DOI: 10.1212/01.wnl.0000265592.74483.a6 2007;69;166-171 Neurology R. Schiffmann and S. Blaser Haginoya, W. Köhler, M. Henneke, A. Dinopoulos, P. Grattan-Smith, K. Brockmann, M. S. van der Knaap, T. Linnankivi, A. Paetau, A. Feigenbaum, K. Wakusawa, K. pathology Hypomyelination with atrophy of the basal ganglia and cerebellum: Follow-up and This information is current as of July 11, 2007 http://www.neurology.org/cgi/content/full/69/2/166 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0028-3878. Online ISSN: 1526-632X. published continuously since 1951. Copyright © 2007 by AAN Enterprises, Inc. All rights reserved. Neurology is the official journal of AAN Enterprises, Inc. A bi-monthly publication, it has been by KAZUHIRO HAGINOYA on July 11, 2007 www.neurology.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

DOI: 10.1212/01.wnl.0000265592.74483.a6 2007;69;166-171 Neurology
R. Schiffmann and S. Blaser Haginoya, W. Köhler, M. Henneke, A. Dinopoulos, P. Grattan-Smith, K. Brockmann,
M. S. van der Knaap, T. Linnankivi, A. Paetau, A. Feigenbaum, K. Wakusawa, K. pathology
Hypomyelination with atrophy of the basal ganglia and cerebellum: Follow-up and
This information is current as of July 11, 2007
http://www.neurology.org/cgi/content/full/69/2/166located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0028-3878. Online ISSN: 1526-632X. published continuously since 1951. Copyright © 2007 by AAN Enterprises, Inc. All rights reserved. Neurology is the official journal of AAN Enterprises, Inc. A bi-monthly publication, it has been
by KAZUHIRO HAGINOYA on July 11, 2007 www.neurology.orgDownloaded from

Hypomyelination with atrophy of thebasal ganglia and cerebellumFollow-up and pathology
M.S. van der Knaap,MD, PhD
T. Linnankivi, MDA. Paetau, MDA. Feigenbaum, MDK. Wakusawa, MDK. Haginoya, MDW. Kohler, MDM. Henneke, MDA. Dinopoulos, MD,PhD
P. Grattan-Smith, MDK. Brockmann, MDR. Schiffmann, MDS. Blaser, MD
ABSTRACT Background and objective: Hypomyelination with atrophy of the basal ganglia and cerebel-lum is a recently defined disorder. Only a few patients have been described. We report on 11 addi-tional patients and new MRI findings and provide histopathologic confirmation of the MRIinterpretation. Methods: We reviewed the patients’ clinical history and present findings. We scored theMRI abnormalities. The histopathology of one patient was re-examined. Results: The patients’ earlypsychomotor development was normal or delayed, followed by increasing extrapyramidal movementabnormalities, ataxia, and spasticity. Mental capacities were variably affected. MRI showed hypomy-elination with, on follow-up, evidence of further myelin loss and variable white matter atrophy. Theputamen was small or, more often, absent; the head of the caudate nucleus was decreased in size. Incontrast, the thalamus and globus pallidus remained normal. Cerebellar atrophy was invariablypresent. Histopathology confirmed the myelin deficiency, probably related to both lack of depositionand low-grade further loss. The degeneration of putamen was subtotal. The cerebellar cortex wasaffected, particularly the granular layer. Conclusion: Hypomyelination with atrophy of the basal gan-glia and cerebellum is a syndrome diagnosed by distinctive MRI findings. Histopathology confirmshypomyelination, low-grade further myelin loss, subtotal degeneration of the putamen, and cerebellarcortical atrophy. All known patients are sporadic, and the mode of inheritance is unclear. NEUROLOGY
2007;69:166–171
Hypomyelination with atrophy of the basal ganglia and cerebellum (HABC) is a childhoodleukoencephalopathy, first described in 2002 in seven patients.1 It has been reported oncethereafter in a single patient.2 The diagnosis of the syndrome is based onMRI findings, whichsuggest hypomyelination and selective atrophy of the neostriatum and cerebellum.
In this study, we provide new MRI data on 11 additional patients with HABC and his-topathologic confirmation of the MRI interpretation.
