Identification of Neonatal Hearing Impairment: Hearing Status at 8 to 12 Months Corrected Age Using a Visual Reinforcement Audiometry Protocol Judith E. Widen, Richard C. Folsom, Barbara Cone-Wesson, Lisa Carty, Janet J. Dunnell, Katherine Koebsell, Ann Levi, Lisa Mancl, Brenda Ohlrich, Susan Trouba, Michael P. Gorga, Yvonne S. Sininger, Betty R. Vohr, and Susan J. Norton Objectives: 1) To describe the hearing status of the at-risk infants in the National Institutes of Health- Identification of Neonatal Hearing Impairment study sample at 8 to 12 mo corrected age (chrono- logic age adjusted for prematurity). 2) To describe the visual reinforcement audiometry (VRA) proto- col that was used to obtain monaural behavioral data for the sample. Design: All neonatal intensive care unit infants and well babies with risk factors (including well babies who failed neonatal tests) were targeted for fol- low-up behavioral evaluation once they had reached 8 mo corrected age. Three thousand one hundred and thirty-four (64.4%) of the 4868 surviv- ing infants returned for at least one behavioral hearing evaluation, which employed a well-defined VRA protocol. VRA thresholds or minimum re- sponse levels (MRLs) were determined for speech and pure tones of 1.0, 2.0, and 4.0 kHz for each ear using insert earphones. Results: More than 95% of the infants were reliably tested with the VRA protocol; 90% provided com- plete tests (four MRLs for both ears). Ninety-four percent of the at-risk infants were found to have normal hearing sensitivity (MRLs of 20 dB HL) at 1.0, 2.0, and 4.0 kHz in both ears. Of the infants, 2.2% had bilateral hearing impairment, and 3.4% had impairment in one ear only. More than 80% of the impaired ears had losses of mild-to-moderate degree. Conclusions: This may be the largest study to at- tempt to follow all at-risk infants with behavioral audiometric testing, regardless of screening out- come, in an effort to validate the results of auditory brain stem response, distortion product otoacoustic emission, and transient evoked otoacoustic emis- sion testing in the newborn period. It is one of only a few studies to report hearing status of infants at 1 yr of age, using VRA on a clinical population. Suc- cessful testing of more than 95% of the infants who returned for the VRA follow-up documents the fea- sibility of obtaining monaural behavioral data in this population. (Ear & Hearing 2000;21;471– 487) The manner in which the newborn test results were validated makes the National Institutes of Health-Identification of Neonatal Hearing Impair- ment (NIH-INHI) project unique in several ways. It is the largest study to attempt to follow its entire sample of at-risk infants, regardless of outcome on newborn test measures, until the final determina- tion of hearing status could be made. Many studies have been limited to follow-up of the group of infants who failed the newborn test. Other studies have compared the results of newborn screening tests with diagnostic tests using similar electrophysi- ologic methods (e.g., auditory brain stem response [ABR] screen to ABR threshold test, otoacoustic emissions screen to ABR threshold test). Hearing is a behavioral response; when the measures of ABR, distortion product otoacoustic emissions, and tran- sient evoked otoacoustic emissions (TEOAEs) are used to screen for neonatal hearing impairment, a behavioral measure of hearing should be the gold standard against which they are compared. A few earlier studies attempted to follow up newborn tests with a later pure-tone audiogram. To test the performance of a High Risk Questionnaire, Crib-o-Gram and ABR, Shimizu, Walters, Proctor, Kennedy, Allen, and Markowitz (1990) followed their subjects with a variety of measures at several time intervals until a pure-tone audiogram could be Multicenter Consortium on Identification of Neonatal Hearing Impairment, Seattle, Washington; University of Kansas Medical Center (J.E.W., S.T.), Kansas City, Kansas; University of Wash- ington (R.C.F., L.M.), Seattle, Washington; Los Angeles County 1 University of Southern California Medical Center (B.C.-W., K.K.), Los Angeles, California; Women and Infants’ Hospital (L.C., B.R.V.), Providence, Rhode Island; Children’s Hospital & Re- gional Medical Center (J.J.D., S.J.N.), Seattle, Washington; House Ear Institute (A.L., Y.S.S.), Los Angeles, California; Boys Town National Research Hospital (B.O., M.P.G.), Omaha, Nebraska. B.C.-W. is currently affiliated with University of Melbourne, Melbourne, Australia. Work supported by the NIDCD (DC01958). 0196/0202/00/2105-0471/0 • Ear & Hearing • Copyright © 2000 by Lippincott Williams & Wilkins • Printed in the U.S.A. 471

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Identification of Neonatal Hearing Impairment:Hearing Status at 8 to 12 Months Corrected Age
Using a Visual Reinforcement Audiometry ProtocolJudith E. Widen, Richard C. Folsom, Barbara Cone-Wesson, Lisa Carty,
Janet J. Dunnell, Katherine Koebsell, Ann Levi, Lisa Mancl, Brenda Ohlrich,Susan Trouba, Michael P. Gorga, Yvonne S. Sininger, Betty R. Vohr,
and Susan J. Norton
Objectives: 1) To describe the hearing status of theat-risk infants in the National Institutes of Health-Identification of Neonatal Hearing Impairmentstudy sample at 8 to 12 mo corrected age (chrono-logic age adjusted for prematurity). 2) To describethe visual reinforcement audiometry (VRA) proto-col that was used to obtain monaural behavioraldata for the sample.
Design: All neonatal intensive care unit infants andwell babies with risk factors (including well babieswho failed neonatal tests) were targeted for fol-low-up behavioral evaluation once they hadreached 8 mo corrected age. Three thousand onehundred and thirty-four (64.4%) of the 4868 surviv-ing infants returned for at least one behavioralhearing evaluation, which employed a well-definedVRA protocol. VRA thresholds or minimum re-sponse levels (MRLs) were determined for speechand pure tones of 1.0, 2.0, and 4.0 kHz for each earusing insert earphones.
Results: More than 95% of the infants were reliablytested with the VRA protocol; 90% provided com-plete tests (four MRLs for both ears). Ninety-fourpercent of the at-risk infants were found to havenormal hearing sensitivity (MRLs of 20 dB HL) at1.0, 2.0, and 4.0 kHz in both ears. Of the infants, 2.2%had bilateral hearing impairment, and 3.4% hadimpairment in one ear only. More than 80% of theimpaired ears had losses of mild-to-moderatedegree.
Conclusions: This may be the largest study to at-tempt to follow all at-risk infants with behavioralaudiometric testing, regardless of screening out-come, in an effort to validate the results of auditorybrain stem response, distortion product otoacousticemission, and transient evoked otoacoustic emis-sion testing in the newborn period. It is one of onlya few studies to report hearing status of infants at 1yr of age, using VRA on a clinical population. Suc-cessful testing of more than 95% of the infants whoreturned for the VRA follow-up documents the fea-sibility of obtaining monaural behavioral data inthis population.
(Ear & Hearing 2000;21;471–487)
The manner in which the newborn test resultswere validated makes the National Institutes ofHealth-Identification of Neonatal Hearing Impair-ment (NIH-INHI) project unique in several ways. Itis the largest study to attempt to follow its entiresample of at-risk infants, regardless of outcome onnewborn test measures, until the final determina-tion of hearing status could be made. Many studieshave been limited to follow-up of the group of infantswho failed the newborn test. Other studies havecompared the results of newborn screening testswith diagnostic tests using similar electrophysi-ologic methods (e.g., auditory brain stem response[ABR] screen to ABR threshold test, otoacousticemissions screen to ABR threshold test). Hearing isa behavioral response; when the measures of ABR,distortion product otoacoustic emissions, and tran-sient evoked otoacoustic emissions (TEOAEs) areused to screen for neonatal hearing impairment, abehavioral measure of hearing should be the goldstandard against which they are compared.
A few earlier studies attempted to follow upnewborn tests with a later pure-tone audiogram. Totest the performance of a High Risk Questionnaire,Crib-o-Gram and ABR, Shimizu, Walters, Proctor,Kennedy, Allen, and Markowitz (1990) followedtheir subjects with a variety of measures at severaltime intervals until a pure-tone audiogram could be
Multicenter Consortium on Identification of Neonatal HearingImpairment, Seattle, Washington; University of Kansas MedicalCenter (J.E.W., S.T.), Kansas City, Kansas; University of Wash-ington (R.C.F., L.M.), Seattle, Washington; Los Angeles County 1University of Southern California Medical Center (B.C.-W., K.K.),Los Angeles, California; Women and Infants’ Hospital (L.C.,B.R.V.), Providence, Rhode Island; Children’s Hospital & Re-gional Medical Center (J.J.D., S.J.N.), Seattle, Washington;House Ear Institute (A.L., Y.S.S.), Los Angeles, California; BoysTown National Research Hospital (B.O., M.P.G.), Omaha,Nebraska.B.C.-W. is currently affiliated with University of Melbourne,Melbourne, Australia.Work supported by the NIDCD (DC01958).
0196/0202/00/2105-0471/0 • Ear & Hearing • Copyright © 2000 by Lippincott Williams & Wilkins • Printed in the U.S.A.
471

