Hypothalamic–pituitary–adrenal axis and smoking and drinking onset among adolescents: the longitudinal cohort TRacking Adolescents’ Individual Lives Survey (TRAILS)Anja C. Huizink 1–3 , Kirstin Greaves-Lord 1 , Albertine J. Oldehinkel 1,2 , Johan Ormel 2 & Frank C. Verhulst 1 Department of Child and Adolescent Psychiatry, Erasmus Medical Center, Rotterdam, the Netherlands, 1 Department of Psychiatry and Graduate Schools for Behavioral and Cognitive Neurosciences, and for Health Research, University Medical Center Groningen and University of Groningen, the Netherlands 2 and Department of Education, Faculty of Behavioral and Social Sciences, University of Amsterdam, the Netherlands 3 ABSTRACT Aims We examined within a prospective longitudinal study whether cortisol levels were associated with smoking or drinking behaviours, taking parental substance use into account. Design The influence of parental substance use on cortisol levels of their adolescent offspring at age 10–12 years was examined. Next, cortisol levels of adolescents who initiated smoking or drinking at the first data collection (age 10–12) were compared to non-users. Finally, we examined whether cortisol levels could predict new onset and frequency of smoking and drinking 2 years later. Setting and participants First and second assessment data of the TRacking Adolescents’ Individual Lives Survey (TRAILS) were used, including 1768 Dutch adolescents aged 10–12 years, who were followed-up across a period of 2 years. Measurements Cortisol was measured in saliva samples at awakening, 30minutes later, and at 8 p.m. at age 10–12. Self-reported substance use at age 10–12 and 13–14, and parental self-reported substance use were used. Findings Only maternal substance use was related to slightly lower adolescent cortisol levels at 8 p.m. Both maternal and paternal substance use were associated with adolescent smoking and drinking at age 13–14, although fathers’ use only predicted the amount used and not the chance of ever use. Finally, higher cortisol levels were related moderately to current smoking and future frequency of smoking, but not to alcohol use. Conclusions In a general population, parental heavy substance use does not seem to affect cortisol levels consistently in their offspring. We found some evidence for higher, instead of lower, hypothalamic–pituitary–adrenal axis activity as a predictor of smoking in early adolescence. Keywords Adolescents, cortisol, drinking, drinking onset, HPA axis, smoking, smoking onset. Correspondence to: Anja C. Huizink, Erasmus Medical Center Rotterdam/Sophia Children’s Hospital, Department of Child and Adolescent Psychiatry, PO Box 2060, 3000 CB Rotterdam, the Netherlands. E-mail: [email protected] Submitted 28 January 2009; initial review completed 29 April 2009; final version accepted 10 May 2009 INTRODUCTION Tobacco use and alcohol use among adolescents is very common, with rates of 16-year-olds reaching almost 60% for ever having smoked a cigarette and about 33% having smoked in the last month, 80% having ever used alcohol in their life-time and 50% being drunk at least once in the last year, according to recent surveys throughout Europe (http://www.espad.org). Early-onset of use of these substances has been shown to be a risk factor for later progression to illicit drugs (e.g. [1,2]), and may lead to a range of adverse social and health problems [3–5]. Therefore, many studies have focused upon a variety of risk factors for early-onset of tobacco and alcohol use [6–10] Only a few studies have examined how one’s vulner- ability to stress may be related to the early use of these substances in adolescence. Nonetheless, several lines of research in adult populations suggest that individual variation in vulnerability to stress, assessed with basal RESEARCH REPORT doi:10.1111/j.1360-0443.2009.02685.x © 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 1927–1936

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hypothalamic–pituitary–adrenal axis and smoking anddrinking onset among adolescents: the longitudinalcohort TRacking Adolescents’ Individual Lives Survey(TRAILS)add_2685 1927..1936
Anja C. Huizink1–3, Kirstin Greaves-Lord1, Albertine J. Oldehinkel1,2, Johan Ormel2 &Frank C. Verhulst1
Department of Child and Adolescent Psychiatry, Erasmus Medical Center, Rotterdam, the Netherlands,1 Department of Psychiatry and Graduate Schools forBehavioral and Cognitive Neurosciences, and for Health Research, University Medical Center Groningen and University of Groningen, the Netherlands2 andDepartment of Education, Faculty of Behavioral and Social Sciences, University of Amsterdam, the Netherlands3
ABSTRACT
Aims We examined within a prospective longitudinal study whether cortisol levels were associated with smoking ordrinking behaviours, taking parental substance use into account. Design The influence of parental substance use oncortisol levels of their adolescent offspring at age 10–12 years was examined. Next, cortisol levels of adolescents whoinitiated smoking or drinking at the first data collection (age 10–12) were compared to non-users. Finally, we examinedwhether cortisol levels could predict new onset and frequency of smoking and drinking 2 years later. Setting andparticipants First and second assessment data of the TRacking Adolescents’ Individual Lives Survey (TRAILS) wereused, including 1768 Dutch adolescents aged 10–12 years, who were followed-up across a period of 2 years.Measurements Cortisol was measured in saliva samples at awakening, 30 minutes later, and at 8 p.m. at age10–12. Self-reported substance use at age 10–12 and 13–14, and parental self-reported substance use were used.Findings Only maternal substance use was related to slightly lower adolescent cortisol levels at 8 p.m. Both maternaland paternal substance use were associated with adolescent smoking and drinking at age 13–14, although fathers’ useonly predicted the amount used and not the chance of ever use. Finally, higher cortisol levels were related moderatelyto current smoking and future frequency of smoking, but not to alcohol use. Conclusions In a general population,parental heavy substance use does not seem to affect cortisol levels consistently in their offspring. We found someevidence for higher, instead of lower, hypothalamic–pituitary–adrenal axis activity as a predictor of smoking in earlyadolescence.
Keywords Adolescents, cortisol, drinking, drinking onset, HPA axis, smoking, smoking onset.
