MAY JOGC MAI 2012 l 443 GYNAECOLOGY Key Words: HPV testing, cervical cytology, cervical cancer screening, cancer prevention Competing Interests: See Acknowledgements Received on December 23, 2011 Accepted on February 8, 2012 HPV Testing in Primary Cervical Screening: A Systematic Review and Meta-Analysis Joan Murphy, MD, 1 Erin B. Kennedy, MHSc, 2 Sheila Dunn, MD, 3 C. Meg McLachlin, MD, 4 Michael Fung Kee Fung, MD, 5 Danusia Gzik, MD, 6 Michael Shier, MD, 7 Lawrence Paszat, MD 8 1 Division of Gynecologic Oncology, University Health Network, Toronto ON 2 Program in Evidence-based Care, Cancer Care Ontario and Department of Oncology, McMaster University, Hamilton ON 3 Family Practice Unit, Women’s College Hospital, Toronto ON 4 London Health Sciences Centre, London ON 5 Ottawa General Hospital, Ottawa ON 6 North Simcoe Muskoka Local Health Integration Network, Huntsville ON 7 Sunnybrook Health Sciences Centre, Toronto ON 8 Institute for Clinical Evaluative Sciences, Toronto ON J Obstet Gynaecol Can 2012;34(5):443–452 Abstract Objective: Previous findings from cross-sectional studies have shown human papillomavirus (HPV) testing to be more sensitive than cytology testing for primary cervical screening This systematic review aims to assess whether the increase in baseline detection with HPV testing corresponds to lower rates in subsequent screening rounds Methods: We searched Medline, EMBASE, and the Cochrane Library for randomized controlled trials (published from 2005 to 2010) comparing HPV-based and cytology-based cervical screening Primary outcomes of interest were relative rates of higher grade cervical intraepithelial neoplasia and invasive cervical cancer Secondary outcomes included test performance characteristics and colposcopy referral rates Results were pooled where possible using a random effects model Results: Seven randomized trials were identified Across studies, HPV testing was more accurate than conventional cytology and detected significantly more CIN3+ in the first screening round (Mantel-Haenszel [M-H] risk ratio 167; 95% CI 127 to 219) and significantly less in the second screening round (M-H RR 049; 95% CI 037 to 066) There were no differences in pooled rates of CIN2+ (M-H RR 119; 95% CI 094 to 150) and CIN3+ (M-H RR 109; 95% CI 084 to 142), but there was a higher pooled rate of CIN2 (M-H RR 137; 95% CI 112 to 168) over two screening rounds A trend towards lower rates of invasive cervical cancer was observed Conclusion: Organized screening programs in higher resource settings should consider adopting HPV testing as the primary screening test for women 30 or 35 years of age and older Further research is needed to determine optimal screening strategies for younger women Résumé Objectif : Les résultats issus d’études transversales menées précédemment ont démontré que le dépistage du virus du papillome humain (VPH) est plus sensible que le dépistage cytologique aux fins du dépistage cervical primaire Cette analyse systématique cherche à établir si la hausse de la détection de base que permet le dépistage du VPH se traduit en taux moindres dans le cadre des rondes de dépistage subséquentes Méthodes : Des recherches ont été menées dans Medline, EMBASE et la Cochrane Library afin d’en tirer les essais comparatifs randomisés (publiés entre 2005 et 2010) comparant le dépistage cervical fondé sur le VPH et le dépistage cervical fondé sur la cytologie Les critères d’évaluation principaux étaient les taux relatifs de néoplasie cervicale intra-épithéliale de haut grade histologique et de cancer du col utérin invasif Parmi les critères secondaires, on trouvait les caractéristiques du rendement des tests et les taux d’orientation en colposcopie Les résultats ont été groupés, dans la mesure du possible, au moyen d’un modèle à effets aléatoires Résultats : Sept essais randomisés ont été identifiés Dans le cadre de toutes ces études, le dépistage du VPH s’est avéré plus précis que la cytologie conventionnelle et a permis la détection d’un nombre considérablement supérieur de NCI3+ au cours de la première ronde de dépistage (risque relatif Mantel- Haenszel [M-H] 1,67; IC à 95 %, 1,27 - 2,19) et celle d’un nombre considérablement moindre au cours de la deuxième ronde de

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MAY JOGC MAI 2012 l 443
GYNAECOLOGY
Key Words: HPV testing, cervical cytology, cervical cancer screening, cancer prevention
Competing Interests: See Acknowledgements .
Received on December 23, 2011
Accepted on February 8, 2012
HPV Testing in Primary Cervical Screening: A Systematic Review and Meta-AnalysisJoan Murphy, MD,1 Erin B. Kennedy, MHSc,2 Sheila Dunn, MD,3 C. Meg McLachlin, MD,4 Michael Fung Kee Fung, MD,5 Danusia Gzik, MD,6 Michael Shier, MD,7 Lawrence Paszat, MD8
1Division of Gynecologic Oncology, University Health Network, Toronto ON2Program in Evidence-based Care, Cancer Care Ontario and Department of Oncology, McMaster University, Hamilton ON3Family Practice Unit, Women’s College Hospital, Toronto ON4London Health Sciences Centre, London ON5Ottawa General Hospital, Ottawa ON6North Simcoe Muskoka Local Health Integration Network, Huntsville ON7Sunnybrook Health Sciences Centre, Toronto ON8Institute for Clinical Evaluative Sciences, Toronto ON
J Obstet Gynaecol Can 2012;34(5):443–452
Abstract
Objective: Previous findings from cross-sectional studies have shown human papillomavirus (HPV) testing to be more sensitive than cytology testing for primary cervical screening . This systematic review aims to assess whether the increase in baseline detection with HPV testing corresponds to lower rates in subsequent screening rounds .
Methods: We searched Medline, EMBASE, and the Cochrane Library for randomized controlled trials (published from 2005 to 2010) comparing HPV-based and cytology-based cervical screening . Primary outcomes of interest were relative rates of higher grade cervical intraepithelial neoplasia and invasive cervical cancer . Secondary outcomes included test performance characteristics and colposcopy referral rates . Results were pooled where possible using a random effects model .
Results: Seven randomized trials were identified . Across studies, HPV testing was more accurate than conventional cytology and detected significantly more CIN3+ in the first screening round (Mantel-Haenszel [M-H] risk ratio 1 .67; 95% CI 1 .27 to 2 .19) and significantly less in the second screening round (M-H RR 0 .49; 95% CI 0 .37 to 0 .66) . There were no differences in pooled rates of CIN2+ (M-H RR 1 .19; 95% CI 0 .94 to 1 .50) and CIN3+ (M-H RR 1 .09; 95% CI 0 .84 to 1 .42), but there was a higher pooled rate of CIN2 (M-H RR 1 .37; 95% CI 1 .12 to 1 .68) over two screening rounds . A trend towards lower rates of invasive cervical cancer was observed .
