Copyright 1988 by The HurnanaPress, Inc. All rights of any naturewhatsoever reserved. House Dust Mite and Dust ControP Susan Pollart, Martin O. Chapman, and Thomas Ao E. Platts-Mills It has been more than two decades since the house dust mite was first implicated as a major source of allergen in house dust. In 1964, Voorhorst et al. (1) demonstrated that positive skin tests to Der- matophagoides pteronyssinus extract were common in patients with a history of allergy. Further investigation identified D. fari- nae as an additional important source of allergen, particularly in the United States. Since then, dust mites have been identified in most parts of the world, and in many areas they are regarded as the single most important allergen associated with asthma (2,3). BothDermatophagoides species and the other mites that occur in house dust avoid light and require warmth and humidity to flourish and, as their genus name implies, use human skin scales as a food source. In keeping with these requirements, any furniture, bed- ding, clothing, or carpeting can act as a "nest" for mites. In addition, the requirement for warmth and humidity can lead to a large sea- sonal variation in mite counts and antigen levels (Fig. 1) (4,5) (Platts-Mills, T. E., Hayden, M. L., Chapman, M. D., Wilkins, S. R., manuscript submitted for publication). Under appropriate cli- matic conditions, high levels of antigen can be found in houses of both allergic or nonallergic persons. In the homes of atopie pa- tients, elevated levels may exacerbate their allergic symptoms. Therapy of mite atlergy consists of symptomatic medical treat- ment, immunotherapy in selected cases, and allergen avoidance. Medical therapy designed to control house dust-related allergic dis- *Address corrrespondence and reprint requests to: Gerald L. Klein, M.D., 2067 W. Vista Way, Vista, CA 92083. Clinical Reviews in Allergy 23 Volume 6, 1988

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Copyright �9 1988 by The Hurnana Press, Inc. All rights of any nature whatsoever reserved.
House Dust Mite and Dust ControP
Susan Pollart, Martin O. Chapman, and Thomas Ao E. Platts-Mills
It has been more than two decades since the house dust mite was first implicated as a major source of allergen in house dust. In 1964, Voorhorst et al. (1) demonstra ted tha t positive skin tests to Der- matophagoides pteronyssinus extract were common in pat ients with a history of allergy. Fur the r investigation identif ied D. fari- nae as an addit ional impor tant source of allergen, par t icular ly in the Uni ted States. Since then, dust mites have been identif ied in most parts of the world, and in m a n y areas they are regarded as the single most impor tant al lergen associated with a s thma (2,3).
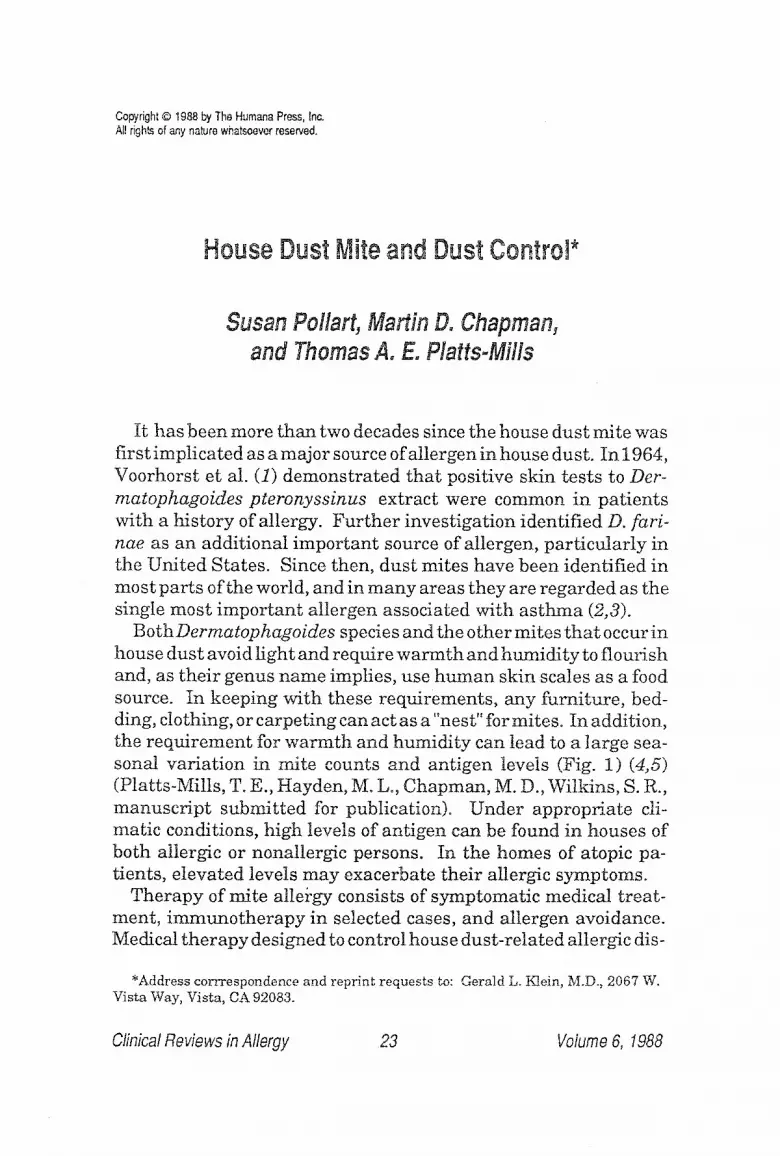
