International Commission on Radiation Units and Measurements (ICRU) Report 50, 62 and 83 SAMIR LAOUI, Ph.D.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

International Commission on Radiation Units and
Measurements
(ICRU) Report 50, 62 and 83
SAMIR LAOUI, Ph.D.
Principal objective of ICRU
Is to develop concepts, definitions and
recommendations for the use of quantities
and their units for ionizing radiation and its
interaction with matter, in particular with
respect to the biological effects induced by radiation

History of ICRU 50, 62 and 83
ICRU Report No: 29 (1978)
“Dose specification for reporting external beam therapy in photons and
electrons
ICRU Report – 50 (1993)
Supersedes and updates Report 29
Prescribing, Recording, and Reporting photon beam therapy
ICRU Report – 62 (1999)
Supplement to ICRU Report No: 50
ICRU Report – 83 (2010)
Prescribing, Recording, and Reporting Photon-beam IMRT


ICRU 50
When delivering a radiotherapy tretament,
parameters such as volume and dose have
to be specified for different purposes:
Prescription
Recording
Reporting
DESCRIBED VOLUMES
Gross target volume
Clinical target volume
Planning target volume
Organs at risk
Treated volume
Irradiated volume
Defined prior
to T/t planning
During T/t
planning

Recommendations for
reporting volumes
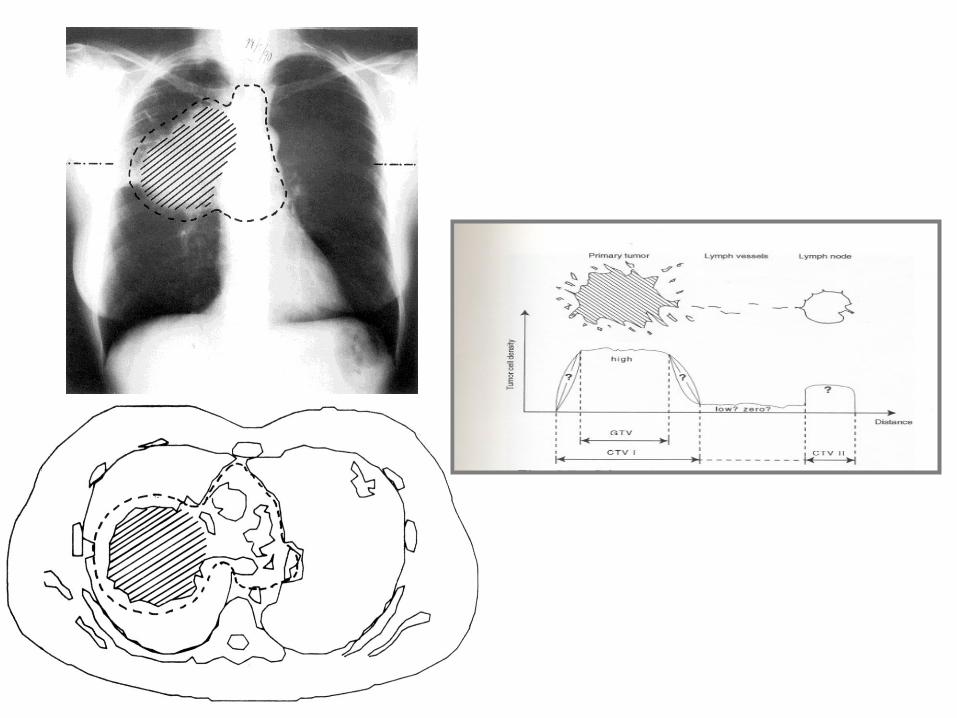
GROSS TUMOR VOLUME ( GTV )
Gross demonstrable extent and location of the
malignant growth
It consists of : Primary tumor(GTV primary)
Metastatic lymphadenopathy(GTV nodal)
Other metastasis(GTV M)
If the tumor has been removed prior to radiotherapy
then no GTV can be defined


