Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hormonal Manipulations in CRPC
NW Clarke
Professor of Urological Oncology
Manchester UK

C
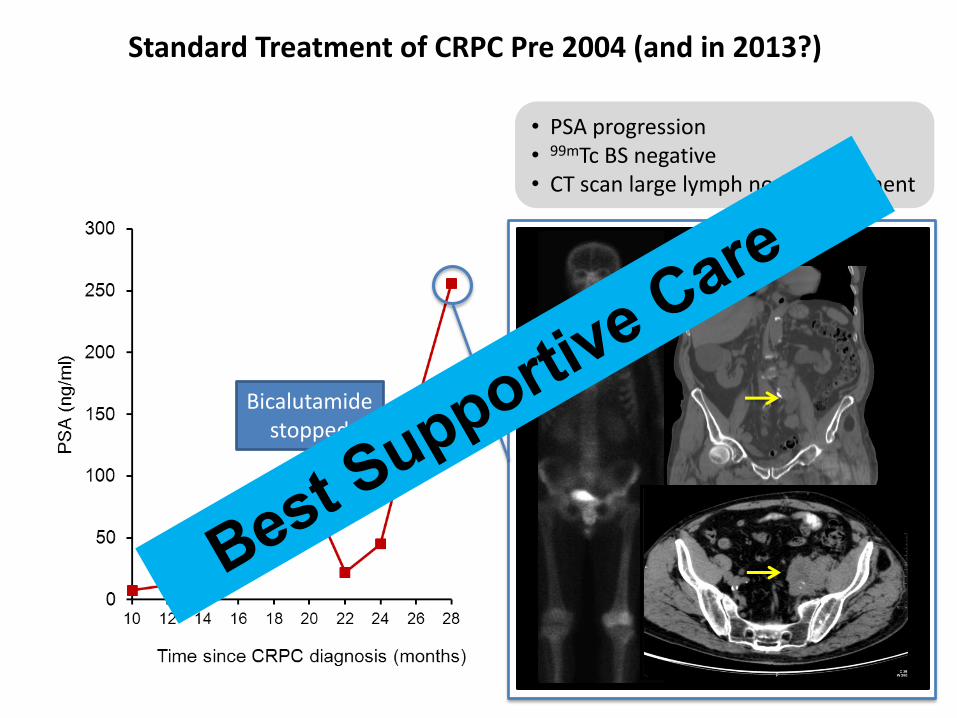
Standard Treatment of CRPC Pre 2004 (and in 2013?)
• PSA progression • 99mTc BS negative • CT scan large lymph node component
Bicalutamide stopped
C
Standard Treatment of CRPC Pre 2004 (and in 2013?)
• PSA progression • 99mTc BS negative • CT scan large lymph node component
Bicalutamide stopped
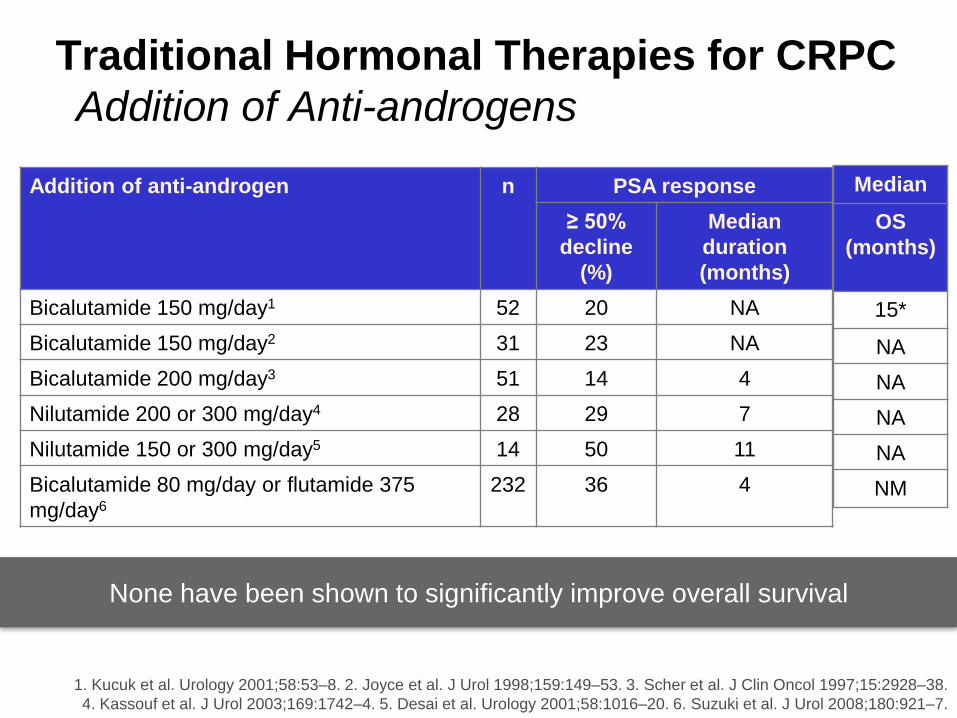
Traditional Hormonal Therapies for CRPC
Addition of Anti-androgens
Addition of anti-androgen n PSA response
≥ 50%
decline
(%)
Median
duration
(months)
Bicalutamide 150 mg/day1 52 20 NA
Bicalutamide 150 mg/day2 31 23 NA
Bicalutamide 200 mg/day3 51 14 4
Nilutamide 200 or 300 mg/day4 28 29 7
Nilutamide 150 or 300 mg/day5 14 50 11
Bicalutamide 80 mg/day or flutamide 375
mg/day6
232 36 4
1. Kucuk et al. Urology 2001;58:53–8. 2. Joyce et al. J Urol 1998;159:149–53. 3. Scher et al. J Clin Oncol 1997;15:2928–38.
4. Kassouf et al. J Urol 2003;169:1742–4. 5. Desai et al. Urology 2001;58:1016–20. 6. Suzuki et al. J Urol 2008;180:921–7.
Median
OS
(months)
15*
NA
NA
NA
NA
NM
None have been shown to significantly improve overall survival

Traditional Hormonal Therapies for CRPC
Corticosteroids / oestrogens
Kelly et al. J Clin Oncol 1995;. Kantoff J Clin Oncol 1999; Tannock . J Clin Oncol 1996. Sternberg et al. Oncology 2005
Venkitaraman et al. BJU Int 2007 Smith. Urology 1998
7. Oh et al. J Clin Oncol 2004. Dawson et al. Cancer 2000.
Corticosteroids n PSA response
≥ 50%
decline
(%)
Median duration
(months)
Hydrocortisone 40 mg/day1 30 20 4
Hydrocortisone 40 mg/day2 123 22 2
Prednisone 10 mg/day3 81 22 4
Prednisone 20 mg/day4 50 9 3
Dexamethasone (0.5 mg/day)5 102 49 7
Oestrogens
DES 1 mg/day6 21 43 NA
DES 3 mg/day7 44 24 4
Transdermal oestradiol 0.6 mg/day8 24 13 3
Median
OS
(months)
NA
12.6*
NM*
11.9*
NA
NM†
NA
NA
None have been shown to improve overall survival significantly

N=270
CV Event Rate 20%
TTP for DAiS (8.6 months) was
significantly longer DA (4.5
months p<0,001)