BothDermatophagoides species and the other mites tha t occur in house dust avoid l ight and require warmth and humid i ty to flourish and, as their genus name implies, use h u m a n skin scales as a food source. In keeping with these requirements , any furni ture, bed- ding, clothing, or carpeting can act as a "nest" for mites. In addition, the requi rement for warmth and humidi ty can lead to a large sea- sonal var ia t ion in mite counts and ant igen levels (Fig. 1) (4,5) (Platts-Mills, T. E., Hayden, M. L., Chapman, M. D., Wilkins, S. R., manuscr ip t submit ted for publication). Under appropriate cli- matic conditions, high levels of ant igen can be found in houses of both allergic or nonallergic persons. In the homes of atopie pa- tients, elevated levels may exacerbate their allergic symptoms.
Therapy of mite atlergy consists of symptomatic medical treat- ment, immuno the rapy in selected cases, and allergen avoidance. Medical therapy designed to control house dust-related allergic dis-
*Address corrrespondence and reprint requests to: Gerald L. Klein, M.D., 2067 W. Vista Way, Vista, CA 92083.
Clinical Reviews in Allergy 23 Volume 6, 1988
24 Poltart, Chapman, and Platts-Mflls
I 0 i 10 ~. 6
E ~ . t 0 4.
W "K
, - g
O3
(9
C.H~ SOFA ~ ,~ ~ ~, . / " ~ / \
g r a s s : ',, + ~
[ ",, " % ,, o If ',
" ~ i ~, \\ Mi tes , , \\~
] /,/ \ '~\\ +/,/0,,. / ,," ,, ,.,
o - - - - - . !/ " " * - <3- . . . . . . . 0 + - - + - - ~ - ' ~ O . . . . . . . . 0 . . . . . . . O - . . . . . . (3- . . . . . . . 0 . . . . . . . O - . . . . . . 0
4-0 2-6 4-9 6"3
FEB APR
- 5 O 0 I I 1
0
-t "0
- 5 0
o cl Q
AbsokJte 15 14 15 8+1 9,4 2-2 4 -5 1-9 H u m i d i t y
I I J t + t t a g /Kg JUN AUG OCT DEC
Fig. 1. Seasonal variation in mite allergen antigen P+ (0-- - -0) and in mites ( . . . . . ) in dust obtained from a sofa in the house of a mite allergic patient with asthma. The figure also shows a peak of grass pollen allergen (0- - -0) in the same dust samples in May and June and the outdoor absolute humidity in the Charlottesville area. The arrows indicate the period during which patient OH showed increasing symptoms. In early October he required an in- crease in his treatment.
ease can be burdensome and expensive, especially in areas where the temperature and humidity during summer and fall can produce very high antigen levels for five months or more. At present, only D. farinae extract is available in the United States, however, the major Dermatophagoides allergens Der f I and Der p I are highly crossreactive and it is unusual to find a patient who is truly allergic to one species and not to the other (6,7). Further investigation needs to be done to elucidate other major and minor cross-reacting allergens. Therefore, on the basis of present information, it would seem preferable to use both species of mites for both immunother- apy and diagnosis (8).
