OBSTETRICS Identification of patients at risk for early onset and/or severe preeclampsia with the use of uterine artery Doppler velocimetry and placental growth factor Jimmy Espinoza, MD; Roberto Romero, MD; Jyh Kae Nien, MD; Ricardo Gomez, MD; Juan Pedro Kusanovic, MD; Luis F. Gonçalves, MD; Luis Medina, MD; Sam Edwin, PhD; Sonia Hassan, MD; Mario Carstens, MD; Rogelio Gonzalez, MD OBJECTIVE: Preeclampsia has been proposed to be an antiangio- genic state that may be detected by the determination of the con- centrations of the soluble vascular endothelial growth factor recep- tor-1 (sVEGFR-1) and placental growth factor (PlGF) in maternal blood even before the clinical development of the disease. The pur- pose of this study was to determine the role of the combined use of uterine artery Doppler velocimetry (UADV) and maternal plasma PlGF and sVEGFR-1 concentrations in the second trimester for the identification of patients at risk for severe and/or early onset preeclampsia. STUDY DESIGN: A prospective cohort study was designed to examine the relationship between abnormal UADV and plasma concentrations of PlGF and sVEGFR-1 in 3348 pregnant women. Plasma samples were obtained between 22 and 26 weeks of gestation at the time of ultrasound examination. Abnormal UADV was defined as the presence of bilateral uterine artery notches and/or a mean pulsatility index above the 95th percentile for the gestational age. Maternal plasma PlGF and sVEGFR-1 concentrations were determined with the use of sensitive and specific immunoassays. The primary outcome was the develop- ment of early onset preeclampsia (34 weeks of gestation) and/or severe preeclampsia. Secondary outcomes included preeclampsia, the delivery of a small for gestational age (SGA) neonate without pre- eclampsia, spontaneous preterm birth at 32 and 35 weeks of ges- tation, and a composite of severe neonatal morbidity. Contingency ta- bles, chi-square test, receiver operating characteristic curve, and multivariate logistic regression were used for statistical analyses. A probability value of .05 was considered significant. RESULTS: (1) The prevalence of preeclampsia, severe preeclampsia, and early onset preeclampsia were 3.4% (113/3296), 1.0% (33/3296), and 0.8% (25/3208), respectively. UADV was performed in 95.4% (3146/3296) and maternal plasma PlGF concentrations were deter- mined in 93.5% (3081/3296) of the study population. (2) Abnormal UADV and a maternal plasma PlGF of 280 pg/mL were independent risk factors for the occurrence of preeclampsia, severe preeclampsia, early onset preeclampsia, and SGA without preeclampsia. (3) Among patients with abnormal UADV, maternal plasma PlGF concentration contributed significantly in the identification of patients destined to de- velop early onset preeclampsia (area under the curve, 0.80; P .001) and severe preeclampsia (area under the curve, 0.77; P .001). (4) In contrast, maternal plasma sVEGFR-1 concentration was of limited use in the prediction of early onset and/or severe preeclampsia. (5) The combination of abnormal UADV and maternal plasma PlGF of 280 pg/mL was associated with an odds ratio (OR) of 43.8 (95% CI, 18.48- 103.89) for the development of early onset preeclampsia, an OR of 37.4 (95% CI, 17.64-79.07) for the development of severe preeclampsia, an OR of 8.6 (95% CI, 5.35-13.74) for the development of preeclampsia, and an OR of 2.7 (95% CI, 1.73-4.26) for the delivery of a SGA neonate in the absence of preeclampsia. CONCLUSION: The combination of abnormal UADV and maternal plasma PlGF concentration of 280 pg/mL in the second trimester is associated with a high risk for preeclampsia and early onset and/or severe preeclampsia in a low-risk population. Among those with ab- normal UADV, a maternal plasma concentration of PlGF of 280 pg/mL identifies most patients who will experience early onset and/or severe preeclampsia. From the Perinatology Research Branch, NICHD/NIH/DHHS, Bethesda, MD, and Detroit, MI (Drs Espinoza, Romero, Nien, Kusanovic, Gonçalves, Edwin, and Hassan); the Department of Obstetrics and Gynecology, Wayne State University/Hutzel Hospital (Drs Espinoza, Gonçalves, and Hassan), and the Center for Molecular Medicine and Genetics, Wayne State University (Dr Romero), Detroit, MI; and CEDIP, Department of Obstetrics and Gynecology, Sotero del Rio Hospital, Puente Alto, Chile (Drs Gomez, Medina, Carstens, and Gonzalez). Reprints not available from the authors. Address correspondence to Roberto Romero, MD, Perinatology Research Branch, NICHD/NIH/DHHS, Wayne State University/Hutzel Women’s Hospital, 3990 John R, Box 4, Detroit, MI 48201; warfi[email protected] Supported by the Intramural Research Program of the National Institute of Child Health and Human Development, NIH, DHHS. 0002-9378/$32.00 © 2007 Mosby, Inc. All rights reserved. doi: 10.1016/j.ajog.2006.11.002 Research www. AJOG.org 326.e1 American Journal of Obstetrics & Gynecology APRIL 2007

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

O
IpvJL
OgctbpuPip
Stowuotsamsdetbmp
FGGCG
RW
S
0©d
Research www.AJOG.org
3
BSTETRICS
dentification of patients at risk for early onset and/or severereeclampsia with the use of uterine artery Dopplerelocimetry and placental growth factor
immy Espinoza, MD; Roberto Romero, MD; Jyh Kae Nien, MD; Ricardo Gomez, MD; Juan Pedro Kusanovic, MD;uis F. Gonçalves, MD; Luis Medina, MD; Sam Edwin, PhD; Sonia Hassan, MD; Mario Carstens, MD; Rogelio Gonzalez, MD
Raa(mUrepcvacicp1(oOa
Cpasnps
BJECTIVE: Preeclampsia has been proposed to be an antiangio-enic state that may be detected by the determination of the con-entrations of the soluble vascular endothelial growth factor recep-or-1 (sVEGFR-1) and placental growth factor (PlGF) in maternallood even before the clinical development of the disease. The pur-ose of this study was to determine the role of the combined use ofterine artery Doppler velocimetry (UADV) and maternal plasmalGF and sVEGFR-1 concentrations in the second trimester for the
dentification of patients at risk for severe and/or early onsetreeclampsia.
TUDY DESIGN: A prospective cohort study was designed to examinehe relationship between abnormal UADV and plasma concentrationsf PlGF and sVEGFR-1 in 3348 pregnant women. Plasma samplesere obtained between 22 and 26 weeks of gestation at the time ofltrasound examination. Abnormal UADV was defined as the presencef bilateral uterine artery notches and/or a mean pulsatility index abovehe 95th percentile for the gestational age. Maternal plasma PlGF andVEGFR-1 concentrations were determined with the use of sensitivend specific immunoassays. The primary outcome was the develop-ent of early onset preeclampsia (�34 weeks of gestation) and/or
evere preeclampsia. Secondary outcomes included preeclampsia, theelivery of a small for gestational age (SGA) neonate without pre-clampsia, spontaneous preterm birth at �32 and �35 weeks of ges-ation, and a composite of severe neonatal morbidity. Contingency ta-les, chi-square test, receiver operating characteristic curve, andultivariate logistic regression were used for statistical analyses. A
robability value of �.05 was considered significant.
rom the Perinatology Research Branch, NICHD/NIH/DHHS, Betheonçalves, Edwin, and Hassan); the Department of Obstetrics and Gonçalves, and Hassan), and the Center for Molecular Medicine andEDIP, Department of Obstetrics and Gynecology, Sotero del Rio Hoonzalez).
eprints not available from the authors. Address correspondence to Robayne State University/Hutzel Women’s Hospital, 3990 John R, Box 4,
upported by the Intramural Research Program of the National Institute
002-9378/$32.002007 Mosby, Inc. All rights reserved.
oi: 10.1016/j.ajog.2006.11.002
26.e1 American Journal of Obstetrics & Gynecology APRIL 2007
ESULTS: (1) The prevalence of preeclampsia, severe preeclampsia,nd early onset preeclampsia were 3.4% (113/3296), 1.0% (33/3296),nd 0.8% (25/3208), respectively. UADV was performed in 95.4%3146/3296) and maternal plasma PlGF concentrations were deter-ined in 93.5% (3081/3296) of the study population. (2) AbnormalADV and a maternal plasma PlGF of �280 pg/mL were independent
isk factors for the occurrence of preeclampsia, severe preeclampsia,arly onset preeclampsia, and SGA without preeclampsia. (3) Amongatients with abnormal UADV, maternal plasma PlGF concentrationontributed significantly in the identification of patients destined to de-elop early onset preeclampsia (area under the curve, 0.80; P � .001)nd severe preeclampsia (area under the curve, 0.77; P � .001). (4) Inontrast, maternal plasma sVEGFR-1 concentration was of limited usen the prediction of early onset and/or severe preeclampsia. (5) Theombination of abnormal UADV and maternal plasma PlGF of �280g/mL was associated with an odds ratio (OR) of 43.8 (95% CI, 18.48-03.89) for the development of early onset preeclampsia, an OR of 37.495% CI, 17.64-79.07) for the development of severe preeclampsia, an ORf 8.6 (95% CI, 5.35-13.74) for the development of preeclampsia, and anR of 2.7 (95% CI, 1.73-4.26) for the delivery of a SGA neonate in thebsence of preeclampsia.
ONCLUSION: The combination of abnormal UADV and maternallasma PlGF concentration of �280 pg/mL in the second trimester isssociated with a high risk for preeclampsia and early onset and/orevere preeclampsia in a low-risk population. Among those with ab-ormal UADV, a maternal plasma concentration of PlGF of �280g/mL identifies most patients who will experience early onset and/orevere preeclampsia.