The clinical Target Volume
CTV
The clinical Target Volume (CTV) is a tissue volume that
contains a demonstrable GTV and/or subclinical
microscopic malignant disease, which has to be
eliminated
2 types of Subclinical extension:-
Around the GTV-CTV I
At a distance (Regional lymph nodes)-CTV II
Planning Target Volume (PTV)
The PTV is a geometrical concept, and it is defined to
select appropriate beam sizes and beam arrangements,
taking into consideration the net effect of all the possible
geometrical variations and inaccuracies in order to ensure
that the prescribed dose is actually delivered to the CTV
Affected by:
Size and shape of the GTV & CTV
Effects of internal motions of organs and the tumor
Treatment technique (beam orientation and patient fixation, daily
setup errors)
Intrafractional errors (During a single session)
Interfractional errors (From one session to another)


TREATED VOLUME
It is the volume enclosed by an isodose surface that is
selected and specified by the radiation oncologist as
being appropriate to achieve the purpose of treatment
(palliation or cure).
Usually taken as the volume enclosed by the 95%
isodose curve.
Ideally dose should be delivered only to the PTV but due
to limitations in the radiation treatment technique.
The shape and size of the Treated Volume relative to the
PTV is an important optimization parameter.
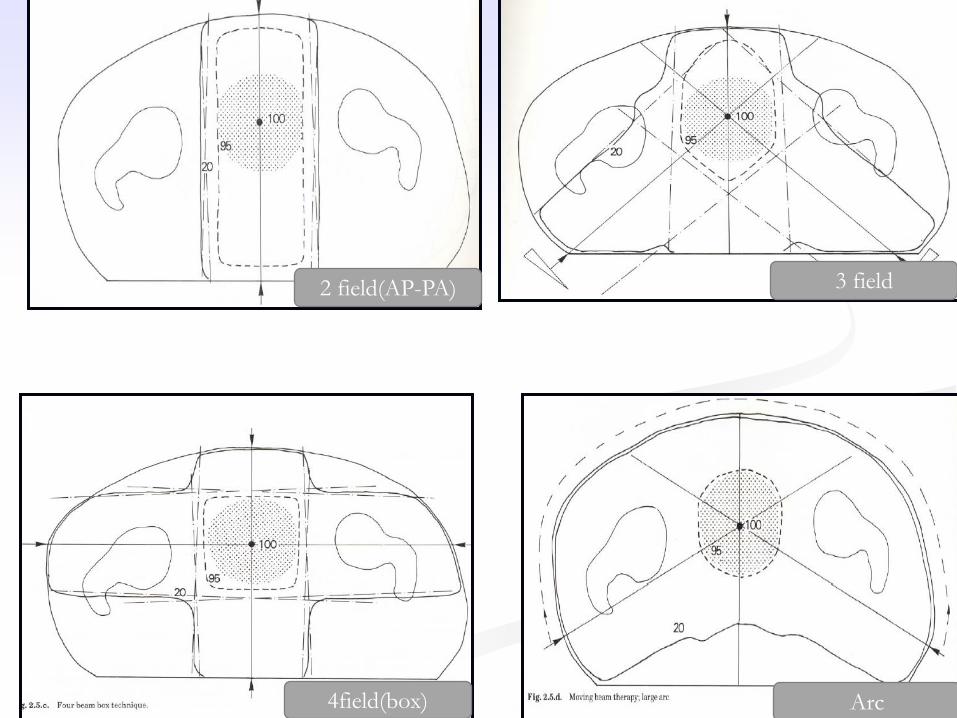
2 field(AP-PA) 3 field
4field(box) Arc
IRRADIATED VOLUME(IRV)
It is the volume that receives a dose considered
significant in relation to normal tissue tolerance
Usually taken as the volume enclosed by the 50%
isodose curve.
It depends on the treatment technique used

ICRU 50: Organs at risk (OR)
OR - Normal tissues whose radiation sensitivity may
significantly influence treatment planning and/or
prescribed dose
Class I – radiation lesions are fatal or result in severe
morbidity
Class II – radiation lesions result in moderate to mild
morbidity
Class III – radiation lesions are mild, transient, and
reversible, or result in no significant morbidity

