REVIEW ARTICLE Immune modulation with dendritic cells N. Panoskaltsis,* C. D. L. Reid* and S. C. Knighty *Department of Haematology, and yAntigen Presentation Research Group, Imperial College London, Northwick Park & St. Mark’s Campus, London, UK Received 28 October 2003; accepted for publication 28 October 2003 Dendritic cells (DCs) are bone marrow-derived cells of haemopoietic origin that have a unique role in the primary presentation of antigen to naı¨ve cells of the effector arm of the immune response (Steinman & Witmer, 1978; Crow & Kunkel, 1982; Knight et al., 1982; Knight et al., 1983; Knight, 1984; Macatonia et al., 1989). Although a relatively young area of study in immunology, there have already been many reviews on the ontogeny, function and use of DCs in clinical trials (Banchereau et al., 2000; Banchereau & Steinman, 1998; Fong & Engleman, 2000; Nestle et al., 2001; Reid, 2001). Rather than recapitulate the details of trials of DCs in immune therapy, in this clinically orientated review, we will provide a perspective on their potential and rational use. Irrespective of their type or tissue of origin, DCs are defined phenotypically by their typical veiled appearance and their surface expression of the major histocompatibility complex (MHC) class II protein human leucocyte antigen (HLA)-DR com- bined with lack of expression of the lineage- associated or progenitor/stem cell markers (lin; CD3, CD14, CD16, CD19, CD34 and CD56) and function- ally by their ability to stimulate a primary lympho- cyte response to antigen (Steinman & Witmer, 1978; Crow & Kunkel, 1982; Knight et al., 1982; Knight et al., 1983; Knight, 1984; Macatonia et al., 1989). In the blood, tissues and lymph node, two subtypes of DCs have been characterized, one myeloid and the other plasmacytoid (Dzionek et al., 2000; Olweus et al., 1997; Robinson et al., 1999). Whether these myeloid and plasmacytoid DCs originate from unique progenitor cell lineages or whether they are derived from a single progenitor cell is controversial (Martin et al., 2000; Manz et al., 2001; Briere et al., 2002; Comeau et al., 2002; Martinez del Hoyo et al., 2002). Both subsets of DCs are similar in their ability to stimulate a primary T-lymphocyte response to antigen, but they differ in their mor- phology, surface phenotype and, possibly, in their functional capabilities [reviewed in (Banchereau et al., 2000)]. MYELOID AND PLASMACYTOID DCs Phenotypically, myeloid DCs are large, mononuclear cells, often with a monocyte-like appearance in the immature stage that, when mature, acquire a veiled appearance due to their characteristic membranous extensions that are used to interact intimately with T cells during antigen presentation (Balfour et al., 1982; Knight, 1984; Knight et al., 1986; Reid et al., 1990). Immature myeloid DCs are specialized in their ability to take up and process antigen for presentation on MHC class I and II receptors (Banchereau et al., 2000; Ridge et al., 1998; Grakoui et al., 1999). In the immature form, myeloid DCs express the a X b 2 integrin cluster designation (CD)11c, the myeloid markers CD33 and CD13, and the scavenger receptor CD36, and may display the tumour necrosis factor (TNF)-like receptor CD40, the CD1 family of lipid antigen-presenting molecules CD1a, CD1b, CD1c (BDCA-1) and CD1d as well as the B72 costimulatory glycoprotein, CD86 and the novel marker, blood DC antigen (BDCA)-3 (Banchereau et al., 2000; Hart, 1997; Dzionek et al., 2000; MacDonald et al., 2002; Vincent et al., 2002). When mature, myeloid DCs lose the expression of CD1a, express higher levels of CD40, CD86, CD11c and HLA-DR and newly up-regulate the immunoglobulin (Ig)-like lectin CD83 and the B71 costimulatory ligand, CD80 (Banchereau et al., 2000; Hart, 1997; Scholler et al., 2001). In vitro and in vivo maturation of DCs may be induced by stimula- tion with foreign antigens, cytokines or necrotic debris in the environment and by the provision of ‘helper’ signals from the surrounding cellular environment, such as CD40 ligand (CD40L) on CD4 þ T cells (Reid et al., 1992; Bennett et al., 1998; Kelleher & Knight, Correspondence: Prof. S. Knight, Antigen Presentation Research Group, Imperial College London, Northwick Park & St Mark’s Campus, Watford Road, Harrow, HA1 3UJ, UK. Tel./Fax: (0) 20- 8869-3532; e-mail: [email protected] Transfusion Medicine, 2004, 14, 81–96 # 2004 Blackwell Publishing Ltd 81

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

REVIEW ARTICLE
Immune modulation with dendritic cells
N. Panoskaltsis,* C. D. L. Reid* and S. C. Knighty *Department of Haematology, and yAntigen Presentation
Research Group, Imperial College London, Northwick Park & St. Mark’s Campus, London, UK
Received 28 October 2003; accepted for publication 28 October 2003
Dendritic cells (DCs) are bone marrow-derived cellsof haemopoietic origin that have a unique role in theprimary presentation of antigen to naı̈ve cells of theeffector arm of the immune response (Steinman &Witmer, 1978; Crow & Kunkel, 1982; Knight et al.,1982; Knight et al., 1983; Knight, 1984; Macatoniaet al., 1989). Although a relatively young area ofstudy in immunology, there have already been manyreviews on the ontogeny, function and use of DCs inclinical trials (Banchereau et al., 2000; Banchereau &Steinman, 1998; Fong & Engleman, 2000; Nestleet al., 2001; Reid, 2001). Rather than recapitulatethe details of trials of DCs in immune therapy, inthis clinically orientated review, we will provide aperspective on their potential and rational use.
Irrespective of their type or tissue of origin, DCsare defined phenotypically by their typical veiledappearance and their surface expression of themajor histocompatibility complex (MHC) class IIprotein human leucocyte antigen (HLA)-DR com-bined with lack of expression of the lineage-associated or progenitor/stem cell markers (lin; CD3,CD14, CD16, CD19, CD34 and CD56) and function-ally by their ability to stimulate a primary lympho-cyte response to antigen (Steinman & Witmer, 1978;Crow & Kunkel, 1982; Knight et al., 1982; Knightet al., 1983; Knight, 1984; Macatonia et al., 1989).In the blood, tissues and lymph node, two subtypesof DCs have been characterized, one myeloid andthe other plasmacytoid (Dzionek et al., 2000;Olweus et al., 1997; Robinson et al., 1999). Whetherthese myeloid and plasmacytoid DCs originate fromunique progenitor cell lineages or whether they arederived from a single progenitor cell is controversial(Martin et al., 2000; Manz et al., 2001; Briere et al.,2002; Comeau et al., 2002; Martinez del Hoyo et al.,
2002). Both subsets of DCs are similar in theirability to stimulate a primary T-lymphocyteresponse to antigen, but they differ in their mor-phology, surface phenotype and, possibly, in theirfunctional capabilities [reviewed in (Banchereauet al., 2000)].
MYELOID AND PLASMACYTOID DCs
Phenotypically, myeloid DCs are large, mononuclearcells, often with a monocyte-like appearance in theimmature stage that, when mature, acquire a veiledappearance due to their characteristic membranousextensions that are used to interact intimately with Tcells during antigen presentation (Balfour et al., 1982;Knight, 1984; Knight et al., 1986; Reid et al., 1990).Immature myeloid DCs are specialized in their abilityto take up and process antigen for presentation onMHC class I and II receptors (Banchereau et al.,2000; Ridge et al., 1998; Grakoui et al., 1999). Inthe immature form, myeloid DCs express the aXb2integrin cluster designation (CD)11c, the myeloidmarkers CD33 and CD13, and the scavenger receptorCD36, and may display the tumour necrosis factor(TNF)-like receptor CD40, the CD1 family of lipidantigen-presenting molecules CD1a, CD1b, CD1c(BDCA-1) and CD1d as well as the B7�2 costimulatoryglycoprotein, CD86 and the novel marker, blood DCantigen (BDCA)-3 (Banchereau et al., 2000; Hart,1997; Dzionek et al., 2000; MacDonald et al., 2002;Vincent et al., 2002). When mature, myeloid DCs losethe expression of CD1a, express higher levels of CD40,CD86, CD11c and HLA-DR and newly up-regulatethe immunoglobulin (Ig)-like lectin CD83 and theB7�1 costimulatory ligand, CD80 (Banchereau et al.,2000; Hart, 1997; Scholler et al., 2001). In vitro and invivo maturation of DCs may be induced by stimula-tion with foreign antigens, cytokines or necrotic debrisin the environment and by the provision of ‘helper’signals from the surrounding cellular environment,such as CD40 ligand (CD40L) on CD4þ T cells (Reidet al., 1992; Bennett et al., 1998; Kelleher & Knight,
Correspondence: Prof. S. Knight, Antigen Presentation Research
Group, Imperial College London, Northwick Park & St Mark’s
Campus, Watford Road, Harrow, HA1 3UJ, UK. Tel./Fax: (0) 20-
8869-3532; e-mail: [email protected]
Transfusion Medicine, 2004, 14, 81–96
# 2004 Blackwell Publishing Ltd 81
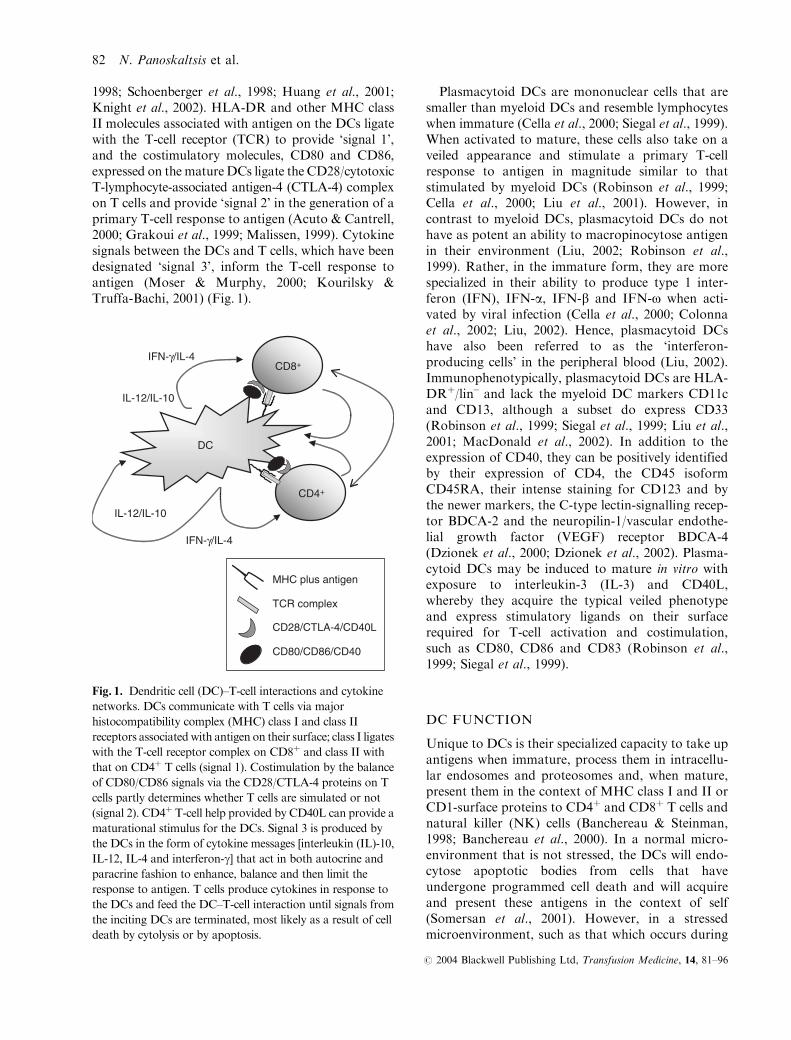
1998; Schoenberger et al., 1998; Huang et al., 2001;Knight et al., 2002). HLA-DR and other MHC classII molecules associated with antigen on the DCs ligatewith the T-cell receptor (TCR) to provide ‘signal 1’,and the costimulatory molecules, CD80 and CD86,expressed on the matureDCs ligate the CD28/cytotoxicT-lymphocyte-associated antigen-4 (CTLA-4) complexon T cells and provide ‘signal 2’ in the generation of aprimary T-cell response to antigen (Acuto & Cantrell,2000; Grakoui et al., 1999; Malissen, 1999). Cytokinesignals between the DCs and T cells, which have beendesignated ‘signal 3’, inform the T-cell response toantigen (Moser & Murphy, 2000; Kourilsky &Truffa-Bachi, 2001) (Fig. 1).
