1 REPUBLIC OF INDONESIA MINISTRY OF HEALTH NATIONAL INSTITUTE OF HEALTH RESEARCH AND DEVELOPMENT BASIC HEALTH RESEARCH 2007 HOUSEHOLD AND INDIVIDUAL QUESTIONNAIRES I. PLACE IDENTIFICATION 1 Province 2 District/city *) 3 Sub-District 4 Village 5 Village Classification 1. Urban 2. Rural 6 a. Census Block Number b. Census Sub Block Number 7 Sample Code Number 8 Consecutive Number of Household Sample 9 Home Address II. HOUSEHOLD INFORMATION 1 Head of household's name: 2 The Number of Household Member: 3 The Number of Interviewed Household Member: 4 The Number of Under Fives: 5 The Number of Household member (ART) Mortality within 12 Months Prior to Survey and Undertaken Verbal Autopsy 6 Is this Household Have Salt? 1. Yes 2. No Block III 7 Conduct Iodine rapid test and record the content 1. Enough (blue/dark purple) 2. Not Enough (Blue/Light purple) 3. No Iodine (No.Color) THE SAMPLE OF SALT WAS COLLECTED FROM 30 SELECTED DISTRICTS/CITIES (SEE THE LIST OF DISTRICT FROM GUIDELINES) 8 STICKER NUMBER FROM SELECTED HOUSEHOLD ATTACH STICKER HERE III. ENUMERATOR INFORMATION 1 Enumerator’s name: 4 Team leader’s name: 2 Date data collection: (dd-mm-yy) -- 5 Date of checking: (dd-mm-yy) -- 3 Enumerator’s signature 6 Team leader’s signature: *) Cross unnecessary items RKD07. RT CONFIDENTIAL

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
REPUBLIC OF INDONESIA MINISTRY OF HEALTH
NATIONAL INSTITUTE OF HEALTH RESEARCH AND DEVELOPMENT
BASIC HEALTH RESEARCH 2007
HOUSEHOLD AND INDIVIDUAL QUESTIONNAIRES
I. PLACE IDENTIFICATION
1 Province 2 District/city *) 3 Sub-District 4 Village 5 Village Classification 1. Urban 2. Rural 6 a. Census Block Number
b. Census Sub Block Number
7 Sample Code Number 8
Consecutive Number of Household
Sample
9 Home Address
II. HOUSEHOLD INFORMATION
1 Head of household's name:
2 The Number of Household Member: 3 The Number of Interviewed Household Member: 4 The Number of Under Fives: 5
The Number of Household member (ART) Mortality within 12 Months Prior to Survey and Undertaken Verbal Autopsy
6 Is this Household Have Salt? 1. Yes 2. No Block III 7 Conduct Iodine rapid test and record the content 1. Enough (blue/dark purple)
2. Not Enough (Blue/Light purple)
3. No Iodine (No.Color)
THE SAMPLE OF SALT WAS COLLECTED FROM 30 SELECTED DISTRICTS/CITIES (SEE THE LIST OF DISTRICT FROM GUIDELINES)
8 STICKER NUMBER FROM SELECTED HOUSEHOLD ATTACH STICKER HERE
III. ENUMERATOR INFORMATION
1 Enumerator’s name: 4 Team leader’s name:
2 Date data collection: (dd-mm-yy) -- 5
Date of checking: (dd-mm-yy) --
3 Enumerator’s signature 6 Team leader’s signature:
*) Cross unnecessary items
RKD07. RT CONFIDENTIAL

2
IV. HOUSEHOLD MEMBER INFORMATION
ART order number
Name of household member (ART)
Rela-
tion
with
Head of
house-
hold
[CODE]
Sex
1. Male 2. Female
Age (year)
Ifage < 1 year
fill “00” If age
≥ 97 years fill
“97”
Maritalstatus
[CODE]
Only for ART ≥ 10 years old
Only Woman 10-54 years
old
Are they pregnant
?
1. Yes 2. No
Did ART sleep in
Mosquito net?
1. Yes 2. No col.12
8. Do not know
col.12
If yes, is the net insecti cied?
1. Yes 2. No 8. Don’t
know
Verifi cation
Highest Educa
tion
[CODE]
Main Job
[CODE]
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12)
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15. USE ADDITIONAL SHEET IF THE NUMBER OF ART > 15 PERSONS
Code for column 3 Relation with head of household:
Code for column 6 marital status
Code for column 6 Highest education
Code column 8 Main Job
Code for column 12 Verification
1 = head of household
2 = Wife/Husband 3 = Chilld 4 = Child inLaw 5 = Grandchild
6 = Parents/ Parents in Law
7 = Another family 8 = Housekeeper 9 = others
2. 1 = Single 2 = Married
3. 3 = Divorced 4. when alive 5. 4 = Divorced due 6. to death
1 = No Schooling 2 = Didn’t pass elementary school
3 = Passed Elementary school 4 = Passed Yunior High 5 = Passed Senior High 6 = Academy/Univeristiy
graduated
01 = Unemployed 08 = Wiraswasta; 02 = Student 09 = Pelayanan jasa;
03 = Housewife 10 = Dagang; 04 = Army/police 05 = Civil servant 06 = BUMN employee
07 = Private employee 11 = Petani;
08 = Enterpreneur/
09 = Service Sector 10 = Farmer 11 = Fisherman 12 = Labor
13 = others
1= No change 2= Change
3 = Dead 4 = Moved 5 = Born 6 = new member
7 = Never exist in sample of household

3
V. MORTALITY
Name ART interviewed: ......................................................................... ART order number interviewed: (see Block IV col. 1)
A death occurred after1 JULI 2004 (including still births of infants) ---- only within the household
1 Was there there a death after 1 JULY 2004 because of a death listed below: (Read and select Disease) Fill with code 1=Yes or 2=NO
a. Diarrhea e. Malaria i. Hypertension CVD m. Accidents b. ARI/ Pneumonia f. DHF j. Stroke n. Pregnancy or birth c. Measles g. Hepatitis k. Diabettes o. Still birth d. Tuberculosis h. Thyphoid l. Cancer p. Lainnya, ..............
If not death occurred before 1 JULI 2004 Go directly to Block VI
No. Urut
Name Of
Deceased
Relationship to
head of household [CODE]
Month and year of
Death After 1 Juli 2004
Gender
1. M 2. F
Age at Death < 1 year (in months)
< 1 month (in days) tulis dalam hari
< 1 day write 00 in column for
days
Still birth 98 in column for days
97 years write 97 in column for
years
[Fill in one: Day or Month or year]
Primary Cause of
Death
[CODE]
For women aged 10 - 54 years that died, did it happend when they were: 1. Pregnant 2. Miscarriage 3. Giving birth 4. Within 60 hr after
giving birth) 5. Other
(2) (3) (4) (5) (6) (7) (8) (9)
1.
Mon
Year
Day
Month
Year
……
……...
2.
Mon
Year
Day
Month
Year
……
……...
3.
Mon
Year
Day
Month
Year
……
……...
4.
Mon
Year
Day
Month
Year
……
……...
If the death occured with 12 months before the survey, continue with the questionairre RKD07.AV after reviewing column seven (age at death) in order to select the correct form
Code column 4 relation to head of household
1 = Head of household 6 = Parents 2 = Wife/husband 7 = Famili lain 3 = Child 8 = Servants 4 = in laws 9 = Other
5 = Grandchild
Code column 8 Cause of death
01 = Diarrhea 06 = DHF 11 = Diabettes
02 = ARI/ Pneumonia 07 = Hepatitus 12 = Cancer 03 = Measles 08 = Typhoid 13 = Accidents 04 = Tuberculosis 09 = Hypertension/CVD 14 = Pregnancy, Birth 05 = Malaria 10 = Stroke 15 = Stillborne
16 = Other.........
Column 7 Age at death
Use Questionnaire:
< 29 days(NEONATAL): RKD07. AV1
29 days - < 5 year: RKD07.AV2
5 or more years :
RKD07.AV3

