By: Huson Amin Coronary Artery Disease Coronary Artery Disease

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
By: Huson Amin
Coronary Artery DiseaseCoronary Artery Disease

cardiovascular disease and cardiovascular disease and coronary heart diseasecoronary heart disease
• cardiovascular disease ( CVD, heart and circulatory disease)– all diseases of the heart and blood vessels
(e.g stroke, congenital heart defects, valvular heart disease, peripheral arterial disease)
• coronary heart disease (CHD, ischaemic heart disease)– disease of the coronary arteries due to
atherosclerosis

the coronary arteriesthe coronary arteries
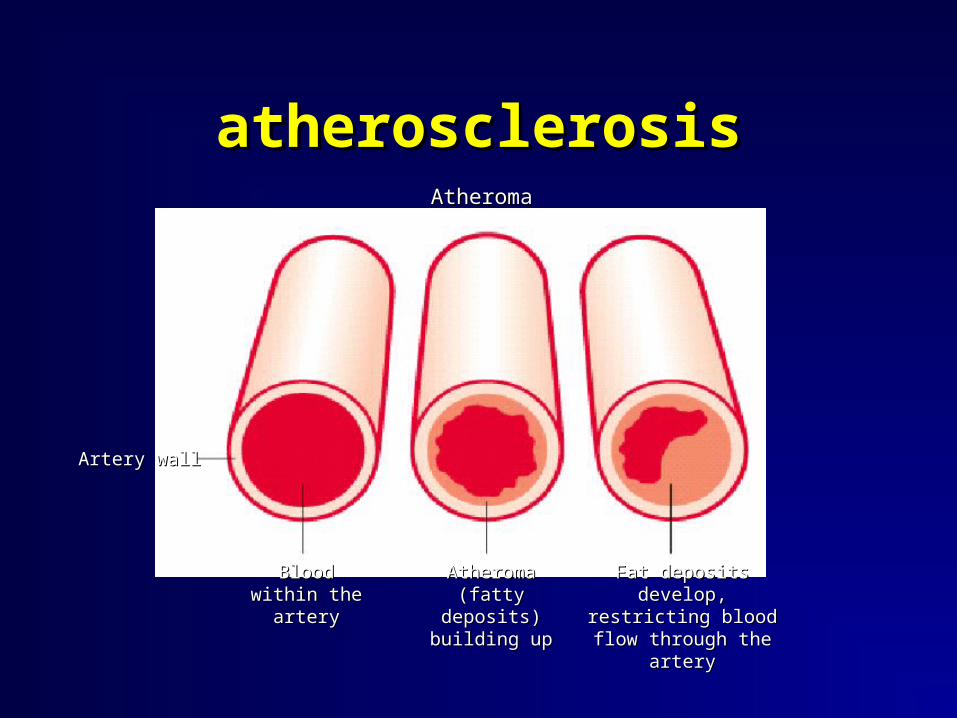
atherosclerosisatherosclerosisAtheromaAtheroma
Artery wallArtery wall
Blood within Blood within the arterythe artery
Atheroma Atheroma (fatty deposits) (fatty deposits)
building upbuilding up
Fat deposits develop, Fat deposits develop, restricting blood flow restricting blood flow
through the arterythrough the artery

coronary artery with coronary artery with atheromaatheroma
AtheromaAtheroma
Coronary Artery Coronary Artery with atherosclerosiswith atherosclerosis
Coronary ArteryCoronary Artery

atheromaatheroma
Atheroma (fatty layer)Atheroma (fatty layer)
Cross SectionCross Section Longitudinal SectionLongitudinal Section

