Benha University Faculty of medicine Surgery department Undersupervision of: Dr/ Sayed El-Kilany By: 1 . ء عاطف مرزوق اسرا2 . ىعمحمد عبد الم اسراء م3 . عبد الرحمه جمال أمل4 . يرة جمال عبد أم العسيس5 . تالعسبحمد طلبان م ايم6 . عيد آيت طه عبد7 . ابراهيمءالديه تيسير ع8 . في السيد عفي جهادمير السيد جهاد س10 . راودا عطيتعبدالحميد.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Benha University
Faculty of medicine
Surgery department
Undersupervision of:
Dr/ Sayed El-Kilany
By:
اسراء محمد عبد المىعم.2اسراء عاطف مرزوق .1 أميرة جمال عبد .4أمل جمال عبد الرحمه .3
العسيسآيت طه عبدهللا عيد.6ايمان محمد طلبتالعسب .5
جهاد السيد عفيفي.8تيسير عالءالديه ابراهيم .7
راودا عطيتعبدالحميد.10 جهاد سمير السيد .
Contents
Ca metabolism.
Definition.
Signs and symptoms.
Causes.
Diagnosis.
Treatment.
"Primary hyperparathyroidism":
Mechanism.
Causes.
Clinical picture.
Diagnosis.
Treatment.
References.
Ca metabolism
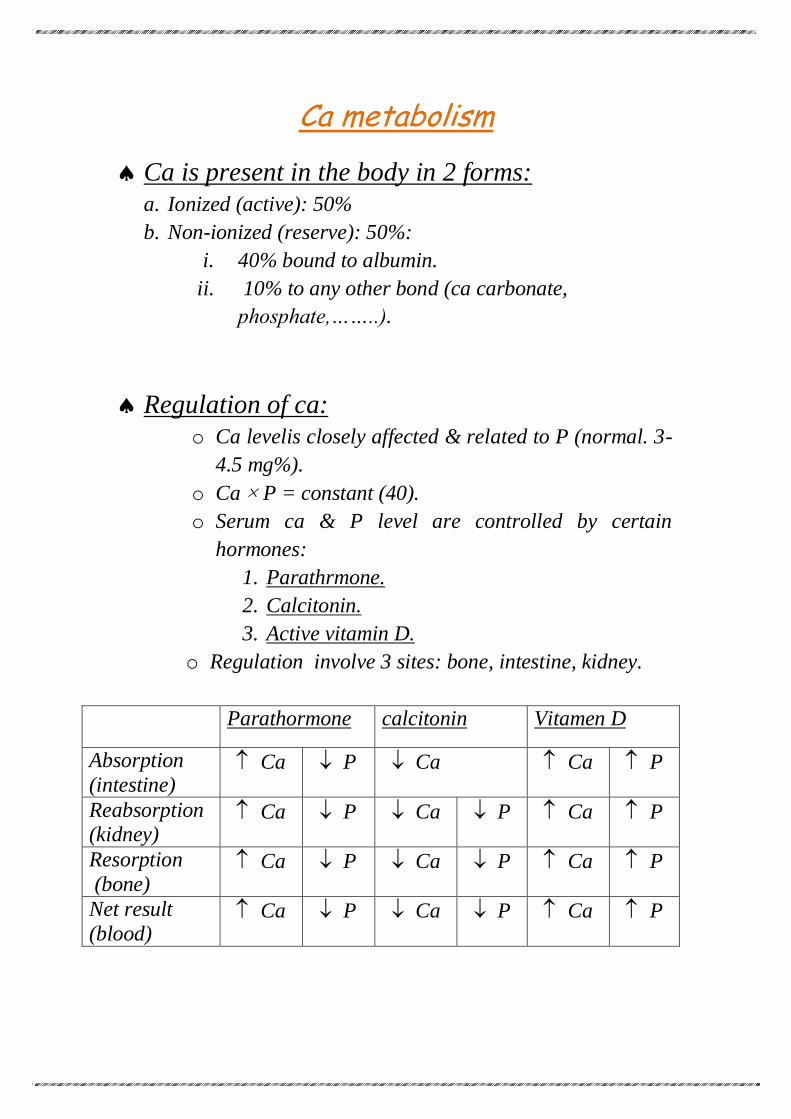
Ca is present in the body in 2 forms:
a. Ionized (active): 50%
b. Non-ionized (reserve): 50%:
i. 40% bound to albumin.
ii. 10% to any other bond (ca carbonate,
phosphate,……..).
