1 Hoofdstuk 2 DM type 1 Uitgangsvraag 1 Met welk insulineschema start je bij een volwassene met een nieuw ontdekte type 1 diabetes zonder acidose? Inleiding Bij Diabetes Mellitus type 1 (DM1) is er sprake van een absoluut insuline tekort en dient de behandeling altijd te bestaan uit het toedienen van insuline. De meest logische en fysiologische behandeling bij DM1 is een basis/bolus regime. Soms wordt echter vanwege praktische redenen gestart met een tweemaal daags regime met mix-insulines of een combinatie van mix- en kortwerkende insuline. De uitgangsvraag is hoe een volwassene met een nieuw ontdekte DM1 zonder acidose optimaal kan worden behandeld: bij welk insulineschema is de kans op acute en late complicaties het kleinst? De relevante uitkomstmaten zijn micro- en macrovasculaire complicaties, glycemische controle (HbA1c), en bijwerkingen (hypoglycemie). Er is gezocht naar literatuur waarin de effectiviteit van insulineschema’s wordt vergeleken bij volwassen patiënten met nieuw ontdekte DM1, met micro- en macrovasculaire complicaties, glycemische controle (HbA1c) en bijwerkingen als uitkomstmaat. De buitenlandse richtlijnen NICE en ADA 2012 geven geen duidelijk advies voor een startschema. Aanvullend is gezocht vanaf 1-1-2008 op systematische reviews en RCT’s, in de databases Medline, Embase en de Cochrane Library. Uit het totaal van 34 treffers werden op basis van titel en abstract, vier studies geselecteerd (Thraikill et al., 2011; Hassan et al., 2008; Rabbone et al., 2008; Skogsberg et al., 2008). Bij analyse van de full text zijn alle vier de RCT’s geëxcludeerd op grond van de studiepopulaties die geheel dan wel grotendeels uit kinderen of adolescenten bestaan. Samenvatting van de literatuur De zoekactie leverde geen RCT’s op die zijn uitgevoerd bij volwassenen met nieuw gediagnosticeerde DM1. Veel studies zijn bij kinderen en adolescenten uitgevoerd. De aanpak bij

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Hoofdstuk 2 DM type 1
Uitgangsvraag 1
Met welk insulineschema start je bij een volwassene met een nieuw ontdekte type 1
diabetes zonder acidose?
Inleiding
Bij Diabetes Mellitus type 1 (DM1) is er sprake van een absoluut insuline tekort en dient de
behandeling altijd te bestaan uit het toedienen van insuline. De meest logische en fysiologische
behandeling bij DM1 is een basis/bolus regime. Soms wordt echter vanwege praktische redenen
gestart met een tweemaal daags regime met mix-insulines of een combinatie van mix- en
kortwerkende insuline.
De uitgangsvraag is hoe een volwassene met een nieuw ontdekte DM1 zonder acidose optimaal
kan worden behandeld: bij welk insulineschema is de kans op acute en late complicaties het
kleinst? De relevante uitkomstmaten zijn micro- en macrovasculaire complicaties, glycemische
controle (HbA1c), en bijwerkingen (hypoglycemie).
Er is gezocht naar literatuur waarin de effectiviteit van insulineschema’s wordt vergeleken bij
volwassen patiënten met nieuw ontdekte DM1, met micro- en macrovasculaire complicaties,
glycemische controle (HbA1c) en bijwerkingen als uitkomstmaat. De buitenlandse richtlijnen
NICE en ADA 2012 geven geen duidelijk advies voor een startschema. Aanvullend is gezocht
vanaf 1-1-2008 op systematische reviews en RCT’s, in de databases Medline, Embase en de
Cochrane Library. Uit het totaal van 34 treffers werden op basis van titel en abstract, vier studies
geselecteerd (Thraikill et al., 2011; Hassan et al., 2008; Rabbone et al., 2008; Skogsberg et al.,
2008). Bij analyse van de full text zijn alle vier de RCT’s geëxcludeerd op grond van de
studiepopulaties die geheel dan wel grotendeels uit kinderen of adolescenten bestaan.
Samenvatting van de literatuur
De zoekactie leverde geen RCT’s op die zijn uitgevoerd bij volwassenen met nieuw
gediagnosticeerde DM1. Veel studies zijn bij kinderen en adolescenten uitgevoerd. De aanpak bij

2
deze patiëntencategorie verschilt echter van de aanpak bij volwassenen, omdat bij kinderen en
adolescenten, groei, hormonale veranderingen en therapietrouw meer op de voorgrond zal
staan dan bij volwassenen. Bij volwassenen ligt de nadruk minder op therapietrouw en meer op
het voorkomen van lange termijn complicaties en hypoglycemieën.
Conclusie
De literatuursearch heeft geen geschikte studies opgeleverd die een antwoord geven op de
uitgangsvraag.
Overwegingen
In het algemeen wordt voor patiënten met DM1 aanbevolen een keuze te maken voor een basis/
bolusschema met een pen (Multiple Daily Injections, MDI) dan wel via Continuous Subcutaneous
Insulin Infusion (CSII). In de praktijk wordt meestal gestart met een langwerkend insuline voor de
nacht in combinatie met een kortwerkend insuline bij elke maaltijd. Een afwijkend schema kan
gebaseerd zijn op een individuele dagindeling, zoals bijvoorbeeld een schema met een pre-mixed
insuline bij het ontbijt, kortwerkend insuline bij het avondeten en langwerkend insuline voor de
nacht. Aangezien er uit de DCCT aanwijzingen zijn dat de complicatie incidentie bij een pre-
mixed schema van tweemaal daags hoger is (DCCT Research Group, 1993; Nathan et al., 2005),
wordt hier in de praktijk alleen voor gekozen als de patiënt hier een sterke voorkeur voor heeft.
Het voordeel van dit schema is dat patiënten minder vaak insuline hoeven te spuiten in
tegenstelling tot 4 dd bij het basis/bolusschema, wat mede als voordeel heeft dat werkende/
studerende patiënten dit thuis kunnen toedienen in plaats van op de werkplek.
In de praktijk wordt vaak gekozen voor een startdosering van 0,2 units/kg, waarbij de helft
daarvan als kortwerkend insuline wordt gegeven en de andere helft als langwerkend insuline.
In de Diabetes Control and Complications Trial (DCCT) en bijbehorende follow-up studie (EDIC,
Epidemiology of Diabetes Interventions and Complications trial) is aangetoond dat glycemische
controle nadat de diagnose DM gesteld is, het risico op lange termijn micro- en macrovasculaire
complicaties vermindert (DCCT Research Group 1993; Nathan et al., 2005; White et al., 2008).
Het verminderde risico bijvoorbeeld op retinopathie, bij de intensief behandelde groep bleef na
10 jaar follow-up bestaan ondanks het feit dat het verschil in HbA1c tussen de intensief
behandelde en conventioneel behandelde groep verdween (DCCT Research Group, 1993; Nathan
et al., 2005). De intensief behandelde groep werd met tenminste drie dagelijkse insuline injecties

3
behandeld of CSII (basis-bolus principe), terwijl de conventionele groep met slechts één-twee
insuline injecties per dag werd behandeld (met name pre-mixed schema’s).
Er zijn een aantal redenen waarom het bereiken van vroege glycemische controle niet altijd
mogelijk is, zoals het optreden van, of de angst voor hypoglycemieën, en de noodzaak voor
intensief dagelijkse management van de diabetes met frequente glucosemetingen en
aanpassingen in insulinedosering. Naast het hoofddoel om vroege glycemische controle te
bereiken, wordt de keuze van het optimale insuline schema dan ook bepaald door een groot
aantal factoren, zoals: leeftijd, leefstijl/dagindeling, beroep, comorbiditeit, motivatie,
mogelijkheid tot zelfcontrole en zelfregulatie.
Samenvattend zijn er na het stellen van de diagnose DM1, in grote lijnen twee startschema’s
met MDI mogelijk:
1) Basis/bolusschema via een insuline pen:
3 dd (ultra)kortwerkende insuline bij de maaltijd + 1-2 dd een (middel)langwerkende
insuline.
2) Pre-mixed insuline:
a) Tweemaal daags schema;
b) Pre-mixed insuline in combinatie met kortwerkende en/of langwerkende insuline
(bijvoorbeeld pre-mixed insuline bij het ontbijt, kortwerkende bij het avondeten en
een langwerkende voor de nacht).
Het voordeel van dit schema is dat patiënten minder vaak insuline hoeven te spuiten. Het grote
nadeel is echter dat het de endogene insuline-excretie niet goed nabootst wordt en er daardoor
minder goede glycemische controle bestaat en striktere voedingsvoorschriften nodig zijn. Dit
schema heeft derhalve niet de eerste voorkeur, maar kan op grond van individuele
patiëntomstandigheden worden overwogen.
Aanbevelingen
Bij patiënten met nieuw gediagnosticeerde diabetes mellitus type 1 zonder acidose:
Start met een basis/bolusschema;
Overweeg in eerste instantie MDI;
Gebruik bij voorkeur geen pre-mixed tweemaal daags schema;
Startdosering van 0,2 units/kg per dag, verdeeld over meerdere injecties.

4
Literatuur
DCCT Research Group. (1993). The effect of intensive treatment of diabetes on the development
and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J
Med., 329, 977-986.
Hassan, K., Rodriguez, L. M., Johnson, S. E., Tadlock, S., & Heptulla, R.A. (2008). A randomized,
controlled trial comparing twice-a-day insulin glargine mixed with rapid-acting insulin analogs
versus standard neutral protamine Hagedorn (NPH) therapy in newly diagnosed type 1 diabetes.
Pediatrics, 121, e466-e472.
Nathan, D.M., Cleary, P.A., Backlund, J.Y., Genuth, S.M., Lachin, J.M., Orchard, T.J., Raskin, P.,
Zinman, B. & Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions
and Complications (DCCT/EDIC) Study Research Group. (2005). Intensive diabetes treatment and
cardiovascular disease in patients with type 1 diabetes. N Engl J Med., 353, 2643-2653.
Rabbone, I., Bobbio, A., Di Gianni, V., Sacchetti, C., & Cerutti, F. (2008) Intensive insulin therapy
in preschool-aged diabetic children: from multiple daily injections to continuous subcutaneous
insulin infusion through indwelling catheters. J Endocrinol Invest., 31, 193-195.
Skogsberg, L., Fors, H., Hanas, R., Chaplin, J. E., Lindman, E., & Skogsberg, J. (2008). Improved
treatment satisfaction but no difference in metabolic control when using continuous
subcutaneous insulin infusion vs. multiple daily injections in children at onset of type 1 diabetes
mellitus. Pediatric diabetes, 9, 472-479.
Thrailkill, K.M., Moreau, C.S., Swearingen, C., Rettiganti, M., Edwards, K., Morales, A.E., Kemp,
S.F., Frindik, J.P., & Fowlkes, J.L. (2011). Insulin pump therapy started at the time of diagnosis:
effects on glycemic control and pancreatic beta-cell function in type 1 diabetes. Diabetes
Technology & Therapeutics, 13, 1023-1030.
White, N.H., Sun, W., Cleary, P.A., Danis, R.P., Davis, M.D., Hainsworth, D.P., Hubbard, L.D.,
Lachin, J.M.,… (2008). Prolonged effect of intensive therapy on the risk of retinopathy
complications in patients with type 1 diabetes mellitus: 10 years after the Diabetes Control and
Complications Trial. Arch Ophthalmol., 126(12), 1707-15.
http://www.ncbi.nlm.nih.gov/pubmed?term=Swearingen%20C%5BAuthor%5D&cauthor=true&cauthor_uid=21718094

5
Uitgangsvraag 2
Welk soort insuline verdient de voorkeur bij behandeling van volwassenen met DM1:
humaan of analoog insuline?
Inleiding
Sinds de beschikbaarheid van insuline analogen zijn de mogelijkheden tot behandeling van het
insulinetekort bij mensen met DM1 duidelijk toegenomen. De humane (middel)langwerkende
insulines hebben als nadeel dat zij een piekwaarde in de vroege nacht geven en de intra- en
interindividuele variatie in werking zeer groot is (resp. 26% en 55%; Kolendorf et al., 1978;
Lepore et al., 2000). Als gevolg van het Dawn fenomeen blijken veel mensen met DM1 hiermee
geen adequate nuchtere glucosewaarde te bereiken. Pomptherapie met variabele basale
insulineafgifte was dan de enige optie. Bij het beschikbaar komen van de langwerkende insuline-
analogen is het voor de meeste patiënten wel mogelijk een normale glucosewaarde voor het
slapen te combineren met een goede nuchtere waarde.
De kortwerkende humane insulines zijn eigenlijk helemaal niet kortwerkend (werkingsduur van
zes-acht) en volgen niet de glucoseopname bij de maaltijden. Dit kan leiden tot postprandiale
hyperglycemie, en enkele uren na de maaltijd, tot hypoglycemie. Daarom moet deze insuline
dan ook in principe ±20 minuten voor de maaltijd worden gespoten. De (ultra)kortwerkende
insuline-analogen hebben deze nadelen niet, kunnen wel direct bij de maaltijd worden
geïnjecteerd, maar kunnen nog steeds een werkingsduur van vijf uur hebben.
Ten aanzien van de insulineanalogen is de hoofdvraag of de bovengenoemde voordelen leiden
tot een verbeterde glycemische regulatie: lagere HbA1c waardes en minder hypoglycemieën, in
vergelijking met humaan insuline.
De uitgangsvraag omvat twee deelvragen:
1. Hebben kortwerkende insulineanalogen (lispro, aspart, glulisine) de voorkeur boven
humaan kortwerkend insuline. Primaire uitkomstmaat: HbA1c, hypoglycemieën;
secundaire uitkomstmaat: postprandiale hyperglycemie.
2. Hebben langwerkende insulineanalogen (detemir, glargine) de voorkeur boven
protamine Hagedorn (NPH insuline). Primaire uitkomstmaat: HbA1c, (nachtelijke)
hypoglycemieen; secundaire uitkomstmaat: nuchtere bloedglucose.

6
Er is gezocht naar literatuur waarin de effectiviteit van kortwerkende insulineanalogen en
humaan insuline wordt vergeleken (deelvraag 1), en literatuur waarin de effectiviteit van
langwerkende insulineanalogen en NPH insuline wordt vergeleken (deelvraag 2), bij patiënten
met DM1, met glycemische controle (HbA1c) en bijwerkingen (hypoglycemische episodes) als
uitkomstmaat.
Er is gezocht in de buitenlandse richtlijnen ADA en NICE, daarnaast is gezocht vanaf 1-1-2008 op
systematische reviews en RCT’s, in de databases Medline, Embase en the Cochrane Library. Uit
het totaal van 287 treffers werden op basis van titel en abstract, vier studies voor deelvraag 1,
en zes studies voor deelvraag 2 geselecteerd. Het betreft systematische reviews van studies
gepubliceerd tot juli 2009 (Rys et al., 2011; deelvraag 1), en tot december 2010 (Sanches et al.,
2011; deelvraag 2). De zoekactie leverde één relevante recentere RCT op (Brock Jacobsen et al.,
2011; deelvraag 1).
Samenvatting van de literatuur
De buitenlandse richtlijn ADA 2012 adviseert insulineanalogen te gebruiken indien
hypoglycemieën optreden. De NICE richtlijn adviseert kortwerkende insulineanalogen voor te
schrijven indien er nachtelijke of late interprandiale hypoglycemieen optreden en langwerkende
insulineanalogen in plaats van NPH insuline indien er nachtelijke hypoglycemieen optreden bij
NPH insuline of indien er in de ochtend hyperglycemieën optreden waardoor de glucose
regulatie overdag moeizaam verloopt.
Ad 1. Hebben kortwerkende insulineanalogen (lispro, aspart, glulisine) de voorkeur boven
humaan kortwerkend insuline (RHI)?
De zoekactie leverde drie systematische reviews op (Rys et al., 2011; Garg et al., 2010; Singh et
al., 2009). Het meest recente systematische review (Rys et al., 2011) is van goede kwaliteit en
includeert 18 RCT’s bij patiënten met DM1, gepubliceerd voor juli 2009. De studies bij patiënten
met DM2 zijn buiten beschouwing gelaten. De zoekactie leverde één relevante recentere RCT op
(Brock Jacobsen et al., 2011).
De inclusiecriteria van Rys et al. (2011) en de belangrijkste karakteristieken van de geselecteerde
studies, inclusief een beoordeling van de studiekwaliteit (Jadad-score), zijn te vinden in de
evidence-tabel (zie bijlage). Vijf van de achttien geïncludeerde RCT’s zijn cross-over studies, de
overige dertien studies hebben een parallel design. De studiegrootte varieert tussen 26 en 1065

7
deelnemers en de studieduur van zeven weken tot negen maanden. Waardes voor HbA1c, post-
prandiaal glucose en nuchter glucose werden als maten voor de glycemische controle vergeleken
tussen de groep behandeld met insuline aspart, en de controlegroep behandeld met
kortwerkend humaan insuline. Onder de dertien studies met voldoende gedetailleerde HbA1c
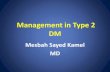
gegevens, was er in vier studies sprake van een statistisch significant grotere reductie in HbA1c
in de insuline aspart groep (0,12-0,35%, p<0,05; follow-up 3-6 maanden). In de overige negen
studies was het verschil tussen interventie- en controlegroep statistisch niet significant. Een
meta-analyse laat een grotere reductie zien in Hb1Ac in de insuline aspart-groep ten opzichte
van de controlegroep (Figuur 1; gewogen gemiddelde verschil, WMD; WMD= 0,11; 95% BI=
[0,16;-0,06]). In tien studies worden de effecten op post-prandiaal glucose voldoende
nauwkeurig beschreven, en zijn statistisch significante reducties te zien in de glucosewaardes na
ontbijt (-1.43 [-1.75; -1.11] mmol/l; meta-analyse van vijf studies), lunch (-1.11 [-1.61; -0.61]
mmol/l; vijf studies), en avondeten (-0.97 [-1.25; -0.69] mmol/l; zes studies). In zeven RCT’s
wordt de frequentie van hypoglycemische episodes vergeleken tussen de insuline aspart- en
controlegroep. De kans op een hypoglycemische episode lijkt marginaal verhoogd in de insuline-
aspart groep (RR=1.06 [1.01; 1.10]; meta-analyse van zes studies), terwijl de kans op nachtelijke
hypoglycemie lijkt af te nemen (0.67 [0.54; 0.83]; meta-analyse van drie studies) en die op
ernstige hypoglycemie niet significant verandert (0.92 [0.75; 1.12]; zeven studies). Aanvulling
van de SR van Rys et al. (2010) met de recente RCT van Brock Jacobsen et al. (2011), leidt niet tot
nieuwe inzichten. Het betreft een kleine cross-over studie (zestien patiënten) waarin geen
statistisch significant verschil wordt waargenomen in HbA1c waardes of de frequentie
hypoglycemie tussen de insuline aspart behandeling en behandeling met humaan kortwerkend
insuline (zie evidence-tabel).

