus rotavirus (RRV) vaccine (serotype G3), a human rotavirus-rhesus rotavirus reassortant vaccine with serotype Gl spectficity, a similar vaccine with serotype G2 spectjicity, or a placebo was administered with bufier orally at 2 months of age to 800 Peruvian infants. Only the RRV vaccine was associated with a febrile response (~38°C) that occurred in 9% of the infants on day 4 after vaccination. Diarrhea or other side-efSects were not associated with administration of vaccine. Vaccine strains were shed by only 12-18% of the infants as determined by examination of a single stool specimen obtained on days 4 or 5 after vaccination. Ftfty per cent of vaccinees developed an IgA ELISA seroresponse; however, a serotype-spectfic seroresponse by plaque reduction neutralization was demonstrated in ~20% of the participants against each of the three candidate vaccine strains. Vaccine eficacy was evaluated by twice-weekly home surveillance for diarrhea1 diseases during 24 months post-immunization. Rotavirus diarrhea1 episodes were identified by ELISA. Only the RRV vaccine had a signtficant protective ejicacy (2976, ~~0.03, chi-square test) against rotavirus diarrhea. Analysis of vaccine eficacy against rotavirus episodes of any severity in which no other enteropathogen was isolated showed a trend towards higher vaccine eficacy. In addition, a similar trend was observed in rotavirus-only episodes in which there was some degree of dehydration or when health services were utilized. Serotype Gl or G2 rotavirus strains were most prevalent during surveillance. Neither serotype Gl or serotype G2 vaccines were protective against serotype I or 2 rotavirus diarrhea, respectively. The serotype G2 vaccine was 84sprotective against serotype 1 and 2 dehydrating rotavirus diarrhea in the small numbers of individuals evaluated. We conclude that one dose of IO4 p.fu. of the RRV, serotype GI, or serotype G2 rotavirus vaccine failed to induce either an adequate serotype-specific seroresponse or serotype- spectjic protection in children immunized at 2 months of age. Only the RRV vaccine induced a low level of protection against rotavirus diarrhea mainly of serotype Gl spect$city. Future studies need to explore whether higher vaccine dose andlor more than one dose would increase the immunogenicity and efficacy of the rotavirus vaccine, especially in developing countries with a high level of baseline rotavirus antibodies. Keywords: Rotavirus vaccines; rhesus rotavirus; reassortants; diarrhea; vaccine; efficacy; Peru *Institute de Investigation Nutritional, Lima, Peru. tDepat-t- ment of International Health, School of Hygiene and Public Health, The Johns Hopkins University, Baltimore, MD, USA. SLaboratory of Infectious Diseases, National Institute of btllergy and Infectious Diseases, National Institutes of iealth, Bethesda, MD, USA. $To whom correspondence should be addressed al: lnstituto de Investigaci6n Nutri- :ionai, A.P.18-0191, Lima-18, Peru. (Received 24 October 994; revised 5 June 1995; accepted 28 June 1995) Severe diarrhea due to rotavirus constitutes one of the most important public health problems of infants and young children in developing countries*. An effec- tive rotavirus vaccine might prevent up to 30% of all diarrhea deaths that occur in children 623 months of age2. The first vaccine candidate evaluated for efficacy, RIT 4237, was prepared from a serotype G6 bovine rotavirus strain. In developed countries, it was shown to Vaccine 1996 Volume 14 Number 3 237

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Elsevier
ELSEVIER 0264-410X(95)00132-8
Vaccine, Vol. 14, No. 3, pp. 237-243, 1996 Copyright 0 1996 Elsevier Science Ltd. All rights reserved
Printed in Great Britain 0264-41 OX/96 515+0.00
Immunogenicity, safety and protective efficacy of one dose of the rhesus rotavirus vaccine and serotype 1 and 2 human-rhesus rotavirus reassortants in children from Lima, Peru
Claudio F. Lanata*§, Robert E. Black*?, Jorge Florest, Francisco Laze*, Betzabe Butron”, Albert0 Linares*, Ana Huapaya*, Gladis Ventura*, Ana Gil* and Albert Z. Kapikianl
In a four cell trial, a single IO4 plaque-forming unit dose of rhesus rotavirus (RRV) vaccine (serotype G3), a human rotavirus-rhesus rotavirus reassortant vaccine with serotype Gl spectficity, a similar vaccine with serotype G2 spectjicity, or a placebo was administered with bufier orally at 2 months of age to 800 Peruvian infants. Only the RRV vaccine was associated with a febrile response (~38°C) that occurred in 9% of the infants on day 4 after vaccination. Diarrhea or other side-efSects were not associated with administration of vaccine. Vaccine strains were shed by only 12-18% of the infants as determined by examination of a single stool specimen obtained on days 4 or 5 after vaccination. Ftfty per cent of vaccinees developed an IgA ELISA seroresponse; however, a serotype-spectfic seroresponse by plaque reduction neutralization was demonstrated in ~20% of the participants against each of the three candidate vaccine strains. Vaccine eficacy was evaluated by twice-weekly home surveillance for diarrhea1 diseases during 24 months post-immunization. Rotavirus diarrhea1 episodes were identified by ELISA. Only the RRV vaccine had a signtficant protective ejicacy (2976, ~~0.03, chi-square test) against rotavirus diarrhea. Analysis of vaccine eficacy against rotavirus episodes of any severity in which no other enteropathogen was isolated showed a trend towards higher vaccine eficacy. In addition, a similar trend was observed in rotavirus-only episodes in which there was some degree of dehydration or when health services were utilized. Serotype Gl or G2 rotavirus strains were most prevalent during surveillance. Neither serotype Gl or serotype G2 vaccines were protective against serotype I or 2 rotavirus diarrhea, respectively. The serotype G2 vaccine was 84sprotective against serotype 1 and 2 dehydrating rotavirus diarrhea in the small numbers of individuals evaluated. We conclude that one dose of IO4 p.fu. of the RRV, serotype GI, or serotype G2 rotavirus vaccine failed to induce either an adequate serotype-specific seroresponse or serotype- spectjic protection in children immunized at 2 months of age. Only the RRV vaccine induced a low level of protection against rotavirus diarrhea mainly of serotype Gl spect$city. Future studies need to explore whether higher vaccine dose andlor more than one dose would increase the immunogenicity and efficacy of the rotavirus vaccine, especially in developing countries with a high level of baseline rotavirus antibodies.
