Human Papillomavirus Testing and Molecular Markers of Cervical Dysplasia and Carcinoma Donna Dehn, PhD Kathleen C. Torkko, PhD Kenneth R. Shroyer, MD, PhD Department of Pathology, University of Colorado at Denver and Health Sciences Center, Aurora, Colo- rado. Cervical cancer is the second most common cancer in women worldwide. Human papillomavirus (HPV) is the etiologic agent for the vast majority of premalignant and malignant lesions, and high-risk HPV types can be detected in almost all cases of cervical dysplasia and carcinoma. HPV testing has been widely adopted for the triage of patients after a cervical cytology screening test (Papanicolaou smear or liquid-based cervical cytology such as ThinPrep or SurePath) interpretation of atypi- cal squamous cells of undetermined significance (ASCUS), and HPV testing is increasingly used for screening in conjunction with cervical cytology. Although cer- vical cytology is a highly effective screening test for cancer, it has limited specificity for clinically significant lesions in cases with low-grade cytologic abnormalities. Up to a quarter of all patients may have a false-negative result on the basis of cervical cytology testing alone. This review focuses on HPV testing methods and molecular markers and their clinical relevance. HPV testing and surrogate molecular markers of HPV infection (p16 INK4a ) may help identify cases that are associated with under- lying high-grade premalignant or malignant lesions and may also reduce aggressive treatment of patients with low-grade lesions. Cancer (Cancer Cytopathol) 2007;111:1–14. Ó 2007 American Cancer Society. KEYWORDS: cervix, dysplasia, CIN, cytology, HPV, p16 INK4a . C ervical cancer is the third most common malignancy of the female genital system and is the second most common cancer in women worldwide. 1 The American Cancer Society estimates that about 9700 American women will be diagnosed with cervical cancer in 2006 and that 3700 will die from the disease. 2 Furthermore, 330,000 new cases of high-grade cervical dysplasia (CIN2/3) and 1.4 million new cases of low-grade cervical dysplasia (CIN1) are diag- nosed in the United States every year. 3 Epidemiologic and laboratory data support the conclusion that human papillomavirus (HPV) is the etiologic agent for the vast major- ity of premalignant and malignant epithelial lesions of the cervical mucosa, as HPV DNA can be detected in 95% to 100% all cases. 4 The estimated incidence of HPV infection in the United States is 6.2 mil- lion per year, with an estimated prevalence of 20 million. 5 In women younger than 25 years of age, HPV infection rates have been reported to range from 28% to 46%. 6,7 In the vast majority of cases, HPV infec- tions are usually transient and do not necessarily lead to clinically sig- nificant lesions of the cervical mucosa. 8 Given the high incidence of HPV infection compared with the low prevalence of cervical cancer, other factors must be involved in the malignant transformation of the cervical mucosa. Cofactors may include smoking, 9,10 oral contracep- tive use, 11 parity, 12 infection with other sexually transmitted diseases such as Herpes simplex-2 13,14 and host factors. Kenneth R. Shroyer is a member of the TriPath Oncology Scientific Advisory Board and has pre- viously received honoraria from TriPath, but this association and these funds are not related to the preparation of this article. Address for reprints: Kenneth R. Shroyer, MD, PhD, Department of Pathology, University of Colorado at Denver and Health Sciences Center, Mail Stop 8104, 12800 East 19 th Avenue, Aurora, CO 80045; Fax: (303) 724-3712; E-mail: ken.shroyer@uchsc. edu Received August 8, 2006; revision received October 20, 2006; accepted October 23, 2006. ª 2007 American Cancer Society DOI 10.1002/cncr.22425 Published online 11 January 2007 in Wiley InterScience (www.interscience.wiley.com). 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Human Papillomavirus Testing and Molecular Markersof Cervical Dysplasia and Carcinoma
Donna Dehn, PhDKathleen C. Torkko, PhDKenneth R. Shroyer, MD, PhD
Department of Pathology, University of Colorado atDenver and Health Sciences Center, Aurora, Colo-rado.
Cervical cancer is the second most common cancer in women worldwide. Human
papillomavirus (HPV) is the etiologic agent for the vast majority of premalignant
and malignant lesions, and high-risk HPV types can be detected in almost all cases
of cervical dysplasia and carcinoma. HPV testing has been widely adopted for the
triage of patients after a cervical cytology screening test (Papanicolaou smear or
liquid-based cervical cytology such as ThinPrep or SurePath) interpretation of atypi-
cal squamous cells of undetermined significance (ASCUS), and HPV testing is
increasingly used for screening in conjunction with cervical cytology. Although cer-
vical cytology is a highly effective screening test for cancer, it has limited specificity
for clinically significant lesions in cases with low-grade cytologic abnormalities. Up
to a quarter of all patients may have a false-negative result on the basis of cervical
cytology testing alone. This review focuses on HPV testing methods and molecular
markers and their clinical relevance. HPV testing and surrogate molecular markers
of HPV infection (p16INK4a) may help identify cases that are associated with under-
lying high-grade premalignant or malignant lesions and may also reduce aggressive
treatment of patients with low-grade lesions. Cancer (Cancer Cytopathol)
2007;111:1–14. � 2007 American Cancer Society.
KEYWORDS: cervix, dysplasia, CIN, cytology, HPV, p16INK4a.
C ervical cancer is the third most common malignancy of the
female genital system and is the second most common cancer in
women worldwide.1 The American Cancer Society estimates that
about 9700 American women will be diagnosed with cervical cancer
in 2006 and that 3700 will die from the disease.2 Furthermore,
330,000 new cases of high-grade cervical dysplasia (CIN2/3) and
1.4 million new cases of low-grade cervical dysplasia (CIN1) are diag-
nosed in the United States every year.3
Epidemiologic and laboratory data support the conclusion that
human papillomavirus (HPV) is the etiologic agent for the vast major-
ity of premalignant and malignant epithelial lesions of the cervical
mucosa, as HPV DNA can be detected in 95% to 100% all cases.4 The
estimated incidence of HPV infection in the United States is 6.2 mil-
lion per year, with an estimated prevalence of 20 million.5 In women
younger than 25 years of age, HPV infection rates have been reported
to range from 28% to 46%.6,7 In the vast majority of cases, HPV infec-
tions are usually transient and do not necessarily lead to clinically sig-
nificant lesions of the cervical mucosa.8 Given the high incidence of
HPV infection compared with the low prevalence of cervical cancer,
other factors must be involved in the malignant transformation of the
cervical mucosa. Cofactors may include smoking,9,10 oral contracep-
tive use,11 parity,12 infection with other sexually transmitted diseases
such as Herpes simplex-213,14 and host factors.
Kenneth R. Shroyer is a member of the TriPathOncology Scientific Advisory Board and has pre-viously received honoraria from TriPath, but thisassociation and these funds are not related to thepreparation of this article.
Address for reprints: Kenneth R. Shroyer, MD, PhD,Department of Pathology, University of Colorado atDenver and Health Sciences Center, Mail Stop8104, 12800 East 19th Avenue, Aurora, CO 80045;Fax: (303) 724-3712; E-mail: [email protected]
Received August 8, 2006; revision receivedOctober 20, 2006; accepted October 23, 2006.
ª 2007 American Cancer SocietyDOI 10.1002/cncr.22425Published online 11 January 2007 in Wiley InterScience (www.interscience.wiley.com).
1

HPV DNA studies have provided unique tools for
cervical cancer screening but depend on various clini-
cal and molecular biologic factors that impact clinical
utility. HPV testing has been widely adopted for the
triage of patients with atypical squamous cells of un-
determined significance (ASCUS) and is increasingly
used for primary screening in conjunction with cervi-
cal cytology testing in patients older than 30 years.
However, HPV testing has limited utility for the triage
of patients with other low-grade cytologic abnormal-
ities or for cervical cancer screening in younger
women. The aims of this article are the of review cur-
rent approaches for HPV testing and consideration of
surrogate molecular markers of HPV infection, such
as p16INK4a, that may help identify cases that are most
likely to be associated with underlying high-grade
premalignant or malignant lesions.
HPV PRIMERThe HPV virus has a double-stranded circularized ge-
nome that can be divided into early (E1-E7) and late
(L1, L2) open reading frames (ORF). The late ORFs L1
and L2 encode the 2 viral capsid proteins, whereas
the early ORFs encode proteins that are involved in
regulation of DNA replication and cell proliferation.
The more than 100 different HPV types are character-
ized on the basis of nucleotide sequence differences
of the L1 ORF; over 40 types are known to infect the
cervical mucosa. Epidemiologic studies have divided
these viruses into low-risk types (including types 6,
11, 40, 42, 54, and 57) and high-risk types (including
types 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58,
59, 66, and 68) for cervical cancer.15,16 Low-risk types
are associated with benign lesions, referred to as geni-
tal warts or condyloma acuminate, whereas high-risk
types (about 90% of cervical infections)17 may result
in dysplastic lesions, including invasive cancer.
