9500 Euclid Avenue, Cleveland, OH 44195 The Cleveland Clinic Foundation is an independent, not-for-profit, multispecialty academic medical center. It is dedicated to providing quality specialized care and includes an outpatient clinic, a hospital with more than 1,000 available beds, an education division and a research institute. © The Cleveland Clinic Foundation 2006 How to Refer a Patient to the Cleveland Clinic Brain Tumor Institute Members of the Brain Tumor Institute are available for consultation 24 hours a day, seven days a week. Their goal is to see patients with diagnosed or suspected brain tumors within 24 to 48 hours. 216.445.8971 or 800.553.5056, ext. 58971 (weekdays 8 a.m. to 5 p.m.) for consultations and/or hospital admission. 216.444.2200 (nights and weekends). Ask for neuro-oncology staff or the chief neurosurgical or neurological resident on call. For pediatric patients, ask for the chief pediatric neurological resident on call. Patient appointment line: 216.445.8971 or 800.223.2273, ext. 58971 Clinical trials information: Toll-free 866.223.8100 (Cancer Answer Line) Cleveland Clinic Florida (Weston): 954.659.5000 For details about the Brain Tumor Institute, please visit clevelandclinic.org/braintumor 06-BTI-003

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

9500 Euclid Avenue, Cleveland, OH 44195
The Cleveland Clinic Foundation is an independent, not-for-profit, multispecialty academic medical center. It is dedicated to providing quality specialized care and includes an outpatient clinic, a hospital with more than 1,000 available beds, an education division and a research institute.
© The Cleveland Clinic Foundation 2006
How to Refer a Patient to the Cleveland Clinic Brain Tumor InstituteMembers of the Brain Tumor Institute are available for consultation 24 hours a day, seven days a week. Their goal is to see patients with diagnosed or suspected brain tumors within 24 to 48 hours.
216.445.8971 or 800.553.5056, ext. 58971 (weekdays 8 a.m. to 5 p.m.) for consultations and/or hospital admission.
216.444.2200 (nights and weekends). Ask for neuro-oncology staff or the chief neurosurgical or neurological resident on
call. For pediatric patients, ask for the chief pediatric neurological resident on call.
Patient appointment line:
216.445.8971 or 800.223.2273, ext. 58971
Clinical trials information:
Toll-free 866.223.8100 (Cancer Answer Line)
Cleveland Clinic Florida (Weston):
954.659.5000
For details about the Brain Tumor Institute, please visit clevelandclinic.org/braintumor
06-BTI-003

Brain Tumor Institute2005 Annual Report prepared by Gene H. Barnett, M.D., Chairman
A team approach to individualized care

III Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
Table of Contents01 Letter from Chairman
02 Executive Summary
02 Invited Lectures
03 Educational Activity
04 Support and Grants
05 Membership
05 Recruitment
06 Research
07 Marketing, Advertising, Media Relations
07 Expanded Services
07 Patient Education
08 Clinical Programs
14 Clinical Research
17 Laboratory Research
26 Publications
33 Appendix A – Adult and Pediatric Clinical Trials
38 Appendix B – Charts and Statistics
39 Appendix C – Articles
44 Faculty
On the Cover: High power photomicrograph of macrophage (stained with green) showing red quantum dots phagocytized inside lysomes within the cells. These cells carry the QDots into the tumors, allowing them to be identified with optical imaging.

2005 Annual Report A team approach to individualized care �
Established in 2001, the Brain Tumor Institute (BTI) at Cleveland Clinic is among the
leading brain tumor centers in the nation. We are serving more patients than ever;
expanding our services and improving patient satisfaction; attracting world-class
physicians and scientists; making giant leaps in research and discovery; and acquiring
much-needed funding, particularly philanthropic support.
In 2005, among the hundreds of clinical studies already under way, the BTI led 26
clinical studies that were funded by corporate sponsors or Cleveland Clinic, or through
consortia. Two of our researchers received a U.S. patent for a blood-brain barrier
technology that may help detect new brain tumors using a simple blood test.
Collaborating with Taussig Cancer Center, the largest cancer program in Ohio, also
grants us access to its clinical and research resources as well as the opportunity to
interact with other health care professionals who deal with cancer patients daily. Using
innovative therapy and a multidisciplinary structure – a model of organization that has
attracted recent national and international interest – we provide a team approach to
individualized care. We look forward to improving care as we continue to measure
our performance.
Gene H. Barnett, M.D.
Chairman, Brain Tumor Institute
Letter from Chairman

2 Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
A Team Approach
Brain Tumor Institute
Executive Summary
an increase in new patient volume of 192 percent
The vision of the BTI is fourfold:1) To provide diagnosis and comprehensive management of brain
and spinal tumors
2) To provide excellent, compassionate care to every patient
3) To advance knowledge of the causes of brain tumor develop-
ment and growth, and develop new treatment options
4) To educate the public and professionals about brain tumors
and their management
Central to the success of the BTI is advancing the care of brain
tumor patients through better understanding of the causes and
mechanisms of these disorders. Our physicians and scientists are
conducting valuable research with the goal of bringing new safe
and effective therapies to patients as quickly as possible. It is this
dedication to improving the lives of our patients and others with
brain tumors that is the cornerstone of our work.
Invited LecturesIn March 2005, the BTI hosted Morris Groves, M.D., Director of
Inpatient Services, Department of Neuro-Oncology, University of
The Cleveland Clinic BTI is a leader in the diagnosis,
treatment and research of brain tumors. Chaired by
neurosurgeon Gene Barnett, M.D., the BTI comprises a
dedicated team of specialists who share the common
goal of advancing the diagnosis, research and treatment
of brain tumors in adults and children. This group of
neurosurgeons, neuro-oncologists, medical oncologists,
neuroradiologists, radiation oncologists, neuropatholo-
gists, advanced practice nurses and nurse practitioners
collaborates on clinical management and research of
brain tumors.
This multidisciplinary approach is used to diagnose and treat
adult and pediatric brain tumor patients, using state-of-the-art
diagnostic and therapeutic methods that can substantially
improve chances for survival and extend hope for a better quality
of life to those with previously untreatable tumors.

2005 Annual Report A team approach to individualized care �
Texas MD Anderson Cancer Center. Dr. Groves spoke on “Anti-
Invasion Strategies for the Treatment of High-Grade Glioma.”
In September, the BTI hosted Hienrich Elinzano, M.D., from the
Neuro-Oncology Branch of the National Institutes of Health. Dr.
Elinzano spoke on “Imaging Angiogenesis in Gliomas.” The BTI
also hosted Maciej Mrugala, M.D., from Massachusetts General
Hospital, who spoke on “Primary Central Nervous System
Lymphomas - Can we predict response to chemotherapy?”
In October, the BTI hosted Simon Lo, M.D., Assistant Professor
of Clinical Radiation Oncology from the Indiana University
Medical Center. Dr. Lo discussed “The Role of Gamma Knife
Radiosurgery in the Management of Unresectable Gross Disease
or Gross Residual Disease After Surgery in Ependymoma.”
In November, the BTI hosted Jann Sarkaria, M.D., Assistant
Professor of Oncology from Mayo Clinic College of Medicine, who
spoke on “Investigating Mechanisms of Temozolomide Sensitivity
in a GBM Xenograft Model.”
Educational ActivitiesContinuing Medical EducationSupporting Professional Education. As part of the BTI’s mission
to advance brain tumor treatment and research through
collaboration and education, the BTI and the Department of
Neurosurgery coordinated and hosted a major symposium in
January 2005, called “Neuro-Oncology 2005: Current Concepts.”
The symposium, which was held in Orlando, Fla., attracted
national and international leaders in the clinical care and
laboratory investigation of brain tumors. This successful event
brought together faculty and participants who spent three days
discussing advances in imaging, molecular biology, surgery,
radiotherapy, chemotherapy and alternative therapies to improve
the care of patients with central nervous system tumors. The BTI
also hosted a neuro-oncology mini-symposium in August.
The BTI hosted a regional physician dinner talk at the Glenmoor
Country Club in Canton, Ohio, in August 2005. Michael
Vogelbaum, M.D., Ph.D., presented on Intracerebral Delivery
of Chemotherapy for Brain Tumors. Recent advances in neuro-
oncology and the possible patient benefit of Convection
Enhanced Delivery were discussed.
The BTI’s Gamma Knife Center, under the direction of John
Suh, M.D., continues to be a major thrust for the BTI. In 2005,
radiosurgeons treated the 1,500th patient since the center
opened in 1997. The BTI is one of only three centers in the world
certified by the manufacturer to train physicians new to Gamma
Knife radiosurgery. In 2005, the Gamma Knife Center upgraded
its system to the most technologically advanced model, the
Model 4C. Cleveland Clinic is one of only eight centers in the
U.S. to have this model. To support education, Cleveland Clinic
held four week-long Gamma Knife radiosurgery training courses
in 2005, in addition to a two-day internal training course for
residents, fellows and Cleveland Clinic staff in January.
Professional EducationSponsoring symposia and publishing papers help to enhance the
reputation of the BTI among peers and patients, as well as to
encourage collaboration with colleagues locally, nationally and
internationally. Papers and abstracts generally are based on the
results of basic, translational and clinical research. Involvement
in these activities demonstrates our commitment to pursuing
a higher standard of research, professional education and,
ultimately, patient care.
to Individualized CareGamma Knife Radiosurgery Course

� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
In 2005, the staff of the BTI continued to increase editorial
activity with more than 100 journal articles, four book chapters
and two books published or in press. Currently, 59 journal
articles, 11 book chapters and two books are works in progress.
In 2005, the BTI published its first edition of outcomes. The
report is a brief summary of the department and a synopsis of its
surgical statistics and outcomes, with a comparison to published
standards and benchmarks. The outcomes booklet was mailed
to appropriate physician specialties across the country.
The BTI continues to place a high priority on hosting and
participating in physician education. In 2006, the BTI will
host two major symposia: “Contemporary Issues in Pituitary
Disease: Case-Based Management Update”, and “Cleveland
Clinic Symposium on Convection-Enhanced Drug (CED)
Delivery to the Brain,” led by an international faculty of top
CED investigators. In May 2006, the BTI will co-sponsor the
international symposium “Neuro-Oncology 2006: Current
Concepts” in Hamburg, Germany, with University Hospital
Hamburg-Eppendorf. Also in May, the BTI will host the “3rd
Brain Tumor Summit,” focusing on glioblastoma. The BTI also
will hold five Gamma Knife radiosurgery training courses for
physicians and physicists new to Gamma Knife radiosurgery.
At the end of 2005, the BTI and Case Western Reserve University
(known jointly as the Cleveland Brain Tumor Initiative) held a Brain
Tumor Biology Retreat in Cleveland to highlight emerging areas of
investigation in the area. Scientific investigators from around the
region working in such fields as cancer, neurosciences, cell growth
and migration attended the daylong conference, with the goals of
fostering interaction and encouraging collaboration.
The program consisted of a series of short talks and an interac-
tive poster session. Some of the topics included molecular
control of tumor cell migration, suppression of brain tumor
growth by agonists of the nuclear receptor PPAR gamma,
preclinical development of glioma vaccines for immunotherapy,
and tracking the migration of human glioma cells ex vivo using
quantum dots in a tissue slice model.
Higher Patient Volume. Between 2001 and 2005, the BTI
experienced an increase in new patient volume of 192 percent;
an increase in outpatient visits of 250 percent; an increase
in surgical cases of 56 percent; and an increase in Gamma
Knife cases of 47 percent. BTI physicians recorded 5,964
outpatient visits and performed 930 surgical, Gamma Knife
and Novalis procedures.
Larger Market Share. The BTI has the highest market share
in the “Cuyahoga County,” “21-county,” and “state of Ohio”
markets and, in 2005, increased its dominance over our closest
competitor, University Hospitals of Cleveland. Future initiatives
focus on increasing market share locally, regionally and nationally.
Support and GrantsPhilanthropy. Never before now has a group of donors been
so involved with and dedicated to the long-term success and sup-
port of the Brain Tumor Institute. Because of the generosity and
involvement of our donors, the BTI is better equipped to pioneer
advanced surgical procedures, develop more accurate imaging
techniques, investigate more effective treatments and, ultimately,
save more lives than we could alone. In January 2005, James
Saporito joined our team as the Director of Development for the
Taussig Cancer Center. Also in 2005, the Brain Tumor Institute
Leadership Board expanded membership and Norma Lerner
became our Honorary Co-Chair of the Board. The Leadership
Board is instrumental in spreading the word about the important
work being conducted by BTI physicians.
Since the BTI was formed, we have secured $13.1 million in
major pledges and contributions, including three endowed chairs.
In addition, this year the BTI obtained a challenge grant for
$750,000 for Gamma Knife Research. Our donors know that
philanthropic support is crucial if we are to continue to advance
the frontier of brain tumor treatment and research. Our needs are
great. Additional philanthropic support will help sustain our
research and educational activities for years to come.
Current Funding. Ongoing funding is crucial for BTI physicians,
researchers and scientists to continue to investigate potential
brain tumor therapies that may be used for treatment in the
future. In 2005, the BTI had 15 clinical studies funded by
corporate sponsors, seven clinical studies supported by Cleveland
Clinic, and four clinical studies funded through consortia. For
example, the BTI’s award of a UO1 grant from the NCI to Dr.
Gene Barnett to support full membership in the NABTT consor-
tium means that some of these research activities receive direct
federal support and that our patients will have access to more
clinical trials, including some that are conducted at just a few
centers across the country. Also, an NIH grant awarded to
Mladen Golubic, M.D., Ph.D., a project scientist in the BTI
laboratories, continues to support his work on the study of
5-lipoxygenases inhibition as an adjuvant glioma therapy.
New Funding. BTI staff members are continually applying for
funding and this year submissions have tripled. Below are examples
of funding awards received by BTI staff members in 2005.
Ali Chahlavi, M.D., of the Department of Neurosurgery and Brain
Tumor Institute received a grant award in 2005 of $40,000 from
the Neurosurgery Research and Education Foundation (NREF).
The award money will be used to study the immunosuppressive
function of glioblastoma multiforme (GBM). “New approaches
are requisite if malignant gliomas are to be treated successfully.
Immunotherapy has been an attractive approach in this disease;
however, due to their unsuccessful treatment so far, a second
modality that will target the immunosuppressive function of GBM
may be of greatest therapeutic relevance.”

2005 Annual Report A team approach to individualized care 5
Dr. Mladen Golubic has been awarded the National Brain Tumor
Foundation’s (NBTF) 2005 Richard A. Hollow, Jr. Quality of
Life Grant. This is a pilot study to examine whether participation
in a stress reduction program would improve quality of life for
patients with malignant brain tumors and their family caregivers.
A research project by Dr. Golubic has also been chosen for
funding by the Bakken Heart Institute.
Steven Toms, M.D., Head of the BTI’s Section of Metastatic Disease,
has been selected to receive development support from the
Innovation Validation Fund. His laboratory has been granted
$30,650 to complete the proposed work for commercial develop-
ment of CCF Innovations Case #04048, titled “Development of
Implantable Fiber Optic System for In Vivo Detection of Quantum
DOTS.” The funds are available as of March 1, 2005, and the
proposed date of completion for this project was February 28, 2006.
MembershipCleveland Clinic will host the International Blood-Brain Barrier
Disruption Consortium mid-year meeting in September 2006.
The consortium, which comprises seven institutions, combines
basic science, research and comprehensive patient care to treat
patients with brain tumors. The consortium is researching the
effective delivery of chemotherapy by outwitting the brain’s
natural defense, the blood-brain barrier, while also protecting
cognitive function.
Recruitment. Attracting and maintaining the best physicians,
researchers and employees to the BTI team are critical to remain
one of the leading brain tumor centers in the U.S. Never before
has employee satisfaction been higher in the BTI. Planned
recruitment for 2006 includes a pediatric neuro-oncologist
and a radiation oncologist.
Clinical Research and Cutting-Edge Clinical Trials. BTI patients
may elect experimental treatments or to participate in clinical
research projects related to their diagnosis. Various chemothera-
pies and growth modifiers are among the experimental drug
protocols developed by the institute’s clinical investigators.
Cleveland Clinic brain tumor patients benefit from clinical trials
designed by Cleveland Clinic physicians as well as those
conducted in conjunction with several national and international
consortia. These groups include: New Approaches to Brain
Tumor Therapy (NABTT) CNS Consortium, International Blood-
Brain Barrier Disruption Consortium (BBBD), Radiation Therapy
Oncology Group (RTOG), Southwest Oncology Group (SWOG),
American College of Surgeons Oncology Group (ACoSOG), and
Children’s Oncology Group (COG). Cleveland Clinic BTI physi-
cians serve as national principal investigators in several of the
trials conducted by these consortia.
Below are examples of projects being conducted in our clinical
research labs.
• Phase II Randomized Evaluation of 5-Lipoxgenase Inhibition by
Dietary and Herbal Complementary and Alternative Medicine
Approach Compared to Standard Dietary Control as an Adjuvant
Therapy in Newly Diagnosed Glioblastoma Multiforme. This
clinical trial, headed by Dr. Mladen Golubic, is the first comple-
mentary and alternative medicine trial launched by the BTI. Dr.
Golubic received NCI funding for this project. This trial seeks to
reduce the degree of edema around brain tumors, a common
and often debilitating aspect of brain cancer.
• A Phase I Study of Convection-Enhanced Delivery (CED) of
IL13-PE38QQR Infusion After Resection Followed by Radiation
Therapy With or Without Temozolomide. Dr. Michael Vogelbaum
serves as national co-principal investigator for a clinical trial that
infuses a novel targeted cancer toxin directly into the brain after
tumor resection. CED allows this large molecule, which otherwise
would be excluded from the brain by the blood-brain barrier,
to reach tumor cells in the brain.
• A Phase I/II Study Utilizing the PEC Intraoperative Radiotherapy
Device for the Treatment of a Resected Solitary Brain Metasta-
sis. Dr. Steven Toms has developed a study that uses a novel
device to deliver radiation therapy directly into the surgical
cavity immediately after resection of a brain metastasis. This
strategy delivers a high dose of radiation to the tumor cavity
immediately, while sparing the rest of the brain from radiation.
• Phase II Trial of Erlotinib with Temozolomide and Concurrent
Radiation Therapy Post-operatively in Patients with Newly
Diagnosed Glioblastoma Multiforme. This trial is designed to build
upon the therapy for patients with GBM by adding erlotinib, an
oral drug that targets a growth signaling protein on the surface
of GBM cells. This study follows initial encouraging data reported
by Dr. Michael Vogelbaum in his trial of erlotinib for recurrent
GBM. The study is headed by Dr. David Peereboom.
• A Phase I/II Trial of BMS-247550 for Treatment of Patients
with Recurrent High-grade Gliomas. This clinical trial examines
an epothilone for patients with recurrent high-grade gliomas.
Dr. David Peereboom is the PI for this national trial conducted
within the NCI-sponsored NABTT CNS Consortium.
• Phase III Trial comparing Whole Brain Radiation Therapy versus
Whole Brain Radiation Therapy plus Efaproxiral for Women with
Brain Metastases from Breast Cancer. Dr. Suh is the PI for this
international phase III trial of a novel radiosensitizer.
• International Registry for CNS Atypical Teratoid/Rhabdoid
tumor. Dr. Joanne Hilden, chair of the Department of Pediatric
Hematology/Oncology at Cleveland Clinic Children’s Hospital,
founded and runs a registry for CNS Atypical Teratoid Tumor of
childhood, which generates an evidence base for the treatment
of this highly malignant tumor. Registry results were used in
part to help design the first COG clinical trial for CNS AT/RT.

� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
BTI clinical investigators continually are developing various
experimental treatment protocols for brain tumor and neuro-
oncology patients. At the BTI’s Center for Translational Therapeu-
tics (CTT), directed by Dr. Michael Vogelbaum, preclinical testing
of the most promising anticancer agents into Phase I and II
clinical trials is under way, giving brain tumor patients more
therapeutic treatment options.
Testing of new agents involves evaluating the toxicity and efficacy
of these compounds in the laboratory and in animals that have
brain tumors. We also are investigating the optimal route of
delivery of these drugs.
Because many new therapeutic agents cannot penetrate the
central nervous system, center researchers are exploring
alternative delivery methods. In addition to investigating the
efficacy of oral delivery, researchers evaluate the efficacy of the
agents when delivered intracerebrally – directly into the brain –
via a specialized neurosurgical technique called convection-
enhanced delivery (CED).
The staff at the CTT is focused on translating these preclinical
results into Phase I and II clinical trials - giving the brain tumor
patient more therapeutic treatment options by broadening the
horizon of potential tools we may use to manage this deadly disease.
The CTT has started research projects with several pharmaceuti-
cal and biotechnology companies, ranging in size from small
startup firms to some of the largest publicly traded companies.
What these companies have in common are novel drugs that are
close to or are in clinical trial and which are rationally designed
to be effective against malignant gliomas, given the molecular
and genetic makeup of these tumors. These drugs are targeted
against molecules such as EGFR, mTOR/Akt, Jak/STAT3 and
Raf-1 kinase. Our first translational clinical trial is with Tarceva/
OSI-774, a selective EGFR kinase inhibitor small molecule drug.
Other projects are focused on developing methods to improve
immune response to gliomas (in collaboration with Dr. James
Finke), understanding the role of NFkB in regulating glioma cell
migration and exploring the use of a new drug that may
sensitize gliomas to temozolomide (in collaboration with
Dr. Stanton Gerson).
Basic Research. Research at Cleveland Clinic continues to
grow and prosper through recruitment of outstanding new
staff, improvement and expansion of facilities, development of
extensive infrastructure and support services, and the enhance-
ment of education programs. Central to the success of the BTI
is advancing the care of brain tumor patients through better
understanding of the causes and mechanisms of tumor develop-
ment. Basic science research efforts are focused on identifying
the genetic, cellular and molecular biology of malignant and
benign brain tumors, investigating the mechanism of tumor
formation and exploring new therapeutic developments for brain
tumor treatments. One example of the promising research being
conducted by BTI physicians is Dr. Robert Weil’s research on
proteomics, which involves analyzing the human genome at
the protein level – the point at which most diseases manifest
themselves. See Appendix C for details.
Below are examples of the projects being conducted in the
basic research labs.
• Developing immunotherapy for malignant glioma using
vaccines formed by fusing tumor cells with dendritic cells
(Dr. Gregory Plautz).
• The tumor antigen profile of brain tumor stem cells is being
characterized to determine whether there are common glioma
antigens, which would make it possible to develop a standard-
ized glioma vaccine (Dr. Gregory Plautz).
• The ability of dendritic cell/tumor cell fusion vaccines and
adoptive transfer of tumor-sensitized T cells to cure established
brain tumors is being tested in mouse models as a prelude to
future clinical trials (Dr. Gregory Plautz).
• Genetic alterations and biological characterization of
primary cell cultures derived from malignant gliomas
(Dr. Olga Chernova).
• Genetic alterations in GBMs (loss or gain of 19q, 1p and other
novel alterations) and their correlations with patient survival
(Dr. Olga Chernova).
• Development of a clinical assay for detection of deletions
in CDKN2A, ARF, PTEN and p53 genes in gliomas
(Dr. Olga Chernova).
• Genotyping arrays as a prognostic tool: glioma model
(Dr. Olga Chernova).
• Distinct alteration of chromosome 1p in astrocytic and
oligodendrocytic tumors (Dr. Olga Chernova).
• An in-vitro and in-vivo model altering GBM immunosuppression
to enhance immunotherapy (Drs. Ali Chahlavi and James Finke).
Research taking place at Cleveland Clinic allows BTI physicians a greater understanding of the mechanisms of brain tumors.

2005 Annual Report A team approach to individualized care �
• NAD(P)H autofluorescence in cell death - NADH and NADPH
are pyridine nucleotides that function as electron donors in
oxidative phosphorylation ( Dr. Steven Toms).
• Role of optical nanocrystals (quantum dots) in molecular
and cancer imaging (Dr. Steven Toms).
Hundreds of basic and clinical cancer research projects are under
way here at any given time, and numerous papers are presented
annually at national and international meetings regarding
research results.
Marketing. Many marketing initiatives have been instituted to
create awareness of the BTI in 2005. Because brain tumor
patients are information savvy and seek out the latest in medical
options for their condition, the BTI Web site is a particularly
important marketing tool. Focus in 2005 has been on increasing
the presence of the Web site among the Overture (Yahoo! and
MSN) and Google search engines. The content has been optimized
to increase the natural rankings of the Web site. The BTI has also
purchased brain tumor-related words on a pay-per-click basis to
maximize Web site traffic. Direct-mail campaigns such as mailing
the BTI annual report to neurosurgeons and neurologists across
the country and a continuous presence in Cleveland Clinic
physician and patient publications ensures information on the
BTI services is being communicated to our target markets.
Advertising. Newspaper print advertising for the Gamma Knife
Center has been expanded to the following markets: Akron/
Canton, Ashtabula, Sandusky, Toledo and Warren, Ohio. The
goal of our advertising is to increase awareness and, ultimately,
patient visits to the BTI. A BTI ad appeared in the Ohio regional
issue of Women’s Day magazine. Return on investment will be
measured for these initiatives, and this information will be used
to plan advertising for 2006.
BTI in the News. In December 2004, a high profile international
athlete was treated with Gamma Knife radiosurgery at the BTI,
for which we were able to obtain media exposure on television, in
print and on the Web. Cleveland Clinic researchers Gene Barnett
and Damir Janigro received a U.S. patent for technology they
developed to measure damage to a person’s blood-brain barrier
that may help detect new brain tumors through a simple blood
test. See Appendix I for details.
Expanded Services. BTI patients can access neuro-oncology
services not only at Cleveland Clinic’s main campus, but also at
Cleveland Clinic’s west side community hospitals (Lakewood,
Lutheran and Fairview). Additionally, Dr. Gene Barnett sees
patients in consult at the Ashtabula County Medical Center
on the far east side.
Lilyana Angelov, M.D., continues to facilitate expansion of the
BTI’s various brain tumor programs into the western region of
Cleveland. She oversees primary and metastatic tumors, as well
as access to BTI protocols through the Moll Cancer Center at
Fairview Hospital and at Lakewood Hospital.
BTI physicians work closely with neurosurgeons in Cleveland
Clinic Florida to provide services for patients. Out-of-state
patients can take advantage of the Clinic’s Medical Concierge
program, a complimentary service that offers facilitation and
coordination of multiple medical appointments; access to
discounts on airline tickets and hotels, when available; help
in making hotel reservations or housing accommodations; and
arrangement of leisure activities.
BTI and Gamma Knife Center specialists also see patients from
out of the country. The special requirements of international
patients are handled through the Cleveland Clinic International
Center. The professionals within the International Center provide
the assistance and services our international patients need to
help them feel at home while they are being treated here. We
employ a large multilingual staff, and interpreters are available
to assist patients. Our staff helps coordinate all the details of a
visit, from scheduling medical appointments and making hotel
and transportation arrangements to transferring and translating
medical records.
Supporting Patient Education. The BTI was a proud sponsor of
the American Brain Tumor Association’s (ABTA) regional patient
meeting in July in Itasca, Ill. More than 400 patients and their
family members, health care providers and volunteers gathered
to learn about various topics, from the biology of brain tumors to
choosing between standard therapy and a clinical trial. The BTI’s
Glen Stevens, D.O., Ph.D., and Kathy Lupica, M.S.N., C.N.P., as
well as marketing associate Kristin Swenson, made information
available to patients. The BTI also sponsored a similar event for
patients and their families at the ABTA’s regional patient meeting
in Dallas, Texas, in November.
The BTI participated in the Cleveland Clinic Medical Miracles
television show in fall 2005. The Strength of the Human Spirit II
follows four patients who were diagnosed with different forms
of cancer and chronicles their lives before diagnosis, during
treatment and throughout their efforts to maintain a normal life.
The episode featured a female patient of the BTI whose breast
cancer metastasized to her brain and was treated with Gamma
Knife radiosurgery. The BTI also partnered with an online support
group, the Pituitary Network Association (PNA), which is an
international nonprofit organization for patients with pituitary
tumors and disorders, their families, loved ones, and the
physicians and health care providers who treat them.
Serving as a Program Model. The success of the BTI can be
measured not only by the advances made toward patient care
at Cleveland Clinic, but also by the way in which these advances
impact the treatment of brain tumor patients everywhere.
National and International interest in the BTI model of organiza-
tion is high, serving as a model for other brain tumor programs
around the country and world.

� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
Clinical Neuro-Oncology Neuro-oncologists, medical oncologists, neurosurgical oncologists,
radiation oncologists, neuro-pathologists, neuroradiologists and
BTI nurses attend daily clinics and twice-weekly tumor boards.
This cooperative approach, proven in more than a decade of use,
provides for consensus management plans that are individualized
and focused on the best mix of medical, surgical and radiotherapy
treatment of both benign and malignant tumors affecting the brain
and spinal cord. In addition to providing conventional treatments,
innovative investigational studies are available – some of these
were developed at Cleveland Clinic – and others are performed as
part of multicenter trials.
Members of the team also provide long-term surveillance and
medical management of patients.
Cutting-edge experimental treatments include use of targeted
immunotoxins delivered by convection-enhanced delivery and
so-called “small molecule therapies” (SMTs) such as Tarceva
(an EGFR inhibitor), and an “mTOR” inhibitor. These, along with
the expanded routine use of molecular and chromosomal testing
used to guide individual patient management, help put the BTI
at the forefront of individualized care and the molecular manage-
ment of brain tumors.
Methods for both surgical and nonsurgical treatments of life-
threatening tumors are advanced by medical innovations in
the following areas:
• Intraoperative MRI – navigational guidance and monitoring
tumor resection
• Stereotactic Neurosurgery – computer-guided surgery using
a three-dimensional software configuration
• Multiple Radiosurgery Options – Gamma Knife for single
Brain Tumor Institute
Clinical Programs
Physicians from several different specialties within the BTI meet weekly to discuss each patient’s case and collaborate on treatment options.
session cranial stereotactic radiosurgery; Novalis System for
cranial radiosurgery in several sessions and spinal radiosurgery;
and the Peacock system for intensity-modulated radiotherapy
• Fractionated Radiotherapy – widespread exposure of the brain
and tumor to repeated low doses of radiation
• Brachytherapy – direct implantation of a radiation source
(solid or liquid) within a tumor site
• Chemotherapy/growth modifiers – traditional anti-tumor drugs
as well as new agents targeted at specific tumor molecules are
being tested
• Immunotherapy – turning the patient’s immune system against
tumor cells or using immunologically targeted toxins
• Convection-Enhanced Delivery (CED) – the slow, continuous
infusion of drugs through the brain to treat certain brain tumors.
Used both in the laboratory and for patients, it permits treatment
with agents that would be too toxic to the body if delivered
conventionally.
• Intra-arterial Chemotherapy with or without Blood-Brain
Barrier Disruption (BBBD) – a procedure by which cancer-
fighting agents are delivered to the brain through the blood
stream with or without opening the normal barriers that
may prevent those drugs from entering the brain.
Clinical Neurosurgical Oncology Pioneers in computer-assisted stereotactic techniques for brain
tumors since the mid-1980s, BTI surgeons have extended the
scope of operable brain tumors by using techniques such as
frame or frameless stereotaxy (surgical navigation), skull-base
techniques, microsurgery, endoscopic surgery, computer-assisted
rehearsal of surgery, intraoperative MRI, radiation implants and
radiosurgery. The development of precision surgical navigation
systems in the late 1980s and early 1990s by the Cleveland
Clinic’s Center for Computer-Assisted Neurosurgery allows for
smaller incisions and GPS-like guidance in the brain that have
resulted in substantial reductions of wound and neurologic
morbidity, length of surgery, hospital costs and length of stay
for many benign and malignant brain tumor surgeries. The
interest in surgical navigation continues as the Department of
Neurosurgery uses several navigation systems as well as
intraoperative imaging using ultrasound and MRI.
In 2005, the department continued the pursuit of cutting-
edge technology with Odin Medical Technologies/Medtronics,
manufacturer of a compact intraoperative MRI. The device
weighs only 1,300 pounds – a fraction of the weight of conven-
tional units. During surgery, the device is stowed below the
operative field, allowing many conventional surgical instruments
to be used. When imaging is required, the magnets are raised

2005 Annual Report A team approach to individualized care �
into position, flanking the patient’s head for scans that range in
time from about one to seven minutes. When not required during
surgery, the imager is placed in a magnetically shielded cage
in the corner of the room, allowing the room to be fully used for
conventional procedures. Cleveland Clinic was the fourth site in the
world to have this system, and we believe that systems like it likely
are to become commonplace by the end of the decade. The device
will be upgraded to the more powerful model N20 in 2006.
FellowshipsIn addition to being a part of the core curriculum in Neurosurgery,
the BTI is active in other areas of postgraduate education. A two-
year fellowship – one year of basic science investigation and the
other year clinical – is offered in Neurosurgical Oncology. Dr. Dae
Kyu Lee completed his clinical Neurosurgical Oncology training,
followed by Drs. Tina Thomas and John Park. Dr. Burak Sade
continues on as the BTI skull-base fellow.
Clinical Radiation Neuro-OncologyRadiation oncologists, focusing on the specific problems of brain
and spinal cord tumors, offer both traditional and innovative
treatments to ensure patients have access to a number of
technologies. In 1989, the Cleveland Clinic’s Radiosurgery
Program was the first in Ohio to treat patients with state-of-the-
art noninvasive ablative therapy using a modified linear accelera-
tor. Since 1997, a number of technologies have be introduced
including Gamma Knife, intensity-modulated radiotherapy
(IMRT), intraoperative radiation therapy (IORT), brachytherapy,
and image-guided radiation therapy (IGRT). These technologies
may control lethal tumors for longer periods than conventional
radiation therapy, decrease the potential side effects of radiation
therapy and may benefit patients whose general health may not
be sufficient to withstand a protracted microsurgical procedure.
A team of personnel including neurosurgeons, radiation oncologists,
radiation physicists and radiation therapists provides treatments.
For Gamma Knife radiosurgery, a single one- to two-hour treatment
is generally required, in which 201 beams of gamma rays are
focused at multiple points throughout the target, with the aim of
matching the delivered radiation to the shape of the tumor. Thus,
the radiation’s destructive potential is concentrated in the tumor,
and fall off in adjacent tissue is exceedingly steep, minimizing
damage to tissue lying in the entry or exit pathways. Because of
this precise focusing ability, aggressive high-dose radiation can be
delivered to stabilize, shrink or destroy some lesions – even
those deep in the cerebral hemispheres or brain stem.
The past year has been a successful one for the Gamma Knife
Center. In 2005, our Gamma Knife equipment was upgraded to
the latest 4C version with software and hardware enhancements.
In 2005, 244 Gamma Knife radiosurgery cases were performed
for a number of indications, which represented our best year.
In addition, a number of papers were presented at national and
international meetings regarding the center’s results.
The Gamma Knife Center is one of three centers worldwide
certified by Elekta (the sole manufacturer of the Gamma Knife)
to train physicians new to Gamma Knife radiosurgery.
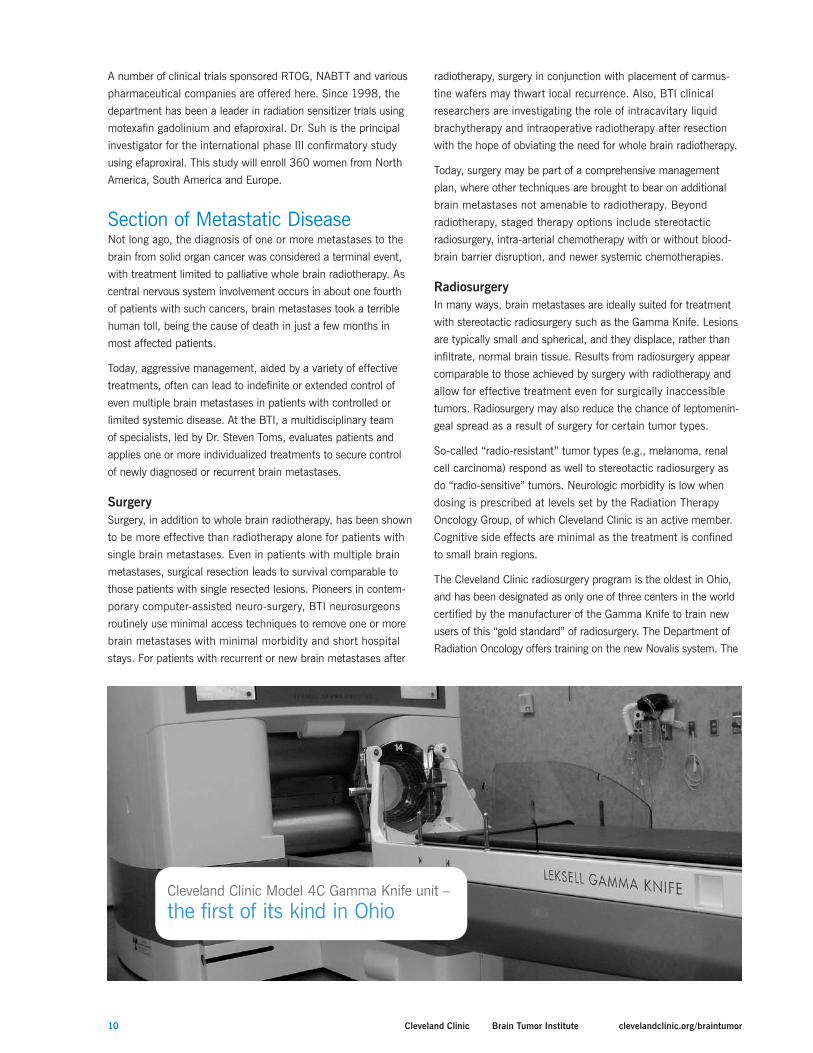
The Model �C Gamma Knife unit – the first of its kind in Ohio
The Novalis System further increases the capabilities within
radiation oncology and allows for radiosurgery and fractionated
radiosurgery treatments for neuro-oncology patients using image
guidance. This technology gives us the ability to treat lesions near
critical structures, such as the optic nerves and chiasm, as well
as re-treat some patients who have undergone conventional
radiotherapy. In general, Gamma Knife is used for single
treatments of focused radiation that conforms to the shape
of small tumors or lesions, while Novalis delivers fractionated
conformal treatment for larger malignant or benign tumors.
Although Novalis was originally developed to treat brain tumors,
Cleveland Clinic physicians recognized its potential for treating
extracranial tumors, particularly primary and metastatic spinal
tumors that are difficult to treat due to their proximity to critical
structures. In 2006, we have plans to promote and expand the
spinal radiosurgery program.
In addition to the Gamma Knife, linear accelerators and Novalis,
we offer intraoperative radiation therapy (IORT) with the
INTRABEAM device, a 50 kVp contact unit that is placed
in the resection cavity. We have an ongoing phase II trial
evaluating the use of INTRABEAM for patients with a single
brain metastasis that has been resected. We also offer
brachytherapy using the GliaSite balloon catheter system
and have participated in several clinical trials.
Cleveland Clinic neurosurgeons continue to perfect brain tumor resection techniques, minimizing damage to delicate brain tissue.
�0 Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
A number of clinical trials sponsored RTOG, NABTT and various
pharmaceutical companies are offered here. Since 1998, the
department has been a leader in radiation sensitizer trials using
motexafin gadolinium and efaproxiral. Dr. Suh is the principal
investigator for the international phase III confirmatory study
using efaproxiral. This study will enroll 360 women from North
America, South America and Europe.
Section of Metastatic DiseaseNot long ago, the diagnosis of one or more metastases to the
brain from solid organ cancer was considered a terminal event,
with treatment limited to palliative whole brain radiotherapy. As
central nervous system involvement occurs in about one fourth
of patients with such cancers, brain metastases took a terrible
human toll, being the cause of death in just a few months in
most affected patients.
Today, aggressive management, aided by a variety of effective
treatments, often can lead to indefinite or extended control of
even multiple brain metastases in patients with controlled or
limited systemic disease. At the BTI, a multidisciplinary team
of specialists, led by Dr. Steven Toms, evaluates patients and
applies one or more individualized treatments to secure control
of newly diagnosed or recurrent brain metastases.
SurgerySurgery, in addition to whole brain radiotherapy, has been shown
to be more effective than radiotherapy alone for patients with
single brain metastases. Even in patients with multiple brain
metastases, surgical resection leads to survival comparable to
those patients with single resected lesions. Pioneers in contem-
porary computer-assisted neuro-surgery, BTI neurosurgeons
routinely use minimal access techniques to remove one or more
brain metastases with minimal morbidity and short hospital
stays. For patients with recurrent or new brain metastases after
radiotherapy, surgery in conjunction with placement of carmus-
tine wafers may thwart local recurrence. Also, BTI clinical
researchers are investigating the role of intracavitary liquid
brachytherapy and intraoperative radiotherapy after resection
with the hope of obviating the need for whole brain radiotherapy.
Today, surgery may be part of a comprehensive management
plan, where other techniques are brought to bear on additional
brain metastases not amenable to radiotherapy. Beyond
radiotherapy, staged therapy options include stereotactic
radiosurgery, intra-arterial chemotherapy with or without blood-
brain barrier disruption, and newer systemic chemotherapies.
RadiosurgeryIn many ways, brain metastases are ideally suited for treatment
with stereotactic radiosurgery such as the Gamma Knife. Lesions
are typically small and spherical, and they displace, rather than
infiltrate, normal brain tissue. Results from radiosurgery appear
comparable to those achieved by surgery with radiotherapy and
allow for effective treatment even for surgically inaccessible
tumors. Radiosurgery may also reduce the chance of leptomenin-
geal spread as a result of surgery for certain tumor types.
So-called “radio-resistant” tumor types (e.g., melanoma, renal
cell carcinoma) respond as well to stereotactic radiosurgery as
do “radio-sensitive” tumors. Neurologic morbidity is low when
dosing is prescribed at levels set by the Radiation Therapy
Oncology Group, of which Cleveland Clinic is an active member.
Cognitive side effects are minimal as the treatment is confined
to small brain regions.
The Cleveland Clinic radiosurgery program is the oldest in Ohio,
and has been designated as only one of three centers in the world
certified by the manufacturer of the Gamma Knife to train new
users of this “gold standard” of radiosurgery. The Department of
Radiation Oncology offers training on the new Novalis system. The
Cleveland Clinic Model 4C Gamma Knife unit –
the first of its kind in Ohio

2005 Annual Report A team approach to individualized care ��
department has been designated a “center of excellence” in the
use of this image-guided technology and is one of the first sites in
the country to use Novalis especially for image-guided “spine radio-
surgery,” in addition to brain tumor treatment.
Treatment with Novalis is indicated for those patients who
tumors are not ideal for Gamma Knife radiosurgery. In addition,
Novalis can be used for extracranial sites such as metastatic
spinal tumors, prostate and lung cancers. Since adding the
Novalis system to its arsenal of radiosurgery programs one year
ago, the Department has treated approximately 150 patients,
with anatomic treatment sites including the brain, spine, lung,
prostate, kidney and bone.
ChemotherapySystemic cancers that are chemotherapy sensitive often take
refuge in the brain, despite systemic control, as most commonly
used chemotherapies have poor penetration through the blood-
brain barrier. Management of such tumors may take several
forms. Patients with metastatic breast cancer to the brain with
tumors that are estrogen-receptor positive may respond to high-
dose tamoxifen, thereby compensating for the drug’s limited
penetration of the brain. Alternatively, temozolomide, a relatively
new orally-administered methylating agent has excellent
penetration into the brain and may be considered for some
patients. More intensive treatment includes use of chemotherapy
injected directly into the carotid vertebral arteries, at times using
hypertonic mannitol to disrupt the blood-brain barrier from
preventing active agents from reaching adequate concentrations
in brain metastases.
Small MoleculesAn exciting area of investigation is the use of small targeted
molecules to treat a variety of malignancies. As the molecular
characterization of various tumors improves, investigational drugs
that target specific molecular pathways may play an increasing
role in the management of brain metastases, and even leptomen-
ingeal disease. The use of these agents and appropriate modes of
delivery are and will continue to be a major thrust of BTI clinical
and laboratory research.
Center for Neurofibromatosis and Benign Tumors (CNBT)The CNBT at Cleveland Clinic continues as a leading center in the
nation in the management of patients with benign brain tumors.
In 2005, the CNBT neurosurgeons saw over 300 new patients
with benign tumors, the two most common tumors being
meningiomas and schwannomas. More than 200 new patients
with meningiomas were seen in 2005. Of these patients,
approximately 100 underwent surgery, 20 had Gamma Knife
radiosurgery and the remaining 80 were treated conservatively.
Over 70 new patients with schwannomas were evaluated in
2005. Fifty patients had surgery, approximately 15 had Gamma
Knife radiosurgery and the remainder had conservative treatment.
These numbers represent one of the largest in the country for
specialized benign tumor management.
Dr. Lee, the Director of CNBT, had six articles and nine papers
accepted for publication. He currently is editing a major
landmark textbook on meningiomas consisting of 70-plus
chapters, with contributions from more than 50 international
leaders in all the basic and clinical disciplines related to
meningiomas. This book is planned for early 2007 publication.
Additionally, a three-year research grant was award to Dr. Lee
by the Integra Neurosciences Foundation for the study of dural
reconstruction following skull base and meningioma surgery.
Dr. Lee also was an invited lecturer at annual meetings of the
Korean Skull Base Society, the European Skull Base Society
and the North American Skull Base Society.
Neuro-Endocrine CenterThe Neuro-Endocrine Center has shown continuous growth since
its inception in 2002, fostered by a close working relationship
among the BTI and the departments of Endocrinology, Diabetes
and Metabolism; Neurological Surgery; Neuro-Ophthalmology;
and Radiation Oncology. The close relationship has led to the
development of highly integrated clinical care pathways, a
common pituitary tumor research database and several joint
research projects (see below).
Clinical Care PathwaysClinical care pathways define the pre-hospital, peri-operative and
postoperative care for patients with secretory and non-secretory
pituitary tumors. The development of new pathways has decreased
patient length of stay and has likely improved outcomes.
Academic ActivitiesA prospective IRB-approved database has been established for
all patients with pituitary tumors seen in the Neuro-Endocrine
Center. Detailed preoperative endocrine testing, including
Cortrosyn stimulation, is routinely performed for comparison
to postoperative findings. New clinical care pathways have
eliminated the routine use of perioperative steroids, thereby
enabling the accurate determination of postoperative pituitary
adrenal activity. Several retrospective analyses have been

�2 Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
recent additions in this regard have been diffusion tensor
imaging, fiber tracking and functional MRI software with
prospective motion correction, real-time monitoring of the data
acquisition and accurate three-dimensional surface localization.
All three 1.5 Tesla systems at the main campus have been
upgraded in the last year, and are located immediately adjacent
to the Gamma Knife Center. These new systems include
upgraded gradient capabilities, an extensive variety of phased
array coils and the software to perform parallel imaging tech-
niques, allowing reduce imaging time, reduce inherent MR
imaging artifacts and improve spatial resolution. One of these
1.5 Tesla systems has a wide, short bore to accommodate our
larger and claustrophobic patients, without the limitations of the
low-field open systems. A 3.0 Tesla whole-body system has
been installed at Cleveland Clinic’s Mellen Center to provide
new research and imaging capabilities. This system will permit
imaging of the spine and head, as well as high-resolution
diffusion tensor imaging, multi-nuclear MR spectroscopy
and phased-array technology. The 3 Tesla system serves
as the primary magnet for functional MR studies.
Neuro-Oncology NursingNurses, physician assistants and technicians specializing in the
care of patients with brain tumors are an integral part of the BTI.
Members of the nursing and physician assistant team, which
includes Cathy Brewer, Gail Ditz, Sandra Ference, Michele Gavin,
Betty Jamison, Debra Kangisser, Kathy Lupica, Mary Miller, Carol
Patton, Rachel Perez, Sherry Soeder, Lisa Sorenson, Laural Turo,
and Carla Yoder, are often the first contact for patients seeking an
opinion or when they come to the outpatient department.
Lisa Sorenson works with patients at the Cleveland Clinic main
campus, Lakewood and Fairview hospitals, as well as with the
Blood-Brain Barrier Disruption (BBBD) program.
Kathy Lupica facilitates our monthly Brain Tumor Support
Group. She also provided patients with information at the
completed and are also in progress, including comparison of
Gamma Knife vs. IMRT for subtotally resected somatotrophic
pituitary adenomas, case review of pituicytoma and a retrospec-
tive analysis of the impact of somatostatin on the efficacy of
radiosurgery for somatotrophic adenoma.
Teaching of residents and fellows has similarly been augmented
through the establishment of the center. Endocrine residents
routinely participate in outpatient evaluation with endocrinologists
and surgeons. The vascular service junior resident spends
one day in the outpatient clinic evaluating pituitary patients.
A joint conference involving endocrinology, neurosurgery, neuro-
ophthalmology, neuroradiology and radiation oncology is held on
the first Friday of each month, during which case presentations
and management or visiting lecturers are presented. In addition,
monthly pathology review sessions, where the pathological
findings of each patient are reviewed jointly by the pathologists,
endocrinologists and neurosurgeons (the Pituitary Interest
Group), continue. These sessions are open to all interested
parties and are held the first Monday of the month in the
Department of Pathology.
Neuro-RadiologyThe Section of Magnetic Resonance Imaging at Cleveland Clinic
provides a wide array of diagnostic capabilities for routine
imaging studies as well as research projects in support of the
BTI. During the last two years, there has been a dramatic
increase in availability to high-field imaging within Cleveland
Clinic hospitals with the installation of a large number of new
magnets. This enables our patients and physicians to schedule
MR imaging appointments at a site that is more convenient for
the patient and more expeditious for patient management. All of
these systems are managed centrally at Cleveland Clinic’s main
campus, and the images are transmitted digitally so they are
immediately available for comparison with prior studies on the
central digital archive. Not only are the images immediately
available to our Diagnostic Neuroradiology staff, but the digital
reports and all imaging studies are also immediately available
to our referring physicians. At the moment, imaging workstations
exist across Cleveland Clinic so the referring services have direct
digital access to the images.
Our MR machines include a large number of 1.5 and 1.0 Tesla
systems. Diagnostic imaging capabilities in our system currently
include routine imaging, diffusion imaging and high-resolution
preoperative planning studies at all of our facilities. At our main
campus, we also provide MR perfusion imaging, diffusion tensor
imaging, functional MRI and MR spectroscopy for more advanced
preoperative planning. Between our own MR physicists and
neuroradiology physicians, as well as our research affiliations
with Siemens Medical Systems and Massachusetts General
Hospital, we’re able to provide access to a host of new software
and hardware for the management of our patients. The most
Cleveland Clinic specialists are pioneers in developing new methods of intergrating image data with surgery