Plasmacytoid DCs are mononuclear cells that aresmaller than myeloid DCs and resemble lymphocyteswhen immature (Cella et al., 2000; Siegal et al., 1999).When activated to mature, these cells also take on aveiled appearance and stimulate a primary T-cellresponse to antigen in magnitude similar to thatstimulated by myeloid DCs (Robinson et al., 1999;Cella et al., 2000; Liu et al., 2001). However, incontrast to myeloid DCs, plasmacytoid DCs do nothave as potent an ability to macropinocytose antigenin their environment (Liu, 2002; Robinson et al.,1999). Rather, in the immature form, they are morespecialized in their ability to produce type 1 inter-feron (IFN), IFN-a, IFN-b and IFN-o when acti-vated by viral infection (Cella et al., 2000; Colonnaet al., 2002; Liu, 2002). Hence, plasmacytoid DCshave also been referred to as the ‘interferon-producing cells’ in the peripheral blood (Liu, 2002).Immunophenotypically, plasmacytoid DCs are HLA-DRþ/lin– and lack the myeloid DC markers CD11cand CD13, although a subset do express CD33(Robinson et al., 1999; Siegal et al., 1999; Liu et al.,2001; MacDonald et al., 2002). In addition to theexpression of CD40, they can be positively identifiedby their expression of CD4, the CD45 isoformCD45RA, their intense staining for CD123 and bythe newer markers, the C-type lectin-signalling recep-tor BDCA-2 and the neuropilin-1/vascular endothe-lial growth factor (VEGF) receptor BDCA-4(Dzionek et al., 2000; Dzionek et al., 2002). Plasma-cytoid DCs may be induced to mature in vitro withexposure to interleukin-3 (IL-3) and CD40L,whereby they acquire the typical veiled phenotypeand express stimulatory ligands on their surfacerequired for T-cell activation and costimulation,such as CD80, CD86 and CD83 (Robinson et al.,1999; Siegal et al., 1999).
DC FUNCTION
Unique to DCs is their specialized capacity to take upantigens when immature, process them in intracellu-lar endosomes and proteosomes and, when mature,present them in the context of MHC class I and II orCD1-surface proteins to CD4þ and CD8þ T cells andnatural killer (NK) cells (Banchereau & Steinman,1998; Banchereau et al., 2000). In a normal micro-environment that is not stressed, the DCs will endo-cytose apoptotic bodies from cells that haveundergone programmed cell death and will acquireand present these antigens in the context of self(Somersan et al., 2001). However, in a stressedmicroenvironment, such as that which occurs during
DC
CD4+
CD8+
IL-12/IL-10
IL-12/IL-10
IFN-γ/IL-4
IFN-γ/IL-4
MHC plus antigen
TCR complex
CD28/CTLA-4/CD40L
CD80/CD86/CD40
Fig. 1. Dendritic cell (DC)–T-cell interactions and cytokine
networks. DCs communicate with T cells via major
histocompatibility complex (MHC) class I and class II
receptors associatedwith antigen on their surface; class I ligates
with the T-cell receptor complex on CD8þ and class II with
that on CD4þ T cells (signal 1). Costimulation by the balance
of CD80/CD86 signals via the CD28/CTLA-4 proteins on T
cells partly determines whether T cells are simulated or not
(signal 2). CD4þ T-cell help provided by CD40L can provide a
maturational stimulus for the DCs. Signal 3 is produced by
the DCs in the form of cytokine messages [interleukin (IL)-10,
IL-12, IL-4 and interferon-g] that act in both autocrine and
paracrine fashion to enhance, balance and then limit the
response to antigen. T cells produce cytokines in response to
the DCs and feed the DC–T-cell interaction until signals from
the inciting DCs are terminated, most likely as a result of cell
death by cytolysis or by apoptosis.
82 N. Panoskaltsis et al.
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96
exposure to foreign pathogens, dying cells will releasethe intracellular molecular chaperones, heat shockproteins (HSPs), that couple with antigen to induceimmunogenic responses in the DCs (Kuppner et al.,2001; Ostberg et al., 2001; Somersan et al., 2001). Theendocytosis of necrotic bodies from the killed cells aswell as exposure to HSPs inform the DCs that themicroenvironment is stressed and that antigens beingtaken up from its surroundings should be presentedin an immunogenic fashion so that an ‘anti-pathogen’response may be elicited (Kuppner et al., 2001;Ostberg et al., 2001). DCs may stimulate not onlythe adaptive immune response in the form of CD4þ
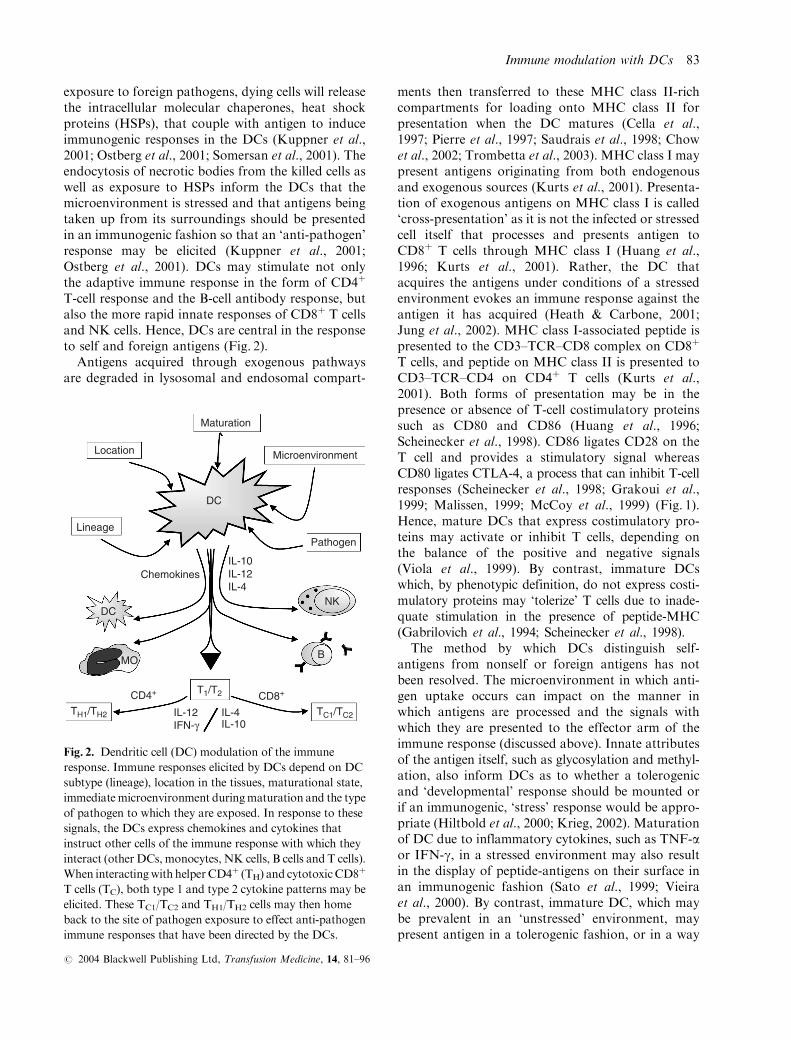
T-cell response and the B-cell antibody response, butalso the more rapid innate responses of CD8þ T cellsand NK cells. Hence, DCs are central in the responseto self and foreign antigens (Fig. 2).
Antigens acquired through exogenous pathwaysare degraded in lysosomal and endosomal compart-
ments then transferred to these MHC class II-richcompartments for loading onto MHC class II forpresentation when the DC matures (Cella et al.,1997; Pierre et al., 1997; Saudrais et al., 1998; Chowet al., 2002; Trombetta et al., 2003). MHC class I maypresent antigens originating from both endogenousand exogenous sources (Kurts et al., 2001). Presenta-tion of exogenous antigens on MHC class I is called‘cross-presentation’ as it is not the infected or stressedcell itself that processes and presents antigen toCD8þ T cells through MHC class I (Huang et al.,1996; Kurts et al., 2001). Rather, the DC thatacquires the antigens under conditions of a stressedenvironment evokes an immune response against theantigen it has acquired (Heath & Carbone, 2001;Jung et al., 2002). MHC class I-associated peptide ispresented to the CD3–TCR–CD8 complex on CD8þ
T cells, and peptide on MHC class II is presented toCD3–TCR–CD4 on CD4þ T cells (Kurts et al.,2001). Both forms of presentation may be in thepresence or absence of T-cell costimulatory proteinssuch as CD80 and CD86 (Huang et al., 1996;Scheinecker et al., 1998). CD86 ligates CD28 on theT cell and provides a stimulatory signal whereasCD80 ligates CTLA-4, a process that can inhibit T-cellresponses (Scheinecker et al., 1998; Grakoui et al.,1999; Malissen, 1999; McCoy et al., 1999) (Fig. 1).Hence, mature DCs that express costimulatory pro-teins may activate or inhibit T cells, depending onthe balance of the positive and negative signals(Viola et al., 1999). By contrast, immature DCswhich, by phenotypic definition, do not express costi-mulatory proteins may ‘tolerize’ T cells due to inade-quate stimulation in the presence of peptide-MHC(Gabrilovich et al., 1994; Scheinecker et al., 1998).
The method by which DCs distinguish self-antigens from nonself or foreign antigens has notbeen resolved. The microenvironment in which anti-gen uptake occurs can impact on the manner inwhich antigens are processed and the signals withwhich they are presented to the effector arm of theimmune response (discussed above). Innate attributesof the antigen itself, such as glycosylation and methyl-ation, also inform DCs as to whether a tolerogenicand ‘developmental’ response should be mounted orif an immunogenic, ‘stress’ response would be appro-priate (Hiltbold et al., 2000; Krieg, 2002). Maturationof DC due to inflammatory cytokines, such as TNF-aor IFN-g, in a stressed environment may also resultin the display of peptide-antigens on their surface inan immunogenic fashion (Sato et al., 1999; Vieiraet al., 2000). By contrast, immature DC, which maybe prevalent in an ‘unstressed’ environment, maypresent antigen in a tolerogenic fashion, or in a way
DC
Lineage
Location
Maturation
Microenvironment
Pathogen
IL-10IL-12IL-4
Chemokines
DCNK
MO B
T1/T2CD4+ CD8+
TH1/TH2 TC1/TC2IL-12IFN-γ
IL-4IL-10
Fig. 2. Dendritic cell (DC) modulation of the immune
response. Immune responses elicited by DCs depend on DC
subtype (lineage), location in the tissues, maturational state,
immediatemicroenvironment duringmaturation and the type
of pathogen to which they are exposed. In response to these
signals, the DCs express chemokines and cytokines that
instruct other cells of the immune response with which they
interact (other DCs, monocytes, NK cells, B cells and T cells).
When interactingwith helper CD4þ (TH) and cytotoxicCD8þ
T cells (TC), both type 1 and type 2 cytokine patterns may be
elicited. These TC1/TC2 and TH1/TH2 cells may then home
back to the site of pathogen exposure to effect anti-pathogen
immune responses that have been directed by the DCs.
Immune modulation with DCs 83
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96
that does not impede the growth of the tissue inwhich it resides (O’Doherty et al., 1994; Bell et al.,1999; Almand et al., 2001; Geissmann et al., 2002).
Type of DC may be an important discriminator inthe self–nonself phenomenon. Plasmacytoid DCsmay deliver tolerogenic signals (Dzionek et al.,2002; Liu et al., 2001; Gilliet & Liu, 2002), unlessthey are infected by virus (Cella et al., 2000; Cellaet al., 1999). Myeloid DCs may deliver both tolerogenicand immunogenic signals (Kelleher et al., 1999; Reidet al., 2000), and the balance of the two DC subsetsdetermines the final antigen-specific immune responseat the site (Moser & Murphy, 2000; Kourilsky &Truffa-Bachi, 2001). Innate pattern recognition recep-tors, such as the Toll-like receptors, may also beinvolved in determining self from nonself (Akira et al.,2001; Beg, 2002). Finally, issues of timing of antigenexposure and antigen dose may play an important rolein tolerance and immunogenicity (Knight et al., 1985;Knight & Bedford, 2001; Knight et al., 2002). Lowdoses of antigen may provide potent responses and Tcells of higher avidity up to a particular threshold(unique to the antigen, number of DCs and numberof responding T cells) (Bullock et al., 2003; Molldremet al., 2003). Beyond this threshold, down-regulation ofantigen-specific responses and selection of lower avid-ity T cells may be interpreted as tolerance (Bullocket al., 2003). These data support the hypothesis of anantigen gradient between DCs that may determine self(Knight et al., 1985; Kleindienst & Brocker, 2003). Inthe absence of a gradient, i.e with widely distributedantigen present over the threshold amount, transfer ofantigen or transfer factor does not occur and the DCsrecognize the antigen as self. However, in the presenceof a gradient, i.e. below the antigen threshold, antigentransfer occurs and the antigen is recognized asforeign (Knight & Bedford, 2001; Knight et al., 2002).This ‘antigen-transfer’ requires at least two DCs forantigen presentation to occur and may occur betweenDC subsets, e.g. between myeloid and plasmacytoidDCs in the lymph node because they enter from differ-ent routes (Knight & Bedford, 2001; Knight et al., 2002;Thery et al., 2002). Alternatively, transfer may occurbetween similar subsets at stages along the migratoryroute of DCs from the tissues into the lymph node.Experiments investigating the transfer phenomena ofDC-derived antigens, possibly in ‘exosomes’ or‘dendrosomes’, show that, in the murine model, bonemarrow-derived DCs are able to transfer antigen to allother DC subsets but are unable to receive antigen(Knight & Bedford, 2001; Knight et al., 2002). Hence,in the setting of a preponderance of bone marrow-derived DC, antigen transfer may be unable to occur.
