
How to approach a child with bleeding disorder
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

How To Approach A
child with Bleeding
Disorder
DR. KAMRAN AKBAR
PGR PEDIATRICS
UNIT 2
Approach includes:
History
Clinical Examination
Laboratory Findings

INHERITED DISORDERS ACQUIRED DISORDERS
Early age of presentation
Family history positive
More sever
Bleeding is the dominant feature
Single factor defect
Later age of presentation
Family history usually negative
Less sever
Clinical picture is dominated by the
underlying disorder e g. DIC
Multiple hemostatic defect

HISTORY:
If child bleeds
from superficial
cut with profuse
bleed?
If fever and
neurological
manifestations?
If history of viral
prodrome ?
Drug related
purpuraMeningococce
mia/TTP
If patient taking
aspirin ,
ibuprofen
,antibiotics.
Coagulation
disorderPlatelet Disorder HUS/ITP
If child bleeds
from injury ,
does the
bleeding stop
and resume?

If patient is
neonate ,
with history of
traumatic
delivery or
low APGAR.
If patient is
neonate , and
mother took
phenytoin .
If patient
receive
multiple
blood
transfusions in
the past.
If other family members
have similar problem of
abnormal bleeding or if
repeated episodes of
bleeding gums , prolonged
bleeding as a result of
circumcision.
DICVitamin K
DeficiencyCongenital Disorder
Post transfusional
purpura or
alloimunizational
HISTORY: continued

Clinical Examination
The examination should determine the presence of :
petechiae,
ecchymosis,
hematomas,
hemarthroses,
or mucous membrane bleeding.

Petechiae Purpura

Senile Purpura DIC

Look For :
Easy Bruising
Individuals with disorders of the collagen matrix and vessel wall may have loose joints and lax skin associated with easy bruising (Ehlers-Danlos syndrome).
Mucocutaneous
Bleed
Patients with
defects in
platelet-blood
vessel wall
interaction (VWD
or platelet
function defects)
Deep Bleed
(muscle or joints)
Individuals with a
clotting factor
deficiency of
factor VIII or IX
(hemophilia A or
B)
Lymphadenopathy +
hepatosplenomegaly
Leukemia
Lymphoma
Infection
Symmetric
Purpura on Legs
and buttocks
Henoch–
schonlein
Purpura
Ecchymotic
Lesions
Extensive and in
various stages of
revolutions
Physical Abuse
Bleeding Disorders
Vessel Wall
DisorderPlatelet Disorder
Coagulation
Factor
Abnormalities
Vessel wall disorder
Acquired Congenital
1. SENILE PURPURA
2. VASCULAR PURPURA
3. HENOCH SCHONLEIN PURPURA
1. HEREDITARY HEMORRHAGIC
TELENGIECTASIA
2. EHLERS DANLOS SYNDROME

