_-- :

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
_-- :
REVIEW ARTICLES
f{ow to tırıaIrıage irregularbleeding or spotting after
I|üG-IUS insertİonSezai Şahmay
Department of Obstetrics and Gynaecology, Diaision of Reproductiae Endocrinology and lğertility,Cerrahpaşa Medical Faculty, lstanbul Uniııersity, Istanbul, Turkey ([email protected])
Introduction
The levonorgestrel-releasing intrauterine system(LNG-IUS; Mirena@) is a long-term, progestogen-onlymethod of contraception [1, 2]. Since its launch inFinland in 7990, it has become available in more than100 countries and today is estimated to be used bymore than 10 million women worldwide [2-4].
The LNG{US was developed primarily as a contra-ceptive device for up to 5 years of use [1, 5]. Its effectsare local and hormonal, including prevention ofendometrial proliferation. A low dose of levo-norgestrel is released into the uterine cavity, causingendometrial suppression and leading to endometrialatrophy, so that for many women its use is associatedwith little or no vaginal bleeding |1,,2, 4, 6f.
Occurrence of irregular bleeding
Irregular bleeding or spotting is the most commonunwanted adverse effect and reason for discontinua-tion, especially in the first few months followinginsertion [2, 4, 7-9]. The term 'spotting' refers to asmall amount of vaginal bleeding that does notrequire the use of sanitary protection; the term 'vagi-nal bleeding' means that sanitary protection isrequired [5, 10-13].
lloııce the endometria7 efficts become.established, in the ınajoritg of woınen the
bleeding pattern graduallg turns tooligomenowho e a or atnenoryhoe a usually
within 6-12 ınonths after insertion.''
Once the endometrial effects become established, inthe majority of women the bleeding pattern graduallyturns to oligomenorrhoea or amenorrhoea usuallywithin 6-12 months after insertion [7, 9].
The rate of adverse effects varies between studies:irregular bleeding or spotting is reported by 75-717oof women following insertion; progestogenic adverseeffects by 24-61,%; and abdomino-pelvic pain by1240%.
The LNG-IUS must be fitted and removed by aqualified practitioner |1, 9, 12-1,5].
Causes of irregular bleeding
The underlying mechanisms that cause irregularbleeding or spotting with progestogen-only contra-ception are not fully understood [3, 11] and may beexplained by multiple factors I11,,74,76].
Bleeding in users of progestogen-only contracep-tives is usually related to estrogen deficiency. Insuffi-cient suppression of ovarian activity is another mech-anism for irregular bleeding. Fewer than half of cyclesin LNG-IUS users are ovulatory 13, 6,73,77l.
