HYPERBILIRUBINEMIA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

HYPERBILIRUBINEMIA

INTRODUCTION
• Hyperbilirubinemia :- An elevated level of the pigment bilirubin in the blood.
• Occurs when ,serum bilirubin >2 mg/dl
• Yellowing of the skin, scleras (white of the eye), and mucous membranes (jaundice)
• A sufficient elevation of bilirubin produces jaundice.
• Hyperbilirubinemia is a biochemical finding but jaundice is a clinical finding for increased bilirubin levels in the blood.

BILIRUBIN METABOLISM
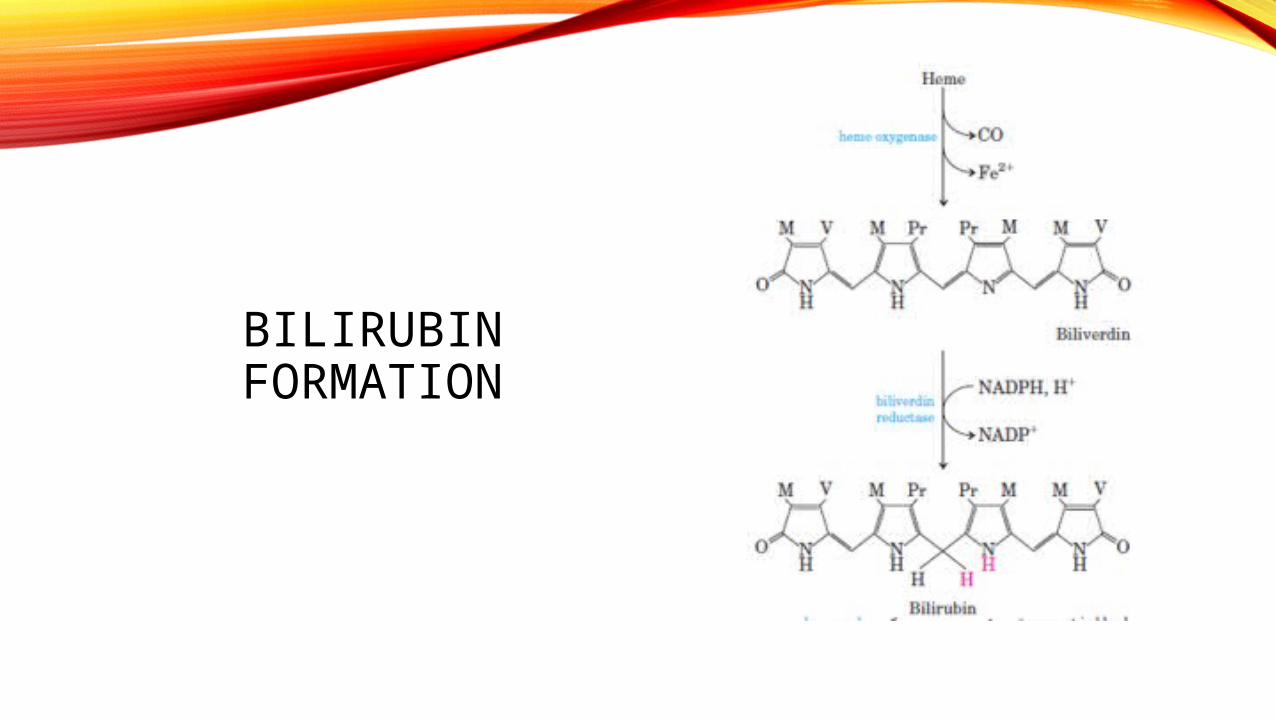
BILIRUBIN FORMATION
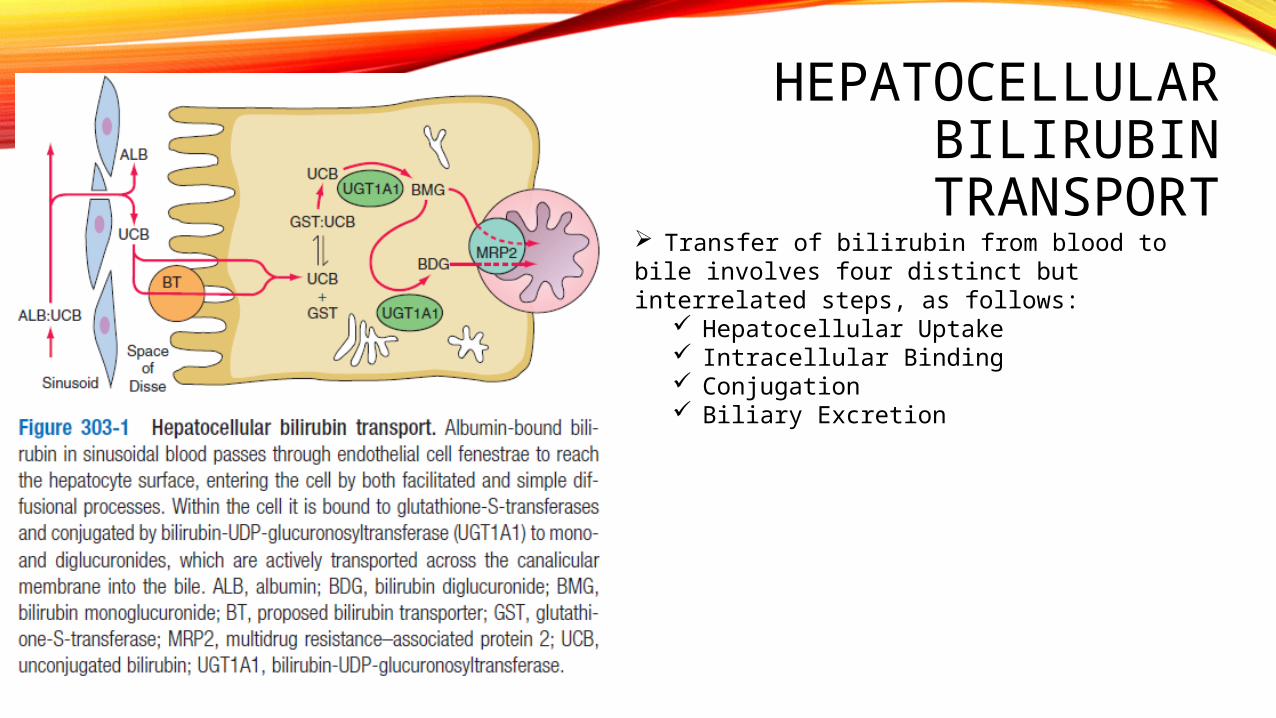
HEPATOCELLULAR BILIRUBIN
TRANSPORT Transfer of bilirubin from blood tobile involves four distinct but interrelated steps, as follows:
Hepatocellular Uptake Intracellular Binding Conjugation Biliary Excretion
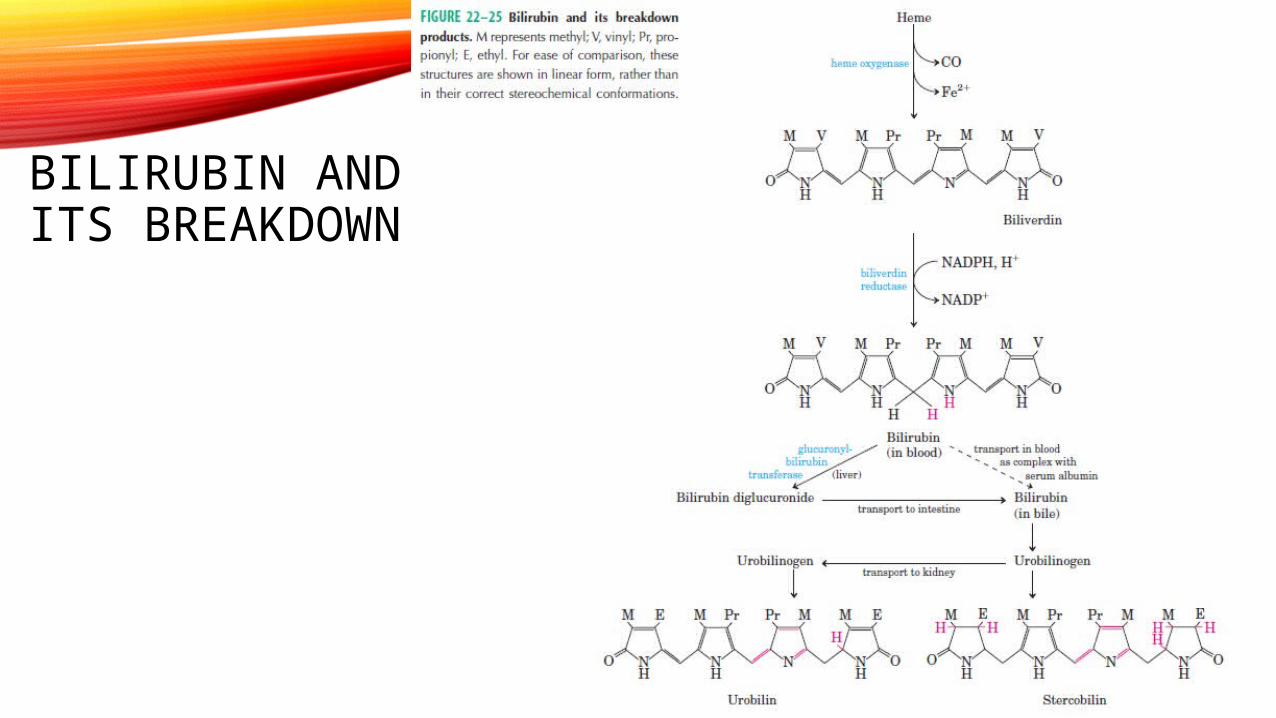
BILIRUBIN AND ITS
BREAKDOWN