, MD, and Detroit, MI (Drs Espinoza, Romero, Nien, Kusanovic,cology, Wayne State University/Hutzel Hospital (Drs Espinoza,netics, Wayne State University (Dr Romero), Detroit, MI; andital, Puente Alto, Chile (Drs Gomez, Medina, Carstens, and
o Romero, MD, Perinatology Research Branch, NICHD/NIH/DHHS,roit, MI 48201; [email protected]
hild Health and Human Development, NIH, DHHS.
sdayneGesp
ertDet
of C

Kp
Ca
PehFttgpptid
lmgrmb2tdcpooatcgm(tttfgcttmagmrfp
www.AJOG.org Obstetrics Research
ey words: gestational hypertension, placental growth factor (PlGF),
reeclampsia. and use of samples wa
rowth factor receptor-1 (VEGFR-1), uterine artery Doppler
reeclampsia, small for gestational age, soluble vascular endothelial velocimetry, vascular endothelial growth factor (VEGF)ite this article as: Espinoza J, Romero R, Nien JK, et al. Identification of patients at risk for early onset and/or severe preeclampsia with the use of uterinertery Doppler velocimetry and placental growth factor. Am J Obstet Gynecol 2007;196:326.e1-326.e13.
reeclampsia is a leading cause of preg-nancy-related maternal death.1-3 The
arlier the gestational age at diagnosis, theigher the risk of maternal death exists.1
or example, the risk of maternal death is 4imes higher if preeclampsia develops be-ween 32 weeks of gestation than after thisestational age. Thus, the identification ofatients at risk for severe and/or early onsetreeclampsia followed by prophylactic in-erventions may prevent or delay the clin-cal presentation of the disease and/or re-uce its severity.Abnormal uterine artery Doppler ve-
ocimetry (UADV)4-8 as well as abnormalaternal plasma concentration of proan-
iogenic and antiangiogenic factors areisk factors for the subsequent develop-ent of preeclampsia.9-14 Recently, it has
een reported that UADV between 22 and5 weeks of gestation is the “best test” forhe identification of patients destined toevelop preeclampsia, compared with bio-hemical indicators in the maternallasma, such as markers for (1) lipid per-xidation (F2-isoprostane), (2) total anti-xidant capacity of plasma (ferric reducingbility of plasma and uric acid concentra-ions), (3) antioxidant enzymes in erythro-ytes (catalase, superoxide dismutase, andlutathione peroxidase), (4) putativearkers for endothelial cell dysfunction
von Willebrand factor, plasminogen ac-ivator inhibitor types 1 and 2, andhrombomodulin), and (5) pro- and an-iangiogenic factors (placental growthactor [PlGF], vascular endothelialrowth factor [VEGF], and soluble vas-ular endothelial growth factor recep-or-1 [sVEGFR-1]).15 The purpose ofhis study was to determine whether the
aternal plasma concentration of thengiogenic factor PlGF and the antian-iogenic factor sVEGFR-1 in the mid tri-ester of pregnancy can improve the
isk assessment determined by UADVor severe and/or early onset
MATERIAL AND METHODS
Study designA prospective cohort study was con-ducted between January 1998 and April2004 to examine the relationship be-tween UADV and plasma concentra-tions of PlGF and sVEGFR-1 in pregnantwomen. Plasma samples were obtainedat the time of ultrasound examinationbetween 22 and 26 weeks of gestation.Preeclampsia was diagnosed in the pres-ence of gestational hypertension (sys-tolic blood pressure �140 mm Hg or di-astolic blood pressure �90 mm Hg on atleast 2 occasions, 6 hours to 1 weekapart) and proteinuria (�300 mg in a24-hour urine collection or 1 dipstickmeasurement of �2�). Patients withpreeclampsia were subclassified as eitherearly-onset (�34 weeks of gestation) orlate-onset (�34 weeks of gestation) dis-ease according to the gestational age atwhich preeclampsia was diagnosed. Se-vere preeclampsia was defined as severegestational hypertension (diastolicblood pressure �110 mm Hg) and mildproteinuria or mild gestational hyper-tension and severe proteinuria (a 24-hour urine sample that contained �3.5 gprotein or a urine specimen of �3� pro-tein by dipstick measurement). Patientswith an abnormal liver function test (as-partate aminotransferase �70 IU/L) andthrombocytopenia (platelet count�100,000/cm3) were also classified ashaving severe preeclampsia. Small forgestational age (SGA) neonate was de-fined as a birthweight of �10th percen-tile for the gestational age at birth, ac-cording to the national birthweightdistribution of a Hispanic population.16
Patients with chronic hypertension,multiple pregnancies, fetal anomalies, orchronic renal disease were excludedfrom the study. All women providedwritten informed consent before the col-lection of plasma samples. The collection
Human Investigation Committee of theSotero del Rio Hospital, Santiago, Chile(an affiliate of the Pontificia CatholicUniversity of Santiago), and the Institu-tional Review Board of the National In-stitute of Child Health and Human De-velopment of the National Institutes ofHealth.
UADVFive experienced sonographers per-formed Doppler ultrasound of the uter-ine arteries at the time of blood samplingusing real-time ultrasound equipment(ACUSON 128-XP; Acuson Corporation,Mountain View, CA) with a 3.5-MHz or a5-MHz curvilinear probe. The right andleft uterine arteries were identified in anoblique plane of the pelvis at the crossoverwith the external iliac arteries, and theDoppler signals were sampled. When 3similar consecutive waveforms were ob-tained, the pulsatility index of the right andleft uterine arteries were measured, and themean pulsatility index of the 2 vessels wascalculated. The presence of an early dia-stolic notch in the uterine arteries was de-termined according to the criteria pro-posed by Bower et al.17 An abnormalUADV was defined as the presence of bi-lateral uterine artery notches and/or amean pulsatility index of �95th percentilefor the gestational age.
Sample collection and humansVEGFR-1 immunoassayVenipuncture was performed, and theblood was collected into tubes that con-tained EDTA. The samples were centri-fuged for 10 minutes at 4°C and stored at�70°C until assayed. The concentra-tions of sVEGFR-1 were measured withan enzyme-linked immunosorbent assay(R&D Systems, Minneapolis, MN). Thedetails of the method have been de-scribed previously.18 The inter- and in-traassay coefficients of variation for hu-
g
s approved by the m
APRIL 2007 America
an sVEGFR-1 immunoassay in our
n Journal of Obstetrics & Gynecology 326.e2

lt1cmm
HAimppchbbmauagPctaaCasg9ItifwCcs2(
SToviplepctrl
rspcorpv
SCpeittpte
tpitgecipandsiptateapsCSPpe
RPTpts
(t(t(Epistf
DvoA1tvmLtapcpSj�pmp(
DvocRadptvesdtdopSjtT
Research Obstetrics www.AJOG.org
3
aboratory were 4.8% and 6.9%, respec-ively. The sensitivity of the assay was7.8 pg/mL. The maternal plasma con-entrations of sVEGFR-1 were deter-ined only among patients with abnor-al UADV.
uman PlGF assaysspecific and sensitive enzyme-linked
mmunosorbent assay was used to deter-ine concentrations of PlGF in maternal
lasma (R&D Systems). Briefly, humanlasma samples were incubated in dupli-ate wells of the microtiter plates, whichad been coated with monoclonal anti-odies to human PlGF. During this incu-ation, plasma PlGF (antigen) binds toonoclonal antibodies of PlGF to form
ntigen-antibody complexes. Afternbound substances were washedway, horseradish peroxidase– conju-ated polyclonal antibodies specific forlGF were added to each well of the mi-rotiter plate. After the second incuba-ion, the unbound antibody-enzyme re-gent was removed by repeated washing,nd a substrate solution was added.olor developed in proportion to themount of PlGF in each well. The inten-ity of the color was measured by a pro-rammable spectrophotometer (Ceres00 Micro plate Workstation; Bio-Teknstruments, Winooski, VT). Concen-rations of the samples were derived bynterpolation of the absorbance readingsrom a standard curve that was generatedith known concentrations of PlGF.alculated inter- and intraassay coeffi-
ients of variation for PlGF immunoas-ays in our laboratory were 4.60% and.27%, respectively. The detection limitsensitivity) of the assay was 10.7 pg/mL.
tudy outcomeshe primary outcome was the diagnosisf early onset preeclampsia and/or se-ere preeclampsia. Secondary outcomesncluded preeclampsia, SGA withoutreeclampsia, spontaneous preterm de-
ivery at �35 and �32 weeks of gestation,xamination-to-diagnosis interval amongatients who had preeclampsia, and aomposite of severe neonatal morbidityhat included intraventricular hemor-hage, necrotizing enterocolitis, and hya-
ine membrane disease with sonographic/ e26.e3 American Journal of Obstetrics & Gynecol
adiologic confirmation. Additionalecondary outcomes included abruptiolacentae and eclampsia. We have also in-luded nonobjective definitions of earlynset preeclampsia (such as “preeclampsiaequiring delivery at �34 weeks”19,20) torovide the basis for comparison with pre-ious reports.
tatistical analysisomparisons between proportions wereerformed with chi-square or Fisher’sxact test. Receiver operating character-stic curves were constructed to describehe relationship between sensitivity andhe false-positive rate (1-specificity) oflasma PlGF and sVEGFR-1 in the iden-ification of patients destined to developarly onset and/or severe preeclampsia.
Survival analysis was used to comparehe examination-to-diagnosis interval inatients who had preeclampsia, accord-
ng to the results of the UADV and ma-ernal plasma PlGF concentration. Lo-istic regression analysis was used toxplore the relationship between the oc-urrence of the outcomes and the follow-ng explanatory variables: maternallasma PlGF concentration, maternalge of �35 years, previous preeclampsia,ulliparity, first trimester body mass in-ex of �30 kg/m2, smoking status, andample storage time. A power analysisndicated that this study had adequateower (�90%) to determine the role ofhe combination of abnormal UADVnd maternal plasma PlGF concentra-ion in the prediction of the outcomes,xcept for spontaneous preterm deliveryt �32 weeks of gestation. The statisticalackages used were SPSS software (ver-ion 12.0; SPSS Inc, Chicago, IL), Med-alc software (version 7.4.4.1; MedCalcoftware, Mariakerke, Belgium), andASS software (NCSS, Kaysville, UT). Arobability value of �0.05 was consid-red significant.
ESULTSrevalence of the outcomeshis study included 3348 patients (52atients were lost to follow-up evalua-ion). The prevalence of preeclampsia,evere preeclampsia, and early onset pre-
clampsia was 3.4% (113/3296), 1.0% togy APRIL 2007
33/3296), and 0.8% (25/3208), respec-ively. UADV was performed in 95.4%3146/3296), and plasma PlGF concen-rations were determined in 93.5%3081/3296) of the study population.arly onset preeclampsia developed in 5atients, severe preeclampsia developed
n 13 patients, and both early onset andevere preeclampsia developed in 20 pa-ients (this group does not include theormer 18 patients).