Lancet Oncology Vol 14 April 2013

Evolving treatment in CRPC
Hormone
therapy
PLUS supportive care
(e.g. denosumab/bisphosphonates/β-emitters)
Docetaxel
Sipuleucel-T Abiraterone
Enzalutamide
Approved for use by FDA/EMA
Approved for use by FDA
mCRPC
post-chemo
Cabazitaxel
Radium 223
Abiraterone
Positive Phase III data
mCRPC
symptomatic
pre-chemo
Chemo
mCRPC
mildly
symptomatic
disease
mCRPC
asymptomatic
disease
(failed ADT)
Hormone
sensitive

mCRPC
post-chemo
Ongoing Phase III Trials in Metastatic CRPC
mCRPC
symptomatic
pre-chemo
Cabozantinib vs.
prednisone (COMET-1)†
Cabozantinib vs.
mitoxantrone +
prednisone (COMET-2)†
Cabazitaxel vs.
Docetaxel (FIRSTANA)
Cabazitaxel 20 mg/m²
vs. 25 mg/m²
(PROSELICA)
Dasatinib vs. placebo
(+ docetaxel, both arms)
(READY*)
Enzalutamide vs.
placebo (PREVAIL)
Ipilimumab vs. placebo
PROSTVAC-V/F ±
GM-CSF vs. placebo
(PROSPECT)
Tasquinimod vs.
placebo
Ipilimumab vs. placebo
following RT
Chemo
Orteronel vs. placebo
Custirsen ± docetaxel +
prednisone (SYNERGY)
Orteronel vs. placebo
Mildly
symptomatic
mCRPC
Asymptomatic
mCRPC
(failed ADT)
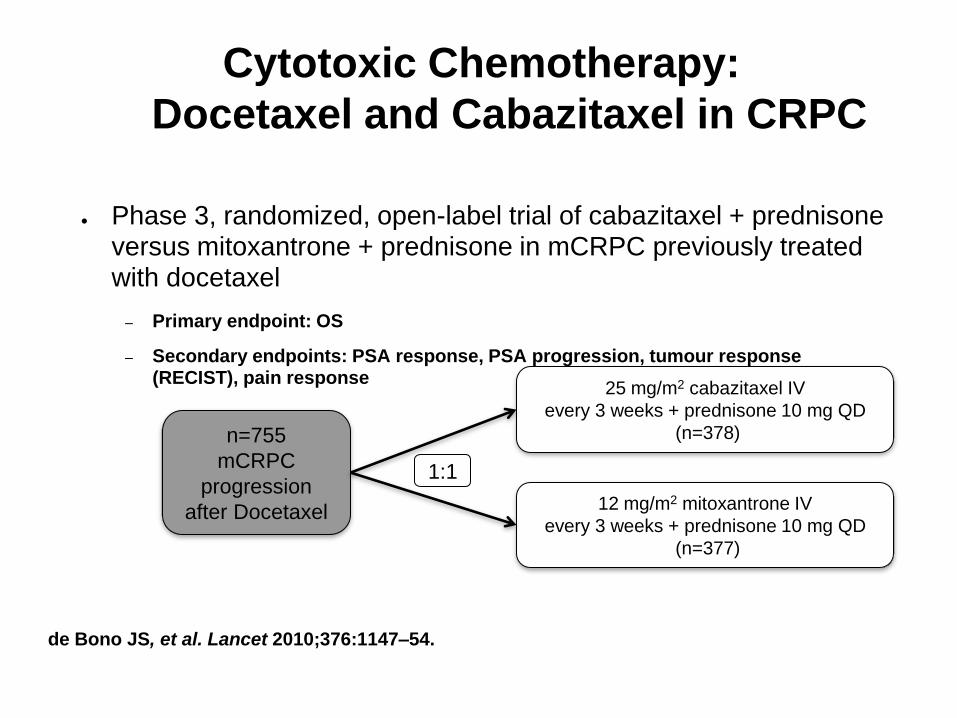
Cytotoxic Chemotherapy:
Docetaxel and Cabazitaxel in CRPC
● Phase 3, randomized, open-label trial of cabazitaxel + prednisone versus mitoxantrone + prednisone in mCRPC previously treated with docetaxel
– Primary endpoint: OS
– Secondary endpoints: PSA response, PSA progression, tumour response (RECIST), pain response
de Bono JS, et al. Lancet 2010;376:1147–54.
n=755
mCRPC
progression
after Docetaxel
25 mg/m2 cabazitaxel IV
every 3 weeks + prednisone 10 mg QD
(n=378)
12 mg/m2 mitoxantrone IV
every 3 weeks + prednisone 10 mg QD
(n=377)
1:1

• Docetaxel is initiated: 8 cycles 75 mg/m2 + prednisone 5 mg bid • Response after 6 cycles: PSA 256 to 162 ng/mL, small decrease on LN
8 cycles of docetaxel 75 mg/m2
Standard Treatment of CRPC Post 2005 ( ? in 2013)

Multiple lymph nodes metastases
99mTC BS
Docetaxel
• Treatment with docetaxel is stopped after 9 cycles due to PSA progression, Grade 3 fatigue and multiple lymph node metastases
• This was followed by a more rapid PSA progression
Standard Treatment of CRPC Post 2005

Multiple lymph nodes metastases
99mTC BS
Docetaxel
• Treatment with docetaxel is stopped after 9 cycles due to PSA progression, Grade 3 fatigue and multiple lymph node metastases
• This was followed by a more rapid PSA progression
Standard Treatment of CRPC Post 2005

Novel Androgenic Approaches in CRPC
Nucleus Cytoplasm
Transcription Nuclear
localisation
Ligand-dependent
1
Alternate
ligands
2
Ligand-independent
AR splice
variants
7
Coactivators
Corepressors
5
6
Receptor tyrosine
kinase
4 Ligand-independent
activation of AR
ACTH LH
LHRH agonists
Androstenedione
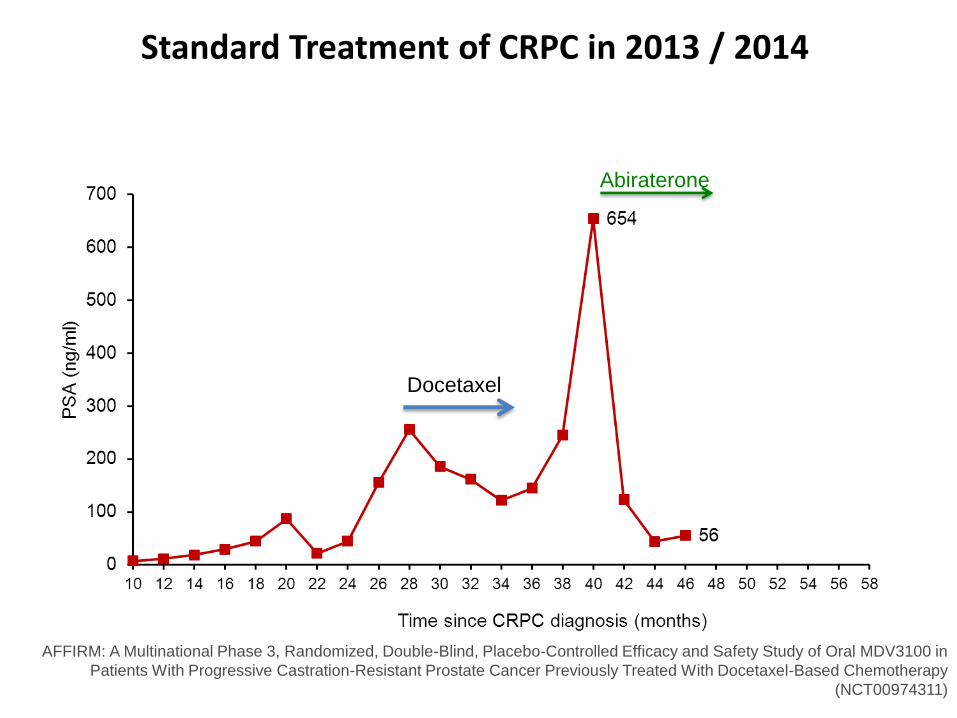
AFFIRM: A Multinational Phase 3, Randomized, Double-Blind, Placebo-Controlled Efficacy and Safety Study of Oral MDV3100 in
Patients With Progressive Castration-Resistant Prostate Cancer Previously Treated With Docetaxel-Based Chemotherapy
(NCT00974311)
Docetaxel
Abiraterone
Standard Treatment of CRPC in 2013 / 2014

