
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


• 20 month old girl case of wiliam syndrome presented with vomiting and dehydration .
• Found to have hypercalcemia • ca 3.96 mmol/l . urine ca/creat ratio 4.6 high.• PO3:1.45 Vit d 55. PTH 3.6.• This is the 4th episode of hypercaclemia over last 2
months .• Patient started on IV hydration , lasix and steroid • after 48 hr, calcium reach 2.6 mmol/l steroid stopped • Ca level start to increase again reaching 3.5 mmol/l
so steroid resumed • ca level maintained below 3 .

• Hypercalcemia is less common in children than in adults.
• It is more likely to be clinically significant in younger patients
• the aetiologies are diverse and age specific.
• Hypercalcaemia is a serious condition that can leads to end-organ damage.

• Normal serum levels of calcium are maintained through the interplay of parathyroid, renal, and skeletal factors.
• a key part of the management is to establish the correct diagnosis promptly.
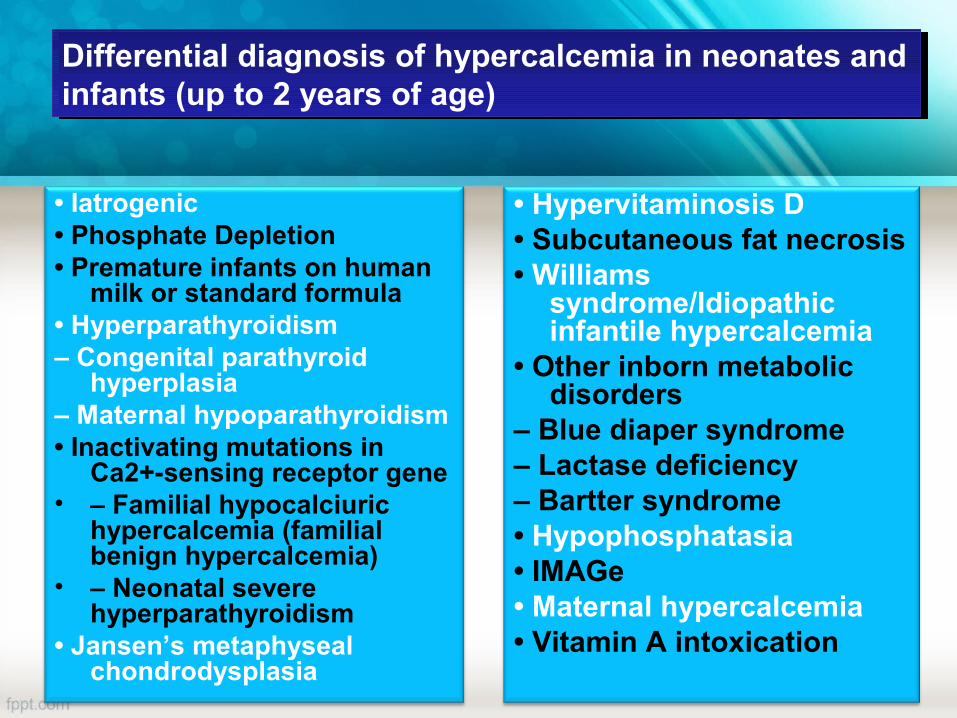
• Iatrogenic• Phosphate Depletion• Premature infants on human
milk or standard formula• Hyperparathyroidism– Congenital parathyroid
hyperplasia– Maternal hypoparathyroidism• Inactivating mutations in
Ca2+-sensing receptor gene• – Familial hypocalciuric
hypercalcemia (familial benign hypercalcemia)
• – Neonatal severe hyperparathyroidism
• Jansen’s metaphyseal chondrodysplasia
• Hypervitaminosis D• Subcutaneous fat necrosis• Williams
syndrome/Idiopathic infantile hypercalcemia
• Other inborn metabolic disorders
– Blue diaper syndrome– Lactase deficiency– Bartter syndrome• Hypophosphatasia• IMAGe• Maternal hypercalcemia• Vitamin A intoxication
Differential diagnosis of hypercalcemia in neonates and infants (up to 2 years of age)Differential diagnosis of hypercalcemia in neonates and infants (up to 2 years of age)