DC TRAFFICKING
Myeloid DCs originate in the bone marrow, traversethrough the peripheral blood and settle in the tissue forvarying lengths of time before travelling via the afferentlymph to the lymph node where the majority of antigenpresentation occurs (Balfour et al., 1982; Knight, 1984;Banchereau et al., 2000). Plasmacytoid DCs also havetheir origins in the CD34þ stem/precursor cell of thebone marrow before they traverse through the bloodand settle in the tissues near the venous channels(Bianca et al., 2002; Briere et al., 2002). Their residencenear the vascular channels aids their migration, prob-ably via the blood, to the lymph node where they arelocated in close apposition to the high endothelialvenules (HEVs) (Cella et al., 1999; Cella et al., 2000).The migration of these DC subsets depends on theco-ordinated up-regulation and down-regulation ofsmall chemotactic proteins that act by way of a gradi-ent (Cyster, 1999; Moser & Loetscher, 2001; Luster,2002). Different types and amounts of these chemo-kines and their receptors are expressed at differentstages of DC maturation, migration and antigen pre-sentation and may be classified as constitutive, forthe homeostatic trafficking of leucocytes, or inflam-matory, up-regulated during infection and tissuedamage (Cyster, 1999; Moser & Loetscher, 2001;Luster, 2002).
CD34þ haemopoietic precursor cells may circulate inthe peripheral blood and provide a potential source forDCs at sites where they are needed, responding tolocally derived chemokines and cytokines for matur-ation to occur (Banchereau et al., 2000; Reid et al.,1992; Heyworth et al., 1997). DCs in the peripheralblood are usually in the immature state, in bothmyeloid(20–40 cellsmL�1) and plasmacytoid (5–20 cellsmL�1)subsets (Ho et al., 2001; Robinson et al., 1999; Soumeliset al., 2001; Knight et al., unpublished observations).The circulation of monocytes in the peripheral bloodalso provides a potential source of CD14þ-derived DCsat sites of injury (Palucka et al., 1998; Randolph et al.,1998). Particularly after encounter with pathogen, mye-loid DCs migrate to the lymph node via the afferentlymphatics in response to chemokines (Knight, 1984;Dieu et al., 1998; Sallusto et al., 1998b; Sallusto et al.,1999). Transendothelial migration into and out of thelymphatic channels may enable their maturation in vivoso that, upon arrival in the lymph node, they are fullycapable of presenting antigen toT cells (Randolph et al.,1998; Sallusto et al., 1998b; Sallusto et al., 1999).Migra-tion of plasmacytoid DCs to the lymph node has notbeen well studied. In the lymph node, as in the tissue,plasmacytoid DCs are located juxtaposed to the HEVs,
84 N. Panoskaltsis et al.
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96

implying that they have migrated from the blood ratherthan from the afferent lymph (Colonna et al., 2002).
CYTOKINE PRODUCTION BY DCs
During antigen presentation, DCs produce cytokines,which, in the case of DC–T-cell interactions, mayalso be referred to as ‘signal 3’. The type of cytokineproduced, its regulation and amount may determinethe type of immune response to pathogen. Hence,cytokine dysregulation at the level of the DC maybe implicated in the pathogenesis of diseases such aschronic infection, autoimmunity and cancer (Moser& Murphy, 2000; Kourilsky & Truffa-Bachi, 2001).
Balance in the immune system is achieved by theliberation of co-ordinated type 1 and type 2 cytokineand chemokine signals (Luther & Cyster, 2001;Mosmann & Sad, 1996; Sallusto et al., 1998a). A type1 response is associated with cytokines such as IL-12and IFN-g and is characterized by activation of thecellular adaptive immune response [reviewed in(Trinchieri, 1995)]. Type 2 responses stimulate humoralimmunity by the predominance of cytokines such asIL-4 and immune ‘tolerance’ or regulation with IL-10(Groux et al., 1997; Trinchieri, 2001; Barrat et al.,2002). Both type 1 and type 2 responses involve helperT cells (CD4þ, TH1 and TH2) and cytotoxic T cells(CD8þ, TC1 and TC2) either providing or receivingthe signals to co-ordinate a response (Kourilsky &Truffa-Bachi, 2001; Mosmann et al., 1986; Mosmannet al., 1997; Moser &Murphy, 2000) (Fig. 2). The initialstimulus for these T-cell responses originates withthe DCs when antigen presentation occurs (Kelleheret al., 1999; Knight et al., 1982; Rissoan et al., 1999;Kourilsky & Truffa-Bachi, 2001). The liberation ofeither type 1 and/or type 2 cytokines with T-cell stimul-ation initially expands the response (e.g. with IL-12 andIFN-g), then balances it as the opposite/regulating cyto-kines are expressed (e.g. IL-10 and IL-4, respectively)(Corinti et al., 2001; Ebner et al., 2001; Kourilsky &Truffa-Bachi, 2001; Schindler et al., 2001). During nor-mal responses, the expanded T-cell population thenretracts into a memory state as the infection is clearedand the initial stimulus disappears with removal of theDCs by apoptosis or NK and cytotoxic T-lymphocyte(CTL)-mediate cell lysis and reinstitution of the normalsteady-state (Shah et al., 1985; Knight et al., 1997;Rissoan et al., 1999; Bertho et al., 2000) (Fig. 1). The‘normal steady-state’ cytokine expression pattern inhumans is unknown. However, the regulatory cytokine,IL-10, has recently been implicated in enforcing balanceduring immune responses in that its expression isrequired to protect uninvolved tissue from normal
inflammatory reactions to pathogens (Fickenscheret al., 2002; Kourilsky & Truffa-Bachi, 2001; Mooreet al., 2001; Panoskaltsis et al., 2003).
Although cytokine expression acting at the DC–T-cell interface may bias towards either a type 1 or type 2immune response, the mechanism by which this polar-ization occurs is controversial. It has been suggestedthat the regulation of type 1 and type 2 responses maybe dependent on the particular DC subset that pre-sents antigen (de Saint-Vis et al., 1998; Pulendran et al.,1999; Rissoan et al., 1999; Zou et al., 2001). Alterna-tively, cytokine expression by different DC subsetsmay be dependent on the cytokine present in theimmediate environment (Hilkens et al., 1997; Satoet al., 1999; Vieira et al., 2000). Although initiallythought to produce primarily the type 1 cytokineIL-12, myeloid DCs may be influenced by IL-4 andIL-10 to stimulate a type 2 response (Liu et al., 1998;Sato et al., 1999). Plasmacytoid DCs cultivated withIL-3 and granulocyte–macrophage colony-stimulatingfactor (GM-CSF) and matured with CD40L haveconsistently been shown to produce IL-10 (Rissoanet al., 1999; Zou et al., 2001; Gilliet & Liu, 2002).This finding had led to the prevailing view that plas-macytoid DCs induce tolerance and that when this DCsubset presents antigen to T cells, a type 2 response iselicited (Dzionek et al., 2002; Pulendran et al., 1999;Rissoan et al., 1999). However, when immature plas-macytoid DCs are infected by virus, they are the pri-mary producers of the type 1 IFNs and evoke a type 1innate response to the viral pathogen (Cella et al., 1999;Siegal et al., 1999; Cella et al., 2000). Hence, bothmyeloid and plasmacytoid DCs are plastic in their cyto-kine repertoire, and this plasticity may depend on theenvironmental cues to which they are exposed (Fig. 2).
CLINICAL USE OF DCs
The development of methods by which to expand DCpopulations in vitro and in vivo from human mono-cytes and CD34þ precursors has enabled the study ofthese rare cells (Caux et al., 1992; Knight et al., 1986;Reid et al., 1992). These techniques have been furthermodified to suit the clinical cell separation and pre-paration laboratory so that the knowledge of DCbiology achieved in the basic research laboratorymight be used to develop treatments of human dis-ease (Gatti et al., 2000; Berger et al., 2002; Pullarkatet al., 2002; Tuyaerts et al., 2002).
The in vitro expansion of myeloid DCs may beachieved by the cultivation of DC precursors withcytokines conducive to DC growth (Caux et al.,1992; Reid et al., 1992; Szabolcs et al., 1995). Periph-eral blood monocytes may be enriched with magnetic
Immune modulation with DCs 85
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96

bead columns and sorting techniques or by plasticadherence and then placed in culture with GM-CSFand IL-4 to generate phenotypic and functional DCs.The DCs produced comprise up to 29% of the start-ing mononuclear cell population by 7–28 days ofculture (Luft et al., 1998; Wong et al., 2001; Bergeret al., 2002; Pullarkat et al., 2002; Tuyaerts et al.,2002; Buchler et al., 2003). Further in vitro matur-ation of these myeloid DCs may be achieved by theaddition of TNF-a, lipopolysaccharide, calciumionophore, monocyte-conditioned medium, PolyI:C, CD40L, CpG oligodeoxynucleotides or antigenfor the last 24–96 h of the culture (Gursel et al., 2002;Reddy et al., 1997; Koski et al., 1999; Lyakh et al.,2000; O’Sullivan & Thomas, 2002).
Both myeloid and plasmacytoid DCs may be gen-erated from CD34þ cells of the bone marrow, cordblood and fetal liver (Banchereau et al., 2000).Myeloid DC expansion from these precursor cellshas been accomplished with the use of the cytokinesGM-CSF, IL-4, stem cell factor (SCF) and TNF-a(Reid et al., 1992; Szabolcs et al., 1995; Young et al.,1995; Saraya & Reid, 1996). Alternative protocolsexpand the precursor cells first, with cytokines suchas fms-like tyrosine kinase ligand (FL), thrombopoietinand SCF; the cells are then directed into a DC lineageby adding the cytokines GM-CSF, IL-6, IL-4 andTNF-a to the culture (Arrighi et al., 1999; Bergeret al., 2002; Liu et al., 2002). Such ‘two-step’ culturetechniques may expand cells up to 250-fold and16,600-fold of the initial number of CD34þ cellsafter 4 and 8 weeks of culture (Arrighi et al., 1999).The expansion of plasmacytoid DCs in vitro has notbeen as successful as the expansion of myeloid DCs,and the use of the cytokines GM-CSF and IL-3 arerequired simply for survival of the cells ex vivo(Kohrgruber et al., 1999; Siegal et al., 1999; Bjorck,2002). However, the use of FL alone in DC culturesof 10 days can generate plasmacytoid DCs andmyeloid DCs as well as maintain a component ofcells with a phenotype similar to that of the initialprecursor population (Bjorck, 2002; Curti et al.,2001). Most of these methods for the in vitro genera-tion of DCs have not included evaluation of theimpact of the cytokines used for their expansion onthe cytokine or chemokine expression pattern of theDCs that have been generated.
Cytokines approved for clinical use, or those in clin-ical trials, have been used for the in vivo expansion ofmyeloid and plasmacytoid DCs for potential therapeu-tic use in humans (Choi et al., 1998; Avigan et al., 1999;Pulendran et al., 2000). The use of GM-CSF canexpand myeloid DCs in healthy human volunteers(Avigan et al., 2001), and in individuals with tumours
entered onto trials of peptide immune therapy, sub-cutaneous or intradermal GM-CSF has been used torecruit immature DCs to the site of peptide injection inorder to enhance the potency of the vaccine (Bendandiet al., 1999; McNeel et al., 1999; Timmerman & Levy,2000). Granulocyte colony-stimulating factor (G-CSF)expands plasmacytoid DCs in the peripheral blood(Arpinati et al., 2000; Klangsinsirikul & Russell, 2002;Vuckovic et al., 2003) and in addition, may increaseIL-10 production in this subset (Arpinati et al., 2000;Pulendran et al., 2000; Volpi et al., 2001). Some invest-igators have proposed that this type 2 cytokine biasmight account for the decreased incidence of acutegraft vs. host disease (GvHD) in patients receivingtransplants of donor cells mobilized with G-CSF(Arpinati et al., 2000; Klangsinsirikul & Russell,2002). FL has also been used in human volunteersand expands both subsets of DCs (Maraskovsky et al.,2000; Pulendran et al., 2000). However, the ability ofFL preferentially to expand the myeloid DCs (Maras-kovsky et al., 2000) or the plasmacytoid subset (Pulen-dran et al., 2000) may depend on the definition of DCsby surface immunophenotype and on the FL dose andschedule. In vivo expansion of DCs in humans has beenpursued in the hopes of using these cells for therapeuticpurposes, such as in tolerance induction in transplanta-tion and in the immune therapy of cancer. Use of DCsin solid organ and stem cell transplantation will not bediscussed in this review.