2005 Annual Report A team approach to individualized care ��
BTI’s exhibit at the ABTA’s patient meetings in Chicago, Ill.,
and Dallas, Texas, in 2005.
Nurse practitioner Sandra Ference manages patients undergoing
BBBD or intra-arterial chemotherapy.
Cathy Brewer and Carol Patton assist with patients who are
interested in participating in or who currently are involved in
research protocols.
Betty Jamison works with patients undergoing Gamma Knife
radiosurgery.
Nurse Practitioners: Sandra Ference, Kathy Lupica,
Sherry Soeder, Lisa Sorenson, Carla Yoder
Nurse Clinicians: Gail Ditz, Betty Jamison, Rachel Perez,
Laural Turo
Research Nurses: Cathy Brewer, Carol Patton
Physician Assistants: Michele Gavin, Debra Kangisser
Pediatric and Young Adult Brain Tumor ProgramDr. Joanne Hilden, Chair of the Department of Pediatric Hematol-
ogy/Oncology, and Dr. Bruce Cohen, BTI staff member, co-direct
the Pediatric and Adolescent Brain Tumor Program. A multidisci-
plinary brain tumor clinic for children and adolescents with brain
tumors takes place twice weekly. Patients can see both Drs.
Hilden and Cohen on the same day, and sedated imaging is
available. Each child has a care coordination team in place,
consisting of a physician, a nurse practitioner and a registered
nurse. Neurosurgeons are available to see patients as needed.
Chemotherapy and radiation therapy are delivered under the
oversight of that team, resulting in continuity of care. The nurse
practitioner/RN team handles follow-up calls at home to ensure
the efficacy of pain control and other medical issues, which
results in fewer emergency room visits.
BTI Clinical and Clinical Research AdministrationIn September 2005, George Lawrence, M.B.A., was appointed
Administrator of the BTI, overseeing all activities of the institute
in coordination with Dr. Gene Barnett, the Cleveland Clinic
Cancer Center, “parent” departments, Center for Clinical
Research and the Lerner Research Institute. Wendi Evanoff
manages the BTI database and Tumor Board conference, and
James Saporito coordinates philanthropic activities for the BTI.
Noreen Flowers manages the BTI’s Web site (clevelandclinic.org/
braintumor) and Martha Tobin oversees all CME activities. Kim
Blevins coordinates the Brain Tumor Fellowship Programs,
which includes two surgical and one nonsurgical program.
The BTI’s clinical research infrastructure is fully integrated with
that of the Cleveland Clinic Taussig Cancer Center’s Experimental
Therapeutics Program. All clinical protocols and correspondences
are funneled into the BTI through Kathy Robinson, the BTI Study
Coordinator, and processed through the Experimental Therapeutics
Program, including IRB submissions (e.g., protocols amendments,
safety reports), protocol budget creation, nursing assignment
and study start-up. Material is dispersed from this central resource
to all appropriate parties. The BTI has two dedicated research
nurses, Cathy Brewer and Carol Patton, who manage all clinical
trials, including patient consent, monitoring and follow-up. These
nurses are part of the Experimental Therapeutics Program and are
backed up by other Experimental Therapeutic nurses. The program
oversees and manages all regulatory matters, IRB submissions and
all data collection / CRF transcription responsibilities through the
dedicated BTI Study Coordinator.
Cleveland Clinic has recently affiliated with Case Western
Reserve University and University Hospitals of Cleveland.
This new relationship provides the opportunity to integrate
an outstanding group of cancer researchers and a large cancer
referral network at one of the nation’s most renowned hospitals
based at Cleveland Clinic, with Northern Ohio’s only National
Cancer Institute-designated Comprehensive Cancer Center
based at Case.
The Case Comprehensive Cancer Center combines, under a single
leadership structure, the cancer research activities of the largest
biomedical research and health care institutions in Ohio – Case
Western Reserve University, Cleveland Clinic and University
Hospitals of Cleveland – into a unified cancer research center.
With this integration, the Case Comprehensive Cancer Center
has strengthened its scientific programs, expanded opportunities
for disease-focused research, and enhanced access and ability
to serve the entire population of Northeast Ohio.
The Cleveland community has fully embraced this exceptional
opportunity to join the region’s two preeminent healthcare
delivery systems and Case, their academic partner, into a single
NCI-designated Comprehensive Cancer Center.
Neuro-Oncology Nursing

�� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
2) Intraoperative radiation therapy for solitary brain metastases –
Dr. Steven Toms is conducting a phase I/II study utilizing a
novel method for delivering intraoperative radiation therapy
(INTRABEAM) for the treatment of a resected solitary brain
metastasis. This method allows the precise delivery of
radiation therapy directly into the tumor cavity and allows
the patient with a solitary resectable brain metastasis to
postpone the need for whole brain radiation.
�) Radiosensitizers for metastatic disease to the brain –
The BTI remains active in using novel radiation sensitizers to
augment the effect of radiotherapy on primary and secondary
(i.e., metastatic) tumors. Dr. John Suh serves as the interna-
tional principal investigator for a large randomized trial testing
standard whole brain radiation therapy with supplemental
oxygen, with or without concurrent RSR3 (efaproxiral), in
women with brain metastases from breast cancer.
�) Intra-arterial chemotherapy with blood-brain barrier
disruption (BBBD) for primary central nervous system
lymphoma (PCNSL) and other tumors – This program, in
its fourth year, has become a mainstay of the treatment and
research of patients with PCNSL at Cleveland Clinic. The BTI
actively enrolls patients on clinical trials of the BBBD Consor-
tium. Two clinical trials are available for patients with PCNSL
(newly diagnosed and recurrent), and one is available for
patients with recurrent or progressive high-grade gliomas. Drs.
Glen Stevens and David Peereboom have played an integral
role in the clinical management of the patients undergoing the
procedures. Dr. Lilyana Angelov has developed a consortium-
wide database for the tabulation of treatment results of this
procedure for patients with PCNSL. The BTI staff has contrib-
uted to the writing of protocols for the consortium as well as
making several presentations at the consortium’s annual
meetings. Several staff members also have contributed to
publication of the proceedings from this meeting.
5) Convection-enhanced delivery of immunotoxins – This
program uses the slow, continuous infusion of an immunotoxin
(IL13-PE38QQR) targeted to recurrent malignant glioma. This
technique has the potential to deliver agents that otherwise
cannot be delivered to the brain or that are too toxic to other
organs for systemic delivery. BTI neurosurgeons are actively
enrolling patients in a clinical trial of IL13-PE38QQR for
patients with newly diagnosed GBM. Dr. Michael Vogelbaum
serves as PI for this trial.
�) Anaplastic Oligodendrogliomas – Members of the BTI have
initiated a trial with the NCI-sponsored clinical trial group
RTOG. This study, titled “A Phase II Trial of Pre-irradiation and
Clinical Protocols/ResearchBrain tumor and neuro-oncology patients may elect experimental
treatments or to participate in clinical research projects related
to their diagnosis. Various chemotherapies and growth modifiers
are among the experimental drug protocols developed by the
institute’s clinical investigators. We are proud to have active
participation in the NABTT Consortium. BTI physicians serve
as protocol chairpersons for this consortium as well as others
including RTOG and the BBBD. Patients may choose to partici-
pate in multicenter management trials from these consortia as
well as the SWOG, ACoSOG or COG.
Protocols and associated clinical programs include:
�) Erlotinib Trials – The BTI initiated a Phase II trial evaluating
erlotinib for the treatment of recurrent/progressive glioblas-
toma multiforme (GBM). Erlotinib is a selective EGFR kinase
inhibitor small molecule drug, which is used in patients with
lung and pancreas cancer. The BTI has two trials for patients
with GBM. The first trial, for patients with recurrent disease, is
being performed under an individual investigator IND assigned
to Dr. Michael A. Vogelbaum. This trial utilizes pre-operative
treatment followed by resection or biopsy followed by further
treatment, thereby providing valuable data on the activity of
the drug in the patient’s tumor. All research costs are being
absorbed by the BTI; Genentech is providing the drug at
no cost. A total of 60 patients will be enrolled in this trial.
Encouraging responses with low toxicity have been seen, and
this trial is accruing well. Another trial, directed by Dr. David
Peereboom, investigates the use of erlotinib with radiotherapy
and temozolomide for patients with newly diagnosed GBM.
The trial opened in 2004 and accrual is expected to be
complete in 2006.
A complete arrary of laboratory facilities and expertise allows us to pursue both basic science and translational research on new therapeutics
Brain Tumor Institute
Clinical Research

2005 Annual Report A team approach to individualized care �5
Concurrent Temozolomide in Patients with Newly Diagnosed
Anaplastic Oligodendrogliomas and Mixed Anaplastic
Oligoastrocytomas,” is chaired by Dr. Michael Vogelbaum;
other BTI study chairs include Dr. John Suh (Radiation
Oncology) and Dr. David Peereboom (Medical Oncology).
This study has completed accrual and the data are currently
being analyzed. Dr. Vogelbaum is involved in the development
of the next RTOG clinical trial for patients with anaplastic
gliomas. Another multicenter trial, initiated at Cleveland Clinic
by Dr. David Peereboom, also tests the use of chemotherapy
as initial management for patients with pure and mixed
anaplastic oligodendrogliomas. This trial is nearing completion.
�) Complementary and alternative medicine – Dr. Mladen
Golubic has received NIH funding for the first BTI trial of
complementary and alternative medicine. His trial, “Phase
II Randomized Evaluation of 5-Lipoxgenase Inhibition by
Dietary and Herbal Complementary and Alternative Medicine
Approach Compared to Standard Dietary Control as an
Adjuvant Therapy in Newly Diagnosed Glioblastoma Multi-
forme,” seeks to minimize brain edema in patients with GBM.
The above clinical trials represent only a portion of those studies
being offered by the BTI. A full listing of clinical trials is included
in the Appendix of this report.
Section of Metastatic DiseaseClinical Research ProjectsPhase I/II Study of Intraoperative Radiotherapy for Newly
Diagnosed Supratentorial Brain Metastasis Using the
“Photon Radiosurgery System”
Multicenter trial using a unique intraoperative radiotherapy device
(the “Photoelectic Cell”) to deliver radiotherapy after the resection
of brain metastases. Currently open and enrolling patients.
The Detection of Glial Tumor Margins and Intraoperative
Optical Spectroscopy
An intraoperative spectroscopy unit designed for the detection of
tumor margins in glial surgery. Currently in data acquisition phase
to improve probe algorithms prior to trials designed to test efficacy.
Radiation OncologyProject �. A Phase III, Randomized, Open-label, Comparative
Study of Standard WBRT w/O2 w/ or w/o RSR–13 in women
with Brain Metastases from Breast Cancer. The Sponsor is Allos
Therapeutics. IRB #6795. The Principal Investigator is Dr. John
Suh and this project is open.
Project 2. Phase II study of tamoxifen with induction of
chemical hypothyroidism as an adjunct to XRT in glioblastoma.
IRB #4473. The principal investigator was Dr. Suh and this
project closed in 2005.
Project �. A Phase III Randomized Study of Radiation and
Temozolomide (IND #60,265) vs. Radiation Therapy & BCNU
for Anaplastic Astrocytoma and Mixed Anaplastic Oligoastrocy-
toma. The Sponsor is RTOG. IRB #3939. The Principal
Investigator is Dr. John Suh and this project is open.
Project �. Prospective study on the short-term adverse effects
from Gamma Knife radiosurgery (IRB #8078). Principal
investigator is Dr. Suh and this study is open.
Project 5. Prospective analysis of wellness for patients with non-
malignant conditions (IRB #7992). Principal investigator is Dr.
Suh and this project is open.
Dr. Suh’s primary clinical activities focus on the use of radiation
therapy and Gamma Knife radiosurgery to treat adult and
pediatric patients with benign and malignant brain tumors.
The radiation modalities used include external beam radiation
therapy, intensity-modulated radiation therapy (IMRT), image-
guided radiation therapy (IGRT), Gamma Knife radiosurgery
and brachytherapy. In addition to brain tumor patients, Dr. Suh
also sees patients with vascular and functional disorders such as
AVM and trigeminal neuralgia who are treated with the Gamma
Knife. Dr. Suh also sees an assortment of other patients in the
Department of Radiation Oncology as the need arises.
Dr. Suh’s clinical research activities focus on enrolling patients
onto various cooperative group, in-house and pharmaceutical-
sponsored studies. He serves as the principal investigator for an
international Phase III study for women who develop brain metas-
tases from breast cancer. This trial uses an allosteric modifier of
hemoglobin, efaproxiral, to enhance oxygen delivery to hypoxic
regions. This is a confirmatory study based on the REACH study,
which he served as co-principal investigator. Dr. Suh also directs
the research efforts for the RTOG and serves as the principal
investigator for Cleveland Clinic, which is one of RTOG’s 32 full-
member institutions and was the 11th leading enroller in 2005.
Dr. Suh serves on the steering committee for the brain tumor
section of RTOG. Over the past year, he has written and
collaborated on multiple manuscripts with residents in Radiation
Oncology and Neurosurgery. He also gave numerous national
and international presentations regarding his research.
Dr. John Suh serves as the Principal Investigator on the
following IRB-approved databases:
Glioblastoma multiforme registry (IRB 6852)
Acoustic neuroma registry (IRB 6988)
Brain metastases registry (IRB 6989)
Low-grade glioma registry (IRB 6990)
Pituitary adenoma registry (IRB 6991)
Meningioma registry (IRB 7044)
Heterotopic bone registry (IRB 7045)
Gamma Knife radiosurgery patient list (IRB 7068)
Clinical Medical OncologyDr. David Peereboom’s activities related to the Brain Tumor
Institute have comprised approximately three fourths of his
clinical efforts, the remainder being connected to attending on

�� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
the inpatient services of the Hematology/Oncology Teaching
Service, Consultation Service and non-BTI outpatient activities.
His clinical trial activity has included authorship and study
chair for three multicenter trials:
1) Continuous Dose Temozolomide in patients with Anaplastic
Mixed and Pure Oligodendrogliomas. This trial involves nine
centers and is the first multicenter trial authored and conduct-
ed by the Cancer Center. To date, 55 of 60 planned patients
have entered the study.
2) BMS 247550 in Recurrent High-grade Gliomas for NABTT.
This trial completed accrual in November 2005 with a
manuscript in preparation.
3) Erlotinib and Sorafenib in Recurrent High-grade Gliomas
for NABTT. This trial will open in 2006.
4) Phase I / II Pilot Study of Patients with Brain Metastasis
Secondary to Breast Cancer Treated with Methotrexate and
Carboplatin in Conjunction with BBBD, with Concurrent
Trastuzumab in HER-2 Postitive Patients for Blood-Brain
Barrier Disruption Consortium. This trial will open in 2006.
In addition, another trial, titled “Erlotinib/temozolomide/radiation
therapy for patients with newly diagnosed glioblastoma” has been
activated, and 25 of 30 planned patients have been enrolled. Dr.
Peereboom has also been active in accrual and management of
patients on in-house clinical trials (e.g., Erlotinib for recurrent
GBM), NABTT trials (Talampanel with radiation/temozolomide for
newly diagnosed GBM; EMD121974 with radiation/temozolomide
for newly diagnosed GBM; Sorafenib for recurrent GBM) BBBD
Consortium trials, and RTOG trials (e.g., RTOG 9402).
Another area of active clinical and investigative work is with the
Blood-Brain Barrier Consortium. Dr. Peereboom is the Director of
the Blood-Brain Barrier Disruption program and has been active
as an attending physician for procedures and post-procedure
inpatient care of patients receiving intra-arterial chemotherapy
with or without BBBD. In addition, he has consulted for the
BBBD Consortium in the development of trials and will serve
as co-principal investigator on an upcoming breast cancer brain
metastasis trial.
Clinical Neuro-OncologyDr. Glen Stevens is the Section Head of Adult Neuro-Oncology
at the BTI and provides longitudinal management as well as
consultative services. He is co-PI of the Cleveland Clinic’s NIH-
supported NABTT program and manages day-to-day medical
activities in NABTT trials, along with research personnel in the
institute and Cleveland Clinic Cancer Center. He is active in
SWOG as well as the Blood-Brain Barrier Consortium. He also
was the local principal investigator on the GO (Glioma Outcomes)
project. Dr. Stevens often participates in the brain tumor support
group and also has an interest in the diagnosis and treatment of
neurofibromatosis in adults.
Pediatric Neuro-OncologyDrs. Bruce H. Cohen and Joanne Hilden lead the Pediatric and
Adolescent Brain Tumor Program. Dr. Cohen is an internationally
known pediatric neuro-oncologist. He is active in many clinical
research activities including serving as Chairman of CCG-99703C
Infant Brain Tumor Study, Children’s Cancer Group; Chairman
of Low-Grade Astrocytoma Discipline Committee, Children’s
Oncology Group; a member of the Brain Tumor Strategy
Committee, Children’s Oncology Group; and a member of
the Professional Advisory Board, The Gathering Place.
Dr. Hilden, Chair of Pediatric Oncology, participates in two brain
tumor committees for the Children’s Oncology Group (high-grade
primitive neuro-ectodermal tumors, and CNS teratoid/rhabdoid
tumors (AT/RT)).
There are 12 ongoing protocols for brain tumors open for
pediatric brain tumor patients, including a protocol for Atypical
Teratoid / Rhabdoid tumors, a very rare and aggressive pediatric
tumor. A national registry for children diagnosed with Atypical
Teratoid / Rhabdoid tumor (AT/RT) has been established by Dr.
Joanne Hilden. The registry, which collects therapy data and
outcomes, can be accessed from our Children’s Hospital Web site
at clevelandclinic.org/childrenshospital. The registry site includes
references and information about AT/RT and how to register
patients. A manuscript reporting therapy and outcomes of the
registry was published in the Journal of Clinical Oncology. Three
protocols for biology studies that collect brain tumor specimens
for molecular and cytogenetic studies are open.
The departments of Pediatric Hematology/Oncology and Pediatric
Neurology hold a combined pediatric brain tumor clinic every
Tuesday and Thursday in the Pediatric Hematology/Oncology
area. A multidisciplinary team provides evaluation, treatment
and continuing care for children and adolescents diagnosed with
tumors of the brain or spinal cord.

2005 Annual Report A team approach to individualized care ��
Dr. Gene Barnett, Chairman of the Brain Tumor Institute,
and Dr. Robert Weil serve as co-directors of Neuro-oncology
Research. Current tumor research focuses on several areas
including molecular genetics, apoptosis, engineering,
immunology, progenitor cells and the blood-brain barrier.
Dr. Weil, Associate Director of Basic Laboratory Research,
currently is directing research in proteomics in one of the four
primary Brain Tumor Institute labs. Prior to his joining
Cleveland Clinic, he collaborated with Cleveland Clinic neurosur-
geon Steven A. Toms, M.D., M.P.H., on proteomics research.
Although the field of proteomics is still in its infancy, the BTI is
committed to pursuing this field of research.
The members of the Weil laboratory focus on four discrete areas,
including work on identifying novel genes and targets in
gliomagenesis; using new technologies, such as novel navigation
systems for brain navigation and brain tumor imaging and high-
throughput proteomics methodologies; identifying novel
mechanisms that promote metastasis of systemic cancers to the
central nervous system (CNS); and developing novel methods to
identify and characterize microRNA targets. The following
paragraphs detail the work carried out in the past year with
relevant publications published or in press:
�. Gliomas and Glioblastomas.Li et al, details our continuing work in protein profiling of brain
tumors. This is very time consuming, laborious work, one tumor
at a time, but is very rewarding in terms of getting greater
understanding of how these tumor may develop, progress, and
respond to therapy, especially with respect to finding new targets.
PLOS Medicine paper is a review of Glioblastomas (GBMs) and
an editorial on a new method developed in the lab that shows
Brain Tumor Institute
Laboratory Research
Implantable osmotic pumps are used to deliver drugs to the brain
potential promise. Years of testing by this group and others will
lie ahead, but it is very interesting. Dr. Weil was honored to be
invited to write this review.
Zeng et al describes one of the proteins that we have identified in
protein profiling, aurora B, which appears to be a marker of more
aggressive GBMS. We are looking a greater numbers of tumors
now to see if this remains true in a larger series, but it is very
provocative.
Li J, Zhuang Z, Akimoto H, Vortmeyer AO, Park DM, Furuta
M, Lee YS, Oldfield EH, Zeng W, Weil RJ. Proteomic profiling
distinguishes astrocytomas of increasing malignancy and
identifies differential tumor markers. Neurology 66: 733-736,
2006. [PMID: 16534112]. Supplemental material is available
at:http://www.neurology.org/cgi/content/full/66/5/733/DC1.
Vogel TW, Zhuang Z, Vortmeyer AO, Furuta M, Lee YS, Zeng W,
Oldfield EH, Weil RJ. Protein and protein pattern differences
between glioma cell lines and glioblastoma multiforme. Clinical
Cancer Research, 11: 3624-3632, 2005. [PMID: 15897557]
Schwartz SA, Weil RJ, Thompson RC, Shyr Y, Moore JH, Toms SA,
Johnson MD, Caprioli RM. Proteomic-based prognosis of brain
tumor patients using direct-tissue MALDI mass spectrometry.
Cancer Research, 65: 7674-7681, 2005. [PMID: 16140934].
Weil, RJ. Glioblastoma Multiforme – Treating a Deadly Tumor
with Both Strands of RNA. PLoS Med. 2006 Jan;3(1):e31.
Epub 2005 Dec 6. No abstract available. [PMID: 16323974].
Zeng W, Navaratne K, Prayson RA, Weil RJ. Aurora B expres-
sion correlates with aggressive behavior in glioblastoma
multiforme. In press, J Clin Pathol, 2006
2. Using novel technologyWith colleagues at Vanderbilt, who developed the system, we have
been able to demonstrate that a simple, inexpensive, portable
system, laser range scanning, can be used to assess, in real time,
brain shift and deformation in the operating room setting.
Toms et al and Lin et al, which are collaborations with the Toms
lab here at CCF, describes the utility of optical spectroscopy
systems, another unique and simple method to use visible light
to identify individual tumor cells, and avoid normal brain cells
and white matter, which may help guide us to more extensive but
safer surgical procedures.
Sinha TK, Miga MI, Cash DM, Galloway RL, Weil RJ. Intraopera-
tive cortical surface characterization using laser-range scanning:
preliminary results. In press, Neurosurgery, 2006.
Sinha TK, Dawant BM, Duay V, Cash DM, Weil RJ, Thompson
RC, Weaver KD, Miga MI. A method to track cortical surface

�� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
deformations using a laser range scanner. IEEE Transactions on
Medical Imaging, 24: 767-81, 2005. [PMID: 15959938]
Toms SA, Lin WC, Weil RJ, Johnson MD, Jansen ED, Mahadevan-
Jansen A. Intraoperative optical spectroscopy identifies infiltrating
gliomas margins with high sensitivity. Neurosurgery 57 [ONS
Suppl 3]: 382-291, 2005. [PMID: 16234690].
Lin WC, Mahadevan-Jansen A, Johnson MD, Weil RJ, Toms SA.
In vivo optical spectroscopy detects radiation damage in brain
tissue. Neurosurgery, 57: 518-525, 2005. [PMID: 16145531]
�. Brain metastasis, especially from breast cancerAnother interest is the development of metastasis to the central
nervous system, especially from breast cancer. Weil et al is a
review article that serves as a state-of the art review to provide
some background for this problem. About 200,000 new cases of
breat cancer develop yearly in the United States, and from10-15%
of these patients will be expected to develop a brain metastasis.
In some subgroups, such as women who over-express the HER-2
receptor, the risk may be 2-3 times greater than the average.
However, one of the difficulties is that at present, it is usually only
after the CNS metastasis has developed that these lesions are
treated. However, recently, as we have outlined in a new article
by Hicks et al, we have identified a new set of markers—found in
the original breast cancer--that may be a useful tool in finding out
which women are more likely to develop a brain metastasis. This
marker, cytokeratin 5/6, in association with basaloid features
histologically, is the strongest marker yet identified.
Weil RJ. CNS Metastases. In: Sid Gilman, Editor-in-chief,
Neurobiology of Disease, San Diego: Elsevier, 2006.
Weil RJ, Palmieri D, Bronder JL, Stark AM, Steeg PS. Breast
cancer metastasis to the central nervous system. American
Journal of Pathology, 167: 913-920, 2005. [PMID: 16192626]
Weil RJ, Lonser RR. Selective Excision of Metastatic Brain
Tumors Originating in the Motor Cortex with Preservation of
Function. Journal of Clinical Oncology, 23: 1209-17. 2005.
[PMID: 15718318]
Hicks DG, Short SM, Prescott NL. Tarr Sm, Coleman KA, Yoder
BJ, Crowe JP, Choueiri TK, Dawson AE, Pettay J, Budd GT,
Tubbs RR, Seitz R, Ross D, Weil RJ. Breast cancers with brain
metastasis are more likely to be estrogen receptor negative,
express the basal cytokeratin CK 5/6 and over-express HER2 and
EGFR. In press, American Journal of Surgical Pathology, 2006.
�. microRNA and mRNA.Finally, in Vatolin et al., we describe a new area of interest,
micro RNA. This paper describes a potentially novel and
universal method to figure out how these micro RNAs work
and influence normal RNA function.
Micro RNAs (miRNAs) are a unique class of small, non-coding
RNA gene whose final product is an approximately 22 nucleotide
(nt) functional RNA molecule. They appear to be critical regulators
of numerous targets genes. miRNAs act in at least one of two
ways: by binding complimentary sites on target mRNAs to induce
cleavage or by repressing translation from the target mRNAs. Over
the past fifteen years it has become increasingly evident that
these and other small RNAs exert an additional layer of gene
control beyond the traditional regulators. In 1993, two groups
found that a small RNA identified in the nematode C. elegans, lin-
4, regulated another gene, lin-14, through direct interactions with
lin-4 mRNA. Since then, investigations have revealed a rich
tapestry of short RNA activities, which suggests that miRNAs
play a potentially vast and pivotal role in the regulation of many
eukaryotic genes, with diverse effects in apoptosis, development,
gene imprinting, metabolism, and tumorigenesis. For example,
miRNAs are believe to constitute at least 1% of the genes in
animals; are highly conserved across a wide range of species; and
mutations in the proteins required for miRNA genesis and function
impair normal development or are lethal.
In spite of their ubiquity, exact functions have been ascribed to
only a handful of the hundreds of known miRNAs. At first, most
miRNAs were identified by arduous cloning and sequencing efforts.
Beyond the complexity of the methods, low-abundance species or
those found in only a specific cell type were difficult to character-
ize. Several bioinformatics approaches have been developed to
predict novel miRNAs. Complimenting these techniques, additional
bioinformatics methods were created to validate the predictions
and to identify potential mRNA targets. However, unlike in plants,
where larger and more individually distinctive miRNA hairpin
precursors are made (which bind their targets with near-perfect
complimentarity), bio-informatic prediction models for eukaryotic
miRNAs and their targets have proven less informative.
To overcome some of these barriers, we recently developed a
novel method that detects intact miRNA-mRNA complexes in
eukaryotic cells. First, we use reverse transcription of cytoplas-
mic extract to increase the length of a miRNA by extending it
with cDNA on the template of a target mRNA. This step
minimizes non-specific annealing in a second round of reverse
transcription, which in turn creates cDNA molecules (“miRNA
signatures”) of 12-14 nucleotides in length, long enough for
sequencing and analysis. The miRNA molecules we detect have
been confirmed in miRNA database searches and are functional.
Vatolin S, Navaratne K, Weil RJ. A novel method to detect
functional miRNA targets. Journal of Molecular Biology 358(4):
983-996, 2006. [PMID: 16564540.]
Most recently, Brain Tumor Institute laboratory researchers
have conducted groundbreaking genomics work focused on the
molecular basis of chemotherapy resistance in gliomas, which
has led to the development of a number of clinically useful
diagnostic tests for brain tumor patients. Ongoing basic
research involves the study of three novel genes in pediatric and
adult brain tumors and the development of an implantable
optical spectroscopy unit to provide clinicians with immediate
feedback on the efficacy of chemotherapy.

