Immunization for Children Immunization for Children รศ.นพ.ภพ โกศลารักษ์ ภาควิชากุมารเวชศาสตร์ คณะแพทยศาสตร์ มหาวิทยาลัยขอนแก ่ น

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Immunization for ChildrenImmunization for Childrenรศ.นพ.ภพ โกศลารักษ์
ภาควชิากมุารเวชศาสตร์
คณะแพทยศาสตร์
มหาวทิยาลยัขอนแก่น

Pediatric vaccination
• Basic knowledge
• Pitfalls in EPI vaccines
• Optional vaccines
• Questions and Answers

Host Defense Mechanism• Physicoanatomical barrier
• Phagocytosis– Circulating phagocytosis e.g. PMN
– Fixed phagocytosis e.g. macrophage
• reticuloendothelial system
• Humoral factors– Complement and properdin system
– Humoral immunity e.g. immunoglobulin
• Cell-mediated immunity

Immunization
• Passive immunization: immunoglobulin
• Active immunization: vaccination
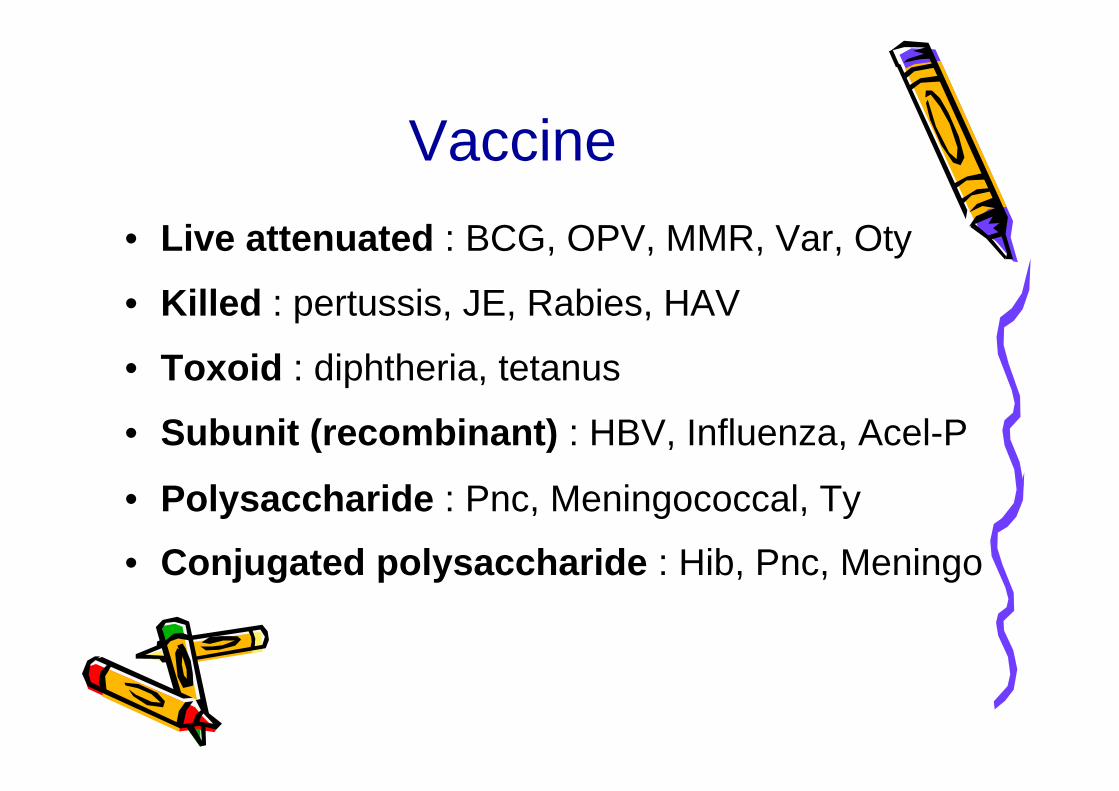
Vaccine• Live attenuated : BCG, OPV, MMR, Var, Oty
• Killed : pertussis, JE, Rabies, HAV
• Toxoid : diphtheria, tetanus
• Subunit (recombinant) : HBV, Influenza, Acel-P
• Polysaccharide : Pnc, Meningococcal, Ty
• Conjugated polysaccharide : Hib, Pnc, Meningo

