Hyperosmolar Therapy Alexandra Serafino, PharmD Pharmacy Resident, Intermountain Medical Center, Intermountain Healthcare; Salt Lake City, UT Objectives: • List the more common causes of elevated intracranial pressures (ICP) • Compare and contrast the pharmacokinetics, pharmacodynamics, and therapeutic applications of hypertonic saline and mannitol • Determine if hypertonic saline or mannitol should be used preferentially when given a patient case

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hyperosmolar Therapy
Alexandra Serafino, PharmD Pharmacy Resident, Intermountain Medical Center, Intermountain
Healthcare; Salt Lake City, UT
Objectives: • List the more common causes of elevated intracranial pressures (ICP) • Compare and contrast the pharmacokinetics, pharmacodynamics,
and therapeutic applications of hypertonic saline and mannitol • Determine if hypertonic saline or mannitol should be used
preferentially when given a patient case

SaltyorSweet‐HowDoYouLikeYourBrain?
ALEXANDRA SERAFINO, PHARM.D.
PGY-2 CRITICAL CARE PHARMACY RESIDENT
INTERMOUNTAIN MEDICAL CENTER
MURRAY, UT

Objectives
» List the more common causes of elevated intracranial pressures (ICP)
» Compare and contrast the pharmacokinetics, therapeutic applications, and administration techniques of hypertonic saline and mannitol
» Given a patient case, determine how to appropriately administer hypertonic saline or mannitol and monitor the patient

ElevatedICP
» Increase in ICP >20 mmHg
» A neurologic emergency
» Potentially devastating
Ropper AH, et al. N Engl J Med 2012; 367:746-52.

CausesofElevatedICP
Traumatic brain injuries
Intracranial bleeding
Brain and CNS tumors
Hydrocephalus
Severe ischemic stroke
Ropper AH, et al. N Engl J Med 2012; 367:746-52.

Epidemiology
» Traumatic brain injuryo ~1.4 million sustained annually in the United States
o ~80,000 severe TBI
» Elevated ICP increases morbidity and mortalityo Mortality of 18% for ICP < 20 mmHg
o Mortality of 56% for ICP > 40 mmHg
» Long term disability is common
Treggiari MM, et al. Neurocrit Care 2007;6:104-12.Thurman DJ, et al. J Head Trauma Rehabil 1999;14:602-15.

PathophysiologyofElevatedICP
Ropper AH, et al. N Engl J Med 2012; 367:746-52.
Increased ICP• Cellular injury• Intracranial hemorrhage
Inflection point• Exponential rise in ICP• Vasoconstriction• Impaired gas exchange
Approaches arterial pressure• ICP 50-60 mmHg• Neuronal cell death

ICPInflectionPoint

HyperosmolarTherapies
» Creates an osmolar gradient between the brain and the systemic circulationo Draws “water” from the brain into systemic
circulation
» Rapidly reduces intracranial pressureo Mitigates neuronal cell death
Ropper AH, et al. N Engl J Med 2012; 367:746-52.

PassiveDiffusion
» Brain parenchyma ~ 80% watero Increased responsiveness to changes in water
contentRopper AH, et al. N Engl J Med 2012; 367:746-52.

HyperosmolarTherapies» Should not cross the blood brain barrier (BBB)
» Reflection coefficiento Ability to create an effective gradient
» Hypertonic saline = 1
» Mannitol = 0.9
» More effective in non-injured portions of brain
Ropper AH, et al. N Engl J Med 2012; 367:746-52.Videen TO, et al. Neurology 2001;57:2120-2.

GoalsofTherapy» Decrease ICP Save brain tissue
» Direct ICP monitoring deviceso Goal ICP < 20
o Cerebral perfusion pressures (CPP) ~50-70
» No direct-pressure monitoringo Serum osmolarity
» Initial target of 300-320 mOsm/L
o Serum sodium » Initial target of 145-150 mEq/L
o Titration to effect
Ropper AH, et al. N Engl J Med 2012; 367:746-52.

Sweet‐Mannitol

Mannitol» Mechanism of action
o Osmotic diuretic
o Causes sustained hyperosmolarity via dehydration
» Possible mechanisms for reducing ICPo Intracellular removal of neuronal brain water
o Decreased production of CSF
Ropper AH, et al. N Engl J Med 2012; 367:746-52.Donato T, et al. Anesth Analg 1994; 78:58-66.

