24 Hour Stroke Window for Non‐ EVT Hospitals 12 TH ANNUAL STATEWIDE STROKE CONFERENCE CHARLES H. MORGAN, M.D.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

24 Hour Stroke Window for Non‐EVT Hospitals12TH ANNUAL STATEWIDE STROKE CONFERENCE
CHARLES H. MORGAN, M.D.

The 4 Eras1. Pre‐1996 Era
2. The TPA Era (1996 forward)
3. The Stent‐Retriever 6‐6‐6 Era (February, 2015 forward)
4. The 24‐hour Window Era (January 2018, forward)

The 4 decision points in your ED#1 >24 hours They need pre‐1996 care
#2 Less than 4 1/2 hours, TPA eligible ‐no large vessel occlusion(LVO)
They need IV TPA(1996 care)
#3 Less than 4 ½ hours, TPA eligible‐ evidence for LVO. They need IV TPA AND immediate evaluation for possible EVT With CTA with Perfusion CT or ASPECTS.(2015 care) immediate transfer if candidate
#4 More than 4 1/2 hours but less than 24 hours they need immediate CTA and ASPECTS or Rapid CT . If LVO found and ASPECTS >6 or Rapid CT shows adequate penumbra they need EVT

The 4 options for your hospital administration/radiology service /ED providers#1 Ignore it , and hope nothing bad happens
#2 Punt
#3 Become an EVT capable center
#4 Become an active part of a STROKE SYSTEM OF CARE

Mechanical Clot Retrieval Has Been A Decade‐Long GoalIn January 2014 the results of 3 Prospective randomized international trials were reported at the international stroke conference they included
The completion trial
MR rescue
IMS III
All of us in vascular neurology looked forward to these being positive trials to show that intra‐arterial clot removal was effective


At that point the only approved treatment for acute ischemic CVA in the United States was T.P.A. although many centers were doing intra‐arterial clot retrieval.
The concept of “Stroke Systems of Care” was mostly academic.Our goal was:◦Rapid diagnosis with non‐contrast CT◦ IV T.P.A.
and that could be accomplished at most hospitals in the U.S.A.

IT WAS ALL ABOUT TIME

Target Stroke Honor Roll<60 minutes >50% of the time

Target Stroke Elite PlusNew “Gold standard” was door to drug <45 minutes
>50% of the time

ISMC has achieved “Elite Plus”

The stroke world changed February 2015 in the auditorium of
the convention center in Nashville, Tennessee with 4
important reports.



In my 44 years of medical practice, this was the first time I ever saw a medical audience give a standing ovation to a scientific presentation.
Two thousand neurologists, standing, cheering, many with tears in their eyes.
Think of it as about as big a deal as the polio vaccine.

Now several important subsets of strokes could be treated and be much more likely to be independent, work, teach Sunday School, take of their family, instead of family taking care of them.

SubsetsThe treatment window went to six hours
Patients who were excluded from IV T.P.A. (i.e., on anticoagulation, recent surgeries) were now eligible

Problem:

What to do if you were not at St. John, St. Francis, Hillcrest, Mercy , IBMC or OUHSC?
It Was About Time, but Tissue Became Important

“door to needle” became “needle to door”At ISMC and other busy hospitals and emergency rooms without EVT(endovascular therapy)the challenge became
(1) make a rapid triage decision whether the patient in your emergency department was a candidate for intravenous TPA, if so get them immediately to CT, if no blood start IV TPA obtain a CTA and if we see a proximal large vessel occlusion of the internal carotid, middle cerebral, or basilar transport to an EVT capable Center with TPA running
(2) if the patient was not an IV TPA candidate but in the “666“ criteria obtain a CTA and if you find a proximal large vessel occlusion transport to the EVT capable Center

Endovascular Therapy Guidelines for AIS666
Age: > 18
Pre‐Stroke mRS of 0‐1
NIHSS score > 6
ASPECTS > 6
Needle poised above groin by 6 hours
Large artery occlusion on CTA◦ Distal ICA◦ Proximal MCA◦ Vertebral/Basilar



Then January 2018 happenedDEFUSE III was presented at the international stroke conference in Los Angeles it provided convincing evidence that the window for EVT could be extended up to 16 hours using perfusion imaging with CT to screen for patients who have a salvageable penumbra compared to the unsalvageable core of the infarct. For DEFUSE III that ratio had to be 1.7.
That trial followed the report of the DAWN trial from 2017. Because DEFUSE III was the second prospective randomized trial with blinded raters showing very similar outcomes the American Heart Association (AHA) American Stroke Association (ASA) and American Academy of Neurological Surgeons (AANS) published major changes in the recommendation for treatment of acute ischemic stroke.