• Excessive calcium intake
• Parenteral nutrition
• Hyperparathyroidism
♦ adenoma/carcinoma
– Genetic primary
♦ autosomal dominant/récessive FHH
♦ familial
♦ MEN types I and IIa
♦ Hyperparathyroidism-Jaw tumor
– Autonomous (tertiary)
• Hypervitaminosis D
– Excessive intake
– Granulomatous diseases: cat scratch fever; sarcoidosis; tuberculosis; histoplasmosis; coccidiomycosis; leprosy; HIV
– Chronic inflammatory disorders
• Immobilization• Malignancy associated hypercalcemia– Primary bone tumors– Metastatic tumors with osteolysis– Tumors secreting PTHrP, • Hepatic disease• Hyperthyroidism• Adrenal insufficiency• Pheochromocytoma• Drugs (thiazides, lithium, systemic retinoid derivatives,)• Chronic renal failure
Differential diagnosis of hypercalcemia in neonates and infants (over 2 years of age)Differential diagnosis of hypercalcemia in neonates and infants (over 2 years of age)

Nervous system
Behavioural changes
Headache
Hallucinations
Unsteady gait
Muscle hypotonia,
Proximal muscle
weakness/
myopathy
Seizures
Irritability/confusion
Encephalopathy, Coma
Renal systemRenal stonesnephrocalcinosis, Polyuria and polydipsiaRenal failureMusculoskeletalBone painEctopic calcificationMiscellaneousConjuctivitisBand keratopathyfailure to thriveArrhythmiacardiomyopathy
Gastrointestinal systemParalytic ileusAbdominal crampingConstipationAnorexiaNauseaVomitingPancreatitis

• History• Symptoms suggestive of hypercalcaemia• Symptoms suggestive of malignancy• Drug history, including vitamin D therapy, • Family history of renal stone, hypercalcaemia,
parathyroidectomy, multiple endocrine neoplasia
• Examination• Assess degree of dehydration• Syndromic features• Presence of ectopic/subcutaneous calcification/rash• Generalised lymphadenopathy, organomegaly• Bone pain, fractures

• investigations • Bone profile, PTH, urine ca.• Investigation of parents for abnormalities
of calcium homeostasis• Imaging:• Renal ultrasound scan• Skeletal survey• Parathyroid gland ultrasound scan• Parathyroid gland SestaMIBI scan

• The management of hypercalcemia depends on the severity and cause of the elevation of serum Calcium.

• Patients with asymptomatic or mildly symptomatic hypercalcemia (calcium <12 mg/dL [3 mmol/L])
• no initial treatment may be necessary .• medical efforts to reach a diagnosis
should be given the preference.

• When hypercalcemia is severe (total serum calcium >14mg/dL) (3.5 mmol/L) .
• Or when there are symptoms .
• Discontinuation of calcium supplements• Discontinue medications that
independently lead to hypercalcaemia, e.g. thiazides, vitamin D, calcitriol
• Increase the weight bearing mobility of the patient

• low calcium formula in the infant .
• Low calcium diet in the older child.

Treatment of underling cause


• Filtered calcium is principally reabsorbed in the proximal tubule and the ascending loop of Henle.
• This process is mainly passive.• whereas active resorption of calcium occurs in the
distal loop under the influence of PTH and to a lesser degree 1,25(OH)2D.
• Proximal reabsorption is inhibited by volume expansion from intravenous saline infusion, which increases delivery of sodium, calcium and water to the loop of Henle.
• administration of a loop diuretic such as furosemide then blocks transport at loop of henle

• Initial treatment of hypercalcemia involves hydration to improve urinary calcium output.
• Isotonic sodium chloride solution is used.• MOA: to increase the glomerular filtration
rate , increasing sodium excretion increases calcium excretion.
• Volume expansion with isotonic saline at 1.5–2.5 maintenance.