8
Figuur 1 Vergelijking in effectiviteit tussen insuline aspart en humaan kortwerkend insuline.
Effectiviteit is gebaseerd op een vergelijking van HbA1c waardes (weighted mean
difference, WMD).
De twee eerdere systematische reviews (Garg et al., 2010; Singh et al., 2009) beperken zich niet
tot insuline aspart, maar includeren ook RCTs die de effecten van insuline glulisine en insuline
lispro vergelijken met kortwerkend humaan insuline. De conclusies in beide studies komen
overeen met die van Rys et al. (2011).
Bij beoordelen van de studies volgens GRADE is de bewijskracht matig voor effecten van
behandeling met ultrakortwerkende insulineanalogen op HbA1c, er is één punt afgetrokken
vanwege ernstige beperkingen in studieopzet (geen verborgen groepstoewijzing en geen
blindering van de behandeling in de meerderheid van de studies). Bij het bepalen van de
bewijskracht voor de effecten op post-prandiaal glucose is een tweede punt afgetrokken
vanwege indirectheid (inclusie van studies aan kinderen en adolescenten) en is de bewijskracht
laag. Tenslotte is de bewijskracht voor de effecten op het optreden van hypoglycemie laag
vanwege de beperkingen in studieopzet en vanwege inconsistentie (grote onverklaarde variatie
tussen studies, en verschil in geschatte effectiviteit afhankelijk van de gebruikte uitkomstmaat,
totaal versus nachtelijk versus ernstige hypoglycemie).
Study or Subgroup
Raskin 2000
Home 2000
Bode 2001
Tamas 2001
Iwamoto 2001
Bode 2002
Boehm 2002
De Vries 2003
Heller 2004
Arslanian 2005
Ampudia-Blasco 2005
Mortensen 2006
Mathiesen 2007
Total (95% CI)
Heterogeneity: Chi² = 14.58, df = 12 (P = 0.27); I² = 18%
Test for overall effect: Z = 4.28 (P < 0.0001)
Mean Difference
-0.15
-0.12
-0.2
-0.16
-0.24
-0.35
0.19
-0.14
0
0
0.14
0.14
-0.08
SE
0.0561
0.051
0.2347
0.0714
0.1684
0.1378
0.1225
0.1071
0.102
0.1786
0.2653
0.2398
0.0714
Weight
21.0%
25.4%
1.2%
13.0%
2.3%
3.5%
4.4%
5.8%
6.4%
2.1%
0.9%
1.1%
13.0%
100.0%
IV, Fixed, 95% CI
-0.15 [-0.26, -0.04]
-0.12 [-0.22, -0.02]
-0.20 [-0.66, 0.26]
-0.16 [-0.30, -0.02]
-0.24 [-0.57, 0.09]
-0.35 [-0.62, -0.08]
0.19 [-0.05, 0.43]
-0.14 [-0.35, 0.07]
0.00 [-0.20, 0.20]
0.00 [-0.35, 0.35]
0.14 [-0.38, 0.66]
0.14 [-0.33, 0.61]
-0.08 [-0.22, 0.06]
-0.11 [-0.16, -0.06]
Year
2000
2000
2001
2001
2001
2002
2002
2003
2004
2005
2005
2006
2007
Mean Difference Mean Difference
IV, Fixed, 95% CI
-0.5 -0.25 0 0.25 0.5
Favours insulin aspart Favours control

9
Conclusies
MATIG
Toepassing van ultrakortwerkende insulineanalogen bij patiënten met type 1
diabetes leidt tot een beperkte, wel statistisch significante, verlaging van het HbA1c
in vergelijking met kortwerkende humaan insuline. De klinische relevantie van deze
verlaging is voor het optreden van complicaties op de lange termijn is nooit
onderzocht.
Rys et al., 2011; Brock Jacobsen et al., 2011; Garg et al., 2010; Singh et al., 2009
LAAG
Toepassing van ultrakortwerkende insulineanalogen ten opzichte van kortwerkende
humaan insuline bij patiënten met type 1 diabetes leidt tot beperkte maar
statistisch significante daling van de post-prandiale glucose.
Rys et al., 2011
LAAG
Toepassing van kortwerkende insulineanalogen bij patiënten met type 1 diabetes
leidt tot minder nachtelijke hypoglycemische episodes ten opzichte van humaan
kortwerkende insuline. De kans op ernstige nachtelijke hypoglycemieën is niet
verschillend.
Rys et al., 2011; Brock Jacobsen et al., 2011; Garg et al., 2010; Singh et al., 2009
Ad 2. Hebben langwerkende insulineanalogen (detemir, glargine) de voorkeur boven
protamine Hagedorn (NPH)?
De zoekactie leverde vijf systematische reviews op (Sanches et al., 2011; Szypowska et al., 2011;
Garg et al., 2010; Monami et al., 2009; Dejgaard et al., 2009). Het meest recente systematische
review (Sanches et al., 2011) is van goede kwaliteit, en includeert 16 RCT’s gepubliceerd tot
december 2010. De belangrijkste uitkomstmaten zijn glycemische controle (HbA1c) en
bijwerkingen in de vorm van hypoglycemie. De zoekactie leverde geen relevante recentere RCT’s
op. De inclusiecriteria van Sanches et al. (2011) en de belangrijkste karakteristieken van de
geselecteerde studies, inclusief een beoordeling van de studiekwaliteit (Jadad-score), zijn te
vinden in de evidence-tabel (zie bijlage). De geïncludeerde RCT’s hebben een parallel design met

10
124 tot 747 deelnemers en een studieduur variërend van vier weken tot ruim twee jaar. Onder
de vijftien studies die HbA1c als maat voor de glycemische controle vergeleken tussen de groep
behandeld met detemir of glargine, en de controlegroep behandeld met NPH insuline, was er in
vier studies sprake van een statistisch significant grotere reductie in HbA1c in de
interventiegroep (0,22-0,40%, p<0,05; follow-up 4-26 maanden). In de overige elf studies was
het verschil tussen interventie- en controlegroep statistisch niet significant. Een meta-analyse
geeft een grotere reductie te zien in Hb1Ac in de interventiegroep dan in de controlegroep, het
verschil is klein maar wel statistisch significant (Figuur 2; gemiddelde verschil, MD; MD=-0,09 [-
0,14; -0,03]). Er wordt geen statistisch significant verschil waargenomen tussen glargine en
detemir (detemir versus NPH, MD=-0,13 [-0,19, -0,06]; glargine versus NPH, MD=-0,06 [-0,14;
0,02]). Bij vergelijking van de frequentie van hypoglycemische episodes tussen glargine (vijf
studies) of detemir (acht studies) en NPH insuline (controlegroep) ontstaat een inconsistent
beeld met een grote verschillen tussen de afzonderlijke studies. Meta-analyses geven geen
statistisch significant verschil te zien in het overall risico op hypoglycemie, of het risico op
nachtelijke hypoglycemie.
Figuur 2 Vergelijking in effectiviteit tussen langwerkende insulineanalogen (glargine of
detemir) en NPH insuline (Effectiviteit is gebaseerd op een vergelijking van HbA1c waardes
(mean difference, MD)).
Study or Subgroup
Ratner 2000
Raskin 2000
Rosenstock 2000b
Rosenstock 2000a
Vague 2003
Home 2004b
Home 2004a
Porcellati 2004
Russell-Jones 2004
Hermansen 2004
Pieber 2005a
Home 2005
Pieber 2005b
De Leeuw 2005
Fulcher 2005
Bartley 2008
Bolli 2009
Total (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 25.71, df = 16 (P = 0.06); I² = 38%
Test for overall effect: Z = 3.13 (P = 0.002)
Mean Difference
0.05
0
0
0
0
-0.17
-0.2
-0.4
0
-0.22
-0.04
-0.11
-0.1
-0.08
-0.3
-0.22
-0.03
SE
0.0714
0.0663
0.0918
0.0918
0.102
0.1225
0.1225
0.1582
0.0765
0.0561
0.1173
0.0714
0.1225
0.1173
0.1327
0.0867
0.0867
Weight
8.1%
8.7%
6.1%
6.1%
5.3%
4.1%
4.1%
2.7%
7.5%
10.0%
4.3%
8.1%
4.1%
4.3%
3.6%
6.5%
6.5%
100.0%
IV, Random, 95% CI
0.05 [-0.09, 0.19]
0.00 [-0.13, 0.13]
0.00 [-0.18, 0.18]
0.00 [-0.18, 0.18]
0.00 [-0.20, 0.20]
-0.17 [-0.41, 0.07]
-0.20 [-0.44, 0.04]
-0.40 [-0.71, -0.09]
0.00 [-0.15, 0.15]
-0.22 [-0.33, -0.11]
-0.04 [-0.27, 0.19]
-0.11 [-0.25, 0.03]
-0.10 [-0.34, 0.14]
-0.08 [-0.31, 0.15]
-0.30 [-0.56, -0.04]
-0.22 [-0.39, -0.05]
-0.03 [-0.20, 0.14]
-0.09 [-0.14, -0.03]
Year
2000
2000
2000
2000
2003
2004
2004
2004
2004
2004
2005
2005
2005
2005
2005
2008
2009
Mean Difference Mean Difference
IV, Random, 95% CI
-0.5 -0.25 0 0.25 0.5
Favours long-acting Favours control (NPH)

11
De drie eerdere systematische reviews (Szypowska et al., 2011; Garg et al., 2010; Monami et al.,
2009) includeren ook cross-over studies, studies bij kinderen en adolescenten, en niet-
gepubliceerde RCT’s. Voor wat betreft de effecten op de glycemische controle (HbA1C), komen
de conclusies in deze studies overeen met die van Sanches et al. (2011). Meta-analyses geven
een geringe extra reductie in HbA1c te zien in de interventiegroep (MD=–0.07 [–0.13; –0.01];
Szypowska et al., 2011; Monami et al., 2009). Het afwijkende inclusiebeleid heeft wel invloed op
de geschatte effecten van langwerkende insulineanalogen op het risico van hypoglycemie. De
studies rapporteren een afname in het overall risico op hypoglycemie (afname met 2-18%), het
risico op nachtelijke hypoglycemie (met 12-31%; p<0,05), en het risico op ernstige hypoglycemie
(met 27-33%; p<0,05).
Bij beoordelen van de studies volgens GRADE is de bewijskracht matig voor effecten van
behandeling met langwerkende insulineanalogen op HbA1c, er is één punt afgetrokken vanwege
ernstige beperkingen in studieopzet (geen verborgen groepstoewijzing en geen blindering van de
behandeling in meerderheid van de studies). De bewijskracht voor de effecten op het optreden
van hypoglycemie zijn laag vanwege de beperkingen in studieopzet, en vanwege inconsistentie
(grote onverklaarde variatie tussen studies).
Conclusies
MATIG
Toepassing van langwerkende insulineanalogen bij patiënten met type 1 diabetes
leidt tot een beperkte, maar statistisch significante, verlaging van het HbA1c ten
opzichte van NPH insuline.
Sanches et al, 2011; Szypowska et al, 2011; Garg et al, 2010; Monami et al, 2009
LAAG
Toepassing van langwerkende insulineanalogen bij patiënten met type 1 diabetes
leidt tot minder nachtelijke hypoglycemieen ten opzichte van NPH insuline.
Er bestaat grote heterogeniteit tussen studies, een afname van nachtelijke
hypoglycemieën wordt niet altijd waargenomen
Sanches et al., 2011; Szypowska et al., 2011; Garg et al., 2010; Monami et al., 2009

12
Overwegingen
Ad 1. Hebben kortwerkende insulineanalogen (lispro, aspart, glulisine) de voorkeur boven
normaal humaan insuline (RHI)?
Bovenstaande meta-analyse (Rys et al., 2011) laat een geringe extra reductie zien in Hb1Ac in de
insuline aspart-groep dan in de controlegroep. Dit verschil is statistisch significant, maar de
klinische relevantie is onduidelijk, en zal ondermeer afhangen van de uitgangswaarde van
HbA1c in de individuele patiënt, en of de extra reductie in HbA1c gepaard gaat met een toename
van hypoglycemie. Hoewel theoretisch insulineanalogen beter de glucosestijging na de maaltijd
opvangen, betekent dit ook dat het nemen van extra koolhydraten tussen de maaltijden
niet/onvoldoende gedekt is bij het gebruik van analogen. In de studies zijn de patiënten niet
geselecteerd op eetgewoonten/eetpatroon hetgeen wel relevant is.
Uit de meta-analyse blijkt tevens dat de kans op een hypoglycemische episode marginaal
verhoogd is in de insuline-aspart groep terwijl de kans op nachtelijke hypoglycemie kleiner is dan
ten opzichte van het gebruik van humaan kortwerkende insuline.
In conclusie, dit literatuuronderzoek laat geen duidelijk voordeel zien voor insuline aspart ten
opzichte van humaan kortwerkend insuline. Waarschijnlijk omdat geen rekening is gehouden
met het eet-/leefpatroon van de patiënt. Bij de keuze voor het type kortwerkend insuline zal
hiermee rekening gehouden moeten worden. Hierdoor kan één patiënt de twee verschillende
kortwerkende insulines gebruiken afhankelijk van zijn/haar koolhydraatintake. Op deze manier
wordt een maximale flexibiliteit bewerkstelligd. Maatwerk voor de individuele patiënt staat dus
op de voorgrond.
Ad 2. Hebben langwerkende insulineanalogen (detemir, glargine) de voorkeur boven NPH
insuline?
Bovenstaande meta-analyse laat een grotere reductie zien van Hb1Ac bij het gebruik van
langwerkende insulineanalogen dan bij het gebruik van NPH insuline (Sanches et al., 2011). Dit
verschil van 0,09% is zeer beperkt, maar statistisch wel significant. De meta-analyses geven geen
statistisch significant verschil van het overall risico op hypoglycemie of het risico op een
nachtelijke hypoglycemie. De drie andere systematische reviews (Szypowska et al., 2011; Garg et
al., 2010; Monami et al., 2009) includeerden ook cross-over studies, studies bij kinderen en
adolescenten, en niet-gepubliceerde RCT’s, waarbij er geconcludeerd werd dat er wel een
afname in het overall risico op hypoglycemieen, nachtelijke hypoglycemieen en ernstige

13
hypoglycemieen was. Naast de absolute kans op een hypoglycemie is de impact van een ernstige
hypoglycemie op de kwaliteit van leven en het risico op slechtere regulatie hierna wegens angst
voor hypoglycemieën zeker ook van belang. Een belangrijk nadeel van NPH insuline is de grote
intra-individuele variatie in de kinetiek van NPH insuline (26%; Kolenberg et al., 1978; Lepore et
al., 2000). Het begin van het glucose verlagend effect van NPH insuline varieert van 1-7 uur en
het maximale effect tussen 5 en 19 uur (Roy et al., 1980) waardoor het effect onbetrouwbaar
wordt. Er zijn ook nog latere studies die hetzelfde laten zien. Overigens zijn insulineanalogen bij
hogere doses ook niet helemaal piekloos. Hierbij kan het veranderen van de tijd van toedienen
en/of de frequentie van de injecties de kans op hypoglycemie verlagen (Roach, 2008).
Vooralsnog zijn er onvoldoende aanwijzingen gevonden dat er een associatie is tussen
langwerkende insulineanalogen en maligniteiten (Colhoun et al., 2009; Currie et al., 2009; Home
& Lagarenne, 2009; Jonasson et al., 2009; Mannucci et al., 2010; Morden et al., 2011;
Rosenstock et al., 2009; Ruiter et al., 2012; Suissa et al., 2011).
In conclusie, aangezien het gebruik van langwerkende insulineanalogen een marginale extra
reductie van het HbA1c laat zien ten opzichte van NPH insuline en er eveneens geen
vermindering van (nachtelijke) hypoglycemieen optreedt bij langwerkende insulineanalogen, is
een duidelijk voordeel van de langwerkende insulineanalogen ten opzichte van NPH insuline niet
bewezen. Langwerkende insuline wordt echter gegeven als basaal insuline en niet om het
glucose te verlagen, een belangrijk effect op het HbA1c wordt dan ook niet verwacht. Omdat in
de studies patiënten met zeer uiteenlopende HbA1c’s zijn onderzocht is er geen goede uitspraak
te doen of bij scherpe instelling wel verschillen zullen zijn. De kans op hypoglycemieën staat dus
meer op de voorgrond. De farmacokinetiek van insulineanalogen is meer fysiologisch en de
intraindividuele variatie in absorptie bij NPH insuline zeer groot. Derhalve, kan op patiëntniveau
toch een goede reden zijn om voor een langwerkend insulineanaloog te kiezen, zoals nachtelijke
hypoglycemieën en het Dawn fenomeen. Omdat bij de insulinebehandeling voor iemand met
DM1 maatwerk op de voorgrond staat, is het van belang dat het gehele arsenaal aan insulines
beschikbaar is.

14
Aanbevelingen
Stem de insuline behandeling af op de individuele eet- en leefpatronen van de patiënt.
Houd hierbij rekening met de farmacokinetische eigenschappen van de verschillende insulines.
Gebruik gezien de grote intraindividuele variatie in absorptie bij voorkeur langwerkende
insuline-analogen in plaats van NPH insuline.
Literatuur
Brock Jacobson, I., Vind, B. F., Korsholm, L., Flyvbjerg, A., Frystyk, J., Holst, J. J., Beck-Nielsen, H.,
& Henriksen, J.E. (2011). Counter-regulatory hormone responses to spontaneous hypoglycaemia
during treatment with insulin Aspart or human soluble insulin: a double-blinded randomized
cross-over study. Acta Physiologica, 202, 337-347.
Colhoun, H. M., SDRN Epidemiology Group (2009). Use of insulin glargine and cancer incidence in
Scotland: a study from the Scottish Diabetes Research Network Epidemiology Group.
Diabetologia 52:1766–1777.
Currie CJ, Poole CD, Gale EA (2009). The influence of glucose-lowering therapies on cancer risk in
type 2 diabetes. Diabetologia 52:1766–1777.
Dejgaard, A., Lynggaard, H., Rastam, J., & Krogsgaard, T. M. (2009). No evidence of increased risk
of malignancies in patients with diabetes treated with insulin detemir: a meta-analysis.
Diabetologia, 52, 2507-2512
Garg, S., Ampudia-Blasco, F. J., & Pfohl, M. (2010). Rapid-acting insulin analogues in Basal-bolus
regimens in type 1 diabetes mellitus. Endocr Pract., 16, 486-505.
Garg, S., Moser, E., Dain, M. P., & Rodionova, A. (2010). Clinical experience with insulin glargine
in type 1 diabetes. Diabetes Technology & Therapeutics, 12, 835-846.
Home, P.D., & Lagarenne, P. (2009). Combined randomised controlled trial experience of
malignancies in studies using insulin glargine. Diabetologia, 52, 2499–2506.

15
Jonasson JM, Ljung R, Talback M, Haglund B, Gudbjornsdottir S, Steineck G. Insulin glargine use
and short-term incidence of malignancies-a population-based follow-up study in Sweden.
Diabetologia. 2009;52:1745–1754.
Kølendorf, K., Aaby, P., Westergaard, S., & Deckert, T. (1978). Absorption, effectiveness and side
effects of highly purified porcine NPH-insulin preparations (Leo). Eur J Clin Pharmacol., 14, 117-
124.
Lepore, M., Pampanelli, S., Fanelli, C., Porcellati, F., Bartocci, L., Di Vincenzo, A., Cordoni, C.,
Costa, E., Brunetti, P., & Bolli, G.B. (2000). Pharmacokinetics and pharmacodynamics of
subcutaneous injection of long-acting human insulin analog glargine, NPH insulin, and ultralente
human insulin and continuous subcutaneous infusion of insulin lispro. Diabetes, 49, 2142-2148.
Mannucci E, Monami M, Balzi D, et al. (2010). Doses of insulin and its analogues and cancer
occurrence in insulin-treated type 2 diabetic patients. Diabetes Care 33:1997–2003.
Monami, M., Marchionni, N., & Mannucci, E. (2009). Long-acting insulin analogues vs. NPH
human insulin in type 1 diabetes. A meta-analysis. Diabetes, Obesity & Metabolism, 11, 372-378.
Morden, N., Liu, S., Smith, J., Mackenzie, T., Skinner, J., & Korc, M. (2011). Further exploration of
the relationship between insulin glargine and incident cancer—a retrospective cohort study of
older Medicare patients. Diabetes Care, 34, 1965–1971.
Roach, P. (2008). New insulin analogues and routes of delivery: pharmacodynamic and clinical
considerations. Clin Pharmacokinet., 47, 595-610.
Rosenstock, J., Fonseca, V., McGill, J.B., et al. (2009). Similar risk of malignancy with insulin
glargine and neutral protamine Hagedorn (NPH) insulin in patients with type 2 diabetes: findings
from a 5 year randomised, open-label study. Diabetologia, 52, 1971–1973.
Roy, B., Chou, M.C., & Field, J.B. (1980). Time-action characteristics of regular and NPH insulin in
insulin-treated diabetics. J Clin Endocrinol Metab., 50, 475-479.
Ruiter, R., Visser, L.E., van Herk-Sukel, M.P.P., Coebergh, J.W.W., Haak, H.R., Geelhoed-
Duijvestijn, P.H., Straus, S.M.J.M., Herings, R.M.C., & Ch. Stricker, B.H. (2012). Risk of cancer in
patients on insulin glargine and other insulin analogues in comparison with those on human
insulin: results from a large population-based follow-up study. Diabetologia, 55, 51–62.
Rys, P., Pankiewicz, O., Lach, K., Kwaskowski, A., Skrzekowska-Baran. I. & Malecki, M. T. (2011).
Efficacy and safety comparison of rapid-acting insulin aspart and regular human insulin in the
treatment of type 1 and type 2 diabetes mellitus: a systematic review. Diabetes & Metabolism,
37, 190-200.

16
Sanches, A. C. C., Correr, C. J., Venson, R., & Pontarolo, R. (2011). Revisiting the efficacy of long-
acting insulin analogues on adults with type 1 diabetes using mixed-treatment comparisons.
Diabetes research and clinical practice, 94, 333-339.
Singh, S. R., Ahmad, F., Lal, A., Yu, C., Bai, Z., & Bpharm, H.B. (2009). Efficacy and safety of insulin
analogues for the management of diabetes mellitus: A meta-analysis. CMAJ, 180, 385-397.
Suissa, S., Azoulay, L., Dell'aniello, S., Evans, M., Vora, J., & Pollak, M. (2011). Long-term effects
of insulin glargine on the risk of breast cancer. Diabetologia, 54, 2254–2262.
Szypowska, A., Golicki, D., Groele, L., & Pankowska, E. (2011). Long-acting insulin analogue
detemir compared with NPH insulin in type 1 diabetes: a systematic review and meta-analysis.
Pol Arch Med Wewn, 121, 237-246.