Conclusion: Organized screening programs in higher resource settings should consider adopting HPV testing as the primary screening test for women 30 or 35 years of age and older . Further research is needed to determine optimal screening strategies for younger women .
Résumé
Objectif : Les résultats issus d’études transversales menées précédemment ont démontré que le dépistage du virus du papillome humain (VPH) est plus sensible que le dépistage cytologique aux fins du dépistage cervical primaire . Cette analyse systématique cherche à établir si la hausse de la détection de base que permet le dépistage du VPH se traduit en taux moindres dans le cadre des rondes de dépistage subséquentes .
Méthodes : Des recherches ont été menées dans Medline, EMBASE et la Cochrane Library afin d’en tirer les essais comparatifs randomisés (publiés entre 2005 et 2010) comparant le dépistage cervical fondé sur le VPH et le dépistage cervical fondé sur la cytologie . Les critères d’évaluation principaux étaient les taux relatifs de néoplasie cervicale intra-épithéliale de haut grade histologique et de cancer du col utérin invasif . Parmi les critères secondaires, on trouvait les caractéristiques du rendement des tests et les taux d’orientation en colposcopie . Les résultats ont été groupés, dans la mesure du possible, au moyen d’un modèle à effets aléatoires .
Résultats : Sept essais randomisés ont été identifiés . Dans le cadre de toutes ces études, le dépistage du VPH s’est avéré plus précis que la cytologie conventionnelle et a permis la détection d’un nombre considérablement supérieur de NCI3+ au cours de la première ronde de dépistage (risque relatif Mantel-Haenszel [M-H] 1,67; IC à 95 %, 1,27 - 2,19) et celle d’un nombre considérablement moindre au cours de la deuxième ronde de

444 l MAY JOGC MAI 2012
GyNAECOLOGy
dépistage (RR M-H, 0,49; IC à 95 %, 0,37 - 0,66) . Bien qu’aucune différence n’ait été constatée en matière de taux groupés de NCI2+ (RR M-H, 1,19; IC à 95 %, 0,94 - 1,50) et de NCI3+ (RR M-H, 1,09; IC à 95 %, 0,84 - 1,42), nous avons constaté un taux groupé accru de NCI2 (RR M-H, 1,37; IC à 95 %, 1,12 - 1,68) sur deux rondes de dépistage . Une tendance à la diminution des taux de cancer du col utérin invasif a été constatée .
Conclusion : Au sein des milieux disposant de ressources élevées, les programmes de dépistage organisés devraient envisager l’adoption du dépistage du VPH à titre de test de dépistage principal pour ce qui est des femmes de 30 ou de 35 ans ou plus . La tenue d’autres recherches s’avère requise pour déterminer les stratégies de dépistage optimales pour ce qui est des jeunes femmes .
INTRODUCTION
The purpose of cervical screening is to reduce the risk of cervical cancer through the detection of lesions
that have the potential to become invasive cervical cancer. A secondary aim is to reduce the risk of advanced cancer through the detection of asymptomatic or early-stage cancer.1 To date in Canada, screening programs have used either the traditional Papanicolaou smear test, or more recently, liquid-based cytology as the primary method for cervical screening. Cytology testing has largely been responsible for the dramatic decline in cervical cancer over the past several decades in developed countries; however, there were still an estimated 1300 new cases and 350 deaths from the disease in Canada in 2011,2 and, as in many other jurisdictions, the decline has plateaued. Furthermore, in many cases the diagnosis of cervical cancer was preceded by normal cytology screening. Lack of progress in reducing the incidence of cervical cancer and the introduction of new technologies has spurred interest in alternatives to traditional cytology-based screening.
HPV DNA is present in 99.7% of cases of cervical squamous carcinomas.3 HPV infection is very common, especially in younger age groups,4 and is often transient in that demographic. Persistent HPV infection can cause cervical intraepithelial neoplasia, which can develop into invasive cervical cancer over time. Testing for HPV requires detecting HPV DNA within cervical cells, as the immunologic response to HPV is insufficient to allow informative serum antibody assays. In Canada, HPV
testing can be used as an adjunct to Papanicolaou smear testing in certain circumstances, such as for triage of ASCUS in women over age 30, and in most provinces it is not an insured service. Recently, HPV testing as a primary screening test has been investigated as a possible way to improve the performance of cervical screening programs.
For HPV testing to be considered for adoption by organized cervical screening programs, it should have
1. greater sensitivity than cytology for detecting existing high-grade cervical lesions;
2. reduced rates of high-grade lesions in subsequent screening rounds, because of detection and treatment of lesions that would have persisted in the absence of HPV testing; and
3. demonstrated safety of extended screening intervals for HPV-negative patients.5
A review of 21 studies found that the sensitivity of a single Hybrid Capture II HPV test (Qiagen, Hilden, Germany) was 33% higher than cytology for CIN grade 2 or more severe disease (CIN2+), thus meeting the first criterion. Specificity, however, was 6% lower.6 Results from several randomized controlled trials of HPV testing as a primary screening test have now been published.7–13 This review uses relative detection rates of potential cancer precursors from these studies to explore whether the increased sensitivity with HPV testing is a result of over-detection of abnormalities that would regress with time, or if it represents a lead-time gain (i.e., an increase in detection of persistent disease). This systematic review was developed as a collaborative effort between the Cancer Care Ontario Prevention and Cancer Control Program and the Cancer Care Ontario Program in Evidence-Based Care.
METHODS
Literature SearchWe conducted a systematic search of the electronic databases Medline and EMBASE for English language articles (published from 2005 to November 2010) using the following text words and medical subject headings (MeSH): “cervix,” “cervical,” “cancer,” “carcinoma,” “screening,” and “mass screening” (as an exploded MeSH term). Search terms related to study design and publication type included “clinical trial” (text word and publication type), “clinical trials” (as an exploded MeSH term), “meta-analysis” (text word and publication type), and “systematic review.” The full search strategy is given in online eAppendix 1. Reference lists of papers and review articles were scanned for additional citations. Cochrane Library was searched for topic-specific reviews published from 2005 to 2010. The Current Controlled Trials registry
ABBREVIATIONSASCUS atypical squamous cells of undetermined significance
CIN cervical intraepithelial neoplasia
M-H Mantel-Haenszel
NPV negative predictive value
QUADAS Quality Assessment of Diagnostic Studies
RDR relative detection rate

MAY JOGC MAI 2012 l 445
HPV Testing in Primary Cervical Screening: A Systematic Review and Meta-Analysis
and ClinicalTrials.gov were searched in December 2010 for the most recently published results from registered RCTs in any language.
