Image-Guided Technique in Neurotology Robert F. Labadie, MD, PhD a, * , Omid Majdani, MD b , J. Michael Fitzpatrick, PhD c a Department of Otolaryngology-Head and Neck Surgery, Vanderbilt University Medical Center, 7209 Medical Center East, South Tower, 1215 21 st Avenue South, Nashville, TN 37232, USA b Department of Otorhinolaryngology, Medical University of Hannover, Hannover, Germany, Carl-Neuberg-Str. 1, 30625 Hannover, Germany c Vanderbilt University, 363 Jacobs Hall, 400 24th Avenue South, Nashville, TN 37212, USA If they haven’t already, systems for image-guided surgery (IGS) are com- ing to an operating room near you. IGS systems are already commonplace for sinus surgery and neurosurgery. The appeal of IGS systems is that they allow real-time tracking of current anatomic position on preoperative CT or MRI scans. (Note: IGS systems differ from real-time intraoperative imag- ing, such as CT/OR or MRI/OR suites, where surgically induced anatomic changes are visible.) Although IGS systems do not replace detailed anatomic knowledge, they have been shown to improve outcomes with inexperienced [1] and experienced surgeons [2,3]. The transition of IGS from sinus surgery and neurosurgery to otology/ neurotology has been stalled by the need for a compact system that has ac- curacy at a level suitable for the skull basedon the order of %1 mm. Com- mercially available systems do not achieve this level of accuracy without bone-implanted fiducial markers. Once this level of accuracy is achieved, however, the use of IGS in skull base surgery will have profound implica- tions, including safety control (eg, turning off the drill when a critical boundary is reached), robotic surgery (eg, robotic milling of the mastoid), and minimally invasive surgery (eg, percutaneous cochlear implantation). Before presenting these exciting applications of IGS in otology/neurotol- ogy, we first must understand the basics of IGS systems. This understanding is crucial in being able to appreciate the strengths and weaknesses of IGS. Contained herein is (1) a description of IGS systems focusing on the * Corresponding author. E-mail address: [email protected] (R.F. Labadie). 0030-6665/07/$ - see front matter Ó 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.otc.2007.03.006 oto.theclinics.com Otolaryngol Clin N Am 40 (2007) 611–624

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Otolaryngol Clin N Am
40 (2007) 611–624
Image-Guided Technique in Neurotology
Robert F. Labadie, MD, PhDa,*, Omid Majdani, MDb,J. Michael Fitzpatrick, PhDc
aDepartment of Otolaryngology-Head and Neck Surgery, Vanderbilt University
Medical Center, 7209 Medical Center East, South Tower, 1215 21st Avenue
South, Nashville, TN 37232, USAbDepartment of Otorhinolaryngology, Medical University of Hannover, Hannover,
Germany, Carl-Neuberg-Str. 1, 30625 Hannover, GermanycVanderbilt University, 363 Jacobs Hall, 400 24th Avenue South,
Nashville, TN 37212, USA
If they haven’t already, systems for image-guided surgery (IGS) are com-ing to an operating room near you. IGS systems are already commonplacefor sinus surgery and neurosurgery. The appeal of IGS systems is that theyallow real-time tracking of current anatomic position on preoperative CT orMRI scans. (Note: IGS systems differ from real-time intraoperative imag-ing, such as CT/OR or MRI/OR suites, where surgically induced anatomicchanges are visible.) Although IGS systems do not replace detailed anatomicknowledge, they have been shown to improve outcomes with inexperienced[1] and experienced surgeons [2,3].
The transition of IGS from sinus surgery and neurosurgery to otology/neurotology has been stalled by the need for a compact system that has ac-curacy at a level suitable for the skull basedon the order of %1 mm. Com-mercially available systems do not achieve this level of accuracy withoutbone-implanted fiducial markers. Once this level of accuracy is achieved,however, the use of IGS in skull base surgery will have profound implica-tions, including safety control (eg, turning off the drill when a criticalboundary is reached), robotic surgery (eg, robotic milling of the mastoid),and minimally invasive surgery (eg, percutaneous cochlear implantation).
Before presenting these exciting applications of IGS in otology/neurotol-ogy, we first must understand the basics of IGS systems. This understandingis crucial in being able to appreciate the strengths and weaknesses of IGS.Contained herein is (1) a description of IGS systems focusing on the
* Corresponding author.
E-mail address: [email protected] (R.F. Labadie).
0030-6665/07/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.otc.2007.03.006 oto.theclinics.com

612 LABADIE et al
‘‘accuracy’’ of such systems, (2) a review of the current commercially avail-able systems, and (3) an overview of future applications of IGS in otology/neurotology.