Vaccine: route
• Oral: OPV, Oral typhoid
• Intramuscular: HBV, HAV, DTP, Rabies, Hib, Influenza, Typhoid
• Subcutaneous: MMR, Varicella, JE, Ty, Hib, Influenza
• Intradermal: BCG, Rabies

Injection Site • Vaccines should not be injected on the hip area
• Infants and young children: antero-lateral of mid-thigh
• Older children: deltoid

Vaccination - aims
• Short term
: Prevention – individual, risk group• Long term
: Eradication
: Smallpox, Polio, Measles, HBV

Vaccination• Mimic natural infection• Low adverse events• Protection
: antibody, antitoxin, CMIR: short term – killed vaccine: long term – attenuated vaccine

Pitfalls in EPI vaccines
• Vaccine schedule• Adverse reaction• Vaccine information system

EPI Schedule for Thai ChildrenEPI Schedule for Thai Children
Birth 1M 2M 4M 6M 9M 18M 4-6Y
BCG
HBV1 HBV2 HBV3
DTP1 DTP2 DTP3
OPV1 OPV2 OPV3
DTP4 DTP5
OPV4 OPV5
MMR1
JE1,2, 3, (4)
MMR2
ThendT q 10 yrs

Rate of ReactogenicityRate of Reactogenicity
0102030405060708090
100
BCG Hib HBV M/MMR OPV T/DT DTP
Local Fever other systemic
Perc
ent

Arthus’ ReactionArthus’ Reaction

BCG LymphadenitisBCG Lymphadenitis

BCG Complications
BCG should not be given at buttock or hip:
- irritation from diaper- contamination with urine/stool- difficult to examine scar

Multiple BCG Does Not Confer Better Immunity

More Local Reaction from Repeated BCG
MOPH no longer give second BCG unless there is no document of BCG at birth and no scar
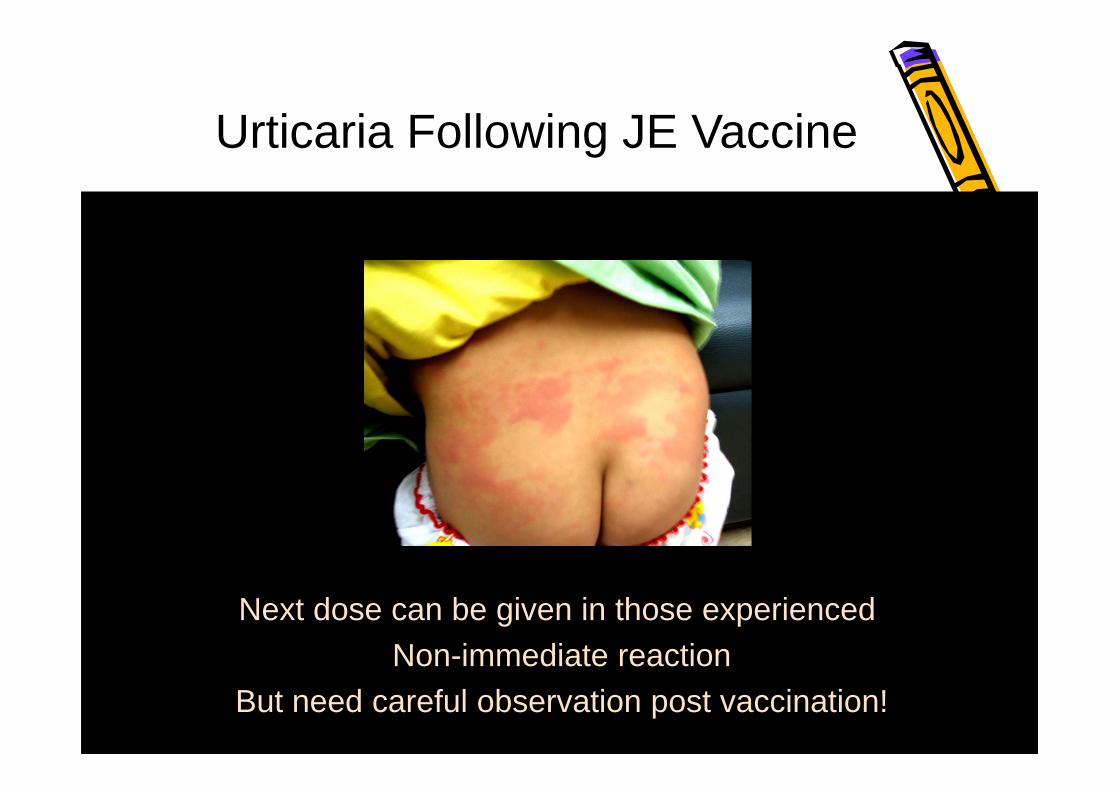
Urticaria Following JE Vaccine
Next dose can be given in those experienced Non-immediate reaction
But need careful observation post vaccination!