Correspondence to: Anja C. Huizink, Erasmus Medical Center Rotterdam/Sophia Children’s Hospital, Department of Child and Adolescent Psychiatry, POBox 2060, 3000 CB Rotterdam, the Netherlands. E-mail: [email protected] 28 January 2009; initial review completed 29 April 2009; final version accepted 10 May 2009
INTRODUCTION
Tobacco use and alcohol use among adolescents is verycommon, with rates of 16-year-olds reaching almost60% for ever having smoked a cigarette and about 33%having smoked in the last month, 80% having ever usedalcohol in their life-time and 50% being drunk at leastonce in the last year, according to recent surveysthroughout Europe (http://www.espad.org). Early-onsetof use of these substances has been shown to be a risk
factor for later progression to illicit drugs (e.g. [1,2]), andmay lead to a range of adverse social and health problems[3–5]. Therefore, many studies have focused upon avariety of risk factors for early-onset of tobacco andalcohol use [6–10]
Only a few studies have examined how one’s vulner-ability to stress may be related to the early use of thesesubstances in adolescence. Nonetheless, several lines ofresearch in adult populations suggest that individualvariation in vulnerability to stress, assessed with basal
RESEARCH REPORT doi:10.1111/j.1360-0443.2009.02685.x
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 1927–1936

functioning of stress systems or with stress reactivitymeasures, is related to substance (ab)use. First, regularintake of substances may affect hypothalamic–pituitary–adrenal (HPA) axis functioning, which represents animportant neuroendocrine system that responds to stress[11]. Numerous studies have shown that HPA axis func-tioning, often assessed by means of cortisol in saliva, isdysregulated in people who have developed a dependenceon alcohol, nicotine or illicit drugs [12]. For instance,adults dependent upon alcohol, nicotine and other drugsshow chronic activation of the HPA axis [13,14], and asimilar pattern is also found in periods of withdrawal[15,16]. Moreover, a blunted cortisol response to physicaland psychological stressors for at least 4 weeks postwith-drawal was found in abstinent alcoholics [12,17,18]. Ingeneral, variation in HPA axis response to stress may alsobe caused by comorbid depression or externalizing ten-dencies, such as novelty seeking [19] and low sociability[20]. However, the blunted responsivity found in theabstinent alcoholics was not caused by these factors, andmay therefore reflect an inhibited HPA axis reactivity dueto prolonged alcohol abuse.
Very similar findings were reported for nicotine-dependent adults. Nicotine is known to be a strong acti-vator of the HPA axis [21]. In regular smokers, smokingonly two cigarettes consistently activates the HPA axis,although the diurnal pattern of cortisol secretion ishardly affected. However, similar to regular alcohol use,smoking induces an attenuated responsiveness of theHPA axis to psychological stress [22,23]. Alternatively,several studies have shown that increased perceived levelsof stress and augmented stress reactivity are associatedwith more frequent or intense smoking and drinking[24,25]. These studies showing altered HPA reactivity insubstance use disorders raise the question of whether thedifferent reactivity is a consequence of addiction, or abiomarker of people at risk for addiction. Unfortunately,prospective longitudinal studies focusing upon this ques-tion are currently lacking in the literature.
A second line of research associating substance(ab)use with vulnerability to stress suggests that a geneticpropensity for alcohol and drug abuse may be accompa-nied by a reduced HPA response to stress. For instance,two studies of Moss et al. [26,27] showed that psychologi-cal stress responses were blunted in adolescent and youngadult males whose father had a history of alcoholism.Individuals with this familial lower responsiveness tostress may experiment more easily with nicotine oralcohol use, to experience an increase of HPA axis arousaleffects [28].
To gain further insight into how individual variationin HPA axis functioning is related to substance (ab)usefrom adolescence onwards, it is necessary to conduct aprospective longitudinal study in which HPA axis activity
is assessed prior to the onset of substance use. Using anequivalent design, we showed previously in a communitysample of adolescents that lower basal cortisol levels30 minutes after awakening at the average age of 11years were related to early onset of cannabis use, i.e.before the age of 13 [29]. Moreover, our findings showedthat cortisol levels at 8 p.m. at age 11 were higher foradolescents with early and later onset of cannabis use,compared to non-using adolescents. In a subsequentanalysis, in response to an editorial by Schumann [30],we tested whether specific forms of externalizing behav-iour, i.e. conduct disorder and oppositional defiant disor-der, interacted with cortisol levels to predict onset ofcannabis use. Our findings indicated that onset of can-nabis use before age 13 was predicted partly by low cor-tisol levels, whereas externalizing behaviour could notdiscriminate between the prediction of early versus lateronset of cannabis use [31].
In the current study, we further explored the rela-tionship between basal HPA axis functioning and sub-stance use by focusing specifically upon two othercommon forms of substance use in adolescence, andexcluding cannabis users: smoking and drinking.Because the HPA axis is an important system to examinein relation to familial risk for substance use, we firstinvestigated whether parental use predicted adolescentcortisol levels. We hypothesized that parental substanceuse is related to lower basal cortisol levels. Secondly, weinvestigated whether parental substance use predictedadolescent use at baseline (T1) and 2 years later (T2).Finally, we tested whether cortisol levels were associatedwith current smoking or drinking, and whether cortisollevels could predict smoking or drinking behaviours 2years later (T2), while accounting for parental sub-stance use.
METHODS
Participants
The TRacking Adolescents’ Individual Lives Survey(TRAILS) is a prospective cohort study of Dutch earlyadolescents aged 10–12 years, who were followed-upover a period of 2 years, and who will have severalfollow-up measurements in the future. Data collection atthe first and second assessment waves ran from March2001 to July 2002, and from September 2003 to May2004, respectively. The TRAILS target sample consisted ofyoung adolescents from five municipalities in the North ofthe Netherlands, including both urban and rural areas[25]. The average age at the first assessment was 11.1years and at the second assessment 13.6 years. Moredetails on the sample selection and procedure have beenpublished elsewhere [32,33].
1928 Anja C. Huizink et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 1927–1936

Of all subjects who were approached (n = 3145),6.7% were excluded because of the following reasons: (i)adolescent incapable of participating because of mentalretardation or a serious physical illness or handicap or (ii)Dutch-speaking parent or parent surrogate not available,and not feasible to administer a part of the measurementsin parent’s own language. Of the remaining target popu-lation of 2935 eligible young adolescents, 76.0% agreedto participate in the TRAILS study [n = 2230, mean age11.09 years, standard deviation (SD) = 55, with 50.8%girls]. Participants in TRAILS did not differ from adoles-cents who did not wish to participate in our study onseveral background characteristics, such as socio-demographic variables, the proportion of single-parentfamilies, mental health outcomes or teacher-ratedproblem behaviour [32].
During the first assessment wave, complete data onadolescent substance use were available for 2200 indi-viduals. Information on parental substance use wasavailable for 2040 mothers and 1732 fathers. Salivasamples were received for cortisol sampling from 1768children. Of these samples, 22 were excluded, due to useof corticosteroid-containing medication. Cortisol valuesthat were greater than 3 SD of the mean were alsoexcluded from the analysis in order to reduce the impactof outliers caused by, e.g. contamination with blood,while values less than 3 SD below the mean were kept.This yielded the following numbers for complete cortisoldata: cortisol at awakening (Cort 1): 1687; cortisol30 minutes after awakening (Cort 2): 1716; cortisol at 8p.m. (Cort 3): 1714; complete cortisol data for all assess-ments: 1643. At the second assessment, 94% of theadolescents (n = 2087) completed the questionnaire onsmoking, drinking and cannabis use. For the currentstudy, individuals who had ever smoked cannabis(n = 150) were excluded. Therefore, the current analyseswere based on cortisol data of n = 1561 for Cort 1,n = 1582 for Cort 2 and n = 1586 for Cort 3.