ENTEROHEPATIC CIRCULATION

HEPATOCELLULAR CONDITIONS THAT MAY PRODUCE JAUNDICE
1. Viral hepatitis• Hepatitis A, B, C, D, and E• Epstein-Barr virus• Cytomegalovirus• Herpes simplex
2. Alcohol
3. Drug toxicity• Predictable, dose-dependent (e.g., acetaminophen)• Unpredictable, idiosyncratic (e.g., isoniazid)
4. Environmental toxins• Vinyl chloride• Jamaica bush tea—pyrrolizidine alkaloids• Kava Kava• Wild mushrooms—Amanita phalloides or A. verna
5. Wilson's disease
6. Autoimmune hepatitis

CHOLESTATIC CONDITIONS THAT MAY PRODUCE JAUNDICE
• 1. Intrahepatic• Viral hepatitis
• 1. Fibrosing cholestatic hepatitis—hepatitis B and C• 2. Hepatitis A, Epstein-Barr virus, cytomegalovirus
• Alcoholic hepatitis• Drug toxicity
• 1. Pure cholestasis—anabolic and contraceptive steroids• 2. Cholestatic hepatitis—chlorpromazine, erythromycin
estolate• 3. Chronic cholestasis—chlorpromazine and
prochlorperazine• Primary biliary cirrhosis• Primary sclerosing cholangitis• Vanishing bile duct syndrome
• 1. Chronic rejection of liver transplants• 2. Sarcoidosis• 3. Drugs
• Inherited• 1. Progressive familial intrahepatic cholestasis• 2. Benign recurrent cholestasis
• Cholestasis of pregnancy
CHOLESTATIC CONDITIONS THAT MAY PRODUCE JAUNDICE
• 1. Intrahepatic• Total parenteral nutrition• Nonhepatobiliary sepsis• Benign postoperative cholestasis• Paraneoplastic syndrome• Venoocclusive disease• Graft-versus-host disease• Infiltrative disease
• 1. TB• 2. Lymphoma• 3. Amyloid
• Infections• 1. Malaria• 2. Leptospirosis

CHOLESTATIC CONDITIONS THAT MAY PRODUCE JAUNDICE
• 2. Extrahepatic• A. Malignant
• 1. Cholangiocarcinoma• 2. Pancreatic cancer• 3. Gallbladder cancer• 4. Ampullary cancer• 5. Malignant involvement of the porta hepatis lymph nodes
• B. Benign• 1. Choledocholithiasis• 2. Postoperative biliary structures• 3. Primary sclerosing cholangitis• 4. Chronic pancreatitis• 5. AIDS cholangiopathy• 6. Mirizzi's syndrome• 7. Parasitic disease (ascariasis)

1) INCREASED BILIRUBIN PRODUCTION Hemolysis
Increased destruction of RBCs eg sickle cell anemia, thalassemia
Drastic increase in the amount of bilirubin produced
Unconj. bilirubin levels rise due to liver’s inability to catch up to the increased rate of RBC destruction
Prolonged hemolysis may lead to precipitation of bilirubin salts in the gall bladder and biliary network result in formation of gallstones and conditions such as
cholecystitis and biliary obstruction
UNCONJUGATED HYPERBILIRUBINEMIA

Clinical manifestation• Unconjugated hyperbilirubinemia• Normal serum level of transaminases,alkaline phosphatase,proteins• Acholuric jaundice (bile pigment absent in urine)• Dark brown color in stool• Increased urinary excretion of urobilinogen
Ineffective erythropoiesis
develoing erythroid cells destroyed in bone marrow
fraction of total bilirubin production increased
unconjugated hyperbilirubinemia
Occurs in• thalassemia major• Megaloblastic anemia • Congenital erythropoietic porphyria• Lead poisoning
Other Degradation of Hb
originating from areas of tissue infarctions and hematomas

2) DECREASED HEPATIC UPTAKE(UNCONJ. HYPERBILIRUBINEMIA)
Several drugs have been reported to inhibit bilirubin uptake by the liver
e.g. novobiocin, flavopiridol, Rifampicin
Bile
MRP2
B + GST
CB
Plasma Hepatic cell
Alb B
Alb :GSTB
sER
B + UDPGA UGT1A1
Impairment in dissociation of bilirubin from albuminDearrangement of binding to cytoplasmic protein –GST
due to defect or deficiency in the enzyme bilirubin-UDP glucurunosyl transferase
Physiological jaundice of Newborn incompletely developed hepatic physiologic processes
decreased UGT1A1 in neonates,alternate excretory pathway
unconjugated bilirubin in the gut (intestinal flora under-developed;bilirubin urobilinogen) enterohepatic circulation of unconjugated bilirubin
unconjugated hyperbilirubinemia (5-10mg/dl) in 2-5 days
In pre-term infants,profound hepatic dysfunction can lead to higher levels of unconjugated hyperbilirubinemia(>20mg/dl)
Complication:kernicterus t/t:Phototherapy,exchange transfusion
3) DISRUPTED INTRACELLULAR CONJUGATION (unconj. Hyperbilirubinemia)
Impaired bilirubin conjugationAcquired conjugation defects• Breast milk jaundice bilirubin conjugation inhibited by certain fatty acid present in breast milk EGF in breast milk is also associated• Diffuse hepatocellular disease Hepatitis cirrhosis• Drugs inhibiting UGT1A1 activity pregnanediol Novobiocin Chloramphenicol Gentamicin


HEREDITARY DEFECTS IN BILIRUBIN CONJUGATION
• Three familial disorders characterized by differing degrees of unconjugated hyperbilirubinemia have long been recognized.
• Differing degrees of deficiency in the ability to conjugate bilirubin.
• Some of the disorders are as follows :-
• Crigler Najjar Syndrome
• Gilbert’s Syndrome