อตัราความครอบคลุมโดยเฉลี่ยของวคัซีนในงานสร้างเสริม
ภมูิคุม้กนัโรคในประเทศไทย
วคัซีน ร้อยละ
บีซีจี 99
คอตีบ-บาดทะยกั-ไอกรน (ดีทีพี) ครั้งที่ 3 98
โปลิโอ ครั้งที่ 3 98
ตบัอกัเสบบี ครั้งที่ 3 96
หดั 96
บาดทะยกัในหญิงมีครรภ ์(2 ครั้งหรือกระตุน้) 93
ไขส้มองอกัเสบครั้งที่ 2 87
จากการสาํรวจดว้ยวธิี cluster survey โดยกรมควบคุมโรค พ.ศ.2546

Impact of Vaccination
Impact of Vaccination

Tetanus Cases Reported in ThailandTetanus Cases Reported in Thailand
0
5
10
15
20
25
Case/100,000
Death%

Pertussis Cases Reported in ThailandPertussis Cases Reported in Thailand
0
2
4
6
8
10
12
Case/100,000
Death%

Measles Cases Reported in ThailandMeasles Cases Reported in Thailand
0
20
40
60
80
100
Case/100,000
Death%

EncephalitisEncephalitis
0
5
10
15
20
25
30
Case/100,000
Death%

2010 Optional Immunization Schedule for Thai Children
2M 4M 6M 9M 12M 18M 4-6Y 11-12Y
VZV1
Hib1 Hib2 Hib3
HAV1,2*
DTaP1 DTaP2 DTaP4DTaP3 DTaP5/Tdap
IPV1 IPV2 IPV3 (IPV4) Tdap then dT
q10y
HPV1,2,3
Rota1 Rota2 (Rota3)
PCV7-1
PCV7-2
(PCV7-3)
Yearly Influenza Vaccine
PCV7-4Live JE 1,2
VZV2
IPV5(Hib4)
* Optional schedule for healthy infants: 2+1 (2, 4, 12-15 m)
* PIDST Recommendation 2010

Optional vaccines
• Increase immunogenicity in infant: conjugated vaccine: H. influenzae B, PCV, Meningococcus
• Less adverse event: IPV, acellular pertussis, rotavirus
• New vaccines: HPV, rotavirus: Varicella, HAV

Pichichero M. Consultant for Pediatricians 2005;June:263-7.
PolysaccharideConjugate Property
NoYesLack of hyporesponsiveness
NoYesBooster effect
NoYesPersistence of protection
NoYesHerd immunity
NoYesReduction of nasopharyngeal carriage of bacteria
NoYesImmune memory
NoYesT-cell-dependent immune response(response by children < 2 yo)
Comparison of Polysaccharide and Conjugate Vaccines