4
VI. The Accessibility & Utilization of Health Service
1a How far is it to nearest health facilities (Hospital, health center, sub-health center,
Doctor’s practice, Nurse practice)
……….Km
…..……meter
1b How long to reach the nearest health facility (Hospital, health center, sub-health
center, Doctor’s practice, Nurse practice) …….... minute
2a How far is the distance to reach the nearest community health facility (Posyandu, Poskesdes, Polindes)?
……….Km
…..……meter
2b How long to get the nearest community health facility (Posyandu, Poskesdes,
Polindes)? …….... minute
3 Is there any public transportation to reach the nearest health facilities? (valid for Q.1a
and Q.2a) 1. Yes 2. No
4 Has this family ever utilized Posyandu/Poskesdes service in the last 3 months 1. Yes
2. No Q.6 5 If yes, what kind of treatment has been received: (READ OUT POINT a TO POINT i)
Fill the answer code with 1=Yes 2=No 7=Not valid
a. Body weighing d. MCH g. Food Supplementation b. Counseling e. Family Planning h. Micronutrient Supl (Vit A, Fe, Multi-mcronutrient)
c. Imumnization f. Medication i. Disease risk consultation
Continue to Q.7
6 If not ever utilized of Posyandu/ Poskesdes, what is the main reason?
1. Far distance 2. There is no Posyandu 3. Incomplete Service 4. Others: ........................
7 Has this family ever utilized Polindes/Village Midwives service in the last 3 months?
1. Yes 2. No Q.9
8 If yes, what kind of treatment has been received: (READ OUT POINT a TO f) Fill the code with 1=YES 2=NO 7= NOT VALID
a. Pregnancy checking c. Postpartum examination e. Infant checking (1-11 month) and/ or under fives (1- 4 year)
b. Delivery d. Neonates checking (<1 month) f. Medication Continue to Q.10
9 If Not ever utilized Polindes/ Village Nurse, what is the main reason?
1. Far distance 3. Incomplete service 5. Others: ................... 2. There is no polindes/Village nurse 4. No demand
10 Has this family ever utilized Village Drug Post (POD)/Village Drug Shop (WOD) in the last 3 months?
1. Yes VII 2. No
11 If not ever utilized POD/ WOD, what is the main reason? 1. Far distance 3. The service incomplete 5. Others: .................... 2. There is no POD/ WOD 4. No Demand

5
VII. Environmental Sanitation
1. How much number of water utilization for Household needs? …........ liter/day 2. How far/long does it take to get the water (round trip)? a. Distance .........Km
b. Time...… Minute
a.
b. 3. Is there any pollution source (chemical waste/cesspool/garbage) surround the
source of water in radius < 10 meters?
1. Yes 2. No 3. No water source
4. Is the water for household needs easily obtained all the year?
1. Yes (easy) 2. Difficult in dry season only 3. Difficult along the year
5. If the water source located outside the house, who is responsible to get it for household needs
1. Adult women 2. Adult men 3. Boys 4. Girls 5. Water source is inside the house
6. How is the physical quality of drinking water? (READ OUT POINT a until POINT e) FILL THE ANSWER CODE WITH 1=YES OR 2=NO
a. Muddy b.Colored c. Contain taste d. Foamy e. Smelly
7. What is the type of container/media used to retain the drinking water before processed? 1. Using no container/used directly from the source 2. Open container 3. Closed Container
8. How is the process to prepare drinking water? (READ OUT POINT a until POINT e) FILL THE ANSWER CODE WITH 1=YES OR 2=NO
a. No process b. Boiled c. Filtered d. Add chemical material e. Others: ..................
9. Where is the sewage canal from bathroom/Laundromat/kitchen? 1. Closed container in the yard 3. Container outside the yard 2. Open container in the yard 4. No container 5. Go directly to the gutter
10. How is the condition of chemical sewage canal from bathroom/Laundromat/kitchen? 1. Open Canal 2. Close Canal 3. Without canal
11. Is there any garbage bin available outside the house? 1. Yes 2. No Q.13 12. If yes, what is the type of that garbage bin available outside the house?
(Read out POINT a and b) FILL THE ANSWER CODE WITH 1=YES OR 2=NO
a. Closed bin
b. Open bin
13. Is there any garbage bin for organic trash inside the house? 1. Yes 2. No Q.15
14. If yes, what kind of garbage bin for organic trash inside the house?
(Read out POINT a and b)) FILL THE ANSWER CODE WITH 1=YES OR 2=NO
a. Closed bin
b. Open bin
15. Did this household use chemical materials included in hazardous and toxic materials during last month
(Read out Point a UNTIL h). FILL THE ANSWER CODE WITH 1=YES OR 2=NO
a. Fragnance Spray e. Spot remover for clothes b. Hair spray/deodorant spray f. Car storage battery c. Floor cleaner g. Paint d. Glass cleaner h. Insecticide/pesticide

6
16. What kind of livestocks this household raise?
Livestocks/pets
Raised?
1. Yes
2. No next livestock
Raised in :
1. Cage inside the house 3. Inside the house, without cage
2. Cage outside the house 4. Outside the house,withouit cage
(1) (2)
a. Poultry(chicken,ducks, birds)
b. Med breeding animals (goats,ships,
pigs)
c. large breeding animals
(cows,buffaloes,horses) d. Dogs,cats,rabbits 17. How far is it from the house to pollution source?
IF DO NOTKNOW FILL ”8888” INCOLUMN (2) DISTANCE (METERS) IF THERE IS NO POLLUTION SOURCE FILL ”9999” IN COLUMN (2) DISTANCE (METERS)
Pollution Source Distance (meters) Pollution Source Distance (meters)
(1) (2) (1) (2)
a. High way/railway e. Terminal/train station/airport b. Dump (for temporary/final)
/Incinerator/Hospital waste installation f. Garage/workshop c. Industries/factories g. High voltage electric source
d. Traditional market h. Livestock/animal slaughtering house (including poultry)
ENUMERATOR'S NOTE

1
BASIC HEALTH RESEARCH (RISKESDAS 2007)
PLACE IDENTIFICATION
Province District/
City Sub-district Village D/K
Cencus Block No
Sub Census
Block No Sampe Code number
Household sample number
Copy from Block I PLACE IDENTIFICATION RKD07.RT
VIII. HOUSEHOLD FOOD CONSUMPTION (IN THE LAST 24 HOURS)
1 Information on the number of ART and visitors (guest) who consumed food by age, sex, and dinner time
Age Group
The number of ART
(copy from Block IV)
Morning AFTERNOON EVENING
M (person)
F (person)
M (person)
F (person)
M (person)
F (person)
ART Guest ART Guest ART Guest ART Guest ART Guest ART Guest
0 – 11 Months
1 - 3 years
4 - 6 years
7 - 9 years
10 – 12 years
13 - 15 years
16 - 18 years
19 - 29 years
30 - 49 years
50 - 64 years
> 64 years
Total
2 INFORMATION ON TOTAL CONSUMPTION OF FOOD IN A DAY (LAST 24 HOURS)
Breakfast ..................persons Afternoon ..................persons Dinner ..................persons
Eating time
Food/Menu Kinds of foodstuffs Consumption Size
Household Size Weight (gram)
RKD07.GIZI CONFIDENTIAL

