HUMAN FETAL CIRCULATION: CHANGES IN THE CARDIOVASCU- LAR SYSTEM AT BIRTH AND DISTURBANCES IN THE POST-NATAL CLOSURE OF THE FORAMEN OVALE AND DUCTUS ARTERIOSUS JOHN LIND AND CARL WEGELIUS Karolinska Institute, Stockholm, Sweden Our present knowledge of fetal circulation and the alterations that take place at birth are based upon anatomical studies and experimental investi- gations in animals, which until recently have not included study of the human fetus. Barclay, Frank- lin and Prichard's angiocardiographic investigation of the circulation in the fetal lamb before and after delivery is considered to be one of the most im- portant contributions to the study of fetal circula- tion (1944). THE COURSE OF THE BLOOD THROUGH THE FETAL HEART The course of the blood through the fetal heart has been the subject of a lively controversy. The principal question has been the degree of separation and mixing of the two caval streams coming into the fetal right atrium. The inferior vena cava con- tains blood from the placenta, the most highly oxygenated blood coming to the heart, in spite of the admixture with venous blood from the lower part of the body. The superior vena cava, on the other hand, brings the poorly oxygenated, unmixed venous blood from the heart and the upper portion of the body. There are two principal theories as to the course of the blood through the fetal heart. One holds that the two streams entering the right atrium are mixed. Therefore, the well oxygenated blood from the pla- centa, diluted once when the ductus venosus joins the inferior vena cava, enters the right atrium and is again diluted by blood from the superior vena cava and coronary sinus. The resulting mixture goes two ways; some enters the right ventricle but approximately half passes through the foramen ovale into the left side of the heart (Pohlman, 1907; Kellogg, 1930). Consequently the aorta and the pulmonary artery are considered to have the same oxygen content, and the upper part of the body, including the fetal heart itself, receives no better oxygen supply than the lower parts of the body and the placenta. If there should be a significant quan- tity of reduced blood entering the left atrium from the fetal lungs, the heart muscle and the brain would get less oxygen than the lower part of the body and the placenta. According to the other theory, the oxygenated blood which is brought from the placenta goes through the ductus venosus and inferior vena cava to the right atrium and is deflected by a fold of endocardium through the foramen ovale into the left atrium. Thus this stream retains its relative arterial character by crossing the flow of the venous blood from the superior vena cava which is de- livered to the right atrium and right ventricle. (Huggett, 1927; Barcroft et al., 1936 and 1938; Windle et al., 1940). Therefore, the fetal heart and brain receive more highly oxygenated blood than the lower portion of the body and the placenta. This conclusion implies that most of the blood from the inferior vena cava crosses directly over to the left atrium, and that the blood returning from the lungs to the left atrium does not greatly diminish the relatively high oxygen content. In this connec- tion, it has been demonstrated by Barcroft and his colleagues (1939) that in goats and sheep the blood leaving the left side of the fetal heart has a higher oxygen content than that from the right. Cineradiography in fetal lambs (Barclay, Frank- lin and Prichard, 1944) provides a striking demon- stration of the partial separation of the two caval streams in the fetal heart of the sheep. Radio-opaque substances were injected into the jugular vein and a series of roentgenograms were made at the rate of four exposures per second. The blood contain- ing a contrast material was followed through the superior vena cava to the right atrium, right ven- tricle and pulmonary artery; some of it went to the lungs and through the ductus arteriosus to the descending aorta. From the inferior vena cava, however, almost all of the radio-opaque material went directly into the left atrium; some entered the right ventricle, but most of it traversed the foramen ovale and reached the left side of the heart, whence it passed into the ascending aorta and into the coronary circulation. HUMAN FETAL CIRCULATION Method The fetus with intact membranes was removed by Caesarean section under ether anesthesia and the angiocardiography was performed immediately. The angiocardiographic table was placed beside the operating table so that the examination could be completed before the umbilical cord was severed. In the actual procedure the membranes were in- cised, the fetus placed in position, and the contrast injected into the umbilical vein as far as possible from the fetus, usually one-half to one minute after incising the membranes. The fetus was kept warm by an infrared lamp and manipulated as little as possible. In the first part of the series 70 per cent Umbradil (Astra) was employed as a contrast medium, but [lO9] Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

H U M A N F E T A L C I R C U L A T I O N : C H A N G E S IN T H E C A R D I O V A S C U - LAR S Y S T E M AT B I R T H AND D I S T U R B A N C E S IN T H E P O S T - N A T A L C L O S U R E OF T H E F O R A M E N OVALE AND D U C T U S A R T E R I O S U S
JOHN LIND AND CARL WEGELIUS Karolinska Institute, Stockholm, Sweden
Our present knowledge of fetal circulation and the alterations that take place at birth are based upon anatomical studies and experimental investi- gations in animals, which until recently have not included study of the human fetus. Barclay, Frank- lin and Prichard's angiocardiographic investigation of the circulation in the fetal lamb before and after delivery is considered to be one of the most im- portant contributions to the study of fetal circula- tion (1944).
THE COURSE OF THE BLOOD THROUGH THE FETAL HEART
The course of the blood through the fetal heart has been the subject of a lively controversy. The principal question has been the degree of separation and mixing of the two caval streams coming into the fetal right atrium. The inferior vena cava con- tains blood from the placenta, the most highly oxygenated blood coming to the heart, in spite of the admixture with venous blood from the lower part of the body. The superior vena cava, on the other hand, brings the poorly oxygenated, unmixed venous blood from the heart and the upper portion of the body.
There are two principal theories as to the course of the blood through the fetal heart. One holds that the two streams entering the right atrium are mixed. Therefore, the well oxygenated blood from the pla- centa, diluted once when the ductus venosus joins the inferior vena cava, enters the right atrium and is again diluted by blood from the superior vena cava and coronary sinus. The resulting mixture goes two ways; some enters the right ventricle but approximately half passes through the foramen ovale into the left side of the heart (Pohlman, 1907; Kellogg, 1930). Consequently the aorta and the pulmonary artery are considered to have the same oxygen content, and the upper part of the body, including the fetal heart itself, receives no better oxygen supply than the lower parts of the body and the placenta. If there should be a significant quan- tity of reduced blood entering the left atrium from the fetal lungs, the heart muscle and the brain would get less oxygen than the lower part of the body and the placenta.
According to the other theory, the oxygenated blood which is brought from the placenta goes through the ductus venosus and inferior vena cava to the right atrium and is deflected by a fold of endocardium through the foramen ovale into the left atrium. Thus this stream retains its relative
arterial character by crossing the flow of the venous blood from the superior vena cava which is de- livered to the right atrium and right ventricle. (Huggett, 1927; Barcroft et al., 1936 and 1938; Windle et al., 1940). Therefore, the fetal heart and brain receive more highly oxygenated blood than the lower portion of the body and the placenta. This conclusion implies that most of the blood from the inferior vena cava crosses directly over to the left atrium, and that the blood returning from the lungs to the left atrium does not greatly diminish the relatively high oxygen content. In this connec- tion, it has been demonstrated by Barcroft and his colleagues (1939) that in goats and sheep the blood leaving the left side of the fetal heart has a higher oxygen content than that from the right.
Cineradiography in fetal lambs (Barclay, Frank- lin and Prichard, 1944) provides a striking demon- stration of the partial separation of the two caval streams in the fetal heart of the sheep. Radio-opaque substances were injected into the jugular vein and a series of roentgenograms were made at the rate of four exposures per second. The blood contain- ing a contrast material was followed through the superior vena cava to the right atrium, right ven- tricle and pulmonary artery; some of it went to the lungs and through the ductus arteriosus to the descending aorta. From the inferior vena cava, however, almost all of the radio-opaque material went directly into the left atrium; some entered the right ventricle, but most of it traversed the foramen ovale and reached the left side of the heart, whence it passed into the ascending aorta and into the coronary circulation.