How image-guided surgery systems work
IGS systems are analogous to global positioning systems but on a muchsmaller, local scale. The typical set-up is depicted schematically in Fig. 1.The systems consist of (1) a set of markers on a patient (called ‘‘fiducialmarkers’’ or simply ‘‘fiducials’’), which are present during preoperativeCT or MRI scanning, (2) a computer tracking system used in the operatingroom that aligns the markers in the CT or MRI to the current anatomy andtracks a patient’s fiducial markers within the operating room. For tracking,most systems (eg, BrainLAB, Feldkirchen, Germany; Medtronic, Minneap-olis, Minnesota; and Stryker, Stryker Leibinger, Inc., Kalamazoo, Michi-gan) use infrared technology, whereas one system (GE Medical Systems,Lawrence, Massachusetts) uses electromagnetic field distortion technology.Infrared systems are limited by line of sight, whereas electromagnetic sys-tems are distorted by metal instruments within the surgical field.
Fig. 1. Typical IGS set-up.
613IMAGE-GUIDED TECHNIQUE IN NEUROTOLOGY
Fiducial markers
The key to IGS systems are the fiducial markers. The familiar computeraxiom that holds that ‘‘garbage in equals garbage out’’ is applicable to IGSsystems because the only items visible to the IGS system are the fiducials.Tracking of unknown anatomy depends on actively matching fiducialmarkers in the preoperative scan to those within the operating room. Thismatching requires an accurate determination of the position of each fiducial,a process that is termed fiducial ‘‘localization.’’ Without excellent fiduciallocalization, all anatomic point localization is compromised. Fiducialmarkersrange from neurosurgical N-frames (rarely used given less cumbersomechoices), bone-implanted screws, proprietary head-frames (eg, GE Instatrackhead frame), skin-affixed adhesive markers, contours of surfaces obtained bylaser scanning, and dental-affixed mouthpieces. The requirements for excel-lent fiducials are that (1) they are repeatedly positioned in exactly the samelocation relative to patient anatomy during radiographic imaging and in theoperating room (a flaw for all non–bone-affixed systems), (2) they surroundthe anatomic region of interest, (3) a sizeable number of markers is used,and (4) they can be accurately localized.
Why are fiducial markers the key? Fiducial markers are the only things vis-ible to the IGS system. Everything else depends on them. Once a CT or MRIscan is loaded into the IGS computer, the operator finds the same fiducialmarkers on the patient in the operating room, and the computer’s job is toalign/superimpose the fiducial markers from the CT or MRI scan to thosefound in the operating room. To the extent that the anatomy is rigid, fiducialalignment ensures that the anatomy, including surgical targets, is also aligned.This process is called ‘‘registration.’’ This important process deserves a precisedefinition: Registration is the alignment of anatomic points from the radio-graphic scan (eg, CT or MRI) with their true positions in the operatingroom. This process is schematically illustrated in Figs. 2–4.
Error within image-guided surgery systems
Asone can imagine, error is inherent to the process.Although not often dis-cussed in brochures or advertisements, an engineering standard does exist inanalysis of IGS. This analysis assigns error to each step of the process, asshown in Fig. 4. First is ‘‘fiducial localization error’’ (FLE), which is the errorin identifying the positions of the fiducial markers in the radiographic images(FLErad) and in the operating room (FLEOR). Contributions to FLErad
include the resolution of the CT or MRI scan, image distortion of the scan,and noise in the scan. Components of FLEOR include human error in identi-fying the fiducial markers and error inherent in the tracking system. Overall,FLE represents the error in finding the fiducial markers. In an ideal world, thelocation of fiducialmarkers could be determined perfectly; given the imperfec-tions of the real world, however, this rarely happens. Thus FLE is rarely zero.When fiducial locations are imperfectly determined, alignment of the markers

614 LABADIE et al
from the radiographic study to the operating room is also imperfect. Theresultant error in aligning fiducial markers is termed ‘‘fiducial registration er-ror’’ (FRE) and is graphically depicted in Fig. 4. To minimize this error,a mathematical best-fit algorithm is used to minimize the differences betweenthe corresponding image and patient fiducials. (Most systems use a strategythat minimizes the sum of the squares of the distances between fiducialmarkers). The FRE or a derivative of it is the number typically displayedon IGS systems after registration as an indication of the goodness of fit.