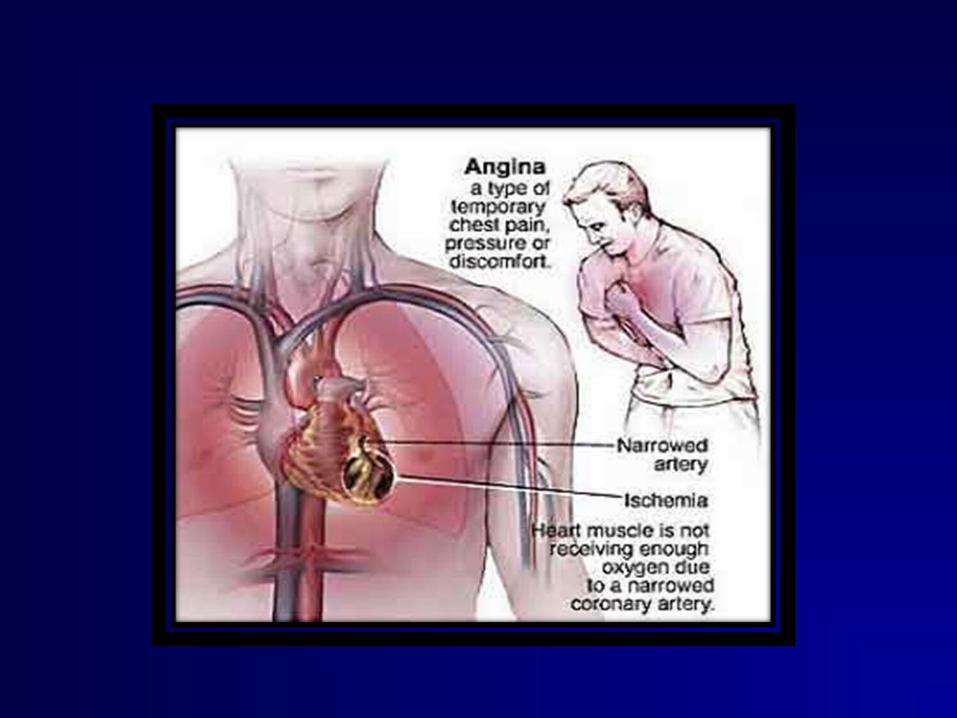
angina and heart attackangina and heart attack• angina
– narrowed coronary artery
– tightness or ache in the chest, breathlessness, sick feeling, dizziness
– comes on with exertion or emotion
– goes away with rest - usually 2-10 mins
• heart attack– due to sudden
blockage of the coronary artery
– chest pain “like a band”, indigestion, breathlessness, sickness, looking pale
– comes on at any time– doesn’t go away - if still
there in 15 minutes call 999
clarifying some termsclarifying some terms
• Heart failure – the pumping action of the heart is less efficient,
possibly caused by raised blood pressure, heart attack, or valve defect
• Heart attack (myocardial infarction)– a coronary artery is suddenly blocked by a blood clot
• Cardiac arrest – the heart stops beating when it quivers or fibrillates
causing the person to collapse• Stroke
– an artery leading to the brain is suddenly blocked with a blood clot or a bleed
main risk factors for main risk factors for coronary heart diseasecoronary heart disease
• smoking• inactivity• obesity and overweight• high blood pressure• raised blood cholesterol• diabetes• family history of coronary heart disease• excessive alcohol intake

SIGNS & SYMPTOMSSIGNS & SYMPTOMS Chest pain (Angina pectoris)Myocardial infarctionDiaphoresisEcg changesDysarrithmiasChest heaviness DyspneaFatigue

ANGINA PECTORISANGINA PECTORIS
• Angina pectoris is a clinical syndrome usually characterised by paroxysms of pain or pressure of anterior lobe.the cause is usually insufficient blood flow

TYPESTYPES
• Stable angina
• Predictable consistent pain that occurs in exertion and is relieved by rest
• Unstable angina• Also called preinfarction angina• Symptoms occur frequently and last longer
than stable angina• Pain may occur at rest

• Variant angina
• Also called prinzmentals angina.
• Pain at rest with reversible ST segment elevation thought to be caused by coronary artery vasospasm
• Microvascular angina
• Patient have chest pain but do not seem to have any blockage in coronary artery
• The pain may be due to tiny vessels that feed heart,arm and neck are not working properly

