Imaging of CT/MRI Anatomy and tumor extension Radiology department, Tokyo Kita Social Insurance Hospital Ayako Tamura, MD 3D IMAGE-GUIDED ADAPTIVE BRACHYTHERAPY FOR GYNECOLOGY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Imaging of CT/MRI Anatomy and tumor extension
Radiology department, Tokyo Kita Social Insurance HospitalAyako Tamura, MD
3D IMAGE-GUIDED ADAPTIVE BRACHYTHERAPY FOR GYNECOLOGY

1. Normal anatomy of the female pelvis2. Imaging of cervical cancers 3. Cervical cancer staging4. Additional findings
- Uterine body invasion- Ovarian metastasis- Lymph node ( LN ) metastasis
Contents
3
1. Anatomy of the female pelvis

Uterine body- endometrium- Junctional zone (JZ)- myometrium
Uterine cervix- epithelium
(endocervical mucosa)- cervical stroma- myometrium
T2WI sag
Vagina
4Zonal anatomy
T2WI ax
- Vaginal fornix
- vaginal part- supravaginal part

T2WI sag
5Vagina
T2WI ax
- mucosal epithelium and mucous secretion- muscle layer- adventitia surrounding vaginal wall
H-shaped

Plicae palmatae
Abdom Imaging. 34:277-9. 2009
T2WI ax
There is a longitudinal line of hypointensity in the cervical canal. This is a relatively large median longitudinal ridge on the endocervical wall, and can be mistaken for a cervical septum.