17
Uitgangsvraag 3
Zijn fluctuaties in glucosewaarden onafhankelijk van het HbA1c geassocieerd met een
hoger risico op microvasculaire of macrovasculaire complicaties bij patiënten met DM1?
Inleiding
Het risico op overlijden van mensen met DM1 is sterk afgenomen, maar nog steeds verhoogd
ten opzichte van de algemene bevolking (Miller et al., 2012). De voornaamste doodsoorzaak is
cardiovasculair. Het HbA1c is gecorreleerd met het optreden van met name microvasculaire
complicaties. Echter, het HbA1c bij DM1 verklaart maar een deel van de variatie in het optreden
van diabetescomplicaties (DCCT). In de literatuur zijn er aanwijzingen dat juist fluctuaties in de
glucosewaarden een oorzaak kunnen zijn van oxidatieve stress en gecorreleerd zijn met
macrovasculaire complicaties, hoewel dit voornamelijk onderzocht is bij DM2 (Nalysnyk et al.,
2010).
Sinds het gebruik van continue glucosemeting (CGM) is duidelijk geworden dat er grote
fluctuaties in de glucosewaarden over de dag/nacht kunnen zijn, terwijl de 4-punts dagcurve
daar geen aanwijzingen voor geeft. Ook is bekend dat met pomptherapie de fluctuaties in de
glucosewaarden minder zijn dan bij een basis-bolus schema.
De vraag is of fluctuaties in de glucosewaarden medeverantwoordelijk kunnen zijn voor het
optreden van diabetes complicaties en dat er daarom, naast een zo normaal mogelijk HbA1c,
ook gestreefd moet worden naar zo weinig mogelijk fluctuaties over de dag.
Er is gezocht naar prognostische studies bij patiënten met DM1 waarin de associatie tussen het
optreden van glucosefluctuaties en het risico op micro- en macrovasculaire complicaties is
onderzocht. Er is gezocht in de database Medline, naar systematische reviews vanaf 1-1-2000, en
zonder beperking op study design naar vergelijkend onderzoek vanaf 1-1-2008. Uit het totaal van
120 treffers werd op basis van titel en abstract, één systematische review (Nalysnyk et al., 2010)
en één aanvullende studie geselecteerd (Lachin et al., 2008).

18
Samenvatting van de literatuur
Het systematische review (Nalysnyk et al., 2010) richt zich op evidence voor een relatie tussen
glucose variabiliteit en het optreden van complicaties bij mensen met DM1 en DM2. Van de acht
geïncludeerde studies uitgevoerd bij patiënten met DM1, beschrijven vijf studies de relatie
tussen glucose variabiliteit en het optreden van microvasculaire complicaties (Bragd et al., 2008;
Kilpatrick et al., 2006; Service & O’Brien, 2001; Moberg et al., 1994; Oyibo et al., 2002), twee
studies de relatie tussen glucose variabiliteit en macrovasculaire complicaties (Gordin et al.,
2008; Kilpatrick et al., 2008), terwijl in één studie een mogelijke relatie tussen glucose
variabiliteit en oxidatieve stress wordt onderzocht (Wentholt et al., 2008). De inclusiecriteria,
belangrijkste karakteristieken, methode van meting van fluctuaties en follow-up zijn beschreven
in de evidence tabel (zie bijlage). Zes van de acht studies gebruiken een directe uitkomstmaat
(micro-/ macroangiopathie), twee studies hebben een indirecte uitkomstmaat voor angiopathie:
arteriële stijfheid (Gordin et al., 2008) of de uitscheiding van prostaglandines in de urine (als
maat voor oxidatieve stress: Wentholt et al., 2008).
Slechts in twee (Bragd et al., 2008; Moberg et al., 1994) van de zeven studies met een directe
uitkomstmaat is sprake van een statistisch significante associatie tussen glucose variabiliteit en
het optreden van microvasculaire of macrovasculaire complicaties, die echter niet standhoudt na
multivariate correctie voor standaard risicofactoren. In geen van beide studies naar
macrovasculaire complicaties wordt een statistisch significante associatie met glucose
variabiliteit waargenomen. Tenslotte wordt ook geen relatie gevonden tussen glucose
variabiliteit en de uitscheiding van prostaglandines in de urine als maat voor oxidatieve stress.
De kwalitatief beste studie met langdurige follow-up (Kilpatrick et al., 2006) analyseert de
variatie in de glucosewaarden van de 7-pts dagcurves die elke drie maanden gemaakt werden in
de DCCT studie, en vindt geen significant verschil in fluctuaties tussen de patiënten met en
zonder microvasculaire complicaties. Ook niet wat betreft fluctuaties in pre- of postprandiale
glucosewaardes. In 2008 publiceerden dezelfde auteurs de DCCT-gegevens over de relatie tussen
glucose fluctuaties en macroangiopathie (Kilpatrick et al., 2008). Bij 34 mensen die een
macrovasculair event hadden gekregen werd, ook na correctie voor standaard risicofactoren,
geen relatie gevonden met HbA1c en de SDMBG (als maat voor glucose variatie), maar wel met
de gemiddelde glucosewaarde.
De overige studies zijn kleiner van omvang en hebben vaak over een korte periode fluctuaties in
glucosewaarden gemeten als “pars pro toto” over een langere periode. In het artikel van Lachin

19
et al. (2008) wordt daarnaast met behulp van additionele analyses aangetoond dat het eerder in
de DCCT gevonden verschil in complicaties bij eenzelfde HbA1c een gevolg waren van
statistische fouten.
Conclusies
HOOG
Er lijkt geen relatie te bestaan tussen glucose fluctuaties en het optreden van micro-
en macrovasculaire complicaties bij patiënten met type 1 diabetes.
A1 Nalysnyk et al., 2010
Overwegingen
Diabetische micro-angiopathie zoals retinopathie, neuropathie en nefropathie zijn specifiek voor
DM en dus gecorreleerd aan afwijkingen in het glucosemetabolisme. Ook bestaat er een
verhoogde kans op macro-angiopathie maar anders dan bij DM2, waarbij macroangiopathie
meestal al vooraf gaat aan afwijkingen in het glucosemetabolisme, treden deze afwijkingen pas
in een latere fase van de ziekte op. Alle complicaties hebben een relatie met verhoogde
glucosewaarden, hoewel niet iedereen met DM1 deze in dezelfde mate ontwikkelt. Blijkbaar zijn
er andere factoren behalve de glucosewaarde op zich die de aanleg voor complicaties bepalen.
Fluctuatie in de glucosewaarden meer dan het gemiddelde glucose over de dag werd
gesuggereerd als één van deze factoren. De grootste studie op het gebied van DM1 die hierover
iets kan zeggen vindt deze relatie niet (DCCT; Lachin et al., 2008). In de praktijk zijn de
glucosefluctuaties over de dag bij DM1 door de volledige afhankelijkheid van insuline veel groter
dan bij DM2. Gezien het veel vroeger en vaker voorkomen van macroangiopathie bij DM2 lijkt
het waarschijnlijker dat een andere factor dan fluctuatie in de glucosewaarden een belangrijke
oorzakelijke factor is.
Nu er meer mogelijkheden zijn om (near)normoglycaemie te bereiken (intensieve insuline
therapie met insulineanalogen en CSII) lijkt het op fysiologische gronden toch logisch te streven
naar een zo normaal mogelijke glucoseregulatie. Het hebben van een goed HbA1c betekent
echter niet automatisch dat de glucosewaarden stabiel zijn. Eenzelfde HbA1c kan bij de ene
persoon stabiele regulatie betekenen, maar bij een ander het resultaat van hoge en lage
glucosewaarden met veel ongemak. Het gebruik van koolhydraat/insuline ratio’s en een

20
correctiefactor voor het corrigeren van een verhoogde bloedglucose gebaseerd op de
individuele gevoeligheid kunnen helpen om stabiliteit te krijgen. Ook het gebruik van een
“blinde” continue glucosemeting om te zien hoe de glucosewaarden variëren over de dag en
welke factoren dit bepalen kan inzicht geven en een hulpmiddel zijn om het insulineregime
(vooral bij CSII, maar ook bij een basis/bolusschema) te optimaliseren. Het optreden van ernstige
hypoglycaemie en hypoglycaemie-unawareness zijn echter belemmerende factoren hierbij. Het
dagelijks en frequent meten van glucosewaarden is voor veel mensen met DM1 een zware
belasting. Een ‘super intensieve’ behandeling met als doel om naast een goede glycemische
regulatie te bereiken (op grond van HbA1c), ook de glucose-fluctuaties weg te nemen, kan dus
ten koste gaan van de veiligheid. Tezamen met het gebrek aan bewijs dat behandeling van
glucose-fluctuaties tot vermindering van incidentie van complicaties leidt, maakt dat de
commissie adviseert terughoudend te zijn om de glycemische regulatie verder te optimaliseren
als er op grond van HbA1c een goede regulatie is bereikt. Methodes als CGM, boluswizard
etcetera kunnen wel een zinvol hulpmiddel zijn bij de diagnostiek en behandeling van DM1
patiënten die nog geen goede glycemische regulatie hebben bereikt.
Aanbevelingen
Streef bij het behandeldoel om micro- en macrovasculaire complicaties zoveel mogelijk te
voorkomen of uit te stellen, naar een goede glycemische regulatie, gebaseerd op een HbA1c
binnen de per patiënt (door arts en patiënt) overeengekomen streefwaarde.
Overweeg een verdergaande behandeling van glucose-fluctuaties als de patiënt deze fluctuaties
als hinderlijk of belemmerend voor het dagelijks functioneren ervaart.

21
Literatuur
Bragd, J., Adamson, U., Bäcklund, L.B., Lins, P.E., Moberg, E., & Oskarsson, P. (2008). Can
glycaemic variability, as calculated from blood glucose self-monitoring, predict the development
of complications in type 1 diabetes over a decade? Diabetes Metab., 34, 612-616.
Gordin, D., Rönnback, M., Forsblom, C., Mäkinen, V., Saraheimo, M., & Groop, P.H. (2008).
Glucose variability, blood pressure and arterial stiffness in type 1 diabetes. Diabetes Res Clin
Pract., 80, e4-7.
Kilpatrick, E.S., Rigby, A.S., & Atkin, S.L. (2006). The effect of glucose variability on the risk of
microvascular complications in type 1 diabetes. Diabetes Care, 29, 1486-1490.
Kilpatrick, E.S., Rigby, A.S. & Atkin, S.L. (2008). Mean blood glucose compared with HbA1c in the
prediction of cardiovascular disease in patients with type 1 diabetes. Diabetologia, 51, 365-371.
Lachin, J.M., Genuth, S., Nathan, D. M., Zinman, B., Rutledge, B. N., & DCCT/EDIC Research
Group. (2008). Effect of glycemic exposure on the risk of microvascular complications in the
diabetes control and complications trial--revisited. Diabetes, 57, 995-1001.
Miller, R.G., Secrest, A.M., Sharma, R.K., Songer, T.J., & Orchard, T.J. (2012). Improvements in
the life expectancy of type 1 diabetes: the Pittsburgh Epidemiology of Diabetes Complications
study cohort. Diabetes, 61, 2987-92.
Moberg, E.A., Lins, P.E., & Adamson, U.K. (1994). Variability of blood glucose levels in patients
with type 1 diabetes mellitus on intensified insulin regimens. Diabete Metab., 20, 546-552.
Nalysnyk, L., Hernandez-Medina, M., & Krishnarajah, G. (2010). Glycaemic variability and
complications in patients with diabetes mellitus: evidence from a systematic review of the
literature. Diabetes, Obesity & Metabolism, 12, 288-98.
Oyibo, S.O., Prasad, Y.D., Jackson, N.J., Jude, E.B., & Boulton, A.J. (2002). The relationship
between blood glucose excursions and painful diabetic peripheral neuropathy: a pilot study.
Diabet Med., 19, 870-873.
Service, F.J., & O'Brien, P.C. (2001). The relation of glycaemia to the risk of development and
progression of retinopathy in the Diabetic Control and Complications Trial. Diabetologia, 44,
1215-20. Erratum in: Diabetologia 45:936.
Wentholt, I.M., Kulik, W., Michels, R.P., Hoekstra, J.B., & DeVries, J.H. (2008). Glucose
fluctuations and activation of oxidative stress in patients with type 1 diabetes. Diabetologia, 51,
183-190.

22
Uitgangsvraag 4
Wanneer starten met een statine bij volwassenen met T1DM: bij welke risicofactoren, en
op welke leeftijd?
Inleiding
De richtlijnen voor het voorschrijven van statines bij mensen met DM2 zijn helder en breed
geaccepteerd: ‘Ja, tenzij’. Volgens de NHG-standaard type 2 diabetes dient hierbij gestreefd te
worden naar een LDL < 2.5 mmol/l of een totaal cholesterol < 4.5 mmol/l. Bij mensen met DM1
zijn de aanbevelingen ten aanzien van het voorschrijven van statines minder eenduidig in de
internationale richtlijnen. Zo hanteren de ADA en SIGN een leeftijdsgrens van boven de 40 jaar.
Hierbij moet er volgens de ADA dan ook nog een cardiovasculaire risicofactor aanwezig zijn,
terwijl er bij SIGN zelfs sprake moet zijn van cardiovasculaire comorbiditeit. Verder is de aan-
/afwezigheid van microalbuminurie in sommige richtlijnen ook een extra argument om een
statine voor te schrijven bij mensen met DM1.
Er is gezocht naar literatuur waarin wordt bekeken wanneer het starten van
cholesterolverlagende therapie zinvol is bij patiënten met DM1, teneinde cardiovasculaire
morbiditeit en mortaliteit te voorkomen. Er is gezocht vanaf 1-1-2004 op systematische reviews,
RCT’s en ander vergelijkend onderzoek in de databases Medline, Embase en de Cochrane
Library. Uit het totaal van 102 treffers werd op basis van titel en abstract, één artikel
geselecteerd. Het betreft een meta-analyse uit 2008 van de Cholesterol Treatment Trialists’(CTT)
Collaborators. De zoekactie leverde geen relevante recentere RCT’s op.
Samenvatting van de literatuur
De zoekactie leverde één meta-analyse op, verricht door de Cholesterol Treatment Trialists’
(CTT) Collaborators, waarin data van 18.686 individuen met diabetes (1466 met type 1 en 17.220
met type 2) worden onderzocht in de context van 71.370 patiënten zonder diabetes in 14
gerandomiseerde trials over statine therapie (Cholesterol Treatment Trialists’ (CTT)
Collaborators, 2008).
De resultaten van een meta-analyse van deze 14 gerandomiseerde statine-trials toonden eerder
dat verlaging van het LDL-cholesterol met 1 mmol/l het risico op major vascular events

23
(gedefinieerd als het samengestelde eindpunt van myocardinfarct, overlijden ten gevolge van
coronairlijden, coronaire revascularisatie of beroerte) met ongeveer een vijfde verlaagde, in een
grote groep van hoog-risico patiënten, grotendeels onafhankelijk van het basale lipidenprofiel of
andere karakteristieken zoals diabetes.
Om in deze groep met diabetespatiënten het afzonderlijke effect van statines op nieuwe
cardiovasculaire events te onderzoeken, alsmede het effect van statines bij diabetespatiënten
zonder bekende vaatziekten, werd de huidige meta-analyse verricht onder de 18.686 patiënten
met diabetes in de 14 statine trials die aan de CTT-meta-analyse deelnamen. De inclusiecriteria
en de geselecteerde studies staan beschreven in de evidence-tabel (zie bijlage). Aangezien
behandeling met een statine een internationaal geaccepteerde standaard is voor secundaire
preventie bij zowel mensen met als zonder diabetes, werd bij de beoordeling van de literatuur
vooral gelet op primaire preventie bij DM1.
Van alle 14 studies zijn de individuele data van deelnemende patiënten met diabetes
beschikbaar en meegenomen in een meta-analyse. In drie van de 14 studies gaat het alleen om
type 2 diabetespatiënten, in de overige 11 zijn in totaal 1466 type 1 diabetespatiënten
onderzocht, variërend van 3 tot 615 (Heart Protection Study Collaborative Group, 2002) per
studie. Hiervan hebben 827 patiënten een voorgeschiedenis van cardiovasculaire ziekte en
betreft het dus secundaire preventie. Bij de overige 639 patiënten is sprake van primaire
preventie, waarvan het merendeel afkomstig is uit de Heart Protection Study, 2002. De
gemiddelde follow-up duur is 4,3 jaar (1,9-5,6 jaar).
Studie deelnemers met diabetes hebben per mmol/l LDL-cholesterol reductie een niet-
significante 9% reductie in all-cause mortality (RR 0.91, 99% BI 0.82-1.01; p=0.02), en een
significante 21% reductie van de incidentie van een nieuw cardiovasculaire event (0.79, 99% BI
0.72-0.86; p<0.0001). Het effect is vergelijkbaar voor patiënten met en zonder symptomatische
cardiovasculaire ziekte in de voorgeschiedenis, met en zonder hypertensie, en ongeacht de
uitgangswaarde van het LDL-cholesterol, geslacht, leeftijd, BMI, roken en eGFR.
In de subgroep met type 1 diabetes wordt in de statine groep per mmol/l verlaging van LDL-
cholesterol een reductie gezien in nieuwe cardiovasculaire events (0.79, 99% BI 0.62-1.01;
p=0.01). Let wel, vanwege de herhaaldelijke onderverdeling van data werd gekozen voor de
strenge alpha van 0,01. Verder werd er in de groep type 1 diabetes geen onderscheid gemaakt
tussen primaire preventie en secundaire preventie.
In de meta-analyse van alle patiënten uit de eerste CTT-cyclus, gaf behandeling met een statine
geen verhoging van het risico op non-vasculair overlijden of kanker wanneer een matige dosis

24
werd gebruikt gedurende vijf jaar. Voor de deelnemers met diabetes gold hetzelfde. Tevens
werd geen verhoogde incidentie van rhabdomyolyse gerapporteerd.
Volgens de auteurs is statine therapie alleen onwenselijk wanneer er dwingende redenen zijn
om de therapie niet toe te passen, zoals bij zorgen over de veiligheid (bijvoorbeeld in de
zwangerschap) of bij een laag korte termijn absoluut risico op cardiovasculaire ziekten (zoals bij
kinderen met type 1 diabetes).
Conclusies
HOOG
Behandeling met een statine leidt niet tot een afname van de totale mortaliteit,
maar wel tot een reductie van nieuwe cardiovasculair events bij patiënten met
diabetes mellitus type 1 (gecombineerde primaire en secundaire preventie).
Cholesterol Treatment Trialists’ (CTT) Collaborators, 2008
MATIG
Het is niet bewezen voor type 1 diabetes dat behandeling met een statine leidt tot
vermindering van cardiovasculaire events in het kader van primaire preventie.
Cholesterol Treatment Trialists’ (CTT) Collaborators, 2008
Overwegingen
Hoewel de overgrote meerderheid van de deelnemers van de CTT meta-analyse type 2 diabetes
heeft, is er geen bewijs dat de effecten van behandeling met een statine op cardiovasculaire
events bij patiënten met type 1 diabetes verschillen van degenen met type 2. In de
bovengenoemde meta-analyse is de reductie van events bij type 1 diabetes bij een strenge alpha
van 0,01 net niet statistisch significant (bij een alpha van 0,05 zou wel statistische significantie
zijn bereikt). Er wordt dus toch enige suggestie gewekt dat het behandelen met een statine
zinvol zou kunnen zijn.
De ADA richtlijn adviseert behandeling met een statine, naast lifestyle adviezen, onafhankelijk
van baseline cholesterolwaarden, voor alle diabetespatiënten met evidente cardiovasculaire

25
comorbiditeit, en voor patiënten zonder cardiovasculaire comorbiditeit die ouder zijn dan 40 jaar
en één of meer cardiovasculaire risicofactoren hebben (level of evidence A). Voor patiënten met
een lager risico en een leeftijd onder de 40 jaar kan behandeling met een statine worden
overwogen wanneer het LDL-cholesterol hoger dan 100mg/dL (2.6 mmol/l) blijft ondanks
lifestyle interventie of bij meerdere cardiovasculaire risicofactoren (expert opinion). De ADA
maakt in hun aanbevelingen geen onderscheidt tussen type 1 en type 2 diabetes.
De aanbevelingen uit bestaande Nederlandse cardiovasculaire risicomanagement adviezen voor
mensen met en zonder diabetes komen al grotendeels overeen met bovenstaande ADA richtlijn,
zeker voor secundaire preventie.
Tot slot dient in de overwegingen te worden meegenomen dat de Heart Protection Study (Heart
Protection Study Collaborative Group, 2002) heeft laten zien dat een generieke statine die leidt
tot een gemiddelde LDL-cholesterol reductie van 1 mmol/l al kosten-effectief is bij patiënten die
een cardiovasculair risico hebben van 1% per jaar. Dit suggereert dat statines waarschijnlijk
kosten-effectief zijn voor vrijwel alle diabetespatiënten en kan meegenomen worden in de
overweging om een statine voor te schrijven.
Ten aanzien van de veiligheid kan gezegd worden dat uit eerdere CTT-meta-analyses geen
duidelijke nadelige effecten van behandeling met statines aan het licht zijn gekomen.
Wel dient bij vrouwen in de fertiele leeftijd en zeker onder de 40 jaar rekening gehouden te
worden met de contra-indicatie voor statines bij zwangerschap. Zwangerschapswens en kans op
ongeplande zwangerschap (anticonceptie) zou actief besproken moeten worden bij de
overweging tot start behandeling met een statine.
Aanbevelingen
Behandel in geval van secundaire preventie patiënten met type 1 diabetes met
cholesterolverlagende therapie in de vorm van een statine.
Behandel in geval van primaire preventie patiënten met type 1 diabetes met een statine bij een
leeftijd boven de 40 jaar én aanwezigheid van één of meerdere cardiovasculaire risicofactoren.
Overweeg behandeling met een statine bij patiënten onder de 40 jaar en meerdere
cardiovasculaire risicofactoren óf een LDL >2,5mmol/l.

