IMMEDIATE POSTOPERATIVE CARE, WITH PARTICULAR , oo s C R STEPHEN, M D I' AND I TALTON, M I) * WITH INCREASED STANDARDS Of trammg i, and improvements m anaesthetic tech- tuques and drugs, anaesthetists now pIade themselves that patients can usually be brought successfully through the most dls of operatwe procedures Where problems arise m g~eater mc:dence is m the :mmediate postoperatwe period It is here that the anaesthetast must play an even more achve role m the future than he is doing at present Recovery rooms, or postanaesthetm to be cared for by specially trained r. World War Our responslblhty as an~ early by Dnpps and Waters, who e: "Stir-up" regime, the :mportance of tu: cough at regular intervals, and urgmg dflJaculty of obtaining the co-operahor suggested the intermittent mhalatmn oJ years has made every anaesthehst reco contmuous admmlstratmn of oxygen, inserted through the nose into the oro test of time treas, whmh allow postoperahve patients lrses, were an outgrowth of the Second testhetists m th~s area ,was pomted out nphas:zed, m a connotatmn called the nmg the patient frequently, hawng him him to breathe deeply :'Recogmzmg the of the patient to breathe deeply, they carbon dmxlde, an idea which m recent ] m horror They also recommended the vhere indicated, by means of a catheter harynx, a technique winch has stood the In the last 20 years, the :ole of adeq}iate ventdatmn postopel.at:vely has been stressed, with part:cular emphas:s on carbon d:oxlde ehmmatlon Mechameal ventilators have been developed, and the rod:cations for their use have mulh- phed as the :mportance of preservmg gas exchange to and from the lungs has been recogmzed Hand m hand w:th lh:s alertness has been the development of ob]echve means of determining the efficacy of respiratory exchange Rehable laboratory tests, wh:ch are not techmcally d:fficult to perform, have allowed us for several years to determine the pH and carbon dioxide tension, more or less at the beds:de W:th special eqmpment lit has also been possible to determine the arterial oxygen saturation But the satmtataon mere]y indicates how much oxygen :s being carried in the blood as a percentage of that which the blood :s capable of carrying under normal clxcumstances A 'much more accurate measurement is the oxygen tension, which indicates the partial pressure of oxygen m the arterial blood, and therefore the avaflabihty or ease with whmh oxygen can be presented to the tissues Within the last two to tl~hree years, as a result of the development of oxygen electrodes, it has for the firstL hme become poss:ble to measure under chn:cal c~rcumstances the oxygen tension exxstmg m blood This breakthrough Is of vital maportance m the .care of patients This paper as concerned pr:manly with the arterial oxygen tlensmns found m *Dlvlsmn of Anesthesmtogy, Duke Umverslty Medmal Center, Durham, North Cmohna '~86 Can Anaes Soc ], re] 11, no 6, November, 1964

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
IMMEDIATE POSTOPERATIVE CARE, WITH PARTICULAR
, oo s
