ORIGINAL PAPER How Religious Coping is Used Relative to Other Coping Strategies Depends on the Individual’s Level of Religiosity and Spirituality Christian U. Kra ¨geloh • Penny Pei Minn Chai • Daniel Shepherd • Rex Billington Published online: 2 November 2010 Ó Springer Science+Business Media, LLC 2010 Abstract Results from empirical studies on the role of religiosity and spirituality in dealing with stress are frequently at odds, and the present study investigated whether level of religiosity and spirituality is related to the way in which religious coping is used relative to other coping strategies. A sample of 616 university undergraduate students completed the Brief COPE (Carver in Int J Behav Med 4:92–100, 1997) questionnaire and was classified into groups of participants with lower and higher levels of religiosity and spir- ituality, as measured by the WHOQOL-SRPB (WHOQOL-SRPB Group in Soc Sci Med 62:1486–1497, 2006) instrument. For participants with lower levels, religious coping tended to be associated with maladaptive or avoidant coping strategies, compared to participants with higher levels, where religious coping was more closely related to prob- lem-focused coping, which was also supported by multigroup confirmatory factor analysis. The results of the present study thus illustrate that investigating the role of religious coping requires more complex approaches than attempting to assign it to one higher order factor, such as problem- or emotion-focused coping, and that the variability of findings reported by previous studies on the function of religious coping may partly be due to variability in religiosity and spirituality across samples. Keywords Coping strategies Á Religious coping Á Religiosity Á Spirituality Á Brief COPE Á WHOQOL-SRPB Introduction The psychological health benefits of religious involvement are very well documented (Koenig et al. 2001; Seybold and Hill 2001), but the mechanisms by which these effects emerge are still unclear. One way in which religion can exert a positive influence on psy- chological well-being is through its function as a resource in dealing with stress. Compared C. U. Kra ¨geloh (&) Á P. P. M. Chai Á D. Shepherd Á R. Billington Department of Psychology, Faculty of Health & Environmental Sciences, Auckland University of Technology, North Shore Campus, Private Bag 92006, Auckland 1142, New Zealand e-mail: [email protected] 123 J Relig Health (2012) 51:1137–1151 DOI 10.1007/s10943-010-9416-x

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ORI GIN AL PA PER
How Religious Coping is Used Relative to Other CopingStrategies Depends on the Individual’s Levelof Religiosity and Spirituality
Christian U. Krageloh • Penny Pei Minn Chai •
Daniel Shepherd • Rex Billington
Published online: 2 November 2010� Springer Science+Business Media, LLC 2010
Abstract Results from empirical studies on the role of religiosity and spirituality in
dealing with stress are frequently at odds, and the present study investigated whether level
of religiosity and spirituality is related to the way in which religious coping is used relative
to other coping strategies. A sample of 616 university undergraduate students completed
the Brief COPE (Carver in Int J Behav Med 4:92–100, 1997) questionnaire and was
classified into groups of participants with lower and higher levels of religiosity and spir-
ituality, as measured by the WHOQOL-SRPB (WHOQOL-SRPB Group in Soc Sci Med
62:1486–1497, 2006) instrument. For participants with lower levels, religious coping
tended to be associated with maladaptive or avoidant coping strategies, compared to
participants with higher levels, where religious coping was more closely related to prob-
lem-focused coping, which was also supported by multigroup confirmatory factor analysis.
The results of the present study thus illustrate that investigating the role of religious coping
requires more complex approaches than attempting to assign it to one higher order factor,
such as problem- or emotion-focused coping, and that the variability of findings reported
by previous studies on the function of religious coping may partly be due to variability in
religiosity and spirituality across samples.
Keywords Coping strategies � Religious coping � Religiosity � Spirituality � Brief COPE �WHOQOL-SRPB
Introduction
The psychological health benefits of religious involvement are very well documented
(Koenig et al. 2001; Seybold and Hill 2001), but the mechanisms by which these effects
emerge are still unclear. One way in which religion can exert a positive influence on psy-
chological well-being is through its function as a resource in dealing with stress. Compared
C. U. Krageloh (&) � P. P. M. Chai � D. Shepherd � R. BillingtonDepartment of Psychology, Faculty of Health & Environmental Sciences, Auckland Universityof Technology, North Shore Campus, Private Bag 92006, Auckland 1142, New Zealande-mail: [email protected]
123
J Relig Health (2012) 51:1137–1151DOI 10.1007/s10943-010-9416-x
to the considerable amount of research that has been published during the last 40 years on
secular coping strategies, religious coping has only recently received more attention in the
psychological literature (Folkman and Moskowitz 2004). The function of religious coping
relative to these other coping strategies is still being debated, and its assignment to higher
order coping factors remains unclear. Tamres et al. (2002), for example, noted that religious
coping could be clearly classified neither as problem nor as emotion-focused coping—a
popular distinction between coping strategies that defines the former as activities directly
addressing the source of the stressor, while the latter are responses aimed to change one’s
own reactions to the stressors (Lazarus and Folkman 1984).
Coping strategies are commonly assessed using a variety of self-report instruments, with
specific ones available to assess religious coping. The RCOPE (Pargament et al. 2000), for
example, is a multidimensional inventory that asks about a very broad range of coping
responses that involve the use of religious concepts. The questionnaire classifies religious
coping as either positive or negative, where positive coping includes forgiveness and
seeking of spiritual support, and negative religious coping includes spiritual discontent and
punishing God reappraisals. This level of detail and sub-classification of religious coping is
obviously not provided in general coping inventories. The COPE questionnaire (Carver
et al. 1989), for example, includes religious coping as one of 15 sub-scales, but it is assessed
by using four items only and not divided further into different types of religious coping. In
the Brief COPE (Carver 1997), the abbreviated version of the COPE, religious coping
remains one of 14 sub-scales, but is assessed by only two items. The limitations of such
general questionnaires to inform about the role of religious coping have been mentioned
(Lavery and O’Hea 2010; Schottenbauer et al. 2006b), but questionnaire length remains a
major consideration in the design and use of survey-based research (Carver 1997).
Because of its brevity the Brief COPE (Carver 1997) can be used easily in conjunction
with other questionnaires. The author of the scale even recommended the use of selected
sub-scales when researchers have very focused interests or need to restrict participant
response burden to a minimum. This flexibility is no doubt the reason for the popularity of
the instrument, which has been used in a wide range of populations, including people
suffering from migraine (Radat et al. 2009), parents of children with end-stage renal
disease (Zelikovsky et al. 2007), emergency workers (Cicognani et al. 2009), genetic
counselors (Udipi et al. 2008), and international university students (Miyazaki et al. 2008).
For the initial development of the Brief COPE, Carver (1997) conducted a principal
component analysis on data collected from a community sample of hurricane survivors and
reported that the two items from the sub-scale turning to religion loaded onto a unique
factor. Based on the recommendation of Carver to use the Brief COPE flexibly, researchers
often conduct a factor analysis to determine how to analyze coping scores in their par-
ticular sample (e.g., Radat et al. 2009; Zelikovsky et al. 2007). While some studies con-
firmed Carver’s (1997) results of turning to religion forming a separate factor (Cicognani
et al. 2009; Miyazaki et al. 2008), results from other studies vary tremendously, with
reports of the religious items loading onto higher order factors, such as together with the
two items from the denial sub-scale (Hastings et al. 2005), the items from the substanceuse sub-scale (Paukert et al. 2009), the items from the behavioral disengagement, denial,and self-blame sub-scales (Liu and Iwamoto 2007), or religious coping items not loading
onto any factor (Welbourne et al. 2007). Other researchers have taken the approach of
conducting exploratory factor analyses by treating sub-scale total scores as indicators
instead of individual items, but results here are equally variable. Farley et al. (2005), for
instance, reported that turning to religion loaded together with positive reframing,
acceptance, and humor, while Schottenbauer et al. (2006a) found that religious coping
1138 J Relig Health (2012) 51:1137–1151
123
loaded together with emotional support and instrumental support. Findings of turning toreligion forming its own factor are also reported (Weininger et al. 2006; Wood and
Rutterford 2006), as are findings of turning to religion failing to have sufficiently high
factor loading scores (Lawrence and Fauerbach 2003; Yang et al. 2008).
