Intro to Health Technology Assessment Cathal Walsh Centre for Health Decision Science (HRB) @CHeDS_ie Biostatistician (NCPE) - Chair of Statistics (UL)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Intro to Health
Technology
Assessment
Cathal Walsh
Centre for Health Decision Science (HRB)
@CHeDS_ie
Biostatistician (NCPE) - Chair of Statistics (UL)
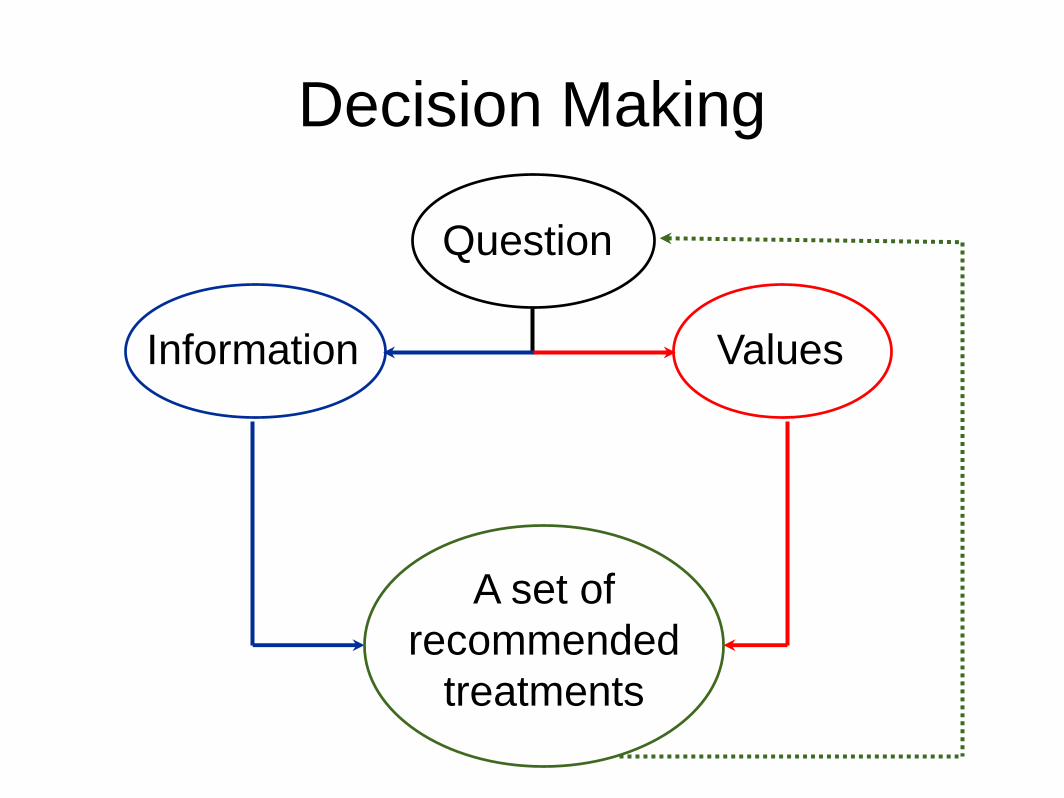
Decision Making
Question
Information Values
A set of
recommended
treatments
Health Technology
Assessment
• In theory, HTA provides a structured
framework for decision making.
• The framework used in Ireland is similar
to that employed in the UK and uses the
QALY and cost tradeoff.
Decision Making … the QALY
• The quality adjusted life year (QALY) is a
function of quality and duration of life.
This is best illustrated by a sketch …
• Note that it explicitly trades side effects,
disability and inconvenience of treatment
(etc!) against outcomes.
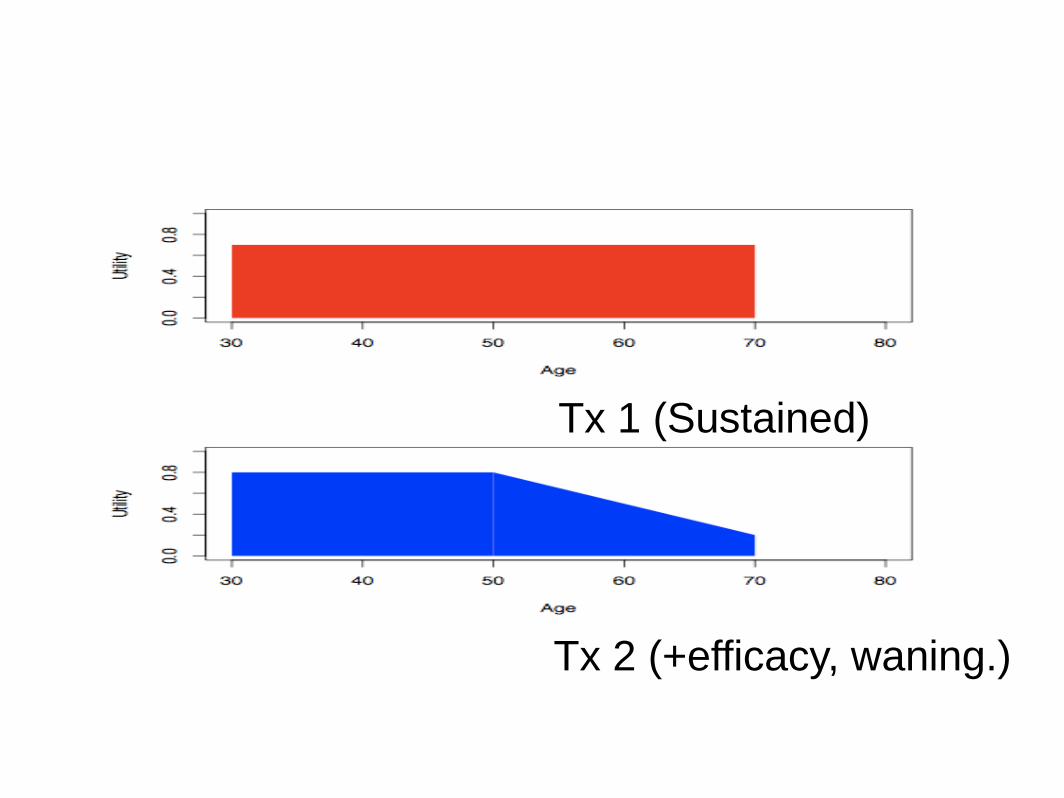
Tx 1 (Sustained)
Tx 2 (+efficacy, waning.)
Notes on the QALY
• In theory we can compare in an
equitable fashion across disease areas.
• This allows consideration of the impact
of interventions in a fair way and in a
univariate fashion.
• Thus a perfect ranking of interventions
can be obtained.