CRIGLER-NAJJAR SYNDROME
• This syndrome is of two types:-
•Crigler Najjar Syndrome Type 1
•Crigler Najjar Syndrome Type 2

CRIGLER NAJJAR SYNDROME TYPE 1
• Characterised by unconjugated hyperbilirubinemia of about 20-45 mg/dL.
• Rare disorder – Shows Autosomal Recessive Inheritence.
• Usually appears in Neonatal period and persists for life.
• Mutation in UGT1 gene.
• Conventional hepatic function tests are normal.
• Hepatic histology is normal but sometimes bile plugs can develop in canaliculi.
• Bilirubin glucuronides – Absent in the bile.
• No detectable constitutive expression of UGT1A1 activity in hepatic tissue.
• Unconjugated bilirubin accumulation (but can be excreted via alternative pathways)
• No response to Phenobarbital or other enzyme inducers.
• Early liver transplantation remains the best hope to prevent brain injury and death.

Crigler Najjar Syndrome
Type IB
Defect is limited largely to bilirubin
conjugation
Mutation is in the bilirubin-specific exon
A1
Type IA
Defects in the glucuronide
conjugation of a spectrum of substrates
Mutations in one of the common exons (2–5) of the UGT1
gene
Type II
CRIGLER NAJJAR SYNDROME TYPE 2• Similar presentation to Crigler Najjar Syndrome Type 1
• Differences:
•Average bilirubin concentrations are lower in CN-II
•CN-II is only infrequently associated with kernicterus
•Bile is deeply colored
•Bilirubin glucuronides are present (Characteristic increase in the proportion of monoglucuronides)
•UGT1A1 in liver is usually present at reduced levels (typically ≤10% of normal)
• Reduction of serum bilirubin concentrations by >25% in response to enzyme inducers such as phenobarbital distinguishes CN-II from CN-I.
• Incidence of kernicterus in CN-II is low

GILBERT SYNDROME• Mild unconjugated hyperbilirubinemia.
• Serum bilirubin concentrations are most often <3 mg/dL
• M>F
• Normal values for standard hepatic biochemical tests
• Normal hepatic histology but modest increase in lipofuscin.
• Association with other conditions like stress, fatigue, alcohol use, etc. can aggrevate the bilirubin levels
• Relieving factors :- enzyme inducing agents
• UGT1A1 activity is reduced to about 10-35% of normal.
• Phenobarbital normalizes serum bilirubin concentration and hepatic bilirubin clearance
• Defect in bilirubin uptake as well as in conjugation


DISORDERS OF BILIRUBIN METABOLISM LEADING TO MIXED
OR PREDOMINANTLY CONJUGATED HYPERBILIRUBINEMIA

DISRUPTED SECRETION OF BILIRUBIN INTO BILE CANALICULI
Dubin–Johnson Syndrome mild conj. hyperbilirubinemia, but can increase with concurrent
illness, pregnancy, and use of oral contraceptives; otherwise asymptomatic
Inability of hepatocytes to secrete CB after it has formed Due to mutation in the MRP2 gene (autosomal recessive trait) Liver histology shows black pigmentation
Bile
MRP2
B + GST
CB
Plasma Hepatic cellAlb
B
Alb :GSTB
sER
B + UDPGAUGT1A1

Rotor Syndrome
• Autosomal recessive condition • Characterized by increased total bilirubin levels due to a rise in CB• Caused by a defect in transport of bilirubin into bile • Similar to Dubin –johnson , but no pigmentation in liver histology• Total urinary coproporphyrin excretion is substantially increased in Rotor
syndrome


BENIGN RECURRENT INTRAHEPATIC CHOLESTASIS(BRIC)
• Autosomal recessive• FIC1 gene mutated• Characterised by recurrent attacks of pruritis and jaundice• Typical episode malaise elevation in serum aminotransferase rise in alkaline phosphatase and conjugated bilirubin onset of jaundice and itching• Benign because it does not lead to cirrhosis or end-stage liver
disease

Progressive familial intrahepatic cholestasis
Byler’s Disease (Progressive FIC type
1)
Infancy
Progresses to malnutrition, growth retardation, and end-stage liver disease during childhood
FIC1 mutation
Progressive FIC type 2
Mutation in the protein named Sister of p-glycoprotein (aka
BSEP)
Progressive FIC type 3
Mutation of MDR3
Required for hepato celluar excretion of
phospholipids
High serum levels of γ-glutamyltransferase
activity

CHOLESTATIC CONDITIONS

CHOLESTATIC DISEASES :CHOLESTASIS
• Cholestasis is caused by:• impaired bile formation and • bile flow
• Gives rise to accumulation of bile pigment in the hepatic parenchyma.
• Can be caused by:• extrahepatic or intrahepatic obstruction of bile channels or• defects in hepatocyte bile secretion.

CHOLESTATIC DISEASES :CHOLESTASIS• Morphologic features of
cholestasis:1. Cholestatic
hepatocytes are enlarged
2. With dilated canalicular spaces
3. Apoptotic cells may be seen
4. Kupffer cells frequently contain regurgitated bile pigments

CHOLESTATIC DISEASES :CHOLESTASIS
• Morphologic features of cholestasis:
5. Bile plug (arrow) showing the expansion of bile canaliculus by bile.
6. FEATHERY DEGENERATION:
Droplets of bile pigment also accumulate within hepatocytes, which can take on a fine, foamy appearance.