Results from exploratory factor analyses such as those mentioned above affect not only
the way coping data are analyzed in those studies, but also any general conclusions that the
researchers might derive about the role and function of religious coping. While it is
certainly valid to argue that low factor loadings of turning to religion with other coping
strategies could indicate that religious coping is a unique and independent strategy (Cook
and Heppner 1997; Hudek-Knezevic et al. 1999), the reasons for the large range of
reported factor structures still require further investigation. Kershaw et al. (2004) found
that religious coping loaded differently depending on whether an exploratory factor
analysis was conducted for patients with breast cancer or for their family caregivers. For
patients, the turning to religion sub-scale loaded together with active coping, planning,
positive reframing, acceptance, and emotional support, while for caregivers religious
coping loaded together with humor, self-distraction, venting, behavioral disengagement,denial, and substance use. This indicates that the characteristics of the sample can have a
substantial effect on the way religious coping is related to other coping strategies.
So far, no study has systematically explored how religious and spiritual beliefs affect
the use of religious coping relative to the secular coping strategies that are assessed by the
Brief COPE (Carver 1997). The varied reports of the role of religious coping in relation to
secular coping methods and the unclear assignment of religious coping to a higher order
factor structure might certainly be a reflection of differences in the role that religion and
spirituality play in different groups of people. In individuals with a religious affiliation,
religious orientation has been found to affect the manner in which religion is used as a
coping resource. An intrinsic religious orientation is more likely to be associated with
problem solving, and an extrinsic orientation more likely to be linked with cognitive
avoidance strategies (Aguilar-Vafaie and Abiari 2007; Pargament et al. 1992). However, in
countries like New Zealand, where more than 30% of the population does not self-identify
with a particular religious denomination (Perrott 2007), the intrinsic–extrinsic religious
orientation differentiation excludes a substantial proportion of people. Therefore, together
with the Brief COPE, participants in the present study completed the 32-item WHOQOL-
SRPB questionnaire (WHOQOL-SRPB Group 2006), which assesses the strength of a
person’s spiritual, religious, and personal beliefs. The advantage of this instrument is that it
is not limited to religiosity only, but also accounts for spiritual and personal beliefs that are
independent of any formal religious denomination. Moreover, the development of this
instrument occurred through an international collaborative project of 18 countries, and the
WHOQOL-SRPB is therefore considered cross-culturally valid and applicable to a wide
range of belief systems. If religious coping indeed plays a different role depending on the
degree of the spiritual and religious beliefs of an individual, it might be found to correlate
differently with the use of other, secular, coping strategies and may therefore also affect to
which higher order factor an exploratory factor analysis might assign religious coping.
Method
Participants
A convenience sample of university undergraduate students at a variety of different fac-
ulties at a university in New Zealand provided data on coping, demographic characteristics
J Relig Health (2012) 51:1137–1151 1139
123

and spiritual, religious and personal beliefs. A total of 712 participants completed the
questionnaire, of which 679 were valid. The mean age of the participants was 22.83 years
(SD = 6.88), and 179 respondents indicated that they were male, compared to 494 who
indicated that they were female. Slightly less than 50% of the participants (N = 330) stated
that they had a religious affiliation.
Instruments
Brief Cope
Participants were given the dispositional form of the Brief COPE (Carver 1997) ques-
tionnaire, which asked them to rate to what extent they usually use a range of strategies to
cope with stressful events. Although four ordinal response categories may be an acceptable
minimum to conduct factor analyses (Lozano et al. 2008), increasing the number to five
categories has been found to lead to clear gains in accuracy of model fits (Johnson and
Creech 1983; Lozano et al. 2008), and for that reason the present study used a five-point
Likert scale instead of the four-point scale that is commonly used for the Brief COPE. No
data were imputed for the Brief COPE, but instead a very stringent inclusion criterion was
used according to which only data from participants who completed all question items
were included.
WHOQOL-SRPB
The 32-item questionnaire asks respondents to rate on a five-point Likert scale their extent
of spiritual, religious or personal beliefs (WHOQOL-SRPB Group 2006). Scores are
presented both as total scores and as one of the following eight facets: spiritual connection,
meaning of life, awe, wholeness, spiritual strength, inner peace, hope, and faith. The facet
awe, for example, includes one question that asks ‘‘To what extent are you able to
experience awe from your surroundings? (e.g., nature, art, music)’’, and one question from
the facet inner peace asks ‘‘To what extent do you feel peaceful within yourself?’’. When
at least three items of a facet were answered, the missing item was imputed by the facet
mean. If more than two items in a facet were missing, no facet score was calculated for that
participant. A participant’s total WHOQOL-SRPB score was only calculated when all facet
scores were available.
Procedure
The research project was introduced to university undergraduate students at the end of class.
Participants were alerted to standard ethical guidelines surrounding research using paper-
and-pencil questionnaire formats, such as anonymity and the right to withdraw or not
choosing to participate. A closed carton box with a slot was provided for participants to
return questionnaires. This research study was approved by the university ethics committee.
Data Analysis
Data analyses were conducted using the program Statistics Package for Social Sciencesversion 16.0 (SPSS 2008). The large sample size of the study afforded parametric Pear-
son’s r bivariate analyses of the association between religious coping and other secular
1140 J Relig Health (2012) 51:1137–1151
123
coping strategies measured by the Brief COPE. These were conducted separately for
groups of participants classified according to whether they had obtained scores higher or
lower than the mean on the WHOQOL-SRPB. There were no a priori reasons why the
sample should have been divided in any particular way, and the sample was categorized
into groups of participants with WHOQOL-SRPB scores above and below the mean in
order to maintain a sufficiently large sample size for the factor analyses. To test whether
group differences in the associations of religious coping with other strategies might also
affect an extracted higher order factor solution, exploratory factor analyses were conducted
separately for the different groups and on the overall dataset. Analyses used sub-scale total
scores as indicators, a technique also known as extension analysis (Bernstein and Teng
1989), which is more robust than conducting factor analyses at item level. Factors were
extracted using the maximum likelihood method of factor extraction as this is one of the
most widely used methods, and factor rotations were conducted using promax. The number
of factors that was extracted for each analysis was based solely on the Kaiser-Guttman
criterion of number of eigenvalues larger than 1.00. Additional criteria, such as inspection
of the scree plot or interpretability of the factor solution were not utilized, since they
require subjective interpretations, and the goal of the present study was to investigate how
the characteristics of the sample determine the factor solutions of the different groups.
To provide a gauge of the adequacy of the extracted solutions, confirmatory factor
analyses were also conducted, using LISREL version 8.8 (Joreskog and Sorbom 1993).