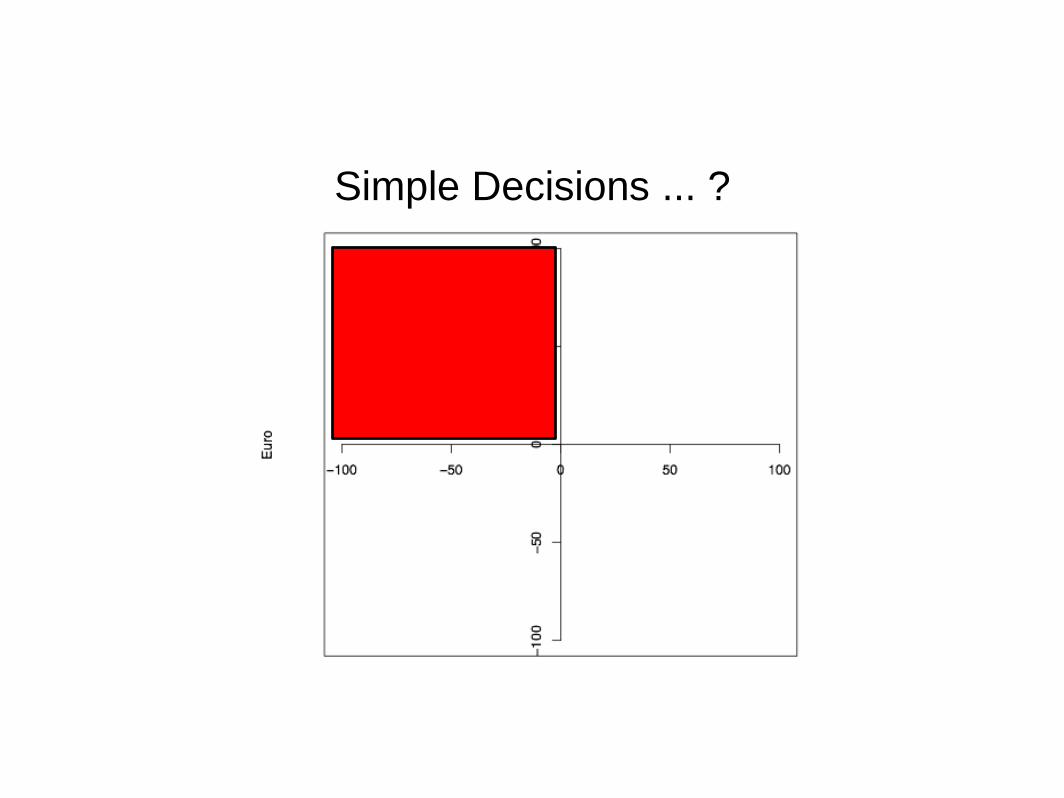
Decision Making - the C/E
plane
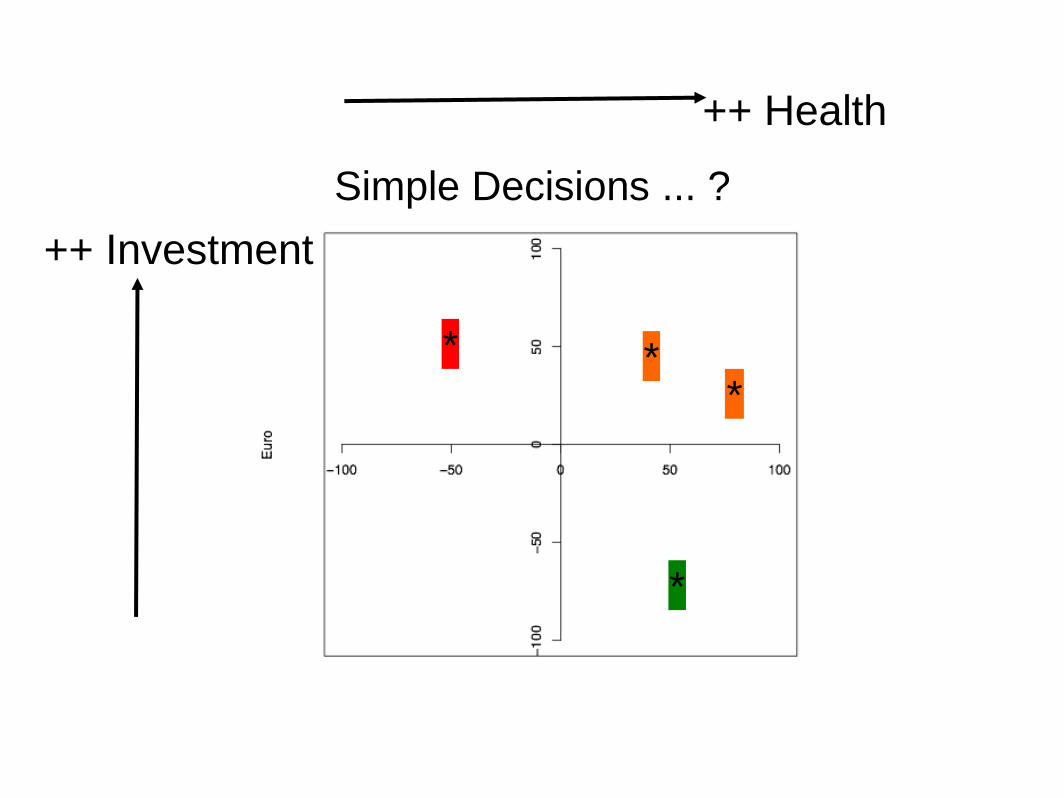
• The cost effectiveness plane is a core
aspect of how outcomes are
communicated and interpreted. It trades
off gains in health outcomes (on the x-
axis) and costs (on the y-axis).