Measures
Adolescent smoking
Smoking tobacco by the participant was measured atthe first assessment (T1) by one self-reported item onhaving ever smoked in one’s life (yes/no). At the secondassessment (T2), adolescents were again asked aboutlife-time use (‘Did you ever smoke, even if you only triedone cigarette or one or two puffs?’) and about their usein the last month, and the amount of smoking each day:‘How many cigarettes did you smoke per week onaverage the last 4 weeks?’ and ‘How many cigarettes doyou smoke each day?’. Based on these two items, onecontinuous variable was computed: ‘number of ciga-rettes per week’.
Adolescent drinking
Drinking alcoholic beverages by the participant was mea-sured at T1 by one self-report item, focusing uponwhether the adolescent had ever drunk an alcoholic bev-erage in his/her life (yes/no). At T2, adolescents wereagain asked about life-time alcohol use and about thenumber of days and drinks the adolescents drank duringthe week, and at the weekends. Based on these scores, acombined continuous variable was computed: ‘number ofalcoholic beverages per week’.
Parental substance use
Parental substance use was assessed during a parentalinterview at T1, usually conducted with the mother. Thefollowing questions were used: ‘Did you smoke during thelast year, and if so, how much?’ and ‘Did you drinkalcohol during the last year, and if so, how much?’. Theanswer categories for smoking were: 1 = no, 2 = a fewtimes, less than one cigarette a day, 3 = yes, one to 10cigarettes a day, 4 = yes, 11–20 cigarettes a day, 5 = yes,one or two packs of cigarettes a day, and 6 = yes, morethan two packs of cigarettes a day. The answer categoriesfor drinking were: 1 = no, 2 = a few times, less than oneglass a week, 3 = yes, one to three glasses a week, 4 = fourto 10 glasses a week, 5 = 11–20 glasses a week and6 = yes, more than 20 glasses a week. The same questionswere repeated for the father. A participant was catego-rized as ‘low maternal risk (0)’ if the mother scored 2 orless on smoking and on drinking. A participant was cat-egorized as ‘moderate maternal risk (1)’ if the motherscored a 3 on smoking or a 3–4 on drinking and as ‘highmaternal risk (2)’ if the mother scored 4–6 on smokingand/or a 5–6 on drinking. A similar categorization wasmade for paternal risk.
Moreover, during the interview, information on life-time parental addiction was obtained. The mother couldindicate if she, and/or the father, had been addicted toalcohol, tranquillizers, cannabis or hard drugs. ‘Maternaladdiction’ or ‘paternal addiction’ would be scored as ‘yes’(1), respectively, if any addiction was reported.
Cortisol
Collection of salivary cortisol is a relatively stress-freeapproach that avoids confounding by stress responses[34]. For the present study we focused upon cortisol mea-sures representing a shortened version of a daytime cor-tisol profile, taken by means of Salivettes shortly afterawakening, while still lying in bed (Cort 1), 30 minutesafter awakening (Cort 2) and at 8 p.m. (Cort 3) to covervarious time-points during the circadian rhythm thathave been found to be relevant [35,36]. Because all par-ticipating schools started at approximately the same time,
HPA axis, smoking and drinking onset 1929
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 1927–1936

the sampling-time variation of the morning samplesamong the children is limited and the estimated corre-sponding times are 7 a.m. for the first sample (Cort 1) and7.30 a.m. for the second sample (Cort 2). The awakeningcortisol response is regarded as a useful index of adreno-cortical activity, is under genetic control and providesimportant information on the reactivity of the HPA axis[36], whereas the evening cortisol level is due mainly toenvironmental influences [37] and reflects a state ofrecovery. TRAILS participants collected their saliva athome, using the Salivette sampling device (Sarstedt,Nümbrecht, Germany), which was handed to the parent,accompanied by a verbal and a written instruction [38].Both the sampling and the preceding day should benormal (school) days, without special events or stressfulcircumstances. Saliva samples were stored by the partici-pants in their freezer directly after sampling and mailed tothe institute as soon as possible. The saliva samples werestored at -20°C until analysis [39]. A time-resolved fluo-rescence immunoassay was used in order to determinethe cortisol concentration in the saliva samples (detailsavailable upon request). All cortisol values were root-transformed to approximate a normal distribution.
Statistical analyses
First, we checked whether participants with incompletecortisol data (‘non-responders’) on our main variablesdiffered from those with complete data (‘responders’)with regard to sex, age, internalizing and externalizingproblems, smoking and drinking behaviour and parentalsubstance use by means of c2 and t-tests. Next, descrip-tives of cortisol levels and adolescent substance use werecomputed for boys and girls separately, and mean cortisollevels for each category of parental use. Secondly, linearregression analyses were performed to examine the asso-ciation between parental substance use and cortisollevels of their adolescent offspring. Thirdly, logisticregressions were performed to investigate whetherparental use predicted ever use of the adolescent at T1and T2, and linear regressions were performed to inves-tigate whether parental use predicted the amount of useby the adolescents at T2. In all analyses we controlled forage and gender. We further controlled for T1 substanceuse when T2 use was the outcome. Post-hoc analyses ofvariance (ANCOVAs) were performed to investigate spe-cific group differences further. Finally, with logisticregressions we investigated whether baseline cortisollevels predicted ever use at T1 and T2 and with linearregressions whether cortisol levels predicted the amountof use at T2, also controlling for sex, age, maternal riskand T1 use. The analyses were carried out in SPSSversion 15.0, and P < 0.05 (two-tailed) was used todetermine statistical significance.
RESULTS
Non-responders analysis
TRAILS participants with incomplete cortisol data, there-fore excluded from the current analyses and regarded asnon-responders, differed from those with complete dataon several characteristics: they were of a slightly olderaverage age [11.2 (SD 0.6) versus 11.1 (SD 0.6) years],and a slightly higher score on externalizing behaviour atT2 [0.28 (SD 0.25) versus 0.22 (SD 0.19)]. Moreover,they differed in several aspects of substance use at T2:ever tried smoking (48% in non-responders versus 29%in responders), mean number of drinks per week at T2(2.74 in non-responders versus 1.14 in responders),mean number of cigarettes per week at T2 (13.05 in non-responders versus 2.09 in responders) and maternalsmoking (38.1% smokers in non-responders versus31.1% in responders). No other significant differenceswere found.
Descriptive information on cortisol levels andadolescent substance use
Table 1 shows that at age 10–12 years a small number ofadolescents had ever smoked or drank alcohol, whereas 2years later the prevalence of ever use of tobacco andalcohol had increased to 30.5% and 71.5%, respectively.However, at age 12–14, the frequency of use of tobaccoand alcohol was still somewhat low, with only very few
Table 1 Mean cortisol levels (nmol/l) and adolescent smokingand drinking prevalence.