Only after registration is done can IGS tracking begin. Once tracking isinitiated, the surgeon identifies a point of anatomic interest. The difference
Correspondingfiducial markers
OperatingRoom
RadiographicImage
surgical target
Fig. 2. Fiducial markers (rectangles) can be seen on the surface of the patient in the radio-
graphic image (left) and in the operating room (right). Also shown is the surgical target (small
oval in the midst of the larger oval), which we are interested in identifying with IGS.
OperatingRoom
RadiographicImage
REGISTRATION:align corresponding
fiducials
Fig. 3. Registration. Corresponding fiducial markers are actively aligned in registering the ra-
diographic image of the patient to the actual patient in the operating room. The active aligning
of the fiducials is paramount in passively aligning all other tissue, including the surgical target
(small oval within larger oval).

615IMAGE-GUIDED TECHNIQUE IN NEUROTOLOGY
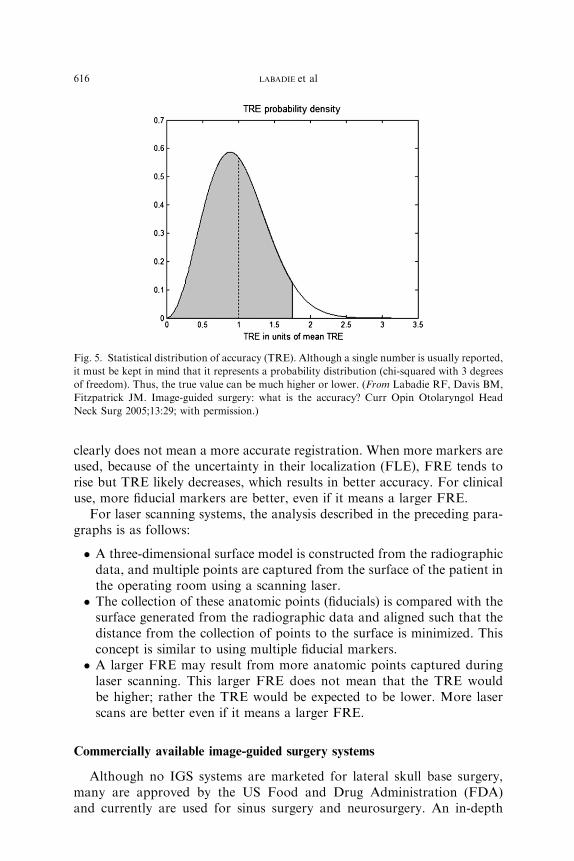
between where the IGS system says the anatomy is located and its trueposition is termed ‘‘target registration error’’ (TRE)dthe accuracy of thesystem. TRE and FRE each statistically depend on FLE via relationshipsthat are beyond the scope of this article. (The interested reader is directedto Fitzpatrick and colleagues [4].) An important point to remember is thatTRE for a system is not well described by a single number but rather a sta-tistical distribution. When one states that the accuracy of a system is 1 mm,what is actually being implied is that the average accuracy of the system is 1mm, but the accuracy may in fact be higher or lower at any particular time.(The statistical distribution is a chi-squared distribution with 3 degrees offreedom [Fig. 5]). When comparing systems, the TRE within the anatomicregion of interest should be compared.
A common misconception is that lower FRE means a more accurate reg-istration, which is not necessarily true. Although most systems have a thresh-old below which FRE must fall to proceed with IGS, lowering FRE furtherbelow this threshold does not mean higher registration accuracy. Some au-thors have called for removal of fiducial points from the registration tolower FRE [5]. This approach is dangerously flawed. Although FRE tendsstatistically to decrease with fewer fiducials, error in target alignment(TRE) tends to increase [6]. Because FRE can be observed directly, it istempting to removal fiducials to see a reassuringly smaller error value dis-played on the IGS screen, but the chances are great that removing themwill increase the error that countsdthe error in hitting the target (ie,TRE). Many examples can be given to illustrate this effect, but the simplestis the case of one fiducial. When only one fiducial is used, FRE may be easilyreduced to zero, but as is depicted in Fig. 6, a zero fiducial registration error
OperatingRoom
RadiographicImage
Fiducial Localization Error(FLErad)
Fiducial Localization Error(FLEOR)
Fiducial Registration Error(FRE)
Target Registration Error (TRE)(a.k.a. ACCURACY)
Fig. 4. Error analysis for IGS. Error occurs when identifying fiducials in the radiographic im-
age (FLErad) and when identifying fiducials in the operating room (FLEOR). Error also occurs
when aligning the fiducials (FRE). The accuracy of the system is the error in finding surgical
targets (TRE). TRE and FRE depend on FLE. The keys to IGS are the fiducial markers.
