JOURNAL OF RESEARCH IN SCIENCE TEACHING VOL. 47, NO. 6, PP. 742–762 (2010) Exploring Identities to Deepen Understanding of Urban High School Students’ Sexual Health Decision-Making Jennie S. Brotman, 1 Felicia Moore Mensah, 1 Nancy Lesko 2 1 Department of Mathematics, Science & Technology, Teachers College, Columbia University, 525 W 120th Street, Box 210, New York, New York 10027 2 Department of Curriculum and Teaching, Teachers College, Columbia University, New York, New York Received 14 May 2009; Accepted 5 January 2010 Abstract: Sexual health is a controversial science topic that has received little attention in the field of science education, despite its direct relevance to students’ lives and communities. Moreover, research from other fields indicates that a great deal remains to be learned about how to make school learning about sexual health influence the real-life choices of students. In order to provide a more nuanced understanding of young people’s decision-making, this study examines students’ talk about sexual health decision-making through the lens of identities. Qualitative, ethnographic research methods with twenty 12th grade students attending a New York City public school are used to illustrate how students take on multiple identities in relation to sexual health decision-making. Further, the study illustrates how these identities are formed by various aspects of students’ lives, such as school, family, relationships, and religion, and by societal discourses on topics such as gender, individual responsibility, and morality. The study argues that looking at sexual health decision-making—and at decision-making about other controversial science topics—as tied to students’ identities provides a useful way for teachers and researchers to grasp the complexity of these decisions, as a step toward creating curriculum that influences them. ß 2010 Wiley Periodicals, Inc. J Res Sci Teach 47: 742–762, 2010 Keywords: health science; biology; socioscientific issues; secondary Science education has the potential to equip students with the knowledge, tools, and motivation to use science in meaningful ways to impact their lives, their communities, their personal health, and the environment. It can influence students to become ‘‘scientifically literate’’ (DeBoer, 2000) citizens of the world that pay attention to and take action around socioscientific issues (Zeidler, Sadler, Simmons, & Howes, 2005). It can teach students to think critically and reason effectively (Sadler, 2004) and to both value and critique the role science plays in society. Despite this potential, students often perceive science education as boring, irrelevant, and unrelated to their lives outside of school. This is partly because science has traditionally been taught as an abstract body of knowledge that students must acquire and master, primarily for the purpose of pursuing science careers (Aikenhead, 2006); however, science may also conflict with students’ cultural ways of knowing, worldviews, religious beliefs, or identities (Aikenhead & Jegede, 1999; Brickhouse, 2001). In order to address this situation, reform-based approaches that aim to make science relevant to students’ lives and decisions are increasingly discussed in the science education literature, and have collectively been referred to as ‘‘progressive science education’’ (Sadler & Zeidler, 2009, p. 911). One such reform-based approach is the use of controversial, real-world topics in the science classroom. We use the term ‘‘controversial science topics’’ to refer to both ‘‘socioscientific issues’’ (SSI), or issues that are ‘‘based on science concepts or problems, controversial in nature, discussed in public outlets, and frequently subject to political and ethical influences’’ (Sadler & Zeidler, 2005, p. 113), as well as science-related issues that are Correspondence to: J.S. Brotman; E-mail: [email protected] DOI 10.1002/tea.20370 Published online 9 February 2010 in Wiley InterScience (www.interscience.wiley.com). ß 2010 Wiley Periodicals, Inc.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

JOURNAL OF RESEARCH IN SCIENCE TEACHING VOL. 47, NO. 6, PP. 742–762 (2010)
Exploring Identities to Deepen Understanding of Urban High School Students’Sexual Health Decision-Making
Jennie S. Brotman,1 Felicia Moore Mensah,1 Nancy Lesko2
1Department of Mathematics, Science & Technology, Teachers College, Columbia University,
525 W 120th Street, Box 210, New York, New York 100272Department of Curriculum and Teaching, Teachers College, Columbia University, New York,
New York
Received 14 May 2009; Accepted 5 January 2010
Abstract: Sexual health is a controversial science topic that has received little attention in the field of science
education, despite its direct relevance to students’ lives and communities. Moreover, research from other fields indicates
that a great deal remains to be learned about how to make school learning about sexual health influence the real-life
choices of students. In order to provide a more nuanced understanding of young people’s decision-making, this study
examines students’ talk about sexual health decision-making through the lens of identities. Qualitative, ethnographic
research methods with twenty 12th grade students attending a New York City public school are used to illustrate how
students take on multiple identities in relation to sexual health decision-making. Further, the study illustrates how these
identities are formed by various aspects of students’ lives, such as school, family, relationships, and religion, and by
societal discourses on topics such as gender, individual responsibility, and morality. The study argues that looking at
sexual health decision-making—and at decision-making about other controversial science topics—as tied to students’
identities provides a useful way for teachers and researchers to grasp the complexity of these decisions, as a step toward
creating curriculum that influences them. � 2010 Wiley Periodicals, Inc. J Res Sci Teach 47: 742–762, 2010
Keywords: health science; biology; socioscientific issues; secondary
Science education has the potential to equip students with the knowledge, tools, and motivation to use
science in meaningful ways to impact their lives, their communities, their personal health, and the
environment. It can influence students to become ‘‘scientifically literate’’ (DeBoer, 2000) citizens of the
world that pay attention to and take action around socioscientific issues (Zeidler, Sadler, Simmons, & Howes,
2005). It can teach students to think critically and reason effectively (Sadler, 2004) and to both value and
critique the role science plays in society. Despite this potential, students often perceive science education as
boring, irrelevant, and unrelated to their lives outside of school. This is partly because science has
traditionally been taught as an abstract body of knowledge that students must acquire and master, primarily
for the purpose of pursuing science careers (Aikenhead, 2006); however, science may also conflict with
students’ cultural ways of knowing, worldviews, religious beliefs, or identities (Aikenhead & Jegede, 1999;
Brickhouse, 2001).
In order to address this situation, reform-based approaches that aim to make science relevant to students’
lives and decisions are increasingly discussed in the science education literature, and have collectively been
referred to as ‘‘progressive science education’’ (Sadler & Zeidler, 2009, p. 911). One such reform-based
approach is the use of controversial, real-world topics in the science classroom. We use the term
‘‘controversial science topics’’ to refer to both ‘‘socioscientific issues’’ (SSI), or issues that are ‘‘based on
science concepts or problems, controversial in nature, discussed in public outlets, and frequently subject to
political and ethical influences’’ (Sadler & Zeidler, 2005, p. 113), as well as science-related issues that are
Correspondence to: J.S. Brotman; E-mail: [email protected]
DOI 10.1002/tea.20370
Published online 9 February 2010 in Wiley InterScience (www.interscience.wiley.com).
� 2010 Wiley Periodicals, Inc.
personally controversial for individuals, as they grapple with their own choices around topics such as
nutrition, medical care, and sexual health. Part of the rationale behind bringing societally and personally
controversial topics into the science classroom is that through the exploration of these topics, students will
become more prepared to make real-life decisions about such issues.
However, the growing body of literature that investigates the informal reasoning and decision-making of
young people as they grapple with socioscientific and personal dilemmas reveals that students’ decision-
making processes about these issues are complex and do not necessarily spotlight or incorporate scientific
understandings learned in school. As might be expected, values, beliefs, personal experiences, social
interactions, emotions, and intuitions impact choices related to controversial issues, often to a greater extent
than scientific knowledge or evidence (Aikenhead, 2006; Grace & Ratcliffe, 2002; Sadler & Zeidler, 2005).
Furthermore, not only is scientific knowledge often not prioritized but also students tend to ignore in
particular scientific content learned in school and to view scientific knowledge as inapplicable to their
everyday lives (Kolstø, 2006; Ratcliffe, 1997; Sadler, 2004).
Sexual health is a controversial science topic that has received little attention in the field of science
education, despite its direct relevance to students’ lives and communities, although a few science education
studies focus on HIV/AIDS education (e.g., Keselman, Kaufman, Kramer, & Patel, 2007; Mutonyi, Nielsen,
& Nashon, 2007). Moreover, research from fields such as health education, public health, and curriculum
studies indicates that a great deal remains to be learned about how to make school learning about sexual health
influence students’ real-life decisions. Quantitative program evaluations that assess the impact of curriculum
on behavior change often describe short-term, unsustainable impacts (DiClemente, Salazar, & Crosby, 2007).
Qualitative studies internationally find that students often perceive HIV/AIDS and sex education curriculum
to be irrelevant to their lives, culturally inappropriate, and unlikely to influence their behavior (Buckingham
& Bragg, 2004; Ward & Taylor, 1992). If we want to bridge this frequent gap between the school curriculum
and students’ lives, a gap also identified in relation to other controversial science topics, we need a deeper
understanding of how students make decisions.
While students’ reasoning and decision-making about controversial science topics are increasingly
researched in the field of science education, studies focus mostly on hypothetical reasoning scenarios as
opposed to students’ thinking about actual decisions of personal consequence to them; do not typically
emphasize how influences outside of the classroom interact with school learning to impact decisions; and
focus little on science issues related to health decisions, such as those related to sexual behavior (Harrison,
2005). Studies from other fields, such as health education, health behavior, and health psychology, especially
those conducted in the US, primarily look for quantitative correlations between ‘‘risky sexual behavior’’ and
many factors. While these studies are informative in that they reveal numerous potential influences on sexual
health decision-making, they do not illuminate the mechanisms by which youth approach decisions, or the
resources in their lives that they draw upon to make choices. Studies also often rely on individualistic
theoretical models, which do not sufficiently account for the multi-leveled influences on human behavior
(DiClemente et al., 2007).
Purpose of Study and Research Question
This study aims to address these gaps in the literature and to provide a more nuanced understanding of
young people’s decision-making by qualitatively examining students’ talk about sexual health decisions
through the lens of identity—with the idea that how students talk about decision-making is one way to begin
to understand potential unexplored influences on students’ ‘‘actual’’ decisions. We argue that identity
provides a useful framework for understanding the complexity of sexual health decisions because this
framework allows for an explicit investigation into the connections between decision-making and how
students position themselves and are positioned as people. Furthermore, the argument that considering
identities has the potential to make school learning and teaching more meaningful to the lives of students and
teachers is increasingly made in recent science education literature (Brickhouse, Lowery, & Schultz, 2000;
Carlone & Johnson, 2007; Moore, 2008). We build upon this literature in the present study, conducted with
twenty 12th grade students attending a health-focused public high school in New York City. We address the
following primary research question: In a health-focused school, what identities do urban high school
IDENTITIES AND SEXUAL HEALTH DECISION-MAKING 743
Journal of Research in Science Teaching

students take on when talking about sexual health decision-making, and what influences the formation of
those identities?