Regulation of ca:
o Ca levelis closely affected & related to P (normal. 3-
4.5 mg%).
o Ca × P = constant (40).
o Serum ca & P level are controlled by certain
hormones:
1. Parathrmone.
2. Calcitonin.
3. Active vitamin D.
o Regulation involve 3 sites: bone, intestine, kidney.
Parathormone calcitonin Vitamen D
Absorption
(intestine) Ca P Ca Ca P
Reabsorption (kidney)
Ca P Ca P Ca P
Resorption
(bone) Ca P Ca P Ca P
Net result
(blood) Ca P Ca P Ca P
Definition
Hypercalcemia is an elevated calcium level in the blood.
(Normal range: 9–10.5 mg/dL or 2.2–
2.6 mmol/L). Because an elevated calcium level is
often indicative of other diseases, a workup should be
undertaken if it persists. It can be due to excessive skeletal
calcium release, increased intestinal calcium absorption,
or decreased renal calcium excretion.
Pathophysiology
o Usually, hypercalcemia is reported as elevation of total plasma calcium levels rather than ionized calcium levels.
o Approximately 50% of total calcium is protein bound, and
the total calcium level will vary with protein-binding capacity. This phenomenon may rarely result in
pseudohypercalcemia—for example, in patients with
hyperalbuminemia secondary to dehydration and in some patients with multiple myeloma. More commonly, lowering
of total calcium levels is observed in patients with low
levels of binding proteins (hypoalbuminemia). This physiology requires that the total plasma calcium level be
corrected for the albumin level.
o Normal calcium levels may range from 9 to 10.5 mg/day, assuming an albumin level of 4.5 g/dL. The calcium
concentration [Ca] usually changes by 0.8 mg/dL for
every 1.0-g/dL change in plasma albumin concentration. Thus, this formula estimates the actual total plasma
calcium level:
Corrected [Ca] = Total [Ca] + (0.8 × [4.5 −
albumin level])
o Acidosis decreases the amount of calcium bound to
albumin, whereas alkalosis increases the bound fraction of calcium.
o A small amount of calcium (about 6%) is complexed to
anions such as citrate and sulfate. The remainder is ionized calcium that is biologically active.
Signs and symptoms
1. ( These symptoms are more common at
high calcium blood values (12.0 mg/dL or
3 mmol/l)) There is a general mnemonic for remembering the
effects of hypercalcaemia: "Stones, Bones, Groans,
Thrones and Psychiatric Overtones":
Stones (renal or biliary) , lead to renal failure .
Bones (bone pain).
Groans (abdominal pain, nausea and vomiting).
Thrones (sit on throne - polyuria).
Psychiatric overtones (Depression 30-40%,
anxiety, cognitive dysfunction, insomnia, coma) Other symptoms can include fatigue, anorexia, and
pancreatitis.
ECG findings of a short QT interval and a
widened T wave suggest hypercalcaemia.
Hypercalcaemia can increase gastrin production,
leading to increased acidity so peptic ulcers may also occur.
2. Severe hypercalcaemia (above 15–16 mg/dL or
3.75–4 mmol/l) "Hypercalcaemic crisis": It is considered a medical emergency: at these levels,
coma and cardiac arrest can result. This can be
explained as following: the high levels of calcium ions decrease neuronal excitability, which leads to
hypotonicity of smooth and striated muscle. This
explains the fatigue, muscle weakness, low tone and
sluggish reflexes in muscle groups. In the gut this causes constipation. The sluggish nerves also explain
drowsiness, confusion, hallucinations, stupor and / or
coma. The main symptoms of a hypercalcaemic crisis are
oliguria or anuria, as well as somnolence or coma.
After recognition, primary hyperparathyroidism should be proved or excluded.
In extreme cases of primary hyperparathyroidism,
removal of the parathyroid gland after surgical neck exploration is the only way to avoid death
. The
diagnostic program should be performed within hours,
in parallel with measures to lower serum calcium.