Squamous maturation supports high levels of HPV
episomal replication in CIN1.18 By contrast, high-grade
lesions often represent nonproductive infections that
may be driven by HPV viral integration but may sup-
port only a low copy number of HPV DNA.18 These fac-
tors are important considerations in the development
of molecular strategies for the specific detection of
high-grade lesions, because the viral load of HPV, per
se, would not be predicted to be a direct reflection of
the levels of genomic integration and malignant trans-
formation. In productive HPV infections, HPV DNA
remains in an episomal state, and the E1/E2 ORFs
repress the expression of the 2 most important HPV
oncoproteins, E6 and E7.18,19 In high-grade dysplasia
and in carcinoma, however, E1/E2 is frequently dis-
rupted by integration of viral DNA into the host ge-
nome, resulting in the unregulated overexpression of
E6 and E7.18,20 The overexpression of E6 promotes the
degradation of the cell cycle regulatory protein p53
through the ubiquitin-mediated pathway, resulting in
unchecked cell cycle progression.15,21 By contrast, the
E7 oncoprotein binds to and promotes the degradation
of the retinoblastoma gene (Rb), resulting in disrup-
tion of the Rb cyclin D/p16INK4a cell cycle regulatory
pathway.22 In turn, down-regulation of Rb results in
hypomethylation of the p16INK4a promoter and a recip-
rocal intense p16INK4a overexpression.23,24
CYTOLOGICAL TESTING AND LIMITATIONS OFCURRENT PRACTICEThe cervical cytology test is the most effective screen-
ing test for cancer that has ever been devised, but it
still has limited specificity for clinically significant
lesions in cases with low-grade cytologic abnormal-
ities, and it may have high false-negative screening
test results. Over 3 million cases are diagnosed in the
United States each year as atypical squamous cells of
undetermined significance (ASCUS), atypical squamous
cells suspicious cannot exclude high-grade squamous
intraepithelial lesion (ASC-H), low-grade squamous in-
traepithelial lesion (LSIL), or atypical glandular cells
(AGC). These cases require further evaluation to identify
the subset of patients that will have clinically significant
high-grade lesions on cervical biopsy (Table 1). Although
colposcopic biopsy has historically been considered
the gold standard, recent reports indicate that cervical
biopsies may miss 33% to 50% of high-grade disease
because of sampling or diagnostic errors.3,25–34 As a
result, it may be difficult to differentiate between false-
positive cervical cytology test results versus false-nega-
tive biopsy results. Nevertheless, patients with a cyto-
logic diagnosis of ASCUS have a 5% to 17% chance of
harboring an underlying CIN2/3 on cervical biopsy,
and the diagnosis of ASC-H carries a 24% to 94%
chance of CIN2/3 on colposcopic biopsy. In LSIL cases
that were referred for colposcopic examination, high-
grade cervical dysplasia (CIN grade 2 or 3) was found
TABLE 1Clinically Equivocal Cytologic Diagnostic Categories*
Cytologic
Diagnosis
Total Cases (Annual
US Population)*
No Clinically Significant
Lesion On Colposcopy
ASCUS >2 million 1.66–1.9 million
ASC-H 0.20 million (estimated) 0.001–0.15 million
LSIL 1.65 million 1.24 million
AGC 0.31 million 0.18–0.25 million
Total >4.16 million 2.66–3.54 million
* Data summarized from references20,122–129
2 CANCER (CANCER CYTOPATHOLOGY) February 25, 2007 / Volume 111 / Number 1

in 25%, CIN1 was found in 45%, but no dysplasia was
found in over 25% of cases.31 Similarly, cases with a di-
agnosis of AGC have been found to have a 9% to 41%
risk of CIN2, CIN3, or adenocarcinoma in situ (AIS),
but the majority of AGC cases do not have clinically
significant lesions of either the squamous or glandular
mucosa.32 Reports of false-negative rates in cervical
cytology have varied widely, from as low as 1.6% to
almost 28 %.35–38 Furthermore, cervical smears from
patients with invasive cervical carcinoma may have an
even higher risk of false-negative cytologic diagnoses
because of the presence of few to rare abnormal cells,
obscuring necrotic debris, inflammation, or bleed-
ing.39–47 Similarly, there is a relatively high false-nega-
tive rate for AIS, and cervical cytology may have a
false-negative rate of up to 50% for invasive endocervi-
cal adenocarcinoma.48,49 Thus, there is a critical clini-
cal need to identify molecular diagnostic adjuncts,
which may also improve specificity of the cervical cy-
tology test for detection of high-grade dysplasia and
carcinoma and reduce the risk of false-negative cervi-
cal cytology test results.
HPV testingThe American Society for Colposcopy and Cervical Pa-
thology consensus-based guidelines (http://www.asccp.
org/edu/practice/cervix.shtml) support the use of HPV
testing as a diagnostic adjunct to triage patients with
ASCUS, but these guidelines do not support the use of
HPV testing for triage of patients with other abnormal
cervical cytology test results. Stoler50 calculated HPV
triage to be equal to or more sensitive than colposcopy
for this group of patients. Although high-risk HPVs are
present in a very high proportion of abnormal cervical
cytology test specimens, many patients with ASCUS
cytology have only mild cytologic manifestations re-
lated to transient HPV infection, effectively limiting
the specificity of HPV testing in this group of patients.
Furthermore, the low prevalence of underlying high-
grade lesions and the high prevalence of transient HPV
infection limits the effectiveness of HPV as a screening
test in the general population under the age of 30 years
in the United States.51 Thus, there continues to be a
need for more effective HPV test methods (those with
increased specificity and high negative predictive
value), for validation of other molecular markers to
better identify patients that are at greatest risk for cer-
vical cancer, and for deferment of aggressive manage-
ment of patients with only low-grade lesions.
Diagnosing HPV infection requires the detection
of HPV genetic information in cellular samples col-
lected from the site of infection. Cytologic samples
are generally collected in PreservCyt (ThinPrep, Cytyc,
Boxborough, Mass) or Specimen Transport Medium
(Digene, Gaithersburg, Md). PreservCyt is a methanol-
based fixative that preserves cellular morphology,
whereas Specimen Transport Medium is a water-based
proprietary aliphatic amine designed as a DNA pre-
servative.52 PreservCyt can be used for recovery and
detection of HPV RNA after 1 year of storage at
�208C.53 One study found that samples stored in Pre-
servCyt should be used within 4 to 5 years before a sig-
nificant loss in DNA integrity is detected by PCR.54
Generally, either collection media can be effectively
used for HPV testing. Specific limitations are addressed
within each method. Formalin-fixed, paraffin-embed-
ded biopsy samples are also used for HPV testing. Type
of fixative and length of fixation can affect the quality
of nucleic acids in paraffin tissue blocks and, therefore,
the usefulness of these samples for testing.
It cannot be overstressed that clinical validation
is necessary for all HPV assays. The Food and Drug
Administration (FDA) has approved only 1 HPV assay,
and part of the approval process included clinical val-
idation.34 Clinical validation is a measure of how a
test performs in the real world. Clinical validation
establishes a test performance relative to a reference
or ‘‘gold standard’’ and provides a statistical measure
for the question, Is a negative test result indicative of
a negative disease state? Given the limitations of cer-
vical biopsy as the gold standard for disease status,
however, clinical validation of any putative marker of
underlying high-grade dysplasia or carcinoma is prob-
lematic. Nevertheless, most HPV assays are measured
against the performance of colposcopy biopsy or the
Hybrid Capture II test, an FDA-approved method,
when validation data are provided at all. Performance
indicators depend on prevalence of both HPV and
cervical disease in the target population and, there-
fore, should be determined by each laboratory on the
basis of the population served.
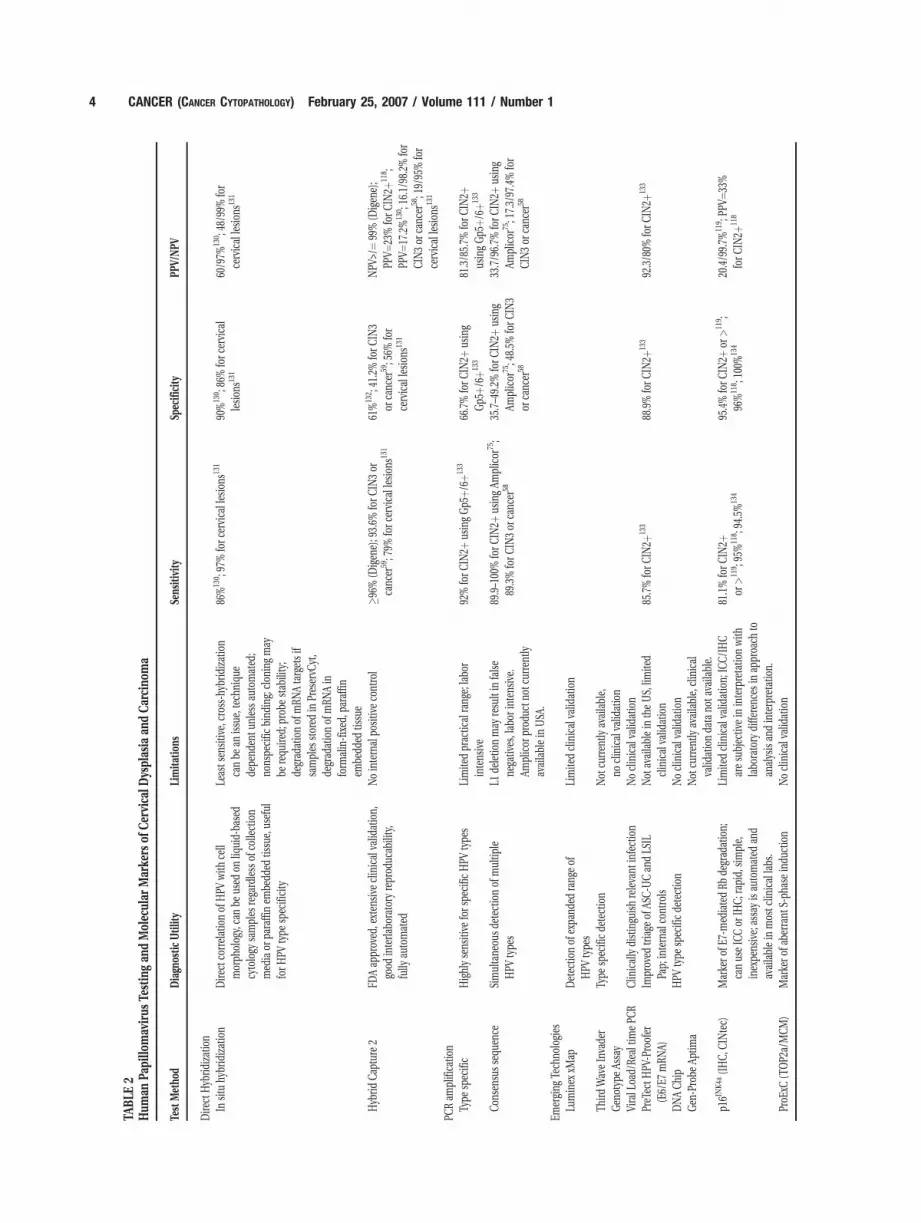
There are 2 main methods for detecting HPV,
direct hybridization (eg, Southern blot, dot blot, in situ
hybridization), and amplification (ie, polymerase chain
reaction [PCR]).Table 2 summarizes the usefulness,
limitations, and sensitivity and specificity (if available)
of the methods discussed below.
Direct hybridizationIn situ hybridization is based on the complementary
pairing of a labeled probe to HPV antigens or nucleic
acids (DNA or mRNA) within either paraffin-embed-
ded tissue biopsies or cervical smears. Biotinylated
probes can then be detected with routine chromogenic
substrates, and the assay can be automated for clinical
use (Ventana Benchmark Staining System, Ventana
Medical Systems, Tucson, Ariz). Improvements in sen-
sitivity have been made by amplification of the signal
HPV Testing and Molecular Markers/Dehn et al. 3
TABLE
2Hum
anPa
pillo
mav
irus
Testingan
dMolec
ular
Marke
rsof
Cervica
lDysplasia
andCarcino
ma
Test
Metho
dDiagn
osticUtility
Limitations
Sens
itivity
Spec
ificity
PPV/
NPV
Direc
tHyb
ridizatio
n
Insitu
hybridization
Directc
orrelatio
nof
HPV
with
cell
morph
olog
y,ca
nbe
used
onliq
uid-ba
sed
cytology
samples
rega
rdless
ofco
llection
med
iaor
paraffinem
bedd
edtis
sue,
useful
forHPV
type
spec
ificity
Leasts
ensitiv
e,cros
s-hy
bridization
canbe
anissu
e,tech
niqu
e
depe
nden
tunlessau
tomated
;
nons
pecific
bind
ing;
clon
ingmay
berequ
ired
;probe
stab
ility;
degrad
ationof
mRN
Atargetsif
samples
stored
inPreservC
yt,
degrad
ationof
mRN
Ain
form
alin-fixed
,paraffin
embe
dded
tissu
e
86%
130 ;97
%force
rvical
lesion
s131
90%
130 ;86
%forc
ervica
l
lesion
s131
60/97%
130 ;48
/99%
for
cervical
lesion
s131
Hyb
ridCap
ture
2FD
Aap
prov
ed,e
xten
sive
clinical
valid
ation,
good
interlab
oratoryreprod
ucab
ility,
fully
automated
Nointernal
positiv
eco
ntrol
�96%
(Digen
e);9
3.6%
forCIN
3or
canc
er59;7
9%forc
ervica
llesions
131
61%
132 ;41
.2%
forCIN
3
orca
ncer
59;5
6%for
cervical
lesion
s131
NPV
>/¼9
9%(D
igen
e);
PPV¼
23%
forCIN
2þ11
8 ;
PPV¼
17.2%
130 ;16
.1/98.2%
for
CIN
3or
canc
er58;1
9/95
%for
cervical
lesion
s131
PCRam
plifica
tion
Type
spec
ific
Highlysens
itive
forsp
ecificHPV
type
sLimite
dprac
tical
rang
e;labo
r
intens
ive
92%
forCIN
2þus
ingGp5
þ/6þ
133
66.7%
forCIN
2þus
ing
Gp5
þ/6þ
133
81.3/85.7%
forCIN
2þus
ingGp5
þ/6þ
133
Con
sens
ussequ
ence
Simultane
ousde
tectionof
multip
le
HPV
type
s
L1de
letio
nmay
resu
ltin
false
nega
tives,lab
orintens
ive.