ICRU 50: Dmax
One can identify the maximum dose within the PTV, and
the maximum dose at tissue outside the PTV
In most cases, high dose to a volume with smallest
diameter <15mm is not clinically meaningful in terms of
normal tissue tolerance
However, maximum dose assessment is important for
organs at risk with small dimension (<15mm) such as
optic nerve

ICRU 50: Dmin, Davg, Dmedian,
and Dmodal Minimum Dose: In contrast to the Dmax, no minimum
volume is recommended when reporting Dmin
Average Dose: is the average of the dose values in the
lattice points
Davg =
The median dose is the central value of the doses at all
lattice points
Modal Dose: is the dose that occurs most frequently at
the lattice points

ICRU 62: Supplement to ICRU
50

ICRU 62 scope
Gives more detailed recommendations on the different
margins that must be considered to account for
anatomical & geometrical variations & uncertainties.
PTV has been separated into two components: an
internal margin and set-up margin.
Classified organs at risk depending on response to
radiation.
Defined planning organ at risk volume (PRV)
Report dose to the OAR/PRV
Introduced conformity index
Gives recommendations on graphics

Volumes

A “Normal” Treatment plan
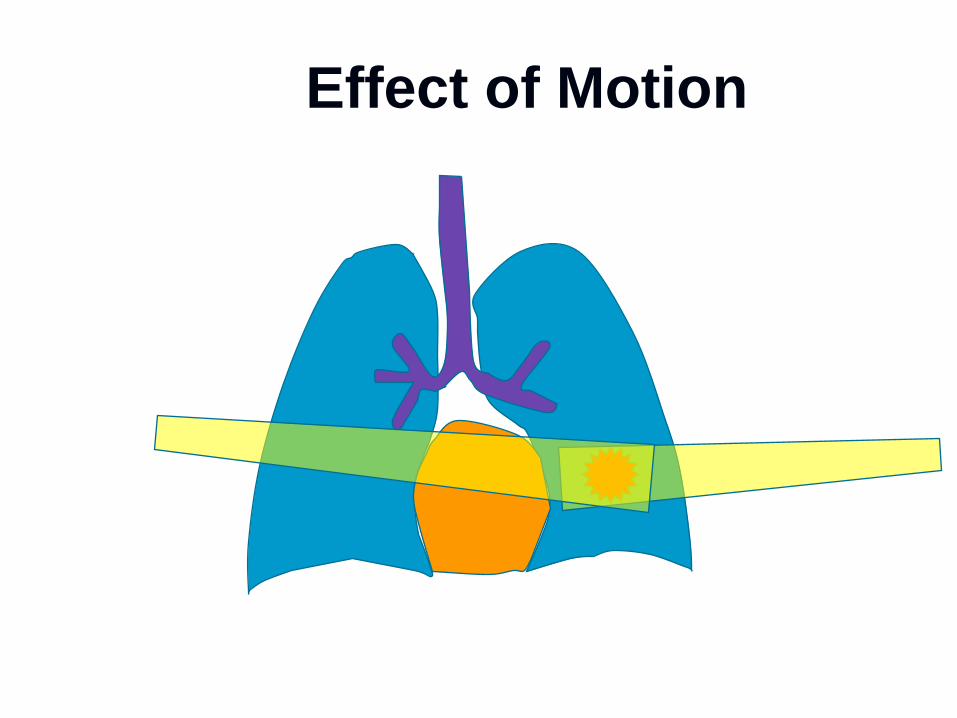
Effect of Motion


Internal Margin (IM)
Compensates for expected physiologic movements and
variations in size, shape , and position of the CTV in relation to
an Internal Reference Point
Commonly asymmetric
May result from respiration, different filling of rectum/bladder,
swallowing, heart beat
These variations cannot be easily controlled
Internal Target Volume (ITV) = CTV + IM
ICRU 62: IM and ITV
PTV = ITV + SM