Study SelectionOur primary outcomes of interest were relative rates of CIN2, CIN2+, CIN3+, and incidence of and mortality due to invasive cervical cancer. For assessment of these outcomes, studies were included if they contained a randomized comparison of cytology-based testing and HPV-based testing with data for two or more screening rounds in the setting of an organized screening program. Secondary outcomes were the colposcopy rates associated with various intervention strategies and the test performance characteristics sensitivity, specificity, negative predictive value, and positive predictive value. Studies were selected for an analysis of test performance if they had submitted all participants or a random sample with negative test results to the same verification test as those who tested positive during initial screening. Any randomized controlled trial comparing cytology-based testing and HPV-based testing was eligible for the comparison of colposcopy rates.
Data Extraction and Quality AssessmentRelative detection rates of CIN2, CIN2+ and CIN3+ were extracted or calculated from available data using the most recently published trial results. RDRs were calculated as the CIN rate in the HPV testing (intervention) group divided by the CIN rate in the cytology (control subjects) group; thus, a rate of detection that was higher in the intervention group for a screening round resulted in an RDR greater than one. The endpoints of invasive cervical cancer incidence and mortality and colposcopy referrals were also extracted where available. Data extraction was verified by a project research assistant. All authors reviewed and discussed a draft of the evidence summary.
Randomized controlled trials identified in the literature search that met the inclusion criteria were assessed for key methodological characteristics. The risk of bias in the included trials was assessed using the following criteria: randomization method, blinding of outcome assessment, intention to treat analysis, withdrawals, funding source, statistical power calculations, length of follow-up, and balance of baseline characteristics. For studies that were included in the analysis of test performance characteristics, additional quality assessment items from the QUADAS tool were evaluated.14 The quality of the evidence base was assessed qualitatively by the authors, without the use of a scoring system or cut-offs, according to the policy of the Program in Evidence-Based Care.
Statistical AnalysisResults from each of two screening rounds and both screening rounds combined for RCTs that assessed rates of
CIN over more than one screening round were pooled using Review Manager software (RevMan version 5.1.4, Cochrane Collaboration). A Mantel-Haenszel random effects model was used for all pooling. A random effects model was chosen because it requires the underlying assumption that different studies estimate different, yet related, intervention effects.15 A probability level for the chi-square statistic of ≤ 10% (P ≤ 0.10) and/or an I2 of greater than 50% were considered indicative of statistical heterogeneity between studies. Results of pooling analyses are expressed as risk ratios with 95% confidence intervals. Analyses were conducted separately for CIN2, CIN2+, and CIN3+.
RESULTS
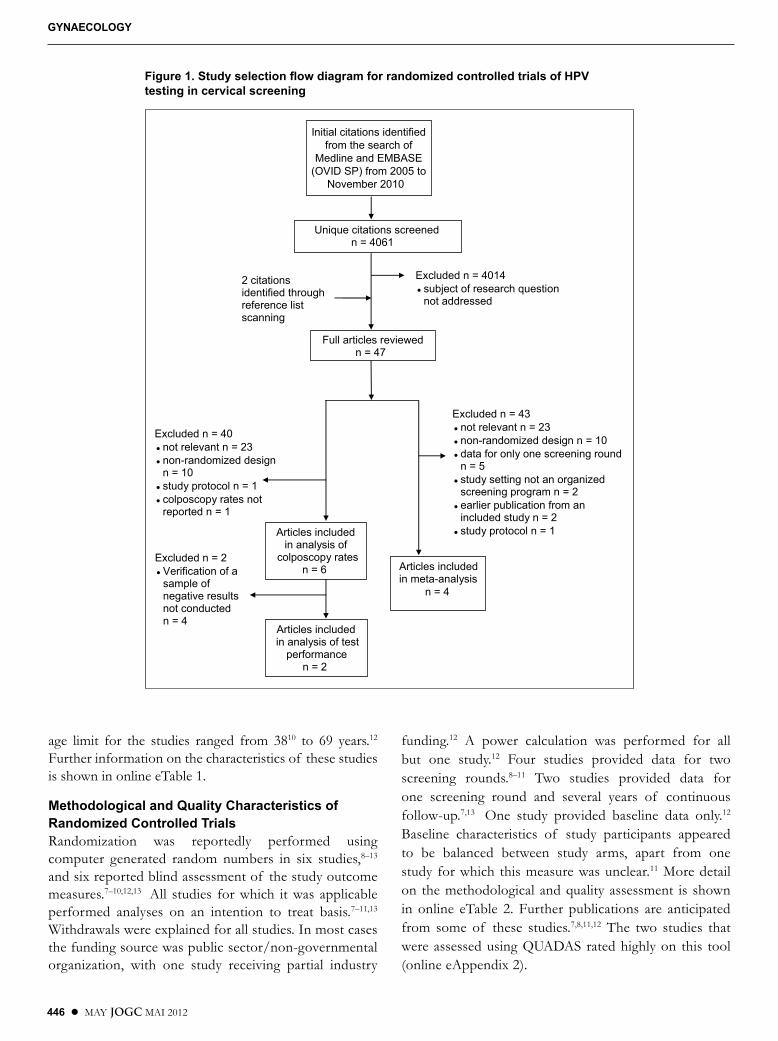
Four thousand sixty-one potentially relevant unique citations were identified through the systematic review (Figure 1). Seven RCTs7–13 that compared HPV testing to cytology testing in primary cervical screening were identified. Four RCTs provided data for more than one screening round in an organized setting and thus were included in the meta-analysis of rates of CIN2, CIN2+, and CIN3+. Six studies reported colposcopy rates with various screening strategies. Because of significant heterogeneity in protocols for referral to colposcopy, a meta-analysis was not performed for this outcome. Two trials had sufficient statistical power to analyze the effect of differences between groups for the outcomes of cervical cancer incidence and mortality. Because of the small numbers of trials that reported this outcome, a meta-analysis for this indicator was not performed. No randomized controlled trials with publications in languages other than English were identified through the search of clinical trials registries.
