Identification of miR-187 and miR-182 as Biomarkers of Early Diagnosis and Prognosis in Patients with Prostate Cancer Treated with Radical Prostatectomy Irene Casanova-Salas, Jos e Rubio-Briones, Ana Calatrava, Caterina Mancarella, Esther Masi a, Juan Casanova, Antonio Fern andez-Serra, Luis Rubio, Miguel Ramı ´rez-Backhaus, Ana Armi ~ n an, Jos e Domı ´nguez-Escrig, Francisco Martı´nez, Zaida Garcı´a-Casado, Katia Scotlandi, Marı ´a J. Vicent and Jos e Antonio L opez-Guerrero* From the Laboratory of Molecular Biology (ICS, AFS, LR, JALG), Service of Urology (JRB, JC, MRB, JDE, ZGC) and Department of Pathology (AC), Fundaci on Instituto Valenciano de Oncologı ´a, Polymer Therapeutics Laboratory, Centro de Investigaci on Prı ´ncipe Felipe (EM, AA, MJV) and Department of Statistics, University of Valencia (FM), Valencia, Spain, and Laboratory of Experimental Oncology, Istituto Ortopedico Rizzoli (CM, KS), Bologna, Italy Purpose: miRNAs are noncoding RNAs that negatively regulate target mRNA gene expression. Aberrant miRNA expression is associated with prostate cancer pathogenesis. We identified miRNAs as potential biomarkers for prostate cancer diagnosis and prognosis. Materials and Methods: Total RNA was obtained from 10 normal prostate and 50 prostate cancer samples, and analyzed using the GeneChipÒ miRNA 2.0 Array. At a median followup of 92 months (range 2 to 189) an independent cohort of 273 paraffin embedded prostate cancer samples was used for validation by quantitative reverse transcriptase-polymerase chain reaction. Another 92 urine samples from patients undergoing prostate biopsy were evaluated for these miRNAs. Results: miR-182 and 187, the miRNAs most differentially expressed between normal and tumor tissue, were selected for further validation. miR-187 inversely correlated with cT (p ¼ 0.125) and pT (p ¼ 0.0002) stages, Gleason score (p ¼ 0.003) and TMPRSS2-ERG status (p ¼ 0.003). The log rank test showed associations of miR-182 with biochemical (p ¼ 0.026) and clinical (p ¼ 0.043) progression-free survival, as also noted on multivariate analysis. A significant independent improvement in the definition of risk of progression was achieved by combining miR-182 expression with Gleason score (p <0.0001). miR-187 detection in urine provided an independent predictive value for positive bi- opsy. A prediction model including serum prostate specific antigen, urine PCA3 and miR-187 provided 88.6% sensitivity and 50% specificity (AUC 0.711, p ¼ 0.001). Conclusions: Results show that miR-182 and 187 are promising biomarkers for prostate cancer prognosis to identify patients at risk for progression and for diagnosis to improve the predictive capability of existing biomarkers. Key Words: prostatic neoplasms, biological markers, microRNAs, diagnosis, prognosis Abbreviations and Acronyms BPFS ¼ biochemical PFS DRE ¼ digital rectal examination FDR ¼ false discovery rate FFPE ¼ formalin fixed, paraffin embedded PCA3 ¼ prostate cancer antigen 3 PCR ¼ polymerase chain reaction PFS ¼ progression-free survival PSA ¼ prostate specific antigen qRT-PCR ¼ quantitative reverse transcriptase-PCR sRNA ¼ small RNA Accepted for publication January 29, 2014. Study received institutional ethics committee approval. Supported by Grants FIS PI10/01206 and FPI11/00505 from the Instituto de Salud Carlos III, Madrid and ACOMP12/029 from the Gen- eralitat Valenciana, Valencia, Spain. * Correspondence: Laboratory of Molecular Biology, Fundacion Instituto Valenciano de Oncologia, C/Profesor Beltr an B aguena 8, 46009 Valencia, Spain (telephone: þ34-961114337; FAX: þ34-961114341; e-mail: [email protected] ). 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105 106 107 108 109 110 111 112 113 114 Dochead: Investigative Urology FLA 5.2.0 DTD ĸ JURO11082_proof ĸ 20 March 2014 ĸ 9:06 pm ĸ EO: JU-13-1929 0022-5347/14/1921-0001/0 THE JOURNAL OF UROLOGY ® © 2014 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH,INC. http://dx.doi.org/10.1016/j.juro.2014.01.107 Vol. 192, 1-8, July 2014 Printed in U.S.A. www.jurology.com j 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657
58596061626364656667686970717273747576
Identification of miR-187 and miR-182 as Biomarkers of EarlyDiagnosis and Prognosis in Patients with Prostate CancerTreated with Radical Prostatectomy
Irene Casanova-Salas, Jos�e Rubio-Briones, Ana Calatrava, Caterina Mancarella,
Esther Masi�a, Juan Casanova, Antonio Fern�andez-Serra, Luis Rubio,
Miguel Ramı́rez-Backhaus, Ana Armi~n�an, Jos�e Domı́nguez-Escrig,
Francisco Martı́nez, Zaida Garcı́a-Casado, Katia Scotlandi,
Marı́a J. Vicent and Jos�e Antonio L�opez-Guerrero*
From the Laboratory of Molecular Biology (ICS, AFS, LR, JALG), Service of Urology (JRB, JC, MRB, JDE, ZGC) and Department
of Pathology (AC), Fundaci�on Instituto Valenciano de Oncologı́a, Polymer Therapeutics Laboratory, Centro de Investigaci�on
Prı́ncipe Felipe (EM, AA, MJV) and Department of Statistics, University of Valencia (FM), Valencia, Spain, and Laboratory of
Experimental Oncology, Istituto Ortopedico Rizzoli (CM, KS), Bologna, Italy
Abbreviations
and Acronyms
BPFS ¼ biochemical PFS
DRE ¼ digital rectal examination
FDR ¼ false discovery rate
FFPE ¼ formalin fixed, paraffinembedded
PCA3 ¼ prostate cancer antigen 3
PCR ¼ polymerase chain reaction
PFS ¼ progression-free survival
PSA ¼ prostate specific antigen
qRT-PCR ¼ quantitative reversetranscriptase-PCR
sRNA ¼ small RNA
Accepted for publication January 29, 2014.Study received institutional ethics committee
approval.Supported by Grants FIS PI10/01206 and
FPI11/00505 from the Instituto de Salud CarlosIII, Madrid and ACOMP12/029 from the Gen-eralitat Valenciana, Valencia, Spain.
* Correspondence: Laboratory of MolecularBiology, Fundacion Instituto Valenciano deOncologia, C/Profesor Beltr�an B�aguena 8, 46009Valencia, Spain (telephone: þ34-961114337;FAX: þ34-961114341; e-mail: [email protected]).