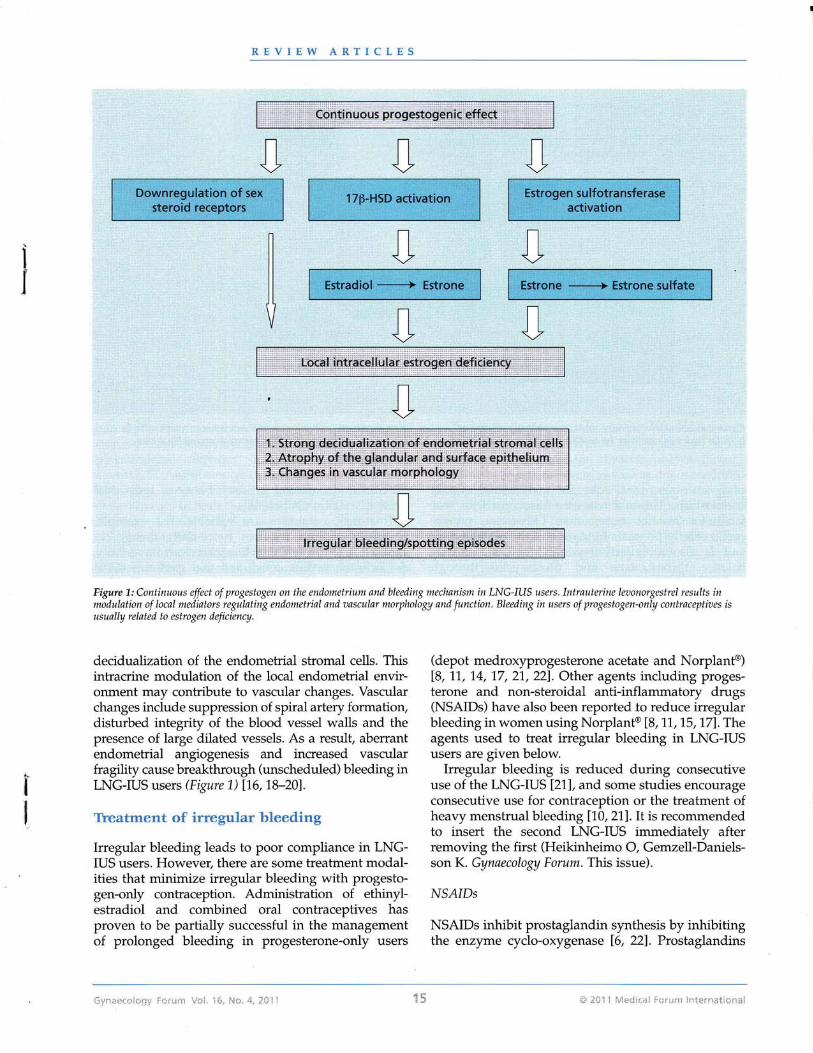
On the other hand, the long-term use of intrauterinelevonorgestrel results in modulation of local media-tors regulating endometfial and vascular morphologyand function. The histological changes begin todevelop from the first month after insertion andpersist until the device is removed.
Endometrial exposure to levonorgestrel results in amarked downregulation of sex steroid receptors(progesterone, estrogen and androgen receptors) in allcellular components of the endometrium [18, 19].
77!-Hydroxysteroid dehydrogenase type 2 (17P-HSD2) is expressed in endometrial glandular epithe-lium and is upregulated by progesterone. 17F-HSD2converts potent estradiol to less potent estrone. Theendometrial glands are exposed to higher levels of theweak estrogen (estrone), and thus the endometriummay develop a local intracellular estrogen-deficientenvironmen t 17 6, 1,8--20].
Over time, exposure of the endometrium to highconcentrations of levonorgestrel results in marked atro-phy of the glandular and surface epithelium and heavy
I
I
ö }ü] ] [,{ıdiııl iııı:ı: iııeııııiiıııı;i ('{nae.L]i.üı| İııııı !/ç|. ]ç, ı;*, ı. , ıül İ

REVIEW ARTICLES
Figure 2: Mechanism of action of NSAIDs in reducing menstrual blood loss. Prostaglandin (PG) leaels are eleaated in women with menorrhagia.NSz{tDs inhibit PG synthesis by inhibiting the enzyme cyclo-oıygenase. NSdDs reduce both endometrial PG concentrations and blood loss.
differences in clinical efficacy between individualprostaglandin inhibitors [6].
Treatment responses ale variable. For example,naProxen sodium requires twice-daily dosing, incontrast to ibuprofen, which is taken four times daily.A Cochrane review concluded that gastrointestinalside effects may be greater with naproxen than withmefenamic acid (in one study) [6]. There is no stan-dard dosage and duration of NSAID usage/ and indi-vidual NSAID treatment is convenient for reducingthe amount of bleeding and severity of pain. Mefe-namic acid is the most'commonly studied agent, theusual dosage being 500 mg three times a day. Thedosage for naproxen is 500 mg twice a day duringthe bleeding or spotting period. The dosage regimenfor ibuprofen is 1200 mg pel day in divided doses16,23l.
NSAIDs should be considered a first-line therapyfor bleeding and pain associated with IUD ııse I22,23]. The optimal NSAID and regimen option isunclear, so the choice may be based on cost/ conveni-ence or side effects. Studies do not support prophy-lactic ibuprofen usage for the first six menses afterIUD insertionI24].