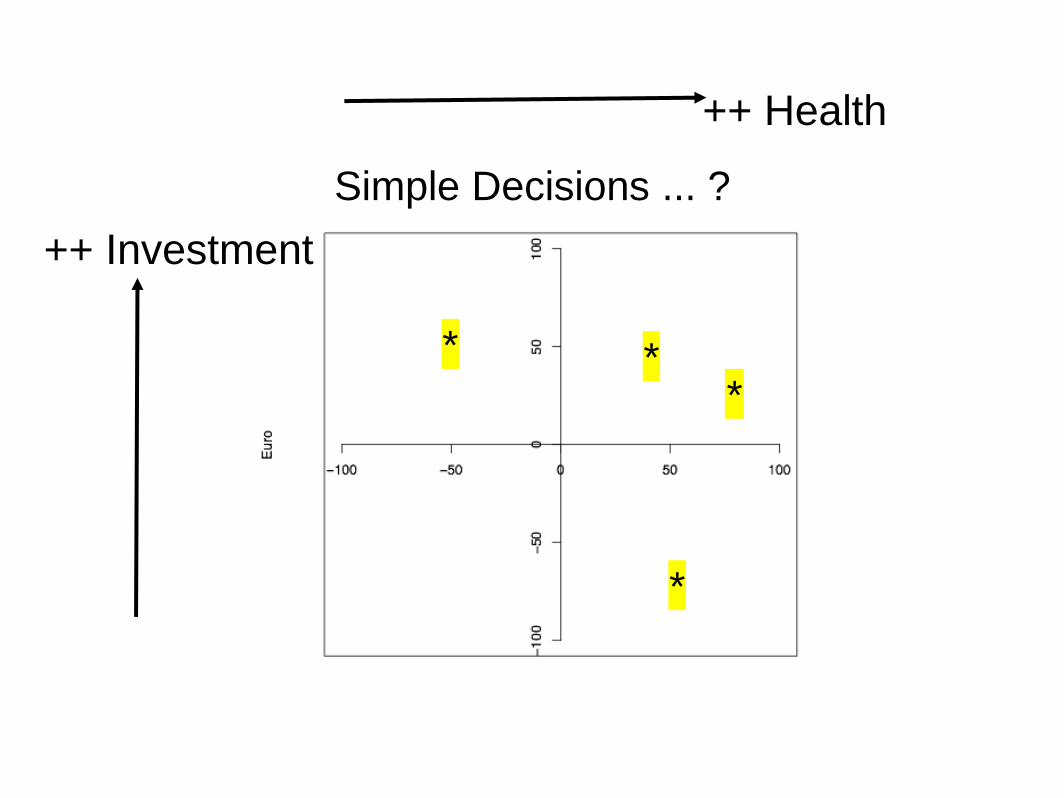
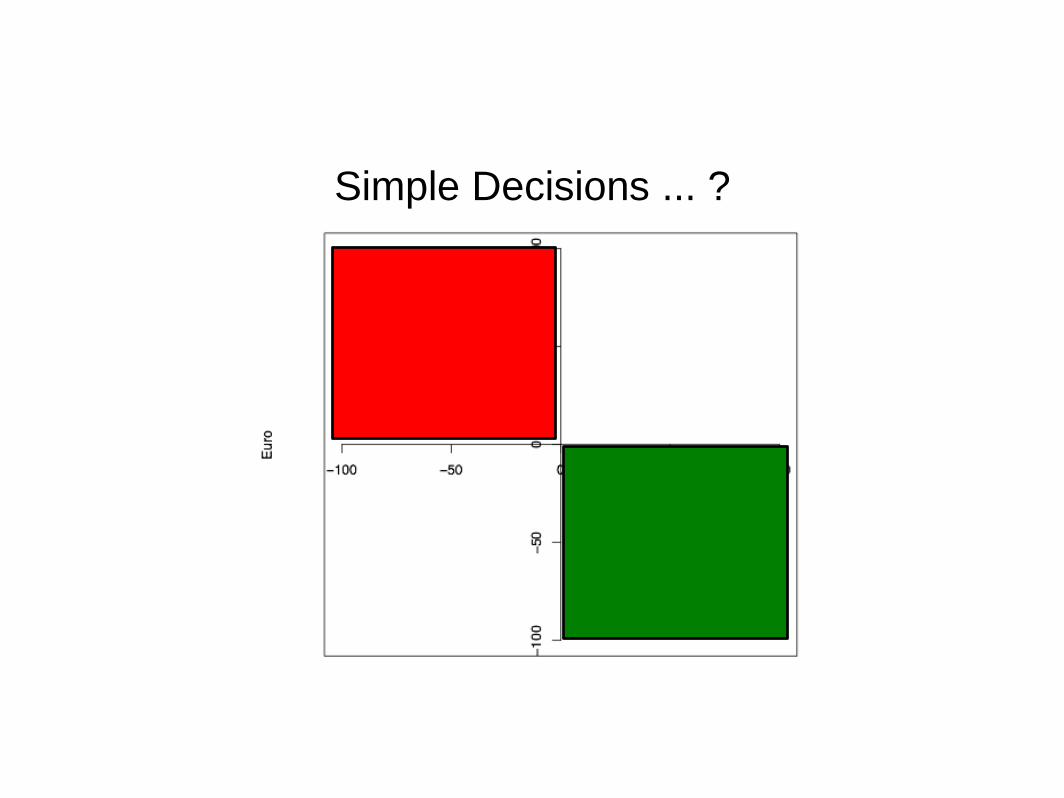
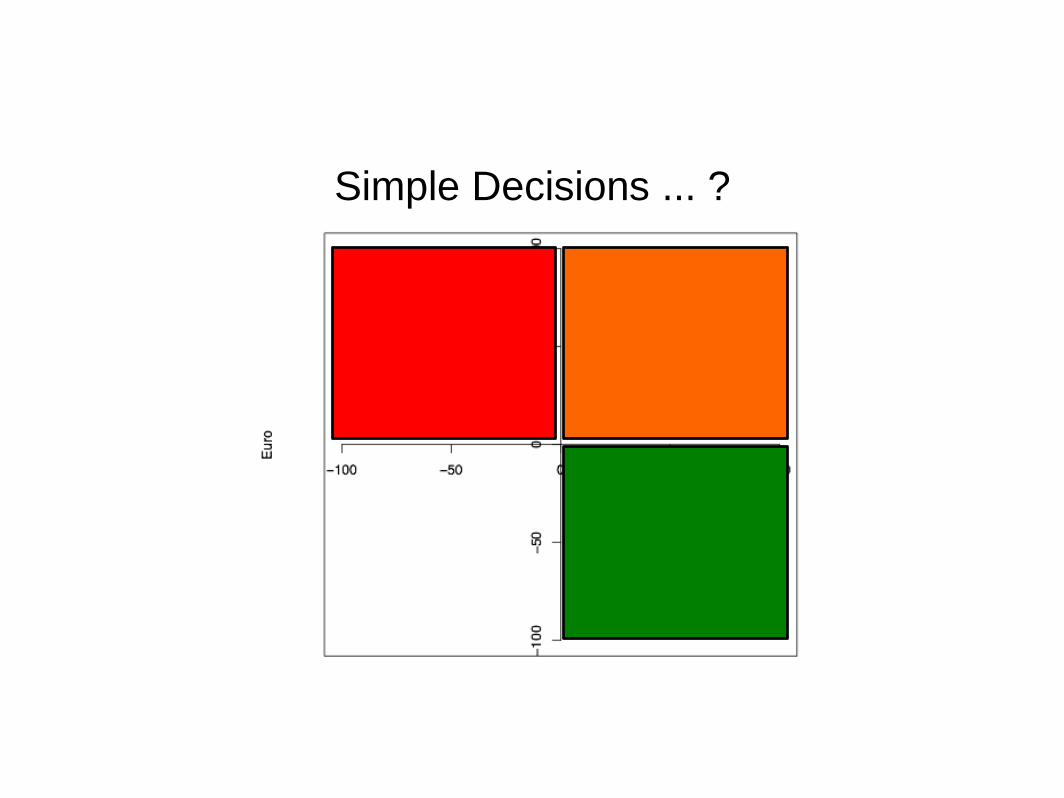
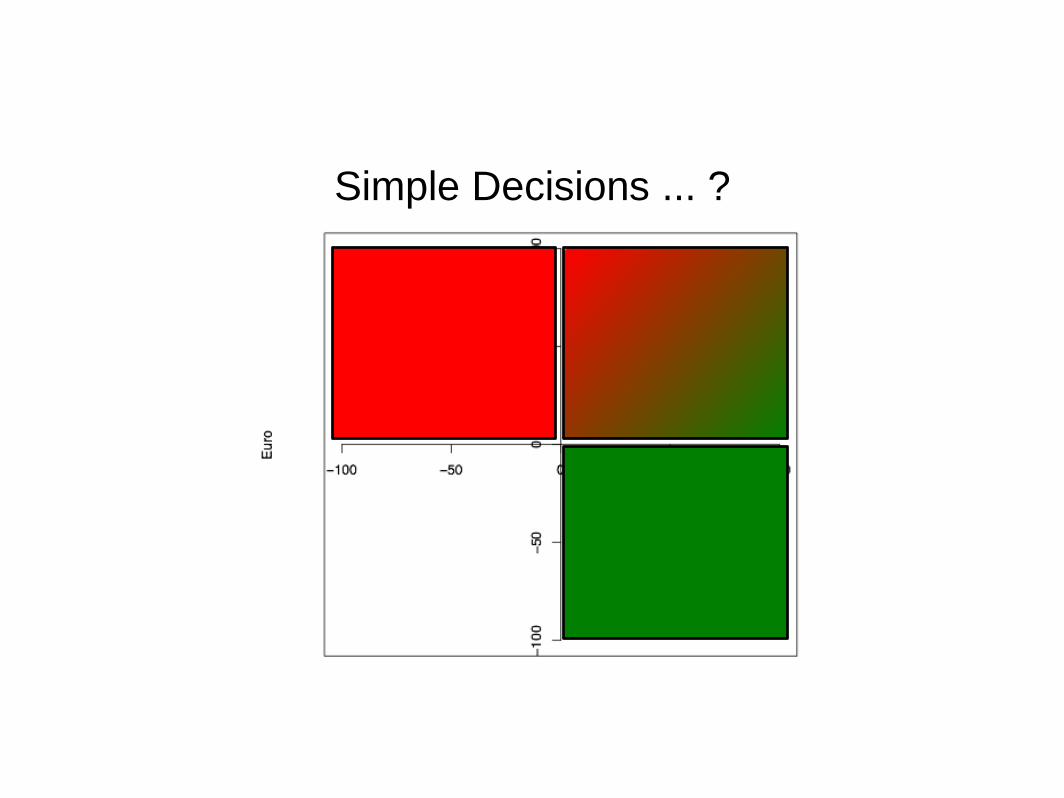
