Hypertensive Pulmonary Edema Sean Collins, MD, MSc Associate Professor Vanderbilt University Department of Emergency Medicine

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Hypertensive Pulmonary Edema
Sean Collins, MD, MScAssociate ProfessorVanderbilt University
Department of Emergency Medicine

Disclosures
• Consultant: Novartis, Cardiorentis, The Medicines Company, Medtronic
• Research Support: NIH, PCORI, Novartis, Cardiorentis, Trinity

AHF and Elevated BP

Hypertensive Pulmonary Edema

Hypertensive Pulmonary Edema

Scenario
• 75 YO F with h/o HTN and HF with SOB• BP- 180/100 P-80 RR-24 Satn- 84%• Moderate respiratory distress• Diffuse rales; +JVD, trace leg edema• CXR = pulmonary edema; U/S = comet tails• Treatment?

Q: Initial stabilization for this patient may include which of the following?
• a) Non invasive ventilation• b) Sublingual/IV nitrates• c) Dobutamine• d) 1) and 2)• e) All of the above

ESC Guidelines for Pulm Edema
McMurray et al. EHJ 2012; 33
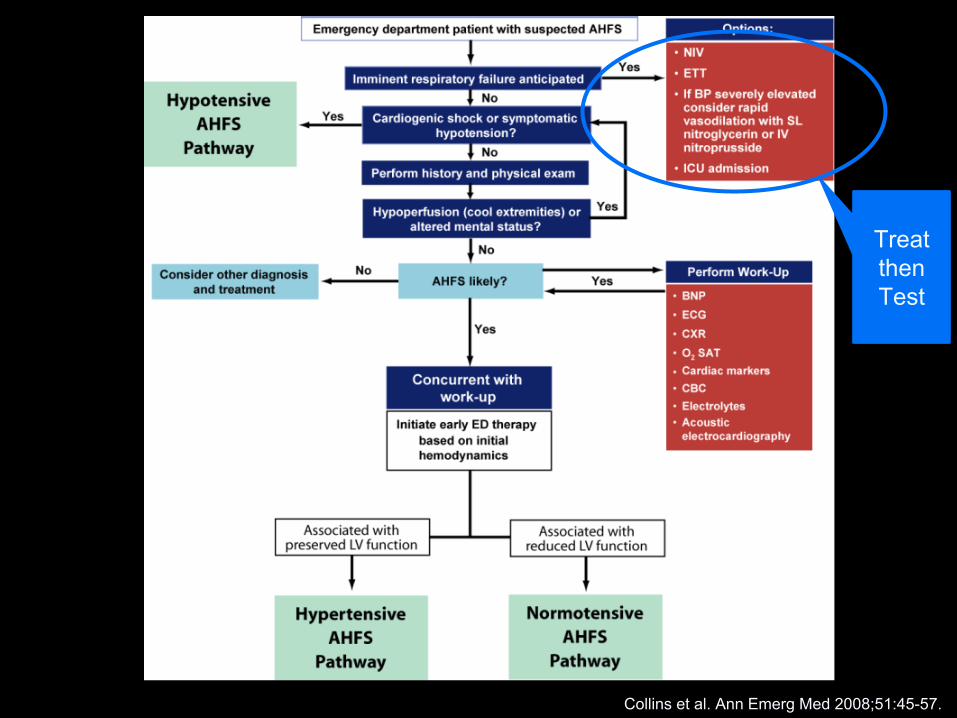
Treat then Test
Collins et al. Ann Emerg Med 2008;51:45-57.