C R STEPHEN, M D I' AND I TALTON, M I) *
WITH INCREASED STANDARDS Of trammg i, and improvements m anaesthetic tech- tuques and drugs, anaesthetists now pIade themselves that patients can usually be brought successfully through the most dls of operatwe procedures Where problems arise m g~eater mc:dence is m the :mmediate postoperatwe period It is here that the anaesthetast must play an even more achve role m the future than he is doing at present
Recovery rooms, or postanaesthetm to be cared for by specially trained r. World War Our responslblhty as an~ early by Dnpps and Waters, who e: "Stir-up" regime, the :mportance of tu: cough at regular intervals, and urgmg dflJaculty of obtaining the co-operahor suggested the intermittent mhalatmn oJ years has made every anaesthehst reco contmuous admmlstratmn of oxygen, inserted through the nose into the oro test of time
treas, whmh allow postoperahve patients lrses, were an outgrowth of the Second testhetists m th~s area ,was pomted out nphas:zed, m a connotatmn called the nmg the patient frequently, hawng him him to breathe deeply : 'Recogmzmg the
of the patient to breathe deeply, they carbon dmxlde, an idea which m recent
] m horror They also recommended the vhere indicated, by means of a catheter harynx, a technique winch has stood the
In the last 20 years, the :ole of adeq}iate ventdatmn postopel.at:vely has been stressed, with part:cular emphas:s o n carbon d:oxlde ehmmatlon Mechameal ventilators have been developed, and the rod:cations for their use have mulh- phed as the :mportance of preservmg gas exchange to and from the lungs has been recogmzed Hand m hand w:th lh:s alertness has been the development of ob]echve means of determining the efficacy of respiratory exchange Rehable laboratory tests, wh:ch are not techmcally d:fficult to perform, have allowed us for several years to determine the pH and carbon dioxide tension, more or less at the beds:de W:th special eqmpment lit has also been possible to determine the arterial oxygen saturation But the satmtataon mere]y indicates how much oxygen :s being carried in the blood as a percentage of that which the blood :s capable of carrying under normal clxcumstances A 'much more accurate measurement is the oxygen tension, which indicates the partial pressure of oxygen m the arterial blood, and therefore the avaflabihty or ease with whmh oxygen can be presented to the tissues Within the last two to tl~hree years, as a result of the development of oxygen electrodes, it has for the firstL hme become poss:ble to measure under chn:cal c~rcumstances the oxygen tension exxstmg m blood This breakthrough Is of vital maportance m the .care of patients
This paper as concerned pr:manly with the arterial oxygen tlensmns found m
*Dlvlsmn of Anesthesmtogy, Duke Umverslty Medmal Center, Durham, North Cmohna
'~86
Can Anaes Soc ] , re] 11, no 6, November, 1964

S T E P H E N & T A L T O N I M M E D I A T E P Q S T O P ~ R A T I V E C A R E
