Hypertrophic cardiomyopathy Dipin.s Junior resident Internal medicine

Hypertrophic cardiomyopathy Dipin.s Junior resident Internal medicine.
Dec 19, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Hypertrophic cardiomyopathy
Dipin.s Junior resident
Internal medicine
• Autosomal dominant disease of the heart muscle, characterized by a small left ventricular cavity and marked hypertrophy of the myocardium with myofibril disarray.
• Overall prevalence is 1:500 to 1:1000• Disease of the myofilaments, with alteration in structure
and function • Most common cause of sudden cardiac death in young
people.

• Asymmetric septal hypertrophy (ASH)• Idiopathic hypertrophic subaortic stenosis
(IHSS)• Muscle subaortic stenosis• Hypertrophic obstructive cardiomyopathy
(HOCM).

Etiology
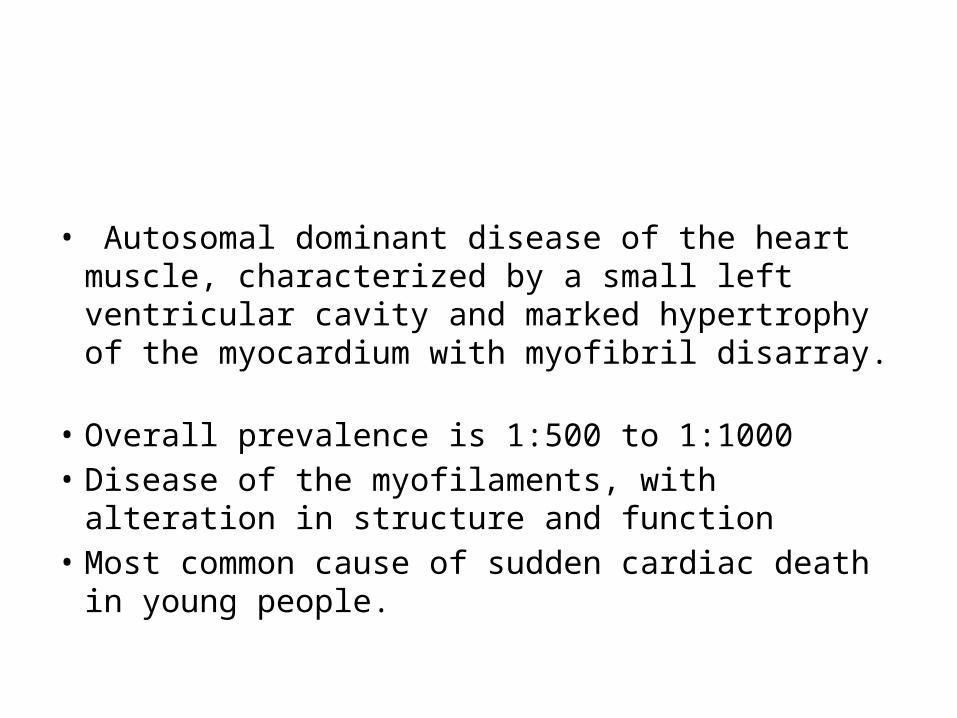
• Most common genetic cardiovascular disease• Mutation in genes encoding proteins of the cardiac
sarcomere myofilaments • Beta-myosin heavy chain, myosin-binding protein C,
cardiac troponin T and I,alpha -tropomyosin, actin, titin, and myosin light chains
• Other genes outside of the sarcomere myofilaments have also been recently implicated
• Deletions, insertions, missense, and splice site mutations.
• Hypothesis is that sarcomeric dysfunction leads to compensatory hypertrophy.
pathology
• Asymmetrical hypertrophy with a small LV cavity
• Mural endocardium thickened by fibrous tissue
• Elongation of chordae and ant. displacement of the hypertrophied papillary muscles
• LA is usually dilated