Factor structures identified by the exploratory factor analyses were simplified, reducing
heavy cross-loadings across factors, and then tested for the two groups separately using
confirmatory factor analysis, as well as using a multigroup configural invariance test (Horn
and McArdle 1992; Meredith 1993). When data are ordinal in nature, researchers are
advised to use an asymptotically distribution-free (ADF) method with polychoric correla-
tions and asymptotic co-variance matrices (Joreskog 1990). The method of diagonally
weighted least squares is a suitable ADF method for small to moderate sample sizes (Flora
and Curran 2004) and was therefore selected for the present study. A set of indices was used
to determine the goodness-of-fit of the alternative factor solutions. Since chi-square
becomes inflated with increases in sample size (Marsh et al. 1988), model fits were eval-
uated using root mean square error of approximation (RMSEA), comparative fit index (CFI)
and standardized root mean square residual (SRMR). Using the frequently quoted guide-
lines by Hu and Bentler (1999), model fits were considered acceptable if RMSEA \ 0.06,
CFI [ 0.90 and SRMR \ 0.08.
Results
With the criterion that a full set of data be available for the Brief COPE (Carver 1997), the
sample size was reduced to 616. The mean total WHOQOL-SRPB score was higher for
female (106.07) than for male (105.65) participants, but this difference was not statistically
significant (t(603) = -0.18, P [ .05). There was a very small but statistically significant
correlation between age and WHOQOL-SRPB scores (r = 0.09, P \ .05). The majority of
kurtosis and skewness values for the Brief COPE sub-scales were within the negligible
range of -1.00 to 1.00 (Muthen and Kaplan 1985), and those outside this range were still
well below the levels at which deviations from normality become problematic (Curran
et al. 1996). For that reason, all sub-scales were included in the subsequent data analyses.
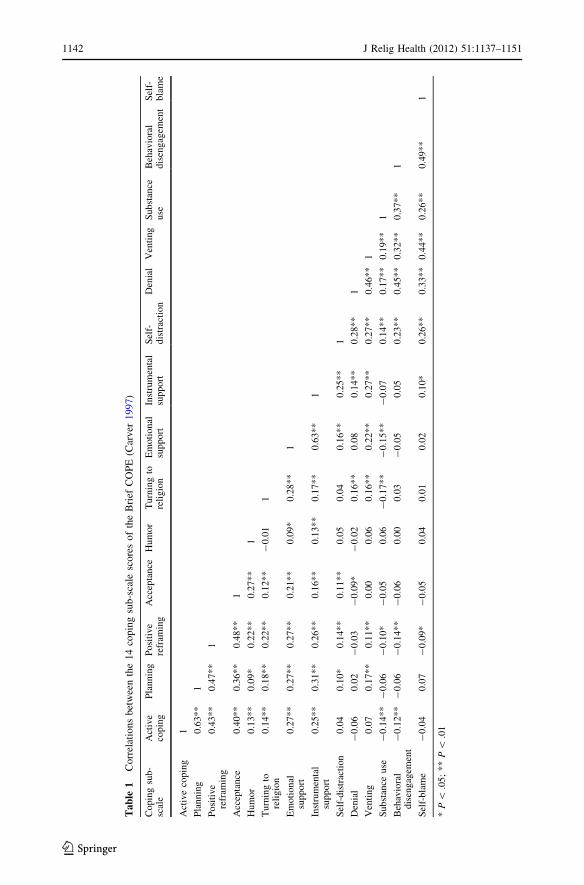
Table 1 shows the correlations between all different coping strategies. Apart from a few
correlations between highly related strategies, such as active coping and planning, most
J Relig Health (2012) 51:1137–1151 1141
123
Tab
le1
Co
rrel
atio
ns
bet
wee
nth
e1
4co
pin
gsu
b-s
cale
sco
res
of
the
Bri
efC
OP
E(C
arv
er1
99
7)
Copin
gsu
b-
scal
eA
ctiv
eco
pin
gP
lannin
gP
osi
tive
refr
amin
gA
ccep
tance
Hum
or
Turn
ing
tore
ligio
nE
moti
onal
support
Inst
rum
enta
lsu
pport
Sel
f-dis
trac
tion
Den
ial
Ven
ting
Subst
ance
use
Beh
avio
ral
dis
engag
emen
tS
elf-
bla
me
Act
ive
copin
g1
Pla
nnin
g0.6
3**
1
Posi
tive
refr
amin
g0.4
3**
0.4
7**
1
Acc
epta
nce
0.4
0**
0.3
6**
0.4
8**
1
Hum
or
0.1
3**
0.0
9*
0.2
2**
0.2
7**
1
Turn
ing
tore
ligio
n0.1
4**
0.1
8**
0.2
2**
0.1
2**
-0.0
11
Em
oti
onal
support
0.2
7**
0.2
7**
0.2
7**
0.2
1**
0.0
9*
0.2
8**
1
Inst
rum
enta
lsu
pport
0.2
5**
0.3
1**
0.2
6**
0.1
6**
0.1
3**
0.1
7**
0.6
3**
1
Sel
f-dis
trac
tion
0.0
40.1
0*
0.1
4**
0.1
1**
0.0
50.0
40.1
6**
0.2
5**
1
Den
ial
-0.0
60.0
2-
0.0
3-
0.0
9*
-0.0
20.1
6**
0.0
80.1
4**
0.2
8**
1
Ven
ting
0.0
70.1
7**
0.1
1**
0.0
00.0
60.1
6**
0.2
2**
0.2
7**
0.2
7**
0.4
6**
1
Subst
ance
use
-0.1
4**
-0.0
6-
0.1
0*
-0.0
50.0
6-
0.1
7**
-0.1
5**
-0.0
70.1
4**
0.1
7**
0.1
9**
1
Beh
avio
ral
dis
engag
emen
t-
0.1
2**
-0.0
6-
0.1
4**
-0.0
60.0
00.0
3-
0.0
50.0
50.2
3**
0.4
5**
0.3
2**
0.3
7**
1
Sel
f-bla
me
-0.0
40.0
7-
0.0
9*
-0.0
50.0
40.0
10.0
20.1
0*
0.2
6**
0.3
3**
0.4
4**
0.2
6**
0.4
9**
1
*P
\.0
5;
**
P\
.01
1142 J Relig Health (2012) 51:1137–1151
123
correlations were weak to moderate. The first eight strategies, sometimes labeled adaptivestrategies (Meyer 2001), were generally correlated with each other, as were the mal-adaptive strategies. Turning to religion was weakly correlated with active coping, plan-ning, positive reframing, acceptance, emotional support, instrumental support, denial and
venting, and negatively correlated with substance use.
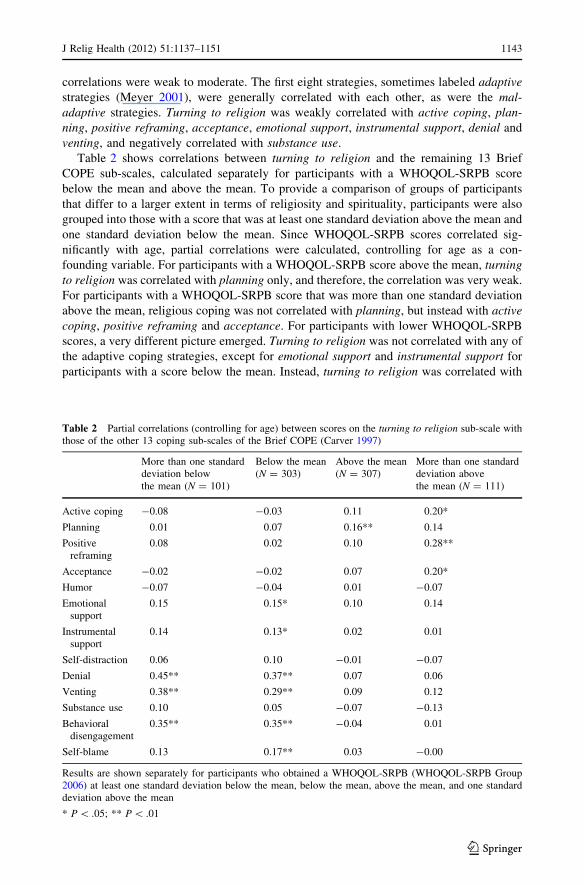
Table 2 shows correlations between turning to religion and the remaining 13 Brief
COPE sub-scales, calculated separately for participants with a WHOQOL-SRPB score
below the mean and above the mean. To provide a comparison of groups of participants
that differ to a larger extent in terms of religiosity and spirituality, participants were also
grouped into those with a score that was at least one standard deviation above the mean and
one standard deviation below the mean. Since WHOQOL-SRPB scores correlated sig-
nificantly with age, partial correlations were calculated, controlling for age as a con-
founding variable. For participants with a WHOQOL-SRPB score above the mean, turningto religion was correlated with planning only, and therefore, the correlation was very weak.