2
3 INFORMATION ON CHILD FOOD CONSUMPTION IN A DAY (THE LAST 24 HOURS)
Child’s name: ..................................................................................... ART order number
Eating time
Food/Menu Kinds of foodstuffs Consumption size
Household size Weight (gram)
ENUMERATOR’S NOTE

1
BASIC HEALTH RESEARCH (RISKESDAS 2007)
PLACE IDENTIFICATION
Province District/
City Sub-district Village R/U
Cencus Block No
Sub Census
Block No Sampe Code number
Household sample number
Copy from Block I PLACE IDENTIFICATION RKD07.RT
IX. INDIVIDUAL INTERVIEW INFORMATION
1. Date of first visit: dd –mm-yy -- 3. Enumerator's Name
2. Date of last visit: dd –mm-yy -- 4. Enumerator's Sign
X. INDIVIDUAL INFORMATION
A. RESPONDENT IDENTIFICATION
A01 Write down the name & order number of ART Name ART …………………… Order number ART:
A02 For ART in A01 < 15 years old/unhealthy condition/parents need to be accompanied, write down the name and consecutive number of ART who accompany
Name ART …………………… Order number ART:
B. COMMUNICABLE DISEASE, NON-COMMUNICABLE DISEASE, AND GENETIC DISEASE HISTORY
[NAME] the following questions refer to the name taken in A01 Question B01-B40 are asked to all age
ACUTE RESPIRATORY INFECTION/INFLUENZA/SORE THROAT
B01 In the last 1 month, has [NAME] ever been diagnosed to suffer from Acute Respiratory Infection by health professionals (doctors/nurses/midwives)?
1. Yes B03 2. No
B02 n the last 1 month, has [NAME] ever suffered from fever with productive cough/dry cough or cold 1. Yes 2. No
PNEUMONIA
B03 In the last 1 month, has [NAME] ever been diagnosed to suffer from Pneumonia by health professionals (doctors/nurses/midwives)?
1. Yes B05 2. No
B04 In the last 1 month, has [NAME] ever suffered from high temperature with productive cough and breathe faster and shorter than usual/asphyxiate with signed by lower chest wall attraction?
1. Yes 2. No
TYPHOID FEVER
B05 In the last 1 month, has [NAME] ever been diagnosed to suffer from typhoid Fever by health professionals (doctors/nurses/midwives)?
1. Yes B07 2. Tidak
B06 In the last 1 month, has [NAME] ever suffered from fever especially in evening occurred > 1 week together with headache, coated tongue with red sign on its side, diarrhea, and constipation
1. Yes 2. No
MALARIA
B07 In the last 1 month, has [NAME] ever been diagnosed to suffer from malaria which confirmed by blood checking taken by health professionals (doctors/nurses/midwives)?
1. Yes B09
2. No B08 In the last 1 month, has [NAME] ever suffered from fever with shivering (feeling cold), periodic rise and drop
temperature, sweating, headache or without malaria symptoms but has already taken malaria drug? 1. Yes 2. No B10
B09 If Yes, Did [NAME] obtain medication using program drugs in the first 24 hours of fever? 1. Yes
2. No DIARRHEA
B10 In the last 1 month, has [NAME] ever been diagnosed to suffer from diarrhea by health professionals (doctors/nurses/midwives)?
1. YES B12 2. No
B11 In the last 1 month, has [NAME] ever suffered from defecation more than 3 times a day in with mushy or liquid feces?
1. Yes 2. No B13
RKD07.IND CONFIDENTIAL

2
B12 When diarrhea occurred, was it handle by oralit/household salt and sugar fluid consumption? 1. Yes 2. No
MEASLES/MORBILY
B13 In the last 12 month, has [NAME] ever been diagnosed to suffer from measles by health professionals (doctors/nurses/midwives)?
1. Yes B15 2.No
B14 In the last 12 months, has [NAME] ever suffered from fever with red and full of dirt eyed, rose spot on skin particularly in neck and chest?
1. Yes 2. No
PULMONARY TUBERCULOSIS (PULMONARY TB)
B15 In the last 12 month, has [NAME] ever been diagnosed to suffer from Pulmonary TB by health professionals (doctors/nurses/midwives)?
1. Yes B17 2. No
B16 In the last 12 months, has [NAME] ever suffered from productive cough > 2 or hemoptysis and difficult to gain/lose weight?
1. Yes 2. No
DENGUE HIGH FEVER (DHF)
B17 In the last 12 month, has [NAME] ever been diagnosed to suffer from Dengue High Fever by health professionals (doctors/nurses/midwives)?
1. Yes B19
2. No
B18 In the last 12 months, has [NAME] ever suffered from fever/high temperature, headache with chest/upper left abdominal pain, nauseous and vomiting, exhaustion, sometimes with rash and/nose bleeding, cold hands/legs?
1. Yes 2. No
HEPATITIS/LIVER DISEASE/YELLOW DISEASE
B19 In the last 12 month, has [NAME] ever been diagnosed to suffer from Dengue High Fever by health professionals (doctors/nurses/midwives)?
1. Yes B21
2. No B20
In the last 12 months, has [NAME] ever suffered from fever, exhaustion, digestion disorder (nauseous, vomiting, loss of appetite), upper abdominal pain, concentrated tea like urine, yellow eyed and skinned?
1. Yes 2. No
FILARIASIS/ELEPHANT FOOT DISEASE
B21 In the last 12 month, has [NAME] ever been diagnosed to suffer from Filariases by health professionals (doctors/nurses/midwives)?
1. Ya B23 2. Tidak
B22 In the last 12 months, has [NAME] ever had inflammation in ilium recurrently or genital/breast/upper and or lower limb enlargement (Filariasis/Elephant Foot)?
1. Ya 2. Tidak
ASTHMA/WHEEZING
B23 In the last 12 month, has [NAME] ever been diagnosed to suffer from asthma by health professionals (doctors/nurses/midwives)?
1. Yes B25 2. No
B24 In the last 12 months, has [NAME] ever had breathlessness with wheezing /stress on chest/awaken in the morning or another time due to feeling stress on the chest, asphyxiate attack/breathlessness without any reason while exercising or doing another physical activities?
1. Yes
2. No
DENTAL AND MOUTH
B25 In the last 12 month, Did [NAME] have dental and or mouth problems? 1. Yes 2. No B28
B26 In the last 12 month, Did [NAME] have treatment or medication from dental nurse, dentist or specialist dentist?
1. Ya 2. Tidak B28
B27 What kinds of treatment or medication for dealing with dental and mouth problem did [NAME] receive? (Read out POINT a UNTIL e) FILL ANSWER CODE WITH 1 = YES OR 2 = NO
a. Medication c. Protease planting or bridge planting e. Another dental treatment. Yes, namely…………
b. Tooth or mouth filling/extraction/ surgery
d. Counseling on dental & mouth care/hygiene
B28 Has [NAME] been losing all original teeth? 1. Yes 2. No