Amplicor
prod
uctn
otcu
rren
tly
availablein
USA
.
89.9–1
00%
forCIN
2þus
ingAm
plicor
75;
89.3%
forCIN
3or
canc
er58
35.7–4
9.2%
forCIN
2þus
ing
Amplicor
75;4
8.5%
forCIN
3
orca
ncer
58
33.7/96.7%
forCIN
2þus
ing
Amplicor
75;1
7.3/97
.4%
for
CIN
3or
canc
er58
Emerging
Tech
nologies
Luminex
xMap
Detec
tionof
expa
nded
rang
eof
HPV
type
s
Limite
dclinical
valid
ation
Third
Wav
eInva
der
Gen
otyp
eAs
say
Type
spec
ificde
tection
Not
curren
tlyav
ailable,
noclinical
valid
ation
ViralL
oad/
Real
timePC
RClin
ically
distingu
ishreleva
ntinfection
Noclinical
valid
ation
PreT
ectH
PV-Proofer
(E6/E7
mRN
A)
Improv
edtriage
ofAS
C-U
Can
dLS
IL
Pap;
internal
controls
Not
availablein
theUS,
limite
d
clinical
valid
ation
85.7%
forCIN
2þ13
388
.9%
forCIN
2þ13
392
.3/80%
forCIN
2þ13
3
DNAChip
HPV
type
spec
ificde
tection
Noclinical
valid
ation
Gen
-Probe
Aptim
aNot
curren
tlyav
ailable,
clinical
valid
ationda
tano
tava
ilable.
p16IN
K4a
(IHC,C
INtec)
Marke
rof
E7-m
ediatedRb
degrad
ation;
canus
eIC
Cor
IHC;rap
id,sim
ple,
inexpe
nsive;
assayis
automated
and
availablein
mos
tclin
ical
labs
.
Limite
dclinical
valid
ation;
ICC/IHC
aresu
bjec
tivein
interpretatio
nwith
labo
ratory
diffe
renc
esin
approa
chto
analysis
andinterpretatio
n.
81.1%
forCIN
2þor
>11
9 ;95
%11
8 ;94
.5%
134
95.4%
forCIN
2þor
>11
9 ;
96%
118 ;10
0%13
420
.4/99.7%
119 ;PP
V¼33
%
forCIN
2þ11
8
ProE
xC(T
OP2
a/MCM)
Marke
rof
aberrant
S-ph
aseindu
ction
Noclinical
valid
ation
4 CANCER (CANCER CYTOPATHOLOGY) February 25, 2007 / Volume 111 / Number 1

(catalyzed reporter deposition or CARD), use of fluo-
rescent probes, more stringent protocols for efficient
observation of the DNA or RNA target,55 use of smaller
nanoprobes to access nuclear antigens (Nanoprobes,
Yaphank, NY), and a combination of techniques.49
However, loss of target nucleic acids through sample
collection, preservation, or processing remains an im-
portant limitation of the technique. Most commer-
cially available DNA probes contain grouped probes
for typing HPV. For example, Enzo Life Sciences, Inc.
(Farmingdale, NY) and DakoCytomation (Copenhagen,
Denmark) in situ screening and typing assays can
detect HPV type 16 and 18 but cannot distinguish be-
tween them. Some vendors (Bio Genex, San Ramon,
Calif) sell both oligonucleotide probe cocktails and
type-specific individual probes. Ventana sells a chro-
mogenic INFORM HPV assay that contains 13 geno-
types for high-risk HPVs.
An advantage of in situ hybridization is that HPV
infection can be identified within specific cells (tumor
versus normal cells or koilocytes), and its physical sta-
tus also may be determined (integration into the cellu-
lar genome or episomal HPV.55 If the detection method
is sufficiently sensitive, the number of integrated HPV
copies can be determined as well. Cost is the major
disadvantage, as multiple in situ hybridization experi-
ments must be undertaken for each sample for HPV
typing.
The only FDA-approved test for HPV detection,
the Hybrid Capture 2 (HC2) technologies from Digene
(Gaithersburg, Md), is a solution-phase hybridization
assay that results in signal amplification. This is the
mostly widely used, clinically validated assay on the
market today. The assay uses RNA probes that react
with 13 high-risk (ie, 16, 18, 31, 33, 35, 39, 45, 51, 52,
56, 58, 59, and 68) or 5 low-risk (6, 11, 42–44) DNA
targets. Because the detection of low-risk types has no
clinical significance, testing is usually done only with
the high-risk probe set.57 These RNA-DNA hybrids are
captured by monoclonal antibodies bound to the
walls of a 96-well plate and detected with antihybrid
antibodies by chemiluminescence.20 Studies have
found that specimens collected in PreservCyt have a
higher level of nonspecific detection than samples col-
lected in Specimen Transport Medium, although both
can be used for this assay.52,58 Results can be expressed
as a ratio of the specimens signal strength in relative
light units (RLU) to that of concurrently tested 1 pg/
mL HPV DNA controls (the FDA-approved threshold
for a positive result). This can provide a semiquantita-
tive measure of viral load relative to 1 pg/ml.57,59,60
However, this assay has no ability to control for the
amount of input DNA. The HC2 Assay is formatted to
detect only the presence of certain high-risk or low-
risk HPV types and will not identify specific types,
but it will report that at least 1 of the high-risk or
low-risk types is present. This is an important limi-
tation of the assay, as genotyping can identify the
presence of persistent high-risk types that are a risk
factor for progression to cervical cancer.59 Although
treatment is currently not defined by specific HPV
type, vaccine usefulness could be limited if there is
presence of infection by certain types. Advantages
of this method include good interlaboratory repro-
ducibility57 and ease of use. The HC2 assay uses a
96-well format similar to enzyme-linked immuno-
sorbent assays (EIA) that are commonly performed
in clinical laboratories.
AmplificationPCR technologies amplify small portions of HPV DNA,
thus allowing testing on samples with less tissue or
cells, poorer quality DNA, or fewer viral copies. A tar-
get DNA sequence can be amplified a million-fold in
about 1 hour.61 All PCR assays are suitable for large-
scale testing in clinical settings, although separate lab-
oratory areas are generally necessary for sample prepa-
ration and PCR reactions. There are 2 main types of
PCR tests available, type-specific and consensus assays.
The type-specific assays are designed to amplify a sin-
gle HPV genotype. Multiple PCR reactions would then
be performed separately, increasing both the time and
cost for genotyping each sample.62 Consensus assays
allow detection of a broad range of HPV types. Primers
are designed to target conserved regions among differ-
ent genotypes. The L1 region is not only highly con-
served, it is used in the formal classification of HPV
types because of sequence relatedness.20,57,62 The most
commonly used primers target the L1 region. Initially,
degenerate primer pairs were used (MY09/11). Use of
oligonucleotides containing degeneracies can result in
a lack of reproducibility and high variation between
PCR runs. These have now been replaced with a set of
oligonucleotide pools obtained by grouping virus types
together by sequence homology over the same MY09/
11 primer regions. This results in 5 upstream oligonu-
cleotides for the PGMY11 primer pool and a set of 13
downstream oligonucleotides for the PGMY09 primer
pool.63 This primer set amplifies a 450-base pair (bp)
fragment. The GP5þ/6þ primer set amplifies a 150-bp
fragment of the L1 region. The SPF10 primers amplify
only a 65-bp region with 10 different PCR primers (6
forward and 4 reverse). These primers contain an ino-
sine nucleotide (matching with any base) to maximize
any target regions of different genotypes.64 Although it
would be expected that this primer set would have
enhanced sensitivity because PCR efficiency is inver-
HPV Testing and Molecular Markers/Dehn et al. 5

sely related to the size of the region amplified, the re-
sults between various investigations comparing primer
sets have had conflicting results.57
Some have argued that the L1 region may be lost
or disrupted during viral integration,65,66 which would
then cause false-negative results. However, others
have found that integration disrupts the E2 ORF,
which results in a loss of transcriptional regulatory
proteins and the continued expression of the E6 and
E7 oncoproteins.20,67 Primer sets targeting the E6 and
E7 regions have been constructed. In a recent study,68
31 primers were constructed for development of an
E7 primer pool to detect a large spectrum of high-risk
HPV types (19 types). Several primers represented more
than 1 HPV type because of homology in the E7 region.
An analysis between this novel primer pool and the
GP5þ/6þ primer set found the E7 PCR and a chip assay
based on an array primer extension (APEX) assay identi-
fied a higher number of infections with multiple HPV
types than did the GP5þ/6þ followed by reverse line
blotting. However, the E7 primer assay was less sensi-
tive for HPV 16. Better sensitivity and lower false-nega-
tive rates may be obtained if L1 and E6/E7 tests are
used in combination.
After amplification of the target DNA by PCR, the
specific type of HPV can be determined with nucleic
acid hybridization, restriction endonucleases, or
sequencing. Nucleic acid hybridization is probably the
most commonly used method for HPV typing. In the
microtiter assay, biotin-labeled, amplified PCR pro-
ducts are attached to the wells of streptavidin-coated
96-well plates. The now immobilized fragments are
denatured, then hybridized with digoxigenin-labeled
DNA probes complementary to the HPV type-specific
sequence. A colorimetric reaction is the final step, and
optical density is determined in a plate reader.69 In the
reverse line probe (line blot; LiPA) poly(dT) tails are
enzymatically added to the 30 end of the DNA probes,
and the probes are immobilized on nitrocellulose or
nylon strips in parallel lines at defined positions.
Hybridization at a specific line defines the HPV type.