616 LABADIE et al
clearly does not mean a more accurate registration. When more markers areused, because of the uncertainty in their localization (FLE), FRE tends torise but TRE likely decreases, which results in better accuracy. For clinicaluse, more fiducial markers are better, even if it means a larger FRE.
For laser scanning systems, the analysis described in the preceding para-graphs is as follows:
� A three-dimensional surface model is constructed from the radiographicdata, and multiple points are captured from the surface of the patient inthe operating room using a scanning laser.� The collection of these anatomic points (fiducials) is compared with thesurface generated from the radiographic data and aligned such that thedistance from the collection of points to the surface is minimized. Thisconcept is similar to using multiple fiducial markers.� A larger FRE may result from more anatomic points captured duringlaser scanning. This larger FRE does not mean that the TRE wouldbe higher; rather the TRE would be expected to be lower. More laserscans are better even if it means a larger FRE.
Commercially available image-guided surgery systems
Although no IGS systems are marketed for lateral skull base surgery,many are approved by the US Food and Drug Administration (FDA)and currently are used for sinus surgery and neurosurgery. An in-depth
Fig. 5. Statistical distribution of accuracy (TRE). Although a single number is usually reported,
it must be kept in mind that it represents a probability distribution (chi-squared with 3 degrees
of freedom). Thus, the true value can be much higher or lower. (From Labadie RF, Davis BM,
Fitzpatrick JM. Image-guided surgery: what is the accuracy? Curr Opin Otolaryngol Head
Neck Surg 2005;13:29; with permission.)
617IMAGE-GUIDED TECHNIQUE IN NEUROTOLOGY
review of the accuracy of such systems was performed for a prior publica-tion [7] and is repeated in this article with permission from the publisher.
The four leading commercial IGS systems used for sinus surgery are (inalphabetical order):
BrainLAB system (BrainLAB, Feldkirchen, Germany)InstaTrak System (GE Medical Systems, Lawrence, Massachusetts)LandmarX and StealthStation system (Medtronic, Minneapolis,
Minnesota)StrykerImage Guidance System (Stryker Leibinger, Kalamazoo,
Michigan)
For each of these systems, the literature was reviewed to find the mostrelevant article reporting accuracy of the system. Each company was con-tacted to determine whether the cited study was the most up-to-date regard-ing error analysis.
BrainLAB
For the BrainLAB system, no error studies could be identified specifically forsinus surgery, but such work has been done for neurosurgical applications,which use similar fiducials and registration methods. In a study performed attheUniversity of Regensburg, Germany, error analysis for 36 patients undergo-ing intracranial surgery was performed [8]. FRE using skin-affixed fiducial
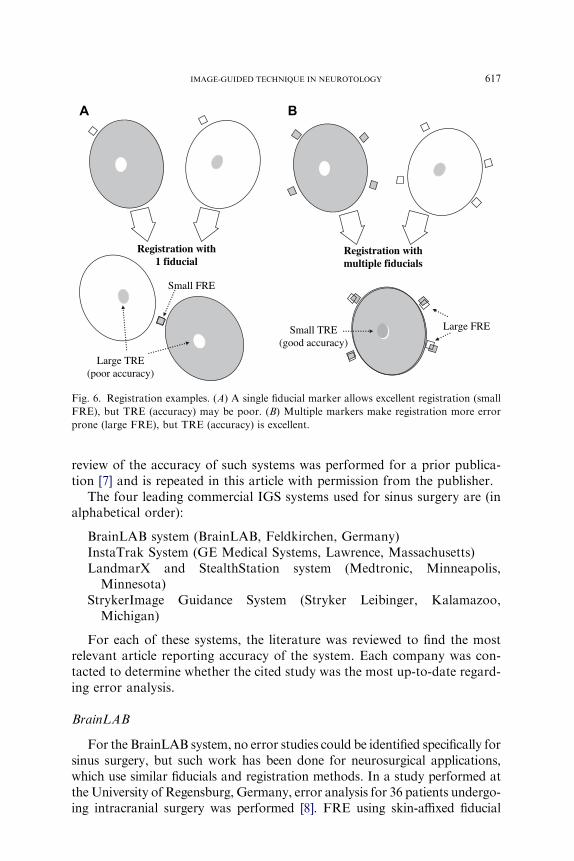
Small TRE(good accuracy)
Small FRE
Large FRE
Large TRE(poor accuracy)
Registration withmultiple fiducials
Registration with1 fiducial
A B
Fig. 6. Registration examples. (A) A single fiducial marker allows excellent registration (small
FRE), but TRE (accuracy) may be poor. (B) Multiple markers make registration more error
prone (large FRE), but TRE (accuracy) is excellent.