Theoretical FrameworkIdentities
Questions of identity are broadly concerned with what it means to ‘‘be a person,’’ to understand or define
ourselves, to have a sense of ‘‘who we are.’’ Elaborating on these ideas, authors and researchers across a
variety of fields, including psychology, sociology, anthropology, cultural studies, and education, theorize
from different standpoints about what ‘‘identity’’ means. Holland, Lachicotte, Skinner, and Cain (1998)
provide a useful overview of predominant theories of self and identity and how these have changed over time.
In particular, they discuss three debated theoretical notions of ‘‘the self’’—the ‘‘universal self,’’ the
‘‘culturally specific self,’’ and the ‘‘socially constructed self.’’ While universalist theories view the self as a
uniform, constant ‘‘complex of natural, species-given structures and processes,’’ culturalist perspectives view
the self as shaped by culture and thus ‘‘malleable’’ from group to group (p. 20).
In contrast, the perspective of the ‘‘socially constructed self’’ critiques both universalist and culturalist
notions for being ‘‘essentialist’’—that is, both universal and cultural definitions of the self give it certain
essential, stable characteristics (whether those static features are explained as natural or formed by culture)
that people or groups of people possess. From a social constructivist perspective, selves are not fixed by either
nature or culture but instead constructed and reconstructed by ‘‘powerful discourses’’ (p. 26) and therefore
subject to change depending on the discourses within which they are positioned or position themselves.
According to this view, ‘‘discourses and practices’’ are ‘‘the tools that build the self’’ (p. 27).
This latter depiction of the ‘‘socially constructed self’’ is rooted in poststructuralist theories.
Highlighting related tensions in the conceptualization of identity to those described by Holland et al. (1998),
Davies (2000) contrasts ‘‘the concept of a person’’ as articulated by ‘‘humanist’’ versus ‘‘poststructuralist’’
theories (p. 57). From the perspective of humanism, ‘‘identity is continuous, unified, rational, and coherent’’
(p. 57). On the other hand, according to poststructuralism, the ‘‘experience of being a person’’ is ‘‘necessarily
contradictory’’ in that it can be different depending upon the situation (p. 57); further, it ‘‘has no fundamental
essence,’’ and it is ‘‘multiple’’ as opposed to ‘‘unitary’’ (p. 55). According to Davies (1989), ‘‘who one is is
always an open question with a shifting answer,’’ allowing people to have different ‘‘possible selves located in
different story-lines’’ (p. 229). Thus, a person does not possess one singular self, but instead can take on one
identity in one context, and a different identity in another. Gee (1997) similarly argues that, ‘‘We are different
situated selves,’’ highlighting the ways in which people can ‘‘feel like, act like, and look like different people’’
depending on the situation (p. xiii).
More specifically, Davies (1989) argues, according to poststructuralist theories, that people take on
different senses of self depending upon how they are positioned and position themselves within particular
discourses; that is, people are ‘‘constituted and reconstituted through the various discursive practices in which
they participate’’ (p. 229). While the concept of ‘‘discourse’’ has been discussed in numerous ways (Davies,
1994), we use the term to describe ‘‘knowledge with a specific vocabulary and syntax,’’ or ‘‘systems of
reasoning’’ utilized by different ‘‘fields and institutions’’ (Lesko, 2001, p. 15) that are articulated through
particular ‘‘beliefs, narratives, images, and metaphors’’ (Davies, 1989, p. 232). Further, these systems of
reasoning can originate at ‘‘the disciplinary, the political, the cultural, and the small group level,’’ and can also
form ‘‘around a specific topic, such as gender or class’’ (Davies, 2000, p. 88). Discourses, more generally, are
the ‘‘public meaning systems’’ that are the ‘‘material for identity formation’’ (Bettie, 2003, p. 54). That is,
through discourses (which, although constructed socially, are often taken as natural, commonsense ways of
understanding the world), we create ‘‘stories through which we make sense of our own and others’ lives’’
(Davies, 1989, p. 229). Within these stories, different kinds of identities are made possible or impossible.
In this study, we use these poststructuralist theories to conceptualize identity as unfixed, dependent upon
context, and situated within discourse (Davies, 1989, 1994; Gee, 1997). More specifically, we use the word
‘‘identities’’ to mean the different ‘‘selves’’ that people enact as they are positioned and position themselves
within discourses. When we say that students ‘‘take on’’ particular identities related to sexual health decision-
making, we mean that when talking about sexual health decision-making, they make connections to particular
selves, to their concepts of themselves as persons, either overtly or implicitly. In doing this, they position
744 BROTMAN, MENSAH, AND LESKO
Journal of Research in Science Teaching
themselves within particular discourses—such as discourses related to gender, religion, morality, or
relationships—and it is those discourses that make the identities they take on possible. Therefore, in writing
about identities, we do not aim to uncover core, static, essential aspects of who these students are; instead, we
aim to articulate the ways in which they enact multiple ‘‘possible selves’’ in different situations as they talk
about sexual health decision-making—and how those ‘‘selves’’ take form via the discourses they encounter in
their lives, ‘‘through a life history of being in the world’’ (Davies, 1994, p. 3).
One advantage of this poststructuralist view of identities as shifting and multiple is that it opens up the
possibility for individuals to ‘‘see ourselves in different ways’’ (Davies, 1989, p. 238)—to change the
identities we take on by positioning ourselves within different discourses. It also opens up the possibility for
schools and classrooms to help produce ‘‘alternative’’ identities by emphasizing different discourses, perhaps
deviating from ‘‘dominant’’ discourses that can constrain the identities people adopt. To take an example
from science education, Hughes (2001) showed how when a curriculum challenged dominant discourses
about both science and gender, this allowed some girls to take on different kinds of scientist identities,
identities which pushed against stereotypical ideas about gender and science. Thus, in taking a
poststructuralist view of identity, we intend to contribute to an understanding of the formation of identities
related to sexual health decision-making as well as to a consideration of how curriculum assists in the
formation of those identities and might perhaps make alternative identities available to students.
Decision-Making
Historically, predominant theories of decision-making and behavior change primarily focus on factors
internal to individuals that might influence their behavior, such as self-efficacy, impulsivity, and the extent to
which they perceive risk (DiClemente, Salazar, Crosby, & Rosenthal, 2005; DiClemente et al., 2007). Many
of these models emphasize rational decision-making processes that portray individuals as carefully weighing
benefits and drawbacks of particular choices. Along these lines, in reviewing approaches to understanding
adolescents’ ‘‘risky decision-making,’’ Reyna and Farley (2006) describe a class of ‘‘explanatory models’’
that emphasize, ‘‘deliberate, quantitative trading off of risks and benefits’’ (p. 1). They describe these
frameworks as rooted in ‘‘traditional behavioral decision theory’’ (p. 32) and adhering to a decision-making
process in which ‘‘options are considered, consequences are evaluated, and a decision is made’’ (p. 16).
Reyna and Farley (2006) critique the inability of these models of ‘‘reasoned’’ decision-making to
explain behavior that seems ‘‘unconscious or irrational,’’ which they argue is often the case in relation to
adolescents’ risk-taking behaviors (p. 17). They therefore propose and empirically support a newer class of
theoretical models that involves a more ‘‘reactive route’’ (p. 18) to decision-making, based more in intuition
than reason, where individuals base choices not on careful cost-benefit analyses, but on ‘‘perceived gists’’ or
‘‘fuzzy mental representation[s] of the general meaning of information or experience’’ (p. 1). That is,
according to models such as ‘‘fuzzy trace theory,’’some individuals base choices on a qualitative sense of risk.
While these latter models deviate from the view that rationality consistently dictates choices, like more
traditional models, they remain embedded in an individualistic framework, focusing on cognitive processes
that happen within individuals as they make decisions. In contrast, yet another emerging paradigm, socio-
ecological theory, explains people’s sexual health decision-making as influenced not only by individual but
also by family, relational, community, and societal factors (DiClemente et al., 2005, 2007). Based upon the
work of Bronfenbrenner (1979), DiClemente et al. (2005) provide evidence from the research literature to
support the importance of the ‘‘multiplicity of influences’’ that ‘‘shape adolescents’ behavior’’ in relation to
sexuality (p. 826). Further, DiClemente et al. (2007) highlight ‘‘society, culture, values, economics,
traditions, laws and mores’’ as ‘‘distal influences’’ that interact with the ‘‘proximal influences’’ of
relationships, family, community, and peers (p. 892).
In this article, we draw upon this socio-ecological perspective on decision-making. The idea that
people’s actions do not occur in a vacuum, but are influenced by the social, cultural, and relational worlds in
which they live, is consistent with the poststructuralist view of identities as constructed through discourse,
and situated within the many contexts of people’s lives. Furthermore, this study seeks to expand
understanding of the ways in which individuals are embedded within social structures that influence their
actions by framing sexual health decision-making in terms of identities. This study therefore uses the lens of
identities within a socio-ecological paradigm to paint a more complex picture of what decision-making
IDENTITIES AND SEXUAL HEALTH DECISION-MAKING 745
Journal of Research in Science Teaching
actually entails. The ethnographic, qualitative methods described below allow for a detailed illustration of the
complexity of students’ talk about sexual health decision-making, as it applies to their lives and the lives of
those around them.
Methods
Setting and Participants
We conducted the study at a New York City public school, which enrolls 479 students in grades 7–12.
The approximate ethnic breakdown of the school as described on its website is as follows: 65% Hispanic, 30%
Black, 2.5% Asian/Pacific Islander, 1.25% American Indian, and 1.25% White. Approximately 10% of the
school’s total students are English Language Learners, about three quarters of the student population is
female, and roughly 75% of students are eligible for the free lunch program. The school has a focus on
preparing students to enter various health professions. Participants came from a class of 29 students in one
12th grade cohort, a group of students who travel together to all of their classes. This particular cohort was
chosen based on ‘‘purposeful’’ or ‘‘purposive’’sampling (Merriam, 1998, p. 61). All 29 students in this cohort
were invited to join the study; however, 20 consented to participate, including18 females and 2 males
(indicative of the high proportion of females that attend this school) of the following self-identified
ethnicities: 7 Latino(a), 7 African American, 3 African, and 3 West Indian. Eight students were born outside
the United States and have lived here between 4 and 17 years. All students were 17 or 18 years of age, except
one girl who was 16.
Data Collection Methods
Each data collection method is described in detail below, including the primary data sources of student
focus groups and interviews, as well as secondary data sources of teacher interviews and participant
observation. All focus groups and interviews, completed over an approximately 3-month period, were audio-
taped and transcribed in their entirety, and reflective field notes were taken after each focus group or interview.