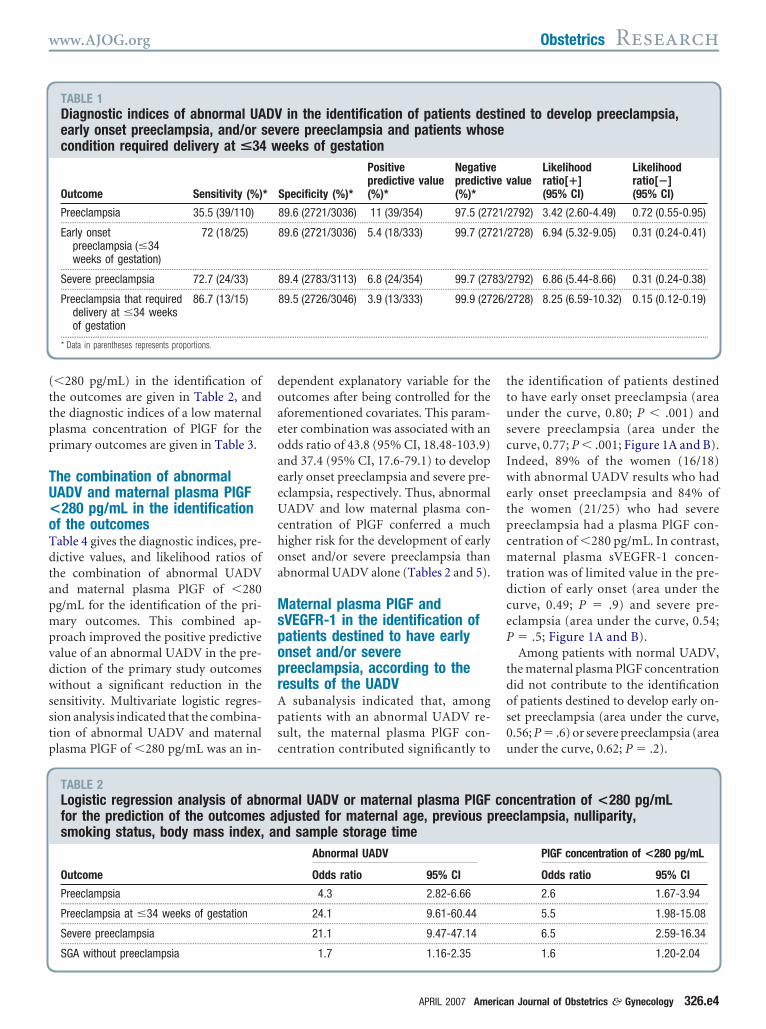
iagnostic indices, predictivealues, and likelihood ratiosf UADVn abnormal UADV was present in1.3% (354/3146) of the study popula-ion. The diagnostic indices, predictivealues, and likelihood ratios for the pri-ary outcomes are displayed in Table 1.
ogistic regression analysis indicatedhat an abnormal UADV, between 22nd 26 weeks of gestation, was an inde-endent explanatory variable for the oc-urrence of preeclampsia, early onsetreeclampsia, severe preeclampsia, andGA without preeclampsia, after an ad-ustment was made for maternal age of
35 years, previous preeclampsia, nulli-arity, smoking, first trimester bodyass index of �30 kg/m2, maternal
lasma PlGF, and sample storage timeTable 2).
iagnostic indices, predictivealues, and likelihood ratiosf maternal plasma PlGFoncentrationeceiver operating characteristic curvenalysis was performed to examine theiagnostic performance of maternallasma PlGF concentrations in the iden-ification of the patient destined to de-elop early onset and/or severe pre-clampsia; a cut-off of 280 pg/mL waselected. Logistic regression analysis in-icated that a maternal plasma concen-ration of PlGF �280 pg/mL was an in-ependent explanatory variable for theccurrence of preeclampsia, early onsetreeclampsia, severe preeclampsia, andGA without preeclampsia after an ad-ustment was made for the aforemen-ioned covariates and abnormal UADV.he odds ratio and 95% CI of a low ma-
ernal plasma PlGF concentration
(ttpp
TU<oTdtapmpvdwsstp
doaeoaeeUchoa
MspoprApsc
ttuscIwetpcmtdceP
tdos0u
www.AJOG.org Obstetrics Research
�280 pg/mL) in the identification ofhe outcomes are given in Table 2, andhe diagnostic indices of a low maternallasma concentration of PlGF for therimary outcomes are given in Table 3.
he combination of abnormalADV and maternal plasma PlGF280 pg/mL in the identification
f the outcomesable 4 gives the diagnostic indices, pre-ictive values, and likelihood ratios ofhe combination of abnormal UADVnd maternal plasma PlGF of �280g/mL for the identification of the pri-ary outcomes. This combined ap-
roach improved the positive predictivealue of an abnormal UADV in the pre-iction of the primary study outcomesithout a significant reduction in the
ensitivity. Multivariate logistic regres-ion analysis indicated that the combina-ion of abnormal UADV and maternallasma PlGF of �280 pg/mL was an in-
TABLE 1Diagnostic indices of abnormal UAearly onset preeclampsia, and/or scondition required delivery at <34
Outcome Sensitivity (%)
Preeclampsia 35.5 (39/110)...................................................................................................................
Early onsetpreeclampsia (�34weeks of gestation)
72 (18/25)
...................................................................................................................
Severe preeclampsia 72.7 (24/33)...................................................................................................................
Preeclampsia that requireddelivery at �34 weeksof gestation
86.7 (13/15)
...................................................................................................................
* Data in parentheses represents proportions.
TABLE 2Logistic regression analysis of abnfor the prediction of the outcomessmoking status, body mass index,
Outcome
Preeclampsia...................................................................................................................
Preeclampsia at �34 weeks of gestation...................................................................................................................
Severe preeclampsia...................................................................................................................
SGA without preeclampsia
ependent explanatory variable for theutcomes after being controlled for theforementioned covariates. This param-ter combination was associated with andds ratio of 43.8 (95% CI, 18.48-103.9)nd 37.4 (95% CI, 17.6-79.1) to developarly onset preeclampsia and severe pre-clampsia, respectively. Thus, abnormalADV and low maternal plasma con-
entration of PlGF conferred a muchigher risk for the development of earlynset and/or severe preeclampsia thanbnormal UADV alone (Tables 2 and 5).
aternal plasma PlGF andVEGFR-1 in the identification ofatients destined to have earlynset and/or severereeclampsia, according to theesults of the UADV
subanalysis indicated that, amongatients with an abnormal UADV re-ult, the maternal plasma PlGF con-entration contributed significantly to
in the identification of patients desere preeclampsia and patients whoeeks of gestation
Specificity (%)*
Positivepredictive value(%)*
Negativpredicti(%)*
89.6 (2721/3036) 11 (39/354) 97.5 (27.........................................................................................................................
89.6 (2721/3036) 5.4 (18/333) 99.7 (27
.........................................................................................................................
89.4 (2783/3113) 6.8 (24/354) 99.7 (27.........................................................................................................................
89.5 (2726/3046) 3.9 (13/333) 99.9 (27
.........................................................................................................................
mal UADV or maternal plasma PlGFjusted for maternal age, previous pd sample storage time
Abnormal UADV
Odds ratio 95% CI
4.3 2.82-6.66.........................................................................................................................
24.1 9.61-60.44.........................................................................................................................
21.1 9.47-47.14.........................................................................................................................
1.7 1.16-2.35
APRIL 2007 America
he identification of patients destinedo have early onset preeclampsia (areander the curve, 0.80; P � .001) andevere preeclampsia (area under theurve, 0.77; P � .001; Figure 1A and B).ndeed, 89% of the women (16/18)ith abnormal UADV results who had
arly onset preeclampsia and 84% ofhe women (21/25) who had severereeclampsia had a plasma PlGF con-entration of �280 pg/mL. In contrast,aternal plasma sVEGFR-1 concen-
ration was of limited value in the pre-iction of early onset (area under theurve, 0.49; P � .9) and severe pre-clampsia (area under the curve, 0.54; � .5; Figure 1A and B).Among patients with normal UADV,
he maternal plasma PlGF concentrationid not contribute to the identificationf patients destined to develop early on-et preeclampsia (area under the curve,.56; P � .6) or severe preeclampsia (areander the curve, 0.62; P � .2).
ed to develop preeclampsia,
alueLikelihoodratio[�](95% CI)
Likelihoodratio[�](95% CI)
2792) 3.42 (2.60-4.49) 0.72 (0.55-0.95)..................................................................................................................
2728) 6.94 (5.32-9.05) 0.31 (0.24-0.41)
..................................................................................................................
2792) 6.86 (5.44-8.66) 0.31 (0.24-0.38)..................................................................................................................
2728) 8.25 (6.59-10.32) 0.15 (0.12-0.19)
..................................................................................................................
ncentration of <280 pg/mLclampsia, nulliparity,
PlGF concentration of <280 pg/mL
Odds ratio 95% CI
2.6 1.67-3.94..................................................................................................................
5.5 1.98-15.08..................................................................................................................
6.5 2.59-16.34..................................................................................................................
1.6 1.20-2.04
DV tinev sew
*
eve v
21/......... .........
21/
......... .........
83/......... .........
26/
......... .........
or coad reean
......... .........
......... .........
......... .........
n Journal of Obstetrics & Gynecology 326.e4

DcpacTauit�ntsUPhsp
esnwwmPt
SacoepFts
oPtsatta(.tlt[
tspb
Research Obstetrics www.AJOG.org
3
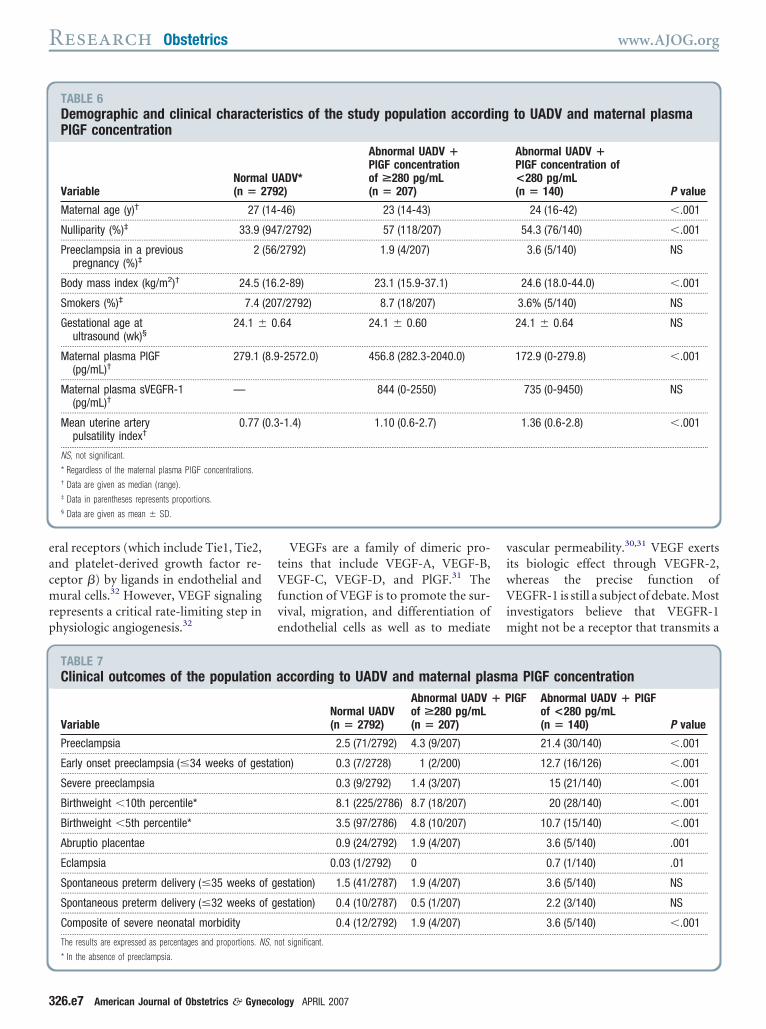
emographic and clinicalharacteristics of the studyopulation, according to UADVnd maternal plasma PlGFoncentrationables 6 and 7 display the demographicnd clinical characteristics of the pop-lation as well as the outcomes accord-
ng to the results of the UADV and ma-ernal plasma PlGF concentration of
280 pg/mL, respectively. There wereo differences in gestational ages at ul-
rasound examination among thetudy groups. Patients with abnormalADV results and maternal plasmalGF concentrations of �280 pg/mLad a higher frequency of preeclamp-ia, early onset preeclampsia, severereeclampsia, SGA without pre-
TABLE 3Diagnostic indices of a maternal Pto develop preeclampsia, early onsrequired delivery at <34 weeks of
OutcomeSensitivity(%)*
Preeclampsia 69.1 (76/110)...................................................................................................................