The majority of RCTs were based in countries that have established, organized screening programs.7–11 A Canadian study included women who sought screening under an opportunistic model.12 Sankaranarayanan et al. studied outcomes with a one-time screening of a population that did not previously have access to screening.13 All studies used conventional cytology testing in the control group, with the exception of one study that used liquid-based cytology11 and one that used standard care.13 The intervention group consisted of screening with HPV testing with the Hybrid Capture II test (Qiagen, Hilden, Germany), or a polymerase chain reaction-based test,9,10
with or without cytology testing. The follow-up times ranged from just over two years11 to eight years.13 Of the seven studies, four included women 29 years of age and older,9,10,12,13 two included women 25 and older,7,8 and one included women from 20 years of age.11 The upper
446 l MAY JOGC MAI 2012
GyNAECOLOGy
Initial citations identifiedfrom the search of
Medline and EMBASE(OVID SP) from 2005 to
November 2010
Unique citations screenedn = 4061
Articles included in meta-analysis
n = 4
Excluded n = 4014● subject of research question
not addressed
Excluded n = 43● not relevant n = 23● non-randomized design n = 10● data for only one screening round
n = 5 ● study setting not an organized
screening program n = 2● earlier publication from an
included study n = 2● study protocol n = 1
Full articles reviewedn = 47
2 citations identified through reference list scanning
Articles included in analysis of
colposcopy ratesn = 6
Excluded n = 40● not relevant n = 23● non-randomized design
n = 10● study protocol n = 1● colposcopy rates not
reported n = 1
Articles included in analysis of test
performancen = 2
Excluded n = 2● Verification of a
sample of negative results not conducted n = 4
Figure 1. Study selection flow diagram for randomized controlled trials of HPV testing in cervical screening
age limit for the studies ranged from 3810 to 69 years.12 Further information on the characteristics of these studies is shown in online eTable 1.
Methodological and Quality Characteristics of Randomized Controlled TrialsRandomization was reportedly performed using computer generated random numbers in six studies,8–13 and six reported blind assessment of the study outcome measures.7–10,12,13 All studies for which it was applicable performed analyses on an intention to treat basis.7–11,13 Withdrawals were explained for all studies. In most cases the funding source was public sector/non-governmental organization, with one study receiving partial industry
funding.12 A power calculation was performed for all but one study.12 Four studies provided data for two screening rounds.8–11 Two studies provided data for one screening round and several years of continuous follow-up.7,13 One study provided baseline data only.12 Baseline characteristics of study participants appeared to be balanced between study arms, apart from one study for which this measure was unclear.11 More detail on the methodological and quality assessment is shown in online eTable 2. Further publications are anticipated from some of these studies.7,8,11,12 The two studies that were assessed using QUADAS rated highly on this tool (online eAppendix 2).

MAY JOGC MAI 2012 l 447
HPV Testing in Primary Cervical Screening: A Systematic Review and Meta-Analysis
Test PerformanceTest performance characteristics are shown in online eTable 3. Only two studies performed verification of disease status for a random sample of patients whose initial screening tests were negative.12,16 In both studies, higher sensitivity and slightly lower specificity were found with HPV testing compared with conventional cytology testing for CIN2+, and CIN3+. In the HPV group, Swedescreen found a significantly higher NPV for CIN2+, and a non-significantly higher NPV for CIN3+.16 The Canadian Cervical Cancer Screening Trial found that the NPV was higher for CIN2+ with HPV screening, although this difference was not statistically significant.12