This assay is also dependent upon a colorimetric reac-
tion and comparison of the resulting line position to
an established base line.64,70–73 The number of indivi-
dual HPV genotypes that can be determined varies
with the specific manufacturer of the strips. Numerous
studies have evaluated various available reverse hybri-
dization methods. Most conclude that there is a high
degree of correlation between methods for observing
single infections.64 Some have found the INNO-LiPA
test (Innogenetics, Temse, Belgium) has a greater sen-
sitivity for multiple infections due to the short PCR
products generated by the SPF10 primers used in the
assay.74
Roche Diagnostics Amplicor HPV test is a PCR
assay that uses L1 consensus biotinylated primers
(165-bp product) and the Linear Array line blot hybri-
dization with immobilized probes (available in the US
for research purposes only). The Amplicor HPV test
can determine the presence of 13 individual high-risk
DNA genotypes (Future versions will expand that to
37 high- and low-risk types.) and the human beta-glo-
bin gene as a positive control.74–77 To assess perform-
ance of the Amplicor HPV test in detection of cervical
pathology, Monsonego et al75 evaluated 270 patients
referred for colposcopy because of an abnormal cervi-
cal cytology. They used biopsy (colposcopic or loop
electrocautery excision procedure [LEEP cone biopsy])
as the gold standard. For detecting CIN2þ, the Ampli-
cor HPV test had a sensitivity of 95.2%, a specificity of
42.4%, a positive predictive value (PPV) of 33.7%, and
a negative predictive value (NPV) of 96.7%, all of which
compared well with colposcopy (96.5%, 36.3%, 30.9%,
and 97.2%, respectively). A recent comparison of the
Digene HC2 assay and Roche’s Amplicor HPV test in
Europe concluded that both tests give comparable
results, although the Amplicor HPV test demonstrated
a higher sensitivity and a slightly better accuracy in de-
tecting CIN3.76 However, the authors concluded that
the slightly different characteristics of the 2 tests may
suggest different optimal clinical uses; for example, the
ability of the Amplicor HPV test to detect CIN3 may
prove more useful in the triage of borderline smear re-
sults. This test is still relatively expensive and may prove
cost-effective only in high-throughput laboratories.
Klassen et al78 developed a high-density DNA mi-
croarray system to detect 53 HPV types with the use of
biotinylated HPV probes immobilized on streptavidin-
coated glass slides. Digoxigenin-labeled PCR products
are hybridized onto the probes, and a colorimetric and/
or fluorescent detection system is used (laser scanning
or light microscopy). Multiple primary amplification re-
actions must take place because of HPV–cluster-specific
PCR primers.78 Other investigators and vendors (Geno-
micTree, South Korea; MyGene, South Korea; Daiichi
Pure Chemicals/Toshiba, Japan) have developed micro-
arrays (DNA Chips) for detection of HPV genotypes,
although no studies have validated the clinical applic-
ability of these assays.79–82
Restriction fragment length polymorphism (RFLP)
requires the digestion of PCR products with various
restriction endonucleases that cut DNA at specified
base pairings. Each endonuclease digest results in frag-
ments of differing sizes that confer a unique banding
pattern for specific HPV types that can be detected by
agarose gel electrophoresis. To select an endonuclease
for use, a restriction map must be prepared for each
HPV genome of interest to enable the determination of
6 CANCER (CANCER CYTOPATHOLOGY) February 25, 2007 / Volume 111 / Number 1

the number of cuts the enzyme will make in the ampli-
fied segment of DNA. For example, Ras I can differenti-
ate between the 6 most common HPV types with 1
(HPV 31) to 4 (HPV 18) cuts generating 2 to 5 frag-
ments.83 Although the use of RFLP is inexpensive, it is
also labor intensive if more than 1 endonuclease is to be
used. Multiple digestions require a large volume of PCR
product, which may increase the cost per sample. Par-
tial digestion of PCR products because of variable ex-
perimental conditions can obfuscate the true results.84
Because RFLP is a manual technique, variations can
occur between each experiment.
Direct sequencing, although relatively expensive
on a per patient basis, can be performed on PCR pro-
ducts, and rapid methods are available for routine
analysis of samples.85 After sequencing data are avail-
able, the genotype can be identified by a BLAST
search for homology to existing sequences in the
database. A disadvantage of direct sequencing is the
lack of sensitivity in detecting multiple HPV types in a
single sample.62 This is a labor-intensive method that
is not routinely performed for HPV genotyping in clini-
cal samples.
Emerging technologiesNew technologies are actively being pursued for
rapid, specific, sensitive, and cost-effective methods
to enable HPV detection and genotype identification
in a clinical setting. The Luminex xMAP suspension
array technology will theoretically allow detection of
100 different HPV genotypes by type-specific oligonu-
cleotide probes coupled to internally dyed (2 spec-
trally distinct fluorochromes) polystyrene microbeads
(5.6 mm diameter) and analyzed on a Luminex 100
reader. Biotin-labeled PCR products are then hybri-
dized to the bead-coupled probes. The Luminex inter-
rogates each individual microbead with 2 separate
lasers in a high-flow fluid stream. The microbead is
classified on its spectral address (specific ratio of the
2 fluorochromes) and quantifies the hybridization on
the surface.86–88 The hybridization signal will depend
upon the PCR products generated and, therefore, the
primers used. If the products are too big, they may
not hybridize well because of steric hindrance at the
bead surface. GP5þ/6þ, MY09/11, and E7 primers
have all been shown to be effective at detecting both
single and multiple infections.87,88
Third Wave Technologies Inc. (Madison Wis) has
not yet released the HPV in vitro diagnostic (IVD) geno-
type assay, but it is assumed that it will be based on its
patented Invader assay. Third Wave currently sells HPV
analyte-specific reagents (ASRs) for use in ‘‘home-
brewed’’ assays. The Invader assay is a signal amplifica-
tion system for differentiating DNA targets on the basis
of sequence variation within a specified region of HPV
DNA. Detection of individual genotypes requires sepa-
rate assays that are performed in 96-well plates, a clini-
cally useful format. All reactions require a target-specific
oligonucleotide probe, a signal probe, and proprietary
Cleavase enzymes that cleave DNA at sites where a sub-
strate has been generated from the addition of oligonu-
cleotide probes. This cleavage product or ‘‘flap’’ enters a
secondary reaction in which Forster resonance energy
transfer (FRET) technology is used to generate a fluores-
cent signal that is detected in a fluorescent plate reader.
This assay generates an amplified signal only when the
specific target DNA sequences are present.89–91 Invader
technology works well for genotyping Hepatitis C virus,
although some experimental variation has been identi-
fied.89 The number of HPV genotypes that will be identi-
fiable by this new technology remains to be seen.
Viral load appears to have a positive correlation
with risk of high-grade cervical lesions and may prove
to be a valuable marker for prediction of disease.
High viral load indicates persistent infection and dis-
ease progression, whereas low viral loads indicate vi-
ral clearance.92 Real-time PCR assays that target type-
specific HPV DNA and normalize to the total human
DNA present provide the best method to determine
the viral copy number in a cervical cytology sample.93
Carcopino et al94 used real-time PCR and an albumin
copy control and found that HPV 16 and 18 viral loads
were related to the severity of the cervical lesion. The
HC2 assay also can be used to provide a semiquanti-
tative estimate of viral load. A comparison of relative
light units to positive controls can estimate viral
load.66 However, in measuring viral load, HC2 can fail
to detect low copy numbers that may be important to
the determination of disease progression.95
Expression of E6/E7 oncogenes is required for
continued degradation of p53 and Rb and the resulting
malignant transformation of cells.96 The PreTect HPV-
Proofer assay (NorChip AS, Klokkarstua Norway) is a
commercially available assay (in Europe only) to detect
E6/E7 mRNA by real-time multiplex nucleic acid
sequence-based amplification and detection of molec-
ular beacon probes.97 An internal control (human U1
small nuclear ribonucleoprotein-specific A protein
mRNA) is used to guard against false-negative results
due to degradation of RNA.98 A positive HPV-Proofer
result should indicate integration of E6/E7 and identify
women at high risk for a persistent infection. To deter-
mine whether HPV testing had prognostic value as an
adjunct to cytology, Molden et al99 carried out a 2-year
follow-up study of 77 women with an initial diagnosis
of ASCUS or LSIL cervical cytology who were enrolled
in the Norwegian Cervical Cancer Screening Program.
Their results indicated that women who tested positive
HPV Testing and Molecular Markers/Dehn et al. 7

with the PreTect HPV-Proofer assay were approxi-
mately 70 times more likely to be diagnosed with
CIN2þ than women who tested negative. Compared
with consensus PCR testing of HPV, women who tested
positive were only 6 times more likely to be diagnosed
with CIN2þ than women who tested negative. Their
findings indicated that the PreTect HPV-Proofer assay
had a sensitivity equal to PCR but higher specificity,
and its use could improve triage of women with an
ASCUS or LSIS cervical cytology interpretation.99
Gen-Probe (San Diego, Calif) has developed an
APTIMA HPV assay that is currently in clinical trials.
This assay is to be the same as their other APTIMA
assays for the detection of Chlamydia trachomatis
and Neisseria gonorrhoeae, which are highly sensitive
and specific for diagnosing infection.100 The APTIMA
assays use target capture to partially purify rRNA
from samples by binding target rRNA to coated mag-
netic beads, isothermal transcription-mediated ampli-
fication to amplify the rRNA, and a dual kinetic assay
to detect RNA amplified products by using chemilu-
minescent-labeled DNA probes that form RNA-DNA
hybrids.101 The APTIMA HPV assay targets E6/E7 and
may, therefore, be useful in identifying women at high
risk for a persistent infection.
SURROGATE MOLECULAR MARKERS OF HPVThe identification of markers that link high-risk HPV
infection with molecular changes that occur in the
neoplastic process could theoretically increase clinical
specificity for detection of cervical disease. Recent
work has focused upon the analysis of genes that are
overexpressed in cervical cancer on the basis of gene
expression microarray studies. One study authored by
Santin and his coworkers102 identified 240 genes by
gene expression microarray that showed greater than
2-fold up-regulation in cervical cancer compared with
normal cervical mucosa. Some genes that showed the
highest levels of differential overexpression in cervical
cancer included p16INK4a, minichromosome mainte-
nance proteins 2, 4, and 5, cyclin D1 prostaglandin E
synthase, topoisomerase 2 alpha (TOP2a), and the E2F
transcription factor 1. In addition, telomerase overex-
pression has been identified as a consistent marker of
cervical dysplasia and cancer in cervical biopsy speci-
mens, but it has not been validated as a sensitive or
specific marker of high-grade premalignant or malig-
nant lesions in cervical cytology specimens.103,104
p16INK4a, a tumor suppressor protein and cyclin-de-
pendent kinase (cdk) inhibitor, acts as a tumor sup-
pressor by blocking cdk4 and cdk6-mediated pRb
phosphorylation, resulting in inhibition of E2F de-
pendent transcription and inhibition of cell cycle pro-
gression at the G1 to S checkpoint.23 The repression of
p16INK4a gene expression by hypermethylation or
mutation is a common occurrence in a wide range of
cancer cell lines and primary human tumors. However,
in most cervical carcinomas, the functional inactiva-
tion of pRb by HPV E7 results in the reciprocal overex-
pression of p16INK4a, because of a negative feedback
loop24,105–108 between pRb and p16INK4a. Thus,
p16INK4a overexpression in cervical neoplasia is a sur-
rogate marker of HPV E7-mediated pRb catabolism,
reflecting disruption of mechanisms that control cell
proliferation and indicating persistent infection with
high risk of development of neoplasia.109,110
Immunohistochemical studies indicate that p16INK4a
is highly expressed in virtually 100% of cases of CIN2,
CIN3, and SCC but is rarely detected in benign squa-
mous mucosa.110,111 Furthermore, immunostaining for
p16INK4a has been found to reduce interobserver dis-
agreement compared with the diagnosis of conven-
tional hematoxylin and eosin (H&E)-stained tissue
sections. In a series of 53 high-grade dysplastic lesions,
the accuracy of p16INK4a staining was reported to be
100%.112 In this same study, the researchers also sug-
gested that p16INK4a expression may help identify low-
grade cervical lesions that are associated with high-
risk HPV types, and, thus, are at an increased risk for
progression to high-grade dysplasia or carcinoma.