Docetaxel
• PSA progression • Patient asymptomatic • Hb 10.5 mg/dL from 12.5 mg/dL
Abiraterone
Standard Treatment of CRPC in 2013 / 2014

Docetaxel
• PSA progression • Patient is now moderately symptomatic in cervical spine
(treated by paracetamol and piroxicam) • Hb 10.5 mg/dL from 12.5 mg/dL
Standard Treatment of CRPC in 2013 / 2014
Abiraterone
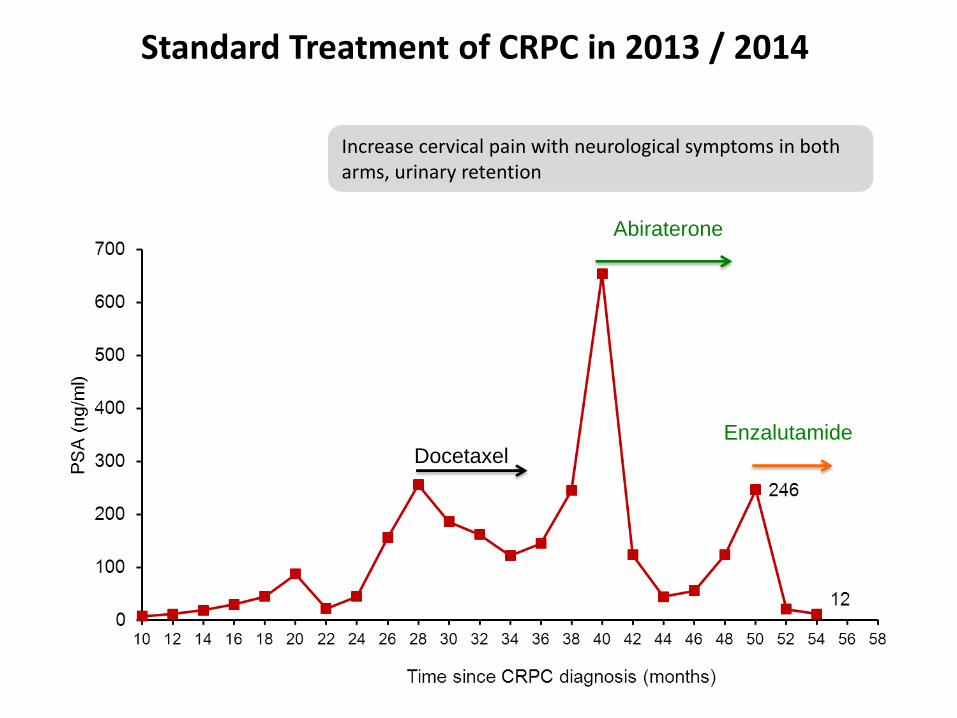
Docetaxel
Increase cervical pain with neurological symptoms in both arms, urinary retention
Abiraterone
Enzalutamide
Standard Treatment of CRPC in 2013 / 2014
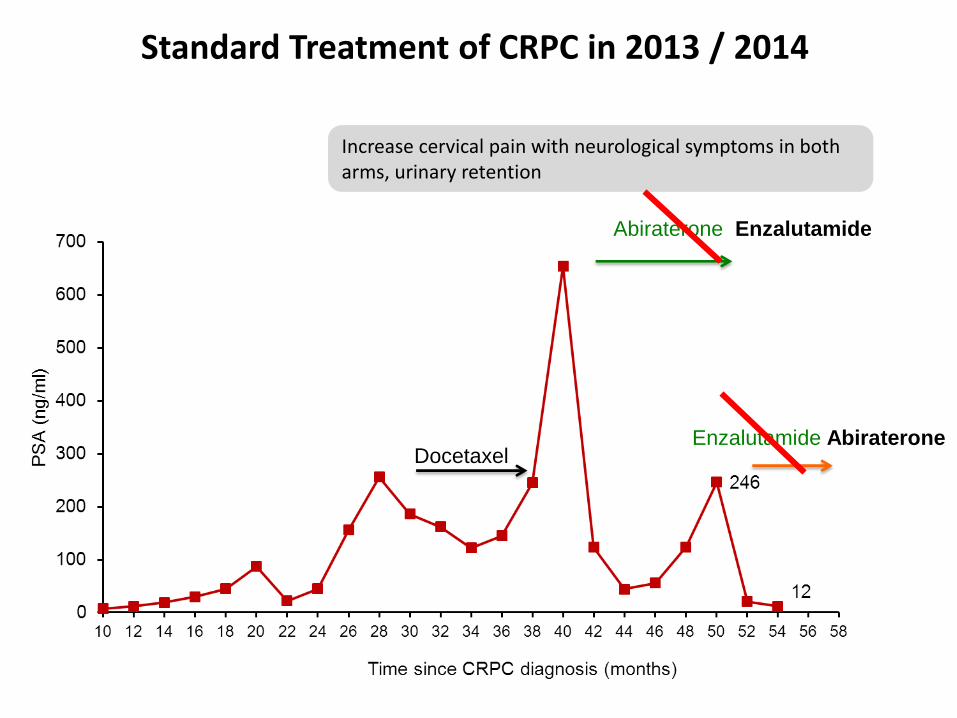
Docetaxel
Increase cervical pain with neurological symptoms in both arms, urinary retention
Abiraterone Enzalutamide
Enzalutamide Abiraterone
Standard Treatment of CRPC in 2013 / 2014
• Who gets the drugs
• Who gives the drugs ?
• What is the optimal sequencing and combination
• What about poor performance status patients
• Who pays the bill…….?
Problems and Uncertainties in CRPC