Cortisol measures (nmol/l)
Boys Girls
Mean SD Mean SD
Cort 1 11.13 4.69 11.83** 4.68Cort 2 14.79 6.32 16.07** 6.90CAR 3.66 6.63 4.11 7.34Cort 3 1.89 1.33 1.98 1.33
Adolescent substance use % nT1 (age 10–12)
Ever smoking 12.2 97 8.8* 74Ever drinking 33.4 265 21.7** 182
T2 (age 12–14)Ever smoking 27.3 217 30.4 255Ever drinking 65.5 520 68.9 578
Parental substance useHigh-risk father 27.8 221 26.3 221High-risk mother 23.2 184 23.8 200Addiction father 4.0 32 5.2 44Addiction mother 2.8 22 1.8 15
Cort 1: cortisol level directly after waking; Cort 2: cortisol level half anhour after waking; CAR: Cort 2—Cort 1; Cort 3: cortisol level at 8 p.m.*P < 0.05; **P < 0.005. SD: standard deviation.
1930 Anja C. Huizink et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 1927–1936
daily smokers and binge drinkers in our cohort. Conse-quently, the average number of cigarettes per week (2.09,SD = 9.67) and average number of alcoholic beveragesconsumed per week (1.14, SD = 3.13) at age 12–14 waslow.
Parental substance use and their adolescent offspringcortisol levels
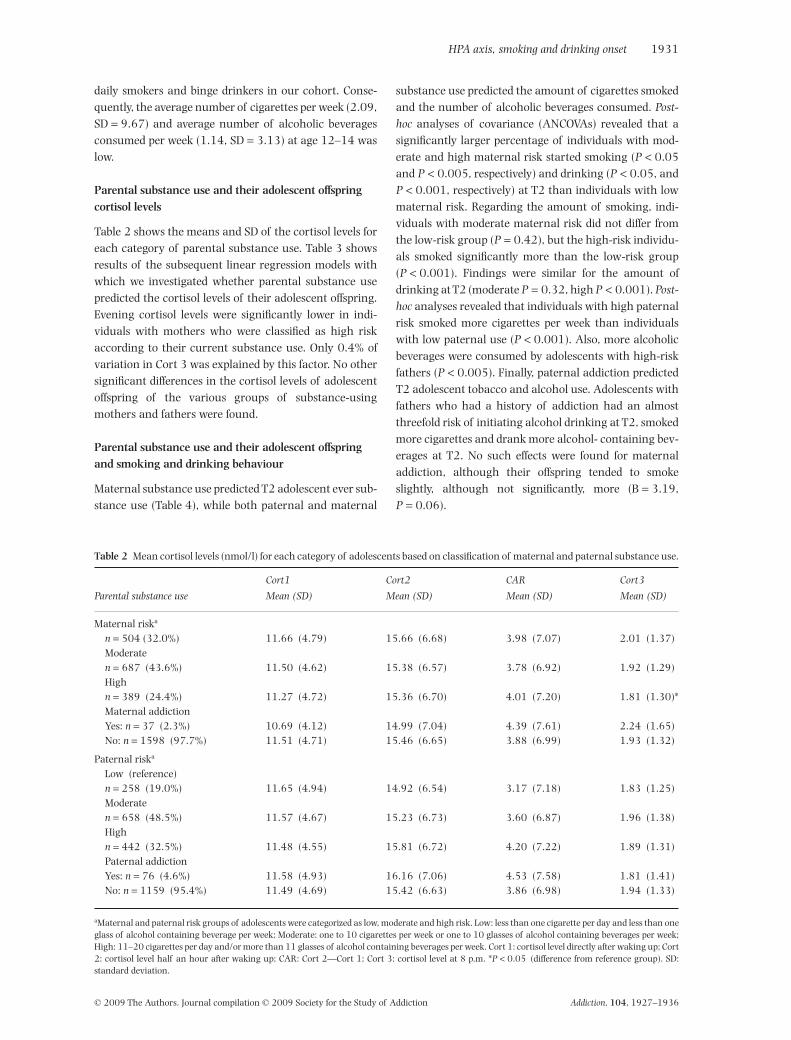
Table 2 shows the means and SD of the cortisol levels foreach category of parental substance use. Table 3 showsresults of the subsequent linear regression models withwhich we investigated whether parental substance usepredicted the cortisol levels of their adolescent offspring.Evening cortisol levels were significantly lower in indi-viduals with mothers who were classified as high riskaccording to their current substance use. Only 0.4% ofvariation in Cort 3 was explained by this factor. No othersignificant differences in the cortisol levels of adolescentoffspring of the various groups of substance-usingmothers and fathers were found.
Parental substance use and their adolescent offspringand smoking and drinking behaviour
Maternal substance use predicted T2 adolescent ever sub-stance use (Table 4), while both paternal and maternal
substance use predicted the amount of cigarettes smokedand the number of alcoholic beverages consumed. Post-hoc analyses of covariance (ANCOVAs) revealed that asignificantly larger percentage of individuals with mod-erate and high maternal risk started smoking (P < 0.05and P < 0.005, respectively) and drinking (P < 0.05, andP < 0.001, respectively) at T2 than individuals with lowmaternal risk. Regarding the amount of smoking, indi-viduals with moderate maternal risk did not differ fromthe low-risk group (P = 0.42), but the high-risk individu-als smoked significantly more than the low-risk group(P < 0.001). Findings were similar for the amount ofdrinking at T2 (moderate P = 0.32, high P < 0.001). Post-hoc analyses revealed that individuals with high paternalrisk smoked more cigarettes per week than individualswith low paternal use (P < 0.001). Also, more alcoholicbeverages were consumed by adolescents with high-riskfathers (P < 0.005). Finally, paternal addiction predictedT2 adolescent tobacco and alcohol use. Adolescents withfathers who had a history of addiction had an almostthreefold risk of initiating alcohol drinking at T2, smokedmore cigarettes and drank more alcohol- containing bev-erages at T2. No such effects were found for maternaladdiction, although their offspring tended to smokeslightly, although not significantly, more (B = 3.19,P = 0.06).
Table 2 Mean cortisol levels (nmol/l) for each category of adolescents based on classification of maternal and paternal substance use.
Parental substance use
Cort1 Cort2 CAR Cort3
Mean (SD) Mean (SD) Mean (SD) Mean (SD)
Maternal riska
n = 504 (32.0%) 11.66 (4.79) 15.66 (6.68) 3.98 (7.07) 2.01 (1.37)Moderaten = 687 (43.6%) 11.50 (4.62) 15.38 (6.57) 3.78 (6.92) 1.92 (1.29)Highn = 389 (24.4%) 11.27 (4.72) 15.36 (6.70) 4.01 (7.20) 1.81 (1.30)*Maternal addictionYes: n = 37 (2.3%) 10.69 (4.12) 14.99 (7.04) 4.39 (7.61) 2.24 (1.65)No: n = 1598 (97.7%) 11.51 (4.71) 15.46 (6.65) 3.88 (6.99) 1.93 (1.32)
Paternal riska
Low (reference)n = 258 (19.0%) 11.65 (4.94) 14.92 (6.54) 3.17 (7.18) 1.83 (1.25)Moderaten = 658 (48.5%) 11.57 (4.67) 15.23 (6.73) 3.60 (6.87) 1.96 (1.38)Highn = 442 (32.5%) 11.48 (4.55) 15.81 (6.72) 4.20 (7.22) 1.89 (1.31)Paternal addictionYes: n = 76 (4.6%) 11.58 (4.93) 16.16 (7.06) 4.53 (7.58) 1.81 (1.41)No: n = 1159 (95.4%) 11.49 (4.69) 15.42 (6.63) 3.86 (6.98) 1.94 (1.33)
aMaternal and paternal risk groups of adolescents were categorized as low, moderate and high risk. Low: less than one cigarette per day and less than oneglass of alcohol containing beverage per week; Moderate: one to 10 cigarettes per week or one to 10 glasses of alcohol containing beverages per week;High: 11–20 cigarettes per day and/or more than 11 glasses of alcohol containing beverages per week. Cort 1: cortisol level directly after waking up; Cort2: cortisol level half an hour after waking up; CAR: Cort 2—Cort 1; Cort 3: cortisol level at 8 p.m. *P < 0.05 (difference from reference group). SD:standard deviation.