Causes
1) Physiologic:
Young, growing dogs, especially large breeds, often have Ca slightly higher than the reference range for
adult dogs.
2) Abnormal parathyroid gland function
Primary hyperparathyroidism :
o Primary parathyroid hyperplasia. o Solitary parathyroid adenoma . o Parathyroid carcinoma. o Multiple endocrine neoplasia (MEN). o Familial isolated hyperparathyroidism.
Tertiary hyperparathyrodism: Associated
with chronic renal failure or vitamen D defficiency.
Lithium use. Familial hypocalciuric hypercalcaemia/familial benign
hypercalcaemia .
3) Malignancy:
Solid tumour with metastasis (e.g. breast cancer or
classically squamous cell carcinoma, which can be
PTHrP-mediated) . Solid tumour with humoral mediation of
hypercalcaemia (e.g. lung cancer, most commonly non-
small cell lung cancer or kidney cancer, phaeochromocytoma) . Haematologic malignancy (multiple myeloma,
lymphoma, leukaemia) . Ovarian small cell carcinoma of the hypercalcemic
type.
N.B. Primary hyperparathyrodism and
malignency accounts for about 90%
of cases of hypercalcaemia.
4)Vitamin-D metabolic disorders:
Hypervitaminosis D (vitamin D intoxication) . Elevated 1,25(OH)2D levels (e.g. sarcoidosis,