Keywords: Rotavirus vaccines; rhesus rotavirus; reassortants; diarrhea; vaccine; efficacy; Peru
*Institute de Investigation Nutritional, Lima, Peru. tDepat-t- ment of International Health, School of Hygiene and Public Health, The Johns Hopkins University, Baltimore, MD, USA. SLaboratory of Infectious Diseases, National Institute of btllergy and Infectious Diseases, National Institutes of iealth, Bethesda, MD, USA. $To whom correspondence should be addressed al: lnstituto de Investigaci6n Nutri- :ionai, A.P.18-0191, Lima-18, Peru. (Received 24 October 994; revised 5 June 1995; accepted 28 June 1995)
Severe diarrhea due to rotavirus constitutes one of the most important public health problems of infants and young children in developing countries*. An effec- tive rotavirus vaccine might prevent up to 30% of all diarrhea deaths that occur in children 623 months of age2. The first vaccine candidate evaluated for efficacy, RIT 4237, was prepared from a serotype G6 bovine rotavirus strain. In developed countries, it was shown to
Vaccine 1996 Volume 14 Number 3 237

Efficacy of rotavirus vaccines in Peruvian children: C.F: Lanata et al.
be effective against rotavirus diarrhea”, mostly of sero- type Gl, but had limited efficacy in developing coun- tries4.5. A second vaccine candidate, the rhesus rotavirus (RRV) strain, prepared from the serotype G3 simian rotavirus strain MMU 18006, was effective against di- arrhea caused by the homotypic serotype in Venezuelan infant@, but in other studies, in which the prevalent strains were predominantly other than serotype G3, the vaccine efficacy was low or nil’-“. This information, together with studies of natural rotavirus infection”.12, suggested that protection against rotavirus diarrhea was G serotype-specific. In an attempt to broaden the antigenic coverage of a rotavirus vaccine, reassortant strains were created using RRV with the single gene from a human rotavirus that determined Gl, G2, G4 serotype’“.14. In this study, we evaluated the safety, immunogenicity and protective efficacy of one dose of RRV (serotype G3), serotype Gl reassortant or serotype G2 reassortant in infants vaccinated at 2 months of age in Lima, Peru.
MATERIALS AND METHODS
Study population
The study was conducted in Canto Grande, a densely populated peri-urban area of low socio-economic status in Lima, Peru, highly endemic for diarrhea1 diseases15. Rotavirus diarrhea is present throughout the year, with a higher incidence during the period from March to May. Potential participating families were recruited by identifying women in late pregnancy or shortly after they had given birth. After explaining the purpose and requirements of the study and the potential risks and benefits from participation, written informed consent was obtained from parents. Mothers and participating children were required to be free of chronic or debilitat- ing illnesses as determined by interviewing the mother and by a complete physical examination of the child by study pediatricians. Infants living in the same household with a pregnant women at the time of vaccination were not allowed to participate.
The study was approved by the Peruvian Ministry of Health, the Peruvian College of Physicians, the Clinical Research Sub-panel of the National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Health (NIH), the ethics committees of the Instituto de Investigation Nutritional, the Johns Hopkins School of Hygiene and Public Health, and the Pan American and World Health Organizations, and by community leaders of the study area.
The study was conducted between August 1987 and October 1990. Vaccination took place between October 1987 and September 1988. A total of 800 children participated in the study.
Study design
The study was a double-blind, placebo-controlled, four-cell field trial in which 2-month-old infants received orally a single dose of one of the following: (a) lo4 plaque-forming units (p.f.u.) of RRV (G3 serotype), (b) lo4 of a reassortant of Gl serotype, (c) lo4 p.f.u. of a reassortant of G2 serotype, or (d) placebo. The study was designed to detect a protective efficacy of 75% or greater against severe rotavirus diarrhea or against G
238 Vaccine 1996 Volume 14 Number 3
serotype 1, 2 or 3 rotavirus diarrhea for cases in which no other enteropathogen was isolated in the stool. Rotavirus infection rates observed in a previous study conducted in the same area4 were used for sample size calculations. A study group of 200 children per cell was considered necessary, allowing for loss of follow-up during surveillance. Routine immunizations with oral poliomyelitis and diphtheria-pertussis-tetanus vaccines were provided by the study pediatricians at 3, 4 and 5 months of age and measles immunization at 9 months of age. BCG immunization was provided by the Peruvian Ministry of Health at birth to most study children and by our study team to those who had not received it before enrollment into the study.
Participating children were allocated to one of 12 letter codes (three for each cell) by a block randomiza- tion using their sequential enrollment number. The vaccine or placebo code was kept at the National Institutes of Health and the World Health Organization and was not revealed until the study was completed. Antecubital venous blood was obtained shortly before and 4 weeks after administration of vaccine or placebo. Serum aliquots were kept frozen at - 20°C until analyzed.