HPA axis, smoking and drinking onset 1931
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 1927–1936

Table 3 Regression models of the relation between categorized parental substance and adolescent cortisol levels.
Cort 1 Cort 2 CAR Cort 3
Maternal riska
B (95% CI) -0.03 (-0.08to0.02) -0.02 (-0.08to0.04) 0.00 (-0.07to0.07) -0.04 (-0.07to-0.01)P-value 0.23 0.43 0.99 <0.05DR2 0.1% <0.01% <0.01% 0.4%
Paternal riska
B (95% CI) -0.01 (-0.06to0.05) 0.06 (-0.01to0.13) 0.07 (-0.01to0.14) 0.00 (-0.04to0.04)P-value 0.74 0.08 0.08 0.93DR2 <0.01% 0.2% 0.2% <0.01%
Maternal addictionb
B (95% CI) -0.11 (-0.34to0.12) -0.06 (-0.35to0.24) 0.05 (-0.27to0.38) 0.10 (-0.06to0.26)P-value 0.36 0.70 0.73 0.23DR2 0.01% <0.01% <0.01% 0.01%
Paternal addictionb
B (95% CI) -0.00 (-0.16to0.16) 0.07 (-0.13to0.28) 0.07 (-0.16to0.29) -0.05 (-0.16to0.06)P-value 0.98 0.48 0.57 0.40DR2 <0.01% <0.01% <0.01% <0.01%
aMaternal and paternal risk groups of adolescents were categorized as low, moderate and high risk. Low: less than one cigarette per day and lessthan one glass of alcohol containing beverage per week; Moderate: one to 10 cigarettes per week or one to 10 glasses of alcohol containingbeverages per week; High: 11–20 cigarettes per day and/or more than 11 glasses of alcohol containing beverage per week. bMaternal and paternaladdiction was based on their life-time history of addiction to any substance (yes) or no addiction (no), and therefore used as a binary variable. Cort 1:cortisol level directly after waking; Cort 2: cortisol level half an hour after waking; CAR: Cort 2—Cort 1; Cort 3: cortisol level at 8 p.m; CI: confidenceinterval.
Table 4 Regression models of the relation of categorized parental substance use with current and future adolescent substance use.
T1 (age 10–12) T2 (age 12–14)
Smokec Drinkc Smokec Drinkc # Cigarettesd # Drinksd
Maternal riska
ORc/Bd 1.20 1.05 1.28 1.36 1.35 0.4195% CI 0.96 to 1.49 0.90 to 1.22 1.09 to 1.50 1.16 to 1.60 0.69 to 2.01 0.20 to 0.63P-value 0.11 0.55 <0.005 <0.001 <0.001 <0.001
Paternal riska
ORc/Bd 1.12 1.10 1.09 1.15 0.79 0.2795% CI 0.87 to 1.45 0.92 to 1.31 0.90 to 0.31 0.97 to 1.38 0.10 to 1.48 0.09 to 0.46P-value 0.38 0.29 0.38 0.12 <0.05 <0.005
Maternal addictionb
ORc/Bd 1.86 1.21 1.13 1.34 3.19 0.3195% CI 0.80 to 4.33 0.60 to 2.43 0.52 to 2.48 0.56 to 3.19 -0.7 to 6.45 -0.76 to 1.37P-value 0.15 0.60 0.75 0.51 0.06 0.57
Paternal addictionb
ORc/Bd 1.17 0.79 1.32 2.88 3.12 1.0895% CI 0.57 to 2.40 0.45 to 1.38 0.77 to 2.25 1.40 to 5.91 0.83 to 5.41 0.32 to 1.82P-value 0.66 0.41 0.31 <0.005 <0.01 <0.005
aMaternal and paternal risk groups of adolescents were categorized as low, moderate, and high risk. Low: less than one cigarette per day and less thanone glass of alcohol containing beverage per week; Moderate: one to 10 cigarettes per week or one to 10 glasses of alcohol containing beverages perweek; High: 11–20 cigarettes per day and/or more than 11 glasses of alcohol containing beverage per week. bMaternal and paternal addiction was basedon their life-time history of addiction to any substance (yes) or no addiction (no), and was therefore used as a binary variable. cLogistic regressions wereperformed yielding odds ratios (OR). Smoke y/n: binary variable about ever smoking, yes or no. Drink y/n: binary variable about ever drinking alcohol,yes or no. dLinear regression analyses were performed yielding unstandardized beta (B) regression coefficients. #Cigarettes: number of cigarettes perweek, #Drinks: number of drinks per week. In all analyses we controlled for gender and age. When predicting T2 use, T1 use was added as a covariate.CI: confidence interval.
1932 Anja C. Huizink et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 1927–1936

Cortisol levels at T1 and current smoking and drinkingbehaviour
In all the analyses we controlled for gender, age andmaternal substance use. Table 5 shows that higher corti-sol levels directly after waking were related to a lower riskof ever smoking at T1 (second column). In contrast, CARand Cort 3 were related positively to ever smoking at T1.No significant associations were found between cortisolmeasures and alcohol onset by T1.
Cortisol levels at T1 and smoking and drinkingbehaviour 2 years later
We further examined whether Cort 1, Cort 2, CAR andCort 3 predicted smoking and drinking onset at T2 andthe frequency of tobacco and alcohol use (Table 5), con-trolling for gender, age, smoking and drinking at T1, andfor maternal substance use, as this latter variable wasrelated to the cortisol levels as well as to T2 use. Bothhigher levels of Cort 1 and Cort 2, representing the cor-tisol morning values, were related to smoking more ciga-rettes at T2. Effect sizes were small [40]. No such effectwas found on alcohol use.
DISCUSSION
In the current longitudinal study of a large communitysample of adolescents, our aim was twofold. First, we
studied how parental vulnerability, expressed as frequentsmoking or drinking by one of the parents, was related totheir offspring’s basal HPA axis functioning, and theirsubstance use at ages 10–12 and 13–14 years. With thisinformation in mind, we further examined how indi-vidual variation in HPA axis functioning at age 10–12was related to current smoking and drinking, andwhether cortisol levels could predict smoking or drinking2 years later.