In 1927, Storm Van Leeuwen (9) demonstrated that asthmatic patients placed in the dust-free environment or a climate chamber for 3 wk showed improvement in their symptoms. In 1970, Kerribijn (10) reported that mite allergic asthmatic children from the Netherlands improved dramatically over the period of a year spent in a sanatorium in Switzerland. TMs sanatorium was in the town ofD avos, had been studied by Spieksma previously, and found
Clinical Reviews in Allergy Volume 6, t988

Dust Mite 25
to have very low mite levels (1). Later work with patients hospi- talized in an allergen-free room for 6 wk or more not only showed an improvement of symptoms but also a reversal of their bronchial hyperreactivity (11). In that study, the mean level of mite allergen in the patients' bedrooms was 13.4 mg Der p I/g of dust, whereas comparable levels in the allergen-free room were <0.2 mg/g. This improvement occurred under conditions that included more than a 95% reduction in mite allergen level. Trials of avoidance in out- patients have had mixed results but have also varied widely in the methods used to reduce mite counts and antigen levels.
Studies in Europe and the United States have found that the areas of highest mite concentration and antigen levels were mat- tresses, bedding, pillows, children's stuffed toys, upholstered fur- niture, and bedroom carpeting (12,13)o The quantity of allergen found in house dust is generally proportional to the number of mite bodies; however, this correlation shows considerable variation and in two situations we found considerable discrepancies. In bed-cov- ers stuffed with "cotton wool" or absorbent cotton, the dust often contains few or no mJtes even when the allergen levels are very high; presumably, the mite bodies stay within the cotton. In a re- cent year-rotmd study (Platts-Mills, T. A. E., Hayden, M. L., Chapman, M. D., Wilkins, S. R., manuscript submitted for publica- tion), it was found that allergen levels rose in parallel with mite numbers and humidity in June and July. However, mite numbers fel! sharply in September and October, whereas mean allergen lev- els stayed high until January. Presumably, this represents a pro- gressive withdrawal of live mites from the surface areas as drying occurs. Certainly this recent study does demonstrate that drying occurs very slowly, away from surface areas, and this explains why mite antigen levels can stay high year round in upholstered furni- ture. Investigations suggest that even with enthusiastic use of ef- ficient vacuum cleaners the efficacy is limited to removal of mite allergen on the surface as the live mites generally live away from the surface areas and are unaffected by vacuum cleaning~ Re- placement or renewal of bedding, mattresses, or carpets for mite allergic patients does not seem effective since recolonization usu- allly occurs in months (14). In a study on allergen avoidance that used regular vacuum cleaning of bedrooms as the major avoidance measure, there was no improvement in the patients' symptoms and
Clinical Reviews in Allergy Volume 6, 1988

26 Pollart, Chapman, and Plata-Mills
also no significant change m the mite antigen levels as measured by radio-aliergosorbent test (RAST) inhibition (14).
The two most successful studies on dust avoidance in the home have applied very strenuous efforts to cleaning of bedrooms, inclu- cling removal of carpeting, covering of mattresses, and regular washing of bedding. The group of children treated by Murray and Ferguson (15) was provided with zippered vinyl covers for pillows, mattresses, and box springs and instructions for making the bed- room as easy to clean as a hospital ward. At the end of a one-month study period, there was not only a marked and statistically sigrS- ficant difference in symptoms and signs of asthma between the treatment and control goups, but also bronchial tolerance to aero- solized histamine significantly improved in the group whose bed- rooms had been modified. Similar results were obtained in a study done by Sarsfield et al. (I6) on dust mite avoidance measures. The subjectivity of reporting by patients limits the interpretation of this data. As techniques for measuring antigen levels in houses ira- prove, future work on the value of dust control can be more object- ively evaluated by relating changes in the quantity of house dust mite allergen in homes to objective measures of lung function.
We agree with the aggressive cleaning approach to reduce mite numbers in houses. Important to note is that washing of bedding as a way to kill mites is only effective at temperatures greater than 70~ and that vacuuming of carpets, although helpful in removing surface dust and fecal pellets, should not be considered equivalent to replacing carpets with vinyl or wooden floors, in addition, vacu- uming with a poor vacuum cleaner with inadequate suction or leak- ing bags can exacerbate the problem by increasing the quantity of airborne allergen (13).
There are very few controled studies on the effects of special vac- uum cleaners either on symtoms or on allergen levels. However, from talking to patients it is clear that many of them think that water trap, double filter, and high suction vacuum cleaners are effective at reducing the allergen that becomes airborne during cleaning. Although we do not specifically recommend the special vacuum cleaners because of the expense, we do not discourage patients who propose buying them. It is clear that mate allergic pa- tients who do their own cleaning should wear a surgical mask dur- ing cleaning and for 10-I 5 rain afterward. However, most masks
Clinical Reviews in Allergy Volume 6, 1988

Dust Mite 27
are only partially effective because much of the air passes around the sides. Clearly detailed studies are overdue on both the allergen level in carpets and the airborne !evels during vacuum cleaning with different types of vacuum cleaners.