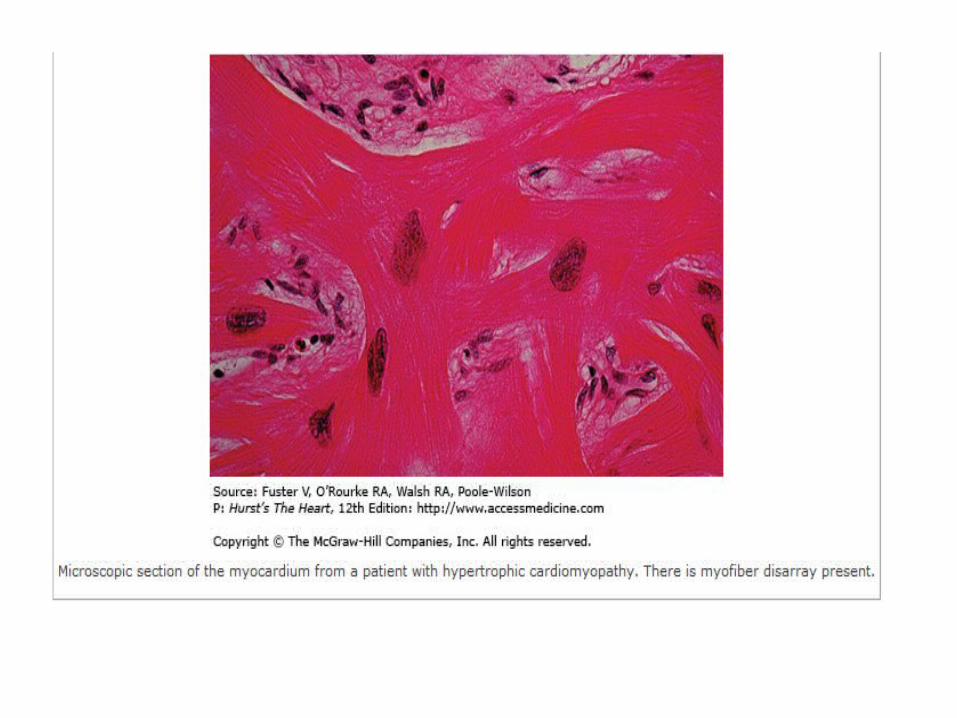
Histology
• Short runs of severely hypertrophied fibers interrupted by connective tissue
• Large and bizarre nuclei and fibrosis , with degenerating muscle fibers.
• Whorling of muscle fibers is characteristic of HCM
Pathophysiology
Diastolic dysfunction• Impaired ventricular relaxation and chamber
stiffness• Compensatory increase in late diastolic filling by
atrial systole.• During exercise or any other type of
catecholamine stimulation, diastolic filling period decreases as well as myocardial ischemia occurs
• Leads to severe diastolic dysfunction- dyspnoea

LVOT obstruction• Multifactorial• During systolic contraction the hypertrophied
basal septum encroaches to the outflow tract• Mitral leaflets are pulled in by the venturi force • In midcavitary region hypertrophied pappillary
muscles pressing against septum may cause obstruction
• LVOT obstruction is dynamic• Increased myocardial contractility, decreased
ventricular volume, or decreased afterload ----increasesMyocardial ischaemia• Supply-demand mismatch• compromised coronary blood flow to the LV
myocardium -- abnormally small and partially obliterated intramural coronary arteries

Autonomic dysfunction• Either a failure of systolic blood pressure to
rise >20 mmHg or a fall in systolic blood pressure during excercise.
• Speculated that there is high degree of abnormal autonomic tone in HCM
• Assoc. with poor prognosis

Mitral regurgitation• Secondary phenomenon due to systolic
anterior motion of leaflets due to LVOT obstruction
• During mid and late systole- jet directed post. and laterally
Clinical presentation
• Most are asymptomatic• Dyspnoea-diastolic dysfunction and elevated
LV filling pressures• Angina – epicardial coronary disease may be
absent• Syncope or presyncope- LV baroreceptors
causes reflex vasodilatation• Atrial fibrillation occurs more in elderly

Physical examination
• Carotid pulse- spike and dome pattern rapid rise (percussion wave) midsystolic drop secondary wave (tidal wave)• Jugular venous pressue- usually normal;
sometimes prominent a wave (hypertrophy and lack of compliant RV and powerful Rt atrial contraction)
• Apical impulse- forceful, sustained, diffuse double or triple apical impulse (outward thrust of ventricular contraction,a presystolic accentuated atrial contraction, and
expansion of early diastolic filling)• Cardiac sounds- usually split sometimes
paradoxically split S4 if severe hypertrophy
• Murmurs =crescendo–decrescendo murmur located primarily at the left sternal border. (usually ends before S2)
• May radiate to the base or apex, but seldom radiation to the carotid arteries.

