Oslo University Hospital www.forensic-psychiatry.no HELSE SØR-ØST Clinical experiences with Version 2 and 3 of the HCR-20 in the SAFE pilot project Stål Bjørkly, Molde University College. Gunnar Eidhammer and Lars Erik Selmer, Clinic of Addiction and Psychiatry, Vestre Viken Trust. Johnny Wærp, Section for Medium Security, Gaustad, Oslo University Hospital. Alexander R. Flaata and Marthe Kjerstad, Section for Maximum Security, Dikemark, Oslo University Hospital. Centre for Forensic Psychiatry, Oslo University Hospital, Oslo, Norway

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
OsloUniversity Hospital
www.forensic-psychiatry.no HELSE SØR-ØST
Clinical experiences with Version 2 and 3 of the HCR-20 in the SAFE
pilot projectStål Bjørkly, Molde University College.
Gunnar Eidhammer and Lars Erik Selmer, Clinic of Addiction and Psychiatry, Vestre Viken Trust.
Johnny Wærp, Section for Medium Security, Gaustad, Oslo University Hospital.
Alexander R. Flaata and Marthe Kjerstad, Section for Maximum Security, Dikemark, Oslo University Hospital.
Centre for Forensic Psychiatry,Oslo University Hospital,
Oslo, Norway

OsloUniversity Hospital
HELSE SØR-ØST
Main research objectives
- Risk assessment - Risk management - Prospective follow-up- Naturalistic design

OsloUniversity Hospital
HELSE SØR-ØST
Setting and sample
One maximum security unit and three medium security units+ Forensic patient+ Major mental illness+ Serious violence towards others + Discharge within 6-12 months

OsloUniversity Hospital
HELSE SØR-ØSTwww.forensic-psychiatry.no
Sample characteristics (n= 22)
Mean age: 32 Gender: 19 male Relationship with partner: No:17 Highest education:Compulsory school (8/2
failed), High school (11/10), University (3/2) Employment/Income: Social support Ethnicity:17 native Caucasian Norwegians

OsloUniversity Hospital
HELSE SØR-ØSTwww.forensic-psychiatry.no
Sample characteristics cont.
Previous psychiatric treatment: 1 – 12 months: 7 1 – 2 years: 3 Over 2 years: 12
Primary diagnoses: Paranoid Schizophrenia 14 Hebephrenic Schizophrenia: 4 Personality disorders: 4

OsloUniversity Hospital
HELSE SØR-ØST
Repeat dynamic risk assessment
Hallucinations (PSYRATS-A) Delusions (PSYRATS-B) TCO (PERI) Hopelesness (The Hopelesness Scale) Dissociation (DES-II) Insight (SAI-E) Warning signs (SWAB, FESAI, ERM) Situational vulnerability (REFA)

OsloUniversity Hospital
HELSE SØR-ØSTwww.forensic-psychiatry.no
Focus in this presentation
• To compare HCR-20 version 2 and 3 • Clinical risk factors and risk
management
OsloUniversity Hospital
HELSE SØR-ØSTwww.forensic-psychiatry.no
Internal consistency and clinical utility
Gunnar Eidhammer, Lars Erik Selmer and Stål Bjørkly