7778798081828384858687888990919293949596979899
100101102103104105106107108
Purpose: miRNAs are noncoding RNAs that negatively regulate target mRNAgene expression. Aberrant miRNA expression is associated with prostate cancerpathogenesis. We identified miRNAs as potential biomarkers for prostate cancerdiagnosis and prognosis.
Materials and Methods: Total RNA was obtained from 10 normal prostateand 50 prostate cancer samples, and analyzed using the GeneChip� miRNA2.0 Array. At a median followup of 92 months (range 2 to 189) an independentcohort of 273 paraffin embedded prostate cancer samples was used for validationby quantitative reverse transcriptase-polymerase chain reaction. Another92 urine samples from patients undergoing prostate biopsy were evaluated forthese miRNAs.
Results: miR-182 and 187, the miRNAs most differentially expressed betweennormal and tumor tissue, were selected for further validation. miR-187 inverselycorrelated with cT (p ¼ 0.125) and pT (p ¼ 0.0002) stages, Gleason score(p ¼ 0.003) and TMPRSS2-ERG status (p ¼ 0.003). The log rank test showedassociations of miR-182 with biochemical (p ¼ 0.026) and clinical (p ¼ 0.043)progression-free survival, as also noted on multivariate analysis. A significantindependent improvement in the definition of risk of progression was achievedby combining miR-182 expression with Gleason score (p <0.0001). miR-187detection in urine provided an independent predictive value for positive bi-opsy. A prediction model including serum prostate specific antigen, urinePCA3 and miR-187 provided 88.6% sensitivity and 50% specificity (AUC 0.711,p ¼ 0.001).
Conclusions: Results show that miR-182 and 187 are promising biomarkersfor prostate cancer prognosis to identify patients at risk for progression andfor diagnosis to improve the predictive capability of existing biomarkers.
Key Words: prostatic neoplasms, biological markers,
microRNAs, diagnosis, prognosis
109110111112113114
Dochead: Investigative Urology FLA 5.2.0 DTD � JURO11082_proof � 20 March 2014 � 9:06 pm � EO: JU-13-1929
0022-5347/14/1921-0001/0
THE JOURNAL OF UROLOGY®
© 2014 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH, INC.
http://dx.doi.org/10.1016/j.juro.2014.01.107
Vol. 192, 1-8, July 2014
Printed in U.S.A.www.jurology.com j 1
½T1�½T1�
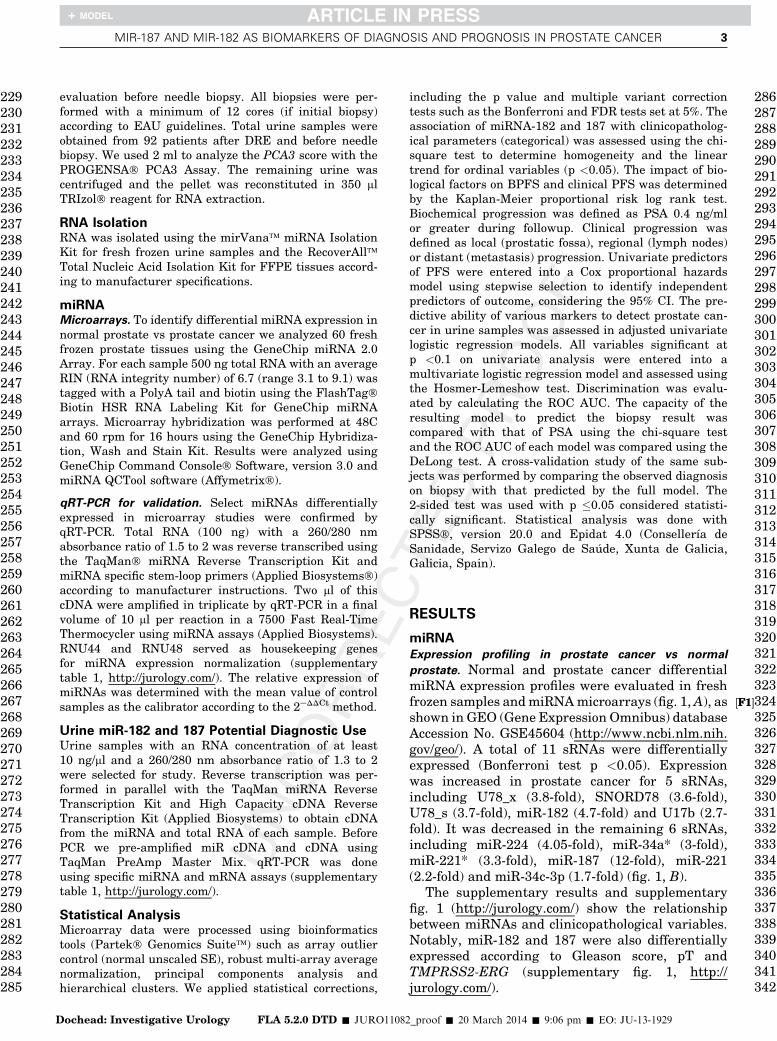
Table 1. Clinicopathological features of analyzed series
No. Fresh Frozen (%) No. Retrospective (%)
Age:* Not availableLess than 68 131 (48)68 or Greater 141 (52)
PSA (ng/ml): Not availableLess than 10 157 (58)10e20 74 (27)Greater than 20 42 (15)
Specimen Gleason score:6 or Less 15 (30) 107 (39)7 25 (50) 134 (49)8e10 10 (20) 32 (12)
cT: Not availablecT2b or less 251 (92.3)cT3a or greater 21 (7.7)
pT:pT2 or less 35 (71) 136 (50)pT3 or greater 14 (29) 136 (50)
pN:† Not availablepN0 239 (95)pN1 or greater 12 (5)
Perineural invasion: Not availableNeg 125 (49)Pos 129 (51)
TMPRSS2-ERG status:11
Neg 15 (37) 118 (43)Pos 26 (63) 155 (57)
*Median 68 years (range 49 to 84).† Lymphadenectomy limited to obturator fossa in most patients at study inclusion.
2 MIR-187 AND MIR-182 AS BIOMARKERS OF DIAGNOSIS AND PROGNOSIS IN PROSTATE CANCER
115116117118119120121122123124125126127128129130131132133134135136137138139140141142143144145146147148149150151152153154155156157158159160161162163164165166167168169170171
172173174175176177178179180181182183184185186187188189190191192193194195196197198199200201202203204205206207208209210211212213214215216217218219220221222223224225226227228
PROSTATE cancer, the most common cancer in men,causes 10% of cancer deaths in Europe. Approxi-mately 1 of 3 men older than 50 years shows his-tological evidence of prostate cancer but only 10%are diagnosed with clinically significant prostatecancer.1 Clinical phenotypes of prostate cancervary from indolent disease requiring no treatmentto tumors that metastasize and escape local therapyeven with early detection.