T2WI sag
Zonal anatomy is unclear on T1WI because of less contrast.
T1WI sag
7

post contrastpre contrast
Zonal anatomy of the uterus is difficult to be identified.
Endometrium central low density
commonly ovoid or triangular in shape
CT : Uterine body
post contrastpre contrast
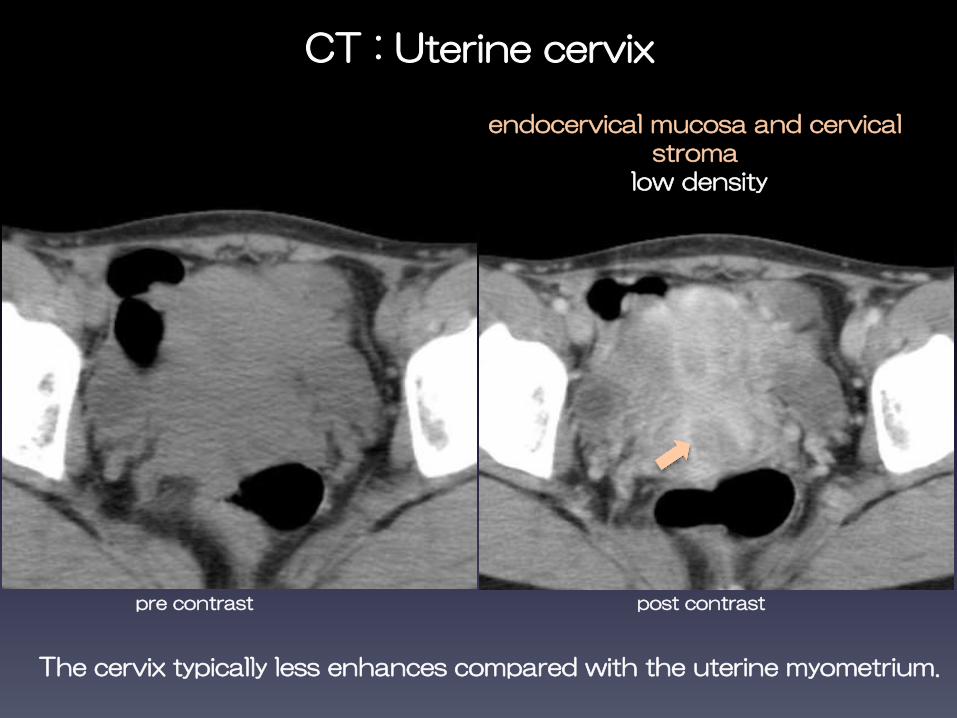
endocervical mucosa and cervical stroma
low density
CT : Uterine cervix
The cervix typically less enhances compared with the uterine myometrium.
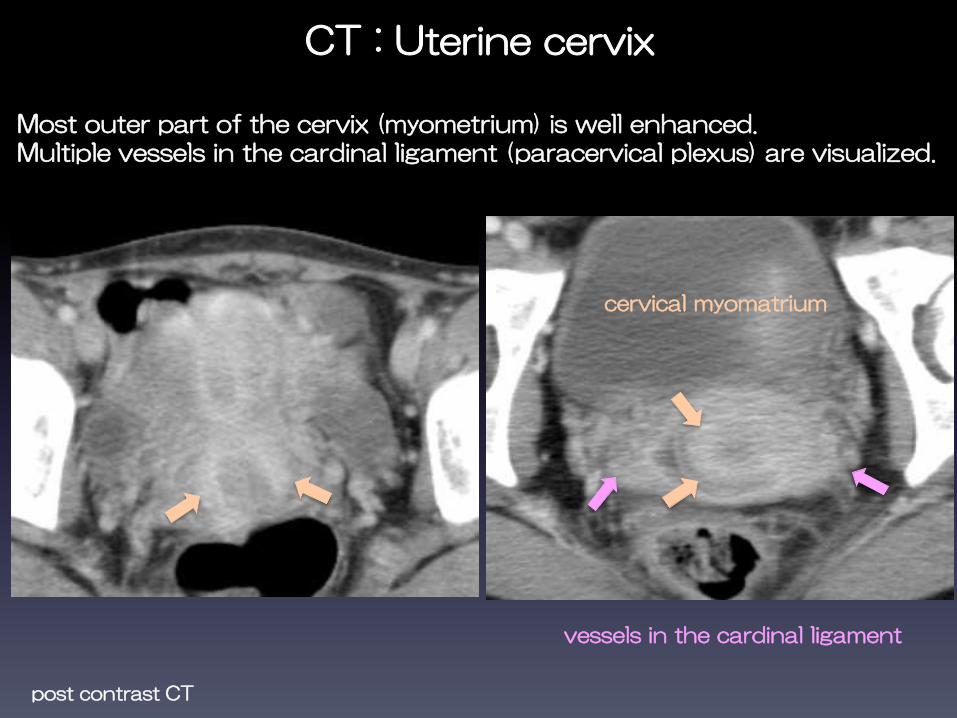
post contrast CT
Most outer part of the cervix (myometrium) is well enhanced. Multiple vessels in the cardinal ligament (paracervical plexus) are visualized.
CT : Uterine cervix
vessels in the cardinal ligament
cervical myomatrium
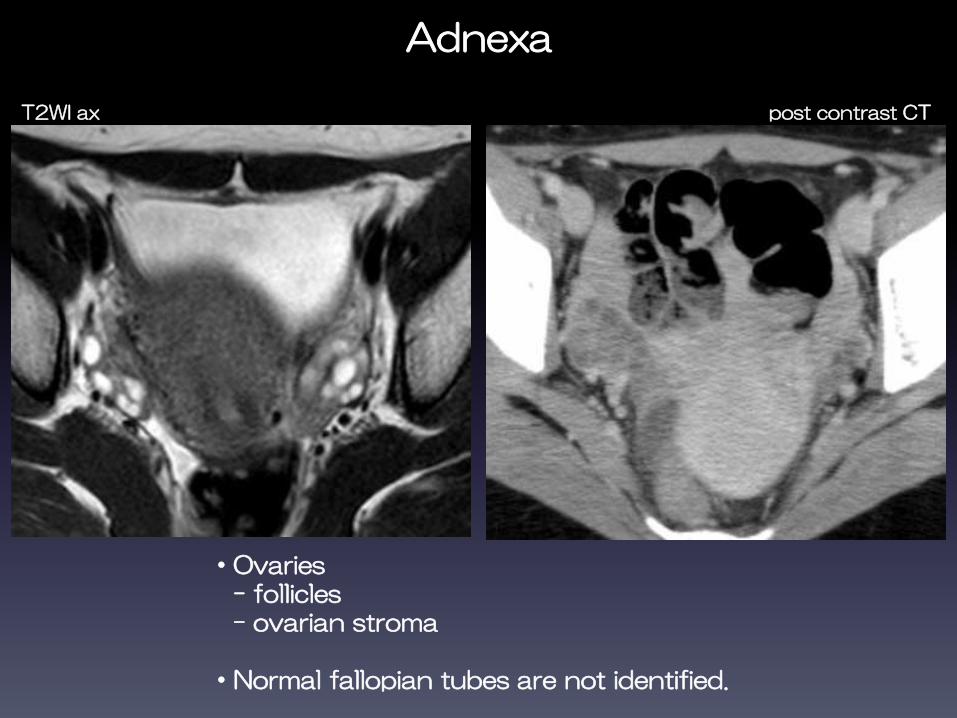
・Ovaries - follicles- ovarian stroma
・Normal fallopian tubes are not identified.
Adnexa 11
T2WI ax post contrast CT
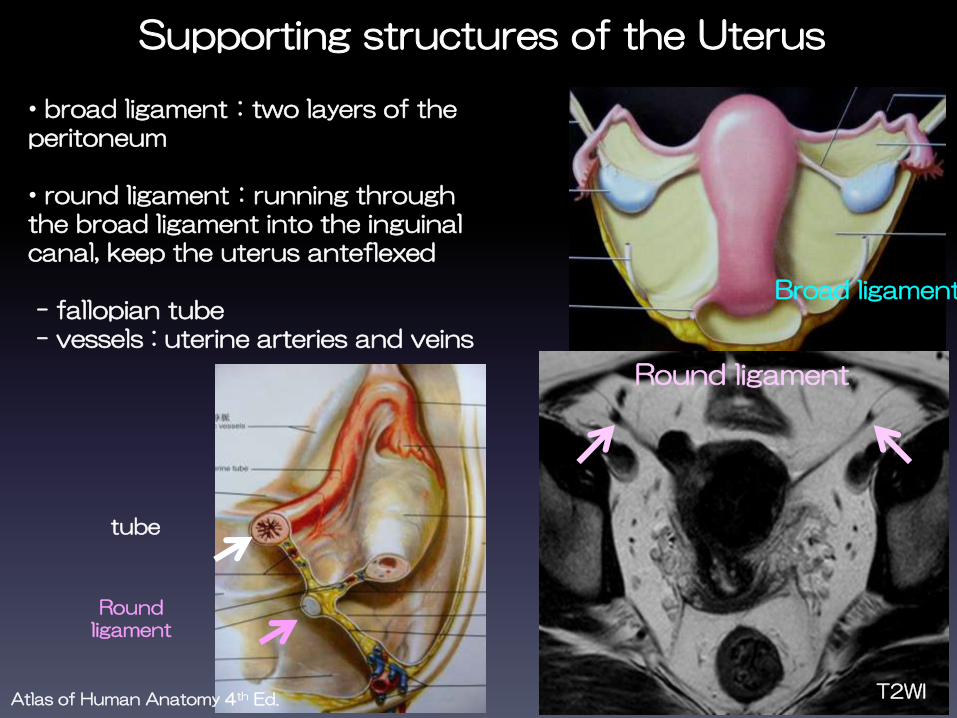
Supporting structures of the Uterus
• broad ligament:two layers of the peritoneum
• round ligament:running through the broad ligament into the inguinal canal, keep the uterus anteflexed
- fallopian tube- vessels : uterine arteries and veins
Round ligament
Broad ligament
Round ligament
tube
T2WIAtlas of Human Anatomy 4th Ed.
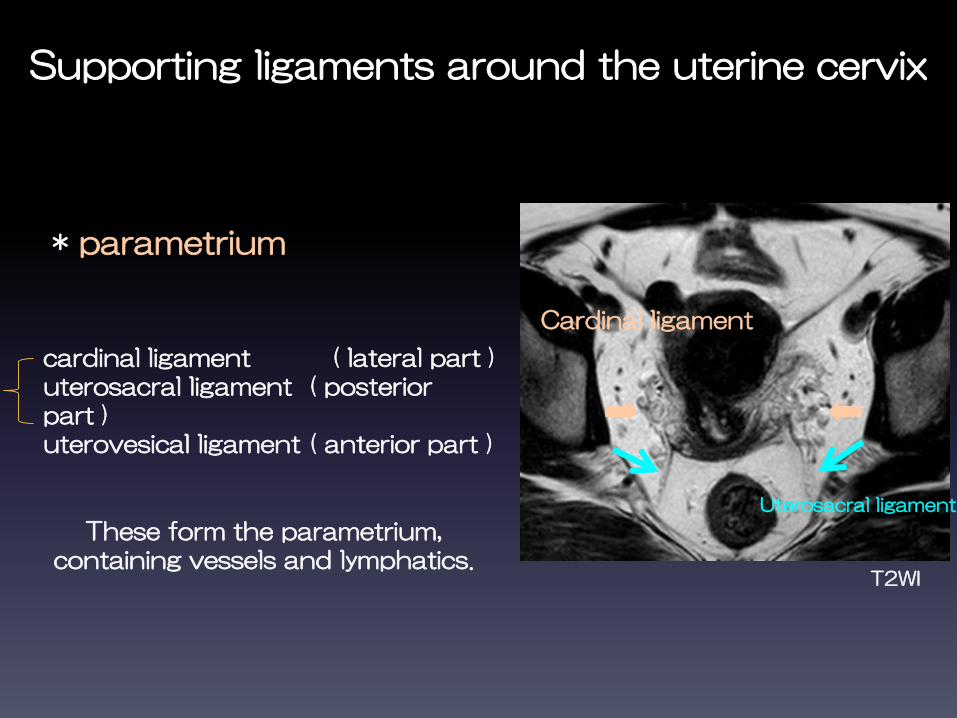
cardinal ligament ( lateral part )uterosacral ligament ( posterior part )uterovesical ligament ( anterior part )
Supporting ligaments around the uterine cervix
Uterosacral ligament
Cardinal ligament
T2WI
13
* parametrium
These form the parametrium, containing vessels and lymphatics.
14
2. Imaging of cervical cancers