2005 Annual Report A team approach to individualized care ��
Role of Optical Nanocrystals (Quantum Dots) in
Molecular and Cancer Imaging – Quantum dots are
optical nanocrystals whose use in in vitro and in vivo
molecular imaging is exploding. In comparison with
organic fluorophores, quantum dots exhibit desirable
properties such as multi-wavelength fluorescence
emission, excellent brightness and resistance to
photobleaching. Their electron-dense metallic cores
suggest they may have utility in computed tomogra-
phy as well as optical imaging. Coreshell zinc sulfide-
cadmium selenide quantum dots were studied in
magnetic resonance and computed tomography
phantoms. In addition, the Qdots were injected
into rat brain using convection-enhanced delivery,
intravenously to co-localize with rat brain tumor
models, and studied with CT and MRI. Data suggests
that current formulations of Qdots are phagocytized
by macrophages and co-localize with brain tumors
in vivo after IV injection. Phantoms and CED imaging
of animals show that Qdots may be imaged with CT,
but not MRI, suggesting that quantum dots have the
potential to function as multimodal imaging platforms
in vivo.
Steven Toms, M.D., directs the Section of Metastatic
Disease for the BTI and devotes the majority of his
clinical operating time on intraoperative monitoring,
awake craniotomy techniques and intraoperative
ultrasound.
Current translational research involves identifying and developing
new compounds that are directed against targets relevant to
malignant gliomas.
Center for Translational Therapeutics“Translating Novel Therapies for Malignant Brain Tumors from the Bench to the Bedside”The cornerstone of the BTI is the Center for Translational
Therapeutics. Directed by Dr. Michael Vogelbaum, aggressive
preclinical testing of the most promising anticancer agents is
under way. One goal of the center is to accelerate the lengthy
and expensive process of testing new drugs targeted against
brain tumors and to safely move them into clinical trials as
quickly as possible, for the benefit of patients.
Physicians, researchers and scientists involved in this center
work with both pharmaceutical companies and other medical
institutions to identify, obtain and test new compounds. The
center’s multi-million dollar efforts, including an international
search for all potential brain tumor-relevant therapies, have
yielded several promising agents for testing.
Testing of new agents involves evaluating the toxicity and efficacy
of these compounds in the laboratory and in animals that have
brain tumors. In addition, we also are investigating the optimal
route of delivery of these drugs.
Because many new therapeutic agents cannot penetrate the
central nervous system, center researchers are exploring
alternative delivery methods. In addition to investigating the
efficacy of oral delivery, researchers evaluate the efficacy of the
agents when delivered intracerebrally – directly into the brain –
via a specialized neurosurgical technique called convection-
enhanced delivery (CED).
The staff of the center is focused on translating these preclinical
results into Phase I and II clinical trials – giving the brain tumor
patient more therapeutic treatment options by broadening the
horizon of potential tools we may use to manage this deadly disease.
The CTT has started research projects with a number of pharmaceu-
tical and biotechnology companies, ranging in size from small
startup firms to some of the largest publicly traded companies.
What these companies have in common are novel drugs that are
close to or are in clinical trial and which are rationally designed to
be effective against malignant gliomas given the molecular and
genetic makeup of these tumors. These drugs are targeted against
molecules such as EGFR, VEGFR, Fas/Apo2, mTOR/Akt, Jak/STAT3
and Raf-1 kinase. Our first translational clinical trial is with Tarceva/
OSI-774, a selective EGFR kinase inhibitor small molecule drug.
CTT Staff Include:Director: Michael A. Vogelbaum, M.D., Ph.D.
Project Scientist: Baisakhi Raychaudhuri, Ph.D.
Technical Assistant: Hamid Daneshvar
Section of Metastatic Disease“Optical Adjuncts to Brain Tumor Therapy” NAD(P)H Autofluorescence in Cell Death – NADH and
NAD(P)H are pyridine nucleotides that function as electron
donors in oxidative phosphorylation. The pyridine nucleotides
also function as antioxidants in mitochondria and serve as major
intracellular fluorophores in their reduced states. Our long-term
goal is to design optical sensors to gauge the effectiveness of
chemotherapeutic drugs by measuring changes in NAD(P)H
fluorescence. We hypothesize that NAD(P)H fluorescence
declines prior to apoptotic cell death. We have observed that
1) the NAD(P)H fluorescence emission peak from UV wavelength
excitation is lost during a variety of insults, including hyperther-
mia, sodium azide poisoning and chemotherapy; 2) mass
spectrometry of cell lysates treated with chemotherapy shows
NAD(P)H losses that parallel cellular fluorescence declines; and
3) the decline in cellular fluorescence precedes nuclear conden-
sation and cell viability loss during apoptosis. Based upon these
observations, we are submitting grants to examine the role of
NAD(P)H in apoptosis, focusing upon changes in fluorescence
signal that may be used to detect cell and tissue viability.

20 Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
Molecular Genetics and Molecular Neuro-OncologyDr. Olga Chernova leads or participates in projects one through
five, while Dr. Mladen Golubic does so for projects six and seven.
Project �. Genetic alterations and biological characterization of
primary cell cultures derived from malignant gliomas. The initial
objectives of this project were a) finding conditions for establish-
ing short-term primary cultures from glial tumors that would
serve as a model for studies of glial tumors; b) establish a
method for fast and reliable evaluation of homogeneity of tumor
culture that would allow monitoring of culture content in different
growth conditions since variable contamination with normal cells
represented a problem. In a course of the work, we found that
modified medium used for propagation of normal neural stem
cells allow selective isolation of tumor cells in primary culture.
A genotyping assay was established, which allows semi-quantita-
tive evaluation of the homogeneity of the cultures. The growing
interest to the role of the stem cells in tumorigenesis prompted
a characterization of the origin and differentiation status of the
cultured tumor cells in collaboration with Dr. Robert Miller. Using
a set of antibodies detecting several neural stem cells markers, at
least two types of glioma cultures, which may potentially originate
from different pools of the neural stem cells, have been identified.
Analysis of tumorigenic potential of these primary tumor cultures
in nude mice is in progress.
Growing interest in stem cells in brain tumors resulted in two
collaborative projects with Cleveland Clinic researchers: (1) a
collaboration with Dr. Gregory Plautz to develop a vaccine for
brain tumors resulted in submission of RO1 NIH proposal; (2)
a collaboration with Drs. Jaharul Haque and Michael Vogelbaum
to study signal transduction pathways and gene expression in
brain tumor stem cells.
Project 2. Genetic alterations in GBMs (loss or gain of ��q, �p
and other novel alterations) and their correlations with patient
survival. Several recently published initial observations indicate
that numerical alterations in chromosomes 1p and 19q may be
predictive of clinical response or survival of patients with GBM.
To confirm and expand these initial observations, well-controlled
groups of 34 patients with newly diagnosed GBMs treated at
Cleveland Clinic and demonstrated either long (>20 months) or
short (between three and nine months) survival were selected.
Ten LOH markers distributed along 1p arm and 4 markers along
19q arm were used. Preliminary data indicate that both types of
allelic imbalance, loss or gain, of 1p and/or 19q could be found
in GBM tumors and occur in both groups of patients. However,
to complete this study, the same tumors should be analyzed
using FISH or multiplex PCR techniques to discriminate true
losses of chromosomes from their gains. Forty percent of the
specimens were analyzed by FISH at the Molecular Pathology
lab. The rest of the specimens are currently studied using
multiplex PCR assays for 1p and 19q. A recently developed
MLPA technique for multiplex PCR analysis of 1p/19q is being
used. This part of the study is in progress.
As an extension of this project, Drs. Chernova, Weil (BTI) and
Wigler (Cold Spring Harbor Laboratory) collaborated. Dr. Wigler
developed a high-density microarray-based comparative genomic
hybridization assay for analysis of numerical alterations in
genomic DNA. Using a set of six DNAs from long-term and
short-term surviving patients with GBM, preliminary data
was obtained that indicates the assay is extremely sensitive
and was able to identify novel regions of alterations.
Project �. Development of a clinical assay for detection of
deletions in CDKN2A, ARF, PTEN and p5� genes in gliomas.
We have developed a semi-quantitative assay for detection of
gene deletions based on multiplex PCR. The goal of the project
is development, validation and introduction of this prognostic
assay to the clinical laboratory. This assay will also be impor-
tant for the “Genotyping Arrays” project as a part of validation
of the array data.
Project �. Genotyping arrays as a prognostic tool: glioma
model. This project is a collaboration with Cleveland BioLabs
and the microarray manufacturing company Nimblegen. The aim
of the project is to develop a genotyping microarray-based assay
that will identify alterations in chromosome copy number and
allelic imbalances in critical chromosomal regions, as well as
mutations in genes that have prognostic significance in glial
tumors and predict response to therapy. Amended STTR
proposal had been resubmitted to the NIH in October 2005.
Project 5. Distinct alteration of chromosome �p in astrocytic
and oligodendrocytic tumors. The extent of 1p deletion in low-
and high-grade gliomas using LOH analysis was characterized.
The results indicate that oligodendroglial tumors almost uniformly
demonstrate very large deletions of 1p arm. Conversely, GBMs
have only partial deletions affecting the terminal part of 1p. This
data indicate that (1) only large deletions on 1p are associated
with positive prognosis (need to perform more statistical
analysis), and (2) partial 1p deletions in GBM are not associated
with positive prognosis (see also GBM survival project).
Project �. Role of Eicosanoids in Glioblastoma Tumorigenesis.
Eicosanoids are special type of fats produced in the human
body from diet-derived fats by the action of enzymes called
cyclooxygenases (COX-1 and COX-2) and lipoxygenases.
We have determined that 5-lipoxygenase (5-LO), an enzyme
that stimulates inflammation, is aberrantly overexpressed in
malignant brain tumors, anaplastic astrocytoma and GBM.
The two main interconnected aspects of this project are (1)
to investigate the expression of other eicosanoid enzymes of
the 5-LO pathway in the GBM tumor tissue and measure
eicosanoids in the blood of patients with GBM; and (2) to
explore novel ways to inhibit 5-LO and COX-2, the two main pro-
inflammatory enzymes that are aberrantly overexpressed in GBM.
To inhibit 5-LO, we are examining the use of Boswellic acids.

2005 Annual Report A team approach to individualized care 2�
Boswellic acids are naturally found in the gum resin exudate from
the Boswellia serrata (frankincense) tree. The herbal preparation
from B. serrata will be used in combination with a low-fat diet as
an adjuvant therapy for patients with GBM in a clinical study (see
Project 6. Molecular characterization of genes that are modulated
by Boswellic acids in GBM cells currently is in progress. The
levels of eicosanoids are measured not only in blood of patients
with GBM, but also in tumor tissue specimens that were surgically
removed. The goal of this collaborative study with Dr. Robert
Newman from the MD Anderson Cancer Center is to correlate
levels of eicosanoids in tumor tissue and blood with clinical
outcomes of patients with GBM.
To suppress the aberrantly overactive COX and 5-LO enzymes in
GBM cells, we are investigating the potential anticancer effects of
an anti-inflammatory herbal preparation (Zyflamend, by New
Chapter, Inc.). It consists of standardized extracts from 10 different
spices (including turmeric, ginger, rosemary and oregano) and
medicinal herbs. We have shown that Zyflamend induces
programmed cell death of GBM cells in vitro and inhibits produc-
tion of eicosanoids in surgically removed GBM tissue specimens.
This work is done in collaboration with Dr. Newman’s laboratory
and is supported by the research grant from New Chapter, Inc.
Recently, we identified more than 150 genes that are either
induced or suppressed in expression when GBM cells are treated
with Zyflamend. Currently, the functional significance of two of
those genes is being investigated further. The obtained results
were presented at the Annual Research Conference of the
American Institute for Cancer Research in Washington, D.C., in
July 2005, and at the 2nd International Conference of the Society
for Integrative Oncology in San Diego, Calif., in November 2005.
Project �. 5-Lipoxygenase Inhibition as an Adjuvant Glioma
Therapy A two-year clinical study supported by a grant from
the National Institutes of Health is currently in progress.
This study builds on knowledge obtained in this laboratory and
from clinical experience by German investigators. The primary
objective is to determine whether a suppression of pro-inflamma-
tory enzymes, including 5-LO, by a combination of an herbal
formulation and a diet can reduce brain swelling caused by GBM.
As brain swelling often causes symptoms, possible effects on
quality of life and survival of patients with GBM will also be
examined. Patients with a newly diagnosed GBM after surgical
removal of the tumor and radiation therapy will be randomly
assigned to two groups. The patients in the intervention group
will use a B. serrata herbal preparation (containing naturally
occurring inhibitors of 5-LO enzyme) in combination with a low-fat
vegan diet as an adjuvant to their main treatment. The control
group will eat a diet according to the guidelines by the American
Cancer Society, also as an adjuvant to their main treatment.
Molecular Biology of Brain Tumors Dr. Andrei Gudkov has established a facility aimed at identifica-
tion of molecular targets and development of target-based
therapies for treatment of brain cancer, based on an integrated
technological platform that includes: 1) gene target identification
based on the combination of novel functional genomic approach-
es with global gene expression profiling and advanced bioinfor-
matics and 2) identification of bioactive compounds with the
desired properties, using small molecule screening facility,
followed by pharmacological optimization of primary hits.
Dr. Gudkov is applying the established technology pipeline to the
generation of a genetic database and identification of candidate
genes associated with brain tumor development and progression,
with specific focus on tumor suppressor genes, drug sensitivity/
resistance genes and diagnostic markers. The aims of this work
are to: 1) identify and test prospective therapeutics among secreted
or membranal protein products of identified disease-specific genes;
2) develop high throughput technology of isolation of new anticancer
therapeutics by screening chemical libraries for prospective gene-
or pathway-specific drugs based on the discovered genes; and 3)
develop diagnostic assays that will grade tumor type and stage
of progression, facilitate selection of optimal therapy, provide an
accurate and reliable prognosis, and initiate a broad program of
clinical validation based on the selected combinations of candidate
disease-specific genes. This effort has already resulted in identifica-
tion of two prospective anticancer treatment molecular targets
that are currently being used for small molecule screening. A small
molecule inhibitor of multidrug resistance with a new mechanism
of activity associated with MRP1 and other multidrug transporters,
4H10, capable of sensitizing glioma cells to a variety of anticancer
agents has been isolated.
The initial stages of this project were funded by a Finding the
Cures for Glioblastoma Award and by the Technology Action
Fund of Ohio Award.
Blood-Brain Barrier, Tumor Markers and Human Gliomas Project Previous attempts in this and other laboratories have failed to
achieve growth of a variety of malignant brain tumors consis-
tently in vitro, perhaps due to the non-physiological conditions
that traditional tissue culture provides. We are attempting to
grow malignant brain tumors (oligodendroglioma and glioblas-
toma) under so-called “dynamic conditions” in a 3-D tissue
culture apparatus where glia-endothelial co-culturing promotes
the establishment of a physiologic blood-brain barrier. When
a blood-brain barrier is formed, we position either solid or
disassociated tumors in the abluminal chamber in direct
proximity to normal glia (astrocytes). We will initially study the
ability of these human tumors to grow under dynamic conditions.
Genotyping and tumor mass determinations will be used to evalu-
ate similarity of growth patterns in vitro vs. in vivo. We also
propose to examine direct vs. indirect drug resistance of the
tumor by injecting chemotherapeutic agents either directly into
the abluminal site or intraluminally, where a blood-brain barrier
separates the “blood compartment” from the brain tumor itself.

22 Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
Another focus of this laboratory is to determine the role of S100
as a potential tumor marker. We are examining changes in S100
level with blood-brain barrier disruption and its correlation with
metastatic and glioma tumor burden. Related projects by Dr. Yan
Xu are examining phospholipid antibodies as a potential tumor
marker. Other markers of deranged p53 mechanisms and small
molecule modulators of blood-brain barrier function are evaluated
by Dr. Andrei Gudkov.
Immunology and Immunotherapy
New approaches are requisite if malignant gliomas are to be
treated successfully. Immunotherapy is an attractive approach in
this disease; however, this form of treatment has not been very
successful clinically. Growing evidence suggests that the poor
response to immunotherapy is likely due to the inability of current
therapeutic approaches to adequately reverse immune suppres-
sion. It is been well-documented that patients with gliomas are
characterized by systemic immune dysfunction, as demonstrated
by impaired cell-mediated immunity, lymphopenia and inability
Table �. Members of the Division of Pathology and Laboratory Medicine Actively Participating in Molecular Neuropathology
Project as of 9/30/05.
NeuropathologistsRichard Prayson, M.D. Specimen diagnosis. Validation of immunohistochemistry reagents Susan Staugaitis, M.D., Ph.D. Specimen diagnosis. Liaison among Pathology Laboratories and Clinicians for Molecular
Neuropathology test development and interpretation. Maintenance of Pathology Glioma Database. Consultant for BTI database.
MolecularGenetic PathologistsRaymond Tubbs, D.O. Director of Molecular Genetic Pathology Laboratory. Supervision of FISH. Review
of FISH results with technologists.Supervision research and development of array- based hybridization assays.
Ilka Warshawsky, M.D., Ph.D. Supervision DNA extraction, PCR based assay development, review of validated PCR based assays.
Gary W. Procop, M.D., Review of FISH results with technologists. James R. Cook, M.D., Marek Skacel, M.D.
Molecular Pathology TechnologistsJames Pettay, M.T. (ASCP), Supervisor, CLIA Compliance Molecular Genomic Laboratory
Marybeth Hartke, B.S., M.T.(ASCP) Development and validation of FISH Assays. Performance of FISH analyses
Kelly Simmerman, M.T. (ASCP), Performance of FISH analyses Karen Keslar, M.S., Rosemary Neelon, B.S.
Tissue Procurement TechnologistsJessica Krimmel, B.S., Transport and processing of blood and tissues from OR. Communications Barbara Bekebrede, B.S., with BTI Specimen Bank Technologists. Jessica Roman, B.S., Carrie Nedbalski
Immunohistochemistry TechnologistsGloria Willis-Eppinger, H.T.(ASCP) Lab Coordinator
Renata Klinkosz, B.S., M.T., Sectioning blocks for immunohistochemistry and genotyping, development and performance of Kathy Maresco, B.S., M.T.(ASCP), immunohistochemistry assays Michelle Wayman, B.S., H.T.(ASCP), Derek Mangalindan, B.S., M.T.
Reference LaboratoryMary Ann Kannenberg, B.S., M.T.(ASCP) Manager, Laboratory Services
(Reference Laboratory).
Kathy Leonhart, Client Services (Marketing)
Laboratory Information SystemsDale Duca Lead Systems Analyst. Contact for development of mechanisms for ordering and reporting test
results in CoPath, transfer to hospital information systems (LastWord, Epic, searches of CoPath for transfer of info to BTI database.

2005 Annual Report A team approach to individualized care 2�
Table 2: Summary of Molecular Genotyping Tests available during Reposting
Period 10/1/04 – 9/30/05.
Test Target specimens Status of test
FISH for 1p/19q All gliomas “FISH for 1p/19q” ordered as a single procedure within CCF and through CCF Reference Laboratory. 1p and 19q may also be ordered individually.
EGFR FISH High grade gliomas Orderable clinical test within CCF and through CCF Reference Laboratory. Tests are also performed on low grade gliomas of CCF patients and billed to research accounts.
1p LOH by PCR Performed upon request to characterize, Orderable clinical test within CCF and through CCF in greater detail, genetic alterations on Reference Laboratory. Chromosome 1p
19q LOH by PCR Performed upon request to characterize, CCF Technical Validation nearly completed. in greater detail, genetic alterations Two tests performed. on Chromosome 19q
TP53 sequencing Upon request on selected anaplastic Orderable clinical test within CCF and through CCF (exons 5-8) oligodendrogliomas. Immunohistochemistry Reference Laboratory. for p53 (>50% of cells positive) is predictive of mutation in most cases.
Table �. Numbers of Molecular Genotyping tests performed by Specimen Class*.
Specimen Class FISH FISH FISH �p LOH ��q LOH TP5� SEQ Totals for �p for ��q for EGFR** by PCR by PCR
Routine Surgical 83 83 73 3 2 0 244 (SX)
Surgical Outside 11 11 5 0 0 0 27 Review (SO)
Surgical Reference 11 7 2 0 0 0 20 Lab Consult (SRC)
Procedure Only 106 106 0 1 0 0 213 (PRS)
Totals 2�� 20� �0 � 2 0 50�
* Specimen Classes SX and SO are patients treated by BTI Physicians.** Numbers to not include approximately 13 tests performed on low grade gliomas of CCF patients and billed to research accounts.
680 surgical procedures were performed in 2005

2� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
to mount delayed-type hypersensitivity reaction. Indeed some
of the immune suppression is likely related to the fact that a
higher percentage of T cells from glioma patients are undergoing
apoptosis as compared to T cells from healthy individuals. It is
important at this time to not only focus on boosting the immune
response to GBM but also to include a second arm in the
therapeutic strategy that will prevent the immune cells from
undergoing tumor-induced immune suppression. Previously we
showed that GBMs mediate immune suppression via promoting
T-cell death through receptor-dependent and receptor-indepen-
dent apoptotic pathways.
Recently we reported that gangliosides produced by GBM
lines contribute to the induction of T-cell apoptosis, since the
glucosylceramide synthase inhibitor PPPP significantly reduced
the abilities of all four GBM apoptogenic lines to kill lymphocytes
(Chahalvi A, et al. Cancer Research 2005). HPLC and mass-
spectroscopy demonstrated that GM2, GD3 and GD1a were
expressed by all four apoptogenic GBM-lines, but not by the two
GBMs lacking activity. The expression of GM2, GD3, GD2 and
GM1 has been recently demonstrated by immunostaining of
GBM lines with antibodies specific for each of these gangliosides.
To define the relative contribution that each of these gangliosides
makes to the tumor-induced killing of T cells, antibodies specific to
each of the gangliosides were added to co-culture of T cells and
CCF-52 cells. The antibodies or isotype control Ig was added at
the beginning of the cultures. These studies revealed that anti-
GM2 antibody was most effective at blocking T cell apoptosis,
while anti-GM1 displayed modest activity, and antibodies to GD2
and GD3 were ineffective. Thus, GM2 expressed by CCF-52 plays
an important role in promoting T-cell apoptosis. These studies are
being repeated using the other GBM lines, CCF4 and U87.
Additional supporting data demonstrating that GM2 is apopto-
genic for T cells was provided by transfecting CCF-52 tumor
cells with siRNA for GM2 synthase. Such treatment causes a
significant reduction in the expression of GM2 that is observed
within 24 hours and lasts for over 72 hours. RT-PCR analysis of
mRNA from these transfected cells revealed that messenger RNA
for GM2 synthase was reduced within 12 hours, with optimal
suppression occurring at 48 hours. The reduction in GM2 expres-
sion following transfection with siRNA for GM2 synthase was
selective since there was no decrease in the expression levels
of GM1 and GD3. Most important, the loss of GM2 expression
coincided with a reduction (50 percent) in the ability of CCF-52
to induce apoptosis in normal T lymphocytes. Similar studies are
planned for the other GBM lines.
Recent findings suggest GM2, which is produced by the CCF-52
cell line, is shed into the supernatant, where it can then bind T
cells. Immunofluorescence staining with anti-GM2 antibodies
demonstrated that T cells from normal individuals do not express
detectable GM2. However, after a one- to two-day incubation of
these T cells with conditioned medium from cultured CCF-52
cells, GM2 was detected by anti-GM2 antibody staining. The
expression of GM2 coincided with the appearance of apoptosis in
the T cells exposed to CCF-52 supernatant but not T cells cultured
in media alone. Similar findings were observed when T cells from
normal donors were co-cultured with a monolayer of CCF-52 cells.
We are now interested in analyzing T cells from GBM patients to
determine whether a portion of these cells are GM2 positive and
whether the presence of GM2+ T cell correlates with increased
levels of GM2 in patient plasma and with T-cell apoptosis.
We are currently testing whether the iron chelator/antioxidant
desferoxamine (DFO) is able to protect T cells in rats that bear the
syngenic transplantable tumor, S635. Previously, we showed that
in vitro DFO can protect T-cells from apoptosis induced by isolated
GBM gangliosides and GBM cell lines by 45 to 85 percent. New
studies show that administration of DFO via an implantable pump
can significantly reduce the percentage of apoptotic T cells that are
present in the peripheral blood and tumor. We are in the process
of testing whether DFO administration will enhance the antitumor
activity of adoptively transferred T cells derived from the draining
lymph nodes of S636-bearing mice.
Cerebrovascular Research Center Dr. Damir Janigro leads the Cerebrovascular Research Center
in cooperation with Dr. Luca Cucullo.
Alternating current electrical stimulation enhanced chemotherapy:
a novel strategy to bypass multidrug resistance in tumor cells.
BMC Cancer. 2006 Mar 17;6(1):72 PMID: 16545134
Tumor burden can be pharmacologically controlled by inhibiting
cell division and by direct, specific toxicity to the cancerous tissue.
Unfortunately, tumors often develop intrinsic pharmacoresistance
mediated by specialized drug extrusion mechanisms such as P-
glycoprotein. As a consequence, malignant cells may become
insensitive to various anticancer drugs. Recent studies have shown
that low intensity, very low frequency electrical stimulation by
alternating current (AC) reduces the proliferation of different tumor
cell lines by a mechanism affecting potassium channels while
intermediate frequencies interfere with cytoskeletal mechanisms of
cell division. The aim of the present study is to test the hypothesis
that permeability of several MDR1 over-expressing tumor cell lines
to the chemotherapeutic agent doxorubicin is enhanced by low
frequency, low intensity AC stimulation.
We grew human and rodent cells (C6, HT-1080, H-1299, SKOV-
3 and PC-3), which over-expressed MDR1 in 24-well Petri
dishes equipped with an array of stainless steel electrodes
connected to a computer via a programmable I/O board.
We used a dedicated program to generate and monitor the
electrical stimulation protocol. Parallel cultures were exposed
for three hours to increasing concentrations (1, 2, 4, and 8 m)
of) M doxorubicin following stimulation to 50 Hz AC (7.5 mA)
or MDR1, inhibitor XR9576. Cell viability was assessed by
determination of adenylate kinase (AK) release. The relationship
between MDR1 expression and the intracellular accumulation