3
INJURY
B29 In the last 12 months, has [NAME] ever had injury which impair daily activities? 1. Yes 2. No B33
B30 Cause of injury (Read out POINT a UNTIL j) FILL THE ANSWER CODE WITH 1 = YES OR 2 = NO
a. Land transportation accident (bus/truck/train/motorbike/car) i. Cataclysm (earthquake, tsunami)
b. Marine transportation accident j. Committed suicide effort (mechanical, chemical)
c. Air transportation accident k. Sinking
d. Falling down l. Electric machine, radiation
e. Injured by sharp and dull object m. Burn, trapped by smoke
f. Aggression (dull/sharp objects, chemical materials) n. Asphyxiation
g. Shot by fire weapon o. Medical complication
h. Contact with toxic materials (animals, plants, chemical materials) p. Others, namely ..............................
B31 Part of body has been injured (Read out POINT a UNTIL j) FILL THE ANSWER CODE WITH 1 = YES OR 2 = NO
a. Head d. Abdominal, backbone, pelvis
bone g. Wrist area and hand j. Toe area and legs
b. Neck e. Upper shoulder and upper arm h. Hip area and upper leg
c. Chest f. Elbow area, forearm i. Knee and lower leg
B32 Types of injury: (Read out POINT a UNTIL j)
ISIKAN KODE JAWABAN DENGAN 1=YA ATAU 2=TIDAK
a. Impact/contusion c. Open wound e. Sprain g. Disjoint motoric
i. Others: ……………
b. Abrasion d. Burn f. Fracture h. Poisoned
CARDIAC DISEASE
B33 Has [NAME] ever been diagnosed to have cardiac disease by health professionals (doctors/nurses/midwives)?
1. Yes B35 2. No
B34 Has [NAME] ever been suffered from any symptoms/medical history: (Read out POINT a UNTIL i) FILL THE ANSWER CODE WITH 1 = YES OR 2 = NO
a. Blueish lips while crying or doing activities c. Fast heart beating without any
reason e. lower legs abscess
b. Pain in the chest/feeling heavy suppressed/breathless when walking in a rush/climbing/walking normally on flat road/heavy work/walk miles
d. Breathless when sleeping without using pillow
DIABETES MELLITUS B35 Has [NAME] ever been diagnosed to have Diabetes Mellitus by health professionals
(doctors/nurses/midwives)? 1. Yes B37 2. No
B36 Has [NAME] ever suffered from increased food intake, frequent urination, increased thirst, exhaustion, and losing weight or taking drugs for diabetes?
1. Yes
2.No

4
TUMOR / CANCER B37 Has (NAME) been diagnosed tumor/cancer by health professionals (doctor/nurse/midwife)? 1.Yes
2.No B40
B38 Since when is (NAME) diagnosed tumor? Year ....................
B39 Where is the location of the tumor/cancer READ POINT a UNTIL m) FILL IN THE ANSWER CODE WITH 1=YES OR 2=NO OR 7=NOT AVAILABLE
a. Eye, brain and part of nerve structure f. Digestion channel (intestines, liver) k. Soft tissue
b. Lips, mouth cavity and throat g. Urinary tract
l. Bone, cartilage bone
c. Thyroid gland and endocrine h. Female genital organ: ovarium, cervix
uteri m. Blood d. Respiratory Tract (lungs)
i. Male genital organ: Prostate
e. Breasts j. Skin
GENETIC DISEASE
B40 Does (NAME) have any medical complaint history of suffer from the following: (READ POINT a UNTIL h) FILL IN THE ANSWER CODE WITH 1=YES OR 2=NO OR 7=NOT AVAILABLE
a. Mental disorder (schizophrenia)/(observation) d. Cleft Lips (observation) g. Thalasemia
b. Color blindness e. Dermatitis allergy h. Hemophilia
c. Glaucoma f. Rhinitis allergy
IF ART 15 YEARS B41
IF ART < 14 TAHUN TO PART C. HEALTH SERVICE RESPONSIVENESS
QUESTIONS B41-B50, FOR ART 15 YEARS
JOINT ILLNESS / RHEUMATIC / GOUT
B41 In the last 12 months, has (NAME) been diagnosed joint illness / rheumatic / gout by health professionals (Doctor/ nurse/midwife)?
1. Yes B43
2. No
B42 In the last 12 months, has (NAME) suffered from feeling sick/pain/stiff/swollen around the joint, stiff around the joint after wake up from sleeping or after long break which emerge because of non accident cause?
1. Yes 2. No
HYPERTENSION / HIGH BLOOD PRESSURE
B43 In the last 12 months, has (NAME) been diagnosed hypertension/high blood pressure disease by health professionals (Doctor, nurse/midwife)?
1. Yes B45 2. No
B44 Is (NAME) still taking antihypertension medicine this time? 1. Yes 2. No
STROKE
B45 In the last 12 months, has (NAME) been diagnosed stroke by health professionals (Doctor, nurse/midwife)? 1.Yes B47 2. No
B46 In the last 12 months, has (NAME) been paralyzed in one part of the body or in the face muscle or voice disorder (lisp) suddenly?
1. Yes 2. No
IF ART 30 YEARS B47
IF ART < 29 YEARS TO PART C. HEALTH SERVICE RESPONSIVENESS
CATARACT (ART 30 YEARS)
B47 In the last 12 months, has one or both eyes of (NAME) been diagnosed/declared (clouded optometry lens) by health professionals (Doctor, nurse/midwife)?
1. Yes B49 2. No 8. Doesn’t know

5
B48 In the last 12 months, has (NAME) been experiencing in: (READ POINT a AND b) FILL IN THE ANSWER CODE WITH 1=YES OR 2=NO
a. Foggy/smoky/dewy or unclear sight
b. Has a sight problem related with light, such as blinded by bright lamp/lighting
a. b.
B49 In the last 12 months, has (NAME) been having cataract operation? 1. Yes 2. No C
B50 After cataract operation, does (NAME) wear glasses? 1. Yes 2. No
C. HEALTH SERVICE RESPONSIVENESS
Ca. INPATIENT SERVICE RESPONSIVENESS
Ca01 In the last 5 years, where did (NAME) go for the last inpatient service? 1. Government Hospital 6. Practiced Health Staff 2. Private Hospital 7. Traditional medication 3. Abroad Hospital 8. Others (Namely.....................................) 4. Maternity Hospital 9. Never had inpatient service Cb01 5. Health Center
Ca02 How much has She/He spent for the last inpatient service (in the last 5 years)? Rp. ……………….. ..
Ca03 Where is the cost source of the inpatient service from ? (READ POINT a UNTIL i) FILL IN THE ANSWER CODE WITH 1=YES OR 2=NO
a. Self financing e. Private insurance i. Healthy card /kartu sehat b. PT ASKES (employee) f. Dana Sehat/ JPKM j. Office reimbursement c. PT ASTEK/ Jamsostek g. Askeskin k. Statement letter of not being affordable/
SKTM d. ASABRI h. Health insurance local
goverment l. Others, Mention ……………………… For the last inpatient service, give assessment in the various aspects with the selection answers as follows:
1. VERY GOOD 2. GOOD 3. FAIR 4. BAD 5. VERY BAD
Ca04 How does (NAME) assess the duration of waiting time before getting inpatient service?
Ca05 How does (NAME) assess the hospitality from health staff in greeting and speaking?
Ca06 How does (NAME) assess the experience to get intelligibility of information related to the disease from the health staff?
Ca07 How does (NAME) assess the experience to participate in making decision about health treatment or the medication?
Ca08 How does (NAME) assess the way of health service to assure the confidentiality or able to talk personally related to the disease?
Ca09 How does (NAME) assess the freedom to choose facility, medium/device and health staff?
Ca10 How does (NAME) assess the cleanliness of inpatient room includes the bath room?
Ca11 How does (NAME) assess the easy access to be visited by family and friends during the inpatient treatment in the health facility?