• Silent ischemia
• Objective evidence of ischemia (such as electrocardiographic changes with a stress test) but patient report no symptoms
ANGINA PAIN FEATURESANGINA PAIN FEATURES
• Squeezing burning tightening aching across chest usually starting behing breast bone.
• The often spread to neck,jaw,arms,shoulders,throat,back,or even teeth
• Attack of stable angina last for 1 – 5 minutes



Acute Coronary SyndromesAcute Coronary Syndromes
Unstable anginaUnstable angina ST-Elevation MIST-Elevation MI(Q-wave MI)(Q-wave MI)
Non-ST Elevation MINon-ST Elevation MI(Non-Q-wave MI)(Non-Q-wave MI)
Stable CADStable CAD
The continuum of acute coronary syndromes ranges from unstable The continuum of acute coronary syndromes ranges from unstable
angina, through non-ST-elevation myocardial infarction (also referred angina, through non-ST-elevation myocardial infarction (also referred
to as to as ““non-Q-wavenon-Q-wave”” myocardial infarction [MI]), to ST-elevation MI myocardial infarction [MI]), to ST-elevation MI
(also referred to as (also referred to as ““Q-waveQ-wave”” MI). MI).

Triggers to Plaque RuptureTriggers to Plaque Rupture
Inflammatorycytokines
Plaque RupturePlaque Rupture
Physical Stress
VulnerablePlaque
EmotionalStress

Causes of Acute Coronary Causes of Acute Coronary SyndromesSyndromes
• Atherosclerosis with superimposed thrombus
• Vasculitic syndromes
• Coronary emboli (e.g., from endocarditis, artificial valves)
• Congenital anomalies of the coronary arteries
• Coronary trauma or aneurysm
• Severe coronary artery spasm (primary or cocaine-induced)
• Increased blood viscosity (e.g., polycythemia vera, thrombocytosis)
• Significantly increased myocardial oxygen demand (e.g., aortic stenosis)
Unstable AnginaUnstable Angina
• Prior stable angina in:
– Frequency
– Duration
– Intensity
• Angina at rest… previously only on provocation
• New onset angina

Acute Myocardial InfarctionAcute Myocardial Infarction
• History and exam
• EKG changes
• Serum markers

SymptomsSymptoms
Pain
Sympathetic response
Parasympathetic response
Inflammatory response
Other
– PressurePressure– Burning (hot)Burning (hot)– Chest/arms/jaw/backChest/arms/jaw/back
– SweatsSweats– TachycardiaTachycardia– Cool, clammy skinCool, clammy skin
– NauseaNausea– VomitingVomiting– WeakWeak
– Mild feverMild fever
– DyspneaDyspnea– AsymptomaticAsymptomatic

Physical FindingsPhysical FindingsPhysical FindingsPhysical Findings
• Inspection
BP - often increase anterior MI
- often decrease inferior MI
HR - often increase anterior MI
- often decrease inferior MI

Diagnosis of ACSDiagnosis of ACS
Typical symptoms Crescendo, rest, or new
onset severe angina
Serum biomarkers No Yes Yes
ECG initial findings ST depression and/or ST depression and/ ST elevation (and Q
T wave inversion or T wave inversion waves later)
Unstable Angina Myocardial Infarction
Prolonged “crushing” chest pain, more
severe and wider radiation than usual angina
NSTEMINSTEMI STEMISTEMI
NSTEMINSTEMI, non-ST-elevation myocardial infarction (MI); , non-ST-elevation myocardial infarction (MI); STEMISTEMI, ST-elevation MI, ST-elevation MI