tuberculosis, lymphoma and other granulomatous
diseases) . Idiopathic hypercalcaemia of infancy. Rebound hypercalcaemia after rhabdomyolysis.
5)Disorders related to high bone-turnover rates:
*Hyperthyroidism . *Prolonged immobilization.
*Thiazide use. *Vitamin A intoxication.
*Paget's disease of the bone
6)Renal failure:
Severe secondary hyperparathyroidism.
Aluminium intoxication.
Milk-alkali syndrome (from calcium antacids) .
7)Others:
Acromegally.
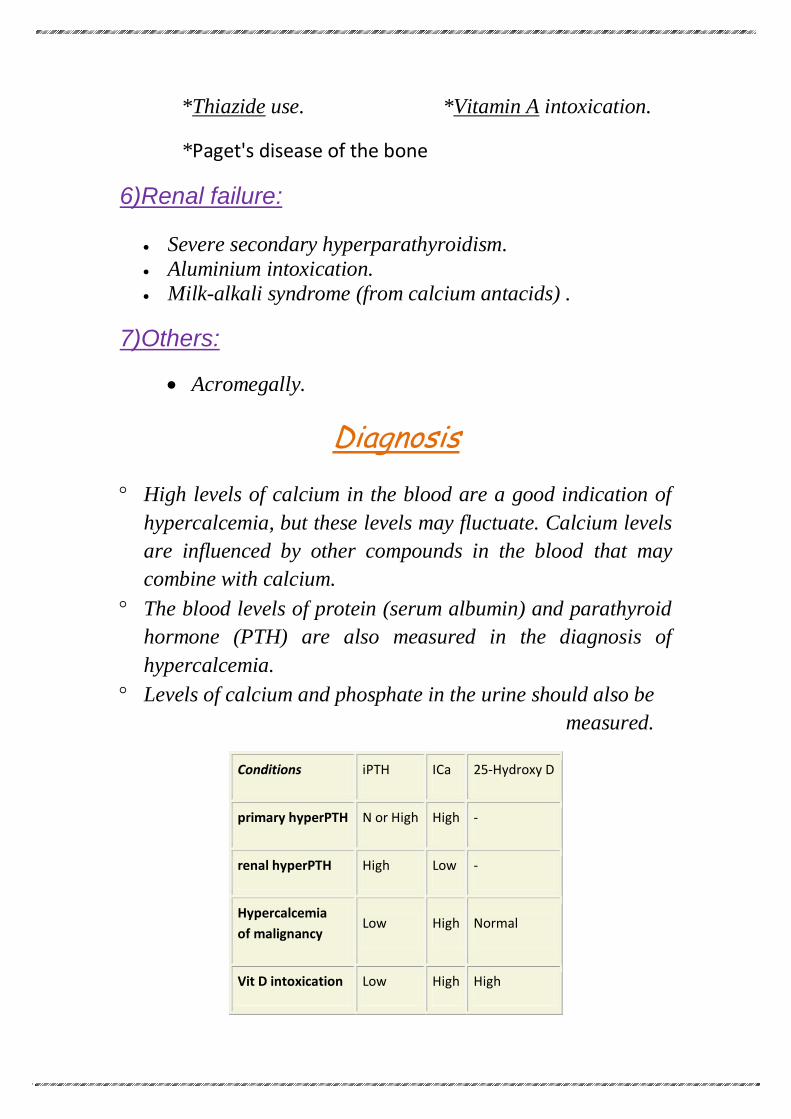
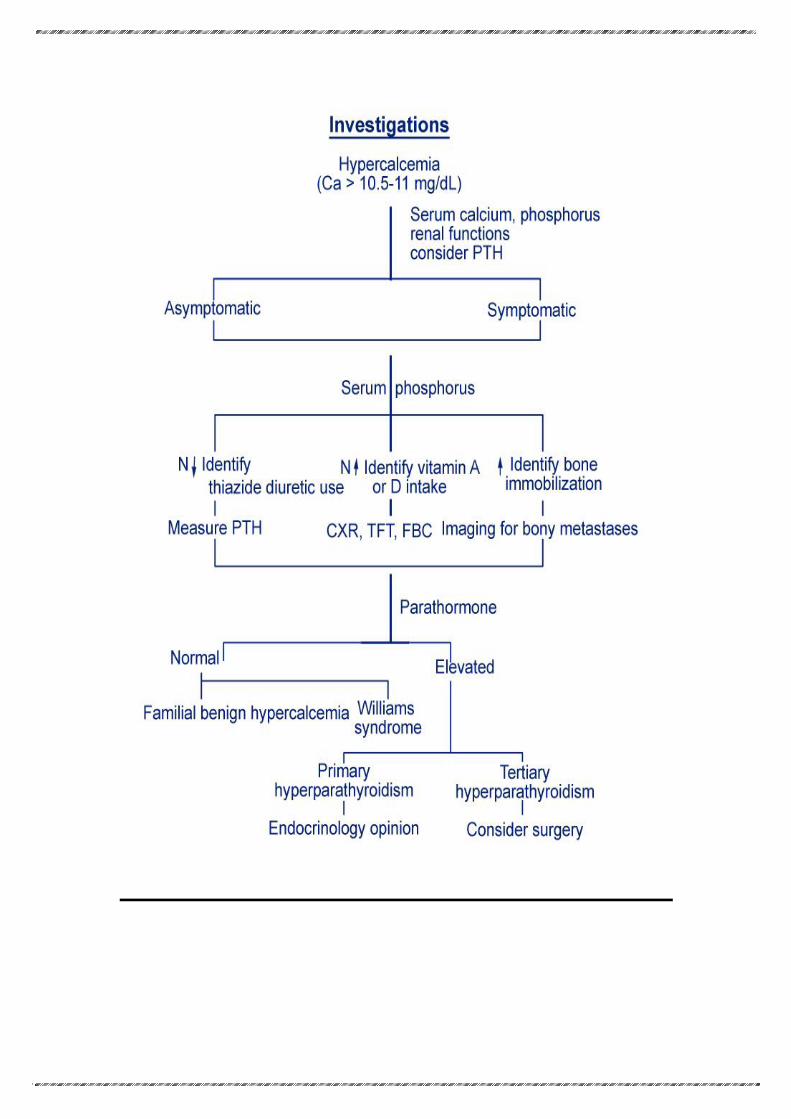
Diagnosis
High levels of calcium in the blood are a good indication of
hypercalcemia, but these levels may fluctuate. Calcium levels
are influenced by other compounds in the blood that may
combine with calcium.
The blood levels of protein (serum albumin) and parathyroid
hormone (PTH) are also measured in the diagnosis of
hypercalcemia.
Levels of calcium and phosphate in the urine should also be
measured.
Conditions iPTH ICa 25-Hydroxy D
primary hyperPTH N or High High -
renal hyperPTH High Low -
Hypercalcemia
of malignancy Low High Normal
Vit D intoxication Low High High
Treatment
The treatment of hypercalcemia depends on how high the
calcium level is and what is causing the elevation.