From the Department of Child Neurology (M.S.v.d.K.), VU University Medical Center, Amsterdam, the Netherlands; Department of PediatricNeurology (T.L.), Hospital for Children and Adolescents, Helsinki University, and Department of Pathology (A.P.), Helsinki University CentralHospital, Finland; Clinical and Metabolic Genetics (A.F.) and Department of Neuroradiology (S.B.), Hospital for Sick Children, Toronto, Ontario,Canada; Department of Pediatrics (K.W., K.H.), Tohoku University School of Medicine, Sendai, Japan; Department of Neurology (W.K.),Sachsisches Krankenhaus Hubertusburg, Wermsdorf, and Department of Pediatrics and Pediatric Neurology (M.H., K.B.), Georg AugustUniversity, Gottingen, Germany; Department of Pediatric Neurology (A.D.), Cincinnati Children’s Hospital Medical Center, OH; Department ofNeurology (P.G.-S.), Sydney Children’s Hospital, Randwick, Australia; and Developmental and Metabolic Neurology Branch (R.S.), NationalInstitute of Neurological Disorders and Stroke, NIH, Bethesda, MD.
Disclosure: The authors report no conflicts of interest.
Supplemental data atwww.neurology.org
Address correspondence andreprint requests to Dr. M.S. vander Knaap, Department of ChildNeurology, VU UniversityMedical Center, P.O. Box 7057,1007 MB Amsterdam, [email protected]
166 Copyright © 2007 by AAN Enterprises, Inc. by KAZUHIRO HAGINOYA on July 11, 2007 www.neurology.orgDownloaded from

METHODS We reviewed the clinical history and currentfindings of the new patients. These new patients were identifiedin different centers; the MRI scans were sent to one center inAmsterdam for review.
MRI examinations included T1-weighted and T2-weightedimages in sagittal and transverse planes. We scored the MRIfor stage of myelination and presence of gray and whitematter signal abnormalities as well as atrophy, as describedpreviously.1,3
Autopsy was performed in Patient 11. The brain and spinalcord were studied after fixation in formalin. Paraffin-embedded samples were sectioned at 6 to 10 �m and stainedusing the following methods: hematoxylin– eosin, periodicacid–Schiff (PAS), Luxol fast blue–cresyl violet (LFB), andHolmes silver impregnation. Selected blocks were additionallystained with Prussian blue (for iron), Fontana (for melanin pig-ment), toluidine blue (for metachromasia), modified rhodaninetechnique (for copper), and Sudan black B (for lipids). Immu-nohistochemial stainings were performed using monoclonal an-tibodies to glial fibrillary acidic protein (GFAP; Dako M0761,1:300; K5007 Envision detection kit, Dako, Carpinteria, CA)
and CD68 (KP 1; Dako M0814 1:400; K5007 Envision detectionkit; Dako).
RESULTS Clinical profiles. The clinical data aresummarized in the table. More details are given intable E-1 (on the Neurology Web site at www.neurology.org). All patients were isolated cases;only the parents of Patient 4 were related. Patients 1,3, and 5 had the most severe phenotype, followed inseverity by Patients 4 and 8. These patients did notachieve walking without support. Patients 2, 6, 7, 9,and 11 had a normal initial development, and allachieved unsupported walking. Over the years,there were increasing signs of spasticity, cerebellarataxia and particularly extrapyramidal movementabnormalities. The patients had a variable cognitivedeficit (table), but even if severe, social awarenesswas preserved. Cognitive decline was observed in
Table Clinical history, current findings, and ages at MRI
Patient no. 1 2 3 4 5 6 7 8 9 10 11
Gender Male Male Male Female Male Male Female Female Male Female Male
Year of birth 2002 2000 1996 1995 1995 1994 1992 1984 1983 1982 1979
Age at presentation 6 mo 3 y 3 mo 7 mo 3 mo 3 y 1 y 6 mo 21⁄2 y 10 mo 2 y
Initial motor development Delayed Normal Delayed Delayed Delayed Normal Mildly delayed Normal Normal Normal Normal
Unsupported walking — 15 mo — 3 y — 15 mo 17 mo — 16 mo �2 y 31⁄2 y
Max. motor milestone Rolling over,holding objects
US walking Rolling over Few steps alone Rolling over US walking US walking US sitting US walking US walking US walking
Onset of motor deterioration 10 mo 11⁄2 y 3 mo 31⁄2 y 2 yr 21⁄2 yr 3 yr 8 mo 21⁄2 yr 7 yr 7 yr
Loss of US walking — 23⁄4 y — 31⁄2 y — 8 y 6 y — 14 y 10 y 71⁄2 y
Max. speech development None 5 words None 20–30 words None Normal 7 words 5 words 5–6 wordsent.