obtained under earphones at 3 to 4 yr. Hyde, Riko,and Malizia (1990) and Durieux-Smith, Picton, Ber-nard, MacMurrary, and Goodman (1991) comparedthe ABR findings from infants and neonates withmonaural pure-tone audiograms at 3 yr of age.Studies using outcome measures that must occurlater in time, as behavioral hearing testing does,often have difficulty maintaining contact with andconvincing families to return for follow-up. Theymust also account for changes that may have oc-curred in the intervening time period. The longerthe time, the more possibilities exist for both loss ofcontact and the occurrence of intercurrent events.
Some researchers have used behavioral hearingmeasures that could be applied sooner than 3 yr.Shannon, Felix, Krumholz, Goldstein, and Harris(1984) attempted to follow newborn ABR tests withbehavioral testing at 1 yr. Swigonski, Shallop, Bull,and Lemons (1987) used sound field conditioned ori-entation response techniques at 6 to 9 mo correctedage to validate ABR screening in the newborn period.In Germany, the results from a nationwide behavioralscreening program at 9 mo were compared with theresults of ALGO screening in the newborn period (vanStraaten, Groote, & Oudesluys-Murphy, 1996). Re-searchers in the United Kingdom have capitalized onthe existence of a community health system to validatenewborn screening. In Ireland, Watson, McClelland,and Adams (1996) used records of infant distractiontests done at 7 to 10 mo and school entry tests at 4 to5 yr to validate ABR screening tests. Results of theinfant distraction tests and the records of more com-plete audiologic evaluations in community audiologydepartments in England were used in a similar way tovalidate the results of newborn screening with TEOAE(Lutman, Davis, Fortnum, & Woods, 1997) and ABR(Mason, Davis, Wood, & Farnsworth, 1998). Watkin(1996), on the other hand, did not use the infantdistraction tests done by health visitors as a goldstandard but rather simply as another screening de-vice to compare with TEOAE screening done in thenewborn period.
In most studies, descriptions of the behavioral fol-low-up procedures with infants are lacking. Stimuliare not described, with the exception of Swigonski etal. (1990) who tested with speech and either narrowband noise or warble tones at 0.5 and 4.0. kHz. In allcases, it appears that behavioral testing was done inthe sound field; thus, only the better ear was evaluateddespite monaural data from the screening tests. Arequirement of the NIH-INHI was that the final de-termination of hearing status for each subject wouldbe based on monaural behavioral thresholds for puretones and speech. These behavioral results would thenbe used to validate the accuracy of the three newborn
measures of ABR, distortion product otoacoustic emis-sion, and TEOAE in detecting hearing loss.
In the present study, visual reinforcement audi-ometry (VRA) was the behavioral method used todetermine hearing status. VRA is a modification ofstandard audiometric testing, designed for infantswho are not able to understand verbal instruction.In VRA, operant conditioning techniques are used toreward a natural orienting response of the infant byproviding an enjoyable event to reinforce the likeli-hood of continued responses. An infant’s naturalresponse to sound is a head turn in the direction ofthe sound source. When that response is rewardedby the activation of a lighted, animated toy, theinfant may continue to respond for a sufficientnumber of stimulus trials to obtain an audiogram.
VRA thresholds for infants as young as 6 mo ofage have been shown to be within 10 dB of adulthearing thresholds (Olsho, Koch, Carter, Halpin, &Spetner, 1988; Wilson & Thompson, 1984). VRAthresholds have been shown to be comparable withthresholds obtained by play audiometry at preschoolages (Diefendorf, 1988; Talbott, 1987). Good agree-ment between VRA and tympanometry indicatesthat the method is sensitive enough to detect evenslight threshold elevations, such as those due tomiddle ear effusion (Nozza & Wilson, 1984; Widen,1990). VRA is not restricted to sound field testing.Numerous reports indicate that VRA testing can bedone reliably under earphones (Diefendorf & Gravel,1996; Gravel, 1989, 1994; Nozza & Wilson, 1984).
Although normal-hearing, normal-developing in-fants can be successfully tested as young as 5 mo of age(Moore, Wilson, & Thompson, 1977), infants bornprematurely who have spent time in neonatal inten-sive care units (NICUs) tend to perform better iftesting is delayed until 6 to 8 mo corrected age (Moore,Thompson, & Folsom, 1992; Widen, 1990). By 12 mo,infants have been shown to need fewer conditioningtrials, be less variable in responses near threshold andyield fewer false positive responses than 6-mo-olds;however older infants tend to reject earphones morefrequently than younger ones (Gravel & Traquina,1992; Nozza & Wilson, 1984).
The purpose of this article is to describe thefollow-up behavioral evaluation of hearing status ofthe infants in the NIH-INHI study sample. Thehearing status of the sample is described as is theinfants’ performance with the VRA protocol usinginsert earphones.
METHOD
Subjects
The subjects for the study have been described byVohr et al. (2000). All 4911 infants graduating from
472 EAR & HEARING / OCTOBER 2000

the NICU, well babies with risk factors, and wellbabies without risk factors who failed neonataltests, were targeted for behavioral testing as de-scribed in the preceding article (Folsom et al., 2000).Of the 4868 infants who survived, 3134 (64.4%)returned for follow-up behavioral testing at 8 to 12mo corrected age. Corrected age was computed bysubtracting the number of weeks premature fromthe infant’s chronologic age, e.g., an infant who wasborn 8 wk prematurely, at 32 wk gestation, wouldreturn for follow-up testing approximately 10 moafter their birth date. The corrected age of 8 mo waschosen as the initial age to begin follow-up testing tomaximize the chance of successfully completing thebehavioral testing protocol. The age range was acompromise between younger ages at which theinfant was most likely to tolerate the earphones andthe older ages at which tests are expected to beperformed more quickly and reliably.
Test Location
Infants were tested with the VRA protocol atseven sites, generally corresponding to the hospitalswhere they were tested as newborns. For example,subjects from Children’s Hospital & Regional Medi-cal Center (CHRMC) and Overlake Hospital MedicalCenter returned to the CHRMC Audiology Clinic.Infants from the University of Washington MedicalCenter came to the Center on Human Development& Disability Audiology Clinic for follow-up testing.Kansas subjects returned to the University of Kan-sas Medical Center to the Audiology Clinic of theDepartment of Hearing and Speech and Child De-velopment Unit. In Omaha, behavioral testing wasconducted at Boys Town National Research Hospital(BTNRH) Audiology Clinic regardless of the locationof the neonatal test, St. Joseph Hospital or Univer-sity of Nebraska Medical Center. Infants from LosAngeles County University of California MedicalCenter (LAC1USCMC) could choose follow-up test-ing at the LAC1USCMC Audiology Clinic or at theCARE Center of the House Ear Institute. In Provi-dence, the behavioral follow-up testing was initiallyconducted at Rhode Island Hospital located adjacentto Women and Infants’ Hospital, the site of neonataltesting, until audiology facilities at Women andInfants’ Hospital were complete. In a few instances,when infants had moved from their original locale,the site most convenient for the family providedbehavioral testing.
Equipment
Comparable test facilities were available at eachsite. All tests were conducted in sound-treated testbooths. Although the rooms were not configured
exactly the same way with respect to size, doors,windows, etc., test room arrangement was similaracross sites. The infant was seated on the parent’slap facing forward with space for the test roomexaminer to sit opposite or adjacent to the infant,while allowing the examiner at the audiometer out-side the booth a free view of the infant’s head turns.At 90 degrees to the infant’s right and left, weresmoked Plexiglass boxes, which housed four ani-mated, toy reinforcers, two on each side. (The rein-forcer systems for four of the seven sites were builtby Intelligent Hearing Systems; the others werecustom-designed.) The test room examiner had awide variety of quiet toys near his or her side to keepthe infant’s attention at midline between stimuluspresentations.
All test sites used clinical diagnostic audiometerscalibrated to ANSI (1989, 1996) standards. At somesites, the equipment was calibrated for ER-3A insertearphones according to the recommendations ofCabot Safety Corporation (1990) and Wilber,Kruger, and Killion (1988). At other sites, soundpressure level differences between standardTDH-39 phones and the ER-3A insert phones werecalculated and correction factors were posted for usewith the insert earphones required for the presentprotocol. In all instances, the insert phones werefitted with small-size, disposable EarLink foam tips.Grason Stadler middle ear analyzers were used forscreening tympanometry; the GSI33 was the modelused for most of the evaluations, with the exceptionof some of the early tests in Rhode Island, whichwere done with a different model (GSI, 1723).
Stimuli
Test stimuli were pulsed warbled FM tones of 1.0,2.0, and 4.0 kHz, as well as speech presented viamonitored live voice. The frequencies representthose most critical for the perception of speech. Theyare also consistent with screening guidelines forolder children and adults (American Speech-Lan-guage-Hearing Association, 1985, 1990, 1997) andwithin the frequency range covered by the newbornmeasures. Speech stimuli were included to corrobo-rate the pure-tone findings, as in most clinical audi-ometry protocols. The speech stimuli were shortphrases such as “baby-baby,” “look over here,” or “hi(Baby Name),” presented via monitored live voice.
Examiners
One experienced pediatric audiologist was desig-nated as the VRA Coordinator for each site. TheVRA Coordinator maintained primary responsibilityfor all VRA testing at a site. This included qualitycontrol monitoring of protocol implementation, data
EAR & HEARING, VOL. 21 NO. 5 473