2005 Annual Report A team approach to individualized care 25
of doxorubicin as well as the cellular distribution of MDR1
was investigated by computerized image analysis immunohisto-
chemistry and Western blot techniques.
By using a variety of tumor cell lines, we show that low frequen-
cy, low intensity AC stimulation enhances chemotherapeutic
efficacy. This effect was due to an altered expression of intrinsic
cellular drug resistance mechanisms. Immunohistochemical,
Western blot and fluorescence analysis revealed that AC not only
decreases MDR1 expression but also changes its cellular distribu-
tion from the plasma membrane to the cytosol. These effects
synergistically contributed to the loss of drug extrusion ability
and increased chemosensitivity.
In the present study, we demonstrate that low frequency, low
intensity alternating current electrical stimulation drastically
enhances chemotherapeutic efficacy in MDR1 drug-resistant
malignant tumors. This effect is due to an altered expression
of intrinsic cellular drug resistance mechanisms. Our data
strongly support a potential clinical application of electrical
stimulation to enhance the efficacy of currently available
chemotherapeutic protocols.
Surgical EngineeringWork in this area was led by Dr. Barnett and Eric LaPresto
and focused on two areas: (1) Development of a brain image
processing program capable of fusing up to 64 sets of images
(CT, MRI, PET, DTI, etc) and correlating location and intensity of
any given point (voxel) over time. This program has moved into
frequent clinical use to fuse low-resolution imaging (such as PET)
with MRI, as well as new modalities such as MR and CT blood
volume imaging. It also has proved useful showing trends in
tumor size over time. (2) Ongoing development of the BTI
research/clinical database – a secure repository of clinical
information, imaging, pathology and results of molecular
investigations in a Web-accessible, IRB-approved format.
IL-�� Induction of Glioma ApoptosisDr. Martha Cathcart directs work in this laboratory that has been
defining the relevant IL-13 receptors in several cell types and
identifying the downstream signal transduction cascades. Her lab
is interested in understanding the IL-13-mediated induction of
apoptosis, the regulation of IL-13 signal transduction pathways
and the regulation by receptor composition. To date Dr. Cath-
cart’s laboratory has identified the heterodimeric receptor
molecules, IL-13Ra1 and IL-4 receptor. They associate with
activated Jak family members, Jak2 and Tyk2. These tyrosine
kinases then phosphorylate Stats 1, 3, 5 and 6. Stats 1 and 3
are also phosphorylated on serine 727 in an IL-13-dependent
manner. Recent studies indicate the Stat serine phosphorylation
is regulated by both p38 MAP kinase as well as PKCd. Her
laboratory is interested in understanding the alternative signal
transduction pathways utilized in normal cells versus glioblas-
toma cells to further understand IL-13 induction of apoptosis.
Recent data indicate the existence of a novel signalosome
complex that is induced by IL-13 and contains Src kinase, p38
MAP kinase, PKCd and Stat3. Each of these molecules has been
shown to be required for 15-lipoxygenase expression, which
appears to regulate apoptosis.
Molecular Pathology of Gliomas: “Glioma Genotyping”Reporting period: 10/1/04 through 9/30/05
During the past reporting period, it was decided that the initiative
for development of tests for possible translation into the clinical
laboratory would begin in the research labs of the BTI. Once the
research laboratories concluded that a specific test was feasible
on biopsy and surgical specimens, and the clinicians indicated
that the results of such tests would be used in treatment
planning, Dr. Susan Staugaitis would bring the test proposal to
the clinical laboratory for prioritization in their test implementa-
tion schedule and assist in coordinating efforts for technical
validation, ordering and reporting.
Several improvements for glioma genotyping ordering and execution
have occurred in the past reporting period. All glioma genotyping
tests are now ordered directly within the Pathology Information
System, CoPATH. This streamlines the process and permits
retrieval of test information for annual reports and other operational
purposes. Microdissection of samples for DNA extraction and LOH
was transferred to the technologists in the Immunohistochemistry
Laboratory. This laboratory performs the microdissection for colon
cancer microsatellite analysis by the same techniques as the glioma
specimens and permits adequate volume to maintain expertise in
the technique by several technologists.
Transcription Factors and Brain Tumors Dr. Michael Vogelbaum directs work in this laboratory. Patients
with malignant gliomas continue to have a very poor prognosis
despite multiple new approaches to their treatment. In particular,
most of these tumors are resistant to DNA-damaging treatments,
including radiation therapy and most standard forms of chemo-
therapy. A growing body of evidence supports the hypothesis that
aberrant activation of key transcription factors is critical for the
development and progression of these tumors. A greater under-
standing of the biology of these transcription factors should help
us develop new, more effective therapeutic modalities.
In collaboration with Dr. Jaharul Haque, Institute’s Department
of Cancer Biology, we have found two transcription factors,
STAT3 and NF-kB, which are aberrantly constitutively activated
in malignant gliomas. Activation of these transcription factors
results in resistance to chemotherapy and/or radiation therapy,
and stimulates tumor cell invasion. The mechanisms underlying
constitutive activation of these transcription factors are being
actively investigated, and we are investigating methods to
reverse the biological effects mediated by these factors.
Together we have received a research grant from the National
Cancer Institute and additional submissions are planned.

2� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
Paper Published or In PressBatra PS, Citardi MJ, Lee JH, Bolger W, Roh HJ, Lanza DC. Endoscopic resection of sinonasal malignancies: A preliminary Report. Am J of Rhinology. 2005. In press.
Batra PS, Citardi MJ, Worley S, Lee JH, Lanza DC. Resection of anterior skull base tumors: Comparison of combined traditional and endoscopic techniques. Am J of Rhinology 2005; 19:521-528.
Chahlavi A, Rayman P, Richmond AL, et al. Glioblastomas Induce Apoptosis of T Lymphocytes By Two Distinct Pathways Involving Gangliosides and CD70. Cancer Research 2005; 65(12):5428-38.
Chahlavi A, Staugaitis SM, Yahya R, Vogelbaum MA. Intracranial collision tumor mimicking an octreotide-SPECT positive and FDG-PET negative meningioma. J Clin Neurosci 2005; 12(6):720-3.
Chao ST, Lee SY, Borden LS, Joyce MJ, Krebs VE, Suh JH. External beam radiation helps prevent heterotopic bone formation in patients with history of heterotopic ossification. J Arthroplasty 2005. In press.
Chao ST, Joyce MJ, Suh JH. Treatment of heterotopic ossification. Orthoped 2005. In press.
Chen PG, Lee SY, Barnett GH, Vogelbaum MA, Saxton JP, Fleming PA, Suh JH. Use of the RTOG RPA classification system and predictors for survival in 19 women with brain metastases from ovarian cancer. Cancer 2005. In press.
Chen PG, Lee SY, Barnett GH, Vogelbaum MA, Saxton JP, Fleming PA, Suh JH. Use of the Radiation Therapy Oncology Group recursive partitioning analysis classification system and predictors of survival in 19 women with brain metastases from ovarian carcinoma. Cancer 2005; 104(10):2174-80.
Cohen BH. Altered States of Conscious-ness. In: Maria BL. Current Management in Child Neurology, 3rd Edition. BE Decker, Hamilton, Ontario, Canada. 2005; 551-562.
Cohen BH. Mitochondrial Cytopathies. In: Maria BL. Current Management in Child
Neurology, 3rd Edition. BE Decker, Hamilton 2005; 551-562.
Doolittle ND, Abrey LE, Blyer WA, et al. New frontiers in translational research in neuro-oncology and the blood-brain-barrier: report of the tenth annual blood-brain barrier consortium meeting. Clinical Cancer Research 2005; 11:421-8.
Dreicer R, Byzova T, Plow E, Klein E, Peereboom D, Elson P. Phase II trial of GM-CSF + thalidomide in patients with androgen-independent metastatic prostate cancer. Urol Oncol 2005; 23:82-6.
Farag E, Deboer G, Cohen BH, Niezgoda J. Metabolic acidosis due to propofol infusion. [comment]. Anesthesiology. 2005; 102(3):697-8.
Farray D, Ahluwalia M, Cohen B, et al. Pre-irradiation 9-Amino [20s] camptoth-ecin (9-AC) in patients with newly diagnosed glioblastoma multiforme. Invest New Drugs. 2005 Aug 2.
Fritz M, Sade B, Wood B, Lee JH. Benign fibrous histiocytoma of the pterigopala-tine fossa with intracranial extension. Acta Neurochirurgica date. 2005 Feb 25. In press.
Hartsell WF, Scott CB, Watkins Bruner D, et al. Phase III randomized trial of 8 Gy in 1 fraction vs. 30 Gy in 10 fractions for palliation of painful bone metastases: Analysis of RTOG 97-14. J Natl Ca Inst 2005. In press.
Hughes G, Lee JH, Ruggieri P. Cystic lesions of the petrous apex. In: Clinical Otology, 3rd Edition (Hughes & Pensak, editors). Thieme, NY, 2005. In press.
Kanner AA, Staugaitis SM, Castilla EA, et al. The Impact of Genotype on the Outcome in Oligodendroglioma: Validation of the loss of chromosome arm 1p as a factor of importance in clinical decision making. J Neurosurgery. March 2006. In press.
Kanner A, Vogelbaum M. Intraoperative MRI. In Computer Assisted Neurosurgery. Barnett GH, Robert D, Maciunas R, eds. 2005. In press.
Kelly TW, Prayson RA, Barnett GH, Stevens GHJ, Cook JR, Hsi ED. Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue arising
in the lateral ventricle: case report and literature review. American J of Surg Path. 2005. In press.
Komaki R, Swan R, Ettinger DS, et al. Phase I study of thoracic radiation dose escalation with concurrent chemotherapy for patients with limited small cell lung cancer: Report of Radiation Therapy Oncology Group (RTOG) Protocol 97-12. Int J Radiol Oncol Biol Phys 2005; 62:342-350.
Latif T, Wood L, Connell C, et al. Phase II Study of Oral Bis (aceto) Ammine Dichloro (cyclohexamin) Platium (IV) (JM-216, BMS-182751) given Daily x 5 in Hormone Refractory Prostate Cancer. Invest New Drugs 2005; 23:79-84.
Lee JH, Evans JJ, Steinmetz MP, Krishnaney AA. Surgical Technique for Removal of Clinoidal Meningiomas. In: Badie B, ed. Neurosurgical Operative Atlas, 2nd ed. Neuro-Oncology. Thieme, NY: 2005. In press.
Lee JH, Krishnaney AA, Steinmetz MP, Lee DK. Intracranial Meningiomas. In: Barnett GH, ed. Computer-Assisted Neuro-surgery. 2005. In press.
Lee JH, Steinmetz M, Krishaney A, Lee DK. Intracranial Meningiomas. In: Barnett G, Roberts D, Maciunas R, eds. Computer-Assisted Surgical Navigation in Neurosur-gery. 2005. In press.
Lee JH, Sade B, Choi E, Prayson R, Golubic M. Midline skull base and spinal meningiomas are predominantly of the meningothelial histologic subtype. J Neurosurgery. In press.
Lee JH, Tobias S, Kwon, JT, Sade B, Kosmorsky G. Wilbrand’s knee: Does it exist? Surgical Neurology. In press.
Lin WC, Mahadevan-Jansen A, Weil RJ, Johnson M, Toms SA. Intraoperative optical spectroscopy accurately distin-guishes radiation necrosis versus recurrent tumor in vivo. Neurosurgery. In press.
Lin WC, Mahadevan-Jansen A, Johnson MD, Weil RJ, Toms SA. In vivo optical spectroscopy detects radiation damage in brain tissue. Neurosurgery, 57:518-525, 2005.
Lo SS, Chang EL, Suh JH. Stereotactic radiosurgery with and without whole-brain
Brain Tumor Institute
Publications

2005 Annual Report A team approach to individualized care 2�
radiotherapy for newly diagnosed brain metastases. Expert Rev Neurotherapeu-tics. 2005; 5(4):487-495.
Lonser RR, Buggage R, Weil, RJ. Malignant cerebellar swelling in a patient with neuro-Behçet’s disease. J Neurosur-gery: Pediatrics. 2005;103: 292.
Mahelas TJ, Lee JH. Neurosarcoidosis: A cause of compressive, infiltrative optic neuropathy. Ocular Surgery News. 2005; 23 (18):64-66.
Mangels KJ, Johnson MD, Weil RJ. Thoracic intermediate-grade melanocy-toma mimicking meningioma. Brain Pathology. 2005. In press.
Mason A, Toms SA, Hercbergs A. Biological Response Modifiers. In: Barnett GH, ed. Malignant Gliomas. 2005. In press.
Moulder S, Johnson D, Toms SA. Metastatic breast cancer. In: Sawaya R ed. Intracranial Metastases: Current Manage-ment Strategies. Armonk; NY: Futura Publishing Co. In press.
Nathoo N, Cavusoglu M, Vogelbaum M, Barnett G. In Touch with Robotics: Neurosurgery for the future. Neurosurgery. March 2005; 56(3):237-242.
Nathoo N, Chalavi A, Barnett GH, Toms SA. Pathobiology of Brain Metastasis. Journal of Clinical Pathology. 2005; 58:237-42.
Nathoo, N, Lautzenheiser F, Barnett GH. George W. Crile, Ohio’s First Neurosur-geon, and his relationship with Harvey Cushing. Journal Neurosurgery. 2005; 103: 378-386.
Nathoo N, Prayson R, Bodnar J, Vargo L, et al. 5-Lipoxygenase is Overexpressed in High-Grade Astrocytomas. Neurosurgery. May 2005. In press.
Nathoo N, Steiner C, Barnett G, Roberts D. Surgical Navigation System Technolo-gies. In: Barnett G, Roberts D, Maciunas R, Peereboom DM, eds. Computer-Assisted Neurosurgery. Chemotherapy in Brain Metastases. Neurosurg Suppl. Nov 2005.
Nathoo N, Nair D, Phillips M, Vogelbaum MA. Mapping prosody: correlation of functional magnetic resonance imaging with intraoperative electrocorticography recordings in a patient with a right-sided temporooccipital glioma. Case illustration. J Neurosurg. 2005; 103(5):930.
Pack SD, Qin LX, Pak E, Wang Y, Ault DO, Mannan P, Jaikumar J, et al. Common
genetic changes in hereditary and sporadic pituitary adenomas detected by compara-tive genomic hybridization (CGH). Genes, Chromosomes, and Cancer. 2005; 43(1):72-82.
Quan AL, Barnett GH, Lee SH, Vogelbaum MA, Toms SA, Staugaitis SM, Prayson RA, et al. Epidermal Growth Factor Receptor Amplification Does Not Have Prognostic Significance In Patients With Glioblastoma Multiforme. International Journal of Radiation Oncology. June 1, 2005.
Rahaman SO, Vogelbaum MA, Haque SJ. Aberrant Stat3 Signaling by Interleukin-4 in Malignant Glioma Cells: Involvement of IL-13R{alpha}2. Cancer Research. 2005; 65(7):2956-63.
Rahaman SO, Vogelbaum MA, Haque SJ. Aberrant Stat3 Signaling by Interleukin-4 in Malignant Glioma Cells: Involvement of IL-13R (alpha)2. Cancer Research. 2005; 65(7):2956-63.
Robinson CG, Prayson RA, Hahn JF, Kalfas IH, Whitfield MD, Lee SY, Suh JH. Long-term survival and functional status of patients with low-grade astrocytomas of the spinal cord. Int J Radiat Oncol Biol Phys. 2005; 63:91-100.
Sade B, Evans JJ, CY Kweon, Lee JH: Enhanced carotico-oculomotor triangle following anterior clinoidectomy: an anatomic morphometric study. Skull Base Surgery. 2005; 15: 157-162.
Sade B, Lee JH: Outcome following meningioma surgery: A personal series of 600 cases. Meningiomas. Springer-Verlag, London. In review.
Sade B, Lee JH, Lee DK. Postoperative psychosis and depression following removal of a giant skull base hemangio-pericytoma. Surgical Neurology. In press.
Sajja R, Barnett GH, Lee SY, Stevens GHJ, Lee J, Suh JH. Intensity-modulated radiation therapy (IMRT) for newly diagnosed and recurrent intracranial meningiomas: the Cleveland Clinic Foundation experience. Technol Cancer Res Treat. December 2005; 4(6): 675-682.
Schwartz SA, Weil RJ, Thompson RC, et al. Proteomic-based prognosis of brain tumor patients using direct-tissue MALDI mass spectrometry. Cancer Research. 2005; 65:7674-7681. (co-senior author).
Sinha TK, Dawant BM, Duay V, et al. A method to track cortical surface deforma-tions using a laser range scanner. IEEE
Transactions on Medical Imaging. 2005; 24:767-81.
Siomin V, Barnett G. Brain Biopsy and Related Procedures. In: Barnett G, Roberts D, Maciunas R., eds. Computer Assisted Neurosurgery. 2005. In press.
Siomin, V., Angelov, L., Liang, L.,Vogelbaum, M.A. Results of a Survey of Neurosurgical Practice Patterns Regarding the Prophylactic Use of anti-EpilepsDrugs in Patients with Brain Tumors. J. Neurooncol. 2005 Sep; 74(2):211-5.
Solares CA, Fakhri S, Batra PS, Lee JH, Lanza DC. Trans-nasal endoscopic resection of lesions of the clivus: a preliminary report. Laryngoscope. 2005; 115:1917-1922.
Song JK, Weil RJ. An unusual cause of acromegaly. Archives of Pathology & Laboratory Medicine. 2005; 129:415-416.
Spencer A, Lee JH, Prayson RA. Optic nerve choristoma: A case report and review of the literature. Ann. of Diagnostic Path. 2005; 9:348-354, 2005.
Steinmetz MP, Krishnaney AA, Lee DK, Lee JH. Convexity Meningiomas. In: Badie b, ed. Neurosurgerical Operative Atlas 2nd Edition. Neuro-Oncology. New York; NY: Thieme 2005. In press.
Stevens G. General Consideration. In: Barnett GH. High-grade Gliomas. Totowa; NJ: Humana Press. 2005. In press.
Stevens GHJ. Antiepileptic Drug Use in Patients with Brain Tumors. Profiles in Seizure Management. 2005; 4:4-9.
Stevens GHJ. Antiepileptic therapy in patients with central nervous system malignancies. In: Lesser G, ed. Current Treatment Options in Oncology. 2005. In press.
Suh JH, Stea B, Nabid N, et al. Results from a phase 3 study evaluating efaproxi-ral as an adjunct to whole brain radiation therapy for the treatment of patients with brain metastases. J Clin Oncol. 2005. In press.
Tobias S, Kim CH, Kosmorsky G, Lee JH. Clinoidal Meningiomas. Surgical Manage-ment. 2005. In press.
Tobias S, Kim CH, Sade B, Lee JH. Benign neuromuscular choristoma of the trigeminal nerve in an adult. Acta Neurochir. 2005. In press.
Toms SA, Lin WC, Weil RJ, Johnson MD, Jansen ED, Mahadevan-Jansen A.

2� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
Intraoperative optical spectroscopy identifies infiltrating gliomas margins with high sensitivity. Neurosurgery. 2005; 57 [ONS Suppl 3]: 382-291.
Ugokwe K, Nathoo N, Prayson R, Barnett GH. Trigeminal nerve schwannoma with ancient change. Journal Neurosurgery. 2005; 102;1163-1165.
Vogel TW, Brouwers FM, Lubensky IA, et al. Differential expression of erythropoietin and its receptor in von Hippel-Lindau-associated and MEN type 2-associated pheochromocytomas. Journal of Clinical Endocrinology and Metabolism. 2005; 90:3747-3751.
Vogel TW, Zhuang Z, Vortmeyer AO, et al. Protein and protein pattern differences between glioma cell lines and glioblastoma multiforme. Clinical Cancer Research. 2005; 11:3624-3632.
Vogelbaum MA. Convection-enhanced Delivery for the Treatment of Malignant Gliomas: Symposium Review. Journal of Neuro-oncology. 2005; 73(1):57-69.
Vogelbaum MA, Masaryk T, Mazzone P, et al. S100beta as a predictor of brain metastases. Cancer. 2005; 104(4):817-24.
Weil RJ, Lonser RR, Quezado MM. Skull and brain metastasis from tibial osteosar-coma. J Clinical Oncology. 2005; 23:4226-4229.
Weil RJ, Lonser RR. Selective Excision of Metastatic Brain Tumors Originating in the Motor Cortex with Preservation of Function. Journal of Clinical Oncology. 2005; 23:1209-17.
Weil RJ, Palmieri D, Bronder JL, Stark AM, Steeg PS. Breast cancer metastasis to the central nervous system. American Journal of Pathology. 2005; 167:913-920.
Books Barnett, GH, Maciunas R, Roberts D, eds. Computer-Assisted Neurosurgery. Ontario, Canada; BC Decker Publishing Co; 2005. In preparation.
Barnett GH, ed. High Grade Gliomas: Diagnosis and Treatment. Totawa, NY; Humana Press. 2005, In preparation.
Prayson, RA, Angelov, L, Barnett, GH. Mixed Neuronal-Glial Tumors. In: Berger, MS, Prados, M.D., eds. Textbook of Neuro-Oncology Philadelphia, PA; Elsevier Saunders; 2005: 222-226.
Book Chapters Barnett GH. Image-Guided Needle Biopsy. In: Advanced Techniques in Image-Guided Brain and Spine Surgery. Thieme Publisher. 2005. In press.
Barnett GH. Intraoperative MRI. Contem-porary Neurosurgery. Baltimore, MD: Williams & Wilkins. 2005. In press.
Barnett GH. Barnett GH, ed. Surgical Techniques. In: High Grade Gliomas: Diagnosis and Treatment. Totawa, NJ: Humana Press. 2005. In preparation.
Barnett GH. Molecular Classifications. In: High Grade Gliomas: Diagnosis and Treatment. Barnett GH, ed. Totawa, NJ: Humana Press. 2005. In preparation.
Barnett GH. Image-Guided Surgery. In: Neurosurgical Oncology. Black P, ed. Totawa, NJ: Humana Press. 2005. In preparation.
Cohen B. Altered States of Consciousness In: Maria BL, ed. Current Management in Child Neurology. 3rd Ed. Ontario, Canada: BE Decker, Hamilton; 2005: 551-562.
Cohen B, Nicholson C. Brainstem Gliomas. In: Schiff D, O’Neill BP, eds. Principles of Neuro-Oncology. New York, NY: McGraw-Hill; 2005: 333-342.
Cohen B. Mitochondrial Cytopathies. In: Maria BL, ed. Current Management in Child Neurology. 3rd Ed. BE Decker, Hamilton; 2005: 277-284.
Prayson R, Angelov L, Barnett GH. Mixed Neuronal-Glial Tumors. In: Berger M, Prados M, eds. Textbook of Neuro-Oncology. Philadelphia, PA: Elsevier Saunders; 2005: 30: 222-226.
Siomin V, Barnett GH. Brain Biopsy and Related Procedures. In: Barnett GH, Maciunas R, Roberts D, eds. Computer-Assisted Neurosurgery. Ontario, Canada: BC Decker, Hamilton; 2005. In preparation.
Suh JH, Barnett GH. Radiosurgery. In: Barnett GH, ed. High Grade Gliomas: Diagnosis and Treatment. Totawa, NJ: Humana Press; 2005. In preparation.
Vogelbaum M and Kanner A. Intraopera-tive MRI. In: Barnett G, Maciunas R, Roberts D, Marcel Dekker, eds. Computer-Assisted Neurosurgery. New York, NY: Inc. Publishers; 2005. In press.
Vogelbaum M and Siomin V. Image-guided Treatment of Metastatic Brain Tumors. In: Barnett G, Maciunas R, Roberts D, eds. Computer-Assisted Neurosurgery. New York, NY: Marcel Dekker Inc. Publishers; 2005. In press.
Abstracts Angelov L. The use if tissue equivalent Super Stuff Bolus ™
material to treat skull metastases with Gamma Knife Radiosurgery. 7th Interna-tional Stereotactic Radiosurgery Society Congress: Poster Presentation. Brussels, Belgium; September 2005.
Angelov L. Blood Brain Barrier Disruption and Intra-Arterial Methotrexate theray for Primary CNS Lymphoma: The Cleveland Clinic Experience. 2005 Congress of Neurological Surgeons Annual Meeting: Talk & Poster Presentation. Boston, MA; Oct 2005.
Brewer CJ, Suh JH, Stevens GHJ, et al. Phase II trial of erlotinib with temozolo-mide and concurrent radiation therapy in patients with newly-diagnosed glioblastoma multiforme. J Clin Oncol. June 1, 2005; 23(16):130S-130S Part 1 Suppl. S.
Chao ST, Barnett GH, Toms SA, et al. Salvage Stereotactic Radiosurgery Effectively Treats Recurrences from Whole Brain Radiation Therapy. ASTRO, 2005.
Fleseriuu M, Weil RJ, Prayson, Hamrahian AH. Lack of significant immunostaining for growth hormone in patients with acro-megaly. Poster presented at: 7th International Pituitary Conference, June 2005, San Diego, CA. Selected for endocrinology fellow’s research award.
Haut JS, Klaas PA, Cohen BH. Cognitive Decline in a 10-Year-Old with MELAS: Regression or Developmental Plateau? The Clinical Neuropsychologist. 2005.
Peereboom DM, Brewer C, Schiff D, et al. Phase II multicenter study of dose-intense temozolomide in patients with newly diagnosed pure and mixed anaplastic oligodendroglioma. Neuro-Oncol. 2005; 7:401. (Abstract 470)
Peereboom D, Carson K, Lawson D, Lesser G, Supko J, Grossman S for The New Approaches to Brain Tumor Therapy Consortium. A phaseI/II trial of BMS-247550 for patients with recurrent high-grade gliomas. Proc Am Soc Clin Oncol. 2005; 23:129s. (Abstract 1563)
Pineyro M, Makdissi A, Hamrahian AH, et al. Poor correlation of serum alpha subunit with postsurgical pituitary MRI in patients with nonfunctional pituitary adenomas: The Cleveland Clinic Experience. Poster presented at: Endocrine Society, 87th Annual Meeting; June 2005; San Diego, CA.