SET-UP MARGIN ( SM )
Accounts for uncertainties, inaccuracies, and lack of
reproducibility in patient positioning and alignment of
the therapeutic beams during treatment planning and all
treatment sessions
Referenced to the external coordinate system
May result from patient positioning variation, mechanical
uncertainties of the equipment, dosimetric uncertainties,
transfer set-up errors, and human factors
Size of this margin might be reduced with record and
verify systems, patient immobilization devices, and
increased skill
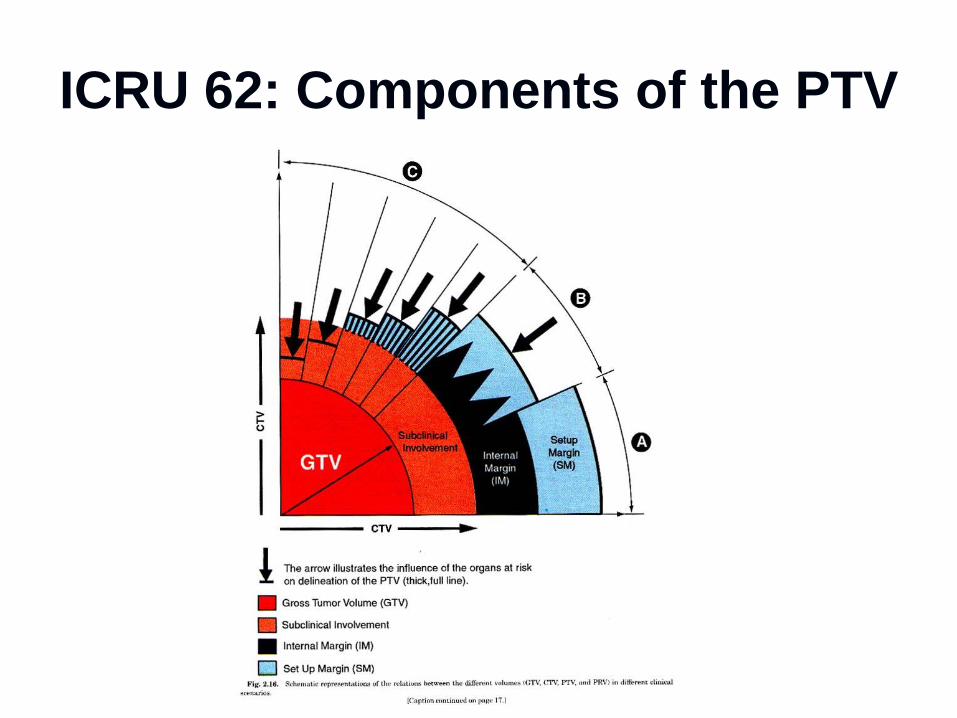
ICRU 62: Components of the PTV

ICRU 62: Treated Volume (TV)
Due to limitations of RT techniques, the volume receiving the prescribed dose does not generally match the PTV
TV - The tissue volume that (according to the approved treatment plan) is planned to receive at least a dose selected and specified by the radiation oncology team as being appropriate to achieve the purpose of treatment
AKA: The volume that receives at least 100% of the dose
ICRU 62: Conformity Index
(CI) Can be employed when the PTV is fully
enclosed by the TV, then it is the quotient
of the TV and the volume of the PTV
CI = TV/PTV
This is concept is used during the
optimization procedure

CLASSIFICATION OF
ORGANS AT RISK Classified as :
Serial – whole organ is a continuous unit and damage at one
point will cause complete damage of the organ (spinal cord,
digestive system). So even point dose is significant
Parallel – organ consists of several functional units and if one part
is damaged, the rest of the organ makes up for the loss (lung,
bladder). Dose delivered to a given volume or average/mean dose
is considered
Serial-parallel – kidney (glomerulus- parallel, tubules- serial),
heart (myocardium- parallel, coronary arteries- serial).