The current standard for prostate cancerscreening consists of a PSA blood test and DRE,2
although the positive predictive value of thesemethods is only 24% and 37%, respectively.2,3 PSAis the single most significant predictive factor toidentify men at increased risk for prostate cancerto date4 but it is not cancer specific and it iscommonly increased in benign conditions.1,5,6 Thus,PSA screening leads to prostate cancer over diag-nosis and overtreatment.
Few biomarkers are currently validated for pros-tate cancer diagnosis. A recent FDA (Food and DrugAdministration) clinical grade urine based assay forthe noncoding transcript PCA3, which is overexpressed in greater than 95% of prostate cancers,was useful when combined with serum PSA for pros-tate cancer detection.7 Another potential biomarkeris the specific TMPRSS2 and ERG rearrangementat 21q22,which is 100% indicative of prostate cancer.1
However, because it is present in only approximately50% of prostate cancers, additional clinically robustbiomarkers are needed that can differentiate indolentfrom aggressive prostate cancer.1
miRNAs are a class of small noncoding RNAconsisting of 19 to 22 nucleotides involved in variousbiological processes, including development, differ-entiation, apoptosis and cell proliferation. miRNAsregulate the expression of more than 60% of proteincoding genes.8 miRNAs can function as tumor sup-pressor genes or oncogenes and they also contributeto the initiation and development of various types ofcancer, including prostate cancer.8 Specific miRNApatterns in body fluids, such as the serum or urineof patients with prostate cancer, suggest a prom-ising role for these molecules as surrogate markers.To date most miRNA studies of prostate cancer haveinvolved relatively small patient cohorts, limitingthe validity and clinical application of potentialmiRNA biomarkers or signatures.9
We identified miR-182 and 187 as the mostdifferentially expressed miRNAs based on themiRNA expression pattern in clinical prostate can-cer and normal prostate specimens. We describetheir clinicopathological significance in a largeretrospective series of 273 prostate cancer cases. Wealso evaluated their potential as biomarkers forearly detection of prostate cancer in patient urineas an alternative to prostate biopsy.
Dochead: Investigative Urology FLA 5.2.0 DTD � JURO110
MATERIALS AND METHODS
Clinical Prostate SpecimensFresh tissue. All study patients provided written informedconsent before tissue collection. The study was approvedby the institutional ethics committee. Ten fresh frozennormal prostatic tissues and 50 prostate cancer specimenswere obtained from the biobanks of the Fundaci�on Insti-tuto Valenciano de Oncologı́a, Hospital Clı́nico Uni-versitario de Valencia and Hospital Universitario Centralde Asturias (table 1).
FFPE tissue. FFPE blocks corresponding to 273 patientswith prostate cancer were retrieved from the archivesof the Fundaci�on Instituto Valenciano de Oncologı́a bio-bank according to certain criteria, including specimensobtained at radical retropubic prostatectomy from 1996and 2002 and no previous treatment for prostate cancer,including androgen deprivation therapy or chemotherapypreoperatively. Table 1 lists patient characteristics.Gleason score was uniformly evaluated by the samepathologist (AC). Ten FFPE samples of normal prostatetissue from patients undergoing radical cystectomy wereanalyzed as controls. TMPRSS2-ERG gene fusion statuswas determined as previously described.10 Followup inthe retrospective series was 92 months (range 2 to 189).Radiological tests such as computerized tomography orbone scan were done when clinically indicated accordingto EAU (European Association of Urology) guidelines.During followup 122 patients (45%) had biochemicalprogression and 74 (27%) had clinical progression.
Urine SamplesTotal urine samples were obtained after DRE in anindependent cohort of 92 men who underwent PCA3
82_proof � 20 March 2014 � 9:06 pm � EO: JU-13-1929
½F1�½F1�
MIR-187 AND MIR-182 AS BIOMARKERS OF DIAGNOSIS AND PROGNOSIS IN PROSTATE CANCER 3
229230231232233234235236237238239240241242243244245246247248249250251252253254255256257258259260261262263264265266267268269270271272273274275276277278279280281282283284285
286287288289290291292293294295296297298299300301302303304305306307308309310311312313314315316317318319320321322323324325326327328329330331332333334335336337338339340341342
D
evaluation before needle biopsy. All biopsies were per-formed with a minimum of 12 cores (if initial biopsy)according to EAU guidelines. Total urine samples wereobtained from 92 patients after DRE and before needlebiopsy. We used 2 ml to analyze the PCA3 score with thePROGENSA� PCA3 Assay. The remaining urine wascentrifuged and the pellet was reconstituted in 350 mlTRIzol� reagent for RNA extraction.
RNA IsolationRNA was isolated using the mirVana� miRNA IsolationKit for fresh frozen urine samples and the RecoverAll�Total Nucleic Acid Isolation Kit for FFPE tissues accord-ing to manufacturer specifications.
miRNAMicroarrays. To identify differential miRNA expression innormal prostate vs prostate cancer we analyzed 60 freshfrozen prostate tissues using the GeneChip miRNA 2.0Array. For each sample 500 ng total RNA with an averageRIN (RNA integrity number) of 6.7 (range 3.1 to 9.1) wastagged with a PolyA tail and biotin using the FlashTag�Biotin HSR RNA Labeling Kit for GeneChip miRNAarrays. Microarray hybridization was performed at 48Cand 60 rpm for 16 hours using the GeneChip Hybridiza-tion, Wash and Stain Kit. Results were analyzed usingGeneChip Command Console� Software, version 3.0 andmiRNA QCTool software (Affymetrix�).
qRT-PCR for validation. Select miRNAs differentiallyexpressed in microarray studies were confirmed byqRT-PCR. Total RNA (100 ng) with a 260/280 nmabsorbance ratio of 1.5 to 2 was reverse transcribed usingthe TaqMan� miRNA Reverse Transcription Kit andmiRNA specific stem-loop primers (Applied Biosystems�)according to manufacturer instructions. Two ml of thiscDNA were amplified in triplicate by qRT-PCR in a finalvolume of 10 ml per reaction in a 7500 Fast Real-TimeThermocycler using miRNA assays (Applied Biosystems).RNU44 and RNU48 served as housekeeping genesfor miRNA expression normalization (supplementarytable 1, http://jurology.com/). The relative expression ofmiRNAs was determined with the mean value of controlsamples as the calibrator according to the 2eDDCt method.
Urine miR-182 and 187 Potential Diagnostic UseUrine samples with an RNA concentration of at least10 ng/ml and a 260/280 nm absorbance ratio of 1.3 to 2were selected for study. Reverse transcription was per-formed in parallel with the TaqMan miRNA ReverseTranscription Kit and High Capacity cDNA ReverseTranscription Kit (Applied Biosystems) to obtain cDNAfrom the miRNA and total RNA of each sample. BeforePCR we pre-amplified miR cDNA and cDNA usingTaqMan PreAmp Master Mix. qRT-PCR was doneusing specific miRNA and mRNA assays (supplementarytable 1, http://jurology.com/).