Recent investigations have found that p16INK4a is also
consistently overexpressed in virtually 100% of cases of
AIS and endocervical adenocarcinoma.112–114 Although
focal positivity has been found in cases of tuboendo-
metrial hyperplasia, both microglandular hyperplasia
and normal endocervical glands have been reported to
be consistently negative for p16INK4a expression.112–114
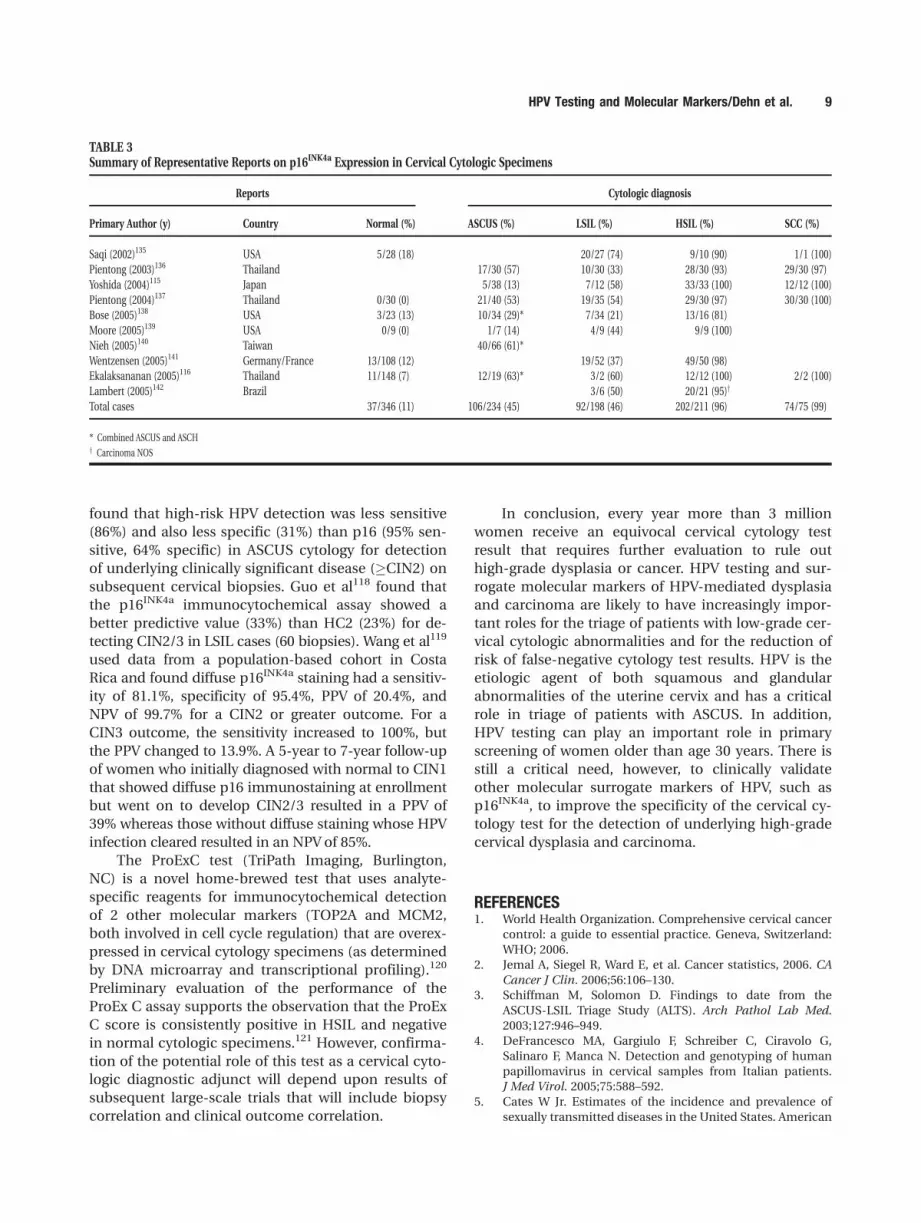
A wide range of studies have reported the immu-
nocytochemical detection of p16INK4a in cervical cyto-
logic specimens to be a marker of cervical dysplasia
and carcinoma (Table 3). In general, the proportion of
p16-positive cases has been closely associated with
the severity of cytologic diagnoses, with a relatively
low proportion of positive cases in normal cytology
specimens (0% to 18%) and a consistently high pro-
portion of p16 INK4a-positive test results in HSIL (81%
to 100%) and in SCC (97% to 100%). p16 is detected in
a subset of cases that test positive for high-risk HPVs
and appears to be closely associated with the pre-
sence of biopsy-confirmed, high-grade dysplasia and
carcinoma. Several previous studies have confirmed
that there is a very close association between p16
overexpression and high-risk HPV detection. Few,
however, have evaluated the relative test performance
of HPV versus p16 testing in cervical cytologic speci-
mens compared with the histologic diagnoses of con-
current or follow-up cervical biopsies.115,116 Nieh117
(66 biopsies, including 21 with high-grade dysplasia)
8 CANCER (CANCER CYTOPATHOLOGY) February 25, 2007 / Volume 111 / Number 1
found that high-risk HPV detection was less sensitive
(86%) and also less specific (31%) than p16 (95% sen-
sitive, 64% specific) in ASCUS cytology for detection
of underlying clinically significant disease (�CIN2) on
subsequent cervical biopsies. Guo et al118 found that
the p16INK4a immunocytochemical assay showed a
better predictive value (33%) than HC2 (23%) for de-
tecting CIN2/3 in LSIL cases (60 biopsies). Wang et al119
used data from a population-based cohort in Costa
Rica and found diffuse p16INK4a staining had a sensitiv-
ity of 81.1%, specificity of 95.4%, PPV of 20.4%, and
NPV of 99.7% for a CIN2 or greater outcome. For a
CIN3 outcome, the sensitivity increased to 100%, but
the PPV changed to 13.9%. A 5-year to 7-year follow-up
of women who initially diagnosed with normal to CIN1
that showed diffuse p16 immunostaining at enrollment
but went on to develop CIN2/3 resulted in a PPV of
39% whereas those without diffuse staining whose HPV
infection cleared resulted in an NPV of 85%.
The ProExC test (TriPath Imaging, Burlington,
NC) is a novel home-brewed test that uses analyte-
specific reagents for immunocytochemical detection
of 2 other molecular markers (TOP2A and MCM2,
both involved in cell cycle regulation) that are overex-
pressed in cervical cytology specimens (as determined
by DNA microarray and transcriptional profiling).120
Preliminary evaluation of the performance of the
ProEx C assay supports the observation that the ProEx
C score is consistently positive in HSIL and negative
in normal cytologic specimens.121 However, confirma-
tion of the potential role of this test as a cervical cyto-
logic diagnostic adjunct will depend upon results of
subsequent large-scale trials that will include biopsy
correlation and clinical outcome correlation.
In conclusion, every year more than 3 million
women receive an equivocal cervical cytology test
result that requires further evaluation to rule out
high-grade dysplasia or cancer. HPV testing and sur-
rogate molecular markers of HPV-mediated dysplasia
and carcinoma are likely to have increasingly impor-
tant roles for the triage of patients with low-grade cer-
vical cytologic abnormalities and for the reduction of
risk of false-negative cytology test results. HPV is the
etiologic agent of both squamous and glandular
abnormalities of the uterine cervix and has a critical
role in triage of patients with ASCUS. In addition,
HPV testing can play an important role in primary
screening of women older than age 30 years. There is
still a critical need, however, to clinically validate
other molecular surrogate markers of HPV, such as
p16INK4a, to improve the specificity of the cervical cy-
tology test for the detection of underlying high-grade
cervical dysplasia and carcinoma.
REFERENCES1. World Health Organization. Comprehensive cervical cancer
control: a guide to essential practice. Geneva, Switzerland:
WHO; 2006.
2. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA
Cancer J Clin. 2006;56:106–130.
3. Schiffman M, Solomon D. Findings to date from the
ASCUS-LSIL Triage Study (ALTS). Arch Pathol Lab Med.
2003;127:946–949.
4. DeFrancesco MA, Gargiulo F, Schreiber C, Ciravolo G,
Salinaro F, Manca N. Detection and genotyping of human
papillomavirus in cervical samples from Italian patients.
J Med Virol. 2005;75:588–592.
5. Cates W Jr. Estimates of the incidence and prevalence of
sexually transmitted diseases in the United States. American
TABLE 3Summary of Representative Reports on p16INK4a Expression in Cervical Cytologic Specimens
Reports Cytologic diagnosis
Primary Author (y) Country Normal (%) ASCUS (%) LSIL (%) HSIL (%) SCC (%)
Saqi (2002)135 USA 5/28 (18) 20/27 (74) 9/10 (90) 1/1 (100)
Pientong (2003)136 Thailand 17/30 (57) 10/30 (33) 28/30 (93) 29/30 (97)
Yoshida (2004)115 Japan 5/38 (13) 7/12 (58) 33/33 (100) 12/12 (100)
Pientong (2004)137 Thailand 0/30 (0) 21/40 (53) 19/35 (54) 29/30 (97) 30/30 (100)
Bose (2005)138 USA 3/23 (13) 10/34 (29)* 7/34 (21) 13/16 (81)
Moore (2005)139 USA 0/9 (0) 1/7 (14) 4/9 (44) 9/9 (100)
Nieh (2005)140 Taiwan 40/66 (61)*
Wentzensen (2005)141 Germany/France 13/108 (12) 19/52 (37) 49/50 (98)
Ekalaksananan (2005)116 Thailand 11/148 (7) 12/19 (63)* 3/2 (60) 12/12 (100) 2/2 (100)
Lambert (2005)142 Brazil 3/6 (50) 20/21 (95)y
Total cases 37/346 (11) 106/234 (45) 92/198 (46) 202/211 (96) 74/75 (99)
* Combined ASCUS and ASCHy Carcinoma NOS
HPV Testing and Molecular Markers/Dehn et al. 9
Social Health Association Panel. Sex Transm Dis. 1999;26:
S2–S7.