Singlewords
4–5 wordsent.
Current motor signs
Truncal hypotonia � � � � � � � � � � �
Spasticity of extremities � � (R � L) � � � � � (R � L) � � � �
Ataxia Not evaluable � Not evaluable � Not evaluable � � � � � �
Tremor � � � � � � � � � � �
Choreoathethosis � � � � � � � � � � �
Dystonia � � (R � L) � � � � � � � � �
Rigidity � � � � � � � � � � �
An-/dysarthria Anarthria � Anarthria anarthria Anarthria Dysarthria Anarthria Anarthria Anarthria Dysarthria Anarthria
Swallowing difficulties � � � � � � � � � � �
Cognitive deficiency* Severe Moderate Severe Severe Severe Moderate Moderate Moderate Moderate Moderate Moderate
Cognitive decline Unclear No Unclear Yes No Yes Yes No Yes Yes No
Vision Normal,nystagmus
Normal Poor visualtracking
Myopia,nystagmus
Nystagmus Normal Normal Normal,nystagmus
Normal Normal Normal
Hearing Normal Decreased Decreased Normal Decreased Normal Normal Normal Decreased Normal Normal
Head circumference �2 SD Normal �2 SD Normal �2 SD Normal �2 SD Normal Normal �2 SD Normal
Stature �2 SD �2 SD �2 SD Normal � �2 SD Normal Normal Normal Normal �2 SD Normal
MRI, y 1, 13⁄4, 3 3, 3, 4 2, 7 2, 3, 7, 8, 9 4, 6, 11 5, 8, 9 12 9, 20 13, 21 22 11
*Moderate deficiency indicates an estimated total IQ between 40 and 55; severe deficiency indicates an estimated total IQ between 25 and 40 (Diagnostic and Sta-tistical Manual for Mental Disorders, 4th ed., criteria for metal retardation).max. � maximum; US � unsupported; sent. � sentences.
Neurology 69 July 10, 2007 167 by KAZUHIRO HAGINOYA on July 11, 2007 www.neurology.orgDownloaded from

most patients, but was milder than the motor de-cline. Patient 3 was the only patient who had epi-lepsy; Patient 10 had a single seizure. Four patientshad a sensorineural hearing loss. Five patients had ashort stature, and five patients had borderline mi-crocephaly. In none of the patients were abnormali-ties of internal organs found on physicalexamination.
Patient 11 died at age 12. He had a prolongedrespiratory tract infection and was unexpectedlyfound dead in his bed. Autopsy did not reveal a di-rect cause of death, which was ascribed to brain-stem degeneration with respiratory insufficiency.
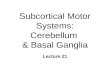
MRI. Twenty-six MRI scans were obtained in our11 patients at ages between 1 and 22 years (table).These studies showed a homogeneous picture of dif-fuse myelin deficit as the most striking finding. Allcerebral hemispheric white matter had a high signalintensity on T2-weighted images, indicative of dif-fuse myelin deficit (figures 1 and 2). Only in Patient2 did T2-weighted images show more myelin withisointensity between the cerebral hemispheric whitematter and the cortex. The state of myelination ofthe corpus callosum, internal capsule, and cerebel-lar white matter was variable. The brainstem had alow signal intensity on T2-weighted images in allpatients; in most patients, the pyramidal tractsstood out with a higher signal intensity (figure 1).On T1-weighted images, the signal intensity of thecerebral hemispheric white matter varied fromisointense to in most cases mildly hyperintense rela-tive to the cortex (figures 1 and 2). In most patients,the white matter volume was mildly reduced withslightly to mildly dilated lateral ventricles.
We had prolonged MRI follow-up in Patients 4,5, 8, and 9 (table). In these patients the MRI showedevidence of progressive myelin loss. This was mostclearly shown by the T1-weighted images. Whitematter structures that initially had a high signal in-tensity lost this high signal and became dark onfollow-up (figure 2). In Patient 4, the volume of thecerebral white matter was initially normal, but se-
vere white matter atrophy occurred over time withserious enlargement of the lateral ventricles (figure2). In Patient 10, severe white matter atrophy was alsoseen at age 22. In Patients 5, 8, and 9, the progressivewhite matter atrophy was much milder. In Patient 3,the cerebral white matter atrophywas alreadymarkedat age 2 and even more severe at age 7.