pahents m the :mmedmte postoperahve permd ithesp'delermmahons have b~en correlated wath the ablhty of pahents to ehminat~ carbon dloxade It is nnportant first to determine what the normal arterml oxygen t~nsmn is The textbooks~ of physmlogy have told us that tins figure is 100 mm Hg w:th the patmnt breathing room mr However, Lambertsen 2 mdmates tha t th~noJmal value for arterial oxygen tensmn as 95 mm Hg More recently Rame aiILd B:shop 8 have shown that age and pos:t:on are factors m the normal values for: I oxygen tens:on In sublects less than 40 years of age, the mean arterial oxygen 'tensmn whale breathing mr was 97 6 mm Hg an the s:ttmg pos:tmn and 95 3 mm Hg m the supine posit!on In sub]ects over 40 years of age, the mean paO~ was~ 90 0 mm Hg m the sitting posture and 88 2 mm Hg while supine In oar own mst:tutmn, the arterial oxygen tensmn m 14 pahents while lying supine m the ward awaiting elec~we surgacal procedures averaged 80 4 mm Hg, w:th a 1 m a 2g-year-old pataent to 57 5 mm Hg m a 68-year average age of these pahents was 47 3 years, wath, years It :s apparent that the "normal" arterial oxyg, indeed may vary from pahent to pat:ent
ange between 100 mm Hg -old pahent (Table I) The
range between 28 and 68 m tensmn as unknown,~and
FABLE I
:paCO2 paO~ Age bex pH (]~m lqg) (mm Hg)
1 28 F 7 40 43 2 93 1 2 28 F 7 42 ,30 7 100 0 3 38 b 7 41 39 6 87 4 4 39 M 7 43 36 4 63 2 5 45 F 7 44 35 6 70 1 6 46 1" 7 46 30 4 74 7 7 46 F 7 39 39 2 88 5 8 46 F 7 44 37 ,3 93 1 9 48 F 7 46 43 ~t 74 7
10 51 M 7 44 87 3 75 9 11 55 M 7 39 41 J 71 3 12 60 5/I 7 42 44 8 80 5 13 64 b 7 41 37 2 96 6 14 t38 M 7 40 37 '2 57 5
~.v 47 3 7 42 38 1 80 4
In our hosp:tal random determinations of blood-gas values during and after operatmn m over 200 pat:ents md:cated that great variations could occur, depend- mg on the phys:cal status of the pat:ent, the type of' operatmn bemg performed, and the care w:th wh:ch the anaesthet:c was being admm,stered It became obv:ous that adequate ehmmat:on of carbon d:ox:de from the lungs dad not necessar:ly ensure a normal arter:a] oxygen tens:on, thus perhaps reafl?rmmg the old phys:olog:cal doctrine that ~t is 20 tames castor to get carbon d:ox:de across
I i the alveolar membrane than it :s oxygen For example, an a 77-year-old woman unde:gomg subtotal gastric resectmn (Fig 1 ), at was not possible to ob!tam a normal arteraal oxygen tens:on, even though ventfiahon was sufflcmnt to produce a defimte resparatory alkalosas In another, patient, a 23-year-old :nan having a closure of a transverse eolostomy (Fig 2), oxygen tensions were above normal during operat:on, but when he was allowed to breathe room atr m the

LANG Vera
Age 77 W F
S~btotal Galstrxc R'esectton
fo~ I Car cxnom&
Thxopental 150 ~ g NzO , OZ. Ether ! ~ucczny~chohn( I00 Mg
F I - 7 ~ 4 8
T~e ~_H ZqPz e~z
1 44 7 48 ~4 5 67
2 20 7 64 ~0 0 50
z 45 7 53 ~o s 60
3 08 7 65 i8 5 56
3 27 7 65 17 0 51
Beginning St~rgery Spon Res]~ B P 160/~0
~o~t R e s p , 13 p lZ0/~0
Cost R e s p l B P lZO/~O
Cont Resp | B P 14o/~o
Cont Respl B P 160190
3 50 7 6Z 77 5 67 Cont R e s p /, B P 1801100