6
Cb. OUTPATIENT SERVICE RESPONSIVENESS
Cb01 In the last 1 month, where did (NAME) go for the last outpatient service? 01. Government hospital 06. Practiced health staff 02. Private hospital 07. Praditional medication 03. Maternity Hospital 08. Others (mention.....................................) 04. Puskesmas/Pustu/Pusling/ Posyandu 09. At home 05. Policlinic/private clinic 10. Never had outpatient service Cb10a
Cb02 How much has She/He spent for the last outpatient service (in the last 1 year)? Rp. ……………….. ..
Cb03 Where is the cost source of the outpatient service from ? (READ POINT a UNTIL i) FILL IN THE ANSWER CODE WITH 1=YES OR 2=NO
a. Self financing e. Private insurance i. Healthy card /kartu sehat
b. PT ASKES (employee) f. Dana Sehat/ JPKM j. Office reimbursement
c. PT ASTEK/ Jamsostek g. Askeskin k. Statement letter of not being affordable/ SKTM
d. ASABRI h. Health insurance local government l. Others, Mention ………………………
For the last outpatient service, give assessment in the various aspects with the selection answers as follows: 1. VERY GOOD 2. GOOD 3. FAIR 4. BAD 5. VERY BAD
Cb04 How does (NAME) assess the duration of waiting time before getting outpatient service?
Cb05 How does (NAME) assess the hospitality from health staff in greeting and speaking?
Cb06 How does (NAME) assess the experience to get intelligibility of information related to the disease from the health staff?
Cb07 How does (NAME) assess the experience to participate in making decision about health treatment or the medication?
Cb08 How does (NAME) assess the way of health service to assure the confidentiality or able to talk personally related to the disease?
Cb09 How does (NAME) assess the freedom to choose facility, medium/device and health staff?
Cb10 How does (NAME) assess the cleanliness outpatient service room includes the bath room? FILL IN WITH CODE ”7” IF THE PLACE FOR OUTPATIENT SERVICE IS (Cb01) “ATHOME”
Cb10a
IF ART 0 - 4 YEARS G. IMMUNIZATION AND GROWTH MONITORING
IF ART 5 - 9 YEARS XI. MEASUREMENT AND EXAMINATION
IF ART >10 YEARS D. KNOWLEDGE, ATTITUDE AND BEHAVIOR
D. KNOWLEDGE, ATTITUDE AND BEHAVIOUR (ALL HOUSEHOLDS ≥ 10 YEARS)
AVIAN INFLUENZA
D01 Has (NAME) ever heard about avian influenza in the human body? 1. Yes
2. No D04 D02 How through what media) the disease spread to human? (POINT "a" UNTIL "g" ARE NOT READ).
FILL IN THE ANSWER CODE WITH 1=YES OR 2=NO
a. Air d. Contact with sick bird g. Others, mention ..............................
b. Close to the sufferer e. Contact with bird's faces c. Fly f. Food

7
D03 What should (NAME) do if there is a sick bird or sudden dead bird? ((POINT "a" UNTIL "f" ARE NOT READ).
FILL IN THE ANSWER CODE WITH 1=YES OR 2=NO
a. Report to the related agency c. Buried/burn sick and dead chicken e. Sell it
b. Clean the poultry cage/place d. Cook and eat f. Others: …………………
HIV/AIDS
D04 Does (NAME) knows about HIV/AIDS? 1. Yes 2. No D08 D05 The spread of HIV/AIDS to human through: (POINT "a" UNTIL "h" ARE NOT READ)
FILL IN THE ANSWER CODE WITH 1=YES OR 2=NO
a. Intercourse d. Share with other in using shaving knives/shaver g. The spreading from mother to baby during pregnant period
b. Injection needle e. The spreading from mother to the baby during delivery process
h. Others: ……………….
c. Blood transfusion f. Use condom in the intercourse
D06 How to prevent from HIV/AIDS? (READ POINT a UNTIL f) FILL IN THE ANSWER CODE WITH 1=YES OR 2=NO
a. No intercourse with others except with permanent partner
c. No intercourse at all e. Do not share injection needle
b. No intercourse with drug user especially the one using injection needle
d. Use condom in the intercourse
f. Do not share shaving knife/shaver
D07 If there is a family member of (NAME) suffers from HIV/AIDS? (READ POINT a UNTIL e) FILL IN THE ANSWER CODE WITH 1=YES, 2=NO OR 8 = DOESN'T KNOW
a. Keep secret c. Counselling and medication e. Excommunicate him/her
b. Talk with other members of the family d. Look for alternative medication
HYGIENIC BEHAVIOUR
D08 Does (NAME) wash hands with soap? (READ POINT a UNTIL d) FILL IN THE ANSWER CODE WITH 1=YES OR 2=NO
a. Before eating c. After defecating/after washing baby's genital/anus
b. Before preparing food d. After holding animals (bird, cat, dog)
D09 Where does (NAME) usually defecate? 1. Latrine 3. River/lake/sea 5. Beach/field/garden/yard 2. Pool/rice field/drain 4. Hole in the ground 6. Others: ...........................
D10a Does (NAME) usually wash teeth every day? D10b When does (NAME) brush teeth? (READ POINT a UNTIL e)
FILL IN THE ANSWER CODE WITH 1=YES OR 2=NO
a. During morning and/evening shower c. After waking up in the morning e. Others, mention………..
b. After having breakfast d. Before going to bed TOBACCO USAGE
D11 Did (NAME) smoke/chew tobacco in the last 1 month? (READ THE SELECTION ANSWERS) 1. Yes,everyday 3. No, but she/he did before D16 2. Yes, sometimes D13 4. Never D18
D12 How old was (NAME) when she/he started to smoke/chew tobacco everyday? FILL IN WITH "88" IF THE RESPONDENT ANSWERS: DON'T REMEMBER
...............years