• Any condition which increases the LVOT outflow gradient – more obstruction – murmur is louder longer and peak late in systole
LVOT obstruction and systolic murmur increased by……….
• A reduction in LV cavity volume and pressure ( less preload)
• A decrease in systemic vascular resistance / arterial pressure ( less after load )
• An increase in LV contractility
• Converse is also true
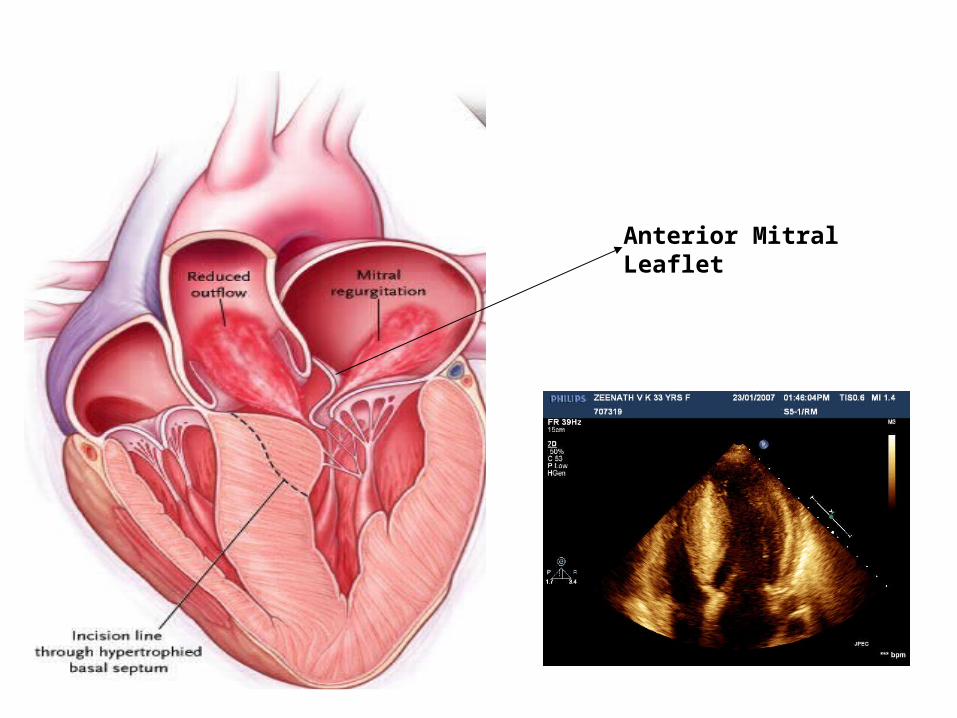
Anterior MitralLeaflet
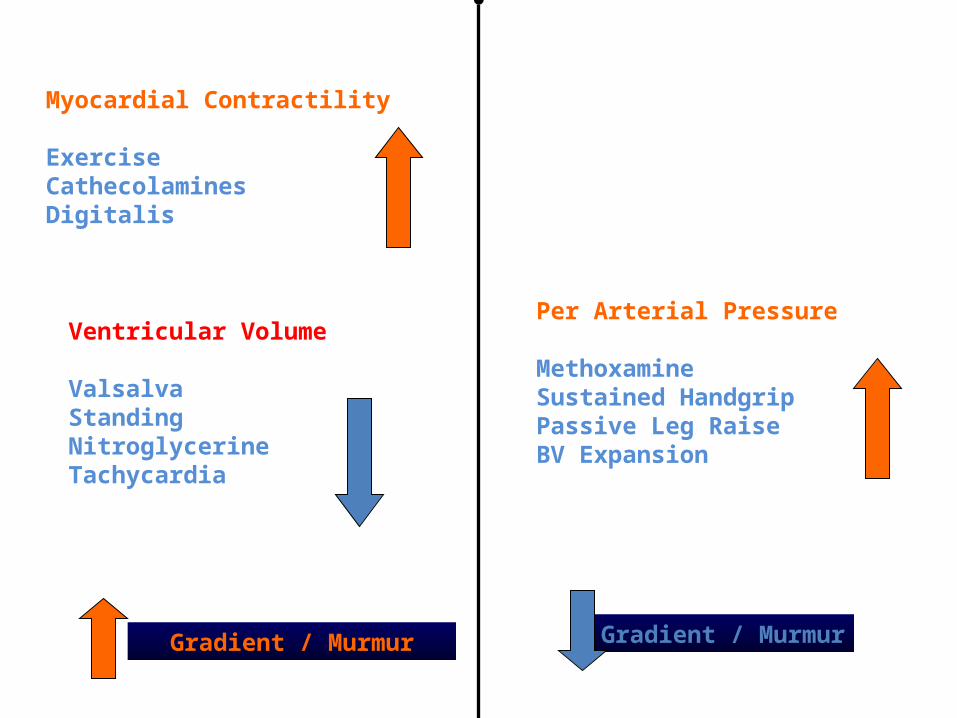
Myocardial Contractility
ExerciseCathecolaminesDigitalis
Ventricular Volume
ValsalvaStandingNitroglycerineTachycardia
Gradient / Murmur
Per Arterial Pressure
MethoxamineSustained HandgripPassive Leg RaiseBV Expansion
Gradient / Murmur
ECG
• Abnormal in 90-95 % patients• LVH• LAE• Deep and narrow q waves in inferolateral
leads• Diminished R waves in lateral precordial leads
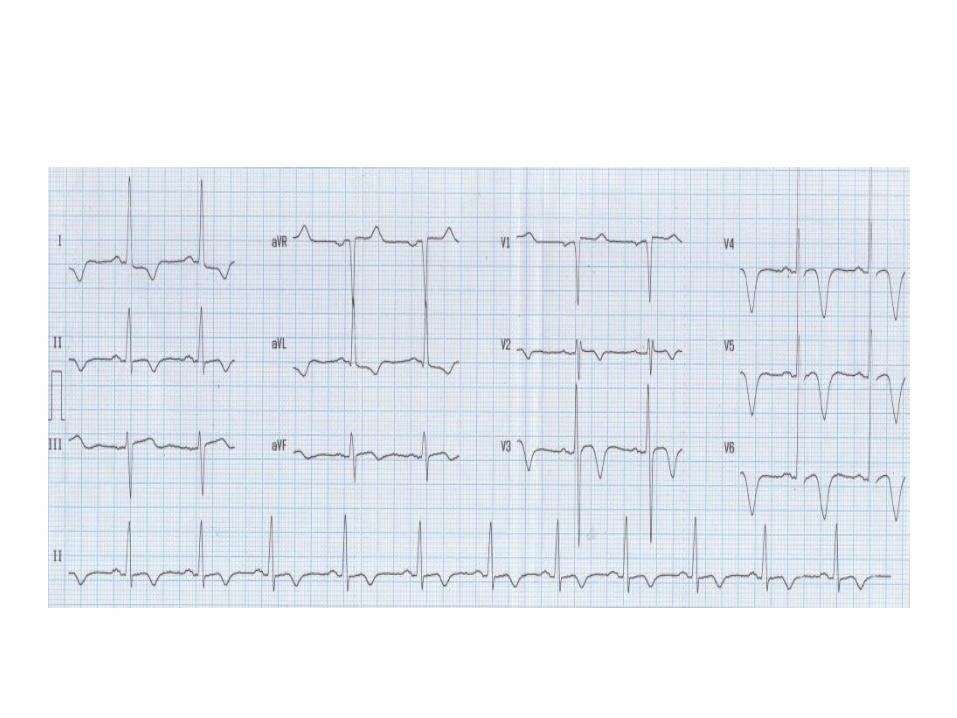
• Large negative precordial T waves• Left axis deviation
• No ECG finding is predictive of future events• Tall R and deep S waves weakly corelated with
magnitude of LV hypertrophy
• SVT 46%• PVCs 43%• Non sustained VT 26%• AF can occur in 25-30% of elderly
Chest X-Ray
• Mild to moderate enlargement of the cardiac silhouette.
• The left ventricular contour is rounded consistent with concentric LVH.
• Enlargement of the left atrium • Right-sided chambers are usually normal.
Echocardiography
• Gold standard for the diagnosis of HCM• Increased wall thickness in the absence of other etiology• Septum>=1.3 times LV post.free wall• Subaortic Gradient > 30mm Hg ( rest) >50(provocation)• Vigorous motion of post. Free wall with reduced septal
excursion• Avg. LV wall thickness in HCM is 20- 22mm• ECG and echo has to be correlated. • Low voltages in ECG in the presence of increased wall
thickness is seen in infiltrative disorder
• Small LV cavity/ Septal immobility• Primary tool for defining the presence and
severity of LVO tract obstruction• Systolic anterior motion of mitral valve• Presence and severity of MR (laterally and posteriorly directed jet in mid to
late systole)Cardiac MRI