F~GvaE 1 Arterial blood-gas values m a 77-year-old womap under- going subtotal gastric resectaon Note low arterial oxygen tensions m presence of reduced respxratory a~kalosls
POOLE I s a a c E9-15-413
Age 23 M C 12 - 20 - 63
Gunsho I Wound Abdomen
Closure T r a n s v e r s e Co los tomy
Thlopental ZS0 Mg Gallarr~xne 80 Mg NzO, 02. Z 5 1 5 Et~aer
T~me pH pCOzl pO 2
10 05 7 39 40 5 118
11 04 7 43 34 6 117
Kecove~ y Room
Durxng 'Surgery Asst , R e s p
End of ]Surgery Breath ing 0 Z
11 15 7 37 40 I 63 Room ~ar
11 30 7 36 42 4 68 Same
12 45 7 36 42 4 87 Same
lZ 0o 7 34 39 I s3 Same tae,tles~
FmURE 2 Arter ,a l b l o o d - g a s i v a l u e s m a 23-year -o ld ma n having a closure of a transverse colostopay Note reduclaon m arterial oxygen tensions m recovery room m splie of preservahon of normal ~eid-base balance
recovery room, the arterial oxygen ten lon ~as reduced to low ]levels, even ~hough the pH and carbon dioxide tensions remained within normal hm~ts
For these reasons an oblechve study was undertaken t O determine[ what happened to pat-tents postoperatxvely.

STEPHEN &: TALTON IIVIMEDIATE POS~FOPE~ATIVE CARE 5~9
Hespwat~m By means of a Wright Resplrom@ter 'ahd a Bennett face-ma!k, respn'atory rates, tldal volumes, and minute volume~s were determined m ~0 patlents the afternoon before operatmn (control), 'mmedmtely on arrival ~n the recovery room, and at i0 and 30 minute interval m the recovery room All types o~ general anaesthesm were used, including ~thyl ether, cyclopropane, ha]othane, and methoxyflurane, and the same ph slclan performed all the measurements Oxygen was not admmlsteled to thls ~ontrol group The average minute ,volume preoperatlvely was 6 0 htres, and thrce readings postoperatlvely differed h~le (Fag 3) The average resprratory ratc before operatlon was 17
MINUTE VOLUME
Conlrol
280
260
240
220
200
t80
160
140
120
I00
80
60
40-
20
0
~ ~_~ _ _
MINUTE VOLUME - CONTROL
FIGURE 3 Minute volumes (average and extremes) m 20 patients the day priori to opera- taon, and m the unmedmte postoperatll:ve period
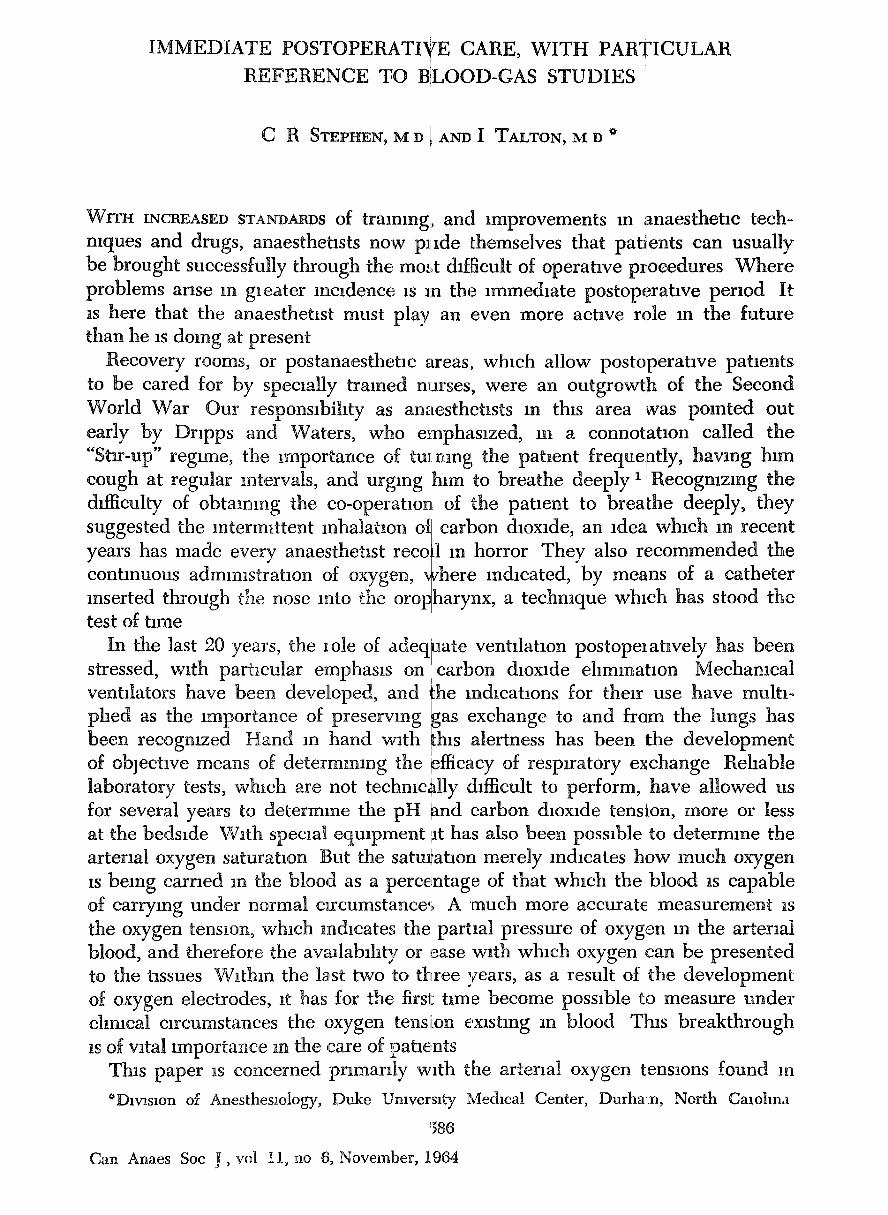
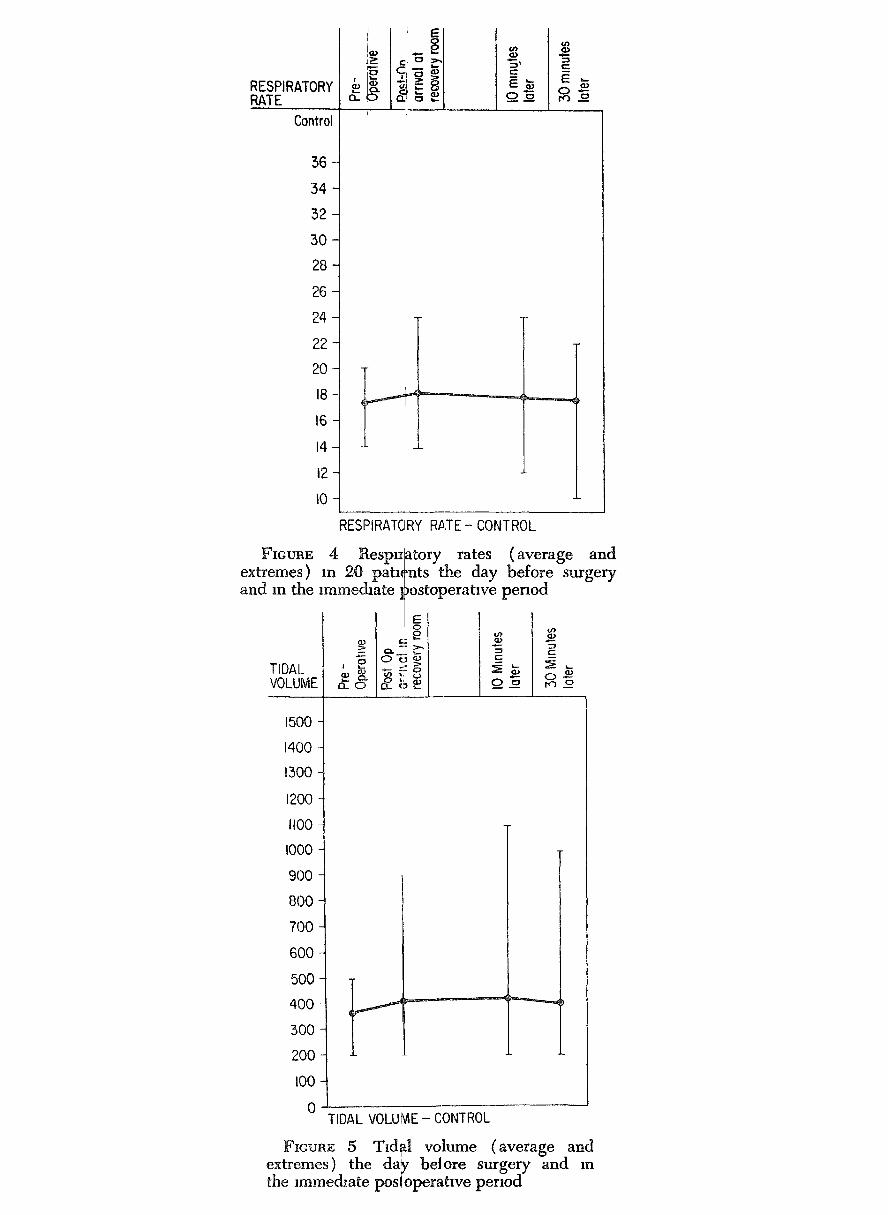
per minute, and the average tidal volume was 350 n~ These values were essen- tially unaltered m the postoperative period (Fags 4 ,and 5) Under the circum- stances of this study, respuatory parameters were not grossly altered by anaesthesia and operation
Blood gas values During anaesthesia an arterial needle was placed m the radlal, ulnar, or brach~al artery, and blood samples were withdrawn at various intervals in hepanmzed syringes under anaerobic con&t~ons W~thm 5 to 10 minutes of obtaining the sample, determinations of pH, carbon &oxide tensmn, and oxygen tension were made, always by the same techmc~an, on an InstrumentatlLon Laboratories apparatus Correctxens were made for body temperature and haema- toer~t
RESPIRATORY RATE ~-
Control
36
34
32
30
28
26
24
22
20
18
16
14
12
IO
L
RESPIRATORY RATE- CONTROL
FIGURE 4 Respt~ extremes) m 20 pah~ and m the immechate 1
TIDAL VOLUME
atory rates (average and 'nts the day before surgery )ostoperahve period