Cervical cancer MRI : T2WI
Moderately higher signal intensity (SI) than cervical stroma on T2WI
T2WI sagT2WI ax

Cervical cancer MRI : DWI
Diffusion is usually restricted ( ADC is lower in cervical cancer compared with normal cervical tissue ).
b1000 ADC
Eur Radiol 15 : 71-78, 2005
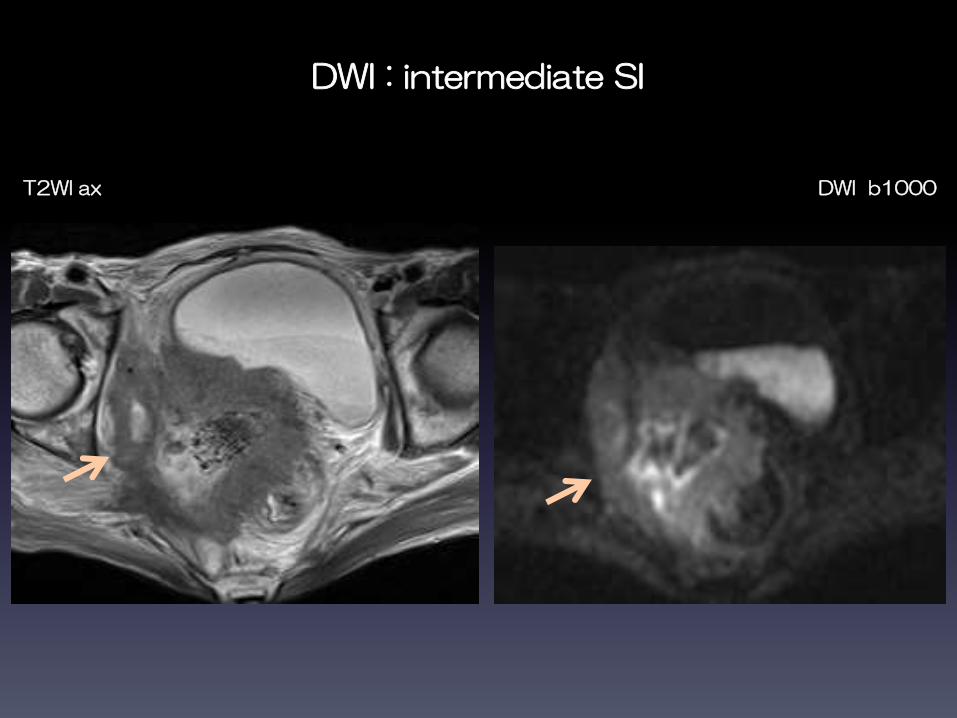
DWI : intermediate SI
T2WI ax DWI b1000
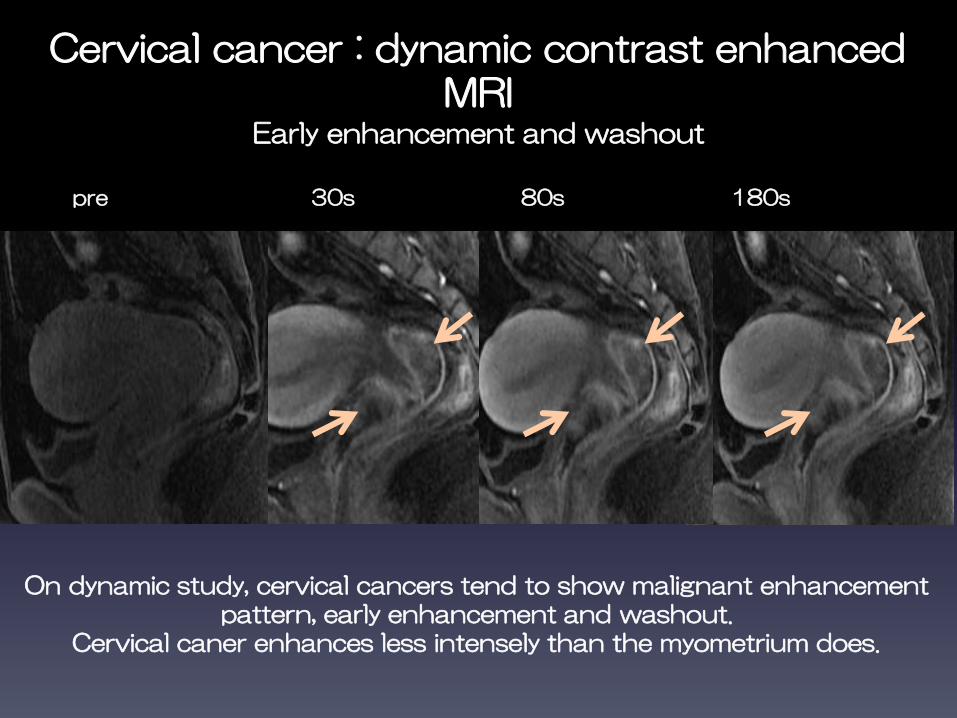
Cervical cancer : dynamic contrast enhanced MRI
Early enhancement and washout
On dynamic study, cervical cancers tend to show malignant enhancement pattern, early enhancement and washout.
Cervical caner enhances less intensely than the myometrium does.
pre 30s 80s 180s
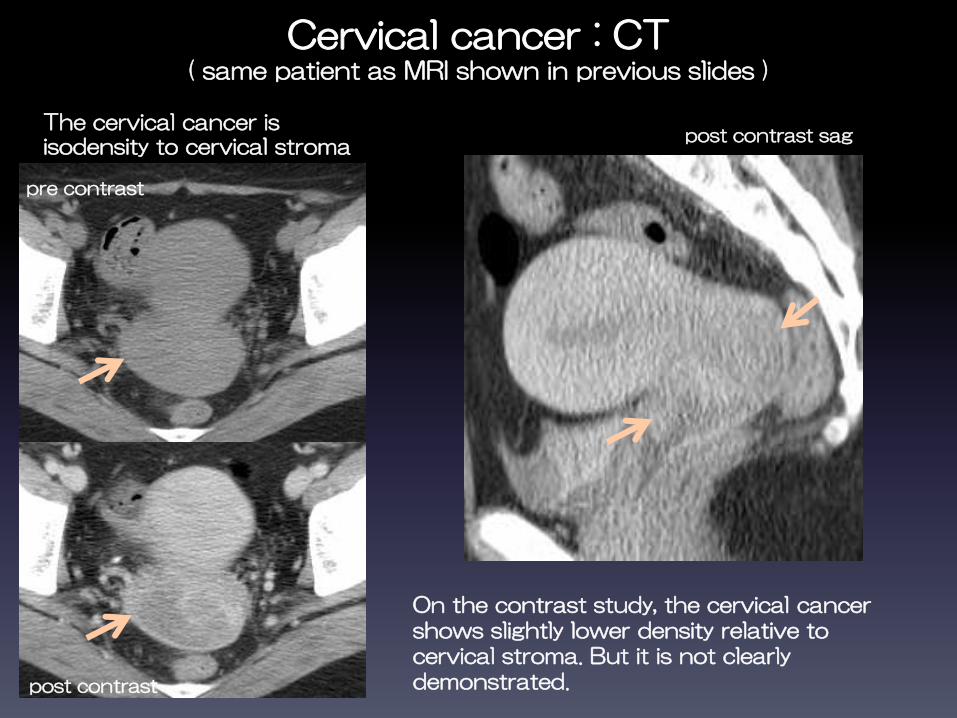
Cervical cancer : CT( same patient as MRI shown in previous slides )
pre contrast
post contrast
post contrast sagThe cervical cancer is isodensity to cervical stroma
On the contrast study, the cervical cancer shows slightly lower density relative to cervical stroma. But it is not clearly demonstrated.