• Who gets the drugs
• Who gives the drugs ?
• What is the optimal sequencing and combination
• What about poor performance status patients
• Who pays the bill…….?
Problems and Uncertainties in CRPC
Non-metastatic PSA increasing
Metastatic
Asymptomatic
Metastatic
Symptomatic
(bone pain)
Pall
iati
on
S
urv
ival
pre
ven
tio
n
Chemotherapy
Radiotherapy
Radionuclide
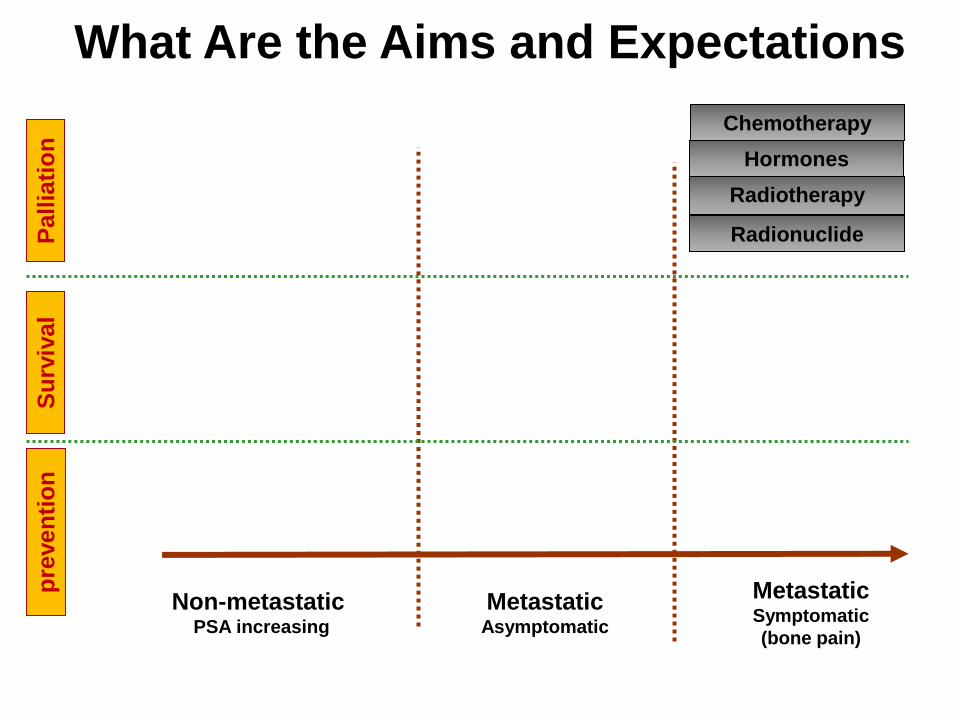
What Are the Aims and Expectations
Hormones

Non-metastatic PSA increasing
Metastatic
Asymptomatic
Metastatic
Symptomatic
(bone pain)
Pall
iati
on
S
urv
ival
pre
ven
tio
n
Chemotherapy
Radiotherapy
Radionuclide
What Are the Aims and Expectations
Hormones
Chemotherapy
Radiotherapy
Radionuclide
Hormones

Non-metastatic PSA increasing
Metastatic
Asymptomatic
Metastatic
Symptomatic
(bone pain)
Pall
iati
on
S
urv
ival
pre
ven
tio
n
Chemotherapy
Radiotherapy
Radionuclide
What Are the Aims and Expectations
Hormones
Chemotherapy
Radiotherapy
Radionuclide
Hormones
Chemotherapy
Radiotherapy
Radionuclide
Hormones

Non-metastatic PSA increasing
Metastatic
Asymptomatic
Metastatic
Symptomatic
(bone pain)
Pall
iati
on
S
urv
ival
pre
ven
tio
n
Chemotherapy
?
What Are the Aims and Expectations

Non-metastatic PSA increasing
Metastatic
Asymptomatic
Metastatic
Symptomatic
(bone pain)
Pall
iati
on
S
urv
ival
pre
ven
tio
n
Chemotherapy
?
What Are the Aims and Expectations

Non-metastatic PSA increasing
Metastatic
Asymptomatic
Metastatic
Symptomatic
(bone pain)
Pall
iati
on
S
urv
ival
pre
ven
tio
n
?
What Are the Aims and Expectations

Non-metastatic PSA increasing
Metastatic
Asymptomatic
Metastatic
Symptomatic
(bone pain)
Pall
iati
on
S
urv
ival
pre
ven
tio
n
?
What Are the Aims and Expectations

Non-metastatic PSA increasing
Metastatic
Asymptomatic
Metastatic
Symptomatic
(bone pain)
Palliate symptoms
Improve survival ?
Prevent onset and complications of bone metastases ?
What Are the Aims and Expectations P
all
iati
on
S
urv
ival
pre
ven
tio
n