26
Wees erg terughoudend met behandeling met statines bij vrouwen onder de 40 jaar.
Literatuur
Cholesterol Treatment Trialists’ (CTT) Collaborators. (2008). Effi cacy of cholesterol-lowering
therapy in 18 686 people with diabetes in 14 randomised trials of statins: a meta-analysis.
Lancet, 371, 117–125.
Cholesterol Treatment Trialists’ (CTT) Collaborators. (2010). Efficacy and safety of more intensive
lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised
trials. Lancet, 376, 1670-1681.
Heart Protection Study Collaborative Group. (2002). Heart Protection Study of cholesterol
lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial.
Lancet, 360, 7-22.
Miller, R. G., Secrest, A. M., Sharma, R. K., Songer, T. J., & Orchard, T. J. (2012). Improvements in
the life expectancy of type 1 diabetes: the Pittsburgh Epidemiology of Diabetes Complications
study cohort. Diabetes, 61, 2987-92.

27
Uitgangsvraag 5
Is toevoeging van metformine aan insulinetherapie van meerwaarde bij volwassen
patiënten met DM1?
Inleiding
Metformine is geneesmiddel van eerste keus bij patiënten met DM2, conform Nederlandse
(NHG) en buitenlandse richtlijnen (NICE, ADA, IDF). Naast het feit dat metformine goedkoop is en
het risico op hypoglycemieën laag, heeft metformine deze eerste keus ook te danken aan
gunstige effecten op vermindering van cardiovasculaire incidenten bij DM2, welke behouden
blijven tot in ieder geval 10 jaar na het einde van de interventie studie (Holman et al., 2008).
Metformine vermindert de glucoseproductie in de lever door remming van de gluconeogenese
en glycogenolyse. Daarnaast neemt de perifere gevoeligheid van insuline toe. Metformine lijkt
derhalve vooral van meerwaarde bij patiënten met overgewicht en insulineresistentie, en wordt
bij DM2 frequent gecombineerd met insulinetherapie. Ook bij mensen met DM1 komt
insulineresistentie voor. De vraag is of het toevoegen van metformine aan de standaard
insulinebehandeling bij DM1 van meerwaarde is, zoals verbetering van metabole controle,
vermindering van totale dagelijkse insulinedosis en verminderen van cardiovasculaire
incidenten.
Er is gezocht naar literatuur waarin de effectiviteit van metformine en placebo wordt vergeleken
bij patiënten met DM1, op glycemische controle (HbA1c) en totale dagelijkse insulinedosis (TDI),
cardiovasculaire morbiditeit en mortaliteit, en bijwerkingen als uitkomstmaat. Er is gezocht
vanaf 1-1-2008 op systematische reviews en RCT’s, in de databases Medline, Embase en the
Cochrane Library. Uit het totaal van 36 treffers werden op basis van titel en abstract, twee
artikelen geselecteerd. Het betreft systematische reviews van studies gepubliceerd tot augustus
2008 (Abdelghaffar & Attia, 2009), en tot oktober 2009 (Vella et al., 2010). De zoekactie leverde
geen relevante recentere RCT’s op.
Samenvatting van de literatuur
De zoekactie leverde twee systematische reviews op (Abdelghaffar & Attia, 2009; Vella et al.,
2010). Het Cochrane review (Abdelghaffar & Attia, 2009) richt zich op de effectiviteit van

28
metformine bij adolescenten met DM1, en includeert twee RCT’s (Hamilton et al., 2003;
Särnblad et al., 2003). Het tweede en recentere systematische review (Vella et al., 2010) richt
zich op alle patiënten met DM1, en includeert naast de twee eerdergenoemde studies nog zeven
RCT’s, waarvan zes uitgevoerd bij volwassenen. De inclusiecriteria van Vella et al. (2010) en de
belangrijkste karakteristieken van de geselecteerde studies zijn te vinden in de evidence-tabel
(zie bijlage). In vrijwel alle gevallen gaat het om patiënten met DM1 en een matige metabole
controle (HbA1c ≥ 8%). Drie van de negen geïncludeerde RCT’s zijn cross-over studies waarin
patiënten in opeenvolgende periodes zowel de interventie als controlebehandeling ondergaan,
de overige zes studies hebben een parallel design. De studiegrootte varieert tussen acht en
honderd deelnemers, en de studieduur van zeven dagen tot twaalf maanden. Geen van de
studies analyseert cardiovasculaire morbiditeit of mortaliteit. In zeven van de negen studies
werden HbA1c en de totale dagelijkse insulinedosis, als maten voor de glycemische controle en
insulinegevoeligheid, vergeleken tussen metformine- en placebogroep. Het gebruik van
metformine (1000 tot 2000 mg per dag) was geassocieerd met een statistisch significante
reductie in HbA1c van 0,6-0,9% in vier van de zeven studies, p<0,05 (follow-up 3-4 maanden). In
de overige drie studies, met follow-up van 6-12 maanden, was het verschil tussen metformine-
en placebogroep statistisch niet significant. Daarnaast was in zes van de zeven studies, de totale
insulinedosis gereduceerd in de metforminegroep ten opzichte van de placebogroep met 5,7-
10,1 units/dag (p<0,05), in één studie was het verschil niet significant.
Een meta-analyse werd mogelijk na exclusie van twee studies met een studieduur korter dan
één maand (Gin et al., 1985; Keen et al., 1987) en twee studies met onvoldoende details over
HbA1c en insuline dosis (Walravens et al., 2000; Khan et al., 2006). In de vijf studies geïncludeerd
in de meta-analyse (Meyer et al., 2002; Särnblad et al., 2003; Hamilton et al., 2003; Lund et al.,
2008; Jacobsen et al., 2009) varieert de studieduur tussen drie en twaalf maanden. De meta-
analyse geeft een statistisch niet significante reductie te zien in Hb1Ac in de metforminegroep
ten opzichte van de placebogroep (Figuur 1; gestandaardiseerd verschil van gemiddelden, SMD;
SMD= 0,10; 95% BI= [0,36; 0,16]), die overeenkomt met een absolute reductie in HbA1c met
0,11% (p=0,42). De meta-analyse geeft wel een statistisch significante reductie in de totale
dagelijkse insulinedosis (TDI) van patiënten in de metforminegroep ten opzichte van de
placebogroep (Figuur 2; SMD= 0,65; 95% BI= [0,92; 0.39]). De reductie in insulinebehoefte in
de metforminegroep ten opzichte van de placebogroep komt overeen met 6,6 E/dag (p<0,001).
Hoewel statisch significant, is het twijfelachtig of een dergelijke beperkte afname in TDI klinisch
relevant is. Meyer et al. (1999) noemt bijvoorbeeld een 20% reductie in TDI succesvol. In

29
bovenbeschreven studies is de gemiddelde dagdosis insuline rond de 1E/kg lichaamsgewicht, wat
neerkomt op maximaal 10% daling in insulinedosis.
Figuur 1 Vergelijking in effectiviteit tussen metformine en placebo. Effectiviteit is gebaseerd op
een vergelijking van HbA1c waardes (standardized mean difference, MSD).
Figuur 2 Vergelijking in effectiviteit tussen metformine en placebo. Effectiviteit is gebaseerd op
een vergelijking van de insulinebehoefte, de totale dagelijkse insulinedosis
(standardized mean difference, MSD).
In zeven van de negen RCT’s wordt de incidentie of frequentie van hypoglycemische episodes
vergeleken tussen de metformine- en placebogroep. De kans op een hypoglycemische episode
lijkt enigszins verhoogd in de metforminegroep, maar bereikt vrijwel nooit statistische
significantie (zie evidence-tabel). In de RCT met de grootste omvang en studieduur (Lund et al.,
2008), is de frequentie van milde hypoglycemie (per patiënt per maand) 9,0 in de
metforminegroep versus 6,4 in de placebogroep (p=0,3; statistisch niet significant). Een ernstige
hypoglycemische episode kwam voor bij 31% van de patiënten in de metforminegroep versus
20% in de placebogroep (p=0,2; statistisch niet significant), waarbij bewusteloosheid optrad in
10 versus 2 gevallen (p<0,05). Het aantal patiënten dat gastrointestinale bijwerkingen
rapporteert was vergelijkbaar tussen de behandelgroepen (43 versus 39; p=0,3; statistisch niet

30
significant). Cardiovasculaire symptomen waren zeldzaam en de incidentie verschilde niet
significant tussen metformin- en placebogroep. Geen van de studies rapporteert lactaat acidose
als mogelijke complicatie.
Bij beoordelen van de studies volgens GRADE is de bewijskracht matig voor effecten van
metformine behandeling op de totale dagelijkse insulinedosis, er is één punt afgetrokken
vanwege ernstige imprecisie (kleine studiegrootte, ook na poolen in de meta-analyse). Bij het
bepalen van de bewijskracht voor de effecten van metformin op HbA1c en het optreden van
bijwerkingen, is een tweede punt afgetrokken voor imprecisie omdat de
betrouwbaarheidsintervallen het nuleffect omvatten. De studiepopulaties bestonden vrijwel
geheel uit patiënten met DM1 met een matige metabole controle. Onbekend is de effectiviteit
van metformine bij DM1 patienten die een goede metabole controle bezitten. Door de korte
duur van de RCT’s kan ook geen uitspraak worden gedaan over de effectiviteit van metformine
behandeling op de langere termijn. Tenslotte is door de korte duur en geringe omvang van de
RCT’s onbekend of metformine de verhoogde cardiovasculaire morbiditeit en mortaliteit van
patiënten met DM1 verlaagt.
Conclusies
LAAG
Metformine behandeling bij patiënten met type 1 diabetes en een matige metabole
controle leidt niet tot reductie van HbA1c.
De effectiviteit van metformine op de langere termijn (> 1 jaar) is onbekend.
De effectiviteit van metformine bij patiënten met type 1 diabetes en een goede
metabole controle is onbekend.
Vella et al., 2010; Abdelghaffar & Attia, 2009; Walravens et al., 2000; Meyer et al.,
2002; Hamilton et al., 2003; Särnblad et al., 2003; Khan et al., 2006; Lund et al.,
2008; Jacobsen et al., 2009
MATIG
Metformine behandeling van patiënten met type 1 diabetes en een matige
metabole controle leidt tot een beperkte reductie in de dagelijkse insulinebehoefte.

31
De effectiviteit van metformine op TDI is op de langere termijn (> 1 jaar) onbekend
De effectiviteit van metformine op TDI bij patiënten met type 1 diabetes en een
goede metabole controle is onbekend.
Vella et al., 2010; Abdelghaffar & Attia, 2009; Walravens et al., 2000; Meyer et al.,
2002; Hamilton et al., 2003; Särnblad et al., 2003; Khan et al., 2006; Lund et al.,
2008; Jacobsen et al., 2009
LAAG
Metformine behandeling bij patiënten met type 1 diabetes en een matige metabole
controle leidt tot een licht verhoogde kans op hypoglycemische episodes.
Vella et al., 2010; Abdelghaffar & Attia., 2009; Keen et al., 1987; Meyer et al., 2002;
Hamilton et al., 2003; Särnblad et al., 2003; Khan et al., 2006; Lund et al., 2008;
Jacobsen et al., 2009
No Grade
De effecten van metformine behandeling van patiënten met type 1 diabetes op
cardiovasculaire morbiditeit en mortaliteit zijn onbekend.
De langetermijneffecten van metformine op andere belangrijke klinische
eindpunten bij patiënten met type 1 diabetes zijn eveneens onbekend.
Vella et al., 2010; Abdelghaffar & Attia, 2009
Overwegingen
Alleen korte termijn studies (<4mnd) tonen een klinisch relevante reductie in Hba1c van 0,6-
0,9% in de metfomine groep. Twee van de drie langere termijn studies, 6-12 maanden (Lund et
al., 2008; Walravens et al., 2000) laten eveneens een significante reductie zien van het HbA1c
(0,5-0,7%) in de metformine groep na drie maanden follow-up; echter is deze reductie na 6-12

32
maanden volledig verdwenen. Metformine toevoegen ter verbetering van de lange termijn
glycemische controle lijkt dus niet zinvol. Toevoeging van metformine bleek wel de totale
dagdosis insuline (TDI) significant te verlagen (6.6 E/dag). Het is sterk de vraag of deze reductie
in TDI klinisch relevant is bij iemand die 4x daags insuline spuit. Echter 6.6 E/dag is natuurlijk een
gemiddelde, voor een individuele patiënt zou dit meer kunnen zijn.
De studie van Särnblat et al. (2003) bij 26 adolescenten (13 per groep), suggereert dat de
insulinegevoeligheid bij de metformine groep is toegenomen na drie maanden behandeling,
bepaald met behulp van een hyperinsulinemische euglycemische clamp. Verder laat de studie
van Meyer et al. (2002; 62 T1D behandeld met CSII, n=31 per behandelgroep, metformine
1700mg vs. placebo, follow-up 6 maanden) zien dat 23% in de metformine groep vs. 0% in de
placebogroep ‘succesvolle responders’ waren (gedefinieerd als een reductie in TDI van >20%,
met stabiel of dalend HbA1c en uitblijven van ernstige hypoglycemieën). De dagdosis basale
insuline was significant afgenomen in de metformine groep, de prandiale dagdosis daalde niet-
significant. Dit pleit ervoor dat metformine ook bij DM1 de hepatische glucose productie kan
verminderen. Hoewel dus een verlaging van 6.6 E/dag niet klinisch relevant lijkt, suggereren de 2
bovengenoemde studies, dat het voor een individuele patiënt, degene met bijvoorbeeld hogere
nuchtere glucoses en/of hoge basale insuline behoefte, voordeel kan hebben om metformine
toe te voegen aan het insuline regime. Dit zouden mensen met DM1 en ook kenmerken van het
metabole syndroom (“double diabetes”) kunnen zijn.
Bij de beslissing om metformine toe te voegen aan insulinetherapie kan verder nog gekeken
worden naar veiligheid. Ten aanzien van de veiligheid is het aantal hypoglycemieën licht
toegenomen na toevoeging van metformine, waarbij dit alleen significant was voor
hypoglycemieën met bewusteloosheid tot gevolg (2 vs. 10 gevallen over studieduur van 1 jaar),
(Lund et al.,2008). Verder is van metformine bekend dat het een verhoogd risico geeft op lactaat
acidose. In geen van de beoordeelde studies wordt hierover iets beschreven. Het risico op
lactaat acidose dient meegenomen te worden in de besluitvorming om een patiënt met DM1
met metformine te behandelen bij risicoverhogende omstandigheden, zoals
nierfunctiestoornissen, hartfalen of dehydratie.
Omdat lange termijn metformine studies bij patiënten met DM1 ontbreken, kan het effect van
metformine op incidentie van cardiovasculaire events en kankerincidentie niet worden
beoordeeld.

33
Aanbevelingen
Voeg geen metformine toe aan de standaard insulinetherapie bij type 1 diabetes om de
metabole controle te verbeteren.
Overweeg in individuele gevallen metformine toe te voegen aan insuline therapie, met name
wanneer er ook kenmerken zijn van een metabool syndroom.
Literatuur
Abdelghaffar, S., & Attia, A.M. (2009). Metformin added to insulin therapy for type 1 diabetes
mellitus in adolescents. Cochrane Database Syst Rev, 1, CD006691.
Gin, H., Messerchmitt, C., Brottier, E., & Aubertin, J. (1985). Metformin improved insulin
resistance in type I, insulin-dependent, diabetic patients. Metabolism, 34, 923–925.
Hamilton, J., Cummings, E., Zdravkovic, V., Finegood, D., & Daneman, D. (2003). Metformin as an
adjunct therapy in adolescents with type 1 diabetes and insulin resistance: a randomized
controlled trial. Diabetes Care, 26, 138–143.
Holman, R.R., Paul, S.K., Bethel, M.A., Matthews, D.R., & Neil, H.A. (2008). 10-year follow-up of
intensive glucose control in type 2 diabetes. N Engl J Med., 359, 1577–1589.
IDF Clinical Guidelines Task Force. (2005). Global guideline for Type 2 diabetes. Brussels:
International Diabetes Federation.
Jacobsen, P.K., Lund, S.S., & Tarnow, L. (2007). Impact of metformin treatment on glycaemic
control and cardiovascular risk-factors in patients with poorly controlled type 1 diabetes (T1DM).
Diabetologia, 50(1), S107.
Keen, H., Collins, A.C.G., & Bending, J.J. (1987). Metformin increases response to insulin in type-1
(insulin-dependent) diabetes. Diabetologia, 30, A538.
Khan, A.S., McLoughney, C.R., & Ahmed, A.B. (2006). The effect of metformin on blood glucose
control in overweight patients with type 1 diabetes. Diabet Med., 23, 1079–1084.

34
Lund, S.S., Tarnow, L., Astrup, A.S., Hovind, P., Jacobsen, P.K., Alibegovic, A.C., Parving, I.,
Pietraszek, L.,…. (2008). Effect of adjunct metformin treatment in patients with type-1 diabetes
and persistent inadequate glycaemic control. A randomized study. PLoS One, 3, e3363.
Meyer, L., Delbachian, I., Lehert, P., Cugnardey, N., Drouin, P., & Guerci, B. (1999). Continuous
subcutaneous insulin infusion in type 1 diabetes: insulin-sparing effect of metformin.
Diabetologia, 42(1), A226.
Nathan, D.M., Buse, J.B., Davidson, M.B., Ferrannini, E., Holman, R.R., Sherwin, R., Zinman, B. &
American Diabetes Association; European Association for Study of Diabetes. (2009). Medical
management of hyperglycaemia in type 2 diabetes mellitus: a consensus algorithm for the
initiation and adjustment of therapy. A consensus statement from the American Diabetes
Association and the European Association for the Study of Diabetes. Diabetologia, 52, 17–30.
National Collaborating Centre for Chronic Conditions (UK). (2008). Type 2 Diabetes: National
Clinical Guideline for Management in Primary and Secondary Care (Update). London: Royal
College of Physicians (UK). (NICE Clinical Guidelines, No. 66.). http://www.nice.org.uk
Särnblad, S., Kroon, M., & Aman, J. (2003). Metformin as additional therapy in adolescents with
poorly controlled type 1 diabetes: randomised placebo-controlled trial with aspects on insulin
sensitivity. Eur J Endocrinol., 149, 323–329.
Vella, S., Buetow, L., Royle, P., Livingstone, S., Colhoun, H. M., & Petrie, J.R. (2010). The use of
metformin in type 1 diabetes: a systematic review of efficacy. Diabetologia, 53, 809-820.
Walravens, P.A., Chase, P.H., Klingensmith, G.J., Ellison, M., Cornell, C., & Monahan, K. (2000).
Low dose metformin in adolescents with type 1 diabetes mellitus: a double blind, controlled
study. Diabetes, 49(1), A128.

35
Uitgangsvraag 6
Heeft het gebruik van e-health meerwaarde op de uitkomst van de behandeling van
patiënten met DM1?
Inleiding
Sinds de wijde beschikbaarheid van internet zijn de mogelijkheden voor e-health toegenomen.
E-health is het toepassen van informatie- en communicatietechnologie ten dienste van de
gezondheidszorg. Naast begeleiden van mensen met chronische aandoeningen via internet met
uitwisseling van gegevens (bijvoorbeeld bloedglucose dagcurve) en adviezen (aanpassing
insuline dosering), kan bijvoorbeeld ook van mobiele telefonie gebruik worden gemaakt, zoals
het sturen van een SMS-alert de dag voor een poliklinische controleafspraak. Bij een chronische
aandoening zoals DM1 komen ‘compliance’ problemen regelmatig voor. E-health zou via diverse
technieken en projecten hierbij kunnen ondersteunen. Vooral in de jongere patiëntencategorie
zoals pubers en transitiegroepen zou e-health van grote meerwaarde kunnen zijn.
Er is gezocht naar systematische reviews en RCT’s bij patiënten met DM1 waarin een vorm van
telemedicine vergeleken werd met usual care. Er is gezocht in de databases Medline en Embase.
Uit het totaal van 149 treffers werden op basis van titel en abstract, 30 studies geselecteerd. Na
bestuderen van de full text werden 3 RCT’s en 1 systematic review geïncludeerd.
Samenvatting literatuur
Er zijn verschillende vormen van telemedicine onderzocht: alleen telefonische contacten,
systemen die transfer van bloedglucosewaarden naar de hulpverlener mogelijk maken met
retrospectieve feedback op de resultaten en PDA’s die automatische feedback geven
(bolusadvies, correctiefactor) met daarnaast telefonische feedback achteraf.
De systematic review van Franc et al. (2011) betreft veel zeer kleine studies bij over het
algemeen matig tot slechte diabetesregulatie. Het gebruik van devices met boluswizard en
correctiefactor tonen een significante en relevante HbA1c daling na 6 en 12 maanden indien
frequente upload naar de hulpverlener plaats vindt en feedback wordt gegeven binnen 24 uur
ten opzicht van usual care of het gebruik van de device zonder feedback.