forms, equipment and its calibration, and training ofnew personnel. In most cases, she was the primarysite tester. At some sites, the Coordinator scheduledthe VRA appointments and entered the VRA data.The Coordinator was the primary contact person forVRA and communicated directly with the co-inves-tigator in charge of VRA (Widen) and the core site.
Two examiners participated in each test. Exam-iners included the audiologist administering the testand a test room examiner. At least one of theexaminers for every infant test was an experiencedpediatric audiologist. In all cases this individual hada minimum of 2 yr of experience, often more, in asetting where the majority, if not all, of the patientswere infants and children. Across the seven sites, 18audiologists conducted 90% of all tests. In manyinstances, the second examiner who was in the testroom with the infant, was another experienced au-diologist. Some of the larger sites, notably BTNRHand LAC1USC, used trained test assistants for therole of test room examiner. Other sites that providedpracticum experience for graduate students (Kan-sas, Rhode Island, Washington) sometimes trainedstudents to be examiners when the usual tester wasnot available. It was the responsibility of the testroom examiner to keep the infant appropriatelyattentive at midline, maintain a quiet environment,provide social reinforcement for correct responses,and maintain rapport with, and the cooperation of,the parent.
Observation and monitoring of VRA testing wasdone at each site on at least two occasions by one ofthe NIH-INHI co-investigators (Widen), once at thebeginning of behavioral follow-up testing and at 1 yrinto VRA data collection. Monthly reports served asa quality assurance measure that allowed sites tocompare their progress and results with others.Despite the fact that all examiners had considerableexperience with pediatric testing, the protocol wassufficiently detailed and rigorous that adjustmentand practice were necessary for all testers. In addi-tion to the direct demonstration and practice pro-vided during the site visits, instruction about theprotocol was also provided through written materialand discussions via telephone and e-mail. The de-scription of the protocol follows.
Scheduling of VRA Follow-Up Visit
To maximize the chance of completing a reliabletest on the first visit, an attempt was made toschedule healthy, rested infants, with intact visionwho were at a developmental level that suggestedthey would be able to perform the VRA task. Fol-low-up testing was not scheduled until the subjecthad reached a corrected age of at least 8 mo. When
making the appointment, parents were queriedabout the baby’s motor development and vision toassure that the baby could sit up, localize, and seethe reinforcement toys. Whenever possible, the ap-pointment was scheduled when the infant was freeof upper respiratory infection and, especially, earinfections. In addition, appointment times were se-lected when the infant was likely to be alert andresponsive. A maximum of three visits for eachsubject was allowed in hopes of obtaining a completefour-stimulus test for each ear. Families were given$20 at the end of each visit to help offset the costsincurred in returning for follow-up.
Procedure
In designing a protocol for behavioral testing,there were two primary concerns: test time and testconsistency across sites. With respect to time, get-ting families to return for follow-up visits is not aneasy task. Thus, practical decisions were made whendesigning the protocol described below. First, it wasa study priority that there be a high probability ofaccomplishing the test protocol in one visit. Based ondata from previous VRA studies, it was estimatedthat most infants could be expected to respondreliably for 30 to 40 stimulus trials (Eilers, Widen,Urbano, Hudson, & Gonzales, 1991; Moore et al.,1977; Widen, 1990). Therefore, the number of teststimuli was limited to eight, (three pure tones andone speech stimulus for each ear). A 10-dB step size(20 down, 10 up) was chosen to allow for quickconvergence on VRA threshold or “minimum re-sponse level” (MRL). For the purposes of this study,“normal” hearing was defined as MRLs of 20 dB HL.Searching for VRA threshold below 20 dB HL couldnot be justified in terms of the additional stimulustrials required, nor was it thought to further theunderstanding of any of the newborn test measures.The stop criterion for MRL was two responses, bothat 20 dB HL for each of the eight test signals or, ifabove 20 dB HL, the lowest level at which the infantresponded to two of three ascending runs. It wasreasoned that such a protocol should yield individ-ual ear data for four stimuli in a reasonable numberof trials, and, thus, in a short enough time toaccommodate an infant’s attention span.
A second study objective was to achieve VRA testconsistency across sites. Just as for the newborn testmeasures, behavioral testing had to be conducted inthe same way at each site. However, the follow-uptesting differed from the earlier newborn testing inways that were critical when designing the protocol.The physiologic measures used to test newborns didnot require the infant’s active participation nor didthey rely entirely on the examiner’s judgment of a
474 EAR & HEARING / OCTOBER 2000

response, but rather many decisions were undercomputer control. In behavioral testing, which re-quires the infant’s cooperation, a protocol may needto accommodate individual infant differences andpreferences. A protocol was designed for this projectthat was stringent enough to assure consistencyacross sites, but also sufficiently flexible to accom-modate individual infant differences or preferences.To this end, probably the most important facet of theprotocol was ensuring that the behavioral responsesof each infant were under stimulus control. Stimu-lus control refers to the strength of the discrimina-tive stimulus (tones, speech) in producing the de-sired response (head turn). The protocol requiredexaminers to demonstrate conditioning with probetrials (presumably suprathreshold stimulus presen-tations used to confirm that the infant was understimulus control) at the beginning of the sessionand/or after conditioning. Throughout the test ses-sion, stimulus control was also monitored with con-trol trials (observation intervals of the same timingand duration as stimulus trials during which nostimulus was present, and in which the examinernoted head-turn behavior but provided no reinforce-ment). The need to demonstrate stimulus controlheightened the importance of the examiner in theroom with the infant. It was the responsibility of thisexaminer to keep the infant appropriately attentiveat midline by modifying her/his actions to suit theinfant’s behavior, so that the infant’s interest in thereinforcers was maintained.
Although it is common clinical practice to beginVRA testing with sound field presentation, oftenwith a speech stimulus, the protocol for this studystipulated that testing was to begin under ear-phones, using the first in a randomized sequence ofpure tones as the initial stimulus. This stipulationwas made in the interest of minimizing stimulustrials when possible, assuming that, if the infantwas able to begin the test in this way, the criticaldata points (pure-tone MRLs for each ear) could beacquired before habituation occurred. Likewise, inan attempt to keep the number of test trials to aminimum, the protocol allowed the infant a chanceto demonstrate what she or he could do spontane-ously. The test sequence is summarized in the Ap-pendix (Fig. A1).
To assure an unbiased distribution of MRLs as afunction of frequency and ear for the entire studysample, the order of test frequency was counter-balanced across subjects. For half the subjects, theright ear was tested first. Within each ear, the orderof frequency was counter-balanced; one third begin-ning with 1.0 kHz, one third with 2.0 kHz and thefinal third with 4.0 kHz. With two ears and threepure-tone frequencies, there were 72 combinations
of possible test sequences. These 72 sequences wererandomized, printed on data sheets, and sent to eachsite for sequential use as each subject returned forfollow-up testing. (An example is shown in theAppendix, Fig. A2.) Examiners could choose to usespeech at any place in the order of testing. For manyinfants, speech was inserted last in the sequence asa hedge against habituation and to renew theirinterest in the reinforcers as the test progressed. Forothers, when conditioning was not easily establishedwith a tone, speech was inserted early in the se-quence to provide a presumably more interestingsignal to facilitate conditioning.
Testing began with a 30 dB HL probe stimulusbefore conditioning or training trials were at-tempted. If the infant responded with a head turn,reinforcement was provided by activating one of thetoys on the side to which the infant turned. A secondcorrect head turn during stimulus presentation atthe same level resulted in reinforcement, and thetest protocol was begun without training.
The infant was given two chances for an uncon-ditioned response, one to a 30-dB stimulus, anotherat 50 dB HL. If the infant did not spontaneously givea head turn toward the side stimulated, training(conditioning) trials were begun by pairing the rein-forcer with the test stimulus at 50 dB HL. After twopaired trials, a probe trial was presented whereinreinforcement was provided only for a correct headturn response. A second correct probe trial wasrequired before the search for MRL was begun. Inthe event that the infant did not respond to thisinitial sequence of conditioning plus probe trials, thetraining sequence of paired trials was repeated byfirst raising the signal level to 70 dB, then bychanging the type of stimulus, the test ear or modeof presentation (usually to sound field, rather thanearphone, presentation). Conditioning was contin-ued until the infant demonstrated stimulus controlwith consecutive correct probe trials or until alloptions for training had been exhausted.
Control trials were inserted at a rate of 25 to 30%,but actually were printed at a rate of 50% on thedata sheets (Appendix, Fig. A2). This frequent ratewas especially important for the normal-hearinginfant who could conceivably hear, and be rewardedfor, every stimulus presented. If the infant re-sponded during control trials more than 30% of thetime, the test was considered invalid and was re-peated either on another day or after a break on thesame day.
Testing was continued until the four MRLs wereobtained for the first test ear. The second ear wasthen tested in the same manner as the first. Thechoice of placing one or both earphones at thebeginning of the test was left up to the examiner.
EAR & HEARING, VOL. 21 NO. 5 475