618 LABADIE et al
markers was reported as 1.10� 0.53 mm; using laser skin contouring, FREwasreported as 1.36 � 0.34 mm. TRE was calculated by comparing a skin-affixedmarker on the patient with that location in the corresponding radiographic im-age; for the skin-affixed marker registration, TRE was reported as 1.31 � 0.87,and for laser skin contouring, TRE was reported as 2.77 � 1.64 mm.
InstaTrak
For the InstaTrak System, a multicenter, multisurgeon study was per-formed and published in Laryngoscope in 1997 [9]. In this study, registrationwas performed either with six skin-affixed markers or a proprietary headset.TRE was measured using two skin-affixed targets placed on the lateral rightand left supraorbital rims. FRE was not reported. For the skin-affixed fidu-cial registration, a TRE of 1.97 mm with a 95% CI, of 1.75 to 2.23 anda maximum value of 6.09 mm was reported. For the headset registration,a TRE of 2.28 mm with a 95% CI, of 2.02 to 2.53 and a maximum valueof 5.08 mm was reported.
LandmarX
For the LandmarX system, Metson and colleagues [10] performed a pro-spective study of 34 physicians performing 754 sinus cases over a 2.5-yearperiod. Using five anatomic key points as fiducials (these points are unde-fined), they reported ‘‘mean accuracy of anatomical localization at the startof surgery was 1.69 � 0.38 mm (range, 1.53 � 0.41 mm to 1.79 � 0.53 mm).’’Although the specific methods are not given, this study seems to reportFLEdthe error associated with repeated identification of the fiducialsdand not TRE. Hence the question mark in Table 1.
Stryker
The Stryker ImageGuidance Systemwas evaluated prospectively on 50 pa-tients undergoing anterior cranial base surgery by Snyderman and colleagues[5]. Each patient had ten skin-affixed fiducials placed over the scalp, lateralface, and mastoid. TRE was not measured in this study. Rather, the authorsreported the error within zone of accuracy, which is an estimate of TRE basedon FRE performed by an algorithm proprietary to Stryker. They reported fortheir clinical applications that the Stryker system estimates that in a zone ofaccuracy, which it demarcates in image space, it has achieved a TRE !2mm. The authors visually validated the registrations, but they reported noindependent error measurements to check these estimates.
Applications of image-guided surgery in otology/neurotology
Within our literature there are limited references to the clinical use of IGS.(Excluded from the current discussion is the use of IGS for virtual training; eg,virtual temporal bone trainers.) Use of IGS clinically has been limited to

619IMAGE-GUIDED TECHNIQUE IN NEUROTOLOGY
confirmation of anatomic identity during surgery. The first published clinicalreference was in 1997, when Sargent and Buccholz [11] reported on the use ofIGS for middle cranial fossa surgery. In 2003, Caversaccio and colleagues [12]reported on the use of IGS during aural atresia drill-outs, stating that itreduced operative time and potentially could reduce morbidity. Also in2003, Raine and colleagues [13] reported on the use of IGS in guiding deepdrilling during split electrode cochlear implant placement.
It is surprising to the authors that IGS has not been exploited more byotologists/neurotologists given (1) the extensive use by neurosurgeons thatshows more complete disease resection in less operative time [2,3] and min-imally invasive surgery for placement of deep brain stimulators [14], (2) thelarge numbersdupwards of 100,000 mastoidectomies per yeardof otologicprocedures performed annually in the United States [15], (3) projections thatIGS will be a part of operating rooms of the future [16], and (4) predictionsthat IGS offers an area of advancement of our field [17]. Areas in which IGSmay have large impact on otology/neurotology include (1) safety constraintsregarding surgical tool control, (2) robotic surgery, and (3) minimally in-vasive surgery, such as percutaneous cochlear implantation.
Safety controls
Perhaps the most practical application of IGS is increased safety control.In otology/neurotology, in which the surgical field is encased in rigid bone,the use of IGS to define boundaries and prevent transgressions has greatappeal. Two groups have been working on this, including the authors [18]and a group from Germany [19].