In undisturbed rooms, it is difficult to detect airborne mite aller- gen, even after prolonged sampling. Whole mite bodies and frag- ments of mite can become airborne dur ingbedmaldng and vacuum- ing, but very little allergen is associated with particles that will remain airborne for more than a few minutes (7). For these rea- sons, it is unlikely that air filtration can significantly reduce aller- gen exposure. Bowler et al. (17) were unable to show any additional clinical benefit from combining pre-existing dust control measures with electrostatic and high efficiency particulate air filters. We do not recommend air filtration because the effect on allergen concen- tration cannot be comparable to the effect of removing carpets, covering mattresses, and hot washing of bedding. However, many air filters will remove very small particles and it is possible that at least some of the patients who feel they are helped by air filtration are helped because of a reduced irr i tant effect of small nonallergen- containing particles. Most of the preceding discussion is related specifically to house dust mites. Although many of the conclusions apply generally to other allergens (e.g., removing carpets), the ob- servations on airborne allergens may not be relevant to other allergens. For cat allergen it is clear that the response of asthmatic patients to cat allergen is often very rapid and dramatic, even in the absence of domestic disturbance. In keeping with this finding, there have been measurements showing the presence of small part- icle allergen in the air of undisturbed rooms. Similar results have been found for airborne rat allergen that similarly can cause acute bronchospasm (8). Removing small particles (i.e., <3 mm diameter) from the air requires filtration or removal of the source. Studies to establish that cat allergen can be removed by filtration have not been done yet.
Humidi ty is an important factor for mite growth that remains difficult to control. In houses that do not contain dampness prob- lems result ing from structural flaws such as leakage or ground moisture, the amounts of water vapor in the indoor air is deter- mined by the water vapor content of the outdoor air plus the added household load produced by the inhabitants and their activities~
Clinical Reviews in Allergy Volume 6, 1988

28 Pollart, Chapman, and Platts-Mills
Korsgaard (19) studied a large number of homes during four sea- sons to try to elucidate reasons for the great differences in the con- centration of house dust mites found in different homes. He found that the contribution of household load to indoor air humidi ty var- ied with the season. It is greatest in the colder months when the median frequency of window opening was i h/d, and almost negligi- ble in summer months when the median frequency was 20 h/d. During the winter months, the level of indoor humidity was a well- defined characteristic for each individual home. His studies and numerous previous surveys have confirmed that seasonal varia- tion in indoor air humidity is associated with seasona! variation in the number of house dust mites. He also found that homes with no or only a few mites in winter as a result of low indoor humidi ty con- t inued to have low mite counts in the summer and fall, despite a rise in humidity. He concluded that the wide differences in the occur- rence of house dust mites in a temperate climate is mainly a ques- tion of whether indoor air humidity conditions permit the survival of mite populations in a few critical dry winter months. The level of absolute humidity necessary for mate growth seems to be 8 g/kg; at an absolute humidity of less than 7 g/kg, Korsgaard could find very few mites in mattresses, bedroom floors, and living room floors (i9). In some new homes the winter drying period appeared to be prevented by the use of insulation and sealants (e.g., in passive so- lar houses), which prevents the ventilation that normally occurs through cracks and openings in the house.
At present, it is not clear to what degree these Danish studies ap- ply generally. In the UK, many houses are built of bricks directly onto clay and a major water load comes through the brickwork and may continue year round, in keepingwith tbAs, in many years there is no or very tittle apparent seasonal change either in mite numbers or mite allergen in London. In the US, weather conditions may be extremely variable: In the Southeast, outside absolute humidi ty can vary from 2 g/kg in January and February to 15 g/kg in June and July. Under these conditions, even carpets that have very few mites in the winter can rapidly develop a mite population in the summer. The regular use of humidifiers in the winter mayincrease water load slightly. However, most humidifiers produce less water than a single additional person, and when outside humidi ty is very low, it takes a considerable effort to raise the inside humidi ty to lev-
Clinical Reviews in Allergy Volume 6, I988

Dust Mite 29
els where mites can grow. By contrast, regular air conditioning re- moves large quantities of water from a house during the summer. Studies by Carpenter in Hawaii have established that continuous air conditioning can reduce mite numbers by as much as tenfold (20). Interestingly, the European studies often are expressed as relative humidity (RH) and they record much higher indoor RH in the summer~ However, those figures are exaggerated because houses in Northern Europe often become colder during the sum- mer. Mean summer temperatures of 66~ and mean winter tem- peratures of 70~ are not uncommon. By contrast, the US mean summer temperatures rise to 74~ and may be higher in the ab- sence of effective air conditioning. Under these conditions, changes in RH are blunted and it is almost certainly absolute humidity that is more important. It is also possible that the rise in temperature makes an important contribution to mite growth in the summer. Assuming an indoor temperature of 70~ it's best to advise patients to try to limit summer relative humidity to 50% and not to use the wholehouse humidifiers that can effectively increase humidity in dry periods.