For participants with a WHOQOL-SRPB score that was more than one standard deviation
above the mean, religious coping was not correlated with planning, but instead with activecoping, positive reframing and acceptance. For participants with lower WHOQOL-SRPB
scores, a very different picture emerged. Turning to religion was not correlated with any of
the adaptive coping strategies, except for emotional support and instrumental support for
participants with a score below the mean. Instead, turning to religion was correlated with
Table 2 Partial correlations (controlling for age) between scores on the turning to religion sub-scale withthose of the other 13 coping sub-scales of the Brief COPE (Carver 1997)
More than one standarddeviation belowthe mean (N = 101)
Below the mean(N = 303)
Above the mean(N = 307)
More than one standarddeviation abovethe mean (N = 111)
Active coping -0.08 -0.03 0.11 0.20*
Planning 0.01 0.07 0.16** 0.14
Positivereframing
0.08 0.02 0.10 0.28**
Acceptance -0.02 -0.02 0.07 0.20*
Humor -0.07 -0.04 0.01 -0.07
Emotionalsupport
0.15 0.15* 0.10 0.14
Instrumentalsupport
0.14 0.13* 0.02 0.01
Self-distraction 0.06 0.10 -0.01 -0.07
Denial 0.45** 0.37** 0.07 0.06
Venting 0.38** 0.29** 0.09 0.12
Substance use 0.10 0.05 -0.07 -0.13
Behavioraldisengagement
0.35** 0.35** -0.04 0.01
Self-blame 0.13 0.17** 0.03 -0.00
Results are shown separately for participants who obtained a WHOQOL-SRPB (WHOQOL-SRPB Group2006) at least one standard deviation below the mean, below the mean, above the mean, and one standarddeviation above the mean
* P \ .05; ** P \ .01
J Relig Health (2012) 51:1137–1151 1143
123
the maladaptive strategies denial, venting and behavioral disengagement, as well as
self-blame for participants with a WHOQOL-SRPB score below the mean.
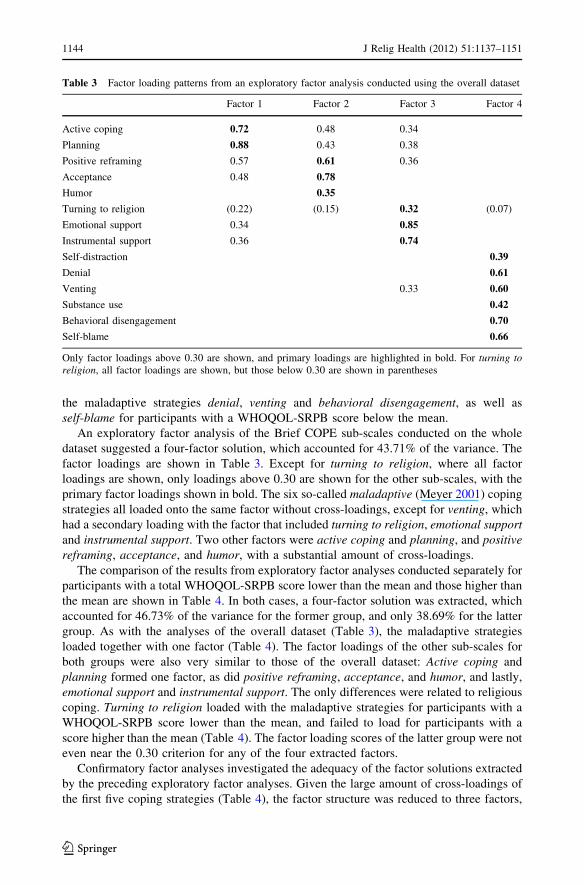
An exploratory factor analysis of the Brief COPE sub-scales conducted on the whole
dataset suggested a four-factor solution, which accounted for 43.71% of the variance. The
factor loadings are shown in Table 3. Except for turning to religion, where all factor
loadings are shown, only loadings above 0.30 are shown for the other sub-scales, with the
primary factor loadings shown in bold. The six so-called maladaptive (Meyer 2001) coping
strategies all loaded onto the same factor without cross-loadings, except for venting, which
had a secondary loading with the factor that included turning to religion, emotional supportand instrumental support. Two other factors were active coping and planning, and positivereframing, acceptance, and humor, with a substantial amount of cross-loadings.
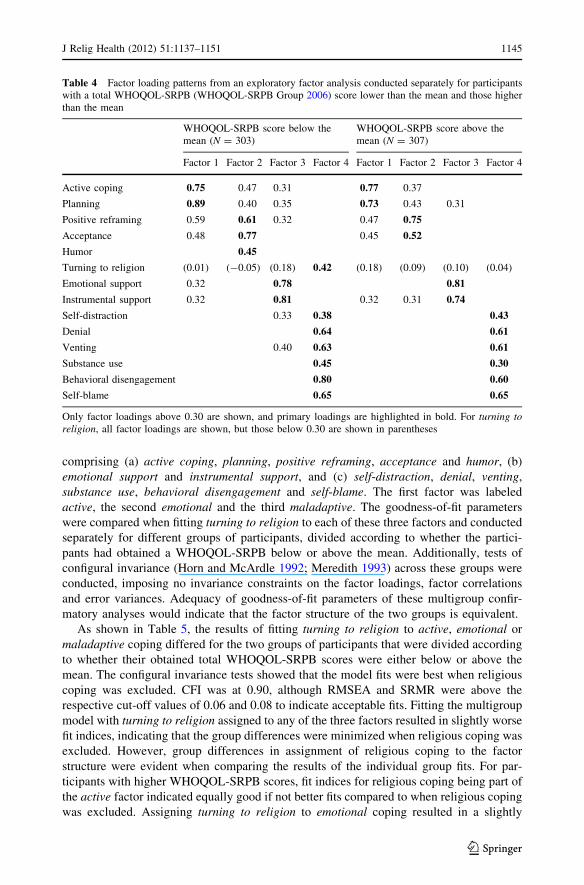
The comparison of the results from exploratory factor analyses conducted separately for
participants with a total WHOQOL-SRPB score lower than the mean and those higher than
the mean are shown in Table 4. In both cases, a four-factor solution was extracted, which
accounted for 46.73% of the variance for the former group, and only 38.69% for the latter
group. As with the analyses of the overall dataset (Table 3), the maladaptive strategies
loaded together with one factor (Table 4). The factor loadings of the other sub-scales for
both groups were also very similar to those of the overall dataset: Active coping and
planning formed one factor, as did positive reframing, acceptance, and humor, and lastly,
emotional support and instrumental support. The only differences were related to religious
coping. Turning to religion loaded with the maladaptive strategies for participants with a
WHOQOL-SRPB score lower than the mean, and failed to load for participants with a
score higher than the mean (Table 4). The factor loading scores of the latter group were not
even near the 0.30 criterion for any of the four extracted factors.