CHOLESTATIC DISEASES :LARGE BILE DUCT OBSTRUCTION
• Most common cause of bile duct obstruction in adults:• Extrahepatic cholelithiasis (gallstones) followed by• Malignancies of the biliary tree or head of the pancreas, and • Strictures resulting from previous surgical procedures.
• Obstructive conditions in children include:• biliary atresia
• cystic fibrosis• choledochal cysts• syndromes in which there are insufficient intrahepatic bile
ducts.

CHOLESTATIC DISEASES :LARGE BILE DUCT OBSTRUCTION
• Acute biliary obstruction, either intrahepatic or extrahepatic, causes • Distention of upstream bile ductsbecome dilated. • Bile ductules proliferate at the portalparenchymal interface, accompanied by
stromal edema and infiltrating neutrophils. These labyrinthine ductules reabsorb secreted bile salts, serving to protect the downstream obstructed bile ducts from their toxic detergent action.
• Histologic hallmark of ascending cholangitis is the influx of these periductular neutrophils directly into the bile duct epithelium and lumen

CHOLESTATIC DISEASES :LARGE BILE DUCT OBSTRUCTION
• Chronic biliary obstruction and ductular reactions: Secondary inflammation initiate
• Periportal fibrosis, eventually leading to hepatic scarring and • Nodule formation, generating secondary or obstructive biliary cirrhosis.



CHOLESTATIC DISEASES :LARGE BILE DUCT OBSTRUCTION
• Chronic biliary obstruction and ductular reactions:Cholestatic features in the parenchyma may be severe with:
• Extensive feathery degeneration of periportal hepatocytes • Cytoplasmic swelling often with Mallory-Denk bodies (periportal predominance)• Formation of bile infarcts from detergent effects of extravasated bile.
• Ascending cholangitis may be superimposed on this chronic process as well, sometimes triggering acute on-chronic liver failure.

CHOLESTATIC DISEASES : CHOLESTASIS OF SEPSIS
• Sepsis may affect the liver by several mechanisms: • Through direct effects of intrahepatic bacterial infection (e.G., Abscess formation
or bacterial cholangitis),• Ischemia relating to hypotension caused by sepsis (particularly when the liver is
cirrhotic), or• In response to circulating microbial products (LPS).
CHOLESTATIC DISEASES : CHOLESTASIS OF SEPSIS
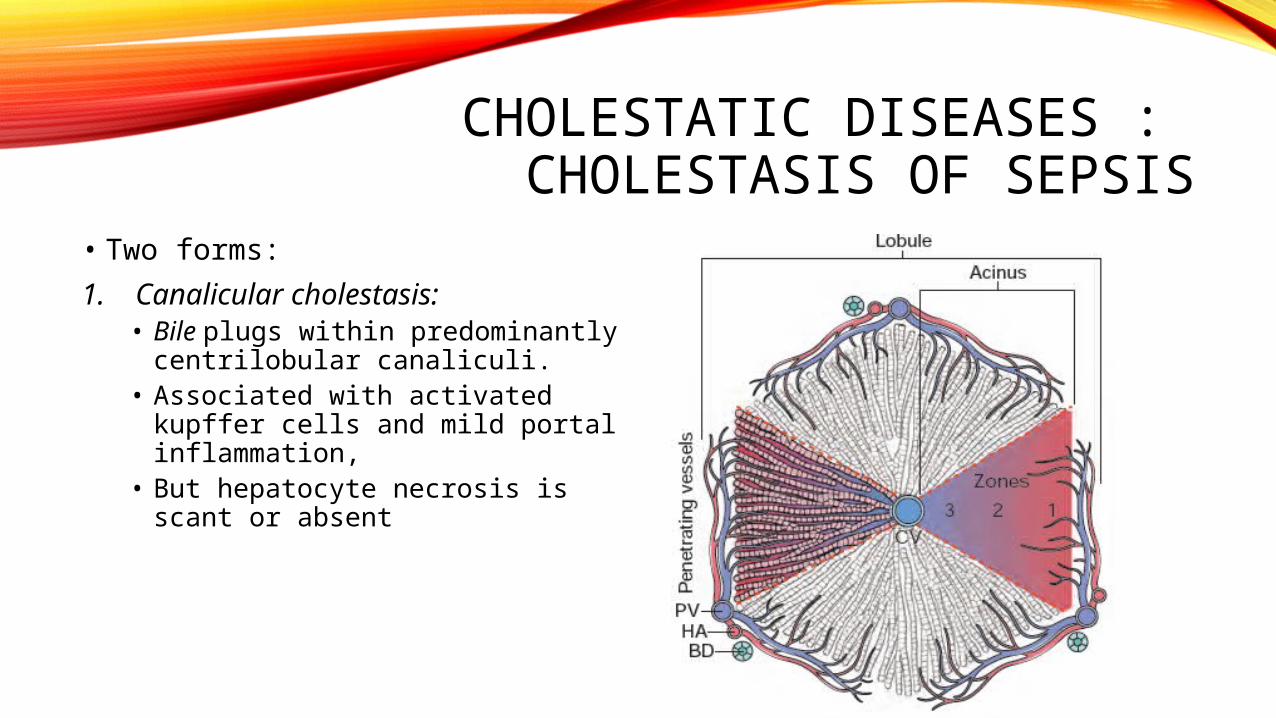
• Two forms:
1. Canalicular cholestasis: • Bile plugs within predominantly
centrilobular canaliculi. • Associated with activated kupffer
cells and mild portal inflammation, • But hepatocyte necrosis is scant
or absent

CHOLESTATIC DISEASES : CHOLESTASIS OF SEPSIS
2. Ductular cholestasis:• More ominous finding• Dilated canals of hering and bile
ductules at the interface of portal tracts and parenchyma become dilated and contain obvious bile plugs
• Often accompanies or even precedes the development of septic shock.