Initial Focus Groups. Sixteen of the 20 participants took part in one initial hour-long focus group, each
containing between two and four participants, for a total of five initial group discussions. We chose focus
groups as the primary data collection method to provide a safe, comfortable setting in which to explore
sensitive issues; to take advantage of the ‘‘synergy’’ of group dialogue (Morgan, 1997, p. 13); and to
efficiently obtain multiple perspectives of many students (Morgan, 1997). We composed focus groups based
on scheduling constraints and a consideration of group dynamics. Initial focus groups were conducted weekly
over the course of 1 month, with one group occurring the following month because of scheduling issues.
Focus groups were semi-structured. As a guide, we used a set of broad, open-ended questions, each
accompanied by a series of probing questions to trigger conversation as needed (see Appendix).1 Questions
addressed specific sexual health decisions as a way to provide a concrete focus for discussion. The focus
group questions were developed through a pilot study. We piloted an initial set of questions with six focus
groups, including a total of 13 high school students, conducted during the summer of 2007. Based on these
pilot data, we then revised the questions to enhance their ability to generate conversation and to ensure that
participants’ words and ideas determined the direction of the conversation as much as possible. Consistent
with our constructivist grounded theory research approach (discussed further below), we aimed to create
‘‘open-ended, non-judgmental questions’’ and to ‘‘encourage unanticipated statements and stories to
emerge’’ (Charmaz, 2006, p. 26). Also consistent with this research approach, we felt free to deviate from
these questions in order to delve more deeply into issues brought up by participants.
Extended Focus Group. Four of the 20 participants (Hana, Illisha, Dina, and Kasandra; all are
pseudonyms) were chosen to be part of the ‘‘extended focus group.’’ These students participated in three
1-hour focus group discussions, which began 2 weeks after the initial focus groups were completed, and
were conducted weekly over the course of 3 weeks. We chose these participants based on a combination of
their willingness and interest, scheduling issues, and a consideration of the group dynamic. The three
discussions with this extended focus group were conducted in a similar manner and covered the same topics
as the initial focus groups, but in greater depth and stretched out over a longer period of time. The first
746 BROTMAN, MENSAH, AND LESKO
Journal of Research in Science Teaching
extended focus group discussion addressed students’ learning about HIV/AIDS, reported elsewhere
(Brotman, 2009). The second extended focus group addressed students’ decision-making (using questions
listed in Appendix), and the third extended focus group addressed students’ school learning about HIV/AIDS
and sexual health, drawing on particular lessons and units witnessed during participant observation. As with
the initial focus groups, we were flexible in our use of our prepared questions and deviated from them as
needed to address what students brought up and to follow-up on students’ comments from prior groups. These
extended conversations allowed for not only more time to discuss decision-making and the various influences
upon it but also for a deeper rapport and comfort level that enhanced conversations during focus groups and
individual interviews (Morgan, 1997).
Individual Student Interviews. The four girls in the extended group were each individually interviewed.
These hour-long, semi-structured interviews took place over the course of the 3 weeks following the
completion of the extended focus groups. These interviews provided the opportunity to follow-up and address
in more depth conversations from the extended focus groups. Therefore, the interview protocol was
developed at the conclusion of the extended focus groups. Interview questions covered the girls’ experiences
during the focus group discussions as well as further thoughts they had about the interview items listed in the
Appendix. We also included a few questions specific to each of the four girls, based on comments they had
made during the focus groups. For example, if participants revealed information about their personal learning
and decision-making during the focus groups, we used the individual interview as an opportunity to ask
further questions about what they had raised; for ethical reasons, we refrained from doing this in depth in the
public setting of the focus groups. Therefore, the interviews also allowed these girls to discuss topics they
were uncomfortable sharing with the group.
Individual Teacher Interviews. At the conclusion of the school year, just after all student focus groups
and interviews were completed, we also conducted semi-structured, hour-long interviews with three health
and science teachers in order to gain additional insight into the school’s curriculum on topics related to HIV/
AIDS and sexual health as well as into the classroom experiences witnessed during participant observation.
We designed a different interview protocol for each teacher, based on his or her particular curriculum and our
observations of it in action. Interview questions covered topics including teachers’ experiences teaching,
goals for, and preparation for relevant units, as well as their overall impressions of the school’s strengths
and challenges. Although these data are not presented in this article, the teacher interviews informed our
overall analysis in that they contributed to the depth of our insight into the school setting, curriculum, and
participants’ school experiences.
Participant Observation. Brotman [first author] was a participant observer in three 12th grade health
and science classes with potential relevance to the topics of HIV/AIDS and sexual health for approximately
one school year (October 2007 to June 2008). These included a biology class focusing on forensics; a health
course covering a variety of topics, from relationships to money management; and an honors-level medicine
course, taught by Mr. P, which focused on medical terminology and human body systems. Classes at earlier
grade levels that participants had taken in prior years were also observed, including a ninth grade HIV/AIDS
and sexuality unit, taught by Mr. P in collaboration with the school’s social workers, which met once a week
for approximately 2 months. This unit was the primary place where HIV/AIDS and sex education were
directly addressed at this school. For approximately 1.5 months, an 11th grade biology course that covered
HIV/AIDS biology and transmission, the immune system, and the reproductive system was also observed.
Participant observation data were used to support and provide additional insight into students’ discussion of
their decision-making during focus groups and interviews. Ethnographic field notes (Emerson, Fretz, &
Shaw, 1995) were written after each class session observed and incorporated both description and reflection.
Data Analysis Methods
We incorporated aspects of grounded theory (Strauss & Corbin, 1998) into the research approach,
drawing primarily on Charmaz’s (2006) articulation of ‘‘constructivist grounded theory,’’ rooted in social
constructivist epistemology, in contrast to earlier ‘‘objectivist’’ versions of grounded theory associated with a
more positivistic worldview (i.e., Glaser & Strauss, 1967). Consistent with this perspective, this study is an
IDENTITIES AND SEXUAL HEALTH DECISION-MAKING 747
Journal of Research in Science Teaching
‘‘interpretive inquiry’’ in which ‘‘researchers make an interpretation of what they see, hear, and understand’’
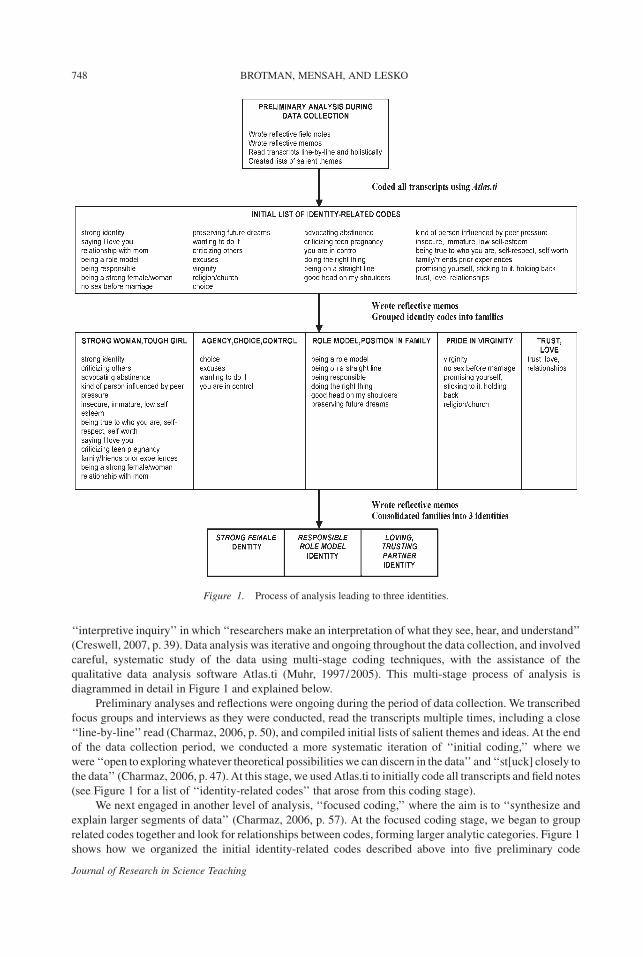
(Creswell, 2007, p. 39). Data analysis was iterative and ongoing throughout the data collection, and involved
careful, systematic study of the data using multi-stage coding techniques, with the assistance of the
qualitative data analysis software Atlas.ti (Muhr, 1997/2005). This multi-stage process of analysis is
diagrammed in detail in Figure 1 and explained below.
Preliminary analyses and reflections were ongoing during the period of data collection. We transcribed
focus groups and interviews as they were conducted, read the transcripts multiple times, including a close
‘‘line-by-line’’ read (Charmaz, 2006, p. 50), and compiled initial lists of salient themes and ideas. At the end
of the data collection period, we conducted a more systematic iteration of ‘‘initial coding,’’ where we
were ‘‘open to exploring whatever theoretical possibilities we can discern in the data’’ and ‘‘st[uck] closely to
the data’’ (Charmaz, 2006, p. 47). At this stage, we used Atlas.ti to initially code all transcripts and field notes
(see Figure 1 for a list of ‘‘identity-related codes’’ that arose from this coding stage).
We next engaged in another level of analysis, ‘‘focused coding,’’ where the aim is to ‘‘synthesize and
explain larger segments of data’’ (Charmaz, 2006, p. 57). At the focused coding stage, we began to group
related codes together and look for relationships between codes, forming larger analytic categories. Figure 1
shows how we organized the initial identity-related codes described above into five preliminary code
Figure 1. Process of analysis leading to three identities.
748 BROTMAN, MENSAH, AND LESKO
Journal of Research in Science Teaching
families. Throughout this process, we wrote ‘‘memos’’ to keep track of emerging interpretations of the data
and to ‘‘raise focused codes to conceptual categories’’ (Charmaz, 2006, p. 72). We also revisited the context of
particular statements, reread unfragmented transcripts, and attempted ‘‘not to iron out inconsistencies,
contradictions, and puzzles’’ in the data (Hollway & Jefferson, 2000, p. 70). Ultimately, through repeated
scrutiny of transcripts, coding categories, and memos, we consolidated these larger categories into the three
identities outlined in the following sections, as indicated in Figure 1.
In addition, as we read and reread the data associated with each of these three identities, we paid
attention to whether students consistently took on only one of the identities, or instead whether they took on
different identities at different times. That is, we highlighted instances where the same student took on one of
the identities at one point and a different identity at another point. In addition to highlighting when these
instances occurred, we wrote reflective memos that attempted to interpret the contributing factors to shifts in
identities. Our explicit attention to this phenomenon of the potential for identities to shift and be multiple
stemmed from the poststructuralist lens on identities described above.
While we went through this systematic process of analysis involving a close study of the data, we take the
position argued by Charmaz that, ‘‘We construct our codes because we are actively naming data’’ and
therefore ‘‘define what we see as significant in the data and describe what we think is happening’’ (p. 47).