Older Men Have a Higher Risk of
Dying Due to PCa
Skosyrev E et al. Cancer 2012;118:3062-70
Cu
mu
lati
ve in
cid
en
ce
90+
85-89
80-84
75-79
<75
Years from prostate cancer diagnosis
Cumulative incidence of PCa-related death
Same treatment
as younger patients
Geriatric intervention
=> Standard
treatment
Geriatric intervention
=> Adapted
treatment (or
palliation)
Only palliative
treatment
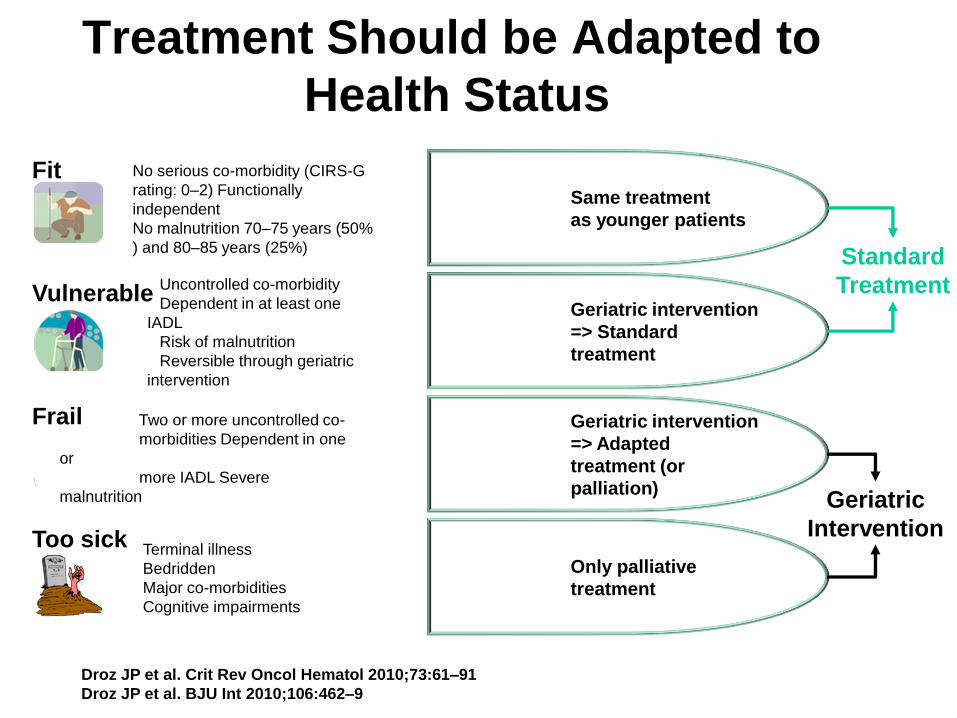
Treatment Should be Adapted to
Health Status
Droz JP et al. Crit Rev Oncol Hematol 2010;73:61–91
Droz JP et al. BJU Int 2010;106:462–9
No serious co-morbidity (CIRS-G
rating: 0–2) Functionally
independent
No malnutrition 70–75 years (50%
) and 80–85 years (25%)
Uncontrolled co-morbidity
Dependent in at least one
IADL
Risk of malnutrition
Reversible through geriatric
intervention
Two or more uncontrolled co-
morbidities Dependent in one
or
more IADL Severe
malnutrition
Terminal illness
Bedridden
Major co-morbidities
Cognitive impairments
Standard
Treatment
Geriatric
Intervention
Fit
Vulnerable
Frail
Too sick
What Do We Combine in CRPC ?
● Advances in the understanding of mCRPC have led to the development of new agents with diverse mechanisms of action:
– Second-generation taxanes
– Androgen-lowering agents
– AR signalling inhibitors
– Radiopharmaceuticals
– Bone Protective Agents
– Tyrosine kinase inhibitors
– Others
Hou X, Flaig TW. Adv Urol 2012;2012;978531; Fizazi K, et al. Ann Oncol 2012;23(Suppl. 10):x264–7.
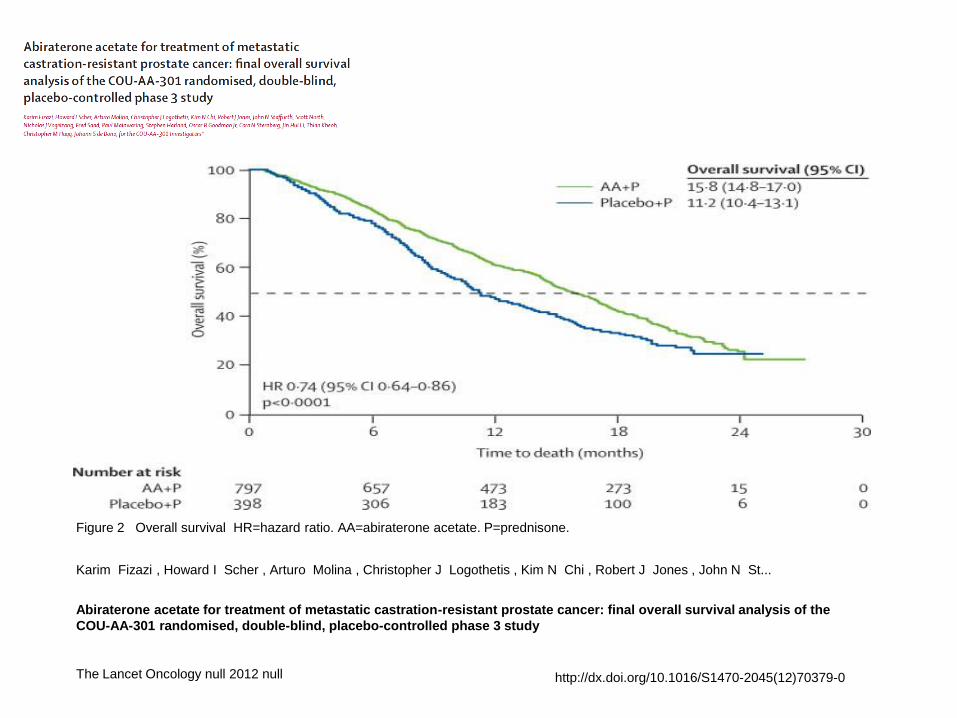
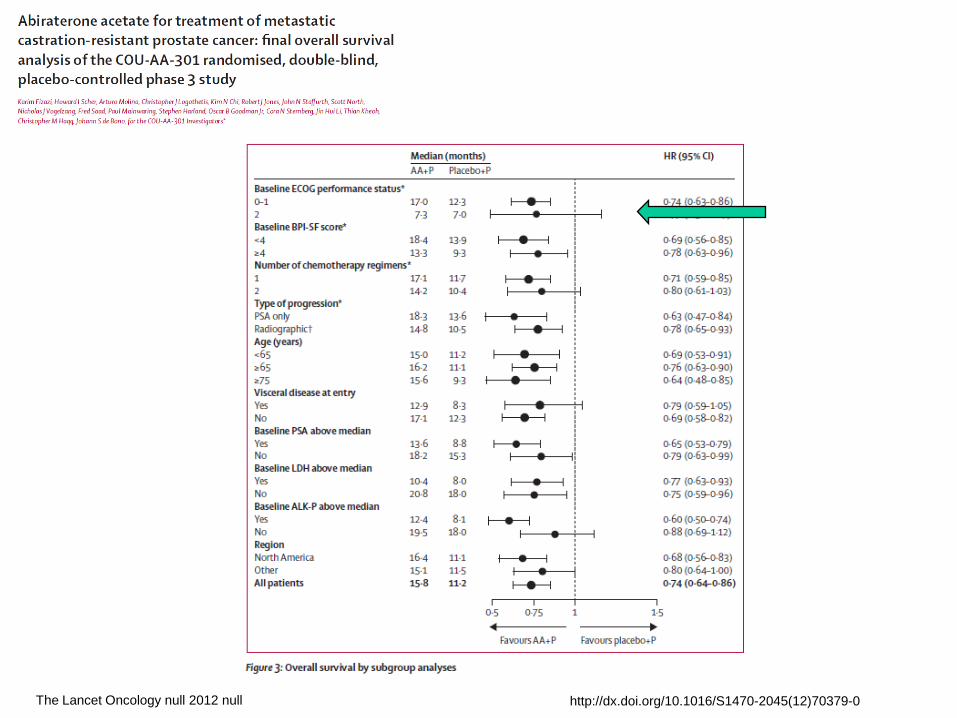
Figure 2 Overall survival HR=hazard ratio. AA=abiraterone acetate. P=prednisone.
Karim Fizazi , Howard I Scher , Arturo Molina , Christopher J Logothetis , Kim N Chi , Robert J Jones , John N St...
Abiraterone acetate for treatment of metastatic castration-resistant prostate cancer: final overall survival analysis of the
COU-AA-301 randomised, double-blind, placebo-controlled phase 3 study
The Lancet Oncology null 2012 null http://dx.doi.org/10.1016/S1470-2045(12)70379-0

The Lancet Oncology null 2012 null http://dx.doi.org/10.1016/S1470-2045(12)70379-0