Vaccines and vaccine administration
The RRV vaccine was prepared from the lot RRV-1 of the MMU-18006 strain of rhesus rotavirus (serotype G3) as previously described8.9. The serotype Gl vaccine was derived by reassortment of the Gl serotype “D” human rotavirus strain and RRV; the serotype 2 vaccine was derived by reassortment of the G2 serotype “DSl” human rotavirus strain and RRV’“. The experimental vaccine lots for the study were prepared by Flow Laboratories, Inc. (McLean, VA, USA Gl vaccines had a titre of lo6 p.f.u. ml- r’.
The RRV and and the DSl x
RRV a titre of lo4 p.f.u. ml-‘. Bulk vaccine preparations were transported on dry ice to Lima and stored at - 70°C. After thawing, mono-dose vials were prepared for each vaccine with assignment of one of the 12 letter study codes to each vial by an NIH investigator, who did not participate in the field procedures. The RRV and Gl vaccines were diluted with flavored rotavirus antibody- free milk to a titre of lo4 p.f.u. ml-‘; the G2 vaccine was not diluted. Thus, each vaccine vial had lo4 p.f.u. in 1 ml volume. The milk utilized to dilute the vaccines was used to prepare two-thirds of the placebo vials, identified with two of the three letter codes for the placebo group. The remainder of the placebo vials was prepared with minimum essential medium (MEM), the medium used for vaccine virus cultivation. The two preparations of placebo were essential because the G2 vaccine was not diluted and had a different color than the RRV and Gl vaccines after they were diluted with milk. Thus, the 12 random letter codes utilized in the study identified 8 milk-based (6 vaccine and 2 placebo) and 4 MEM-based (3 vaccine and 1 placebo) mono-dose vials. All vials were kept at - 70°C. On each vaccination day, the number of vials required in the field were transported with cold packs and thawed just prior to vaccination. The vaccine titre was examine+ I ‘er code by titration at the end of the study; the titres in the nine vaccine-containing vials ranged from 1 x lo4 to 8 x lo4 p.f.u. ml-‘, whereas each of the three controls had no detectable virus.
Infants were vaccinated if they were free from reported fever for 48 h and of diarrhea for 72 h prior to

Efficacy of rotavirus vaccines in Peruvian children: C.F: Lanata et al.
vaccination. Vaccines were given orally immediately after the administration of 30 ml of reconstituted evaporated milk free of vaccine virus-neutralizing activity (GloriaR, Arequipa, Peru), mixed with 400 mg sodium bicarbonate. Breast feeding was withheld for 1 h before and after immunization.
Surveillance
Surveillance for post-vaccination side-effects was conducted at home for a period of 6 days after immu- nization by twice-daily visits to all study children by trained field workers (7 days a week). Rectal tempera- ture was taken on each home visit and daily information was collected about the occurrence of fever, respiratory symptoms, diarrhea and other gastrointestinal signs and symptoms. A stool sample or a rectal swab was obtained at day 4 or 5 post-immunization to investigate vaccine virus excretion. Additionally, stool samples or rectal swabs were collected when acute diarrhea occurred.
Diarrhea1 surveillance throughout the trial was con- ducted by trained field ,workers who visited each child twice a week, collected information on diarrhea1 epi- sodes and collected stool specimens or rectal swabs. Diarrhea was defined as three or more liquid or semi- liquid stools passed in a 24 h period; the episode was considered terminated on the last day of diarrhea that was not followed by a day meeting the diarrhea defi- nition for 48 h16. A maximum recall period of 7 days was utilized. Field workers obtained daily clinical informa- tion during diarrhea1 episodes; WHO guidelines were followed for the classification of dehydration. Mothers were instructed in the use of oral rehydration solution provided by the study and were told to bring the children to the study field clinic or any health facility if dehydration or severe illness occurred. Specific anti- biotics were provided by the study pediatricians for dysenteric illness or cullure-proven, treatable diarrhea1 disease, particularly shigellosis, and for clinical pneumonia. Children were dropped from surveillance at 2 years 3 months of age, i.e. when they completed 24 months of follow-up after the rotavirus immunization.
Laboratory procedures
Stools or rectal swabs were placed in a calcium- containing Tris buffer, in Cary Blair transport media with and without Skirrow’s antibiotic supplement for detection of CampylobaNcter (10 mg 1-l of vancomycin, 2500 IU 1“ of polymyxin B, 5 mg 1-l of trimethoprim) and in addition, in a vial containing merthiolate, iodine and formalin (MIF) solution for parasitologic examina- tion. Specimens were transported with cold packs to the laboratory where they were processed on the same day of collection. Stool samples were tested for rotavirus daily, using the DAKOPATTSR rotavirus ELISA kit (Dako Laboratories, Copenhagen, Denmark)“. Rotavirus-positive stool specimens were serotyped directly at NIAID, NIH, by a G serotyping ELISA, using monoclonal antibodiesIs; stool samples that could not be serotyped or that yielded ambiguous results on direct examination were amplified in roller tube cultures of MA104 cells for retyping. To identify rotavirus vaccine shedding, a random sample of stool specimens obtained on days 4-5 post-immunization were tested directly or after cultivation in MA104 cell cultures, by confirmatory ELISA.
Salmonella, ShigelEa, and Campylobacter sp. were sought in all stool samples, using standard techniques”. Enterotoxigenic Escherichia coli (ETEC), entero- adherent Escherichia coli (EAEC), Vibrio sp. and Cryptosporidium sp. were tested only in rotavirus positive stool samples. ETEC were identified by colony DNA hybridization with the genetic sequence corre- sponding to the heat-stable and heat-labile entero- toxin2’, utilizing a commercial kit (DuPonT, Boston, MA, USA). EAEC were identified by the HEp-2 cell adhesion assay, where all three types of adhesion patterns were considered: localized, diffuse and auto- agglutinated adhesion2’. Cryptosporidium sp. were identified in slide stool smears usin the Kinyoun modification of the Ziehl-Neelsen stain $2 .