Cervical cancer MRI vs. CT
T2WI ax DWI b1000 contrast CT
CT has limited value in cervical cancer evaluation, especially when it is small, because of the inferior soft tissue contrast compared with MRI.

Uterine cervix : CT
25y normal cervix
Normal uterine cervix sometimes looks large as cervical cancer.
pre contrast
49y with cervical cancer

22
3. Cervical cancer staging
Cervical cancer staging : CT vs. MRI
・MRI is the method of choice for tumor staging and treatment planning. It has a superior accuracy in determining the size and location of the tumor, depth of stromal and parametrial invasion.
・CT is mainly used in the detection of lymphadenopathy and distant metastasis, and for guiding percutaneous biopsies and planning radiation treatment.
MRI is better than CT in cervical cancer staging.
Radiology 175 : 45-51, 1990Cancer 116 : 5093-5101, 2010Gynecol Oncol 91 : 59-66, 2003J Reprod Med. 56 : 485-90, 2011

Cervical cancer : MRI
・T2WI is the most useful sequence in tumor depiction and staging, because it provides optimal contrast resolution between the tumor and the cervical stroma.
・Optional oblique plane images perpendicular to the axis of the endocervical canal may improve staging accuracy.
・The use of dynamic contrast-enhanced MRI in assessing tumor staging is controversial.
Eur Radiol 21 : 1850-1857, 2011
Cervical cancer staging ( FIGO 2008 )

ⅠA:Invasive carcinoma which can be diagnosed only by microscopy not visible on images
ⅠB:Clinically visible lesions limited to the cervix uteri or pre-clinical cancers greater than stage ⅠA
ⅠB1 : ≦ 4.0 cm in greatest dimensionⅠB2 : > 4.0 cm in greatest dimension
The carcinoma is strictly confined to the cervix ( extension to the corpus would be
disregarded )
T2WI
26
ⅠB : Moderately high SI cervical cancers are surrounded by low SI cervical stroma.
Stage Ⅰ
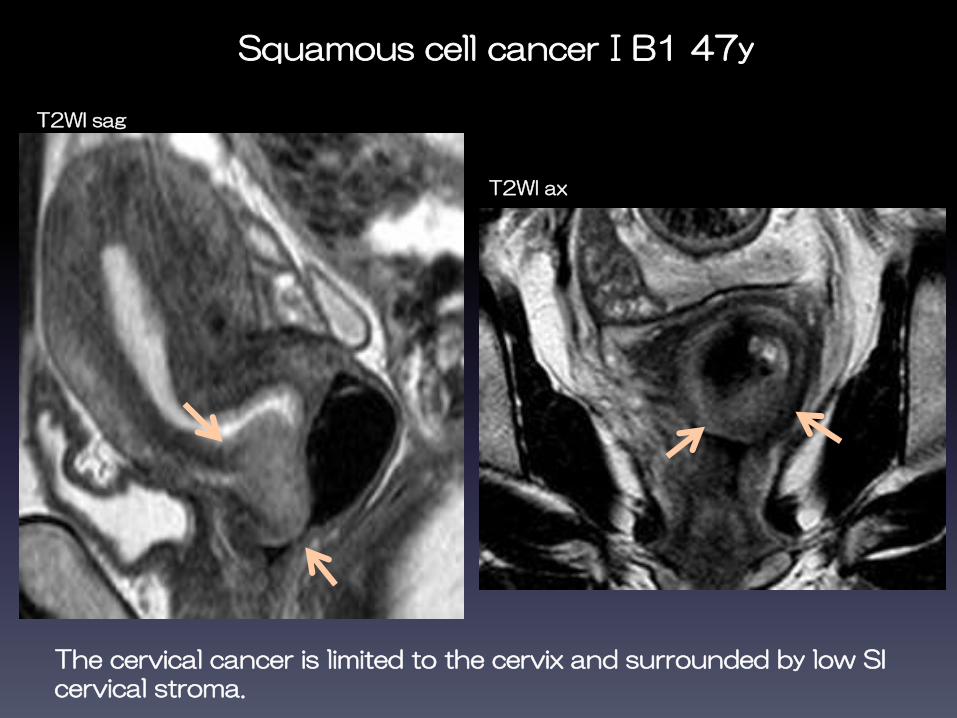
Squamous cell cancerⅠB1 47y
T2WI sag
The cervical cancer is limited to the cervix and surrounded by low SI cervical stroma.
T2WI ax

Adenosquamous cancer ⅠB2 43y
Sagittal T2WI shows a large cervical cancer that protrudes into the upper vagina.Although the tumor is adjacent to the vaginal wall, low SI vaginal wall is intact and the cancer is limited to the cervix.
T2WI sag T2WI ax