6. Burk RD, Ho GY, Beardsley L, Lempa M, Peters M, Bierman R.
Sexual behavior and partner characteristics are the predo-
minant risk factors for genital human papillomavirus infec-
tion in young women. J Infect Dis. 1996;174:679–689.
7. Bauer HM, Ting Y, Greer CE, et al. Genital human papillo-
mavirus infection in female university students as deter-
mined by a PCR-based method. JAMA. 1991;265:472–477.
8. Meijer CJ, Helmerhorst TJ, Rozendaal L, van der Linden JC,
Voorhorst FJ, Walboomers JM. HPV typing and testing in
gynaecological pathology: has the time come? Histopathol-
ogy. 1998;33:83–86.
9. Plummer M, Herrero R, Franceschi S, et al. Smoking and
cervical cancer: pooled analysis of the IARC multi-centric
case–control study. Cancer Causes Control. 2003;14:805–814.
10. McIntyre-Seltman K, Castle PE, Guido R, Schiffman M,
Wheeler CM, and the ALTS Group. Smoking is a risk factor
for cervical intraepithelial neoplasia grade 3 among onco-
genic human papillomavirus DNA-positive women with
equivocal or mildly abnormal cytology. Cancer Epidemiol
Biomarkers Prev. 2005;14:1165–1170.
11. Moreno V, Bosch FX, Munoz N, et al, and the International
Agency for Research on Cancer. Multicentric Cervical Can-
cer Study Group. Effect of oral contraceptives on risk of
cervical cancer in women with human papillomavirus
infection: the IARC multicentric case-control study. Lancet.
2002;359:1085–1092.
12. Munoz N, Franceschi S, Bosetti C, et al, and the Interna-
tional Agency for Research on Cancer. Multicentric Cervical
Cancer Study Group. Role of parity and human papilloma-
virus in cervical cancer: the IARC multicentric case-control
study. Lancet. 2002;359:1093–1101.
13. Castellsague X, Diaz M, de Sanjose S, et al, and the Interna-
tional Agency for Research on Cancer Multicenter Cervical
Cancer Study Group. Worldwide human papillomavirus eti-
ology of cervical adenocarcinoma and its cofactors: implica-
tions for screening and prevention. J Natl Cancer Inst. 2006;
98:303–315.
14. Hildesheim A, Mann V, Brinton LA, Szklo M, Reeves WC,
Rawls WE. Herpes simplex virus type 2: a possible interac-
tion with human papillomavirus types 16/18 in the devel-
opment of invasive cervical cancer. Int J Cancer. 1991;49:
335–340.
15. Wolf JK, Ramirez PT. The molecular biology of cervical cancer.
Cancer Invest. 2001;19:621–629.
16. zur Hausen H. Papillomaviruses in human cancers. Proc
Assoc Am Physicians. 1999;111:581–587.
17. Stoler M. Human papillomavirus biology and cervical neo-
plasia, implications for diagnostic criteria and testing. Arch
Pathol Lab Med. 2003;127:935–939.
18. Doorbar J. The papillomavirus life cycle. J Clin Virol. 2005;
32(suppl 1):S7–15
19. Andersson S, Hansson B, Norman I, et al. Expression of E6/
E7 mRNA from ‘high risk’ human papillomavirus in relation
to CIN grade, viral load and p16INK4a. Int J Oncol. 2006;
29:705–711.
20. Scheurer ME, Tortolero-Luna G, Adler-Storthz K. Human
papillomavirus infection: biology, epidemiology, and pre-
vention. Int J Gynecol Cancer. 2005;15:727–746.
21. zur Hausen H. Papillomavirus infections—a major cause of
human cancers. Biochim Biophys Acta. 1996;1288:F55–F78.
22. Martin CM, Astbury K, O’Leary JJ. Molecular profiling of
cervical neoplasia. Expert Rev Mol Diagn. 2006;6:217–229.
23. Zhang HS, Postigo AA, Dean DC. Active transcriptional
repression by the Rb-E2F complex mediates G1 arrest trig-
gered by p16INK4a, TGFbeta, and contact inhibition. Cell.
1999;97:53–61.
24. Dyson N, Howley PM, Munger K, Harlow E. The human
papilloma virus-16 E7 oncoprotein is able to bind to the
retinoblastoma gene product. Science. 1989;243:934–937.
25. Kobelin MH, Kobelin CG, Burke L, Lavin P, Niloff JM, Kim
YB. Incidence and predictors of cervical dysplasia in
patients with minimally abnormal Papanicolaou smears.
Obstet Gynecol. 1998;92:356–359.
26. Crum CP, Genest DR, Krane JF, et al. Subclassifying atypical
squamous cells in ThinPrep cervical cytology correlates
with detection of high-risk human papillomavirus DNA.
Am J Clin Pathol. 1999;112:384–390.
27. Schoolland M, Sterrett GF, Knowles SA, Mitchell KM, Kur-
inczuk JJ. The ‘‘Inconclusive—possible high grade epithelial
abnormality’’ category in Papanicolaou smear reporting.Cancer. 1998;84:208–217.
28. Malik SN, Wilkinson EJ, Drew PA, Bennett BB, Hardt NS.
Do qualifiers of ASCUS distinguish between low- and high-
risk patients? Acta Cytol. 1999;43:376–380.
29. Chhieng DC, Elgert P, Cangiarella JF, Cohen JM. Variation
in the incidence of AGUS between different patient popula-
tions. Acta Cytol. 2001;45:287–293.
30. Wright TC Jr, Cox JT, Massad LS, Twiggs LB, Wilkinson EJ,
and the ASCCP-Sponsored Consensus Conference. 2001 Con-
sensus Guidelines for the management of women with cervi-
cal cytological abnormalities. JAMA. 2002;287:2120–2129.
31. ASCUS-LSIL Triage Study (ALTS) Group. A randomized trial
on the management of low-grade squamous intraepithelial
lesion cytology interpretations [published comment appears
in Am J Obstet Gynecol. 2003;188:1381–1382]. Am J Obstet
Gynecol. 2003;188:1393–1400.
32. Levine L, Lucci JA III, Dinh TV. Atypical glandular cells:
new Bethesda Terminology and Management Guidelines.
Obstet Gynecol Surv. 2003;58:399–406.
33. Gage JC, Hanson VW, Abbey K, et al, and the ASCUS LSIL
Triage Study (ALTS) Group. Number of cervical biopsies
and sensitivity of colposcopy [published comment appears
in Obstet Gynecol. 2006;108:246–247]. Obstet Gynecol. 2006;
108:264–272.
34. Titus K. Making a valid point about HPV tests. CAP Today.
2005;19.
35. Naryshkin S. The false-negative fraction for Papanicolaou
smears: how often are ‘‘abnormal’’ smears not detected by
a ‘‘standard’’ screening cytologist? Arch Pathol Lab Med.
1997;121:270–272.
36. Krieger P, Naryshkin S. Random rescreening of cytologic
smears: a practical and effective component of quality
assurance programs in both large and small cytology labo-
ratories. Acta Cytol. 1994;38:291–298.
37. Tabbara SO, Sidawy MK. Evaluation of the 5-year review of
negative cervical smears in patients with high grade squa-
mous intraepithelial lesions. Diagn Cytopathol. 1996;15:7–10.
38. Guo M, Hu L, Martin L, Liu S, Baliga M, Hughson MD. Ac-
curacy of liquid-based Pap tests: comparison of concurrent
liquid-based tests and cervical biopsies on 782 women with
previously abnormal Pap smears. Acta Cytol. 2005;49:132–
138.
39. DeMay RM. The Pap Smear. In: The art and science of cyto-
pathology. Exfoliative cytology. Chicago: ASCP Press; 1996;
61–205.
40. DeMay RM. Cytopathology of false negatives preceding cer-
vical carcinoma. Am J Obstet Gynecol. 1996;175:1110–1113.
10 CANCER (CANCER CYTOPATHOLOGY) February 25, 2007 / Volume 111 / Number 1

41. Benoit AG, Krepart GV, Lotocki RJ. Results of prior cytologic
screening in patients with a diagnosis of Stage I carcinoma
of the cervix. Am J Obstet Gynecol. 1984;148:690–694.
42. Berkeley AS, LiVolsi VA, Schwartz PE. Advanced squamous
cell carcinoma of the cervix with recent normal Papanico-
laou tests. Lancet. 1980;2:375–376.
43. Gay JD, Donaldson LD, Goellner JR. False-negative results
in cervical cytologic studies. Acta Cytol. 1985;29:1043–1046.
44. Pairwuti S. False-negative Papanicolaou smears from women
with cancerous and precancerous lesions of the uterine cer-
vix. Acta Cytol. 1991;35:40–46.
45. Robertson JH, Woodend B. Negative cytology preceding
cervical cancer: causes and prevention. J Clin Pathol. 1993;
46:700–702.
46. van der Graaf Y, Vooijs GP, Gaillard HL, Go DM. Screening
errors in cervical cytologic screening. Acta Cytol. 1987;31:
434–438.
47. van der Graaf Y, Vooijs GP. False-negative rate in cervical
cytology. J Clin Pathol. 1987;40:438–442.
48. Lee KR, Minter LJ, Granter SR. Papanicolaou smear sensi-
tivity for adenocarcinoma in situ of the cervix. A study of
34 cases. Am J Clin Pathol. 1997;107:30–35.
49. Krane JF, Granter SR, Trask CE, Hogan CL, Lee KR. Papanico-
laou smear sensitivity for the detection of adenocarcinoma
of the cervix: a study of 49 cases. Cancer. 2001;93:8–15.
50. Stoler MH. Testing for human papillomavirus: data driven
implications for cervical neoplasia management. Clin Lab
Med. 2003:23:569–583.
51. Cox JT. Human papillomavirus testing in primary cervical
screening and abnormal Papanicolaou management. Obstet
Gynecol Surv. 2006;61:S15–S25.
52. Carozzi FM, Del Mistro A, Confortini M, et al. Reproduci-
bility of HPV DNA testing by Hybrid Capture 2 in a screen-
ing setting. Am J Clin Pathol. 2005;124:716–721.
53. Tarkowski TA, Rajeevan MS, Lee DR, Unger ER. Improved
detection of viral RNA isolated from liquid-based cytology
samples. Mol Diagn. 2001;6:125–130.
54. Castle PE, Solomon D, Hildesheim A, et al. Stability of ar-
chived liquid-based cervical cytologic specimens. Cancer.
2003;99:89–96.
55. Hopman AH, Kamps MA, Smedts F, Speel EJ, Herrington CS,
Ramaekers FC. HPV in situ hybridization: impact of differ-
ent protocols on the detection of integrated HPV. Int J Can-
cer. 2005;115:419–428.
56. Hacker GW, Su H, Hauser-Kronberger C, Hainfeld JF, Tubbs R.
Sensitive in situ hybridization with catalyzed reporter depo-
sition, streptavidin-Nanogold, and silver acetate autometal-
lography: detection of single-copy human papillomavirus
[published comment appears in Am J Pathol. 1997;151:
1172–1173]. Am J Pathol. 1997;150:1553–1561.