Q: All of the following are true about Non-invasive ventilation except:
• a) It improves acidosis• b) It improves work of breathing• c) It decreases overall mortality • d) It is relatively easy to apply

Non-invasive Ventilation - A Therapy
• Consider if acute respiratory distress– CPAP: continuous positive airway pressure 1,2
• Reduction in need for ETI by 26 %• Trend towards ↑ survival
– BiPAP: bilevel positive airway pressure 3,4,5
• ↓ time to symptom resolution (30 vs. 105 min)• ↓ intubation rate (~ 23 %)
1 Berstein et al. NEJM 1991;325.2 Pang et al. Chest 1998;114.3 Masip et al. Lancet 2000;3564 Levitt MA. J Emerg Med 2001;21.5 Nava et al. Am J Resp Crit Care Med 2003;168

Collins S. Ann Emerg Med 2006;48:260-69
Prevents Intubation in ED Patients
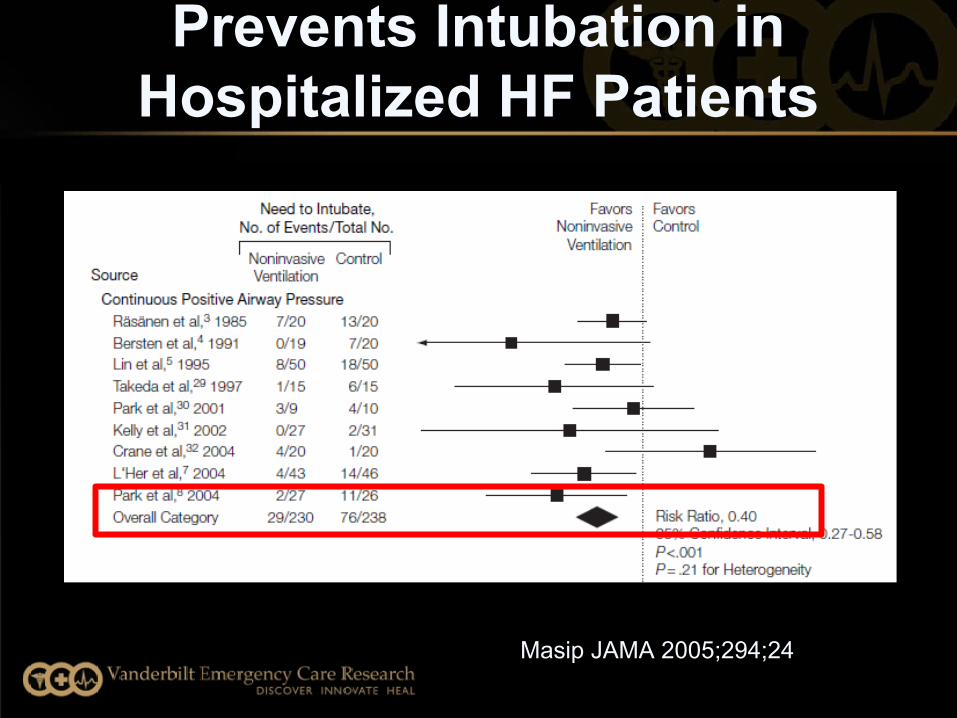
Prevents Intubation in Hospitalized HF Patients
Masip JAMA 2005;294;24
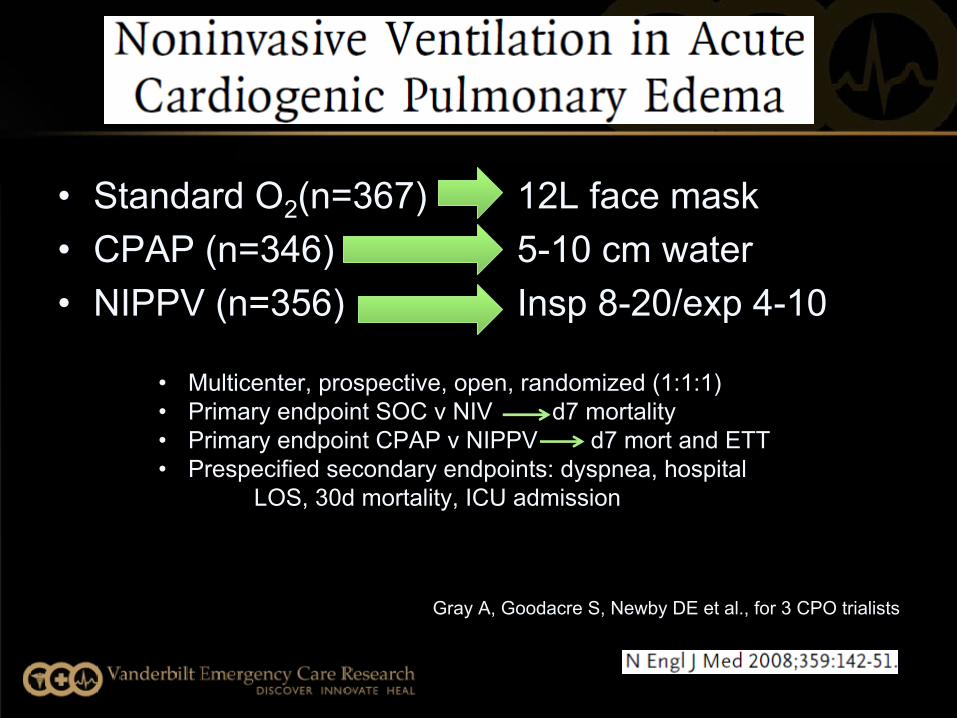
12L face mask 5-10 cm water Insp 8-20/exp 4-10
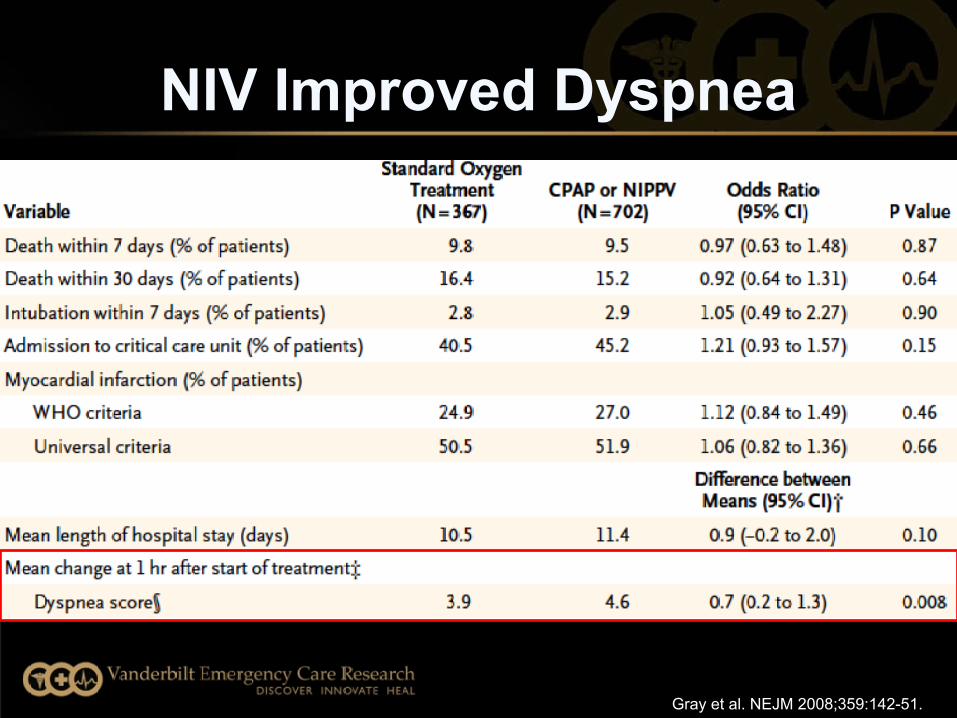
• Standard O2(n=367)• CPAP (n=346)• NIPPV (n=356)
Gray A, Goodacre S, Newby DE et al., for 3 CPO trialists
• Multicenter, prospective, open, randomized (1:1:1)• Primary endpoint SOC v NIV d7 mortality• Primary endpoint CPAP v NIPPV d7 mort and ETT• Prespecified secondary endpoints: dyspnea, hospital
LOS, 30d mortality, ICU admission