DC IMMUNE THERAPY FORMALIGNANCY
Tumour cells may express ‘fetal antigens’, or proteinsthat are expressed and signal early in development(Brickman & Burdon, 2002). In some cases, viralantigens or other molecules entirely specific to indi-vidual tumours may be expressed (Gilboa, 1999;Offringa et al., 2000). The therapy of murine cancerwith DCs loaded with these tumour-associated anti-gens (TAAs) suggested that DCs could break the‘tolerance’ imposed by the tumour environmentwhich allowed the tumour to grow and that humancancer might also be amenable to DC therapies(Knight et al., 1985). This observation and theimproved prognosis of patients who had a highernumber of DCs in their tumours compared withthose who did not (Troy & Hart, 1997; Iwamotoet al., 2003) encouraged clinical implementation ofDC-based protocols for the therapy of human can-cers (Fong & Engleman, 2000; Gunzer et al., 2001;Reid, 2001). These protocols involve the generationof large number of DCs from the peripheral blood
86 N. Panoskaltsis et al.
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96
monocytes or CD34þ-derived bone marrow precur-sor cells of the patient (Hsu et al., 1996; Nestle et al.,1998; Brossart et al., 2000; Schuler-Thurner et al.,2002). The DCs are then pulsed with TAAs or necro-tic tumour cells prior to their administration back tothe patient via an intravenous, subcutaneous, intra-dermal or intralymphatic route (Fong et al., 2001b;Hsu et al., 1996; Fong & Engleman, 2000; Nestleet al., 2001). Alternatively, the DCs may be used toexpand tumour-specific T cells in vitro so that the Tcells may then be used in adoptive transfer protocols(Brossart et al., 1999; Nieda et al., 1998; Yee et al.,2002). The best results for DCs or T-cell-basedimmune therapy for malignancy in animal modelsare observed when the cells are administered prophy-lactically as a true vaccine or when the tumour is in aminimal residual disease (MRD) state (Knight et al.,1985; Fong & Engleman, 2000; Reid, 2001). Interest-ingly, the initial murine study that reported the use ofDCs in the immune therapy of cancer indicated thatthe best therapeutic result for established disease wasnot with the use of tumour-pulsed DCs, but ratherwith DCs that did not bear tumour antigens (Knightet al., 1985). Effectiveness of the DC therapy in thismodel was indirectly correlated with the dose oftumour antigen to which the DCs were exposedprior to administration. Hence, with increasingtumour antigen exposure prior to administration,the anti-tumour potency of the DC therapydecreased. However, DCs exposed to tumour antigenwere most effective when administered on the sameday as the tumour cells, mimicking a state of MRD.This observation suggested that an antigen gradientmay be required for the recognition of nonself anti-gens or the reversal of tolerance and that this gradi-ent may operate between two DCs that transfer theantigen in question (Knight & Bedford, 2001; Klein-dienst & Brocker, 2003).
APPLICATION OF DCs IN CLINICAL TRIALS
DCs from patients with cancer, like those from healthyvolunteers, may be generated by in vitro culture ofperipheral blood monocytes or CD34þ-derived bonemarrow precursor cells (Fong & Engleman, 2000;Reid, 2001) and by the use of cytokines for their invivo expansion (Pulendran et al., 2000; Curti et al.,2001; Fong et al., 2001c; Disis et al., 2002). Althoughinhibitory factors in these patients may alter the DCsthat are generated in vivo so that they do not stimulateeffective anti-tumour responses, DCs derived from pre-cursors in vitro are fully functional (Gabrilovich et al.,1996a; Gabrilovich et al., 1996b; Pulendran et al.,
2000). Monocytes are easily accessible from peripheralblood and hence may be preferable as precursors for invitro generation of DCs for use in human trials (Fong& Engleman, 2000; Nestle et al., 2001; Reid, 2001).However, CD34þ-derived cells may be better due toenhanced anti-tumour effects and more type 1 cytokinebias (Huang et al., 1994; Mortarini et al., 1997;Ferlazzo et al., 1999; Fujii et al., 1999). Because mostmonocyte-derived DCs are exposed to GM-CSF andIL-4 only and those derived from bone marrow pre-cursors have been exposed to other cytokines as wellincluding IL-6, TNF-a, FL and IFN-g, the effects ofdifferent cytokines in the environment of the DCs dur-ing maturation may impact their cytokine bias (Satoet al., 1999; Vieira et al., 2000). These effects had notbeen studied, and DCs generated in vitro with cyto-kines, such as IL-4, that may bias towards a type 2immune response have been used in clinical trials ofDC immune therapy for cancer (Sato et al., 1999; Tarte& Klein, 1999; Gunzer et al., 2001).
The first studies of human DCs for therapy ofcancer were in patients with lymphoma (Hsu et al.,1996) and malignant melanoma (Mukherji et al.,1995; Nestle et al., 1998; Dallal & Lotze, 2000).These DCs were isolated directly from leucapheresisproducts or generated from peripheral blood mono-cytes using GM-CSF and IL-4. Since then, there havebeen many trials using DCs prepared with pulsingusing known tumour-associated peptide or necrotictumour cells, fusion of DCs with tumour cells or theuse of tumour-specific idiotype with which to pulseDCs either in vitro or in vivo in the form of a peptidevaccine (Fong et al., 2001c; Reid, 2001). Often the‘vaccine’ is administered with an adjuvant, such asincomplete Freund’s adjuvant (Rosenberg et al.,1998), GM-CSF (McNeel et al., 1999) or with anotherpeptide for which in vitro responses can be studiedsuch as keyhole limpet haemocyanin (Hsu et al.,1996; Hsu et al., 1997) that, incidentally, also hasadjuvant properties (Timmerman & Levy, 2000). Vari-able responses to these DC therapies have beenobserved (Fong & Engleman, 2000), none of whichcorrelate with in vitro testing for the efficacy of thevaccine (Rosenberg et al., 1998; McNeel et al., 1999;Clay et al., 2001; Whiteside et al., 2003). These in vitrocorrelates have included the delayed type hypersensi-tivity reaction to antigen, CTL responses, ELISPOT,enzyme-linked immunosorbent assay (ELISA), flowcytometry with and without intracellular cytokinedetermination and tetramer staining (Clay et al.,2001; Knutson et al., 2001; Whiteside et al., 2003).The best determinant of response to DC therapy isthe clinical response itself, as enhanced anti-tumourresponses in vitro have been observed in patients with
Immune modulation with DCs 87
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96

progressive disease (Hsu et al., 1997; Nestle et al.,1998; Rosenberg et al., 1998; Fong et al., 2001a;Timmerman et al., 2002). One report that showedpromising results using DC therapy in human malig-nancy has been retracted recently (Kugler et al., 2000).
A special case in DC immune therapies is that ofacute myeloid leukaemia (AML). In AML, theleukaemic blasts are the malignant counterpart ofhaemopoietic progenitors arrested at an early stageof maturation. DCs may be generated in vitro fromprimary AML blasts of different subtypes (Robinsonet al., 1998; Choudhury et al., 1999; Harrison et al.,2001; Panoskaltsis et al., 2002). Thus, under specificcytokine and growth conditions known to enhancethe generation of DCs, these leukaemic cells up-regulate T-cell costimulatory proteins on their surfaceand stimulate primary lymphocyte responses (Boyeret al., 2000; Charbonnier et al., 1999; Choudhuryet al., 1999; Harrison et al., 2001; Panoskaltsis et al.,2002). These AML-derived DCs (AML-DCs) arisefrom the leukaemic clone, because they continue toharbour the cytogenetic abnormality characteristic ofthe clonal population. AML-DCs require furtherstudy prior to their effective use in immune therapy.Our own observations suggest that AML-DCs main-tain an innate capacity to produce IL-4 in vitro,despite the cytokines to which they are exposed dur-ing maturation (Panoskaltsis, Reid and Knight,manuscript in preparation). This type 2 cytokinebias may be undesirable for the use of these cells inthe immune therapy of patients with AML. However,the haemopoietic origin of the cells and the possibil-ity that they may harbour leukaemia-associated anti-gens specific for the tumour suggests that AML-DCsmight be harnessed for leukaemia-specific andpatient-specific immune modulation.
FINAL CONSIDERATIONS
Although we have learned much about DCs sincetheir discovery 30 years ago, there remain more ques-tions than answers about whether these cells shouldbe used therapeutically and, if so, how best to usethem and in whom. However, the ineffectiveness ofDC therapy at such an early stage in their careershould not discourage the use of these cells in thefuture when more rational implementation might beachieved. In order to fulfil this potential, there areseveral points to consider. First, prior to the admin-istration of in vitro modified DCs to patients, itshould be determined whether cells with the potentialto respond to DCs and the DCs themselves arealready present. Hence, standardized techniques areneeded to characterize the number, type, distribution
and function of these populations in situ. These fac-tors will be altered by chemotherapeutic regimenscurrently used for cancer treatment and need to beconsidered when using DCs. DCs may be most effect-ive in the host with MRD and a functional immunesystem. Second, any antigen that is already widelypresented in vivo and inefficient in providing protect-ive immunity may be ineffective; new antigens notwidely distributed or tolerogenic need to be identi-fied. Third, in vitro-generated DCs should express thechemokines, chemokine receptors and adhesion pro-teins necessary to encourage the migration of thesecells to the appropriate site, e.g. to the lymph nodefor antigen presentation, and that this site and routeof administration is tailored to the particular clinicalneed. Fourth, cytokine polarization of DCs needs tobe appropriate for the type of response required.Hence, in vitro culture techniques need to be adaptedto provide DCs with not only a specific surfaceimmunophenotype but also with a particular cyto-kine repertoire. Fifth, the possibility should be con-sidered that DCs may be permissive of, or evenpromote, tumourogenesis, and the use of these cellsin tumour therapy may have an effect quite oppositeto that which was initially intended (Knight et al.,1985; Almand et al., 2001). With considerations suchas these in mind, instead of ‘immune therapy’ withDCs, we should perhaps consider in vivo or in vitro‘immune modulation’ with DCs. DC subsets areunique and their function is partially influenced bytheir immediate microenvironment as well as by thecells with which they are able to interact; the use ofDCs to modulate the function of these other cells invivo will rationalize their therapeutic potential.
ACKNOWLEDGMENTS
This work was supported by the Medical ResearchCouncil, UK and the Leukaemia Research Fund.
REFERENCES
Acuto, O. & Cantrell, D. (2000) T cell activation and the
cytoskeleton. Annual Review of Immunology, 18, 165–184.
Akira, S., Takeda, K. & Kaisho, T. (2001) Toll-like recep-
tors: critical proteins linking innate and acquired immun-
ity. Nature Immunology, 2, 675–680.
Almand, B., Clark, J.I., Nikitina, E., van Beynen, J.,
English, N.R., Knight, S.C., Carbone, D.P. & Gabrilovich,
D.I. (2001) Increased production of immature myeloid cells in
cancer patients: amechanismof immunosuppression in cancer.
Jounal of Immunology, 166, 678–689.
Arpinati, M., Green, C.L., Heimfeld, S., Heuser, J.E. &
Anasetti, C. (2000) Granulocyte-colony stimulating
88 N. Panoskaltsis et al.
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96

factor mobilizes T helper 2-inducing dendritic cells.
Blood, 95, 2484–2490.
Arrighi, J.-F., Hauser, C., Chapuis, B., Zubler, R.H. &
Kindler, V. (1999) Long-term culture of human CD34þprogenitors with flt3-ligand, thrombopoietin, and stem
cell factor induces extensive amplification of a CD34-
CD14– and a CD34-CD14þ dendritic cell precursor.
Blood, 93, 2244–2252.
Avigan, D., Pirofski, L.-A. & Lazarus, H.M. (2001) Vaccina-
tion against infectious disease following hematopoietic stem
cell transplantation. Biology of Blood and Marrow Trans-
plantation, 7, 171–183.
Avigan, D., Wu, Z., Gong, J., Joyce, R., Levine, J., Elias, A.,
Richardson, P., Milano, J., Kennedy, L., Anderson, K. &
Kufe, D. (1999) Selective in vivo mobilization with
granulocyte macrophage colony-stimulating factor (GM-
CSF)/granulocyte-CSF as compared to G-CSF alone of
dendritic cell progenitors from perpheral blood progenitor
cells in patients with advanced breast cancer undergoing
autologous transplantation. Clinical Cancer Research, 5,
2735–2741.