CHOLESTATIC DISEASES : PRIMARY HEPATOLITHIASIS
• Hepatolithiasis is a disorder of intrahepatic gallstone formation that leads to
• Repeated bouts of ascending cholangitis • Progressive inflammatory destruction of hepatic parenchyma• Predisposes to biliary neoplasia.

CHOLESTATIC DISEASES : PRIMARY HEPATOLITHIASIS
• Hepatolithiasis has pigmented calcium bilirubinate stones in distended intrahepatic bile ducts.
• The ducts show chronic inflammation, mural fibrosis, and peribiliary gland hyperplasia, all in the absence of extrahepatic duct obstruction.
• Biliary dysplasia may be seen and may evolve to invasive cholangiocarcinoma.

CHOLESTATIC DISEASES : NEONATAL CHOLESTASIS
• Prolonged conjugated hyperbilirubinemia in the neonate beyond 14-21 days after birth.
• Major causes:• Neonatal Hepatitis• Biliary Atresia
• Differentiation between two must: surgical correction for Biliary Atresia


CHOLESTATIC DISEASES : NEONATAL CHOLESTASIS
• Neonatal hepatitis is not a specific entity
• Nor are the disorders necessarily inflammatory.
• Morphologic findings• Lobular disarray with focal liver
cell apoptosis and necrosis• Panlobular giant-cell
transformation of hepatocytes• Prominent hepatocellular and
canalicular cholestasis
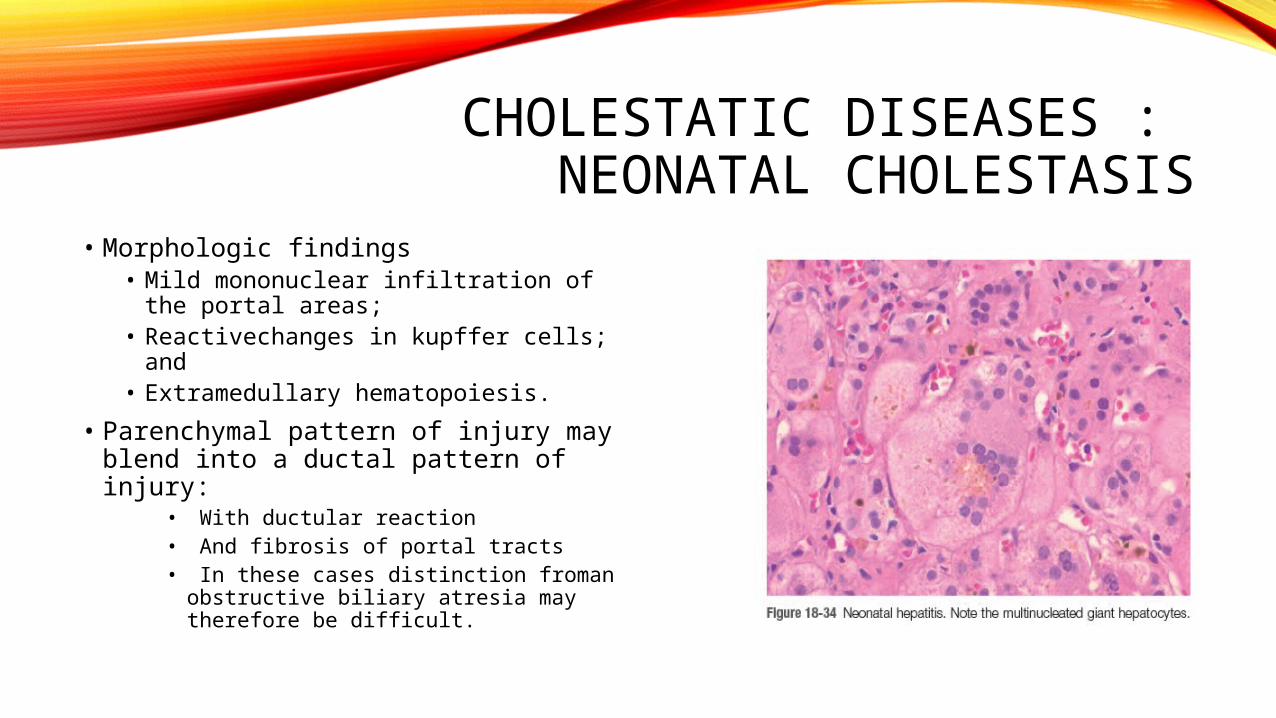
CHOLESTATIC DISEASES : NEONATAL CHOLESTASIS
• Morphologic findings• Mild mononuclear infiltration of the
portal areas; • Reactivechanges in kupffer cells;
and • Extramedullary hematopoiesis.
• Parenchymal pattern of injury may blend into a ductal pattern of injury:
• With ductular reaction• And fibrosis of portal tracts• In these cases distinction froman
obstructive biliary atresia may therefore be difficult.