Mannitol‐ Dosing
» Suppliedo 20% (20 g mannitol/100 mL solution)
o 25% (12.5 g/50 mL solution)
» Dosingo 0.25 – 1 g/kg body weight
o 1 g/kg initial load
o 0.25-1 g/kg repeat doses q6-8h
Bullock MR, et al. Neurotrauma 2007;24:Suppl 1: S14-S20.

Mannitol‐Monitoring» Serum osmolality: daily or “trough”
» Osmole gap is a better predictor of mannitol clearance
o Recommend gap closure prior to subsequent doses regardless of serum osmolality
Bullock MR, et al. Neurotrauma 2007;24:Suppl 1: S14-S20.
Garcia-Morales EJ, et al. Crit Care Med 2004; 32(4): 986-991.

Mannitol‐ AdverseEffects» Renal failure
o Likely due to Intravascular volume depletion combined with intrarenal vasoconstriction
o > 200 g daily
» Volume contraction alkalosis» Hypokalemia» Hypochloremia» Hyperglycemic, hyperosmolar encephalopathy
o Confusion
o Seizures
Better OS, et al. Kidney Int 1997;52:886-94.Ropper AH, et al. N Engl J Med 2012; 367:746-52.
MannitolAdministration
» Peripheral or central venous catheter
» Can be given IV push
» IV filter must be usedo 0.22 micron in-line filter
» Vials must be drawn up individually and administered

MannitolPearls
» Crystallization occurs at lower temperatureso Store in heated cabinet ≤ 60°Co Allow to cool prior to administration
Crystallization

ManagingExtravasation
» Stop the infusion
» Aspirate any extravasated medication
» Elevation
» Monitor the area
» Apply compresso Warm vs. cold
Goutos I, et al. The Journal of Hand Surgery 2014;39E(8):808–818.

Salty‐ HypertonicSaline
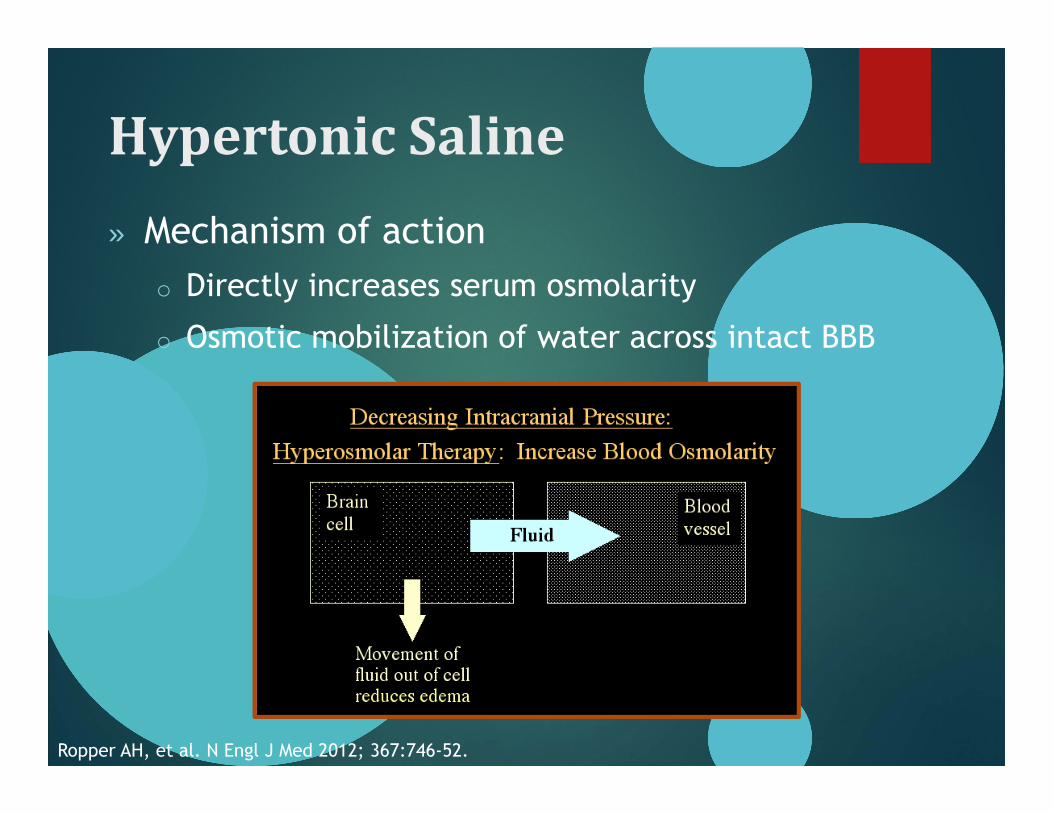
HypertonicSaline» Mechanism of action
o Directly increases serum osmolarity
o Osmotic mobilization of water across intact BBB
Ropper AH, et al. N Engl J Med 2012; 367:746-52.