Sera were tested for IgA rotavirus antibodies by ELISA using RRV as antigen, starting at a 1:50 dilution2’. Plaque reduction neutralization (PRN) assay 24 was carried out on all sera available from infants who subsequently developed rotavirus illness and on some randomly selected sera from infants who did not. PRN assays were performed with the following viruses: Wa (human serotype Gl), DSl (human serotype G2) and P (human serotype G3).
Data analysis
Of the 800 children who received vaccine or placebo, 782 were under surveillance for more than 30 days and were included in the analysis; 685 (86% of vaccinated children) completed 24 months of surveillance. The surveillance period was defined to begin 14 days after the vaccine administration. Reasons for withdrawal from the study included the following: death in 13 cases, refusal to continue in the study (mostly due to rejection of the second blood sample) in 15 cases; and migration out of the study area in 87 cases. The 782 children under surveillance generated a total of 1371 child-years (ch-y) of observation; the children were distributed similarly among the four study groups (347 in the Gl group, 347 in the G2 group, 338 in the RRV group, and 339 in the placebo group).
Rotavirus diarrhea1 rates were calculated using all rotavirus-positive diarrhea1 episodes or only those rotavirus-positive diarrhea1 episodes in which Salmonella, Shigella, Camp_vlobacter sp., Vibrio sp., ETEC, EAEC and Cryptosporidium sp. were not identified in the stool sample (rotavirus-only diarrhea). Rotavirus diarrhea1 episodes were analyzed by severity utilizing several clinical indicators or a combined severity score (Kapikian’s severity score, a modification of that used by Flores et a/.(j with 20 points as the possible maximum). Vaccine efficacy and 95% confi- dence intervals (CI) were calculated as previously describedz5. Student’s t-test, Fisher’s exact test or chi-square with Yates correction were used as indicated.
RESULTS
Side-effects and vaccine shedding
The prevalence of diarrhea (Table I) or the mean number of liquid or semi-liquid stools per day (data not shown) was similar between the vaccine and placebo groups for each of the 6 post-immunization days. Only the RRV vaccine was associated with fever on day 4
Vaccine 1996 Volume 14 Number 3 239

Efficacy of rotavirus vaccines in Peruvian children: C.F: Lanata et al.
Table 1 Per cent of children with diarrhea or rectal temperature “.d
X38.1 “C by day post-immunization ---Cl
Symptom by Day Day Day Day Day Day vaccine or placebo group 1 2 3 4 5 6
._______ G2
- RRV -m- Placebo
DIARRHEA Placebo 5.6 10.6 7.6 14.1 13.7 14.1
I$ 2.5 5.5 10.6 14.1 8.6 13.6 11.7 12.1 11.2 11.2 13.2 11.5 RRV 6.6 10.1 12.6 12.6 14.3 15.8 RECTAL TEMP s38.1”C Placebo
:: A::, 0.5
1.2 2.4 2.4 1.8 1.3
1.2 1.8 0.6 2.9 2.9 3.6 1.8 1.2 2.4 2.5 RRV 0.6 0.0 1.8 8.aa 3.4 3.0
0.1 -
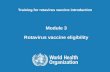
3-5 6-8 9-11 12-14 IS-17 IS-20 21-23 24-+
“p=O.O2 chi-square test, RRV vs placebo Figure 1 Incidence of rotavirus diarrhea (episodes/child-year) by age and vaccine group
post-immunization (8.8% vs 2.4% RRV vs placebo, p=O.O2, chi-square test) (Table I)_ No association was found for any of the vaccines and cough, vomiting or other signs and symptoms.
Rotavirus was shed by 12% of Gl, 18% of G2 and 17% of RRV vaccine recipients and by 5% of placebo recipients in the single stool sample taken on day 4 or 5 post-immunization (141-150 stool samples per group).
was observed most strongly in children aged 6-17 months, where the difference between the rotavirus diarrhea rate in the children who received RRV vaccine and those who received placebo was highly significant (pcO.001, chi-square for trend, Figure 1).
Vaccine efficacy
An overall diarrhea rate of about nine episode&h-y was observed in each group (Table 2). Of the 12 104 diarrhea1 episodes in all groups detected during the surveillance period, 7739 (64%) were tested by ELISA for rotavirus; 308 (4%) of the 7739 were rotavirus- positive.
Of the 308 rotavirus-positive diarrhea1 episodes, 122 (40%) yielded at least one additional possible entero- pathogen as follows: 10 with Campylobacter sp.; 59 with EAEC; 25 with ETEC; 2 with Shigellu; and 2 with Cryptosporidium sp. Twenty-four episodes yielded two or more of these agents. There was no significant vaccine efficacy against those rotavirus diarrhea1 episodes with mixed infections (data not shown). In the analysis of rotavirus-only diarrhea, the efficacy of the Gl, G2, and RRV vaccines were 6, 23 and 18%, respectively, none reaching statistical significance (Table 2).