• MOA: inhibit the reabsorption of calcium, especially in the presence of sodium, further promoting calciuresis.
• Furosemide :• 1–2 mg/kg/d, as divided doses every 4–6
hours.• 1mg/kg every six hours.• It works within hours and can lower serum
calcium levels by 1-3 mg/dL within a day.

• If hypercalcemia does not respond to initial measures, agents that block bone-resorption may be useful as adjuvant therapy.
• Insome cases, hypercalcemia is due osteoclastic bone resorption.
• agents that inhibit or destroy osteoclasts will be effective treatments.

• MOA:• 1- increasing renal calcium excretion .• 2- by decreasing bone resorption via
interference with osteoclast function• works within hours.• lowering the serum calcium concentration
by a maximum of 1 to 2 mg/dL (0.3 to 0.5 mmol/L)
• only for 2-3 days because of tachyphylaxis

• given at doses of 2–4 IU/kg SC/IM .• If a hypocalcemic response is noted, then the
patient is calcitonin-sensitive and the calcitonin can be repeated every 6 to 12 hours.
• it is useful in combination with hydration for the initial management of severe hypercalcemia
• Can be administer along with a bisphosphonate

• is safe and relatively nontoxic • Adverse effects : nausea, abdominal pain,
and flushing.• One benefit of calcitonin is that it has
analgesic properties.

• nonhydrolyzable analogs of inorganic pyrophosphate .
• MOA: inhibit calcium release by interfering with osteoclast-mediated bone resorption by inhibit ing osteoclast action and inducing osteoclast apoptosis
• Helpful when hypercalcemia is primarily driven by the mobilization of calcium from bone as in cases:
• 1-tumor induced hypercalcemia.• 2- immobilization. • 3-vitamin D intoxication • 4- primary hyperparathyroidism

• they are more potent than calcitonin and saline for patients with moderate or severe hypercalcemia .
• Their maximum effect occurs in two to four days• The lowering of serum calcium levels can be of
days to weeks duration
• The nitrogen-containing bisphosphonates, including :
• alendronate, ibandronate, pamidronate, risedronate, and zoledronic acid,

• the most potent inhibitor of bone resorption identified to date.
• 0.025-0.05 mg/kg intravenously IV over 30-45 minutes.
• is superior to pamidronate in reversing hypercalcemia related to malignancy

• Bisphosphonates are extremely effective in children with moderate to severe hypercalcaemia
• 0.5–1 mg/kg/dose of pamidronate as an IV infusion over 4–6 h
• they decrease serum calcium in 2-4 days with a nadir at 5-7 days.
• may last for 2–4 weeks

Pamidronate
• Side effects:
• Fever, arthralgias, myalgia, fatigue, bone pain.
• hypocalcemia, hypophosphatemia, and hypomagnesemia.
• Uveitis.
• impaired renal function, nephrotic syndrome
• osteonecrosis of the jaw*.
• Neridronic acid is an IV/intramuscular (IM) bisphosphonate currently licensed in Europe; some pediatric data are available, including some in neonates.

Decrease Intestinal Calcium Absorption
• Glucocorticoid • MOA: • prevent renal calcium reabsorption• inhibit the production and activity of 1,25(OH)2D, thus
decreasing intestinal calcium absorption
• Uses:• vitamin D intoxication.• in patients with chronic granulomatous diseases (eg,
sarcoidosis) .• patients with lymphoma.• Idopathic infantile hypercalcemia.