Henoch-schonlein purpuraEhlers-Danlos syndrome
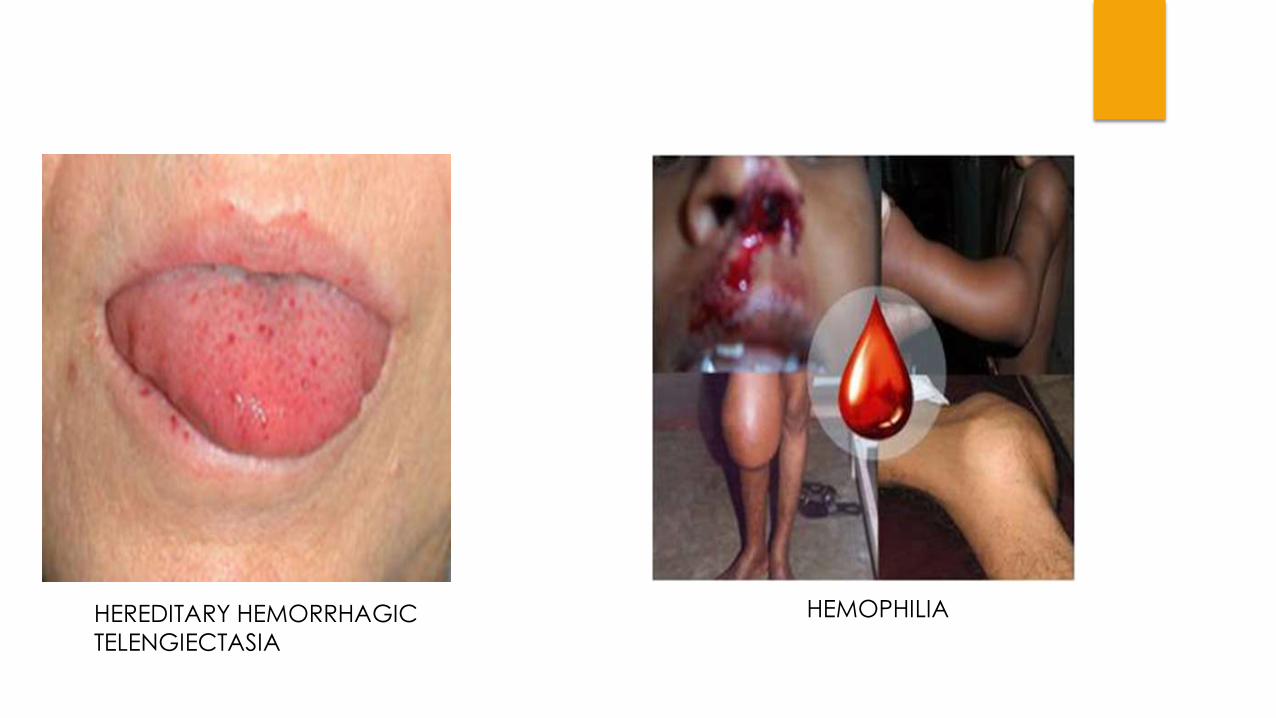
HEREDITARY HEMORRHAGIC
TELENGIECTASIA
HEMOPHILIA
Platelet Disorders
Qualitative Quantitative
• THROMBASTHENIA
• BERNARD-SOULIER SYNDROME
• DRUGS(ASPIRIN,TXA2,INDOMATHACIN
• THROMBOCYTOPENIA
• THROMBOCYTHEMIA
Coagulation
Factor
Abnormalities
Hereditary Acquired
1. HEMOPHILIA A(factor VIII deficiency)2. HEMOPHILIA B(factor IX deficiency)3. von WILLEBRAND DISEASE4. DISORDERS OF FIBRINOGEN-
HEREDITARY AFIBRINOGENAEMIA HYPOFIBRINOGENAEMI DYSFIBRINOGENAEMIA
1. DISSEMINATED INTRAVASCULAR COAGULATION(DIC)2. LIVER DISEASE3. VIT K DEFICIENCY4. MASSIVE TRANSFUSION OF STORED BLOOD5. ACQUIRED INHIBITORS OF COAGULATION6. HEPARIN OR ORAL ANTICOAGULANT THERAPY7. RENAL DISEASE
1. Full blood count and blood film
2. Bleeding time
3. Prothrombin time with INR – measure factors II, V,
VII, X.
4. Activated Partial thromboplastin time measures II, V,
VIII, IX, X, XI and XII.
5. Mixing studies
6. Thrombin Time
7. Quantitative fibrinogen assay
8. D-Dimers
9. Biochemical Screen for renal and Liver function tests
10. Platelet aggregation studies