Stage Ⅱ
ⅡA : Without parametrial invasionⅡA1 : ≦ 4.0 cm in greatest dimensionⅡA2 : > 4.0 cm in greatest dimension
ⅡB : With obvious parametrial invasion
ⅡADisruption of low SI vaginal wall by high SI tumor.
Stage
Ⅱ
頸部をこえた進展
ⅡBNodular or irregular tumor extension into
the parametrium.
T2WI
29
Cervical carcinoma invades beyond the uterus, but not to the pelvic wall or to the lower third of the vagina
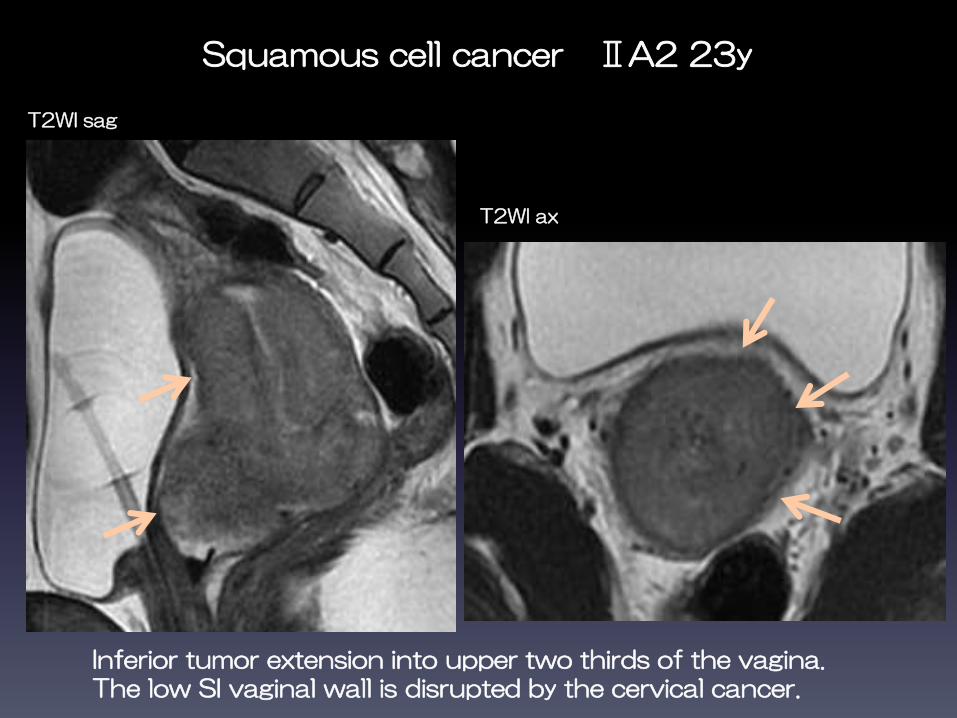
Squamous cell cancer ⅡA2 23y
T2WI sag
T2WI ax
Inferior tumor extension into upper two thirds of the vagina. The low SI vaginal wall is disrupted by the cervical cancer.

ⅠB or ⅡA
ⅠB2 ⅡA2
T2WI sag
Preservation of the normal low SI of the vaginal wall suggests stage ⅠB.When tumor invades to the vagina, the low SI vaginal wall is replaced by high SI tumor.
ⅡB
Obvious parametrial invasion

Squamous cell cancer ⅡB 41y
Disruption of the low SI stromal ring with nodular or irregular tumor SI extension into the parametrium.
T2WI ax

ⅡB : T2WI vs. DWI
Tumor extension into the parametrium is better visualized on T2WI than on DWI.
DWI b1000T2WI ax
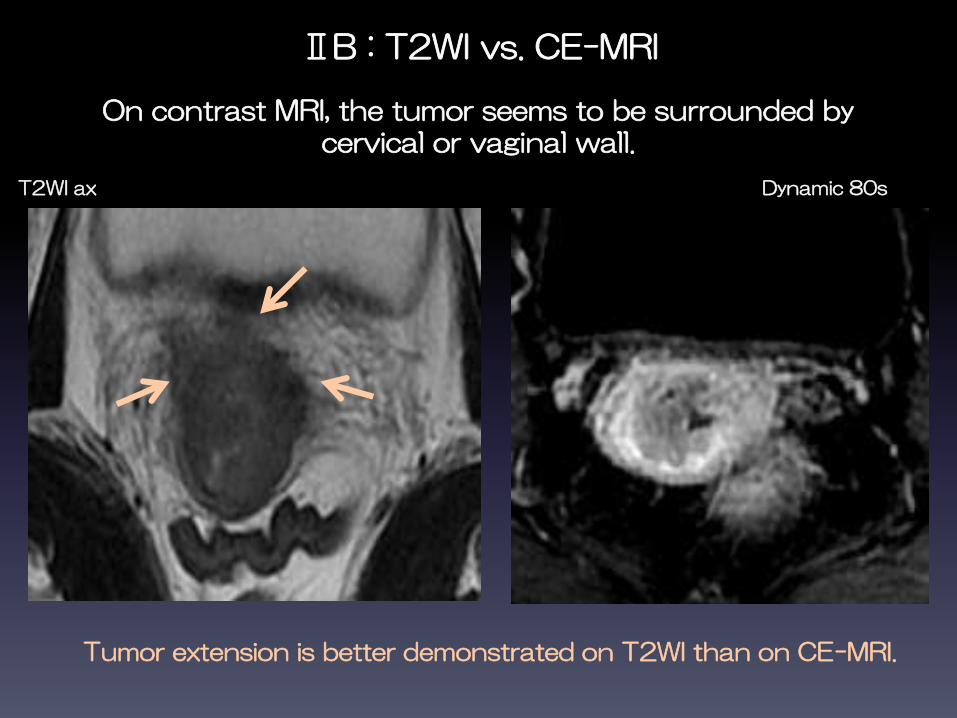
ⅡB : T2WI vs. CE-MRI
On contrast MRI, the tumor seems to be surrounded by cervical or vaginal wall.
Dynamic 80s
Tumor extension is better demonstrated on T2WI than on CE-MRI.
T2WI ax