HUMAN FETAL CIRCULATION Method
The fetus with intact membranes was removed by Caesarean section under ether anesthesia and the angiocardiography was performed immediately. The angiocardiographic table was placed beside the operating table so that the examination could be completed before the umbilical cord was severed. In the actual procedure the membranes were in- cised, the fetus placed in position, and the contrast injected into the umbilical vein as far as possible from the fetus, usually one-half to one minute after incising the membranes. The fetus was kept warm by an infrared lamp and manipulated as little as possible.
In the first part of the series 70 per cent Umbradil (Astra) was employed as a contrast medium, but
[lO9]
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from
110 IOHN LIND AND CARL WEGELIUS
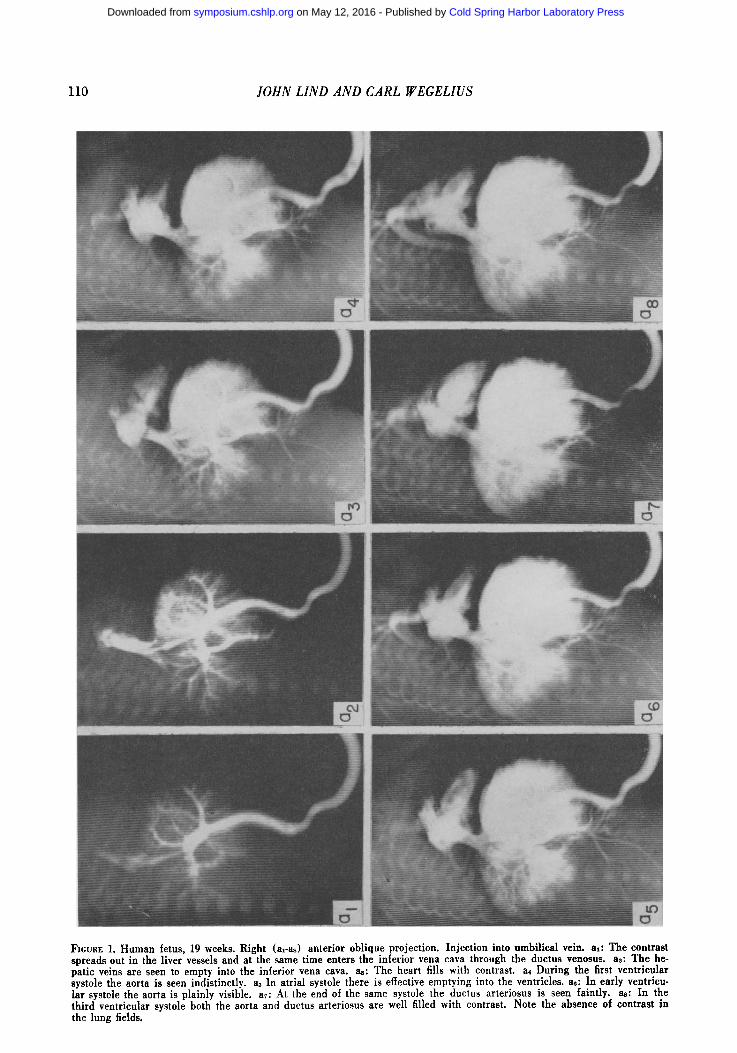
FIGURE 1. Human fetus, 19 weeks. Right (al-as) anterior oblique projection. Injection into umbilical vein. al: The contrast spreads out in the liver vessels and at the same time enters the inferior vena eava through the duetus venosus, as: The he- patic veins are seen to empty into the inferior vena cava. as: The heart fills with contrast, a~ During the first ventrieular systole the aorta is seen indistinctly, a5 In atrial systole there is effective emptying into the ventricles, ae: In early ventrieu- lar systole the aorta is plainly visible, a~: At the end of the same systole the duetus arteriosus is seen faintly, as: In the third ventrieular systole both the aorta and ductus arteriosus are well filled with contrast. Note the absence of contrast in the lung fields.
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from

HUMAN FETAL CIRCULATION 111
later 70 per cent Isodyne (Astra) was used, because it has the same streaming properties as blood. The amount used was one to three ml in fetuses, and three to five ml in newborn infants.
Roentgenographic Technique A direct serial roentgenographic technique was
used, with photography in two planes simultaneous- ly at 0.08 second intervals. The apparatus was originally built by the authors in collaboration with the SchSnander X-ray Company for angiocardiog- raphy on children and is described in detail by Fredzell, Lind, Ohlson and Wegelius (1950). This report is restricted to the main features of construc- tion and the mode of operation of the apparatus.
There are certain principal differences between this technical method and that used by Barclay, Franklin and Prichard, and other authors. The central feature of this method is direct roentgenog- raphy with a rapid exchange of cassettes. An in- crease of the rate of exposure beyond approximately two pictures per second has to date been practicable only in the so-called cinematographic fluorography, that is, photography of the image on the fluorescent screen with substandard film. The authors previ- ously mentioned, however, as well as other workers in angiocardiography, stress the superior quality of direct full-sized photography as compared with fluorography. There is not only the advantage of a conveniently interpretable primary material in the form of full-sized roentgen film, which does not re- quire the projective enlargement of the fluoro- graphic film, but also of the better reproduction of detail in the directly photographed picture which is superior in both contrast and clarity. The smaller the object, the greater is the importance of this factor.
The present series included human fetuses 12 to 25 weeks of age, where the great efferent vessels, the aorta, pulmonary artery and ductus arteriosus, have a caliber of approximately one half to one mm and lie adjacent to each other; the need for a meticulous reproduction of detail is naturally great- er in these subjects than in the adult in whom these vessels have a caliber 20 to 30 times larger. Direct roentgenography with its qualitative superiority was thus the method of choice in this study.
It is necessary to have an exposure sequence sufficiently rapid to follow the dynamic processes; the direction and rate of flow of the blood stream, the morphologic changes of the heart, and the re- lationships of the great vessels during various phases of the cardiac cycle. In these respects 10 to 12 exposures per second afford comparatively good results. Moreover, serial photography with 40 pictures in four seconds permit~ an acceptable cinematozraphic visualization of the course of the angiocardiograDhv. Thus the "slow", detailed, di- rect: photography is combined with "rapid" indirect photography, which is less detailed although service- able for dynamic angiocardiographic studies.
Synchronous bi-plane radiology is of importance in the morphologic and functional study of the heart; in no single view is it possible to avoid overlapping of the various chambers, but the use of two projections provides information valuable to the study of cardiac dynamics. The two views must be taken synchronously, however, in order to localize accurately the contrast medium in the in- dividual chambers of the heart.
Controls In a number of cases the angiocardiography find-
ings were verified by autopsy; a solidifying contrast medium was injected through the vessels of the cord and the roentgenographic study carried out with the subject in a position corresponding to that used in the angiocardiography. The anatomic find- ings at autopsy were then compared with the find- ings from the roentgenographic studies.
RESULTS The InJerior Vena Caval Stream
The right anterior oblique projection is well suited to the study of the dynamics of the heart. In this view the two sides of the heart are superim- posed, but the atrium and ventricle are viewed separately. It is impossible to observe the stream of contrast from the right atrium into the left, but the amount entering the right ventricle will be clearly seen. Figure 1 shows the opaque material entering the umbilical vein and flowing through the ductus venosus into the inferior vena cava and the hepatic circulatory system. In this projection the left atrium is superimposed on the right, making it impossible to observe the mechanism of filling of the atria. With the first ventricular systole follow- ing the filling of the atria, the aorta is well filled with the contrast material, but the pulmonary artery and lung vessels are only faintly opacified. This gives an estimate of the proportion of blood flowing through these two great vessels.