Table 1
TRE for commercially available otolaryngologic IGS systems
IGS system Manufacturer TRE (mm) Fiducial Author/reference
BrainLAB BrainLAB,
Feldkirchen,
Germany
1.31 � 0.87
2.77 � 1.64
Skin-affixed
markers
Laser skin
contour
Schlaier, 2002 [8]
InstaTrak GE Medical
Systems,
Lawrence,
MA
2.28 � 0.91 Proprietary
headset
Fried, 1997 [9]
LandmarX Medtronic,
Minneapolis,
MN
1.69 � 0.38 (?) Skin-affixed
markers
Metson, 2000
[10]
Stryker
Navigational
System
Stryker
Leibinger,
Inc.,
Kalamazoo,
MI
!2 mm
‘‘zone of
accuracy’’
Skin-affixed
markers
Snyderman, 2004
[5]
Data from Labadie RF, Davis BM, Fitzpatrick JM Image-guided surgery: what is the
accuracy? Curr Opin Otolaryngol Head Neck Surg 2005;13:27–31

620 LABADIE et al
The concept is simple: define the boundaries of the surgical field (eg, teg-men, sigmoid, external auditory canal, facial nerve, labyrinth), track the po-sition of the drill, and turn it off when the drill approaches vital anatomy.Although both groups have limited experimentation in nonhuman models,volumetric speed of drilling is increased using such IGS-controlled drillcut-off, especially for inexperienced surgeons.
Robotic mastoidectomy
Robots have been used in operating theaters for more than 20 years.Their advantages are many, including reliability, repeatability, and lack oftremor. Probably best known is the da Vinci Surgical System (IntuitiveSurgical, Sunnyvale, California), which has been cleared by the US FDAfor laparoscopic procedures [20]. The daVinci system is considered a ‘‘mas-ter–slave’’ system, meaning that the robot mimics the surgeon’s motions,eliminating tremor and miniaturizing motions. It acts as an extension ofthe surgeon and depends on the surgeon performing the procedure. In con-trast to master–slave robots, autonomously acting robots offer the potentialof replacing the surgeon for at least portions of surgical procedures. Auton-omous robots have use in several surgical applications in which the proce-dure can be planned a priori. The FDA-approved ROBODOC (IntegratedSurgical Systems, Davis, California) is an example of an autonomous robotused to perform a component of total hip replacement surgery [21,22].(Note: Novatrix Biomedical Inc., San Clemente, California, has an agree-ment of purchase for Integrated Surgical Systems at the time of this writing.)To use this system, the surgeon first locates fiducial markers attached to thefemur and visible in the CT scan. The ROBODOC system then registers thepreoperative CT scan with the surgical anatomy and plans an optimalmilling of the femur for placement of a prosthetic shaft. The robot alignsitself to the optimal trajectory and drills a cylinder of specified diameterand depth.
In otologic surgery, autonomous robots have been used to surface millthe temporal bone to a depth of 4.5 mm to create a receiving well for theinternal processor of a cochlear implant device [23]. Recently, our group ex-tended this work with the goal of performing a robotic mastoidectomy. Toaccomplish such a task we have built an open-architecture, autonomous ro-bot and incorporated it with an IGS system. Preliminary studies with thissystem show that it can drill the volume of a mastoid cavity repeatedly inapproximately 4 minutes. Given the ‘‘x-ray vision’’ afforded by IGS, thetypical strategy of visual identification of mastoid boundaries may be re-placeable by more effective edge routing techniques, which remove the mas-toid en bloc. Note that such a system is not intended to replace the surgeon.Rather it is intended to carry out low-level milling and allow the surgeon toconcentrate on the high-level tasks of fine drilling on vital structures (eg,facial nerve, internal auditory canal).

621IMAGE-GUIDED TECHNIQUE IN NEUROTOLOGY
Minimally invasive surgery: percutaneous cochlear implantation
Perhaps the most powerful aspect of IGS applied to otology/neurotologyis the concept of truly minimally invasive surgery. The authors from Van-derbilt have been working on the concept of minimally invasive surgery asapplied to cochlear implantation for the past 5 years [24,25]. The authorfrom the University of Hanover also has been performing similar work [26].
The concept (Fig. 7) is to use radiographic guidance to drill directly fromthe surface of the skull to the cochlea without injuring vital structures. Toachieve the necessary accuracy in avoiding the facial nerve, bone-implantedfiducials are placed around the temporal bone. Initial efforts were performedfree-hand, analogous to the way functional endoscopic sinus surgery is cur-rently performed [24]. Majdani and colleagues [26] reported a similar ap-proach using robots. Extensions of this work include automated pathsconstrained by drill guides [25]. After CT scanning, a proposed drill pathis predicted using a computer program. If the surgeon accepts the proposedpath, an electronic plan is sent for rapid prototyping of a drill guide, whichmounts on the bone-implanted fiducials and constricts the motion of thedrill to pass through the facial recess and intersect the basal turn of the
Fig. 7. The concept of percutaneous cochlear implant. With IGS, a path from the lateral cortex
of the mastoid to the cochlea avoiding vital structures (eg, the facial nerve) can be planned.