2005 Annual Report A team approach to individualized care 2�
Usmani A, Makdissi A, Hamrahian A, Reddy S, Weil R, et al. Hypothalamic-pituitary-adrenal axis testing using a twenty-five microgram Cotrosyn stimula-tion test. American Academy of Clinical Endocrinologists 2005 Annual Meeting.
Weil R, DeVroom, Vortmeyer A, et al. Adeomas confined to the neurohypophysis in Cushing’s Disease. Endocrine Society 87th Annual Meeting; June 2005; San Diego, CA.
Presentations Barnett GH. Gamma Knife Planning, Stereotactic Frame Application, Gamma Knife Shot Strategy, AVM Planning, Wizard Software. Cleveland Clinic Gamma Knife Course, Cleveland, OH; Jan 2005.
Barnett GH. Surgery for Gliomas. Cleveland Clinic Neuro-oncology Sympo-sium, Lake Buena Vista, FL; Jan 2005.
Barnett GH. Moderator: Gliomas II. Cleveland Clinic Neuro-oncology Sympo-sium, Lake Buena Vista, FL; Jan 2005.
Barnett GH. Stereotactic Frame Applica-tion, Introduction to Planning System, Gamma Knife Shot Strategy, Functional Planning and Procedures, AVM Planning. Cleveland Clinic Gamma Knife Course, Cleveland, OH; April 2005.
Barnett GH. Practical Course 386/387: Non-Invasive Preoperative and Intraopera-tive Brain Mapping. American Association of Neurological Surgeons Annual Meeting, New Orleans, LA; April 2005.
Barnett GH. Moderator: Scientific Session I: Tumors, American Association of Neurological Surgeons Annual Meeting, New Orleans, LA; April 2005.
Barnett GH, Nathoo N, Lautzenheiser F. Crile: Ohio’s First Neurosurgeon and his relationship to Harvey Cushing. American Association of Neurological Surgeons Annual Meeting, New Orleans, LA; April 2005.
Barnett GH. Stereotactic Navigation, Cleveland Clinic Neurosurgery Resident Lecture; May 2005.
Barnett GH. Stereotactic Frame Applica-tion, Introduction to Planning System, Gamma Knife Shot Strategy, AVM Planning. Cleveland Clinic Gamma Knife Course, Cleveland, OH; June 2005.
Lee DK, Lee JH. Surgical management of tentorial meningiomas. Oral presentation: Korean Skull Base Society Annual Meeting, Seoul, Korea; December 2005.
Lee, JH. Grand Skull base surgery: basic principles: Invited Lecture: Grand Rounds, Interdisciplinary Skull Base Surgery Conference, Cleveland Clinic, Cleveland, OH; January 2005.
Lee, JH. Unique features of meningothelial meningiomas. Invited Lecture: Cleveland Clinic Neuro-Oncology Symposium, Orlando, Florida; January 2005.
Lee, JH. Meningiomas: When and when not to operate?: Invited Lecture: Mayfield Clinic/Cleveland Clinic Neuroscience Symposium, Snowmass, CO; February 2005.
Lee, JH. Twelve years of skull base surgery: the lessons learned. Invited Lecture: Mayfield Clinic/Cleveland Clinic Neuroscience Symposium, Snowmass, CO; February 2005.
Lee, JH. When and when not to operate?: Invited Lecture: Grand Rounds, Interdisci-plinary SBS Conference, Cleveland Clinic, Cleveland, OH; March 2005.
Lee JH, Sade B, Park BJ. A novel ‘CLASS’ algorithm for patient selection in menin-gioma surgery. Oral presentation: The 7th Congress of the European Skull Base Society. Fulda, Germany; May 2005.
Peereboom DM. Hematology Oncology Associates Grand Rounds State of the Art Treatment Approaches for Brain Metasta-ses. Syracuse, NY; January 2005.
Peereboom DM. Palliative Medicine Grand Rounds Multidisciplinary Management of Brain Metastases: State of the Art 2005. Cleveland, OH; January 2005.
Peereboom DM. University of Utah Neurosciences Grand Rounds New Strategies in Primary Brain Tumors. Salt Lake City, UT; April 2005.
Peereboom DM. Failure of Chemotherapy for Brain Tumors: Focus on Drug Delivery and Drug Resistance Chemotherapy for High-Grade Gliomas: Pitfalls and Possibilities. Cleveland, OH; March, 2005.
Peereboom DM. Cleveland Clinic International Neuro-oncology Symposium. Role of Chemotherapy in High-grade Gliomas. Cleveland, OH; August, 2005.
Peereboom DM. Cleveland Clinic Neuro-oncology Symposium: Current Concepts Emerging Medical Therapies for High-grade Gliomas: Where do we stand and where are we going?. Orlando, FL; January 2005.
Peereboom DM. Cleveland Clinic NeuroOncology 2005: Current Concepts.
Clinical Trials of NABTT (New Approaches to Brain Tumor Therapy) Consortium. Orlando, FL; January 2005.
Peereboom DM. World Federation of Neuro-Oncology. Phase II multicenter study of dose-intense temozolomide in patients with newly diagnosed pure and mixed anaplastic oligodendroglioma. Edinburgh, UK; May 2005.
Peereboom DM. Cleveland Clinic Taussig Cancer Center ASCO Review. CNS Malignancies. Cleveland, OH; June 2005.
Peereboom DM. The Human Epidermal Growth Factor Receptor as a Target for Therapy of Solid Tumors. Akron, OH; January 2005.
Peereboom DM. Schering-Plough Oncology North America Temodar Investigator Advisory Board Meeting .Alternative Dosing Regimens for Temo-zolomide: Do they work? Atlanta, GA; February 2005.
Peereboom DM. Schering-Plough Oncology North America Temodar Investigator Advisory Board Meeting. Temozolomide for Newly Diagnosed Pure and Mixed Anaplastic Oligodendroglioma.Atlanta, GA; February 2005.
Peereboom DM. St. Luke’s Medical Center Cancer Conference
“The Human Epidermal Growth Factor Receptor as a Target for Therapy of Solid Tumors” Madison, WI; February 2005.
Peereboom DM. Blood-Brain Barrier Consortium Meeting. State of the Art Treatment Approaches for Brain Metasta-ses. Portland, OR; March 2005.
Peereboom DM. Cleveland Metro General Hospital Oncology Speaker Series. Management of Primary Brain Tumors: 2005. Cleveland, OH; April 2005.
Peereboom DM. Gliadel Wafer Investigator Meeting. Chemotherapy for Brain Metastases: State of the Art 2005. Miami, FL; June 2005.
Peereboom DM. Glioblastoma Multiforme: The Multidisciplinary Approach to Treatment. Cleveland, OH; September 2005.
Peereboom DM. Glioblastoma Multiforme: The Multidisciplinary Approach to Treatment. Peioria, IL; November 2005.
Peereboom DM. Blood-Brain Barrier Consortium Meeting. Treatment of CNS Metastases – Summary Discussion. Portland, OR; March 2005.

�0 Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
Peereboom DM. Blood-Brain Barrier Consortium Meeting. Conflict of Interest Management and Policy Development for the Blood-Brain Barrier Consortium. Minneapolis, MN; September 2005.
Prayson R, Barnett GH. Current Concepts in the Diagnosis of Gliomas. United States & Canadian Academy of Pathology Annual Meeting. San Antonio, TX; March 2005.
Sade B, Lee JH. Clinoidal meningiomas: Surgical outcome in 41 patients. Oral presentation, Annual Meeting, NASBS, Toronto, ON Canada; April 2005.
Suh JH. Advances in Pituitary Radiothera-py. Pituitary update conference. Lake Buena Vista, FL; Jan 2005.
Suh JH. Moderator for new therapeutic approaches for brain tumors. Cleveland Clinic Neuro-oncology Symposium. Lake Buena Vista, FL; Jan 2005.
Suh JH. Moderator for complementary medicine for brain tumors. Cleveland Clinic Neuro-oncology Symposium. Lake Buena Vista, FL; Jan 2005.
Suh JH. Overview of Brain Metastases. European Investigator’s meeting for ENRICH study. Paris, France; Feb 2005.
Suh JH. Review of RT-009 study. European Investigator’s meeting for the ENRICH study. Paris, France; Feb 2005.
Suh JH. Management of Efaproxiral toxicity. European Investigator’s meeting for the ENRICH study. Paris, France; Feb 2005.
Suh JH. Radiation Oncology. Cleveland Clinic Taussig Cancer Center National Leadership Board meeting. Cleveland, OH; June 2005.
Suh JH. Overview of Gamma Knife Radiosurgery. Cleveland Clinic Interna-tional Neuro-oncology Symposium. Cleveland, OH; Aug 2005.
Toms SA. Optical Imaging in Neuro-Oncology: New Techniques and Their Applications. 7th Neuro-oncology Update 2005; January 2005.
Toms SA. Quantum dots detect malignant glioma. Cambridge Healthtech Institute›s 6th Annual Targeted Nanodelivery for Therapeutics and Molecular Imaging; August 2005.
Toms SA. Video presentation: «Surgical resection of brain metastasis», Congress of Neurological Surgeons; October 2005.
Toms SA. Surgical Resection of Brain
Metastasis: Basic and Special Techniques. Congress of Neurological Surgeons; October 2005.
Toms SA. Quantum dots detect malignant glioma. OpticsEast; October 2005.
Toms, SA. Quantum Dots are phagocy-tized by macrophages and detect experimental malignant glioma. Interna-tional Association for Nanotechnology; November 2005.
Usmani A, Makdissi A, Hamrahian A, Reddy S, Weil RJ, Faiman C. Hypotha-lamic-pituitary-adrenal (HPA) axis testing using a twenty-five (25) microgram Cotrosyn stimulation test. Poster presented at: American Academy of Clinical Endocrinologists, Annual meeting; 2005.
Vatolin S, Navaratne K, Weil RJ. Method for detection of microRNA targets. Plat-form presentation: RNAi course; Cold Spring Harbor Laboratory; September 28-October 2, 2005.
Videtic GM, Reddy CA, Chao ST, et al. Women with Brain Metastases from Non-Small Cell Lung Cancer Live Longer than Men: An outcomes study utilizing the RTOG RPA class stratification. ESTRO, 2005.
Vogelbaum MA. Mayfield Clinic-Cleveland Clinic-Mayo Clinic Winter Neuroscience Symposium. Overview of Convection-enhanced Delivery. Snowmass, CO; February 2005.
Vogelbaum MA. Tumor Margin Dose Affects Local Control Following Stereotac-tic Radiosurgery of Brain Metastases; February 2005.
Vogelbaum MA. Radiation Therapy Oncology Group Brain Tumor Symposium. Convection-enhanced Drug Delivery; June 2005.
Vogelbaum MA, Berkey B, Peereboom D, et al. RTOG 0131: Phase II Trial of Pre-Irra-diation and Concurrent Temozolomide in Patients with Newly Diagnosed Anaplastic Oligodendrogliomas and Mixed Anaplastic Oligodendrogliomas. ASCO, 2005.
Vogelbaum MA, Sampson JH, Kunwar S, et al. Convection-enhanced delivery of cintredekin besudotox (IL13-PE38QQR) followed by radiation therapy without and with temozolomide. A phase I study in newly diagnosed malignant glioma patients. CNS, 2005.
Vogelbaum MA, Mazzone P, Masaryk T, et al. Low serum S100 levels in patients with
newly diagnosed lung cancer correlate with an absence of brain metastases on MRI. World Federation of Neuro-Oncology, 2005.
Weil RJ, DeVroom, Vortmeyer AO, Nieman L, Oldfield EH. Adenomas confined to the neuro-hypophysis in Cushing’s Disease. Poster presented at: Endocrine Society, 87th Annual Meeting; June 2005; San Diego, CA.
Weil RJ. Advances in Tumor Diagnostics: Genomics, Epigenomics, and Proteomics. Cleveland Clinic Neuro-oncology Sympo-sium. Orlando, FL; January 2005.
Weil RJ. Potential Proteomic Approaches to Analysis of Drug Resistance Proteins in Gliomas. Invited Speaker, Cleveland Clinic Foundation Cancer Center Symposium, Failure of Chemotherapy in Malignant Brain Tumors: The Roles of the Blood-Brain-Barrier and Drug Resistance Genes. Cleveland, OH; March 2005.
Weil, RJ. CNS Metastases in Women with Breast Cancer: Challenges and Opportuni-ties. Invited speaker, Molecular and Genetic Markers in Breast Cancer Working Group and the Cleveland Clinic Women’s Center. Cleveland, OH; May 2005.
Weil RJ. Pituitary Surgery and Endoscopic Approaches: Overview, Problems, and Expectations. Invited faculty member and speaker, Cleveland Clinic Foundation Neuro-Endoscopy Surgical Techniques Course. May 2005.
Weil RJ. Pituitary Surgery: Conventional and Endoscopic Approaches. Invited speaker and faculty member, Cleveland Clinic Foundation International Neuro-oncology Symposium, Cleveland Clinic Foundation. August 2005.
Weil RJ. Invited lecturer and panelist, Congress of Neurological Surgeons. Medical and Surgical Management of Seizures in patients with low-grade gliomas. Luncheon Seminar T-24, Manage-ment of low-grade gliomas: current strategies and dilemmas. CNS Annual Meeting. Boston, MA; October 2005.
Manuscripts Submitted Angelov L, Barnett GH. Awake Craniotomy and Intra-op Imaging. In Image guided Surgery (Barnett, Maciunas,Roberts eds). Marcel Dekker, Inc. New York 2005. Submitted.
Barnett G and Thomas T. Imaged-Guided Surgery. In: Black P, ed. Neurosurgical

2005 Annual Report A team approach to individualized care ��
Oncology.
Barnett GH, Park J. Craniopharyngioma. In: Ragahaven, ed. Textbook of Uncom-mon Cancer, 3rd ed. Sent to publisher August 2005.
Chahlavi A, Borsellino S, Barnett GH, Vogelbaum MA. The use of skull-implanted fiducials for computer-assisted sterotactic brain stem and posterior fossa brain biopsies. Submitted.
Chen PG, Lee SY, Barnett GH, Vogelbaum MA, Saxton JP, Fleming PA, Suh JH. Use of the RTOG RPA classification system and preditors of survival in 19 women with brain metastases from ovarian cancer. Cancer. March 16, 2005. Submitted.
Hercbergs AA, Suh JH, Toms SA, et al. Propylthiouracil-induced thyroid hormone depletion improves survival and response rates in recurrent high-grade glioma patients treated with tamoxifen. Cancer, August 2005. Submitted.
Kanner A, Marton LJ, Barnett GH, Vogelbaum MA. Targeting Polyamines. A strategy to treat brain neoplasms. 2005. In review.
Kanner A, Vogelbaum MA, Staugaitus S, Chernova O, Prayson RA, Suh JH, Lee SY, Barnett GB. Effect of allelic loss of chromosome 1p on survival in oligoden-drogliomas independent of therapy. 2005 J Neurosurg. Submitted.
Lee JH, Sade B, Choi E, Golubic M, Prayson R. Midline Skull Base and Spinal Meningiomas are Predominantly of the Meningothelial Histological Subtype. Journal of Neurosurgery. June 8, 2005. Submitted.
Lee JH, Sade B, Park BJ. Surgical Technique for Removal of Clinoidal Meningiomas. Neurosurgery for their Operative Nuances issue. June 29, 2005. Submitted.
Lee JH. Management options and basic surgical principles. Meningiomas. Springer-Verlag, London. In review.
Lee JH. Meningioma surgery: Personal philosophy. Meningiomas. Springer-Verlag, London. In review.
Lupica K, Ditz G. Nursing Considerations. In High-Grade Gliomas: Diagnosis and Treatment.
Mahmoud-Ahmed A, Suh J, Lee SY, Hamrahian A, Barnett GH, Mayberg MR. Gamma Knife Radiosurgery Induces Biochemical Cure in Patients with
Acromegaly Faster than External Beam Radiation. 2005. Submitted.
Mason A, Toms SA, Hercbergs A. Biological Modifiers. In High-grade Gliomas. Submitted.
Taban M, Cohen B, Rothner D, Traboulsi E. Association of Optic Nerve hypoplasia with Mitochondrial Cytopathies. Submit-ted.
Nathoo N, Chahlavi, A, Barnett GH, Toms, SA. Pathobiology of Brain Metastasis. 2005. Submitted.
Nathoo N, Ugokwe K, Chang A, et al. The Role of 111 indium-octreotide brain scintigraphy in the diagnosis of cranial, dural-based meningiomas. Neurosurgery. March 2005. Submitted.
Rogers LR, Rock JP, Sills AK, et al. Brain Metastasis Study Group, Shaw EG. Results of a phase II trial of GliaSite Radiation Therapy System for the treatment of newly diagnosed resected single brain metasta-ses. J Neurosurg. July 2005. Submitted.
Sajja R, Barnett GH, Lee SY, Stevens GH, Lee J, Suh JH. Intensity-Modulated Radiation Therapy (IMRT) for Newly Diagnosed and Recurrent Intracranial Meningiomas: The Cleveland Clinic Foundation Experience. International Journal Radiology Oncology, Biology, Physiology. 2005. Submitted.
Sajja R, Barnett GH, Lee SY, Vogelbaum M, Stevens G, Lee JH, Suh J. Local control of intracranial meningiomas with Gamma Knife radiosurgery: The Cleveland Clinic Foundation Experience. International Journal Radiology Oncology, Biology, Physiology. 2005. In review.
Sajja R, Barnett GH, Lee SY, Vogelbaum MA, Stevens GHJ, Lee J, Suh JH. Local control on intracranial meningiomas with gamma knife radiosurgery (GKRS): The Cleveland Clinic Foundation Experience. 2005. Submitted.
Sajja R, Barnett GH, Lee SY, Stevens GHJS, Lee JH, Suh J: Intensity-modulated radiation therapy (IMRT) for newly diagnosed and recurrent intracranial meningiomas: The Cleveland Clinic Foundation Experience. Journal Radiology Oncology, Biology, Physiology. 2005. In review.
Suh JH, Curran W, Mehta MP, et al. Predictors for survival for patients with brain metastases: results of a randomized phase III trial. Int J Radiat Oncol Biol Phys. August 2005. Submitted.
Taban M, Cohen B, Rother D, et al. Association of Optic Nerve hypoplasia with Mitochondrial Cytopathies. 2005. Submitted.
Tobias S, Kim C-H, Burak S, Staugaitis SM, Lee JH. Benign neuromuscular choristoma of the trigeminal nerve in an adult: Case report and literature review. Acta Neurochirurgica February 2005. Submitted.
Ugokwe K, Nathoo N, Prayson R, Barnett GH. Trigeminal Nerve Schwannoma with Ancient Change: Case Report and Review of the Literature. 2005. Submitted.
Vogelbaum M, Thomas T. Contemporary Investigational Treatments for Malignant Brain Tumors: Small Molecule Agents. In: Barnett GH. High-grade Gliomas: Diagnosis and Treatment. Totawa, NJ: Humana Press. 2005. Submitted.
Vogelbaum MA, Angelov L, Lee SY, Li L, Barnett GH, Suh JH. Local control of Brain Metastases by Stereotactic Radiosurgery Depends Upon the Dose to the Tumor Margin. Journal of Neurosurgery. February 2005. Submitted. (Accepted with revisions.)
Vogelbaum MA, Barnett, GH. Response of Recurrent Glioblastoma Multiforme to Tarceva (OSI774) with Subsequent Leptomeningeal Failure. 2005. Submitted.
Vogelbaum, M. A., Angelov, L., Lee, S-Y., Barnett, G.H., Suh, J.H., Factors affecting local control in patients with metastatic brain tumors treated with Gamma Knife stereotactic radiosurgery. Journal of Neurosurgery. 2005. Submitted.
WIP Angelov L, Lee SY, Barnett GH, Suh JH, Vogelbaum MA. The response to treatment of melanoma brain metastasis with stereotactic radiosurgery alone or in combination with whole brain radiation therapy. In progress.
Angelov L, Vogelbaum MA, Barnett GH, Stevens GHJ, Suh JH, Miller M, Peere-boom DM. Temozolomide therapy in the management of primary central nervous system lymphomas. In progress.
Barnett GH. High-Grade Gliomas. Diagnosis and Treatment. In progress.
Chahlavi A, Krishnany A, Nagel S, Lee JH. Aggressive and Malignant Meningiomas are Rare in the Skull Base Locations. In progress.

�2 Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
Chahlavi A, LaPresto E, Vogelbaum MA. Analysis of Patients with Glioblastoma Multiforme and amplified EGFR. In progress.
Chahlavi A, Park J, Staugatis S, Lee JH. Incidental Intraoperative Finding of Vestibular Nerve Heterotopia: case report. In preparation.
Golubic M, Lee JH. Emerging treatment modalities for meningiomas: Targeting the NF-2 and Ras pathways. Meningiomas. Springer-Verlag, London. In review.
Golubic M, Angelov L, Sade B, Lee JH. Molecular basis of meningioma tumorigen-esis and progress. Meningiomas. Springer-Verlag, London. In review.
Krishnaney A, Steinmetz MP, Golubic M, Lee JH. Meningioma location is associ-ated with histologic subtype and risk of aggressive behavior. Manuscript. In progress.
Krishnany A, Chahlavi A, Nagel S, Lee J. Meningiomas of the midline / paramedian skull base are predominantly meningothe-lial. In preparation.
Lee JH, Sade B, Park BJ. The «CLASS» algorithmic scale for patient selection in meningioma surgery: rationale and validity – a retrospective study. In progress.
Lee JH, Sade B. Dural reconstruction following meningioma resection: Non-watertight closure. Meningiomas. Springer-Verlag, London. In progress.
Lee JH, Sade B. Meningiomas of the central neuraxis. Unique tumors. Meningiomas. Springer-Verlag, London. In review.
Lee JH, Sade B. Surgical management of clinoidal meningiomas. Meningiomas. Springer-Verlag, London. In review.
Lee JH, Sade B. The factors influencing outcome in meningioma surgery. Meningiomas. Springer-Verlag, London. In review.
Lin WC, Mahadevan J, Chari R, Toms SA. Optics of cell and tissue viability. In preparation.
Mahelas TJ, Lee JH. Sequential visual loss from skull base neurosarcoidosis. In review.
Mason A, Barnett G. Retrospective review and case report of peritumoral malignant edema from perisagital meningiomas after gamma knife. In review.
Park BJ, Kim HK, Lee JH. Epidemiology of meningiomas. Meningiomas. Springer-Verlag, London. In review.
Quan AL, Ross JS, Lee SY, et al. Prognos-tic implication of multicentric and multifocal disease in patients with glioblas-toma multiforme. In preparation.
Sade B, Lee JH. Tuberculum sellae meningiomas: surgical management and outcome. In progress.
Sade B, Chahlavi A, Krishnaney A, Nagle S, Choi E, Lee JH. The WHO Grade II and III meningiomas are rare in the skull base and spinal locations. Neurosurgery. In review.
Sade B, Lee JH, Lee DK, Hughes GB, Prayson R. Cavernous angioma of the petrous bone. Laryngoscope. In review.
Sade B, Lee JH. Recovery of low frequency sensori-neuronal hearing loss following resection of a greater superficial petrous and nerve schwannoma. Journal of Neurosurgery. In review.
Sade B, Lee JH. Validity and utility of the ‘CLASS’ algorithmic scale. Meningiomas. Springer-Verlag, London. In review.
Sade B, Park BJ, Lee JH. The factors influ-encing early outcome in meningioma surgery. In progress.
Sade B, Prayson R, Lee JH. Giosarcoma with infratemporal fossa extension. Journal of Neurosurgery. In review.
Sajja R, Barnett GH, Lee SY, et al. Gamma Knife radiosurgery for newly diagnosed and recurrent intracranial meningiomas. In progress.
Siomin V, Toms SA. En bloc resection of skull base metastasis is achievable with good clinical outcomes. In preparation.
Spotta A, Nathoo N, Stevens GHJ, Barnett GH. Primary cranial vault lymphoma with complete occlusion of the superior saggital sinus and subgaleal extension without bone erosion: A case report and review of the literature. In preparation.
Stevens GHJ, Vogelbaum MA, Peereboom DA, Suh J, Barnett GH. Brain tumor patients and driving: special considerations regarding seizures. In preparation.
Stevens GHJ, Vogelbaum MA, Peereboom DA, Suh J, Barnett GH. Brain tumor patients and treatment of epilepsy: Is it time for a paradigm shift? The Cleveland Clinic experience for conversion of phenytoin to levatriracitam. In preparation.
Suh JH, Barnett GH, Regine WF. Role of radiosurgery for brain metastases. Principles and Practice of Stereotactic Radiosurgery.
Toms SA, Muhammed O, Damishear H, Vogelbaum MA. Computed tomography detects quantum dots in vivo. In prepara-tion.
Toms SA, Daneshvar H, Nelms J, Muhammed O, Jackson H, Vogelbaum MA, Bruchez M. Optical Detection of Brain Tumors Using Quantum Dots. In prepara-tion.
Toms SA, Konrad P, Weil RJ, Lin WC. Neurological applications of optical spectroscopy. In preparation.
Toms SA, Muhammed O, Damishear H, Vogelbaum MA. Gradient echo MRI detects quantum dots in vivo. In prepara-tion.
Toms SA, Tasch J, Muhammed O, Jackson H, Lin W-C. Decline in NAD(P)H Autofluorescence Precedes Apoptotic Cell Death from Chemotherapy. In preparation.
Toms SA, Yuan S, Miller DW, Muhammed O, Tasch J, Williams BRG. Identification of an alternate splice of hSLK, hSLKS. In preparation.
Ugokwe K, Toms SA. Renal Cell Carci-noma Brain Metastases. Renal Cell Carcinoma. In preparation.
Vogelbuam M. Small Molecule Agents. High-Grade Gliomas. Diagnosis and Treatment.