Early onsetpreeclampsia (�34weeks of gestation)
80 (20/25)
...................................................................................................................
Severe preeclampsia 81.8 (27/33)...................................................................................................................
Preeclampsia that requireddelivery at �34 weeksof gestation
86.7 (13/15)
...................................................................................................................
* Data in parentheses represents proportions.
TABLE 4Diagnostic indices of a combinatiopg/mL in the identification of patieand/or severe preeclampsia and p
OutcomeSensitivity(%)*
Preeclampsia 27.3 (30/110)...................................................................................................................
Early onsetpreeclampsia (�34weeks of gestation)
64 (16/25)
...................................................................................................................
Severe preeclampsia 63.6 (21/33)...................................................................................................................
Preeclampsia that requireddelivery at �34 weeksof gestation
73.3 (11/15)
...................................................................................................................
* Data in parentheses represents proportions.
26.e5 American Journal of Obstetrics & Gynecol
clampsia, placental abruption, eclamp-ia, and a composite of severe neo-atal morbidity than both patientsith normal UADV results and thoseith abnormal UADV results and aaternal plasma concentration of
lGF of �280 pg/mL (chi-square forrend; P � .001).
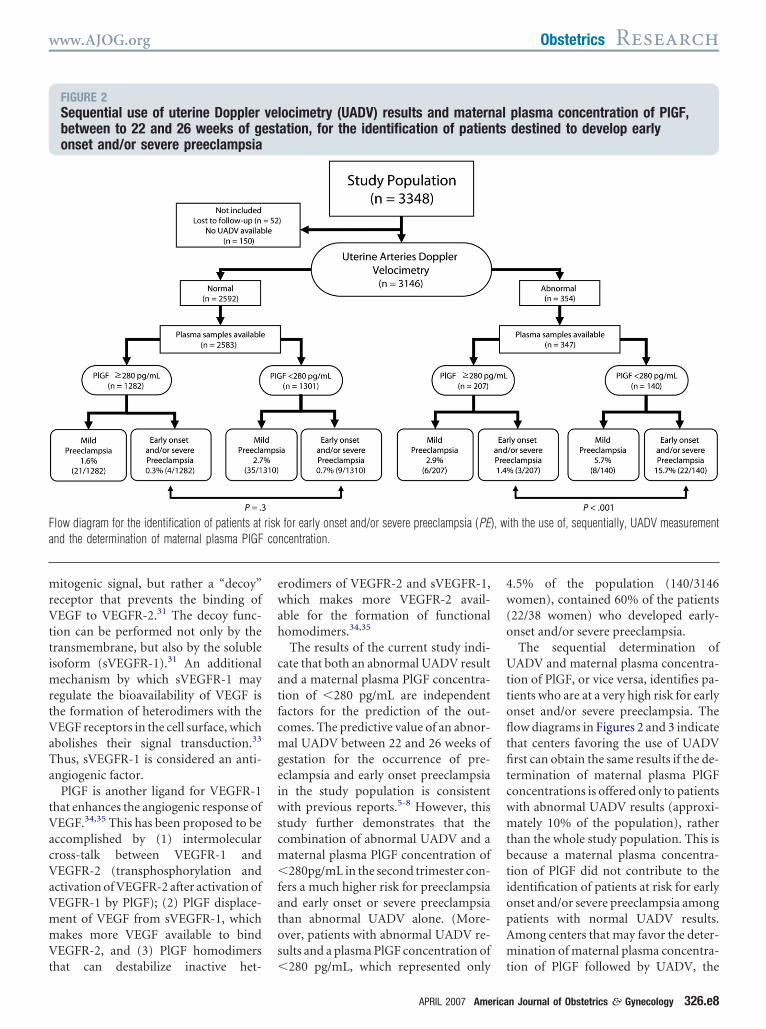
equential screening with UADVnd maternal plasma PlGFoncentration in the identificationf patients destined to developarly onset and/or severereeclampsiaigures 2 and 3 display the distribution ofhe study population according to the re-ults of sequential assessment with the use
F concentration of <280 pg/mL in tpreeclampsia, severe preeclampsia
estation
ecificity (%)*
Positivepredictive value(%)*
Negativepredictiv(%)*
.4 (1536/2988) 5 (76/1528) 97.8%(15.........................................................................................................................
.4 (1527/2971) 1.4 (20/1464) 99.7 (15
.........................................................................................................................
.0 (1555/3048) 1.8 (27/1520) 99.6 (15.........................................................................................................................
.3 (1530/2981) 0.9% (13/1464) 99.9 (15
.........................................................................................................................
of abnormal UADV and maternal plas destined to develop preeclampsiaents whose condition required deliv
cificity (%)*
Positivepredictive value(%)*
Negativepredictive(%)*
4 (2926/3036) 21.4 (30/140) 97.3 (2926/.........................................................................................................................
5 (3066/3176) 12.7 (16/126) 99.7 (3066/
.........................................................................................................................
3 (3136/3255) 15.0 (21/140) 99.6 (3136/.........................................................................................................................
4 (3071/3186) 8.7 (11/126) 99.9 (3071/
.........................................................................................................................
ogy APRIL 2007
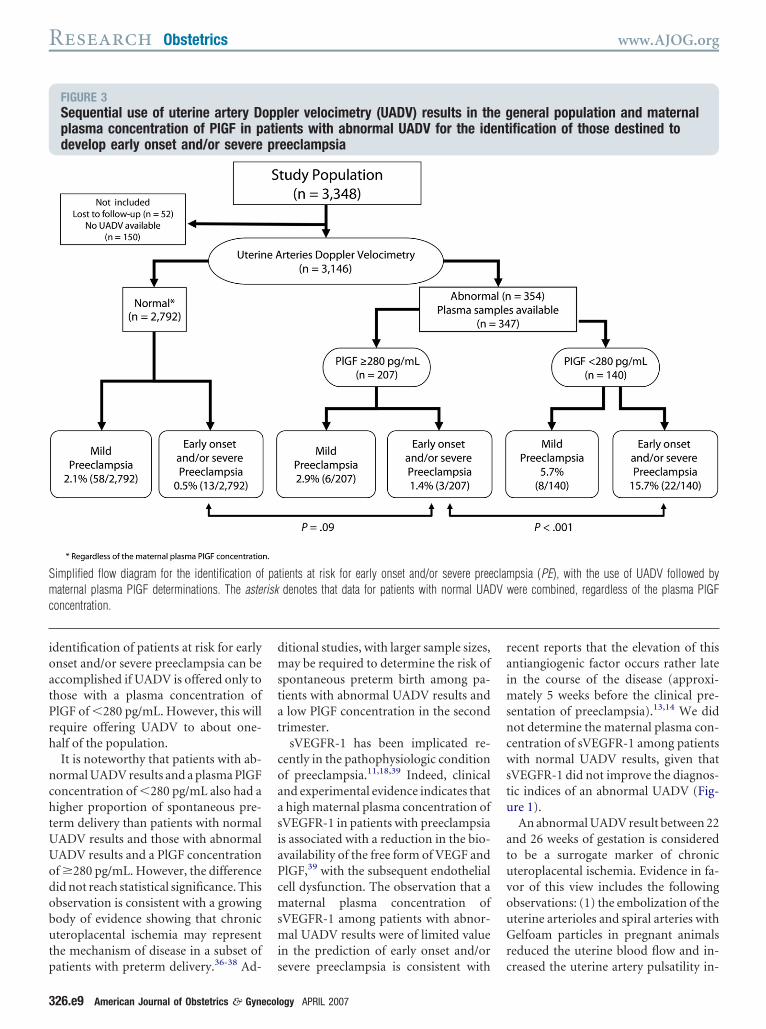
f UADV followed by maternal plasmalGF determinations in the second trimes-
er. The prevalence of early onset and/orevere preeclampsia among patients withbnormal UADV and PlGF concentra-ions of �280 pg/mL was 11 times higherhan among those with abnormal UADVnd PlGF concentrations of �280 pg/mL15.7% [22/140] vs 1.4% [3/207]; P �001) and 30 times higher than among pa-ients with normal UADV results, regard-ess of the maternal plasma PlGF concen-ration (15.7% [22/140] vs 0.5%13/2792]; P � .001; Figure 3).
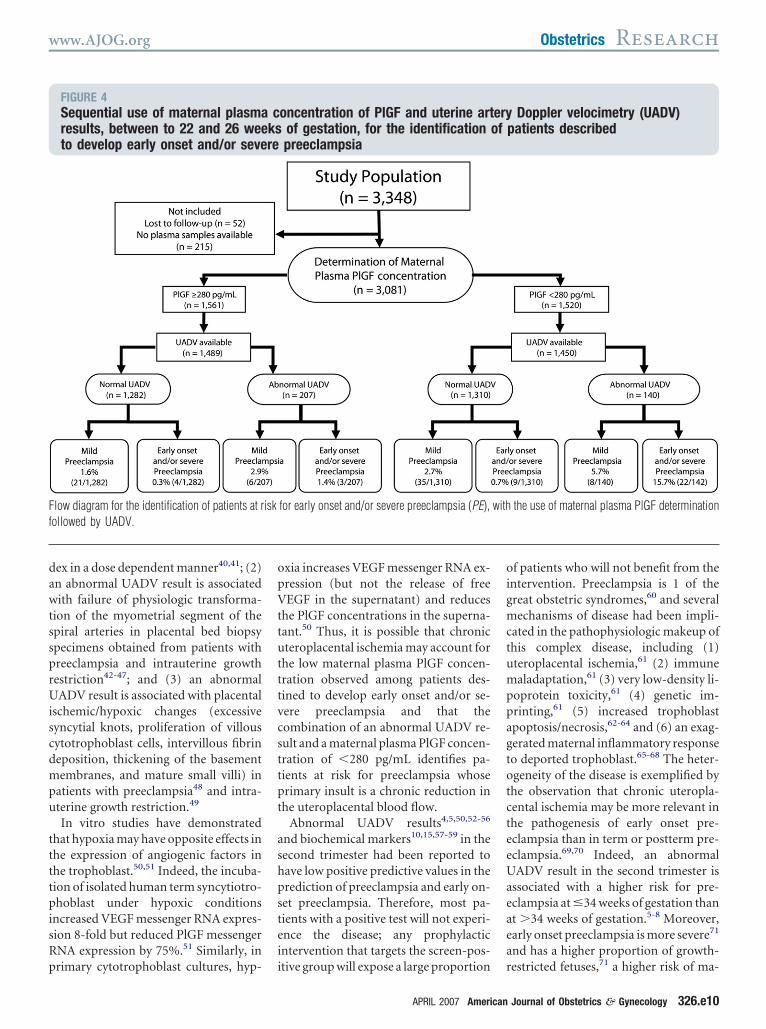
Figure 4 displays the distribution ofhe study population as a result of theequential determination of maternallasma concentration of PlGF followedy UADV. This flow diagram was gener-
identification of patients destinednd patients whose condition
alueLikelihoodratio[�](95% CI)
Likelihoodratio[�](95% CI)
/1570) 1.42 (1.25-1.62) 0.60 (0.53-0.68)..................................................................................................................