OsloUniversity Hospital
HELSE SØR-ØSTwww.forensic-psychiatry.no
Participants and setting
Setting Raters Assessment of 20 forensic mental health patients All patients were male
OsloUniversity Hospital
HELSE SØR-ØSTwww.forensic-psychiatry.no
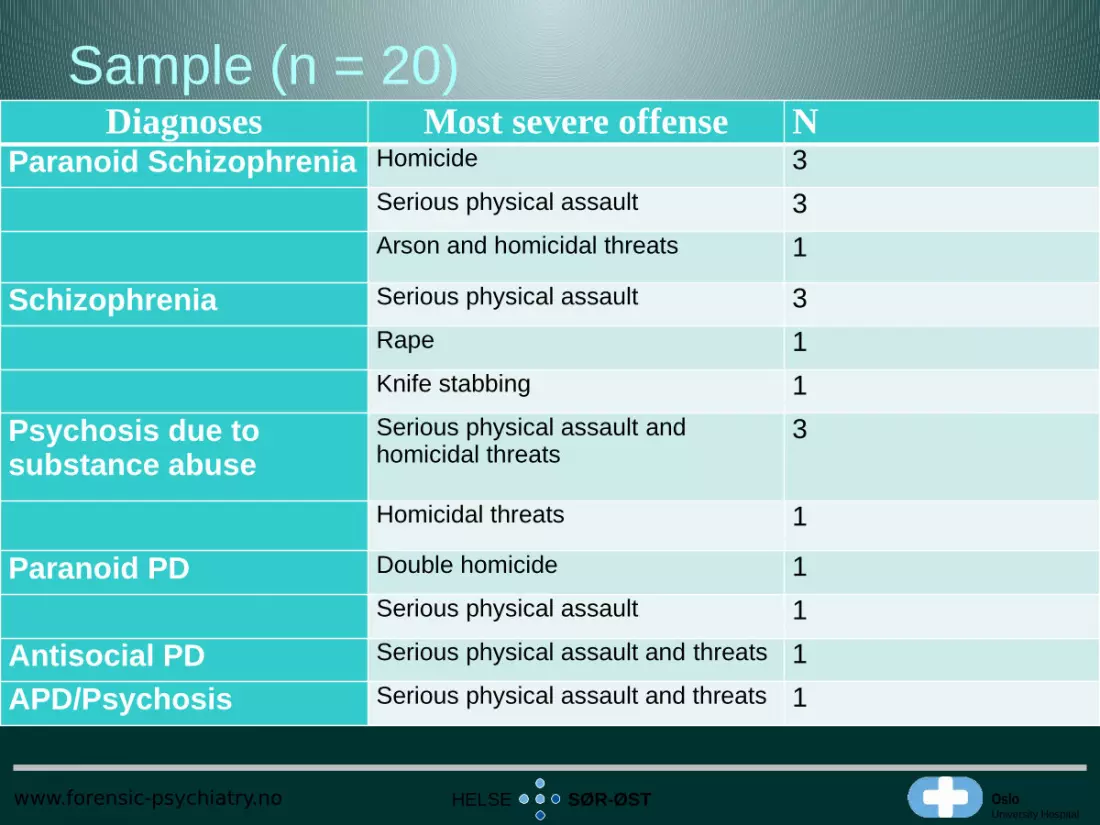
Sample (n = 20)Diagnoses Most severe offense N
Paranoid Schizophrenia Homicide 3Serious physical assault 3Arson and homicidal threats 1
Schizophrenia Serious physical assault 3Rape 1Knife stabbing 1
Psychosis due to substance abuse
Serious physical assault and homicidal threats
3
Homicidal threats 1
Paranoid PD Double homicide 1Serious physical assault 1
Antisocial PD Serious physical assault and threats 1
APD/Psychosis Serious physical assault and threats 1

OsloUniversity Hospital
HELSE SØR-ØSTwww.forensic-psychiatry.no
Internal consistency ICC: Two-way mixed effects model (rater effects random and measures
effects fixed) Cronbach's alpha (95%CI)
H-items .854 (.726 - .940)C-items .586 (.256 - .809)R-items .812 (.662 - .913)All items of HCR-20 and V3 .842 (.708 - .935)C-items: p < .001; Other items: p < .000
Significant differences for H-items (t=-2.797, df=19, p<.012) and C-items (t=-4.040, df,=19, p<.001), but not for R-items (t=.218, df=19, p<.830).
OsloUniversity Hospital
HELSE SØR-ØSTwww.forensic-psychiatry.no
Clinical utility: coding Change from 0, 1, 2, omit (V2) to y, p, n, o (V3)
makes the V3 more adapted to clinical practice. Mitigates the risk of importing an actuarial
approach into the use of the V3 Protects against misuse of numbers in decision
making processes The new structure reduces the risk of empirically
unfounded conclusions

OsloUniversity Hospital
HELSE SØR-ØSTwww.forensic-psychiatry.no
Clinical utility: Presence / Relevance
Presence: The principal common risk factors Evidence-/knowledge-based
Relevance: The principal individual risk factors Person-specific

OsloUniversity Hospital
HELSE SØR-ØSTwww.forensic-psychiatry.no
Clinical utility: Risk formulations
Risk formulations inform and enhance clinical practise through individualized risk management strategies
An example: Combining the Early Recognition Method (ERM) and R item analysis to develop risk management strategies
OsloUniversity Hospital
HELSE SØR-ØSTwww.forensic-psychiatry.no
Concluding remarks The 7-step structure 1. Gather and document basic case information 2. Identify presence 3. Assess relevance 4. Integrate information into case formulation 5. Identify risk scenarios 6. Recommend risk management strategies7. Risk judgment documentation
V3 = A more systematic, comprehensive and individualized violence risk analysis
“Risk analysis” = assessment + management

OsloUniversity Hospital
HELSE SØR-ØST
Changes in repeated HCR-20 measurement
Johnny Wærp
www.forensic-psychiatry.no

OsloUniversity Hospital
HELSE SØR-ØST
Clinical Comparison HCR-20 V2-V3
Clinical items V2 C1 Lack of insight C2 Negative attitudes C3 Active symptoms of
major mental disorder C4 Impulsivity C5 Unresponsive to
treatment
Clinical items V3 C1 Insight C2 Violent ideation or
intent C3 Symptoms of major
mental disorder C4 Instability C5 Treatment
supervision response
OsloUniversity Hospital
HELSE SØR-ØST
Rihanna
Diagnosis F 60.3 Emotionally unstable personality disorder (DSM:Borderline)
Single, 34 yrs History of:
sexual abuse psychiatric hospitalisations (last 10 years) violence towards others self harm and suicidal behaviour
OsloUniversity Hospital
HELSE SØR-ØST
Repeated Measurements HCR-20 V2
T1
Total: 24
C3: 1
T2
Total 23
C3:1
T3
Total 21
C3:0
OsloUniversity Hospital
HELSE SØR-ØST
Changes in repeated measurement
Psyrats A&B T1
Score 0
Score 0
Psyrats A&B T2
Score 0
Score 0
Psyrats A&B T3
Score 0
Score 0