PLANNING ORGAN AT RISK
VOLUME(PRV) PRV to OAR is analogous to the PTV for the CTV.
Aim is to account for movements of the OAR due to
movements, changes in size and shape and setup
uncertainties.
PTV and PRV may overlap, then it is the responsibility of
the radiation oncologist to decide depending on the
importance of the treatment versus risk of critical organ
damage.

GRAPHICS
These are used to delineate the different volumes and the
other landmarks
These are in different colors for an easy and uniform
interpretation
The convention recommended and used in ICRU 62 are: GTV - Dark Red
CTV – Light Red
ITV – Dark Blue
PTV – Light Blue
OR – Dark Green
PRV – Light Green
Landmarks - Black
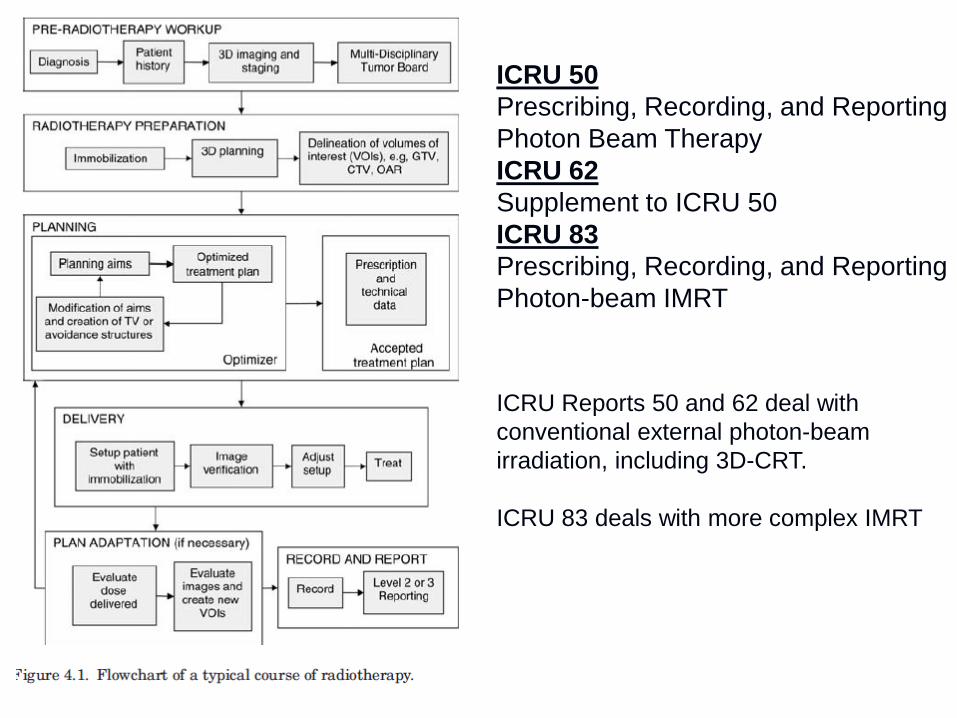
ICRU 50
Prescribing, Recording, and Reporting
Photon Beam Therapy
ICRU 62
Supplement to ICRU 50
ICRU 83
Prescribing, Recording, and Reporting
Photon-beam IMRT
ICRU Reports 50 and 62 deal with
conventional external photon-beam
irradiation, including 3D-CRT.
ICRU 83 deals with more complex IMRT