57. Davies P, Kornegay J, Iftner T. Current methods of testing for
human papillomavirus. Best Pract Res Clin Obstet Gynaecol.
2001;15:677–700.
58. Peyton CL, Schiffman M, Lorincz AT, et al. Comparison of
PCR- and hybrid capture-based human papillomavirus de-
tection systems using multiple cervical specimen collection
strategies [published correction appears in J Clin Microbiol.
1999;37:478]. J Clin Microbiol. 1998;36:3248–3254.
59. Schiffman M, Wheeler CM, Dasgupta A, Solomon D, Castle PE,
and The ALTS Group. A comparison of a prototype PCR
assay and Hybrid Capture 2 for detection of carcinogenic
human papillomavirus DNA in women with equivocal or
mildly abnormal Papanicolaou smears. Am J Clin Pathol.
2005;124:722–732.
60. Ronco G, Segnan N, Giorgi-Rossi P, et al, and the New Technol-
ogies for Cervical Cancer Working Group. Human papilloma-
virus testing and liquid-based cytology: results at recruitment
from the new technologies for cervical cancer randomized
controlled trial. J Natl Cancer Inst. 2006;98:765–774.
61. Malloy C, Sherris J, Herdman C. HPV DNA testing: techni-
cal and programmatic issues for cervical cancer prevention
in low-resource settings. Seattle: PATH; 2000.
62. van Doorn LJ, Kleter B, Quint WG. Molecular detection and
genotyping of human papillomavirus. Expert Rev Mol
Diagn. 2001;1:394–402.
63. Gravitt PE, Peyton CL, Alessi TQ, et al. Improved amplifica-
tion of genital human papillomaviruses. J Clin Microbiol.
2000;38:357–361.
64. van Doorn LJ, Quint W, Kleter B, et al. Genotyping of
human papillomavirus in liquid cytology cervical speci-
mens by the PGMY line blot assay and the SPF(10) line
probe assay. J Clin Microbiol. 2002;40:979–983.
65. Morris BJ. Cervical human papillomavirus screening by
PCR: advantages of targeting the E6/E7 region. Clin Chem
Lab Med. 2005;43:1171–1177.
66. Brink AA, Snijders PJ, Meijer CJ, Berkhof J, Verheijen RH.
HPV testing in cervical screening. Best Pract Res Clin Obstet
Gynaecol. 2006;20:253–266.
67. Fujii T, Masumoto N, Saito M, et al. Comparison between
in situ hybridization and real-time PCR technique as a
means of detecting the integrated form of human papillo-
mavirus 16 in cervical neoplasia. Diagn Mol Pathol. 2005;
14:103–108.
68. Gheit T, Landi S, Gemignani F, et al. Development of a sensi-
tive and specific assay combining multiplex PCR and DNA
microarray primer extension to detect high-risk mucosal
human papillomavirus types. J Clin Microbiol. 2006;44:2025–
2031.
69. Kleter B, van Doorn LJ, ter Schegget J, et al. Novel short-
fragment PCR assay for highly sensitive broad-spectrum
detection of anogenital human papillomaviruses [pub-
lished comment appears in Am J Pathol. 1998;153:1667–
1671]. Am J Pathol. 1998;153:1731–1739.
70. Gravitt PE, Peyton CL, Apple RJ, Wheeler CM. Genotyping
of 27 human papillomavirus types by using L1 consensus
PCR products by a single-hybridization, reverse line blot
detection method. J Clin Microbiol. 1998;36:3020–3027.
71. Coutlee F, Gravitt P, Kornegay J, et al. Use of PGMY primers
in L1 consensus PCR improves detection of human papillo-
mavirus DNA in genital samples. J Clin Microbiol. 2002;40:
902–907.
72. Melchers WJ, Bakkers JM, Wang J, et al. Short fragment po-
lymerase chain reaction reverse hybridization line probe
assay to detect and genotype a broad spectrum of human
papillomavirus types. Clinical evaluation and follow-up.
Am J Pathol. 1999;155:1473–1478.
73. Kleter B, van Doorn LJ, Schrauwen L, et al. Development
and clinical evaluation of a highly sensitive PCR-reverse
hybridization line probe assay for detection and identifica-
tion of anogenital human papillomavirus. J Clin Microbiol.
1999;37:2508–2517.
74. Gillio-Tos A, De Marco L, Ghisetti V, et al. Human papillo-
mavirus typing with GP5þ/6þ polymerase chain reaction
reverse line blotting and with commercial type-specific
PCR kits. J Clin Virol. 2006;36:126–132.
75. Monsonego J, Bohbot JM, Pollini G, et al. Performance of the
Roche AMPLICOR human papillomavirus (HPV) test in pre-
diction of cervical intraepithelial neoplasia (CIN) in women
with abnormal PAP smear. Gynecol Oncol. 2005;99:160–168.
HPV Testing and Molecular Markers/Dehn et al. 11
76. Sandri MT, Lentati P, Benini E, et al. Comparison of the
Digene HC2 Assay and the Roche AMPLICOR human papil-
lomavirus (HPV) test for detection of high-risk HPV geno-
types in cervical samples. J Clin Microbiol. 2006;44:2141–
2146.
77. van HamMA, Bakkers JM, Harbers GK, Quint WG, Massuger
LF, Melchers WJ. Comparison of two commercial assays for
detection of human papillomavirus (HPV) in cervical scrape
specimens: validation of the Roche AMPLICOR HPV test as
a means to screen for HPV genotypes associated with a
higher risk of cervical disorders. J Clin Microbiol. 2005;43:
2662–2667.
78. Klaassen CH, Prinsen CF, de Valk HA, Horrevorts AM,
Jeunink MA, Thunnissen FB. DNA microarray format for
detection and subtyping of human papillomavirus. J Clin
Microbiol. 2004;42:2152–2160.
79. Oh TJ, Kim CJ, Woo SK, et al. Development and clinical eva-
luation of a highly sensitive DNA microarray for detection
and genotyping of human papillomaviruses. J Clin Micro-
biol. 2004;42:3272–3280.
80. Kim CJ, Jeong JK, Park M, et al. HPV oligonucleotide micro-
array-based detection of HPV genotypes in cervical neo-
plastic lesions. Gynecol Oncol. 2003;89:210–217.
81. Choi YD, Jung WW, Nam JH, Choi HS, Park CS. Detection
of HPV genotypes in cervical lesions by the HPV DNA Chip
and sequencing. Gynecol Oncol. 2005;98:369–375.
82. Kim KH, Yoon MS, Na YJ, Park CS, Oh MR, Moon WC. De-
velopment and evaluation of a highly sensitive human pap-
illomavirus genotyping DNA chip. Gynecol Oncol. 2006;100:
38–43.
83. Chen S, Tabrizi SN, Fairley CK, Borg AJ, Garland SM. Simul-
taneous detection and typing strategy for human papillo-
maviruses based on PCR and restriction endonuclease
mapping. Biotechniques. 1994;17:138–40,142–143.
84. Lungu O, Wright TC Jr, Silverstein S. Typing of human
papillomaviruses by polymerase chain reaction amplifica-
tion with L1 consensus primers and RFLP analysis. Mol
Cell Probes. 1992;6:145–152.
85. Arens M. Clinically relevant sequence-based genotyping of
HBV, HCV, CMV, and HIV. J Clin Virol. 2001;22:11–29.
86. Dunbar SA, Vander Zee CA, Oliver KG, Karem KL, Jacobson
JW. Quantitative, multiplexed detection of bacterial patho-
gens: DNA and protein applications of the Luminex Lab-
MAP system. J Microbiol Methods. 2003;53:245–252.
87. Jiang HL, Zhu HH, Zhou LF, Chen F, Chen Z. Genotyping of
human papillomavirus in cervical lesions by L1 consensus
PCR and the Luminex xMAP system. J Med Microbiol.
2006;55(pt 6):715–720.
88. Schmitt M, Bravo IG, Snijders PJ, Gissmann L, Pawlita M,
Waterboer T. Bead-based multiplex genotyping of human
papillomaviruses. J Clin Microbiol. 2006;44:504–512.
89. Germer JJ, Majewski DW, Yung B, Mitchell PS, Yao JD. Eva-
luation of the invader assay for genotyping hepatitis C vi-
rus. J Clin Microbiol. 2006;44:318–323.
90. Thyagarajan B, Anderson KE, Kong F, Selk FR, Lynch CF,
Gross MD. New approaches for genotyping paraffin wax
embedded breast tissue from patients with cancer: the
Iowa women’s health study. J Clin Pathol. 2005;58:955–961.
91. Hjertner B, Meehan B, McKillen J, McNeilly F, Belak S. Ad-
aptation of an Invader assay for the detection of African
swine fever virus DNA. J Virol Methods. 2005;124:1–10.
92. Snijders PJ, van den Brule AJ, Meijer CJ. The clinical rele-
vance of human papillomavirus testing: relationship be-
tween analytical and clinical sensitivity. J Pathol. 2003;201:
1–6.
93. Gravitt PE, Peyton C, Wheeler C, Apple R, Higuchi R, Shah
KV. Reproducibility of HPV 16 and HPV 18 viral load quan-
titation using TaqMan real-time PCR assays. J Virol Meth-
ods. 2003;112:23–33.
94. Carcopino X, Henry M, Benmoura D, et al. Determination
of HPV type 16 and 18 viral load in cervical smears of
women referred to colposcopy. J Med Virol. 2006;78:1131–
1140.
95. Gravitt PE, Burk RD, Lorincz A, et al. A comparison
between real-time polymerase chain reaction and Hy-
brid Capture 2 for human papillomavirus DNA quantita-
tion. Cancer Epidemiol Biomarkers Prev. 2003;12:477–
484.
96. Hudson JB, Bedell MA, McCance DJ, Laiminis LA.
Immortalization and altered differentiation of human ke-
ratinocytes in vitro by the E6 and E7 open reading frames
of human papillomavirus type 18. J Virol. 1990;64:519–
526.
97. Molden T, Kraus I, Karlsen F, Skomedal H, Hagmar B.
Human papillomavirus E6/E7 mRNA expression in women
younger than 30 years of age. Gynecol Oncol. 2006;100:95–
100.
98. Lie AK, Risberg B, Borge B, et al. DNA- versus RNA-based
methods for human papillomavirus detection in cervical
neoplasia. Gynecol Oncol. 2005;97:908–915.
99. Molden T, Nygard JF, Kraus I, et al. Predicting CIN2þ when
detecting HPV mRNA and DNA by PreTect HPV-proofer
and consensus PCR: a 2-year follow-up of women with
ASCUS or LSIL Pap smear. Int J Cancer. 2005;114:973–
976.
100. Schachter J, Chernesky MA, Willis DE, et al. Vaginal swabs
are the specimens of choice when screening for Chlamydia
trachomatis and Neisseria gonorrhoeae: results from a
multicenter evaluation of the APTIMA assays for both in-
fections. Sex Transm Dis. 2005;32:725–728.