/1532) 1.65 (1.35-2.01) 0.39 (0.32-0.48)
..................................................................................................................
/1561) 1.67 (1.42-1.97) 0.36 (0.30-0.42)..................................................................................................................
/1532) 1.78 (1.46-2.18) 0.26 (0.21-0.32)
..................................................................................................................
a PlGF concentration of <280rly onset preeclampsia,at <34 weeks of gestation
eLikelihoodratio[�](95% CI)
Likelihoodratio[�](95% CI)
6) 7.53 (5.27-10.75) 0.75 (0.53-1.08)..................................................................................................................
5) 18.48 (13.07-26.13) 0.37 (0.26-0.53)
..................................................................................................................
8) 17.41 (12.74-23.79) 0.38 (0.28-0.52)..................................................................................................................
5) 20.32 (14.26-28.95) 0.28 (0.19-0.40)
..................................................................................................................
lG heet , ag
Spe v
51 36......... .........
51 27
......... .........
51 55......... .........
51 30
......... .........
n smnt , ea
ati ery
Spevalu
96. 300......... .........
96. 307
......... .........
96. 314......... .........
96. 307
......... .........

aS
pPdo.
CTca
tapea
tttmUov
ltcp
fimssfdrm2iHeotatau
agndcptemnmpbncoath
gVOpcfncmc
Md.pp
www.AJOG.org Obstetrics Research
ted because many centers in the Unitedtates do not use UADV.The survival analysis indicated that
atients with abnormal UADV and lowlGF have a shorter examination-to-iagnosis interval than those in thether 2 groups (log rank test, 37.9; P �
001; Figure 5).
OMMENThe results of this study indicate that aombination of an abnormal UADVnd a maternal plasma PlGF concen-
FIGURE 1Receiver operating characteristic cconcentration of PlGF and sVEGFRpatients destined to develop early
aternal plasma PlGF concentration (solid line) cestined to develop A, early onset preeclampsia
001). In contrast, maternal plasma sVEGFR-1 crediction of A, early onset preeclampsia (area ureeclampsia (area under the curve, 0.54; P �
TABLE 5Logistic regression analysis of a cmaternal plasma PlGF concentratioof the outcomes that are adjustedpreeclampsia, nulliparity, smokingand sample storage time
Outcome
Preeclampsia...................................................................................................................
Preeclampsia at �34 weeks of gestation...................................................................................................................
Severe preeclampsia...................................................................................................................
SGA without preeclampsia
ration of �280 pg/mL, between 22nd 26 weeks of gestation, identifiesatients at a very high risk for pre-clampsia, early onset preeclampsia,nd severe preeclampsia.These novel observations are consis-
ent with previous reports indicatinghat a low maternal plasma concentra-ion of PlGF in the first9,12 or second tri-
ester of pregnancy9-11,21 and abnormalADV results between 23 and 25 weeksf gestation5-8 are risk factors for the de-elopment of preeclampsia. Similarly, a
ves of the maternal plasmafor the identification ofset or severe preeclampsia
tributed significantly to the prediction of patients; P � .001) and B, severe preeclampsia (P �
entration (dotted line) was of limited use in ther the curve [AUC], 0.49; P � .9) and B, severe.
bination of abnormal UADV andof <280 pg/mL for the predictionr maternal age, previousatus, body mass index,
Abnormal UADV � PlGFconcentration of <280 pg/mL
Odds ratio 95% CI
8.6 5.35-13.74..................................................................................................................
43.8 18.48-103.89..................................................................................................................
37.4 17.64-79.07..................................................................................................................
2.7 1.73-4.26
r
APRIL 2007 America
ow urine concentration of PlGF be-ween 25 and 28 weeks has been asso-iated recently with a high risk forreeclampsia.13
The results presented herein differrom those reported recently,22 indicat-ng a lack of association between abnor-
al UADV and low PlGF. Differences inample size, gestational age at ultra-ound, and study outcomes may accountor these discrepancies. A recent longitu-inal study that included 81 patients atisk for preeclampsia reported that theaternal plasma PlGF concentration at
4 weeks of gestation contributed signif-cantly to the prediction of the disease.23
owever, this study did not includenough patients to determine the valuef maternal plasma PlGF for the predic-ion of early onset preeclampsia, and theuthors cautioned that “large prospec-ive cohort studies in unselected womenre required to ascertain any clinicalsefulness.”23
The regulation of vascular growthnd remodeling, also known as angio-enesis, is considered to be central toormal placental and fetal growth andevelopment.24-26 In the human pla-enta, angiogenesis is biphasic, witheaks at mid gestation and at term ashe result of endothelial proliferationarly in pregnancy and vascular re-odeling in the second half of preg-
ancy.27 This is consistent with theodel of placental angiogenesis pro-
osed by Kingdom et al, 28 wherebyranching angiogenesis is predomi-ant in the first trimester and is asso-iated with high placental productionf VEGF. In contrast, nonbranchingngiogenesis is predominant in thehird trimester and is associated with aigh placental production of PlGF.28
Angiogenesis is regulated by at least 3rowth factor families, which includeEGFs, angiopoietins, and ephrins.29
ther nonspecific factors that have beenroposed to regulate angiogenesis in-lude fibroblast growth factors, trans-orming growth factors � and �, tumorecrosis factor �, interleukin-8, hepato-yte growth factor, angiogenin, andembers of the Notch family.26,30,31 Re-
ent evidence indicates that angiogenesis
ur-1on
on(PE
oncnde.5)
omnfost
.........
.........
.........
equires the sequential activation of sev-
n Journal of Obstetrics & Gynecology 326.e6
eacmrp
tVfve
viwVim
Research Obstetrics www.AJOG.org
3
ral receptors (which include Tie1, Tie2,nd platelet-derived growth factor re-eptor �) by ligands in endothelial andural cells.32 However, VEGF signaling
epresents a critical rate-limiting step inhysiologic angiogenesis.32
TABLE 6Demographic and clinical charactePlGF concentration
VariableNorma(n � 2
Maternal age (y)† 27...................................................................................................................
Nulliparity (%)‡ 33.9...................................................................................................................
Preeclampsia in a previouspregnancy (%)‡
2
...................................................................................................................
Body mass index (kg/m2)† 24.5...................................................................................................................
Smokers (%)‡ 7.4...................................................................................................................
Gestational age atultrasound (wk)§
24.1 �
...................................................................................................................
Maternal plasma PlGF(pg/mL)†
279.1
...................................................................................................................
Maternal plasma sVEGFR-1(pg/mL)†
—
...................................................................................................................
Mean uterine arterypulsatility index†
0.77
...................................................................................................................
NS, not significant.
* Regardless of the maternal plasma PlGF concentrations.† Data are given as median (range).‡ Data in parentheses represents proportions.§ Data are given as mean � SD.
TABLE 7Clinical outcomes of the populatio
Variable
Preeclampsia...................................................................................................................
Early onset preeclampsia (�34 weeks of ges...................................................................................................................
Severe preeclampsia...................................................................................................................
Birthweight �10th percentile*...................................................................................................................
Birthweight �5th percentile*...................................................................................................................
Abruptio placentae...................................................................................................................
Eclampsia...................................................................................................................
Spontaneous preterm delivery (�35 weeks o...................................................................................................................
Spontaneous preterm delivery (�32 weeks o...................................................................................................................
Composite of severe neonatal morbidity...................................................................................................................
The results are expressed as percentages and proportions. N
* In the absence of preeclampsia.
26.e7 American Journal of Obstetrics & Gynecol
VEGFs are a family of dimeric pro-eins that include VEGF-A, VEGF-B,EGF-C, VEGF-D, and PlGF.31 The
unction of VEGF is to promote the sur-ival, migration, and differentiation ofndothelial cells as well as to mediate
tics of the study population accord
ADV*2)
Abnormal UADV �PlGF concentrationof >280 pg/mL(n � 207)
46) 23 (14-43).........................................................................................................................
/2792) 57 (118/207).........................................................................................................................
2792) 1.9 (4/207)
.........................................................................................................................
2-89) 23.1 (15.9-37.1).........................................................................................................................
/2792) 8.7 (18/207).........................................................................................................................
64 24.1 � 0.60
.........................................................................................................................
-2572.0) 456.8 (282.3-2040.0)
.........................................................................................................................
844 (0-2550)
.........................................................................................................................
-1.4) 1.10 (0.6-2.7)
.........................................................................................................................
ccording to UADV and maternal pla
Normal UADV(n � 2792)
Abnormal UADVof >280 pg/mL(n � 207)
2.5 (71/2792) 4.3 (9/207).........................................................................................................................
on) 0.3 (7/2728) 1 (2/200).........................................................................................................................
0.3 (9/2792) 1.4 (3/207).........................................................................................................................
8.1 (225/2786) 8.7 (18/207).........................................................................................................................
3.5 (97/2786) 4.8 (10/207).........................................................................................................................
0.9 (24/2792) 1.9 (4/207).........................................................................................................................
0.03 (1/2792) 0.........................................................................................................................
station) 1.5 (41/2787) 1.9 (4/207).........................................................................................................................
station) 0.4 (10/2787) 0.5 (1/207).........................................................................................................................
0.4 (12/2792) 1.9 (4/207).........................................................................................................................
ot significant.
ogy APRIL 2007
ascular permeability.30,31 VEGF exertsts biologic effect through VEGFR-2,hereas the precise function ofEGFR-1 is still a subject of debate. Most
nvestigators believe that VEGFR-1ight not be a receptor that transmits a
to UADV and maternal plasma
Abnormal UADV �PlGF concentration of<280 pg/mL(n � 140) P value
24 (16-42) �.001..................................................................................................................
54.3 (76/140) �.001..................................................................................................................
3.6 (5/140) NS
..................................................................................................................
24.6 (18.0-44.0) �.001..................................................................................................................
3.6% (5/140) NS..................................................................................................................
24.1 � 0.64 NS
..................................................................................................................
172.9 (0-279.8) �.001
..................................................................................................................
735 (0-9450) NS
..................................................................................................................
1.36 (0.6-2.8) �.001
..................................................................................................................
a PlGF concentrationlGF Abnormal UADV � PlGF
of <280 pg/mL(n � 140) P value
21.4 (30/140) �.001..................................................................................................................
12.7 (16/126) �.001..................................................................................................................
15 (21/140) �.001..................................................................................................................
20 (28/140) �.001..................................................................................................................
10.7 (15/140) �.001..................................................................................................................
3.6 (5/140) .001..................................................................................................................
0.7 (1/140) .01..................................................................................................................
3.6 (5/140) NS..................................................................................................................
2.2 (3/140) NS..................................................................................................................
3.6 (5/140) �.001..................................................................................................................
ris ing
l U79
(14-......... .........