Simple Decisions ... ?
*
++ Health
++ Investment
***
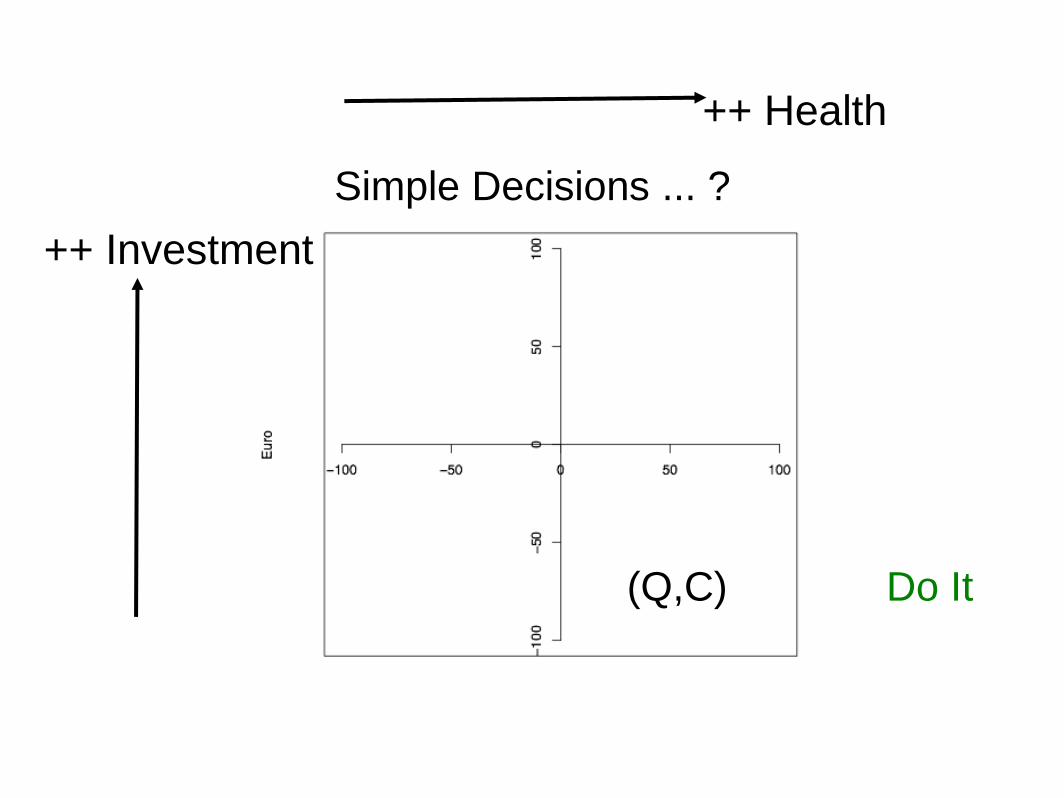
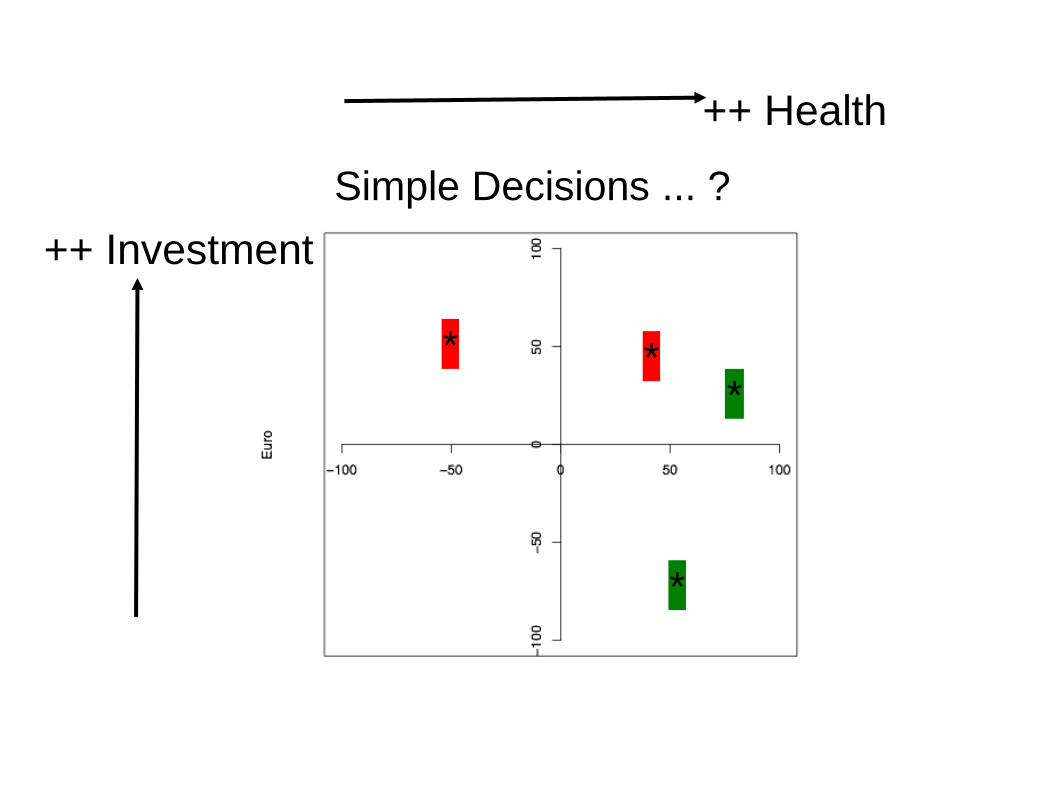
Simple Decisions ... ?
(Q,C) Do It