• Subaortic gradient >30 is a determinant of heart failure but risk of sudden death
• Elderly patients are not targeted for risk stratification(SCD is uncommon and survival to old age itself suggests low risk)
• Beta myosin heavy chain and trop T mutations are assoc. with higher risk for premature death.

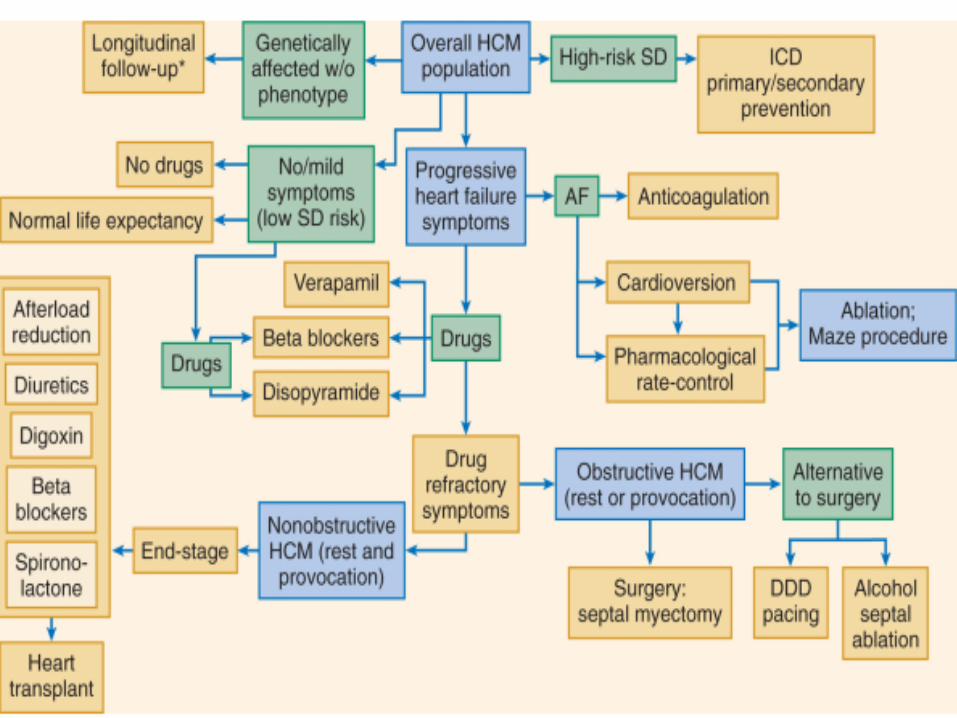
Management
Prevention of SCD• ICD implantation – as primary prevention
following cardiac arrest -as secondary prevention if
one or more high risk factors
• Empirical pharmacological therapy with amiodarone is now obsolete
Medical treatment
Heart failure • Beta blockers (slows heart rate, reduce force of
LV contraction, augments ventricular filling and relaxation, decreases myocardial O2 demand, blunts outflow gradient triggered by sympathetic activity)
• Verapamil (improves LV relaxation and filling)• Disopyramide• End stage failure –ACE ,ARBs, ICD to prevent SCD
• Atrial fibrillation- most common sustained arrhythmia in HCM
• Paroxysmal AF occurs in 20%• Increases with age and is related to LA dilatation• Acute decompensation- cardioversion• Amiodarone prevents reccurences• Rate control with beta blockers or verapamil• Started on anticoagulation
Diuretics……………..