Confirmatory factor analyses investigated the adequacy of the factor solutions extracted
by the preceding exploratory factor analyses. Given the large amount of cross-loadings of
the first five coping strategies (Table 4), the factor structure was reduced to three factors,
Table 3 Factor loading patterns from an exploratory factor analysis conducted using the overall dataset
Factor 1 Factor 2 Factor 3 Factor 4
Active coping 0.72 0.48 0.34
Planning 0.88 0.43 0.38
Positive reframing 0.57 0.61 0.36
Acceptance 0.48 0.78
Humor 0.35
Turning to religion (0.22) (0.15) 0.32 (0.07)
Emotional support 0.34 0.85
Instrumental support 0.36 0.74
Self-distraction 0.39
Denial 0.61
Venting 0.33 0.60
Substance use 0.42
Behavioral disengagement 0.70
Self-blame 0.66
Only factor loadings above 0.30 are shown, and primary loadings are highlighted in bold. For turning toreligion, all factor loadings are shown, but those below 0.30 are shown in parentheses
1144 J Relig Health (2012) 51:1137–1151
123
comprising (a) active coping, planning, positive reframing, acceptance and humor, (b)
emotional support and instrumental support, and (c) self-distraction, denial, venting,
substance use, behavioral disengagement and self-blame. The first factor was labeled
active, the second emotional and the third maladaptive. The goodness-of-fit parameters
were compared when fitting turning to religion to each of these three factors and conducted
separately for different groups of participants, divided according to whether the partici-
pants had obtained a WHOQOL-SRPB below or above the mean. Additionally, tests of
configural invariance (Horn and McArdle 1992; Meredith 1993) across these groups were
conducted, imposing no invariance constraints on the factor loadings, factor correlations
and error variances. Adequacy of goodness-of-fit parameters of these multigroup confir-
matory analyses would indicate that the factor structure of the two groups is equivalent.
As shown in Table 5, the results of fitting turning to religion to active, emotional or
maladaptive coping differed for the two groups of participants that were divided according
to whether their obtained total WHOQOL-SRPB scores were either below or above the
mean. The configural invariance tests showed that the model fits were best when religious
coping was excluded. CFI was at 0.90, although RMSEA and SRMR were above the
respective cut-off values of 0.06 and 0.08 to indicate acceptable fits. Fitting the multigroup
model with turning to religion assigned to any of the three factors resulted in slightly worse
fit indices, indicating that the group differences were minimized when religious coping was
excluded. However, group differences in assignment of religious coping to the factor
structure were evident when comparing the results of the individual group fits. For par-
ticipants with higher WHOQOL-SRPB scores, fit indices for religious coping being part of
the active factor indicated equally good if not better fits compared to when religious coping
was excluded. Assigning turning to religion to emotional coping resulted in a slightly
Table 4 Factor loading patterns from an exploratory factor analysis conducted separately for participantswith a total WHOQOL-SRPB (WHOQOL-SRPB Group 2006) score lower than the mean and those higherthan the mean
WHOQOL-SRPB score below themean (N = 303)
WHOQOL-SRPB score above themean (N = 307)
Factor 1 Factor 2 Factor 3 Factor 4 Factor 1 Factor 2 Factor 3 Factor 4
Active coping 0.75 0.47 0.31 0.77 0.37
Planning 0.89 0.40 0.35 0.73 0.43 0.31
Positive reframing 0.59 0.61 0.32 0.47 0.75
Acceptance 0.48 0.77 0.45 0.52
Humor 0.45
Turning to religion (0.01) (-0.05) (0.18) 0.42 (0.18) (0.09) (0.10) (0.04)
Emotional support 0.32 0.78 0.81
Instrumental support 0.32 0.81 0.32 0.31 0.74
Self-distraction 0.33 0.38 0.43
Denial 0.64 0.61
Venting 0.40 0.63 0.61
Substance use 0.45 0.30
Behavioral disengagement 0.80 0.60
Self-blame 0.65 0.65
Only factor loadings above 0.30 are shown, and primary loadings are highlighted in bold. For turning toreligion, all factor loadings are shown, but those below 0.30 are shown in parentheses
J Relig Health (2012) 51:1137–1151 1145
123
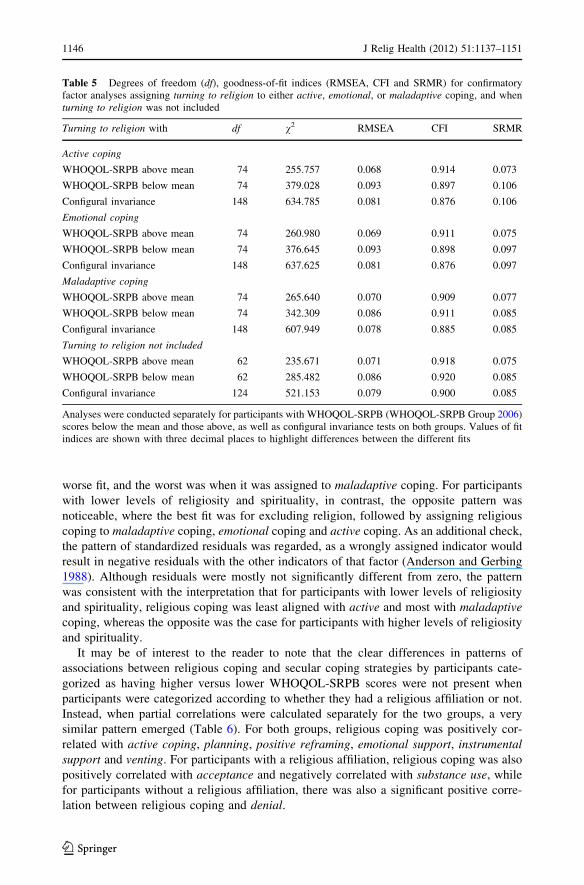
worse fit, and the worst was when it was assigned to maladaptive coping. For participants
with lower levels of religiosity and spirituality, in contrast, the opposite pattern was
noticeable, where the best fit was for excluding religion, followed by assigning religious
coping to maladaptive coping, emotional coping and active coping. As an additional check,
the pattern of standardized residuals was regarded, as a wrongly assigned indicator would
result in negative residuals with the other indicators of that factor (Anderson and Gerbing
1988). Although residuals were mostly not significantly different from zero, the pattern
was consistent with the interpretation that for participants with lower levels of religiosity
and spirituality, religious coping was least aligned with active and most with maladaptivecoping, whereas the opposite was the case for participants with higher levels of religiosity
and spirituality.