Lilly. Pathophysiology of Heart Disease, 4th Ed. Lippincott Williams, 2007. Page 182
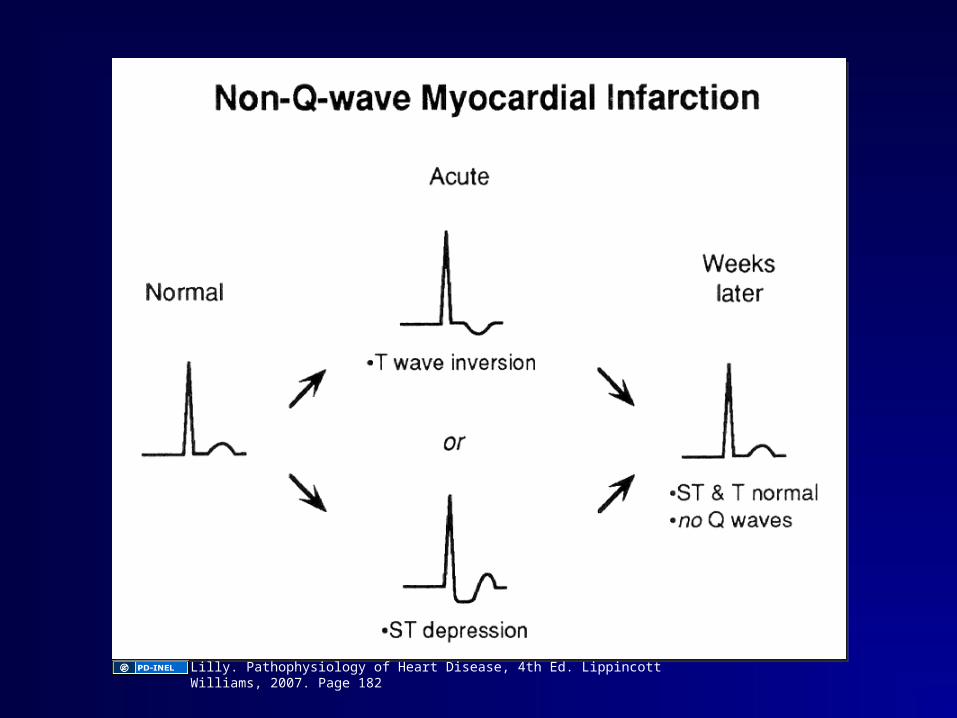
Lilly. Pathophysiology of Heart Disease, 4th Ed. Lippincott Williams, 2007. Page 182
Serum Markers ofSerum Markers ofMyocardial InfarctionMyocardial Infarction
Serum Markers ofSerum Markers ofMyocardial InfarctionMyocardial Infarction
• Myocardial necrosis causes sarcolemma
disruption
• Intracellular macromolecules are released
• Can be measured by serial blood testing
• Pattern and level of rise correlates with
timing and size of MI

Cardiac-Specific TroponinsCardiac-Specific Troponins
• Regulatory protein that controls interaction
between actin & myosin
• 3 subunits: TnC, I, T
• Unique cardiac troponins I and T exist - absent in
serum of healthy people
• Powerful marker of myocyte damage
• Rise at 3-4 hours post-MI, peak 18-36 hrs,
decline slowly 10-14 days
Skeletal &Skeletal &cardiac musclecardiac muscle

Creatinine KinaseCreatinine Kinase
• Enzyme that converts ADP to ATP
• Found in many tissues: heart, brain, skeletal muscle, kidney, etc.
• Can be elevated after injury to any of these tissues
• 3 isoenzymes: - CK-MM- CK-MB- CK-BB

CPK-MBCPK-MB
• Makes up 1-3% of skeletal CK
• Makes up much higher % of cardiac CK
• Rises 4-8 hours after MI, peaks by 24 hours
• Returns to normal in 48-72 hours

Treatment of AcuteTreatment of Acute
Coronary Syndromes:Coronary Syndromes:
STE vs. Non STESTE vs. Non STE

