This article was downloaded by: [Dalhousie University] On: 08 October 2014, At: 13:00 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Home Health Care Services Quarterly Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/whhc20 Home Care Safety Markers: A Scoping Review Marilyn Macdonald PhD a , Ariella Lang PhD b , Jan Storch PhD c , Lynn Stevenson PhD d , Susan Donaldson MHSc e , Tanya Barber MA a & Kristine Iaboni MA b a Dalhousie University , Halifax , Nova Scotia , Canada b VON Canada , Ottawa , Ontario , Canada c University of Victoria , Victoria , British Columbia , Canada d Vancouver Island Health Authority , Victoria , British Columbia , Canada e Canadian Home Care Association , Port Perry , Ontario , Canada Accepted author version posted online: 13 Mar 2013.Published online: 16 May 2013. To cite this article: Marilyn Macdonald PhD , Ariella Lang PhD , Jan Storch PhD , Lynn Stevenson PhD , Susan Donaldson MHSc , Tanya Barber MA & Kristine Iaboni MA (2013) Home Care Safety Markers: A Scoping Review, Home Health Care Services Quarterly, 32:2, 126-148, DOI: 10.1080/01621424.2013.783523 To link to this article: http://dx.doi.org/10.1080/01621424.2013.783523 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
This article was downloaded by: [Dalhousie University]On: 08 October 2014, At: 13:00Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Home Health Care Services QuarterlyPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/whhc20
Home Care Safety Markers: A ScopingReviewMarilyn Macdonald PhD a , Ariella Lang PhD b , Jan Storch PhD c ,Lynn Stevenson PhD d , Susan Donaldson MHSc e , Tanya Barber MA a
& Kristine Iaboni MA ba Dalhousie University , Halifax , Nova Scotia , Canadab VON Canada , Ottawa , Ontario , Canadac University of Victoria , Victoria , British Columbia , Canadad Vancouver Island Health Authority , Victoria , British Columbia ,Canadae Canadian Home Care Association , Port Perry , Ontario , CanadaAccepted author version posted online: 13 Mar 2013.Publishedonline: 16 May 2013.
To cite this article: Marilyn Macdonald PhD , Ariella Lang PhD , Jan Storch PhD , Lynn StevensonPhD , Susan Donaldson MHSc , Tanya Barber MA & Kristine Iaboni MA (2013) Home CareSafety Markers: A Scoping Review, Home Health Care Services Quarterly, 32:2, 126-148, DOI:10.1080/01621424.2013.783523
To link to this article: http://dx.doi.org/10.1080/01621424.2013.783523
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &
Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014
Home Health Care Services Quarterly, 32:126–148, 2013Copyright © Taylor & Francis Group, LLCISSN: 0162-1424 print/1545-0856 onlineDOI: 10.1080/01621424.2013.783523
Home Care Safety Markers: A Scoping Review
MARILYN MACDONALD, PhDDalhousie University, Halifax, Nova Scotia, Canada
ARIELLA LANG, PhDVON Canada, Ottawa, Ontario, Canada
JAN STORCH, PhDUniversity of Victoria, Victoria, British Columbia, Canada
LYNN STEVENSON, PhDVancouver Island Health Authority, Victoria, British Columbia, Canada
SUSAN DONALDSON, MHScCanadian Home Care Association, Port Perry, Ontario, Canada
TANYA BARBER, MADalhousie University, Halifax, Nova Scotia, Canada
KRISTINE IABONI, MAVON Canada, Montreal, Quebec, Canada
Safety in home care is a new research frontier, and one in whichdemand for services continues to rise. A scoping review of thehome care literature on chronic obstructive pulmonary diseaseand congestive heart failure was thus completed to identify safety
The results of the conducted scoping review have been presented (but not published)at the following conferences: Canadian Association of Schools of Nursing, “Innovation inResearch and Knowledge Exchange,” Toronto, Ontario, May 7–10, 2012; Ontario Home CareAssociation, “Showcasing Our Best!,” Mississauga, Ontario, May 24, 2012; The CanadianAssociation for Health Services and Policy Research, “Innovations for Health SystemImprovement: Balancing Costs, Quality and Equity,” Montreal, Quebec, May 29–31, 2012;The Ontario Association of Community Care Access Centres, “Knowledge and Inspiration,”Toronto, Ontario, June 17–19, 2012; and Canadian Nurses Association, “Nurses: Movers andShapers,” Vancouver, British Columbia, June 18–20, 2012.
The authors acknowledge the Canadian Institutes for Health Research, without whomthis research would not have been possible.
Address correspondence to Marilyn Macdonald, PhD, Dalhousie University,5869 University Avenue, P.O. Box 15000, Halifax, Nova Scotia B3H 4R2, Canada. E-mail:[email protected]
126
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

Home Care Safety Markers 127
markers that could serve to develop our understanding of safetyin this sector. Results generated seven safety markers: (a) Homealone; (b) A fixed agenda in a foreign language; (c) Strangers inthe home; (d) The butcher, the baker, the candlestick maker; (e)Medication mania; (f) Out of pocket: The cost of caring at home;and (g) My health for yours: Declining caregiver health.
KEYWORDS CHF, chronic obstructive pulmonary disease,congestive heart failure, COPD, home care, safety
INTRODUCTION
Client safety is a new frontier within the home care context. Given the dra-matic increase in the amount of care provided within the home and thecomplexity inherent in care delivery within this sector, it is essential todevelop our understanding of safety and or antecedents to safety. To this enda scoping review of the home care literature focused on chronic obstructivepulmonary disease (COPD) and congestive heart failure (CHF) was con-ducted. The review was focused on these two chronic illnesses based onthe prevalence and burden of COPD and CHF, the volume of home careliterature, and study resources.
Globally, COPD affects 64 million people. The European Unionaccounted for 13.8 million (European COPD Coalition, n.d.), the UnitedStates of America 16 million (COPD International, 2012), and Canadaapproximately 772,200 (Public Health Agency of Canada [PHAC], 2012).Canadians affected described their health as fair to poor, or steadily declining(PHAC, 2012). Worldwide, 26 million people have CHF including 5.7 mil-lion Americans (Centers for Disease Control and Prevention [CDC], 2012),6.5 million Europeans, and approximately 350,000 Canadians (CanadianHeart Failure Network, 2013; López-Sendón, 2011). Individuals living withthese chronic illnesses do so at home, and the majority of care is providedby family caregivers (Reinhard, Levine, & Samis, 2012; Canadian Home CareAssociation [CHCA], 2008).
BACKGROUND
The CHCA (2008) reported that from 1997 to 2007 home care grew by51%. The prevalence of COPD and CHF in the population means increas-ing demands on home care, and is associated with considerable client,caregiver, and societal burden. Clients have multiple health problems includ-ing dementia, experience sensory loss, and persistently use acute care
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