Hypercalcemia can be life-threatening and rapid reduction
may be necessary.
If the patient has normal kidney function, fluids can be
given by vein (intravenously) to clear the excess calcium.
The amount of fluid taken in and eliminated must be
carefully monitored.
If the patient's kidneys are not working well, acute
hemodyalysis is probably the safest and most effective
method to reduce dangerous calcium levels. In this
procedure, blood is circulated through tubes made of semi-
permeable membranes against a special solution that
filters out unwanted substances before returning the blood
to the body.
Drugs:
Furosemide\"loop diuretics" can be given after
adequate fluid intake is established. These drugs
inhibit calcium reabsorption in the kidneys and
promote urine production.
Drugs that inhibit bone loss, such as calcitonin,
biphosphates, and plicamycin, are helpful in
achieving long-term control.
Phosphate pills help lower high calcium levels
caused by a deficiency in phosphate.
Anti-inflammatory agents such as steroids are
helpful with some cancers and toxic levels of vitamin
D.
Treatment of the underlying cause of the
hypercalcemia will also correct the imbalance.The
hypercalcemia caused by cancer is difficult to treat
without controlling the cancer.
Prognosis
Surgery to remove the parathyroid glands and any
misplaced tissue that is producing excessive amounts of
hormone succeeds in about 90% of all cases. Outcome is
also influenced by whether any damage to the kidneys
can be reversed. Mild hypercalcemia can be controlled through good fluid
intake and the use of effective drugs. Hypercalcemia generally develops as a late complication
of cancer and the expected outlook is grim without
effective anticancer therapy.
N.B. Since the primary hyperparathyroidism is the most common cause of hypercalcaemia,
we find that we must talk briefly about it.
"Primary hyperparathyroidism"
Mechanism:
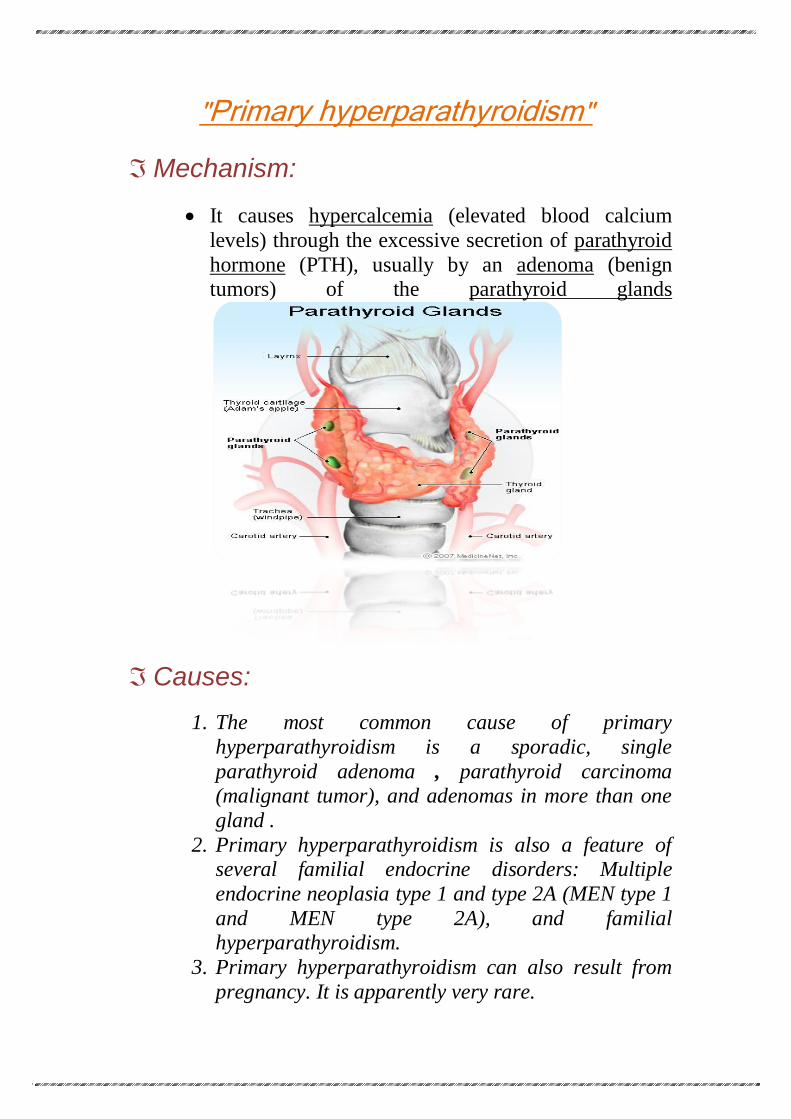
It causes hypercalcemia (elevated blood calcium
levels) through the excessive secretion of parathyroid
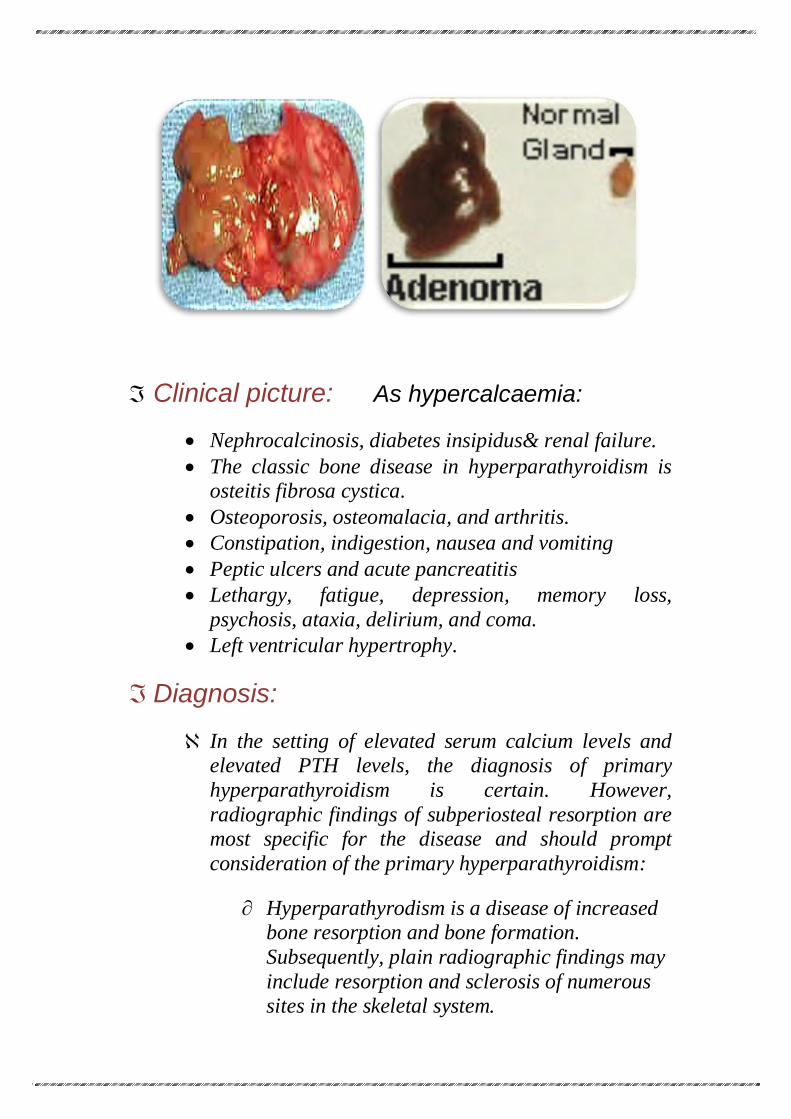
hormone (PTH), usually by an adenoma (benign tumors) of the parathyroid glands
Causes:
1. The most common cause of primary
hyperparathyroidism is a sporadic, single
parathyroid adenoma , parathyroid carcinoma (malignant tumor), and adenomas in more than one
gland .
2. Primary hyperparathyroidism is also a feature of several familial endocrine disorders: Multiple
endocrine neoplasia type 1 and type 2A (MEN type 1
and MEN type 2A), and familial hyperparathyroidism.
3. Primary hyperparathyroidism can also result from
pregnancy. It is apparently very rare.
Clinical picture: As hypercalcaemia:
Nephrocalcinosis, diabetes insipidus& renal failure.
The classic bone disease in hyperparathyroidism is osteitis fibrosa cystica.