Mild to severe cerebellar atrophy was seen in allpatients from early on, affecting the vermis morethan the hemispheres (figure 1), with slow progressionover time. The thalamus and globus pallidus had anormal appearance. The putamen was small butpresent on the first MRI at ages 1 and 13⁄4 in Patient 1,but was no longer visible at age 3. In all other patients,there was no visible putamen (figures 1 and 2). Thehead of the caudate nucleus had either a normal or amildly reduced size and became smaller on follow-up.In Patients 3 and 4, the head of the caudate nucleusbecame entirely flat (figure 2).
Histopathology. Brain autopsy was performed in Pa-tient 11. Brain weight was marginally reduced to1,200 g. The surface of the cerebral hemispheres wasunremarkable. The brainstem was slightly atrophic,especially at the basis of the pons and the pyramids.The cerebellum was atrophic, particularly the ver-mis. Coronal sections displayed a normal corticalribbon, but the central white matter was slightlygrayish and reduced, especially in the parieto-occipital region. Another prominent macroscopicchange was a very thin, slightly yellowish putamen,while the globus pallidus and thalamus were normaland the caudate nucleus was only slightly reduced insize. The brainstem showed signs of pyramidal tractdegeneration in the crura cerebri, pons, and medullaoblongata. Cerebellar cortical atrophy was noted.The spinal cord appeared unremarkable.
On microscopic examination, the cerebral whitematter was somewhat better preserved in the imme-diately subcortical regions, but deeper in the cen-trum semiovale, there was a marked lack of myelin(figure 3A). The myelin deficiency seemed to be re-lated to both hypomyelination and mild myelin de-
Figure 1 MRI of Patient 5Axial T2-weighted images (Aand C) and axial (B) andsagittal T1-weighted (D)images of Patient 5 at age12. The cerebral whitematter has a high signal onboth T2-weighted (A) and T1-weighted (B) images. There isno visible putamen (A). Thethalamus (arrowhead in A)and globus pallidus (arrow inA) have a normal size. Thepyramidal tracts in thebrainstem have a high signalon T2-weighted images(arrows in C). The cerebellarvermis is atrophic (D).
168 Neurology 69 July 10, 2007 by KAZUHIRO HAGINOYA on July 11, 2007 www.neurology.orgDownloaded from

generation, because also a few macrophages couldbe seen focally in perivascular regions. By the use ofmyelin staining, silver impregnations, toluidineblue, PAS, iron, melanin, and copper stains, knownleukodystrophies were excluded. The silver stainsdemonstrated slightly reduced density of axons inthe white matter, which as such were quite well pre-served (figure 3B). Anti-GFAP staining showed amoderate astrogliosis (figure 3C). Anti-CD68 stain-ing demonstrated a strong microglial response, butonly a few macrophages (figure 3D). The density ofwhite matter oligodendrocytes appeared reduced, asjudged by light microscopy.
The cerebral cortex was normal. The degener-ation of putamen was subtotal (figure 3E). It re-mained as a 2- to 3-mm-wide structure. Therewere only few remaining neurons (figure 3F),many of them pyknotic, and there was a clear-cutgliosis (figure 3G). However, putaminopallidalmyelinated nerve fiber bundles were quite intact(figure 3E). The caudate nucleus showed slightnarrowing due to a diffuse neuronal loss and glio-sis, especially subependymally. The thalamus andglobus pallidus were intact. The cerebellar cortexwas atrophic as demonstrated by the paucicellu-lar granular layer (figure 3H). The molecularlayer was narrowed and slightly gliotic. Purkinjecells showed only a minor patchy dropout. Themyelinated fibers were depleted, especially in thecerebellar cortical folia.
In the brainstem, the pyramidal tracts showedmarked degeneration with equal loss of axons andmyelin (figure 3I). The pyramidal tract degenerationwas also seen to some extent in the spinal cord.