128 M. Macdonald et al.
services (Reinhard et al., 2012; Hirdes, 2011; Mitchell, 2010). Their caregiversare usually middle aged or older, and are required to coordinate clientcare that grows exponentially with little assistance resulting in negativeexperiences and depression (Reinhard et al., 2012). The financial cost asso-ciated with CHF and COPD annually in the United States is 34 and 32 billionrespectively (CDC, 2012; COPD International, 2012).
Client safety research is an area largely neglected within the homecare context. This has resulted in a significant knowledge gap regardinghome care safety in general, and specifically in how it relates to home carerecipients and their unpaid caregivers (Lang & Edwards, 2006).
PURPOSE
The purpose of this scoping review was to identify markers that can belinked to safety in home care for clients and/or caregivers.
METHODS
Overview
The aim of a scoping review is to achieve breadth rather than depth on atopic. These reviews do not typically begin with a defined question like asystematic review, but rather remain open to what the literature may revealthroughout (Arksey & O’Malley, 2005; Weeks & Strudsholm, 2008). Teammembers worked in a collaborative manner to share information and makedecisions throughout the review process. The following section describes thesources, search terms, inclusion and exclusion criteria, synthesizing process,and analysis of the data.
Sources
The primary sources used to obtain evidence for this review included: (a)electronic bibliographic databases (12); (b) grey literature from governmentand professional association websites (5 sources); and (c) manual searchesof publications conducted on professional journals and academic periodi-cals. The full list of data sources used for this literature review is listed inTable 1.
Search Terms
The initial search strategy of including COPD and CHF in the subject, keyword, and descriptor fields yielded very few articles; therefore, the team
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