When the second test ear was initially stimulated, ifthe infant turned spontaneously, reinforcement wasprovided on the side to which he or she turnedregardless of the test ear. If the infant did not turnspontaneously, conditioning trials were provided, aswith the first ear, with reinforcement provided tothe side of the second ear. Testing was continueduntil all MRLs were complete or until further test-ing was not possible. This latter condition occurredfor a variety of reasons: failure to condition; habitu-ation (failure to respond to signals for which earlierresponses were obtained, despite reconditioning tri-als); crying or fidgeting; refusing to wear earphones;or by generally responding inconsistently or unreli-ably. For the judgment of “good, fair, or poor” reli-ability, the audiologists used a variety of indicatorsof test reliability, including responses during controltrials, lack of response during probe trials, variabil-ity around threshold (MRL) and a high number oftrials to arrive at MRL.
Immittance Measurements
Middle ear immittance measurements were ob-tained at each follow-up visit. Once again, the prac-tical consideration of time limited the amount ofdata collected. At most sites, tympanograms wereobtained using the GSI33 in screening mode, using a226 Hz probe tone, which yielded the followingmeasures: physical volume, static admittance, peakpressure, and either tympanometric gradient orwidth (depending on site). At LAC1USCMC, thediagnostic mode was used. For the purpose of theanalyses that follow, abnormal tympanograms weredefined as those for which static immittance andtympanometric width could not be calculated (re-ported as NP or “no measurable peak” with theGrason Stadler equipment and referred to in thisarticle as “flat”). Physical volume data were used toidentify cases with pressure-equalization tubes.
As discussed in the article on follow-up (Folsom etal., 2000), middle ear effusion was expected to be themajor intercurrent event that might affect hearingstatus between the newborn and follow-up periods.Immittance measurements served as a way of deter-mining whether middle ear status had an influenceon hearing status, allowing a possible explanation ofelevated VRA thresholds. Because the intent of thisproject was not to detect hearing loss due to tran-sient middle ear effusion, but rather permanenthearing loss of any type, additional follow-up ses-sions were permitted to maximize the chance ofobtaining VRA results when an infant’s ears werefree of fluid. For the purpose of this study, if theinfant responded at 20 dB HL but had flat tympa-nograms, hearing status was regarded as “within
normal limits.” Because subsequent testing whenthe ears were clear would not result in differentaudiometric results, the subject’s participation inthe study was complete. However, because flat tym-panograms could be an indication of middle earpathology, the infant was referred for medical fol-low-up. Subjects with flat tympanograms who didnot respond to VRA testing at 20 dB HL were askedto return for reevaluation after medical evaluationand treatment was completed because elevatedMRLs might be the result of middle ear effusion andnot a consequence of sensorineural hearing loss.
Return Visits
Besides return visits for infants with elevatedMRLs due to possible middle ear effusion, returnvisits were also required for infants who did notcomplete the follow-up session for reasons related totheir ability to perform the tasks necessary to com-plete the test (for example, those who could not beconditioned, were fussy, or tired of the reinforcers).Two return visits, or a total of three attempts, wereallowed to complete participation in the protocol.More than three was considered outside the realm ofreasonable budget and effort. In a few instances(fewer than 10 cases) results from a 4th visit wereused. This occurred when a child who had been astudy subject returned to the clinic for routine clin-ical evaluation.
Data Management
On completion of a behavioral follow-up visit, thecharacteristics of each subject’s test session wereentered into the database. Details included 1) date,time, and examiners; 2) parental report of intercur-rent events such as ear infections or hospitaliza-tions; 3) data about the VRA session, such as lengthof session, number of stimulus and control trials,number of conditioning and reconditioning trials; 4)MRLs for each frequency tested; 5) tympanometricdata; and 6) disposition (whether or not the fol-low-up protocol was completed, and if not, possiblereasons why not). An example is given in the FigureA3 of the Appendix.
Once the follow-up protocol was finished, eachsubject’s behavioral hearing status was defined asthe lowest MRL reported for each test stimulus. Forexample, if a subject completed the protocol in onevisit, the MRLs for that visit were stored as his orher final MRLs for each ear. If an infant requiredtwo sessions for completion, the lowest MRLs overthe two visits were recorded as the final results. Ifan infant had elevated MRLs and a flat tympano-gram at the first visit, but returned for a second visitat which normal tympanograms were obtained, the
476 EAR & HEARING / OCTOBER 2000

MRLs obtained on that second date would be re-corded as his or her final MRLs. Likewise, if aninfant’s responses on the first visit were unreliable,the MRLs from a return visit when data wereobtained with greater reliability were considered“final” estimates. In the end, the lowest MRLs re-gardless of tympanogram outcome were recorded.“Finishing” the protocol meant that the infant wouldnot return for further visits; it did not always meanthat the infant had completed the protocol. Thus,summarizing the data is complicated by the fact thatnot every subject completed the protocol. Of the 3134infants who returned for behavioral assessment, 8%did not return for the recommended second or thirdsession and, therefore, did not complete the protocol.Another 5% of the subjects had not completed theprotocol after three sessions. Thus, the “final” MRLoutcome for some subjects may not include MRLs foreach test stimulus for each ear. A second complicat-ing factor are those instances where tympanogramswere never normal and the MRLs were elevated; inthese cases, the MRLs may reflect a hearing loss dueto transient middle ear effusion.
RESULTS
Results from the VRA protocol will be presentedin two sections. The first section describes the in-fants’ performance on the protocol and presentssummary details about how the protocol worked.The second section presents the data about thehearing status of the sample.
Infants’ Performance with the VRA Protocol
The characteristics of the follow-up sample areprovided in Table 1. All infants from the at-riskgroups, which included the 4911 infants from theNICUs and the well babies with risk factors (includ-ing the well babies considered at risk because offailure on neonatal tests), were slated for behavioralhearing evaluation regardless of the outcome of the
neonatal test procedures. This was a necessary fea-ture of the overall design of the study. By followingbabies who “passed” the neonatal test, we are able toestimate the sensitivity to hearing loss of the peri-natal procedures. By following babies who “failed”the neonatal tests, we are able to estimate thespecificity for each of the perinatal tests. Had wechosen to follow only those babies who did not passthe neonatal tests, we would not have the datanecessary to describe test sensitivity.
Of the 4868 infants who survived the perinatalperiod, 3134 returned for behavioral testing. The1734 who were inactivated without follow-up aredescribed in Folsom et al. (2000). The 3134 return-ing infants included all who came for at least onefollow-up visit. Of those 3134, 2995 (95.6%) weresuccessfully conditioned for VRA and contributed tothe data set; that is, in 95% of the infants, we wereable to obtain MRLs under earphones that werejudged to be reliable by the examiners. Many, butnot all, of the 2995 infants completed the full proto-col (eight data points, four stimuli for each ear). Thecompleteness of the data set will be described sub-sequently. Only 139 (or 4.4% of those who returned)provided no reliable VRA data. This latter groupincluded infants who could not be conditioned be-cause of developmental delay or visual impairment(20%), and the remaining 80% included infantswhose responses were either consistently unreliableor who failed to return for further testing after anunsuccessful first test. In summary, the VRA proto-col worked for 95% of the sample who returned.Because 64% of the infants returned, reliable behav-ioral data are available for 61% of infants who weretested with ABR and evoked otoacoustic emissionsin the newborn period and targeted for follow-up.
On the average, infants were 10 mo corrected age(SD 5 2.5) at the first VRA test. Because additionalvisits were sometimes required, the average cor-rected age when VRA was completed was 12 mo(mean 5 11.7, SD 5 3.9). A few subjects were tested
TABLE 1. Characteristics of the study follow-up sample
N %
NICU and well babies with risk factors 4911Expired before 8 months 43
Infants eligible for follow-up protocol 4868Inactivated with no follow-up visit 1734 (35.3% of at-risk infants)
Infants with at least one follow-up visit 3134 of 4868 (64.4% of survivors)Could not be tested reliably with VRA 139 (4.4% of returning sample)
Infants who provided reliable VRA data 2995 of 3134 (95.6% of returning infants)2995 of 4911 (61.0% of total at-risk sample)
NICU 5 neonatal intensive care unit; VRA 5 visual reinforcement audiometry.
EAR & HEARING, VOL. 21 NO. 5 477