Because of January 2018. . .This amazing breakthrough in the treatment of stroke clearly demarcates hospitals into 2 separate categories:◦ Endovascular Therapy (EVT) capable hospitals◦ Non‐EVT capable hospitals (this includes my hospital and your hospital)

Protocol from DAWN and DEFUSE IIIThe protocol called for CTA, looking for a proximal occlusion of internal carotid, the first segment of the middle cerebral (M1) or the second segment ( M2),
Both protocols required a diffusion/perfusion mismatch, both protocols utilized either MRI or CT (RapidCT)
45% of patients evaluated had the perfusion mismatch
Patients that had the perfusion mismatch were randomized 1 to 1 to either clot retrieval with the stent retriever or standard medical therapy with aspirin, statins, blood pressure monitor

OutcomesPatients who were candidates and had stent retriever treatment (EVT) in the 6‐24 hour window had the following outcomes:◦ 50% achieved a modified Rankin scale 2 (mR2) at 90 days versus 13% who were randomized to treatment by current guidelines for medical therapy at some of the most accomplished medical centers in the world
◦ 14% of the EVT group had combined outcome of death/symptomatic intracerebral hemorrhage leading to a modified Rankin scale of 4 or 5 (mR4 or mR5) compared to 26% in the current guidelines medical therapy group.

ProtocolIn the DIFUSE III trail “wake up” strokes were 50% of the cases, known last seen well (LSW) greater than 6 hours were 50% of the cases.
In the LSW>6 hour group, the median time from LSW to randomization was 11 hours.
The procedure takes some time. Imaging to reperfusion averaged approximately 90 minutes, even in these very experienced centers.

OutcomesThe odds ratio of a favorable outcome with stent retriever therapy (EVT) compared to treatment by current guidelines was an astonishing 3.4
The p Value of this study was 0.0001
The number needed to treat (NNT) to save a brain was an astonishing 2
Compare this with the NNT of 9 for intravenous alteplase (IV TPA) for ischemic stroke and an NNT of 6 for carotid endarterectomy for symptomatic carotid stenosis>70%,and an NNT of 4 for CABG for Left Main coronary artery stenosis

This mandates change in the triage and transport protocol in the field as well as at your and my ED.

Pre‐Hospital Care1. The EMT professional should do a screen for a LVO (large vessel occlusion). There are several available. The two most commonly used include FAST‐ED and VAN. All 6 of the EVT capable stroke centers in this state recommend using VAN.

VANKathy Stilwell, Neurovascular R.N.(NVRN)
Stroke Coordinator, ISMC
Best Mom on Earth and Great Teacher

Options if you are a non EVT hospital(1) Ignore it ,hope nothing bad happens.

The problems with ignoring it:You live there.
Your spouse/significant other lives there.
Your family, neighbors, friends, co‐workers ,parents , church family , dentist, veterinarian, newspaper publisher , and plaintiff attorneys live there.
Strokes are very common, the above groups will be experiencing strokes in the coming months/years.
They will all expect you to provide the standard of care. They all read,(WSJ) (Washington Post) , watch the news on television( NBC) and all have access to the internet (ask your children to Google “stroke treatment”)

A 2nd option “PUNT”Contact your EMS provider(s) and tell them you are not capable of treating LVO strokes,
Have ongoing CME training for EMS in your hospital/community teaching the VAN , and NIH stroke scale. Reinforce the protocol of bypassing your hospital unless the Pt is VAN negative or outside of the 24 hour window
Actively reach out to your community to inform them that you are not the place to go with stroke signs. I.E. Give an interview with the local newspaper, offer to put on a presentation to local civic organizations

3rd OptionA few of the larger community hospitals may be able to put together the resources to become an “EVT capable primary stroke center ” and serve as a regional hub.