HTS‐ DoseCalculation
» Estimated Na+ requirements
» Dosingo 1.8% NaCl = 308 mEq/L
o 3% NaCl = 513 mEq/L
o 23.4% NaCl = 4004 mEq/L
» Requires frequent sodium monitoring!

Mannitolvs.HTS
Agent Osmolarity (mOsm/L) Sodium (mEq/L)
0.9% NaCl 308 154
1.5% NaCl 513 256
1.8% NaCl 616 308
3.0% NaCl 1026 513
7.5% NaCl 2566 1026
23.4% NaCl 8008 4004
Mannitol 20% 1098 n/a
**Only ≤900 mOsm/L can be administered peripherally**

IVNaCl vs.NaCl Tablets
Agent Na+ mEq / L
0.9% NaCl 154
3.0% NaCl 513
“Salt Tablets”
1 tablet 1000 mg 17 mEq
154 mEq / 17 mEq = 9 tablets

HTS‐Monitoring
» Signs/symptoms of fluid overload
» Frequent serum Na+ or BMP lab drawso Generally every 4-6 hours
o More frequent monitoring may be necessary with continuous infusions of HTS
o Prevent rapid sodium changes
» Sodium goals may change

HTS‐ AdverseEffects
» Phlebitiso Always infuse HTS > 1.8% NaCl through a central line
» Volume overload
» Hypokalemia, hyperchloremia
» Osmotic demyelination syndromeo Alcoholism, liver disease, hypoglycemia, SIADS
o 22% of all documented cases secondary to HTS» Severe, chronic hyponatremia corrected too quickly
Ropper AH, et al. N Engl J Med 2012; 367:746-52.Kleinschmidt-Demaster BK, et al. J Neuropathol Exp Neurol 2006;65:1-11.

HTS‐ AdverseEffects

Phlebitis
» Preventiono Central vs. peripheral line
o “Good” peripheral» Gauge
» Location
» Management

MANNITOL VS.HYPERTONIC SALINECLINICAL TRIALS

StudiesofMannitolvs.HTS
Mortazavi MM, et al. J Neurosurg 2012; 116:210-21

Hypertonicsalinefortreatingraisedintracranialpressure:literaturereviewwithmeta‐analysis
Mortazavi et al, J Neurosurg 2012

Mortazavi,etalStudy Design Systematic review & Meta-analysis
Studies included HTS for elevated ICP
Studies included (#) 36
RCTs (#) 10
RCTs comparing mannitol to HTS (#)
7
Results1 RCT showed improved GOS at 1-year; 6/7 RCTssuggest improved ICP lowering with HTS vs. mannitol
Conclusions
HTS decreases ICP to a greater extent vs. mannitol, whether used as a bolus or continuous infusion, but has been not shown to improve neurologic outcomes
Mortazavi MM, et al. J Neurosurg 2012; 116:210-21

Mortazavi,etal
Mortazavi MM, et al. J Neurosurg 2012; 116:210-21

Meta‐AnalysesandReviews
» Other meta-analyses have made similar conclusionso HTS is more effective at decreasing ICP
o Limited long-term and neurologic outcome data
» Mean difference in ICP lowering is smallo ~1.5-2.5 mmHg
» Less therapeutic failures with HTS vs. mannitol
Kamel H, et al. Crit Care Med 2011; 39:554-9Hinson HE, et al. J Intensive Care Med 2013; 28(1):3-11Lazaridis C, et al. Crit Care Med 2013; 41:1353-60
Rickard AC, et al. Emerg Med J 2013