(947......... .........
(56/
......... .........
(16.......... .........
(207......... .........
0.
......... .........
(8.9
......... .........
......... .........
(0.3
......... .........
n a sm� P
......... .........
tati......... .........
......... .........
......... .........
......... .........
......... .........
......... .........
f ge......... .........
f ge......... .........
......... .........
S, n
mrVttimrtVaTa
tVacVaVmmVt
ewah
catfcmgeiwscm�fatos
4w(o
UttofltfitcwmtbtiopAm
Fa
www.AJOG.org Obstetrics Research
itogenic signal, but rather a “decoy”eceptor that prevents the binding ofEGF to VEGFR-2.31 The decoy func-
ion can be performed not only by theransmembrane, but also by the solublesoform (sVEGFR-1).31 An additional
echanism by which sVEGFR-1 mayegulate the bioavailability of VEGF ishe formation of heterodimers with theEGF receptors in the cell surface, which
bolishes their signal transduction.33
hus, sVEGFR-1 is considered an anti-ngiogenic factor.
PlGF is another ligand for VEGFR-1hat enhances the angiogenic response ofEGF.34,35 This has been proposed to be
ccomplished by (1) intermolecularross-talk between VEGFR-1 andEGFR-2 (transphosphorylation and
ctivation of VEGFR-2 after activation ofEGFR-1 by PlGF); (2) PlGF displace-ent of VEGF from sVEGFR-1, whichakes more VEGF available to bindEGFR-2, and (3) PlGF homodimers
FIGURE 2Sequential use of uterine Dopplerbetween to 22 and 26 weeks of geonset and/or severe preeclampsia
low diagram for the identification of patients atnd the determination of maternal plasma PlGF
hat can destabilize inactive het- �
rodimers of VEGFR-2 and sVEGFR-1,hich makes more VEGFR-2 avail-
ble for the formation of functionalomodimers.34,35
The results of the current study indi-ate that both an abnormal UADV resultnd a maternal plasma PlGF concentra-ion of �280 pg/mL are independentactors for the prediction of the out-omes. The predictive value of an abnor-al UADV between 22 and 26 weeks of
estation for the occurrence of pre-clampsia and early onset preeclampsian the study population is consistentith previous reports.5-8 However, this
tudy further demonstrates that theombination of abnormal UADV and aaternal plasma PlGF concentration of280pg/mL in the second trimester con-
ers a much higher risk for preeclampsiand early onset or severe preeclampsiahan abnormal UADV alone. (More-ver, patients with abnormal UADV re-ults and a plasma PlGF concentration of
ocimetry (UADV) results and maternation, for the identification of patien
for early onset and/or severe preeclampsia (PE)ncentration.
280 pg/mL, which represented only t
APRIL 2007 America
.5% of the population (140/3146omen), contained 60% of the patients
22/38 women) who developed early-nset and/or severe preeclampsia.The sequential determination ofADV and maternal plasma concentra-
ion of PlGF, or vice versa, identifies pa-ients who are at a very high risk for earlynset and/or severe preeclampsia. Theow diagrams in Figures 2 and 3 indicate
hat centers favoring the use of UADVrst can obtain the same results if the de-
ermination of maternal plasma PlGFoncentrations is offered only to patientsith abnormal UADV results (approxi-ately 10% of the population), rather
han the whole study population. This isecause a maternal plasma concentra-ion of PlGF did not contribute to thedentification of patients at risk for earlynset and/or severe preeclampsia amongatients with normal UADV results.mong centers that may favor the deter-ination of maternal plasma concentra-
plasma concentration of PlGF,destined to develop early
ith the use of, sequentially, UADV measurement
vel alst ts
risk , wco
ion of PlGF followed by UADV, the
n Journal of Obstetrics & Gynecology 326.e8
ioatPrh
nchtUUodobutp
dmstat
coaasiaPcmsmi
raimsncwstu
atuvouGr
Smc
Research Obstetrics www.AJOG.org
3
dentification of patients at risk for earlynset and/or severe preeclampsia can beccomplished if UADV is offered only tohose with a plasma concentration oflGF of �280 pg/mL. However, this willequire offering UADV to about one-alf of the population.It is noteworthy that patients with ab-
ormal UADV results and a plasma PlGFoncentration of �280 pg/mL also had aigher proportion of spontaneous pre-erm delivery than patients with normalADV results and those with abnormalADV results and a PlGF concentrationf �280 pg/mL. However, the differenceid not reach statistical significance. Thisbservation is consistent with a growingody of evidence showing that chronicteroplacental ischemia may represent
he mechanism of disease in a subset of
FIGURE 3Sequential use of uterine artery Dplasma concentration of PlGF in pdevelop early onset and/or severe
implified flow diagram for the identification ofaternal plasma PlGF determinations. The aste
oncentration.
atients with preterm delivery.36-38 Ad- s
26.e9 American Journal of Obstetrics & Gynecol
itional studies, with larger sample sizes,ay be required to determine the risk of
pontaneous preterm birth among pa-ients with abnormal UADV results andlow PlGF concentration in the second
rimester.sVEGFR-1 has been implicated re-
ently in the pathophysiologic conditionf preeclampsia.11,18,39 Indeed, clinicalnd experimental evidence indicates thathigh maternal plasma concentration of
VEGFR-1 in patients with preeclampsias associated with a reduction in the bio-vailability of the free form of VEGF andlGF,39 with the subsequent endothelialell dysfunction. The observation that aaternal plasma concentration of
VEGFR-1 among patients with abnor-al UADV results were of limited value
n the prediction of early onset and/or
ler velocimetry (UADV) results in thents with abnormal UADV for the ideeeclampsia
tients at risk for early onset and/or severe preedenotes that data for patients with normal UAD
evere preeclampsia is consistent with c
ogy APRIL 2007
ecent reports that the elevation of thisntiangiogenic factor occurs rather laten the course of the disease (approxi-
ately 5 weeks before the clinical pre-entation of preeclampsia).13,14 We didot determine the maternal plasma con-entration of sVEGFR-1 among patientsith normal UADV results, given that
VEGFR-1 did not improve the diagnos-ic indices of an abnormal UADV (Fig-re 1).An abnormal UADV result between 22
nd 26 weeks of gestation is consideredo be a surrogate marker of chronicteroplacental ischemia. Evidence in fa-or of this view includes the followingbservations: (1) the embolization of theterine arterioles and spiral arteries withelfoam particles in pregnant animals
educed the uterine blood flow and in-
eneral population and maternalification of those destined to
psia (PE), with the use of UADV followed bywere combined, regardless of the plasma PlGF
opp e gati ntpr
pa clamrisk V
reased the uterine artery pulsatility in-
dawtssprUiscdmpu
ttttpisRp
opVttutttvcsttpt
ashpstei
oigmctumppagtotcteeUaeaea
Ff
www.AJOG.org Obstetrics Research
ex in a dose dependent manner40,41; (2)n abnormal UADV result is associatedith failure of physiologic transforma-
ion of the myometrial segment of thepiral arteries in placental bed biopsypecimens obtained from patients withreeclampsia and intrauterine growthestriction42-47; and (3) an abnormalADV result is associated with placental
schemic/hypoxic changes (excessiveyncytial knots, proliferation of villousytotrophoblast cells, intervillous fibrineposition, thickening of the basementembranes, and mature small villi) in
atients with preeclampsia48 and intra-terine growth restriction.49
In vitro studies have demonstratedhat hypoxia may have opposite effects inhe expression of angiogenic factors inhe trophoblast.50,51 Indeed, the incuba-ion of isolated human term syncytiotro-hoblast under hypoxic conditions
ncreased VEGF messenger RNA expres-ion 8-fold but reduced PlGF messengerNA expression by 75%.51 Similarly, in
FIGURE 4Sequential use of maternal plasmaresults, between to 22 and 26 weeto develop early onset and/or seve
low diagram for the identification of patients at rollowed by UADV.
rimary cytotrophoblast cultures, hyp- i
xia increases VEGF messenger RNA ex-ression (but not the release of freeEGF in the supernatant) and reduces
he PlGF concentrations in the superna-ant.50 Thus, it is possible that chronicteroplacental ischemia may account for
he low maternal plasma PlGF concen-ration observed among patients des-ined to develop early onset and/or se-ere preeclampsia and that theombination of an abnormal UADV re-ult and a maternal plasma PlGF concen-ration of �280 pg/mL identifies pa-ients at risk for preeclampsia whoserimary insult is a chronic reduction inhe uteroplacental blood flow.
Abnormal UADV results4,5,50,52-56
nd biochemical markers10,15,57-59 in theecond trimester had been reported toave low positive predictive values in therediction of preeclampsia and early on-et preeclampsia. Therefore, most pa-ients with a positive test will not experi-nce the disease; any prophylacticntervention that targets the screen-pos-
oncentration of PlGF and uterine artof gestation, for the identificationpreeclampsia
for early onset and/or severe preeclampsia (PE),
tive group will expose a large proportion r
APRIL 2007 American
f patients who will not benefit from thentervention. Preeclampsia is 1 of thereat obstetric syndromes,60 and severalechanisms of disease had been impli-
ated in the pathophysiologic makeup ofhis complex disease, including (1)teroplacental ischemia,61 (2) immunealadaptation,61 (3) very low-density li-
oprotein toxicity,61 (4) genetic im-rinting,61 (5) increased trophoblastpoptosis/necrosis,62-64 and (6) an exag-erated maternal inflammatory responseo deported trophoblast.65-68 The heter-geneity of the disease is exemplified byhe observation that chronic uteropla-ental ischemia may be more relevant inhe pathogenesis of early onset pre-clampsia than in term or postterm pre-clampsia.69,70 Indeed, an abnormalADV result in the second trimester is
ssociated with a higher risk for pre-clampsia at �34 weeks of gestation thant �34 weeks of gestation.5-8 Moreover,arly onset preeclampsia is more severe71
nd has a higher proportion of growth-
Doppler velocimetry (UADV)patients described
the use of maternal plasma PlGF determination
c eryks ofre
isk with
estricted fetuses,71 a higher risk of ma-
Journal of Obstetrics & Gynecology 326.e10

tpl
pmitopcadbpsfnoasaao
hat�oreMcioarsllbowpt
cmetttbmv
brpatetmVpiitpthhgd
isatwtasrmUstatUtbp
CawUsp9
Research Obstetrics www.AJOG.org
3
ernal death,1 and a higher frequency oflacental pathologic condition72,73 than
ate onset preeclampsia.Because of the syndromic nature of
reeclampsia,74 it is unlikely that a singlearker or combination of markers will
dentify all patients destined to develophis pregnancy complication, regardlessf their mechanism of disease. We haverovided the diagnostic indices of aombination of abnormal UADV resultnd low PlGF concentration for the pre-iction of the outcomes to provide theasis for comparison with previous re-orts. However, we propose that risk as-essment of preeclampsia should notocus on the prediction of this heteroge-eous disorder, but on the identificationf patients at high risk for the earlynd/or a more severe form of preeclamp-ia, in whom prophylactic interventionsre more likely to reduce the morbiditynd mortality rates associated with thisbstetric syndrome.Collectively, the results presented
erein indicate that a combination ofn abnormal UADV result and a ma-ernal plasma concentration of PlGF of
280 pg/mL between 22 and 26 weeksf gestation is associated with a highisk for preeclampsia, early onset pre-clampsia, and severe preeclampsia.
oreover, a maternal plasma PlGFoncentration of �280 pg/mL candentify most patients at risk for earlynset and/or severe preeclampsiamong patients with abnormal UADVesults. The identification of this sub-et of patients may allow for prophy-actic interventions, such as the modu-ation of the antiangiogenic stateefore the clinical presentation of earlynset and/or severe preeclampsia,hich potentially could reduce theerinatal and maternal mortality ratehat is associated with this syndrome.