(From Labadie RF, Choudhury P, Cetinkaya E, et al. Minimally-invasive, image-guided, facial
recess approach to the middle ear. Otology Neurotology 2005;26:560; with permission.)
622 LABADIE et al
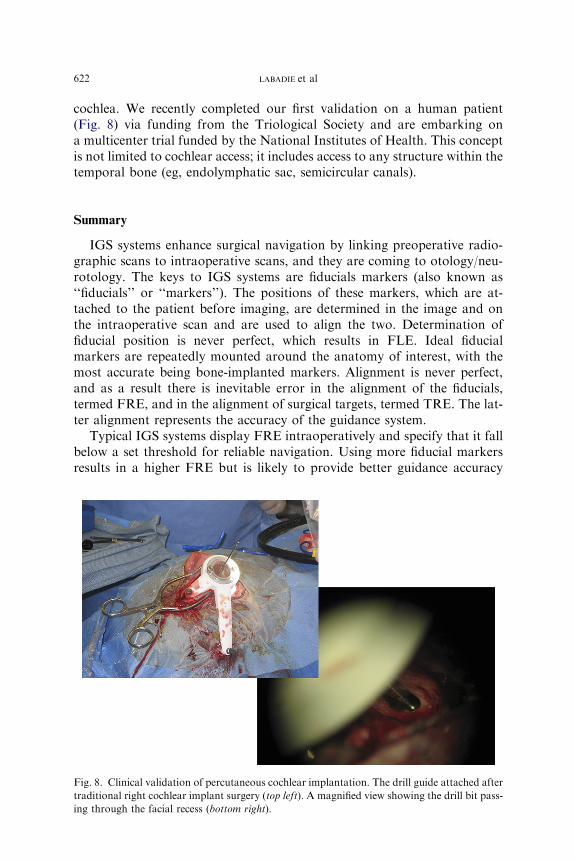
cochlea. We recently completed our first validation on a human patient(Fig. 8) via funding from the Triological Society and are embarking ona multicenter trial funded by the National Institutes of Health. This conceptis not limited to cochlear access; it includes access to any structure within thetemporal bone (eg, endolymphatic sac, semicircular canals).
Summary
IGS systems enhance surgical navigation by linking preoperative radio-graphic scans to intraoperative scans, and they are coming to otology/neu-rotology. The keys to IGS systems are fiducials markers (also known as‘‘fiducials’’ or ‘‘markers’’). The positions of these markers, which are at-tached to the patient before imaging, are determined in the image and onthe intraoperative scan and are used to align the two. Determination offiducial position is never perfect, which results in FLE. Ideal fiducialmarkers are repeatedly mounted around the anatomy of interest, with themost accurate being bone-implanted markers. Alignment is never perfect,and as a result there is inevitable error in the alignment of the fiducials,termed FRE, and in the alignment of surgical targets, termed TRE. The lat-ter alignment represents the accuracy of the guidance system.
Typical IGS systems display FRE intraoperatively and specify that it fallbelow a set threshold for reliable navigation. Using more fiducial markersresults in a higher FRE but is likely to provide better guidance accuracy
Fig. 8. Clinical validation of percutaneous cochlear implantation. The drill guide attached after
traditional right cochlear implant surgery (top left). A magnified view showing the drill bit pass-
ing through the facial recess (bottom right).

623IMAGE-GUIDED TECHNIQUE IN NEUROTOLOGY
(lower TRE). Current FDA-approved IGS systems for otolaryngology-headand neck surgery have accuracies (TREs) on the order of 2 mm with nonin-vasive fiducials (ie, skin-affixed markers, proprietary headsets, laser scan-ning of facial features).
To date, clinical application of IGS otology/neurotology has been lim-ited, but a large potential market and numerous applications support itsuse. Such applications include control of surgical instruments (eg, turningoff a drill when close to an anatomic boundary), robotic surgery (eg, roboticmastoidectomy), and minimally invasive surgery (eg, percutaneous cochlearimplantation).
References
[1] Casiano RR, NumaWA. Efficacy of computed tomography image-guided endoscopic sinus
surgery in residency training programs. Laryngoscope 2000;110:1277–82.
[2] Weinberg JS, Lang FF, Sawaya R. Surgical management of brain metastases. Curr Oncol
Rep 2001;3(6):476–83.
[3] Wisoff JH, Boyett JM, Berger MS, et al. Current neurosurgical management and the impact
of the extent of resection in the treatment of malignant gliomas of childhood: a report of the
Children’s Cancer Group trial no. CCG-945. J Neurosurg 1998;89(1):52–9.