Therefore, we aim to make a well-supported argument to substantiate the basis for our interpretation of the
data in subsequent sections, and to articulate the interpretive, theoretical lenses through which we approached
the analysis; however, we acknowledge the possibility of multiple, alternative interpretations. Furthermore,
we used prolonged engagement and persistent observation in the research setting, triangulation of multiple
data sources, peer debriefing, and ‘‘rich, thick description’’ to enhance the trustworthiness of our
interpretation (Creswell, 2007; Guba & Lincoln, 1989).
Findings
Based on the analysis described above, we discuss three identities students take on during focus groups
and interviews in relation to sexual health decision-making, which we label as strong female; responsible role
model; and loving, trusting partner. Consistent with the above discussion of a poststructuralist view of
identities, we define each of these identities as an enactment of a particular ‘‘self’’ that finds a place within and
is made possible through discourses, or ‘‘public meaning systems’’ (Bettie, 2003, p. 54). In the following
sections, we describe each identity and the discourses within which students position themselves as they take
on these identities. For each identity, we also explore what factors potentially influence its formation.
Also consistent with the theoretical view that identities are unfixed and shifting, these three identities are
not mutually exclusive; that is, the same participant often takes on more than one identity in different
situations and conversations. In the context of one focus group discussion, therefore, it is possible that a
student spoke at certain points as a strong female and at other points as a responsible role model. One person
could even position herself within two related discourses simultaneously, therefore enacting two identities at
once—connecting talk about decision-making to herself in two different ways. For instance, some
participants spoke of themselves as both loving, trusting partners and as responsible role models at the same
time. The discussion of the different identities that follows includes exemplars where the same students’
words are used to illustrate more than one identity. That said, while we feel it important to note that identities
were not entirely fixed within particular individuals, this article does not present a deep analysis of the
phenomenon of shifting identities. Examining in detail specific instances where students take on different
identities depending upon the context, as well as the causes and implications of this, is taken up in Brotman
(2009) and would be a worthy area for additional future analysis as well.
Furthermore, in some instances, an identity was taken on briefly and never became a significant part of
the conversation, while in other instances, the same identity was expressed multiple times in multiple ways.
We use these latter cases where identities were expressed strongly and became threads that ran through
conversations to illustrate each identity below. For each identity, we explain the extent to which it was present
in the data and clarify the groups or individuals that we focus on in describing that identity. Also, because our
data most thoroughly support the identities students took on in the context of focus groups and interviews, we
primarily discuss the identities students took on in this context; however, we present some analysis of how
their talk indicates the likely identities they take on in other contexts, such as within their family lives.
IDENTITIES AND SEXUAL HEALTH DECISION-MAKING 749
Journal of Research in Science Teaching
Finally, in order to respect students’ privacy, this study investigated students’ talk as opposed to their
‘‘actual’’ sexual decisions and behaviors; however, on numerous occasions, students volunteered specific
information about their own personal choices, and these examples are included in the following sections as
well.
Strong Female
Participants who took on what we have labeled a strong female identity during focus groups and
interviews positioned themselves primarily within a gendered discourse that describes males as predators and
females as victims in sexual situations. Relying on this discourse, when taking on strong female identities,
participants described themselves as people who are able to resist boys’ frequent pressures around sex and
condom use. They defined themselves in contrast to ‘‘other girls,’’ who they criticized for not being able to do
the same. Furthermore, in taking on strong female identities, some participants also positioned themselves
within a related discourse about individuals being in complete control of their personal choices and made
strong claims about individual responsibility for actions. The formation of this identity seemed to be
influenced by students’ relationships to powerful, independent mothers, by their witnessing of friends and
family in challenging situations they wished to avoid, and possibly by aspects of their school’s culture and
curriculum.
This identity was taken on most strongly and repeatedly by participants in two of the five initial focus
groups, and in the extended focus group (including Hana, Illisha, Dina, and Kasandra). The discourses
underlying this identity appear briefly in the other groups as well. We use data from these three groups to
articulate this identity. Because of our prolonged conversations with the four extended focus group
participants, many (but not all) of the examples we use below, particularly those related to our interpretation
of the formation of this identity, draw from our repeated discussions with this extended group.
The narrative underlying the strong female identity is one in which boys attempt in various ways to take
advantage of and pressure girls around issues of sexuality. Most girls are ‘‘gullible,’’ or ‘‘don’t have a high
mentality,’’ and so ‘‘fall for that’’; those who are ‘‘smart enough’’ and ‘‘strong female[s]’’ are able to resist
these pressures, as illustrated in the following dialogue:
Kasandra: . . .When girls get persuaded [to have sex], that’s when they don’t have a high mentality as
to what guys are gonna tell them.
Illisha: Yeah some girls . . .
Kasandra: . . . they’re gullible
Illisha: Some girls are like really really really aggressive, when it comes down to anything else,
but when it comes down to a boy, they get sensitive.
Kasandra: Yes.
Illisha: They give in . . .
Kasandra: Yes, exactly. All the boys are sayin’ . . . I really like you and all that . . . we could be
together . . .
Illisha: All that’s BS, you could easily read behind something like that.
Kasandra: Yeah, because they’re cliche, they have been said so many times that it’s played out
already.
Illisha: Well, when you’re a strong female like I am, that...doesn’t do anything to me.
This dialogue illustrates how students took on strong female identities by contrasting themselves to
‘‘other’’ girls who ‘‘fall into the boy’s trap.’’ They defined themselves as not those girls. Participants taking on
strong female identities commonly took on an angry, frustrated tone when setting themselves apart from
‘‘other’’ girls, using words like ‘‘hideous,’’ ‘‘totally wrong,’’ and ‘‘ridiculous.’’ They denounced what they
perceived to be girls’ misguided rationales for sexual choices and their participation in their own
manipulation.
In addition to this general frustration with girls who are manipulated by boys, participants also made
more specific claims about the kinds of people who succumb to pressure and manipulation. Some explained
that certain girls are ‘‘seduced by peer pressure’’ because they are ‘‘insecure,’’ ‘‘immature,’’ or ‘‘have low
self-esteem.’’ They spoke of the ‘‘type of person that . . . let[s] peer pressure get to them,’’ as being ‘‘easily
750 BROTMAN, MENSAH, AND LESKO
Journal of Research in Science Teaching
influenced,’’ or ‘‘a soft person.’’ They contrasted these types of girls who are ‘‘tryin’ to find your place’’ with
those who ‘‘have a strong sense of yourself,’’ who ‘‘stick to what [you] think.’’
A related critique of other girls used in taking on strong female identities was mounted by the extended
focus group in particular, who contrasted themselves with ‘‘a lot of girls’’ who were ‘‘the toughest girls’’ in
school, the ‘‘fightin’’’ girls who ‘‘can’t take nothin’ from nobody,’’ but who became ‘‘sensitive’’ and
sentimental around boyfriends. Setting herself apart from this pattern, Hana talked about how she speaks her
mind in relationships, ‘‘hold[s] nothin’ back’’ and does not use nicknames like ‘‘baby,’’ adding, ‘‘you would
think I’m the man and they’re the girls.’’ She further described how when she is in a relationship, ‘‘I love you is
not in my vocabulary’’; she does not use the words or want to hear them because they are so often ‘‘fake’’ and
used to ‘‘play’’ girls so they could ‘‘fall into’’ their male partner. Participants across groups also criticized the
ways in which presumptions of love are used as a rationale for girls’ choices, sometimes leading to unsafe
behaviors such as not using condoms.
The extended focus group in particular also relied upon a discourse that emphasized individual
responsibility and control over sexual choices in order to critique others and thus make claims about
themselves as strong females. The central argument this group made repeatedly during focus groups and
interviews was that, ‘‘you choose your own actions,’’ and do things such as have sex because you ‘‘want to,’’
despite the fact that people often try to come up with other ‘‘excuses’’ to divert their own personal
responsibility for and investment in their actions. For example, Hana argued that many girls claim they had
sex because they were ‘‘caught in the moment,’’ when in fact, she believed ‘‘the only way that you will
actually proceed in having sex is if you want to have sex.’’ Illisha similarly argued, ‘‘Everyone has their own
mind, so it’s up to you and how you feel, how you wanna do things.’’
There seem to be several potential influences on the formation of strong female identities. The
participants in the extended focus group compared themselves to their mothers, who were strong women who
stood up to the men in their lives. For instance, Illisha attributed her own ability to stand up to others to her
mother, ‘‘a real independent woman’’:
I seen my mom actually leave my dad for a long period, like 6 months. Like left the house, found her
own house, put all her stuff in there. My mom is like a real independent woman . . . she doesn’t take
anything from anyone, from anyone. So I’ve learned not to take anything from anyone as well.
In response to this comment Illisha and Hana then both added that they ‘‘especially’’ learned not be
pushed around ‘‘by a guy.’’ Hana and Dina also shared stories about their mothers’ strength in the face of
difficult situations with their husbands.
In addition to referencing the experiences of their mothers, the difficult experiences of friends, family
members, and people they see in their neighborhoods, mostly related to pregnancy, figured prominently in
extended focus group discussions and seemed to contribute as well to the formation of these girls’ strong
female identities. As a group, they were highly critical of girls who got pregnant at young ages and their
resulting dire situation, heavily invoking the discourses of personal choice and responsibility outlined above.
They criticized young mothers for not only ruining their chances at furthering their education but also for
being ignorant of the economic consequences of young motherhood:
Hana: You can’t go to college ‘cause you have a kid, nah, sweetie, no.
Illisha: Tight, yep.
Hana: Tight, you don’t even got, you don’t even got a crib for you and your baby, you livin’ in your
mother’s house on welfare.
Illisha: That’s my sister.
Hana: With your son, your daughter, you don’t even got food, for the pampers, and alla that—on the
WIC line [referring to The Special Supplemental Nutrition Program for Women, Infants and
Children]. Nah, chill.
Dina: And there’s girls like that and they still have another kid.
Hana: There’s people that I know on the welfare line like, ‘Oh my god I’m pregnant and they don’t
wanna give me food stamps.’ Get a job. Nobody told you to get pregnant. You need to have a job.
Dina: That’s sad.
Hana: Before you think about havin’ a kid, make sure you have the money for a kid, space for a kid.
IDENTITIES AND SEXUAL HEALTH DECISION-MAKING 751
Journal of Research in Science Teaching

The group’s exposure to ‘‘so many stories about pregnancies,’’ some very close to home as in the case of
Illisha’s pregnant sister, seemed to fuel the strength of their critiques. Illisha affirmed Kasandra’s suggestion
that because of what Illisha has seen her sister go through, ‘‘you will make sure that it would never happen to
you.’’ They spoke of groups of girls, some former elementary school classmates, walking on the street with
baby carriages, looking ‘‘tacky’’ and ‘‘ridiculous,’’ and exclaiming that ‘‘once you have a child at a young
age, life is over.’’ In addition to teenage pregnancy, they shared disapproving stories of friends who non-
chalantly have unprotected sex leading to repeated abortions.