IMRT METHODS


Objective functions in IMRT
Based on soft tissue constraints using least-square
minimization
Tends to enforce absorbed-dose homogeneity within PTV
and reduce it in normal tissue
Where IPTV is the relative importance of the PTV.
TPTV is the number of voxels
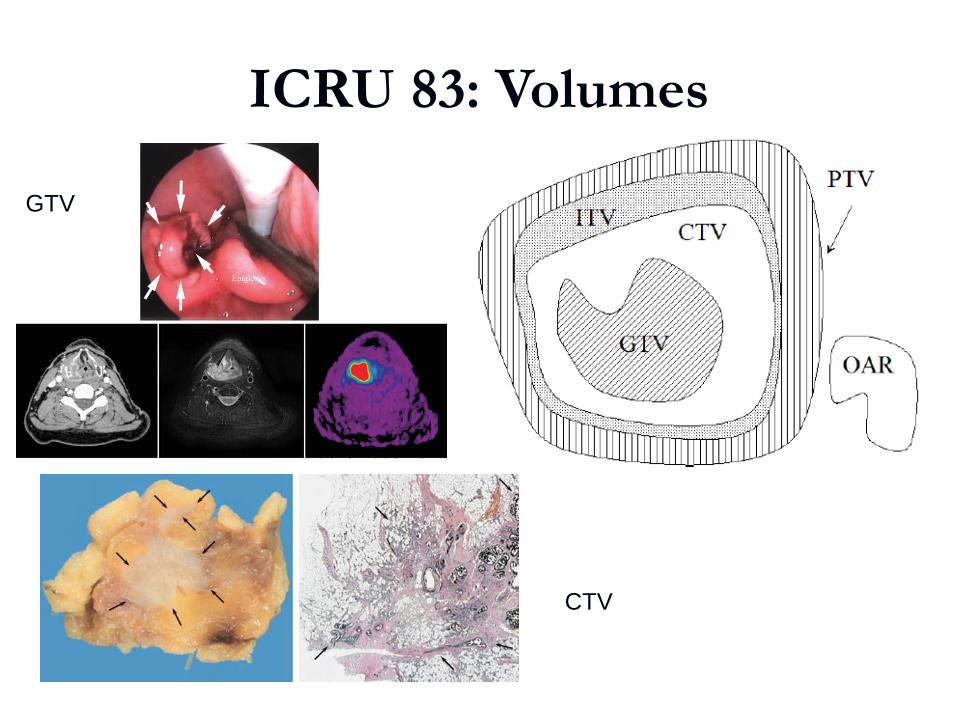
ICRU 83: Volumes
GTV
CTV

Dose Prescribing and
reporting for IMRT Absorbed-dose and volume information obtained from
DVHs
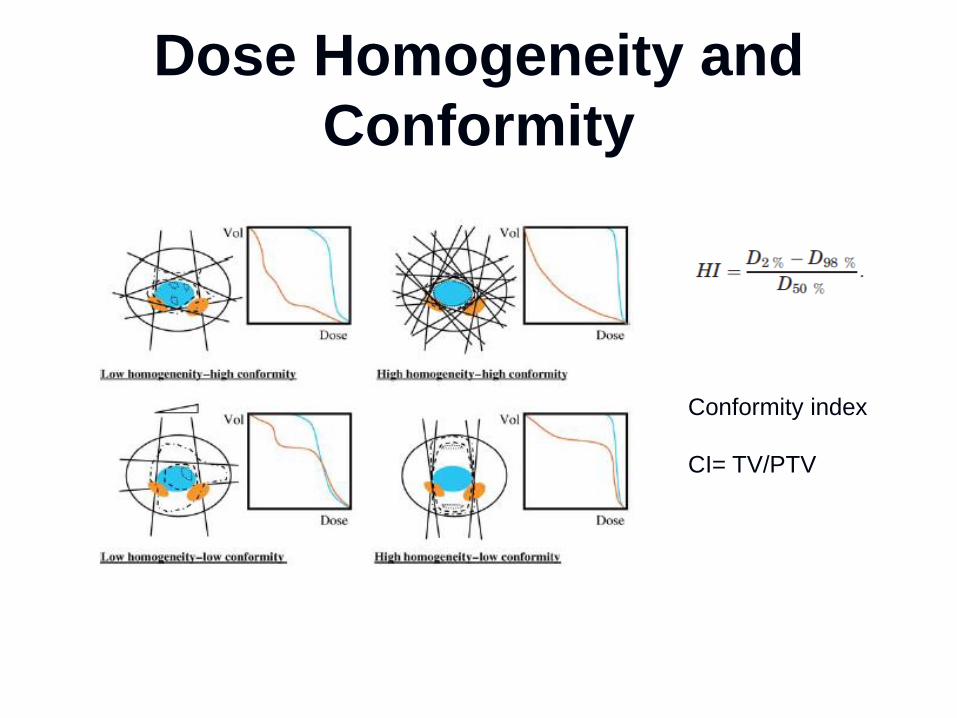
Dose Homogeneity and
Conformity
Conformity index
CI= TV/PTV