With regard to our first aim, our findings showed onlya limited effect of parental substance use on cortisol mea-sures of adolescents at age 10–12. Although one signifi-cant association was found between maternal heavysmoking or drinking and her adolescent offspring cortisolmeasures, this was in a positive direction, yielding higherrather than lower levels of evening cortisol. This could, ofcourse, reflect a chance finding, because we ran multipletests and no consistent pattern of associations betweenparental substance use and other cortisol measures wasfound. It could also signify that maternal heavy sub-stance use provides a less optimal environment to theadolescent, as it has been shown that children from lowsocio-economic status and children whose mother havedepressive symptoms have higher salivary cortisol levelsin the morning [41].
Our study is the first to test these associations in apopulation-based large cohort of adolescents. Previousstudies of Moss et al. [24,25] showed a mainly blunted
Table 5 Regression models concerning the relation of cortisol levels with current and future substance use.
T1 (age 10–12) T2 (age 12–14)
Smokea Drinka Smokea Drinka # Cigarettesb # Drinksb
Cort 1ORa/Bb 0.75 1.01 1.06 1.13 0.73 0.0995% CI 0.59 to 0.96 0.85 to 1.19 0.89 to 1.26 0.95 to -1.34 0.01 to 1.45 -0.15 to 0.32P-value <0.05 0.93 0.51 0.18 <0.05 0.48
Cort 2ORa/Bb 1.01 1.09 1.08 1.04 0.58 0.0995% CI 0.84 to 1.21 0.96 to 1.24 0.94 to 1.23 0.90 to 1.19 0.02 to 1.15 -0.10 to 0.28P-value 0.94 0.19 0.30 0.61 <0.05 0.34
CARORa/Bb 1.20 1.08 1.06 0.97 0.14 0.0595% CI 1.00 to 1.44 0.95 to 1.22 0.94 to 1.21 0.86 to 1.10 -0.39 to -0.66 -0.13 to 0.22P-value <0.05 0.24 0.35 0.64 0.61 0.60
Cort 3ORa/Bb 1.63 1.07 1.04 1.25 0.44 0.0395% CI 1.15 to 2.30 0.84 to 1.37 0.81 to -1.35 0.97 to 1.61 -0.63 to 1.51 -0.32 to 0.38P-value <0.01 0.56 0.76 0.08 0.42 0.86
Cort 1: cortisol level directly after waking up; Cort 2: cortisol level half an hour after waking up; CAR: Cort 2—Cort 1; Cort 3: cortisol level at 8 p.m.aLogistic regressions were performed yielding odds ratios (OR). bLinear regression analyses were performed yielding unstandardized beta (B) regressioncoefficients). Smoke y/n: binary variable about ever smoking, yes or no. Drink y/n: binary variable about ever drinking alcohol, yes or no; #Cigarettes:number of cigarettes per week; #Drinks: number of drinks per week. In all analyses we controlled for maternal risk; when predicting T2 use, T1 use wasadded as a covariate. CI: confidence interval.
HPA axis, smoking and drinking onset 1933
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 1927–1936

response of the HPA axis in male adolescents whosefathers had a history of alcoholism, although basal cor-tisol levels were not reported. In these previous studies,an adverse family environment yielding chronic stress forthe adolescent may have explained part of the bluntedcortisol response to stress. In our population sample wehad only a small number of mothers (n = 37) and fathers(n = 76) who reported a history of addiction to any sub-stance. Their adolescent male and female offspringshowed no differences in basal HPA axis functioning. Wecan conclude from our findings within a population-based cohort that more moderate use of alcohol andtobacco by either of the parents did not seem to affectconsistently basal cortisol levels of their adolescent chil-dren. These findings indicate that a familial liability tosubstance use is not related to a clearly altered vulnerabil-ity to potential threats from the environment, expressedas consistently lower cortisol levels.
Next, we investigated whether parental use predictedadolescent use at baseline (T1) and 2 years later (T2). Notsurprisingly, we did find that parental substance use ispredictive of their adolescent offspring’s substance use,although maternal risk factors appear to be more impor-tant for onset of use than are paternal risk factors at age12–14. In general, twin studies have shown that onset ofadolescent substance use is influenced more strongly byenvironmental factors than by genetic factors [42].Perhaps at this age, mothers provide more environmentalcontext to adolescents [41] and have a stronger model-ling function for onset of use, particularly as they maysmoke or drink at home, while fathers may use sub-stances more often outside the home situation, forexample in a pub after work. Both maternal and paternalsubstance use was related to the amount of cigarettessmoked or alcoholic beverages consumed by their adoles-cent offspring at T2. This could indicate a familial liabilityto substance use, which is in line with findings of severaltwin studies showing that progression of substance use isaffected more strongly by genetic factors [42]. Some evi-dence for such familial liability can be deduced from ourfinding that particularly a paternal history of addictionyielded an almost threefold risk of alcohol use onset inboth male and female 12–14-year-olds. In contrast withour expectations, and with this line of reasoning,however, we did not find early-onset use of tobacco oralcohol, i.e. use reported at T1 (age 10–12) more fre-quently in adolescents whose mother or father reportedheavy use of alcohol or tobacco. Several researchers havesuggested that particularly early onset of smoking ordrinking reflects high risk-taking behaviour, which isexplained partly by genetic vulnerability[43–45]. In ourstudy, we found no evidence for transmission of familialrisk for risk-taking behaviour, represented by heavyparental use on one hand, and early-onset adolescent
substance use, i.e. use at T1, on the other hand. Perhapsfocusing upon particularly early onset of tobacco andalcohol use in parents as predictors of early onset of usein their adolescent offspring would yield a stronger rela-tionship. Unfortunately, we do not have this informationavailable for parents in our study.
Finally, we tested whether cortisol levels were associ-ated with current smoking or drinking, and whether cor-tisol levels reflecting basal HPA axis functioning couldpredict smoking or drinking 2 years later (T2), whiletaking account of maternal substance use. Several mea-sures of HPA axis functioning were found to be related tosmoking behaviour. In general, our findings showed thathigher levels of cortisol at T1 were associated positivelywith current (experimentation with) smoking, and withthe number of cigarettes smoked 2 years later. Thisfinding is in line with previous studies among adultpopulations, showing activation of the HPA axis afternicotine exposure [13,21]. The literature also shows thatthe number of life events among adolescents, as an indexof stress [24], or stress-induced increases in cortisol,were associated positively with an increase in smokingover a 6-month period in adults [25]. However, to ourknowledge, our study is the first to study this relation-ship between tobacco use and basal HPA axis activityprospectively. Because only a few of the adolescents inour sample were regular smokers at T2, we do not expectthat higher cortisol levels at T1 were caused by heavynicotine use. Rather, our findings suggest that HPA axisactivity is already higher in individuals who start tosmoke in adolescence, before the pharmacological effectsof nicotine on HPA axis activity have taken place. Noconsistent associations were found between cortisolmeasures and alcohol use at these ages. We reported ahigh rate of ever alcohol use at T2. This could partlyhave explained the lack of findings for at least thisoutcome, because it may, perhaps, be regarded as nor-mative behaviour rather than risk behaviour at this agein our sample.