Treatment of Acute Coronary Treatment of Acute Coronary SyndromesSyndromes
• Anti-ischemic therapiesAnti-ischemic therapies
• General measures:General measures:
• Antithrombotic therapiesAntithrombotic therapiesAntiplatelet agents:Antiplatelet agents:
Anticoagulants (use one):Anticoagulants (use one):
• Adjunctive therapies:Adjunctive therapies:
• ΒΒ-blocker-blocker• NitratesNitrates• +/- Calcium channel blocker+/- Calcium channel blocker
• Pain control (morphine)Pain control (morphine)• Supplemental OSupplemental O22 if needed if needed
• AspirinAspirin• Clopidogrel (or prasugrel)Clopidogrel (or prasugrel)
• LMWH (enoxaparin)LMWH (enoxaparin)• Unfractionated intravenous heparinUnfractionated intravenous heparin• FondaparinuxFondaparinux• Bivalirudin (should be used in ACS Bivalirudin (should be used in ACS
patient only if undergoing PCI)patient only if undergoing PCI)
• StatinStatin• Angiotensin converting-enzyme inhibitorAngiotensin converting-enzyme inhibitor
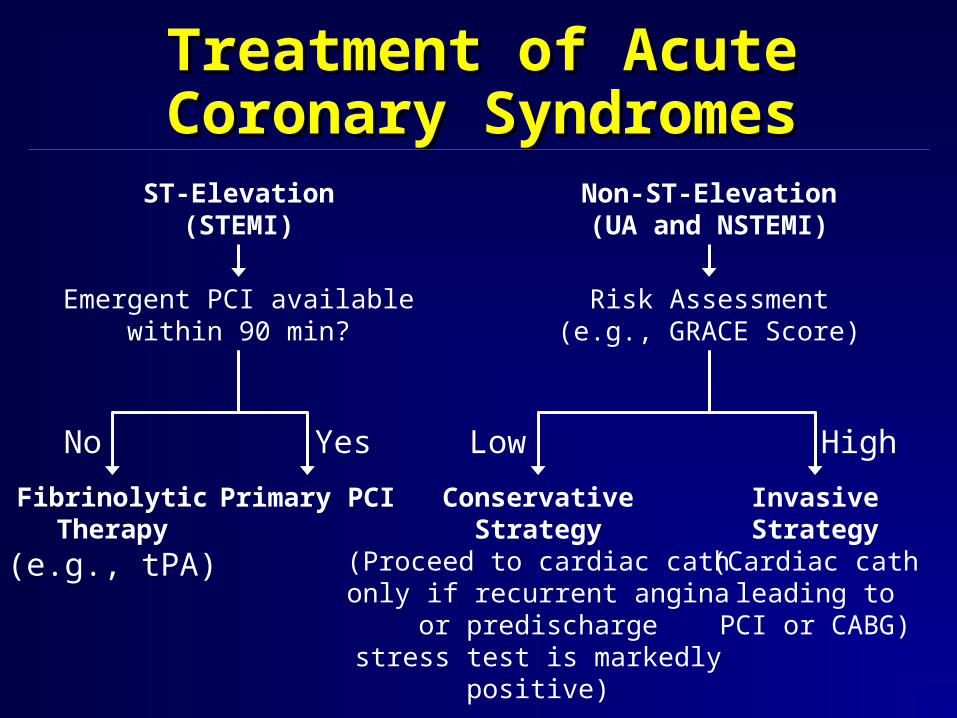
Treatment of Acute Coronary Treatment of Acute Coronary SyndromesSyndromes
ST-Elevation(STEMI)
Emergent PCI availablewithin 90 min?
FibrinolyticTherapy
(e.g., tPA)
Non-ST-Elevation(UA and NSTEMI)
Risk Assessment(e.g., GRACE Score)
Primary PCI ConservativeStrategy
(Proceed to cardiac cathonly if recurrent angina
or predischargestress test is markedly
positive)
InvasiveStrategy
(Cardiac cathleading to
PCI or CABG)
No Yes Low High

NitratesNitrates
• Reduce ischemia (not mortality)
• Venodilation: R heart return
• Coronary vasodilation
• Usually given SL then IV

Beta BlockersBeta Blockers
• Sympathetic drive; HR & BP
• O2 demand
• Shear stress
• Sudden death, death, recurrent MI