36
In de studie van McCarrier et al. (2009) bestond de telemedicine uit een web-based programma
met de volgende elementen: eigen medische gegevens, mogelijkheid tot uploaden van
glucosewaarden naar een viewer voor zowel patiënt als hulpverlener, dagboek voor registratie
van genomen medicatie, voeding, activiteiten etcetera, een actieplanner voor verbetering self-
efficacy en zelfmanagement en een educatie site. De HbA1c daling in the interventie groep was
0,37%, de controle groep steeg 0,11%. Het verschil tussen de groepen was statistisch niet
significant. Hierbij moet vermeld worden dat tweederde van de deelnemers al vooraf een HbA1c
tussen 7 en 8% had. Hoewel vooraf een onderscheid gemaakt wordt tussen mensen met een
HbA1c<8% en >8% wordt niet gemeld of er een verschil in HbA1c daling tussen deze twee
groepen optrad. Mogelijk waren de aantallen hiervoor ook te klein.
De studie van Rossi et al. (2010) vergeleek een PDA met app voor KH berekening, boluswizard en
correctiefactor met conventionele educatie over het rekenen met koolhydraten, KH/I ratio en
correctiefactor. Beide groepen verbeterden evenveel in HbA1c. De PDA met app was minder
kostbaar in tijd en gaf een significant betere tevredenheid over de behandeling (WHO-DTSQ-
score). De mensen in de PDA groep bleven stabiel wat betreft gewicht, de controle groep kwam
gemiddeld 1,5kg aan in gewicht, doch dit verschil was statistisch niet significant.
De studie van Charpentier et al. (2011) betrof een PDA met boluswizard en correctiefactor
waarbij niet alleen koolhydraten maar ook activiteiten kunnen worden ingevoerd (Diabeo). De
interventie van zes maanden betrof ofwel alleen zelf met het Diabeo systeem werken of dit in
combinatie met tweewekelijkse telefonische contacten met de hulpverlener. De controle groep
kreeg de reguliere driemaandelijkse controles. Het HbA1c bij de start was in alle groepen gelijk
(9%). Aan het eind van de studie was het HbA1c in de groep die het Diabeo systeem gebruikte
gedaald naar 8,6%, in de groep die daarnaast ook regelmatig telefonische contacten onderhield
8,4%. De daling was alleen statistisch significant voor de laatste groep. De groep met alleen
Diabeo gebruik verbeterde ook, maar statistisch niet significant ten opzichte van de controle
groep. Opgemerkt wordt dat de beide interventie groepen in de zes maanden durende studie vijf
uur meer polikliniekbezoeken hadden dan de controlegroep in verband met invoeren en wijzigen
bolusadvies en correctiefactor.
Bij beoordelen van de studies volgens GRADE is de bewijskracht laag voor effecten van het
gebruik van e-health/telemedicine op glycemische regulatie; er is één punt afgetrokken vanwege
ernstige imprecisie (kleine studiegrootte, ook na poolen in de meta-analyse) en één punt voor de
korte follow-up. Ook voor het gebruik van een PDA voor het berekenen van KH, gebruik van

37
boluswizard en correctiefactor is de bewijskracht bewijs laag in verband met het (nog) kleine
aantal studies en de beperkte follow-up. Tevens bleek dat mondelinge educatie over het gebruik
van KH/Insuline ratio’s bij het bepalen van de boluswizard even effectief was als met een PDA.
Het gebruik van de PDA leverde wel tijdswinst op en verbetering van welbevinden. Er zijn
langere termijn studies nodig om te beoordelen of de effecten van het gebruik van PDA voor
bolusadvies etcetera op de lange duur effectief blijft.
Conclusies
LAAG
Het consequent gebruik van e-health in de vorm van een device met boluswizard en
correctiefactor geeft op korte termijn een statisch significante en klinisch relevante
daling van het HbA1c. Dit effect is meer uitgesproken indien er <24hr feedback is op
de data door de behandelaar.
Rossi et al., 2010; Charpentier et al., 2011; Franc et al.,2011
LAAG
Mondelinge educatie over het rekenen met koolhydraten, gebruik van KH/I ratio’s
en correctiefactor is even effectief in het verlagen van het HbA1c als het werken
met een device met boluswizard en correctiefactor. Het gebruik van de device leidt
tot een betere tevredenheid met de behandeling.
Rossi et al., 2010
Overwegingen
Om een zo goed mogelijke diabetesregulatie te verkrijgen kunnen hulpmiddelen nuttig zijn.
Voorwaarde voor het nut van hulpmiddelen is wel dat educatie over het beste gebruik hiervan
gegeven wordt. Het is van belang dat iemand met DM1 in staat is tot zelfmanagement, dat wil
zeggen om de insuline behandeling aan te passen aan de dagelijkse variatie in eten en activiteit.
Dit vereist kennis van de werkingsduur van de verschillende insulines, de KH-samenstelling van
de voeding en het effect van lichamelijke activiteit. Ook moet de patiënt in staat zijn een te hoge
of te lage glucosewaarde op een juiste manier te corrigeren.

38
De bovengenoemde studies laten zien dat de beschreven toepassingen met daarbij gebruik van
e-health een verbetering van het HbA1c kunnen geven, maar arbeidsintensief is en veel vraagt
van patiënt en hulpverlener. Veel mensen met DM1 hebben echter een smartphone. Het gebruik
van een app hierop die, afhankelijk van de ingestelde KH/I ratio en correctiefactor, een
dosisadvies geeft maakt het een stuk makkelijker deze ook te gebruiken. Vaak wordt ook gebruik
gemaakt van apps die ook het berekenen van de KH hoeveelheid per maaltijd vergemakkelijkt.
Het dagelijks gebruik is niet voor iedereen haalbaar, maar bij goede resultaten en stabielere
instelling motiveert het wel tot verder gebruik. Het is nog te vroeg om te weten of langdurig
consequent gebruik ook leidt tot een betere regulatie op de lange termijn en een mogelijk
gunstig effect op het optreden van complicaties.
Aanbevelingen
Overweeg bij iedere patient met DM type I, een educatieprogramma over het gebruik van KH/I
ratio, correctiefactor en het juist berekenen van KH intake, ofwel een glucosemeter of
insulinepomp met boluswizard al of niet in combinatie met een smartphone.
Literatuur
Charpentier, G., Benhamou, P.Y., Dardari, D., Clergeot, A., Franc, S., Schaepelynck-Belicar, P.,
Catargi, B., Melki, V.,…. (2011). The Diabeo software enabling individualized insulin dose
adjustments combined with telemedicine support improves HbA1c in poorly controlled type 1
diabetic patients: a 6-month, randomized, open-label, parallel-group, multicenter trial (TeleDiab
1 Study). Diabetes Care, 34, 533-539.
Franc, S., Daoudi, A., Mounier, S., Boucherie, B., Dardari, D., Laroye, H., Neraud B, Requeda E,….
(2011). Telemedicine and diabetes: achievements and prospects. Diabetes & Metabolism, 37,
463-476.
McCarrier, K.P., Ralston, J.D., Hirsch, I.B, Lewis, G., Martin, D.P., Zimmerman, F.J., & Goldberg,
H.I. (2009). Web-based collaborative care for type 1 diabetes: a pilot randomized trial. Diabetes
Technol Ther., 11, 211-217.
Rossi, M.C., Nicolucci, A., Di, B.P., Bruttomesso, D., Girelli, A., Ampudia, F.J., Kerr D, Ceriello A,…

39
(2010). Diabetes Interactive Diary: a new telemedicine system enabling flexible diet and insulin
therapy while improving quality of life: an open-label, international, multicenter, randomized
study. Diabetes Care, 33, 109-115.

40
Uitgangsvraag 7
Wat is de meerwaarde van een endocrinoloog of diabetoloog in vergelijking tot een internist
(generalist / ander deelspecialisme) in de behandeling van volwassenen met DM1?
Inleiding
DM1 is een chronische ziekte met een hoge complexiteit, die meestal al op jonge leeftijd
ontstaat en waarmee mensen met DM1 de rest van hun leven dienen om te gaan. Iedere
levensfase kan opnieuw problemen met zich meebrengen die specifieke aandacht vereist van de
medische professional, zoals opstandigheid gedurende de puberteit, op stap gaan en uitslapen,
alcohol drinken, arbeid, intensief sporten, zwangerschapswens.
Daarbij komt nog dat DM1 gepaard kan gaan met andere auto-immuun aandoeningen, zoals
meest voorkomend auto-immuun geïnduceerde hypothyreoidie (bij 25%), maar ook alle andere
onderdelen van polyendocriene syndromen (bijnierschorsinsufficiëntie, hypoparathyreoïdie,
vitamine B12 deficiëntie, prematuur ovarieel falen). Ook coeliakie komt vaker voor bij mensen
met DM1.
Tot slot zijn er ook nog de reguliere ziektespecifieke aandachtspunten, zoals goede metabole
controle bereiken, voorkomen hypoglycemieën en ‘hypoglycemia unawareness’, voorkomen en
behandelen van de complicaties van DM.
Bovengenoemde punten vereisen begeleiding van een medische professional die zich bewust is
van deze problematiek en die ook voldoende up to date is ten aanzien van nieuwe
ontwikkelingen in bijvoorbeeld CSII, CGM en e-health. Uit praktisch oogpunt komt het in
Nederland voor dat een patiënt met DM1 behandeld wordt door een internist met een niet-
endocrinologisch aandachtsgebied.
Wij vragen ons af of er bewijs voor is, dat de complexe zorg voor een DM1 patiënt door een
internist-endocrinoloog gegeven dient te worden, of dat er specifieke indicaties zijn om de zorg
over te dragen aan een internist-endocrinoloog.
Er is gezocht naar literatuur waarin het effect van behandeling door een endocrinoloog of
diabetoloog wordt vergeleken met behandeling door een internist (generalist) ten aanzien van
glycemische controle (HbA1c), hypoglycemieën en complicaties als uitkomstmaat. Er is gezocht
vanaf 1-1-2000 op systematische reviews, RCT’s, en ander vergelijkend onderzoek, in de
databases Medline, Embase en the Cochrane Library. Uit het totaal van 145 treffers werden op
basis van titel en abstract, twee artikelen geselecteerd (Zgibor et al., 2000; Zgibor et al., 2002).

41
Samenvatting van de literatuur
De zoekactie leverde twee artikelen op van dezelfde onderzoeksgroep betreffende een Noord-
Amerikaans cohortstudie, waarbij de oudste studie een cross-sectionele analyse betreft (Zgibor
et al., 2000) en de tweede studie prospectieve (10-jaars follow-up) resultaten beschrijft (Zgibor
et al., 2002). Het gaat om 429 DM1 patiënten, waarvan 212 behandeld werden door een
geregistreerd endocrinoloog of diabetoloog (interventie) en 217 behandeld werden door een
generalist/niet-specialist (controle). Uitkomstmaten in de cross-sectionele studie zijn met name
glycemische controle en in de prospectieve studie de incidentie van diabetescomplicaties.
In de beschrijving van de ‘Methodes’ wordt helaas niet duidelijk omschreven wat de definitie van
de generalist is: of dit een huisarts of een internist betreft. ‘Specialist care’ wordt heel duidelijk
gedefinieerd als een specialist die bij de American Board van Medisch Specialisten geregistreerd
staat als endocrinoloog of diabetoloog. Maar de beschrijving van de ‘Nonspecialist’ ontbreekt in
het geheel. Verder zijn de patiënten niet gerandomiseerd en is de indeling per groep dus
gebaseerd op hoe ze historisch in de groep terecht zijn gekomen. Waarbij uit de cross-sectionele
studie naar voren kwam dat in de ‘Specialist care’ groep het gemiddelde opleidingsniveau en
inkomensniveau hoger is (Zgibor et al., 2000). In de ‘Specialist care’ groep was er significant
vaker een HbA1c bekend van de afgelopen zes maanden (85% vs 66% in de ‘nonspecialist’ groep,
p<0,001) en het HbA1c was significant lager in de ‘Specialist care’ groep: 9,7% vs. 10,3%,
p<0.001. Er is echter een duidelijke bias op grond van socio-economische status. In de
prospectieve studie (10 jaar follow-up) werden de 429 deelnemers gesplitst in ‘nonspecialist’
groep (n=215) die <65% van hun diabetes duur behandeld waren in ‘Specialist care’ setting en
‘Specialist’ groep (n=214) die >65% van hun diabetesduur behandeld waren in ‘Specialist care’
setting (=door geregistreerd endocrinoloog of diabetoloog). Multivariaat analyse, waarbij
gecontroleerd werd voor diabetes duur, demografische karakteristieken en ziektespecifieke
risicofactoren (zoals HbA1c, lipiden profiel, hypertensie etcetera), toonde dat hogere
consumptie binnen de ‘Specialist care’ onafhankelijk beschermend was voor ontwikkeling van
klinisch manifeste nefropathie (OR 0.43, 95% BI 0.21-0.88) en mogelijk beschermend was tegen
coronaire hartziekten (statistisch niet significant; OR 0.54, 95% BI 0.37-1.1).
Bij het beoordelen van deze twee studies is het belangrijkste bezwaar dat de vergelijking die in
deze studies wordt gemaakt niet relevant is voor de Nederlandse situatie. Aangezien DM1 in
Nederland in de tweede lijn wordt behandeld heeft het voor de Nederlandse situatie geen zin
om eerste en tweede lijn met elkaar te vergelijken. Omdat het observationele studies betreft, en

42
punten moeten worden afgetrokken vanwege indirectheid en ernstige tekortkomingen in
studieopzet (zie boven), is de bewijskracht volgens GRADE zeer laag.
Conclusies
ZEER LAAG
Er zijn geen goede studies beschikbaar waarbij uitkomstmaten/kwaliteit van zorg bij
type 1 diabetes wordt vergeleken tussen een internist-endocrinoloog en een
internist zonder endocrinologie of diabetes als aandachtsgebied.
Overwegingen
De literatuur geeft ons geen antwoord op de vraag of iemand met DM1 door een endocrinoloog
of diabetoloog behandeld dient te worden. Op grond van de lage prevalentie van DM1 en
specifieke ziektegerelateerde problemen, zou naar analogie van ‘volume normen’ in de
chirurgie, gesteld kunnen worden dat een internist zonder het aandachtsgebied/profiel
endocrinologie/diabetes te weinig ervaring kan hebben met een aantal situaties die voorkomen
bij DM1.
Derhalve zouden er omstandigheden gedefinieerd kunnen worden, waarbij de patiënt met DM1
baat zou kunnen hebben bij begeleiding door een endocrinoloog/internist met diabetesprofiel:
- Transitiegroep/jong volwassenen (acceptatie/alcohol/(top)sporters;
- Vrouwen met een (toekomstig) kinderwens en zwangeren;
- DM1 patiënten met preterminaal nierfalen: screening nier-/pancreastransplantatie?
- Hypoglycemia unawareness;
- CSII;
- Indicaties voor CGM (continuous glucose monitoring);
- Alle nieuwe DM1 patiënten ter beoordeling indicatie immunosupressiva.
Het nut van ondersteuning van de diabetes specialist door diabetesverpleegkundige is
onomstotelijk bewezen. Een niet-internist-endocrinoloog dient dan ook tenminste nauw samen
te werken met een diabetesverpleegkundige.
In de Landelijke Transmurale Afspraken (Sluiter et al., 2012), opgesteld door het NHG en de NIV,
staat dat DM1 in de tweede lijn behandeld dient te worden.

43
De ADA richtlijn adviseert het screenen op andere auto-immuun aandoeningen (zoals
hypothyreoidie, vitamine B12 deficiëntie en coeliaki) in overweging te nemen, in het bijzonder in
aanwezigheid van specifieke symptomen. Periodieke screening wordt niet aanbevolen.
Aanbevelingen
Behandel mensen met type 1 diabetes altijd binnen een multidisciplinair behandelteam
(internist, diabetesverpleegkundige, diëtist, voetenteam en op afroep, psycholoog, gynaecoloog,
en anderen) in de tweede lijn. Interacteer als internist actief binnen dit behandelteam.
Literatuur
ADA Guidelines 2012: Standards of Medical Care in Diabetes. (2012). Diabetes Care, 35(1), S11-
S63. http://www.diabetes.org
Sluiter, A.C., Van Wijland, J.J., Arntzenius, A.B., Bots, A.F.E., Dijkhorst-Oei, L.T., Van der Does,
F.E.E., Palmen, J.V.H., Potter van Loon, B.J.,…(2012). Landelijke Transmurale Afspraak Diabetes
Mellitus type 2. Huisarts Wet, 55, S1-12.
Zgibor, J.C., Songer, T.J., Kelsey, S.F., Weissfeld, J., Drash, A.L., Becker, D., & Orchard, T.J. (2000).
The association of diabetes specialist care with health care practices and glycemic control in
patients with type 1 diabetes: a cross-sectional analysis from the Pittsburgh epidemiology of
diabetes complications study. Diabetes Care, 23, 472-6.
Zgibor, J.C., Songer, T.J., Kelsey, S.F., Drash, A.L., & Orchard, T.J. (2002). Influence of health care
providers on the development of diabetes complications: long-term follow-up from the
Pittsburgh Epidemiology of Diabetes Complications Study. Diabetes Care, 25, 1584-90.

44
BIJLAGEN

45
Evidence table for intervention studies
Research question: Does the addition of rapid-acting insulin analogs to the basal insulin regime improve treatment of patients with type 1 diabetes?
Study reference
Study characteristics Patient characteristics Intervention (I)
Comparison / control (C)
Follow-up Outcome measures and effect size Comments
Rys et al, 2011 (individual study characteristics deduced from Rys et al, 2011)
SR and meta-analysis of 18 RCTs Literature search up to July 2009 A Ampudia-Blasco, 2005 B Arslanian, 2005 C Bode, 2001 D Bode, 2002 E Boehm, 2002 F Bott, 2003 G Chen, 2006 H Cherubini, 2006 I Danne, 2007 J De Vries, 2003 K Heller, 2004 L Home, 1998 M Home, 2000 N Iwamoto, 2001 O Mathiesen, 2007 P Mortensen, 2006 Q Raskin, 2001 R Tamas, 2001 Parallel design (A-F, H, J, M-P, R) or cross-over design (G, I, K, L, Q) 14 RCTs adults, 4 children/ adolescents (B, H, I, P) 3 adequate allocation concealment (J, K, R) 2 CSII (C, D)
Inclusion criteria SR: DM1 (DM2 not presented in this table), RCTs insulin aspart vs regular human insulin, no restriction on age, studies ≥ 4 wks, subgroup analysis ≥ 12 wks for HbA1c. Exclusion criteria SR: N < 10, < 4 wks, gestational or secondary DM. N/N, mean age (yrs) A 28/26; 32.3 B 187/96; 11.7 C 19/10; 36.6 D 59/59; 42.7 E 88/102; >18 F 283/141; 36.9 G 27; 44.8 H 30; 8.1 I 26/26; 5 J 186/181; 36.9 K 155; 35.7 L 104; 34.3 M 707/358; 38 N 143/62; 33.4 O 157/165; 29.0 P 86/81; 14.4 Q 596/286; 39.2 R 213/213; 36 HbA1c at baseline (%) A 8.5 B 8.3 C 7.2 D 7.4 E ≤ 11.0 F 7.5 G not reported
Rapid-acting analogs (RAA) Insulin aspart (IAsp) Insulin regimen (basal insulin) A MDI B MDI C CSII D CSII E Biphas F MDI G Biphas H MDI I MDI J MDI K MDI L MDI M MDI N MDI O MDI P Biphas Q MDI R MDI MDI with NPH, except A (glargine
Regular human insulin (RHI) Same insulin regimen as in intervention group
Duration of follow-up (months): A 6 B 6 C 7 wks D 4 E 3 F 6 G 2 x 3 H 4.5 I 2 x 3 J 16 K 2 x 4 L 2 x 1 M 6 N 6 O 9 P 4 Q 6 R 3
For how many participants were no complete outcome data available? Not stated
Effect on glycemic control (HbA1c , post-prandial glucose [PPG]), fasting glucose, quality of life/ treatment flexibility, adverse effects; weighted mean difference (WMD), standardized mean difference (SMD), relative risk (RR) [meta-analysis]; [95%CI] Effect on HbA1c I minus C (WMD; %)); 13 studies pooled <0 favours I (IAsp) >0 favours C (RHI) 16 studies measured HbA1c Excluded: 3 studies lacking sufficient numerical data (G,H,I) A 0.14 [-0.38; 0.66] B 0.00 [-0.35; 0.35] C -0.20 [-0.66; 0.26] D -0.35 [-0.62; -0.08] E 0.19 [-0.05; 0.43] J -0.14 [-0.35; 0.07] K 0.00 [-0.20; 0.20] M -0.12 [-0.22; -0.02] N -0.24 [-0.57; 0.09] O -0.08 [-0.22; 0.06] P 0.14 [-0.33; 0.61] Q -0.15 [-0.26; -0.04] R -0.16 [-0.30; -0.02] Overall: -0.11 [-0.16; -0.06] Heterogeneity: I2=17.5%; p=0.27 Subgroup-analyses based on basal insulin treatment: Subgroup-CSII (C,D; 2 studies pooled) Overall: -0.31 [-0.55; -0.08] Subgroup-basal bolus (A,B,J,K,M,N,O,Q,R; 9 studies pooled) Overall: -0.12 [-0.17; -0.06] Effect on post-prandial glucose (PPG; self-measured) I minus C (mmol/l) Reported in 10 studies; studies w/o suff numerical data were excluded Post-breakfast glucose (5 studies) -1.43 [-1.75; -1.11] Post-lunch glucose (5 studies) -1.11 [-1.61; -0.61] Post-dinner glucose (6 studies) -0.97 [-1.25; -0.69] Effect on fasting glucose (FG)
Authors conclude that IAsp compared with RHI resulted in moderately better metabolic control, as demonstrated by reductions in HbA1c and PPG, and no change in FG; IAsp also resulted in greater treatment satisfaction and a significant reduction of risk for nocturnal hypoglycaemic episodes, but not severe hypoglycaemias or hypoglycaemia in general Note that it is unclear whether the extra reduction in HbA1c by 0.11 % is clinically relevant Note that the 2 studies with CSII regimen had the most favourable HbA1c reduction (-0.31 [-0.55; -0.08]) as compared to 9 studies with basal-bolus (MDI) regimen ( -0.12 [-0.17; -0.06]) Note that in most studies, no blinding or allocation concealment was applied (high risk of bias), and that the data reported in some studies were incomplete (HbA1c was measured in most studies, but PPG or hypoglycaemic episodes only in some studies); SR provides no data on risk of publication bias Quality of RCTs (Jadad score): R1 Random allocation R2 with appropriate rand. method B0 Not double-blind B1 Double-blind W0 No info on reasons withdrawal W1 information provided A R1 B0 W0 B R1 B0 not reported C R1 B0 W1 D R2 B0 W1