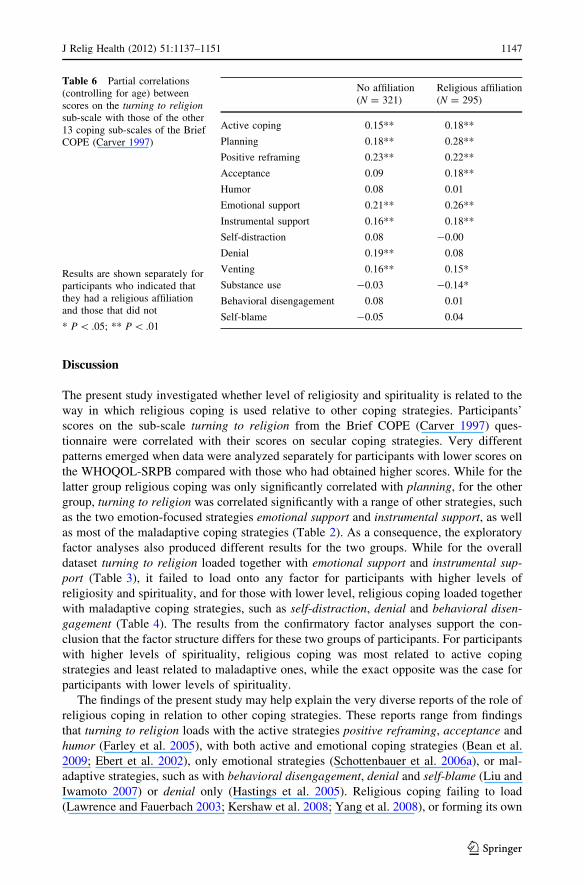
It may be of interest to the reader to note that the clear differences in patterns of
associations between religious coping and secular coping strategies by participants cate-
gorized as having higher versus lower WHOQOL-SRPB scores were not present when
participants were categorized according to whether they had a religious affiliation or not.
Instead, when partial correlations were calculated separately for the two groups, a very
similar pattern emerged (Table 6). For both groups, religious coping was positively cor-
related with active coping, planning, positive reframing, emotional support, instrumentalsupport and venting. For participants with a religious affiliation, religious coping was also
positively correlated with acceptance and negatively correlated with substance use, while
for participants without a religious affiliation, there was also a significant positive corre-
lation between religious coping and denial.
Table 5 Degrees of freedom (df), goodness-of-fit indices (RMSEA, CFI and SRMR) for confirmatoryfactor analyses assigning turning to religion to either active, emotional, or maladaptive coping, and whenturning to religion was not included
Turning to religion with df v2 RMSEA CFI SRMR
Active coping
WHOQOL-SRPB above mean 74 255.757 0.068 0.914 0.073
WHOQOL-SRPB below mean 74 379.028 0.093 0.897 0.106
Configural invariance 148 634.785 0.081 0.876 0.106
Emotional coping
WHOQOL-SRPB above mean 74 260.980 0.069 0.911 0.075
WHOQOL-SRPB below mean 74 376.645 0.093 0.898 0.097
Configural invariance 148 637.625 0.081 0.876 0.097
Maladaptive coping
WHOQOL-SRPB above mean 74 265.640 0.070 0.909 0.077
WHOQOL-SRPB below mean 74 342.309 0.086 0.911 0.085
Configural invariance 148 607.949 0.078 0.885 0.085
Turning to religion not included
WHOQOL-SRPB above mean 62 235.671 0.071 0.918 0.075
WHOQOL-SRPB below mean 62 285.482 0.086 0.920 0.085
Configural invariance 124 521.153 0.079 0.900 0.085
Analyses were conducted separately for participants with WHOQOL-SRPB (WHOQOL-SRPB Group 2006)scores below the mean and those above, as well as configural invariance tests on both groups. Values of fitindices are shown with three decimal places to highlight differences between the different fits
1146 J Relig Health (2012) 51:1137–1151
123
Discussion
The present study investigated whether level of religiosity and spirituality is related to the
way in which religious coping is used relative to other coping strategies. Participants’
scores on the sub-scale turning to religion from the Brief COPE (Carver 1997) ques-
tionnaire were correlated with their scores on secular coping strategies. Very different
patterns emerged when data were analyzed separately for participants with lower scores on
the WHOQOL-SRPB compared with those who had obtained higher scores. While for the
latter group religious coping was only significantly correlated with planning, for the other
group, turning to religion was correlated significantly with a range of other strategies, such
as the two emotion-focused strategies emotional support and instrumental support, as well
as most of the maladaptive coping strategies (Table 2). As a consequence, the exploratory
factor analyses also produced different results for the two groups. While for the overall
dataset turning to religion loaded together with emotional support and instrumental sup-port (Table 3), it failed to load onto any factor for participants with higher levels of
religiosity and spirituality, and for those with lower level, religious coping loaded together
with maladaptive coping strategies, such as self-distraction, denial and behavioral disen-gagement (Table 4). The results from the confirmatory factor analyses support the con-
clusion that the factor structure differs for these two groups of participants. For participants
with higher levels of spirituality, religious coping was most related to active coping
strategies and least related to maladaptive ones, while the exact opposite was the case for
participants with lower levels of spirituality.
The findings of the present study may help explain the very diverse reports of the role of
religious coping in relation to other coping strategies. These reports range from findings
that turning to religion loads with the active strategies positive reframing, acceptance and
humor (Farley et al. 2005), with both active and emotional coping strategies (Bean et al.
2009; Ebert et al. 2002), only emotional strategies (Schottenbauer et al. 2006a), or mal-
adaptive strategies, such as with behavioral disengagement, denial and self-blame (Liu and
Iwamoto 2007) or denial only (Hastings et al. 2005). Religious coping failing to load
(Lawrence and Fauerbach 2003; Kershaw et al. 2008; Yang et al. 2008), or forming its own
Table 6 Partial correlations(controlling for age) betweenscores on the turning to religionsub-scale with those of the other13 coping sub-scales of the BriefCOPE (Carver 1997)
Results are shown separately forparticipants who indicated thatthey had a religious affiliationand those that did not
* P \ .05; ** P \ .01
No affiliation(N = 321)
Religious affiliation(N = 295)
Active coping 0.15** 0.18**
Planning 0.18** 0.28**
Positive reframing 0.23** 0.22**
Acceptance 0.09 0.18**
Humor 0.08 0.01
Emotional support 0.21** 0.26**
Instrumental support 0.16** 0.18**
Self-distraction 0.08 -0.00
Denial 0.19** 0.08
Venting 0.16** 0.15*
Substance use -0.03 -0.14*
Behavioral disengagement 0.08 0.01
Self-blame -0.05 0.04
J Relig Health (2012) 51:1137–1151 1147
123

factor (Saroglou and Anciaux 2004; Weininger et al. 2006; Wood and Rutterford 2006), is
also frequently reported. The fact that religious coping loaded differently in the present
study for groups classified by their WHOQOL-SRPB scores suggests that variability in the
reported factor structures across different studies may be partly due to variability of the
extent of religiosity and spirituality of the participants sampled.
A large number of studies using the Brief COPE use the individual sub-scale scores
(e.g., Li and Lambert 2007; Pritchard and McIntosh 2003; Taylor et al. 2004), but when
coping is analyzed as higher order factors, such as emotion-focused coping, the way in
which composite scores are calculated is frequently based on a prior exploratory factor
analysis of the specific sample. While this practice reduces the overall likelihood that
religious coping is assigned to an inadequate factor, it still makes the assumption that the
extracted factor structure applies to the entire sample in the same manner. The present
study showed that, at least in respect to religious coping, this assumption cannot always be
justified. Kershaw et al. (2004) also reported that the factor structure was different,
depending on whether the factor analysis was conducted for caregivers or care recipients
with breast cancer, and one might need to question whether other studies would equally
have found such variations within their samples. Studies making comparisons of sub-
groups within their sample are therefore advised to ascertain that the intended comparisons
are valid by demonstrating that religious coping aligns with other factors in the same
manner for all the groups that are to be compared.