Rosenberg N.M. NEJM 2001;345(14):1042-53.
Principle of Polysaccharide-Protein Conjugate VaccinePrinciple of Polysaccharide-Protein Conjugate Vaccine

WHO. 2004 Global Immunization Data. Available at: http://www.who.int/immunization_monitoring/data/GlobalImmunizationData.pdf. Accessed July 11, 2008.
Pneumococcal disease
Measles Rotavirus Hib Pertussis Tetanus Other* Meningococcus
*Polio, diphtheria, yellow fever
Estim
ated
num
ber o
f dea
ths
(WH
O 2
002)
Global PerspectiveVaccine-Preventable Deaths (WHO)
Global PerspectiveVaccine-Preventable Deaths (WHO)
0
500,000
1,000,000
1,500,000
2,000,000
All agesChildren < 5 years
Streptococcus pneumoniae is the leading cause of vaccine-preventable deaths globally

IPD( Invasive Pneumococcal Disease )
Atkinson W, et al, eds. Epidemiology and Prevention of Vaccine-Preventable Diseases. CDC Pink Book. 11th ed. Washington DC: Public Health Foundation; 2009:217-230. 30
Seve
rity
of D
isea
seMeningitis
Bacteremia
Acute otitis media
Bacteremic pneumonia
Pneumonia
IPD

Coverage of Invasive Pneumococcal Isolates by PCV in Thai Children 2000-2005
Collaborative study: Siriraj, NIH, Chula, Bhumipol, QSNICH
0
20
40
60
80
100
7 - valent 9 - valent 11 - valent 13 - valent
<1 yo
<2 yo
<5 yo
Cover by:
%
N=11571 69
74 7476 76 7476 7785 86 88
Wanatpreeya Phongsamart, et al. Vaccine 2007; 25:1275-80