when they were considerably older than 12 mo.Later tests were usually the result of an extendedperiod of waiting until the infant was free of middleear effusion, was developmentally ready, or delaysin locating a family.
Review of the brief history taken at the time ofthe first follow-up visit (Appendix, Fig. A3, items 4to 9) indicates that 95% of the parents thought theirbaby was hearing normally. On the day of test, 70%of the infants were reported to be not congested.Fifty-six percent reported that their baby had hadone or more ear infections before the visit. Ninepercent reported that the infant had been seriouslyill, requiring hospitalization, since discharge fromthe nursery.
Most VRA test sessions lasted 15 minutes (medi-an 5 15; mean 5 17; SD 5 10.2). Test specifics areincluded in items 10 to 17 on the Appendix (Fig. A3).A median of two conditioning trials (mean 5 3.6, SD5 3.8) were required at the beginning of the sessionand two reconditioning trials (mean 5 3.4, SD 5 4.5)later in the session. An average session contained 27reinforced stimulus trials (mean 5 27, SD 5 10.7)and nine control trials (mean 5 8.6, SD 5 4.8).Although an “average” session can be described, thestandard deviations indicate that there was a greatdeal of variability among subjects.
The 3134 infants were tested over 4933 visits.Fifty-six percent came for one VRA session, 30% hadtwo visits, and the remaining 14% were tested inthree visits. The reasons why an infant requiredadditional test sessions fell into two categories.Some reasons related to the test procedure (failed tocondition, habituated, refused earphones). The otherreason related to the likelihood that the infant hadtransient hearing loss due to middle ear effusionunrelated to the hearing status that the newborntests were designed to identify. Thus, if the infanthad elevated MRLs (.20 dB HL) in the presence ofan abnormal tympanogram, they were referred formedical examination and asked to return, hopefullywhen the ears were free of fluid. There were 2217sessions that required a revisit. Reasons for revisitsin order of occurrence were: Habituated (44%),Failed to condition (32%), Fussy (30%), AbnormalTympanogram and MRL .20 dB HL (29%), PoorTest Reliability (19%), and Refused Earphones (6%)(Appendix, Fig. A3, follow-up item 23). More thanone descriptor could be chosen to explain why thebaby did not complete the test. Therefore, althoughthe most frequent reason for failing to complete theVRA protocol in one visit was habituation, the sameinfant may also have been fussy and had middle eareffusion. Likewise, if a baby did not condition, it mayhave been because they were fussy. Rejection ofearphones was rarely a problem.
Some infants could not be tested either becausethey could not be conditioned for the task or becausetheir responses were unreliable for other reasons. Inmost of these instances, an MRL was not recorded.In others, an MRL may have been recorded based onthe rules of the protocol; in these circumstances,however, a record was made that the test resultswere considered to be of poor reliability. Because theexaminer judgement of test reliability was used as acriterion for inclusion in the database, these datawere excluded for analysis purposes. The remainingdata set reflects the MRLs that were reliably ob-tained. These are the data to which the newborntests will be compared (Norton et al., 2000).
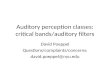
The completeness of the VRA data set is shown inFigure 1. Two thousand nine hundred and ninety-five infants could be tested reliably. Two thousandseven hundred and six infants, or 90.4% of the 2995who could be tested reliably and completed theprotocol; that is, 90.4% of the testable infants pro-vided MRLs at 1.0, 2.0, and 4.0 kHz and speech foreach ear. Another 142 (4.7%) completed a full dataset for one ear, but were incomplete for the otherear. The remaining infants had partial data, rangingfrom three data points to just one, for one or bothears. The number and percentage of ears contribut-ing to the data set are also given in Figure 1. Fivethousand eight hundred and fifty-five ears (97.7%)contributed to the data on hearing status. Four-stimuli audiograms were complete for 92.7% of theears. Another 5.0% had one to three data points. The135 ears (2.3%) with no reliable data often reflectmissing data from visits when a test was incompletebecause the infant habituated, then did not return tocomplete the test at a later visit.
Figure 1. Completeness of visual reinforcement audiometrydata set.
478 EAR & HEARING / OCTOBER 2000

Hearing Status of the Follow-Up Sample
The data reported in this next section representonly those tests for which examiners reported goodor fair confidence in the results, i.e., data from the2995 infants mentioned in Table 1. They include allears with at least one reliable data point of thepossible 4 points.
The final MRLs for the follow-up sample aredescribed completely in Table 2. The number andpercent of ears with MRLs at each level (in dB HL)are listed for pure tones (1.0, 2.0, and 4.0 kHz) andfor speech for the right and left ears. The totalnumber of infants contributing to each stimulus setis given at the top of the respective columns. Thehigher numbers for speech indicate that slightlymore infants provided MRLs to speech stimuli thanto tones. Review of MRLs in each column show thatthe vast majority of the infants responded at 20 dBHL. There is no apparent difference between ears oramong tonal frequencies; however, speech MRLstended to be slightly better than tones.
Although descriptive of the overall sample, Table2 does not describe the relationship of MRLs at eachfrequency within individual ears. A classificationscheme was needed that allowed us to classify eachear as normal or impaired, as opposed to makingthis determination on a frequency-by-frequency ba-sis. For the purposes of categorizing ears as normalor impaired, hearing impairment was defined as two
MRLs equal to or greater than 30 dB HL or one MRLequal to or greater than 40 dB (thus, a pure-toneaverage of .27 for 1.0, 2.0, and 4.0 kHz). Using thisapproach, 234 ears (4%) in the follow-up samplewere found to have hearing impairment (see Table3). These 234 ears represent 168 infants, or 5.6% ofthe infants who were tested. Sixty-six (2.2%) of theinfants had bilateral hearing impairment; 102(3.4%) had unilateral impairment.
Using this definition of hearing impairment, nor-mal-hearing ears include those with MRLs of 20 dBHL or with one MRL at 30, and the rest at 20 dB HL.The rationale for allowing one 30 dB HL responsewas based on the likelihood that infant responsesmay be slightly elevated from normal adult valuesfor nonauditory reasons (Nozza, 1995). Nonauditorycauses for elevated response levels include lack ofattention to the task, especially when first learningthe task or when beginning to fatigue. It was feltthat the length of the test session and the 10-dB step
TABLE 2. Hearing status by frequency
RE
1k 2k 4k Speech
N % N % N % N %
Total 2834 2848 2837 288420 2667 94.1 2747 96.5 2709 95.5 2820 97.830 109 3.8 58 2.0 72 2.5 35 1.240–50 36 1.3 21 0.7 30 1.1 13 0.560–70 7 0.2 6 0.2 11 0.4 7 0.280–90 6 0.2 6 0.2 4 0.1 4 0.1100–110 5 0.2 3 0.1 3 0.1 3 0.1No resp 4 0.1 7 0.2 8 0.3 2 0.1
LE
1k 2k 4k Speech
N % N % N % N %
Total 2831 2838 2821 288020 2675 94.5 2724 96.0 2689 95.3 2816 97.830 93 3.2 66 2.3 84 3.0 36 1.340–50 36 1.3 27 1.0 29 1.0 18 0.660–70 11 0.4 4 0.1 5 0.2 5 0.280–90 7 0.2 7 0.2 5 0.2 3 0.1100–110 5 0.2 4 0.1 2 0.1 1 0.0No resp 4 0.1 6 0.2 7 0.2 1 0.0
For each test stimulus, the number (N) and percent (%) of ears with minimum response levels at each level in dB HL are given, beginning with the right ear (RE) to tones at 1.0, 2.0, and 4.0kHz and speech, then left ear (LE).No resp 5 no response at limits of equipment.
TABLE 3. Hearing status of infants and ears
Infants Ears
N % N %
Normal hearing 2827 (94.4) 5621 (96.0)Hearing impairment 168 (5.6) 234 (4.0)
Bilateral 66 (2.2)Unilateral 102 (3.4)
EAR & HEARING, VOL. 21 NO. 5 479