Bolusvs.ContinuousInfusion
Mortazavi MM, et al. J Neurosurg 2012; 116:210-21
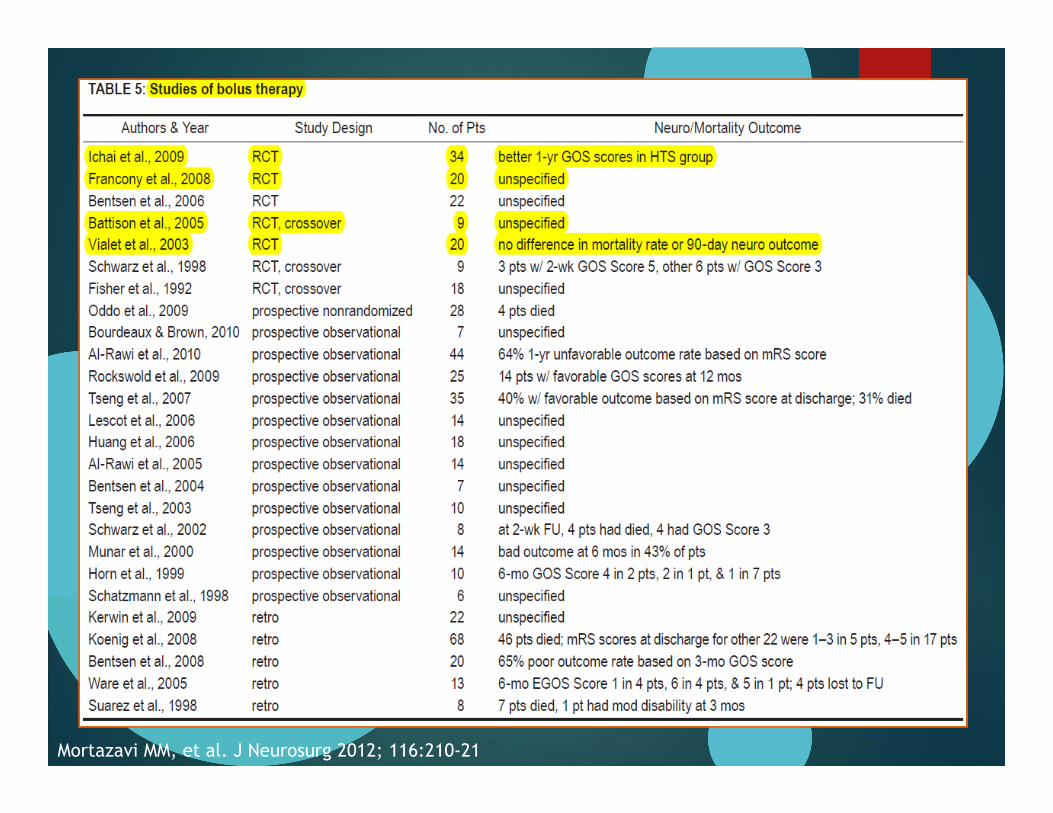
Bolusvs.ContinuousInfusions
Mortazavi MM, et al. J Neurosurg 2012; 116:210-21

Bolusvs.ContinuousInfusion
» No recommendation can be made with regards to continuous infusion vs. bolus mannitol
» Significantly more data on bolus HTS administration
» Available data suggest bolus and continuous infusion HTS is effective at reducing ICP
Mortazavi MM, et al. J Neurosurg 2012; 116:210-21Bullock MR, et al. Neurotrauma 2007;24:Suppl 1: S14-S20.

GuidelineRecommendations
Bullock MR, et al J Neurotrauma. 2007;24 Suppl 1:S14-20

Choices– SaltyorSweet?
» HTS vs. Mannitolo Decreases ICP to a greater extent
o Effects last longer, realized more quickly
o Lower risk of rebound ICP elevations
o Fewer adverse effects
» Clinical outcome data to support the use of one agent over the other is lacking
» Recent study of neurointensivists reports trend in increasing HTS use (55% vs. 45%)
Hays AN,. Neurocrit Care 2011, 14:222-228.

Take‐AwayPoints
» HTS over mannitol in most situations
» Either therapy will require frequent laboratory monitoringo Sodium
o Serum osmolarity
» Watch for adverse effects
» Always use a filter for mannitol
» Central vs. peripheral administration

Questions?
Related Documents