Home Care Safety Markers 129
TABLE 1 Data Sources for Literature Review
Electronic bibliographicdatabases searched Grey literature searched
British Nursing IndexCINAHLCochraneEMBASEMedlineOvidPsychInfoProQuest Dissertations
and Theses Full TextPubMedSociological AbstractsTheses Canada PortalWeb of Science
Canadian government websites: Canadian Agency for Drugsand Technologies in Health
(http://www.cadth.ca/en/products/health-technology-assessment)
Institute for Safe Medication Practices(http://www.ismp-canada.org/index.htm)Professional association websites: Institute of Electrical and
Electronics EngineersConference Proceedings, 1st Transdisciplinary Conference on
Distributed Diagnosis and Home Healthcare(http://ieeexplore.ieee.org/xpl/mostRecentIssue.
jsp?punumber=10817)National Institute for Health and Clinical Excellence(http://pathways.nice.org.uk/pathways/chronic-heart-
failure)(http://pathways.nice.org.uk/pathways/chronic-obstructive-
pulmonary-disease)
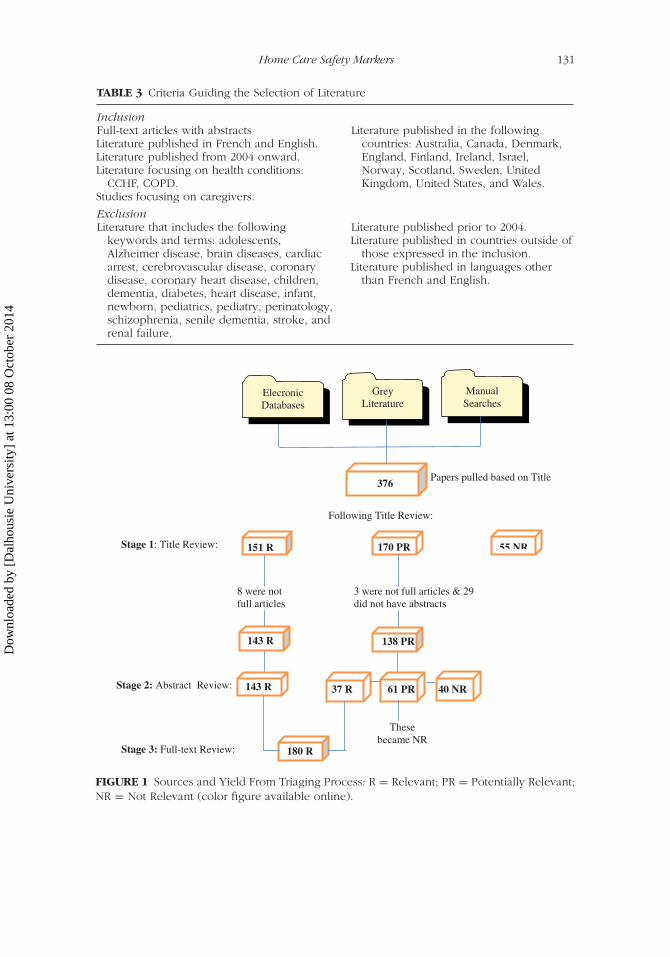
used the search strategy of placing COPD and CHF in the title fields with anestablished list of search terms included in the subject/keyword/descriptorfields (see Table 2), and terms to be excluded from the search process (seeTable 3). This produced 376 potential articles. Further screening resulted in180 articles included in this scoping review.
Inclusion/Exclusion
The criteria employed in identifying relevant publications included geo-graphical location of study, publication, and language. The literature deemedrelevant and used for the review was published between 2004 and 2011;though a significant portion was published between 2007 and 2009. All pub-lications are in English, except for grey literature available in French andEnglish. Table 3 lists the criteria guiding the selection of literature includedas well as excluded in the final review.
Triaging Process
This process involved three stages, with designated team members rankingthe titles, abstracts, or full-text articles as: (a) relevant, (b) potentially rele-vant, or (c) not relevant. In Stage 1, all titles retrieved were ranked by fourmembers of the research team. Those titles ranked as relevant and potentiallyrelevant were carried over to Stage 2. In Stage 2, the abstracts of all relevantand potentially relevant articles were reviewed and ranked by four teammembers. Only articles ranked as relevant from Stage 2 were carried over to
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014
130 M. Macdonald et al.
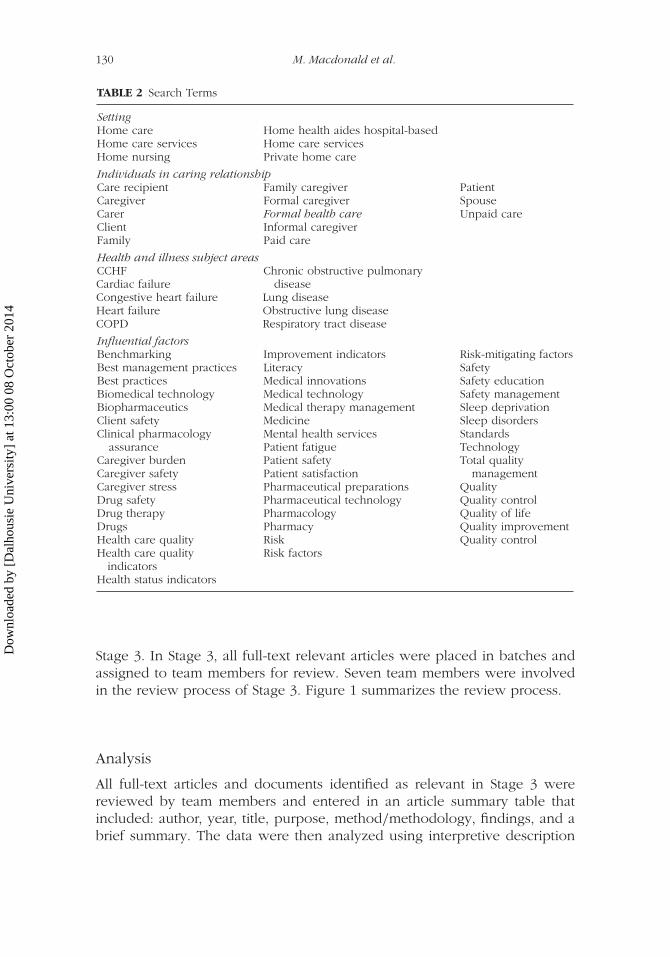
TABLE 2 Search Terms
SettingHome care Home health aides hospital-basedHome care services Home care servicesHome nursing Private home care
Individuals in caring relationshipCare recipient Family caregiver PatientCaregiver Formal caregiver SpouseCarer Formal health care Unpaid careClient Informal caregiverFamily Paid care
Health and illness subject areasCCHFCardiac failureCongestive heart failureHeart failureCOPD
Chronic obstructive pulmonarydisease
Lung diseaseObstructive lung diseaseRespiratory tract disease
Influential factorsBenchmarking Improvement indicators Risk-mitigating factorsBest management practices Literacy SafetyBest practices Medical innovations Safety educationBiomedical technology Medical technology Safety managementBiopharmaceutics Medical therapy management Sleep deprivationClient safety Medicine Sleep disordersClinical pharmacology Mental health services Standards
assurance Patient fatigue TechnologyCaregiver burden Patient safety Total qualityCaregiver safety Patient satisfaction managementCaregiver stress Pharmaceutical preparations QualityDrug safety Pharmaceutical technology Quality controlDrug therapy Pharmacology Quality of lifeDrugs Pharmacy Quality improvementHealth care quality Risk Quality controlHealth care quality
indicatorsRisk factors
Health status indicators
Stage 3. In Stage 3, all full-text relevant articles were placed in batches andassigned to team members for review. Seven team members were involvedin the review process of Stage 3. Figure 1 summarizes the review process.
Analysis
All full-text articles and documents identified as relevant in Stage 3 werereviewed by team members and entered in an article summary table thatincluded: author, year, title, purpose, method/methodology, findings, and abrief summary. The data were then analyzed using interpretive description
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014
Home Care Safety Markers 131
TABLE 3 Criteria Guiding the Selection of Literature
InclusionFull-text articles with abstractsLiterature published in French and English.Literature published from 2004 onward.Literature focusing on health conditions:
CCHF, COPD.Studies focusing on caregivers.
Literature published in the followingcountries: Australia, Canada, Denmark,England, Finland, Ireland, Israel,Norway, Scotland, Sweden, UnitedKingdom, United States, and Wales.
ExclusionLiterature that includes the following
keywords and terms: adolescents,Alzheimer disease, brain diseases, cardiacarrest, cerebrovascular disease, coronarydisease, coronary heart disease, children,dementia, diabetes, heart disease, infant,newborn, pediatrics, pediatry, perinatology,schizophrenia, senile dementia, stroke, andrenal failure.
Literature published prior to 2004.Literature published in countries outside of
those expressed in the inclusion.Literature published in languages other
than French and English.
Papers pulled based on Title
8 were not full articles
Elecronic Databases
Grey Literature
Manual Searches
376
Stage 3: Full-text Review:
143 R
138 PR 143 R
151 R 170 PR 55 NR
Following Title Review:
Stage 1: Title Review:
3 were not full articles & 29 did not have abstracts
Stage 2: Abstract Review: 37 R 61 PR 40 NR
180 R
These became NR
FIGURE 1 Sources and Yield From Triaging Process: R = Relevant; PR = Potentially Relevant;NR = Not Relevant (color figure available online).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

132 M. Macdonald et al.
TABLE 4 Definition of Terms
Client Term used to define those individuals who are receiving health careservices within the home. Using the term “client” acknowledgesthe autonomy and choice individuals have in pursuing andobtaining health care services. It also serves to break thehierarchical patterns that often exist when individuals are seen as,or identify as, patients within the health system.
Caregiver Refers to “individuals who are in an unpaid role but are responsiblefor caring for the client. Caregivers are often family members orfriends. Family members are individuals identified by the clientand/or caregiver as being close to the client through blood, legal,or emotional ties and who may or may not reside in the samehome as the identified client” (Macdonald & Lang, 2010, p. 8).Caregivers may live with the client to whom they provide care orlive separately from the client, visiting as needed. In this review,two populations of caregivers were then identified: live-incaregivers and visiting caregivers.
Personal supportworkers
The regulated and non-regulated workers who are paid employeesof organizations providing home support services. These workersmay assist with personal care, bathing, meal preparation, andhousekeeping. They may work with, but are a separate body from,health care professionals such as nurses, therapists, case managers,pharmacists, and doctors.
Well-being The term “well-being” relates to both client and caregiver in thisscoping review and encompasses the physical, emotional, andpsychological health of these two populations.
Safety marker Refers to indicators of safety related to the client and/or caregiver.These indicators may embody conditions or situations thatcompromise the safety of home care clients and caregivers, butmay not habitually be acknowledged or identified as such(Macdonald & Lang, 2010).
methodology (Thorne, Kirkham, & O’Flynn-Magee, 2004) to identify pat-terns deemed to represent safety markers for clients and/or caregivers. Thedefinition of terms used in the manuscript is appended in Table 4.
RESULTS AND DISCUSSION
Seven markers were identified as relevant to safety in home care for clientsand/or caregivers: (a) Home alone; (b) A fixed agenda in a foreign language;(c) Strangers in the home; (d) The butcher, the baker, the candlestick maker;(e) Medication mania; (f) Out of pocket: The cost of caring at home; and (g)My health for yours: Declining caregiver health. These markers are intention-ally presented in this order to illustrate how they are linked to each otherand to client and caregiver health and safety.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