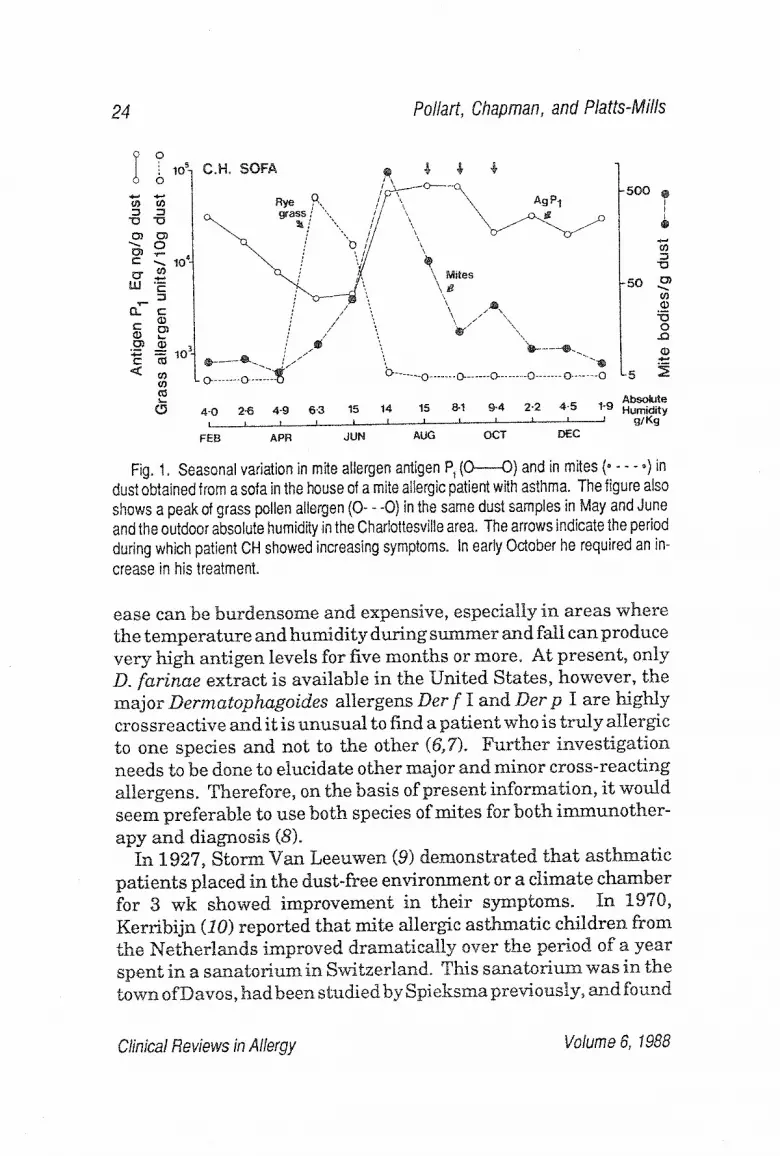
The use of chemical substances for house dust mite removal and prevention of reinfestation would be a useful adjunct to stringent cleaning measures and humidity control. However, most chemi- cals are either ineffective against mites or are too toxic to recom- mend. Numerous acaricides have been looked at in laboratory and clinical settings, including lindane, pirimiphos-methyl, benzyl benzoate, dibutyl phthalate, and diethyl m-toluamid. In Helter- Haupt and Busvine's study (21) of these and seven other com- pounds, l indane was found to be the most potent acaricide, followed by pirin~phos-methyl. Lindane gave the longest period of acarici- dat action in these experiments~ Later work with pirimiphos- methyl by Mitchell et al. (22) showed its acaricidal effects persisted at least 3 wk afLer application (Fig. 2). Whereas lindane's toxicity is well known and would substantially limit its use as a generally recommended acaricide, pirimiphos-methyl has low mammal i an toxicity and appears to be a nonirritant to asthmatic lungs. Since pirimiphos-methyl (or Actelic) is already used in the US as a treat- ment for cockroaches, it is probably also acting as an acaricide in those houses. However, no studies have been carried out to test the acaricidal effect ofpirimiphos-methyi in the form in which it is used