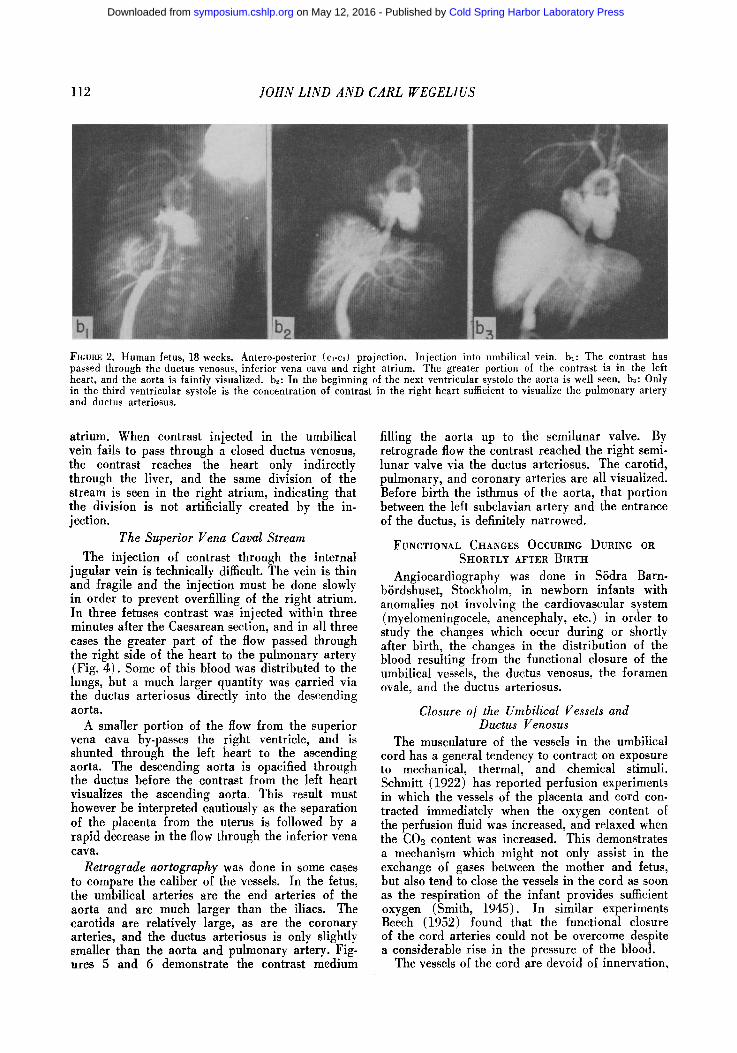
In the left anterior oblique view, the two sides of the heart are seen separately, but on each side the ventricle is superimposed on the atrium. In Figure 2 the contrast can be seen to pass through the um- bilical vein, ductus venosus and inferior vena cava into the right atrium. Here the contrast is split into two streams; some goes on to the right ven- tricle, but a large portion goes through the foramen ovale into the left atrium then to the left ventricle and the aorta. Note the absence of opacification of the pulmonary artery. The figure clearly demon- strates the large stream of contrast flowing into the left atrium.
From Figure 3 it can be seen that the contrast, on entering the heart, divides on the free edge of the interatrial septum (crista dividens) into a large left and a small right stream. The former passes through the foramen ovale and apparently does not become significanth, diluted to any considerable extent by pulmonary venous return in the left
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from
112 JOHN LIND AND CARL WEGELIUS
FIGURE 2. Human fetus, 18 weeks. Antero-posterior (cl-c~) projection. Injection into umbilical vein. bl: The contrast has passed through the ductus venosus, inferior vena cava and right atrium. The greater portion of the contrast is in the left heart, and the aorta is faintly visualized, b~: In the beginning of the next ventricular systole the aorta is well seen. ba: Only in the third ventricular systole is the concentration of contrast in the right heart sumcient to visualize the pulmonary artery and ductus arteriosus.
atrium. When contrast iniected in the umbilical vein fails to pass through a closed ductus venosus, the contrast reaches the heart only indirectly through the liver, and the same division of the stream is seen in the right atrium, indicating that the division is not artificially created by the in- jection.
The Superior Vena Caval Stream
The injection of contrast through the internal jugular vein is technically difficult. The vein is thin and fragile and the injection must be done slowly in order to prevent overfilling of the right atrium. In three fetuses contrast was injected within three minutes after the Caesarean section, and in all three cases the greater part of the flow passed through the right side of the heart to the pulmonary artery (Fig. 4). Some of this blood was distributed to the lungs, but a much larger quantity was carried via the ductus arteriosus directly into the descending aorta.
A smaller portion of the flow from the superior vena cava by-passes the right ventricle, and is shunted through the left heart to the ascending aorta. The descending aorta is opacified through the ductus before the contrast from the left heart visualizes the ascending aorta. This result must however be interpreted cautiously as the separation of the placenta from the uterus is followed by a rapid decrease in the flow through the inferior vena cava.
Retrograde aortography was done in some cases to compare the caliber of the vessels. In the fetus, the umbilical arteries are the end arteries of the aorta and are much larger than the iliacs. The carotids are relatively large, as are the coronary arteries, and the ductus arteriosus is only slightly smaller than the aorta and pulmonary artery. Fig- ures 5 and 6 demonstrate the contrast medium
filling the aorta UP to the semilunar valve. By retrograde flow the contrast reached the right semi- lunar valve via the ductus arteriosus. The carotid, pulmonary, and coronary arteries are all visualized. Before birth the isthmus of the aorta, that portion between the left subclavian artery and the entrance of the ductus, is definitely narrowed.
FUNCTIONAL CHANGES OCCURING DURING OR SHORTLY AFTER BIRTH
Angiocardiography was done in SSdra Barn- biJrdshuset, Stockholm, in newborn infants with anomalies not involving the cardiovascular system (myelomeningocele, anencephaly, etc.) in order to study the changes which occur during or shortly after birth, the changes in the distribution of the blood resulting from the functional closure of the umbilical vessels, the ductus venosus, the foramen ovale, and the ductus arteriosus.
Closure o] the Umbilical Vessels and Ductus Venosus
The musculature of the vessels in the umbilical cord has a general tendency to contract on exposure to mechanical, thermal, and chemical stimuli. Schmitt (1922) has reported perfusion experiments in which the vessels of the placenta and cord con- tracted immediately when the oxygen content of the perfusion fluid was increased, and relaxed when the CO2 content was increased. This demonstrates a mechanism which might not only assist in the exchange of gases between the mother and fetus, but also tend to close the vessels in the cord as soon as the respiration of the infant provides sufficient oxygen (Smith, 1945). In similar experiments Beech (1952) found that the functional closure of the cord arteries could not be overcome despite a considerable rise in the pressure of the blood.
The vessels of the cord are devoid of innervation,
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from

HUMAN FETAL CIRCULATION 113
FICURE 3. Human fetus, 13 weeks. Right (al-as) and left (bl-b~) anterior oblique projections. Injection into umbilical vein. axbl: Contrast has passed through the ductus venosus into the inferior vena cava. a.~b~: The right and left atrium fill simul- taneously, a~b3: There is more contrast in the left side of the heart than in the right, a~b4: The heart is opacified in ven- tricular diastole. The right ventricle is filled up to the pulmonary valve. There is retrograde filling of the entire inferior vena eava. a~b~: In ventricular systole the pulmonary artery and ductus arteriosus are clearly shown, but no contrast is seen in the branches of the pulmonary artery. The aorta is well visualized. Note the narrowing of the pulmonary eonus.
and the functional closure is the result of smooth- muscle contraction. After birth it may take some minutes for this closure to be effected. The actual obliteration of the lumen takes three to five weeks, and isolated portions of the vessels may retain a vestigial lumen for a much longer time (Patten, 1953).