Hana also spoke with resolve about her desire to avoid single parenthood because of how she has ‘‘seen
my mother struggle with all of us and there was no father figure there’’ and has seen her sister struggle with an
abusive and ultimately absent husband, who left her in economic hardship. The group strongly lambasted
absent fathers, wondering angrily, ‘‘why are guys jerks?’’ They debated the possibility of raising sons so that
they ‘‘don’t treat girls’’ badly, yet some argued that this was unachievable.
In addition to the ways in which the social context of these girls’ lives, including their family
experiences and relationships, seemed to influence the adoption of strong female identities, it is possible
that discourses embedded in the school’s culture and curriculum may potentially impact the adoption
of this identity as well. First, the school culture positioned these students as strong, capable, and
knowledgeable, likely reinforcing their sense of control and confidence over their decisions. Illustrating
this point, one girl described how the school’s HIV/AIDS and sex education ‘‘makes a person more
aggressive when making their decisions because then, no one can overthrow what you feel you wanna
do . . .’’ In addition, some participants interpreted their health teacher, Mr. P, as espousing elements of
the discourses of personal choice and control they themselves put forth during focus groups and
interviews. For instance, multiple participants from the extended focus group praised Mr. P for the
following approach: ‘‘He tells us what’s right and what’s wrong, and we make the decision. He doesn’t say
don’t do this, don’t do that . . .You choose what to do.’’ Lastly, the school’s sexual health curriculum
seemed to include to a certain extent, perhaps unintentionally, the discourse underlying the strong female
identity that positioned girls as victims of boys’ pressure. For example, multiple focus groups referenced
positively those activities during health classes that supported this discourse, such as the acting out of
scenarios showing ‘‘peer pressure . . . your boyfriend bein’ like oh, come on, everybody’s doin’ and . . . the
girl falls into it.’’
Responsible Role Model
In taking on the identity of responsible role model, participants positioned themselves within discourses
of responsibility that linked sexual decisions to morality, framing choices in terms of ‘‘right’’ and ‘‘wrong.’’
They invoked the metaphors of being on the ‘‘right track,’’ of not going ‘‘sideways,’’ and emphasized the
importance of making responsible, safe decisions in general. For many, they also spoke of how they either
acted as models of responsible behavior for others in their lives, or how they were singled out by people in
their lives as exemplars of responsible behavior. This identity was taken on most strongly by the participants
of two of the initial focus groups as well as the extended focus group. The detailed stories of three extended
focus group participants, Dina, Illisha, and Kasandra, are used to show how positions within their families—
as faithful adherent to a family’s deeply held religious beliefs about sexuality, as the daughter on the ‘‘right
track’’ in contrast to other family members, and as one who will achieve future career goals not attained by
others in the family—shaped this identity. These examples also illustrate that students took on multiple,
shifting identities during focus groups, as Dina, Illisha, and Kasandra were described above as taking on
identities as strong females as well.
Across focus groups, participants who took on responsible role model identities talked about ‘‘doing the
right thing’’ and ‘‘being responsible’’ in relation to sexual health decisions, and referenced their desire to
encourage others to do the same. For example, one participant argued that, ‘‘Having sex is great when you do
it the right way,’’ elaborating that ‘‘doing it right’’ meant ‘‘tak[ing] the proper procedures,’’ such as ‘‘using a
condom and talking with your partner,’’ which she described learning from her health teacher. Echoing this
sentiment, another member of the group advocated for ‘‘being responsible,’’ adding, ‘‘If you’re responsible
you’re gonna have a happy ending.’’ A participant from another group argued for the importance of
752 BROTMAN, MENSAH, AND LESKO
Journal of Research in Science Teaching
encouraging students to ‘‘do the right thing’’ and ‘‘protect themselves.’’ Language of protection and
responsibility was frequently invoked during focus groups.
For some participants, in addition to contrasting the ‘‘right way’’ and the ‘‘wrong way’’ to act in relation
to sexual health decisions, they emphasized their desires and attempts to set an example and influence others
in their lives to make responsible choices. In doing this they set themselves and their actions apart from others
in their lives. For instance, one male participant argued that because they received thorough sex education in
high school, it was important that they shared how they were ‘‘using condoms and protecting ourselves’’ with
‘‘friends that don’t know about it,’’ and ‘‘telling them that they should do the right thing.’’ He later argued in a
similar vein that his school curriculum influenced him and his classmates to ‘‘talk to others that don’t know,
and educate others, try to spread the word, so the world could be a better place.’’ These examples illustrate
how receiving a high school education they felt was thorough and distinct from the frequent lack of
educational opportunities at other schools influenced the formation of this identity. Other participants also
spoke of questioning friends ‘‘over and over again,’’ asking them ‘‘How are you not using condoms?’’ and
articulating that seeing friends pay the consequences for unsafe choices also ‘‘influences you to do the right
thing.’’
Moreover, in addition to the influences of school education and friends’ experiences, Dina, Illisha, and
Kasandra’s talk indicated that their positions within their families and the discourses they encountered in their
family lives were integral to the formation of their identities as responsible role models. Dina took on this
identity in the context of a family with strong religious beliefs against premarital sex, beliefs by which she
took pride in abiding. She spoke of being a ‘‘role model’’ for her younger cousin, wanting to provide the
‘‘right example for her to follow.’’ She elaborated that:
. . .when it comes to asking questions about religion, or what does the Bible say . . . since I have
knowledge and . . . I know about it, she ask me when it comes to things about school, and when she
needs advice she always comes to me.
Dina expressed, ‘‘I’m a virgin and I’m proud of it,’’ and described this decision as something she was
‘‘pretty strong about’’ and had ‘‘thought about’’ at length. In addition to being a role model for her cousin, who
described Dina as her ‘‘inspiration,’’ she spoke of the importance of adhering to the beliefs of her family that
‘‘really care[d]’’ about preserving virginity until marriage. She spoke specifically about wanting to abide by
her mother’s wishes:
I also think about what my mother would think . . . if I do lose my virginity before marriage and she
ever finds out, how she’ll feel. And I think that it’s not fair to her if I do something like that ‘cause of
the way she raised me. There’s no reason why I should not stay a virgin.
Dina spoke of valuing her mother’s praise of her for her decision to remain a virgin, saying that it ‘‘makes
you feel good when someone talks positive about you,’’ which gave her ‘‘more strength to hold back and not
do it.’’ Her image before God also impacted her choice; she said, ‘‘if I were to ever do it, then I would feel
guilty because of the relationship that I have with God,’’ and how that would be ‘‘not pleasant before his
eyes.’’ She further spoke in moral terms of being influenced by ‘‘what’s right and wrong according to [her]
religion.’’
Illisha positioned herself as a responsible role model also in relation to the place she held in her family
and the way she was viewed by her mother. She described her two sisters as having ‘‘led the worst lifestyle
ever,’’ and how as a result she was ‘‘the only one [in her family] that seems to have a good head on [her]
shoulders.’’ She further articulated how her mother often talked to her about sex and heavily influenced her
choices, giving her advice that she had followed to ‘‘wait ‘til you’re ready,’’ until you ‘‘understand what
you’re doing,’’ and to not ‘‘be in a rush’’ to have sex. Illisha described appreciating her mom’s advice, seeing it
as a sign that ‘‘she cares and that . . . she wants to make sure I’m on the right track.’’
In a similar way to Dina, Illisha talked about how she was ‘‘kinda tryin’ to do it [wait to have sex until she
is 18] for [her] mom.’’ Also like Dina, Illisha expressed pride in her choice to wait to have sex, saying that it
‘‘makes you feel so much better about yourself,’’ and setting herself apart from others by asking, ‘‘Who do
IDENTITIES AND SEXUAL HEALTH DECISION-MAKING 753
Journal of Research in Science Teaching
you know that could wait ‘til . . . 18 to lose their virginity? Not too many females do that nowadays.’’
It seemed that for Dina and Illisha, the fervor with which they chose to remain abstinent was tied to issues of
identity, to the senses of self they adhered to, particularly in the context of their families. Virginity being
linked to identity was a significant influence on these girls’ decisions.
Finally, Kasandra took on a responsible role model identity within a family that emphasized the impact
of her choices on her ability to pursue her goal of becoming a doctor. Kasandra spoke of how her aunts,
frequent sources of advice and education for her, did not advise her not to have sex but instead told her to
‘‘make sure no pregnancies, no STDs ‘cause you’re gonna be a doctor someday,’’ and they did not want her to
miss the opportunity to ‘‘do whatever you want.’’ She similarly spoke of how her father was strict with her
because of her future as a doctor:
. . . ever since I have been like 5 years old, I’m gonna, I wanna be a pediatrician. So he thinks that if he
lets me out more . . . that I’m not gonna pursue the goal that I wanna pursue. So he’s tryin’ to do almost
anything to actually keep me on that path so I won’t like, go sideways.
In delivering these messages to Kasandra, her family members contrasted their own past experiences
with what they wanted for her, such as when one aunt said, ‘‘I don’t want you to be like me, 15 with a kid, not
finishin’ high school.’’ For Kasandra, being responsible did not require her to avoid sex, but instead to
‘‘put . . . school before anything else.’’ In addition to family influences, Kasandra also spoke of Mr. P’s role in
keeping her and her classmates on ‘‘a straight line’’ in relation to sexual decisions through his advice,
education, and one-on-one support.
Loving, Trusting Partner
The third identity was that of the loving, trusting partner. This identity was based on the extent
that love and trust in a relationship were central to students’ reasoning around sexual decision-making;
in taking on this identity students positioned themselves within discourses of mutual, faithful commitment.
The themes of love, trust, and relationship dynamics as underlying decisions came up in multiple groups
in various ways as they spoke about their own and others’ sexual health decision-making; however,
the analysis below focuses on the three participants of one focus group (Wil, Olivia, and Luisa), who
positioned themselves most strongly as loving, trusting partners whose sexual decisions depended upon this
identity. This identity seemed to be formed by these participants’ current status as part of committed
relationships.
In contrast to those who took on the strong female identity and linked sexual health decisions with
resisting pressure and standing up to manipulation, these three participants primarily spoke of mutual, shared
decisions to have sex, motivated foremost by the level of love and trust they had with their partner. For
instance, Olivia argued that ‘‘you have to establish trust first before you have sex’’ and critiqued others in her
class for arguing that love was not an essential precursor to sex. In regard to her own decisions, she said:
I stayed abstinent until like sophomore, junior year, junior year, and I’ve been in those circumstances
where I could have had sex but I . . . chose not to because my mind wasn’t in it and my heart either. But
this year . . . I have a boyfriend . . . I’m in a monogamous relationship, so I felt like I could trust the
person so then . . . sex came into place.