Clinical Reviews in Allergy Volume 6, 1988
30 Pollart, Chapman, and Platts-Mitts 5 0 0 - 4 0 0 -
3 0 0 -
200-
I 0 0 - - - - ~ " Start ing level r l
g Pirimiphos Solvent
~ methyl alone
2 5 - - ~ cerpet 0 ..... 0 ....... O-.,-m.,.~ choir 0 - . ~ - 0
I - I 1 I 0 2 4 6 weeks
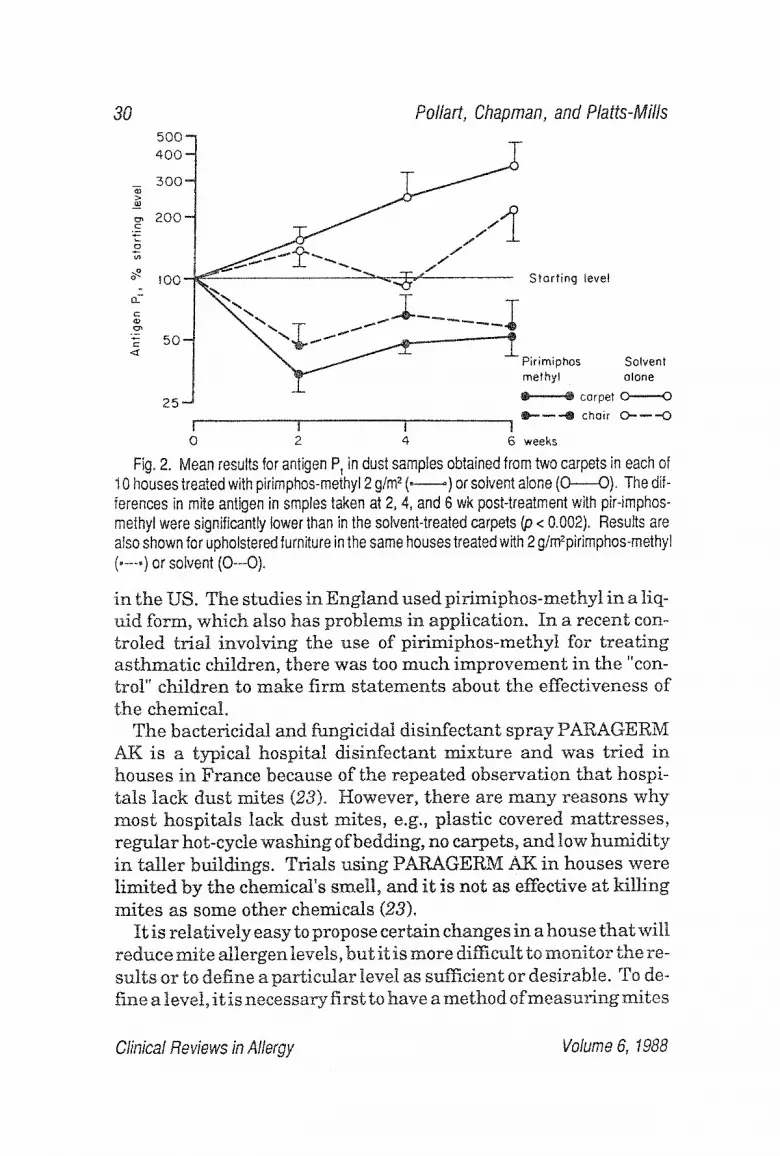
Fig. 2. Mean results for antigen P~ in dust samples obtained from two carpets in each of 10 houses treated with pirimphos-methyl 2 gtm 2 (,---.~) or solvent alone (0----0). The dif- ferences in mite antigen in staples taken at 2, 4, and 6 wk post-treatment with pir-imphos- methyl were significantly lower than in the solvent-treated carpets (p < 0.002). Results are also shown for upholstered furniture in the same houses treated with 2 gtm2pirimphos-m ethyl ( ..... ) or solvent (0--0).
in the US. The studies in England used pirimiphos-methyl in a liq- uid form, which also has problems in application. In a recent con- troled trial involving the use of pirimiphos-methyt for treating asthmatic children, there was too much improvement in the "con- trol" children to make firm statements about the effectiveness of the chemical.