Statistical AnalysisMicroarray data were processed using bioinformaticstools (Partek� Genomics Suite�) such as array outliercontrol (normal unscaled SE), robust multi-array averagenormalization, principal components analysis andhierarchical clusters. We applied statistical corrections,
ochead: Investigative Urology FLA 5.2.0 DTD � JURO11082
including the p value and multiple variant correctiontests such as the Bonferroni and FDR tests set at 5%. Theassociation of miRNA-182 and 187 with clinicopatholog-ical parameters (categorical) was assessed using the chi-square test to determine homogeneity and the lineartrend for ordinal variables (p <0.05). The impact of bio-logical factors on BPFS and clinical PFS was determinedby the Kaplan-Meier proportional risk log rank test.Biochemical progression was defined as PSA 0.4 ng/mlor greater during followup. Clinical progression wasdefined as local (prostatic fossa), regional (lymph nodes)or distant (metastasis) progression. Univariate predictorsof PFS were entered into a Cox proportional hazardsmodel using stepwise selection to identify independentpredictors of outcome, considering the 95% CI. The pre-dictive ability of various markers to detect prostate can-cer in urine samples was assessed in adjusted univariatelogistic regression models. All variables significant atp <0.1 on univariate analysis were entered into amultivariate logistic regression model and assessed usingthe Hosmer-Lemeshow test. Discrimination was evalu-ated by calculating the ROC AUC. The capacity of theresulting model to predict the biopsy result wascompared with that of PSA using the chi-square testand the ROC AUC of each model was compared using theDeLong test. A cross-validation study of the same sub-jects was performed by comparing the observed diagnosison biopsy with that predicted by the full model. The2-sided test was used with p �0.05 considered statisti-cally significant. Statistical analysis was done withSPSS�, version 20.0 and Epidat 4.0 (Consellerı́a deSanidade, Servizo Galego de Sa�ude, Xunta de Galicia,Galicia, Spain).
RESULTS
miRNA
Expression profiling in prostate cancer vs normal
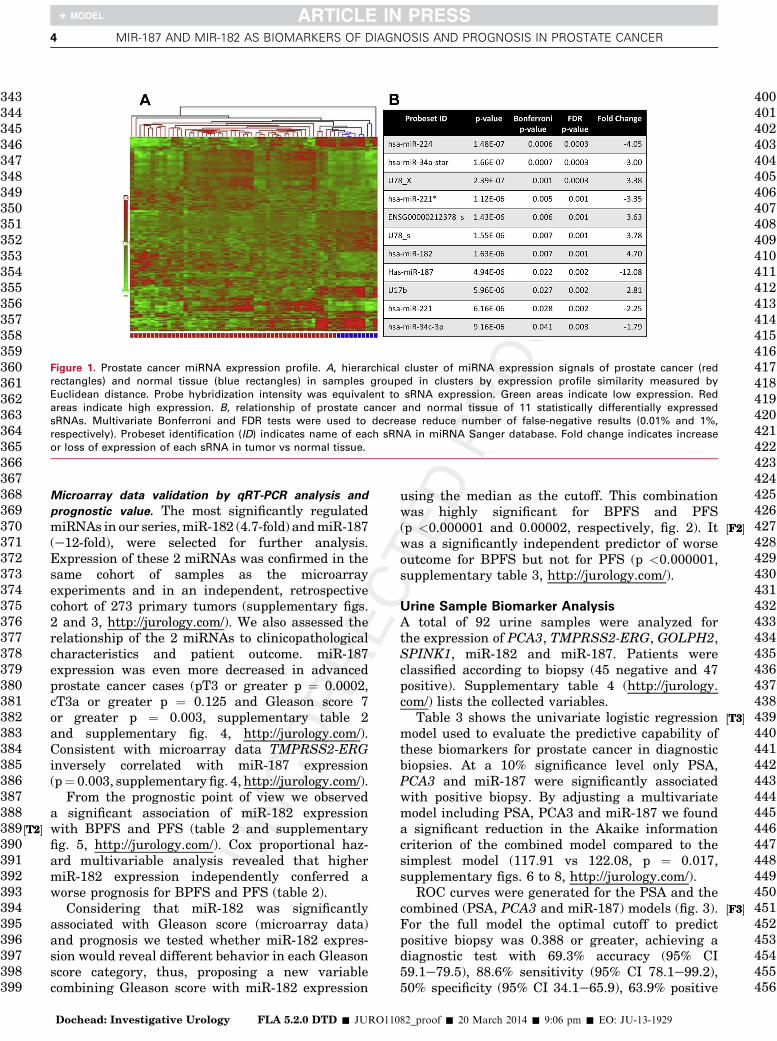
prostate. Normal and prostate cancer differentialmiRNA expression profiles were evaluated in freshfrozen samples andmiRNAmicroarrays (fig. 1,A), asshown in GEO (Gene Expression Omnibus) databaseAccession No. GSE45604 (http://www.ncbi.nlm.nih.gov/geo/). A total of 11 sRNAs were differentiallyexpressed (Bonferroni test p <0.05). Expressionwas increased in prostate cancer for 5 sRNAs,including U78_x (3.8-fold), SNORD78 (3.6-fold),U78_s (3.7-fold), miR-182 (4.7-fold) and U17b (2.7-fold). It was decreased in the remaining 6 sRNAs,including miR-224 (4.05-fold), miR-34a* (3-fold),miR-221* (3.3-fold), miR-187 (12-fold), miR-221(2.2-fold) and miR-34c-3p (1.7-fold) (fig. 1, B).
The supplementary results and supplementaryfig. 1 (http://jurology.com/) show the relationshipbetween miRNAs and clinicopathological variables.Notably, miR-182 and 187 were also differentiallyexpressed according to Gleason score, pT andTMPRSS2-ERG (supplementary fig. 1, http://jurology.com/).
_proof � 20 March 2014 � 9:06 pm � EO: JU-13-1929
½T2�½T2�
½F2�½F2�
½T3�½T3�
½F3�½F3�
Figure 1. Prostate cancer miRNA expression profile. A, hierarchical cluster of miRNA expression signals of prostate cancer (red
rectangles) and normal tissue (blue rectangles) in samples grouped in clusters by expression profile similarity measured by
Euclidean distance. Probe hybridization intensity was equivalent to sRNA expression. Green areas indicate low expression. Red
areas indicate high expression. B, relationship of prostate cancer and normal tissue of 11 statistically differentially expressed
sRNAs. Multivariate Bonferroni and FDR tests were used to decrease reduce number of false-negative results (0.01% and 1%,
respectively). Probeset identification (ID) indicates name of each sRNA in miRNA Sanger database. Fold change indicates increase
or loss of expression of each sRNA in tumor vs normal tissue.
