Barry J. Maron, MD Hypertrophic Cardiomyopathy Institute Tufts Medical Center Boston, MA Disclosures: Medtronic (Grantee) GeneDx (Consultant) How Hypertrophic Cardiomyopathy Became a Contemporary Treatable Genetic Disease With Low Mortality Shaped by 50 Years of Clinical Research and Practice

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Barry J. Maron, MDHypertrophic Card iomyopa thy Ins titu te
Tufts Medica l Cente rBos ton , MA
Dis c los ures :Medtronic (Grantee )GeneDx (Cons ultan t)
How Hypertrophic CardiomyopathyBecame a Contemporary TreatableGenetic Disease With Low Mortality
Shaped by 50 Years of Clinical Researchand Practice

Highes t
In te rmedia te
Lowes t
2° preventionCardiac arres t/s us ta ined VT
1° preventionFamily his to ry HCM-SDUnexp la ined s yncopeMultip le -repe titive NSVT (Holter)Abnormal exerc is e BP res pons eLGE ≥ 15% of LV mas sMas s ive LVH ≥ 30 mm
Rare subgroups/potential arbitratorsEnd-s tage (EF < 50%)LV apica l aneurys mMarked LV outflow obs truction (res t)Modifiab le
In tens e competitive s portsCAD
LGE ≥ 15% of LV mas sAge ≥ 60yAlcohol s ep ta l ab la tion (? )
ICD

Highes t
In te rmedia te
Lowes t
2° preventionCardiac arres t/s us ta ined VT
1° preventionFamily his to ry HCM-SDUnexp la ined s yncopeMultip le -repe titive NSVT (Holter)Abnormal exerc is e BP res pons eLGE ≥ 15% of LV mas sMassive LVH ≥ 30 mm
Rare subgroups/potential arbitratorsEnd-s tage (EF < 50%)LV apica l aneurys mMarked LV outflow obs truction (res t)Modifiab le
In tens e competitive s portsCAD
LGE ≥ 15% of LV mas sAge ≥ 60yAlcohol s ep ta l ab la tion (? )
ICD
U.S./Canada: ACC/AHA: 2011


0
2
4
6
8
10
12
14
16
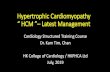
<15 16-19 20-24 25-29 30
Max. LV Wall Thicknes s (mm)
%P
ati
en
tsW
ith
SC
DRe la tio n Be twe e n LV Th ic kn e s s &
S CD in 482 HCM P a tie n ts

Highes t
In te rmedia te
Lowes t
2° preventionCardiac arres t/s us ta ined VT
1° preventionFamily his to ry HCM-SDUnexp la ined s yncopeMultip le -repe titive NSVT (Holter)Abnormal exerc is e BP res pons eLGE ≥ 15% of LV mas sMas s ive LVH ≥ 30 mm
Rare subgroups/potential arbitratorsEnd-s tage (EF < 50%)LV apica l aneurys mMarked LV outflow obs truction (res t)Modifiab le
In tens e competitive s portsCAD
LGE ≥ 15% of LV mas sAge ≥ 60yAlcohol s ep ta l ab la tion (? )
ICD
U.S./Canada: ACC/AHA 2011

0
10
20
30
40
50
60
70
Alive Non-
Cardiac
De ath
Non-HCM
Cardiac
De ath
Embolic
S troke
He art
Failure
SCD
%o
fH
CM
Co
ho
rt
65%
13% 12%
2% 1%
0.2%/y
Outcome of HCM Patien ts Firs t Eva lua ted ≥ 60 Years
1%
HCM Death
Aging is Good in HCM
Maron BJ et. a l.Circ 2013; 127: 585

Intermediate
LowRisk
Risk Stratification for Sudden Death in HCM
Moderate
High
No risk factors
Family historyof suddendeath
NonsustainedVT
Unexplainedsyncope
ExtremeLVH
AbnormalBPresponsetoEx
0.5%/year