CBC complete blood count, F factor PFA platelet function analyzer, PT prothrombin time, PTT activated partialthromboplastin time, RIPA ristocetin -induced platelet aggregation, vWD von Willebranddisease, vWF von Willebrand factor, vWF : R Co ristocetin cofactor activity.
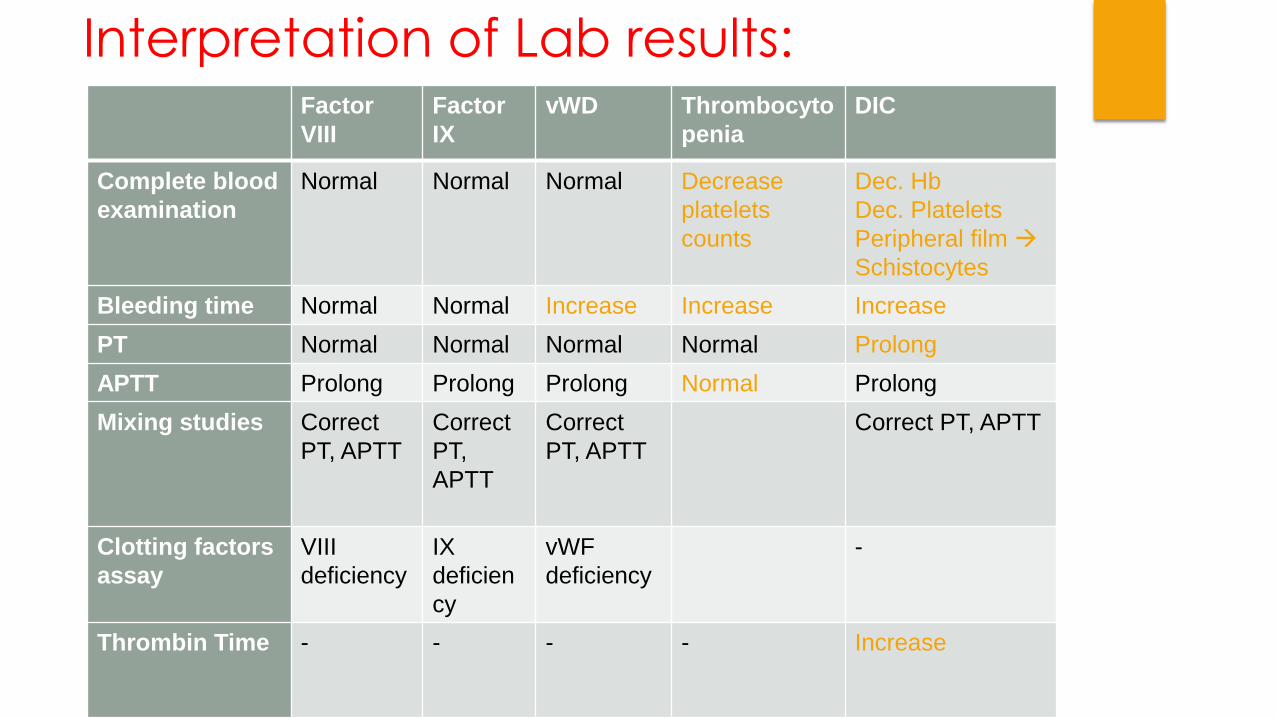
Interpretation of Lab results:Factor
VIII
Factor
IX
vWD Thrombocyto
penia
DIC
Complete blood
examination
Normal Normal Normal Decrease
platelets
counts
Dec. Hb
Dec. Platelets
Peripheral film
Schistocytes
Bleeding time Normal Normal Increase Increase Increase
PT Normal Normal Normal Normal Prolong
APTT Prolong Prolong Prolong Normal Prolong
Mixing studies Correct
PT, APTT
Correct
PT,
APTT
Correct
PT, APTT
Correct PT, APTT
Clotting factors
assay
VIII
deficiency
IX
deficien
cy
vWF
deficiency
-
Thrombin Time - - - - Increase
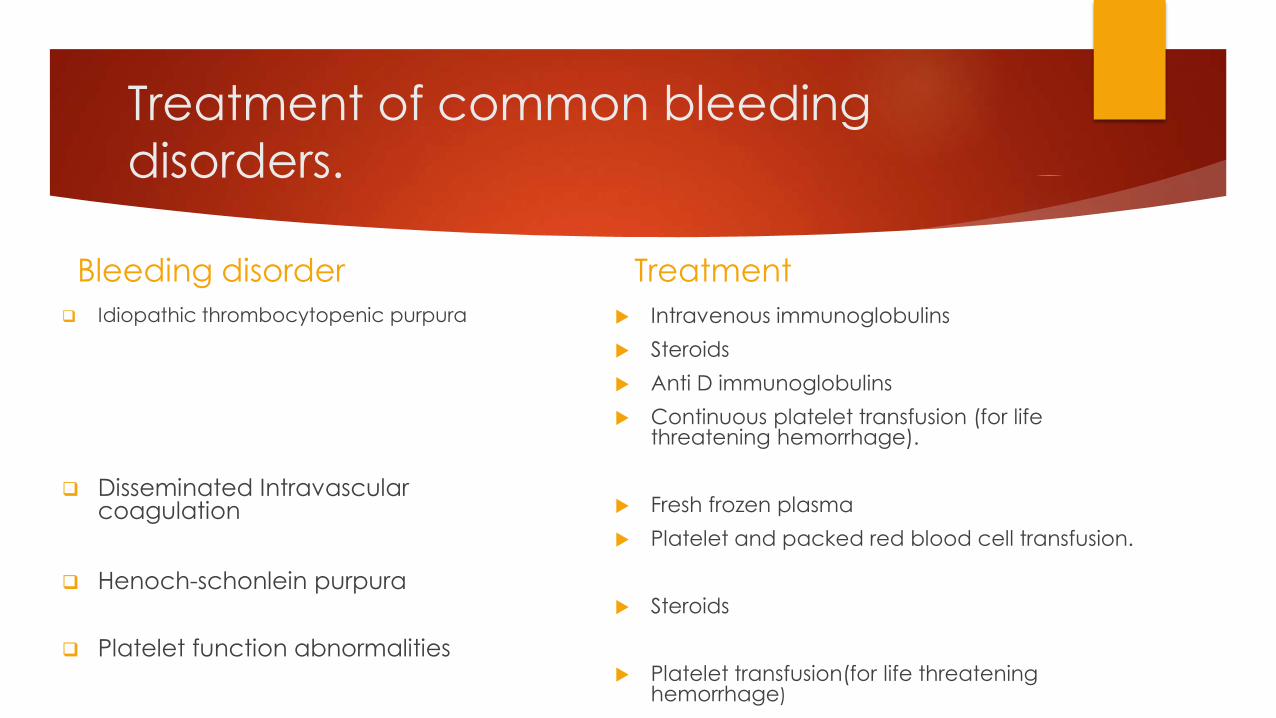
Treatment of common bleeding
disorders.
Bleeding disorder
Idiopathic thrombocytopenic purpura
Disseminated Intravascular coagulation
Henoch-schonlein purpura
Platelet function abnormalities
Treatment
Intravenous immunoglobulins
Steroids
Anti D immunoglobulins
Continuous platelet transfusion (for life threatening hemorrhage).
Fresh frozen plasma
Platelet and packed red blood cell transfusion.
Steroids
Platelet transfusion(for life threatening hemorrhage)

Bleeding disorder
Von willebrand
disease (vWD)
Treatment
Desmopressin acetate (DDAVP)
Treatment of common bleeding
disorders (continued)


Related Documents