ⅡB : T2WI vs. CECT
Axial contrast-enhanced CT shows the cervical cancer as a heterogeneous low attenuation mass.There seems to be soft tissue density in the parametrial fat, but indistinct.
CECT
T2WI ax
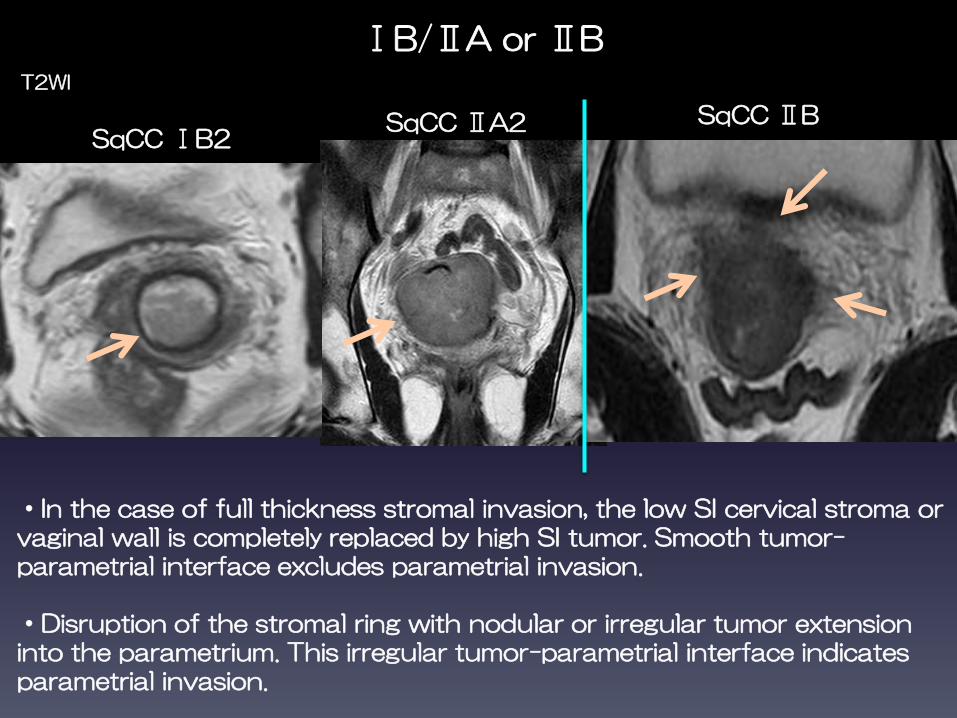
SqCC ⅠB2
T2WI
ⅠB/ⅡA or ⅡB
SqCC ⅡA2 SqCC ⅡB
・In the case of full thickness stromal invasion, the low SI cervical stroma or vaginal wall is completely replaced by high SI tumor. Smooth tumor-parametrial interface excludes parametrial invasion.
・Disruption of the stromal ring with nodular or irregular tumor extension into the parametrium. This irregular tumor-parametrial interface indicates parametrial invasion.
Stage Ⅲ
Stage Ⅲ
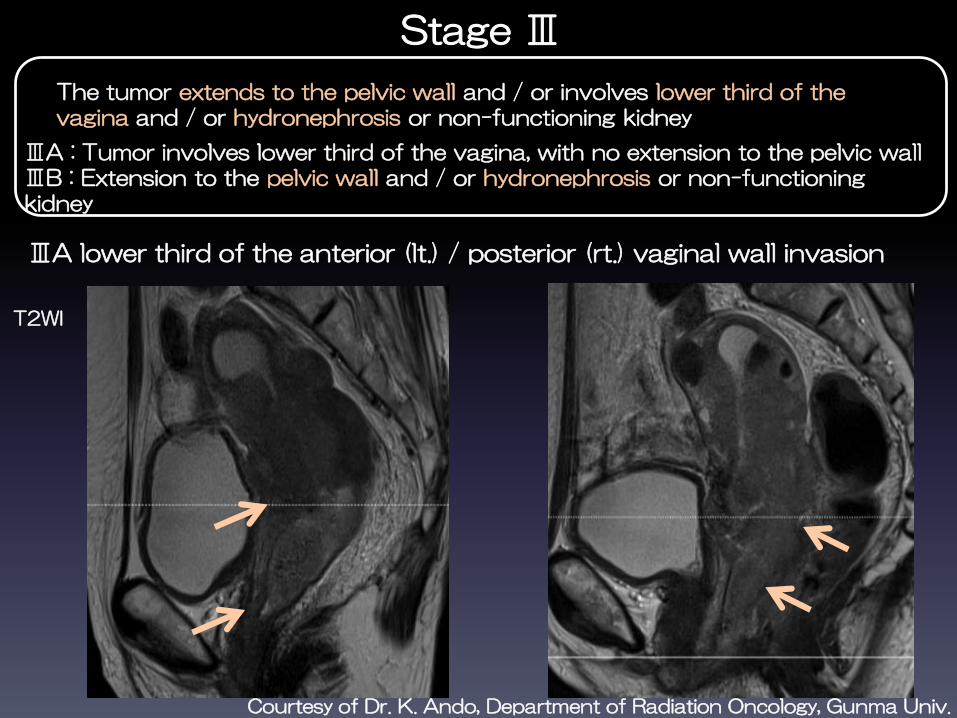
ⅢA : Tumor involves lower third of the vagina, with no extension to the pelvic wallⅢB : Extension to the pelvic wall and / or hydronephrosis or non-functioning kidney
The tumor extends to the pelvic wall and / or involves lower third of the vagina and / or hydronephrosis or non-functioning kidney
T2WI
ⅢA lower third of the anterior (lt.) / posterior (rt.) vaginal wall invasion
Courtesy of Dr. K. Ando, Department of Radiation Oncology, Gunma Univ.

Tumor extension to the left pelvic wall.This is classified as stage ⅢB as well.
IIIB
T2WI ax
Courtesy of Dr. K. Ando, Department of Radiation Oncology, Gunma Univ.
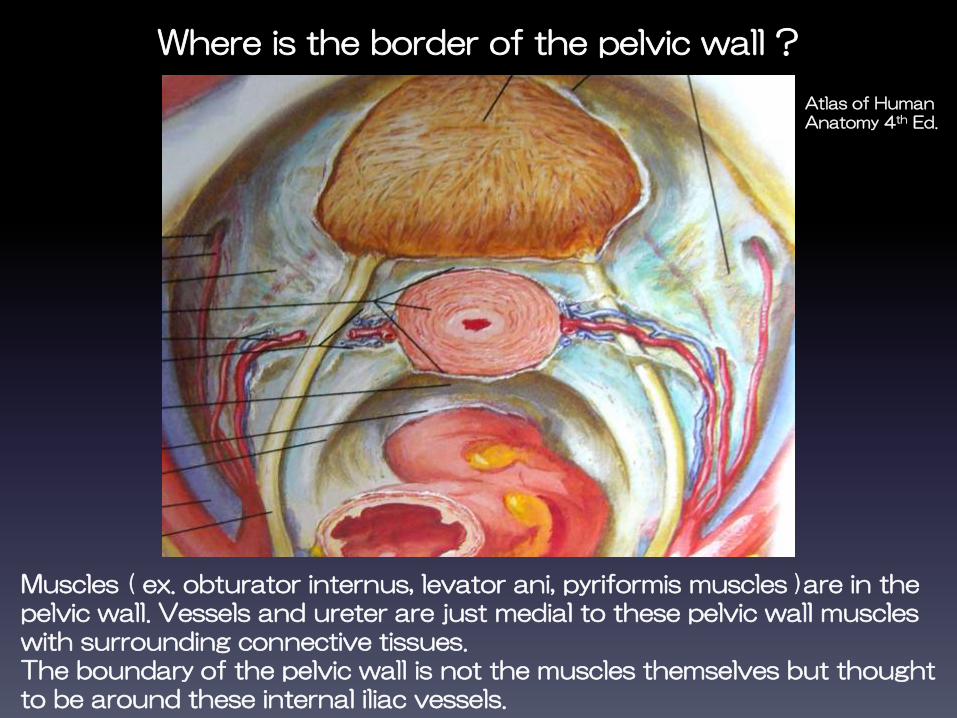
Where is the border of the pelvic wall ?
Muscles ( ex. obturator internus, levator ani, pyriformis muscles )are in the pelvic wall. Vessels and ureter are just medial to these pelvic wall muscles with surrounding connective tissues.The boundary of the pelvic wall is not the muscles themselves but thought to be around these internal iliac vessels.
Atlas of Human Anatomy 4th Ed.