The results of the present study also illustrate that investigating the role of religious
coping requires more complex answers than simply assigning it to one factor, such as
active or emotion-focused coping. As shown in the present study, religious coping tends to
be used in a more problem-focused manner by individuals with higher levels of religiosity
and spirituality. This implies the use of one’s religion and spirituality to assist gathering or
focusing resources on solving the problem that causes the individual stress. For individuals
with lower levels of spirituality, in contrast, religion and spirituality might instead be
associated with avoidant or escapist strategies such as denying the problem or seeking
distraction that helps avoid directly addressing the source of the problem. As with indi-
viduals with an extrinsic religious orientation (Aguilar-Vafaie and Abiari 2007; Pargament
et al. 1992), these may be desperate religious coping strategies called upon predominantly
in times of stress, unlike those utilized by individuals with an intrinsic orientation, where
religious coping is not driven by immediate personal needs, but tends to be more deeply
rooted in religious belief systems.
For the purposes of the present study, the term maladaptive coping was used, although
the usefulness of the distinction between adaptive and maladaptive strategies is certainly
contentious (Lazarus 2000; Zuckerman and Gagne 2003). Effectiveness of coping
responses depends on the situational context, and supposedly adaptive coping strategies are
not necessarily always effective, and maladaptive ones ineffective (David et al. 2006).
Future research is necessary to explore further how exactly religious coping interacts with
the use of other strategies, particularly different types of religious coping, such as positive
and negative religious coping (Pargament et al. 2000). Further work is also required to
investigate specifically how spiritual and existential contemplations are used as coping
resources in the nonreligious. As Hwang et al. (in press) highlighted, this group is very
diverse and is therefore likely to have a wide range of personal, spiritual and existential
beliefs that may be utilized in dealing with stress. This type of research is especially
important in countries like New Zealand, where a substantial proportion of people are not
directly affiliated with a particular religion (Perrott 2007). The results shown in Table 6
demonstrate that religious affiliation is not a good indicator of the way in which religious
1148 J Relig Health (2012) 51:1137–1151
123

coping is utilized in relation to other strategies, unlike level of spiritual, religious and
personal beliefs (WHOQOL-SRPB), which are very clearly linked to different patterns of
associations (Table 2).
As also previously reported by Hsu et al. (2009), more than 50% of university students
do not consider themselves to be part of a religious denomination, unlike the 30% reported
in the 2006 New Zealand national census (Perrott 2007). Generalizations of the findings of
the present study are therefore limited by the fact that data were collected from a con-
venience sample of university undergraduate students. Furthermore, the dispositional form
of the Brief COPE (Carver 1997) was administered, which asked the participants how they
usually respond to a stressful situation, as opposed to asking them how they dealt with
stress in a specific situation. The frequency and types of strategies that individuals report to
use generally can differ significantly from the frequency and types individuals report to use
in specific stressful situations. Gillen (2006), for instance, found such discrepancies in
individuals who had a stroke, although turning to religion was one of the strategies that
was relatively stable, and scores of the situational and dispositional formats correlated
positively. However, future research may investigate whether the differences in the way
that religious coping relates to other coping strategies for individuals with lower and higher
levels of religiosity and spirituality are also present when inquiring about specific stressful
events, and not only when assessing coping using a dispositional format.
References
Aguilar-Vafaie, M. E., & Abiari, M. (2007). Coping response inventory: Assessing coping among Iraniancollege students and introductory development of an adapted Iranian coping response inventory (CRI).Mental Health, Religion & Culture, 10, 489–513.
Anderson, J. C., & Gerbing, D. W. (1988). Structural equation modeling in practice: A review and rec-ommended two-step approach. Psychological Bulletin, 103, 411–423.
Bean, M. K., Gibson, D., Flattery, M., Duncan, A., & Hess, M. (2009). Psychosocial factors, quality of life,and psychological distress: Ethnic differences in patients with heart failure. Progress in Cardiovas-cular Nursing, 24, 131–140.
Bernstein, I. H., & Teng, G. (1989). Factoring items and factoring scales are different: Spurious evidence formultidimensionality due to item categorization. Psychological Bulletin, 105, 467–477.
Carver, C. S. (1997). You want to measure coping but your protocol’s too long: Consider the Brief COPE.International Journal of Behavioral Medicine, 4, 92–100.
Carver, C. S., Scheier, M. F., & Weintraub, J. K. (1989). Assessing coping strategies: A theoretically basedapproach. Journal of Personality and Social Psychology, 56, 267–283.
Cicognani, E., Pietrantoni, L., Palestini, L., & Prati, G. (2009). Emergency workers’ quality of life: Theprotective role of sense of community, efficacy beliefs and coping strategies. Social IndicatorsResearch, 94, 449–463.
Cook, S. W., & Heppner, P. P. (1997). A psychometric study of three coping measures. Educational andPsychological Measurement, 57, 906–923.
Curran, P. J., West, S. G., & Finch, J. F. (1996). The robustness of the test statistics to nonnormality andspecification error in confirmatory factor analysis. Psychological Methods, 1, 16–29.
David, D., Montgomery, G. H., & Bovbjerg, D. H. (2006). Relations between coping responses and opti-mism-pessimism in predicting anticipatory psychological distress in surgical breast cancer patients.Personality and Individual Differences, 40, 203–213.
Ebert, S. A., Tucker, D. C., & Roth, D. L. (2002). Psychological resistance factors as predictors of generalhealth status and physical symptom reporting. Psychology, Health, & Medicine, 7, 363–375.
Farley, T., Galves, A., Dickinson, L. M., & de Jesus Diaz Perez, M. (2005). Stress, coping, and health: Acomparison of Mexican immigrants, Mexican-Americans, and Non-hispanic whites. Journal ofImmigrant Health, 7, 213–220.
Flora, D. B., & Curran, P. J. (2004). An empirical evaluation of alternative methods of estimation forconfirmatory factor analysis with ordinal data. Psychological Methods, 9, 466–491.
J Relig Health (2012) 51:1137–1151 1149
123
Folkman, S., & Moskowitz, J. T. (2004). Coping: Pitfalls and promise. Annual Review of Psychology, 55,745–774.
Gillen, G. (2006). A comparison of situational and dispositional coping after a stroke. Occupational Therapyin Mental Health, 22, 31–59.
Hastings, R. P., Kovshoff, H., Brown, T., Ward, N. J., Espinosa, F. D., & Remington, B. (2005). Copingstrategies in mothers and fathers of preschool and school-age children with autism. Autism, 9, 377–391.
Horn, J. L., & McArdle, J. J. (1992). A practical and theoretical guide to measurement invariance in agingresearch. Experimental Aging Research, 18, 117–144.
Hsu, P. H.-C., Krageloh, C. U., Shepherd, D., & Billington, R. (2009). Religion/spirituality and quality oflife of international tertiary students in New Zealand: An exploratory study. Mental Health, Religion &Culture, 12, 385–399.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventionalcriteria versus new alternatives. Structural Equation Modeling, 6, 1–55.
Hudek-Knezevic, J., Kardum, I., & Vukmirovic, Z. (1999). The structure of coping styles. A comparativestudy of Croatian sample. European Journal of Personality, 13, 149–161.
Hwang, K., Hammer, J. H., & Cragun, R. T. (in press). Extending religion-health research to secularminorities: Issues and concerns. Journal of Religion and Health.
Johnson, D. R., & Creech, J. C. (1983). Ordinal measures in multiple indicator models: A simulation studyof categorization error. American Sociological Review, 48, 398–407.
Joreskog, K. G. (1990). New developments in LISREL: Analysis of ordinal variables using polychoriccorrelations and weighted least squares. Quality & Quantity, 24, 387–404.
Joreskog, K. G., & Sorbom, D. (1993). LISREL 8: Structural equation modelling with the SIMPLIS com-mand language. Hillsdale, NJ: Erlbaum Associates.