Stroke “systems of care” are now essentialIf a patient in the United States has an acute ischemic stroke with unknown time of onset, or if patient wakes up in the morning with stroke signs, or if the patient was witnessed to have the abrupt onset of stroke and it is within the timeframe to be able to get them to an EVT capable Center within 24 hours they need to be evaluated for potential EVT whether they are living in Elk City, Oklahoma, or Oklahoma City.
This is the new standard of care for Oklahoma, and the United States

An option for you if you decide not to ignore it, punt, or become EVT capableThe essential modifications to be in an integrated stroke system of care require
(1)24 hour coverage in your ED capable of working thru the many possible scenarios that will present. Telestroke can help achieve this.
(2) 24 hour CT scan capability , including CTA .The door to CT completed goal is 20 minutes .Teleradiology can help achieve this. Your CT technician must send the axial source images to the radiologist without taking the time to reformat the images
(3) Although not absolutely essential having Rapid CT perfusion imaging is extraordinarily helpful to you , your patient’s families and your hospital bottom line
(4) An EVT capable hospital that you can count on to talk to you when you call

YOUR ED in an integrated Stroke System of CareIf the patent is within the 4½ hour window the protocol remains the same as it is currently with two exceptions:
1. If the CT shows no bleed and no well‐defined low density area, you should be giving the TPA on the CT table,
2. With TPA running, you should get a CTA and the CT technician should forward the axial images without reformatting to the Radiologist during the daytime hours and during the nighttime hours to“ Night Rays” and/or the Neurologist on call for the Stroke System of Care
If a LVO is seen the ED physician should immediately call the transport center for bed availability at whatever EVT center you are connected with. If “yes”, the transfer center should immediately connect the ED physician with neuro‐intervention. If no bed available immediately call an alternative center
Telestroke can be very helpful here

YOUR EDIf the patient arrives at your ED outside of the 4½ hour window, but within the 24 hour window, the patient should be taken immediately for non‐contrast CT of the head.
If:◦ 1. There is no blood on CT, and◦ 2. No well‐developed low density area, and◦ 3. ASPECTS is 6 or higher, then◦ A CTA should be done immediately as in the protocol on the previous slide.

Case #168 y/o male presented by private vehicle 11/8/16 to Non‐EVT Hospital ED with ◦ Chief complaint: Frequent falls◦ He gave a 2 day hx of unexpected falls. He described it as “My legs just get weak.”
◦ Also complained of intermittent LEFT UE vague weakness and numbness lasting minutes associated with the falls.

Case #1 cont..PMH‐ HTN, DM type IIMeds‐Metoprolol, MetforminNKDA

Case #1 cont..Initial neurologic exam completely WNL
BP 190/90 Orthostatic vital signs repeated x 2, no significant orthostasis
Initial plan was MRI brain and C spine, do not try to lower B.P., give ASA per rectum

Case #1 cont..Within minutes after neuro exam patient got up to go to restroom and had abrupt onset dense LEFT Hemiparesis, severe dysarthria, LEFT central 7th, RIGHT gaze preference, associated with mild HA headache
BAT called by RN within seconds of clinical change
NIHSS 10

Case #1 cont…With good evidence for brief recurrent symptoms the last several days, complete recovery by the time he had the neurological exam ,now with dense L hemiparesis with (important) finding of R gaze, What is the most likely diagnosis?(a) ischemic stroke with critical stenosis in R carotid distribution(b) focal seizure with Todd’s paralysis(c) conversion disorder(d) aneurysmal rupture R hemisphere(e) either (a) or (d) I can’t tell and we need to know

Is this Patient VAN positive? YES/NO
What do you do now?
(a)STAT CT Scan without contrast if no bleeding give 0.9 mg/kg %10 in first minute, the rest over the following 59 minutes then CTA with TPA running(b)STAT CT Scan with CTA wait for radiology to call back(c) Immediate full anticoagulation(d) MRI of brain


What do you do next?A. Give anticoagulant dose of heparin/LMWH?B. Give ASA per rectum?C. Get MRI?D. Give alteplase 0.9mg/kg %10 in first minute, remaining
over next 59 minutes and get CTA head and neck with TPA going
E. Get CTA Head and Neck wait for results to treat?