The sealing off of the umbilical end of the ductus venosus is effected soon after delivery by a sphincter of considerable size, as shown in lambs by Barclay,
Franklin and Prichard (1944). They suggested that the sphincter can contract against the portal venous pressure but not against full pressure in the um- bilical vein.
In six full term newborn infants of the present series one to two ml of contrast medium was injected through the umbilical vein five to ten minutes after delivery. In each case there was an initial high resistance to the injection, due to marked contrac- tion of the ductus venosus (Fig. 7). In one case the
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from

114 /OLIN LIND AND CARL WEGELIUS
FIGURE 4. Human fetus, 14 weeks. Right (al-as) and left (bl-b~) anterior oblique projections. Injection into internal jugu- lar vein; 3 minutes after delivery by Caesarean section, a~bl: The contrast which enters the right atrium flows into both the left atrium and right ventricle, a2b2: There is the same concentration of contrast on both sides of the heart. The right ven- tricle is filled up to the pulmonary valve. There is retrograde filling of the inferior vena cava. a~b3: In ventricular systole the right ventricle diminishes in size and the pulmonary artery is filled with contrast. The ductus arteriosus and descending aorta are visualized simultaneously with the pulmonary artery. The ascending and transverse portions of the aorta are only faintly visualized in bs. a&4: In the succeeding ventricular systole the ascending and transverse portions of the aorta appear dis- tinctly. Note the contraction of the pulmonary conus, a~b~: Early in the following ventricular systole the aorta and pul- monary artery are both well visualized. The innominate, carotid, and subclavian arteries are well opacified. Note the small amount of contrast in the branches of the pulmonary artery.
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from

HUMAN FETAL CIRCULATION 115
Fxeua~ 5. Human fetus, 12 weeks. Antero-posterior (c~-c.~) an l latcral (d,-d~) projections. Injection into common carotid artery, cldl: There is simultaneous filling of the aorta, ductus and pulmonary artery, c~d~: The aorta, ductus, and pulmonary artery are of approximately the same size. It is interesting to note the poor filling of the branches ot the pulmonary artery in contrast to the prompt and profuse opacification of the liver vessels (Fig. 1).
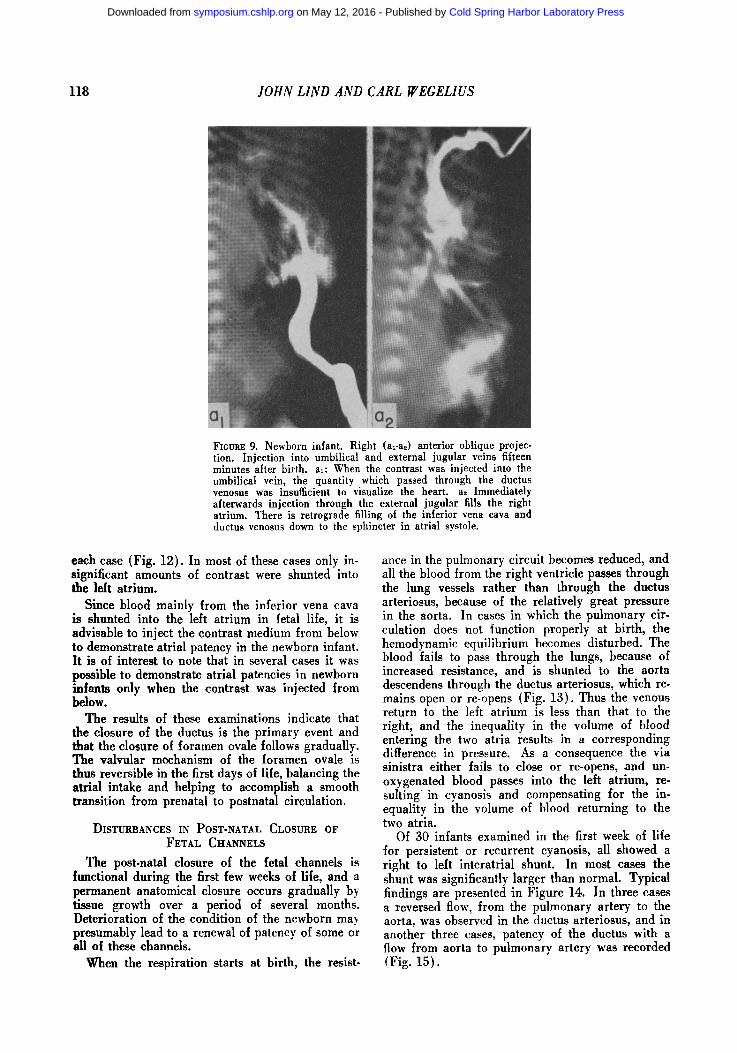
ductus could be seen to contract rhythmically (Fig. 8) , indicating an intermittent constriction, and the umbilical vein showed alternate areas of constric- tion and dilatation. A marked narrowing of the caliber of the umbilical vein at the level of the um- bilicus was often observed. Figure 9 shows that failure of filling of the ductus in the human fetus is apparently due to contraction of the sphincter at the umbilical end of the vessel.
Closure of the Ductus arteriosus About a hundred years ago Langer (1857) recog-
nized the histologic difference between the ductus arteriosus and the vessels it unites. The wall is mainly muscular, and the intima is proportionately thicker but with considerable variations in thick- ness. Because of its muscularity and the special arrangement of the muscle bundles, the ductus has been compared to a sphincter (Boyd, 1941).
Some authorities believe that in human infants the functional closure of foramen ovale and duetus arteriosus is gradual. They maintain that in the late weeks of fetal life the pulmonary vessels are already
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from

116 IOHN LIND AND CARL I~'EGELIUS
FLOURS 6. Fetus aged approximately 19 weeks. Left an- terior oblique position. Injection needle in one of umbilical arteries.
Intensive contrast filling of aorta, ductus arteriosus and great arteries departing from arch and the descendent part of aorta. Pulmonary artery and its branches appear filled. Note the difference between the markedly larger calibers of the arteries of the upper as compared to those of the lower half of the body. The small calibers of the hepatic as well as the mesenteric arteries are striking. The aorta termi- nally divides into the two large-sized umbilical arteries. The passage of dye through the coronary circulation pro- duces a shadow of the whole heart.
minutes), mechanical or electrical stimulation of the ductus (15-30 seconds), insumation of the lungs with oxygen, intracardiac injection of adrenalin (3-4 minutes), acute significant bleeding (6 minutes), and intravenous injection of oxygen. They con- cluded that respiration is the most important phy- siologic stimulus when the inspired air contains oxygen.
The second phase of physiologic post natal clo- sure of the ductus is a slow anatomical obliteration. The lumen is gradually occluded by an over-growth of intimal tissue, a process recognizable even in the last months of fetal life. According to data compiled by Scammon and Norris (1918) the obliterative process is very slow during the first two weeks of life and does not reach a maximum until the second month. Christie (1930) has presented the findings from an anatomical study of 558 infants, in which the ductus was still patent in 65 per cent at the age of 2 weeks, in 44 per cent at 4 weeks, in 12 per cent at 8 weeks, in 3 per cent at 20 weeks, in 2 per cent at 32 weeks, and in more than 1 per cent at the age of I year.