Osteoporosis, osteomalacia, and arthritis.
Constipation, indigestion, nausea and vomiting
Peptic ulcers and acute pancreatitis
Lethargy, fatigue, depression, memory loss,
psychosis, ataxia, delirium, and coma.
Left ventricular hypertrophy.
Diagnosis:
In the setting of elevated serum calcium levels and elevated PTH levels, the diagnosis of primary
hyperparathyroidism is certain. However,
radiographic findings of subperiosteal resorption are most specific for the disease and should prompt
consideration of the primary hyperparathyroidism:
Hyperparathyrodism is a disease of increased bone resorption and bone formation.
Subsequently, plain radiographic findings may
include resorption and sclerosis of numerous sites in the skeletal system.
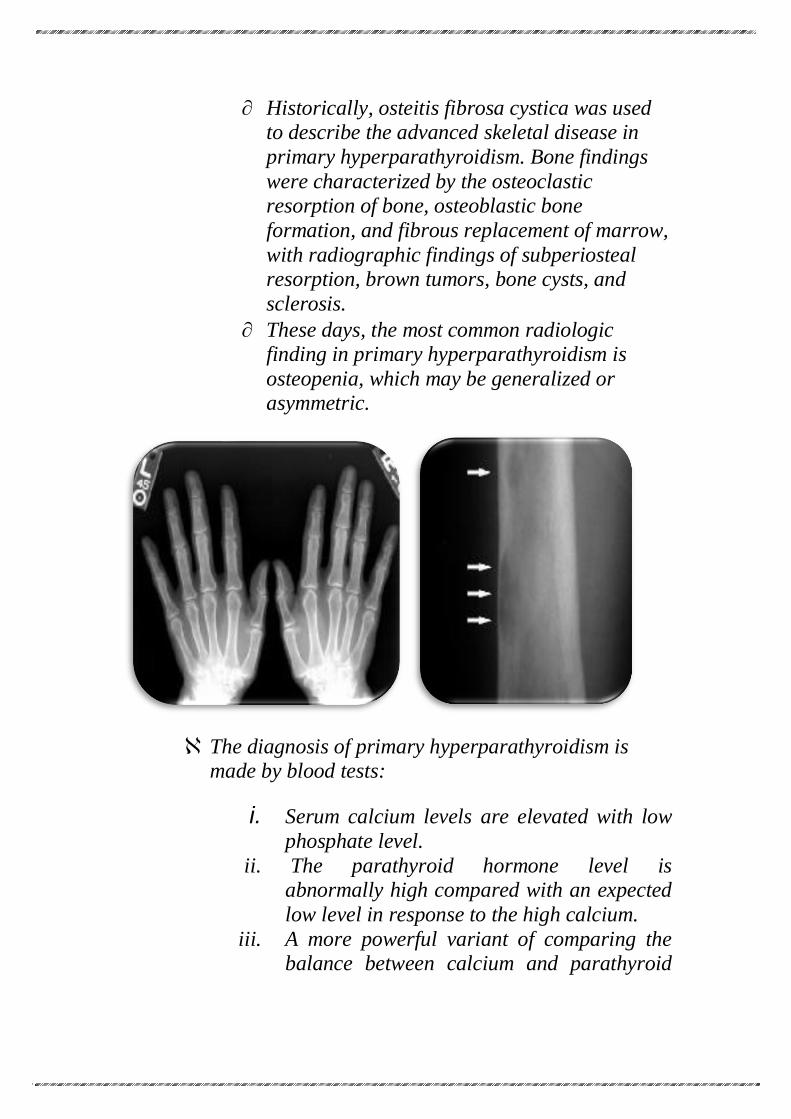
Historically, osteitis fibrosa cystica was used to describe the advanced skeletal disease in
primary hyperparathyroidism. Bone findings
were characterized by the osteoclastic resorption of bone, osteoblastic bone
formation, and fibrous replacement of marrow,
with radiographic findings of subperiosteal resorption, brown tumors, bone cysts, and
sclerosis.
These days, the most common radiologic finding in primary hyperparathyroidism is
osteopenia, which may be generalized or asymmetric.