Balfour, B., O’Brien, J.A., Perera, M., Clarke, J.,
Sumerska, T. & Knight, S.C. (1982) The effect of veiled
cells on lymphocyte function. Advances in Experimental
Medicine and Biology, 149, 447–454.
Banchereau, J., Briere, F., Caux, C., Davoust, J., Lebecque, S.,
Liu, Y.-J., Pulendran, B. & Palucka, K. (2000) Immuno-
biology of dendritic cells.Annual Review of Immunology, 18,
767–811.
Banchereau, J. & Steinman, R.M. (1998) Dendritic cells
and the control of immunity. Nature, 392, 245–252.
Barrat, F.J., Cua, D.J., Boonstra, A., Richards, D.F.,
Crain, C., Savelkoul, H.F., de Waal-Malefyt, R.,
Coffman, R.L., Hawrylowicz, C.M. & O’Garra, A.
(2002) In vitro generation of interleukin 10-producing
regulatory CD4þ T cells is induced by immunosuppres-
sive drugs and inhibited by T helper type 1 (Th1) - and
Th2-inducing cytokines. The Journal of Experimental
Medicine, 195, 603–616.
Beg, A.A. (2002) Endogenous ligands of Toll-like receptors:
implications for regulating inflammatory and immune
responses. Trends in Immunology, 23, 509–512.
Bell, D., Chomarat, P., Broyles, D., Giorge, N., Harb, G.M.,
Lebecque, S., Valladeau, J., Davoust, J., Palucka, K.A. &
Banchereau, J. (1999) In breast carcinoma tissue,
immature dendritic cells reside within the tumor,
whereas mature dendritic cells are located in peritumoral
areas. The Journal of Experimental Medicine, 190,
1417–1425.
Bendandi, M., Gocke, C.D., Kobrin, C.B., Benko, F.A.,
Sternas, L.A., Pennington, R., Watson, T.M.,
Reynolds, C.W., Gause, B.L., Duffey, P.L., Jaffe, E.S.,
Creekmore, S.P., Longo, D.L. & Kwak, L.W. (1999)
Complete molecular remissions induced by patient-specific
vaccination plus granulocyte-monocyte colony-stimulating
factor against lymphoma. Nature Medicine, 5, 1171–1177.
Bennett, S.R.M., Carbone, F.R., Karamalis, F., Flavell, R.A.,
Miller, J.F.A.P. & Heath, W.R. (1998) Help for cytotoxic-
T-cell responses is mediated by CD40 signalling. Nature,
393, 478–480.
Berger, T.G., Feuerstein, B., Strasser, E., Hirsch, U.,
Schreiner, D., Schuler, G. & Schuler-Thurner, B. (2002)
Large-scale generation of mature monocyte-derived den-
dritic cells for clinical application in cell factories. Jour-
nal of Immunological Methods, 268, 131–140.
Bertho, N., Drenou, B., Laupeze, B., Le Berre, C., Amiot, L.,
Grosset, J.-M., Fardel, O., Charron, D., Mooney, N. &
Fauchet, R. (2000) HLA-DR-mediated apoptosis suscept-
ibility discriminates differentiation stages of dendritic/
monocytic APC. Journal of Immunology, 164, 2379–2385.
Bianca, B., Ligthart, S.J.W.C., Schotte, R. & Spits, H.
(2002) Developmental origin of pre-DC2. Human
Immunology, 63, 1072–1080.
Bjorck, P. (2002) The multifaceted murine plasmacytoid
dendritic cell. Human Immunology, 63, 1094–1102.
Boyer, M.W., Waller, E.K., Bray, R.A., Unangst, T.,
Johnson, T.S., Phillips, C., Jurickova, I., Winton, E.F.
& Yeager, A.M. (2000) Cytokine upregulation of the
antigen presenting function of acute myeloid leukemia
cells. Leukemia, 14, 412–418.
Brickman, J.M. & Burdon, T.G. (2002) Pluripotency and
tumorigenicity. Nature Genetics, 32, 557–558.
Briere, F., Bendriss-Vermare, N., Delale, T., Burg, S.,
Corbet, C., Rissoan, M.-C., Chaperot, L., Plumas, J.,
Jacob, M.-C., Trinchieri, G. & Bates, E.E.M. (2002)
Origin and filiation of human plasmacytoid dendritic
cells. Human Immunology, 63, 1081–1093.
Brossart, P., Spahlinger, B., Grunebach, F., Stuhler, G.,
Reichardt, V.L., Kanz, L. & Brugger, W. (1999)
Induction of minor histocompatibility antigen HA-1-
specific cytotoxic T cells for the treatment of leukemia
after allogeneic stem cell transplantation. Blood, 94,
4374–4376.
Brossart, P.,Wirths, S., Stuhler,G.,Reichardt, V.L.,Kanz, L.&
Brugger, W. (2000) Induction of cytotoxic T-lymphocyte
responses in vivo after vaccinations with peptide-pulsed den-
dritic cells. Blood, 96, 3102–3108.
Buchler, T., Hajek, R., Bourkova, L., Kovarova, L.,
Musilova, R., Bulikova, A., Doubek, M., Svobodnik, A.,
Mareschova, I., Vanova, P., Tuzova, E., Vidlakova, P.,
Vorlicek, J. & Penka, M. (2003) Generation of antigen-
loaded dendritic cells in a serum-free medium using differ-
ent cytokine combinations. Vaccine, 21, 877–882.
Bullock, T.N.J., Mullins, D.W. & Engelhard, V.H. (2003)
Antigen density presented by dendritic cells in vivo dif-
ferentially affects the number and avidity of primary,
memory, and recall CD8þ T cells. Journal of Immunol-
ogy, 170, 1822–1829.
Caux, C., Dezutter-Dambuyant, C., Schmitt, D. &
Banchereau, J. (1992) GM-CSF and TNF-a cooperate
in the generation of dendritic Langerhans cells. Nature,
360, 258–261.
Immune modulation with DCs 89
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96
Cella,M., Engering, A., Pinet, V., Pieters, J. &Lanzavecchia, A.
(1997) Inflammatory stimuli induce accumulation of MHC
class II complexes on dendritic cells. Nature, 388, 782–786.
Cella, M., Facchetti, F., Lanzavecchia, A. & Colonna, M.
(2000) Plasmacytoid dendritic cells activated by influenza
virus and CD40L drive a potent Th1 polarization. Nature
Immunology, 1, 305–310.
Cella, M., Jarrossay, D., Facchetti, F., Alebardi, O.,
Hakajima, H., Lanzavecchia, A. & Colonna, M. (1999)
Plasmacytoid monocytes migrate to inflamed lymph
nodes and produce large amounts of type I interferon.
Nature Medicine, 5, 919–923.
Charbonnier, A., Gaugler, B., Sainty, D., Lafage-
Pochitaloff, M. & Olive, D. (1999) Human acute myelo-
blastic leukemia cells differentiate in vitro into mature
dendritic cells and induce the differentiation of cytotoxic
T cells against autologous leukemias. European Journal
of Immunology, 29, 2567–2578.
Choi, D., Perrin, M., Hoffmann, S., Chang, A.E.,
Ratanatharathorn, V., Uberti, J., McDonagh, K.T. &
Mule, J.J. (1998) Dendritic cell-based vaccines in the setting
of peripheral blood stem cell transplantation: CD34þ cell-
depleted mobilized peripheral blood can serve as a source of
potent dendritic cells.Clinical Cancer Research, 4, 2709–2716.
Choudhury, A., Liang, J.C., Thomas, E.K., Flores-Romo, L.,
Xie, Q.S., Agusala, K., Sutaria, S., Sinha, I., Champlin, R.E.
& Claxton, D.F. (1999) Dendritic cells derived in vitro from
acute myelogenous leukemia cells stimulate autologous,
antileukemic T-cell responses. Blood, 93, 780–786.
Chow, A., Toomre, D., Garrett, W. & Mellman, I. (2002)
Dendritic cell maturation triggers retrograde MHC class
II transport from lysosomes to the plasma membrane.
Nature, 418, 988–994.
Clay, T.M., Hobeika, A.C., Mosca, P.J., Lyerly, H.K. &
Morse, M.A. (2001) Assays for monitoring cellular
immune responses to active immunotherapy of cancer.
Clinical Cancer Research, 7, 1127–1135.
Colonna, M., Krug, A. & Cella, M. (2002) Interferon-
producing cells: on the front line in immune responses
against pathogens. Current Opinion in Immunology, 14,
373–379.
Comeau, M.R., Van der Vuurst de Vries, A.-R.,
Maliszewdki, C.R. & Galibert, L. (2002) CD123bright
plasmacytoid predendritic cells: progenitors under-
going cell fate conversion? Journal of Immunology,
169, 75–83.
Corinti, S., Albanesi, C., La Sala, A., Pastore, S. &
Girolomoni, G. (2001) Regulatory activity of autocrine
IL-10 on dendritic cell functions. Journal of Immunology,
166, 4312–4318.
Crow, M.K. & Kunkel, H.G. (1982) Human dendritic cells:
major stimulators of the autologous and allogeneic
mixed leukocyte reactions. Clinical and Experimental
Immunology, 49, 338–346.
Curti, A., Fogli, M., Ratta, M., Tura, S. & Lemoli, R.M.
(2001) Stem cell factor and FLT3-ligand are strictly
required to sustain the long-term expansion of primitive
CD34þDR– dendritic cell precursors. Journal of Immu-
nology, 166, 848–854.
Cyster, J.G. (1999) Chemokines and cell migration in sec-
ondary lymphoid organs. Science, 286, 2098–2102.
Dallal, R.M. & Lotze, M.T. (2000) The dendritic cell and
human cancer vaccines. Current Opinion in Immunology,
12, 583–588.
de Saint-Vis, B., Fugier-Vivier, I., Massacrier, C., Gaillard, C.,
Vanbervliet, B., Ait-Yahia, S., Banchereau, J., Liu, Y.-J.,
Lebecque, S. & Caux, C. (1998) The cytokine profile
expressed by human dendritic cells is dependent on cell
subtype and mode of activation. Journal of Immunology,
160, 1666–1676.
Dieu, M.-C., Vanbervliet, B., Vicari, A., Bridon, J.-M.,
Oldham, E., Ait-Yahia, S., Briere, F., Zlotnik, A.,
Levecque, S. & Caux, C. (1998) Selective recruitment of
immature and mature dendritic cells by distinct chemokines
expressed in different anatomic sites. The Journal of Experi-
mental Medicine, 188, 373–386.
Disis, M.L., Rinn, K., Knutson, K.L., Davis, D., Caron, D.,
de la Rosa, C. & Schiffman, K. (2002) Flt3 ligand as a
vaccine adjuvant in association with HER-2/neu peptide-
based vaccines in patients with HER-2/neu-overexpressing
cancers. Blood, 99, 2845–2850.
Dzionek, A., Fuchs, A., Schmidt, P., Cremer, S., Zysk, M.,
Miltenyi, S., Buck, D.W. & Schmitz, J. (2000) BDCA-2,
BDCA-3, and BDCA-4: thre markers for distinct subsets
of dendritic cells in human peripheral blood. Journal of
Immunology, 165, 6037–6046.
Dzionek, A., Inagaki, Y., Okawa, K., Nagafune, J., Rock, J.,
Sohma, Y., Winkels, G., Zysk, M., Yamaguchi, Y. &
Schmitz, J. (2002) Plasmacytoid dendritic cells: from
specific surface markers to specific cellular functions.
Human Immunology, 63, 1133–1148.
Ebner, S., Ratzinger, G., Krosbacher, B., Schmuth, M.,
Weiss, A., Reider, D., Kroczek, R.A., Herold, M.,
Heufler, C., Fritsch, P. & Romani, N. (2001) Production
of IL-12 by human monocyte-derived dendritic cells is
optimal when the stimulus is given at the onset of
maturation, and is further enhanced by IL-4. Journal of
Immunology, 166, 633–641.
Ferlazzo, G., Wesa, A., Wei, W.-Z. & Galy, A. (1999)
Dendritc cells generated either from CD34þ progenitor
cells or from monocytes differ in their ability to activate
antigen-specific CD8þ T cells. Journal of Immunology,
163, 3597–3604.
Fickenscher, H., Hor, S., Kupers, H., Knappe, A.,
Wittmann, S. & Sticht, H. (2002) The interleukin-10
family of cytokines. Trends in Immunology, 23, 89–96.
Fong, L., Brockstedt, D., Benike, C., Breen, J.K., Strang, G.,
Ruegg, C.L. & Engleman, E.G. (2001a) Dendritic cell-based
xenoantigen vaccination for prostate cancer immuno-
therapy. Journal of Immunology, 167, 7150–7156.