++ Health
++ Investment
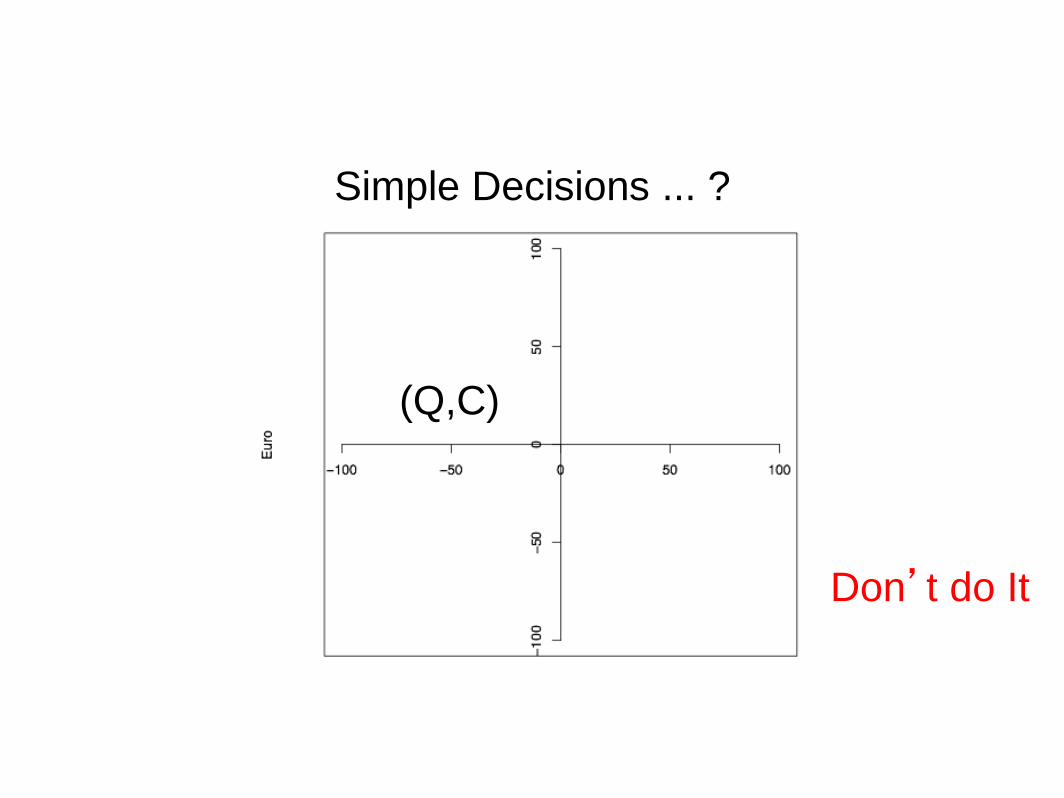
Simple Decisions ... ?
(Q,C)
Don’t do It
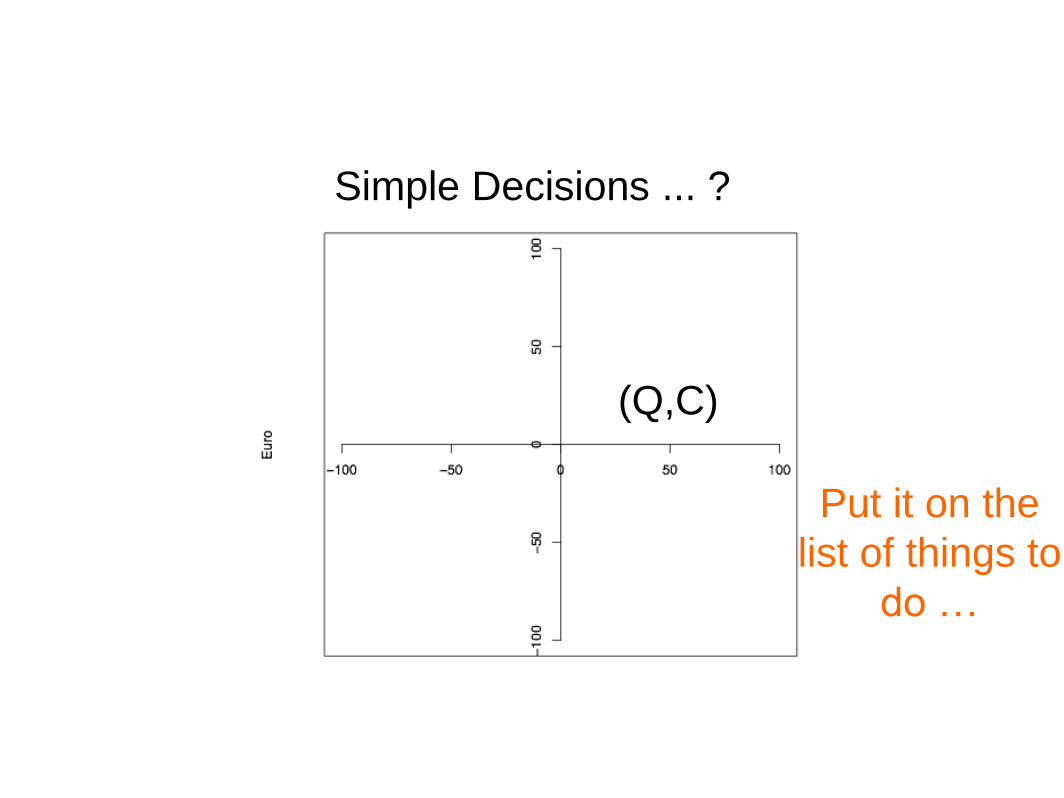
Simple Decisions ... ?