• Prednisone at 1–2 mg/kg/d (or 20–40 mg/m2/d), given as divided doses every 4-12 hours
• Hydrocortisone 1mg/kg dose 12 hourly.
• dexamethasone 0.4 mg/kg/day
• onset of action is expected within 24–72 hours.
• Steroids can be combined with calcitonin

• Cinacalcet • MOA: It changes the configuration of the
transmembranal calcium-sensing receptor on chief cell of parathyroid gland in a manner that makes it more sensitive to serum calcium.
• lowers PTH levels• Also results in concomitant decrease of
serum calcium levels by affecting renal reabsorption.

• Uses:• NSHPT• chronic renal disease and secondary
hyperparathyroidism.

• can be used in life-threatening cases .• particularly in patients with renal failure• haemodialysis is more effective than
peritoneal dialysis at lowering calcium levels.

• is recommended for all children with primary hyperparathyroidism.
• Including NSPHT.• Subtotal parathyroidectomy can be
performed, or complete parathyroidectomy can be chosen with reimplantation of a small amount of tissue in the forearm.
• Neonatal severe hyperparathyroidism requires total parathyroidectomy

Intervention Mode of actionOnset of action
Duration of action
Isotonic salineRestoration of intravascular volumeIncreases urinary calcium excretion Hours
During infusion
CalcitoninInhibits bone resorption via interference with osteoclast functionPromotes urinary calcium excretion
4 to 6 hours
48 hours
Bisphosphonates
Inhibit bone resorption via interference with osteoclast recruitment and function
24 to 72 hours
2 to4 weeks
Loop diureticsIncrease urinary calcium excretion via inhibition of calcium reabsorption in the loop of Henle
HoursDuring therapy
Glucocorticoids
Decrease intestinal calcium absorptionDecrease 1,25-dihydroxyvitamin D production by activated mononuclear cells in patients with granulomatous diseases or lymphoma
2 to 5 daysDays to weeks
CalcimimeticsCalcium sensing receptor agonist, reduces PTH (parathyroid carcinoma, secondary hyperparathyroidism in CKD)
2 to 3 daysDuring therapy
Dialysis Low or no calcium dialysate Hours During treatment


• A 2-year-old girl presents to the emergency department with abdominal pain, constipation, and vomiting without fever. The parents report that she lost her appetite in the last few days and has been drinking and urinating more than usual. Physical examination reveals an elevated blood pressure of 137/89 mm Hg; there is mild diffuse tenderness of the abdomen. Her dietary history is unremarkable except for the fact that she does not like to drink milk, so for several weeks she has been taking 1 mL of a liquid cholecalciferol (vitamin D3) preparation that her parents purchased through the Internet. When you ask to see the bottle, you note that the concentration is 5000 IU cholecalciferol per milliliter.

• Laboratory test results:• Calcium = 14.7 mg/dL (3.68 mmol/L) (reference
range: 8.5-10.5 mg/dL [2.13-2.63 mmol/L])Phosphorus = 5 mg/dL (1.6 mmol/L) (reference range: 3.6-6.0 mg/dL [1.2-1.9 mmol/L])Intact PTH, undetectable25-Hydroxyvitamin D = 109 ng/mL (20-68 ng/mL) (272.1 nmol/L [49.9-169.7 nmol/L])1,25-Dihydroxyvitamin D = 82 pg/mL (15-75 pg/mL) (213.2 pmol/L [39.0-195.0 pmol/L])Intravenous normal saline is initiated, and the parents are instructed to discontinue the vitamin D supplement.