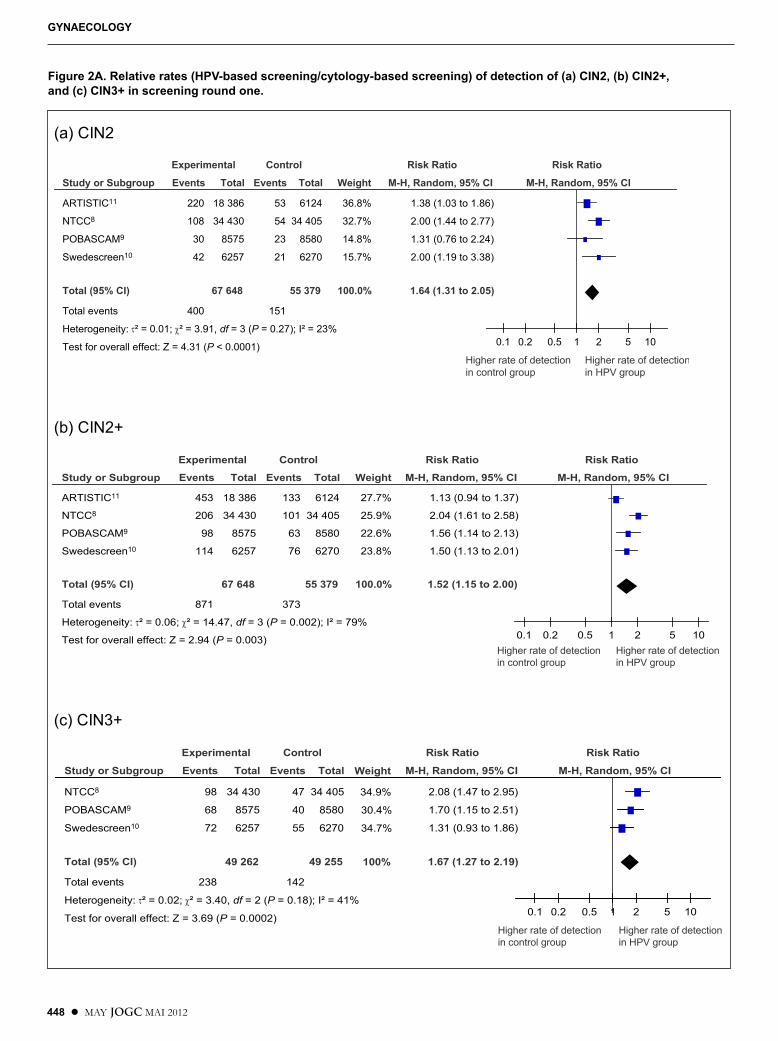
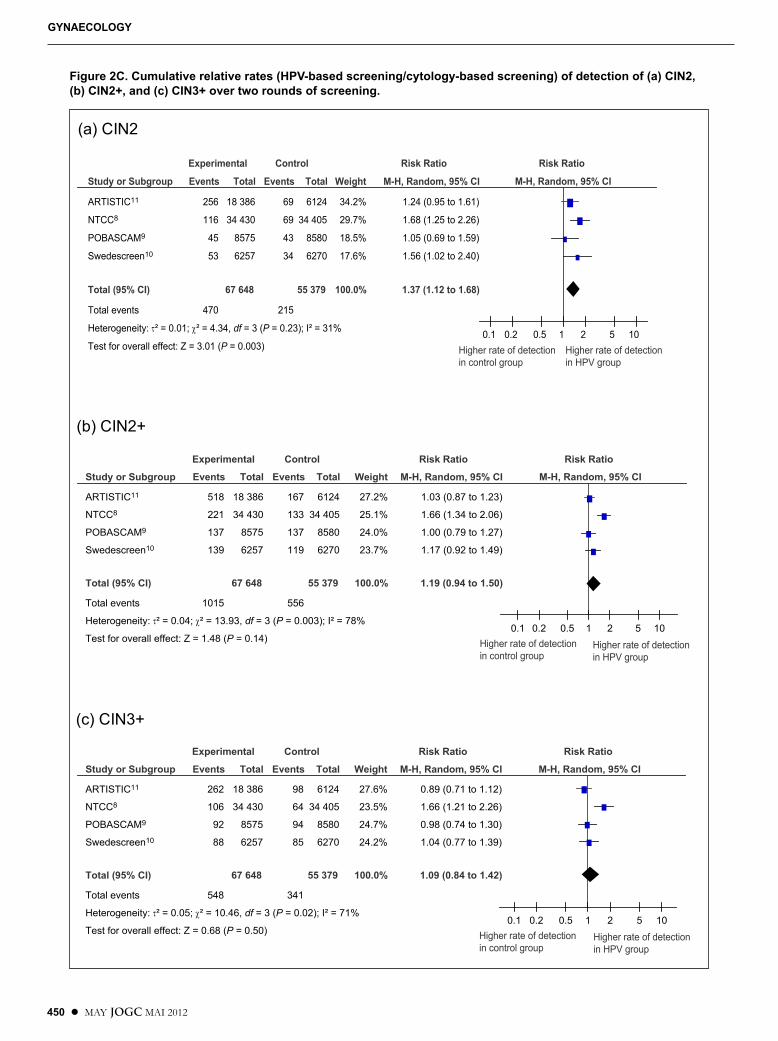
Relative Detection Rates for CINMeta-analysis results are presented in Figure 2A–C. Significant statistical heterogeneity was found between studies for the assessment of CIN2+ (I2 = 79%) and CIN3+ (I2 = 79%) in the first screening round and of CIN2+ (I2 = 78%) and CIN3+ (I2 = 71%) over both screening rounds. One study found significantly more cases in the HPV-based testing group over two rounds, which was possibly due to a protocol for HPV-positive test results that led to the detection of more potentially regressive lesions.8 The exclusion of this study resulted in the reduction of the I2 value to 0 for all analyses, but the estimate of the effect was unchanged. Therefore, this study was not excluded from the analysis. Likewise, as the meta-analysis of relative rates of CIN2+ in round 1 was unaffected by the removal of a specific study11 that was largely responsible for the high estimate of heterogeneity, the original estimate, with all studies included, was used in the final analysis. The source of heterogeneity in the analysis of CIN3+ in screening round 1 was removed because it significantly affected the summary estimate.
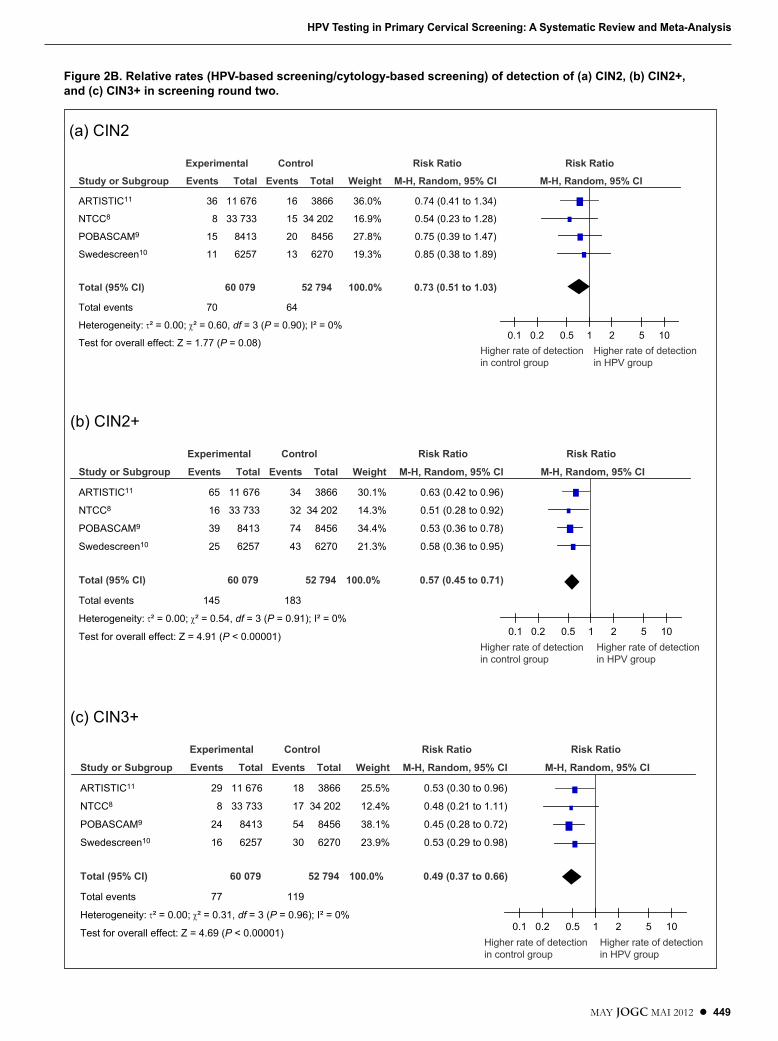
Overall, significantly more cases of CIN2, CIN2+, and CIN3+ were detected in the first round of screening in the HPV-based testing group (Figure 2A–C). Fewer cases of CIN2+ and CIN3+ were detected in the HPV-based testing group in the second screening round, but not CIN2. Over both rounds there was no difference in the rates of CIN2+ (RDR = 1.19; 95% CI 0.94 to 1.50) and CIN3+ (RDR = 1.09; 95% CI 0.84 to 1.42) between the HPV testing group and the cytology testing group. Over both rounds, significantly more CIN2 (RDR = 1.37; 95% CI 1.12 to 1.68) was detected in the HPV testing group.
Additional results from the NTCC trial (data not shown in Figure 2A-C) indicate that for the 25 to 34 age group, detection of CIN2 was more than four times higher (RDR = 4.54; 95% CI 3.00 to 6.88) for the intervention group (i.e., comparing co-testing to cytology testing
alone), and CIN2+ detection was over three times higher (RDR = 3.03; 95% CI 2.28 to 4.03). Overall detection over both rounds was significantly higher in the HPV-based group, with RDRs of 3.11 (95% CI 2.20 to 4.39) and 2.21 (95% CI 1.73 to 2.81), respectively.
Cervical Cancer Incidence and MortalityOnly two trials had enough statistical power to assess the relatively infrequent outcomes of cervical cancer incidence and mortality.8,13
In the New Technologies in Cervical Cancer trial there were no cases of invasive cervical cancer in the second round in the HPV group, versus nine cases in the cytology group (P = 0.004), with the proportion of adenocarcinomas in this group being approximately four times the national average in Italy. The number of cases of invasive cervical cancer was significantly lower (P = 0.028) over both study rounds in the HPV group.8
Sankaranarayanan et al.13 reported a hazard ratio for the incidence of stage II+ cervical cancer with HPV testing compared with standard care of 0.47 (95% CI 0.32 to 0.69), while the hazard ratio for cytology testing compared to standard care was 0.75 (95% CI 0.51 to 1.10). The study found a reduction in mortality from invasive cervical cancer with a single HPV test (HR 0.52; 95% CI 0.33 to 0.83) but no reduction with a single screening with cytology or visual inspection with acetic acid.