size might contribute to an occasional 30 dB MRL innormal-hearing infants. Of the 5621 ears classifiedwith normal hearing, 5310 of them had 20 dB MRLsat all four test frequencies and 311 (or 5.5% of thetotal number of ears) had one MRL at 30 dB HL andthe rest at 20 dB HL. When considering infants,rather than ears, of the 2827 infants with normalhearing, 281 had one ear with one 30 dB MRL andonly 15 had a 30 dB MRL in both ears.
Table 4 further categorizes the 234 hearing-impaired ears with respect to the magnitude of theloss. The majority of ears with hearing impairment fall
in the mild to moderate ranges. Forty ears (17%) are inthe severe to profound categories. This group of infantswith hearing impairment is the focus of the companionarticle in this issue by Cone-Wesson et al. (2000).
Influence of Middle Ear Status on VRAResults
It is well accepted that there is not a direct relation-ship between middle ear status and hearing status.Nonetheless, a comparison of MRLs to the tympano-gram obtained on the same day may shed light on typeof hearing impairment. Table 5 summarizes tympano-metric results recorded at the same visit as the MRLs.Tympanograms were separated into two groups: thosein which a pressure peak was recorded and those withno peak (i.e., “flat”). [Presumably, ears with normalhearing and sensorineural loss should fall into the“pressure peak” category and ears with conductive lossshould be in the “no peak” categories.] Ears withpressure-equalization tubes were excluded from thisparticular analysis. Although bone conduction testing
TABLE 4. Categories of hearing impairment (HI) by ear
Definition of Hearing Loss N (%) Degree of HI
PTA . 27 # 40 dB HL 152 (65) MildPTA . 40 and # 60 dB HL 42 (18) ModeratePTA . 60 and , 90 dB HL 19 (8) SeverePTA $ 90 dB HL or no response 21 (9) Profound
PTA 5 pure-tone average at 1, 2, and 4 kHz.
TABLE 5. Number and percent of ears with tympanograms with peak pressure versus those with no peak pressure (i.e., flat) as afunction of MRLs in dB HL for each of the four test stimuli. Includes both right and left ears (except ears with P-E tubes). Data are fromall VRA visits in which reliable MRLs and tympanograms were obtained.
Tympanometric Data
Peak No Peak Total
N % N % N
MRL@1K20 4492 89.90 504 10.10 499630 272 66.00 140 34.00 41240–50 150 53.00 133 47.00 28360–70 20 64.50 11 35.50 3180–90 8 72.70 3 27.30 11100–no response 18 81.80 4 18.20 22
MRL@2K20 4597 88.50 595 11.50 519230 202 65.40 107 34.60 30940–50 107 53.80 92 46.20 19960–70 21 84.00 4 16.00 2580–90 12 92.30 1 7.70 13100–no response 20 87.00 3 13.00 23
MRL@4K20 4546 89.20 551 10.8 509730 212 65.40 112 34.6 32440–50 124 53.20 109 46.8 23360–70 27 67.50 13 32.5 4080–90 10 83.30 2 16.7 12100–no response 19 86.40 3 13.6 22
Speech MRL20 5149 87.90 707 12.1 585630 147 56.10 115 43.9 26240–50 58 54.70 48 45.3 10660–70 12 100.00 0 0.0 1280–90 10 71.40 4 28.6 14100–no response 11 84.60 2 15.4 13
MRL 5 minimum response level; VRA 5 visual reinforcement audiometry.
480 EAR & HEARING / OCTOBER 2000

was not included (and, thus, it is not possible toidentify ears with “conductive” hearing loss), onemight anticipate that a high proportion of ears withnormal MRLs would produce tympanograms withpeaks. Examination of Table 5 suggests that the pre-sumption is generally correct. At 20 dB HL, approxi-mately 90% of ears had a pressure peak. In the mildand moderate impairment levels (30 to 50 dB HL)there is a high percentage (34 to 47%) of flat (“nopeak”) tympanograms, suggesting that responses atthose levels may represent both conductive and senso-rineural impairment. At levels above 60 dB, peakedtympanograms predominate. Although one would ex-pect no difference in the incidence of middle ear dys-function (as reflected by tympanograms) in relation tothe magnitude of hearing loss, it is also unlikely thathearing loss exceeding 50 to 60 dB HL would be solelythe result of middle ear dysfunction. These MRL dataare not the final hearing status data presented inearlier tables. Return visits were successful in reduc-ing the number of MRLs obtained when tympano-grams were flat. In the end, 10% of the normal-hearingbabies had flat tympanograms with final MRLs of 20dB HL. In the group with hearing impairment, thenumber with flat tympanograms was effectivelyhalved with subsequent visits, with 15 to 20% of themild-to-moderately impaired groups having flat tym-panograms at the time of final testing.
Interaction of Hearing Status on VRA TestPerformance
One of the findings from the newborn testmeasures was that babies who did not meet stopcriteria (presumably including hearing-impairednewborns) took longer to test. A consequence oflengthy testing was sometimes incomplete neona-tal test data for that particular infant. Similarobservations were made with VRA testing. InTable 6, infants are compared on several testparameters depending on their hearing category.For this comparison, the normal-hearing groupwas divided into those with 20 dB MRLs for allfour stimuli and those with one 30 and the rest 20dB MRLs (borderline normal). The group labeled“HI” are the infants with hearing impairmentlisted in Table 3. Table 6 displays the results fromall VRA visits. The first two items in Table 6,beginning and reconditioning trials, reflect theease with which conditioning was established. Thethird item, Percent Correct control trials, is ameasure of stimulus control. Although there aredifferences across groups, from a clinical perspec-tive these differences are minimal. Stimulus trialsand length of session are both measures of testtime. On average, VRA sessions took 3 to 5 min-utes longer for infants with MRLs above 20 dB
TABLE 6. Comparison of VRA test performance for infants with normal hearing (all MRLs at 20 dB HL), those classified as borderlinenormal (one 30 dB MRL, the rest 20s), and infants with hearing impairment (HI) by the study definition (one MRL > 40 dB HL or twoMRLs > 30 dB HL). This is performance over all visits.
NormalBorderline
Normal HI
Number of visits used for calculation 3815 476 368Beginning trials (N) Mean 3.36 3.21 3.88
Median 2.00 2.00 2.00SD 3.51 2.94 4.35
Reconditioning trials (N) Mean 3.23 3.65 3.90Median 2.00 2.00 2.50SD 4.38 4.17 4.48
Correct control trials (%) Mean 88.91 89.72 89.12Median 92.00 94.00 100.00SD 14.32 15.24 17.20
Stimulus trials (N) Mean 43.14 49.95 53.41Median 40.00 48.00 52.00SD 19.88 18.90 21.59
Length of session (minutes) Mean 16.09 18.05 21.11Median 15.00 15.00 20.00SD 9.92 9.62 13.38
Test reliability Poor 10.3% 15.8% 24.2%Fair 14.3% 22.3% 35.1%Good 75.4% 62.0% 40.8%
Number of visits 1 66.0% 57.8% 45.7%2 27.1% 30.9% 32.1%3 6.8% 11.1% 22.3%
Percentage of ears with complete data 96.3% 87.5% 73.1%
VRA 5 visual reinforcement audiometry; MRL 5 minimum response level.
EAR & HEARING, VOL. 21 NO. 5 481