DISCUSSION The term “hypomyelination” is as arule used for leukoencephalopathies characterizedby a significant permanent deficit in the amount of
myelin deposited in the brain as compared with nor-mal.1 There are several known disorders character-ized by diffuse hypomyelination, includingPelizaeus–Merzbacher disease,4,5 Salla disease,6
Cockayne syndrome type II,7 trichothiodystrophy,8
mutations in SOX10,9,10 a Pelizaeus–Merzbacher-like syndrome with mutations in connexin 46.6,11,12
a syndrome characterized by hypomyelination andcataracts13 and a syndrome characterized by hypo-myelination, and hypodontia.14,15 Patients with Pel-izaeus–Merzbacher are almost exclusively boys.The diagnosis can be confirmed by a search for du-plications, deletions, or mutations of the PLP1gene.4,5 Salla disease is most commonly seen in pa-tients from Scandinavian ancestry. The appropriatelaboratory screening test is assessment of sialic acidin urine.6 Patients with Cockayne syndrome and tri-chothiodystrophy (almost) invariably have an asso-ciated hypersensitivity of the skin to sunlight. Thediagnosis can be confirmed by ultra-violet irradia-tion of fibroblasts.7,8 Patients with SOX10 muta-tions have a Waardenburg–Hirschsprung syndromein combination with hypomyelination of the centraland peripheral nervous system.9,10 Patients with mu-tations in connection 46.6 are clinically similar topatients with Pelizaeus–Merzbacher disease, butwith an autosomal recessive mode of inheritance.The appropriate laboratory test is mutational anal-ysis of GJA12.11,12 Patients with hypomyelinationand cataracts should be tested for mutations in therecently identified gene HYCCIN.13 Hypomyelina-tion with hypodontia is a clinical diagnosis. In olderpatients, hypogonadotropic hypogonadism can betested for.14,15 Unfortunately, most patients with hy-pomyelination remain without a specific diagnosis.Among the children with a leukoencephalopathy ofunknown origin, “hypomyelinating disorders” con-
Figure 2 MRI of Patient 3
Sagittal T1-weighted images (A and C) and axial T2-weighted images (B and D) of Patient 3 at ages 2 (A and B) and 9 (C and D). Atage 2, the cerebral white matter has a high signal on T1-weighted images (A), whereas most of the cerebral white matter has a lowsignal on T1-weighted images at age 9 (C). The axial T2-weighted images show that the cerebral white matter has a moderatelyelevated signal and a normal volume at age 2 (B), whereas the white matter has a much higher signal and is seriously reduced involume at age 9 (D). The putamen is not visible at ages 2 and 9 (B and D). The head of the caudate nucleus is small at age 2 (arrowin B), whereas it is flat at age 9 (arrow in D). The thalamus has a normal size (arrowheads in B and D).
Neurology 69 July 10, 2007 169 by KAZUHIRO HAGINOYA on July 11, 2007 www.neurology.orgDownloaded from

stituted the largest single category.3 Patients with ahypomyelinating disorder of unknown origin have ahighly variable clinical picture, making it unlikelythat they represent a single disease entity.3
One of the newly recognized hypomyelinatingdisorders is HABC.1,2 The hypomyelination inHABC is partial.1,2 In most HABC patients, the cere-bral hemispheric white matter has a high signal onboth T2-weighted and T1-weighted images. Whitematter that contains no or very little myelin has along T1 and T2, resulting in low signal intensity onT1-weighted images and high signal intensity onT2-weighted images.16-18 With myelin depositionand its associated biochemical and structuralchanges, there is an earlier and more pronouncedT1 shortening than T2 shortening.16-18 Because ofthis, diffuse deposition of a small amount of myelin
results in high signal intensity on T2-weighted im-ages and intermediate or high signal intensity onT1-weighted images. In most patients with HABC,MRI is suggestive of a diffuse but partial hypomyeli-nation of the cerebral hemispheres. A new MRIfinding is that further loss of myelin occurs on pro-longed follow-up with disappearance of the highsignal on the T1-weighted images. Histopathologicfindings confirm this MRI interpretation and showthat there is a lack of myelin in the cerebral hemi-spheres with evidence of both hypomyelination anda low-grade myelin loss. A previous proton MRSstudy showed that within the cerebral white matterthe levels of myo-inositol and creatine are highly in-creased and N-acetylaspartate is normal.1 Thesefindings were interpreted as evidence for white mat-ter gliosis and preservation of axons.1 This interpre-
Figure 3 Paraffin sections of the brain of Patient 11 at age 12
(A) Luxol fast blue–cresyl violet (LFB) stain (magnification �200) shows a lack of myelin in the occipital white matter. Above thecentral vessel to the right, myelinated fibers are somewhat better preserved (arrow). (B) Holmes silver staining (magnification�200) of the same area demonstrates that the axons, although somewhat reduced in density, are much better preserved.(C) In glialfibrillary acidic protein (GFAP) staining (magnification �400), a moderate white matter astrogliosis with scattered hypertrophicastrocytes (arrow) is seen. (D) CD68 staining (magnification �400) demonstrates a strong activation of rod-shaped microglial cellswithin the white matter, but only few plump macrophages (arrow). (E) LFB staining (magnification �100) shows the highly narrowedputamen with obliquely horizontally running myelinated putaminopallidal fibers between arrows. Note the near-total loss ofneuronal cells and the widened perivascular spaces. In the lower left corner, some myelinated putaminopallidal fiber bundles arepreserved. (F) Hematoxylin–eosin stain (magnification �400). The putamen is seen to harbor only a few preserved neurons(arrow).(G) GFAP staining (magnification �400) demonstrates astrogliosis of the putamen (arrow). (H) LFB stain (magnification�40). Cerebellar cortical folia are atrophic with narrowed molecular layer, slight dropout of Purkinje cells, and hypocellular granularlayer (between arrows). Myelinated fibers (blue) are sparse in the foliar white matter. (I) LFB stain (magnification �40). Thedegenerated right pyramid of the medulla is shown between arrows.