Sub structures for optimization
Priority rules when overlapping

ICRU 83 Update on Organs at
Risk Remaining Volume at Risk (RVR) = Imaged volume within
the patient excluding OAR and the CTVs
RVR aids in optimization
RVR Can be used to estimate late effect
Treatment planning
Volumes +Objectives
Optimization
Dose calculations
Correction-based
Model based
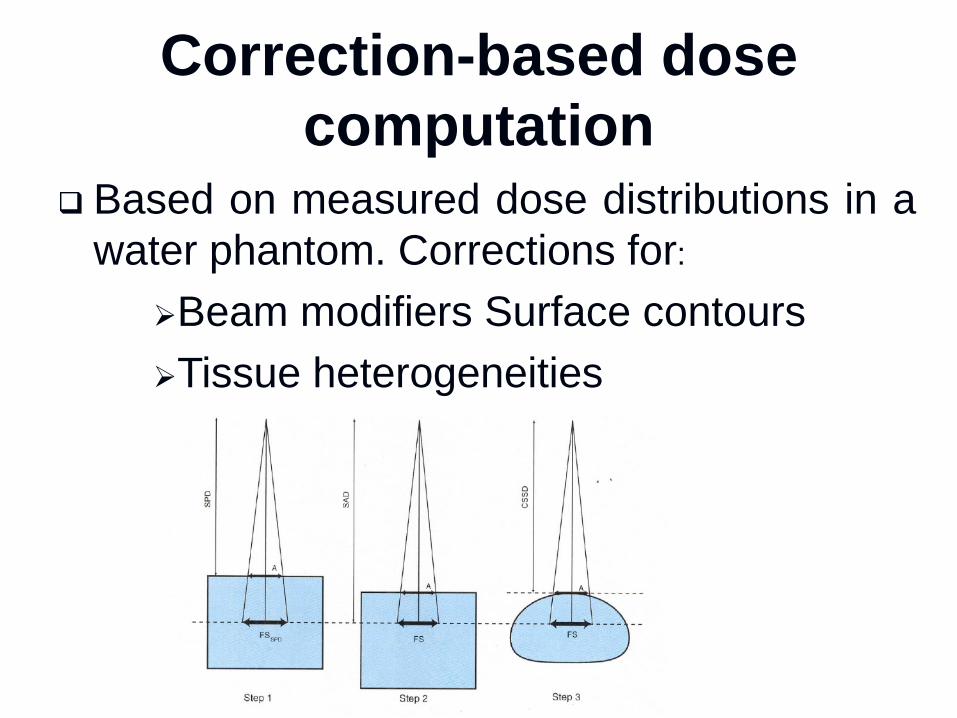
Correction-based dose
computation Based on measured dose distributions in a
water phantom. Corrections for:
Beam modifiers Surface contours
Tissue heterogeneities

Model based calculation
Compute patient dose considering the actual
physics interactions in the radiation transport
process.
Consider patient contour/homogeneity from
start, as opposed to correcting water dose
distribution
Model-based dose computations use monitor
unit calculations based on beam intensity (e.g.,
energy fluence) rather than dose in a phantom.
The beam has to be modeled
Summary of Changes Between ICRU
50 & 62 and IMRT ICRU (83)
More emphasis on statistics.
No longer use ICRU-Reference Point.
Want median dose D50 reported.
Use model-based dose calculations
Include the effect of tissue heterogeneities
Related Documents