Gray et al. NEJM 2008;359:142-51.
Gray et al. NEJM 2008;359:142-51.
NIV Improved Dyspnea
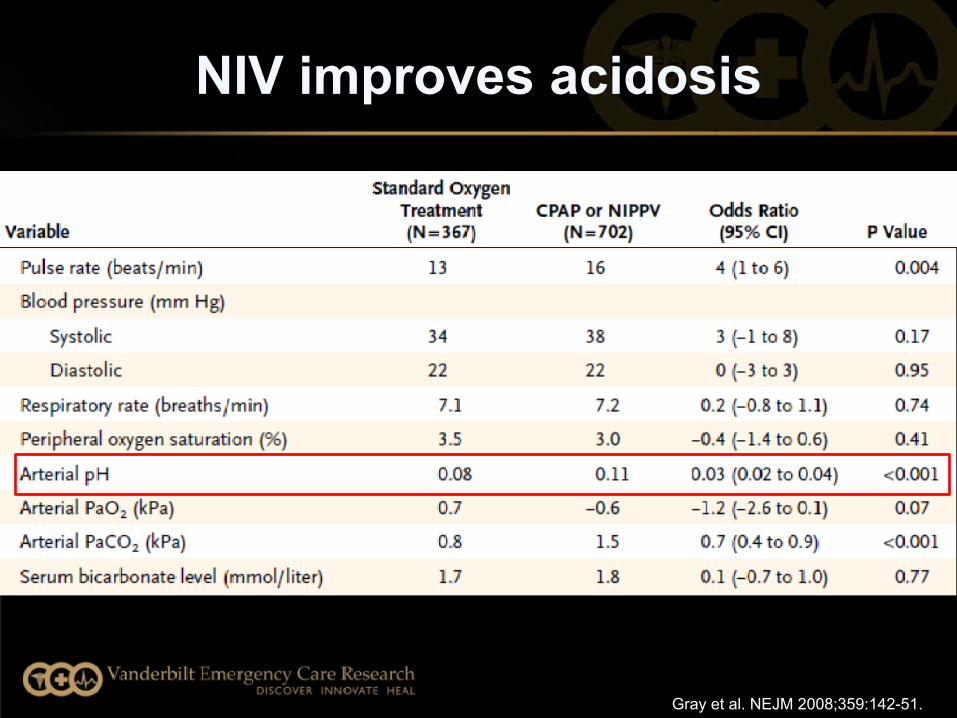
NIV improves acidosis
Gray et al. NEJM 2008;359:142-51.
Gray A, Goodacre S, Newby DE et al., for 3 CPO trialists
• No difference in tracheal intubation (overall rate 2.8%)
• No increase in MI in NIV
• No mortality benefit• Earlier improvement
of dyspnea
Take home points:
-May not save lives-Improves symptoms and resp
distress-Provides time for other therapies
to be started