than for MRLs at 20 dB; part of this difference canbe explained by the protocol because MRL was notbracketed for infants responding at 20 dB HL.Test reliability was the examiners’ measure oftheir confidence in the results of individual testsessions. It is related to other measures in severalways. For example, all tests with poor reliabilitywere repeated, which in turn leads to greaternumber of visits. This does not mean that we haveless confidence in the final MRLs for the infantswith hearing impairment, but that the infants hadto return for second or third visits more often thannormally hearing infants. Other items are inter-related as well. Infants who required more condi-tioning trials received more stimulus trials; thelonger the session, the more likely the infantwould habituate, requiring a second visit to com-plete the protocol. Although not critical to theprimary focus of the main study, these observa-tions are relevant to the current study because oftheir effect on the completeness of the data. Justas with the newborn measures, testing of subjectswho did not have normal responses took longerthan tests of subjects with normal responses.Consequently, the data for hearing-impaired sub-jects were more often incomplete than the data fornormal-hearing subjects.
DISCUSSION
The data set reported here is different from manyprevious reports of hearing status in infants. Withrespect to the primary goals of the NIH-INHIproject, it is unique in that an effort was made tofollow all at-risk infants tested as newborns regard-less of their newborn test results. In that way, it isthe largest study to report follow-up of infants who“passed” the newborn tests and thus should providea good estimate of false negative rate. In addition,this is the only follow-up study of which the authorsare aware that has obtained ear-specific behavioralaudiograms on infants.
A limitation of all longitudinal studies is attrition.The 64.4% return rate for the NIH-INHI project wascomparable with other studies that required sub-jects to return months or years later. The rate isbetter than some studies; Shannon et al. (1984)reported a 30% return rate and Durieux-Smith et al.(1991) were able to follow 55%. The rate was not asgood as Hyde et al. (1990) or Shimizu et al. (1990),who followed 72 to 74% of screened infants out to 4yr of age. Follow-up is imperfect even in countriesthat have an established health-care follow-up sys-tem. Watson et al. (1996) followed 89% of the passes,whereas van Straaten et al. (1996) followed 78.5%.
One level on which the NIH-INHI project differsfrom these other studies is in sample size, with fourtimes the number of subjects compared with thenext largest study (Hyde et al., 1990).
None of the studies that validated newbornscreening with behavioral hearing tests in infancyprovided sufficient information about the follow-upprocedures to judge whether their gold standard wasas rigorously administered as their screening testshad been, making it difficult to compare their re-sults to the performance of our VRA protocol. De-spite numerous research studies using VRA, thereare few reports of its use in a clinical population.When VRA is used as a method in studies of infantperception, subjects who cannot be quickly condi-tioned and/or who have possible hearing loss areusually excused from the study. Therefore, there aremany studies based on highly selected groups ofnormally hearing infants but few studies based ondata from unselected infants and/or infants withhearing impairment (Carney, 1992). With respect tothe percentage of infants from a clinical populationthat can be conditioned for VRA, Widen (1990)reported success with VRA in 86% of NICU gradu-ates who were 7 to 8 mo corrected age and 95% forinfants at 12 mo corrected age. However, theseinfants were tested in the sound field with only twostimuli. Gravel and Traquina (1992) reported that90% of infants between 6 and 24 mo of age providedat least three pure-tone thresholds for air-conductedtonal stimuli (either under earphones or in soundfield). Eighty-four percent could be assessed withstandard earphones, with younger infants (6 to 12mo) achieving more success (90%) than 13- to 24-mo-olds. Using insert earphones, a higher success ratewas achieved in the present study.
Despite numerous research studies and clinicalreports of its effectiveness (Diefendorf & Gravel,1996; Gravel & Traquina, 1992; Thompson & Fol-som, 1984, 1985; Wilson & Thompson 1984), therewas no generally accepted standard clinical protocolfor VRA when we began this project. Descriptionsfrom some of these studies served as guidelines forthe development of the protocol designed for theNIH-INHI project. Once the testers became accus-tomed to the protocol and worksheet, they generallyreported confidence in the approach. The protocolworked well, as evidenced by the high percentage ofinfants on whom it was successful. Ninety-five per-cent of the infants tested in our study could do theVRA task under earphones, and of those, 90% gavefour-frequency audiograms for each ear. When theVRA protocol was designed, a great deal of attentionwas placed on obtaining monaural data with insertearphones. As the project progressed, it becameapparent that testing could be accomplished easily
482 EAR & HEARING / OCTOBER 2000

using insert earphones. Other clinical misconcep-tions about the need to begin testing in the soundfield and with speech were not supported by theobservation that infants responded to conditioningwith tones under earphones.
The primary purpose of the follow-up behavioraltesting was to determine each subject’s permanenthearing status for comparison with his or her new-born tests. This comparison is reported in a laterarticle by Norton et al. (2000). Aside from its role ofproviding the “gold standard” for the newborn tests,the data set stands alone as a report of hearingstatus in high-risk infants at 8 to 12 mo correctedage. These data can then be compared with othersthat have reported the incidence of hearing impair-ment in infants at risk for hearing loss. The defini-tion of hearing loss is a critical consideration inmaking comparisons across studies. Four percent ofthe ears in our sample had hearing levels of 30 dBHL or greater at two frequencies or 40 dB HL orgreater at one frequency. By this definition, 5.6% ofthe infants had one or both ears with hearingimpairment. This estimate of prevalence does notinclude the infants whose hearing status could notbe documented by behavioral means, and thus maybe an underestimate compared with other publishedreports. On the other hand, this report probablyincludes subjects with conductive hearing impair-ment due to otitis media acquired after the newbornperiod. The way in which these infants were sepa-rated from the permanent congenital losses is ad-dressed in Cone-Wesson et al. (2000).
Although the NIH-INHI project was not designedto study middle ear status in infants 8 to 12 mo ofage, by focusing on this age range, the data providesome evidence of the prevalence of otitis media witheffusion. Parent report of history of otitis media(55%), the presence of flat tympanograms and ele-vated MRLs (30% of the visits) and the report of PEtubes in 144 (4.6%) support reports in the literaturethat middle ear effusion is prevalent at this age(Teele, Klein, & Rosner, 1980, 1989) and in gradu-ates of NICUs (Balkany, Berman, Simmons, &Jafek,1978). One of the most difficult tasks in thisstudy was to obtain the behavioral data when in-fants were free of middle ear effusion, becausemiddle ear effusion has its highest prevalence in thisage range and may be unrelated to middle earcondition and hearing status in the newborn period.Every effort was made to minimize the problems ofmiddle ear effusion in the analysis. Despite efforts toobtain VRA data on healthy, uncongested infantsand by providing up to three VRA visits, somesubjects did not complete the protocol when tympa-nograms were normal, and presumably their middleears were clear. Either they did not return for
additional visits or they did not provide all eightdata points when their middle ears were clear (asdetermined by tympanometry). Durieux-Smith et al.(1991), Hyde et al. (1990), van Straaten et al. (1996),and Watson et al. (1996) all acknowledged that theirfinal estimates of hearing loss included conductivehearing impairments that may not have beenpresent at the time of the neonatal tests. For thepresent study, an independent diagnosis of middleear pathology or middle ear condition was not a partof the protocol. In addition, the tympanometric mea-sures used to judge middle ear state were imprecise,being based on screening (not diagnostic) tympano-grams, using a broadly defined criterion (presence orabsence of peak pressure) to define normal andabnormal ears. Bone conduction testing was notdone. Thus, inferences about the contribution ofmiddle ear pathology to elevated MRLs must bemade tentatively.
A problem closely related to that of obtainingMRLs that reflect ears that were free of effusion isthat the ultimate “final” audiogram is not the samefor all subjects. For the majority of subjects, the finalaudiogram includes four data points for each earwhen ears were free of fluid and when the infantresponded reliably to testing. In 5% of subjects, thedata were incomplete with fewer than four datapoints per ear. In isolated instances, the “final”audiogram may be mixed in that some MRLs wereobtained on a visit with normal tympanograms andother MRLs on a visit when tympanograms wereflat. Another way that the “final” audiogram maydiffer across infants relates to intercurrent events.Some infants’ “final” MRLs reflect hearing statusafter some intercurrent event (such as PE tubes)and others reflect the pretreatment condition. Thesedifferences will need to be considered in the finalcomparison of newborn test results to hearing statusat 8 to 12 mo of age. Some of these instances areaddressed specifically in the following article, titled“Infants with Hearing Loss” (Cone-Wesson et al.,2000).
In summary, 94.4% of the at-risk infants whoreceived follow-up behavioral evaluation had nor-mal hearing sensitivity at 1.0, 2.0, and 4.0 kHz inboth ears. Of the infants, 2.2% had bilateral hearingimpairment, and 3.4% had impairment in one earonly. More than 80% of the impaired ears had lossesof mild-to-moderate degree. These data were ob-tained with a well-defined VRA protocol using insertearphones. Successful testing of 95% of the infantswho returned for follow-up behavioral evaluationdocuments the feasibility of obtaining monauralbehavioral data in this population.
EAR & HEARING, VOL. 21 NO. 5 483