Fong, L., Brockstedt, D., Benike, C.,Wu, L. & Engleman, E.G.
(2001b) Dendritic cells injected via different routes induce
90 N. Panoskaltsis et al.
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96
immunity in cancer patients. Journal of Immunology, 166,
4254–4259.
Fong, L. & Engleman, E.G. (2000) Dendritic cells in
cancer immunotherapy. Annual Review of Immunology,
18, 245–273.
Fong,L.,Hou,Y.,Rivas,A.,Benike,C.,Yuen,A.,Fisher,G.A.,
Davis, M.M. & Engleman, E.G. (2001c) Altered peptide
ligand vaccination with Flt3 ligand expanded dendritic cells
for tumor immunotherapy. Proceedings of the National
Academy of Sciences of the United States of America, 98,
8809–8814.
Fujii, S.-i., Fujimoto, K., Shimizu, K., Ezaki, T., Kawano, F.,
Takatsuki, K., Kawakita, M. & Matsuno, K. (1999) Pre-
sentation of tumor antigens by phagocytic dendritic cell
clusters generated from human CD34þ hematopoietic
progenitor cells: induction of autologous cytotoxic T
lymphocytes against leukemic cells in acute myelogenous
leukemia patients. Cancer Research, 59, 2150–2158.
Gabrilovich, D.I., Ciernik, I.F. & Carbone, D.P. (1996a)
Dendritic cells in antitumor immune responses. I. Defec-
tive antigen presentation in tumor-bearing hosts. Cellular
Immunology, 170, 101–110.
Gabrilovich, D.I., Nadaf, S., Corak, J., Berzofsky, J.A. &
Carbone, D.P. (1996b) Dendritic cells in antitumor
immune responses. II. Dendritic cells grown from bone
marrow precursors, but not mature DC from tumor-
bearing mice, are effective antigen carriers in the
therapy of established tumors. Cellular Immunology, 170,
111–119.
Gabrilovich, D.I., Woods, G.M., Patterson, S., Harvey, J.J.
&Knight, S.C. (1994) Retrovirus-induces immunosuppres-
sion via blocking of dendritic cell migration and
down-regulation of adhesion molecules. Immunology, 82,
82–87.
Gatti, E., Velleca, M.A., Biedermann, B.C., Ma, W.,
Unternaehrer, J., Ebersold, M.W., Medzhitov, R.,
Pober, J.S. & Mellman, I. (2000) Large-scale culture
and selective maturation of human langerhans cells from
granulocute colony-stimulating factor-mobilized C34þprogenitors. Journal of Immunology, 164, 3600–3607.
Geissmann,F.,Dieu-Nosjean,M.C.,Dezutter,C.,Valladeau, J.,
Kayal, S., Leborgne, M., Brousse, N., Saeland, S. &
Davoust, J. (2002) Accumulation of immature langerhans
cells in human lymph nodes draining chronically inflamed
skin. The Journal of Experimental Medicine, 196, 417–430.
Gilboa, E. (1999) The makings of a tumor rejection antigen.
Immunity, 11, 263–270.
Gilliet, M. & Liu, Y. (2002) Human plasmacytoid-derived
dendritic cells and the induction of T-regulatory cells.
Human Immunology, 63, 1149–1155.
Grakoui, A., Bromley, S.K., Sumen, C., Davis, M.M.,
Shaw, A.S., Allen, P.M. & Dustin, M.L. (1999) The
immunological synapse: a molecular machine controlling
T cell activation. Science, 285, 221–227.
Groux, H., O’Garra, A., Bigler, M., Rouleau, M.,
Antonenko, S., de Vries, J.E. & Roncarolo, M.G.
(1997) A CD4þ T-cell subset inhibits antigen-specific -
cell responses and prevents colitis. Nature, 389, 737–742.
Gunzer, M., Janich, S., Varga, G. & Grabbe, S. (2001) Den-
dritic cells and tumor immunity. Seminars in Immunology,
13, 291–302.
Gursel, M., Verthelyi, D. & Klinman, D.M. (2002) CpG
oligodeoxynucleotides induce human monocytes to
mature into functional dendritic cells. European Journal
of Immunology, 32, 2617–2622.
Harrison, B.D., Adams, J.A., Brigs, M., Brereton, M.L. &
Liu Yin, J.A. (2001) Stimulation of autologous prolifera-
tive and cytotoxic T-cell responses by ‘leukemic dendritic
cells’ derived from blast cells in acute myeloid leukemia.
Blood, 97, 2764–2771.
Hart, D.N.J. (1997) Dendritic cells: unique leukocyte
populations which control the primary immune response.
Blood, 90, 3245–3287.
Heath, W.R. & Carbone, F.R. (2001) Cross-presentation,
dendritic cells, tolerance and immunity. Annual Review of
Immunology, 19, 47–64.
Heyworth, C.M., Testa, N.G., Buckle, A.-M. &Whetton, A.D.
(1997) Growth factors and the regulation of haemopoietic
stem cells. In: Stem Cells (ed. Potten, C.S.). Academic
Press Ltd, London.
Hilkens, C.M.U., Kalinski, P., de Boer, M. &
Kapsenberg, M.L. (1997) Human dendritic cells require
exogenous interleukin-12-inducing factors to direct the
development of naive T-helper cells toward the Th1 phe-
notype. Blood, 90, 1920–1926.
Hiltbold, E.M., Vlad, A.M., Ciborowski, P., Watkins, S.C.
& Finn, O.J. (2000) The mechanism of unresponsiveness
to circulating tumor antigen MUC1 is a block in intra-
cellular sorting and processing by dendritic cells. Journal
of Immunology, 165, 3730–3741.
Ho, C.S.K., Lopez, J.A., Vuckovic, S., Pyke, C.M.,
Hosckey, R.L. & Hart, D.N.J. (2001) Surgical and phy-
sical stress increases circulating blood dendritic cell
counts independently of monocyte counts. Blood, 98,
140–145.
Hsu, F.J., Benike, C., Fagnoni, F., Liles, T.M., Czerwinski, D.,
Taidi, B., Engleman, E.G. & Levy, R. (1996) Vaccination of
patients with B-cell lymphoma using autologous antigen-
pulsed dendritic cells. Nature Medicine, 2, 52–58.
Hsu, F.J., Caspar, C.B., Czerwinski, D., Kwak, L.W.,
Liles, T.M., Syrengelas, A., Taidi-Laskowski, B. &
Levy, R. (1997) Tumor-specific idiotype vaccines in the
treatment of patients with B-cell lymphoma – long-term
results of clinical trial. Blood, 89, 3129–3135.
Huang, A.Y.C., Bruce, A.T., Pardoll, D. & Levitsky, H.I.
(1996) Does B7–1 expression confer antigen-presenting
cell capacity to tumors in vivo? The Journal of Experi-
mental Medicine, 183, 769–776.
Huang, A.Y.C., Golumbek, P., Ahmadzadeh, M., Jaffee, E.
& Pardoll, D. (1994) Role of bone marrow-derived cells in
presenting MHC class I-restricted tumor antigens.
Science, 264, 961–965.
Immune modulation with DCs 91
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96
Huang, Q., Liu, D., Majewski, P., Schulte, L.C.,
Korn, J.M., Young, R.A., Lander, E.S. & Hacohen, N.
(2001) The plasticity of dendritic cell responses to
pathogens and their components. Science, 294, 870–875.
Iwamoto, M., Shinohara, H., Miyamoto, A., Okuzawa, M.,
Mabuchi, H., Nohara, T., Gon, G., Toyoda, M. &
Tanigawa, N. (2003) Prognostic value of tumor-infiltrating
dendritic cells expressing CD83 in human breast carcino-
mas. International Journal of Cancer, 104, 92–97.
Jung, S., Unutmaz, D., Wong, P., Sano, G.-I., De los
Santos, K., Saprwasser, T., Wu, S., Vuthoori, S., Ko, K.,
Zavala, F., Pamer, E.G., Littman, D.R. & Lang, R.A.
(2002) In vivo depletion of CD11cþ dendritic cells
abrogates priming of CD8þ T cells by exogenous cell-
associated antigens. Immunity, 17, 211–220.
Kelleher, P. & Knight, S.C. (1998) IL-12 increases CD80
expression and the stimulatory capacity of bone marrow-
derived dendritic cells. International Immunology, 10,
749–755.
Kelleher, P., Maroof, A. & Knight, S.C. (1999) Retrovirally
induced switch from production of IL-12 to IL-4 in
dendritic cells. European Journal of Immunology, 29,
2309–2318.
Klangsinsirikul, P. & Russell, N.H. (2002) Peripheral blood
stem cell harvests from G-CSF-stimulated donors con-
tain a skewed Th2 CD4 phenotype and a predominance
of type 2 dendritic cells. Experimental Hematology, 30,
495–501.
Kleindienst, P. & Brocker, T. (2003) Endogenous dendritic
cells are required for amplification of T cell responses
induced by dendritic cell vaccines in vivo. Journal of
Immunology, 170, 2817–2823.
Knight, S.C. (1984) Veiled cells – ‘dendritic cells’ of the
peripheral lymph. Immunobiology, 168, 349–361.
Knight, S.C., Askonas, B.A. & Macatonia, S.E. (1997)
Dendritic cells as targets for cytotoxic T lymphocytes.
Advances in Experimental Medicine and Biology, 417,
389–394.
Knight, S.C., Balfour, B.M., O’Brien, J., Buttifant, L.,
Sumerska, T. & Clarke, J. (1982) Role of veiled cells in
lymphocyte activation. European Journal of Immunology,
12, 1057–1060.
Knight, S.C. & Bedford, P.A. (2001) Dendritic cell/
dendritic cell interaction. In: Dendritic Cells: Biology and
Clinical Applications (Thompson, A.W. & Lotze, M.T.,
eds.), pp. 289–298. Academic Press, London.
Knight, S.C., Burke, F. & Bedford, P.A. (2002) Dendritic
cells, antigen distribution and the initiation of primary
immune responses to self and non-self antigens. Seminars
in Cancer Biology, 12, 301–308.
Knight, S.C., Farrant, J., Bryant, A., Edwards, A.J.,
Burman, S., Lever, A., Clarke, J. & Webster, A.D.B.
(1986) Non-adherent, low-density cells from human
peripheral blood contain dendritic cells and mono-
cytes, both with veiled morphology. Immunology, 57,
595–603.
Knight, S.C., Hunt, R., Dore, C. & Medawar, P.B. (1985)
Influence of dendritic cells on tumor growth. Proceedings
of the National Academy of Sciences of the United States
of America, 82, 4495–4497.
Knight, S.C., Mertin, J., Stackpoole, A. & Clark, J. (1983)
Induction of immune responses in vivo with small num-
bers of veiled (dendritic) cells. Proceedings of the National
Academy of Sciences of the United States of America, 80,
6032–6035.
Knutson, K.L., Schiffman, K. & Disis, M.L. (2001)
Immunization with a HER-2/neu helper peptide vaccine
generates HER-2/neu CD8 T-cell immunity in cancer
patients. The Journal of Clinical Investigation, 107, 47–484.
Kohrgruber, N., Halanek, N., Groger, M., Winter, D.,
Rappersberger, K., Schmitt-Egenolf, M., Stingl, G. &
Maurer, D. (1999) Survival, maturation, and function
of CD11c– and CD11cþ peripheral blood dendritic
cells are differentially regulated by cytokines. Journal of
Immunology, 163, 3250–3259.
Koski, G.K., Schwartz, G.N., Weng, D.E., Gres, R.E.,
Engels, F.H.C., Tsokos, M., Czerniecki, B.J. & Cohen, P.A.
(1999) Calcium ionophore-treatedmyeloid cells acquiremany
dendritic cell characteristics independent of prior differ-
entiation state, transformation status, or sensitivity to biologic
agents. Blood, 94, 1359–1371.
Kourilsky, P. & Truffa-Bachi, P. (2001) Cytokine fields and
the polarization of the immune response. Trends in
Immunology, 22, 502–509.
Krieg, A.M. (2002) CpG motifs in bacterial DNA and their
immune effects. Annual Review of Immunology, 20, 709–760.
Kugler, A., Stuhler, G., Walden, P., Zoller, G.,
Zoabywalski, A., Brossart, P., Trefzer, U., Ullrich, S.,
Muller, C.A., Becker, V., Gross, A.J., Hemmerlein, B.,
Kanz, L., Muller, G.A. & Ringert, R.-H. (2000) Regres-
sion of human metastatic renal cell carcinoma after vac-
cination with tumor cell–dendritic cell hybrids. Nature
Medicine, 6, 332–336.
Kuppner, M.C., Gastpar, R., Gelwer, S., Nossner, E.,
Ochmann, O., Scharner, A. & Issels, R.D. (2001) The
role of heat shock protein (hsp 70) in dendritic cell
maturation: Hsp70 induces the maturation of immature
dendritic cells but reduces DC differentiation from
monocyte precursors. European Journal of Immunology,
31, 1602–1609.