Highes t
In te rmedia te
Lowes t
2° preventionCardiac arres t/s us ta ined VT
1° preventionFamily his to ry HCM-SDUnexp la ined s yncopeMultip le -repe titive NSVT (Holter)Abnormal exerc is e BP res pons eLGE ≥ 15% of LV mas sMas s ive LVH ≥ 30 mm
Rare subgroups/potential arbitratorsEnd-s tage (EF < 50%)LV apical aneurysmMarked LV outflow obs truction (res t)Modifiab le
In tens e competitive s portsCAD
LGE ≥ 15% of LV mas sAge ≥ 60yAlcohol s ep ta l ab la tion (? )
ICD
U.S./ Canada (ACC/AHA) 2011

C
D E F
D
P
VS
B
P
D
** *
**
*
Figure1.

1.0
0.8
0.6
0.4
0.0
0 5 1510 20
HCM pat ient s w i t hout LV apic a l aneur ysm sHCM pat ient s w i t h LV apic a l aneur ysm
Lo g-r ank t es t p<0 .00 1
Years f rom Fi rst Eva luat ion
Su
rviv
al
fre
efr
om
HC
Mre
late
dm
ort
ali
tya
nd
ad
ve
rse
ev
en
ts
0.2
H CM Re lat ed Deat h o r A dve r se Cl in ic a l Even t sin 93 Pat ien t s w i t h LV A p ic a l A neu r ysm s
8 .1% /yea r
1 .7% /yea r

LA
LA
V S
RV
LV VS
A B C
D E F
Pr eva lenc eo f LGE = 55 -70%

LGE
LGELGE
Extent of LGE vs. Sudden Death Risk in HCM
Follow-up (years )
Su
rviv
al
LGE (-)LGE < 10%
LGE 10-20%
LGE > 20%
Chan RH et. a l.Circ 2014; 130(6):484-95

Highes t
In te rmedia te
Lowes t
2° preventionCardiac arres t/s us ta ined VT
1° preventionFamily his to ry HCM-SDUnexp la ined s yncopeMultip le -repe titive NSVT (Holter)Abnormal exerc is e BP res pons eLGE ≥ 15% of LV massMas s ive LVH ≥ 30 mm
Rare subgroups/potential arbitratorsEnd-s tage (EF < 50%)LV apica l aneurys mMarked LV outflow obs truction (res t)Modifiab le
In tens e competitive s portsCAD
LGE ≥ 15% of LV massAge ≥ 60yAlcohol s ep ta l ab la tion (? )
ICD

0
0.5
1
1.5
2
%H
CM
Mo
rta
lity
HCM-Re la te d Mo rta lity
0
0.5
1.5
1
6
Genera l U.S .Popula tion
0.8%/y
0.5%/y
1.5%/y
3-6%/y
Early HCMReferra l Cohorts
HCM Cohorts :P rior to u tiliza tion
of cu rren t trea tments tra teg ies /
in te rven tions
ICD inte rve ntionHeart trans p lant/myectomy
OHCA/d efib rilla tion/hypo thermia
Pres ent HCMCohort:
Contempora rytrea tment

ICD
S u d d e n
De a th
Progres s iveHeart
Fa ilure(obs tructive)
AdvancedHeart Fa ilure& End Stage
(non-obs tructive)
AF
&
S tro ke
Benign/S table(n o rm a l lo n g e vity)
DrugsSep ta l Myec tomy(Alcohol Abla tion)
Trans plant DrugsAnticoagulan ts
Abla tion
Profiles in Prognosis for HCM

(15%)
(15%)
(7%)
(7%)
(<1%)
(<1%)
(<1%)
(<1%)
(<1%)
(<1%)

25-Year Contemporary In itia tives inHypertrophic Card iomyopa thy
Genetic (molecu la r)S ingle s arcomere muta tion
hypothes is “ Clin ic ians ”
0 ThousandsLive s
S a ve d
0 Many thousandsIm p ro ve d
Qu a lity o f
Life
Related Documents