8
D13 How many cigarette/cigar/pipe/quid of tobacco does (NAME) consume in average per day? ...........pieces D14 Mention the varian of cigarette/tobacco that is usually smoked by [NAME]:: (READ OUT POINT a UNTIL h)
FILL WITH 1 = YES OR 2 = DOESN'T KNOW
a. Cloves cigarette with filter d. Hand-rolled cigarette g. Chewed tobacco (quid, betel)
b. Cloves cigarette without filter e. Pipe cigarette h. Others: ………………
c. Cigarette f. Cigar D15
Is [NAME] used to smoke inside the house while gathering with another household members?
1. Yes D17 2. No D17 D16 How old is [NAME] when start to stop smoking/not smoking/not chewing any tobacco at all?
FILL IN WITH "88" IF THE RESPONDENT ANSWERS: DON'T REMEMBER ............... year
D17 How old is [NAME] at the first time to smoke/chew tobacco?? FILL IN WITH "88" IF THE RESPONDENT ANSWERS: DON'T REMEMBER
............... year ALCOHOL
Note (USE SIMULATOR CARD): 1 unit of standard alcohol drink contains 8 - 13 g ethanol, for example in: 1 glass/small bottle/can (285 - 330 ml) of beer
1 cone glass (60 ml) of aperitif 1 Small glass/sloki (30 ml) of whiskey 1 cone glass (120 ml) of wine
D18 In the last 12 months, is [NAME] consuming alcohol drink? (branded alcohol drink such as beer, vodka, wine, etc, and traditional drink like tuak, poteng, sopi)?
1. Yes
2. No D22
D19 In the last 12 months, has [NAME] ever consumed alcohol? 1. Yes 2. No D22
D20 In the last 1 month, how often did [NAME] drink alcohol? (GIVE THE PROVIDED ANSWERS) 1. 5 days or more every week 3. 1 - 3 days every month 2. 1 - 4 days every week 4. < 1x every month
D21a Most consumed alcohol 1. Beer 2. Whiskey/ Vodka
D21b While drinking alcohol, how many unit of drinking standard in average that usually taken by [NAME] in a day? FILL WITH "88" IF THE RESPONDENT SAID UNKNOWN
………..unit’s
(USE SIMULATOR CARD) PHYSICAL ACTIVITY
Bellow are questions on physical activity in relation with occupation, leisure time and transportation
D22 Is [NAME] used to have heavy physical activity that happened continuously during 10 minutes
in minimum every time it occurs
1. Yes
2. No D25
D23 How many days in a week does [NAME] usually have the mentioned heavy physical activity? ………….day D24 Usually at the day [NAME] has heavy physical activity, how long totally it spent to finish all
those activities?
………….hour
……….minute
D25 Is [NAME] used to have moderate physical activity? 1 Yes
2. NO D28 D26 Usually how many days in a week does [NAME] has the mentioned moderate physical activity? ………….days D27
Usually at the day [NAME] has moderate physical activity, how long totally it spent to finish all
those activities?
…………hours
……….minutes
D28 Does [NAME] usually take a walk or bicycling continuously at least 10 minutes?
1. Yes
2. No D31

9
D29 Usually how many days in a week does [NAME] take a walk or bicycling during 10 minutes
minimally? ………….day
D30 Usually in one day, how long [NAME] takes totally for walking or bicycling? ………….hour
……….minute
FOOD CONSUMPTION BEHAVIOR
D31 Usually in one week, how many days does [NAME] eat fresh fruit? (Use Simulation card) IF THE ANSWER IS “0”`Go to D33
…… day D32 How many portions of fresh fruits averagely [NAME] eats in a day on the mentioned days?
(Use Simulation card) …….portion
D33 Biasanya dalam 1 minggu, berapa hari [NAMA] mengkonsumsi sayur-sayuran segar? (Use Simulation card) IF THE ANSWER IS “0”`Go to D35
……day D34 Berapa porsi rata-rata [NAMA] mengkonsumsi sayur-sayuran segar dalam sehari?
(Use Simulation card) …….portion
ASK THE POINT D35 WITHOUT SIMULATOR CARD AND FILL THE PROVIDED ANSWER CODE: 1 > once a day 4 1-2 times a week 2 once a day 5 < 3 times per month 3 3-6 times a week 6 Never
D35
Usually how many times [NAME] consumes the following food: (READ OUT POINT a UNTIL h
a. Sweet meals/drinks d. Innards (intestines, babat, paru) g. Caffeine drinking b. . Salty food e. Grilled/baked food h. Additive flavor (vetsin, ketchup,
terasi) c. Fatty food f. Preserved food
D35a
IF HOUSEHOLD MEMBER 10 - 14 YEARS → XI. MEASUREMENT AND CHECKING
IF HOUSEHOLD MEMBER > 15 YEARS ® E. DISABILITY
Now I will ask about health condition by [NAME]'s own perception The concerned health condition here is both physical and mental condition of [NAME]'s
E. DISABILITIES (HOUSEHOLD MEMBER AGED > 15 YEARS)
FOR POINT E01 - E11, READ OUT THE QUESTION & ALTERNATIVE ANSWERS. FILL THE ANSWER CODE WITH::
1. None 3. Moderate 5. Serious 2. Mild 4. Severe
In the last 1 month, how severe did [NAME] get short breath after having mild exercise. For example go upstairs with 12 traps?
E01 In the last 1 month, how difficult is it for [NAME] to see and recognize people across the street (in about 20 meters) although using glasses/soft lens aid?
E07
In the last 1 month, how severe did [NAME] suffer from cough or sneeze for 10 minutes or more in one onset?
E02 In the last 1 month, how difficult is it for [NAME] to see and recognize an object as far as arm/reading distance (30 cm) although using glasses/soft lens aid?
E08
In the last 1 month, how often did [NAME] suffer from sleeping disorder (such as easily feel sleepy, awaken frequently at midnights or earlier than usual)?
E03 In the last 1 month, how difficult is it for [NAME] to hear someone's speaking with normal voice and standing at another side in one room although using hearing aid?
E09
In the last 1 month, how severe did [NAME] get difficulties to remain standing in 30 minutes?
E04 In the last 1 month, how difficult is it for [NAME] to hear someone's speaking to another person in a silent room although using hearing aid?
E10
In the last 1 month, how severe did [NAME] get difficulties to remain standing in 30 minutes?
E05 In the last 1 month, how difficult is it for [NAME] to hear someone's speaking to another person in a silent room although using hearing aid?
E11 In the last 1 month, how severe did [NAME] get problems to walk far along 1 kilometer approximately?

10
FOR POINT E12 - E20, READ OUT THE QUESTION & ALTERNATIVE ANSWERS. FILL WITH PROVIDED ANSWER CODE: 1. None 2. Mild 3. Moderate 4. Difficult 5. Very Difficult
E12 In the last 1 month, how difficult for [NAME] to concentrate on a certain activity or recall something in 10 minutes?
E17 In the last 1 month, how difficult for [NAME] to interact/socialize with unrecognized people?
E13 In the last 1 month, how difficult for [NAME] to clean the whole body like taking a bath? E18
In the last 1 month, how difficult for [NAME] to maintain friendship?
E14 In the last 1 month, how difficult for [NAME] to put on clothes? E19
In the last 1 month, how difficult for [NAME] to do [NAME]'s responsibilities as household member?
E15 In the last 1 month, how difficult for [NAME] to run daily activities? E20
In the last 1 month, how difficult for [NAME] to get involve in social activity (gathering, religious activity or others?
E16 In the last 1 month, how difficult for [NAME] to understand someone's talking?
FOR QUESTIONS E21 - E23, READ THEM OUT & FILL WITH CODE 1 = YES OR 2 = NO
E21 In the last 1 month, did [NAME] need assistance from other people to take care [NAME]'s life (eating, taking a bath, dressing) E22
In the last 1 month, did [NAME] need assistance from other people to do some activities/movement (such as wake up, walk in the house or go out)
E23 In the last 1 month, did [NAME] need assistance from other people to communicate (talking and can be understood by counterpart)
F. MENTAL HEALTH (ALL HOUSEHOLD MEMBERS > 15 YEARS OLD)
THESE WERE ASKED FOR CONDITION IN THE LAST 1 MONTH To get more understanding on health condition of [NAME] we will ask 20 questions that require "Yes" or "No" answer Kalau If [NAME] doesn't really understand, we will read once again but we will not explain/discuss it If [NAME] has question we will discuss after finishing the whole 20 questions.
FILL WITH CODE 1 = YES OR 2 = NO
F01 Does [NAME] often get headache? F11 Does [NAME] feel uncomfortable in stomach?
F02 Does [NAME] lose appetite? F12
Does [NAME] feel hard to enjoy daily activities?
F03 Is [NAME] difficult to sleep? F13 Does [NAME] feel hard to make decision?
F04 Is [NAME] easy to get scared? F14
Is [NAME]'s daily activity impaired?
F05 Does [NAME] feel tense or worried? F15 Is [NAME] not able to create meaningful things in
life? F06 Is [NAME]'s hands shaking? F16
Does [NAME] lose interest on numerous things?
F07 Is [NAME]'s digestion impaired? F17 Does [NAME] feel unworthy?
F08 Is [NAME] difficult to think clearly? F18
Does [NAME] has a though to end [NAME]'s life?
F09 Is [NAME] feel unhappy? F19 Does [NAME] feel exhausted all time?
F10 Is [NAME] crying more often? F20 Is [NAME] easy to feel exhausted?
CHECK AGAIN, QUESTION F01 UNTIL F20 MUST BE ANSWERED
CONTINUE TO → BLOCK XI. MEASUREMENT and EXAMINATION