Kurts, C., Cannarile, M., Klebba, I. & Brocker, T. (2001)
Cutting edge: dendritic cells are sufficient to cross-
present self-antigens to CD8 T cells in vivo. Journal of
Immunology, 166, 1439–1442.
Liu, Y.-J. (2002) Uncover the mystery of plasmacytoid
dendritic cell precursors or type 1 interferon producing
cells by serendipity. Human Immunology, 63, 1067–1071.
Liu, Y.-J., Kanzler, H., Soumelis, V. & Gilliet, M. (2001)
Dendritic cell lineage, plasticity and cross-regulation.
Nature Immunology, 2, 585–589.
Liu, L., Rich, B.E., Inobe, J., Chen, W. & Weiner, H.L.
(1998) Induction of Th2 cell differentiation in the
92 N. Panoskaltsis et al.
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96
primary immune response: dendritic cells isolated from
adherent cell culture treated with IL-10 prime naive
CD4þ T cells to secrete IL-4. International Immunology,
10, 1017–1026.
Liu,A.,Takahashi,M.,Narita,M.,Zheng,Z.,Knanzawa,N.,
Abe, T., Nikkuni, K., Furukawa, T., Toba, K., Fuse, I. &
Aizawa, Y. (2002) Generation of functional and
mature dendritic cells from cord blood and bone marrow
CD34þ cells by two-step culture combined with calcium
ionophore treatment. Journal of Immunological Methods,
261, 49–63.
Luft, T., Pang, K.C., Thomas, E., Bradley, C.J., Savoia, H.,
Trapani, J. & Cebon, J. (1998) A serum-free culture
model for studying the differentiation of human dendritic
cells from adult CD34þ progenitor cells. Experimental
Hematology, 26, 489–500.
Luster, A.D. (2002) The role of chemokines in linking
innate and adaptive immunity. Current Opinion in
Immunology, 14, 129–135.
Luther, S.A. & Cyster, J.G. (2001) Chemokines as
regulators of T cell differentiation. Nature Immunology,
2, 102–107.
Lyakh, L.A., Koski, G.K., Telford, W., Gress, R.E.,
Cohen, P.A. & Rice, N.R. (2000) Bacterial lipopolysac-
charide, TNF-a, and calcium ionophore under serum-free
conditions promote rapid dendritic cell-like differentiation
in CD14þ monocytes through distinct pathways that acti-
vate NF-kB. Journal of Immunology, 165, 3647–3655.
Macatonia, S.E., Taylor, P.M., Knight, S.C. & Askonas, B.A.
(1989) Primary stimulation by dendritic cells induces
antiviral proliferative and cytotoxic T cell responses
in vitro. The Journal of Experimental Medicine, 169,
1255–1264.
MacDonald, K.P.A., Munster, D.J., Clark, G.J., Dzionek, A.,
Schmitz, J. & Hart, D.N.J. (2002) Characterization of
human blood dendritic cell subsets. Blood, 100, 4512–4520.
Malissen, B. (1999) Dancing the immunological two-step.
Science, 285, 207–208.
Manz, M.G., Traver, D., Miyamoto, T., Wissman, I.L. &
Akashi, K. (2001) Dendritic cell potentials of early
lymphoid and myeloid progenitors. Blood, 97, 3333–3341.
Maraskovsky, E., Daro, E., Roux, E., Teepe, M.,
Maliszeski, C.R., Hoek, J., Caron, D., Lebsack, M.E.
& McKenna, H.J. (2000) In vivo generation of
human dendritic cell subsets by Flt3 ligand. Blood, 96,
878–884.
Martin, P., Martinez del Hoyo, G., Anjuere, F., Ruiz, S.R.,
Arias, C.F., Marin, A.R. & Ardavin, C. (2000) Concept
of lymphoid versus myeloid dendritic cell lineages revis-
ited: both CD8a- and CD8aþ dendritic cells are gener-
ated from CD4low lymphoid-committed precursors.
Blood, 96, 2511–2519.
Martinez del Hoyo, G., Martin, P., Vargas, H.H., Ruiz, S.,
Arias, C.F. & Ardavin, C. (2002) Characterization of a
common precursor population for dendritic cells. Nature,
415, 1043–1047.
McCoy, K.D., Hermans, I.F., Fraser, J.H., Le Gros, G. &
Ronchese, F. (1999) Cytotoxic T lymphocyte-associated
antigen 4 (CTLA-4) can regulate dendritic cell-induced
activation and cytotoxicity of CD8þ T cells independ-
ently of CD4þ T cell help. The Journal of Experimental
Medicine, 189, 1157–1162.
McNeel, D.G., Schiffman, K. & Disis, M.L. (1999) Immun-
ization with recombinant human granulocyte-
macrophage colony-stimulating factor as a vaccine adju-
vant elicits both a cellular and humoral response to
recombinant human granulocyte-macrophage colony-
stimulating factor. Blood, 93, 2653–2659.
Molldrem, J.J., Lee, P.P., Kant, S., Wieder, E., Jiang, W.,
Lu, S., Wang, C. & Davis, M.M. (2003) Chronic myelo-
genous leukemia shapes host immunity by selective dele-
tion of high-avidity leukemia-specific T cells. The Journal
of Clinical Investigation, 111, 639–647.
Moore, K.W., Malefyt, R., Coffman, R.L. & O’Garra, A.
(2001) Interleukin-10 and the interleukin-10 receptor.
Annual Review of Immunology, 19, 683–765.
Mortarini, R., Anichini, A., Di Nicola, M., Siena, S.,
Bregni, M., Belli, F., Molla, A., Gianni, A.M. &
Parmiani, G. (1997) Autologous dendritic cells derived
from CD34þ progenitors and from monocytes are not
functionallly equivalent antigen-presenting cells in ther
induction of melan-A/mart-127�35-specific CTLs from
peripheral blood lymphocytes of melanoma patients
with low frequency of CTL precursors. Cancer Research,
57, 5534–5541.
Moser, B. & Loetscher, P. (2001) Lymphocyte traffic con-
trol by chemokines. Nature Immunology, 2, 123–128.
Moser, M. & Murphy, K.M. (2000) Dendritic cell regulation
of Th1-Th2 development. Nature Immunology, 1, 199–205.
Mosmann, T.R., Cherwinski, H., Bond, M.W.,
Giedlin, M.A. & Coffman, R.L. (1986) Two types of
murine helper T cell clone. I. Definition according to
profiles of lymphokine activities and secreted proteins.
Journal of Immunology, 136, 2348–2357.
Mosmann, T.R., Li, L. & Sad, S. (1997) Functions of CD8
T-cell subsets secreting different cytokine patterns. Semi-
nars in Immunology, 9, 87–92.
Mosmann, T.R. & Sad, S. (1996) The expanding universe
of T-cell subsets: Th1, Th2 and more. Immunology
Today, 17, 138–146.
Mukherji, B., Chakraborty, N.G., Yamasaki, S., Okino, T.,
Yamase, H., Sporn, J.R., Kutzman, S.K., Ergin, M.T.,
Ozols, J. &Meehan, J. (1995) Induction of antigen-specific
cytolytic T cells in situ in human melanoma by immuniza-
tion with synthetic peptide pulsed autologous antigen
presenting cells. Proceedings of the National Academy of
Sciences of the United States of America, 92, 8078–8082.
Nestle, F.O., Alijagic, S., Gilliet, M., Sun, Y., Grabbe, S.,
Dummer, R., Burg, G. & Schadendorf, D. (1998)
Vaccination of melanoma patients with peptide- or
tumor lysate-pulsed dendritic cells. Nature Medicine, 4,
328–332.
Immune modulation with DCs 93
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96
Nestle, F.O., Banchereau, J. & Hart, D. (2001) Dendritic
cells: on the move from bench to bedside. Nature Medi-
cine, 7, 761–765.
Nieda, M., Nicol, A., Kikuchi, A., Kashiwase, K., Taylor, K.,
Suzuki, K., Tadokoro, K. & Juji, T. (1998) Dendritic cells
stimulate the expansion of bcr-abl specific CD8þ T cells
with cytotoxic activity against leukemia cells from patients
with chronic myeloid leukemia. Blood, 91, 977–983.
O’Doherty, U., Peng, M., Gezelter, S., Swiggard, W.J.,
Betjes, M., Bhardwaj, N. & Steinman, R.M. (1994)
Human blood contains two subsets of dendritic cells,
one immunologically mature and the other immature.
Immunology, 82, 487–493.
Offringa, R., van der Burg, S.H., Ossendorp, F.,
Toes, R.E.M. & Melief, C.J.M. (2000) Design and
evaluation of antigen-specific vaccination strategies
against cancer. Current Opinion in Immunology, 12,
576–582.
Olweus, J., BitMansour, A., Warnke, R., Thompson, P.A.,
Carballido, J., Picker, L.J. & Lund-Johansen, F. (1997)
Dendritic cell ontogeny: a human dendritic cell lineage of
myeloid origin. Proceedings of the National Academy of
Sciences of the United States of America, 94, 12551–12556.
Ostberg, J.R., Gellin, C., Patel, R. & Repasky, E.A. (2001)
Regulatory potential of fever-range whole body
hyperthermia on langerhans cells and lymphocytes in an
antigen-dependent cellular immune response. Journal of
Immunology, 167, 2666–2670.
O’Sullivan, B.J. & Thomas, R. (2002) CD40 ligation con-
ditions dendritic cell antigen-presenting function through
sustained activation of NF-kB. Jounral of Immunology,
168, 5491–5498.
Palucka, K., Taquet, N., Sanchez-Chapuis, F. &
Gluckman, J.C. (1998) Dendritic cells as the terminal
stage of monocyte differentiation. Journal of Immuno-
logy, 160, 4587–4595.
Panoskaltsis, N., Belanger, T.J., Liesveld, J.L. & Abboud, C.N.
(2002) Optimal cytokine stimulation for the enhanced gen-
eration of leukemic dendritic cells in short-term culture.
Leukemia Research, 26, 191–201.
Panoskaltsis, N., Reid, C.D.L. & Knight, S.C. (2003)
Quantification and cytokine production of circulating
lymphoid and myeloid cells in acute myelogenous
leukemia (AML). Leukemia, 17, 716–725.
Pierre, P., Turley, S.J., Gatti, E., Hull, M., Meltzer, J.,
Mirza, A., Inaba, K., Steinman, R.M. & Mellman, I.
(1997) Developmental regulation of MHC class II trans-
port in mouse dendritic cells. Nature, 388, 787–792.
Pulendran, B., Banchereau, J., Burkeholder, S., Kraus, E.,
Guinet, E., Chalouni, C., Caron, D., Maliszewski, C.,
Davoust, J., Fay, J. & Palucka, K. (2000) Flt3-ligand and
granulocyte colony-stimulating factor mobilize distinct
human dendritic cell subsets in vivo. Journal of Immunology,
165, 566–572.
Pulendran, B., Smith, J.L., Caspary, G., Brasel, K., Pettit, D.,
Maraskovsky, E. &Maliszewski, C.R. (1999) Distinct den-
dritic cell subsets differentially regulate the class of immune
response in vivo. Proceedings of the National Academy of
Sciences of the United States of America, 96, 1036–1041.
Pullarkat, V., Lau, R., Lee, S.-M., Bender, J.G. &Weber, J.S.
(2002) Large-scale monocyte enrichment coupled with a
closed culture system for the generation of human dendritic
cells. Journal of Immunological Methods, 267, 173–183.
Randolph, G.J., Beaulieu, S., Lebecque, S., Steinman, R.M.
& Muller, W.A. (1998) Differentiation of monocytes into
dendritic cells in a model of transendothelial trafficking.
Science, 282, 480–483.
Reddy, A., Sapp, M., Feldman, M., Subklewe, M. &
Bhardwaj, N. (1997) A monocyte conditioned medium
is more effective than define cytokines in mediating the
terminal maturation of human dendritic cells. Blood, 90,
3640–3646.
Reid, C.D.L. (2001) Dendritic cells and immunotherapy for
malignant disease. British Journal of Haematology, 112,
874–887.
Reid, C.D.L., Fryer, P.R., Clifford, C., Kirk, A., Tikerpae, J.
& Knight, S.C. (1990) Identification of hematopoietic
progenitors of macrophages and dendritic langerhans
cells (DL-CFU) in human bone marrow and peripheral
blood. Blood, 76, 1139–1149.
Reid, C.D.L., Stackpoole, A., Meager, A. & Tikerpae, J.
(1992) Interactions of tumor necrosis factor with
granulocyte-macrophage colony-stimulating factor and
other cytokines in the regulation of dendritic cell growth
in vitro from early bipotent CD34þ progenitors in
human bone marrow. Journal of Immunology, 149,
2681–2688.