46
H 7.5 I 7.8 J 8.38 K 8.6 L 7.1 M 7.97 N 7.5 O 6.9 P 9.6 Q 7.9 R 8.325
), and N (not reported)
I minus C (mmol/l); 5 studies pooled Reported in 12 studies; in 3 studies RHI was superior over insuline aspart, in 9 studies differences were not significant; 5 studies provided numerical data Fasting glucose 0.15 [-0.55; 0.86) Heterogeneity: I2=72.8%; p=0.005 Adverse effects (hypoglycemic episodes) I minus C (RR) Reported in 7 studies, in 6 studies episodes were self-reported All hypoglycaemic episodes (6 studies) 1.06 [1.01; 1.10] Reported in 3 studies Nocturnal hypoglyc episodes (3 studies) 0.67 [0.54; 0.83] Reported in 8 studies, 7 with sufficient numerical data Severe hypoglyc episodes (7 studies) 0.92 [0.75; 1.12] Quality of life / treatment flexibility I minus C (SMD; DTSQ questionnaire score) Reported in 3 studies, the flexibility part in only 2 Total score (3 studies) 0.30 [0.20;0.40] Flexibility score (2 studies) 0.31 [0.15; 0.47]
E R2 B0 W1 F R1 B0 W0 G R1 B0 W1 H R1 B0 W0 I R1 B0 W0 J R2 B0 W1 K R2 B1 W1 L R1 B1 W1 M R1 B0 W1 N R1 B0 W0 O R2 B0 W0 P R1 B0 W0 Q R1 B0 W1 R R2 B0 W0 Level of evidence: GRADE MODERATE* IAsp vs RHI Effect on HbA1c LOW** IAsp vs RHI Effect on PPG MODERATE*** IAsp vs RHI Effect on FG LOW**** IAsp vs RHI Adverse effects (hypoglycemic episodes) *Downgraded 1 point because of serious study limitations: lack of blinding (12 out of 13 studies) and allocation concealment (10 out of 13 studies) **Downgraded 2 points because of serious study limitations (lack of blinding and allocation concealment), and indirectness (3 out of 5 [PBG], 1 out of 5 [PLG], and 2 out of 6 [PDG] studies included children/adolescents) *** Downgraded 1 point because of serious study limitations (lack of blinding and allocation concealment) ****Downgraded 2 points because of serious study limitations (lack of blinding and allocation concealment), and inconsistency (inconsistent results across studies; difference in estimate of treatment effect depending on outcome measure [overall vs nocturnal vs severe hypoglycemic episodes])

47
A significant reduction of postprandial glucose levels was found in the groups receiving insulin aspart compared to regular human insulin (pooled results of 5-6 studies) The risk of nocturnal hypoglycaemia measured in 3 studies, was significantly lower in insulin aspart group than in the regular human insulin group (RR= 0.67 [0.54; 0.83]) In contrast, the insulin aspart group showed a slight, but statistically significant, risk increase of all hypoglycaemic episodes compared to the regular human insulin group (RR=1.06 [1.01; 1.10]; pooled result of 6 studies) Pooled analysis of 2 studies showed that using insulin aspart instead of regular human insulin resulted in greater treatment satisfaction
Brock Jacobsen et al, 2011
Cross-over study; double-blind, randomized, 2 periods Funding: supported by Novo Nordisk
Inclusion criteria: type 1 DM for > 1 year; age 18–60 years; BMI of 18–27.5; required to use soluble human insulin before breakfast, lunch and dinner and NPH at bedtime for at least 3 months before entering study Exclusion criteria: pregnancy, impaired vision, impaired renal or hepatic function, cardiac diseases, uncontrolled hypertension, hypoglycaemic unawareness 13 men, 3 women Age 44.4 ± 8.2 years BMI 24.6 ± 1.3 HbA1c 7.8 ± 1.1% Diab duration 19± 10 years At baseline, mean daily insulin dose was: soluble insulin 29.4 IU and NPH 22.3 IU
Insulin aspart (IAsp) Novo-Rapid; 3X/d N=16 Insulin regimen (basal insulin): NPH 2X/d
Regular human insulin (RHI) Actrapid; 3X/d N=16 Same insulin regimen as in intervention group
Duration of follow-up: 2X8 weeks
After 8 weeks of treatment, patients were hospitalized for 22 h For how many participants were no complete outcome data available? 2/16 (13%); patients left ‘for personal reasons’
Effect on glycemic control (HbA1c , post-prandial glucose [PPG]), patient satisfaction, adverse effects; absolute amount, counts, frequency [SD] Effect on HbA1c (%) I: 7.0 ± 0.2 C: 7.0 ± 0.2 P=NS Adverse effects (hypoglycemic episodes) I: 214 events (3 nocturnal; 2 extreme [≤ 3.5 mmol/l] C: 297 events (5 nocturnal; 3 extreme) Hypoglycaemic frequency (events/week) I: 0.9 ± 0.1 C: 1.1 ± 0.2 P=NS Patient satisfaction (VAS; 0-6) P=NS During hospitalization: Effect on post-prandial glucose (PPG) I versus C (mmol/l; p-value) Post-breakfast: 8.2 ± 1.0 vs 12.6 ± 1.1 (P = 0.005) Post-lunch: 3.6 ± 0.4 vs 4.5 ± 0.6 (P = 0.02) Post-dinner: 7.9 ± 1.2 vs 9.9 ± 1.3 (P = 0.01) statistically significant lower PPG during IAsp treatment
Authors conclude that IAsp did not improve glycaemic control, and no difference in hypoglycaemic frequency was observed IAsp elicited a slightly different physiological response to spontaneous hypoglycaemia compared with human insulin; however, the physiological and clinical relevance of these effects remain speculative Note: during hospitalization, a statistically significant lower PPG was observed during IAsp treatment Level of evidence: GRADE see above, this study does not alter the conclusion based on Rys et al (2011; note the small study size (N=16) as compared to the studies included in the meta-analysis)

48
Evidence table for intervention studies
Research question: Does the use of long-acting insulin analogs instead of NPH human insulin improve treatment of patients with type 1 diabetes?
Study reference
Study characteristics
Patient characteristics
Intervention (I) Comparison / control (C)
Follow-up Outcome measures and effect size
Comments
Sanches, 2011 [individual study charac-teristics deduced from Sanches, 2011]
SR and meta-analysis of 16 RCTs Literature search up to Dec 2010 A: Home, 2005 B: Porcellati, 2004 C: Raskin, 2000 D: Ratner, 2000 E: Rosenstock, 2000a F: Bolli, 2009 G: Fulcher, 2005 H: Bartley, 2008 I: De Leeuw, 2005 J: Hermansen, 2004 K: Home, 2004a L: Home, 2004b M: Pieber, 2005a N: Pieber, 2005b O: Russell-Jones, 2004 P: Pieber, 2007 Source of funding: 3 studies on glargine and 6 on detemir were sponsored by pharmaceutical industry
Inclusion criteria SR: RCT, adult patients with established type 1 diabetes, received long-acting insulin analogue (glargine or detemir) or NPH insulin alone or in combination with rapid acting insulin analogues (Lispro or Aspart) for at least 4 weeks Exclusion: studies with crossover design N; mean age A: 585; 39.0 yrs B: 124; 35.0 yrs C: 619; 39.2 yrs D: 534; 38.6 yrs E: 344; 37.7 yrs F: 175; 40.5 yrs G: 125; 36.3 yrs H: 495; 35.0 yrs I: 315; 40.5 yrs J: 585; 39.0 yrs K: 585; 39.8 yrs L: 271; 39.6 yrs M: 268; 40.0 yrs N: 261; 40.7 yrs O: 747; 40.3 yrs
Long-acting analogs (LAA) Glargine dose (U/Kg/Day) A: 0.27 B: 0.66 C: NA D: NA E: NA F: 0.28 G: 0.39 Detemir dose (U/Kg/Day) H: 0.37 I: 0.36 J: 0.44 K: 0.48 L: 0.48 M: 0.35 N: 0.34 O: 0.31 In 2 studies (P; one study not detailed), Glargine was compared to Detemir dose (U/Kg/Day) P: 0.39 (glargine) vs 0.36 (detemir)
NPH dose (U/Kg/Day) A: 0.28 B: 0.64 C: NA D: NA E: NA F: 0.28 G: 0.39 H: 0.36 I: 0.36 J: 0.38 K: 0.48 L: 0.48 M: 0.32 N: 0.32 O: 0.31
Endpoint of follow-up: Treatment duration (weeks) A: 28 B: 54 C: 16 D: 28 E: 4 F: 30 G: 30 H: 108 I: 54 J: 18 K: 16 L: 16 M: 16 N: 16 O: 28 P: 52
For how many participants were no complete outcome data available? Not stated
Effect on glycemic control (HbA1c), adverse effects (any hypoglycemia episode, nocturnal hypoglycemia); mean difference, OR [95%CI] Mean difference HbA1c (1) Glargine minus NPH A: -0.11 [-0.25, 0.03] B: -0.40 [-0.71, -0.09] C: 0.00 [-0.13, 0.13] D: 0.05 [-0.09, 0.19] E: 0.00 [-0.18, 0.18] F: -0.03 [ -0.20, 0.14] G: -0.30 [ -0.56, -0.04] Total: -0.06 [-0.14, 0.02] Heterogeneity: I2=44% (2) Detemir minus NPH (2a) Detemir once a day H: -0.22 [-0.39, -0.05] O: 0.00 [-0.15, 0.15] Subtotal: -0.11 [-0.32, 0.11] Heterogeneity: I2=71% Note: only 2 studies (2b) Detemir twice a day I: -0.08 [-0.31, 0.15] J: -0.22 [-0.33, -0.11] K: -0.20 [-0.44, 0.04] L: -0.17 [-0.41, 0.07] M: -0.04 [-0.27, 0.19] N: -0.10 [-0.34, 0.14] Subtotal : -0.14 [-0.22, -0.07] Heterogeneity: I2=0%
Authors conclude that there are no significant differences in HbA1c change between glargine or detemir (once daily) and conventional human insulin (NPH insulin). Twice daily regimen of detemir caused a difference in HbA1c that favored detemir (-0.14% [-0.22; -0.07]). No significant differences between glargine and detemir in safety or HbA1c mean change Note that results for hypoglycemia were inconsistent (high heterogeneity; I2); also note that the definition of hypoglycemia was not consistent across the studies Quality of RCTs (Jadad score): Max=5 A: 2 B: 4 C: 2 D: 0 E: 5 F: 2 G: 2 H: 2 I: 2 J: 2 K: 2

49
Study reference
Study characteristics
Patient characteristics
Intervention (I) Comparison / control (C)
Follow-up Outcome measures and effect size
Comments
P: 320; 41.0 yrs BMI (kg/m2) A: 24.9 B: 23.1 C: 25.6 D: 25.8 E: 24.3 F:23.5 G: 26.6 H: 24.7 I:24.5 J:24.8 K:25.2 L:25.2 M:25.2 N:25.2 O:25.3 P: 25.6
Total: -0.13 [-0.19, -0.06] Heterogeneity: I2=13% (3) Glargine or detemir (minus NPH): (1) and (2) combined Total: -0,09 [-0,14; -0,03] Heterogeneity: I2=38% (4) Glargine minus detemir P: -0.13 [-0.32, 0.06] Total (95%CI): -0.07 [-0.19, 0.06] Heterogeneity: I2=0% Note: only 2 studies Adverse effects (hypoglycemia) OR [95%CI] (1) Glargine vs. NPH Hypoglycemia 1.12 [0.69-1.81] Nocturnal 1.93 [0.78-4.79] High heterogeneity (I2>66%) (2) Detemir vs. NPH: Hypoglycemia 0.88 [0.52-1.51] Nocturnal 0.91 [0.52-1.60] High heterogeneity (I2>83%) (3) Glargine vs. Detemir: Hypoglycemia 2.05 [0.98-4.29] Nocturnal 1.24 [0.83-1.84] Only 2 studies included
L: 2 M: 2 N: 2 O: 2 P: 3 Level of evidence: GRADE Across all studies analysed MODERATE* LAA vs NPH Effect on HbA1c LOW** LAA vs NPH Adverse effects (hypoglycemic episodes) *Downgraded 1 point because of serious study limitations: low Jadad score (lack of blinding and allocation concealment) **Downgraded 2 points because of serious study limitations (low Jadad score), and imprecision (high heterogeneity; wide confidence intervals)
Szypowska, 2011
SR and meta-analysis of 10 RCTs Literature search up to Nov 2010
Inclusion criteria SR: RCTs ≥ 12
weeks; basal‑bolus therapy; DM type 1 with history ≥1 year Crossover trials and
Long-acting analogs (LAA) Detemir
NPH Endpoint of follow-up: Treatment duration 4-24 months
For how many participants were no complete outcome data available? Not stated
Effect on glycemic control (HbA1c), adverse effects (any / nocturnal / severe hypoglycemia); weighted mean difference, OR [95%CI] Mean difference HbA1c Detemir minus NPH Total: –0.073 [–0.135; –0.011]
Authors conclude that detemir, as compared with NPH, provided a minor benefit in terms of the HbA1c, and
reduced the risk of all‑day, nocturnal, and severe hypoglycemic episodes

50
Study reference
Study characteristics
Patient characteristics
Intervention (I) Comparison / control (C)
Follow-up Outcome measures and effect size
Comments
trials with children or adolescents not excluded Unpublished trials (Novo Nordisk) were also included
Heterogeneity: I2=0% Adverse effects(hypoglycemia) RR [95%CI] Detemir vs. NPH: All 0.98 [0.961; 0.996]; I2=26% Nocturn 0.88 [0.82; 0.94]; I2=0 Severe 0.67 [0.55; 0.81]; I2=51
Note: meta-analysis differs from that in Sanches et al (2011) in that a cross-over study and a study on children/adolescents was included as well as 3 unpublished trials from the Novo Nordisk trial registry Level of evidence: GRADE (analyzed collectively; see Sanches, 2011)
Garg, 2010 SR of 19 RCTs 9 RCTs comparing glargine with NPH (MDI regimen) No meta-analysis Literature search up to Feb 2010
Inclusion criteria SR: RCTs ≥ 12 weeks; patients (adult, children, adolescents) using once-daily insulin glargine Exclusion: pregnant women; studies not providing separate data on T1DM Crossover trials and trials with children or adolescents not excluded Very small studieswith ≤50 patients were also included
Long-acting analogs (LAA) Glargine
NPH (MDI) Endpoint of follow-up: Treatment duration 3-12 months
For how many participants were no complete outcome data available? Not stated
Effect on glycemic control (HbA1c), adverse effects (any / nocturnal / severe hypoglycemia); p-values No meta-analysis Effects on HbA1c out of 9 RCTS: 4 showed statistically significantly greater improvements with glargine compared with NPH insulin 4 showed no difference 1 showed slightly increased HbA1c (P=NS) Adverse effects(hypoglycemia) Out of 9 RCTs: 5 showed significantly reduced risk of symptomatic hypoglycemia 4 showed no difference in risk
Authors conclude that glycemic control with glargine is at least comparable to that with NPH, while the risk for hypoglycemia is significantly reduced Note: SR differs from Sanches et al (2011) in that a cross-over study, a subgroup analysis and a very small study were included, and no meta-analysis was performed
Monami, 2009
SR and meta-analysis of 20 RCTs Literature search up to
Inclusion criteria SR: RCTs ≥ 12 weeks; T1DM patients
Long-acting analogs (LAA) Detemir Glargine
NPH
Effect on glycemic control (HbA1c), adverse effects (any /severe /nocturnal hypoglycemia); mean
Authors conclude that long-acting analogues as basal insulin replacement DMT1 patients had a small

51
Study reference
Study characteristics
Patient characteristics
Intervention (I) Comparison / control (C)
Follow-up Outcome measures and effect size
Comments
Apr 2008
Exclusion criteria: prandial insulin not comparable in treatment arms Crossover trials and trials with children or adolescents not excluded 4 unpublished trials were also included
Prandial insulin: RHI (4 RCTs), short-acting insulin analogues (16 RCTs)
Prandial insulin: indentical to treatment arm
difference, OR [95%CI] Mean difference HbA1c Total: -0.07 [-0.13; -0.01]; different LAA (detemir, glargine) yielded similar results Adverse effects (hypoglycemia) OR [95%CI]; MH estimates Any/severe/nocturnal 12 / 15 /13 RCTs Any 0.82 [0.61; 1.07] Severe 0.73 [0.60; 0.89] Nocturnal 0.69 [0.55; 0.86] similar point-estimates for glargine and detemir, but OR estimates for severe and nocturnal hypoglycemia not statistically significant for glargine (these RCTs enrolled fewer patients)
(beneficial) effect on HbA1c, and also reduced the risk of nocturnal and severe hypoglycaemia (by about 30%) Note that the overall incidence of hypoglycemia does not appear to be different between LAAs and NPH insulin Note: meta-analysis differs from that in Sanches et al (2011) in that cross-over studies, studies on children/adolescents were included as well as 3 unpublished trials
Dejgaard, 2009
SR and IPD meta-analysis of 21 RCTs (all open-labelled) Source of funding: Individual patient data (IPD) analysis of Novo Nordisk-sponsored RCTs; authors are employed by Novo Nordisk
Inclusion criteria SR: Novo Nordisk sponsored RCTs with type 1 or type 2 diabetes (IPD available); insulin detemir versus NPH insulin or insulin glargine; duration > 12 weeks Exclusion criteria (IPD analysis): children 21 Novo Nordisk
Long-acting analogs (LAA) Detemir In 5 out of 21 studies, detemir was compared to glargine (instead of NPH)
NPH
Endpoint of follow-up: Median exposure Detemir: 24.0 weeks NPH: 23.9 weeks In studies comparing detemir to glargine: 51 weeks
For how many participants were no complete outcome data available? Not stated
Malignant neoplasm (cancer); OR, adjusted OR [95%CI] Outcome assessment: suspected treatment-emergent malignant tumours were identified in a blinded manner from databases of adverse events Malignant neoplasm (cancer) Cases; rate/100 exposure years; OR; adjusted OR (stratified; MH estimate) Detemir versus NPH
Authors conclude that patients treated with insulin detemir had a lower or similar occurrence of a cancer diagnosis compared with patients treated with NPH insulin or insulin glargine Note that incidence rate of cancer in this study population is low (probably due to inclusion and exclusion criteria of the RCTs), and length of followup is short: low number of cases; study does not allow definitive conclusions on risk of cancer promotion by insulin

52
Study reference
Study characteristics
Patient characteristics
Intervention (I) Comparison / control (C)
Follow-up Outcome measures and effect size
Comments
studies met the criteria N= 8,693 (total): detemir (3,983) versus NPH (2,661), and detemir (1,219) versus glargine (830) Patient characteristics (mean) Mean age 48-52 y Type 1 diab 37-52% Diab duration 13-15 y BMI 27-29 kg/m2 HbA1c 8.1-8.6% Male 54-56%
Cases: 8 versus 13 Rate: 0.36 versus 0,92 Crude OR: 2.44 [1.01–5.89] Adjusted OR: 2.53 [1.02–6.28] stratified on trial Adjusted OR: 2.35 [0.97–5.70] stratified on DM type Detemir versus glargine Cases: 8 versus 8 Rate: 0.87 versus 1.27 Crude OR: 1.47 (0.55–3.94) Adjusted OR: 1.32 [0.51–3.43] stratified on trial Adjusted OR: 1.46 [0.55–3.90] stratified on DM type
analogues Note: literature was not searched systematically for insulin analogs in relation to cancer risk; e.g. also see Home et al (2009; Diabetologia 52:2499-2506), and Ruiter et al (2012; Diabetologia 55:51-62) Level of evidence: GRADE LOW* LAA vs NPH Adverse effects (cancer) *Downgraded 2 points because of imprecision (low number of cases) and indirectness (low incidence of cancer in study population; short length of followup)