In human fetuses investigated by injection of con- trast through the umbilical vein, the ductus was always visualized simultaneously with the pulmo- nary artery and with the same degree of opacifica- tion. However, the opacification of the ductus was less than that of the aorta and its main branches, which is indirect evidence that contrast is passing through the ductus from the pulmonary artery to
carrying enough blood to sustain life and that there is no great and sudden increase in the pulmonary flow at birth, but rather a smooth steady rise during the first few weeks (Patten and Toulmin, 1930). It is believed that during these early weeks func- tional closure of the ductus arteriosus and the fora- men ovale is gradual and that to maintain the cir- culation smoothly, these passages continue to allow the passage of decreasing amounts of blood until the blood flow of the pulmonary circuit becomes equal to that of the systemic circuit.
In 1900, Gerard suggested the theory of primary occlusion and secondary obliteration of the ductus; Barclay et al. verified this theory by experiments on fetal lambs. According to this work closure of the ductus never occurs before ligation of the cord but in a healthy birth takes place rapidly, completely, and permanently when the cord is ligated. From ex- periments on the guinea pig fetus Kennedy and Clark (1942) concluded that functional occlusion by muscular contraction of the ductus takes place even after interruption of all pathways for neuro- genic impulses. The following stimuli caused con- striction of the ductus: normal respiration (5
FIGURE 7. Newborn infant. Right (aO anterior oblique projection. Injection into umbilical vein immediately after birth.
a~: The umbilical vein is heavily opacified, and the prox- imal portion of the ductus venosus, where the sphincter is located, is thread-like in diameter.
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from

HUMAN FETAL CIRCULATION 117
FIGURE 8. Newborn infant. Left (bl-b4) anterior oblique projection. Injection into umbilical vein. bl-b,: The ductus venosus alternately appears and disappears, suggesting an intermittently functioning sphincter.
the aorta. In one case repeated contraction of the ductus was observed(Fig. 10). Angiocardiography by peripheral intravenous injection in ten new- borns within twelve hours of delivery showed no sign of patency of the ductus arteriosus. In four newborns retrograde aortogram through the brach- ial artery within two hours of birth also failed to make visible the ductus (Fig. 11) directly and in- directly, by opacification of the pulmonary artery.
Closure o/ the Foramen ovale
It has long been known that the foramen ovale closes shortly after birth, completing the arrange- ment by which all the blood returning from the body goes to the lungs. However, there is still a difference of opinion as to how promptly this open- ing closes.
With the expansion of the lungs the flow of blood through the lungs increases, more blood returns to the left atrium, and the pressure in this chamber increases. The immediate closure of the ductus at the initiation of respiration raises the pressure in the pulmonary circulation, and the resulting change in relative pressure tends to close the valve of the foramen ovale and keep it closed. The work of Barclay, Franklin and Prichard (1944) indicates
that the actual mechanical contraction of the left atrium closes the foramen ovale, and that this clo- sure occurs physiologically before that of the ductus arteriosus.
After birth there is a progressive reduction in the size of the interatrial communication to a narrow slit between the valve and the septum. For several months the foramen may be regarded as function- ally closed. Thereafter connective tissue converts the valve into a fixed septal structure in six to eight months, and finally, there is an adhesion of the valve to the septum. There is a great variation in the age at which the final closure occurs (Patten, 1954).
Since the injection of contrast medium cannot be performed through the umbilical vein before the ductus venosus closes, the state of patency of the foramen ovale and the ductus arteriosus after birth must be studied in another way. In six newborn infants in whom angiocardiography was carried out by injection into the antecubital vein within twelve hours of delivery, a diagnosis of atrial septal patency was made in three cases. In another six newborns, however, in whom injection was done through a malleolar vein, the diagnosis of atrial septal patency with a right to left shunt was made in
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from
118 JOHN LIND AND CARL g/EGELIUS
FIGURE 9. Newborn infant. Right (ara,) anterior oblique projec- tion. Injection into umbilical and external jugular veins fifteen minutes after birth, al: When the contrast was injected into the umbilical vein, the quantity which passed through the ductus venosus was insufficient to visualize the heart, a.~ Immediately afterwards injection through the external jugular fills the right atrium. There is retrograde filling of the inferior vena cava and ductus venosus down to the sphincter in atrial systole.
each case (Fig. 12). In most of these cases only in- significant amounts of contrast were shunted into the left atrium.
Since blood mainly from the inferior vena cava is shunted into the left atrium in fetal life, it is advisable to inject the contrast medium from below to demonstrate atrial patency in the newborn infant. It is of interest to note that in several cases it was possible to demonstrate atrial patencies in newborn infants only when the contrast was injected from below.
The results of these examinations indicate that the closure of the ductus is the primary event and that the closure of foramen ovale follows gradually. The valvular mechanism of the foramen ovale is thus reversible in the first days of life, balancing the atrial intake and helping to accomplish a smooth transition from prenatal to postnatal circulation.
DISTURBANCES IN POST-NATAL CLOSURE OF FETAL CHANNELS
The post-natal closure of the fetal channels is functional during the first few weeks of life, and a permanent anatomical closure occurs gradually by tissue growth over a period of several months. Deterioration of the condition of the newborn may presumably lead to a renewal of patency of some or all of these channels.
When the respiration starts at birth, the resist-
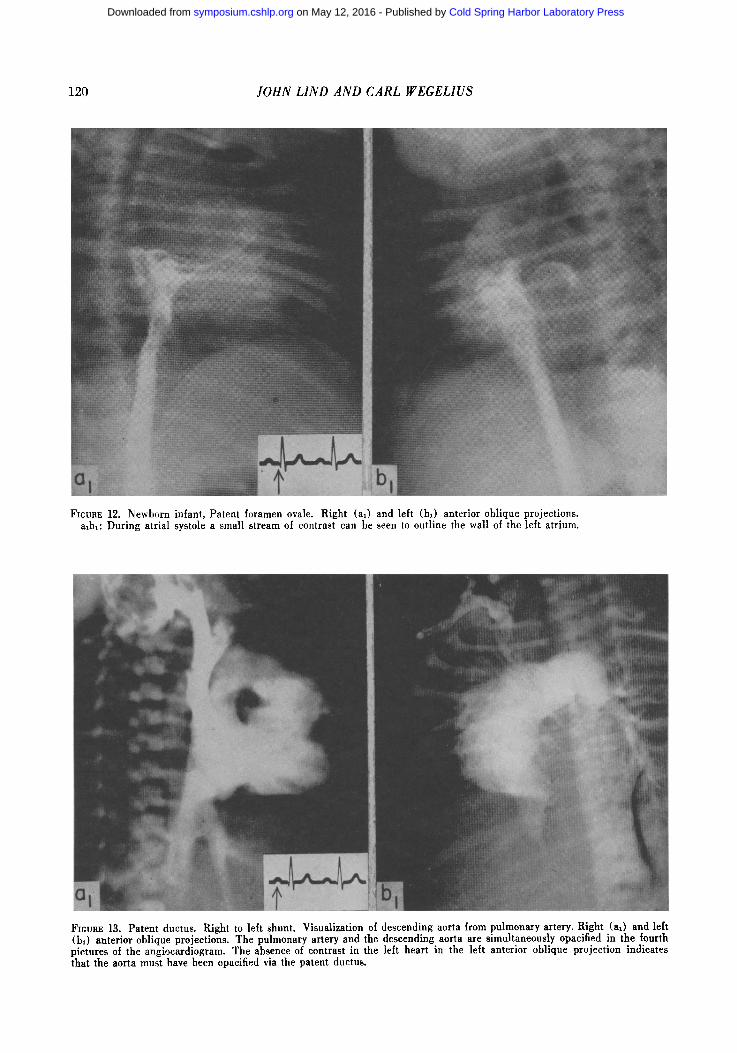
ance in the pulmonary circuit becomes reduced, and all the blood from the right ventricle passes through the lung vessels rather than through the ductus arteriosus, because of the relatively great pressure in the aorta. In cases in which the pulmonary cir- culation does not function properly at birth, the hemodynamic equilibrium becomes disturbed. The blood fails to pass through the lungs, because of increased resistance, and is shunted to the aorta descendens through the ductus arteriosus, which re- mains open or re-opens (Fig. 13). Thus the venous return to the left atrium is less than that to the right, and the inequality in the volume of blood entering the two atria results in a corresponding difference in pressure. As a consequence the via sinistra either fails to close or re-opens, and un- oxygenated blood passes into the left atrium, re- suiting in cyanosis and compensating for the in- equality in the volume of blood returning to the two atria.