• Which one of the following statements about vitamin D metabolism is true?
A. Vitamin D is predominantly cleared by the kidneys, allowing for quick correction of hypercalcemia once the drug is discontinued
B. 1,25-Dihydroxyvitamin D has a long half-life, which will result in prolonged hypercalcemia even after the cholecalciferol is discontinued
C. 25-Hydroxyvitamin D has a short half-life, so the effects of the overdose will be quickly reversed once the drug is discontinued
D. Cholecalciferol has a large volume of distribution, which can result in prolonged hypercalcemia
E. Most 25-hydroxyvitamin D will be converted to 24,25-dihydroxyvitamin D, allowing for rapid correction of the hypercalcemia

• A 10-year-old girl presents to her pediatrician with severe back pain after falling while kicking a soccer ball. Radiographs show severe osteopenia and multiple compression fractures throughout the thoracic spine. Upon questioning, the family reports she has been fatigued for the past several months and has had worsening constipation over the past few weeks. Laboratory workup shows the following:
• Calcium = 13.5 mg/dL (3.38 mmol/L) (reference range, 8.8-10.8 mg/dL [2.2-2.7 mmol/L])

• Phosphorus = 3.8 mg/dL (1.2 mmol/L) (reference range, 4.0-5.5 mg/dL [1.3-1.8 mmol/L])Spot urine calcium-to-creatinine ratio = 1.8 mg/mg (reference range, <0.2 mg/mg)25-Hydroxyvitamin D = 80 ng/mL (199.7 nmol/L) (reference range, 20-80 ng/mL [49.9-199.7 nmol/L])White blood cell count = 28,000/µL (28.0 x 109/L) (reference range, 4300-10,800/µL [4.3-10.8 x 109/L])Hemoglobin = 8.4 g/dL (84 g/L) (reference range, 12.0-16.0 g/dL [120-160 g/L])Platelet count = 105 x 103/μL (105 x 109/L) (reference range, 150-400 x 103/μL [150-400 x 109/L])PTH = <3 pg/mL

• Which of the following is the most likely etiology of this patient’s hypercalcemia?
• CHOOSE ONE• A. An inactivating mutation in the gene encoding
the calcium-sensing receptor • B. Increased intestinal calcium absorption • C. Destruction of bone tissue by invasion from
tumor cells• D. Increased production of 1,25-dihydroxyvitamin
D • E. Activation of the PTH-1 receptor

• You are asked to consult on a 1-month-old infant in the neonatal intensive care unit with hypercalcemia. He was delivered by emergency cesarean section due to placental abruption and fetal heart decelerations. He was floppy, cyanotic, and unresponsive at delivery and required prolonged resuscitation. He was intubated immediately and put on a cooling regimen at 2 hours after birth. On his fifth day, he developed a rash on his back (Figure). The rash resolved over the next 2 weeks.


• He remains intubated. He has had normal laboratory study results until yesterday, when his serum calcium was elevated at 12.7 mg/dL (3.17 mmol/L).
• Of the following, in contrast to patients with hypercalcemia resulting from immobilization, your patient would MOST likely be expected to have
• A. higher parathyroid hormone set point • B. hypercalciuria • C. increased calcitriol synthesis • D. increased osteoclastic activity • E. reduced osteoblastic activity

• You are seeing a 16-year-old adolescent in your clinic with hypercalcemia. She had been seen in the urology clinic previously with repeated episodes of nephrolithiasis, and was found to have a serum calcium concentration of 10.8 mg/dL (2.7 mmol/L). She is a student in school and when seen in your clinic her height is 162 cm and her weight is 75 kg. She has normal facies. Her general physical examination is also normal.
• You obtain the following laboratory studies: • Phosphate 3.1 mg/dL (1.0 mmol/L) (RR 0.8-1.45
mmol/L) • PTH 8 pg/ml (RR 15-65 mmol/L) • 24 hour urine calcium: 400 mg/24 hours

• Of the following genetic tests, the MOST likely to be positive in this patient is
• A. activating PTHR1 (PTH/PTHrP receptor) mutation
• B. compound heterozygous inactivating CYP24A1 (24-hydroxylase) mutations
• C. dominantly inherited CDC73 (parafibromin) mutation
• D. hemizygous 7q11.23 deletion including general transcription factor IIi
• E. heterozygous gain of function CASR (calcium sensing receptor) mutation
• A 9 year old girl presents with confusion, vomiting and abdominal pain .she is tachycardia. On blood tests, her creatinine is 1.8 mg/dl, BUN 45, and her calcium is 14.2 mg/dl. what is th most appropriate initial management.
• 1- furosemide 1mg/kg IV.• 2-pamidronate 0.5-1 mg/kg.• 3-isotonic saline bolus IV.• 4-calcitonin SC.• 5- dietary calcium restriction.