Colposcopy Referral RatesColposcopy rates were generally higher with HPV testing at baseline screening and among younger women, reflecting higher detection rates among these groups (online eTable 4). The variety of different management strategies resulted in referral rates ranging from 1.1% for women aged 30 to 69 who underwent primary HPV testing (referral threshold of 1 pg/mL) with cytology triage of positive results (referral threshold of ASCUS),12 to 13.0% for women aged 25 to 34 who were directly referred to colposcopy after a positive HPV test (referral threshold of 1 pg/mL).17
DISCUSSION
Previously published studies have established the higher accuracy of HPV testing for detecting precancerous cervical lesions.18 In this systematic review, relative detection rates over more than one screening round in several randomized trials are used to explore whether higher sensitivity translates to a reduction in cervical cancer precursors and invasive cervical cancer over time.
This study included a meta-analysis of trials with results reported for more than one round of screening. A
448 l MAY JOGC MAI 2012
GyNAECOLOGy
(a) CIN2
Study or Subgroup
ARTISTIC11
NTCC8
POBASCAM9
Swedescreen10
Total (95% CI)
Total events
Heterogeneity: τ² = 0.01; χ² = 3.91, df = 3 (P = 0.27); I² = 23%
Test for overall effect: Z = 4.31 (P < 0.0001)
Events
220
108
30
42
400
Total
18 386
34 430
8575
6257
67 648
Events
53
54
23
21
151
Total
6124
34 405
8580
6270
55 379
Weight
36.8%
32.7%
14.8%
15.7%
100.0%
M-H, Random, 95% CI
1.38 (1.03 to 1.86)
2.00 (1.44 to 2.77)
1.31 (0.76 to 2.24)
2.00 (1.19 to 3.38)
1.64 (1.31 to 2.05)
Experimental Control Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.1 0.2 0.5 1 2 5 10
Higher rate of detection in control group
Higher rate of detectionin HPV group
(b) CIN2+
Study or Subgroup
ARTISTIC11
NTCC8
POBASCAM9
Swedescreen10
Total (95% CI)
Total events
Heterogeneity: τ² = 0.06; χ² = 14.47, df = 3 (P = 0.002); I² = 79%
Test for overall effect: Z = 2.94 (P = 0.003)
Events
453
206
98
114
871
Total
18 386
34 430
8575
6257
67 648
Events
133
101
63
76
373
Total
6124
34 405
8580
6270
55 379
Weight
27.7%
25.9%
22.6%
23.8%
100.0%
M-H, Random, 95% CI
1.13 (0.94 to 1.37)
2.04 (1.61 to 2.58)
1.56 (1.14 to 2.13)
1.50 (1.13 to 2.01)
1.52 (1.15 to 2.00)
Experimental Control Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.1 0.2 0.5 1 2 5 10Higher rate of detection in control group
Higher rate of detectionin HPV group
(c) CIN3+
Study or Subgroup
NTCC8
POBASCAM9
Swedescreen10
Total (95% CI)
Total events
Heterogeneity: τ² = 0.02; χ² = 3.40, df = 2 (P = 0.18); I² = 41%
Test for overall effect: Z = 3.69 (P = 0.0002)
Events
98
68
72
238
Total
34 430
8575
6257
49 262
Events
47
40
55
142
Total
34 405
8580
6270
49 255
M-H, Random, 95% CI
2.08 (1.47 to 2.95)
1.70 (1.15 to 2.51)
1.31 (0.93 to 1.86)
1.67 (1.27 to 2.19)
Experimental Control Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.1 0.2 0.5 1 2 5 10
Higher rate of detection in control group
Higher rate of detectionin HPV group
Weight
34.9%
30.4%
34.7%
100%
Figure 2A. Relative rates (HPV-based screening/cytology-based screening) of detection of (a) CIN2, (b) CIN2+, and (c) CIN3+ in screening round one.
MAY JOGC MAI 2012 l 449
HPV Testing in Primary Cervical Screening: A Systematic Review and Meta-Analysis
(a) CIN2
Study or Subgroup
ARTISTIC11
NTCC8
POBASCAM9
Swedescreen10
Total (95% CI)
Total events
Heterogeneity: τ² = 0.00; χ² = 0.60, df = 3 (P = 0.90); I² = 0%
Test for overall effect: Z = 1.77 (P = 0.08)
Events
36
8
15
11
70
Total
11 676
33 733
8413
6257
60 079
Events
16
15
20
13
64
Total
3866
34 202
8456
6270
52 794
Weight
36.0%
16.9%
27.8%
19.3%
100.0%
M-H, Random, 95% CI
0.74 (0.41 to 1.34)
0.54 (0.23 to 1.28)
0.75 (0.39 to 1.47)
0.85 (0.38 to 1.89)
0.73 (0.51 to 1.03)
Experimental Control Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.1 0.2 0.5 1 2 5 10Higher rate of detectionin control group
Higher rate of detectionin HPV group
(b) CIN2+
Study or Subgroup
ARTISTIC11
NTCC8
POBASCAM9
Swedescreen10
Total (95% CI)
Total events
Heterogeneity: τ² = 0.00; χ² = 0.54, df = 3 (P = 0.91); I² = 0%
Test for overall effect: Z = 4.91 (P < 0.00001)
Events
65
16
39
25
145
Total
11 676
33 733
8413
6257
60 079
Events
34
32
74
43
183
Total
3866
34 202
8456
6270
52 794
Weight
30.1%
14.3%
34.4%
21.3%
100.0%
M-H, Random, 95% CI
0.63 (0.42 to 0.96)
0.51 (0.28 to 0.92)
0.53 (0.36 to 0.78)
0.58 (0.36 to 0.95)
0.57 (0.45 to 0.71)
Experimental Control Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.1 0.2 0.5 1 2 5 10Higher rate of detectionin control group
Higher rate of detectionin HPV group
(c) CIN3+
Study or Subgroup
ARTISTIC11
NTCC8
POBASCAM9
Swedescreen10
Total (95% CI)
Total events
Heterogeneity: τ² = 0.00; χ² = 0.31, df = 3 (P = 0.96); I² = 0%
Test for overall effect: Z = 4.69 (P < 0.00001)
Events
29
8
24
16
77
Total
11 676
33 733
8413
6257
60 079
Events
18
17
54
30
119
Total
3866
34 202
8456
6270
52 794
Weight
25.5%
12.4%
38.1%
23.9%
100.0%
M-H, Random, 95% CI
0.53 (0.30 to 0.96)
0.48 (0.21 to 1.11)
0.45 (0.28 to 0.72)
0.53 (0.29 to 0.98)
0.49 (0.37 to 0.66)
Experimental Control Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.1 0.2 0.5 1 2 5 10Higher rate of detectionin control group
Higher rate of detectionin HPV group
Figure 2B. Relative rates (HPV-based screening/cytology-based screening) of detection of (a) CIN2, (b) CIN2+, and (c) CIN3+ in screening round two.