(Q,C)
Put it on the
list of things to
do …
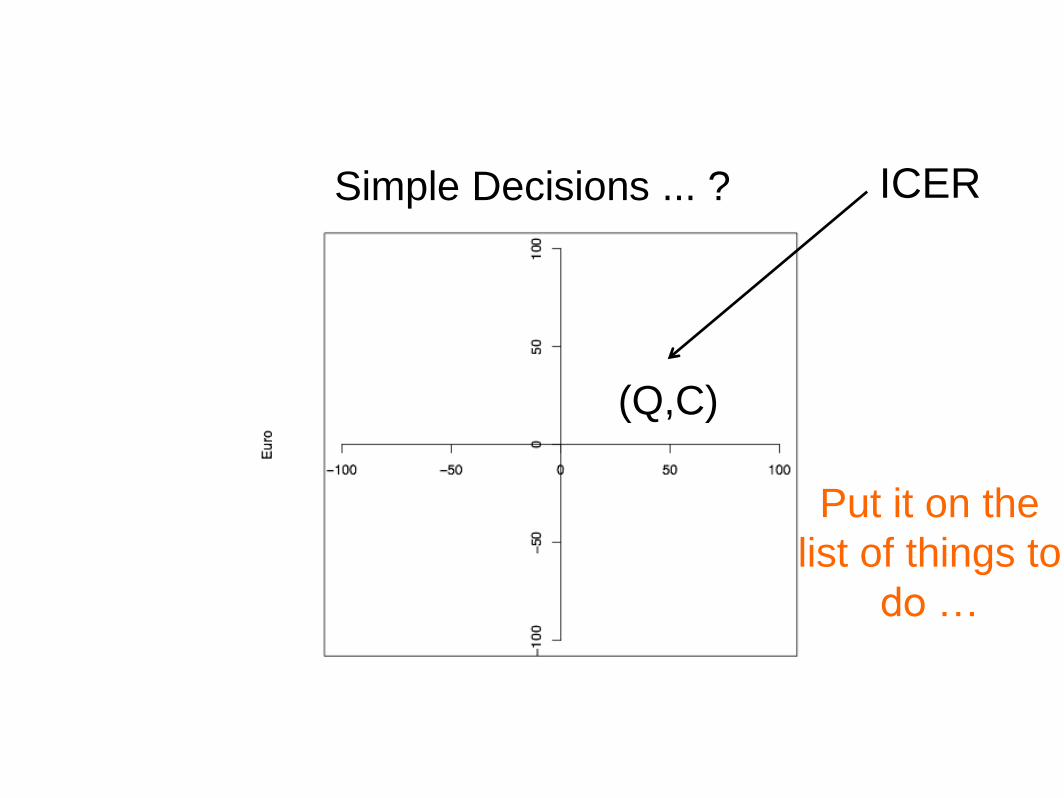
Simple Decisions ... ?
(Q,C)
Put it on the
list of things to
do …
ICER
Simple Decisions ... ?
Simple Decisions ... ?
Simple Decisions ... ?
Simple Decisions ... ?
Simple Decisions ... ?
*
++ Health
++ Investment
***
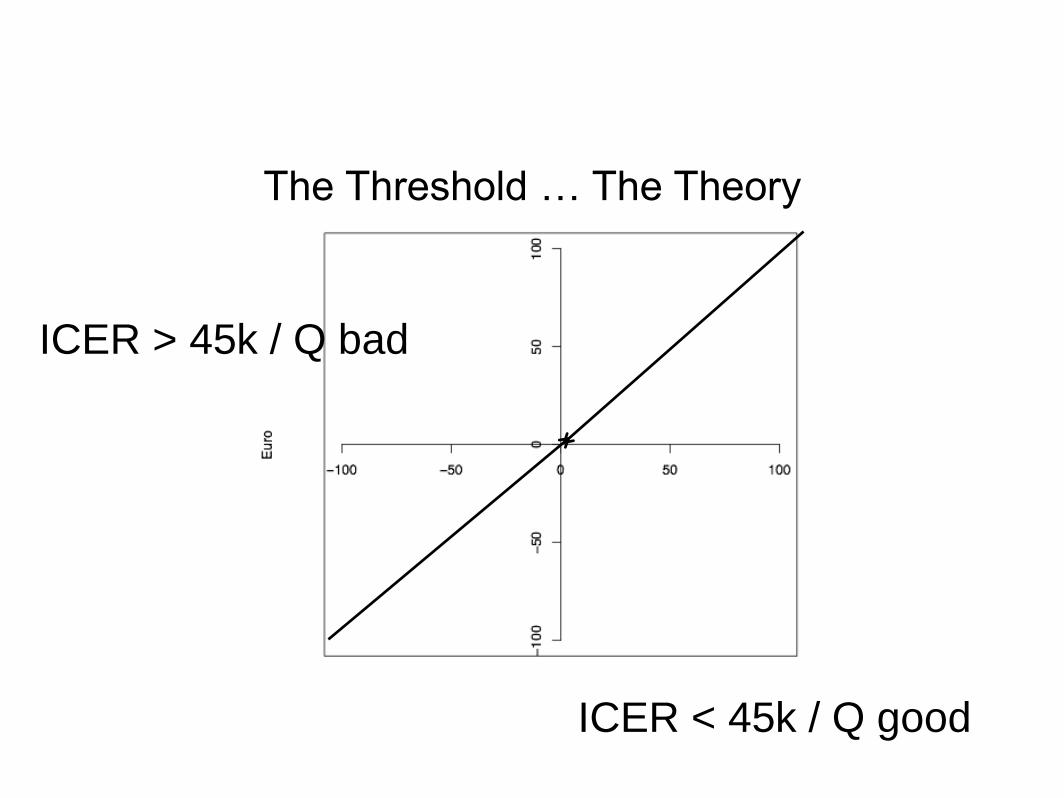
The Threshold … The Theory
ICER < 45k / Q good
ICER > 45k / Q bad
Simple Decisions ... ?