2005 Annual Report A team approach to individualized care ��
Consortia: NABTT: New Approaches Brain Tumor Therapy ACOSOG: American College of Surgeons Oncology Group BBBD: Blood-Brain Barrier Disruption RTOG: Radiation Therapy Oncology Group SWOG: South West Oncology Group COG: Children’s Oncology Group
Adult ProtocolsIV Chemotherapy for High-Grade Gliomas Description: Phase II Clinical Trial of Patients with High-Grade Glioma Treated with Intra-arterial Carboplatin-based Chemotherapy, Randomized to Treatment with or without Delayed Intravenous Sodium Thiosulfate as a Potential Chemoprotectant against Severe ThrombocytopeniaEligibility: Histologically confirmed high-grade glioma, age 18-75.Study Design: Phase II, multi-institutional trialContact: Glen Stevens, D.O., Ph.D., 216.445.1787
AP2�5�� in Progressive or Recurrent Malignant GliomaDescription: A Phase I Sequential Ascending Dose Trial of AP23573 in Patients with Progressive or Recurrent Malignant GliomaEligibility: Radiographically suspected progressive or recurrent primary malignant glioma (glioblastoma multiforme, gliosarcoma or WHO Grade 4) and must have failed standard therapy. Patients may not have received any systemic therapy for the treatment of this recur-rence or relapse. Age >= 18.Study Design: Phase I, multi-institutionalContact: TEMPORARILY NOT ACCEPT-ING PATIENTS
Erlotinib with Temozolomide & Radiation for Newly Diagnosed GBMDescription: A Phase II Trial of Erlotinib with Temozolomide & Concurrent Radiation Therapy Post-operatively in Patients with Newly Diagnosed Glioblastoma Multiforme Eligibility: Newly diagnosed glioblastoma multiforme, ≥18 years old. Study Design: Phase II internal study
Contact: David Peereboom, M.D., 216.445.6068
Celecoxib & Anticonvulsants for Newly Diagnosed GBM’s undergo-ing Radiation TherapyDescription: A Pharmacokinetic Study of the Interaction between Celecoxib & Anticonvulsant Drugs in Patients with Newly Diagnosed Glioblastoma Multiforme Undergoing Radiation Therapy (NABTT 2100) Eligibility: Histologically confirmed supratentorial grade IV astrocytoma (glioblastoma multiforme). Age ≥18. Study Design: Pharmacokinetic cooperative group study Contact: CURRENTLY NOT ACCEPTING PATIENTS
Tarceva (Recurrent/Progressive Glioblastoma Multiforme)Description: A Phase II study of OSI-744 used alone in patients with recurrent malignant gliomas. Eligibility: Patients must be at least 18 years of age and have Histologically confirmed WHO grade IV astrocytoma (glioblastoma multiforme), with radio-graphic evidence of recurrence. Study Design: Internal, Phase II Contact: Michael Vogelbaum, M.D., Ph.D., 216.444.856
ACOSOG Z0�00 (One to Three Cerebral Metastases)Description: A Phase III Randomized Trial of the Role of Whole Brain Radiation Therapy in Addition to Radiosurgery in the Management of Patients with One to Three Cerebral Metastases Eligibility: Patient must be at least 18 years of age Study Design: ACOSOG Consortium, Phase III Contact: CURRENTLY NOT ACCEPTING PATIENTS
BMS (Recurrent Malignant Glioma)Description: A Phase I/II Study of BMS-24755A Phase I/II Study of BMS-247550 for Treatment of Patients with Recurrent Malignant Gliomas (NABTT 2111) Eligibility: Patients must be 18 years of age or older and have histologically proven malignant glioma (anaplastic astrocytoma or glioblastoma multiforme), which is
progressive or recurrent following radiation therapy ± chemotherapy. Patients with previous low-grade glioma who pro-gressed after radiotherapy +/- chemo-therapy and are biopsied and found to have a high-grade glioma are eligible. Study Design: NABTT consortium, Phase I/II Contact: David Peereboom, M.D., 216.445.6068
OXALIPATIN (Newly Diagnosed Glioblastoma Multiforme) Description: Phase I/II Trial of Oxaliplatin as Neoadjuvant Treatment in Adults with Newly Diagnosed Glioblastoma Multi-forme NABTT 9902 Eligibility: Patients must be at least 18 years of age and have histologically confirmed supratentorial grade IV astrocytoma (glioblastoma multiforme). Study Design: NABTT consortium, Phase I/II Contact: CURRENTLY NOT ACCEPTING PATIENTS
Karenitecin (Recurrent Malignant Gliomas)Description: Phase I Evaluation of the Safety of Karenitecin in the Treatment of Recurrent Malignant Gliomas NABTT 2006 Eligibility: Patients must be 18 years of age or older and have histologically proven malignant glioma (anaplastic astrocytoma, anaplastic oliogodendroglioma or glioblastoma multiforme) which is progressive or recurrent following radiation therapy +/- chemotherapy. Patients with previous low-grade glioma who pro-gressed after radiotherapy +/- chemo-therapy and are biopsied and found to have a high-grade glioma are eligible. Study Design: NABTT consortium, Phase I Contact: CURRENTLY NOT ACCEPTING PATIENTS
Tamoxifen-Hypothyroid GBM Description: High-dose Tamoxifen in combination with reduction of thyroid hormone during and post external beam radiotherapy. Study Design: Internal study: Phase II Eligibility: Newly diagnosed GBM, Age >18yrs Contact: CURRENTLY NOT ACCEPTING PATIENTS
Brain Tumor Institute
Appendix A – Clinical Trials

�� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
RTOG-���� (Anaplastic Astrocytoma) Description: Radiation with randomization to one of three chemotherapy options Study Design: RTOG-98-13, Phase I/III trial Eligibility: Anaplastic astocytoma, Age 18 yrs Contact: John Suh, M.D., 216.444.5574
NABTT ��0� (Gliadel and O�-BG for Malignant gliomas) Description: Surgical resection and placement of gliadel wafer with systemic O6BG Study Design: Phase I study Eligibility: Supratentorial malignant glioma, Age >18yrs Contact: CURRENTLY NOT ACCEPTING PATIENTS
NABTT ��0� (procarbazine for malignant gliomas)Description: oral procarbazine, 2 arm: P450 vs. non P450 inducing medications Study Design: NABTT 9901, Phase I/II study Eligibility: recurrent high-grade glioma, 3 months post XRT, only one prior chemo Contact: CURRENTLY NOT ACCEPTING PATIENTS
NABTT ��0� (Col-� for recurrent malignant gliomas) Description: Col-3 (anti-angiogenesis) for high-grade gliomas Study Design: NABTT 9809, Phase I/II trial, P450 and non P 450 arms Eligibility: recurrent high-grade glioma, 2 or less prior chemos and 3 months post XRT Contact: CURRENTLY NOT ACCEPTING PATIENTS
SWOG S000�: Upfront Treatment for Newly Diagnosed GBMsDescription: Randomization to Radiation therapy + O6-BG + BCNU vs. Radiation + BCNU Alone Study Design: Phase III SWOG study Eligibility: Newly diagnosed GBM, KPS >60Contact: CURRENTLY NOT ACCEPTING PATIENTS
IL-��Description: Pre-Operative IL13-PE38QQR Infusion in Patients with Recurrent or Progressive Supratentorial Malignant Glioma Study Design: A Phase I/II Study Eligibility: Patients must have prior histologic diagnosis of supratentorial malignant gliomas. Eligible histologies: glioblastoma multiforme, anaplastic astrocytoma, or malignant mixed oligoas-trocytoma (excludes glioma of know grade or “pure” oligodendroglioma). Patients with
clinical /radiographic diagnosis of malignant glioma may be registered pending histologic confirmation. Patients must have recurrent or progressive supratentorial tumor compared with a previous study. Patients must be > 18 years old.Contact: CURRENTLY NOT ACCEPTING PATIENTS
IL-��Description: Phase I study of convection-enhanced delivery (CED) of IL13-PE38QQR cytotoxin after resection and prior to radiation therapy with or without temozolomide in patients with newly diagnosed supratentorial malignant glioma Study Design: Phase I Eligibility: Age > 18 years old., must have undergone a gross total resection of the solid contrast-enhancing lesions(s) > 1.0 cm in diameter, must be able to have catheters placed within 14 days of tumor resection (including a planned Gross Total Resection following an initial biopsy or subtotal resection) and must have histopathologic documentation of malignant glioma from resection speci-men. Diagnosis must be consistent with either GBM, AA or mixed OA. Contact: Mike Vogelbaum, M.D., 216.444.5381
IL-��Description: Phase III Randomized Evaluation of Convection-enhanced Delivery of IL13-PE38QQR Compared to Gliadel Wafer with Survival Endpoint in Glioblastoma Multiforme Patients at First Recurrence Study Design: Phase III Eligibility: Patients with glioblastoma multiforme (GBM) at first recurrence who are considered candidates for resection and meet the specified eligibility criteria may be enrolled in the study. Contact: CURRENTLY NOT ACCEPTING PATIENTS
WBRT +/- RSR�� in Women with Brain Metastases from Breast CancerDescription: A Phase III Randomized, Open-label Comparative Study of Standard Whole Brain Radiation Therapy with Supplemental Oxygen, with or without Concurrent RSR13 (efaproxiral), in Women with Brain Metastases from Breast Cancer Study Design: Phase III Eligibility: Age >= 18 years old, histologically or cytologically confirmed breast cancer in women with radiographi-cally confirmed metastases to the brain.
Contact: John Suh, M.D., 216.444.5574
Melatonin for Brain MetastasesDescription: A Randomized Phase II Study of A.M. and P.M. Melatonin for Brain Metastases in RPA Class II Patients Study Design: Phase II Eligibility: Brain metastasis from histologically documented solid tumors (except germ cell tumors). Biopsy proof from the brain metastasis is preferred when clinical history and radiologic findings are equivocal. Contact: CURRENTLY NOT ACCEPTING PATIENTS
Focal Radiation for �-� Brain MetastasesDescription: A Phase II Study Utilizing Focal Radiation in Patients with 1-3 Brain Metastases Study Design: Phase II Eligibility: Have 1 to 3 newly diagnosed supratentorial metastatic brain lesions with at least one being dominant and eligible for surgical resection as visualized on enhanced MRI scan. Have histological evidence of metastatic carcinoma on intraoperative pathology (frozen section) or final pathology report. Contact: Mike Vogelbaum, M.D., Ph.D., 216.444.5381
Temozolomide for Anaplastic Oligodendrogliomas & Mixed OligoastrocytomaDescription: Phase II Trial of Continuous Dose Temozolomide in Patients with Newly Diagnosed Anaplastic Oligodendro-gliomas and Mixed Oligoastrocytoma Study Desgin: Phase II trial Eligibility: Newly Diagnosed Anaplastic Oligodendroglioma, Newly Diagnosed Mixed Anaplastic Oligodendroglioma Contact: David Peereboom, M.D., 216.445.6068
Intraoperative Optical Spectroscopy for Glial TumorsDescription: Detection of glial tumor margins with intraoperative optical spectroscopy Study Design: Internal study Eligibility: Unifocal or multifocal supratentorial glial neoplasm suspected on MRI & patient is a surgical candidate for craniotomy Contact: Steven Toms, M.D., 216.445.7303
Gliasite BrachytherapyDescription: Phase I Brachytherapy Dose Escalation Using the Gliasite RTS in Newly Diagnosed Glioblastoma Multi-
2005 Annual Report A team approach to individualized care �5
forme in Conjunction with External Beam Radiation Therapy Study Design: Phase I trial Eligibility: Newly Diagnosed GBM Contact: Michael Vogelbaum, M.D., Ph.D., 216.444.8564
Dietary & Herbal Complementary Alternative Medicine ApproachDescription: Phase II Randomized Evaluation of 5-Lipoxgenase Inhibition by Dietary and Herbal Complementary and Alternative Medicine Approach Compared to Standard Dietary Control as an Adjuvant Therapy in Newly Diagnosed Glioblastoma Multiforme Study Design: Phase II Randomized Eligibility: Newly Diagnosed GBM Contact: Mladen Golubic, M.D., Ph.D., 216.445.7641
Bay ��-�00� for Recurrent/Progres-sive Malignant GliomasDescription: A Phase I Trial of Bay 43-9006 for Patients with Recurrent or Progressive Malignant Glioma Study Design: Phase I trial Eligibility: Recurrent Anaplastic Astrocy-toma, Recurrent Anaplastic Oligodendro-glioma, Recurrent GBM, Recurrent Gliosarcoma Contact: David Peereboom, M.D., 216.445.6068
EMD & RT for Newly Diagnosed GBM’sDescription: A Safety Run-In/Randomized Phase II Trial of EMD 121974 in Conjunc-tion with Radiation Therapy in Patients with Newly Diagnosed Glioblastoma Multiforme NCI #: NABTT 0306Study Design: NABTT Cooperative Phase II TrialEligibility: Newly Diagnosed GBM, Newly Diagnosed GliosarcomaContact: David Peereboom, M.D., 216.445.6068
Temozolomide for Low-grade GliomasDescription: A Phase II Study of Temozolo-mide-Based Chemotherapy Regimen for High Risk Low-Grade GliomasStudy Design: Phase II trialEligibility: Low-Grade GliomasContact: John Suh, M.D., 216.444.5574
Talampanel w/RT & Temozolomide for Newly Diagnosed GBM’sDescription: A Phase II Trial of Talam-panel in Conjunction with Radiation Therapy with Concurrent and Adjuvant Temozolomide in Patients with Newly Diagnosed Glioblastoma Multiforme
Study Design: Phase II TrialEligibility: Newly Diagnosed GBM, Newly Diagnosed GliosarcomaContact: David Peereboom, M.D., 216.445.6068
Lymphoma Blood-Brain Barrier Disruption (Primary Central Nervous System Lymphoma) Description: A Phase II Trial involving Patients with Recurrent PCNSL Treated with Carboplatin/BBBD, by Adding Rituxan (Rituximab), an anti-CD-20 Antibody, to the Treatment RegimenEligibility: Patients must be 18-75 yrs of age histologically confirmed Primary CNS Lymphoma as documented by brain biopsy, or cytology (analysis from CSF or vitrectomy), & CD20 positive. Study Design: Internal, Phase II, multi-institutionalContact: CURRENTLY NOT ACCEPTING PATIENTS
Blood-Brain Barrier Disruption (Primary Central Nervous System Lymphoma)Description: Combination Chemotherapy (Methotrexate, Cyclophosphamide and Etoposide Phosphate) Delivered in Conjunction with Osmotic Blood-Brain Barrier Disruption (BBBD), with Intraventricular Cytarabine +/- Intra-Ocular Chemotherapy, in Patients with Primary CNSEligibility: 16-75 years old; histologically confirmed intermediate/high-grade primary CNS lymphoma Study Design: Internal, multi-institutional Contact: Glen Stevens, D.O., Ph.D., 216.445.1787
Meningioma SWOG-���� (Benign Meningioma)Description: Chemotherapy with hydroxyurea Study Design: Phase II, cooperative group Eligibility: Primary, recurrent or residual benign meningioma which is unresect-able, Age >18yrs, XRT > 1 yr Contact: CURRENTLY NOT ACCEPTING PATIENTS
MetastasisZeiss INTRABEAM System for Solitary Brain MetastasisDescription: A Phase I/II Study Utilizing the Zeiss INTRABEAM System for the Treatment of a Resected Solitary Brain
MetastasisEligibility: Newly diagnosed supratentorial single metastatic brain tumor as visualized on enhanced MRI scan that is surgically resectable. CT scans may be substituted for MRI only for those patients in whom MRI scans cannot be safely performed. Age >= 18.Study Design: Phase I/II, internal study.Contact: Steven Toms, M.D., 216.445.7303
WBRT with Temozolomide or Placebo for Non-Small Cell Lung Cancer Brain MetastasesDescription: A Randomized, Double-Blind, Placebo-Controlled, Phase III Study of Temozolomide or Placebo added to Whole Brain Radiation Therapy for the Treatment of Brain Metastases from Non-Small Cell Lung CancerEligibility: Histologically or cytologically confirmed non-small cell lung cancer. Eligible histologies include squamous cell and adenocarcinoma (including large cell carcinoma) and non-small cell cancer not otherwise specified. A biopsy of meta-static disease in the brain is not required for study enrollment. Age >= 18.Study Design: Phase III, randomized, double-blind, placebo controlled.Contact: John Suh, M.D., 216.444.5574
Radiation therapy plus Thalidomide for Multiple Brain MetastasesDescription: A Phase III Study of Conventional Radiation Therapy Plus Thalidomide vs. Conventional Radiation Therapy for Multiple Brain Metastases (RTOG 0118) Eligibility: Histopathologically confirmed extracranial primary malignancy. Age ≥18. Study Design: Phase III cooperative group study Contact: CURRENTLY NOT ACCEPTING PATIENTS
WBRT +/- RSR�� in Women with Brain Metastases from Breast CancerDescription: A Phase III Randomized, Open-label Comparative Study of Standard Whole Brain Radiation Therapy with Supplemental Oxygen, with or without Concurrent RSR13 (efaproxiral), in Women with Brain Metastases from Breast CancerStudy Design: Phase IIIEligibility: Age >= 18 years old, histologically or cytologically confirmed breast cancer in women with radiographi-cally confirmed metastases to the brain.Contact: John Suh, M.D., 216.444.5574

�� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
Xcytrin for Non-Small Cell Lung Cancer Brain MetastasesDescription: Randomized Phase III Trial of Xcytrin® (Motexafin Gadolinium) Injections for the Treatment of Brain Metastases in Patients with Non-Small Cell Lung Cancer Undergoing Whole Brain Radiation Therapy. Study Design: Phase III Randomized trial Eligibility: Non-small cell lung cancer with brain metastases Contact: CURRENTLY NOT ACCEPTING PATIENTS
WBRT & SRS +/- Temozolomide/Gefitinib for Non-Small Cell Lung Cancer & Brain MetastasesDescription: RTOG 0320: A Phase III Trial Comparing Whole Brain Radiation and Stereotactic Radiosurgery Alone Versus with Temozolomide or Gefitinib in Patients with Non-Small Cell Lung Cancer and 1-3 Brain MetastasesStudy Design: RTOG Cooperative Phase III TrialEligibility: Non-Small Cell Lung Cancer with Brain MetastasesContact: John Suh, M.D., 216.444.5574
Motexafin Gadolinium with WBRT & SRS Boost for Brain MetastasesDescription: Phase II Trial of Motexafin Gadolinium with Whole Brain Radiation Therapy Followed by Stereotactic Radiosurgery Boost in the Treatment of Patients with Brain MetastasesStudy Design: Phase II trialEligibility: Brain MetastasesContact: John Suh, M.D., 216.444.5574
Child and Adolescent Protocols
Newly Diagnosed MalignanciesHead Start III: Dose-Intensive Chemotherapy for Children Less Than �0 Years of Age Newly Diagnosed with Malignant Brain TumorsDescription: The study uses an intensified chemotherapeutic regimen for five months followed by a highly intensive single-drug treatment course and stem cell rescue with lower-dose radiation to try to increase the chance of cure for children with certain malignant brain tumors.Eligibility: Children less than 10 years (120 months) of age at time of histologic or cytologic diagnosis of malignant brain tumor who have not previously received
irradiation or chemotherapy (except corticosteroids). Patients with the following tumor types ma y be eligible: medulloblastoma, primitive neuroecto-dermal tumor, ependymoma, choroid plexus carcinoma, atypical teratoid/rhabdoid tumor, or malignant glioma. Specific criteria apply depending on brain tumor type.Study Design: Nonrandomized Phase II study with 2-stage design.Contact: Joanne M. Hilden, M.D., 216.444.8407, or Bruce H. Cohen, M.D., 216.444.9182.
Chemo-Radiation Therapy for CNS AT/RT (IRB #���0)Description: The study represents a multi-institutional effort to estimate activity of an aggressive multimodality (systemic and intrathecal) chemotherapeutic regimen for highly malignant atypical teratoid-rhabdoid tumors of the CNS. Treatment showed promising results in a very limited number of these extremely rare cases. Favorable study results may occasion a full-scale national trial proposal.StudyDesign: Phase II.Eligibility: Patients must be < 18 years of age. Target tumors: histologically confirmed primary intracranial CNS AT/RT or tumor that possesses the INI1 gene mutation.Contact: Joanne M. Hilden, M.D., 216.444.8407, or Bruce H. Cohen, M.D., 216.444.9182
C.O.G.-ACNS0�2�: A Phase II Trial of Conformal Radiation Therapy for Pediatric Patients with Localized Ependymoma, Chemotherapy Prior to Second Surgery for Incompletely Resected Ependymoma, and Observa-tion for Completely Resected Differ-entiated, Supratentorial EpendymomaDescription: The study attempts to define a standard for treatment of intracranial ependymoma based on tumor location, degree of resection, and histological characteristics. Treatment will fall into one of four groups. The study will include children under 3 years of age for treatment with conformal radiation.Eligibility: Patients must be > 12 months and < 21 years of age at time of enrollment. Patients must have had no prior treatment except previous surgery or corticosteroid therapy. Target tumors: histologically confirmed intracranial ependymoma. Patients with differentiated or anaplastic ependymoma are eligible. (Patients with primary spinal cord ependy-moma, myxopapillary ependymoma,
subependymoma, ependymoblastoma, or mixed gliomas are not eligible.)Study Design: Phase II clinical trial with four treatment arms, based on tumor loca-tion, degree of resection, and histology.Contact: Joanne M. Hilden, M.D., 216.444.8407 or Bruce H. Cohen, M.D., 216.444.9182.
C.O.G.-ACNS0�22: A Phase II Study to Assess the Ability of Neoadjuvant Chemotherapy +/– Second-Look Surgery to Eliminate All Measurable Disease Prior to Radiotherapy for NGGCTDescription: The protocol aims to improve progression-free survival and overall survival of children with nongerminomatous germ cell tumor through a new therapy regimen combining anticancer drugs, radiation therapy, and, based on response, “second-look” surgery and potentially stem cell transplant.Eligibility: Patients must be at least 3 years old and less than 25 years of age at diagnosis of one of the following: endoder-mal sinus tumor (yolk sac tumor), embryonal carcinoma, choriocarcinoma, immature teratoma and teratoma with malignant transformation, or mixed germ cell tumor.Study Design: Phase II. During the first 18 weeks, patients receive three-drug chemotherapy regimen for induction with subsequent status assessment. Status will direct further treatment options—conformal radiation versus second-look surgery followed by radiation or further chemotherapy.Contact: Joanne M. Hilden, M.D., 216.444.8407, or Bruce H. Cohen, M.D., 216.444.9182.
C.O.G.-ACNS0�2�: A Phase II Study of Temozolomide in the Treatment of Children with High-Grade GliomasDescription: The protocol tests the effectiveness of FDA-approved temozolomide combined with radiation therapy against hard-to-treat high-grade gliomal or diffuse intrinsic pontine gliomal brain tumors.Eligibility: Patients must be > 3 years of age and < 22 years of age at time of enrollment. Target tumors: anaplastic astrocytoma, glioblastoma multiforme, gliosarcoma, and diffuse intrinsic pontine gliomas. Patients with primary spinal cord malignant gliomas are also eligible. Patients with high-grade gliomas must have histologic verification of diagnosis. Metastatic disease-ineligible.Study Design: Phase II. Initially patients receive temozolomide concurrently with

2005 Annual Report A team approach to individualized care ��
radiation therapy on 42-day schedule. Four weeks after radiation therapy, patients receive temozolomide daily for 5 days, beginning a new cycle every 28 days; 10 cycles total.Contact: CLOSED TO PATIENT ACCRUAL.
C.O.G.-ACNS0���: A Study Evaluat-ing Limited-Target Volume Boost Irradiation and Reduced-Dose Craniospinal Radiotherapy (��.00 Gy) and Chemotherapy in Children with Newly Diagnosed Standard-Risk Medulloblastoma: A Phase III Double-Randomized TrialDescription: The trial seeks to reduce nervous system damage caused by radiation therapy in children diagnosed with medulloblastoma. Children at least 3 years of age to less than 8 years of age will receive craniospinal radiation dosing at a rate reduced by 25%, supplemented by moderate intensification of adjuvant chemotherapy. The study will also explore the safety of reducing boost-volume irradiation dosing from the whole posterior fossa to the tumor bed area plus a circumscribed margin by using conformal radiation.Eligibility: Patients must be at least 3 years old and less than 22 years of age when diagnosed with posterior fossa medulloblastoma.Study Design: Phase III, randomized trial.Contact: Joanne M. Hilden, M.D., 216.444.8407, or Bruce H. Cohen, M.D., 216.444.9182.
C.O.G.-P����: Systemic Chemothera-py, Second-Look Surgery, and Conformal Radiation Therapy Limited to the Posterior Fossa and Primary Site for Children > � Months and < � Years with Nonmetastatic MedulloblastomaDescription: The study serves as a historical control to see if the proposed chemotherapy and conformal radiation treatment plan will be more effective (in terms of one-year event-free survival rates) than the combined treatments given to children of the same age and extent of disease on the POG-9233 trial.Eligibility: Patients greater than 8 months of age and less than three years of age with primary histology diagnosis of medulloblastoma or posterior fossa primitive neuroectodermal tumor (PNET) and no evidence of metastases.Study Design: Phase III trial; no randomization.Contact: Joanne M. Hilden, M.D.,
216.444.8407, or Bruce H. Cohen, M.D., 216.444.9182.
Refractory / Progressive / Relapsed MalignanciesCCG-A��52: Chemotherapy for Progressive Low-Grade Astrocytoma in Children Less Than Ten Years OldDescription: The study compares event-free survival rates of two chemotherapeu-tic regimens in children less than ten years old who have progressive or incompletely resected astrocytoma or other glioma.Eligibility: Children less than 10 years old (120 months) with low-grade astrocyto-mas (grade 1 and 2) or other low-grade gliomas and who have progressive disease following surgical excision or an incom-plete excision (< 95% or > 1.5 cm2 residual tumor) with necessity to begin treatment because of risk of neurologic impairment with progression.Study Design: Phase III trial, two randomized regimens. NF1 patients, however, will be nonrandomly assigned.Contact: CLOSED TO PATIENT ACCRUAL.
C.O.G.-ACNS022�: A Phase II Study of R��5��� (Zarnestra) (NSC# �02���, IND# 5��5�) in Children with Recurrent or Progressive High-Grade Glioma, Medulloblastoma/PNET or Brainstem GliomaDescription: The protocol tests effective-ness of investigational drug R115777 (Zarnestra) in treating recurrent malignant childhood brain tumors.Eligibility: Patients must be < 21 years of age at enrollment. Target tumors: recurrent or progressive anaplastic astrocytoma, glioblastoma multiforme, gliosarcoma, anaplastic oligodendroglio-ma, recurrent or refractory medulloblas-toma/PNET, or diffuse intrinsic brainstem glioma. Patients must have histopatho-logic verification of diagnosis from either initial presentation or at time of recurrence except for brainstem glioma patients. Patients must have radiographically documented measurable disease and have relapsed or become refractory to conventional therapy. Patients must have life expectancy of at least 8 weeks. Patients are excluded for uncontrolled infection, allergy to azoles, or for taking enzyme-inducing anticonvulsants.Study Design: Phase II. Patients receive study drug for 21 days followed by 7-day rest period. The 28-day cycles may be
repeated for up to two years in the absence of disease progression or unacceptable toxicity.Contact: CLOSED TO PATIENT ACCRUAL.
ADVL0�2�: A Phase II Study of Oxaliplatin in Children with Recurrent Solid TumorsDescription: The study seeks to determine the response rate of various disease strata of recurrent or refractory malignant tumors of childhood to the investigational drug oxaliplatin.Eligibility: Patients must be no more than 21 years of age inclusive when originally diagnosed. The trial includes the following malignancies for the brain tumor stratum: recurrent or refractory high-grade astrocytoma, multiforme glioblastoma, low-grade astrocytoma, brain stem glioma and ependymoma.Study Design: Phase II trial.Contact: Joanne M. Hilden, M.D., 216.444.8407, or Bruce H. Cohen, M.D., 216.444.9182.
C.O.G.-P���2: A Phase II Trial of Intrathecal Topotecan in Patients with Refractory Meningeal MalignanciesDescription: The study seeks to determine the therapeutic activity (response rate and time to CNS progression) of intrathecal topotecan in patients with recurrent or refractory neoplastic meningitis.Eligibility: Patients must be at least 1 year of age but less than 22 years of age at study entry. Patients must have neoplastic meningitis. Patients with meningeal lymphoma or leukemia must be refractory to conventional therapy including radiation therapy (meaning 2nd or greater relapse).Study Design: Phase II trial.Contact: Joanne M. Hilden, M.D., 216.444.8407, or Bruce H. Cohen, M.D., 216.444.9182.
C.O.G.-P����: A Phase II Trial of Irinotecan in Children with Refractory Solid TumorsDescription: The study seeks to determine efficacy of irinotecan in treatment of refractory pediatric brain tumors.Eligibility: Children must be at least one year and no more than 21.99 years of age at original diagnosis. Patients with histologi-cally documented brain tumors who exhibit recurrent or refractory tumor growth will be eligible. Patients will be stratified based on histology into the following groups: medulloblastoma/PNET, ependymoma, brain stem glioma, other CNS tumors.Study Design: In this Phase II trial,

�� Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
500
1000
0
Surgical Procedures | Annualized
‘01 ‘02 ‘03 ‘04 ‘05
Gamma Knife Cases
Surgical Cases
The Brain Tumor Institute (BTI) continues to grow in
volume of procedures. More than 240 stereotactic
radiosurgery (Gamma Knife) and 680 surgical procedures
were performed in 2005, which is a 57 percent increase
compared with 2001.
Brain Tumor Institute
Appendix B – Charts & Statistics
3250
6500
0
Total Outpatient Visits
‘01 ‘02 ‘03 ‘04 ‘05
Total outpatient visits increased by
250 percent over the past five years,
reaching a high point of more than
5,900 visits in 2005.
patients receive irinotecan 5 of every 21 days; patients demonstrating continued response or stable disease without significant toxicity may continue treat-ment. Subsequent radiographic evalua-tions would be performed every 3 months as indicated.Contact: CLOSED TO PATIENT ACCRUAL.
RegistryATT/RT Registry (IRB #5���): Central Nervous System Atypical Teratoid/Rhabdoid Tumor RegistryDescription: The registry collects information (with patient consent) about the clinical course, treatment, and outcomes of patients with atypical teratoid/rhabdoid tumor of the CNS.Eligibility: Patients with atypical teratoid/rhabdoid tumor of the central nervous system.Contact: Joanne M. Hilden, M.D., 216.444.8407, or Bruce H. Cohen, M.D., 216.444.9182.
Biology StudiesCCG-B���: Protocol for Collection of Biology Specimens for Research StudiesDescription: The study provides a specimen accrual mechanism within C.O.G.-participating institutions for human pediatric cancer tissues.Eligibility: All patients up to and including 21 years of age who have had biology specimen(s) suspected of malignancy obtained and/or enrolled in a C.O.G. thera-peutic trial.Contact: CLOSED TO PATIENT ACCRUAL.
CCG-B���: Prognostic Significance of Ki-�� Proliferative Index Utilizing the MIB-� Antibody in Low-Grade Gliomas in Young ChildrenDescription: This biology study attempts to determine the value of the Ki-67 proliferative index utilizing the MIB-1 antibody in predicting time to progression in low-grade gliomas in young children a) following initial diagnosis and b) at time of tumor progression if surgery is performed.Eligibility: Patients entered on CCG-A9952.
Study Design: Unstained slides are sent to C.O.G. at time of study entry.Contact: Joanne M. Hilden, M.D., 216.444.8407 or Bruce H. Cohen, M.D., 216.444.9182.
CCG-B���: Molecular Biology of Pediatric Brain TumorsDescription: This biology study will correlate molecular and cytogenetic findings with outcomes on C.O.G. clinical trials.Eligibility: All patients less than 21 years of age with a primary CNS malignancy consistent with PNET/MB or ATT/RT who are entered on CCG front-line studies. Patients cannot have received any prior radiation treatment before the tissue was obtained. Study credit will be given for specimens obtained retrospectively on closed CCG studies, providing samples are adequate for analysis.Study Design: Tissue is accessed at time of study entry.Contact: CLOSED TO PATIENT ACCRUAL.

2005 Annual Report A team approach to individualized care ��
250
500
0
New Outpatient Visits
‘01 ‘02 ‘03 ‘04 ‘05
New patient visits have increased by 192 percent since
2001, setting a new mark
of 529 visits in 2005.
250
500
0
Patient Enrollment
‘01 ‘02 ‘03 ‘04 ‘05
Therapeutic Trials
Genetic Trials
Over the past five years, the number of patients on
research trials has increased from 94 to 431, or 358
percent.
Brain Tumor Institute
Appendix C – ArticlesClinic Researchers Earn Patent for Blood-Brain Barrier TechnologyCleveland Clinic researchers have received a U.S. patent for technology they developed to measure damage to a person’s blood-brain barrier. The patent covers the researchers’ work to develop a blood test capable of indicating when a person’s blood-brain barrier has been compromised, if neuronal damage exists, and when the person might be more responsive to therapies that need to reach the brain to treat tumors or other neurological disorders.
The patent was issued to Cleveland Clinic researchers Damir Janigro, Ph.D., and Gene Barnett, M.D. Dr. Janigro is a professor of molecular medicine and director of cerebrovascular research for Cleveland Clinic Lerner College of Medicine. Dr. Barnett is chairman of the Cleveland Clinic Brain Tumor Institute and professor of surgery and oncology.
“Determining the integrity of the blood-brain barrier is crucial in understanding disease states,” Dr. Janigro says. “This blood test is a quick and easy way to determine the most appropriate treatment for many different patients.”
The blood test would provide a minimally invasive alternative to painful spinal taps currently used to assess the condition of a patient’s blood-brain barrier. In addition, Dr. Janigro says, this blood test has the potential to save millions of dollars in MRI and CT scan costs.
MRI FLAIR Axial View with Enhancement
Axial View with Enhancement
Coronal View with Enhancement
Axial View MRI FLAIR
S-100 beta levels in patient with small (top) vs. larger brain metastases (bottom). Higher numbers indicate greater breakdown of the blood-brain barrier.
Small Metastases 0.��
Large Metastases 0.��

�0 Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
CCF Innovations, the Cleveland Clinic’s technology transfer arm, is actively working to commercialize the technology through a license or a new company.
The work of Drs. Janigro and Barnett has shown that when a high level of S100b, a protein normally found in brain cells, is detected in the blood stream, it can signal a disruption of the blood-brain barrier. This disruption, in turn, can indicate the
Proteomic Profiling Holds Promise for Identifying Markers of InterestRobert J. Weil, M.D., Associate Director of Basic Research, Brain Tumor Institute
Early detection of cancer is crucial for its treatment, control and prevention. Identifica-tion of diagnostic and prognostic markers, as well as therapeutic targets, is a major goal in cancer research. Correlation of morphologic phenotypes of cancer with their expres-sion profile is a promising approach to detecting unique markers that can assist in the diagnosis and management of disease or serve as targets for therapy. A variety of new and powerful methods have been developed in recent years to foster these goals, including microarrays (DNA or “gene” chips).
Among recent technologic advances, proteomics (modeling of many proteins, the products of the genes, which are the source of all the action inside normal, as well as cancerous, cells) may have great potential as a facile tool to identify a number of
presence of a brain tumor or brain injury. In contrast, when an individual’s blood-brain barrier is intact or working properly, the level of S100b in the bloodstream is low or even undetectable.
“This test could prove useful in the early detection of brain tumors, particularly in patients with lung, breast or other systemic cancers where the risk of their cancer spreading to the brain is one in four,” Dr. Barnett says.
Robert J. Weil, M.D.

2005 Annual Report A team approach to individualized care ��
Figure LegendsFigure �. A schematic representation of the method of analyzing tissues with two-dimensional gel electrophoresis and identifying the unique proteins with mass spectrometry (LC/MS/MS).
Figure 2. Representative picture of the two types of GBMs with proteins common to the two types and unique to one or the other type. The boxes below show a small segment of a 2-D gel to illustrate the individual proteins.
Figure �. Matrix-assisted laser desorption/ionization mass spectrometry (MALDI-MS) methodology. A nitrogen laser is shot at cells, and the absorption of energy leads to scattering of individual proteins, which are picked up in the mass
spectrometer and characterized. Sophisticated computer programs are used to smooth out the data, which are first studied to get information about tumor type and then compared to different tumors to detect subtle differences between tumors of the same type.
Figure �. An example of how comparing the spectra from tumors of the same type can reveal subtle differences in otherwise similar-appearing tumors of the same type, for example, gliomas. Here we see that it is possible to divide a group of patients, followed over many years, into those who are likely to do well (blue line, top) from those who are less responsive to treatment (red line, bottom).
markers of interest. Proteomic profiling to characterize the expression patterns of benign cells and to compare them with cancer cells appears to be a promising approach to identifying markers of interest.
A variety of methods, including two-dimensional gel electrophore-sis (2DGE), matrix-assisted laser desorption/ionization mass spectrometry (MALDI-MS), surface-enhanced laser desorption-ionization (SELDI), and protein microarrays, have been utilized to study normal and cancer cells, as well as a selection of body fluids, such as blood, saliva and urine, to look for changes that predict the presence of cancer. In the study of gliomas, we have focused recently on two methods, 2DGE and MALDI-MS.
Gliomas are the most common primary brain tumors of adults, with a yearly incidence of approximately 25,000 cases in the United States. The most common form of glioma is the glioblas-toma multiforme (GBM), an aggressive and malignant tumor. Despite decades of research on tumor biology and treatment, patients with GBMs continue to have a poor prognosis, with a median survival of one year following aggressive surgical and adjuvant therapy. GBMs account for an estimated 2.5 percent of all cancer deaths in the United States, and treating these tumors remains a high priority for researchers and clinicians.
2DGE protein identification and proteomic profiling methods have seen considerable technological improvements since 2DGE was first used to analyze gliomas in the 1980s. 2DGE analysis is an effective method to identify proteins involved in human disease. Despite its potential, however, many proteomic methodologies are limited by the complexity of cancer tissues, where a mixture of neoplastic and non-neoplastic cells can hamper the effort to acquire a pure tumor cell signature. In addition, heterogeneity among tumor types at a single site can increase the complexity of proteomics and other gene expression approaches.
Further refinements in gene expression and protein profiling were realized with the more recent development of selective tissue microdissection, which enables the procurement of pure populations of cells of interest. In concert with colleagues at the National Institutes of Health, we used selective tissue microdis-section of primary tumor samples to study a group of GBMs.
Two types of GBMs have previously been described: de novo or primary GBMs, which typically arise in older individuals, and secondary or progressive GBMs, which arise several years after the first manifestation of a lower grade glioma, typically found in younger patients.
We used selective tissue microdissection to procure pure populations of glioblastoma cells and analyzed them by 2DGE. In each case, the protein expression patterns could be classified into one of two groups, which coincided with the clinical distinction of primary or secondary. Unique expression of a number of proteins was identified on a large scale between members of the primary or secondary tumors. We isolated and sequenced some of these proteins and identified several proteins known or suspected in gliomas and/or other cancers. In addition, we identified several proteins not previously known to be expressed in normal brain and glial tissue or to be a part of gliomagenesis.
In a second study, in collaboration with colleagues at the National Institutes of Health and Vanderbilt University, we used a direct-tissue protein profiling approach to tumor analysis using mass spectrometry (MALDI-MS) to correlate protein patterns obtained directly from tumor biopsies with patient survival trends. MALDI is not only a powerful method to confirm the diagnosis of a brain tumor, but it also can be used to “crunch” a tremendous amount of information to distinguish between people with the same type of tumor—for example, a GBM—and to identify protein patterns that predict different survival trends.
Both of these types of protein studies, along with others, can be used to improve diagnosis; identify prognostic markers in tumors and other tissues and fluids, like the blood; and, in the future, serve as useful adjuncts for predicting response to treatment and overall outcome.
These studies are still in their infancy; not just technologically, but also as predictive tools. These and other methods will be developed and studied in the Brain Tumor Institute in a larger group of patients, where their uses and limitations will become better understood.

�2 Cleveland Clinic Brain Tumor Institute clevelandclinic.org/braintumor
Surgical Management of Spinal Tumors Revolutionizes TreatmentThe days of a single therapeutic approach to all metastatic spine tumors are coming to a close.
For more than 20 years, external beam radiation has been the standard of care for patients with these tumors. Now the paradigm is shifting to surgical treatment prior to radiation as a better option for many patients, a strategy that Cleveland Clinic physicians Steven Toms, M.D., M.P.H., and Edward Benzel, M.D., believe offers significant advantages.
“There is compelling evidence that aggressive management of these tumors, including radiosurgery or surgical resection and decompression, followed by radiotherapy to sterilize the tumor bed, improves pain control and ambulation, preserves or restores bowel and bladder function and may confer a survival benefit,” Dr. Toms says.
Based on their personal experience as well as data from several small retrospective studies, Dr. Benzel, Chairman of the Cleveland Clinic Spine Institute, and Dr. Toms, a neurosurgeon in the Cleveland Clinic Brain Tumor Institute, have been promot-ing this broader treatment approach for patients with meta-static spine tumors for several years. A recent study in Lancet (2005;366(9486):643-648), in which surgery plus radiothera-py resulted in significantly better outcomes in quality of life measures and pain control compared with radiosurgery alone, has sparked wide-spread interest in surgical treatment as an adjunct to radiotherapy for these patients.
At Cleveland Clinic, surgical resection and spinal reconstruction, kyphoplasty to stabilize the spine, radiosurgery with the Novalis system, external beam radiation and chemotherapy all are potential elements of the treatment plan for spinal tumor patients.
“The key is to create an individualized plan for each patient based on tumor stage, the levels of the spine involved, the patient’s age and life expectancy, and quality of life considerations,” Dr. Benzel notes. Because of the often complex nature of these cases, the treatment decision is best made by a multidisciplinary team that includes spine surgeons, oncologists and radiation oncologists, he adds.
To implement this strategy at Cleveland Clinic, Drs. Toms and Benzel have established a Spine Tumor Board, an interdisciplin-ary committee that meets regularly to discuss these cases and plan appropriate treatment. The main candidates for consider-ation are patients with primary renal cell carcinoma, melanoma, or lung or breast cancer that has metastasized to the spine.
This multidisciplinary approach also offers advantages in the management of multiple myeloma. Cleveland Clinic orthopaedic surgeon Isador Lieberman, M.D., pioneered the use
of kyphoplasty in multiple myeloma patients to stabilize the spine prior to chemotherapy and/or tumor resection and spinal decompression. He has demonstrated that kyphoplasty can be performed at multiple levels in the spine and relieves pain, improves the ability to walk and significantly improves quality of life for these patients.
“Patients with pancoast tumors that have penetrated to the vertebral bodies are another population that may benefit from more aggressive surgical management,” Dr. Toms adds. At least one study has demonstrated that resection with negative margins and spinal reconstruction followed by radiotherapy confers a significant survival benefit in these patients.
To refer patients with spinal tumors to the Spine Tumor Board, call the Cleveland Clinic Spine Institute at 216.444.2225 or 800.223.2273, ext. 42225.
Figure 1 [L5 spine met files]: Patient presented with low back pain and leg pain with a history of renal cell carcinoma. Preoperative saggital MRI shows a collapsed vertebral body at the fifth lumbar level (L5) with tumor extending into the pedicle and causing compression of an exiting nerve root. The tumor was removed using a posterior approach and reconstructed with methylmeth-acrylate (bone cement), Steinmann pins and pedicle screws fixation. The patient’s pain resolved, and he remained ambulatory after surgery.
Figure 2: Patient presented with a persistent cough and new hand pain and numbness. Pre-operative axial MRI shows a lesion of the apex of the lung (superior sulcus) representing a primary lung cancer. The tumor, which had invaded the brachial plexus and vertebral body of the spine, was removed via thoracotomy. The brachial plexus was identified, and arm and hand motor function preserved. A partial vertebrectomy was performed to remove the tumor from the vertebral body while avoiding the need for anterior spinal column reconstruction. The extensive bony and soft tissue resection did require spine stabalization using lateral mass and pedicle screws from a posterior approach in a staged second surgery.

2005 Annual Report A team approach to individualized care ��
Mladen Golubic, M.D., Ph.D.
A Dietary and Herbal Approach to Reducing Peritumoral Brain EdemaCleveland Clinic cancer researchers have initiated a clinical study of the effect of a vegan diet combined with herbal therapy on edema caused by glioblastoma multiforme (GBM). The two-pronged approach will be used as an adjuvant to standard therapy.
Because 5-LO-derived eicosanoids stimulate tumorigenesis and inflammation that lead to development of peritumoral brain edema, inhibition of 5-LO is an attractive therapeutic target.
“Cancer results from complex interactions between a genetically susceptible host and a variety of environmental factors. Diet is an important, modifiable environmental factor. Foods contain a spectrum of compounds that may modulate carcinogenesis by several mechanisms, including pro- and antioxidant effects, regulation of enzymes that detoxify carcinogens and alterations of hormone metabolism. Modulation of inflammation by compounds found in foods and herbs has recently attracted a lot of attention because of identification of critical molecular links between the processes of inflammation and carcinogenesis,” says Principal Investigator Mladen Golubic, M.D., Ph.D., of the Cleveland Clinic’s Brain Tumor Institute and Center for Integrative Medicine.
Dr. Golubic’s team recently demonstrated that a pro-inflamma-tory 5-lipoxygenase (5-LO) enzyme is aberrantly upregulated in GBM. 5-LO oxidizes nutritionally relevant fatty acids present in abnormally high concentrations in GBM, turning them into biologically active eicosanoids. Because 5-LO-derived eico-sanoids stimulate tumorigenesis and inflammation that lead to development of peritumoral brain edema, inhibition of 5-LO is an attractive therapeutic target. The research team is hoping their twopronged approach will inhibit 5-LO eicosanoid production and decrease peritumoral brain edema with fewer side effects than glucocorticoids.
In this study, funded by the national cancer institute, patients are randomized to a low-fat vegan diet plus boswellia serrata (frankincense) or to a diet recommended for cancer survivors by the american cancer society. B. serrata resin contains boswellic acids that inhibit 5-LO in a direct, non-redox, and non-competi-tive way distinct from that of other inhibitors. In two small german studies, crude herbal preparation of B. serrata was found to be beneficial in reducing brain edema in some patients with GBM. However, patients were not asked to reduce intake of dietary fats, which 5-LO uses to produce pro-inflammatory and pro-tumorigenic eicosanoids.
In the Cleveland Clinic study, B. serrata is combined with a low-fat vegan diet. Arachidonic acid, the key fatty acid from which eicosanoids are produced, is derived almost exclusively from animal sources. Thus, the intervention diet will consist exclusively of plant foods such as vegetables, legumes, unrefined whole grains, spices and fruits. A novel standardized preparation of B. serrata is used in place of crude extract. Because the preparation is solubilized in lipids, boswellic acids are expected to be more bioavailable.
GBM tumor growth, peritumoral brain edema and use of glucocorticoids are monitored every two months. Plasma measurements of 5-LO eicosanoids and boswellic acids are taken to evaluate adherence to therapy. “Incorporation of a combina-tion of dietary and herbal approaches as an adjuvant to standard
care allows patients to take charge of their lives, which is a major reason why patients with GBM are attracted to nutritional and herbal therapies,” says Dr. Golubic. To reach Dr. Mladen Golubic, call 216.445.7641 or e-mail [email protected].
Frankincense, Key Medicinal Herb of the Ancient WorldTWO THOUSAND YEARS AGO, the “bestselling drug” was frankincense. The herb, with medicinal properties, is the product of a medium-to-large tree, Boswellia serrata, found in the dry hills of North Africa, the Middle East and India. The resin, exuded by the tree during winter months and deposited on the bark, contains oils, terpenoids and gum.
Historically, crude preparations of oleoresin exudate from the frankincense tree were widely used to treat wounds and various types of skin lesions. Hippocrates used frankincense to treat persistent ulcers. Avicenna, the foremost Arab physician of the 11th century, recommended it for inflammation, infections of the urinary tract, tumors, fevers, vomiting and dysentery. In Indian Ayurvedic medicine, frankincense is used as a remedy for rheumatism as well as inflammatory conditions of the eye and respiratory system. Modern clinical studies concur with ancient medical wisdom regarding its effectiveness in patients with bronchial asthma, ulcerative colitis, Crohn’s disease and osteoarthritis.

NeurosurgeryGene H. Barnett, M.D., F.A.C.S. Chairman, Brain Tumor Institute
Lilyana Angelov, M.D.
William Bingaman, M.D.*
Nicholas Boulis, M.D. *
Joseph F. Hahn, M.D.*
Damir Janigro, M.D.*
Joung Lee, M.D. Director, Section of Neurofibromatosis and Benign Tumors Head, Section of Skull Base Surgery
Mark Luciano, M.D., Ph.D.*
Peter Rasmussen, M.D.*
Samuel Tobias, M.D.*
Steven Toms, M.D., M.P.H. Head, Section of Metastatic Disease
Michael A. Vogelbaum, M.D., Ph.D. Director, Center for Translational Therapeutics
Robert Weil, M.D. Section Head, Pituitary and Neuroendocrine Surgery and Associate Director of Basic Laboratory Research
Henry Woo, M.D.*
NeurologyBruce H. Cohen, M.D.* Co-Director, Pediatric & Adolescent Brain Tumor Program
Glen H. Stevens, D.O., Ph.D. Head, Section of Adult Neuro-Oncology
Radiation OncologyAleck Hercbergs, M.D.*
Roger M. Macklis, M.D.*
John H. Suh, M.D. Director, Gamma Knife Center
Radiation Physics Christopher Deibel, Ph.D.
Gennady Neyman, Ph.D.
Martin S. Weinhous, Ph.D.
NeuropathologyRichard Prayson, M.D.*
Susan Staugaitis, M.D., Ph.D.*
Hematology & Medical OncologyBrian Bolwell, M.D.*
Medical OncologyDavid Peereboom, M.D. Head, Section of Medical Oncology
Pediatric OncologyKate Gowans, M.D.*
Joanne Hilden, M.D.* Chair, Pediatric Hematology & Oncology Co-Director, Pediatric & Adolescent Brain Tumor Program
Michael Levien, M.D.*
Gregory Plautz, M.D.*
Jawhar Rawwas, M.D.*
NeuroradiologyThomas Masaryk, M.D.*
Jeffrey S. Ross, M.D.*
Paul Ruggieri, M.D.*
Andrew Tievsky, M.D.*
Rehabilitative MedicineVinod Sahgal, M.D.*
ResearchGene H. Barnett, M.D. Chairman, Brain Tumor Institute
Nabila Bennani-Baiti, Ph.D.
Olga Chernova, Ph.D.
Peter Cohen, M.D.*
Mladen Golubic, M.D., Ph.D.
Andrei Gudkov, Ph.D.*
Jaharul Haque, M.D.*
Damir Janigro, Ph.D.*
Robert Miller, Ph.D. Senior Consultant
Gregory Plautz, M.D., Ph.D.*
Suyu Shu, Ph.D.*
Susan Staugaitis, M.D., Ph.D.*
Steven Toms, M.D., M.P.H. Head, Section of Metastatic Disease
Bruce Trapp, Ph.D.*
Raymond Tubbs, D.O.*
Michael A. Vogelbaum, M.D., Ph.D. Director, Center for Translational Therapeutics
Ilka Warshawsky, M.D.*
Robert Weil, M.D. Associate Director, Basic Laboratory Research Section Head, Pituitary and Neuro-Endocrine Surgery
Bryan Williams, Ph.D.*
Nursing/Physician AssistantsCathy Brewer, R.N.
Gail Ditz, R.N., B.S.N.
Sandra Ference, M.S.N., C.N.P.
Michele Gavin, M.P.A.S., P.A.-C.
Betty Jamison, R.N., B.S.N.
Debra Kangisser, P.A.-C.
Kathy Lupica, M.S.N., C.N.P.
Mary Miller, R.N., B.S.N.
Carol Patton, R.N.
Rachel Perez, R.N., B.S.N.
Sherry Soeder, M.S.N., C.N.P.
Lisa Sorenson, M.S.N., A.C.N.P.
Laural Turo, R.N., B.S.N.
Carla Yoder, M.S.N., C.N.P.
AdministrationKim Blevins Medical Secretary Work Leader
Michael Lawson, MBA Taussig Cancer Center Division Administrator
George Lawrence IV, MBA BTI Administrator
Henrietta-English West Patient Access Coordinator
Wendi Evanoff, B.A.
Noreen Flowers*
Charlotte Horner Patient Access Coordinator
Eric LaPresto
Systems Engineer
Sally McCartney
James Saporito Executive Director of Development
Kristin Swenson, MBA* Marketing Associate
Martha Tobin* Continuing Medical Education
Sherri Wilson
Tanya Wray, MBA* Marketing Manager
Cancer Center Research SupportJoanne Civic
Robert Gerlach
John Pellecchia
Kathy Robinson
Patricia Weiss, R.N.
Brain Tumor Institute Faculty*Denotes joint appointment

2005 Annual Report A team approach to individualized care �5
Members of the Brain Tumor Institute are available for consultation 24 hours a day, seven days a week. Their goal is to see patients with diagnosed or suspected brain tumors within 24 to 48 hours.
216.445.8971 or 800.553.5056, ext. 58971 (weekdays 8 a.m. to 5 p.m.) for consultations and/or hospital admission.
216.444.2200 (nights and weekends). Ask for neuro-oncology staff or the chief neurosurgical or neurological resident on call. For pediatric patients, ask for the chief pediatric neurological resident on call.
How to Refer a Patient to the Cleveland Clinic Brain Tumor Institute
Patient appointment line: 216.445.8971 or 800.223.2273, ext. 58971
Clinical trials information: Toll-free 866.223.8100 (Cancer Answer Line)
Cleveland Clinic Florida (Weston): 954.659.5000
For details about the Brain Tumor Institute, please visit clevelandclinic.org/braintumor
Related Documents