The Gl or G2 vaccine failed to protect against any rotavirus diarrhea whereas the RRV vaccine yielded a protective efficacy of 29% (CI of 447% efficacy, ~~0.03, chi-square test) (Table 2). Moreover, the vaccine efficacy
There was a tendency towards a higher vaccine effi- cacy in preventing rotavirus diarrhea1 episodes with some indicators of severity, in particular those with some degree of dehydration or with utilization of health
1
Table 2 Rotavirus diarrhea1 episodes and vaccine efficacy by type of episode and vaccine group
Characteristic Placebo n;33ga
Gl vaccine I?=347
G2 vaccine rJ=347
RRV vaccine 1~338
Diarrhea incidence Any rotavirus diarrhea Any rotavirus diarrhea with -dehydration -health service use Rotavirus-onlyd diarrhea Rotavirus-only diarrhea with -dehydration -health service use Any Serotype 1 rotavirus diarrhea Any Serotype 1 rotavirus diarrhea with -dehydration -health service use Rotavirus Serotype 1 -only diarrhea Rotavirus Serotype 1 -only diarrhea with -dehydration -health service use Any Serotype 2 rotavirus diarrhea Any Serotype 2 rotavirus diarrhea with -dehydration -health service use Rotavirus Serotype 2-only diarrhea Rotavirus Serotype 2-only diarrhea with -dehydration -health service use
8.85 8.76 8.67 9.05 82 84 (O%)b a4 (0%) 58 (29%)C
26 18 (32%) 16 (40%) 17 (34%) 40 38 (7%) 41 (0%) 31 (22%) 28 27 (6%) 22 (23%) 23 (18%)
12 5 (59%) 2 (84%)’ 6 (50%) 13 13 (2%) 11 (17%) 12 (7%) 32 32 (2%) 39 (0%) 22 (31%)
10 9 (12%) 9 (12%) 6 (40%) 18 17 (8%) 23 (0%) 10 (42%) 11 14 (0%) 10 (11%) 10 (9%)
6 s I?’ 1 (84%)’ 2(67%) 7 00 5 (30%) 5 (28%) 17 20 (0%) 13 (25%) 15 (12%)
6 6 (2%) 1 (84%)’ 4 (33%) 7 7 (2%) 3 (58%) 6 (14%) 6 4 (35%) 4 (35%) 6 (0%)
3 2 (35%) 0 (100%) 1 (67%) 2 2 (2%) 1 (51%) 1 (50%)
“Child-years observed. ‘Numbers in parentheses indicate protective efficacy when compared to placebo group. cp=0.03 vs placebo, chi-square test with Yates correction. “Negative for other enteropathogens. =p=O.Ol vs placebo, chi-square test with Yates correction. ‘p=O.O7 vs placebo, Fisher’s exact test, two-tailed
240 Vaccine 1996 Volume 14 Number 3

Efficacy of rotavirus vaccines in Peruvian children: C./T Lanata et al.
services (Table Z), and when some individual severity indicators were analyzed (data not shown). Only the G2 vaccine gave significant protection against rotavirus diarrhea1 episodes with some degree of dehydration (84% vaccine efficacy, p=O.Ol) (Table 2).
Serotype-specific protection
Of the 308 rotavirus diarrhea1 episodes, only 196 (64%) could be serotyped by ELISA, despite several attempts to amplify the virus in tissue culture. Of these. 125 (64%) were serotype Gl, 65 (33%) serotype G2, 3 (2%) serotype G3 (1 in the placebo, 1 in the G2, and 1 in the RRV groups) and 14 (7%) serotype 4 (2 in the placebo, 2 in the Gl, 7 in the G2 and 3 in the RRV groups). Eleven samples were positive for more than one G serotype and are inclu’ded in both serotype groups for analysis.
None of the vaccines, offered significant protection against either serotype Gl or G2 rotavirus diarrhea (Table 2). A trend towards protection was observed against any serotype G.1 rotavirus diarrhea in RRV recipients (31% vaccine ,:fficacy), and against any sero- type G2 rotavirus diarrhea among G2 recipients (25%; vaccine efficacy). Efficacy was not observed for the “rotavirus-only” diarrhea1 episodes. Again, a tendency towards efficacy was observed when analysing diarrhea1 episodes by severity indicators. The G2 vaccine was 84% protective against diarrhi:a with dehydration in serotype Gl rotavirus-only diarrhea and in serotype G2 rotavirus diarrhea @=0.07, Fisher’s exact test, two-tailed, data not shown) and 100% protective against febrile serotype G2 rotavirus-only diarrhea @=0.06, Fisher’s exact test, two- tailed, data not shown). Because of insufficient cases of G serotype 3 or 4 rotavirus diarrhea, we could not determine the protection offered by these vaccines against these serotypes.