Kershaw, T. S., Mood, D. W., Newth, G., Ronis, D. L., Sanda, M. G., Vaishampayan, U., & Northouse, L. L.(2008). Longitudinal analysis of a model to predict quality of life in prostate cancer patients and theirspouses. Annals of Behavioral Medicine, 36, 117–128.
Kershaw, T., Northouse, L., Kritpracha, C., Schafenacker, A., & Mood, D. (2004). Coping strategies andquality of life in women with advanced breast cancer and their family caregivers. Psychology andHealth, 19, 139–155.
Koenig, H. G., McCullough, M. E., & Larson, D. B. (2001). Handbook of religion and health. Oxford:Oxford University Press.
Lavery, M. E., & O’Hea, E. L. (2010). Religious/spiritual coping and adjustment in individuals with cancer:Unanswered questions, important trends, and future directions. Mental Health, Religion & Culture, 13,55–65.
Lawrence, J. W., & Fauerbach, J. A. (2003). Personality, coping, chronic stress, social support and PTSDsymptoms among adult burn survivors—A path analysis. Journal of Burn Care and Rehabilitation, 24,63–72.
Lazarus, R. S. (2000). Toward better research on stress and coping. American Psychologist, 55, 665–673.Lazarus, R. S., & Folkman, S. (1984). Stress appraisal and coping. New York: Springer.Li, J., & Lambert, V. A. (2007). Coping strategies and predictors of general well-being in women with breast
cancer in the People’s Republic of China. Nursing and Health Sciences, 9, 199–204.Liu, W. M., & Iwamoto, D. K. (2007). Conformity to masculine norms, Asian values, coping strategies, peer group
influences and substance use among Asian American men. Psychology of Men & Masculinity, 8, 25–39.Lozano, L. M., Garcıa-Cueto, E., & Muniz, J. (2008). Effect of the number of response categories on the
reliability and validity of rating scales. Methodology, 4, 73–79.Marsh, H. W., Balla, J. R., & McDonald, R. P. (1988). Goodness-of-fit indexes in confirmatory factor
analysis: The effect of sample size. Psychological Bulletin, 103, 391–410.Meredith, W. (1993). Measurement invariance, factor analysis and factorial invariance. Psychometrika, 58,
525–543.Meyer, B. (2001). Coping with severe mental illness: Relations of the Brief COPE with symptoms, func-
tioning, and well-being. Journal of Psychopathology and Behavioral Assessment, 23, 265–277.Miyazaki, Y., Bodenhorn, N., Zalaquett, C., & Ng, K.-M. (2008). Factorial structure of Brief COPE for
international students attending US colleges. College Student Journal, 42, 795–806.Muthen, B., & Kaplan, D. (1985). A comparison of some methodologies for the factor analysis of non-
normal Likert variables. British Journal of Mathematical and Statistical Psychology, 38, 171–189.Pargament, K. I., Koenig, H. G., & Perez, L. M. (2000). The many methods of religious coping: Devel-
opment and initial validation of the RCOPE. Journal of Clinical Psychology, 56, 519–543.Pargament, K. I., Olsen, H., Reilly, B., Falgout, K., Ensing, D. S., & van Haitsma, K. (1992). God help me
(II): The relationship of religious orientations to religious coping with negative life events. Journal forthe Scientific Study of Religion, 31, 504–513.
1150 J Relig Health (2012) 51:1137–1151
123
Paukert, A. L., LeMaire, A., & Cully, J. A. (2009). Predictors of depressive symptoms in older veterans withheart failure. Age & Mental Health, 13, 601–610.
Perrott, K. (2007). Atheism and religious diversity. Aotearoa Ethnic Network Journal, 2(2), Article 8.Pritchard, M. E., & McIntosh, D. N. (2003). What predicts adjustment among law students? A longitudinal
panel study. The Journal of Social Psychology, 143, 727–745.Radat, F., Lanteri-Minet, M., Nachit-Ouinekh, F., Massiou, H., Lucas, C., Pradalier, A., et al. (2009). The
GRIM2005 study of migraine consultation in France. III: Psychological features of subjects withmigraine. Cephalalgia, 29, 338–350.
Saroglou, V., & Anciaux, L. (2004). Liking sick humor: Coping styles and religion as predictors. Humor, 17,257–277.
Schottenbauer, M. A., Klimes-Dougan, B., Rodriguez, B. F., Arnkoff, D. B., Glass, C. R., & Lasalle, V. H.(2006a). Attachment and affective resolution following a stressful event: General and religious copingas possible mediators. Mental Health, Religion & Culture, 9, 448–471.
Schottenbauer, M. A., Rodriguez, B. F., Glass, C. R., & Arnkoff, D. B. (2006b). Religious coping researchand contemporary personality theory: An exploration of Endler’s (1997) integrative personality theory.British Journal of Psychology, 97, 499–519.
Seybold, K. S., & Hill, P. C. (2001). The role of religion and spirituality in mental and physical health.Current Directions in Psychological Science, 10, 21–24.
SPSS, Inc. (2008). SPSS for windows, version 16.0. Chicago, USA: SPSS, Inc.Tamres, L. K., Janicki, D., & Helgeson, V. S. (2002). Sex differences in coping behavior: A meta-analytic
review and an examination of relative coping. Personality and Social Psychology Review, 6, 2–30.Taylor, S. E., Sherman, D. K., Kim, H. S., Jarcho, J., Takagi, K., & Dunagan, M. S. (2004). Culture and
social support: Who seeks it and why? Journal of Personality and Social Psychology, 87, 354–362.Udipi, S., Veach, P. M., Kao, J., & LeRoy, B. S. (2008). The psychic costs of emphatic engagement:
Personal and demographic predictors of genetic counselor compassion fatigue. Journal of GeneticCounseling, 17, 459–471.
Weininger, C. F., Shalev, A. Y., Ofek, H., Freedman, S., Weissman, C., & Einav, S. (2006). Posttraumaticstress disorder among hospital surgical physicians exposed to victims of terror: A prospective, con-trolled questionnaire survey. Journal of Clinical Psychiatry, 67, 890–896.
Welbourne, J. L., Eggerth, D., Hartley, T. A., Andrew, M. E., & Sanchez, F. (2007). Coping strategies in theworkplace: Relationships with attributional style and job satisfaction. Journal of Vocational Behavior,70, 312–325.
WHOQOL-SRPB Group. (2006). A cross-cultural study of spirituality, religion, and personal beliefs ascomponents of quality of life. Social Science and Medicine, 62, 1486–1497.
Wood, R. L. L., & Rutterford, N. A. (2006). Demographic and cognitive predictors of long-term psycho-social outcome following traumatic brain injury. Journal of the International NeuropsychologicalSociety, 12, 350–358.
Yang, H.-C., Brothers, B. M., & Andersen, B. L. (2008). Stress and quality of life in breast cancerrecurrence: Moderation or mediation of coping? Annals of Behavioral Medicine, 35, 188–197.
Zelikovsky, N., Schast, A. P., & Jean-Francois, D. (2007). Parent stress and coping: Waiting for a child toreceive a kidney transplant. Journal of Clinical Psychology in Medical Settings, 14, 320–329.
Zuckerman, M., & Gagne, M. (2003). The COPE revised: Proposing a 5-factor model of coping strategies.Journal of Research in Personality, 37, 169–204.
J Relig Health (2012) 51:1137–1151 1151
123All in-text references underlined in blue are linked to publications on ResearchGate, letting you access and read them immediately.
Related Documents