The Affirm Study
NEJM Sept 2012
MDV3100 Placebo
Median OS (months) 18.4 13.6
Hazard ratio 0.63
P value < 0.0001
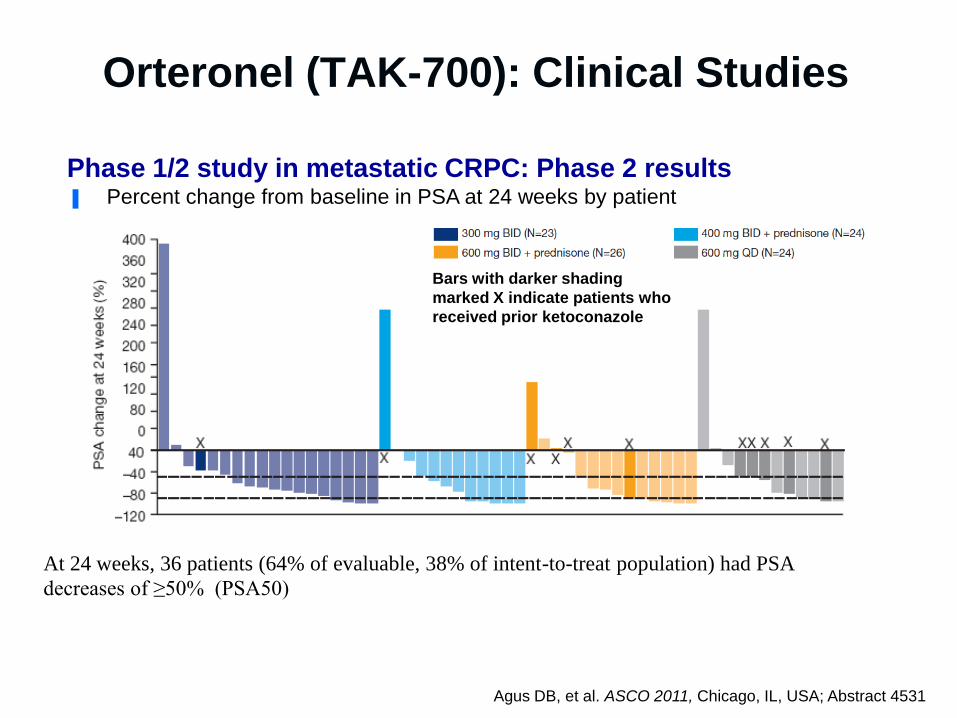
Orteronel (TAK-700): Clinical Studies
At 24 weeks, 36 patients (64% of evaluable, 38% of intent-to-treat population) had PSA
decreases of ≥50% (PSA50)
Phase 1/2 study in metastatic CRPC: Phase 2 results ▐ Percent change from baseline in PSA at 24 weeks by patient
Agus DB, et al. ASCO 2011, Chicago, IL, USA; Abstract 4531
Bars with darker shading
marked X indicate patients who
received prior ketoconazole

Patients • 1,083 patients,
progressive,
mCRPC
• Failed 1 or 2
chemotherapy
regimens, one
of which
contained
docetaxel
Orteronel (TAK-700) Registration Study C21005: mCRPC Following Docetaxel Failure
Efficacy
Endpoints Primary:
• OS
Secondary:
• PSA response
• Pain response
• rPFS
Orteronel po BID
Prednisone po BID
Placebo po BID
Prednisone po BID
rPFS = radiographic progression-free survival
www.clinicaltrials.gov; accessed June 2011

Phase III PREVAIL Trial: Study Design
CRPC R
1:1
MDV3100 160 mg daily
Placebo
Co-primary endpoints: overall survival and progression-free survival Secondary endpoints: time to first SRE; time to start of chemotherapy
Key inclusion criteria: • No prior treatment with cytotoxic chemotherapy • Asymptomatic or mildly symptomatic Estimated primary completion date – September 2014
Clinicaltrials.gov identifier # NCT00974311

Updated Interim Analysis (55% OS)
of COU-AA-302, a Randomized Phase 3
Study of Abiraterone Acetate in Metastatic
Castration-Resistant Prostate Cancer
Patients Without Prior Chemotherapy
Dana Rathkopf,1 Matthew R Smith,2 Johann S. de Bono,3 Christopher Logothetis,4 Neal D. Shore,5
Paul de Souza,6 Karim Fizazi,7 Peter F.A. Mulders,8 Paul Mainwaring,9 John D. Hainsworth,10
Tomasz M. Beer,11 Scott North,12 Yves Fradet,13 Tom Griffin,14 Youn C. Park,15 Thian Kheoh,14
Eric J. Small,16 Howard I. Scher,1,17 Arturo Molina,14 Charles J. Ryan18 on behalf of the COU-AA-302
Investigators
Rathkopf et al. ASCO GU 2013; Abstract 5 (Oral Presentation)

Abiraterone and Time to rPFS
100
80
60
40
20
0
0
Su
bje
cts
Witho
ut P
rogre
ssio
n
or
Dea
th (
%)
6 12 18 30 36 24
546
542
389
244
240
133
157
78
20
7
0
0
Abiraterone
Prednisone
117
45
Months From Randomization
Abiraterone
Prednisone
Abiraterone (median, mos): 16.5
Prednisone (median, mos): 8.3
HR (95% CI): 0.53 (0.45-0.62)
p Value: < 0.0001
15 9 3 21 27 33
485
406
311
176
195
99
131
62
66
20
4
0
Rathkopf et al. ASCO GU 2013; Abstract 5 (Oral Presentation)

Abiraterone and Overall Survival
100
80
60
40
20
0
0
Su
bje
cts
Witho
ut D
ea
th (
%)
6 12 18 30 36 24
546
542
524
508
482
465
421
400
68
67
0
0
Abiraterone
Prednisone
333
283
Months From Randomization
Abiraterone
Prednisone
Abiraterone (median, mos): 35.3
Prednisone (median, mos): 30.1
HR (95% CI): 0.79 (0.66-0.95)
p Valuea: 0.0151
15 9 3 21 27 33
538
534
503
492
452
437
393
361
175
153
15
9
Rathkopf et al. ASCO GU 2013; Abstract 5 (Oral Presentation)
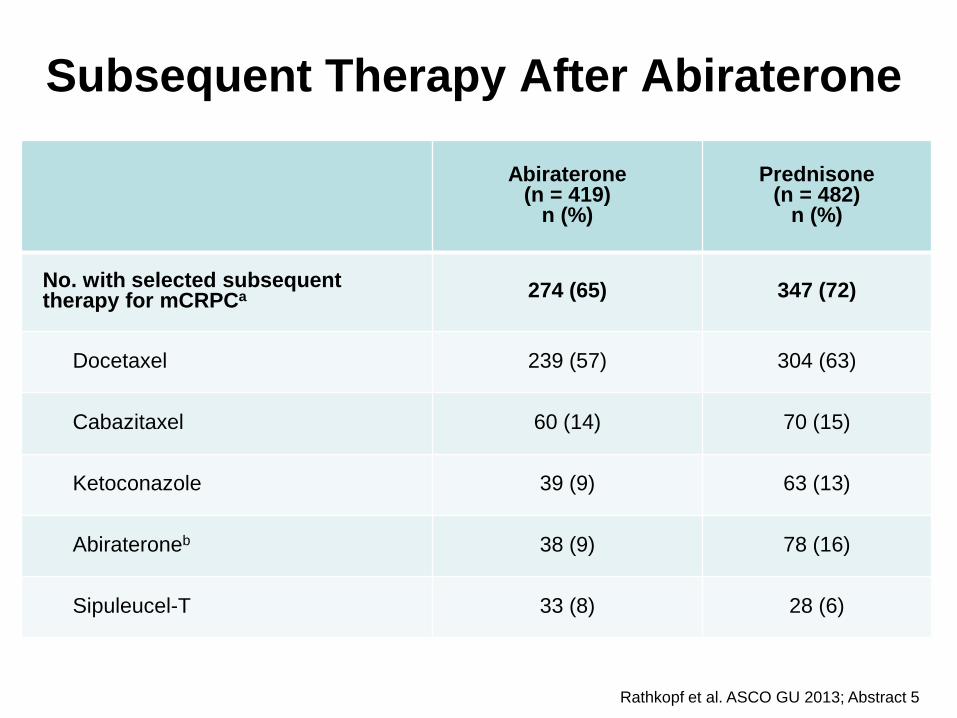
Subsequent Therapy After Abiraterone
Abiraterone (n = 419)
n (%)
Prednisone (n = 482)
n (%)
No. with selected subsequent therapy for mCRPCa 274 (65) 347 (72)
Docetaxel 239 (57) 304 (63)
Cabazitaxel 60 (14) 70 (15)
Ketoconazole 39 (9) 63 (13)
Abirateroneb 38 (9) 78 (16)
Sipuleucel-T 33 (8) 28 (6)
Rathkopf et al. ASCO GU 2013; Abstract 5