Tranexamic acid
Plasminogen acüvators are a group of enzymes thatcause fibrinolysis (the dissolution of clots). Womenwith bleeding problems have high levels of plasmino-
p|ay an important role in endometrial vesselhaemostasis. Thromboxane is a vasoconstrictor thatfacilitates platelet aggregation. Otherwise, prosta-cyclin chiefly prevents formation of the platelet plugand is also an effective vasodilator. All NSAIDsbalance thromboxane and prostacyclin throughprostaglandin synthase inhibition. Prostaglandinsynthase inhibitors decrease menstrual bleeding by50% (Figure 2). Most studies have shown that NSAIDsare effective therapy for irregular bleeding and painrelated to the use of IUDs l1,4,22-24].
"Iwegular bleeding is redwced duingconsecutiue use of the LNG-IUS, &nd *ome
studİes encourage consecutİue use forcontracepıtioıı or tha treatment of heavgmenstrual bleeding. It is recoınmended
to inseıi the second lNG-IUS imınediatelgafter remouing the first."
It has been shown that prostaglandin levels areelevated in women with excessive menstrual bleeding.NSAIDs reduce endometrial prostaglandin concentra-tions as well as the amount of blood loss [6,24l.
NSAIDs include mefenamic acid, naproxen, ibupro-fery flurbiprofen, meclofenamic acid, diclofenac,indomethacin and acetylsalicylic acid. There are no


REVIEW ARTICLES
Warner et al. [4] studied the use oi CDB-291,4 50mg/day orally for 3 consecutive days, with separatetreatments starting 27,49 and77 days after LNG-IUSinsertion. The effect of CDB-2914 on bleeding/spot-ting was initially beneficial but by the third treatmentperiod was less advantageous than placebo.
conclusion
NSAIDs and tranexamic acid offer simple and effec-tive therapies and should be considered as first-linetherapy options in LNG-IUS-related bleeding/spot-ting and pain. Tranexamic acid is more effective thanNSAIDs in decreasing bleeding.
If bleeding is associated with pain, NSAIDs shouldbe considered as first-line therapy. Tianexamic acid issuitable in cases with only bleeding/spotting, since itoffers no pain relief.
References
1. National Collaborating Centre for Women's and Children'sHealth, National Institute for Health and Clinical Excellence.Heavy rnenstrual bleeding. Clinical guideline 44. London:RCOG Press, 2007. Available at: http://guidance.nice.ory.ıık / CG44 / Guidance /pdf / English. Accessed 1 5 July 2011.
2. Endrikat J, Vilos G, Muysers C, et al. The levonorgestrel-releas-ing intrauterine system provides a reliable, long-term treatmentoption for women with idiopathic menorrhagia. Arch GynecolObstet 2011; Apr 8 [Epub ahead of print].
3. Inki P. Long-term use of the levonorgestrel-releasing intrauter-ine system. Contraception 2007;75 (suppl 6): 5767-6.
4. Warner P, Guttinger A, Glasier AF, et al. Randomized placebo-controlled trial of CDB-2914 in new users of a levonorgestrel-releasing intrauterine system shows only short-lived amelio-ration of unscheduled bleeding. Hum Reprod 201,0; 25:345_53,
5. Jensen Jl Nelson AL, Costales AC. Subject and clinician experi-ence with the levonorgestrel-releasing intrauterine system.Contraception 2008; 77 : 22-9.
6. Lethaby A, Augood C, Duckitt K, Farquhar C. Nonsteroidalanti-inflammatory drugs for heaılı menstrual bleeding.Cochrane Database Syst Rev 2007; 4: CD000400.
7. ESHRE Capri Workshop Group. Intrauterine devices andintrauterine systems. Hum Reprod Update 2008; 74: 1,97 -208.
8. Lal S, Kriplani A, Kulshrestha V, et al. Eihcacy of mifepristonein reducing intermenstrual vaginal bleeding in users of thelevonorgestrel intrauterine system. Int J Gynecol Obstet 2010;109: 128-30.
9. Chi C, Huq FY, Kadir RA. Levonorgestrel-releasing intrauterinesystem for the management of heaıy menstrual bleeding in
. women with inherited bleeding disorders: long-term follow-up. Contraception 2011; 83:242-7.