170 Neurology 69 July 10, 2007 by KAZUHIRO HAGINOYA on July 11, 2007 www.neurology.orgDownloaded from

tation is currently confirmed by histologic findings.MRI shows a better myelination of the brain stemand in most patients signal abnormalities in the py-ramidal tracts of the brainstem1 (current study). Inconformity, histopathology shows marked degener-ation of the pyramidal tracts of brainstem.
The putamen is always severely affected. In onlytwo patients1 (current study), a small putamen wasseen on an earlyMRI, which disappeared on follow-up. In the other patients, the putamen was neverseen on MRI. Histopathology reveals that the puta-men is reduced to a few-millimeters-wide glioticstructure, apparently below the level of detectionfor MRI. The caudate nucleus is less severely af-fected, whereas the globus pallidus and thalamusare strikingly preserved, both on MRI and in histo-pathology. The cerebral cortex looks normal onMRI1,2 (current study). Previous MRS data sug-gested a normal composition of the cerebral cortexwith a normal N-acetylaspartate level.1 Current au-topsy findings confirm the absence of cerebral corti-cal involvement. The cerebellum is atrophic onMRI. Histopathology shows that especially thegranular layer of the cerebellar cortex is affected,whereas the molecular layer and Purkinje cells areaffected to a lesser degree. As the clinical pictureincludes progressive cerebellar ataxia, we assumethat the decrease in granular neurons representsatrophic loss rather than developmental hypoplasia.
This study confirms that HABC is a recognizabledisease entity with a homogeneous MRI pattern.The highly distinctive pattern of MRI findings, incombination with the similarities in clinical findingsamong the patients, makes it likely that we are deal-ing with a nosologic entity. The putative commonfactor responsible for the selective vulnerability ofthe central myelin, neostriatum, and cerebellum isunclear. Most hypomyelinating disorders are inher-ited. Although all patients are isolated cases, it islikely that HABC is genetically determined. Themode of inheritance could be autosomal recessive orautosomal dominant, all patients having a de novomutation.
Received July 17, 2006. Accepted in final form February 20,2007.
REFERENCES1. Van der Knaap MS, Naidu S, Pouwels PJW, et al. New
syndrome characterized by hypomyelination with atro-
phy of the basal ganglia and cerebellum. AJNRAm J Neuroradiol 2002;23:1466–1474.
2. Mercimek-Mahmutoglu S, van der Knaap MS, Baric I,Prayer D, Stoeckler-Ipsiroglu S. Hypomyelination withatrophy of the basal ganglia and cerebellum (H-ABC). Re-port of a new case. Neuropediatrics 2005;36:223–226.
3. Van der Knaap MS, Breiter SN, Naidu S, et al. Definingand categorizing leukoencephalopathies of unknown ori-gin: MR imaging approach. Radiology 1999;213:121–133.
4. Van der Knaap MS, Valk J. The reflection of histology inMR imaging of Pelizaeus–Merzbacher disease. AJNRAm J Neuroradiol 1989;10:99–103.
5. Schneck L, Adachi M, Volk BW. Congenital failure ofmyelinization: Pelizaeus–Merzbacher disease. Neurology1971;21:817–824.