450 l MAY JOGC MAI 2012
GyNAECOLOGy
(a) CIN2
Study or Subgroup
ARTISTIC11
NTCC8
POBASCAM9
Swedescreen10
Total (95% CI)
Total events
Heterogeneity: τ² = 0.01; χ² = 4.34, df = 3 (P = 0.23); I² = 31%
Test for overall effect: Z = 3.01 (P = 0.003)
Events
256
116
45
53
470
Total
18 386
34 430
8575
6257
67 648
Events
69
69
43
34
215
Total
6124
34 405
8580
6270
55 379
Weight
34.2%
29.7%
18.5%
17.6%
100.0%
M-H, Random, 95% CI
1.24 (0.95 to 1.61)
1.68 (1.25 to 2.26)
1.05 (0.69 to 1.59)
1.56 (1.02 to 2.40)
1.37 (1.12 to 1.68)
Experimental Control Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.1 0.2 0.5 1 2 5 10Higher rate of detectionin control group
Higher rate of detectionin HPV group
(b) CIN2+
Study or Subgroup
ARTISTIC11
NTCC8
POBASCAM9
Swedescreen10
Total (95% CI)
Total events
Heterogeneity: τ² = 0.04; χ² = 13.93, df = 3 (P = 0.003); I² = 78%
Test for overall effect: Z = 1.48 (P = 0.14)
Events
518
221
137
139
1015
Total
18 386
34 430
8575
6257
67 648
Events
167
133
137
119
556
Total
6124
34 405
8580
6270
55 379
Weight
27.2%
25.1%
24.0%
23.7%
100.0%
M-H, Random, 95% CI
1.03 (0.87 to 1.23)
1.66 (1.34 to 2.06)
1.00 (0.79 to 1.27)
1.17 (0.92 to 1.49)
1.19 (0.94 to 1.50)
Experimental Control Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.1 0.2 0.5 1 2 5 10Higher rate of detectionin control group
Higher rate of detectionin HPV group
(c) CIN3+
Study or Subgroup
ARTISTIC11
NTCC8
POBASCAM9
Swedescreen10
Total (95% CI)
Total events
Heterogeneity: τ² = 0.05; χ² = 10.46, df = 3 (P = 0.02); I² = 71%
Test for overall effect: Z = 0.68 (P = 0.50)
Events
262
106
92
88
548
Total
18 386
34 430
8575
6257
67 648
Events
98
64
94
85
341
Total
6124
34 405
8580
6270
55 379
Weight
27.6%
23.5%
24.7%
24.2%
100.0%
M-H, Random, 95% CI
0.89 (0.71 to 1.12)
1.66 (1.21 to 2.26)
0.98 (0.74 to 1.30)
1.04 (0.77 to 1.39)
1.09 (0.84 to 1.42)
Experimental Control Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.1 0.2 0.5 1 2 5 10Higher rate of detectionin control group
Higher rate of detectionin HPV group
Figure 2C. Cumulative relative rates (HPV-based screening/cytology-based screening) of detection of (a) CIN2, (b) CIN2+, and (c) CIN3+ over two rounds of screening.

MAY JOGC MAI 2012 l 451
HPV Testing in Primary Cervical Screening: A Systematic Review and Meta-Analysis
meta-analysis of these trials has been controversial,19 because of differences between trials in management of subjects and other factors. However, other sources indicate that a pooled analysis is needed, because consistent results have been observed across trials.20,21 Thus, the results presented here should be interpreted cautiously. Nonetheless, the findings indicate that HPV testing provided a means of earlier detection of clinically significant lesions. In addition, two studies showed that HPV testing groups had lower rates of cervical cancer incidence and mortality over time than did cytology-based testing groups. In the study that specifically assessed women 25 to 34 years of age, the overall detection rate was more than three times greater in the intervention group.8 Likewise, in Finland the overall rate of positive HPV tests is 8%, rising to 15% to 25% in the youngest targeted age groups.22 HPV testing performs better in older age groups because the proportion of transient to clinically meaningful infections is higher in younger women.23 Furthermore, HPV screening can more often lead to detection of CIN1 and CIN2 lesions in younger women that would have regressed on their own, thus affecting quality of life. More research is needed to determine what primary screening test is optimal for younger women, and at what age screening should be initiated.
Previous studies have shown that women are at low risk of cervical cancer for a long interval after a negative HPV test.24 In this analysis, low rates of detection of CIN3+ at the second screening round in the intervention group and high NPVs in the studies that referred a sample of HPV-negative women for colposcopy indicates that lengthening of the screening interval from the current standard of two years to three years25 may be safe and feasible for HPV-negative women. Results from a third round of screening in the ARTISTIC trial,26 published after this systematic review had been completed, showed that a negative HPV test had a significantly more protective effect than cytology testing, suggesting that an extension of the screening interval to six years with HPV testing as the primary screen would be feasible.
A recent systematic review that included randomized and non-randomized studies concluded that more research would be needed before HPV-enhanced screening strategies could be recommended.19 This conclusion was made in the context of current practice in the United States in the absence of population-wide organized screening programs. While that analysis rated the RCTs individually as fair, our data quality assessment resulted in a consensus-based conclusion that the body of evidence as whole is good, based on factors such as the integration of these large scale trials into established screening programs, and the consistency of results across trials.
In applying these findings to population-based screening programs, the loss of specificity that accompanies the increased sensitivity associated with HPV testing is a concern. This can potentially be mitigated by a triage step before referral to colposcopy, possibly cytology testing, or genotyping for strains of HPV that are known to be more persistent or carcinogenic. Whatever the triage method, it must be implemented within an organized screening program with an information system to facilitate invitations, recalls, and communication and follow-up of abnormal results. Such systems are essential, as intensified follow-up of positive results and longer screening intervals for HPV-negative women will likely be features of programs that implement HPV testing for primary screening.
CONCLUSION
Evidence has accumulated from good quality RCTs supporting cervical cancer prevention via primary screening with HPV testing starting at age 30 or 35. The finding that CIN3+ rates are lower in a second screening round is reassuring. Finding similar relative detection rates across multiple studies, in the context of established or usual screening protocols, suggests that the findings are generalizable to the average-risk screening population in higher resource locations. Further results from some trials are anticipated, and should inform the degree to which the increased detection rate in the intervention group represents a timely gain in detection of significant lesions versus over-detection of transient lesions.