ACKNOWLEDGMENTS:It would seem that the 14 co-authors of this article (the VRACoordinators and the Co-PIs from each of the seven sites) shouldinclude every one involved in VRA testing efforts. In fact, otherindividuals shared major responsibility for VRA coordinationover the course of the data collection period, and we want toacknowledge them here: Janice Loggins at the Care Center ofHouse Ear Institute and Ann Kalberer and Brenda Hoover atBoys Town National Research Hospital. In addition, numerousothers assisted in locating, scheduling, and testing the babies.Their help was invaluable. And, to the families who kept theircommitment for follow-up, we are most grateful. Thanks also toDrs. Susan Jerger, Judy Gravel, Deborah Hayes, and four otheranonymous reviewers for their careful review and helpful com-ments on the previous version of this manuscript.
Address for correspondence: Judith E. Widen, Ph.D., Departmentof Hearing and Speech, University of Kansas Medical Center,3901 Rainbow Boulevard, Kansas City, Kansas 66160-7605.
Received January 28, 2000; accepted May 26, 2000
REFERENCES
American National Standards Institute (1989). Specification foraudiometers 53.6–1989. New York: ANSI.
American National Standards Institute (1996). Specification foraudiometers 53.6–1996. New York: ANSI.
American Speech-Language-Hearing Association (1985). Guide-lines for identification audiometry. Asha, 27, 49–52.
American Speech-Language-Hearing Association (1990). Guide-lines for screening for hearing impairments and middle eardisorders. Asha, 32(Suppl. 2), 17–24.
American Speech-Language-Hearing Association (1997). Guide-lines for Audiologic Screening. Rockville, MD: AmericanSpeech-Language-Hearing Association.
Balkany, T. J., Berman, S. A., Simmons, M. A., & Jafek, B. W.(1978). Middle ear effusion in neonates. Laryngoscope, 88,398–405.
Cabot Safety Corporation (1990). Instructions for Use of E-A-RTONE 3A Insert Earphones. Indianapolis, IN: Cabot SafetyCorporation.
Carney, A. E. (1992). Bridging the gap between developmentalpsychoacoustics and pediatric audiology. In L. A. Werner & E.W Rubel (Eds.), Developmental Psychoacoustics (pp. 333–349).Washington, DC: American Psychological Association.
Cone-Wesson, B., Vohr, B. R., Sininger, Y. S., Widen, J. E.,Folsom, R. C., Gorga, M. P., & Norton, S. J. (2000). Identifica-tion of neonatal hearing impairment: Infants with hearing loss.Ear and Hearing, 21, 488–507.
Diefendorf, A. O. (1988). Behavioral evaluation of hearing im-paired children. In F. N. Bess (Ed.), Hearing Impairment inChildren (pp.133–151). Parkton, MD: York Press, Inc.
Diefendorf, A. O., & Gravel, J. S. (1996). Behavioral observationand visual reinforcement audiometry. In S. E. Gerber (Ed.),The Handbook of Pediatric Audiology (pp. 55–83). Washington,DC: Gallaudet Press.
Durieux-Smith, A., Picton, T. W., Bernard, P., MacMurrary, B., &Goodman, J. T. (1991). Prognostic validity of brainstem electricresponse audiometry in infants of a neonatal intensive careunit. Audiology, 30, 249–265.
Eilers, R. E., Widen, J. E., Urbano, R., Hudson, T., & Gonzales, L.(1991). Optimization of automated hearing test algorithms: Acomparison of data from simulations and young children. Earand Hearing, 12, 199–204.
Folsom, R. C., Widen, J. E., Vohr, B. R., Cone-Wesson, B., Gorga,M. P., Sininger, Y. S., & Norton, S. J. (2000). Identification ofneonatal hearing impairment: Recruitment and follow-up. Earand Hearing, 21, 462–470.
Gravel, J. S. (1989). Behavioral assessment of auditory function.Seminars in Hearing, 10, 216–228.
Gravel, J. S. (1994). Auditory assessment of infants. Seminars inHearing, 15, 100–113.
Gravel, J. S., & Traquina, D. N. (1992). Experience with theaudiologic assessment of infants and toddlers. InternationalJournal of Pediatric Otorhinolaryngology, 23, 59–71.
Hyde, M. L., Riko, K., & Malizia, K. (1990). Audiometric accuracyof the click ABR in infants at risk for hearing loss. Journal ofAmerican Academy of Audiology, 1, 59–66.
Lutman, M. E., Davis, A. C., Fortnum, H. M., & Wood, S. (1997).Field sensitivity of targeted neonatal hearing screening bytransient-evoked otoacoustic emissions. Ear and Hearing, 18,265–276.
Mason, S., Davis, A., Wood, S., & Farnsworth, A. (1998).Field sensitivity of targeted neonatal hearing screeningusing the Nottingham ABR screener. Ear and Hearing, 19,91–102.
Moore, J. M., Thompson, G., & Folsom, R. C. (1992). Auditoryresponsiveness of premature infants utilizing visual reinforce-ment audiometry (VRA). Ear and Hearing, 13, 187–194.
Moore, J. M., Wilson, W. R., & Thompson, G. (1977). Visualreinforcement of head-turn responses in infants under 12months of age. Journal of Speech and Hearing Disorders, 42,328–334.
Norton, S. J., Gorga, M. P., Widen, J. E., Folsom, R. C., Sininger,Y. S., Cone-Wesson, B., Vohr, B. R., Mascher, K. E., Fletcher,K. A. (2000). Identification of neonatal hearing impairment:Evaluation of TEOAE, DPOAE and ABR test performance. Earand Hearing, 21, 508–528.
Nozza, R. J. (1995). Estimating the contribution of non-sensoryfactors to infant-adult differences in behavioral thresholds.Hearing Research, 91, 72–78.
Nozza, R. J., & Wilson, W. R. (1984). Masked and unmaskedpure-tone thresholds of infants and adults: Development ofauditory frequency selectivity and sensitivity. Journal ofSpeech and Hearing Research, 27, 613–622.
Olsho, L. W., Koch, E. G., Carter, E. A., Halpin, C. F., & Spetner,N. B. (1988). Pure tone sensitivity of human infants. Journal ofthe Acoustical Society of America, 84, 1316–1324.
Shannon, D. A., Felix, J. K., Krumholz, A., Goldstein, P. J., &Harris, K. C. (1984). Hearing screening of high risk newbornswith brainstem auditory evoked potentials: A follow-up study.Pediatrics, 73, 22–26.
Shimizu, H., Walters, R. J., Proctor, L. R., Kennedy, D. W., Allen,M. C., & Markowitz, R. K. (1990). Identification of hearingimpairment in the neonatal intensive care unit population:Outcome of a five year project at the Johns Hopkins hospital.Seminars in Hearing, 11, 151–166.
Swigonski, N., Shallop, J., Bull, M. J., & Lemons, J. A. (1987).Hearing screening of high risk newborns. Ear and Hearing, 8,26–30.
Talbott, C. B. (1987). A longitudinal study comparing responses ofhearing impaired infants to pure tones using visual reinforce-ment and play audiometry. Ear and Hearing, 8, 175–179.
Teele, D. W., Klein, J. O., & Rosner, B. A. (1980). Epidemiology ofotitis media in children. Annals of Otology, Rhinology, andLaryngology, 89(Suppp. 68), 5–6.
Teele, D., W., Klein, J. O., & Rosner, B. (1989). Epidemiology ofotitis media during the first seven years of life in children ingreater Boston. Journal of Infectious Diseases, 160, 83–94.
Thompson, G., & Folsom, R. C. (1984). A comparison of twoconditioning procedures in the use of visual reinforcement
484 EAR & HEARING / OCTOBER 2000

audiometry (VRA). Journal of Speech and Hearing Disorders,49, 241–245.
Thompson, G., & Folsom, R. C. (1985). Reinforced and nonrein-forced head-turn responses of infants as a function of stimulusbandwidth. Ear and Hearing, 6, 125–129.
Thompson, G., & Wilson, W. R. (1984). Clinical application of visualreinforcement audiometry. Seminars in Hearing, 5, 85–99.
van Straaten, H. L. M., Groote, M. E., & Oudesluys-Murphy,A. M. (1996). Evaluation of an automated auditory brainstemresponse infant hearing screening method in at risk neonates.European Journal of Pediatrics, 155, 702–705.
Vohr, B. R., Cone-Wesson, B., Widen, J. E., Sininger, Y. S., Gorga,M. P., Folsom, R. C., & Norton, S. J. (2000). Identification ofneonatal hearing impairment: Characteristics of infants in theneonatal intensive care unit (NICU) and well baby nursery.Ear and Hearing, 21, 373–382.
Watkin, P. M. (1996). Outcomes of neonatal screening for hearingloss by otoacoustic emissions. Archives of Disease in Childhood,75, F158–F168.
Watson, D. R., McClelland, R. J., & Adams, D. A. (1996). Auditorybrainstem response screening for hearing loss in high riskneonates. International Journal of Pediatric Otorhinogology,36, 147–183.
Widen, J. E. (1990). Behavioral screening of high-risk infantsusing visual reinforcement audiometry. Seminars in Hearing,11, 342–356.
Wilber, L. A., Kruger, B., & Killion, M. (1988). Reference thresh-olds for the ER-3A insert earphone. Journal of the AcousticalSociety of America, 83, 669–676.
Wilson, W. R., & Thompson, G. (1984). Behavioral audiometry. InJ. Jerger (Ed.), Pediatric Audiology. San Diego: College HillPress. Figure A1. Visual reinforcement audiometry protocol summary.
EAR & HEARING, VOL. 21 NO. 5 485

Figure A2. Example of visual reinforcement audiometry protocol worksheet.
486 EAR & HEARING / OCTOBER 2000

Figure A3. Data recorded for each visual reinforcement audiometry visit.
EAR & HEARING, VOL. 21 NO. 5 487
Related Documents