• Q: T/F: High-dose IV Nitrates have been used safely in the prehospital and ED environment for AHF
• A) True• B) False

High-Dose Ntg for Hypertensive Pulm Edema
• Entry criteria– Systolic BP 160 mmHg or MAP 120– Failed initial tx: O2, SL Ntg x 3, furosemide
• Protocol– 2 mg IV Ntg bolus, titration and repeat q3 mins– May repeat x 10
Levy Ann Emerg Med 2007 Aug; 50(2)
20,000 μgm30 mins
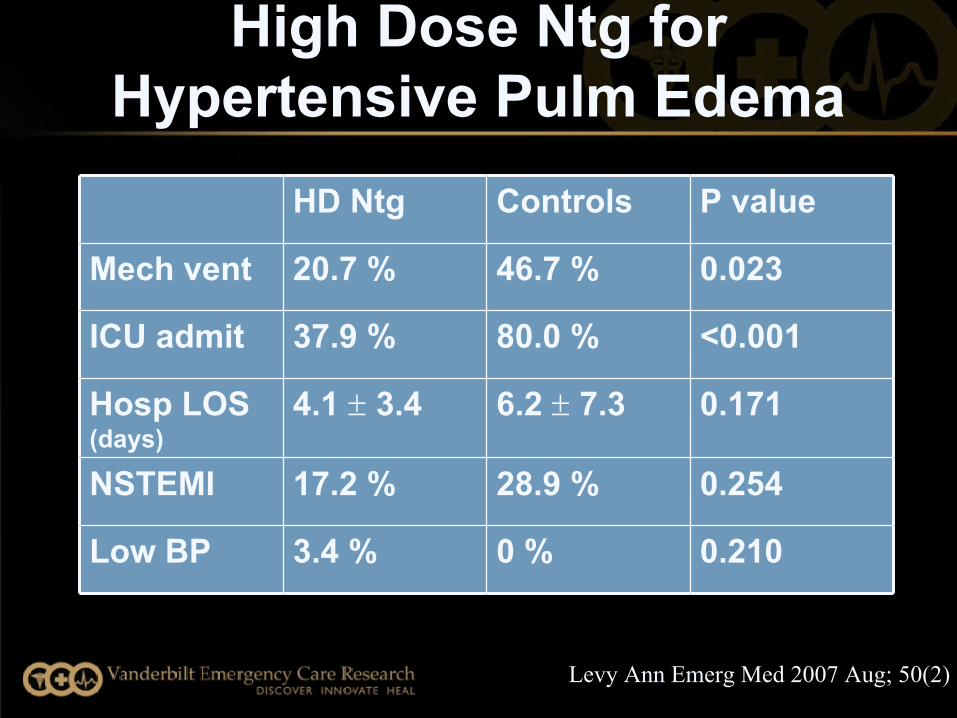
HD Ntg Controls P value
Mech vent 20.7 % 46.7 % 0.023
ICU admit 37.9 % 80.0 % <0.001
Hosp LOS (days)
4.1 3.4 6.2 7.3 0.171
NSTEMI 17.2 % 28.9 % 0.254
Low BP 3.4 % 0 % 0.210
Levy Ann Emerg Med 2007 Aug; 50(2)
High Dose Ntg for Hypertensive Pulm Edema

• IV ISDN 3 mg q 5 min (n = 52) vs. IV furosemide (N = 52) 80 mg q 15 min– Mean dose ISDN = 11.4 (± 6.8) mg– Mean dose furosemide = 200 (± 65) mg
Cotter et al. Lancet 1998:351:389-3.

How Are Nitrates Usually Dosed?
• Isosorbide dinitrate (ISDN)– Widely used outside the US– Typical range: 1-4 mg/hr
• Increase by 1 mg/hr every 10 min as needed
• Nitroglycerin (NTG)– Nitrate of choice in US– Typical range: 10-20 mcg/min
• Increase 5 mcg/min every 5 min as needed
1 Mebazza et al. Crit Care Med 2008; 36:S129–S139.2 Chatti et al. Heart Fail Rev 2007;12:113-7.3 Kirk et al. Crit Pathways in Cardiol 2008;7:103-10.

ESC Guidelines
McMurray et al. EHJ 2012; 33
2 mg bolus every 3 minutes!
3 mg bolus every 5 minutes!