No tumor invasion to the pelvic wall.
post contrast CT
T2WI ax
No fat infiltration around the iliac vessels

Squamous cell cancer ⅢB
Left pelvic wall invasion
T2WI ax CEax
43
Irregular low SI on T2WI and strong enhancement extends around the left internal iliac vessels.

Hydronephrosis ⅢB
post contrast CT
Hydronephrosis is an indication of ureteral invasion. Evaluation of the urinary tract is better on CT than on MRI.
Courtesy of Dr. K. Ando, Department of Radiation Oncology, Gunma Univ.
Stage Ⅳ
45
ⅣA : Spread of the growth to adjacent organsⅣB : Spread to distant organs
The carcinoma has extended beyond the true pelvis or has involved ( biopsy proven ) the mucosa of the bladder or rectum. A bullous edema, as such, does not permit a case to be allotted to stage Ⅳ.

Urinary bladder invasion ⅣA
cystoscopy
T2WI sag
T2WI shows a large cervical cancer invading the posterior urinary bladder wall. Mucosal invasion was proved by cystoscopy.
T2WI ax
Courtesy of Dr. K. Ando, Department of Radiation Oncology, Gunma Univ.
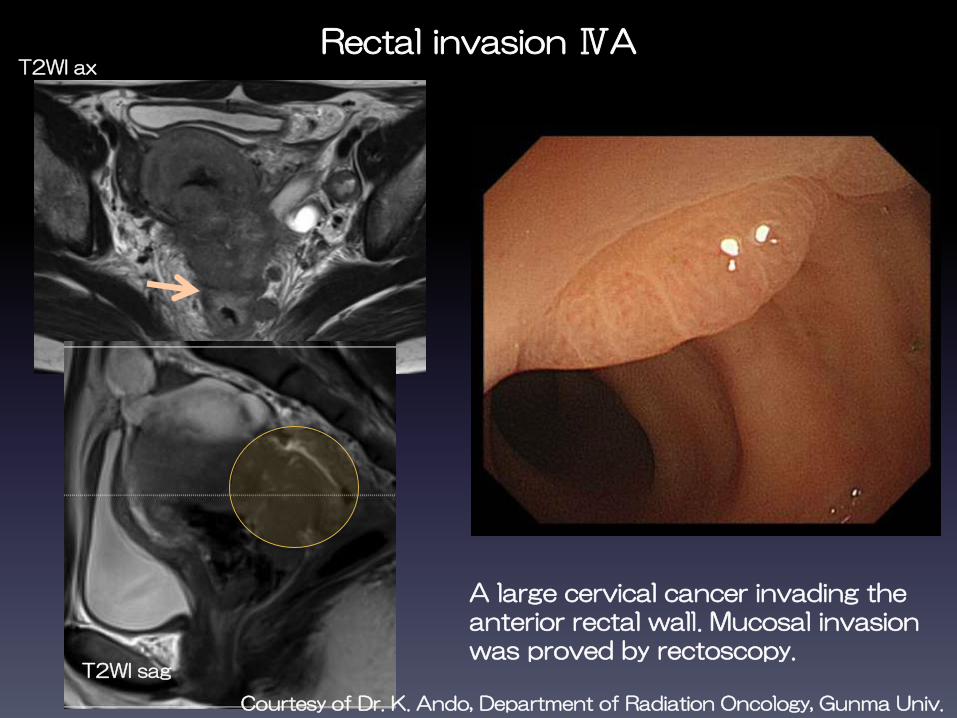
Rectal invasion ⅣAT2WI ax
T2WI sag
A large cervical cancer invading the anterior rectal wall. Mucosal invasion was proved by rectoscopy.
Courtesy of Dr. K. Ando, Department of Radiation Oncology, Gunma Univ.

IVB distant metastasis
Liver metastasis para-aortic LN metastasis
post contrast CT
49
4. Additional findings
- uterine body invasion- ovarian metastasis- lymph node (LN) metastasis
Although these are not the criteria in staging, but closely related to prognosis and affect treatment planning.

Uterine body invasion
Squamous cell cancer ⅡA2 with uterine body invasion, 56y
Dynamic 80sT2WI sag
MRI shows a large cervical cancer that extends and invades to lower uterine body ( also extends into the upper vagina ).

Metastasis to the left adnexa
CEAX DWI b2000
Endocervical mucinous adenocarcinoma ⅡA 46y
dynamic 30s
Heterogeneous strong enhancement is noted in the left ovary. DWI shows slightly high SI. Ovarian metastasis is proved histopathologically.
Ovarian metastasis is rare (ⅠB 0.2%, ⅡB 2%). The frequency is higher in adenocarcinoma than in squamous cell carcinoma.
Gynecol Oncol 101 : 234-236, 2006

Lymph node (LN) metastasis

Lymphatic drainage of the uterus
Main drainage route of the cervical cancer is route 1)
route 1) parametrial LN → pelvic LN → para-aortic LNroute 2) along the ovarian suspensory ligament → para-aortic LNroute 3) along the round ligament → inguinal LN (rare)

Regional LNs of the cervical cancer
Parametrial nodes Obturator nodes
・parametrial nodes・obturator nodes・external iliac nodes・internal iliac nodes・common iliac nodes・sacral nodes
post contrast CT