Luisa echoed this sentiment. When asked how high school students decide about having sex, she
responded, ‘‘They trust that person. If I love you.’’ Similarly, Wil claimed, ‘‘for some people sex, you don’t
necessarily have to be in love to have sex . . . I have to trust the person before I have sex.’’ He later elaborated:
To me, sex is not something you do, it’s something you feel, like in order to get to that stage when you
feel like you need to have sex, you gotta feel something first . . . you have to have a reason behind it,
and I think the reason behind it is the way you feel about the person, and if you get that same feeling
back, then there’s no problem in, not even making that decision, like you wanna have sex, it just comes
naturally.
754 BROTMAN, MENSAH, AND LESKO
Journal of Research in Science Teaching

In addition to asserting that love and trust were the basis for their decisions to have sex, these participants
all used trust to justify their decisions to stop using condoms in committed relationships. For example, while
at the start of our focus group, Wil claimed that because of the awareness he developed during his high school
sex education, he ‘‘always use[s] a condom every time.’’ Later, he qualified this statement:
But to be honest, I’ve been in a relationship for two and a half years, and I feel like the person I’m with
is the person I’m gonna be with for the rest of my life, so honestly, I don’t feel like I should use
protection ‘cause she’s with me and I’m with her, and we have that connection like we’re not seeing
nobody else but each other . . . even though people tell me, you never know . . . she might lie to
you . . . you should still use a condom, but the way I feel is like, she’s my one and only, I’m her one and
only, there should be no type of line between us like, we’ve built a relationship that we don’t have to lie
to each other . . . so like, with her, I don’t necessarily have to use a condom every time, but even though
I know I should ‘cause I don’t know, but like we’ve made that relationship, we have that bond, that we
can trust each other, so we made the decision to stop usin’ ‘em, but I still use them though.
The back-and-forth nature of the above quotation seems to indicate Wil’s ambivalence about admitting
that he had made a conscious choice not to use condoms because of trust with his partner. Despite repeatedly
justifying why he believed he did not need to use condoms with his current partner, he ended by reverting to
his original claim that, ‘‘I still use them though.’’ This statement suggests that in addition to positioning
himself as a loving, trusting partner in this example, it was important to him, at least in the context of our focus
group, to also position himself as a responsible role model, as someone who made ‘‘responsible’’ choices,
according to what he had been taught in school and elsewhere. This example therefore illustrates how students
sometimes took on multiple identities simultaneously.
Olivia and Luisa in a more straightforward way described their choices not to use condoms with their
long-term partners. They asserted that couples who still used condoms after a long time do so ‘‘because they
have problems,’’ and were ‘‘on and off,’’ which meant that they were uncertain about who their partners had
been with during periods of separation. Olivia further argued, ‘‘Unprotected sex is not safe when you don’t
trust the partner . . .’’ (implying that it is safe if you do). She explained that she trusted her partner because
‘‘before anything happened I got to know him . . . and his family.’’
Decisions about HIV testing were also linked to love and trust for these participants. Luisa and Olivia
revealed that before stopping condom use with their partners, they asked them to get tested. Luisa explained
how, since asking a guy to get tested might ‘‘offend’’ him because it implied that you think he might be ‘‘with a
lot of girls,’’ using love was an effective way for her to convince her partner, to whom she described saying, ‘‘if
you really love me and you wanna protect me, go get yourself tested.’’ Olivia explained how her boyfriend’s
ability to be ‘‘so open’’ about getting tested countered her own shyness around talking about those issues; she
spoke of how together they ‘‘established that trust,’’ enabling her to advocate, ‘‘let’s go to the clinic and get
checked out.’’ Unfortunately, these participants did not reveal how frequently they got tested, or whether they
used other forms of birth control to prevent pregnancy.
Luisa highlighted that her focus group’s commitment to relationships heavily explained their
perspectives on decision-making. She observed: ‘‘I’ve noticed that everybody here, it’s ‘cause they have
something serious. They want to spend the rest of their lives with them so they really want to make sure they
get tested.’’ These comments support how for this group, being in long-term, serious relationships contributed
to the formation of their loving, trusting partner identities. It is also likely that these participants took on this
identity even more strongly because all of them were in similar situations, allowing them to highlight their
loving, trusting partner aspects of themselves during the focus group discussion by relating to each others’
experiences.
Discussion and Implications
Through analyzing identities, this study reveals the intricate ways in which family, gender, religion,
relationships, communities, curriculum, and broader discourses all influence the formation of identities that
contribute to these students’ thinking about decision-making. We argue that looking at sexual health decision-
making—and at decision-making about other controversial science topics—as tied to students’ shifting and
IDENTITIES AND SEXUAL HEALTH DECISION-MAKING 755
Journal of Research in Science Teaching

changing identities provides a useful way for teachers and researchers to grasp the complexity of these
decisions. That is, these decisions are connected to the ways in which students position themselves and are
positioned in their worlds. This complexity talks back to simplistic models of decision-making that portray it
as a uniform, straightforward, individual process, thus complicating the endeavors of educators and
researchers concerned with how school curriculum can influence students’ choices.
In the following discussion, we address three layers of complexity related to sexual health decision-
making illustrated by this study’s analysis of identities, as well as their implications for curriculum and
research. First, this study illustrates how identities related to sexual health decision-making are shaped by
numerous factors in students’ lives. Second, identities, though in some cases overlapping, are also diverse,
showing that students can position themselves in multiple ways in relation to sexual health decision-making.
Third, identities are constructed by societal discourses. In discussing how these discourses are often dominant
ways of framing particular issues, we raise the question of how challenging these discourses might make
alternative identities available to students.
The first layer of complexity in students’ thinking about decision-making revealed by this study is the
extent to which students’ identities are situated within the myriad, multi-leveled contexts of students’ lives.
The ways in which students speak as particular ‘‘selves’’ are linked to their family dynamics, histories, and
relationships; to peer and partner interactions; and to issues of gender and class that play out in their worlds,
all of which influence their identity formation. While school and science learning do in fact play a powerful
role in influencing identities and decision-making in this setting, they do so among these other influences that
stem from students’ unique life experiences (Moore, 2008). For instance, as discussed, the formation of the
responsible role model identity seems to be influenced by familial and religious aspects of students’ lives, as
well as by a science and health education that provided students with thorough knowledge on issues of sexual
health and positioned them as having the potential to influence others. Therefore, this suggests that instead of
considering how the school curriculum in isolation can influence students’ choices, educators might consider
the ways in which school learning interacts with other facets of students’ lives to shape their identities and
ideas about decision-making.
The second layer of complexity revealed by the study is that, in many cases, different students have
different relationships with decision-making—a finding related to the fact that identity formation is affected
by diverse life experiences, as just discussed. Furthermore, even within one individual, these relationships can
change depending on context, situation, and time. This study calls attention to the multiple ways in which
students can position themselves in relation to decision-making. Even in this particular school setting, where
students generally express similar views on the appropriate choices to make (recognizing the importance of
‘‘safe sex,’’ communicating with partners, getting HIV testing), important distinctions arise in the nuances of
those views, depending on the identities they take on.
The strong female identity and the loving, trusting partner identity provide a useful contrast to illustrate
these distinctions. In taking on these different identities, students express significantly different views about
relationships and their involvement in them. In taking on strong female identities, partner relationships are
characterized by pressure, manipulation, and a need to guard oneself against proclamations of love and
expressions of sensitivity that might make one vulnerable. Several of the girls who take on this identity allude
to or proclaim they are abstaining from having sex, and others assert the importance of avoiding being
convinced to not use condoms. Relationships with mothers, in some instances, as opposed to relationships
with partners, are a salient influence on decision-making. In contrast, for those who take on loving, trusting
partner identities, relationships are viewed as places of mutual trust and respect. Sex is an expression of love,
and good relationships are characterized by shared decision-making. These participants, involved in
committed relationships, choose consciously to stop using condoms with their partners because of this trust,
despite acknowledging the theoretical risk of this choice. This identity therefore allows students to justify a
choice that is different from the choices strong females claim to make.
Therefore, taking on different identities can lead to different views on sex and relationships, as well as
different actual choices. And, this is the case even among students who place significantly overlapping value
on concepts such as protected sex and acting ‘‘responsibly,’’ evidenced by the fact that many students who
take on both strong female and loving, trusting partner identities, also take on responsible role model
identities. This illustrates the potential importance of recognizing differences in identities, even subtle ones,
756 BROTMAN, MENSAH, AND LESKO
Journal of Research in Science Teaching

as they have implications for differing ideas and actions around decisions. Furthermore, other settings and
students might reveal even more dramatic distinctions between identities, ideas, and actions around decision-
making than were revealed here.
Moreover, educators who understand these differences in how different students position themselves in
relation to decision-making might use this to inform curricular discussions of decision-making. For instance,
in this school setting, the discourse of making responsible choices that underlies the responsible role model
identity was part of the curriculum and seems, in interaction with other facets of students’ lives, to have
influenced the consistent value students place on safe, responsible choices. However, some of the subtler
points about the influence of relationship dynamics on choices raised by the strong female and loving, trusting
partner identities were less emphasized in the curriculum, although they appear to be a significant influence
on students’ ideas and decisions. With an understanding of the potential impact of these issues on students’
decision-making, the curriculum at multiple grade levels might have more critically addressed relationships
in the context of both gender dynamics as well as ideas about love and trust. Each of these discourses might
resonate differently with different students and provide opportunities for the curriculum to both influence and
challenge students’ ideas and choices even more deeply. Relationship issues in fact have been implicated in
prior literature as influential on sexual health decisions (e.g., Patel, Gutnik, Yoskowitz, O’Sullivan, &
Kaufman, 2006), and this study provides further support for this being an important area to include in
discussions with students about sexual health decision-making.
A final layer of complexity related to decision-making that this study identifies is the ways in which
students’ talk about sexual health decision-making is shaped by discourses about these issues that circulate in
society. Seemingly without being aware of it, several participants positioned themselves within dominant
ideas about gender, teenage pregnancy, success in life, relationships, and morality that reflect common ways
of framing these issues in our society—when in fact there might be alternative ways of framing them and thus
alternative potential identities around sexual health decision-making that could be beneficial to students.
For instance, the strong female identity is deeply embedded in several interacting discourses. First, it
depends heavily on stereotypical ideas about gender that position girls as victims and boys as aggressors in
sexual situations, exemplifying a discourse of ‘‘sexuality as victimization’’ that Fine (1988) argues is
prevalent in US schools in relation to female sexuality. One consequence of this discourse is that it perpetuates
binary ideas that describe girls as one way and boys as another. Fine highlights how this discourse limits
acknowledgement of girls’ desires for sexual activity (positioning them instead as always resisting the
advances of boys). It similarly fails to recognize that boys do not have to be ‘‘jerks’’ who ruthlessly take
advantage of girls. Furthermore, it is clear how this discourse also perpetuates the idea that heterosexuality is
the norm. If these discourses were discussed and analyzed with students, a different kind of strong female
identity might be made possible—one that maintains the confidence and strength these girls exuded without
positioning it exclusively within binary ideas about the roles girls versus boys play in sexual situations, and
within visions of relationships that are inevitably centered around avoidance of manipulation.