Recommendation
Recommendation was Alteplase and immediate CTA Head and Neck with TPA running

CTA head and neck

Case #1 cont..Patient transferred urgently to IBMC after consultation with Neurointerventional radiology.
Seen at IBMC by Manuel Fortes MD
NIHSS 10
ASPECTS 10

Thrombus
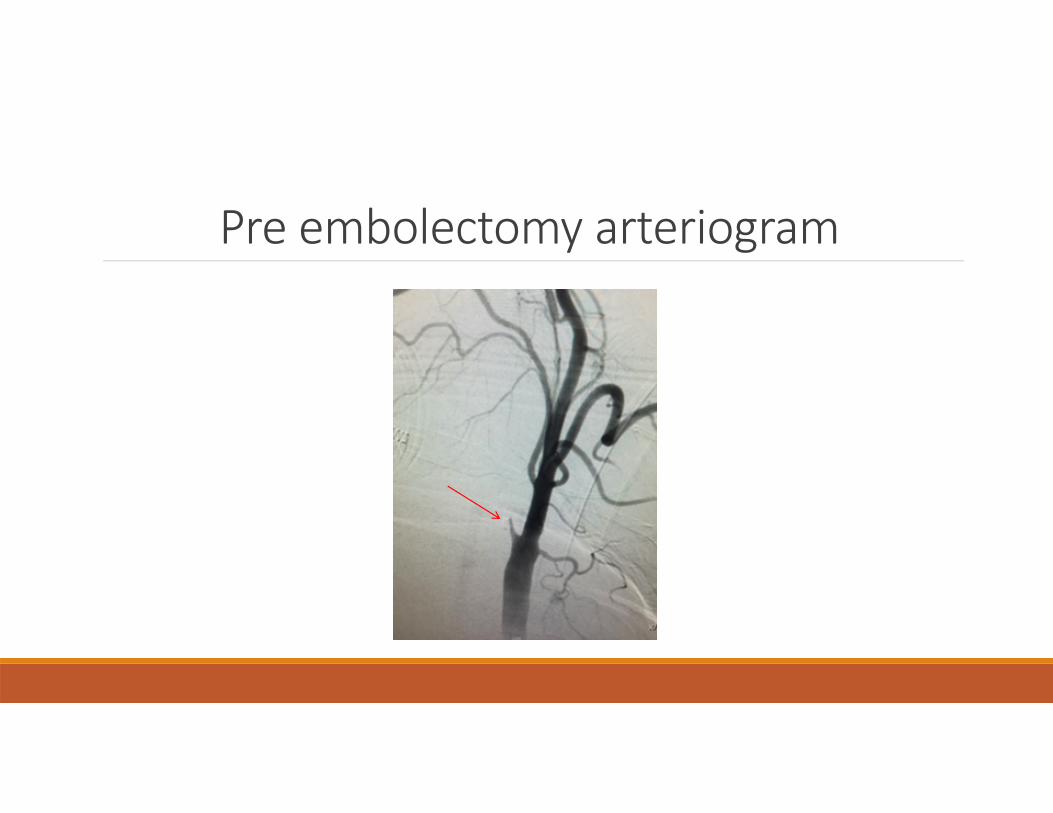
Pre embolectomy arteriogram

Post embolectomy arteriogram

Case #1 cont..ONE DAY POST EMBOLECTOMY, NIHSS 1
ONE WEEK POST EMBOLECTOMY, NIHSS 0
HAD UNEVENTFUL RIGHT CEA AT IBMC 3 DAYS LATER

Case #277 y/o male seen as telestroke consult in far NE OK.
Reliable witness reports abrupt onset 45 minutes prior to arrival in ED, fell to ground , LEFT hemiparesis, dysarthria, LEFT visual field loss, confusion. Unable to follow commands or answer questions.
NIHSS 17
ASPECTS 8

Case #2 cont..Recently dx with DVT now on Eliquis, took his dose earlier today.
IS this Pt VAN + Y/N
Is he an IV tPA candidate ? Y/N
Would he be an IV tPA candidate if he had been on DVT prevention doses of LMW Heparin? Y/N
Recommendation is urgent CTA head and neck.