*
++ Health
++ Investment
***
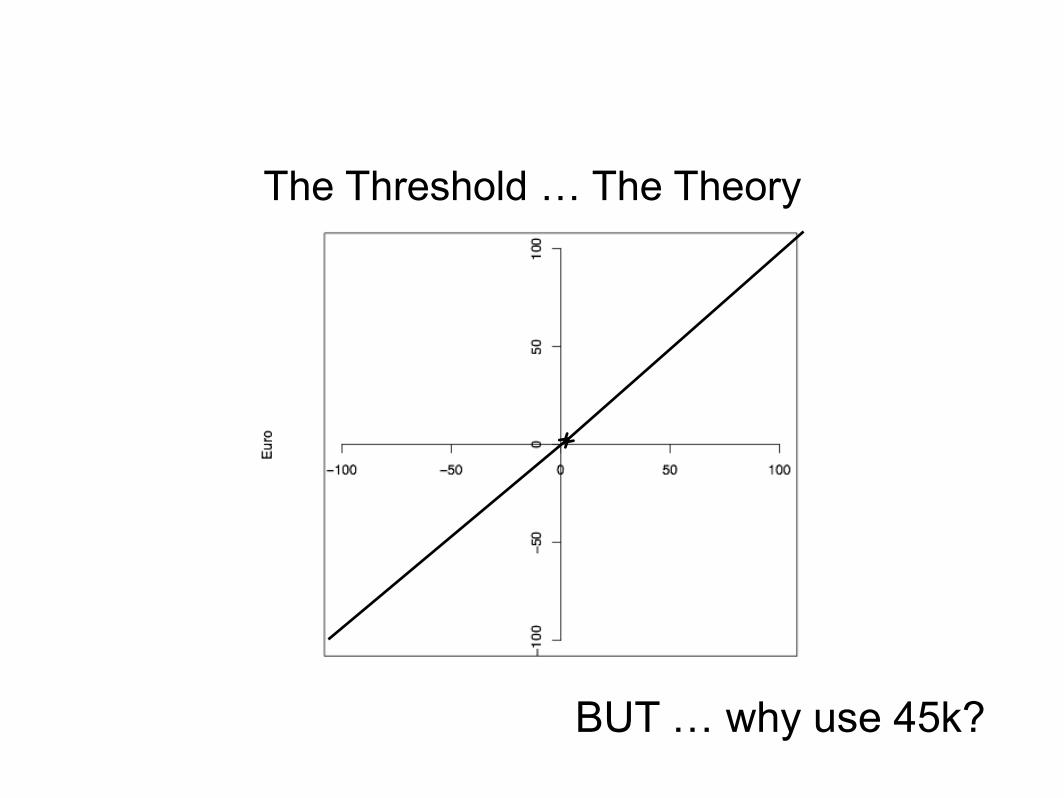
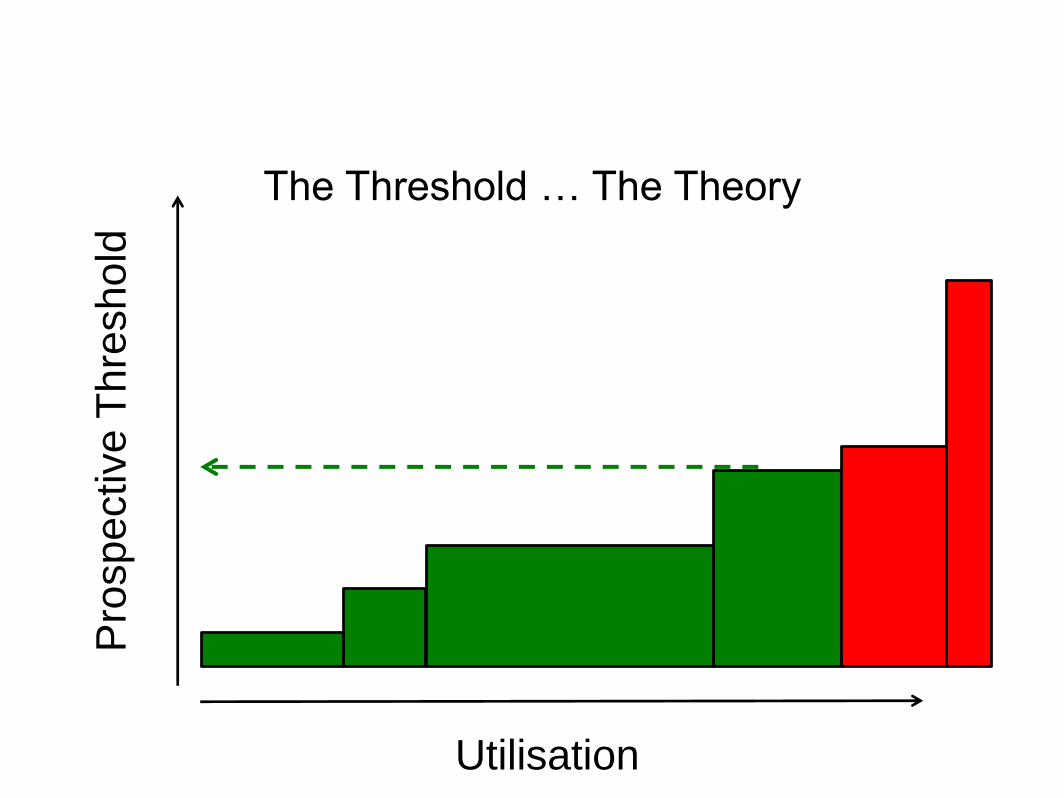
The Threshold … The Theory
BUT … why use 45k?