• Can be use alone judiciously or with betablockers / verapamil to lessen pulmonary congestion
Non medical treatment
Surgery • Severe drug refractory heart failure symptoms • Severe functional disability (NYHA class III , IV)• Associated with LV outflow obstruction at rest
or with physiological exercise (>50mm gradient)• Transaortic ventricular septal myectomy
(morrow procedure)-small portion from basal septum
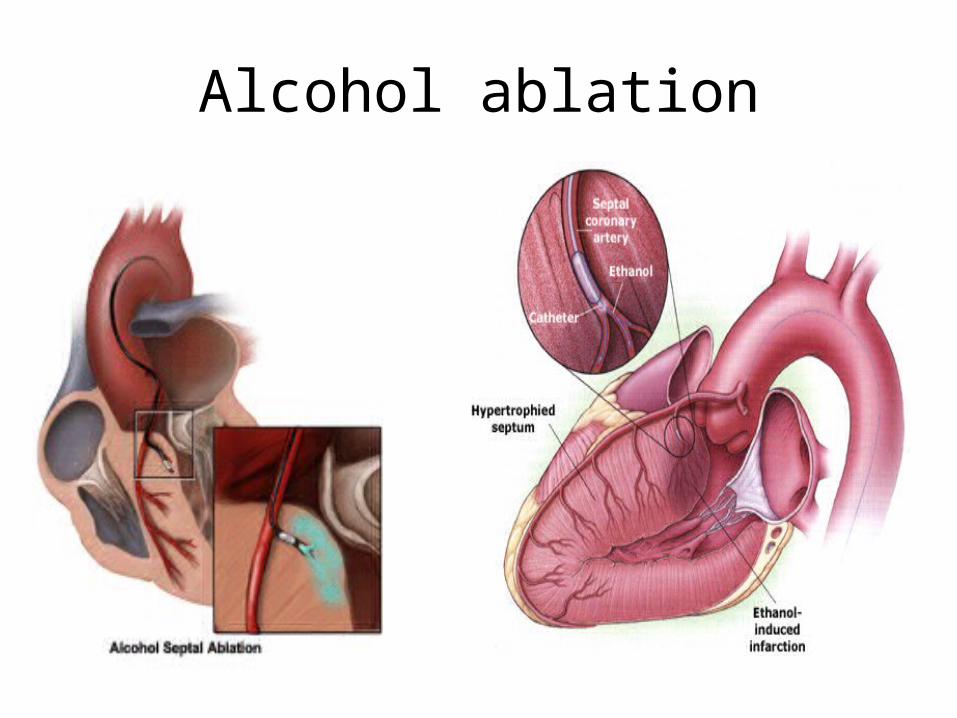
Alcohol ablation
• 96-98 % ethanol (1-3 ml)introduced into major septal perforator vessel
• Necrosis and permanent MI in proximal septum is created
• Thinning and reduced excursion of septum, Outflow tract enlarges- reduction of subaortic obstruction and MR
• alternative treatment strategy for selected patients— (advanced age, significant comorbidity and increased operative risk, without access to expert surgical centers, or pt.against surgical intervention)
Alcohol ablation
• Dual chamber pacing – no definite evidence
Infective endocarditis
• Vegetations most commonly seen on anterior mitral leaflet or septal endocardium at the site of mitral valve–septum contact
• standard antimicrobial prophylaxis is indicated prior to dental or surgical procedures
Thank you
Related Documents