Paper PCV7 PCV10 PCV13 Years N** Method
Phongsamart W, et al. Vaccine 2007;25:1275-1280 1
73.9% 77.4% 87.8%2000-2005
(4 institutes in BKK+NIH)
115 Sterile sites
Baggett HC, et al. CID 2009;48:S65-742 79% 84% 95%
May05-June07(Sa Kaeo, Nakorn
phanom)19 Blood
Cultures
Srifeungfung S, et al. Vaccine 2010; 28:3440-34443
70.3% 70.3% 81.2%
Jan 06-Feb 09(4 tertiary care public hosp, 6 private and 4 public hosp)
106(64+42)
Sterile site and Non
Sterile site
Rhodes J, et al. 7th
ISPPD.*4 73% 75% 88% 1998-2008(>50 Hosp.) 223 Normally
sterile sites
Dejsirilert S, et al. 7th
ISPPD.*5 74% 80% 92%
1998-2008 (33 Hosp. in
1998-2004, 60 Hosp. in 2005-
2008)
113 Sterile sites
* Poster presentation 7th ISPPD, Mar 10, Tel aviv, Israel, ** Isolates from children < 5 years old
Serotype Coverage by 7-, 10-, 13-valent PCV of Normal Sterile Sites in Thai Children < 5 Years Old
Summary of PCV CoveragePCV7: 62‐79% PCV10: 70‐84%PCV13: 81‐95%
, 70%, 80%, 90%
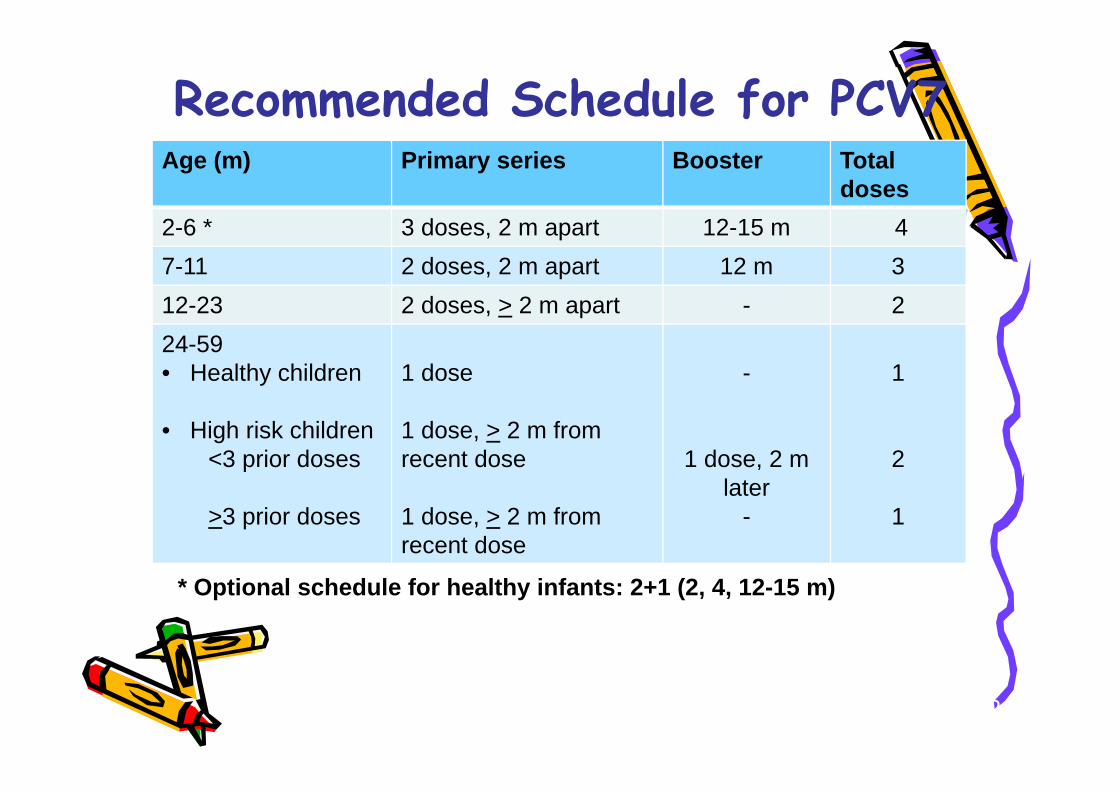
Recommended Schedule for PCV7Age (m) Primary series Booster Total
doses2-6 * 3 doses, 2 m apart 12-15 m 47-11 2 doses, 2 m apart 12 m 312-23 2 doses, > 2 m apart - 224-59• Healthy children
• High risk children<3 prior doses
>3 prior doses
1 dose
1 dose, > 2 m from recent dose
1 dose, > 2 m from recent dose
-
1 dose, 2 m later
-
1
2
1
AAP. Pediatrics 2000;106:362-6.* PIDST Recommendation 2010
* Optional schedule for healthy infants: 2+1 (2, 4, 12-15 m)

1997
1998
1999
2000
2001
2002
2003
2004
2005
0
50
100
150
200
250<112-4
Year
IPD
rat
e / 1
00 0
00
http://www.cdc.gov/ncidod/dbmd/abcs/survreports.htm
PCV7
Impact on Invasive Pneumococcal Diseases

Centers for Disease Control and Prevention. MMWR 2005;54:893-7.
Routine use of PCV in 2000

Pneumococcal Disease Burden in ThailandA prospective study of meningitis in Lampang and Phisanulok:
Population < 5 yo = 105,269N Rate/105<5yo
Potential meningitis (LP) 598 568Probable meningitis 28 26Laboratory confirmed 7 6.7
Hib 4 3.8 (1.0-9.7)
N.meningitidis 2 <3S.pneumoniae 1 (+1 pos H/C) <3
ATB detected in CSF 20/455 (4.4%)
Rerks-Ngarm S. Vaccine 2004;22:975-83.