• Treatment with a bisphosphonate can cause which adverse effects?
• 1- hypocalcemia and hyperphosphatemia.• 2- hypophosphatemia and vit d defciency.• 3- flu like symptoms and hypocalcemia.• 4- ostonecronesis of jaw and vitamin d toxicity.• 5-erosive esophagitis and
hypoparathyrodisim.

• A 16 year old male was found to have hypercalcemia during an admission for appendicitis he has been generally healthy , and has not had any fractures ,or kidney stones. His father had two failed parathyroidectomies. And his 26 year old sister also had a parathyroidectomy but still has high calcium .there are no other endocrine disorder in his family .
• His exam is unremarkable. His laboratory tests include : ca 11mg/dl (2.8 mmol/l), phosph 2.5 mg/dl (0.83 mmol/l), ALK 122 , 25hydroxy vit d 44 ng/ml (109.8), 1,25(OH)2 vitamin d and creatinine normal and his urine calcium is 40mg/24hr. PTH is 75 pg/ml (normal 10-65 pg/ml)

• what is the most appropriate next step management?
• 1- referral to surgery for parthyroidectomy..
• 2- IV bisphosphonate.• 3- calcium restricted diet• 4- no specific treatment.• 5- oral bisphosphonate.

• A 26 year old woman gives birth to a full-term baby girl. She feeds poorly, vomits and becomes lethargic in the neonatal period . Family history is notable for multiple family member s with mild hypercalcemia despite attempted parathyroidectomy including mother whose calcium is 11mg/dl (2.8 mmol/l) .the infant tachycardic, and dose not have dysmorphic features. Otherwise exam is unremarkable.
• Her cbc normal ,ca is 17 mg/dl (4.3mmol/l) phosphorus 4.2 mg/dl (1.4mmol/l) creatinine is 1.7 mg/dl and PTH is 425pg/ml .she is started on IV fluids

• Which of the followinf best charactizes her disorder?
• 1- parathyroidectomy can be life saving.• 2- her mother is vitamin D toxic causing baby
hypercalcemia.• 3- the baby is profoundly vitamin D deficient
causing secondary hyperparathyrodisim.• 4-The baby father is carrier for inactivating
vitamin d receptor mutation • 5- no specific treatment is required.

• In counseling about pamidronate therapy , which one of the following is correct?
• A-patient may experience bone pain because pamidronate is a potent stimulator of osteoblasts.
• B- regular dental evaluation are important because ostonecrosis of the jaw is a frequent complication of pamidronate therapy in children.

• C-Future fertility may be compromised because pamidronate has a half life of many years.
• D- hypocalcemia can occur during treatment.
• E- esophagitis can be avoided by remaining upright for 30 min after the pamidronate infusion.

• A 6 year-old , previously healthy boy was in motor vechile crash 6 weeks ago , resulting in a spinal cord injure and paraplegia. He has been living in resdintal rehabilitation facility reciving daily physical therapy . He consumes a regular oral diet including one can of pediatric nutrinional drink daily.his calcium intake is estimated to be 1000mg daily and his vitamin D intake is 600 IU daily . Over last 2 weeks his caregiver have noticed decreased appetite, nausea and increased urination.

• Laboratory test result: • Electrolyte normal• BUN 18 mg/dl (5-18)• Cretinine 0.5 mg/dl (0.16-0.39)• Calcium 13.1 mg/dl (8.5-10.5 mg /dl)• Intact PTH <3 pg/ml (16-65)• ALK 126 (129-291)• 25 hydroxy vitamin d 52.2 ng/ml (25-80)• Which of the follwing best explaines this
patient’s hypercalcemia?