The bactericidal and fungicidal disinfectant spray PARAGERM AK is a typical hospital disinfectant mixture and was tried in houses in France because of the repeated observation that hospi- tals tack dust mites (23). However, there are many reasons why most hospitals lack dust mites, e.g, plastic covered mattresses, regular hot-cycle washing of bedding, no carpets, and low humidi ty in taller buildings. Trials using PARAGERM AK in houses were limited by the chemical's smell, and it is not as effective at killing mites as some other chemicals (23).
It is relatively easy to propose certain changes in a house that will reduce mite allergen levels, but it is more difficult to monitor the re- sults or to define a particular level as sufficient or desirable. To de- fine a level, it is necessary first to have a method of measuring mites
Clinical Reviews in Aflergy Volume 6, 1988
Dust Mite 31
or mite allergen that is truly reproducible. Most studies in the past have been carried out using mite counts. In two studies, it was pos- sible to suggest that a given mite content was a risk factor for asthma. In Papua, New Guinea, blankets with a mean level of1380 mites/g of dust were associated with an "epidemic" of asthma (24). In Denmark, it was proposed that an absolute indoor humidity level of 8 g/kg and a mite count of more than 100 mites/g of fine dust should be regarded as risk factors for developing asthma (25). However, counting mites requires microscopic examination and is both slow and very difficult to standardize. We have used measure- ments of antigen Derp I in ~g/g of dust (6,8,13,27). Based on these measurements, we have proposed that levels >I0 pg/g of dust often are associated with symptoms, whereas levels less than I gg/g ap- pear to be "safe." These levels cannot be translated directly into mite counts, but 10 ~g/gDerp I is approximately equivalent to 200 mites/gs of dust (8,26)~ Obviously, no specific level of mite allergen canbe regarded as a threshold for causing symptoms. Nonetheless, we believe that it could be very useful to define standards of mite allergen in houses that should be regarded as significant for mite allergic patients. Whether itis also possible to define a level of mite allergen in house dust that will lead to anincreased number of indi- viduals becoming allergic is a more difficult question. If, as seems likely, sensitization takes a prolonged period of time, one would need to know whether the mean level or peak levels were impor- tant. In a prospective cohort study in England, in which mite al- lergen levels were sampled only once, an increased incidence of positive skin tests and IgE ab to mites was found in young children whose houses contained >5 ~g Der p I/g of dust (27). If measure- ments of mite allergen were to be used widely, it would be necessary to have simple accurate assays. Recent developments with mono- clona] antibodies to mite allergens appear to offer a way of devel- oping rapid, cheap, and accurate assays (28) (Chapman, M. D., Heymann, P. W., Wilkins, S. R., Brown, M. J., and Platts-Mills, T. A. E., manuscript submitted for publication).
CONCLUSION
The available methods for controling dust mites in houses consist of washing bedding regularly-, covering mattresses, and, when pos-
Clinical Reviews in Allergy Volume 6, 1988

32 Pollart, Chapman, and Platts-Mills
sible, removing carpets. This leaves the problem of f i t ted carpets in living rooms, as welt as the problem of sofa and chair upholster- ies. These can be improved by vacuum cleaning, controling humid- ity, and perhaps using certain acaricides. However, there is no per- fect regime and very inadequate da ta on the resul ts of different measures . Control of other allergens in house dust requires intel- l igent observation and persistence~ Cat allergen m a y t ake months to remove. Fungal allergens are still poorly defined, bu t can be helped by cleaning measures , reducing humidity, and removing plants. Pollen can definitely enter house dus t in significant quan- tities and it m a y be impor tan t to encourage a i r conditioning during the pollen seasons to reduce this. Although cockroaches are almost certainly an impor tan t cause of as thma, very little is known about the factors tha t influence the quanti t ies of cockroach al lergens in houses.
Pe rhaps the most impor tan t conclusion is t h a t mite and other foreign proteins present in house dust are responsible for a large number of cases of respira tory disease and tha t the methods neces- sary for controling these proteins need to be t aken more seriously.
ACKNOWLEDGMENTS
This work was supported N tH Gran t AI20565-03. Figure 2 is repr in ted w i t h permiss ion of the authors of Cl in icalAl lergy (1, 235, 1985) (22). We are grateful to Nancy Malone for p repar ing the manuscr ip t .