PRONTO- IV Calcium Channel Blocker
• Open label, randomized 1:1 (CLV vs. SOC)• Acute Heart Failure (AHF) with SBP ≥ 160 mmHg• Primary objective:
– To evaluate the safety and efficacy of clevidipine vs. SOC IV anti-HTNs in ED AHF with hypertension
Peacock Am Heart J 2014 Apr; 167(4):529-36
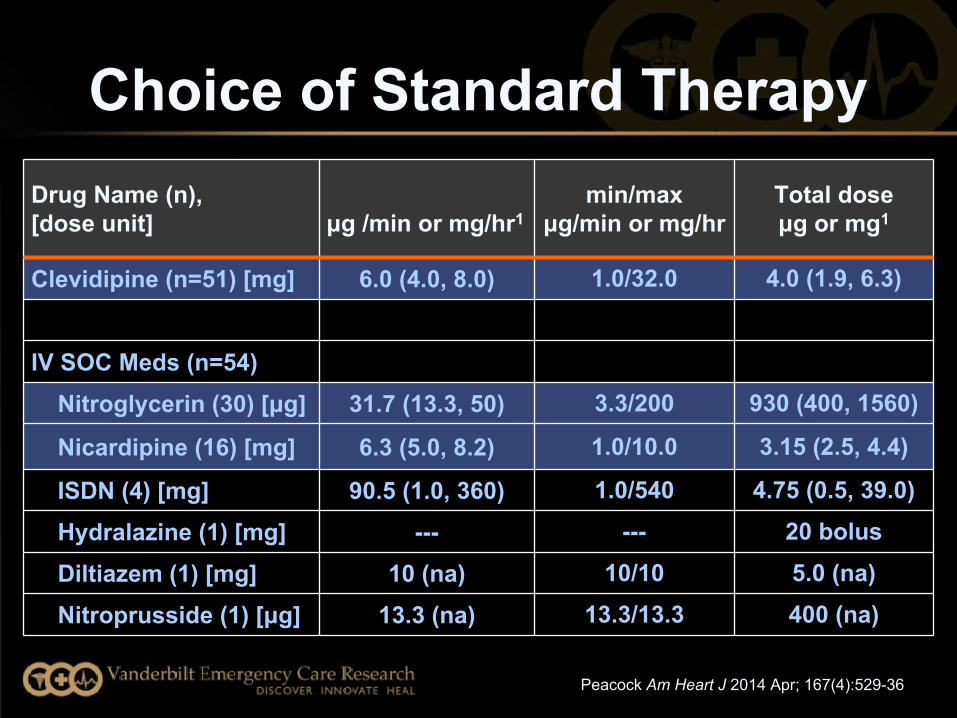
Choice of Standard TherapyDrug Name (n), [dose unit] μg /min or mg/hr1
min/maxμg/min or mg/hr
Total dose μg or mg1
Clevidipine (n=51) [mg] 6.0 (4.0, 8.0) 1.0/32.0 4.0 (1.9, 6.3)
IV SOC Meds (n=54) Nitroglycerin (30) [μg] 31.7 (13.3, 50) 3.3/200 930 (400, 1560)
Nicardipine (16) [mg] 6.3 (5.0, 8.2) 1.0/10.0 3.15 (2.5, 4.4)
ISDN (4) [mg] 90.5 (1.0, 360) 1.0/540 4.75 (0.5, 39.0)
Hydralazine (1) [mg] --- --- 20 bolus
Diltiazem (1) [mg] 10 (na) 10/10 5.0 (na)
Nitroprusside (1) [μg] 13.3 (na) 13.3/13.3 400 (na)
Peacock Am Heart J 2014 Apr; 167(4):529-36

Mean Change in BP
Peacock Am Heart J 2014 Apr; 167(4):529-36

SECONDARY ENDPOINTVAS score over time (Confirmed AHF)
VAS
scor
e, m
m (m
ean
± SE
)
Time From Initiation of Study Medication (hrs)
*** ***
*∆ = -10.4 mm, p = 0.017
** ∆ = -11.7 mm, p = 0.020
*** ∆ = -14.0 mm, p = 0.015
p = 0.037 for treatment x time effect
Peacock Am Heart J 2014 Apr; 167(4):529-36

Safety of BP Reduction Safety
CLV N = 51
SOC N = 53
SAE 12 (24%) 10 (19%)
30-day mortality 3 (%) 2 (%)
Patients with drug–related TEAEs 5 (10%) 7 (13%)
Cardiac 1 (2%) 0 (0%) Respiratory 0 (0%) 0 (0%) Gastrointestinal 2 (4%) 0 (0%) Renal 0 (0%) 0 (0%) CNS (all headache) 1 (2%) 7 (13%)* Vascular 1 (2%) 0 (0%)
p > 0.05 CLV vs. SOC*p > 0.05 CLV vs. SOC

Alexander Am J Emer Med 2015 Feb 133-41
8 on nitrates, 20 on nesiritide
• Hydralazine- 1 study with limitations1
• Enalaprilat - 2 studies- 34 total AHF patients1
• “Evidence Free Zone”
Alexander Am J Emer Med 2015 Feb 133-41

Collins et al, Acad Em Med Jan 2015

Summary: Hypertensive Pulm Edema
• AHF + Significant BP elevation• Early and aggressive treatment improves
symptoms- outcomes??• NIV, Nitrates/vasodilators, Diuretics
• Rapid improvement if hemodynamics addressed early

Thank You
Related Documents