[4] Fitzpatrick J,Hill D,Maurer C. Registration. In: SonkaM, Fitzpatrick JM, editors.Medical
image processing: handbook of medical imaging. Bellingham (Washington): SPIE Press;
2000. p. 447–513.
[5] Snyderman C, Aimmer LA, Kassam A. Sources of registration error with image guidance
systems during anterior cranial base surgery. Otolaryngol Head Neck Surg 2004;131:145–9.
[6] West JB, Fitzpatrick JM, Toms SA, et al. Fiducial point placement and the accuracy of
point-based rigid body registration. Neurosurgery 2001;48:810–7.
[7] Labadie RF, Davis BM, Fitzpatrick JM. Image-guided surgery: what is the accuracy? Curr
Opin Otolaryngol Head Neck Surg 2005;13:27–31.
[8] Schlaier J,Warnat J, BrawanskiA. Registration accuracy and practicability of laser-directed
surface matching. Comput Aided Surg 2002;7:284–90.
[9] Fried MP, Kleefield J, Gopal H, et al. Image-guided endoscopic surgery: results of accuracy
and performance in a multi-center clinical study using an electromagnetic tracking system.
Laryngoscope 1997;107:594–601.
[10] MetsonRB, Cosenza JM,CunninghamMJ, et al. Physician experience with an optical image
guidance system for sinus surgery. Laryngoscope 2000;110:972–6.
[11] Sargent EW, Buccholz RD. Middle cranial fossa surgery with image-guided instrumenta-
tion. Otolaryngol Head Neck Surg 1997;117:131–4.
[12] Caversaccio M, Romualdez J, Vaecgker Rm, et al. Valuable use of computer-aided surgery
in congenital bony aural atresia. J Laryngol Otol 2003;117:241–8.
[13] RaineCH, StrachanD,GopichandranT.Howwe do it: using a surgical navigation system in
the management of the ossified cochlea. Cochlear Implants Int 2003;4:96–101.
[14] Fitzpatrick JM, Konrad PE, Nickele C, et al. Accuracy of customized miniature stereotactic
platforms. Stereotact Funct Neurosurg 2005;83:25–31.
[15] French LC, Dietrich MS, Labadie RF. The frequency of mastoidectomy procedures
performed annually in the United States. Ear Nose Throat J, in press.
[16] Cleary K, Kinsella A. OR 2020: the operating room of the future. J Laparoendosc Adv Surg
Tech A 2005;15(5):497–573.
[17] AlexiadesG. Emerging technologies: a glimpse into the future of neurotology. TheAmerican
Neurotology Society Meeting. Otol Neurotol 2005;26:2–4.

624 LABADIE et al
[18] LabadieRF,Fitzpatrick JM. Systemandmethod for surgical instrument disablement via im-
age-guided position feedback. United States Patent Application Publication No. US 2005/
0228256 A1, October 13, 2005.
[19] Strauss G, Koulechov K, Hofer M, et al. The navigation-controlled drill in temporal bone
surgery: a feasibility study. Laryngoscope 2007;117:434–41.
[20] Guthart GS, Salisbury JK. The intuitive telesurgery system: overview and application. Pro-
ceedings of the Institute of Electrical and Electronics Engineers International Conference on
Robots and Automation 2000;4:618–21.
[21] PaulHA,Mittlestadt B, BargarWL, et al. A surgical robot for total hip replacement surgery.
Proceedings of the Institute of Electrical andElectronics Engineers International Conference
on Robots and Automation 1992;1:606–11.
[22] HonlM, Dierk O, Gauck C, et al. Comparison of robotic-assisted andmanual implantation
of a primary total hip replacement. J Bone Joint Surg Am 2003;85:1470–8.
[23] Federspil PA, Geisthoff UW, Henrich D, et al. Development of the first force-controlled
robot for otoneurosurgery. Laryngoscope 2003;113:465–71.
[24] Labadie RF, Choudhury P, Cetinkaya E, et al. Minimally-invasive, image-guided, facial
recess approach to the middle ear. Otol Neurotol 2005;26:557–62.
[25] Warren FM, Balachandran R, Fitzpatrick JM, et al. Percutaneous cochlear access using
bone-mounted, customized drill guides: demonstration of concept in-vitro. Otol Neurotol
2007;28(3):325–9.
[26] Baron S, Eilers H, Hornung O, et al. Conception of a robot assisted cochleostomy: first
experimental result. In Proceedings of the 7th International Workshop on Research and
Education in Mechatronics, REM2006. Stockholm (Sweden); June 15–16, 2006.
Related Documents