REFERENCES
1. Voorhorst, R., Spieksma, F. T. H., and Varekamp, H. (1969), House Dust Atopy and the House Dust Mite, Stafleu's Scientific Publishing Co., Leiden, The Netherlands.
2. Miyamoto, T., Oshima, S., and Ishizaki, T. (1969), J. Allergy 44, 282. 3. Smith, J. M., Disney, M. E., Williams, J. D., and Goels, Z. A. (1969), Br.
Med. J. 2, 723. 4. Murray, A. B. and Zuk P. (1979), J. Allergy Clin. Immunol. 64, 266-269. 5. Arlian, L. G., Bernstein, I. L., and Gallegher, J. S. (1982), J. Allergy Clin.
Immunol. 69, 527. 6. Heymann, P. W., Chapman, M. D., and Platts-Mills, T. A. E., J. Immunot.,
(in press). 7. Heymann, P. W., Chapman, M. D., and P]atts-Mills, T. A. E. (1919), J.
Allergy Clin. tmmunol. 77~ 129.
Clinical Reviews in Allergy Volume 6, 1988
Dust Mite 33
8. Smith, T. F., Kelly, L. B., Heymann, P. W., Wilkens, S. R., and Platts-Mills, T. Ao E. (1985), J. Clin. Immunol. 7G 782-788.
9. Storm Van Leeuwen, W. (1927), Br. Med. J. ii, 344-347. 10. Kerrebjin, K.. (1970), Bronchitis III, van der Lende, R. (ed.) The Nether-
lands, Royal Vangorcum, pp. 38-48. 1I. Plaits-Mills, T. A. E., Tovey, E. R., Mitchell, E. B., Mozarro, N., Nock, P.,
and Wilkins, S. R. (1982), Lancet ii, 675-678. 12. Carswell, F., Robinson, D. W., Oliver, J., Clark, J., Robinson, P., and
Wadsworth, J. (1982),Clin. Allergy 12, 533--545. 13. Tovey, E. R., Chapman, M. D.,Wells, C. W, and Platts-Mills, T. A. E. (1981),
Am. Rev. Respir. Dis. 124, 630--635. 14. Burr, U. L., Dean, B. V., Herbet, T. G., Neale, E., and Verrer-Jones, E. R.
(1980),Thorax 35, 506-512. t5. Murray, A. B. and Ferguson, A. C. (1983), Pediatrics 71, 418-422. 16. Sarsfield, J. K., Garland, G., Toy, R., and Norman, A. L. E. (1974), Arch. Dis.
Childhood 49, 716-721. 17. Bowler, S. D., Mitchell, C. A., and Miles, J. (1985), Annals Allergy 55, 498-
500. 18. Platts-Mills, T. A. E., Longbottom, J. L., and Wilkin s, S. R., J. Allergy Clin.
Immunol., (in press). 19. Korsgaard, J. (1983), Allergy 38, 85-92~ 20. Carpenter, M. D., Win, G. H., Furumizo, R. T., Massey, D. G., and Ortiz, A.
A~ (1985), J. Allergy Clin. Immunol. 75, 121. 21. Heller-Haupt, A. and Busvine, J. R. (1974), J. Med. Entomol 2, 551-558. 22. Mitchell, E. B, Wilkins, S. R., Deighton, J. M., and Platts-Mills, T. A. E.
(1985), Clin. Allergy 15,235-240. 23. Penaud, A~, Nourrit, J., Autran, P., Timon-David, P., Jocquet-Francillon,
M., and Charpin, J. (1975), Clin. Allergy 5~ 109-114. 24. Dowse, G. K., Turner, K_ J., Stewart, G. A., Alpers, M. P., and Woolcock, A.
J. (1985), J. Allergy Clin. ImmunoL 75, 75. 25. Korsgaard, J. (1983), Am. Rev. Respir. Dis. 128, 231. 26. Platts-Mills,T. A. E., Chapman, M. D., Heymann, P. W., Hayden, M. L., and
Wilkins, S. R. (1986), J. Allergy Clin. Immunol. 78, 398. 27~ Rowntree, S., Cogswell, J. J., Ptatts-Mills, T. A. E., and Mitchell, E. B.
(1985), Arch. Dis. Child. 60, 727. 28. Chapman, M. D., Sutherland, W. M., and Platts-Mills, T. A. E. (1984), J.
immunol. 133, 2488.
Cfinical Reviews in Allergy Volume 6, t988
Related Documents