Home Care Safety Markers 133
Home Alone
Individuals suffering from chronic illnesses such as COPD and CHF often facesymptoms that restrict their ability to engage in social activities, hobbies, andother interests. The marker “Home Alone” refers to home care clients’ (andoften their caregivers’) perceptions that they have been left by themselves todeal with their illness. This perception is a result of feelings of seclusion, lackof support, and decreased socialization experienced by clients with live-infamily or spousal support, as well as those who live alone.
Researchers have found that clients with COPD and CHF arefrustrated and are no longer able to participate in their social sup-port networks due to diminished physical ability to visit friends andfamily, as well as limited engagement in previously enjoyed hob-bies and activities (Aldred, Gott, & Gariballa, 2005; Cortis & Williams,2007; Elofsson & Ohlén, 2004). Specifically, it is the unpredictabilityof their illness and health status, as well as the presence of symp-toms such as breathlessness, fatigue, insomnia, headaches, falls andreduced mobility, that contribute to clients being housebound or highlydependent on others for commitments inside and outside the home(Aldred et al., 2005; Brännström, Ekman, Norberg, Boman, & Strandberg,2006).
Home care clients describe feeling abandoned or neglected by friendsand family members whose visits became less frequent as the illnessprogressed (Brännström et al., 2006; Elofsson & Ohlén, 2004). These feel-ings of abandonment extended to include health care professionals aswell. Clients with COPD and/or CHF reported feeling that they wereleft on their own to manage an illness; an illness they may not fullyunderstand due to a lack of communication, education, and informationprovided by health care professionals (Aldred et al., 2005; Brännströmet al., 2006; Hopp, Thornton, & Martin, 2010). Home care clients wholive alone were shown to experience greater loneliness than those wholived with a spouse (Brännström et al., 2006). In addition, these clientshad a higher risk for non-adherence to prescribed medication and dietaryrestrictions, both significant safety issues, thus likely requiring more fre-quent follow-up and support (Brännström et al., 2006; Davidson, Paull,Rees, Daly, & Cockburn, 2005; Sauvé, Lewis, Blankenbiller, Rickbaugh, &Pressler, 2009). Researchers also identified living alone as a predictor ofdepression and anxiety in clients with COPD and CHF (Albert & Zeller,2009; Havranek, Spertus, Masoudi, Jones, & Rumsfeld, 2004). Depressionand anxiety are important safety markers for clients as they are associatedwith higher mortality, an increased degree of health care usage, reducedquality of life, and an overall negative impact on an individual’s ability tofunction (Hasson et al., 2008; Yohannes, Willgoss, Baldwin, & Connolly,2010).
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

134 M. Macdonald et al.
A “Fixed” Agenda in a “Foreign” Language
A “fixed agenda” refers to the reality that the information provided toclients and their families about how to manage their chronic illness athome often follows a pre-determined script that does not recognize thespecific information needs required for each case. Often, this informationis provided using clinical terminology or medical jargon described by clientsas hearing a “foreign” language. The barriers to effective transmission ofrelevant information identified in this scoping review included: (a) lack oftime for communication from health care professionals, (b) varying difficul-ties in client or caregivers’ reception of information, and (c) problems inunderstanding the technology necessary for safe care.
LACK OF TIME FOR ADEQUATE COMMUNICATION
BY HEALTH CARE PROFESSIONALS
Despite the information needs of clients suffering from COPD and CHF athome, evidence suggests that there is a perceived lack of time and effortby health care professionals in communicating such information to clientsand answering questions based upon individual client needs (Aldred et al.,2005; Hopp et al., 2010). Lack of specific guidance or explanations about anillness or about symptoms may also lead to increased hospitalizations (Hoppet al., 2010) or create unnecessary client anxiety that may contribute to amismanagement of health symptoms (Hasson et al., 2009) and increase strainfor caregivers when making decisions about home care (Hasson et al., 2008).
CLIENT AND CAREGIVER RECEPTION OF INFORMATION
Individual client and caregiver characteristics influence effective communi-cation and capacity to receive information (Michaels & Meek, 2004; Myers,Grant, Lugn, Holbert, & Kvedar, 2006; Sauvé et al., 2009; Scherr et al., 2009).For example, several researchers have identified that cognitive impairments,such as memory loss and decreased functionality resulting from illness ormedications, may challenge a client’s ability to learn and thereby createsafety concerns because self-care decisions are based on misunderstandingthe shared information (Bartoli, Zanaboni, Masella, & Ursini, 2009; Dansky,Vasey, & Bowles, 2008; Horton, 2008; Law & Lehoux, 2004; Slater, Neander, &Carey, 2006).
Reception of information can be further confounded by cultural andlanguage barriers due to differences in the care management and infor-mation needs of clients from different cultural backgrounds (Evangelista,Ter-Galstanyan, Moughrabi, & Moser, 2009). This poses a safety risk becausethe care needs required for this group of clients may not be fully met.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

Home Care Safety Markers 135
Therefore, there is a need to avoid a “fixed agenda” for providing informationto home care clients (Horton, 2008).
TECHNOLOGY CONCERNS
Technology was found to pose an additional challenge to the reception ofinformation for clients with a diagnosis of COPD and/or CHF. Technology isregarded as a positive and important tool that increases self-management andmonitoring capacity among home care clients and increases communicationbetween clients and health care professionals. However, impairments suchas diminished attention and slower motor reactions associated with CHFhave been shown to challenge a client’s ability to properly learn; utilize; andmaintain devices, equipment, or technology (Bartoli et al., 2009; Myers et al.,2006; Radai et al., 2008; Sauvé et al., 2009; Scherr et al., 2009).
Strangers in the Home
Home care is a unique environment where clients and their families haveauthority in the home, and health care professionals and personal supportworkers are guests within their clients’ homes. “Strangers in the home” refersto the number of professionals and personal support workers and staff fromvarious agencies involved in most home care settings, contributing to theclient’s home life and feelings of safety being somewhat contested whilesearching for continuity in care providers.
THE SEARCH FOR CONTINUOUS CARE
Depending on the model, the delivery of home care can alter the routineof the home setting, leaving the client and family feeling somewhat uneasywhile striving to remain in charge. Models that involve the use of severalagencies may result in numerous individuals from various agencies engagingwith a client in a manner that lacks coordination (Chattoo & Atkin, 2009).This lack of coordination leaves clients feeling overwhelmed by variouspeople coming into the home. Communication between health care pro-fessionals and personal support workers from multiple agencies can also bedifficult, which can pose safety risks associated with either the omission orduplication of specific care delivery tasks for clients (Aldred et al., 2005;Corsello & Tinkelman, 2008; Hasson et al., 2008).
Clients and their families valued continuity of care from their personalsupport workers and health care professionals with whom they can buildeffective and supportive relationships (Barnett, 2005; Boyd et al., 2009;British Thoracic Guideline Development Group, 2004; Davidson et al.,2005). Without continuity of care, it becomes extremely difficult for clientsand caregivers to develop trust for any one health care professional, thereby
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