==
1500
1400
1300
1200
II00
I000
9(30
800
700
6OO
50O
400
30O
200
I00
0 TIDAL VOLUME - CONTROL
FICURE 5 Tld~l volume (average and extremes) the day bet ore surgery and m the ~mmedlate posioperahve period

~w I pCO~
7 5 5 - 55-
75O- 50-
7 4 5 - 45-
7 4 0 - 40"4
7 5 5 - 55.4
7 5 0 - 50-~
725- 25-"
720- 20-
POST OP 5 mm I ,om,o, I 'C',, m'"
I
pO~ mmHg
-400
- 350
- 5 0 0
-250
- 200
- 1 5 0
- 1 0 0
75
50 ,,,,J
6 PATIENTS
FIcum~ 6 pH, paCOo, and paO 2 values In six pahents who did not receive oxygen postoperatively Note normal acid-base balance, but bvldenee o{ arterial hylY)xaemla
pH o
760-
755-
750-
745-
740-
7 3 5 -
750-
725-
720-
p 30z nHg
x
50-
55-
50-
451
4off
554
5 0 -
POST I OP 5 mm I0 mln mmHg
TT
/ i
%
20 4- ,.02 02 by
by M a s k - - - ~ N a s o l ~ (:,atheter
-400
350
'500
- 2 5 0
- 2 0 0
-150
- I 0 0
75
50
6 PATIENTS ,
FIcram~ 7 pH, paCO 2, and paO 2 values, m six patients who received oxygen m postopelratlve period Note normal acid-base balance and satisfactory oxy- gen tension values

592 I # CANADIAN ANAESTH~TIS'I S ] SOG~LETY ]OUBNAL
In 6 patients followed postoperataqely for 30 inmutes, m who m a vigorous stir-up regime was maintained, but to, wh~[,m no oxygen was gwen, the pH and paCO.~ were essentmlly within normal hr. the range of 80ram Hg (Fig 6) Aseco oxygen was administered, first by bag aI showed marked increases m oxygen ten values remained within normal hmlts
nts, but the paO2 (average) was in ad similar group of pahents to whom d mask and then by nasal catheter, ~mn (Fig 7) The pH and paCO=
pH o
760-
7 5 5 -
7 5 0 -
7 4 5 -
740~
7 5 5 -
7 3 0 -
7 2 5 -
7 2 0 -
pCOz mmHg
x
60-
55-
50-
4 5 -
40-
35-
30-
25-
20-
Oor,noIRecov I" I" 60 0p [Ro0m 1 n'!..!_n___J~rnin_.l mm
POe mmHg
o
- 400
- 350
- 300
-250
- 200
- 150
- I 0 0
- 7 5
- 5 0
6 PA'FI E N]S
FIGUAE 8 pH, paCO 2, and paO 2 values obtained m s~x pabents during anaesthesm and for 69 minutes m postoperahve permd pabents dld not receive oxy- gen postoperahvely Note normal acid-base values, but arterial hypoxaemm posto]?erabve|y
In a thard group of 6 patmnts (Fig 8), who were followed for 60 minutes posteperahvely, an arterial blood sample was, taken while undeJr anaesthesm During surgery the average pH was 7 48, the paCO2 was 30 mm Hg, and the paO~ was 160 mm Hg It would appear that these patients wel'~e being ade- quately venhlated and oxygenated during anaesthesia However, m the post- operahve period, although the pH and paCO2 values were within normal hmlts, arterial hypoxaemla was again present Over a period of one hour there was a gradual increase in the paO2, and at 60 minutes it was approaching normal values
A fourth group of 8 pabents were also followed for 60 minutes after operation, but oxygen by nasal catheter (6 to 7 htres per minute) was begun on arrival in the recovery room (Fag 9) These patients again were able to ehmmate carbon dioxide sabsfactonly, and the addlbonal oxygen provided served to maintain a satisfactory oxygen tensaon m most instances

STEPHEN & TALTON I1VI/vIEDIATE PO~TOPI~RATiV E CARE ~;93