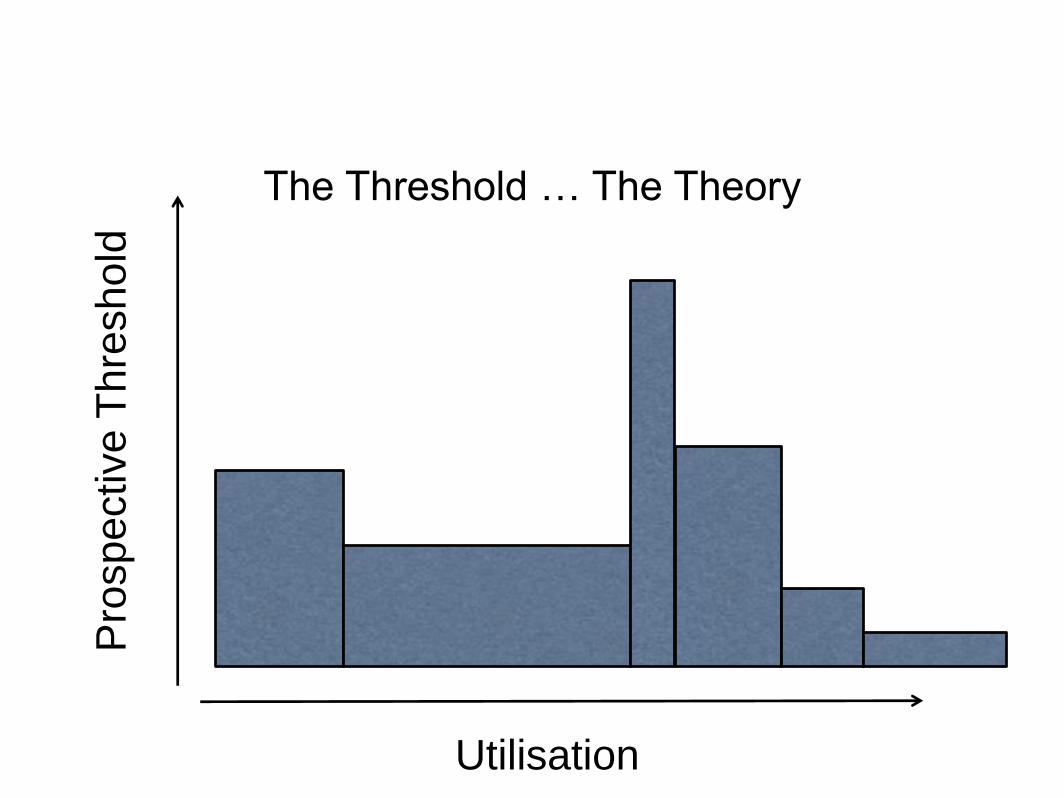
The Threshold … The Theory
Utilisation
Pro
sp
ective
Th
resh
old
The Threshold … The Theory
Utilisation
Pro
sp
ective
Th
resh
old
The Threshold … Estimation in Practice
• What is the cost per QALY of the things
we stop doing to afford the new things?
• What is the cost per QALY of the things
we should stop doing to afford the new
things?
• On average, what is the marginal cost
per QALY in our health system?
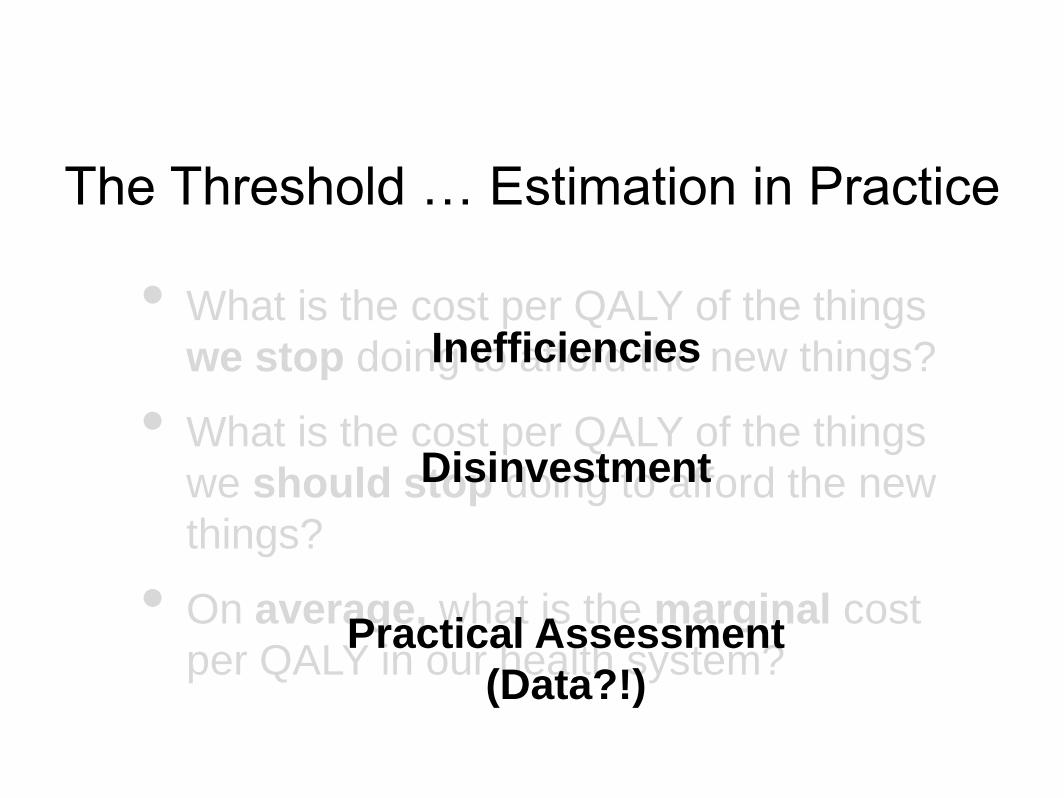
The Threshold … Estimation in Practice
• What is the cost per QALY of the things
we stop doing to afford the new things?
• What is the cost per QALY of the things
we should stop doing to afford the new
things?
• On average, what is the marginal cost
per QALY in our health system?
Inefficiencies
Disinvestment
Practical Assessment
(Data?!)
Other considerations
• The Value set we use.
• The Uncertainty associated with the
parameters.
• The comparators used in the models.
• Indications for treatment.
• Structural uncertainty in models.
• Societal vs healthcare payer perspective.
Workarounds (Fudges)
• QALY loadings.
• Disease specific threshold.
• Selective alternative perspectives.
• Ring fenced budgets for selected
conditions.
• Differential discounting.
• MCDA (perhaps?).
Multi Criteria Decision
Analysis
• Affects the Value side alone.
• Allows explicit incorporation of other
factors into the value function.
• Strictly speaking cost per QALY is a form
of MCDA.
• Cannot change the budget available –
just the ordering of the interventions we
fund.
What do we do now?
• An ‘informal’ MCDA approach.
• A 45,000 / QALY ‘initial’ threshold.
• Reimbursement occurs for some
interventions above this level.
• A process for broader consideration of
the decision exists.
Exercise
Related Documents