Safety Profile
Abiraterone (n = 542)
%
Prednisone (n = 540)
%
Adverse event All grades Grades 3/4 All grades Grades 3/4
Fatigue 40 2 35 2
Fluid retention 29 1 24 2
Hypokalemia 17 3 13 2
Hypertension 22 4 14 3
Hyperglycemia 9 3 8 2
Weight gain 5 0 7 0
Cardiac disorders 21 7 18 4
ALT increased 12 6 5 1
AST increased 11 3 5 1
. Rathkopf et al. ASCO GU 2013; Abstract 5

COU-AA-302
Updated Interim Analysis: Summary
8.2 months rPFS improvement (16.5 vs 8.3 months)
5.2 months OS improvement (35.3 vs 30.1 months)
9.7 months delay chemotherapy (26.5 vs 16.8 months)
Delayed time to opiate use (NR vs 23.7 months)
Improved QoL
Tolerated treatment with longer exposure
Rathkopf et al. ASCO GU 2013; Abstract 5 (Oral Presentation)

• Who gets the drugs
• Who gives the drugs ?
• What is the optimal sequencing and
combination
• What about poor performance status patients
• Who pays the bill…….?
Problems and Uncertainties in CRPC

Chemotherapy or Hormonal
Treatment First ?

When Should Chemotherapy be Started?
● Not all men are suitable for chemotherapy
● Both QoL and pain can be improved by chemotherapy
● Men with minimal symptoms had prolonged survival
Berthold, D. R. et al. J Clin Oncol; 26:242-245 2008

Should Docetaxel Responders be Re-Treated
• Re-Treatments of Initial Responders
• 59% Response to 1st Line
• 90% Response to 2nd Line
• 71% Response to 3rd Line
• Duration of Response 24 + 21 Weeks
• N Sepsis 2.9 1st Line /4.2 2nd Line /5.2 % 3rd Line
Ansari et al GU ASCO 2009 # 185

TROPIC results: Efficacy
● Median follow-up: 12.8 months
● Median OS:
– Cabazitaxel 15.1 months
– Mitoxantrone 12.7 months
CI=confidence interval; HR=hazard ratio. de Bono JS, et al. Lancet 2010;376:1147–54.
0
20
40
60
80
100
0 6 12 18 24 30
Mitoxantrone (n) 377 300 188 67 11
Cabazitaxel (n) 378 321 231 90 28
Mitoxantrone
Cabazitaxel
1
4
Su
rviv
al (%
)
Months
HR=0.70 (95% CI: 0.59–0.83); p<0.0001
30% reduction in risk of death
Novel Androgen Receptor Signalling
● Should all patients receive this routinely as the first 2nd line agent
● How do we decide whether to give chemotherapy 1st or 2nd
● How will regulation affect sequencing ?

Novel Androgen Receptor Signalling
● Should all patients receive this routinely as the first 2nd line agent
● How do we decide whether to give chemotherapy 1st or 2nd
● How will regulation affect sequencing ?
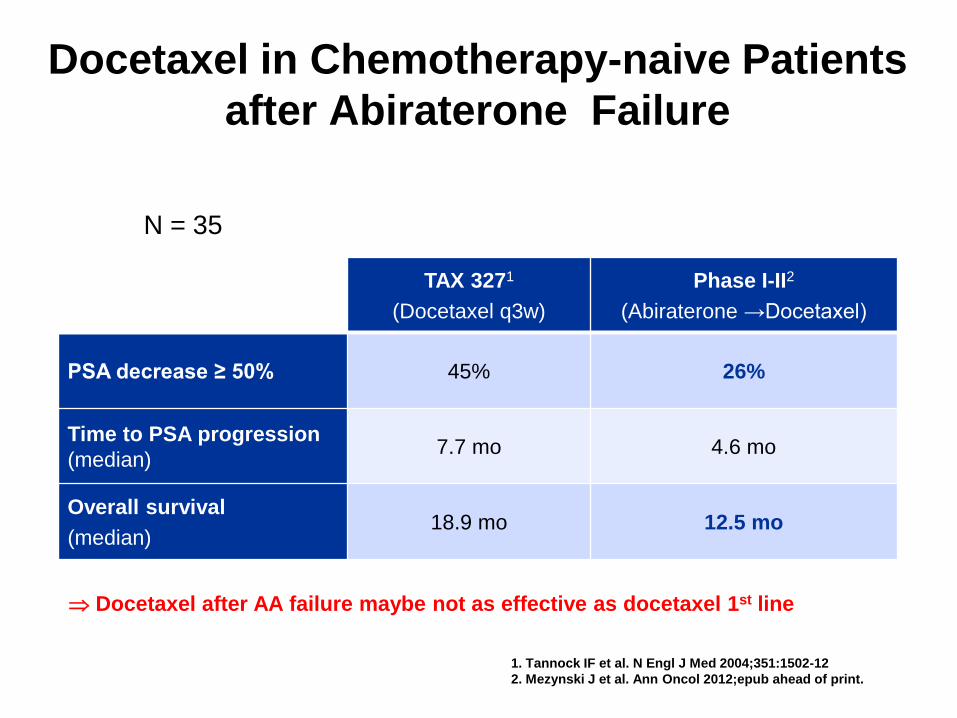
Docetaxel in Chemotherapy-naive Patients
after Abiraterone Failure
N = 35
TAX 3271
(Docetaxel q3w)
Phase I-II2
(Abiraterone →Docetaxel)
PSA decrease ≥ 50% 45% 26%
Time to PSA progression
(median) 7.7 mo 4.6 mo
Overall survival
(median) 18.9 mo 12.5 mo
1. Tannock IF et al. N Engl J Med 2004;351:1502-12
2. Mezynski J et al. Ann Oncol 2012;epub ahead of print.
Docetaxel after AA failure maybe not as effective as docetaxel 1st line

Androgen Receptor Inhibition After
Chemotherapy
COU-AA-3011
(Abiraterone vs Placebo)
AFFIRM2
(Enzalutamide vs Placebo)
OS after 1 prior line
chemotherapy 17.1 vs 11.7 mo NR vs 14.2 mo
OS after 2 prior lines
chemotherapy 14.2 vs 10.4 mo 15.9 vs 12.3 mo
1. Fizazi K et al. Lancet Oncol 2012
2. Scher H et al. N Engl J Med 2012;367:1187-97
Abiraterone and enzalutamide both effective after 2 lines of chemotherapy

Malik Z et al. J Clin Oncol 2012;30 (Suppl):abstract e15135
Abiraterone
Median OS 8 months
Cabazitaxel
Median OS 18 months
Cu
mu
lati
ve
su
rviv
al
1.
0
0.
8
0.
6
0.
4
0.
2
0
0 3 6 9 12 15 18 21
Months (Treatment start)
─ Docetaxel → Cabazitaxel
─ Docetaxel → Abiraterone
Sequence after Docetaxel Failure

• Who gets the drugs
• Who gives the drugs ?
• What is the optimal sequencing and combination
• What about poor performance status patients
• Who pays the bill…….?
Problems and Uncertainties in CRPC
The Lancet Oncology null 2012 null http://dx.doi.org/10.1016/S1470-2045(12)70379-0