po~4 J pCOz
760H 6 0 -
7 5 5 " 55 -
7 5 0 - 50 -
7 4 5 - 4 5 -
7 4 0 - 40-
735- 35-
7 3 0 - 30-
7 25- 25-
7 20- 20-
Oor'n l..covl .,5 Op J Room I_ mln I mlr~ J mblln' ..
D
-,d
i
o~ by. "' Nasal---
Catheter
!pO,, mmHg
I 0
-400
-350
- 3 0 0
-2_50
200
150
- I 0 0
-75
-50
8 PATIENTS
Fzcurm 9 pH, paCO 2, and paO 2 val~es obtained m eight pahents during anaesthesm ~and for 60 minutes postoperahvely Oxygen gwen by nasal catheter Note normal ac:d-base balance and satls- factory oxygen tensions
The oxygen tension values obtained in the recovery room were broken down into age groups In pabents over 50 years of age Who breathed only roo m m r m the recovery room, the paO2 was consistently ]usti over 60 mm Hg (Fig ~0) When pahents of tins age group were given oxygen by mask, more than adequate oxygen tensions were attained, however, with oxyg,'~n by nasal catheter, bg~ely satisfactory tensmns were found (Fig 11) In the age group under 50 )~ears breathmg room air, more adequate oxygen tensr average fell short of the "normal" (Fig 12) Hm
I
oxygen to this group resulted m h:gh oxygen tenslol was by nasal catheter (Fig 13)
ms 'were attained, but, the fever, the admmlstratlop of Is, even w h e n admlmstrgtaon
DLSCUSS:ON
,, The onaus o s to tr s smay arelfew but significant (1)'The normal arterial oxygen tension ~s unknown and may vary from one perscn to
another, depending on Ins physical status and agd (2) The adrmmstraUon of anaesthesia and the performance of surgery lead to a stale of arterial hypoxa, zmla m the nnmedlate postoperative period (3) The redgct~on in arterial oxyger ten- s:on exists m the presence of a minute volume g~s exchange which u s u a y is suftlc~ent to maintain a normal pi t and arterial, car0on dioxide tension (4) The adm]mstratlon of oxygen postoperatively serves to correct the arterial hypoxatemla

594 c.~',~,,_on~N ANZkESTI~TISTtl' SOCIETY JOURNAL
sahsfactonly m most pat!ents It is obvlous,i then, that all patients s[muld recewe oxygen followm g admmlstratmn of g en eral anaesthesm
The natural questmn whmh arises is why pat~ents become hyI3oxaemm follow- mg anaesthesm and operataon The first thoughts that come to mind are the apparent ones assocmted wath resptrator!y depressmn following the use of anaesthetm drugs postoperative pare hmltmg respiratory exchange, or unusual positrons m the operating room leading to madequate ventalatmn These factors cannot be luled out, and one or more of them may play a part m individual patmnts However, an thls group of patients, minute volume and t~dal volume exchange dad not d~ffe[ s~gmficanfly m the ~estmg preoperative and postoperattve permds Also, parenthetmal]y, there was great varmt~on m the resting preopera- tive oxygen tensmn values
The fact that arterial oxygen tensmns were lower m the older age group leads to the possibility that daffuston defects~cross the alveolar membrane may be responsible {or the hypoxaemm Ilame and ~3~shop ~ doubt that tbas explanatmn ~s vahd However, ~t has yet to be ~uled out
I E E
o (3...