136 M. Macdonald et al.
limiting their ability to communicate effectively with these individuals(Aldred et al., 2005). This limitation in trust and communication alsodecreases comfort levels in the home as clients feel like a burden to thesestrangers (Hasson et al., 2008).
The Butcher, the Baker, the Candlestick Maker
The role of the caregiver in the context of home care is multifaceted. Unlikethe team of health care professionals that are trained and prepared forvarying situations, caregivers receive no such formal education or training.The caregiver, in attempting to meet all the responsibilities and changingexpectations, becomes “the butcher, the baker, the candlestick maker” andany other role that is required in caring for a loved one. This attempt tobe everything within the caregiver role can cause strain and result in safetyrisks for both the client and caregiver. This marker encompasses two mainissues for caregivers that link to safety: (a) increasing responsibilities and (b)changes in roles.
INCREASING RESPONSIBILITIES
Caring for a client at home is complex. Most care within the home is carriedout by family members who face multiple responsibilities and expectationswith little preparation or information regarding managing an illness (Aldredet al., 2005; Clark et al., 2007; Hasson et al., 2009). Demands and respon-sibilities placed on them continue to intensify as the ill family member’scapabilities decrease. The caregiver must therefore fulfill the physical andsocial functions and needs of the client (Goodlin, 2009), particularly whenpersonal support workers or health care professionals are unavailable oroff duty. Many times, caregivers are expected to take on these responsi-bilities without hesitation, help, or support from other family members orhealth care professionals (Aldred et al., 2005) despite their already intensify-ing burden, stress, and drained levels of functioning (Ågren, Frisman, Berg,Svedjeholm, & Strömberg, 2009).
The more the client relies upon the caregiver, the greater the increase insafety risks; since there are more things to remember, do, and take care of fortheir loved one and for themselves. These responsibilities place a consider-able burden on caregivers (Abernethy, Currow, Clarke, Newton, & Davidson,2009; Goodlin, 2009; Leff et al., 2005; Narsavage & Chen, 2008; Saunders,2008), and these overwhelming tasks can create many unforeseen safetyrisks for both caregiver and client at home. For example, managing multipleand growing tasks can lead to added exhaustion and declining health for thecaregiver (Brewin, 2004; Hwang & Dracup, 2010), decreased emotional well-being within the caregiver (Bakas, Pressler, Johnson, Nauser, & Shaneyfelt,2006; Luttik, Lesman-Leegte, & Jaarsma, 2009), an inability to cope with stress
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

Home Care Safety Markers 137
due to their caregiver role (Bakas et al., 2006; Pressler et al., 2009), andnegative perceived caregiver outcomes such as a deteriorating future out-look and diminished financial well-being (Bakas et al., 2006; Bennett, Bakas,Johnson, & Shaneyfelt, 2004; Hasson et al., 2009).
CHANGES IN ROLES
As roles and responsibilities change, caregivers may feel they are losing theirself-sufficiency and independence (Freydberg, Strain, Tsuyuki, McAlister, &Clark, 2010). Not only do many caregivers work outside of the home, theycontinue working within the home (Saunders, 2010). These changes withinthe caregiver’s life may leave them feeling resentful and burdened on top ofthe already stressful task of taking care of their loved one (Aldred et al., 2005;Nordtug & Holen, 2011; Spence et al., 2008). Caregivers identified negativerole changes such as taking on multiple roles (e.g., wife, husband, daughter,son, sibling, nurse, doctor, etc.; Harris, 2007; Spence et al., 2008) and under-taking tasks that were previously the responsibility of the current client (e.g.,housework and cooking for many men, gardening and house maintenancefor many women, or managing all household finances; Bennett et al., 2004;Hasson et al., 2008; Hwang, Luttik, Dracup, & Jaarsma, 2010). These changesin roles frequently led caregivers to feel as though their identity was lost(Brewin, 2004; Spence et al., 2008).
On the other hand, clients reported feeling badly or frustrated watchingtheir spouses contend with what they saw as “gender-specific” work, such asmale spouses doing domestic labor and female spouses performing generalhouse maintenance activities such as mowing the lawn. This may result fromthe inability of the client to continue fulfilling the roles and responsibilitiesthey previously held themselves (Aldred et al., 2005). Feelings of frustrationand worry that develop as a result of taking on the caregiver role may evenlead to aggravation or incidences of violence toward the client by caregivers(Brewin, 2004; Woolfe, McMillan, & Conway, 2007).
Medication Mania
Medication management is a challenge when living with chronic illness.Individuals with COPD, for instance, vary widely in relation to lung func-tion, co-morbidities, cognitive functions, hand strength, and lifestyle; all ofwhich impact on the number and types of medications and devices used,as well as the degree to which these are properly managed (Caress, Luker,Chalmers, & Salmon, 2009; Fromer, Goodwin, & Walsh, 2010). The safetymarker “Medication Mania” refers to the myriad of medications needing orga-nization and monitoring by clients, caregivers, and health care professionalswithin the home care system and is characterized by changing medicationregimes and overcoming medication-related barriers.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