The results of 2 recent randomizedlinical trials of vitamin C and E supple-entation for the prevention of pre-
clampsia in low-75 and high-risk76 pa-ients yielded negative results. Thus,here is a need for alternative prophylac-ic interventions. VEGF and PlGF haveeen proposed as potential candidates toodulate the antiangiogenic state in se-
ere preeclampsia.77 Recently, it has a
26.e11 American Journal of Obstetrics & Gyneco
een reported that the administration ofecombinant VEGF121 to a rat model ofreeclampsia, which was induced by thedministration of adenovirus expressinghe sVEGFR-1 gene, attenuated the pre-clamptic phenotype. Indeed, the au-hors reported that the subcutaneous ad-
inistration of 100, 200, or 400 �g/kg ofEGF121 reduced the systolic bloodressure, limited the kidney damage (as
ndicated by a lower glomerular lesionndex), and reduced proteinuria amonghe treated animals.78 The authors pro-osed that VEGF121 could be a potentialherapeutic agent for preeclampsia inumans.78 Similarly, VEGF and PlGFad been reported to stimulate angio-enesis in an animal model of myocar-ial and limb ischemia.79 However, PlGF
FIGURE 5Cumulative hazard ratio for the cliaccording to the results of uterineand maternal plasma concentratio
umulative hazard ratios for the clinical presentnd maternal plasma PlGF concentrations amoere included in this analysis). The examinatioADV and plasma PlGF of �280 pg/mL (medignificantly shorter than in patients with abnormg/mL (median, 94 days; interquartile range, 84-9 days; interquartile range, 91-107 days) who
ppears to be a better candidate for clin- o
logy APRIL 2007
cal trials, because it did not induce theide effects associated with VEGF (suchs edema, hypotension, bleeding, andhe formation of fragile capillaries thatere prone to regression).79 If clinical
rials prove that proangiogenic factorsre effective in delaying the clinical pre-entation of preeclampsia and/oreducing its severity, we have esti-ated that 15 patients with abnormalADV results (95% CI, 11-26) in the
econd trimester would need to bereated to prevent 1 case of early onsetnd/or severe preeclampsia. In con-rast, only 7 patients with abnormalADV results and low PlGF concen-
rations (95% CI, 5-11) would need toe exposed to these interventions torevent 1 case of severe and/or early
al presentation of preeclampsiatery Doppler velocimetry (UADV)f PlGF
n of preeclampsia (PE) according to the UADVstudy groups (only patients with preeclampsiao-diagnosis interval in patients with abnormal69 days; interquartile range, 58-88 days) was
UADV and plasma PlGF concentration of �280days) and patients with normal UADV (median,preeclampsia (log rank, 37.9; P � .001)
nicar
n o
ationgn-t
ian,al
106had
nset preeclampsia. f

R1ne2u33MRH4psaG5Catrb16Pfag7Stt28Gevg29Dge11s(wpn1ce1Scnre91ps1af
tM1iomf11[c21lni11etts1Ccs322efE12gpp2JflP2lwG2Spgt22a2Jgt2doc72mt
2are13c23o23tR3bmp23Pltcfl23acF3Fri23aspG3Mtpb53c(te4ctde4clup14Rfln
www.AJOG.org Obstetrics Research
EFERENCES. MacKay AP, Berg CJ, Atrash HK. Preg-ancy-related mortality from preeclampsia andclampsia. Obstet Gynecol 2001;97:533-8.. Redman CW, Sargent IL. Latest advances innderstanding preeclampsia. Science 2005;08:1592-4.. Roberts JM, Pearson G, Cutler J, Lindheimer. Summary of the NHLBI Working Group onesearch on Hypertension During Pregnancy.ypertension 2003;41:437-45.. Bower S, Bewley S, Campbell S. Improvedrediction of preeclampsia by two-stagecreening of uterine arteries using the early di-stolic notch and color Doppler imaging. Obstetynecol 1993;82:78-83.. Harrington K, Cooper D, Lees C, Hecher K,ampbell S. Doppler ultrasound of the uterinerteries: the importance of bilateral notching inhe prediction of pre-eclampsia, placental ab-uption or delivery of a small-for-gestational-ageaby. Ultrasound Obstet Gynecol 1996;7:82-8.. Albaiges G, Missfelder-Lobos H, Lees C,arra M, Nicolaides KH. One-stage screening
or pregnancy complications by color Dopplerssessment of the uterine arteries at 23 weeks’estation. Obstet Gynecol 2000;96:559-64.. Papageorghiou AT, Yu CK, Cicero S, Bower, Nicolaides KH. Second-trimester uterine ar-
ery Doppler screening in unselected popula-ions: a review. J Matern Fetal Neonatal Med002;12:78-88.. Papageorghiou AT, Yu CK, Bindra R, Pandis, Nicolaides KH. Multicenter screening for pre-clampsia and fetal growth restriction by trans-aginal uterine artery Doppler at 23 weeks ofestation. Ultrasound Obstet Gynecol001;18:441-9.. Tidwell SC, Ho HN, Chiu WH, Torry RJ, TorryS. Low maternal serum levels of placentarowth factor as an antecedent of clinical pre-clampsia. Am J Obstet Gynecol 2001;84:1267-72.0. Krauss T, Pauer HU, Augustin HG. Pro-pective analysis of placenta growth factorPlGF) concentrations in the plasma of womenith normal pregnancy and pregnancies com-licated by preeclampsia. Hypertens Preg-ancy 2004;23:101-11.1. Levine RJ, Maynard SE, Qian C, et al. Cir-ulating angiogenic factors and the risk of pre-clampsia. N Engl J Med 2004;350:672-83.2. Stepan H, Faber R, Wessel N, Wallukat G,chultheiss HP, Walther T. Relation betweenirculating angiotensin II type 1 receptor ago-istic autoantibodies and soluble fms-like ty-osine kinase 1 in the pathogenesis of pre-clampsia. J Clin Endocrinol Metab 2006;1:2424-7.3. Levine RJ, Thadhani R, Qian C, et al. Urinarylacental growth factor and risk of preeclamp-ia. JAMA 2005;293:77-85.4. Chaiworapongsa T, Romero R, Kim YM, etl. Plasma soluble vascular endothelial growth
actor receptor-1 concentration is elevated prior Jo the clinical diagnosis of pre-eclampsia. Jatern Fetal Neonatal Med 2005;17:3-18.5. Parra M, Rodrigo R, Barja P, et al. Screen-
ng test for preeclampsia through assessmentf uteroplacental blood flow and biochemicalarkers of oxidative stress and endothelial dys-
unction. Am J Obstet Gynecol 2005;193:486-91.6. Gonzalez RP, Gomez RM, Castro RS, et al.
A national birth weight distribution curve ac-ording to gestational age in Chile from 1993 to000]. Rev Med Chil 2004;132:1155-65.7. Bower S, Schuchter K, Campbell S. Dopp-
er ultrasound screening as part of routine ante-atal scanning: prediction of pre-eclampsia and
ntrauterine growth retardation. BJOG 1993;00:989-94.8. Chaiworapongsa T, Romero R, Espinoza J,t al. Evidence supporting a role for blockade ofhe vascular endothelial growth factor system inhe pathophysiology of preeclampsia. Am J Ob-tet Gynecol 2004;190:1541-7.9. Haddad B, Deis S, Goffinet F, Paniel BJ,abrol D, Siba BM. Maternal and perinatal out-omes during expectant management of 239evere preeclamptic women between 24 and3 weeks’ gestation. Am J Obstet Gynecol004;190:1590-5.0. Hall DR, Grove D, Carstens E. Early pre-clampsia: What proportion of women qualifyor expectant management and if not, why not?ur J Obstet Gynecol Reprod Biol 2006;28:169-74.1. Tjoa ML, van Vugt JM, Mulders MA, Schut-ens RB, Oudejans CB, van Wijk IJ. Plasmalacenta growth factor levels in mid trimesterregnancies. Obstet Gynecol 2001;98:600-7.2. Muller PR, James AH, Murtha PP, Yonish B,amison MG, Dekker G. Circulating angiogenicactors and abnormal uterine artery Doppler ve-ocimetry in the second trimester. Hypertensregnancy 2006;25:183-92.3. Chappell LC, Seed PT, Briley A, et al. A
ongitudinal study of biochemical variables inomen at risk of preeclampsia. Am J Obstetynecol 2002;187:127-36.4. Wulff C, Wilson H, Dickson SE, WiegandJ, Fraser HM. Hemochorial placentation in therimate: expression of vascular endothelialrowth factor, angiopoietins, and their recep-ors throughout pregnancy. Biol Reprod002;66:802-12.5. Carmeliet P. Mechanisms of angiogenesisnd arteriogenesis. Nat Med 2000;6:389-95.6. Yancopoulos GD, Davis S, Gale NW, RudgeS, Wiegand SJ, Holash J. Vascular-specificrowth factors and blood vessel formation. Na-ure 2000;407:242-8.7. Mayhew TM. Fetoplacental angiogenesisuring gestation is biphasic, longitudinal andccurs by proliferation and remodeling of vas-ular endothelial cells. Placenta 2002;23:42-50.8. Kingdom J, Huppertz B, Seaward G, Kauf-ann P. Development of the placental villous
ree and its consequences for fetal growth. Eur
Obstet Gynecol Reprod Biol 2000;92:35-43. cAPRIL 2007 American
9. Gale NW, Yancopoulos GD. Growth factorscting via endothelial cell-specific receptor ty-osine kinases: VEGFs, angiopoietins, andphrins in vascular development. Genes Dev999;13:1055-66.0. Matsumoto T, Claesson-Welsh L. VEGF re-eptor signal transduction. Sci STKE001;112:RE21.1. Ferrara N, Gerber HP, LeCouter J. The bi-logy of VEGF and its receptors. Nat Med003;9:669-76.2. Ferrara N. Vascular endothelial growth fac-or: basic science and clinical progress. Endocrev 2004;25:581-611.3. Barleon B, Reusch P, Totzke F, et al. Solu-le VEGFR-1 secreted by endothelial cells andonocytes is present in human serum andlasma from healthy donors. Angiogenesis001;4:143-54.4. Autiero M, Luttun A, Tjwa M, Carmeliet P.lacental growth factor and its receptor, vascu-