CHOLESTATIC DISEASES : NEONATAL CHOLESTASIS
• Biliary Atresia:• Biliary atresia is defined as a complete or partial obstruction of the lumen of the extrahepatic
biliary tree within the first 3 months of life.
• Two forms:1. Fetal form:
• aberrant intrauterine development of the extrahepatic biliary tree
1. Perinatal form: presumed normally developed biliary tree is destroyed
following birth. Etiology unknownviral infection (Reovirus, rotavirus,and
cytomegalovirus) and autoimmunereactions are leading suspects.

CHOLESTATIC DISEASES : NEONATAL CHOLESTASIS
• Variability in the anatomy of biliary atresia:• Common duct (type I) • Right and/or left hepatic bile ducts (type II)• Obstruction of bile ducts at or above the porta hepatis(type III)
• Salient features of biliary atresia:• Inflammation and fibrosing stricture of the hepatic or common bile ducts• Periductular inflammation may progress into the intrahepatic bile
ductsprogressive destruction of the intrahepatic biliary tree

• Primary Biliary Cirrhosis• PBC is an autoimmune disease characterized by nonsuppurative,
inflammatory destruction of small and medium sized intrahepatic bile ducts. Large intrahepatic ducts and the extrahepatic biliary tree are not involved.
• Pathogenesis• AMA : recognize the E2 component of the pyruvate dehydrogenase complex (PDC-E2)• PDC-E2–specific T cells• Aberrant expression of MHC class II molecules on bile duct epithelial cells, accumulation
of autoreactive T cells around bile ducts, and antibodies against other cellular components
CHOLESTATIC DISEASES : AUTOIMMUNE CHOLANGIOPATHIES

• Primary Biliary Cirrhosis:• Sagittal section: liver
enlargement, nodularity indicative of cirrhosis, and green discoloration due to cholestasis.
CHOLESTATIC DISEASES : AUTOIMMUNE CHOLANGIOPATHIES
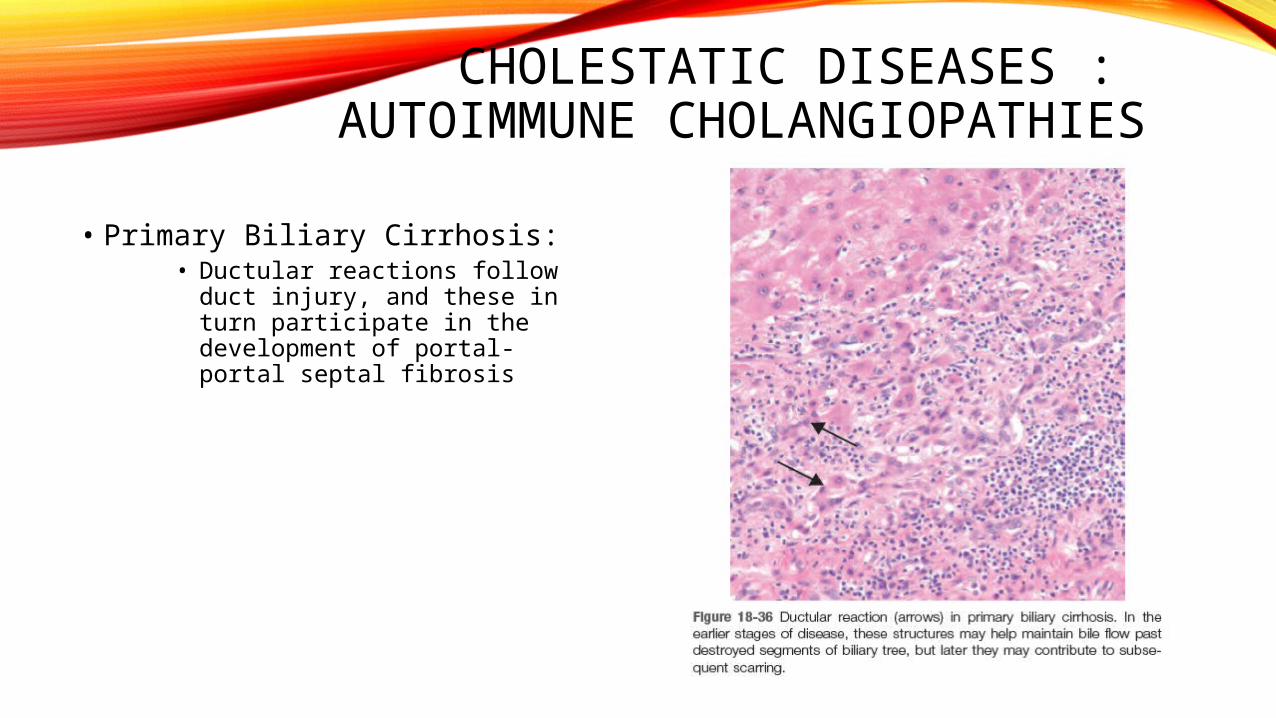
• Primary Biliary Cirrhosis:• Ductular reactions follow duct
injury, and these in turn participate in the development of portal-portal septal fibrosis
CHOLESTATIC DISEASES : AUTOIMMUNE CHOLANGIOPATHIES