Reid, S.D., Penna, G. & Adorini, L. (2000) The control of
T cell responses by dendritic cell subsets. Current Opinion
in Immunology, 12, 114–121.
Ridge, J.P., Di Rosa, F. & Matzinger, P. (1998) A
conditioned dendritic cell can be a temporal bridge
between a CD4þ T-helper and a T-killer cell. Nature,
393, 474–478.
Rissoan, M.-C., Soumelis, V., Kadowaki, N., Grouard, G.,
Briere, F., Malefyt, R. & Liu, Y.-J. (1999) Reciprocal
control of T helper cell and dendritic cell differentiation.
Science, 283, 1183–1186.
Robinson, S.P., English, N., Jaju, R., Kearney, L., Knight, S.C.
& Reid, C.D.L. (1998) The in-vitro generation of dendritic
cells from blast cells in acute leukaemia. British Journal of
Haematology, 103, 763–771.
Robinson, S.P., Patterson, S., English, N., Davies, D.,
Knight, S.C. & Reid, C.D.L. (1999) Human peripheral
blood contains two distinct lineages of dendritic cells.
European Journal of Immunology, 29, 2769–2778.
Rosenberg, S.A., Yang, J.C., Schwartzentruber, D.J., Hwu, P.,
Marincola, F.M., Topalian, S.L., Restifo, N.P.,
Dudley, M.E., Schwarz, S.L., Spiess, P.J., Wunderlich, J.R.,
Parkhurst, M.R., Kawakami, Y., Seipp, C.A., Einhorn, J.H.
& White, D.E. (1998) Immunologic and therapeutic evalua-
tion of a synthetic peptide vaccine for the treatment of
94 N. Panoskaltsis et al.
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96
patients with metastatic melanoma. Nature Medicine, 4,
321–327.
Sallusto, F., Lanzavecchia, A. & Mackay, C.R. (1998a)
Chemokines and chemokine receptors in T-cell priming
and Th1/Th2-mediated responses. Immunology Today,
19, 568–574.
Sallusto, F., Palermo, B., Lenig, D., Miettinen, M.,
Matikainen, S., Julkunen, I., Forster, R., Burgstahler, R.,
Lipp, M. & Lanzavecchia, A. (1999) Distinct patterns and
kinetics of chemokine production regulate dendritic cell
function. European Journal of Immunology, 29, 1617–1625.
Sallusto, F., Schaerli, P., Loetscher, P., Schaniel, C., Lenig, D.,
Mackay, C.R., Qin, S. & Lanzavecchia, A. (1998b) Rapid
and coordinated switch in chemokine receptor expression
during dendritic cell maturation. European Journal of
Immunology, 28, 2760–2769.
Saraya, K. & Reid, C.D.L. (1996) Stem cell factor and the
regulation of dendritic cell production from CD34þprgenitors in bone marrow and cord blood. British Jour-
nal of Haematology, 93, 258–264.
Sato, M., Iwakabe, K., Kimura, S. & Nishimura, T. (1999)
Functional skewing of bone marrow-derived dendritic
cells by Th1- or Th2-inducing cytokines. Immunology
Letters, 67, 63–68.
Saudrais, C., Spehner, D., de la Salle, H., Bohbot, A.,
Cazenave, J.-P., Goud, B., Hanau, D. & Salamero, J.
(1998) Intracellular pathway for the generation of functional
MHC class II peptide complexes in immature human den-
dritic cells. Journal of Immunology, 160, 2597–26907.
Scheinecker, C., Machold, K.P., Majdic, O., Hocker, P.,
Knapp, W. & Smolen, J.S. (1998) Initiation of the auto-
logous mixed lymphocyte reaction requires the expres-
sion of costimulatory molecules B7–1 and B7–2 on
human peripheral blood dendritic cells. Journal of
Immunology, 161, 3966–3973.
Schindler, H., Lutz, M.B., Rollinghoff, M. & Bogdan, C.
(2001) The production of IFN-g by IL-12/IL-18-activated
macrophages requires STAT4 signaling and is inhibited by
IL-4. Journal of Immunology, 166, 3075–3082.
Schoenberger, S.P., Toes, R.E.M., van der Voort, E.I.H.,
Offringa, R. & Melief, C.J.M. (1998) T-cell help for
cytotoxic T lymphocytes is mediated by CD40–CD40L
interactions. Nature, 393, 480–483.
Scholler, N., Hayden-Ledbetter, M., Hellstrom, K.-E.,
Hellstrom, I. & Ledbetter, J.A. (2001) CD83 is a sialic
acid-binding Ig-like lectin (Siglec) adhesion receptor that
binds monocytes and a subset of activated CD8þ T cells.
Journal of Immunology, 166, 3865–3872.
Schuler-Thurner, B., Schultz, E.S., Berger, T.G., Weinlich, G.,
Ebner, S., Woerl, P., Bender, A., Feuerstein, V.,
Fritsch, P.O., Romani, N. & Schuler, G. (2002) Rapid
induction of tumor-specific type 1 T helper cells in
metastatic melanoma patients by vaccination with
mature, cryopreserved, peptide-loaded monocyte-
derived dendritic cells. The Journal of Experimental
Medicine, 195, 1279–1288.
Shah, P.D., Gilbertson, S.M. & Rowley, D.A. (1985) Den-
dritic cells that have interacted with antigen are targets
for natural killers. The Journal of Experimental Medicine,
162, 625–636.
Siegal, F.P., Kadowaki, N., Shodell, M., Fitzgerald-
Bocarsly, P.A., Shah, K., Ho, S., Antonenko, S. &
Liu, Y.-J. (1999) The nature of the principal type 1
interferon-producing cells in human blood. Science,
284, 1835–1837.
Somersan, S., Larsson, M., Fonteneau, J.F., Basu, S.,
Srivastava, P. & Bhardwaj, N. (2001) Primary tumor
tissue lysates are enriched in heat shock proteins and
induce the maturation of human dendritic cells. Journal
of Immunology, 167, 4844–4852.
Soumelis, V., Scott, I., Gheyas, F., Bouhour, D., Cozon, G.,
Cotte, L., Huang, L., Levy, J.A. & Liu, Y.-J. (2001)
Depletion of circulating natural type 1 interferon-
producing cells in HIV-infected AIDS patients. Blood,
98, 906–912.
Steinman, R.M. &Witmer, M.D. (1978) Lymphoid dendritic
cells are potent stimulators of the primary mixed leukocyte
reaction in mice. Proceedings of the National Academy of
Sciences of the United States of America, 75, 5132–5136.
Szabolcs, P., Moore, M.A.S. & Young, J.W. (1995)
Expansion of immunostimulatory dendritic cells among
the myeloid progeny of human CD34þ bone marrow
precursors cultured with c-kit ligand, granulocyte-
macrophage colony-stimulating factor, and TNF-a.Journal of Immunology, 154, 5851–5861.
Tarte, K. & Klein, B. (1999) Dendritic cell-based vaccine: a
promising approach for cancer immunotherapy. Leuke-
mia, 13, 653–663.
Thery, C., Duban, L., Segura, E., Veron, P., Lantz, O. &
Amigorena, S. (2002) Indirect activation of naive CD4þT cells by dendritic cell-derived exosomes. Nature Immu-
nology, 3, 1156–1162.
Timmerman, J.M., Czerwinski, D.K., Davis, T.A., Hsu, F.J.,
Benike, C., Hao, Z.M., Taidi, B., Rajapaksa, R.,
Caspar, C.B., Okada, C.Y., van Beckhoven, A., Liles, T.M.,
Engleman, E.G.&Levy, R. (2002) Idiotype-pulsed dednritic
cell vaccination for B-cell lymphoma: clinical and immune
responses in 35 patients.Blood, 99, 1517–1526.
Timmerman, J.M. & Levy, R. (2000) Linkage of foreign
carrier protein to a self-tumor antigen enhances the
immunogenicity of a pulsed dendritic cell vaccine. Jour-
nal of Immunology, 164, 4797–4803.
Trinchieri, G. (1995) Interleukin-12: a proinflammatory
cytokine with immunoregulatory functions that bridge
innate resistance and antigen-specific adaptive immunity.
Annual Review of Immunology, 13, 251–276.
Trinchieri, G. (2001) Regulatory role of T cells producing
both interferon g and interleukin 10 in persistent infection.
The Journal of Experimental Medicine, 194, F53–F57.
Trombetta, E.S., Ebersold, M., Garrett, W., Pypaert, M. &
Mellman, I. (2003) Activation of lysosomal function
during dendritic cell maturation. Science, 299, 1400–1403.
Immune modulation with DCs 95
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96

Troy, A.J. & Hart, D.N.J. (1997) Dendritic cells and
cancer: progress toward a new cellular therapy. Journal
of Hematotherapy, 6, 523–533.
Tuyaerts, S., Noppe, S.M., Corthals, J., Breckpot, K.,
Heirman, C., De Greef, C., Van Riet, I. & Thielemans, K.
(2002) Generation of large numbers of dendritic cells in a
closed system using Cell FactoriesTM. Journal of Immuno-
logical Methods, 264, 135–151.
Vieira, P.L., de Jong, E.C., Wierenga, E.A., Kapsenberg, M.L.
& Kalinski, P. (2000) Development of Th1-inducing capacity
in myeloid dendritic cells requires environmental instruction.
Journal of Immunolgy, 164, 4507–4512.
Vincent, M.S., Leslie, D.S., Gumperz, J.E., Xiong, X., Grant,
E.P. & Brenner, M.B. (2002) CD1-dependent dendritic cell
instruction.Nature Immunology, 3, 1163–1168.
Viola, A., Schroeder, S., Sakakibara, Y. & Lanzavecchia, A.
(1999) T lymphocyte costimulation mediated by reorganiza-
tion of membrane microdomains. Science, 283, 680–650.
Volpi, I., Perrucio, K., Tosti, A., Capanni, M., Ruggeri, L.,
Posati, S.,Aversa,F.,Tabilio,A.,Romani,L.,Martelli,M.F.
& Velardi, A. (2001) Postgrafting administration of granulo-
cyte colony-stimulating factor impairs functional immune
recovery in recipients of human leukocyte antigen haplotype-
mismatched hematopoietic transplants.Blood, 97, 2514–2521.
Vuckovic, S., Kim, M., Khalil, D., Turtle, C.J., Crosbie, G.V.,
Williams,N., Brown, L.,Williams,K., Kelly, C., Stravos, P.,
Rodwell, R., Hill, G.R., Wright, S., Taylor, K., Gill, D.,
Marlton, P., Bradstock, K. & Hart, D.N.J. (2003) Granu-
locyte-colony stimulating factor increases CD123hi blood
dendritic cells with altered CD62L and CCR7 expression.
Blood, 101, 2314–2317.
Whiteside, T.L., Zhao, Y., Tsukishiro, T., Elder, E.M.,
Gooding, W. & Baar, J. (2003) Enzyme-linked immuno-
spot, cytokine flow cytometry, and tetramers in the
detection of T-cell responses to a dendritic cell-based
multipeptide vaccine in patients with melanoma. Clinical
Cancer Research, 9, 641–649.
Wong, E.C.C., Maher, V.E., Hines, K., Lee, J., Carter, C.S.,
Goletz, T., Kopp, W., Mackall, C.L., Berzofsky, J.A. &
Read, E.J. (2001) Development of a clinical-scale method
for generation of dendritic cell from PBMC for use in
cancer immunotherapy. Cytotherapy, 3, 19–29.
Yee, C., Thompson, J.A., Byrd, D., Riddell, S.R., Roche, P.,
Celis, E. & Greenberg, P.D. (2002) Adoptive T cell
therapy using antigen-specific CD8þ T cell clones for
the treatment of patients with metastatic melanoma: in
vivo persistence, migration, and antitumor effect of
transferred T cells. Proceedings of the National Academy
of Sciences of the United States of America, 99,
16168–16173.
Young, J.W., Szabolcs, P. & Moore, M.A.S. (1995) Identi-
fication of dendritic cell colony-forming units among
normal human CD34þ bone marrow progenitors that
are expanded by c-kit-ligand and yield pure dendritic
cell colonies in the presence of granulocyte/macro-
phage colony-stimulating factor and tumor necrosis
factor-a. The Journal of Experimental Medicine, 182,
1111–1120.
Zou, W., Borvak, J., Wei, S., Isaeva, T., Curiel, D.T. &
Curiel, T.J. (2001) Reciprocal regulation of plasmacytoid
dendritic cells and monocytes during viral infection.
European Journal of Immunology, 31, 3833–3839.
96 N. Panoskaltsis et al.
# 2004 Blackwell Publishing Ltd, Transfusion Medicine, 14, 81–96
Related Documents