100
80
60
40
20
Surv
ival (%
)
0
0 3 6 9 12 15 18 21
Time to Death (Months)
AA ECOG 0-1
15.3 months
Placebo ECOG 0-1
11.7 months
AA ECOG 2
7.3 months
Placebo ECOG 2
7 months
OS: ECOG status (0-1 vs 2)
ECOG Status
Scher et al. J Clin Oncol 2011; 25 (suppl 7); Abstract 4 (oral presentation)
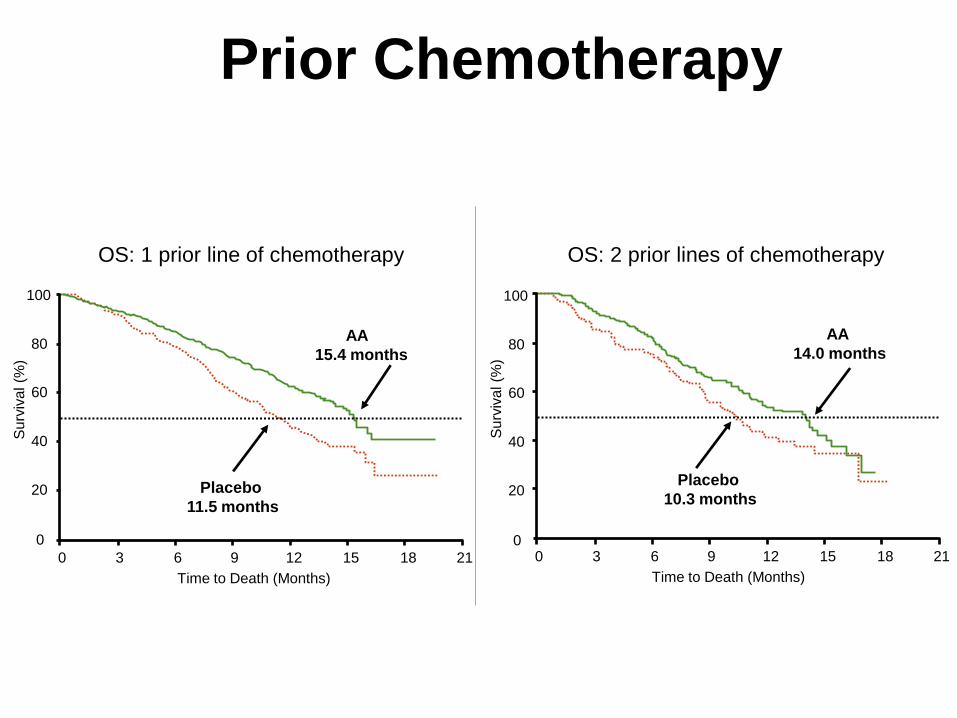
Prior Chemotherapy
OS: 1 prior line of chemotherapy OS: 2 prior lines of chemotherapy
100
80
60
40
20
Su
rviv
al (%
)
0
0 3 6 9 12 15 18 21
Time to Death (Months)
AA
15.4 months
AA
14.0 months
Placebo
10.3 months
100
80
60
40
20 S
urv
iva
l (%
)
0 0 3 6 9 12 15 18 21
Time to Death (Months)
Placebo
11.5 months
de Bono et al. Ann Oncol 2010; 21 (10 suppl 8): Abstract LBA5 (oral presentation)
Scher et al. J Clin Oncol 2011; 25 (suppl 7): Abstract 4 (oral presentation)

Pain Status
OS: Pain
(0-3 [absent]) OS: Pain
(4-10 [present])
100
80
60
40
20
Su
rviv
al (%
)
0 0 3 6 9 12 15 18 21
Time to Death (Months)
100
80
60
40
20
Su
rviv
al (%
)
0 0 3 6 9 12 15 18 21
Time to Death (Months)
AA
16.2 months
Placebo
13 months
AA
12.6 months
Placebo
8.9 months
Scher et al. J Clin Oncol 2011; 25 (suppl 7); Abstract 4 (oral presentation)
*Brief Pain Inventory scale

• Who gets the drugs
• Who gives the drugs ?
• What is the optimal sequencing and combination
• What about poor performance status patients
• Who pays the bill…….?
Problems and Uncertainties in CRPC

Costs
• £2930 / Month ($4640)
• £46,800-50,000 / QALY
• Initially rejected by NICE:
“Too Costly”
• Accepted June 2012 after
“Renegotiation of the
price”
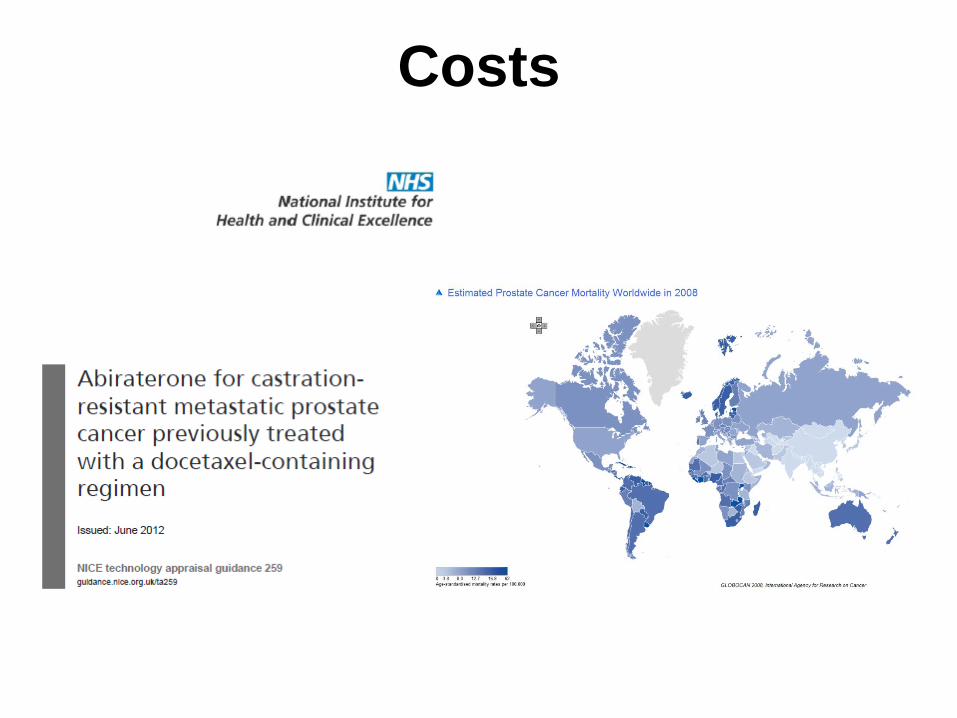
Costs
• £2930 / Month ($4640)
• £46,800-50,000 / QALY
• Initially rejected by NICE:
“Too Costly”
• Accepted June 2012 after
“Renegotiation of the
price”
Costs

Hormonal Manipulations in CRPC
NW Clarke
Professor of Urological Oncology
Manchester UK
Related Documents

![Research Paper Nuclear receptor ERRα contributes to ... · the management of CRPC . In fact, xenograft [5, 6] models of CRPC and CRPC tissues show increased expressions of multiple](https://static.cupdf.com/doc/110x72/5ed997291b54311e7967d8e3/research-paper-nuclear-receptor-err-contributes-to-the-management-of-crpc.jpg)