138 M. Macdonald et al.
MULTIPLE MEDICATION REGIMES
The management of medication poses a significant safety concern for homecare recipients and caregivers. Clients and their caregivers are commonlyresponsible for multiple medications (Caress et al., 2009; Hwang et al.,2010; Slater et al., 2006; Triller & Hamilton, 2007; Upadaya et al., 2004),with some of these medications needing specific and complex devices,techniques, or guidelines for administration (Fromer et al., 2010; Quinn,2005). Failure to execute one step or adding an additional step in a med-ication regime can considerably diminish its efficacy, as well as presentpotential safety concerns, such as worsening symptoms or increases in thefrequency of exacerbations (Fromer et al., 2010). Furthermore, if the pur-pose of the medication is not clearly explained or understood, this canimpact on how or if clients continue to take a particular medication. Forinstance, VanderSchaaf, Olson, Billups, Hartsfield, and Rice (2010) reasonedthat participants stopped using inhalers because they felt they were not effec-tive in relieving their symptoms, when the actual purpose of the inhalerwas not to relieve symptoms but to prevent exacerbations. This examplehighlights important safety implications that are intertwined with medical lit-eracy and adequate medical education to help clients and caregivers managemedications safely.
It is evident from the home care literature that without a certainlevel of medication literacy and proper medication management by clients,caregivers, and health care professionals, the health status of clients candecline (Horne & Payne, 2004; Morgan et al., 2006; Schmidt, Sheikzadeh,Beil, Pattern, & Stettin, 2008).
BARRIERS TO MEDICATION MANAGEMENT
Variations in managing medications were also caused by barriers the clientsand caregivers faced when making decisions regarding their medicationtreatments (Dickson & Riegel, 2009). Issues or areas of concern leading toresistance in medication management include:
● confusion and knowledge deficits regarding their medications and how totake them (Morgan et al., 2006; Polzien, 2007; Roberts, Leeder, & Robinson,2008; Smith, 2010; VanderSchaaf et al., 2010);
● lack of physical ability (e.g., inability to open medication bottles;Dickson & Riegel, 2009);
● unwanted or unpleasant side effects with taking the medication (e.g.,increased urination from diuretics, insomnia, fatigue, sexual dysfunction,etc.; Freydberg et al., 2010; Horne & Payne, 2004; Smith, 2010);
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

Home Care Safety Markers 139
● obstacles in the health care system (e.g., difficulties getting in touch withhealth care personnel, tiring travel time, long waiting time, supply short-ages, medication costs, etc.; Clark et al., 2007; Davidson et al., 2005;Lundman, Brännström, Hägglund, & Strandberg, 2009; Upadaya et al.,2004; VanderSchaaf et al., 2010).
Overall, medication management in the context of home care is empha-sized as a significant safety marker that may jeopardize the health and safetyof the client.
Out of Pocket: The Cost of Caring at Home
The economics of caring is a growing issue within the home care context.Responsibilities for patient care are increasingly being moved from publicinstitutions to client homes. This creates a personal burden—both economicand emotional—for home care clients and their caregivers, thus raising safetyconcerns regarding their physical, psychological, and economic well-being.Recipients of home care frequently find themselves “out of pocket” from thehigh expenditures, lack of funding, and other personal and financial costs ofreceiving care at home.
OUT OF POCKET FOR EQUIPMENT AND SERVICES
Many home care recipients experienced high personal expenditures forhealth care equipment and services. For example, Hasson et al. (2009)reported that many caregivers had made modifications to their homes, suchas installing modified shower facilities as caregivers and clients did not wantto face long waiting lists or shortages of available equipment through fundedprograms. Clients and caregivers vary in their personal capacity to incur addi-tional costs, and this can result in inequities in the degree of quality and safetyof home care. For those with limited funds, incurring costs may well increasestress. For example, clients with COPD often require oxygen therapy. Forthese clients, the ability to access treatments such as liquid oxygen therapyholds benefits that include the provision of a lighter, more convenient sourcefor oxygen therapy outside the home. But as Law (2005) indicates, this typeof oxygen is associated with costs four times higher than standard oxygentherapy. If the liquid oxygen therapy is not covered by public funding, thenclients and caregivers are faced with the difficult decision to go with themore cumbersome traditional forms of portable oxygen, go without, or incurhigh costs out of their own pockets for the more convenient liquid portableoxygen (Law, 2005). Safety implications are significant because when themore portable forms of oxygen are not feasible, those clients may make the
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

140 M. Macdonald et al.
decision to forgo using oxygen during outings completely, creating a healthsafety risk (Law, 2005).
CHALLENGES TO NAVIGATING THE SYSTEM
Home care clients have also expressed frustration in their attempts to nav-igate various systems for publically funded services and equipment. Thosewho can, incur the costs for the resources required privately, increasingfinancial stress; while those who cannot afford the private path are left feel-ing helpless and without the resources they need. Clients also expressedthat overall support and advice regarding the economic or financial side ofreceiving care at home was not readily available (Brewin, 2004; Hasson et al.,2009). For example, in Hasson et al.’s (2009) study, participants reported thatinformation on available support services was sporadic and that the onlyinformation on benefit or funding programs came from hospital and clinicpamphlets, which were very limited in detail. Similarly, Brewin’s (2004) studyexamining the quality of life of caregivers found that participants were con-fused as to what assistance programs they would qualify for. These examplesillustrate those who cannot afford to pay are at a higher risk because theyare waiting longer for needed equipment and services.
CARING, WORK, AND WAGES
The costs of caring at home include growing financial burdens, stress inoverseeing household bills and health expenditures for services and equip-ment, and changes in financial well-being or status for both the client and thecaregiver (Bennett et al., 2004; Hasson et al., 2009; Hwang & Dracup, 2010).These changes are amplified by reduced working hours for pay due to anillness or caring for those who are ill. For instance, clients with a chronicillness are often forced to stop working years earlier than expected dueto their poor health (e.g., decreased mental and physical capacity to workwithout the necessary rest; Brewin, 2004; Lundman et al., 2009). Likewise,family caregivers commonly decrease their working hours to part-time sta-tus, take pay-cuts to acquire flexible schedules, or incur travel costs in orderto provide care for their loved ones (Brewin, 2004; Mendoza et al., 2009).Caregivers then have to adjust not only to a reduced income, but also tolower status employment, sometimes going from more “professional” rolesto “menial” work (Brewin, 2004). These adjustments result in the family’sincreasing financial stress and negative outlooks regarding their present andfuture economic state, often leading to depression and poor health (Bennettet al., 2004; Brewin, 2004; Evangelista et al., 2009; Hwang & Dracup, 2010;Suwanno, Petpichetchian, Riegel & Issaramalai, 2009). Overall, the healthand well-being of home care clients and family caregivers are put at risk dueto the economic costs of managing care at home.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