6. Sonninen P, Autti T, Varho T, et al. Brain involvement inSalla disease. AJNR Am J Neuroradiol 1999;20:433–443.
7. Nishio H, Kodama S, Matsuo T, et al. Cockayne syn-drome: magnetic resonance images of the brain in a severeform with early onset. J Inherit Metab Dis 1988;11:88–102.
8. Østergaard JR, Christensen T. The central nervous sys-tem in Tay syndrome. Neuropediatrics 1996;27:326–330.
9. Inoue K, Tanabe Y, Lupski JR. Myelin deficiencies inboth the central and the peripheral nervous systems asso-ciated with a SOX10 mutation. Ann Neurol 1999;46:313–318.
10. Inoue K, Shilo K, Boerkoel CF, et al. Congenital hypomy-elinating neuropathy, central dysmyelination, and Waar-denburg–Hirschsprung disease: phenotypes linked bySOX10 mutation. Ann Neurol 2002;52:836–842.
11. Uhlenberg B, Schuelke M, Ruschendorf F, et al. Muta-tions in the gene encoding gap junction protein �12 (con-nexin 46.6) cause Pelizaeus–Merzbacher-like disease.Am J Hum Genet 2004;75:251–260.
12. Bugiani M, Al Shahwan S, Lamantea E, et al. GJA12 mu-tations in children with recessive hypomyelinating leu-koencephalopathy. Neurology 2006;67:273–279.
13. Zara F, Biancheri R, Bruno C, et al. Deficiency of hyccin,a newly identified membrane protein, causes hypomyeli-nation and congenital cataract. Nat Genet 2006;38:1111–1113.
14. Wolf NI, Harting I, Boltshauser E, et al. Leukoencepha-lopathy with ataxia, hypodontia, and hypomyelination.Neurology 2005;64:1461–1464.
15. Timmons M, Tsokos M, Abu Asab M, et al. Peripheraland central hypomyelination with hypogonadotropic hy-pogonadism and hypodontia. Neurology 2006;67:2066–2069.
16. Barkovich AJ, Kjos BO, Jackson DE, Norman D. Normalmaturation of the neonatal and infant brain: MR imagingat 1.5 T. Radiology 1988;166:173–180.
17. Hittmair K, Wimberger D, Rand T, et al. MR assessmentof brain maturation: comparison of sequences. Am J Neu-roradiol AJNR 1994;15:425–433.
18. Barkovich AJ. Concepts of myelin and myelination inneuroradiology. AJNR Am J Neuroradiol 2000;21:1099–1109.
Neurology 69 July 10, 2007 171 by KAZUHIRO HAGINOYA on July 11, 2007 www.neurology.orgDownloaded from

DOI: 10.1212/01.wnl.0000265592.74483.a6 2007;69;166-171 Neurology
R. Schiffmann and S. Blaser Haginoya, W. Köhler, M. Henneke, A. Dinopoulos, P. Grattan-Smith, K. Brockmann,
M. S. van der Knaap, T. Linnankivi, A. Paetau, A. Feigenbaum, K. Wakusawa, K. pathology
Hypomyelination with atrophy of the basal ganglia and cerebellum: Follow-up and
This information is current as of July 11, 2007
& ServicesUpdated Information
http://www.neurology.org/cgi/content/full/69/2/166including high-resolution figures, can be found at:
Supplementary Material http://www.neurology.org/cgi/content/full/69/2/166/DC1
Supplementary material can be found at:
Subspecialty Collections
e_cnshttp://www.neurology.org/cgi/collection/all_demyelinating_diseas
Demyelinating disease (CNS)All http://www.neurology.org/cgi/collection/all_clinical_neurology
Clinical NeurologyAll http://www.neurology.org/cgi/collection/basal_ganglia
gangliaBasal http://www.neurology.org/cgi/collection/all_pediatric
PediatricAll http://www.neurology.org/cgi/collection/leukodystrophies
Leukodystrophies edhttp://www.neurology.org/cgi/collection/metabolic_disease_inherit
(inherited)Metabolic disease http://www.neurology.org/cgi/collection/mri
MRIfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.neurology.org/misc/Permissions.shtmlor in its entirety can be found online at: Information about reproducing this article in parts (figures, tables)
Reprints http://www.neurology.org/misc/reprints.shtml
Information about ordering reprints can be found online:
by KAZUHIRO HAGINOYA on July 11, 2007 www.neurology.orgDownloaded from
Related Documents