Bacterial Meningitis in Thai Children Etiology and Mortality (N=618)
Bacterial Meningitis in Thai Children Etiology and Mortality (N=618)
Chotpitayasunondh C. Southeast Asian J Trop Med Public Health 1994;25:107-115.
%
Hib S.pneumo N.mening Salmonella Others0
5
10
15
20
25
30
35
40Proportion Mortality

Rotavirus

Pathogenesis Rotaviruses adhere to the GI tract epithelia
(jejunal mucosa)
Atrophy of the villi of the gut
* *
Loss of absorptive area
Flux of water and electrolytes
NSP4 viral enterotoxin
Enteric nervous system activation
VOMITING AND
diarrhoea
*Rotavirus infection in an animal model of infection. Photographs are from an experimentally infected calf. Reproduced with permission from Zuckerman et al, eds. Principles and Practice of Clinical Virology. 2nd ed. London: John Wiley & Sons; 1990:182.
Micrographs courtesy of Dr. Graham Hall, Berkshire, UK.

Epidemiology- Global Perspective
Bacteria
Unknown Rotavirus
Calicivirus
Rotavirus
Escherichia coli
Parasites
Otherbacteria
Developed Countries
Adenovirus
CalicivirusAstrovirusAdenovirus
Astrovirus
Unknown
Less Developed Countries
From Kapikian AZ, Chanock RM. Rotaviruses. In: Fields Virology 3rd ed 1996; 1659. Philadelphia, PA: Lippincott-Raven.
Distribution of pathogens reported to cause endemic/epidemic gastroenteritis & infantile vomiting & diarrhea

Estimated global burden of rotavirus disease
24 million outpatient visits
114 million domiciliary episodes
1 : 205
1 : 50
EventRisk of Particular Event
611,000 deaths
2.4 million inpatient visits
1 : 5
1 : 1
Rotavirus- Burden of Disease
Glass R, et al. Lancet 2006; 368: 323–332.

Rotavirus Disease Burden in ThailandRotavirus Disease Burden in Thailand
56,000 rotavirus diarrhea inpatient visit
131,000 rotavirus diarrhea health care visit
586,000 Rotavirus diarrhea episode
4.8 million diarrhea episodes(in children < 5 yo)
1 : 85
1 : 36
1 : 8
1 : 1
Risk Events
Jiraphongsa C et al. JID 2005: 192 (suppl 1)May be underestimated!
2001-3, of the 1095 stools from hospitalized
diarrhea, rotavirus positive in 838 (43%)



0
5
10
15
20
0 10 20 30 40 50 60 70
RotaShield™ RIX4414/placebo
Occurrence of Definite IS Cases Compared with RotaShield-associated Cases
V = VaccineP = Placebo
VP P
P PV V
VVP
VP P
Dose one
Dose two
V PVP P
P P P
IS cases
IS cases
75 83
107 145
VP
P P
1. Murphy TV, et al. N Engl J Med 2001;344(8):56472. 2. Vesikari T, et al. 23rd Annual Meeting of the European Society for PaediatricInfectious DiseasesESPID, Valencia, Spain, 1820 May 2005.
0
5
10
15
20
0 10 20 30 40 50 60 70

Recommendation for Use of Rotavirus Vaccines
Pentavelent (HBRV) Monovalent (HRV)
Route Oral OralAge of 1st dose 6-12 week > 6 weekGeneral schedule 2, 4, 6 mo 2, 4 moInterval of dose 4-10 week >4 weeksAge of last dose 32 week 24 weeksConcurrent OPV not mention 14 d apart for 1st doseOther concurrent vac OK OKBreast feeding OK OKContraindication Immunocommpromised, age out-of-range
allergic to vaccine/component, Ac illness

Rotavirus vaccine
• high protection against severe RVGE
– 85%–100% efficacy against all rotavirus GE-
related hospitalizations
Efficacy

Children’s Vaccine Initiative’s “Ideal Vaccine”
Children’s Vaccine Initiative’s “Ideal Vaccine”
• Oral• 1 - 2 doses• Early in life• Well tolerated
• Efficacious 100%• Safe• Can be administered:
- According to local schedule- With other vaccines
• Heat Stable• Affordable
The current vaccines: 2-3 doses Expensive Efficacy 70-90% Heat sensitive Interfered by OPV
World Health Forum 1992; 13 (1):93

Thank you
Related Documents