These findings contrast our previous report on theassociation between early-onset cannabis use and similarindices of HPA axis functioning [27], in which we foundsome evidence for lower basal cortisol levels as a riskfactor for experimenting with cannabis use before the ageof 13. This could indicate that HPA axis functioning hasdifferential associations with the various types of sub-stances used, although more prospective research isclearly needed in order to examine this hypothesis inmore detail. An alternative explanation for the higherlevels of cortisol found in future smokers could be thatthese individuals were exposed to more environmentalstressors, such as peer pressure, which added to the risk ofsmoking initiation and caused part of the increase in HPAaxis activity we reported.
1934 Anja C. Huizink et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 1927–1936

The present study is not without limitations. First, weused a population-based cohort, which is representative,but the prevalence of heavy substance use in our youngadolescent sample was low, which may have influencedour results. Secondly, paternal substance use wasassessed mainly by maternal report, which could haveresulted in an underestimation of actual paternal sub-stance use. Thirdly, the high rate of ever alcohol use inour cohort, which may perhaps be regarded as normativebehaviour rather than risk behaviour, could haveexplained the lack of findings for this outcome. Fourthly,participants with incomplete cortisol data, thus excludedfrom our analyses, seem to be more of a high-risk group(including more substance use at T2), which could haveled to underestimation of the actual effect size of the asso-ciations. Further, we had no afternoon assessment of cor-tisol, which prevented us from calculating an area underthe curve measure that would have reflected the kineticsof cortisol secretion during the day. The cortisol responseto stress was not assessed in this study, which may be abetter indicator of risk-taking behaviour reflected bysmoking or drinking in adolescence. Finally, the 8 p.m.measure of cortisol may have been affected slightly bynicotine use in some of our adolescents, although we donot think that this influenced our findings.
In conclusion, the present study shows some evidencefor a relationship between higher basal levels of cortisoland smoking at age 12–14 years. In our population-based cohort, parental substance use does not seem toaffect their offspring’s HPA axis activity consistently,while maternal substance use, in particular, has an effecton adolescent smoking and drinking onset.
Declarations of interest
None.
Acknowledgements
This research is part of the TRacking Adolescents’ Indi-vidual Lives Survey (TRAILS). Participating centres ofTRAILS include various departments of the UniversityMedical Center and University of Groningen, the ErasmusUniversity Medical Center Rotterdam, the University ofUtrecht, the Radboud Medical Center Nijmegen and theTrimbos Institute, all in the Netherlands. Principal inves-tigators are Professor Dr J. Ormel (University MedicalCenter Groningen) and Professor Dr F. C. Verhulst(Erasmus University Medical Center). TRAILS has beensupported financially by various grants from the Nether-lands Organization for Scientific Research NWO (MedicalResearch Council programme grant GB-MW 940-38-011; ZonMW Brainpower grant 100-001-004; ZonMwRisk Behavior and Dependence grants 60-60600-98-018 and 60-60600-97-118; ZonMw Culture and Health
grant 261-98-710; Social Sciences Council medium-sized investment grants GB-MaGW 480-01-006 andGB-MaGW 480-07-001; Social Sciences Council projectgrants GB-MaGW 457-03-018, GB-MaGW 452-04-314,an GB-MaGW 452-06-004; NWO large-sized investmentgrant 175.010.2003.005); the Sophia Foundation forMedical Research (projects 301 and 393), the Dutch Min-istry of Justice (WODC) and the participating universities.We are grateful to all adolescents, their parents andteachers who participated in this research and to every-one who worked on this project and made it possible.Work for the current paper was funded partly by theEuropean Research Advisory Board (EA 0609: to K. G.-L.)and the NWO Vidi-Scheme, the Netherlands (452-06-004 to A. C. H.).
References
1. Kandel D. B., Yamaguchi K., Klein L. C. Testing theGateway hypothesis. Addiction 2006; 101: 470–2; discus-sion 4–6.
2. Rosmalen J. G., Oldehinkel A. J., Ormel J., de Winter A. F.,Buitelaar J. K., Verhulst F. C. Determinants of salivary cor-tisol levels in 10–12 year old children; a population-basedstudy of individual differences. Psychoneuroendocrinology2005; 30: 483–95.
3. World Health Organization. Neuroscience of PsychoactiveSubstance Use and Dependence. Geneva: World Health Orga-nization; 2004.
4. Kalant H. Adverse effects of cannabis on health: an updateof the literature since 1996. Prog NeuropsychopharmacolBiol Psychiatry 2004; 28: 849–63.
5. Moore T. H., Zammit S., Lingford-Hughes A., Barnes T. R.,Jones P. B., Burke M. et al. Cannabis use and risk of psychoticor affective mental health outcomes: a systematic review.Lancet 2007; 370: 319–28.
6. Buckner J. D., Schmidt N. B., Lang A. R., Small J. W.,Schlauch R. C., Lewinsohn P. M. Specificity of social anxietydisorder as a risk factor for alcohol and cannabis depen-dence. J Psychiatr Res 2008; 42: 230–9.
7. Huizink A. C., Ferdinand R. F., van der Ende J., Verhultst F. C.Symptoms of anxiety and depression in childhood and useof MDMA: prospective, population based study. BMJ 2006;332: 825–8.
8. Compton W. M., Conway K. P., Stinson F. S., Colliver J. D.,Grant B. F. Prevalence, correlates, and comorbidity ofDSM-IV antisocial personality syndromes and alcohol andspecific drug use disorders in the United States: results fromthe national epidemiologic survey on alcohol and relatedconditions. J Clin Psychiatry 2005; 66: 677–85.
9. Otten R., Engels R. C., van de Ven M. O., Bricker J. B. Parentalsmoking and adolescent smoking stages: the role of parents’current and former smoking, and family structure. J BehavMed 2007; 30: 143–54.
10. Vink J. M., Willemsen G., Engels R. C., Boomsma D. I.Smoking status of parents, siblings and friends: predictors ofregular smoking? Findings from a longitudinal twin-familystudy. Twin Res 2003; 6: 209–17.
11. Tsigos C., Chrousos G. P. Hypothalamic–pituitary–adrenalaxis, neuroendocrine factors and stress. J Psychosom Res2002; 53: 865–71.
HPA axis, smoking and drinking onset 1935
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 1927–1936

12. Lovallo W. R., Dickensheets S. L., Myers D. A., Thomas T. L.,Nixon S. J. Blunted stress cortisol response in abstinentalcoholic and polysubstance-abusing men. Alcohol Clin ExpRes 2000; 24: 651–8.
13. Steptoe A., Ussher M. Smoking, cortisol and nicotine. Int JPsychophysiol 2006; 59: 228–35.
14. Wand G. S., Dobs A. S. Alterations in the hypothalamic–pituitary–adrenal axis in actively drinking alcoholics. J ClinEndocrinol Metab 1991; 72: 1290–5.