The diagnosis of primary hyperparathyroidism is made by blood tests:
i. Serum calcium levels are elevated with low
phosphate level. ii. The parathyroid hormone level is
abnormally high compared with an expected
low level in response to the high calcium.
iii. A more powerful variant of comparing the balance between calcium and parathyroid
hormone is to perform a 3 hour calcium
infusion. iv. The serum chloride/phosphate ratio is 33 or
more in most patients with primary
hyperparathyroidism. However, usage of thiazide medications have been reported to
causes ratios above 33.
Urinary cAMP is occasionally measured; this is generally elevated.
Treatment:
Treatment is usually surgical removal of the gland(s) containing adenomas.
1) Medications:
Medications include estrogen replacement therapy in postmenopausal women and bisphosphonates.
Newer medications termed "calcimimetics" used in
secondary hyperparathyroidism are now being used in Primary hyperparathyroidism. Calcimimetics
reduce the amount of parathyroid hormone released
by the parathyroid glands. They are recommended in patients in whom surgery is inappropriate.
2) Surgery:
The symptoms of the disease, listed above, are indications for surgery. Surgery reduces all cause
mortality as well as resolving symptoms. However,
cardiovascular mortality is not significantly reduced.
A consensus statement in 2002 recommended the
following indications for surgery in asymptomatic
hyperparathyroidism:
Serum calcium: 1.0 mg/dl above upper
limit of normal .
24-h urinary calcium >400 mg.
Creatinine clearance reduced by 30%
compared with age-matched subjects.
Bone mineral density t-score <−2.5 at any
site .
Age <50
More recently, three randomized controlled trials
have studied the role of surgery in patients with
asymptomatic hyperparathyroidism. The largest study reported that surgery showed increase in bone
mass, but no improvement in quality of life after one
to two years among patients with:
Untreated, asymptomatic primary
hyperparathyroidism .
Serum calcium between 2.60–2.85 mmol/liter
(10.4–11.4 mg/dl) .
Age between 50 and 80 yr .
No medications interfering with Ca
metabolism
No hyperparathyroid bone disease .
No previous operation in the neck .
Creatinine level < 130 µmol/liter
(<1.47 mg/dl)
3) Future therapies:
Future developments such as calcimimetic agents
(e.g. cinacalcet) which activate the parathyroid calcium-sensing receptor may offer a good
alternative to surgery.
References
1. Dorland's Medical Dictionary . 2. Wesson, L.; Suresh, V.; Parry, R. (2009). "Severe
hypercalcaemia mimicking acute myocardial infarction". Clinical medicine (London, England) .
3. Serafi S, Vliek C, Taremi M (2011) "Osborn waves in a hypothermic patient" The Journal of Community Hospital Internal Medicine Perspectives .
4. Mitchell, Richard Sheppard; Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson. Robbins Basic Pathology.
5. Tierney, Lawrence M.; McPhee, Stephen J.; Papadakis, Maxine A. (2006). Current Medical Diagnosis and Treatment 2007 (Current Medical Diagnosis and Treatment).
6. Online 'Mendelian Inheritance in Man' (OMIM) . 7. Online 'Mendelian Inheritance in Man' (OMIM) . 8. Online 'Mendelian Inheritance in Man' (OMIM) . 9. Deshmukh, R. G.; Alsagoff, S. A. L.; Krishnan, S.; Dhillon, K.
S.; Khir, A. S. M. (1998). "Primary hyperparathyroidism presenting with pathological fracture".
10. Bilezikian, John P.; Silverberg, Shonni J. (2002). "Primary hyperparathyroidism: Epidemiology and clinical consequences". Clinical Reviews in Bone and Mineral Metabolism.
11. Bolland, M. J.; Grey, A. B.; Gamble, G. D.; Reid, I. R. (2004). "Association between Primary Hyperparathyroidism and Increased Body Weight: A Meta-Analysis". Journal of Clinical Endocrinology & Metabolism .
12. Barreras, R. F.; Donaldson, R. M. (1967). "Role of Calcium in Gastric Hypersecretion, Parathyroid Adenoma and Peptic Ulcer". New England Journal of Medicine .

13. Stefenelli T, Abela C, Frank H, et al. (1997). "Cardiac abnormalities in patients with primary hyperparathyroidism: implications for follow-up".