Another discourse underlying the strong female identity that might be worthy of further examination
with students is the idea that individuals are in complete control of their decisions. The participants, angered
by the struggling circumstances in which they see their family and peers, echo popular discourses of
‘‘individual responsibility and self-control’’ (Burns & Torre, 2004, p. 133) that view individuals as solely to
blame for making ‘‘bad decisions.’’ Harris (2004) provides a detailed analysis of how, through this prevalent
discourse, girls in today’s society are ‘‘disciplined into creating their own successful life trajectories and
taking personal responsibility if they fail’’ (p. 10). She describes the resulting construction of two opposing
kinds of girls: the ‘‘can do’’ and the ‘‘at risk’’ girls. The ‘‘can do’’ girls, the face of success in modern society,
are positioned as being able to achieve anything through their own strength, confidence, and personal merit;
the ‘‘at risk’’ girls are those who fail because of their own personal deficiencies. Unable to take control of their
lives, the narrative continues that they often end up following life paths that are looked down upon, such as
becoming teen mothers.
Strong female participants’ calls for taking responsibility for your own decisions, and their critiques of
young pregnant peers for whom ‘‘life is over’’ can in part be understood through linking their words to the
discourses that divide ‘‘can do’’ from ‘‘at risk’’ girls. These participants may also be drawing on what Tolman
(2002) describes as a ‘‘master narrative of ruination’’ (p. 177)—commonly used by the girls living in urban
IDENTITIES AND SEXUAL HEALTH DECISION-MAKING 757
Journal of Research in Science Teaching

environments in her study of young women’s sexual desire. That is, unlike girls interviewed from suburban
communities, urban girls fear that their lives could be ‘‘ruined’’ by poor choices around sexuality,
indoctrinated with this belief by family members and others. Finally, the strong female identity also perhaps
draws upon aspects of what Hill Collins (2000) calls ‘‘Black feminist thought.’’ Hill Collins traces the
historical roots of what she describes as Black women’s frequent prioritization of ‘‘self-reliance and
independence’’ (p. 116), values often transferred within typically strong relationships between powerful
mothers and their daughters. These ideas perhaps relate in particular to Illisha’s strong relationship with her
mother, who she praises for being ‘‘a real independent woman.’’
In reaction to these narratives of individual responsibility and self-reliance, many scholars emphasize
how young people’s decisions might instead be understood within a larger societal context, where, in addition
to personal responsibility, inequitable policies and societal conditions may also play a role in their actions.
For instance, Fine and McClelland (2006) argue for ‘‘policies and research that recognize how macro-
structures, public institutions, practices, and relationships affect ‘personal decisions,’ particularly for those
without private supports and buffers’’ (p. 328). They argue that inequitable conditions of high poverty
communities in areas such as education and health care, in addition to a lack of access to comprehensive sex
education, all contribute to people’s choices. Harris (2004) similarly argues that the consequence of
exclusively emphasizing the power of personal, individual effort is that, ‘‘Structural disadvantage is recast as
poor personal choices, laziness, and incompetent family practices’’ (p. 25).
The findings and implications from this study raise questions of how curriculum in science and health
might support students in taking on identities that recognize both their own agency and power over their lives,
as well as the nuances of how societal context and macro-structures influence people’s circumstances. In fact,
striking this balance between agency and recognition of potential structural limitations might contribute to
the development of the kind of scientific literacy through which ‘‘individuals with different expertise
coparticipate in resolving the complex problems that their communities, countries, and humanity as a whole
face today’’ (Roth & Calabrese Barton, 2004, p. 13). Creating science and health curriculum that impacts
students’ personal decisions as well as their broader awareness of the complex structural and social influences
on people’s choices is an important consideration in light of the emerging shift in the field of health education
from individualistic to more socio-ecological frameworks for understanding decision-making.
A similar analysis can be done of the discourses that construct each of the other identities as well. For
instance, the responsible role model identity to a certain extent draws upon discourses that frame sexuality in
terms of ‘‘right’’ and ‘‘wrong.’’ These kinds of associations between particular sexual behaviors and morality
are integral to how sexuality is framed in political and social discourse in the US. For instance, currently,
federal funding for sex education exclusively supports abstinence-only programs; these programs are
required to not only discourage young people from having sex and prohibit advocacy for contraception, but
they also must privilege marriage as the appropriate place for sexual activity and, ‘‘teach that sexual activity
outside of marriage is wrong and harmful’’ (Guttmacher Institute, 2006), an indication of the moral ideology
behind this legislation. The sociohistorical roots of this morally-charged emphasis on abstinence until
marriage have been examined by several scholars (e.g., Irvine, 2002; Luker, 2006). The value placed on long-
term, committed relationships by those speaking as loving, trusting partners, while not focused on marriage,
in some ways also echoes this societal privileging of monogamy.
While neither those taking on responsible role model nor loving, trusting partner identities exactly
mirror these discourses about morality, abstinence, and marriage as the only appropriate context for sexual
activity, aspects of their talk are linked to these moral messages and ways of framing these issues that are so
widespread in broader contexts. These kinds of dominant discourses within which students situate
themselves, even partially or without intending to, and the implications of those discourses for themselves
and others, might be a useful object of analysis and conversation between teachers and students within science
and health classrooms.
Relevance to Science Education
While this study has clear relevance to health and sex education, we argue that the findings and
implications discussed above have direct relevance in the field of science education as well. First, US science
teachers are often required to address topics related to sexual health in science classes. For example, in New
758 BROTMAN, MENSAH, AND LESKO
Journal of Research in Science Teaching
York City, the 11th grade Regents biology curriculum covers the reproductive system as well as HIV/AIDS in
the context of the immune system. In addition, New York City has a mandated K-12 HIV/AIDS curriculum,
often taught by science teachers; beyond covering the biology of HIV/AIDS, this curriculum explicitly aims
to influence students’ sexual health decision-making (NYC Department of Education, 2005). This study
suggests that curriculum efforts such as these might consider the complexity of students’ decision-making
and its potential connections to identities, if the aim of affecting students’ decisions is to be realized.
Moreover, beyond the specific topic of sexual health, there is increasing focus in the field of science
education on curriculum and teaching that aims to influence students’ ability to make decisions about
controversial science topics (Sadler & Zeidler, 2009). The field has already acknowledged and investigated
the ways in which morality, intuition, and emotion are critical for socioscientific decision-making and
therefore cannot be ignored in science classrooms (Sadler & Zeidler, 2005). Researchers have even proposed
that science education become a vehicle for the development of students’ moral sensitivity (Fowler, Zeidler,
& Sadler, 2009) and for character education (Zeidler, Sadler, Applebaum, & Callahan, 2009). However, there
is considerably less emphasis in the science education literature about controversial science topics on the
other aspects of students’ lives and identities that presumably influence their decisions. While these kinds of
broader influences on students’ science-related decisions have been acknowledged as important and even
noted as secondary findings (Sadler & Zeidler, 2003), the specific ways in which family, relationships,
personal experiences, societal discourses, and other influences factor into decision-making typically remain
as peripheral considerations in the literature on controversial science topics. We argue that these aspects of
students’ worlds that potentially influence identity formation and decision-making should be a direct object
of investigation in science education, and we contribute to that investigation with this study.
Also critical to consider are the specific ways in which science knowledge and learning influence and
interact with students’ identities and decisions. While we touch upon this issue briefly in this article,
particularly in reference to how the responsible role model identity is formed by a combination of a thorough
science and health education and outside factors, we investigate this question more thoroughly elsewhere—
and show how science knowledge and learning become important to students’ thinking about sexual health
decision-making when they resonate with students’ forming identities (Brotman, 2009). The purpose of the
present study, however, is to begin to uncover the myriad influences upon and complexities inherent in
science-related decision-making.
Further, we intend for this study to provide a framework for future science education research that aims
to understand the relationship between identities and decision-making related to other controversial science
topics. For instance, what identities do students take on in relation to environmental issues, such as global
climate change, or other health issues, such as nutrition? How are those identities embedded within the multi-
leveled contexts of those students’ lives? Investigating questions such as these could potentially inform more
influential science curriculum and teaching about these issues.
In addition to investigating identities related to controversial science topics through research, this study
also suggests that science curriculum and teaching focused on decision-making address issues of identity.
That is, how might we find ways for teachers to elicit students’ identities in relation to decision-making
through curriculum, and to apply those understandings of students’ identities to curricular learning? Further,
how can science classes focused on decision-making engage students in an examination of the influence of
identities, life experiences, and discourses on decision-making about controversial science topics?
These questions raise the point that, if a significant aim of science education is to prepare students to
make decisions in their lives, it may be necessary to expand the parameters of what kinds of topics are
typically addressed in science classes, as has been suggested elsewhere (Fensham, 2009; Sadler & Zeidler,
2009). Admittedly, this is not a simple task. The literature already highlights the challenges science teachers
face addressing controversial science topics, particularly in relation to teachers’ discomfort in mixing science
with ethics and values (Sadler, Amirschokoohi, Kazempour, & Allspaw, 2006). One potential strategy for
supporting teachers in expanding the boundaries of science education might be collaboration with teachers of
other disciplines, such as health (Harrison, 2005) and the humanities (Moje et al., 2004). Despite the
challenges it entails, we argue that acknowledging in science curriculum that science-related decision-
making is tied to issues of identity will potentially allow science education to have a more prominent impact
on students’ decisions.
IDENTITIES AND SEXUAL HEALTH DECISION-MAKING 759
Journal of Research in Science Teaching
Note
1This study is part of a larger study that investigated students’ learning about HIV/AIDS in different contexts of
their lives, in addition to their identities around decision-making. Therefore, questions about students’ learning were
addressed during these focus groups as well, and these data are reported elsewhere (Brotman, 2009).
The authors would like to thank the students and teachers who participated in this study.
References
Aikenhead, G.S. (2006). Science education for everyday life: Evidence based practice. New York: Teachers College
Press.
Aikenhead, G.S., & Jegede, O.J. (1999). Cross-cultural science education: A cognitive explanation of a cultural
phenomenon. Journal of Research in Science Teaching, 36(3), 269–287.
Bettie, J. (2003). Women without class: Girls, race, and identity. Berkeley, CA: University of California Press.
Brickhouse, N.W. (2001). Embodying science: A feminist perspective on learning. Journal of Research in Science
Teaching, 38(3), 282–295.
Brickhouse, N.W., Lowery, P., & Schultz, K. (2000). What kind of girl does science? The construction of school
science identities. Journal of Research in Science Teaching, 37(5), 441–458.