OsloUniversity Hospital
HELSE SØR-ØST
Perceived threat and control override symptoms (TCO)
Monitored weekly for TCO- symptoms for 18 months. At T3 a risk management plan was formulated: -
focus on TCO- symptoms - associated with irregular menstruation.
Presence of TCO- symptoms: Risk factor and, Warning sign (SWAB) For vilolence toward self/others
Patient acknowledged this relationship Medication with birth pills.

OsloUniversity Hospital
HELSE SØR-ØST
Changes in repeated measurements of TCO
T1
TCO symptoms present
Other psychotic symptoms present
T2
TCO symptoms present in pattern
Other Psychotic symptoms present
in pattern
T3
TCO symptoms not present
Only 1 other symptom present

OsloUniversity Hospital
HELSE SØR-ØST
C3 Formulation in V2 vs. in V3
V2 FormulationC3 Active symptoms of major mental disorder
T1: 1, T2: 1, T3: 0 Psyrats A
No score (T1, T2, T3) Psyrats B
No score (T1, T2, T3 ) Peri - TCO
Scores present at T1 andT2, not present at T3. TCO weekly monitoring
still shows pattern related to irregular menstruation
V3 Formualtion C3 Active symptoms of major mental disorder Sub-item: Psychotic disorders Does not meet ICD- criteria for schizophrenia. Not present and not relevant,but Shows active TCO symptoms in relevant pattern recorded on SWAB and REFA (short term)Sub-item: Major mood disorders Meets criteria for major mood disorder in remission Not present, but relevant for long term riskSub-item: Intellect/executive/ social NP tests show some memory problems Present and moderately relevant
OsloUniversity Hospital
HELSE SØR-ØST
Conclusion
Sub-items structure judgement Presence and relevance help define
formulations Specification of time frame and priority of
case enhance structure of risk mangement procedure
Formulation becomes more specific and useful for next level of treatment

OsloUniversity Hospital
HELSE SØR-ØST
A single-case illustration from a high security ward
Alexander R. FlaataMarthe Kjerstad
www.forensic-psychiatry.no
OsloUniversity Hospital
HELSE SØR-ØST
Method
Two independent raters One patient: Justin, in his late twenties Raters completed HCR-20 (V2/V3) together
with hospital staff Outcome of violence risk assessment,
violence risk management plan, and clinical utility was discussed
OsloUniversity Hospital
HELSE SØR-ØST
Justin Alcohol abuse: 12 years old Drug abuse (cannabis, amphetamine and heroine) Age at first psychiatric admission: 21 19 hospitalisations F20.0 Paranoid Schizophrenia Transferred from medium to high security ward : 24
years old Numerous severe physical assaults against mental
health professionals
OsloUniversity Hospital
HELSE SØR-ØST
Dynamics of violence in high security ward. Paranoid delusions:
Controlled by the personnel (by a device in his brain) Own thoughts broadcasted Emotional distress: Psychotic anxiety
Somatic delusions: Body changes (penis and face) Emotional distress: Dysmorphophobic anxiety He felt to be in urgent need of medical examination Reality orientation: increased risk of violence.
Antisocial (instrumental) violence: Persistent demand of sedatives, violent movies, discharge… Verbal threats, and physical violence to get what he wanted.

OsloUniversity Hospital
HELSE SØR-ØST
Comparison of clinical utility
V2 Less support in the assessment process More broad and general risk management planning
V3 Clear structure for assessment procedure Requires more spesific inquiry into how risk factors
contribute to present risk of violence Method for identifying significant individual risk
factors

OsloUniversity Hospital
HELSE SØR-ØST
Clinical utility (II)
V3 Systematic approach to develop realistic scenarios Relevance scores enhance risk assessment accuracy
Assessment of Justin: Splitting factor: Items with low relevance This contributed to different outcomes: v2: moderat
v3: low to moderate,

OsloUniversity Hospital
HELSE SØR-ØST
Conclusion
Both versions have significant clinical utility in formulating violence risk and management
V3 provides a better structure of the assessment process
V3 is more comprehensive regarding the whole process of violence risk assessment
V3 is more time-consuming

OsloUniversity Hospital
www.forensic-psychiatry.no HELSE SØR-ØST
Contact information
Stål Bjø[email protected]
Centre for Forensic Psychiatry,Oslo University Hospital,
Oslo, Norway
Related Documents