11
G. IMMUNIZATION AND GROWTH MONITORING
(SPECIAL FOR HOUSEHOLD MEMBER AGED 0 – 59 MONTHS/UNDER FIVES
G01 A1. NAME]’s age in months a2. NAME]'s age in months b. Date of birth: (dd-mm-yy) --
G02 In the last 6 months, how many times has [NAME] been weighed? IF THE ANSWER IS NEVER, FILL WITH "00" OR IF IT IS "DOESN'T KNOW", FILL
WITH "88" → GO TO G04
........... times G03 Where has [NAME] been weighed mostly?
1. Hospital 2. Puskesmas/ Pustu 3. Polindes 4. Posyandu 5. Other: ......……… G04 In the last 6 months, did [NAME] receive vitamin A capsule (USE SIMULATOR CARD) 1. Yes 2. No G05 Has [NAME] ever received immunization such as: (THE INFORMATION CAN BE COLLECTED FROM MANY SOURCES
a. BCG immunization to TBC that is initially given at 1 day old and
injected on upper arm or thigh and leave scar? 1. Yes
2. No G05.c 8. Don’t know G05.c
b. How old did [NAME] receive BCG immunization? (FILL WITH
DAYS OR MONTHS) ((IF IT IS UNKNOWN, FILL WITH CODE "88" IN DAY &
MONTH))
............ Day ........ Month
c. Polio immunization in which red or white liquid is usually given at 2
months age and dropped to mouth? 1. Yes
2. No G05.f 8. Don’t know G05.f
d. How old was [NAME] receive polio immunization for the first time??
(IF IT IS UNKNOWN, FILL WITH CODE "88" IN MONTH)) ............. Month
e. How many times was [NAME] immunized polio? .......... Times
f. DPT immunization that is usually injected on thigh and initially given
at 2 months age together with polio immunization? 1. Yes
2. No G05.h 8. Don’t know G05.h
g. How many times has [NAME] received DPT immunization? .......... Times h. Measles immunization that is usually given once at age 9 months and
injected on thigh?? 1. Yes
2. No 8. Don’t know
i. Hepatitis B immunization that is usually given at age 1 day and
injected on thigh? 1. Yes
2. No G06 8. Don’t know G06
j. How old did [NAME] receive BCG immunization for the first time?
(FILL WITH DAYS OR MONTHS) (IF IT IS UNKNOWN, FILL WITH CODE "88" IN DAY &
MONTH)
.......... Day ......... Month
How many times has [NAME] received Hepatitis B immunization? .......... times G06
Among the whole immunizations [NAME] received in the last 2 years,
is there any of them [NAME] received at National Immunization Week
(PIN)?
1. Yes 2. No
3. No immunization 8. Don’t know
G07 Does [NAME] has KMS? (request them to show KMS)
1. Yes, able to show it with immunization notes 2. Yes, able to show it without immunization notes →G09
3. Yes, unable to show it →G09 4. Doesn't have →G09
G08 Copy from KMS, date…/month./year… of immunization for each kind WRITE '88' IN COLUMN 'DATE/MONTH/YEAR', IF THE CARD SHOWS THAT IMMUNIZATION HAS BEEN
GIVEN BUT THE DATE/MONTH/YEAR IS EMPTY. WRITE DOWN '99' IF IMMUNIZATION WAS NOT GIVEN
a. BCG // g. DPT2 // b. Polio 1 // h. DPT3 //
c. Polio 2 // i. Measles //
12
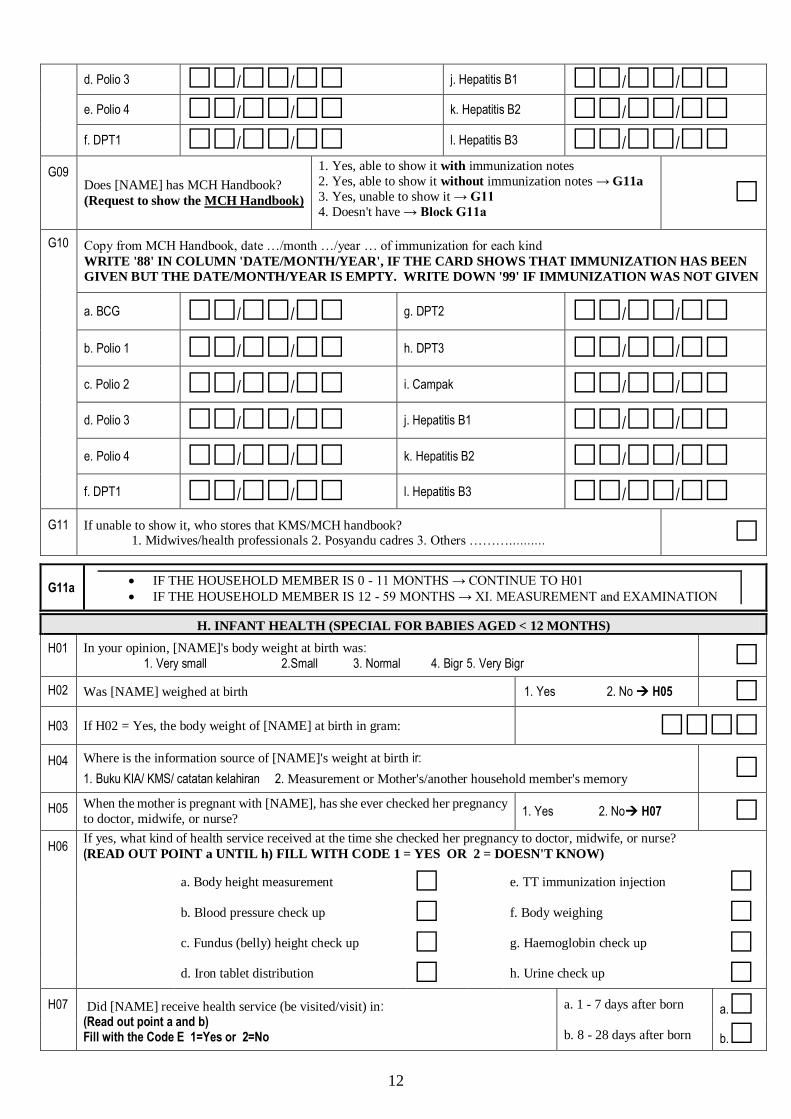
d. Polio 3 // j. Hepatitis B1 // e. Polio 4 // k. Hepatitis B2 //
f. DPT1 // l. Hepatitis B3 // G09
Does [NAME] has MCH Handbook?
(Request to show the MCH Handbook)
1. Yes, able to show it with immunization notes
2. Yes, able to show it without immunization notes → G11a
3. Yes, unable to show it → G11
4. Doesn't have → Block G11a
G10 Copy from MCH Handbook, date …/month …/year … of immunization for each kind WRITE '88' IN COLUMN 'DATE/MONTH/YEAR', IF THE CARD SHOWS THAT IMMUNIZATION HAS BEEN
GIVEN BUT THE DATE/MONTH/YEAR IS EMPTY. WRITE DOWN '99' IF IMMUNIZATION WAS NOT GIVEN
a. BCG // g. DPT2 //
b. Polio 1 // h. DPT3 //
c. Polio 2 // i. Campak //
d. Polio 3 // j. Hepatitis B1 // e. Polio 4 // k. Hepatitis B2 //
f. DPT1 // l. Hepatitis B3 // G11 If unable to show it, who stores that KMS/MCH handbook?
1. Midwives/health professionals 2. Posyandu cadres 3. Others ……….………
G11a IF THE HOUSEHOLD MEMBER IS 0 - 11 MONTHS → CONTINUE TO H01
IF THE HOUSEHOLD MEMBER IS 12 - 59 MONTHS → XI. MEASUREMENT and EXAMINATION
H. INFANT HEALTH (SPECIAL FOR BABIES AGED < 12 MONTHS)
H01 In your opinion, [NAME]'s body weight at birth was: 1. Very small 2.Small 3. Normal 4. Bigr 5. Very Bigr
H02 Was [NAME] weighed at birth 1. Yes 2. No H05 H03 If H02 = Yes, the body weight of [NAME] at birth in gram:
H04 Where is the information source of [NAME]'s weight at birth ir:
1. Buku KIA/ KMS/ catatan kelahiran 2. Measurement or Mother's/another household member's memory
H05 When the mother is pregnant with [NAME], has she ever checked her pregnancy
to doctor, midwife, or nurse? 1. Yes 2. No H07
H06 If yes, what kind of health service received at the time she checked her pregnancy to doctor, midwife, or nurse? (READ OUT POINT a UNTIL h) FILL WITH CODE 1 = YES OR 2 = DOESN'T KNOW)
a. Body height measurement e. TT immunization injection b. Blood pressure check up f. Body weighing c. Fundus (belly) height check up g. Haemoglobin check up d. Iron tablet distribution h. Urine check up H07 Did [NAME] receive health service (be visited/visit) in:
(Read out point a and b) Fill with the Code E 1=Yes or 2=No
a. 1 - 7 days after born b. 8 - 28 days after born
a.
b.