ACKNOWLEDGEMENTS
Funding: The work of the Program in Evidence-based Care is supported by the Ontario Ministry of Health and Long-Term Care through Cancer Care Ontario, and is editorially independent from its funding source.
Conflict of Interest: Sheila Dunn reported involvement in a clinical trial on this topic. Laurence Paszat reported grant support from the Canadian Institutes of Health Research for research on a related topic. Michael Shier reported receiving consulting fees, honoraria, and/or other support from GlaxoSmithKline and Graceway Pharmaceuticals, and contributing to several publications on this topic in the past five years.
REFERENCES
1. Sasieni P, Castanon A, Cuzick J. What is the right age for cervical cancer screening? Women’s Health 2010;6:1–4.
2. Canadian Cancer Society’s Steering Committee on Cancer Statistics. Canadian cancer statistics 2011. Toronto, ON: Canadian Cancer Society; 2011.
452 l MAY JOGC MAI 2012
GyNAECOLOGy
3. Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kummer JA, Shah KV, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol 1999;189:12–9.
4. Dunne EF, Unger ER, Sternberg M, McQuillan G, Swan DC, Patel SS, et al. Prevalence of HPV infection among females in the United States. JAMA 2007;297:813–9.
5. Franco EL. Is the UK ready to embrace HPV testing? Lancet Oncol 2009;10:643–4.
6. Cuzick J, Arbyn M, Sankaranarayanan R, Tsu V, Ronco G, Mayrand MH, et al. Overview of human papillomavirus-based and other novel options for cervical cancer screening in developed and developing countries. Vaccine 2008;26(Suppl 10):K29–41.
7. Anttila A, Kotaniemi-Talonen L, Leinonen M, Hakama M, Laurila P, Tarkkanen J, et al. Rate of cervical cancer, severe intraepithelial neoplasia, and adenocarcinoma in situ in primary HPV DNA screening with cytology triage: randomised study within organised screening programme. BMJ 2010;340:c1804.
8. Ronco G, Giorgi-Rossi P, Carozzi F, Confortini M, Dalla Palma P, Del Mistro A, et al. Efficacy of human papillomavirus testing for the detection of invasive cervical cancers and cervical intraepithelial neoplasia: a randomised controlled trial. Lancet Oncol 2010;11:249–57.
9. Bulkmans NW, Berkhof J, Rozendaal L, van Kemenade FJ, Boeke AJ, Bulk S, et al. Human papillomavirus DNA testing for the detection of cervical intraepithelial neoplasia grade 3 and cancer: 5-year follow-up of a randomised controlled implementation trial. Lancet 2007;370:1764–72.
10. Naucler P, Ryd W, Tornberg S, Strand A, Wadell G, Elfgren K, et al. Human papillomavirus and Papanicolaou tests to screen for cervical cancer. N Engl J Med 2007;357:1589–97.
11. Kitchener HC, Almonte M, Thomson C, Wheeler P, Sargent A, Stoykova B, et al. HPV testing in combination with liquid-based cytology in primary cervical screening (ARTISTIC): a randomised controlled trial. Lancet Oncol 2009;10:672–82.
12. Mayrand M, Duarte-Franco E, Rodrigues I, Walter SD, Hanley J, Ferenczy A, et al. Human papillomavirus DNA versus Papanicolaou screening tests for cervical cancer. N Engl J Med 2007;357:1579–88.
13. Sankaranarayanan R, Nene BM, Shastri SS, Jayant K, Muwonge R, Budukh AM, et al. HPV screening for cervical cancer in rural India. N Engl J Med 2009;360:1385–94.
14. Whiting P, Rutjes A, Reitsma J, Bossuyt P, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Method 2003;3:25.
15. Higgins JPT Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. Available at: http://www.cochrane-handbook.org. Accessed March 12, 2011.
16. Naucler P, Ryd W, Tornberg S, Strand A, Wadell G, Elfgren K, et al. Efficacy of HPV DNA testing with cytology triage and/or repeat HPV DNA testing in primary cervical cancer screening. J Natl Cancer Inst 2009;101:88–99.
17. Ronco G, Giorgi-Rossi P, Carozzi F, Confortini M, Dalla Palma P, Del Mistro A, et al. Results at recruitment from a randomized controlled trial comparing human papillomavirus testing alone with conventional cytology as the primary cervical cancer screening test. J Natl Cancer Inst 2008;100(7):492–501.
18. Davies P, Arbyn M, Dillner J, Kitchener HC, Meijer CJ, Ronco G, et al. A report on the current status of European research on the use of human papillomavirus testing for primary cervical cancer screening. Int J Cancer 2006;118:791–6.
19. Whitlock EP, Vesco KK, Eder M, Lin JS, Senger CA, Burda BU. Liquid-based cytology and human papillomavirus testing to screen for cervical cancer: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med 2011;155:687–97.
20. Arbyn M, Cuzick J. International agreement to join forces in synthesizing evidence on new methods for cervical cancer prevention [Review]. Cancer Lett 2009;278:1–2.
21. Ronco G, Meijer CJ, Cuzick J, Giorgi-Rossi P, Peto J, Segnan N, et al. Human papillomavirus testing to screen for cervical cancer. Ann Intern Med [online] November 11, 2011. Available at: http://www.annals.org/content/155/10/687.figures-only/reply#annintmed_el_127598. Accessed February 27, 2012.
22. Leinonen M, Nieminen P, Kotaniemi-Talonen L, Malila N, Tarkkanen J, Laurila P, et al. Age-specific evaluation of primary human papillomavirus screening vs conventional cytology in a randomized setting. J Natl Cancer Inst 2009;101:1612–23.
23. Bartholomew DA. Human papillomavirus infection in adolescents: a rational approach. Adolesc Med Clin 2004;15:569–95.
24. Dillner J, Rebolj M, Birembaut P, Petry KU, Szarewski A, Munk C, et al. Long term predictive values of cytology and human papillomavirus testing in cervical cancer screening: joint European cohort study. BMJ 2008;337:a1754.
25. McLachlin CM, Mai V, Murphy J, Fung-Kee-Fung M, Chambers A, Oliver TK, et al.; Cervical Screening Guidelines Development Committee of the Ontario Cervical Screening Program; Gynecology Cancer Disease Site Group of Cancer Care Ontario. Ontario cervical cancer screening clinical practice guidelines. J Obstet Gynaecol Can 2007;29:344–53.
26. Kitchener HC, Gilham C, Sargent A, Bailey A, Albrow R, Roberts C, et al. A comparison of HPV DNA testing and liquid based cytology over three rounds of primary cervical screening: extended follow up in the ARTISTIC trial. Eur J Cancer 2011;47:864–71.
Related Documents