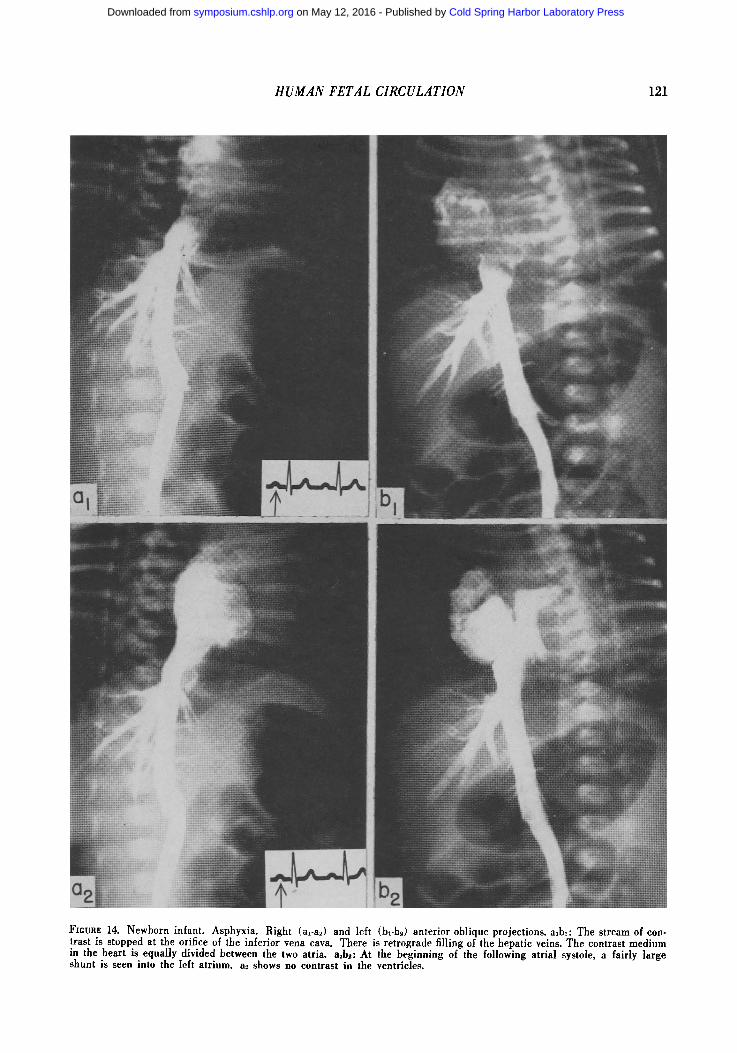
Of 30 infants examined in the first week of life for persistent or recurrent cyanosis, all showed a right to left interatrial shunt. In most cases the shunt was si~ificantly larger than normal. Typical findings are presented in Figure 14. In three cases a reversed flow, from the pulmonary artery to the aorta, was observed in the ductus arteriosus, and in another three cases, patency of the ductus with a flow from aorta to pulmonary artery was recorded (Fig. 15).
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from
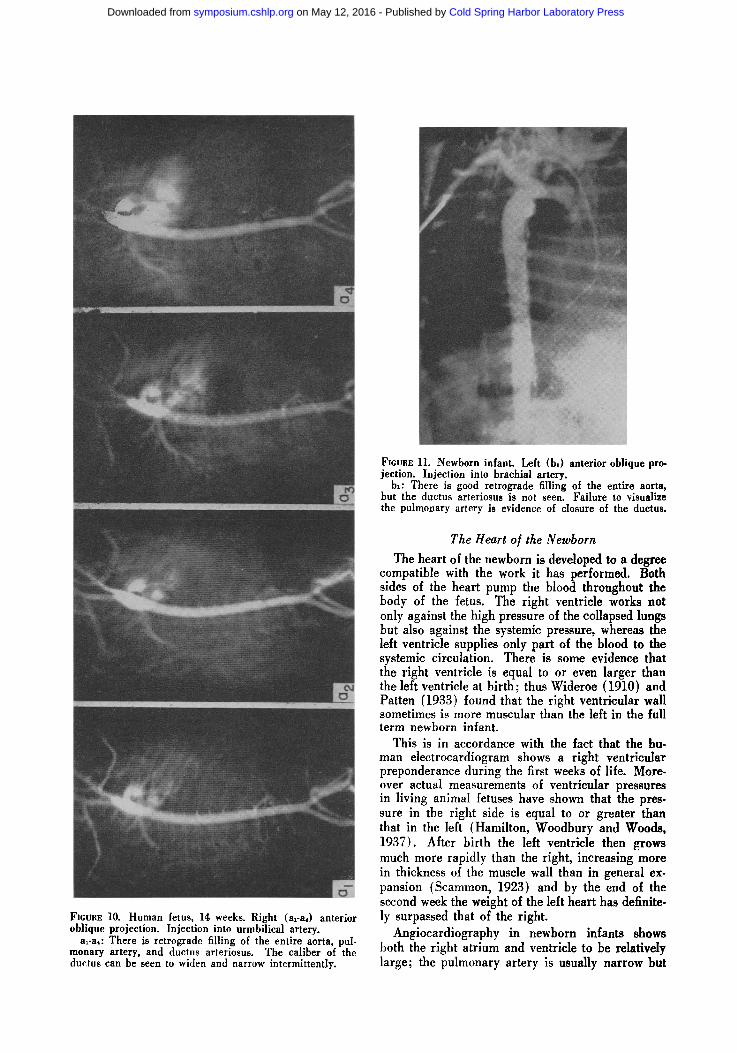
Ftcvar. 10. Human fetus, 14 weeks. Right (arab) anterior oblique projection. Injection into urmbilical artery.
a~-a4: There is retrograde filling of the entire aorta, pul- monary artery, and ductus arteriosus. The caliber of the ductus can be seen to widen and narrow intermittently.
FICURE 11. Newborn infant. Left (bl) anterior oblique pro- jection. Injection into brachial artery.
bl: There is good retrograde filling of the entire aorta, but the ductus arteriosus is not seen. Failure to visualize the pulmonary artery is evidence of closure of the ductus.
The Heart o] the Newborn
The heart of the newborn is developed to a degree compatible with the work it has performed. Both sides of the heart pump the blood throughout the body of the fetus. The right ventricle works not only against the high pressure of the collapsed lungs but also against the systemic pressure, whereas the left ventricle supplies only part of the blood to the systemic circulation. There is some evidence that the right ventricle is equal to or even larger than the left ventricle at birth; thus Wideroe (1910) and Patten (1933) found that the right ventricular wall sometimes is more muscular than the left in the full term newborn infant.