Bronfenbrenner, U. (1979). The ecology of human development. Cambridge, MA: Harvard University Press.
Brotman, J.S. (2009). Urban high school students’ talk about HIV/AIDS decision-making: Learning, identities, and
the influence of school. Ph.D. Dissertation, Columbia University, New York. Retrieved December 18, 2009, from
Dissertations & Theses: Full Text (Publication No. AAT 3373708).
Buckingham, D., & Bragg, S. (2004). Young people, sex and the media: The facts of life? Houndmills & New York:
Palgrave.
Burns, A., & Torre, M.E. (2004). Shifting desires: Discourses of accountability in abstinence-only education in the
United States. In A. Harris (Ed.), All about the girl: Culture, power, and identity (pp. 127–137). New York: Routledge.
Carlone, H.B., & Johnson, A. (2007). Understanding the science experiences of women of color: Science identity as
an analytic lens. Journal of Research in Science Teaching, 44(8), 1187–1218.
Charmaz, K. (2006). Constructing grounded theory: A practical guide through qualitative analysis. London: Sage
Publications Ltd.
Creswell, J.W. (2007). Qualitative inquiry and research design: Choosing among five approaches (2nd ed.) Thousand
Oaks: Sage Publications, Inc.
Davies, B. (1989). The discursive production of the male/female dualism in school settings. Oxford Review of
Education, 15(3), 229–241.
Davies, B. (1994). Poststructuralist theory and classroom practice. Melbourne: Deakin University.
Davies, B. (2000). A body of writing 1990–1999. Walnut Creek, CA: AltaMira Press.
DeBoer, G.E. (2000). Scientific literacy: Another look at its historical and contemporary meanings and its
relationship to science education reform. Journal of Research in Science Teaching, 37(6), 582–601.
DiClemente, R.J., Salazar, L.F., & Crosby, R.A. (2007). A review of STD/HIV preventive interventions for
adolescents: Sustaining effects using an ecological approach. Journal of Pediatric Psychology, 32(8), 888–906.
DiClemente, R.J., Salazar, L.F., Crosby, R.A., & Rosenthal, S.L. (2005). Prevention and control of sexually
transmitted infections among adolescents: The importance of a socio-ecological perspective—A commentary. Public
Health, 119, 825–836.
Emerson, R.M., Fretz, R.I., & Shaw, L.L. (1995). Writing ethnographic fieldnotes. Chicago: University of Chicago
Press.
Fensham, P.J. (2009). Real world contexts in PISA science: Implications for context-based science education. Journal
of Research in Science Teaching, 46(8), 884–896.
Fine, M. (1988). Sexuality, schooling, and adolescent females: The missing discourse of desire. Harvard Educational
Review, 58(1), 29–52.
Fine, M., & McClelland, S.I. (2006). Sexuality education and desire: Still missing after all these years. Harvard
Educational Review, 76(3), 297–338.
Fowler, S.R., Zeidler, D.L., & Sadler, T.D. (2009). Moral sensitivity in the context of socioscientific issues in high
school science students. International Journal of Science Education, 31(2), 279–296.
Gee, J.P. (1997). Forward: A discourse approach to language and literacy. In C. Lankshear, Changing literacies
(pp. xiii–xix). Buckingham, UK: Open University Press.
Glaser, B., & Strauss, A. (1967). The discovery of grounded theory. Chicago: Aldine.
760 BROTMAN, MENSAH, AND LESKO
Journal of Research in Science Teaching
Grace, M.M., & Ratcliffe, M. (2002). The science and values that young people draw upon to make decisions about
biological conservation issues. International Journal of Science Education, 24(11), 1157–1169.
Guba, E., & Lincoln, Y. (1989). Judging the quality of fourth generation evaluation. In Fourth generation evaluation
(pp. 228–251). Newbury Park, CA: Sage.
Guttmacher Institute. (2006). Facts on sex education in the United States. Retrieved June 24, 2007, from http:/ /
www.guttmacher.org/pubs/fb_sexEd2006.html.
Harris, A. (2004). Future girl: Young women in the twenty-first century. New York: Routledge.
Harrison, J.K. (2005). Science education and health education: Locating the connections. Studies in Science
Education, 41, 51–90.
Hill Collins, P. (2000). Black feminist thought: Knowledge, consciousness, and the politics of empowerment
(2nd ed.). New York: Routledge.
Holland, D., Lachicotte, W., Jr., Skinner, D., & Cain, C. (1998). Identity and agency in cultural worlds. Cambridge,
MA: Harvard University Press.
Hollway, W., & Jefferson, T. (2000). Doing qualitative research differently: Free association, narrative and the
interview method. London: Sage Publications.
Hughes, G. (2001). Exploring the availability of student scientist identities within curriculum discourse: An anti-
essentialist approach to gender-inclusive science. Gender and Education, 13(3), 275–290.
Irvine, J.M. (2002). Talk about sex: The battles over sex education in the United States. Berkeley: University of
California Press.
Keselman, A., Kaufman, D.R., Kramer, S., & Patel, V.L. (2007). Fostering conceptual change and critical reasoning
about HIV and AIDS. Journal of Research in Science Teaching, 44(6), 844–863.
Kolstø, S.D. (2006). Patterns in students’ argumentation confronted with a risk-focused socio-scientific issue.
International Journal of Science Education, 28(14), 1689–1716.
Lesko, N. (2001). Act your age! A cultural construction of adolescence. New York: Routledge Falmer.
Luker, K. (2006). When sex goes to school: Warring views on sex—and sex education—since the sixties. New York:
W.W. Norton & Company.
Merriam, S.B. (1998). Qualitative research and case study applications in education. San Francisco: Jossey-Bass.
Moje, E., Ciechanowski, K., Kramer, K., Ellis, L., Carrillo, R., & Collazo, T. (2004). Working toward third space in
content area literacy: An examination of everyday funds of knowledge and Discourse. Reading Research Quarterly, 39(1),
38–70.
Moore, F.M. (2008). Positional identity and science teacher professional development. Journal of Research in Science
Teaching, 45(6), 684–710.
Morgan, D.L. (1997). Focus groups as qualitative research (2nd ed.) Thousand Oaks: Sage Publications, Inc.
Muhr, T. (1997/2005). Atlas.ti (Version 5.2 for Windows). Berlin: Atlas.ti Scientific Software Development GmBh.
Mutonyi, H., Nielsen, W., & Nashon, S. (2007). Building scientific literacy in HIV/AIDS education: A case study of
Uganda. International Journal of Science Education, 29(11), 1363–1385.
NYC Department of Education. (2005). The updated HIV/AIDS curriculum. Retrieved January 11, 2009, from
http:/ /schools.nyc.gov/Academics/FitnessandHealth/StandardsCurriculum/HIVAIDScurriculum.
Patel, V.L., Gutnik, L.A., Yoskowitz, N.A., O’Sullivan, L.F., & Kaufman, D.R. (2006). Patterns of reasoning and
decision making about condom use by urban college students. AIDS Care, 18(8), 918–930.
Ratcliffe, M. (1997). Pupil decision-making about socio-scientific issues within the science curriculum. International
Journal of Science Education, 19(2), 167–182.
Reyna, V.F., & Farley, F. (2006). Risk and rationality in adolescent decision making: Implications for theory, practice,
and public policy. Psychological Science in the Public Interest, 7(1), 1–44.
Roth, W.-M., & Calabrese Barton, A. (2004). Rethinking scientific literacy. New York: Routledge.
Sadler, T.D. (2004). Informal reasoning regarding socioscientific issues: A critical review of research. Journal of
Research in Science Teaching, 41(5), 513–536.
Sadler, T.D., Amirschokoohi, A., Kazempour, M., & Allspaw, K.M. (2006). Socioscience and ethics in science
classrooms: Teacher perspectives and strategies. Journal of Research in Science Teaching, 43(4), 353–376.
Sadler, T.D., & Zeidler, D.L. (2003). The morality of socioscientific issues: Construal and resolution of genetic
engineering dilemmas. Science Education, 88(1), 4–27.
Sadler, T.D., & Zeidler, D.L. (2005). Patterns of informal reasoning in the context of socioscientific decision making.
Journal of Research in Science Teaching, 42(1), 112.
Sadler, T.D., & Zeidler, D.L. (2009). Scientific literacy, PISA, and socioscientific discourse: Assessment for
progressive aims of science education. Journal of Research in Science Teaching, 46(8), 909–921.
Strauss, A.L., & Corbin, J. (1998). Basics of qualitative research: Techniques and procedures for developing
grounded theory (2nd ed.) Thousand Oaks: Sage Publications, Inc.
IDENTITIES AND SEXUAL HEALTH DECISION-MAKING 761
Journal of Research in Science Teaching
Tolman, D.L. (2002). Dilemmas of desire: Teenage girls talk about sexuality. Cambridge, MA: Harvard University
Press.
Ward, J.V., & Taylor, J.M. (1992). Sexuality education for immigrant and minority students: Developing a culturally
appropriate curriculum. In J.T. Sears (Ed.), Sexuality and the curriculum: The politics and practices of sexuality education
(pp. 183–202). New York: Teachers College Press.
Zeidler, D.L., Sadler, T.D., Applebaum, S., & Callahan, B.E. (2009). Advancing reflective judgment through
socioscientific issues. Journal of Research in Science Teaching, 46(1), 74–101.
Zeidler, D.L., Sadler, T.D., Simmons, M.L., & Howes, E.V. (2005). Beyond STS: A research-based framework for
socioscientific issue education. Science Education, 89(3), 357–377.
Appendix: Focus Group Protocol
(1) How do you think high school students decide whether or not to have sex?
(2) How do you think high school students decide whether or not to use condoms (/have safe sex)?
(3) How do you think high school students decide whether or not to talk to their partners about using
condoms (/safe sex)?
(4) How do you think high school students decide whether or not to get tested for HIV?
(5) How do you think high school students decide whether or not to talk to their partners about getting
tested for HIV?
(6) What other kinds of decisions do high school students have to make about these issues?
(a) For each of the above scenarios, prompt as needed:
(i) What do they think about?
(ii) What goes through their heads when deciding?
(iii) What kinds of things affect their decisions?
(iv) What has the biggest affect on their decisions?
(7) How do you think school learning influences high school students’ decisions (at this school)?
(a) Ask specifically about what they took away from 9th, 11th, and 12th grade health/science
classes, if they don’t come up.
(8) What do you think would make school learning more relevant to your lives and decisions/more
influential?
(a) Is there anything you wanted to learn about but didn’t in school? What was missing?
(9) Is there anything else you’d like to say about this topic?
762 BROTMAN, MENSAH, AND LESKO
Journal of Research in Science Teaching
Related Documents