Home Care Safety Markers 141
My Health for Yours: Declining Caregiver Health
The health of caregivers is largely affected by their caregiving responsibilities,which are often complex, and ever-mounting. Many caregivers experiencereal and perceived expectations that compel them to be present for theirloved ones 24 hours a day, often to the detriment of their own health.Therefore, caregivers often end up sacrificing their own health for the careand health of their loved ones.
TAKING ON THE CAREGIVER ROLE
Health care responsibilities have been increasingly transferred from publicinstitutions to the family (Jónsdóttir, 2008). For instance, family caregiverstend to be the one’s providing the majority of care within the home forclients with a major chronic illness (Jansen, Wouters, Schols, & Spruit, 2008;Luttik, Jaarsma, Lesman, Sanderman, & Hagedoom, 2009; Pressler et al., 2009;Quinn, 2006). When individuals take on the caregiver role, they often feelobliged to meet all expectations of caring while balancing their usual domes-tic tasks. As a result, the caregiver role has been compared to “being on arollercoaster,” as the caregiver is trying to maintain normality in the homedespite abnormal circumstances (Brännström, Ekman, Boman, & Strandberg,2007b)—such as lack of respite care, divergent opinions between caregiver,health care professional, and client; and long, strenuous hours in the care-giving role (Boyd et al., 2009; Brännström, Ekman, Boman, & Strandberg,2007a; Hasson et al., 2009; Heart Failure Society of America, 2010; Saunders,2008; Wilson, Ross, Goodridge & Davis, 2008; Woolfe et al., 2007). Thecaregiver is “on call” 24 hours a day, trying to balance activities and relax-ation for themselves and their loved one. This has been shown to lead tocaregivers’ feelings of burden and of resentment (Brännström et al., 2007a,2007b) culminating in caregiver ill health.
CAREGIVER HEALTH DECLINE AND ITS CONSEQUENCES
Declining caregiver health is an example of a negative health issue fac-ing caregivers who manage clients at home (Hasson et al., 2008; Molloy,Johnston, & Witham, 2005). The literature has indicated the followinghealth-related issues for caregivers:
● significant stress and pressure (Hasson et al., 2008; Luttik, Blaauwbroek,Dijker, & Jaarsma, 2007; Wolfe et al., 2007);
● fatigue, loss of concentration, and lack of sleep (Hasson et al., 2008, 2009;Luttik et al., 2007; Spence et al., 2008);
● feelings of helplessness, guilt, and frustration about their situation (Ågrenet al., 2009; Brewin, 2004; Harris, 2007; Hasson et al., 2009; Spence et al.,2008);
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

142 M. Macdonald et al.
● confusion and tension between wanting to prolong a loved one’s life andknowing they must plan for a loved one’s death (Brännström et al., 2007a;Chattoo & Atkin, 2009);
● lower quality of life (Luttik et al., 2007);● increased depression (Harkness, 2009; Narsavage & Chen, 2008; Saunders,
2008);● feelings of social isolation (Ågren et al., 2009; Hwang et al., 2010; Molloy
et al., 2005).
These consequences have been shown to restrict caregivers in pursuingtheir own activities (Pressler et al., 2009; Saunders, 2008). In addition, poorphysical health and distress may influence the ability of caregivers to givesafe care (Ågren et al., 2009; Pressler et al., 2009; Rohrbaugh, Shoham, Cleary,Berman, & Ewy, 2009) or make appropriate decisions for their loved ones(Harkness, 2009). This, in turn, can result in increased hospital readmissionfor the client (Molloy et al., 2005; Narsavage & Chen, 2008), and increasedmorbidity (Luttik et al., 2007), and mortality in caregivers (Luttik et al., 2007;Saunders, 2008).
CONCLUSION
This scoping review confirmed significant safety-related information not pre-viously identified that is meaningful for clients and caregivers. The literaturereviewed did not unilaterally link client and caregiver safety, therefore somemarkers appear more client than caregiver focused and vice versa. Clientand caregiver health and safety are linked through the identified markers.Clients and caregivers felt left on their own to manage; that the informa-tion they were provided was not what they needed; that they did not get toknow their providers yet were expected to take on a variety of responsibili-ties including managing many medications. In order to remain at home theyincurred numerous out-of-pocket expenses. This cascade of markers culmi-nated in the caregiver experiencing health problems that limited ability tocare for the client placing the health and safety of both at risk.
REFERENCES
Abernethy, A. P., Currow, D. C., Clarke, K., Newton, P. J., & Davidson, P. M. (2009).The heart failure care giving experience: Findings from a population basedstudy. Journal of Cardiac Failure, 15(6S), 326.
Ågren, S., Frisman, G. H., Berg, S., Svedjeholm, R., & Strömberg, A. (2009).Addressing spouses’ unique needs after cardiac surgery when recovery iscomplicated by heart failure. Heart & Lung, 38(4), 284–291.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