53
Evidence table for prognostic studies
Research question: Are fluctuations in blood glucose associated with an increased risk of microvascular or macrovascular complications in patients with type 1 diabetes? Study reference
Study characteristics
Patient characteristics Prognostic factor(s) Follow-up
Outcome measures and effect size Comments
Nalysnyk et al, 2010 [individual study characteristics deduced from Nalysnyk et al, 2010; with corrections if required] Only relevant data (on patients with type 1 diabetes) included in the evidence table
Type of study: Systematic review; all study designs incl. randomized and non-randomized controlled trials, prospective and retrospective cohort studies and uncontrolled case series Literature search Jan 1990 – Nov 2008 SR of patients with type 1 diabetes: 8 studies included Cohort (A,B,C,G), cross-sectional (D,E,F), or case-control (H) A: Bragd, 2008 B: Kilpatrick, 2006 C: Service, 2001 D: Moberg, 1994 E: Oyibo, 2002 F: Gordin, 2008 G: Kilpatrick, 2008 H: Wentholt, 2008 Country: A: Sweden B: UK C: USA D: Sweden
Inclusion criteria: studies evaluating effect of glucose variability on risk of microvascular and/or macrovascular complications in adults with type 1 or type 2 diabetes; reporting measures of glycaemic variability [MAGE, MODD, SDBG]; outcomes of interest (mortality, CV events, diabetic retinopathy, neuropathy, nephropathy or their surrogate markers) N, mean age, %M A: 100, 45 yrs, 56% B: 1441, 27 yrs, 53% C: 565, 27 yrs, 54% D: 98 E: 20, 52 yrs, 55% F: 22, 26 yrs, 100% G: 1441, 27 yrs, 53% H: 25 (and 24 controls) Note: in E, patients with type 1 diabetes and (!) symptomatic diabetic neuropathy were recruted
Measures of glycaemic variability [MAGE, MODD, SDBG] A: SDBG B: mean AUC glucose; SDBG C: SDBG; MAGE; M-value D: SDBG E: MAGE; M-value F: MAGE G: SDBG H: MAGE; MODD; CONGA SDBG, SD of blood glucose; MAGE, mean amplitude of glucose excursions; AUC, area under curve; M-values, measure of glucose deviations from arbitrarily selected point; MBG, mean blood glucose; MODD, mean of daily differences; CONGA, continuous overlapping net glycaemic action SD, standard deviation
Endpoint of follow-up: A: 11 years B: 9 years (analysis on 5 yrs fup) C: ≥ 4 years D: 1 month E: - F: - G: 9 years H: 48 hours
For how many participants were no complete outcome data available? N (%): A: 19/100 (19%) B: DCCT (<5%) C: DCCT (<5%) D: - E: - F: - G: DCCT (<5%) H: 1/49 (2%)
Micro- and macrovascular complications (incidence), mortality; OR, HR [95%CI], correlation coefficient (p-values) Microvascular complications (A,B,C,D,E) A: multivariate analysis Periph neuropathy SDBG: HR= 1.73 [0.94-3.19] Prolif neuropathy SDBG: HR=1.37 [0.77-2.43] Nephropathy SDBG: HR=1.75 [0.89-3.40] B: multivariate analysis Nephropathy MBG(AUC): HR= 1.03 [0.96-1.11] SD MBG (AUC): HR= 0.96 [0.82-1.11] SD (intra): HR= 1.01 [0.99-1.03] Preprand. mean: HR= 1.08 [0.94-1.24] Postprand. mean: HR= 0.99 [0.89-1.12] Retinopathy MBG (AUC): HR= 1.15 [1.06-1.25] SDMBG (AUC): HR= 0.97 [0.81-1.16] SD (INTRADAY): HR= 1.02 [0.99-1.04] Preprand. mean: HR= 1.11 [0.95-1.30] Postprand. mean: HR= 1.08 [0.94-1.24] C: univariate analysis Retinopathy: HR 3-step progression per 10-unit change (univariate analysis) MBG: HR= 1.14 (p<0.01) M-value: HR= 1.12 (p<0.01) MAGE: HR= 1.10 (p<0.01) SD MBG: HR= 1.25 (p<0.01) In multivariate analysis, with HbA1c added to
6 of 8 studies use a direct outcome (micro- or macrovascular complications) 2 studies use an indirect (proxy) outcome (F: arterial stifness and blood pressure; H: prostaglandin excretion into urine) 3 (4) of 8 studies use multivariate analysis, adjusting for important (potential) confounding risk factors: A, B, and G (in C, both univariate and multivariate analysis is used; see below) 5 of 8 studies use univariate analysis (correlation analysis), and are potentially biased (: no adjustment for confounders) 3 of 8 studies have very small size, including only 20-25 patients with type 1 diabetes (E,F,H) Overall conclusion (Nalysnyk et al, 2010): only in 2 of 8 type 1 DM studies glucose variability had a significant association with microvascular, but not with macrovascular complications; glucose variability appears to have little impact on development of diabetic complications in type 1 DM A: SDBG was found to be a predictor of the prevalence of

54
Study reference
Study characteristics
Patient characteristics Prognostic factor(s) Follow-up
Outcome measures and effect size Comments
E: UK F: Finland G: UK H: NL :
the model, updated MBG was a significant risk factor (p<0.006), but MAGE (and other measures of glycaemic variability) was not (p = 0.06) D: univariate analysis SDBG per group (p-value) Nephropathy (no/yes) 3.8/4.6 (p = 0.03) Retinopathy (no/yes) 3.8/4.1 (p = 0.64) Neuropathy (no/yes) 3.9/4.1 (p = 0.39) Any late complication (no/yes) 3.9/4.0 (p = 0.65) E: univariate analysis (correlation) Neuropathy No correlation between number or degree of painful episodes and number or amplitude of glycaemic excursions Macrovascular complications and mortality (F,G) F: univariate analysis (correlation) Indirect outcome measures measures of glucose control did not correlate with change in arterial stiffness; MAGE correlated with change in aortic diastolic blood pressure: r = 0.52, p =< 0.01 G: multivariate analysis CVD MBG (AUC): HR= 1.11 [1.02–1.21] SD MBG (AUC): HR= 1.04 [0.85–1.27] Preprandial BG: HR= 1.11 (1.02–1.20) Postprandial BG: HR= 1.08 (1.01–1.16) HbA1c: HR= 1.03 (0.76–1.38) All macrovascular (angina, MI, coron. revasc., major ECG events)
peripheral neuropathy (p = 0.03), but not its incidence (p= 0.07) B: blood glucose variability does not appear to be an additional factor in the development of microvascular complications C: In multivariate analysis, updated MBG was a significant risk factor (p<0.006), but MAGE and other measures of glycaemic variability were not D: patients with nephropathy had more variable blood glucose values, compared with patients without signs of nephropathy (note: no adjustment for confounders) E: Patients with painful neuropathy have possibly poorer diabetes control, compared with patients with painless neuropathy (note: no adjustment for confounders) F: study suggests that high mean daily blood glucose but not glucose variability per se is associated with arterial stiffness G: MBG appears predictive of a cardiovascular event even after adjustment for HbA1c values and glucose variability; HbA1c or glucose variability are not predictive H: report no relationship between glucose variability and urinary PGF2α (as a proxy for oxidative stress)

55
Study reference
Study characteristics
Patient characteristics Prognostic factor(s) Follow-up
Outcome measures and effect size Comments
MBG (AUC): HR= 1.05 [1.00–1.11] SD MBG (AUC): HR= 1.03 [0.93–1.14] Preprandial BG: HR= 1.05 [1.01–1.10] Postprandial BG: HR= 1.04 [1.00–1.07] HbA1c: HR= 1.01 [0.87–1.17] Oxidative stress (H) H: univariate analysis (correlation) Indirect outcome measure excretion of 8-iso PGF2α Spearman r MODD: r= −0.112 MAGE: r= −0.381 CONGA: r= −0.177
Lachin et al, 2008
Type of study: Re-analysis of the DCCT (DCCT Research Group, 1995) DCCT presented statistical models suggesting that subjects with similar A1C levels had a higher risk of retinopathy progression in the conventional treatment group than in the intensive treatment group Analysis has been cited to support hypothesis that specific patterns of glucose variation, in particular postprandial hyperglycemia, contribute
DCCT DCCT DCCT Performed statistical evaluations of the DCCT-models and additional analyses to assess whether the original analyses were flawed Statistically, study shows that the original results are an artifact of the assumptions of the statistical model used Additional analyses show that virtually all (96%) of the beneficial effect of intensive versus conventional therapy on progression of retinopathy is explained by the reductions in the mean A1C levels, similarly for other outcomes
Study concludes that A1C explains virtually all of the difference in risk of complications between intensive and conventional groups, and a given A1C level has similar effects within the two treatment groups While other components of hyperglycemia, such as glucose variation, may contribute to the risk of complications, such factors can only explain a small part of the differences in risk between intensive and conventional therapy over time

56
Study reference
Study characteristics
Patient characteristics Prognostic factor(s) Follow-up
Outcome measures and effect size Comments
uniquely to an increased risk of microvascular complications above and beyond that explained by the A1C level

57
Table of quality assessment – prognostic studies
Research question: Are fluctuations in blood glucose associated with an increased risk of microvascular or macrovascular complications in patients with type 1 diabetes?
Study reference (first author, year of publication)
Was there a representative and well-defined sample of patients at a similar point in the course of the disease? (yes/no/unclear)
Was follow-up sufficiently long and complete? (yes/no/unclear)
Was the outcome of interest defined and adequately measured? (yes/no/unclear)
Was the prognostic factor of interest defined and adequately measured? (yes/no/unclear)
Was loss to follow-up / incomplete outcome data described and acceptable? (yes/no/unclear)
Was there statistical adjustment for all important prognostic factors? (yes/no/unclear)
Level of evidence
Bragd 2008 Yes yes yes No yes yes B
Kilpatrick 2006 Yes yes yes yes yes yes A2
Service 2001 Yes Yes Yes Yes Yes Yes**** B
Moberg 1994 Yes No** Yes No Yes No D
Oyibo 2002 Yes* No** Yes Yes -** No D
Gordin 2008 Yes* No** Yes*** Yes -** No D
Kilpatrick 2008 Yes Yes Yes Yes Yes yes A2
Wentholt 2008 Yes* Yes Yes*** Yes Yes No C *small sample size (20-25 patients with type 1 diabetes) **cross-sectional analysis ***use indirect (proxy) outcome measure ****use both univariate and multivariate analysis

58
Evidence table for intervention studies
Research question:
Study reference
Study characteristics Patient characteristics Intervention (I) Comparison / control (C)
Follow-up Outcome measures and effect size
Comments
CTT collaborators,2008
Type of study: SR/meta-analysis Setting: multiple Country: multiple Source of funding: Most of the trials were supported by research grants from the pharmaceutical industry Trials: 1. 4S, Lancet 1994; 24 (0.5)
type 1 diabetes, secondary prevention
2. WOSCOPS, NEJM 1995; 8 (0.1%) type 1 diabetes, primary prevention
3. CARE, NEJM 1996; 193 (4.6%) type 1 diabetes, secondary prevention
4. Post-CABG, NEJM 1997; 27 (2.0%) type 1 diabetes, secondary prevention
5. AFCAPS/ TexCAPS, JAMA 1998; no type 1 diabetes
6. LIPID, NEJM 1998; 106 (1.2%) type 1 diabetes, secondary prevention
7. GISSI-P, Ital Heart J 2000; 120 (2.8%) type 1 diabetes, secondary prevention
8. LIPS, JAMA 2002; 39 (2.3%) type 1 diabetes,
Inclusion criteria: Randomised trials of statin therapy
- The main effect of at least one of the trial interventions is modifying lipid levels
- Unconfounded with respect to this intervention
- ≥ 1000 participants, treatment duration at least 2 yaers
N= the 18686 participants with diabetes in the 14 statin trials contributing to the CTT-meta-analysis. 1466 with type 1 17220 with type 2 71370 no diabetes Mean age ± SD: No diabetes: 61.8 (9,5) Diabetes 63.1 (8,9) Sex: % M / % F No diabetes: M 78% Diabetes: M 67%
Statin treatment
No statin treatment Endpoint of follow-up: All cause mortality
- Vascular causus: CHD/non-CHD
- Non-vascular Major vascular events
Major vascular events in type 1 diabetes (total 1466): Treatment 147 (20.5%) Control 196 (26.2%) RR (99% CI) 0.79 (0.62-1.01) PS. note the 99% CI (i.e. alpha= 0.01)
‘Although the majority of participants in these trials had type 2 diabetes, there was no evidence that the effects of statin therapy on major vascular events in people with type 1 diabetes differed from that in those with type 2; indeed, the reduction in major vascular events in people with type 1 diabetes was statistically significant’

59
secondary prevention 9. HPS, Lancet 2002; 615
(3.0%) type 1 diabetes, combined primary and secondary prevention
10. PROSPER, Lancet 2002; 51 (0,9%) type 1 diabetes, combined primary and secondary prevention
11. ALLHAT-LLT, JAMA 2002; no type 1 diabetes
12. ASCOT-LLA, Lancet 2003; no type 1 diabetes
13. ALERT, Lancet 2003; 280 (13.3%) type 1 diabetes, primary prevention
14. CARDS, Lancet 2004; 3 (0.1%) type 1 diabetes, primary prevention

60
Evidence table for intervention studies
Research question: Does addition of metformin to the insulin regime improve treatment of patients with type 1 diabetes?
Study reference
Study characteristics
Patient characteristics
Intervention (I) Comparison / control (C)
Follow-up Outcome measures and effect size
Comments
Vella et al, 2010 [individual study characteristics deduced from Vella et al, 2010]
SR and meta-analysis of 9 RCTs Literature search up to Oct 2009 Parallel group (C,D,E,F,H,I), or cross-over design (A,B,G)
A: Gin, 1985 B: Keen, 1987 C: Walravens, 2000 D: Meyer, 2002 E: Hamilton, 2003 F: Särnblad, 2003 G: Khan, 2006 H: Lund, 2008 I: Jacobsen, 2009 B/C: abstract only (further data not available) Source of funding: D: LIPHA France (manufacturer metformin) E: non-commercial F: non-commercial; supported by Merck (provided drug and placebo) H: non-commercial; authors report
Inclusion criteria SR: randomisation, informed consent., patients with type 1 diabetes, metformin vs placebo or comparator drug, study duration ≥ 1 week; 9 studies included Studies typically include patients with poor metabolic control (HbA1c ≥ 8%) N, mean age A: 10 patients, 41 yrs B: 8 patients, ‘adults’ C: 80 patients, 16 yrs D: 62 patients, 41 yrs E: 30 patients, 16 yrs F: 30 patients, 17 yrs G: 15 patients, 48 yrs H: 100 patients, 46 yrs I: 24 patients, 40 yrs HbA1c (%) at baseline A: 10.0 B: not stated C: 9.6 D: 7.6 E: 9.4 (I), 8.9 (C) F: 9.3 G: 8.6 H: 9.5 I: 8.9 (I), 9.3 (C)
Mean weight (kg)
Metformin Daily metformin dose A: 1,700 mg B: 1,500 mg C: 1,000 mg D: 1,700 mg E: up to 2,000 mg (weight dep.) F: forced titration to 2,000 mg G: forced titration to 2,000 mg H: forced titration to 2,000 mg I: forced titration to 2,000 mg
Placebo
Endpoint of follow-up: A: 7 days (!) B: 3 wks (!) C: 6 months D: 6 months E: 3 months F: 3 months G: 4 months H: 12 months I: 6 months
For how many participants were no complete outcome data available? A: 0 (0%) B: not stated C: not stated D: 3/62 (5%) E: 3/30 (10%) F: 4/30 (13%) G: 0 (0%) H: 8/100 (8%) I: 1/24 (4%)
Effect on HbA1c , effect on insulin dose, adverse effects; overall standardized mean difference (meta-analysis); p-value, [95%CI] Effect on HbA1c I minus C A: not stated B: not measured C: -0.7% at 3 months (p<0.05); no difference at 6 months D -0.02%; p=NS E: -0.6% (p=0.03) F: -0.9% [–1.6, –0.1]; p<0.05 G: -0.7% (p<0.005) H: +0.13% [–0.19,0.44]; p=NS I: -0.31%; p=NS Effect on insulin dose I minus C A: Fixed by design (HEC / Biostator) B: No change (fixed CSII) C: -10% in men at 6 months only D: -6.0 U/day (p=0.004) E: -0.16 U kg–1 day–1 (p=0.01) F: No significant change G: -8 U/day (p<0.05) H: -5.7 U/day [–8.6, –2.9]; p<0.001 I: -8.8 U/day [–14.6, –3.0]; p=0.004 Adverse effects Hypoglycemic events (I vs C) A: not stated B: 7 vs 0; p=NS C: not stated
Authors conclude that Metformin reduces insulin-dose requirement in type 1 diabetes but that there is no clear evidence of an improvement in glycemic control; it is unclear whether insulin dose reduction is sustained beyond 1 year and whether there are benefits for cardiovascular and other key clinical outcomes Metformin was associated with reductions in: (1) insulin-dose requirement (5.7–10.1 U/day in 6 of 7 studies); (2) HbA1c (0.6–0.9% in 4 of 7 studies); (3) weight (1.7–6.0 kg in 3 of 6 studies); and (4) total cholesterol (0.3–0.41 mmol/l in 3 of 7 studies). Metformin was well tolerated, albeit with a trend towards increased hypoglycaemia. Formal estimates of combined effects from 5 trials indicated a significant reduction in insulin dose (6.6 U/day, p<0.001) but no significant reduction in HbA1c (absolute reduction 0.11%, p=0.42) Note: studies typically include patients with poor metabolic control (HbA1c ≥ 8%) Level of evidence: GRADE MODERATE* Metformin vs placebo Effect on insulin dose LOW** Metformin vs placebo Effect on HbA1c

61
equity in Novo Nordisk; drugs provided by Hexal A/S I: non-commercial; drugs provided by GEA A/S
A: 62 B: 84 C: 68 D: 76 E: 63 (I), 71 (C) F: 68 G: 92 H: 80 I: 90
G/I: only included patients with overweight
D: minor 47 vs 45 patient–1 month–
1 major 19 vs 8; p=NS E: minor 1.8 vs 0.9 patient–1 week–
1 (p=0.03); major 2 vs 1 F: minor not stated; major none G: minor 12 vs 11 patient-1 per 4 weeks (p=NS); major none H: minor 48% of patients vs 49%; major 15% vs 10%; p=NS; leading to unconsciousness 10 vs 2; p<0.05 I: 0.7 vs 0.3 patient–1week–1; p=0.005 no reports of lactic acidosis; rates of gastrointestinal adverse effects only reported in H and I (in largest study [H], rates are similar in both groups) Meta-analysis Standard. mean difference (SMD) SMD <0 favours I (metformin) SMD >0 favours C (placebo) Excluded: very short studies (A,B), studies not stating mean and SD (C,G) Effect on HbA1c D: –0.01 [–0.51, 0.48] E: –0.86 [–1.65, –0.07] F: –0.37 [–1.14, 0.41] H: 0.17 [–0.23, 0.56] I: –0.41 [–1.24, 0.42] Overall: –0.10 [–0.36, 0.15] Heterogeneity: I2=36.9%; p=0.175 translates into an absolute difference of 0.11 units lower %HbA1c in the metformin groups (not statistically significant) Effect on insulin dose D: –0.68 [–1.19, – 0.17] E: – 0.94 [–1.74, –0.14] F: – 0.00 [– 0.77, 0.76] H: – 0.80 [–1.21, –0.39] I: – 0.44 [–1.27, 0.38] Overall: – 0.65 [–0.92, –0.39] Heterogeneity: I2= 0.0%; p=0.410 translates into an absolute difference in insulin dose requirement of 6.6 U/day lower in the metformin groups (p<0.001)
LOW*** Metformin vs placebo Adverse effects *Downgraded 1 point because of serious imprecision: small study size (also after pooling) **Downgraded 2 points because of serious imprecision: small study size, CIs include no effect (also after pooling) ***Downgraded 2 points because of serious imprecision: small study size, CIs include no effect Sensitivity analyses, excluding small studies (<30 patients) i.e. only including Meyer et al (2002) and Lund et al (2008): (1) overall effect on HbA1c 0.10 [-0.21, 0.41], (2)
overall effect on insulin dose 0.75
[1.07, 0.43]

62
Table of quality assessment – intervention studies (The criteria used in this checklist are adapted from GRADE)
Research question: Does addition of metformin to the insulin regime improve treatment of patients with type 1 diabetes?
Study reference (first author, year of publication)
There was adequate concealment of allocation (yes/no/unclear)
Participants receiving care were kept ‘blind’ to treatment allocation (yes/no/unclear)
Care providers were kept ‘blind’ to treatment allocation (yes/no/unclear)
Outcome assessors were kept ‘blind’ to participants’ exposure to the intervention (yes/no/unclear)
Use of unvalidated or intermediate outcomes (yes/no/unclear)
Selective outcome reporting on basis of the results (yes/no/unclear)
Loss to follow-up/incomplete outcome data described and acceptable (yes/no/unclear)
Analysis by intention to treat (yes/no/unclear)
Other limitations (yes/no/unclear)
Meyer, 2002 Unclear1 Yes Yes Yes No No Yes No2 No
Hamilton, 2003 Yes Yes Yes Yes No No Yes No3 Yes4,5
Sarnblad, 2003 Unclear1 Yes Yes Yes No No Yes No6 Yes4,5
Lund, 2008 Yes Yes Yes Yes No No Yes No7 No
Jacobsen, 2009 Unclear1 Yes Yes Yes No No Yes No8 Yes9
1Randomization method not described; 2stated ITT but 3 patients interupted the trial because of drug intolerance; 3three patients dropped out; 4small studies (15-30 patients; cf. Meyer et al, 2002 and Lund et al, 2008, with 62 and 100 patients respectively); 5adolescents (instead of adult patients); 6four patients dropped out; 7eight patients dropped out; 8one patient dropped out; 9Only overweight patients included (bmi >25 kg/m2)