This is in accordance with the fact that the hu- man electrocardiogram shows a right ventricular preponderance during the first weeks of life. More- over actual measurements of ventricular pressures in living animal fetuses have shown that the pres- sure in the right side is equal to or greater than that in the left (Hamilton, Woodbury and Woods, 1937). After birth the left ventricle then grows much more rapidly than the right, increasing more in thickness of the muscle wall than in general ex- pansion (Scammon, 1923) and by the end of the second week the weight of the left heart has definite- ly surpassed that of the right.
Angiocardiography in newborn infants shows both the right atrium and ventricle to be relatively large; the pulmonary artery is usually narrow but
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from
120 JOHN LIND AND CARL IVEGELIUS
FIGURE 12. Newborn infant, Patent foramen ovale. Right (al) and left (b~) anterior oblique projections. albt: During atrial systole a small stream of contrast can be seen to outline the wall of the left atrium.
FICURE 13. Patent ductus. Right to left shunt. Visualization of descending aorta from pulmonary artery. Right (a~) and left (bl) anterior oblique projections. The pulmonary artery and the descending aorta are simultaneously opacified in the fourth pictures of the angiocardiogram. The absence of contrast in the left heart in the left anterior oblique projection indicates that the aorta must have been opacified via the patent ductus.
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from
HUMAN FETAL CIRCULATION 121
Ftcun~. 14. Newborn infant. Asphyxia. Right (arab) and left (bl-b~) anterior oblique projections, a~bl: The stream of con- lrast is stopped at the orifice of the inferior vena eava. There is retrograde filling of the hepatic veins. The contrast medium in the heart is equally divided between the two atria, a2b~: At the beginning of the following atrial systole, a fairly large shunt is seen into the left atrium, a~ shows no contrast in the ventricles.
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from

FIGURE 15. Newborn infant. Patent ductus arteriosus. Right (al-aa) and left (bl-b~) anterior oblique projection, a~bl: In ventricular systole the pulmonary artery is well seen in both projections, a~b~: In the following ventricular diastole the contrast me- dium has almost completely disappeared from the pulmonary artery, a~b~: In the following ventricular systole the pulmonary artery is again well opacified.
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from
HUMAN FETAL CIRCULATION 123
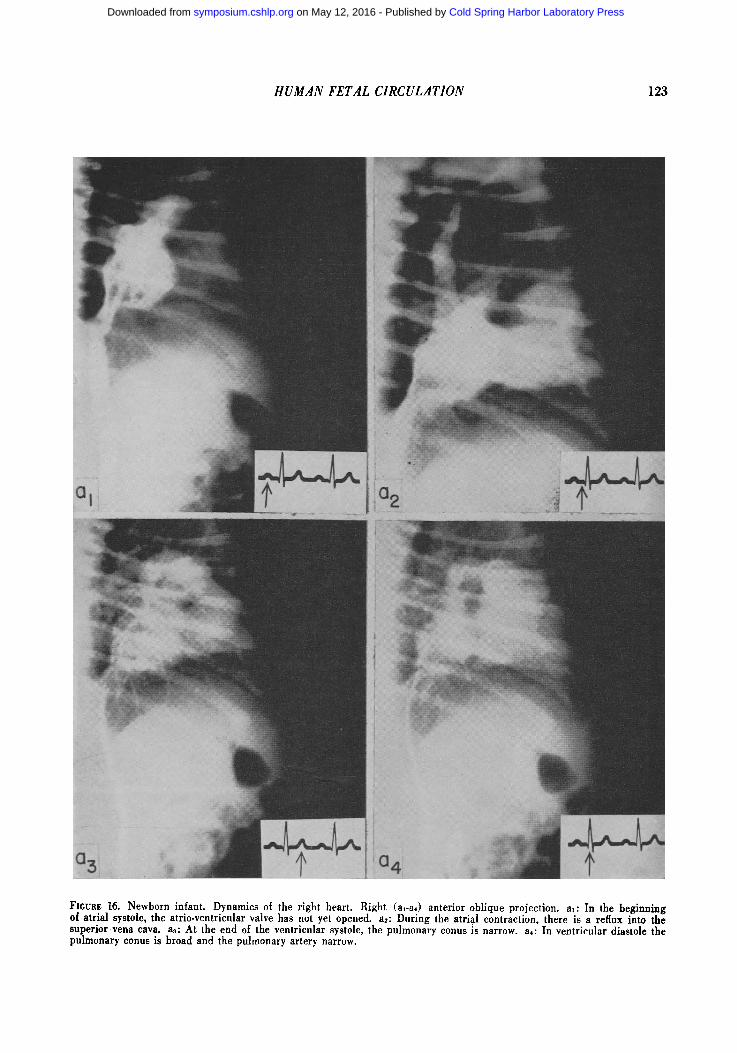
FICURE 16. Newborn infant. Dynamics of the right heart. Right (al-a,) anterior oblique projection, al: In the beginning ot atrial systole, the atrio-ventricular valve has not yet opened, a2: During the atrial contraction, there is a reflux into the superior vena cava. a3: At the end of the ventricular systole, the pulmonary conus is narrow, a4: In ventricular diastole the pulmonary eonus is broad and the pulmonary artery narrow.
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from

124 JOHN L I N D A N D C A R L W E G E L I U S
dilates strikingly during ventricular systole (Fig. 16). A typical finding during the first week of life is a systolic or diastolic shunt through the foramen ovale (Table 1) indicating that the pressure in the right atrium equals or slightly exceeds that in the left.
<6 hours 7-12 "
13-24 " 2. 3 days 4-6 7-12 "
TABLE 1.
Interatrial shunts Number R-L L-R of cases
6 3 6 4 2 5 4 1 5 3 1 5 3 0 5 1 0 5
Functional disturbance of the right atrium is indirect evidence of the relative right ventricular hypertrophy. It can be shown that the right ven- tricle fills slowly immediately after ventricular sys- tole and only after the atrial contraction does it fill rapidly. As a reflection of the increased resistance to atrial emptying, a reflux of contrast medium into the vena cava often occurs (Fig. 16).
TABLE 2. AVERAGE HEART VOLUME IN 20 NEWBORN INFANTS
Days of life 1 2 4 6 Heart volume in ml 42 35 32 30 Birth weight 3000-3500 gms. Error of the method, calculated from the difference in double determinations, is 2.7 per cent.
I t is known that the heart of the newborn infant is relatively large and that it decreases in size dur- ing the first week of life. The ratio of heart volume to body weight does not change, however, if the weight of the placenta is included with the body weight at birth.
The loss of the placental circulation at birth decreases the vascular bed by 25 per cent and the vascular volume by only 10 to 15 per cent, there- fore the heart of the newborn infant must circulate 90 per cent of the former blood volume through only 75 per cent of the former vascular bed (Smith, 1951). The increase in muscular tonus at this time, however, simultaneously increases the peripheral resistance. As a reflexion of the extra burden im- posed on the cardiovascular system at birth, roent- genographic studies show that the heart has a ten- dency to increase in size during the first hour of extrauterine life.
TABLE 3. AVERAGE HEART VOLUME IN 24 NEWBORN INFANTS Hours of life 0 1A 1/2 1 2 3 Heart volume in ml 38 45 44 41 38 37
After the initial increase in size, the actual heart volume decreases during the next 24 hours (Table 3). No significant decrease occurs in the following week (Table 2) , since the heart volume is closely correlated with blood volume, and the latter remains constant during the first week of life in spite of a decrease in hemoglobin concentration (Karlberg
and Lind, unpublished data) . In anoxic infants, however, the heart value is often abnormally large and remains so for the duration of the anoxia, prob- ably as a result of the abnormally high vascular resistance in the atelectatic lungs.