ar endothelial growth factor receptor-1: novelargets for stimulation of ischemic tissue revas-ularization and inhibition of angiogenic and in-ammatory disorders. J Thromb Haemost003;1:1356-70.5. Autiero M, Waltenberger J, Communi D, etl. Role of PlGF in the intra- and intermolecularross talk between the VEGF receptors Flt1 andlk1. Nat Med 2003;9:936-43.6. Kim YM, Bujold E, Chaiworapongsa T, et al.ailure of physiologic transformation of the spi-al arteries in patients with preterm labor andntact membranes. Am J Obstet Gynecol003;189:1063-9.7. Kim YM, Chaiworapongsa T, Gomez R, etl. Failure of physiologic transformation of thepiral arteries in the placental bed in pretermremature rupture of membranes. Am J Obstetynecol 2002;187:1137-42.8. Arias F, Rodriquez L, Rayne SC, Kraus FT.aternal placental vasculopathy and infection:
wo distinct subgroups among patients withreterm labor and preterm ruptured mem-ranes. Am J Obstet Gynecol 1993;168:85-91.9. Maynard SE, Min JY, Merchan J, et al. Ex-ess placental soluble fms-like tyrosine kinase 1sFlt1) may contribute to endothelial dysfunc-ion, hypertension, and proteinuria in pre-clampsia. J Clin Invest 2003;111:649-58.0. Ochi H, Matsubara K, Kusanagi Y, Tanigu-hi H, Ito M. Significance of a diastolic notch inhe uterine artery flow velocity waveform in-uced by uterine embolisation in the pregnantwe. BJOG 1998;105:1118-21.1. Ochi H, Suginami H, Matsubara K, Tanigu-hi H, Yano J, Matsuura S. Micro-bead embo-
ization of uterine spiral arteries and changes interine arterial flow velocity waveforms in theregnant ewe. Ultrasound Obstet Gynecol995;6:272-6.2. Aardema MW, Oosterhof H, Timmer A, vanooy I, Aarnoudse JG. Uterine artery Dopplerow and uteroplacental vascular pathology inormal pregnancies and pregnancies compli-
ated by pre-eclampsia and small for gesta-Journal of Obstetrics & Gynecology 326.e12

t44Arm14Atao24utian4Tlt14mbM4Bvsg4Nirt15Cldvo15Cgrc5bin5Klpt
5Pgfla5BueE45rao25rtoe5SopA5Pamn6be6gA6msaf26DtmeA6BpA6Ste16
pP6Iip6Tn6bn7Bmuqsc7Sf7KpaG7elv7ceA7Dac17Snr27gG7Onetes7g(g
Research Obstetrics www.AJOG.org
3
ional age fetuses. Placenta 2001;22:05-11.3. Lin S, Shimizu I, Suehara N, Nakayama M,ono T. Uterine artery Doppler velocimetry in
elation to trophoblast migration into the myo-etrium of the placental bed. Obstet Gynecol995;85:760-5.4. Madazli R, Somunkiran A, Calay Z, Ilvan S,ksu MF. Histomorphology of the placenta and
he placental bed of growth restricted foetusesnd correlation with the Doppler velocimetriesf the uterine and umbilical arteries. Placenta003;24:510-6.5. Olofsson P, Laurini RN, Marsal K. A highterine artery pulsatility index reflects a defec-ive development of placental bed spiral arteriesn pregnancies complicated by hypertensionnd fetal growth retardation. Eur J Obstet Gy-ecol Reprod Biol 1993;49:161-8.6. Sagol S, Ozkinay E, Oztekin K, Ozdemir N.he comparison of uterine artery Doppler ve-
ocimetry with the histopathology of the placen-al bed. Aust N Z J Obstet Gynaecol999;39:324-9.7. Voigt HJ, Becker V. Doppler flow measure-ents and histomorphology of the placentaled in uteroplacental insufficiency. J Perinated 1992;20:139-47.8. Ferrazzi E, Bulfamante G, Mezzopane R,arbera A, Ghidini A, Pardi G. Uterine Dopplerelocimetry and placental hypoxic-ischemic le-ion in pregnancies with fetal intrauterinerowth restriction. Placenta 1999;20:389-94.9. Iwata M, Matsuzaki N, Shimizu I, Mitsuda N,akayama M, Suehara N. Prenatal detection of
schemic changes in the placenta of the growth-etarded fetus by Doppler flow velocimetry ofhe maternal uterine artery. Obstet Gynecol993;82:494-9.0. Nagamatsu T, Fujii T, Kusumi M, et al.ytotrophoblasts up-regulate soluble fms-
ike tyrosine kinase-1 expression under re-uced oxygen: an implication for the placentalascular development and the pathophysiol-gy of preeclampsia. Endocrinology 2004;45:4838-45.1. Shore VH, Wang TH, Wang CL, Torry RJ,audle MR, Torry DS. Vascular endothelialrowth factor, placenta growth factor and theireceptors in isolated human trophoblast. Pla-enta 1997;18:657-65.2. Steel SA, Pearce JM, McParland P, Cham-erlain GV. Early Doppler ultrasound screening
n prediction of hypertensive disorders of preg-ancy. Lancet 1990;335:1548-51.3. North RA, Ferrier C, Long D, Townend K,incaid-Smith P. Uterine artery Doppler flow ve-
ocity waveforms in the second trimester for therediction of preeclampsia and fetal growth re-
ardation. Obstet Gynecol 1994;83:378-86. g26.e13 American Journal of Obstetrics & Gyneco
4. Irion O, Masse J, Forest JC, Moutquin JM.rediction of pre-eclampsia, low birthweight forestation and prematurity by uterine artery bloodow velocity waveforms analysis in low risk nullip-rous women. BJOG 1998;105:422-9.5. Harrington KF, Campbell S, Bewley S,ower S. Doppler velocimetry studies of theterine artery in the early prediction of pre-clampsia and intra-uterine growth retardation.ur J Obstet Gynecol Reprod Biol 1991;2(suppl):S14-20.6. Aquilina J, Barnett A, Thompson O, Har-ington K. Comprehensive analysis of uterinertery flow velocity waveforms for the predictionf pre-eclampsia. Ultrasound Obstet Gynecol000;16:163-70.7. Aquilina J, Maplethorpe R, Ellis P, Har-ington K. Correlation between second trimes-er maternal serum inhibin-A and human chori-nic gonadotrophin for the prediction of pre-clampsia. Placenta 2000;21:487-92.8. Masse J, Forest JC, Moutquin JM, Marcoux, Brideau NA, Belanger M. A prospective studyf several potential biologic markers for earlyrediction of the development of preeclampsia.m J Obstet Gynecol 1993;169:501-8.9. Stamilio DM, Sehdev HM, Morgan MA,ropert K, Macones GA. Can antenatal clinicalnd biochemical markers predict the develop-ent of severe preeclampsia? Am J Obstet Gy-
ecol 2000;182:589-94.0. Romero R, Lockwood C, Oyarzun E, Hob-ins JC. Toxemia: new concepts in an old dis-ase. Semin Perinatol 1988;12:302-23.1. Dekker GA, Sibai BM. Etiology and patho-enesis of preeclampsia: current concepts.m J Obstet Gynecol 1998;179:1359-75.2. Austgulen R, Isaksen CV, Chedwick L, Ro-undstad P, Vatten L, Craven C. Pre-eclamp-
ia: associated with increased syncytialpoptosis when the infant is small-or-gestational-age. J Reprod Immunol004;61:39-50.3. Crocker IP, Cooper S, Ong SC, Baker PN.ifferences in apoptotic susceptibility of cy-
otrophoblasts and syncytiotrophoblasts in nor-al pregnancy to those complicated with pre-
clampsia and intrauterine growth restriction.m J Pathol 2003;162:637-43.4. Leung DN, Smith SC, To KF, Sahota DS,aker PN. Increased placental apoptosis inregnancies complicated by preeclampsia.m J Obstet Gynecol 2001;184:1249-50.5. Sargent IL, Germain SJ, Sacks GP, Kumar, Redman CW. Trophoblast deportation and
he maternal inflammatory response in pre-clampsia. J Reprod Immunol 2003;59:53-60.6. Johansen M, Redman CW, Wilkins T, Sar-
ent IL. Trophoblast deportation in human 2logy APRIL 2007
regnancy: its relevance for pre-eclampsia.lacenta 1999;20:531-9.7. Knight M, Redman CW, Linton EA, Sargent
L. Shedding of syncytiotrophoblast microvillinto the maternal circulation in pre-eclampticregnancies. BJOG 1998;105:632-40.8. Chua S, Wilkins T, Sargent I, Redman C.rophoblast deportation in pre-eclamptic preg-ancy. BJOG 1991;98:973-9.9. Rasmussen S, Irgens LM. Fetal growth andody proportion in preeclampsia. Obstet Gy-ecol 2003;101:575-83.0. Aardema MW, Saro MC, Lander M, De WolfT, Oosterhof H, Aarnoudse JG. Second tri-ester Doppler ultrasound screening of the
terine arteries differentiates between subse-uent normal and poor outcomes of hyperten-ive pregnancy: Two different pathophysiologi-al entities? Clin Sci (Lond) 2004;106:377-82.1. Odegard RA, Vatten LJ, Nilsen ST,alvesen KA, Austgulen R. Preeclampsia and
etal growth. Obstet Gynecol 2000;96:950-5.2. Moldenhauer JS, Stanek J, Warshak C,houry J, Sibai B. The frequency and severity oflacental findings in women with preeclampsiare gestational age dependent. Am J Obstetynecol 2003;189:1173-7.3. Sebire NJ, Goldin RD, Regan L. Term pre-clampsia is associated with minimal histopatho-
ogical placental features regardless of clinical se-erity. J Obstet Gynaecol 2005;25:117-8.4. Ness RB, Roberts JM. Heterogeneousauses constituting the single syndrome of pre-clampsia: a hypothesis and its implications.m J Obstet Gynecol 1996;175:1365-70.5. Rumbold AR, Crowther CA, Haslam RR,ekker GA, Robinson JS. Vitamins C and End the risks of preeclampsia and perinatalomplications. N Engl J Med 2006;354:796-806.6. Poston L, Briley AL, Seed PT, Kelly FJ,hennan AH. Vitamin C and vitamin E in preg-ant women at risk for pre-eclampsia (VIP trial):andomised placebo-controlled trial. Lancet006;367:1145-54.7. Levine RJ, Karumanchi SA. Circulating an-iogenic factors in preeclampsia. Clin Obstetynecol 2005;48:372-86.8. Zhang Y, Jing-Ying M, Almirez R, et al.verexpression of soluble FMS-like tyrosine ki-ase-1 (sFLT-1) induced experimental pre-clampsia in rats and attenuation of preeclamp-ic phenotype by recombinant vascularndothelial growth factor 121 (VEGF121) [ab-tract]. J Soc Gynecol Investig 2006;2:287A.9. Luttun A, Tjwa M, Carmeliet P. Placentalrowth factor (PlGF) and its receptor Flt-1
VEGFR-1): novel therapeutic targets for angio-enic disorders. Ann N Y Acad Sci
002;979:80-93.
Related Documents