Seroresponse
Pre- and post-immunization pairs of sera were avail- able from 611 infants. T:he remaining 189 sera were lost in transport between Li:ma and Bethesda. At baseline, 293 (48%) serum samples tested for IgA rotavirus anti- bodies by ELISA had a titre of ~150, equally distrib- uted among study groups (Table 3). After immunization, all vaccine groups had a significant rise in IgA rotavirus geometric mean titre (GMT) compared with placebo recipients (Table 3). A fourfold seroresponse was ob- served in 18% of placebo recipients, compared with 48%
Table 3 Pre- and post-immunization antibody titres tested by IgA ELISA and plaque reduction neutralization (PRN) test by vaccine
type
Characteristic and Placebo Gl G2 RRV antigen used in assay vaccine vaccine vaccine
IgA ELISA No. tested 154 150 158 149 No. with negative 73 (47%) 76 (51%) 68 (43%) 76 (51%) (c1:50) baseline titres GMTa ure GMT post No. with fourfold seroresponse PRN test vs indicated antigen Wa virus (Gl) No. tested GMT pre- GMT post- No. with fourfold seroresponse DSl virus (G2) No. tested GMT pre- GMT post- No. with fourfold seroresponse P virus (G3) No. tested GMT pre- GMT post- No. with fourfold seroresponse
55+3 55+3 58+3 51+3 77+4b 161k5 306k4” 167+4 28 (18%)b 72 (48%) 104 (66%)’ 73 (49%)
49 142 23 69 116k3b 79+2 52+3 64+2 66+3 7023 4523 52+3 7 (14%) 27 (19%)“ 2 (9%) 5 (7%)
34 9 127 2 34+2 47+2 33+2 40+3 33k2 32k2 33+2 20+0 6 (18%) 0 (0%) 18 (14%) 0 (0%)
27 0 0 103 56+2 - 63+2 35+2 - 4422 2 (7%) - : 6 (6%)
aGMT= geometric mean titre, mean f standard deviation. bPIacebo significantly different (&O.OOl) than any vaccine type, Student’s t-test or chi-square with Yates correction. %2 vaccine significantly different (~0.01) than the other two vaccine types. dGl vaccine vs RRV vaccines, ~0.05 chi-square with Yates correction
for the Gl group, 66% for G2 group and 49% for the RRV group (p<O.OOl, chi-square test). G2 vaccine re- cipients had a significant higher seroresponse rate and post-immunization GMT than children receiving the other two vaccines. There was a strong correlation between baseline antibody titre and the rate of signifi- cant seroresponses (p~O.0001, chi-square for trend) as titres of 1: 100 or greater inhibited a serologic response. Seroresponses were also related to post-immunization rotavirus shedding. A fourfold seroresponse was ob- served in 53% of Gl, 89% of G2, 88% of RRV, and 100% of placebo recipients who shed rotavirus during
Table 4 Serotype 1 and 2 rotavirus diarrhea and vaccine efficacy in children who did or did not develop a seroresponse by plaque reduction neutralization assay with the lhomologous strain by study group
Rotavirus diarrhea associated with indicated VP7 serotype
Placebo
Wa (Gl) PRN sero-negativea
;;A (G2)
sero-negative
Gl Vaccine
Wa (Gl) PRN sero-negative
Wa (Gl) PRN sero-positiveb
G2 Vaccine
DSl (G2) PRN sero-negative
DSl (G2) PRN sero-positive
Serotype 1 Rate Vaccine efficacy (%) Serotype 2 Rate Vaccine efficacy (%)
16i77’ -
-
-
- 221203 3144 - - - 48’ 67e - -
6151 - - 14/l 87 2132 - - - 36 46
eFailed to develop a 2fourfolcl antibody rise by PRN to indicated virus. bDeveloped a >fourfold antibody rise by PRN to indicated virus. T\lo. diarrhea1 episodes/child-yr observed. dp=0.05, chi-square test with Yates correction. ep0.08, chi-square test with Yates correction
Vaccine 1996 Volume 14 Number 3 241

Efficacy of rotavirus vaccines in Peruvian children: C.E Lanata et al.
the week post-immunization, compared with 42%, 62% @<0.05), 41% (p~O.001) and 18% (p~O.001) of each group, respectively, who did not shed rotavirus during the same week.
None of the vaccines induced serotype-specific sero- responses, as measured by the PRN, that were signifi- cantly different than the rate observed in placebo recipients (Table 3). The serotype-specific response rates were higher in the Gl and the G2 vaccinees (19 and 14%, respectively) than in the RRV vaccine group (6%). All PRN GMT were higher in the pre- than post- immunization sera. Placebo recipients had significantly higher Wa (serotype Gl) GMT at baseline than vaccinees.
Vaccine efficacy was not significantly different in children with and without an IgA rotavirus seroresponse (data not shown). There was a trend towards higher vaccine efficacy for the homologous rotavirus strain in children who developed serotype-specific seroresponse compared with placebo recipients who did not (Table 4).
DISCUSSION
Vaccination may be the only way to prevent serious diarrhea1 illness due to rotavirus. Two rotavirus proteins induce immune responses with neutralizing activity: VP4 (determining the P serotype), the protein responsible in certain strains for the viral hemagglutinin that forms spike-like projections on the viral surface, and VP7 (determining the G serotype), the outer capsid glyco- protein. Studies of the natural history of rotavirus diarrhea indicate that natural infections, symptomatic or asymptomatic, induce protective immunity, mostly against the homotypic G serotype”.‘*.
This trial shows that RRV vaccine was significantly effective in reducing rotavirus diarrhea. Neither the serotype Gl or the serotype G2 reassortant vaccines showed any efficacy against all rotavirus diarrhea or even rotavirus diarrhea due to strains homotypic with respect to those vaccines. The G2 vaccine gave signifi- cant protection against serotype Gl or G2 rotavirus diarrhea with dehydration.
Several factors could explain these results. The most striking one is the low frequency of serotype-specific seroresponse induced by any of the vaccines, despite the fact that most infants developed rotavirus-specific IgA seroresponses after vaccination. The low immunogenic- ity of the vaccines in our setting was correlated with their low reactogenicity, where only the RRV vaccine was associated with low grade fever, with a rate much lower than that observed in Venezuela6 and in developed countries7p10.26.27. Vaccine shedding was quite low com- pared to the Venezuelan study6. The prevalence of baseline antibodies was high in our setting, indicating previous exposures of the infant to rotavirus and/or the presence of maternal antibodies. Finally, the serore- sponse rate observed in the placebo group indicated a high rate of natural exposure to wild rotavirus infection in infants occurring at the time of the rotavirus vaccine administration.