SUMMARY
Human fetal circulation and the changes that take place in the circulatory system at birth have been studied by a rapid angiocardiographic technique using a constrast medium that has the same stream- ing properties as the blood. The effect on the heart of the closure of the fetal channels and the common disturbances in closure are discussed.
REFERENCES
BARCLAY, A. E., FRANKLIN, K. J., and PnICHARD, M. M. L., 1944, The Foetal Circulation. 1st ed. Oxford, Blackwell Scientific Publications.
BARCROF% J., 1936, Foetal circulation and respiration. Physiol. Rev. 16: 103-128.
BARCROFT, J., BARRON, D. H., KRAMER, K., and MILIKAN, G. A., 1938, Factors which influence the oxygen supply of the brain at birth. J. Physiol. U.S.S.R. 24: 43-55.
BANCROFT, J., KENNEnY, J. A., and MASON, M. F., 1939, The direct determination of the oxygen consumption of the foetal sheep. J. Physiol. 95: 269-275.
BOYD, J. D., 1941, The nerve supply of the mammalian ductus arteriosus. J. Anat., Paris. 75: 457.
CHRISTIE, A., 1930, Normal closing time of the foramen ovale and the ductus arteriosus: an anatomic and sta- tistical study. Amer. J. Dis. Child. 40: 323-326.
FnEDZELL, G., LIND, J., OHLSON, E., and WEGELmS, C., 1950, Direct serial roentgenography in two planes simul- taneously at 0.08 second intervals. Amer. J. Roentg. Had. Therapy. 63: 548-558.
G~RARD, G., 1900, De 1' oblitGration du canal artGriel, Les thGories et les rafts. J. Anat., Paris. 36: 323.
HAMILTON, W. F., WOODBURY, R. A., and Woops, E. B., 1937, The relation between systemic and pulmonary blood pressure in the fetus. Amer. J. Physiol. 119: 206.212.
HUCGETT, A. ST. G., 1927, Foetal blood-gas tensions and gas transfusion through the placenta of the goat. J. Physiol. 62: 373.
KELLOGG, H. B., 1930, St,dies on the fetal circulation of mammals. Amer. J. Physiol. 91: 637.
KENNEDY, J. A., and CLARK, S. L., 1942, Observations on the physiological reactions of the ductus arteriosus. Amer. J. Physiol. 136: 140.
LANCER, C., 1857, Zur Anatom;e der fiitalen Kreislauf- sorgane. Z. ~es. ~.rzte Wien 13: 328.
LIND. J., 1950, Heart Volume in Normal Infants. 1st ed. Stockholm, Alb. Bonnets Boktryckeri.
LtND, J., and WEGEUUS, C., 1949, Angiocardiographic studies on the human foetal circulation. Pediatrics, Oct. 392-400.
PATTEN, B. M., 1933, The Circulatory System: Embryo- logical. In: Growth and Development of the Child; Part 2: Anatomy and Physiology. The White House Conference. New York, The Century Company.
PATTEN. B. M., 1953, The Pathology of the Heart. 1st ed. Springfield, Charles C Thomas.
PATTEN, B. M.. and TOULMIN, K., 1930, Certain measure- ments of the foetal heart and their significance. Anat. Rec. 45: 237.
POHLMAN, A. G.. 1907. The fetal circulation through the heart. Bull. Johns Hopkins Hosp. 18: 409.
SCAMMON, R. E., 1923, Summary of the Anatomy of the Infant and Child. Chapter 3, Vol. 1: Pediatrics, ed. I. A. Abt. Philadelphia, W. B. Saunders Company.
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from

HUMAN FETAL CIRCULATION 125
SCAMMON, . E., and NoRms, E. H., 1918, On the time of the post-natal obliteration of the fetal blood passages (foramen ovale, duetus arteriosus, ductus venosus). Anat. Rec. 15: 165.
SCHMITT, W., 1922, Untersuchungen zur Physiologic der Plazentargef/isse. Z. Biol. 75: 19-78.
StsITa, C. A., 1951, The Physiology of the Newborn Infant. 2rid ed. Springfield, Charles C Thomas.
WtNDLE, W. F., and BECKER, R. F., 1940, The course of the blood through the fetal heart. An experimental study in the cat and guinea pig. Anat. Ree. 77: 417-426.
DISCUSSION
PoPJXK: May I ask what was the X-ray dosage received by the newborn infants during cardioangi- ography and the contrast material used?
LIND: The newborns who were examined with the hi-plane technique including 20 to 30 pictures in each projection got 4 to 5 r, a close which is con- sidered to be quite safe. The reason why the X-ray doses can be kept so low is the short exposure time. With the image amplifier 150 pictures in an ex- amination of 5 seconds duration correspond to an X-ray dosage of 2 to 3 r.
The contrast media used were Umbradil (Astra) 70 per cent in newborns, and in fetuses, Isodyne (Astra) 70 per cent, worked out for studies of the peripheral circulation and which have the same streaming properties as the blood.
GRUENWALD: I believe I have seen in some of your illustrations that the contrast medium injected into the umbilical vein fills the small vessels of the left half of the liver before it enters the right half. I wonder whether this is true; if so, it would con- firm under more natural conditions my injection experiments on livers of newborn infants excised at autopsy.
I also wonder whether you have autopsy studies
on any of the malformed infants in which you demonstrated an open ductus arteriosus. In that event, is there any correlation between the appear- ance of the ductus at autopsy and the angiograms?
LIND: Judging from our pictures, the phenome- non you refer to concerning the liver is a regular finding.
Concerning autopsy, none of the children ex- amined has died during the stay in the hospital, so I have never made any comparison between the X-ray findings and the anatomy.
McCANCE: I would like to ask one or two ques- tions if I may. Have you made any of these ex- periments on normal babies and if so do you con- sider the experimental procedure quite free from any danger, immediate or remote? Would you, for example, feel quite happy to have such an experi- ment made on your own child? Do you in this work of yours ask the mother for her permission to make these investigations?
I ask these questions purely for information, and my reason for asking them is my interest for many years in the ethics of experimentation on human subjects.
LIND: As I may have mentioned in the paper, no normal infant has been examined with angiocardi- ography. The risks involved in the procedure are, I think, of the same magnitude as urography with contrast medium. The accidents which have been reported have occurred in cases of severe congenitM malformations of the heart and in eases with heart failure, and mainly after repeated examinations. I have personal experience of 600 to 700 angiocar- diographies and up to the present I have not had any severe accident. The mother is always asked for her permission to have the examination made.
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from
10.1101/SQB.1954.019.01.015Access the most recent version at doi: 1954 19: 109-125Cold Spring Harb Symp Quant Biol
John Lind and Carl Wegelius THE FORAMEN OVALE AND DUCTUS ARTERIOSUSDISTURBANCES IN THE POST-NATAL CLOSURE OFCARDIOVASCULAR SYSTEM AT BIRTH AND HUMAN FETAL CIRCULATION: CHANGES IN THE
References
http://symposium.cshlp.org/content/19/109#related-urlsArticle cited in:
http://symposium.cshlp.org/content/19/109.refs.htmlat:This article cites 17 articles, 1 of which can be accessed free
serviceEmail alerting
hereclicksign up in the box at the top right corner of the article or
Receive free email alerts when new articles cite this article -
http://symposium.cshlp.org/subscriptions go to: Cold Spring Harbor Symposia on Quantitative BiologyTo subscribe to
Copyright © 1954 Cold Spring Harbor Laboratory Press
Cold Spring Harbor Laboratory Press on May 12, 2016 - Published by symposium.cshlp.orgDownloaded from
Related Documents