Non DihydropyridineNon DihydropyridineCalcium Channel BlockersCalcium Channel Blockers
• Heart rate
• Vasodilate
• Relieve ischemia, not mortality
• Don’t give in patients with sx/signs
of heart failure

Non - STE ACS:Non - STE ACS:
Conservative vs. EarlyConservative vs. Early
Invasive ApproachInvasive Approach

Early InvasiveEarly Invasive
• Urgent catheterization performed after
initial medical Rx
• Allows rapid identification & Rx of
critical CAD
• More PCI/CABG
Acute Treatment: STE MIAcute Treatment: STE MI
• Reperfusion: Thrombolysis vs. PTCA
• ASA
• O2
• Beta blockers
• Nitrates
• ACE inhibitors
• Morphine
• Anticoagulants

Additional Rx: STE MIAdditional Rx: STE MI
• Maintain vessel patency
• Restore balance between 02 supply
and demand
• Relieve chest pain
• Prevent complications

AspirinAspirin
• Reduces mortality & reinfarction
• Give immediately on presentation
and daily thereafter
• If aspirin allergy, use clopidogrel
HeparinHeparin
• Give 1-2 days IV after PCI or lysis with tPA, rPA, or TNK-tPA… NOT SK
• Also if:
– Atrial fibrillation
– LV thrombus
– New anterior MI with large wall motion change
• All others: SQ heparin while at bed rest to prevent DVT

ß- Blockersß- Blockers
• Risk arrhythmia, reinfarction, rupture,
death
• Give IV, then orally unless
contraindication exists (asthma,
hypotension, significant bradycardia)

NitratesNitrates
• Reduce pain/ischemia
• Relieve pain
• Reduce pulmonary congestion in
heart failure

ACE - InhibitorsACE - Inhibitors
• Limit adverse LV remodeling
• Heart failure/death
• MI
• Benefit additive ASA, BB
• Esp. benefit anterior MI and/or LV
dysfunction

StatinsStatins
• Reduce reinfarction, death
• More benefit when started early
• Give if LDL cholesterol is > 100

Acute MI: ComplicationsAcute MI: Complications
• Recurrent ischemic/reinfarction
• Arrhythmias
• Myocardial dysfunction
• Mechanical complications
• Pericarditis
• Thromboembolism

Complications of MIComplications of MIMyocardial InfarctionMyocardial Infarction
VentricularVentricularthrombusthrombus ContractilityContractility ElectricalElectrical
instabilityinstabilityTissueTissue
necrosisnecrosisPericardialPericardial
inflammationinflammation
EmbolismEmbolism ArrhythmiasArrhythmias PericarditisPericarditis
PapillaryPapillarymusclemuscle
infarction/infarction/ischemiaischemia
VentricularVentricularseptalseptaldefectdefect
VentricularVentricularrupturerupture
MitralMitralregurgitationregurgitation
CongestiveCongestiveheart failureheart failure
CoronaryCoronaryperfusionperfusionpressurepressure
IschemiaIschemia HypotensionHypotension
CardiogenicCardiogenicshockshock
CardiacCardiactamponadetamponade
Standard Discharge RxStandard Discharge Rx• 3 to 5 day length of stay• ASA; clopidogrel• Beta blocker• ACE for CHF; LVEF < 40%, perhaps all• Warfarin as noted• Cardiac Rehab• PRN Nitrates• Exercise prescription• Low fat diet• Smoking Cessation• Statin if LDL cholesterol > 100 mg/dl
Related Documents






![Digitpa CAD.ppt [modalità compatibilità] · 2011. 6. 20. · The Kubus Method Innovation Fund Blue Ocean Strategy A typical week in 202x Open Space Scenario Building ... Cellulari](https://static.cupdf.com/doc/110x72/6121f02ccc1d473a785b6686/digitpa-cadppt-modalit-compatibilit-2011-6-20-the-kubus-method-innovation.jpg)