In a study in Venezuela of the safety and immuno- genicity of Gl and G2 vaccine strains, as compared with RRV, Flores et aL2* demonstrated that PRN sero- conversion against the Wa (serotype Gl) virus was higher in children with lower baseline antibodies, in
242 Vaccine 1996 Volume 14 Number 3
children who shed the vaccine virus, and in children 3-5 months of age, compared with l-2 months of age. These results also indicated that the VP4 of RRV is more immunogenic than the VP7 and that VP4 antibodies represent an important component in the responses induced by the vaccines.
The importance of serum antibodies (directly or as a surrogate marker for local antibodies) in protection against rotavirus diarrhea remains enigmatic with some studies demonstrating and other failing to show an association29x30. Indeed, even the role of serotype- specific neutralizing antibodies once considered to be the keystone of protection has had to be reevaluated because of conflicting results. Clearly, further studies are needed to elucidate the role of the various facets of the immune system, including cell-mediated mechanisms, as effecters of protection against rotavirus disease. Never- theless, we postulate that the low reactogenicity and immunogenicity of the RRV and reassortant vaccines in Lima was due to interference from baseline antibodies, present at the time of immunization in these young (2 months of age) infants. These antibodies may have been derived from transplacental transfer or acquired in breast milk.
The heterotypic protection seen only with the RRV vaccine and not with the reassortant vaccines is difficult to explain. It appears that the reassortants are less reactogenic than the RRV, suggesting that they may be more attenuated than the parental RRV strain. The heterotypic protection given by the RRV in Peru is similar to the level of protection seen in studies using the same dose in developed countries7-” and lower than the homotypic protection seen in Venezuela6. It may be postulated that the RRV may yield a low level of general protection against diarrhea caused by rotaviruses other than serotype G3, by unknown mechanisms, and higher efficacy against the homotypic rotavirus diarrhea. We have not studied the VP4 (P serotype) characterization of the rotavirus diarrhea seen in the study nor the P serotype seroresponse induced by the vaccines. It is clear from this study that in order to elicit serotype-specific seroresponses and protection, the vaccine titre may need to be increased and/or more than one dose of the vaccine may need to be given. Our results also suggest that in order to make them comparable, the reassortant vac- cines may need to be given in a higher dose than the RRV vaccine.
In conclusion, one dose of lo4 p.f.u. of the RRV, Gl and G2 rotavirus vaccines failed to induce high level serotype-specific seroresponses or serotype-specific pro- tection in children immunized at 2 months of age. Only the RRV vaccine induced a low level of heterotypic protection, mainly against serotype Gl rotavirus diarrhea. Future studies need to explore how a higher vaccine titre and/or more than one dose may be able to make the vaccines more immunogenic and effective against homotypic rotavirus diarrhea in developing countries in which infants have a high level of baseline rotavirus antibodies.
ACKNOWLEDGEMENTS
This study was presented at the Conference Vaccines for Enteric Diseases, Cambridge, UK, April 1992. The study was supported by the Diarrhoeal Diseases Control

Efficacy of rotavirus vaccines in Peruvian children: C./T Lanata et al.
Programme of the World Health Organization and by the Vaccine Developmem Participating Agencies Service Agreement between the United States Agency for International Development and National Institutes of Health, US Public Health Service (via the Pan-American Health Organization). Data analysis was also sup- ported by the United Kingdom Overseas Development Administration by means of a grant for Dr Claudio F. Lanata to be a Visiting Research Fellow in the Maternal and Child Epidemiology Unit, London School of Hygiene and Tropical Medicine. The authors are grate- ful to Irene Perez-Schael. for her help with the vaccine coding and randomization, Annie Pittman and Johnna Sears for performing the serological studies, Hector Verastegui for his help in data analysis and to the study field workers, field supervisors and field doctors for their great care and efficiency in conducting this study.
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
Institute of Medicine. Prospects for immunizing against rota- virus. In: New Vaccine Development. Establishing Priorities. Appendix D-13 (Diseases of importance in Developing Countries, Vol 2). National Academy Press, Washington, DC, 1986, pp. 308-318 De Zoysa, I. and Feachern, R.G. Interventions for the control of diarrhoeal diseases among young children: rotavirus and cholera immunization. Bull. W/-/O 1985, 63, 569-583 Vesikari, T., Isolauri, E., Delem, A. et al. Clinical efficacy of the RIT 4237 live attenuated bovine rotavirus vaccine in infants vaccinated before a rotavirus epidemic. J. Pediatr. 