15. Adinoff B., Krebaum S. R., Chandler P. A., Ye W., BrownM. W., Williams M. J. Dissection of hypothalamic–pituitary–adrenal axis pathology in 1-month-abstinent alcohol-dependent men, part 2: response to ovine corticotropin-releasing factor and naloxone. Alcohol Clin Exp Res 2005;29: 528–37.
16. Adinoff B., Krebaum S. R., Chandler P. A., Ye W., BrownM. W., Williams M. J. Dissection of hypothalamic–pituitary–adrenal axis pathology in 1-month-abstinent alcohol-dependent men, part 1: adrenocortical and pituitaryglucocorticoid responsiveness. Alcohol Clin Exp Res 2005;29: 517–27.
17. Bernardy N. C., King A. C., Parsons O. A., Lovallo W. R.Altered cortisol response in sober alcoholics: an examina-tion of contributing factors. Alcohol 1996; 13: 493–8.
18. Errico A. L., Parsons O. A., King A. C., Lovallo W. R.Attenuated cortisol response to biobehavioral stressorsin sober alcoholics. J Stud Alcohol 1993; 54: 393–8.
19. Oswald L. M., Mathena J. R., Wand G. S. Comparison of HPAaxis hormonal responses to naloxone vs psychologically-induced stress. Psychoneuroendocrinology 2004; 29: 371–88.
20. Sorocco K. H., Lovallo W. R., Vincent A. S., Collins F. L.Blunted hypothalamic–pituitary–adrenocortical axis res-ponsivity to stress in persons with a family history ofalcoholism. Int J Psychophysiol 2006; 59: 210–17.
21. Rohleder N., Kirschbaum C. The hypothalamic–pituitary–adrenal (HPA) axis in habitual smokers. Int J Psychophysiol2006; 59: 236–43.
22. Chen H., Fu Y., Sharp B. M. Chronic nicotine self-administration augments hypothalamic–pituitary–adrenalresponses to mild acute stress. Neuropsychopharmacology2008; 33: 721–30.
23. Matta S. G., Fu Y., Valentine J. D., Sharp B. M. Responseof the hypothalamic–pituitary–adrenal axis to nicotine.Psychoneuroendocrinology 1998; 23: 103–13.
24. Koval J. J., Pederson L. L. Stress-coping and other psychoso-cial risk factors: a model for smoking in grade 6 students.Addict Behav 1999; 24: 207–18.
25. de Wit H., Vicini L., Childs E., Savla M. A., Terner J. Doesstress reactivity or response to amphetamine predictsmoking progression in young adults? A preliminary study.Pharmacol Biochem Behav 2007; 86: 312–19.
26. Moss H. B., Vanyukov M., Yao J. K., Kirillova G. P. Salivarycortisol responses in prepubertal boys: the effects of paren-tal substance abuse and association with drug use behaviorduring adolescence. Biol Psychiatry 1999; 45: 1293–9.
27. Moss H. B., Vanyukov M. M., Martin C. S. Salivary cortisolresponses and the risk for substance abuse in prepubertalboys. Biol Psychiatry 1995; 38: 547–55.
28. Majewska M. D. HPA axis and stimulant dependence: anenigmatic relationship. Psychoneuroendocrinology 2002; 27:5–12.
29. Huizink A. C., Ferdinand R. F., Ormel J., Verhulst F. C.Hypothalamic–pituitary–adrenal nal axis activity and earlyonset of cannabis use. Addiction 2006; 101: 1581–8.
30. Schumann G. Hypothalamic–pituitary–adrenal axis andsubstance use: so many questions—and we can answerthem. Addiction 2006; 101: 1538–9.
31. Huizink A. C., Ferdinand R. F., Ormel J., Verhulst F. C. HPAaxis activity: a response to comments by Gunter Schumann.Addiction 2006; 101: 1833–4.
32. de Winter A. F., Oldehinkel A. J., Veenstra R., BrunnekreefJ. A., Verhulst F. C., Ormel J. Evaluation of non-responsebias in mental health determinants and outcomes in a largesample of pre-adolescents. Eur J Epidemiol 2005; 20: 173–81.
33. Huisman M., Oldehinkel A. J. de Winter A., Minderaa R. B.,de Bildt A., Huizink A. C. et al. Cohort profile: the Dutch‘TRacking Adolescents’ Individual Lives’ Survey’; TRAILS.Int J Epidemiol 2008; 37: 1227–35.
34. Kirschbaum C., Hellhammer D. H. Salivary cortisol inpsychoneuroendocrine research: recent developmentsand applications. Psychoneuroendocrinology 1994; 19: 313–33.
35. Clow A., Thorn L., Evans P., Hucklebridge F. The awakeningcortisol response: methodological issues and significance.Stress 2004; 7: 29–37.
36. Wust S., Federenko I., Hellhammer D. H., Kirschbaum C.Genetic factors, perceived chronic stress, and the free corti-sol response to awakening. Psychoneuroendocrinology 2000;25: 707–20.
37. Bartels M., Van den Berg M., Sluyter F., Boomsma D. I.,de Geus E. J. Heritability of cortisol levels: review and simul-taneous analysis of twin studies. Psychoneuroendocrinology2003; 28: 121–37.
38. Shirtcliff E. A., Granger D. A., Booth A., Johnson D. Lowsalivary cortisol levels and externalizing behavior problemsin youth. Dev Psychopathol 2005; 17: 167–84.
39. Aardal E., Holm A. C. Cortisol in saliva—reference rangesand relation to cortisol in serum. Eur J Clin Chem ClinBiochem 1995; 33: 927–32.
40. Cohen J. Statistical Power Analysis for the Behavioral Sciences,2nd edn. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988.
41. Lupien S. J., King S., Meaney M. J., McEwen B. S. Child’sstress hormone levels correlate with mother’s socio-economic status and depressive state. Biol Psychiatry 2000;48: 976–80.
42. Hopfer C. J., Crowley T. J., Hewitt J. K. Review of twin andadoption studies of adolescent substance use. J Am AcadChild Adolesc Psychiatry 2003; 42: 710–19.
43. Dick D. M., Aliev F., Wang J. C., Grucza R. A., Schukit M.,Kuperman S. et al. Using dimensional models of externaliz-ing psychopathology to aid in gene identification. Arch GenPsychiatry 2008; 65: 310–18.
44. Pagan J. L., Rose R. J., Viken R. J., Pulkkinen L., Kaprio J.,Dick D. M. Genetic and environmental influences on stagesof alcohol use across adolescence and into young adult-hood. Behav Genet 2006; 36: 483–97.
45. Schumann G., Johann M., Frank J., Preuss U., Dahmen N.,Laucht M. et al. Systematic analysis of glutamatergic neu-rotransmission genes in alcohol dependence and adolescentrisky drinking behavior. Arch Gen Psychiatry 2008; 65:826–38.
1936 Anja C. Huizink et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 1927–1936
Related Documents