3 4 0 -
320 -
3 0 0 -
280 -
260 -
2 4 0 -
220 -
2 0 0 -
180
160 -
1 4 0 -
120 -
D00 -
8 0 -
6 0 -
4 0
ARTERIAL BLOOD
r CE
03 E LO
Room Atr
or"
o ~ -
Artenol Blood P02 Post-0p Age Group Over 50 Yeors
F m u a s 10 Postoperative oxygen tensaons m patmnts over 50 years o~ age who breathed room aar m recovery room
E E
o
-
,520 -
300 -
2 8 0 -
2 6 0 -
2 4 0 -
'220 -
200 -
B O -
1 6 0 -
Q 4 0 -
1 2 0 -
IO0 -
80 -t 60-
40-
ARTERIAL BLOOD
02 by Mosk
i GeE I
~, 0
tu~
4.-
! /
Artenol Blood P02 Post-Op Age Group Over 50 Years
Fm~raE 11 Postoperative oxygen tensions m age group over 50 who breathed first oxygen by mask and then ~recelved oxygen by nasal catheter Note relatavely low oxy- gen tensions associated wlt[l nasal catheter admlmstratmn

S T E P H E N & T A L T O N I M M E D I A T E I~OSTOPF.t]IATIVE C A . I t E 5 ~ 5
- r E E o J
O t~
340
320
300
280
260
240
220
200
180
160
140
120
100 -
8 0 -
6 0 -
4 0
ARTERIAL BLOOD
e-.
g i f )
c -
O 0
t-..
t O
Room h~r
r
I
O
,.- - r
E E E o r
N ~ O:: O Q _
hderml Blood PO 2 Pos'( Op Age Group 17-49 Years
FIGtraE 12 Postoperahve oxygen tensmns m age group under 50 years who breathed room mr m recovery room
!ARTERIAL BLOOD
540 -
.320 -
.300 -
280 -
260 -
240 -
220 -
200
180
~60
t20 -
I00 -
8 0 -
6 0 -
40
0z by Mnsk
, E ~ -
Arterial Blood P()2 Post-Op Age Group~ 20-49 Years
Fm~mE 13 Postoperahve oxygen tensmns an patients under 50 years of age wlho recewed oxygen Note satisfactory values a t all bmes
Bendaxen and colleagues, ~ who have noted consasl oxygen tensmn during and after procedures m winch ]ated w~th "normar' bdal volumes, beheve that the small, mdmry areas of atelectas~s that develop durra, hdal ventflatmn They hypothesize that, unless dee prowded, as the awake person does involuntarily e' logmal shunts develop through whlch blood flows, 1 oxygenated because of the surrounding ateleetatm a could occur m the recovery room, o{ course, where
.ent reductmns m arterial patmnts have been ventl- hypoxaemm results from the course of consistent
? slginng resplratmns are ,ery few minutes, physm- mt whmh cannot become lveoh A similar sxtuab, m the pahent cannot or wall
not take deep breaths In tins respect, the old therap~ of carbon dioxide mha] bons to promote deep breathing may have real m6nt At the present tm analephc drugs are being mveshgated as pharmacol~glc stimulants to prom( deep bleatinng postoperabvely 5 i
Perhaps the most wadely accepted explanation for the arterial hypoxaemla is tll an alteration occurs m the venhiatmn-perfuslon ratios ~)etween gas and perfus~ blood an the lungs 6,7 In older pabents with chest dasease, 1t is recognmed that 1 equahty of ventfiatmn-perfuslon rahos is the commonest cause of arterial oxyg,
a ~
Le,
te
at
n-
~n

596 CANADIAN ANAESTHETISTS' S(~TY JOURNAL
unsaturatlon It is more than likely tI disturb the ventMatlon-perfumon ratio ventilation, most of the inhaled gas winch most of the blood is flowm movement of gas During controlk greater proportion of the gas being t thus upsettmg the ventilation-perfus!on r
Arterial hypoxaemm may also result space, winch alter the ventilatlon-~pert physiological dead space, and the adml
at certain te~hmques of anae~ It l~ known that, during non
r 1 I -- i ,oesl to th e lower lobes of t h, Thq diaphragm plays a W
d re splratlon, wath the drop ,ush, d in goes to the upper p;
lao
~thesm !may hlsa aal sp6ntanelou~ , I l . lung s thro~,g~ tal part m IthlS hragm i qmekt, trts of the l~n~l
irom increases m ph)~s:ologlcal dead aslon ratio Hypotensloh increases I the alstratlon of ethyl etherl and halothane,
by some mechanism as yet unknown, also increases this parameter Tamhn et al s have recently :mpl~cate~ atloplne as a cause of I arterial hypox-