1985, 107, 189-195 Lanata, C.F., Black, R.E., Del Aguila, R. et a/. Protection of Peruvian children against rotavirus diarrhea of specific sero- types by one, two, or three doses of the RIT 4237 attenuated bovine rotavirus vaccine. J. Infect. Dis. 1989, 159, 452-459 Hanlon, P., Hanlon, L., Marsh, V. et al. Trial of an attenuated bovine rotavirus vaccine (RIT 4237) in Gambian children. Lancef 1987, 1, 1342-l 345 Flores, J., Perez-Schael, I., Gonzales, M. et a/. Protection against severe rotavirus cliarrhoea by Rhesus rotavirus vaccine in Venezuelan infants. Lancet 1987, 1, 882-884 Christy, C., Madore, H.P., Pichichero, M.E. et al. Field trial of rhesus rotavirus vaccine in infants. Pediatr. Infect. Dis. J. 1988, 7, 645-650 Rennels, M., Losonsky, G.A., Young, A.E., Shindledecker, C.L., Kapikian, A.Z. and Levine, M.M. An efficacy trial of the rhesus rotavirus vaccine in Marlland. Am. J. Dis. Child. 1990, 144, 601-604 Vesikari, T., Rautanen, T., Varis, T., Beards, G.M. and Kapikian, A.Z. Rhesus rotavirus candidate vaccine. Clinical trial in children vaccinated between 2 and 5 months of age. Am. J. Dis. Child. 1990, 144, 285-289 Gothefors, L., Wadell, G., Juto, P., Taniguchi, K., Kapikian, A.Z. and Glass, R.I. Prolonged efficacy of rhesus rotavirus vaccine in Swedish children. J. Infect Dis. 1989, 159, 753-757 Chiba, S., Yokoyama, T., Nakata, S. et a/. Protective effect of naturally acquired homotypic and heterotypic rotavirus anti- bodies. Lancet 1986, 2, 4 17-421 Gerna, G., Sarasini, A., Torsellini, M., Torre, D., Parea, M. and Battaglia, M. Group- and type-specific serologic response in infants and children with primary rotavirus infections and gastroenteritis caused by a strain of known serotype. J. Infect. Dis. 1990, 161, 1105-1111
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
Midthun, K., Greenberg, H.B., Hoshino, Y., Kapikian, A.Z., Wyatt, R.G. and Chanock R.M. Reassortant rotaviruses as potential live rotavirus vaccine candidates. J. Viral. 1985, 53, 949-954 Midthun, K., Hoshino, Y., Kapikian, A.Z. and Chanock, R.M. Single gene substitution rotavirus reassortants containing the major neutralization protein (VP7) of human rotavirus serotype 4. J. C/in. Microbial. 1986, 24, 822-826 Yeager, B.A.C., Lanata, C.F., Lazo, F., Verastegui, H. and Black, R.E. Transmission factors and socioeconomic status as determinants of diarrhoeal incidence in Lima, Peru. J. Diarrhoeal Dis. Res. 1991, 9, 186-193 Baqui, A.H., Black, R.E., Yunus, M.D., Azimui-Hoque, A.R., Chowdhury, H.R. and Sack, R.B. Methodological issues in diarrhoeal diseases epidemiology: definition of diarrhoeal episodes. Int. J. Epidemiol. 1991, 20, 1057-l 063 Flewett, T.H., Arias, C.F., Avendano, L.F. et a/. Comparative evaluation of the WHO and DAKOPATTS enzyme-linked immunoassay kits for the rotavirus detection. Bull. W/-/O 1989, 67, 369-374 Taniguchi, K., Urasawa, T., Morita, Y., Greenberg, H.B. and Urasawa, S. Direct serotyping of human rotavirus in stools by an enzyme-linked immunosorbent assay using serotype l-, 2-, 3-, and 4 specific monoclonal antibodies to VP7. J. infect. Dis. 1987,155, 1159-1166 Lennette, E.H., Balows, A., Hansler, W.H. and Shadomy, H.J. (Eds). Manual of Clinical Microbiology, 4th ed. American Society for Microbiology, Washington, DC, 1985 Moseley, S.L., Echevarria, P., Seriwatana, J., Tirapat, C., Chaicumpa, W., Sakuldaipeara, T. and Falkow, S. Identification of enterotoxigenic Escherichia co/i by colony hybridization using three enterotoxin gene probes. J. Infect. Dis. 1982, 145, 863-869 Nataro, J.P., Kaper, J.B., Robinson-Browne, R. eta/. Patterns of adherence of diarrheagenic Escherichia co/i to Hep-2 cells. Pediatr. Infect. Dis. J. 1987, 6, 829-831 Garcia, L.S., Bruckner, D.A., Brewer, T.C. and Shumizu, R.Y. Techniques for the recovery and identification of Cryptosporid- ium oocysts from stool specimens. J. C/in. Microbial. 1983, 18, 185-l 90 Losonsky, G.A., Rennels, M.B., Lim, Y., Krall, G., Kapikian, A.Z. and Levine, M.M. Systemic and mucosal immune responses to rhesus rotavirus vaccine MMU 18006. Pediafr. Infect. Dis. J. 1988, 7, 388-393 Hoshino, Y., Wyatt, R.G., Greenberg, H.B., Flores, J. and Kapikian, A.Z. Serotypic similarity and diversity of rotaviruses of mammalian and avian origin as studied by plaque reduction neutralization. J. infect. Dis, 1984, 149, 694-702 Orenstein, W.A., Bernier, R.H., Dondero, T.J., Hinman, A.R., Marks, J.S., Bart, K.J. and Sirotkin, 8. Field evaluation of vaccine efficacy. Bull. W/-/O 1985, 63, 1055-l 068 Santoshan, M., Letson, G.W., Wolff, M. eta/. Afield study of the safety and efficacy of two candidate rotavirus vaccines in a native American population. J. Infect. Dis. 1991, 163, 483-487 Madore, H.P., Christy, C., Pichichero, M. et a/. Field trial of rhesus rotavirus or human-rhesus rotavirus reassortant vaccine of VP7 serotype 3 or 1 specificity in infants. J. Infect. Dis. 1992, 166, 235-243 Flores, J., Perez-Schael, I., Blanco, M. et a/. Reactions to and antigenicity of two human-rhesus rotavirus reassortant vaccine candidates of serotypes 1 and 2 in Venezuelan infants. J. C/in. Microbial. 1989, 27, 512-518 Kapikian, A.Z. Rhesus rotavirus-based human rotavirus vac- cines and observations on selected non-Jennerian approaches to rotavirus vaccination. In: Viral infections of the Gastro- intestinal Tract (Ed. Kapikian, A.Z.). Marcel Dekker Inc., New York, 1994, pp. 443-470 Glass, R.I., Gertsch, J. and Smith, J.C. Rotavirus vaccines: success by reassortment. Science 1994, 265, 1389-l 391
Vaccine 1996 Volume 14 Number 3 243
Related Documents