4 MIR-187 AND MIR-182 AS BIOMARKERS OF DIAGNOSIS AND PROGNOSIS IN PROSTATE CANCER
343344345346347348349350351352353354355356357358359360361362363364365366367368369370371372373374375376377378379380381382383384385386387388389390391392393394395396397398399
400401402403404405406407408409410411412413414415416417418419420421422423424425426427428429430431432433434435436437438439440441442443444445446447448449450451452453454455456
Microarray data validation by qRT-PCR analysis and
prognostic value. The most significantly regulatedmiRNAs in our series,miR-182 (4.7-fold) andmiR-187(e12-fold), were selected for further analysis.Expression of these 2 miRNAs was confirmed in thesame cohort of samples as the microarrayexperiments and in an independent, retrospectivecohort of 273 primary tumors (supplementary figs.2 and 3, http://jurology.com/). We also assessed therelationship of the 2 miRNAs to clinicopathologicalcharacteristics and patient outcome. miR-187expression was even more decreased in advancedprostate cancer cases (pT3 or greater p ¼ 0.0002,cT3a or greater p ¼ 0.125 and Gleason score 7or greater p ¼ 0.003, supplementary table 2and supplementary fig. 4, http://jurology.com/).Consistent with microarray data TMPRSS2-ERGinversely correlated with miR-187 expression(p¼ 0.003, supplementary fig. 4, http://jurology.com/).
From the prognostic point of view we observeda significant association of miR-182 expressionwith BPFS and PFS (table 2 and supplementaryfig. 5, http://jurology.com/). Cox proportional haz-ard multivariable analysis revealed that highermiR-182 expression independently conferred aworse prognosis for BPFS and PFS (table 2).
Considering that miR-182 was significantlyassociated with Gleason score (microarray data)and prognosis we tested whether miR-182 expres-sion would reveal different behavior in each Gleasonscore category, thus, proposing a new variablecombining Gleason score with miR-182 expression
Dochead: Investigative Urology FLA 5.2.0 DTD � JURO110
using the median as the cutoff. This combinationwas highly significant for BPFS and PFS(p <0.000001 and 0.00002, respectively, fig. 2). Itwas a significantly independent predictor of worseoutcome for BPFS but not for PFS (p <0.000001,supplementary table 3, http://jurology.com/).
Urine Sample Biomarker Analysis
A total of 92 urine samples were analyzed forthe expression of PCA3, TMPRSS2-ERG, GOLPH2,SPINK1, miR-182 and miR-187. Patients wereclassified according to biopsy (45 negative and 47positive). Supplementary table 4 (http://jurology.com/) lists the collected variables.
Table 3 shows the univariate logistic regressionmodel used to evaluate the predictive capability ofthese biomarkers for prostate cancer in diagnosticbiopsies. At a 10% significance level only PSA,PCA3 and miR-187 were significantly associatedwith positive biopsy. By adjusting a multivariatemodel including PSA, PCA3 and miR-187 we founda significant reduction in the Akaike informationcriterion of the combined model compared to thesimplest model (117.91 vs 122.08, p ¼ 0.017,supplementary figs. 6 to 8, http://jurology.com/).
ROC curves were generated for the PSA and thecombined (PSA, PCA3 and miR-187) models (fig. 3).For the full model the optimal cutoff to predictpositive biopsy was 0.388 or greater, achieving adiagnostic test with 69.3% accuracy (95% CI59.1e79.5), 88.6% sensitivity (95% CI 78.1e99.2),50% specificity (95% CI 34.1e65.9), 63.9% positive
82_proof � 20 March 2014 � 9:06 pm � EO: JU-13-1929
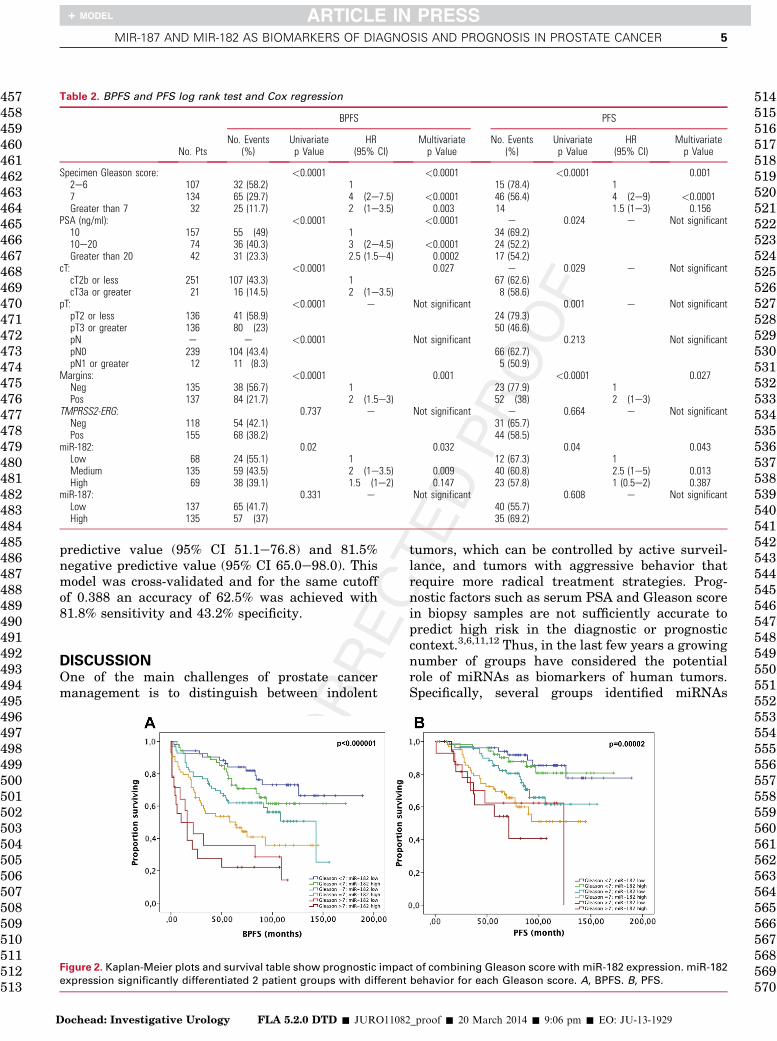
Table 2. BPFS and PFS log rank test and Cox regression
No. Pts
BPFS PFS
No. Events(%)
Univariatep Value
HR(95% CI)
Multivariatep Value
No. Events(%)
Univariatep Value
HR(95% CI)
Multivariatep Value
Specimen Gleason score: <0.0001 <0.0001 <0.0001 0.0012e6 107 32 (58.2) 1 15 (78.4) 17 134 65 (29.7) 4 (2e7.5) <0.0001 46 (56.4) 4 (2e9) <0.0001Greater than 7 32 25 (11.7) 2 (1e3.5) 0.003 14 1.5 (1e3) 0.156