63
Evidence table for intervention studies
This table is also suitable for diagnostic studies that compare the effectiveness of two or more tests. This only applies if the test is included as part of a test-and-treat strategy – otherwise the evidence table for studies of diagnostic test accuracy should be used.
Research question: Does eHealth improve treatment compliance, metabolic control and quality of life in patients with type 1 diabetes?
Study reference Study characteristics
Patient characteristics
Intervention (I) Comparison / control (C)
Follow-up Outcome measures and effect size
Comments
Mc Carrier 2009
RCT Poliklinisch USA
Type 1DM N=77 Exclusion: no MDI or pump, language problems, serious physical or mental illness Interventie groep: 41
I: Computer only Standardized and personal education: Living with Diabetes Program
Usual Care; Physician and diabetes nurse DVK
12mnd HbA1c, D(iabetes)E(mpowerment)S(cale)= measure for self efficacy HbA1c: non significant decrease in intervention group Sign increase in self-efficacy in intervention group P=0.04
Randomization random number tables Concealment of central randomization Not blinded Drop-outs: 14,2/19,4%
Charpentier 2011
RCT, open label, parallel F’rijk
Type 1 N=180, HbA1c chronisch >8%
G1= usual care G2= Diabeo software op smartphone (wizzard) G3= Diabeo+elke 2wk telecom
Contact 1xper 3mnd
6mnd HbA1c G1=8,9 to 9.1% G2=9,2 to 8,6% p<0.001 vs G1 G3=9,1 to 8,4% p<0.001 vs G1
G2 en G3 in 6 mnd 5 hr more hospital visits
Rossi 2010 RCT, multicenter
N=130
Device for KH/I ratio, boluswizzard and correction factor
Personal education on KH counting, bolus calculation and correction factor
6mnd I: HbA1c 8,2 naar 7,8% C: HbA1c 8,4 naar 7,9% No difference between groups I: QoL better p<0.05
Education time I: 6hr, C:12hr Less costs in time and more QoL Gew> I ns minder dan in C
Franc 2011 Systematic Review
Thompson 1999 Montori 2004 Accucheck link RCT/parallel Jansa 2006 RCT/parallel Gomez 2002 RCT, cross-over
Type 1 N=23 N=31 HbA1c>7,8% N=40, “poor controle” N=10
I: 50%:3xper week! 15min contact with diabetes nurse I:every 2wks telefon feedback <24hr Glucobeep 2x/wk, 9 telefo, 3face-to-face contacts DIABTELl with feedback <24hr
C usual care C: every 2 wk transmission of data, feedback on demand 12 face-to-face contacts Glucometer with memory; dairy
6mnd 6mnd 6mnd + 6mnd follow-up 2x6mnd
HbA1c I: 9,6 to 7,8% p<0.01 C: 9,4 to 8,9%p<0.05 HbA1c I: 9.to 7,8% C: 8,8 to 8,2% I versus C: p=0.03 HbA1c I: 8,4 to 7,5(6m) en 7,6%(12m); C: 8,9 to 7,7 (6m) en 7,6(12m) No difference between groups I: HbA1c 8,4 to 7,9% p=0,053 C: HbA1c 8,1 to 8,2% No difference between groups
Th:the nurse spent 17.25h /wk calling pats =a part-time post to cover 23pats 12 contacts in 6mnd! Also less hypo’s and better QoL Many techn problems with transmission of data via GlucoBeep

64
Rigla 2007 RCT, crossover Benhamou 2007 RCT, crossover Framer 2005 RCT parallel
N=10 CSII N=30 CSII N=93 HbA1c 8-11%
DIABTEL with feedback <24hr GlucoNet: datatransmission with weekly feedback via SMS and webbased coach T+ system with datatransmission and at least every 2wks feedback
DIABTEL no feedback GlucoNet no SMS feedback T+ system without datatransmission and feedback
8wks 2x6mnd 9mnd
I: HbA1c 8,0 to 7,8% p=0,073 C: HbA1c no change No difference between groups I: HbA1c 8,3 to 8,2% C: HbA1c 8,2 to 8,3% No difference between groups I: HbA1c 9,2 to 8,6% C: HbA1c 9,3 to 8,9% No difference between groups

65
Zoekverantwoording hoofdstuk DM type 1
Onderwerp: Database Zoekstrategie Aantal ref.
Met welk insulineschema start je bij een volwassene met een nieuw ontdekte type 1 diabetes zonder acidose?
Medline (OVID), 2008-mei 2012 Engels
Cochrane Library (Wiley)
1 exp *Diabetes Mellitus, Type 1/dt [Drug Therapy] (5415) 2 (diabetes adj1 type adj1 "1").ti. (88) 3 (type adj1 "1" adj1 diabetes).ti. (10062) 4 1 or 2 or 3 (14294) 9 exp Insulins/ad [Administration & Dosage] (14404) 10 regimen*.ti,ab. (155957) 11 basal-bolus.ti,ab. (325) 12 (daily or MDI).ti,ab. (308181) 13 (intensive adj2 therapy).ti,ab. (7771) 14 exp Insulins/ (150523) 15 insulin*.ti,ab. (244792) 16 10 or 11 or 12 or 13 (450940) 17 14 or 15 (276995) 18 16 and 17 (16022) 19 9 or 18 (27710) 20 4 and 19 (3633) 21 ((new or newly or novo or recent* or time) adj3 (diagnose* or onset)).ti,ab. (53257) 22 21 and 20 (177) 23 ((initial adj3 treatment) or (initial adj3 therap*)).ti,ab. (30765) 24 4 and 23 (32) 25 22 or 24 (202) 26 limit 25 to (english language and yr="2008 -Current") (54) 28 SR zoekfilter (1) 57 limit 26 to randomized controlled trial (13) 65 RCT (zoekfilter) (23) 87 56 or 86 (23)
#1 MeSH descriptor Diabetes Mellitus, Type 1 explode all trees #2 (diabetes and "type 1"):ti #3 (#1 OR #2) #4 MeSH descriptor Insulin explode all trees with qualifier: AD #5 (regimen* or basal-bolus or daily or MDI or(intensive and therapy)):ti #6 MeSH descriptor Insulin explode all trees #7 (insulin):ti #8 (( #6 OR #7 ) AND #5) #9 (#4 OR #8) #10 (#9 AND #3) #11 (#10), from 2008 to 2012 #12 (new or newly or novo or recent* or time ) and ( diagnose* or onset ):ti,ab,kw #13 ("initial treatment") or ("initial therapy"):ti,ab,kw #14 (#12 OR #13) #15 (#11 AND #14) 13 trials, 5 uniek
34

66
Embase (Elsevier)
(regimen*:ab,ti OR 'basal bolus':ab,ti OR
daily:ab,ti OR mdi:ab,ti OR (intensive NEAR/2 therapy):ab,ti OR scheme:ab,ti) AND ('insulin'/exp/mj OR insulin*:ab,ti) AND (((new OR newly OR novo OR recent* OR time) NEAR/3 (diagnose* OR onset)):ab,ti OR (initial NEAR/3 treatment):ab,ti OR (initial NEAR/3 therap*):ab,ti) AND [english]/lim AND [embase]/lim AND [2008-2012]/py OR ('insulin dependent diabetes mellitus'/exp/mj OR (diabetes NEAR/1 'type 1'):ti OR iddm:ab,ti [embase]/lim AND [2008-2012]/py SR of RCT > 17 , 7 uniek
Welk soort insuline bij T1DM: humaan of analoog?
Medline (OVID), 2008-mei 2012 Engels Cochrane Library (Wiley) Embase Elsevier)
1 exp *Diabetes Mellitus, Type 1/dt [Drug Therapy] (5415) 2 (diabetes adj1 type adj1 "1").ti. (88) 3 (type adj1 "1" adj1 diabetes).ti. (10062) 4 1 or 2 or 3 (14294) 9 exp Insulins/ad [Administration & Dosage] (14404) 10 ("rapid acting insuline analogues" or lispro or aspart or glulisine or "regular human insulin*" or "insuline analogues" or detemir or glargin or "neutral protamine Hagedorn" or NPH).ti,ab. (3401) 11 Insulin/aa (3270) 12 9 or 10 or 11 (18245) 13 4 and 12 (3145) 14 limit 13 to (english language and yr="2008 -Current") (725) 15 zoekfilter SR (38) 44 limit 14 to randomized controlled trial (157) 45 limit 14 to (guideline or practice guideline) (1) 46 "Practice Guidelines as Topic"/ (67640) 47 14 and 46 (7) 48 43 or 47 (44)- RL of SR #1 MeSH descriptor Diabetes Mellitus, Type 1 explode all trees #2 (diabetes and "type 1"):ti #3 (#1 OR #2) #4 MeSH descriptor Insulin explode all trees with qualifier: AD #16 ("rapid acting insuline analogues" or lispro or aspart or glulisine or "regular human insulin*" or "insuline analogues" or detemir or glargin or "neutral protamine Hagedorn" or NPH):ti,ab,kw #17 MeSH descriptor Insulin explode all trees with qualifier: AA #18 (#4 OR #16 OR #17) #19 (#18 AND #3) #20 (#19), from 2008 to 2012 195 referenties, 36 uniek insulin dependent diabetes mellitus'/exp/mj OR (diabetes NEAR/1 'type 1'):ti OR iddm.ti,ab AND ('insulin'/exp/mj/dd_ad OR 'rapid acting insuline analogues':ab,ti OR lispro:ab,ti OR aspart:ab,ti OR
287

67
glulisine:ab,ti OR 'regular human insulin':ab,ti OR 'insuline analogues':ab,ti OR detemir:ab,ti OR glargin:ab,ti OR 'neutral protamine hagedorn':ab,ti OR nph:ab,ti OR 'insulin derivative'/exp/mj OR 'isophane insulin'/exp OR 'insulin lispro'/exp) AND [english]/lim AND [embase]/lim AND [2008-2012]/py 173 referenties > 63 uniek
Zijn fluctuaties in glucosewaarden onafhankelijk van het HbA1c geassocieerd met een hoger risico op microvasculaire of macrovasculaire complicaties bij patiënten met type 1 diabetes (T1DM)?
Medline (OVID), 2008-mei 2012 Engels SR vanaf 2000
1 exp *Diabetes Mellitus, Type 1/ (44989) 2 (diabetes adj1 type adj1 "1").ti. (88) 3 (type adj1 "1" adj1 diabetes).ti. (10040) 4 "Diabetes Complications"/ (31948) 5 1 or 2 or 3 or 4 (77127) 12 (Glycaemic adj3 varia*).ti,ab. (99) 13 5 and 12 (35) 26 (glucose adj3 fluctuat*).ti,ab. (486) 27 Hyperglycemia/bl, me [Blood, Metabolism] (5554) 28 (postprandial adj3 hyperglycemia).ti,ab. (850) 29 (Glycaemic adj3 varia*).ti,ab. (99) 30 (Glycaemic adj3 fluctua*).ti,ab. (13) 31 26 or 27 or 28 or 29 or 30 (6822) 32 5 and 31 (823) 33 limit 32 to (english language and yr="2000 -Current") (493) 35 *"Diabetes Complications"/ (15334) 36 *"Diabetes Mellitus, Type 1"/ (44742) 37 risk factors/ (481580) 38 prognosis/ (318249) 39 exp cardiovascular diseases/ or coronary artery disease/ (1710868) 40 exp blood vessels/ or coronary vessels/ (576025) 41 (micro* adj4 macrovascular adj3 complications).ti,ab. (945) 42 ((macrovascular or micro* or vascular) adj3 complications).ti,ab. (11418) 43 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 (2642015) 45 33 and 43 (455) 46 exp epidemiological study/ (1405698) 47 45 and 46 (63) 48 limit 45 to (clinical conference or clinical trial, all or clinical trial or comparative study or consensus development conference or consensus development conference, nih or controlled clinical trial or government publications or guideline or meta analysis or multicenter study or practice guideline or randomized controlled trial or "research support, american recovery and reinvestment act" or research support, nih, extramural or research support, nih, intramural or research support, non us gov't or research support, us gov't, non phs or research support, us gov't, phs or "review" or validation studies) (349) 49 47 or 48 (373)
120

68
50 limit 49 to animals (98) 51 limit 50 to humans (50) 52 49 not (50 not 51) (325) 53 "Diabetes Mellitus, Type 2"/ not (1 or 2 or 3) (64449) 54 52 not 53 (308) 55 limit 54 to "all child (0 to 18 years)" (82) 56 limit 55 to "all adult (19 plus years)" (37) 57 54 not (55 not 56) (263) 58 SR (zoekfilter) (15) 13 uniek 87 limit 57 to yr="2008 -Current" (121) 88 87 not 86 (112) 107 uniek
Wanneer starten met een statine bij T1DM: bij welke risicofactoren, en op welke leeftijd?
Medline (OVID), 2008-mei 2012 Engels Embase (Elsevier) Cochrane Library
1 exp *Diabetes Mellitus, Type 1/ (44989) 2 (diabetes adj1 type adj1 "1").ti. (88) 3 (type adj1 "1" adj1 diabetes).ti. (10049) 4 1 or 2 or 3 (45708) 9 exp anticholesteremic agents/ (43922) 10 (statin* or Pravastatin or Simvastatin or Lovastatin).af. (29333) 11 ((drug* adj1 anticholesteremic) or (hypocholesteremic adj1 agent*) or (cholesterol adj1 inhibitor*) or (anticholesteremic adj1 agent*)).ti,ab. (113) 12 (Fluvastatin or Atorvastatin or pitavastatin or rosuvastatin).af. (7765) 13 9 or 10 or 11 or 12 (54650) 14 8 and 13 (2) 15 4 and 13 (131) 16 zoekfilter SR (2) (2) 45 limit 15 to (yr="2004 -Current" and english) (76) 46 limit 45 to animals (14) 47 limit 46 to humans (2) 48 45 not (46 not 47) (64) 49 44 or 48 (64) 50 49 not 44 (62) 'insulin dependent diabetes mellitus'/exp/mj OR (diabetes NEAR/1 'type 1'):ti AND ('hydroxymethylglutaryl coenzyme a reductase inhibitor'/exp/mj OR (drug* NEAR/1 anticholesteremic):ab,ti OR (hypocholesteremic NEAR/1 agent*):ab,ti OR (cholesterol NEAR/1 inhibitor*):ab,ti OR (anticholesteremic NEAR/1 agent*):ab,ti OR statin*:ab,ti OR pravastatin:ab,ti OR simvastatin:ab,ti OR lovastatin:ab,ti OR fluvastatin:ab,ti OR atorvastatin:ab,ti OR pitavastatin:ab,ti OR rosuvastatin:ab,ti) AND [english]/lim AND [embase]/lim NOT ('conference abstract':it AND [2004-2012]/py) AND [2004-2012]/py NOT 'animal experiment'/exp NOT ('insulin dependent diabetes mellitus'/exp/mj OR (diabetes NEAR/1 'type 1'):ti Embase: 33 uniek #1 MeSH descriptor Diabetes Mellitus, Type 1 explode all trees #2 (diabetes and type 1):ti #3 (#1 OR #2) #4 MeSH descriptor Hydroxymethylglutaryl-
102

69
(Wiley)
CoA Reductase Inhibitors explode all trees #5 (statin* or Pravastatin or Simvastatin or Lovastatin or Fluvastatin or Atorvastatin or pitavastatin or rosuvastatin):ti,ab,kw #6 (#4 OR #5) #7 (#3 AND #6) 2 SR (dubbel), 22 divers, 5 uniek
Is toevoeging van metformine aan insulinetherapie van meerwaarde bij patiënten met diabetes type 1?
Medline (OVID), 2008-mei 2012 Engels Cochrane (Wiley) Embase (Elsevier)
1 exp *Diabetes Mellitus, Type 1/ (44989) 2 (diabetes adj1 type adj1 "1").ti. (88) 3 (type adj1 "1" adj1 diabetes).ti. (10049) 4 1 or 2 or 3 (45708) 5 "The use of metformin in type 1 diabetes: a systematic review of efficacy".m_titl. (1) 6 Adjunct therapy for type 1 diabetes mellitus.m_titl. (1) 7 Metformin added to insulin therapy for type 1 diabetes mellitus in adolescents.m_titl. (1) 8 5 or 6 or 7 (3) 9 4 and 8 (3) 10 ("insulin dependent diabetes" or IDDM).ti. (9188) 11 4 or 10 (48990) 12 11 not 4 (3282) 13 Metformin/ (5566) 14 metformin.af. (8006) 15 13 or 14 (8006) 16 4 and 15 (125) 17 limit 16 to (english language and yr="2008 -Current") (32) 18 Zoekfilter SR (5) 47 Zoekfilter RCT (10) 69 46 or 68 (10) – SR en RCTs #1 MeSH descriptor Diabetes Mellitus, Type 1 explode all trees #2 (diabetes and type 1):ti #3 (#1 OR #2) #4 MeSH descriptor: [Metformin] explode all trees #5 metformin:ti,ab,kw #6 (#4 OR #5) #7 (#3 AND #6) 21 referenties,15 uniek ('insulin dependent diabetes mellitus'/exp/mj OR (diabetes NEAR/1 'type 1'):ti) AND ('metformin'/exp/mj OR metformin:ab,ti) AND [english]/lim AND [embase]/lim AND [2008-2012]/py 19 referenties (SR en RCTs), 11 uniek
36
Heeft het gebruik van e-Health meerwaarde op de uitkomst van de behandeling van T1D?
Medline (OVID), 2008-juli 2012 Engels, Nederlands
1 exp *Diabetes Mellitus, Type 1/ (45639) 2 ((diabetes adj1 type adj1 "1") or (type adj1 "1" adj1 diabetes)).ti. (10355) 3 ("insulin dependent diabetes" or IDDM).ti. (9198) 4 1 or 2 or 3 (49668) 9 Telemedicine/ (9281) 10 "Internet"/ (41760)
149

70
Embase (Elsevier)
11 "Remote Consultation"/ (3285) 12 "Cellular Phone"/ (3073) 13 (telemedic* or e-health or internet or "social media" or telecare or webbased or web-based or telehealth or "mobile phone*" or telemonitoring or real-time or app?).ti,ab. (164771) 14 9 or 10 or 11 or 12 or 13 (195188) 15 4 and 14 (468) 16 limit 15 to (yr="2000 -Current" and (dutch or english or french or german)) (423) 17 zoekfilter SR (13) 46 zoekfilter RCTs (100) 68 exp epidemiological studies/ (1437723) 69 16 and 68 (54) – niet bijgevoegd. 70 67 or 69 (144) 71 70 not 45 (136) 'insulin dependent diabetes mellitus'/exp/mj OR (diabetes NEAR/3 'type 1'):ti OR 'insulin dependent diabetes mellitus':ti OR iddm:ti AND ('telemedicine'/exp/mj OR 'internet'/exp/mj OR 'mobile phone'/exp OR 'teleconsultation'/exp/mj OR telemedic*:ab,ti OR 'e health':ab,ti OR internet:ab,ti OR 'social media':ab,ti OR telecare:ab,ti OR webbased:ab,ti OR 'web based':ab,ti OR telehealth:ab,ti OR (mobile NEAR/2 phone*):ab,ti OR telemonitoring:ab,ti OR 'real time':ab,ti OR app?:ab,ti) AND [embase]/lim AND [2000-2013]/py SR (14) en RCTs (73) (filters) – 36 uniek
Wat is de optimale organisatie van zorg voor DM1 patiënten in de tweedelijn?
Medline (OVID), 2000-aug. 2012 Engels
1 exp *Diabetes Mellitus, Type 1/ (45639) 2 ((diabetes adj1 type adj1 "1") or (type adj1 "1" adj1 diabetes)).ti. (10361) 3 ("insulin dependent diabetes" or IDDM).ti. (9198) 4 1 or 2 or 3 (49674) 9 "Specialization"/ (20678) 10 4 and 9 (30) 11 (endocrinologist* or "diabetes specialist" or diabetologist*).ti,ab. (2784) 12 "specialist care".ti,ab. (916) 13 (endocrinologist* or "diabetes specialist*" or diabetologist*).ti,ab. (2836) 14 endocrinology/ (4000) 15 or/11-14 (7409) 16 4 and 15 (282) 17 limit 16 to (english language and yr="2000 -Current") (145)
Zoekfilters voor systematische reviews en gerandomiseerd klinisch onderzoek zijn gebaseerd op de zoekfilters van het Scottish Intercollegiate Guidelines Network (SIGN) - http://www.sign.ac.uk/
Related Documents