Para-aortic LN metastasis = distant metastasis = ⅣB
* Mediastinal LN, supraclavicular LN metastases are also distant metastasis
post contrast CT
Assessing LN metastasis
・Microscopic LN metastasis will me missed.・To differentiate enlarged reactive lymph nodes from malignant lymph nodes is difficult.
・The presence of central necrosis and compactly-grouped LNs are likely to be metastasis.・LN metastasis frequency is closely related to advanced stage, tumor size and vascular invasion.
The only accepted criterion is size, short axis dimension ≧ 10mm

Squamous cell cancer ⅡA2 Left obturator node metastasis
T2WI ax
T2WI sag
Left obturator node is enlarged with slightly irregular margin.
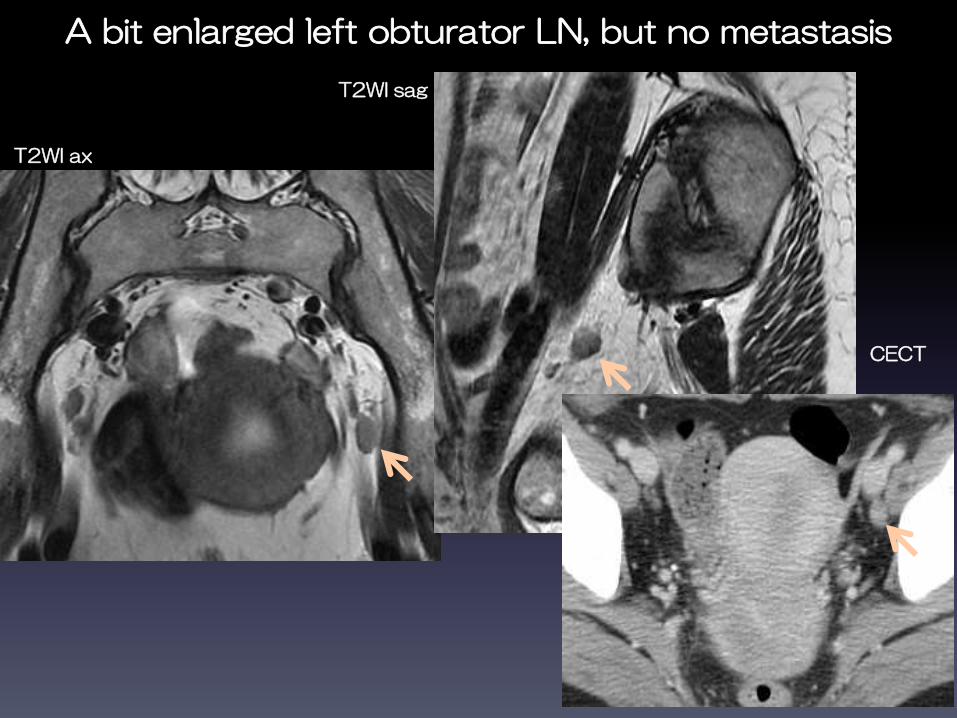
A bit enlarged left obturator LN, but no metastasis
T2WI ax
T2WI sag
CECT
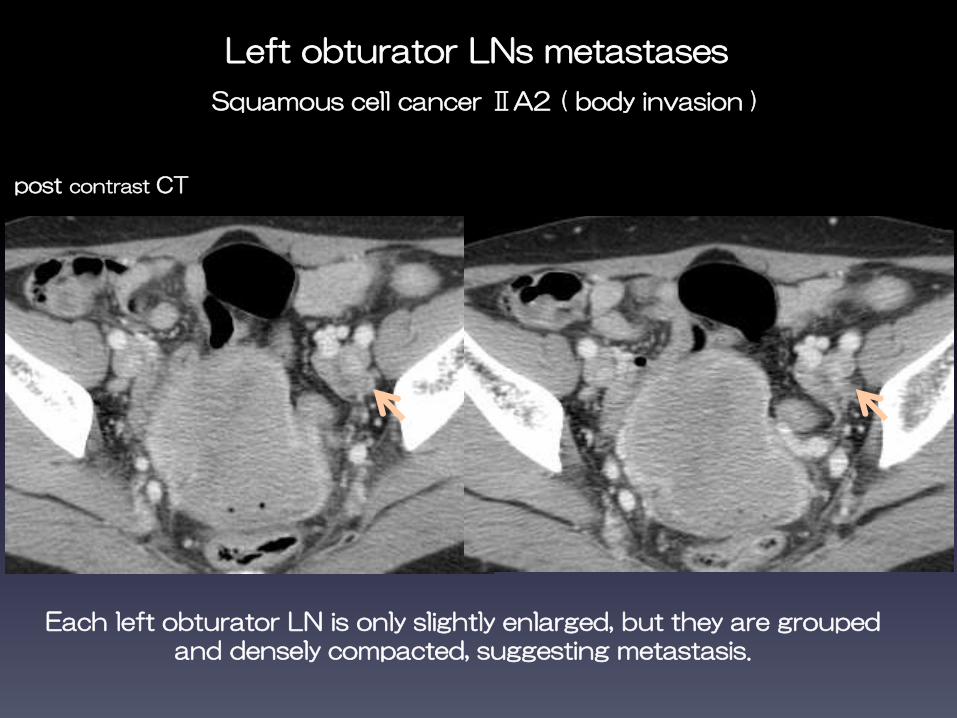
Left obturator LNs metastases
Squamous cell cancer ⅡA2 ( body invasion )
post contrast CT
Each left obturator LN is only slightly enlarged, but they are grouped and densely compacted, suggesting metastasis.

LN metastasis
・CT and MRI have been found to have similar sensitivity and specificity in assessing lymph node metastasis.
・PET-CT (positron emission tomography-computer tomography) is a good modality to evaluate distant metastasis.
・PET-CT also has higher sensitivity (90-91%) and specificity (95-100%) in detection of lymph node metastasis. But regional LN metastasis is not included in staging criteria, and because of the limited spatial resolution of PET and limited soft tissue contrast of CT, the use of PET-CT for local staging of the cervical cancer is currently not routinely recommended.
Gynecol Oncol 91 : 59-66, 2003Gynecol Oncol 97 : 183-191, 2005Cancer Sci 101 : 1471-1479, 2010

Conclusion
・In cervical cancer detection and staging, MRI surpasses CT because of its superior soft tissue contrast.
・MRI can accurately determine tumor size, location, depth of stromal invasion and tumor extension.
・T2WI is the most important sequence for cervical cancer staging.・The use of contrast enhancement in cervical cancer evaluation is controversial.
・The major limitation of CT is the inadequacy in differentiating between tumor, normal cervical tissue and parametrial tissue.・CT is mainly used in the detection of lymphadenopathy, distant metastasis, and for guiding percutaneous biopsies and planning radiation treatment.
Related Documents