PSA (ng/ml): <0.0001 <0.0001 e 0.024 e Not significant10 157 55 (49) 1 34 (69.2)10e20 74 36 (40.3) 3 (2e4.5) <0.0001 24 (52.2)Greater than 20 42 31 (23.3) 2.5 (1.5e4) 0.0002 17 (54.2)
cT: <0.0001 0.027 e 0.029 e Not significantcT2b or less 251 107 (43.3) 1 67 (62.6)cT3a or greater 21 16 (14.5) 2 (1e3.5) 8 (58.6)
pT: <0.0001 e Not significant 0.001 e Not significantpT2 or less 136 41 (58.9) 24 (79.3)pT3 or greater 136 80 (23) 50 (46.6)pN e e <0.0001 Not significant 0.213 Not significantpN0 239 104 (43.4) 66 (62.7)pN1 or greater 12 11 (8.3) 5 (50.9)
Margins: <0.0001 0.001 <0.0001 0.027Neg 135 38 (56.7) 1 23 (77.9) 1Pos 137 84 (21.7) 2 (1.5e3) 52 (38) 2 (1e3)
TMPRSS2-ERG: 0.737 e Not significant e 0.664 e Not significantNeg 118 54 (42.1) 31 (65.7)Pos 155 68 (38.2) 44 (58.5)
miR-182: 0.02 0.032 0.04 0.043Low 68 24 (55.1) 1 12 (67.3) 1Medium 135 59 (43.5) 2 (1e3.5) 0.009 40 (60.8) 2.5 (1e5) 0.013High 69 38 (39.1) 1.5 (1e2) 0.147 23 (57.8) 1 (0.5e2) 0.387
miR-187: 0.331 e Not significant 0.608 e Not significantLow 137 65 (41.7) 40 (55.7)High 135 57 (37) 35 (69.2)
MIR-187 AND MIR-182 AS BIOMARKERS OF DIAGNOSIS AND PROGNOSIS IN PROSTATE CANCER 5
457458459460461462463464465466467468469470471472473474475476477478479480481482483484485486487488489490491492493494495496497498499500501502503504505506507508509510511512513
514515516517518519520521522523524525526527528529530531532533534535536537538539540541542543544545546
D
predictive value (95% CI 51.1e76.8) and 81.5%negative predictive value (95% CI 65.0e98.0). Thismodel was cross-validated and for the same cutoffof 0.388 an accuracy of 62.5% was achieved with81.8% sensitivity and 43.2% specificity.
547548549550551
DISCUSSIONOne of the main challenges of prostate cancermanagement is to distinguish between indolent
Figure 2. Kaplan-Meier plots and survival table show prognostic impac
expression significantly differentiated 2 patient groups with different
ochead: Investigative Urology FLA 5.2.0 DTD � JURO11082
tumors, which can be controlled by active surveil-lance, and tumors with aggressive behavior thatrequire more radical treatment strategies. Prog-nostic factors such as serum PSA and Gleason scorein biopsy samples are not sufficiently accurate topredict high risk in the diagnostic or prognosticcontext.3,6,11,12 Thus, in the last few years a growingnumber of groups have considered the potentialrole of miRNAs as biomarkers of human tumors.Specifically, several groups identified miRNAs
t of combining Gleason score with miR-182 expression. miR-182
behavior for each Gleason score. A, BPFS. B, PFS.
552553554555556557558559560561562563564565566567568569570
_proof � 20 March 2014 � 9:06 pm � EO: JU-13-1929
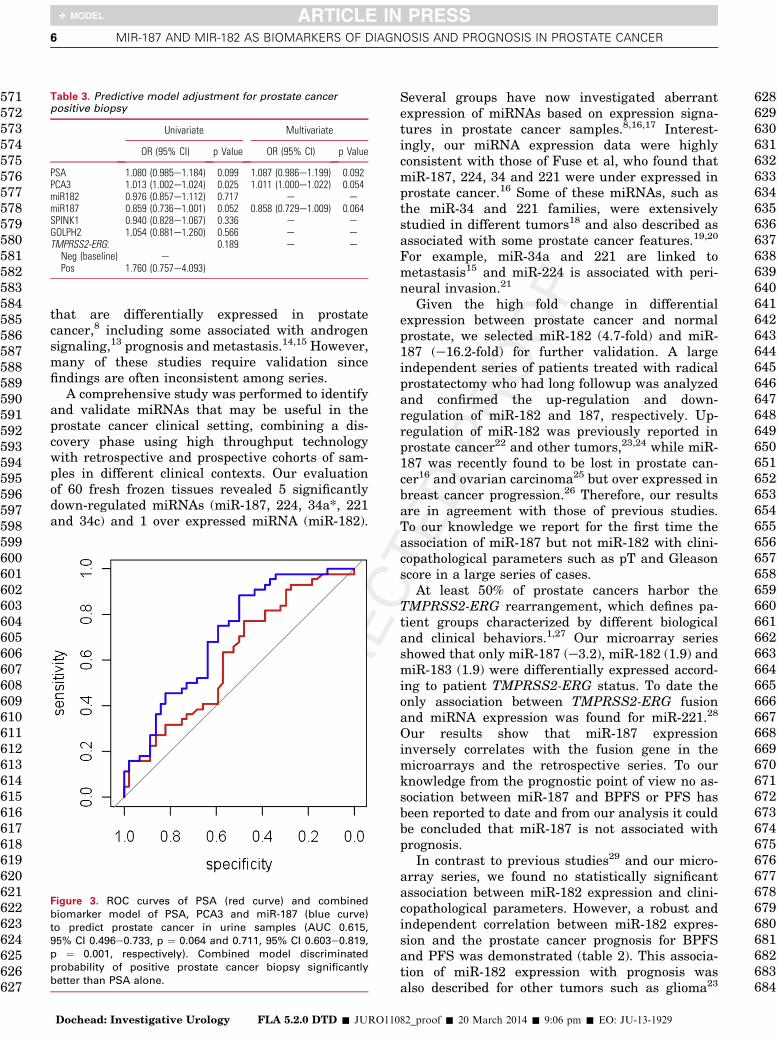
Table 3. Predictive model adjustment for prostate cancerpositive biopsy
Univariate Multivariate
OR (95% CI) p Value OR (95% CI) p Value
PSA 1.080 (0.985e1.184) 0.099 1.087 (0.986e1.199) 0.092PCA3 1.013 (1.002e1.024) 0.025 1.011 (1.000e1.022) 0.054miR182 0.976 (0.857e1.112) 0.717 e emiR187 0.859 (0.736e1.001) 0.052 0.858 (0.729e1.009) 0.064SPINK1 0.940 (0.828e1.067) 0.336 e eGOLPH2 1.054 (0.881e1.260) 0.566 e eTMPRSS2-ERG: 0.189 e e
Neg (baseline) ePos 1.760 (0.757e4.093)
6 MIR-187 AND MIR-182 AS BIOMARKERS OF DIAGNOSIS AND PROGNOSIS IN PROSTATE CANCER
571572573574575576577578579580581582583584585586587588589590591592593594595596597598599600601602603604605606607608609610611612613614615616617618619620621622623624625626627
628629630631632633634635636637638639640641642643644645646647648649650651652653654655
that are differentially expressed in prostatecancer,8 including some associated with androgensignaling,13 prognosis and metastasis.14,15 However,many of these studies require validation sincefindings are often inconsistent among series.