aemm, although they offer no reasons ~or thetr behef A poss!ble explan~taon would be on the basis of atropine mcLreasmg physiological d~ad space ~he findings reported m their paper are ~ot too convincing, m that the oxygen tensions were derived mdtrectly, the ages o,f the patients were not taken into conslderahon, and the varmtlons noted lr~ the oxygen tensions of patients with and ~ thou t administration of atropine w~re ~ot marked ,
It is apparent that the cause o~ ariemal hypoxaemia in the postoperative period is ufiknown it may be a summ~tlon of several factors 19 some patients Nor is the duration of this abnormahty knowaa Much mformataon remains to be collected and interpreted one pred:ets that, with the newer laboratory techmques now available, great activity wall be seen m thts area m the next 10 years
1 The present concept that the "normal" arterial oxygen ten~lon is 100 mm Hg may have to be altered In patients being prepared for elective surgical procedures, the average oxygen tensron Was 80 4 mm Hg
2 In the mamedlate postoperahve period, arterial hypoxaeml~ was preser~t m all patients who were allowed to breathe~ room air At the same time, the i p H and carbon choxlde tens:ons of the arterial blood were within normal hmlts
3 Patients m the age group over 50 showed greater degrees o~ artemal hypox- aemla than those under 50
catheter osto era vel 4 The administration of oxygen by mask or nasal :l P P ~ Y corrected the low arterml oxyge n tenslo~as All patients should r~celve oxygen m the postoperative period
5 The most hkely explanation ror the m tenal hypoxaemla Is a disturbance in the ventflat:on-perfuslon ratio m the h~ngs
1 I1 faut changer le concept actuel que la tension "normale" de l'oxyg6ne art6nel, est de 100 mm de mercure, Chr le,,, malades prepares' ' pour la cinr0rgle electwe, la tenmon moyenne de 1 oxyger~e etalt, de 80 4 mm de rpercure
2 Durant la p6node postop6ratolre e I nmnedlate, 11 y avaltlde lqaypox~mle

STEPHEN & TALTON IMMEDIATE POSTOPEI~_TIVE CARE ~97
'l �9 A trt&lelle chez tous les malades qm resplrment 1 mr de la ~nece Au meme moment[, [e pH et les tensions d'aclde carbomque du sangi artdrlel se tenment dans le~ hmltes de la normale
3 Les malades de plus de 50 ans ont pr~sent~ Une l~ypox6mle artdrlelle plus mportante que ceux de morns de 50 ans
4 L'admxmstrahon d'oxyg~ne par masque ou catheter nasal a corngd |es basses tensmns d'oxyg~ne art&lel Tous les malade,, i, devrment recevolr de ?oxygbne durant la p&mde postop& atolre
5 L'exphcahon la plus vrmsemblable de cette hypoxdmle art&lelle est qu'fi se Drodmt un trouble dans le rapport ventfiahon-perfusmn dans ]es poumons
ACKNOWLEDGMENTS
GIahtude as expressed to Mr Ray Andlews for te~l~hnlcal help and to the Recovery Room nurses for their constant co-operahon
This work was supported m pair by a grant from the A H Robins Co, Rich. mond, Virginia
!-~EFERENCES
1 DmPPs, R D & WATERS, ~:{ M Nursing Care of Surglbal Patients The "'Slar-up" Am J Nursing 41 (May, 1941)
2 LAMBERTSEN, C J Gas Exchanges of the Atmosphere, Lulngs ~,nd Blood Chapter 36~ Medical Phymology, edited by P Bard St Louis C V Molby (]961)
3 RAL~'E, J M & BISHOP, J M A-a D~fference m O~ Ten'lion and Physiological Dead. Space in Normal Man J Appl Phymol i8 284-288 ~May~963)
4 BENDIY~N, H H, HEDLEY-WHYTE, J , • LAVER, M B Impaired Oxygenahon m Surgical Patients during General Anaesthesia with Controlled Venhlahon New Engl ]. Med 269 991-996 (1963)
5 STEPHEN, C R & TALTON, I Inveshgahon of Doxapram as l a Fostanesthetae Resptratory Stimulant Anesth & Analg ( In press )
6 CONWAY, C M & PAYNE, J P Post-operatwe Hypoxaemla I and Oxygen Therapy Bnt Med ] 1 844-845 (1963)
7 WEST, ] B Blood-Flow, Ventllahon, and Gas Exchang( l m the Lung Lancet n 1055-1058 (1963)
8 TA~IL~, P J , CONWAY, C W~, ~ PAYNE, J P Hypoxaeml,!L due to Atropine Lancet 1 14-16 (1964)
Related Documents