• Primary Biliary Cirrhosis:• THE FLORID DUCT LESION:
Interlobular bile ducts are actively destroyed by lymphoplasmacytic inflammation with or without granulomas
CHOLESTATIC DISEASES : AUTOIMMUNE CHOLANGIOPATHIES
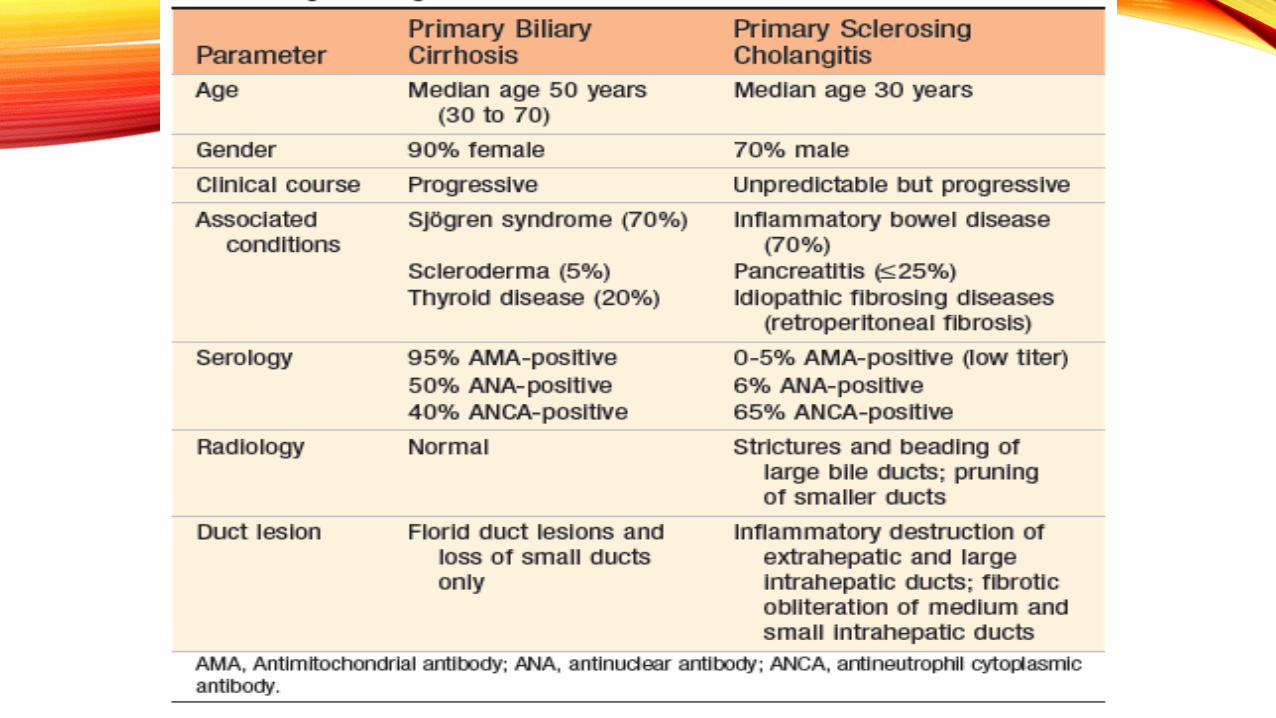

• Primary Sclerosing Cholangitis (PSC)• PSC is characterized by inflammation and obliterative fibrosis of intrahepatic and
extrahepatic bile ducts with dilation of preserved segments.• Pathogenesis:
• Immunologically mediated injury to bile ducts:• T cells in the periductal stroma• Presence of circulating autoantibodies• Association with HLA-B8 and other MHC antigens• Linkage to ulcerative colitis
• It has been proposed that T cells activated in the damaged mucosa of patients with ulcerative colitis migrate to the liver where they recognize a cross-reacting bile duct antigen.
• Autoantibody profiles in PSC are not as characteristic as they are in PBC
CHOLESTATIC DISEASES : AUTOIMMUNE CHOLANGIOPATHIES

• Primary Sclerosing Cholangitis (PSC):• Large duct inflammation:
• Similar to ulcerative colitis• Acute, neutrophilic infiltration of
the epithelium superimposed on a chronic inflammatory background.
• Inflamed areas develop strictures because edema and inflammation narrows the lumen or because of subsequent scarring.
• Smaller ducts:• Little inflammation• Striking circumferential
“onion skin” fibrosis around an increasingly atrophic duct lumen eventually leading to obliteration by a “tombstone” scar.
CHOLESTATIC DISEASES : AUTOIMMUNE CHOLANGIOPATHIES

• Primary Sclerosing Cholangitis (PSC):• Because the likelihood of sampling smaller duct lesions on
a random needle biopsy is miniscule, diagnosis depends on radiologic imaging of the extrahepatic and larger intrahepatic ducts.
CHOLESTATIC DISEASES : AUTOIMMUNE CHOLANGIOPATHIES


Related Documents