A comprehensive study was performed to identifyand validate miRNAs that may be useful in theprostate cancer clinical setting, combining a dis-covery phase using high throughput technologywith retrospective and prospective cohorts of sam-ples in different clinical contexts. Our evaluationof 60 fresh frozen tissues revealed 5 significantlydown-regulated miRNAs (miR-187, 224, 34a*, 221and 34c) and 1 over expressed miRNA (miR-182).
Figure 3. ROC curves of PSA (red curve) and combined
biomarker model of PSA, PCA3 and miR-187 (blue curve)
to predict prostate cancer in urine samples (AUC 0.615,
95% CI 0.496e0.733, p ¼ 0.064 and 0.711, 95% CI 0.603e0.819,p ¼ 0.001, respectively). Combined model discriminated
probability of positive prostate cancer biopsy significantly
better than PSA alone.
656657658659660661662663664665666667668669670671672673674675676677678679680681682683684
Dochead: Investigative Urology FLA 5.2.0 DTD � JURO110
Several groups have now investigated aberrantexpression of miRNAs based on expression signa-tures in prostate cancer samples.8,16,17 Interest-ingly, our miRNA expression data were highlyconsistent with those of Fuse et al, who found thatmiR-187, 224, 34 and 221 were under expressed inprostate cancer.16 Some of these miRNAs, such asthe miR-34 and 221 families, were extensivelystudied in different tumors18 and also described asassociated with some prostate cancer features.19,20
For example, miR-34a and 221 are linked tometastasis15 and miR-224 is associated with peri-neural invasion.21
Given the high fold change in differentialexpression between prostate cancer and normalprostate, we selected miR-182 (4.7-fold) and miR-187 (e16.2-fold) for further validation. A largeindependent series of patients treated with radicalprostatectomy who had long followup was analyzedand confirmed the up-regulation and down-regulation of miR-182 and 187, respectively. Up-regulation of miR-182 was previously reported inprostate cancer22 and other tumors,23,24 while miR-187 was recently found to be lost in prostate can-cer16 and ovarian carcinoma25 but over expressed inbreast cancer progression.26 Therefore, our resultsare in agreement with those of previous studies.To our knowledge we report for the first time theassociation of miR-187 but not miR-182 with clini-copathological parameters such as pT and Gleasonscore in a large series of cases.
At least 50% of prostate cancers harbor theTMPRSS2-ERG rearrangement, which defines pa-tient groups characterized by different biologicaland clinical behaviors.1,27 Our microarray seriesshowed that only miR-187 (e3.2), miR-182 (1.9) andmiR-183 (1.9) were differentially expressed accord-ing to patient TMPRSS2-ERG status. To date theonly association between TMPRSS2-ERG fusionand miRNA expression was found for miR-221.28
Our results show that miR-187 expressioninversely correlates with the fusion gene in themicroarrays and the retrospective series. To ourknowledge from the prognostic point of view no as-sociation between miR-187 and BPFS or PFS hasbeen reported to date and from our analysis it couldbe concluded that miR-187 is not associated withprognosis.
In contrast to previous studies29 and our micro-array series, we found no statistically significantassociation between miR-182 expression and clini-copathological parameters. However, a robust andindependent correlation between miR-182 expres-sion and the prostate cancer prognosis for BPFSand PFS was demonstrated (table 2). This associa-tion of miR-182 expression with prognosis wasalso described for other tumors such as glioma23
82_proof � 20 March 2014 � 9:06 pm � EO: JU-13-1929

MIR-187 AND MIR-182 AS BIOMARKERS OF DIAGNOSIS AND PROGNOSIS IN PROSTATE CANCER 7
685686687688689690691692693694695696697698699700701702703704705706707708709710711712713714715716717718719720721722723724725726727728729730731732733734735736737738739740741
742743744745746747748749750751752753754755756757758759760761762763764765766767
D
and colorectal cancer.24 Interestingly, our analysisshows agreement between our microarray data andthe direct association found by Tsuchiyama et albetween miR-182 and Gleason score29 as well asthe independent behavior of these variables onmultivariate analysis in our retrospective series.As a result, a combined variable between Gleasonscore and miR-182 levels was obtained thatperfectly discriminates different patient groups ac-cording to the risk of progression. In this respectpatients with Gleason score less than 7 and lowmiR-182 expression were at lowest risk for pro-gression compared to patients with Gleason scoregreater than 7 and miR-182 over expression (fig. 2).This classification could be used to better distin-guish patients who are suitable candidates foractive surveillance alone from those who need moreaggressive treatment.
Another clinical setting in which miRNA stabilitymay provide an advantage is cancer diagnosis inextracellular body fluids such as plasma, serum,saliva or urine.9 In prostate cancer the usefulness ofurine based testing for PCA3 expression (PCA3-PROGENSA� assay) was already documented in alarge series.7 Moreover, Laxman et al reported theusefulness of generating a multiplexed, urine based
ochead: Investigative Urology FLA 5.2.0 DTD � JURO11082
diagnostic test combining several biomarkers (PSA,PCA3, GOLPH2, SPINK1 and TMPRSS2-ERG)for prostate cancer.30 In our study and to reproducethe results of Laxman et al we also used a seriesof 92 urine samples from patients undergoing nee-dle biopsy, incorporating the analysis of miR-182and 187. As a result, we established a predictionmodel including serum PSA, urine PCA3 and miR-187 with significantly greater accuracy than PSAalone. This predictive model achieved 88.6% sensi-tivity and 50% specificity with 69.3% diagnosticprecision, suggesting that miR-187 could be apromising biomarker for early diagnosis of PCa. Inconclusion, our results provide preliminary evidenceof 2 miRNAs with a role in prostate cancer patho-genesis that have potential as biomarkers in thecontext of prognosis to identify patients at risk forprogression and in the diagnostic setting to improvethe predictive capability of existing biomarkers.