• A- suppresed PTH secretion inhibiting urinary calcium excretion.
• B- increased one alph hydroxylase activity in kideny.
• C- excessive dietry calcium and vitamin d intake.
• D- increased bone resorption resulting in skeletal release of calcium .
• E- ectopic PTH related protien secretion induced by spinal cord inflammation.

• A 10 month old girl presents to the pediatrician with poor weight gain .she was the product of full term .uncomplicated pregnancy and delivery except for birth weight of 2200 g (-2.8SD) no infectious causes for intrautrine growth retardation were idintified and she was discharged to home at 3 days of age. She was formula fed 4 ounces every 3 hours, but she has not tolerated solid food because of swallowing problem she takes no medication her parents describe her as being otherwise well with only mild delay in developmental mile stones

• On physical she appears irritable and weak with decreased muscle tone and normal vital signs. Weight is 6.5 kg (-3SD), length is 61.5 cm (-3.5SD), head circumference is 41.5 (-3.5SD), facies are remarkable for upslanting palpebral fissure,epicanthal folds,shallow nasal bridge, long philtrum ,wide mouthand micrognathia.

• Lab:• Ca 20 mg/dl (8-10.5)• Phosphorus 4.5 mg/dl (3.2-6.3)• Creatinin 0.6 mg/dl (0.2-0.4 mg/dl)• Urinary calcium to creatinine ratio 1.9 (<0.6)• PTH 13.4 pg/ml (16-87)• ALK 186• 25 hydroxy vit d 31ng/ml • 1.25 hydroxy vit d <8 ng/ml (24-86 ng/ml)

• Cardiac evalution demonestrate peripheral pulmonic stenosis, renal us shows bilatral mild echogencity of medullary pyramids chromosomal microarray reveals 1.4-Mb contiguous gene deletIon in 7 q11.23
• At age of 7 years this child will most likely exhibit which of the following?
• A-hypercalcemia.
• B- immune deficency.
• C- thrombocytopenia.
• D-Renal insufficency
• E- normocalcemia.

• Which of the folowing is true about bisphosphonates?
• A-in excess, they paradoxically decrease bone density.
• B-they are administered by deep IM injection.• C- they act by incorporating into bone marrow
precurser cells, thus prolonging their life span.
• D-they augment bone mineralization by increasing osteoblastogenesis.
• E- they are retained in bone for many years.

• Which of the following describe the william-beuren syndrome of infantile hypercalcemia?
• A- chactrized by mitral valve prolapse , extremely fine facial features and overgrowth.
• B- it is realted to loss of function of BAZ1B.• C- it is the result of increased functional activity of
WINAC (WSTF)• D- it is dependent on increased activity of hepatic
25 hydroxylase.• E- it is transmitted as a sex linked recessive trait.

• A 13 year old girl presents with fatigue, cough dyspnea and ployurea. She is tachycardic and her blood pressure is 87/46 . She has joint swelling and wheezes on exam. She has lymphadenopathy on chest radiographs. Her laboratory test result are:
• Total calcium 13.4 mg/dl (3.4mmol/l)• Phosphorus 4.2 mg/dl (1.4 mmol/l)• Creatinine 2.1 mg/dl (168 ummol/l)• PTH <5pg/ml (<0.53 pmol/l)• 1,25 dihydroxy vitamin D 112pg/ml (291 pmol/l)

• What is true about appropriate intial management of hypercalcemia in this patient?
• A- diuretics alone will be effective for mangement.• B- treatment with an IV bisphosphonate can
acutely worsen renal function.• C- urgent parathyroidectomy is required and can
be life saving• D- an IV bisphosphonate will begin to lower
serum calcium faster than calcitionin• E- isotonic saline should be given only after
bisphosphonate have safely lowered the calcium.
• You are evaluting a patient with hypercalcemia associated with an increased PTH level. Before referring your patient to a parathyroid surgeon , you remember from studies for the board examination that you need to exclude FHH as acause of benign nonoeprative hyperparathyrodism . You also remember that the cutoff for diagnosis of FHH is calcium creatinine clearence ratio of less than 1%.as happen most of the time in real life and not on exam , the results come back with CaCl/CrCl ratio of exactly 1%