13
XI. MEASUREMENT AND EXAMINATION
THE MEASUREMENT OF ANTHROPOMETRY, BLOOD PRESSURE, ABDOMINAL CIRCUMFERENCE
ALL AGES
1. Body Weight (kg) , 2a. Body height/Body
Length (cm) ) ,
2b. Special for under fives, Body Height/Body Length 1. Standing 2. Lying
SPECIAL FOR HOUSEHOLD MEMBER AGED > 15 YEARS
3 Blood Pressure (mmHg)
EXAMINATION 1 EXAMINATION 2 EXAMINATION 3
a. Systolic 1 b. Diastolik 1 d. Systolic 2 e. Diastolik 2
Hanya dilakukan bila selisih pengukuran tekanan darah 1 dan 2 > 10 mmHg
g. Systolic 3 h. Diastolik 3
c. Artery 1 f. Artery 2 i. Artery 3
4 Abdominal Circumference ……............. cm ,
SPECIAL FOR REPRODUCTIVE AGED WOMEN (15 - 45 YEARS OLD) INCLUDING PREGNANT MOTHERS
5 Mid-Upper Arm Circumference …................ cm ,
VISUS EXAMINATION (SPECIAL FOR HOUSEHOLD MEMBER AGED > 5 YEARS
6 Is any trouble with [NAME]'s eyes: (DO THE OBSERVATION)
Rigth Left
a. Cross-eyed 1. Yes 2. No a1. 1. Yes 2. No a2.
b. Pterigium 1. Yes 2. No b1. 1. Yes 2. No b2.
c. Cornea Scar 1. Yes 2. No c1. 1. Yes 2. No c2.
d. Cataract 1. Yes 2. No d1. 1. Yes 2. No d2.
7. Using glasses (far and or near sighted)? 1. Yes 2. No
VISUS EXAMINATION: 1. If [NAME] is not using glasses, the visus examination is still carried out 2. 2. If [NAME] is using glasses, conduct the visus examination by keep wearing glasses
8. Without Pinhole a. Right: / b. Left /
9. With Pinhole a. Right: / b. Left /
NOTE FOR RESPONDENTS WHO ARE UNABLE TO SEE SNELLEN CARD OR E CARD → DO FINGER COUNT 1. If [NAME] can see FINGER COUNT in 3 meters → WRITE 03/060
2. If [NAME] can see FINGER COUNT in 2 meters → WRITE 02/061 3. If [NAME] can see FINGER COUNT in 1 meter → WRITE 01/062
4. If [NAME] can only see a HANDSHAKE in 1 meter → WRITE 01/300
5. If [NAME] can only see FLASHLIGHT → WRITE 01/888
6. If [NAME] can not see a light (TOTAL BLIND) → WRITE 00/000

14
PERMANENT TEETH EXAMINATION (SPECIAL FOR HOUSEHOLD MEMBER AGED > 12 YEARS
10. Give D, M, or F code in every dentogram room below:
D (decayed) Cavity
M (missing) = tooth have been extracted/remain tooth root
F (filling) = filled tooth
IF ON THE SAME TOOTH THERE IS A CAVITY AND FILLING AS WELL THEN WRITE "DF" IN ONE
DENTOGRAM ROOM
(I) Right Left (II) 8 7 6 5 4 3 2 1 1 2 3 4 5 6 7 8
III Kanan Kiri IV 8 7 6 5 4 3 2 1 1 2 3 4 5 6 7 8
(III) Right Left (IV)
FILED BY ENUMERATOR DATA
∑D-T ∑M-T ∑F-T
1 = Incisivus 1 (gigi seri 1) 4 = Premolar 1 (geraham kecil 1) 7 = Molar 2 (geraham besar 2) 2 = Incisivus 2 (gigi seri 2) 5 = Premolar 2 (geraham kecil 2) 8 = Molar 3 (geraham besar 3) 3 = Caninus (taring) 6 = Molar 1 (geraham besar 1)
BLOOD AND URINE CHECK
11. Is blood speciem extracted 1. Yes 2. No → Go to XI.13 or to ENUMERATOR'S NOTE
12. BLOOD NUMBER STICKER ATTACH THE STICKER HERE
13 Is urine sample collected (Special for household
member aged 6 - 12 years)
1. Yes 2. No → Go to ENUMERATOR'S NOTE
14. URINE NUMBER STICKER ATTACH THE STICKER HERE
ENUMERATOR'S NOTE
Related Documents