10. Gemzell-Danielsson K, Inki P, Boubli L, et al. Bleeding patternand safety of consecutive use of the levonorgestrel-releasingintrauterine system (LNG-IUS) - a multicentre prospectivesfudy. Hum Reprod 2070;25: 354-9.
11. Mansour D, Bahamondes L, Critchley H, et al. The manage-ment of unacceptable bleeding patterns in etonogestrel-releas-ing contraceptive implant users. Contraception 2011,; 83:.
202-10.12. Hidalgo M, Bahamondes L, Perrotti M, et al. Bleeding patterns
and clinical performance of the levonorgestrel releasingintrauterine system (Mirena@) up to two years. Contraception2002;65:129-32.
13. Backrnan T, Huhtala S, Blom T, et al. Length of use and s;.mp-toms associated with premafure removal of the levonorgestrelintrauterine system: a nation-wide study of 17,360 users. Br JObstet Gynaecol 2000; 1,07:335-9.
14. Abdel-Aleem H, d'Arcangues C, Vogelsong KM, GulmezogluAM. Treatment of vaginal bleeding irregularities induced byprogestin only contraceptives. Cochrane Database Syst Rev2007;4: CD003449.
15. Ewies AAA. Levonorgestrel-releasing intrauterine system -the discontinuing story. Gynecol Endocrinol 2009 ; 25: 668-73.16. Guttinger A, Critchley HO. Endometrial effects of intrauterine
levonorgestrel. Contraception 2007;75 (6 suppl): 593-8.17. Şahmay S. Menstrual cycle and dysfunctional uterine bleeding
[in Turkish]. Istanbul: Esin Ofset,2007.18. Burton K, Henderson TA, Hillier SG, et a1. Local levonorgestrel
regulation of androgen receptor and l7P-hydroxysteroid dehy-drogenase type 2 expression in human endometrium. HumReprod 2003; 18: 261,0-17.
19. Critchley HO, Wang H, Kelly RW, et al. Progestin receptorisoforms and prostaglandin dehydrogenase in theendometrium of women using a levonorgestrel-releasingintrauterine system. Hum Reprod 7998; 73: 1210,1,7.
20.
27.
Smith MOP, Critchley HO. Progestogen only contraception andendometrial breakthrough bleeding. Angiogenesis 2005; 7:
1-10.Heikinheimo O, Inki R Kunz M, Gemzell-Danielsson K. Predic-tors of bleeding and user satisfaction during consecutive use ofthe levonorgestrel-releasing intrauterine system. Hum Reprod2010;25:7423-7.
22. Şahırıay S, Erfungealp E, Arvas M, Atasu T. Antiprostaglandinsin therapy for side effects of intrauterine contraceptive devices[in Turkish]. Cerrahpaşa Tıp Fakii-ltesı Dergisı1987;18: 75-83.
23. Şahmay S, Kaleli S, Oral E, et al. Effect of different types ofintrauterine devices on intrauterine activity. Int J FertilWomen's Med 1999; 44:'],50-5.
24. Grimes DA, Hubacher D,,Lopez LM, Schulz KF, Non-steroidalanti-inflaınmatory drugs for heavy bleeding or pain associatedwith intrauterine-device use. Cochrane Database Syst Rev 2006;4: CD006034.
25. Lethaby A, Farquhar C, Cooke I. Antifibrinolytics for heavymenstrual bleeding. Cochrane Database Syst Rev 2000; 4:
CD000249.26. Phihpp CS. Antifibrinolytics in women with menorrhagia.
Thromb Res 2011; 727 (sıpp| 3): 5113-15.27. Milsorn I, Andersson K, Andersch B, Rybo G. A comparison of
flurbiprofen, tranexamic acid, and a levonorgestrel-releasingintrauterine contraceptive device in the treatment of idiopathicmenorrhagia. Am I Obstet Glmecol 1997;764: 879-a3.
O İ*j] lİt{il-ıi ıı)l*ı,: iıicıı;İ;.ıı: l:ı.,ıı.:*r;iıÇ! jiııı;ı 1ı'ı:i. :Ç- fuı. ı , ]ii ]
Related Documents