• What is the quickest ,easiest , and least expensive way to make the diagnosis of FHH?
• A- check serum calcium of patients parents.• B- send DNA for mutation analysis of CaSR
gene.• C- assess whether calcium loading is able to
suppress PTH.• D- measure urinary cyclic AMP in response
to PTH infusion.

• At the insistence of her mother, a 12 year old girl is referred to you by her primary care physician following a pathologic fracture of her left proximal femur. The mother has done extensive research in internet and insist that you do gene testing to diagnose her daughters disorder her physical examination is normal except for a large ragged bordered hyperpigmentated macular lesion extending from her midline toward her right shoulder.

• You decide to biopsy an area of affected tissue to test for mutation in which of the following gene?
• A- CASR.• B-GNAS• C- neurofibromin• D- menin

MCQ 17MCQ 17
• A 14-year-old, previously healthy white girl presents with clinical and biochemical features of pancreatitis and nephrolithiasis at an outside hospital.
• She has a history of a 25-lb weight loss and has been trying to lose weight.

• serum calcium level of 15.0 mg/dL (3.75 mmol/L), • serum phosphorous of 2.2 mg/dL (0.71 mmol/L), • serum magnesium of 1.3 mg/dL. • She has normal blood urea nitrogen of 14
mg/dL(5 mmol/L) • serum creatinine of 0.6 mg/dL (53.04 μmol/L). • Her serum 25-hydroxyvitamin D concentration is
9 ng/mL (22 nmol/L).• Her 125-hydroxyvitamin D concentration is 118
pg/mL (307 pmol/L).

• Of the following, the MOST likely reason for her hypophosphatemia is
• A. inadequate dietary phosphate
• B. primary hyperparathyroidism
• C. refeeding syndrome
• D. tertiary hyperparathyroidism
• E. vitamin D deficiency

MCQ 18MCQ 18
• A 3-day-old newborn presents with lethargy, poor suck, and vomiting. The mother’s pregnancy was uneventful and there was no history of maternal illness. The newborn’s physical examination is unremarkable.

• Laboratory evaluation showed the following:
• PTH, 80 pg/mL
• Total calcium, 14.0 mg/dL
• Ionized calcium, 7.1 mg/dL
• Phosphorus, 1.3 mg/dL
• 25 hydroxyvitamin D, 30 ng/dL
• 1,25-dihydroxyvitamin D, 72 ng/mL
• Urine calcium/creatinine ratio, 0.3

• Of the following, the MOST likely cause of this newborn’s hypercalcemia is
• A. heterozygous inactivating mutations of the calcium-sensing receptor
• B. homozygous activating mutations of the calcium-sensing receptor
• C. homozygous inactivating mutations of the calcium-sensing receptor
• D. maternal hyperparathyroidism
• E. maternal hypocalcemia

MCQ 19MCQ 19
• 3 year old boy presented with loss of mandibular incsior without trauma . Refer to you by dentist when he notice mild root resorption.
• On eaxm patient having widened wrists and ankle. Lab showed:
• Bicarb 27 ,albumin 3.9 g/dl , calcium 10.2 mg/dl ,phosphorus 6.2 mg/dl , Alkaline phosphatase :65 U/L PTH 25 pg/ml
• Vitamin d 25 hydroxy 30 ng/ml

• Clinical finding in this patient most likely due to :
• A- increased bone resorption.
• B- increased inorganic pyrophosphate.
• C- increased phosphate .
• D- blount disease.
• E. increased FGF23

Related Documents