ACKNOWLEDGMENTSMarı́a Garcı́a Flores, Tania Mazcu~n�an Vitiello andPatricia Carretero Hinojosa provided technicalassistance. David Harrison assisted with manu-script editing.
768
769770771772REFERENCES
773774775776777778779780781782783784785786787788789790791792793794795796797798
1. Barbieri CE, Demichelis F and Rubin MA:Molecular genetics of prostate cancer: emergingappreciation of genetic complexity. Histopathol-ogy 2012; 60: 187.
2. Bunting PS: Screening for prostate cancer withprostate-specific antigen: beware the biases.Clin Chim Acta 2002; 315: 71.
3. Thompson IM, Ankerst DP, Chi C et al: Assessingprostate cancer risk: results from the ProstateCancer Prevention Trial. J Natl Cancer Inst 2006;98: 529.
4. Fleshner NE and Lawrentschuk N: Risk ofdeveloping prostate cancer in the future:overview of prognostic biomarkers. Urology2009; 73: S21.
5. Schroder FH, Hugosson J, Roobol MJ et al:Screening and prostate-cancer mortality in arandomized European study. N Engl J Med 2009;360: 1320.
6. Lucia MS, Darke AK, Goodman PJ et al: Patho-logic characteristics of cancers detected in theProstate Cancer Prevention Trial: implications forprostate cancer detection and chemoprevention.Cancer Prev Res (Phila) 2008; 1: 167.
7. Loeb S and Partin AW: Review of the literature:PCA3 for prostate cancer risk assessment andprognostication. Rev Urol 2011; 13: e191.
8. Casanova-Salas I, Rubio-Briones J, Fernandez-Serra A et al: miRNAs as biomarkers in pros-tate cancer. Clin Transl Oncol 2012; 14: 803.
9. Kuner R, Brase JC, Sultmann H et al: microRNAbiomarkers in body fluids of prostate cancerpatients. Methods 2013; 59: 132.
10. Fernandez-Serra A, Rubio L, Calatrava A et al:Molecular characterization and clinical impactof TMPRSS2-ERG rearrangement on prostatecancer: comparison between FISH and RT-PCR.Biomed Res Int 2013; 2013: 465179.
11. Draisma G, Etzioni R, Tsodikov A et al: Lead timeand overdiagnosis in prostate-specific antigenscreening: importance of methods and context.J Natl Cancer Inst 2009; 101: 374.
12. Etzioni R, Falcon S, Gann PH et al: Prostate-specific antigen and free prostate-specific anti-gen in the early detection of prostate cancer: docombination tests improve detection? CancerEpidemiol Biomarkers Prev 2004; 13: 1640.
13. Ribas J, Ni X, Haffner M et al: miR-21: anandrogen receptor-regulated microRNA thatpromotes hormone-dependent and hormone-independent prostate cancer growth. CancerRes 2009; 69: 7165.
14. Brase JC, Johannes M, Schlomm T et al:Circulating miRNAs are correlated with tumor
_proof � 20 March 201
progression in prostate cancer. Int J Cancer2011; 128: 608.
15. Watahiki A, Wang Y, Morris J et al: MicroRNAsassociated with metastatic prostate cancer. PLoSOne 2011; 6: e24950.
16. Fuse M, Kojima S, Enokida H et al: Tumor sup-pressive microRNAs (miR-222 and miR-31)regulate molecular pathways based on micro-RNA expression signature in prostate cancer.J Hum Genet 2012; 57: 691.
17. Szczyrba J, Loprich E, Wach S et al: The micro-RNA profile of prostate carcinoma obtained bydeep sequencing. Mol Cancer Res 2010; 8: 529.
18. He L, He X, Lowe SW et al: microRNAs join thep53 networkeanother piece in the tumour-suppression puzzle. Nat Rev Cancer 2007; 7: 819.
19. Rokhlin OW, Scheinker VS, Taghiyev AF et al:MicroRNA-34 mediates AR-dependent p53-induced apoptosis in prostate cancer. CancerBiol Ther 2008; 7: 1288.
20. Galardi S, Mercatelli N, Giorda E et al: miR-221and miR-222 expression affects the proliferationpotential of human prostate carcinoma cell linesby targeting p27Kip1. J Biol Chem 2007; 282:23716.
21. Prueitt RL, Yi M, Hudson RS et al: Expression ofmicroRNAs and protein-coding genes associated
4 � 9:06 pm � EO: JU-13-1929
8 MIR-187 AND MIR-182 AS BIOMARKERS OF DIAGNOSIS AND PROGNOSIS IN PROSTATE CANCER
799800801802803804805806807808809810811812813814815816817818819820821822823824825826827828829830831832833834835836837838839840841842843844845846847848849850851852853854855856857858859860
861862863864865866867868869870871872873874
with perineural invasion in prostate cancer.Prostate 2008; 68: 1152.
22. Schaefer A, Jung M, Mollenkopf HJ et al:Diagnostic and prognostic implications ofmicroRNA profiling in prostate carcinoma. IntJ Cancer 2010; 126: 1166.
23. Jiang L, Mao P, Song L et al: miR-182 as aprognostic marker for glioma progression andpatient survival. Am J Pathol 2010; 177: 29.
24. Liu H, Du L, Wen Z et al: Up-regulation ofmiR-182 expression in colorectal cancer tissuesand its prognostic value. Int J Colorectal Dis2013; 28: 697.
Dochead: Investigative Urology FLA
25. Chao A, Lin CY, Lee YS et al: Regulation ofovarian cancer progression by microRNA-187through targeting Disabled homolog-2. Onco-gene 2012; 31: 764.
26. Mulrane L, Madden SF, Brennan DJ et al:miR-187 is an independent prognostic factor inbreast cancer and confers increased invasivepotential in vitro. Clin Cancer Res 2012; 18:6702.
27. Rubio-Briones J, Fernandez-Serra A, Calatrava Aet al: Clinical implications of TMPRSS2-ERGgene fusion expression in patients with pros-tate cancer treated with radical prostatectomy.J Urol 2010; 183: 2054.
5.2.0 DTD � JURO11082_proof � 20 March 2
28. Gordanpour A, Stanimirovic A, Nam RK et al:miR-221 Is down-regulated in TMPRSS2:ERGfusion-positive prostate cancer. Anticancer Res2011; 31: 403.
29. Tsuchiyama K, Ito H, Taga M et al: Expressionof microRNAs associated with Gleason gradingsystem in prostate cancer: miR-182-5p is auseful marker for high grade prostate cancer.Prostate 2013; 73: 827.
30. Laxman B, Morris DS, Yu J et al: Afirst-generation multiplex biomarker analysis ofurine for the early detection of prostate cancer.Cancer Res 2008; 68: 645.
875
876877878879880881882883884885886887888889890891892893894895896897898899900901902903904905906907908909910911912913914915916917918919920921922014 � 9:06 pm � EO: JU-13-1929
Related Documents