101. Chernesky MA, Jang DE. APTIMA transcription-mediated
amplification assays for Chlamydia trachomatis and
Neisseria gonorrhoeae. Expert Rev Mol Diagn. 2006;6:
519–525.
102. Santin AD, Zhan F, Bignotti E, et al. Gene expression pro-
files of primary HPV16- and HPV18-infected early stage
cervical cancers and normal cervical epithelium: identi-
fication of novel candidate molecular markers for cervi-
cal cancer diagnosis and therapy. Virology. 2005;331:269–
291.
103. Jarboe EA, Liaw KL, Thompson LC, et al. Analysis of telo-
merase as a diagnostic biomarker of cervical dysplasia and
carcinoma. Oncogene. 2002;21:664–673.
104. Jarboe EA, Thompson LC, Heinz D, McGregor JA, Shroyer
KR. Telomerase and human papillomavirus as diagnostic
adjuncts for cervical dysplasia and carcinoma. Hum Pathol.
2004;35:396–402.
105. Sherr CJ. Cancer cell cycles. Science. 1996;274:1672–
1677.
106. Kamb A, Gruis NA, Weaver-Feldhaus J, et al. A cell cycle
regulator potentially involved in genesis of many tumor
types. Science. 1994;264:436–440.
107. Khleif SN, DeGregori J, Yee CL, et al. Inhibition of cyclin D-
CDK4/CDK6 activity is associated with an E2F-mediated
induction of cyclin kinase inhibitor activity. Proc Natl Acad
Sci U S A. 1996;93:4350–4354.
108. Jones DL, Munger K. Interactions of the human papilloma-
virus E7 protein with cell cycle regulators. Semin Cancer
Biol. 1996;7:327–337.
12 CANCER (CANCER CYTOPATHOLOGY) February 25, 2007 / Volume 111 / Number 1
109. Keating JT, Cviko A, Riethdorf S, et al. Ki-67, cyclin E, and
p16INK4 are complementary surrogate biomarkers for human
papilloma virus-related cervical neoplasia. Am J Surg Pathol.
2001;25:884–891.
110. Klaes R, Friedrich T, Spitkovsky D, et al. Overexpression of
p16(INK4A) as a specific marker for dysplastic and neo-
plastic epithelial cells of the cervix uteri. Int J Cancer.
2001;92:276–284.
111. Klaes R, Benner A, Friedrich T, et al. p16INK4a immu-
nohistochemistry improves interobserver agreement in
the diagnosis of cervical intraepithelial neoplasia [pub-
lished comment appears in Am J Surg Pathol. 2003;27:
1284; author reply 1284]. Am J Surg Pathol. 2002;26:
1389–1399.
112. Murphy N, Ring M, Killalea AG, et al. p16INK4A as a
marker for cervical dyskaryosis: CIN and cGIN in cervical
biopsies and ThinPrep smears. J Clin Pathol. 2003;56:56–
63.
113. Cameron RI, Maxwell P, Jenkins D, McCluggage WG. Im-
munohistochemical staining with MIB1, bcl2 and p16
assists in the distinction of cervical glandular intraepithe-
lial neoplasia from tubo-endometrial metaplasia, endome-
triosis and microglandular hyperplasia. Histopathology.
2002;41:313–321.
114. Negri G, Egarter-Vigl E, Kasal A, Romano F, Haitel A, Mian C.
p16INK4a is a useful marker for the diagnosis of adenocarci-
noma of the cervix uteri and its precursors: an immunohis-
tochemical study with immunocytochemical correlations.
Am J Surg Pathol. 2003;27:187–193.
115. Yoshida T, Fukuda T, Sano T, Kanuma T, Owada N,
Nakajima T. Usefulness of liquid-based cytology specimens
for the immunocytochemical study of p16 expression and
human papillomavirus testing: a comparative study using
simultaneously sampled histology materials. Cancer. 2004;
102:100–108.
116. Ekalaksananan T, Pientong C, Sriamporn S, et al. Useful-
ness of combining testing for p16 protein and human pap-
illomavirus (HPV) in cervical carcinoma screening. Gynecol
Oncol. 2006;103:62–66.
117. Nieh S, Chen SF, Chu TY, et al. Is p16(INK4A) expression
more useful than human papillomavirus test to determine
the outcome of atypical squamous cells of undetermined
significance-categorized Pap smear? A comparative analy-
sis using abnormal cervical smears with follow-up biopsies.
Gynecol Oncol. 2005;97:35–40.
118. Guo M, Hu L, Baliga M, He Z, Hughson MD. The predictive
value of p16INK4a and Hybrid Capture 2 human papillo-
mavirus testing for high-grade cervical intraepithelial neo-
plasia. Am J Clin Pathol 2004;122:894–901.
119. Wang SS, Trunk M, Schiffman M et al. Validation of
p16INK4a as a marker of oncogenic human papillomavirus
infection in cervical biopsies from a population-based co-
hort in Costa Rica. Cancer Epidemiol Biomarkers Prev 2004;
13:1355–1360.
120. Malinowski DP. Molecular diagnostic assays for cervical ne-
oplasia: emerging markers for the detection of high-grade
cervical disease. Biotechniques. 2005;(suppl):17–23.
121. Shroyer KR, Homer P, Heinz D, Singh M. Validation of a
novel immunocytochemical assay for topoisomerase II-
alpha and minichromosome maintenance protein 2 expres-
sion in cervical cytology. Cancer Cytopathol. 2006;108:324–
330.
122. Kjaer SK, Chackerian B, van den Brule AJ, et al. High-risk
human papillomavirus is sexually transmitted: evidence
from a follow-up study of virgins starting sexual activity
(intercourse). Cancer Epidemiol Biomarkers Prev. 2001;10:
101–106.
123. Winer RL, Lee SK, Hughes JP, Adam DE, Kiviat NB, Koutsky
LA. Genital human papillomavirus infection: incidence and
risk factors in a cohort of female university students [pub-
lished correction appears in Am J Epidemiol. 2003;157:858].
Am J Epidemiol. 2003;157:218–226.
124. Fairley CK, Gay NJ, Forbes A, Abramson M, Garland SM.
Hand-genital transmission of genital warts? An analysis of
prevalence data. Epidemiol Infect. 1995;115:169–176.
125. Herrero R, Castellsague X, Pawlita M, et al. Human papillo-
mavirus and oral cancer: the International Agency for
Research on Cancer multicenter study. J Natl Cancer Inst.
2003;95:1772–1783.
126. Bosch FX, Lorincz A, Munoz N, Meijer CJ, Shah KV. The
causal relation between human papillomavirus and cervi-
cal cancer [published comment appears in J Clin Pathol.
2002;55:241–242]. J Clin Pathol. 2002;55:244–265.
127. Durst M, Gissmann L, Ikenberg H, zur Hausen H. A pap-
illomavirus DNA from a cervical carcinoma and its preva-
lence in cancer biopsy samples from different geographic
regions. Proc Natl Acad Sci U S A. 1983;80:3812–3815.
128. Boshart M, Gissmann L, Ikenberg H, Kleinheinz A,
Scheurlen W, zur Hausen H. A new type of papillomavirus
DNA, its presence in genital cancer biopsies and in cell
lines derived from cervical cancer. EMBO J. 1984;3:1151–
1157.
129. Magnusson PK, Lichtenstein P, Gyllensten UB. Heritability
of cervical tumours. Int J Cancer. 2000;88:698–701.
130. Ginocchio CC. Assays for the detection of human papillo-
mavirus. Pan American Society for Clinical Virology News-
letter. March 2004;31(1):1–3. Published online at: http://
www.virology.org/newsletters/2004march.pdf
131. Qureshi MN, Rudelli RD, Tubbs RR, Biscotti CV, Layfield LJ.
Role of HPV DNA testing in predicting cervical intraepithe-
lial lesions: comparison of HC HPV and ISH HPV. Diagn
Cytopathol 2003;29:149–155.
132. Jin XW, Brainard J, Nielsen C, Yen-Lieberman B. New ad-
vances transform the management of women with abnor-
mal pap tests. Pan American Society for Clinical Virology
Newsletter. March 2004;31(1):4–5. Published online at: http://
www.virology.org/newsletters/2004march.pdf
133. Molden T, Kraus I, Karlsen F, Skomedal H, Nygard JF,
Hagmar B. Comparison of human papillomavirus messen-
ger RNA and DNA detection: A cross-sectional study of
4,136 women >30 years of age with a 2-year follow-up of
high-grade squamous intraepithelial lesion. Cancer Epide-
miol Biomarkers Prev. 2005;14:367–372.
134. Schorge JO, Lea JS, Elias KJ, et al. P16 as a molecular bio-
marker of cervical adenocarcinoma. Am J Obstet Gynecol.
2004;190:668–673.
135. Saqi A, Pasha TL, McGrath CM, Yu GH, Zhang P, Gupta P.
Overexpression of p16INK4A in liquid-based specimens
(SurePath) as marker of cervical dysplasia and neoplasia.
Diagn Cytopathol. 2002;27:365–370.
136. Pientong C, Ekalaksananan T, Swadpanich U, et al. Immu-
nocytochemical detection of p16INK4a protein in scraped
cervical cells. Acta Cytol. 2003;47:616–623.
137. Pientong C, Ekalaksananan T, Kongyingyoes B, et al.
Immunocytochemical staining of p16INK4a protein from
conventional Pap test and its association with human
papillomavirus infection. Diagn Cytopathol. 2004;31:235–
242.
HPV Testing and Molecular Markers/Dehn et al. 13

138. Bose S, Evans H, Lantzy L, Scharre K, Youssef E. p16(INK4A)
is a surrogate biomarker for a subset of human papilloma
virus-associated dysplasias of the uterine cervix as deter-
mined on the Pap smear. Diagn Cytopathol. 2005;32:21–24.
139. Moore GD, Lear SC, Wills-Frank LA, Martin AW, Snyder JW,
Helm CW. Differential expression of cdk inhibitors p16, p21cip1,
p27kip1, and cyclin E in cervical cytological smears prepared by
the ThinPrepmethod. Diagn Cytopathol. 2005;32:82–87.
140. Nieh S, Chen SF, Chu TY, Lai HC, Fu E. Expression of p16
INK4A in Papanicolaou smears containing atypical squa-
mous cells of undetermined significance from the uterine
cervix. Gynecol Oncol. 2003;91:201–208.
141. Wentzensen N, Bergeron C, Cas F, Eschenbach D,
Vinokurova S, von Knebel Doeberitz M. Evaluation of a nu-
clear score for p16INK4a-stained cervical squamous cells
in liquid-based cytology samples. Cancer. 2005;105:461–
467.
142. Lambert AP, Anschau F, Schmitt VM. p16INK4A expression
in cervical premalignant and malignant lesions. Exp Mol
Pathol. 2006;80:192–196.
14 CANCER (CANCER CYTOPATHOLOGY) February 25, 2007 / Volume 111 / Number 1
Related Documents