Case #2 cont..Recently dx with DVT now on Eliquis, took his dose earlier today.
IS this Pt VAN + Y/N
Is he an IV tPA candidate ? Y/N
Would he be an IV tPA candidate if he had been on DVT prevention doses of LMW Heparin? Y/N
Recommendation is urgent CTA head and neck.
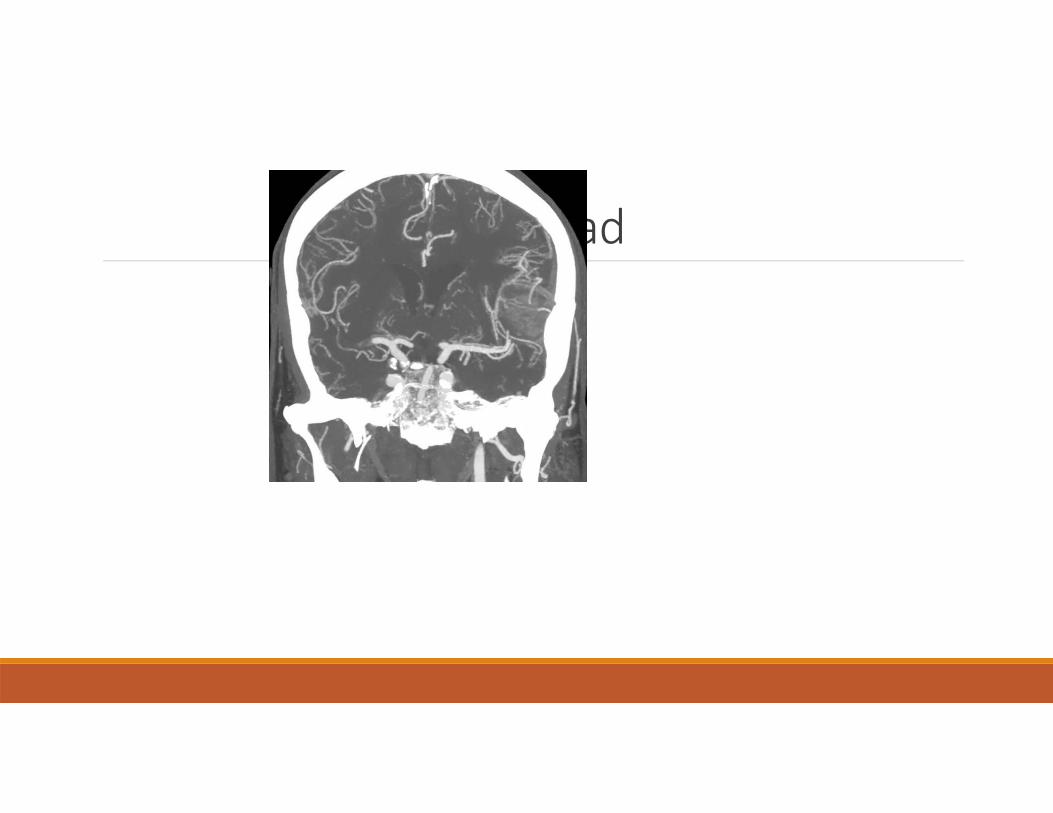
CTA head

Case #2 cont..Transfer Center contacted
Due to time required for ground transport to IBMC and severe weather in area; Transfer center connected ED physician with St Johns in Tulsa OK.

Case #2 cont..Clot retrieval accomplished at 5 ½ hours after onsetPost retrieval NIHSS 7

Same case except it is now post Jan 2018,and he arrives at 4 ¼ hoursWhat do you do?
(ANSWER‐IT DEPENDS on your capability)

Case #385 y/o female seen in ED of spoke hospital
Sudden onset LEFT hemiparesis witnessed by spouse. In ER well within the time frame to consider tPA.

CT

Case #3 cont..PMH‐ Atrial fibrillation. Had been on warfarin but it had to be DC’d two weeks prior due to significant GI bleeding.
HgB 5.4 at that time; transfused with 5 units, HgB now 8.4
Hemeoccult positive stools earlier in this week
Hx of Ulcerative Colitis
Therefore not an IV tPA candidate

Case #3 cont.Creatinine 2.3, was 2.1 two weeks prior
MRI‐MRA available “tomorrow”

Case #3 cont..NIHSS 13
ASPECTS 10

What do you do next?Review risk/benefits of CTA with patient and wife, do immediate CTA?
Give antiplatelet therapy and H2 Blockers?


Case #3 cont..Creatinine 2.3, was 2.1 two weeks prior
Risks/benefits of CTA discussed with patient and wife, CTA done urgently and reveals RIGHT M1 occlusion.

Case #3 cont..Transfer center contacted No ICU beds at IBMC
Transfer center put ED physician in contact with OUHSC
Transferred for possible endovascular clot retrieval
Clot retrieval accomplished
NIHSS 18
Post retrieval NIH 7
Related Documents