Home Care Safety Markers 143
Albert, N. M., & Zeller, R. (2009). Depressed patients understand heart failureprognosis but not how to control it. Heart & Lung, 38, 382–391.
Aldred, H., Gott, M., & Gariballa, S. (2005). Advanced heart failure: Impacton older patients and informal carers. Journal of Advanced Nursing, 49(2),116–124.
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodologicalframework. International Journal of Social Research Methodology, 8(1), 19–32.
Bakas, T., Pressler, S. J., Johnson, E. A., Nauser, J. A., & Shaneyfelt, T. (2006). Familycaregiving in heart failure. Nursing Research, 55(3), 180–188.
Barnett, M. (2005). Caring for a patient with COPD: A reflective account. NursingStandard, 19(36), 41–46.
Bartoli, L., Zanaboni, P., Masella, C., & Ursini, N. (2009). Systematic review oftelemedicine services for patients affected by chronic obstructive pulmonarydisease (COPD). Telemedicine and E-Health, 15(9), 877–883.
Bennett, S. J., Bakas, T., Johnson, E. A., & Shaneyfelt, T. (2004). What about familycaregivers of patients with heart failure? Journal of Cardiac Failure, 10(4S), 303.
Boyd, K. J., Worth, A., Kendall, M., Pratt, R., Hockley, J., Denvir, M., & Murray, S. A.(2009). Making sure services deliver for people with advanced heart failure: Alongitudinal qualitative study of patients, family carers, and health professionals.Palliative Medicine, 23(8), 767–776.
Brännström, M., Ekman, I., Boman, K., & Strandberg, G. (2007a). Being a close rela-tive of a person with severe, chronic heart failure in palliative advanced homecare—A comfort but also a strain. Scandinavian Journal of Caring Sciences, 21,338–344.
Brännström, M., Ekman, I., Boman, K., & Strandberg, G. (2007b). Narratives of aman with severe chronic heart failure and his wife in palliative advanced homecare over a 4.5-year period. Contemporary Nurse, 27 , 10–22.
Brännström, M., Ekman, I., Norberg, A., Boman, K., & Strandberg. (2006). Livingwith severe chronic heart failure in palliative advanced home care. EuropeanJournal of Cardiovascular Nursing, 5, 295–302.
Brewin, A. (2004). The quality of life of carers of patients with severe lung disease.British Journal of Nursing, 13(15), 906–912.
British Thoracic Guideline Development Group. (2004). Intermediate care—Hospital-at-home in chronic obstructive pulmonary disease: British ThoracicSociety guideline. Thorax: An International Journal of Respiratory Medicine,62, 200–210.
Canadian Heart Failure Network. (2013). Facts about heart failure in Canada.Retrieved from http://www.chfn.ca/facts-about-chf-in-canada
Canadian Home Care Association. (2008). Home care—The next essential ser-vice: Meeting the needs of our aging population. Retrieved from http://www.cdnhomecare.ca/media.php?mid=1914
Caress, A. L., Luker, K. A., Chalmers, K. I., & Salmon, M. P. (2009). A review ofthe information and support needs of family carers of patients with chronicobstructive pulmonary disease. Journal of Clinical Nursing, 18, 479–491.
Centers for Disease Control and Prevention. (2012). Heart failure factsheet. Retrieved from http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_heart_failure.htm
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014
144 M. Macdonald et al.
Chattoo, S., & Atkin, K. (2009). Extending specialist palliative care to people withheart failure: Semantic historical and practical limitations to policy guidelines.Social Science & Medicine, 69, 147–153.
Clark, A., Reid, M. E., Morrison, C. E., Capewell, S., Murdoch, D. L., & McMurray,J. J. (2007). The complex nature of informal care in home-based heart failuremanagement. The Journal of Advanced Nursing, 61(4), 373–383.
COPD International. (2012). COPD statistics. Retrieved from http://www.copd-international.com/library/statistics.htm
Corsello, P., & Tinkelman, D. (2008). Optimizing disease management of chronicobstructive pulmonary disease. Disease Management and Health Outcomes,16(5), 289–296.
Cortis, J. D., & Williams, A. (2007). Palliative and supportive needs of older adultswith heart failure. International Nursing Review, 54, 263–270.
Dansky, K. H., Vasey, J., & Bowles, K. (2008). Use of telehealth by older adults tomanage heart failure. Research in Gerontological Nursing, 1(1), 25–32.
Davidson, P., Paull, G., Rees, D., Daly, J., & Cockburn, J. (2005). Activities of home-based heart failure nurse specialists: A modified narrative analysis. AmericanJournal of Critical Care, 14(5), 426–433.
Dickson, V. V., & Riegel, B. (2009). Are we teaching what patients need to know?Building skills in heart failure self-care. Heart & Lung: The Journal of Acute andClinical Care, 38(3), 253–261.
Elofsson, L. C., & Ohlén, J. (2004). Meanings of being old and living with chronicpulmonary disease. Palliative Medicine, 18, 611–618.
European COPD Coalition. (n.d.). Prevalence in EU . Retrieved from http://www.copdcoalition.eu/about-copd/prevalence
Evangelista, L., Ter-Galstanyan, A., Moughrabi, S., & Moser, D. K. (2009). Anxiety anddepression in ethnic minorities with chronic heart failure. Journal of CardiacFailure, 15(7), 572–579.
Freydberg, N., Strain, L., Tsuyuki, R. T., McAlister, F. A., & Clark, A. M. (2010). “Ifhe gives in, he will be gone”: The influence of work and place on experi-ences, reactions and self-care of heart failure in rural Canada. Social Science &Medicine, 70, 1077–1083.
Fromer, L., Goodwin, E., & Walsh, J. (2010). Customizing inhaled therapy to meetthe need of COPD patients. Postgraduate Medicine, 122(2), 83–93.
Goodlin, S. J. (2009). End-of-life care in heart failure. Current Cardiology Reports,11(3), 184–191.
Harkness, K. I. (2009). Uncertainty and emotional distress in patients with heartfailure and their primary caregivers: A novel study. Journal of Cardiac Failure,15(6S).
Harris, S. (2007). COPD and coping with breathlessness at home: A review of theliterature. British Journal of Community Nursing, 12(9), 411–415.
Hasson, F., Spence, A., Waldron, M., Kernohan, G., McLaughlin, D., Watson,B., & Cochrane, B. (2008). I can not get a breath: Experiences of livingwith advanced chronic obstructive pulmonary disease. International Journalof Family Nursing, 14(11), 526–531.
Hasson, F., Spence, A., Waldron, M., Kernohan, G., McLaughlin, D., Watson, B., &Cochrane, B. (2009). Experiences and needs of bereaved carers during palliative
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

Home Care Safety Markers 145
and end-of-life care for people with chronic obstructive pulmonary disease.Journal of Palliative Care, 25(3), 157–163.
Havranek, E. P., Spertus, J. A., Masoudi, F. A., Jones, P. G., & Rumsfeld, J. S. (2004).Predictors of the onset of depressive symptoms in patients with heart failure.Journal of the American College of Cardiology, 44(12), 2333–2338.
Heart Failure Society of America. (2010). Executive summary: HFSA 2010 com-prehensive heart failure practice guideline. Journal of Cardiac Failure, 16(6),475–539.
Hirdes, J. (2011). Because this is the rainy day: A discussion paper on home careand informal caregiving for seniors with chronic health [Report]. Toronto, ON,Canada: The Change Foundation.
Hopp, F. P., Thornton, N., & Martin, L. (2010). The lived experience of heart failureat the end of life: A systematic literature review. Health & Social Work, 35(2),109–117.
Horne, G., & Payne, S. (2004). Removing the boundaries: Palliative care for patientswith heart failure. Palliative Medicine, 18, 291–296.
Horton, K. (2008). The use of telecare for people with chronic obstructive pulmonarydisease: Implications for management. Journal of Nursing Management, 16 ,173–180.
Hwang, B., & Dracup, K. (2010, September). Impact of caregiving on familycaregivers of patients with heart failure. Paper presented at the 14th AnnualScientific Meeting of the Heart Failure Society of America, San Diego, CA.
Hwang, B., Luttik, M. L., Dracup, K., & Jaarsma, T. (2010). Family caregiving forpatients with heart failure: Types of care provided and gender differences.Journal of Cardiac Failure, 16(5), 398–403.
Jansen, D. J. A., Wouters, E. F. M., Schols, J. M. G. A., & Spruit, M. A. (2008).Self-perceived symptoms and care needs of patients with severe to very severechronic obstructive pulmonary disease, congestive heart failure or chronic renalfailure and its consequences for their closest relatives: The research protocol.BMC Palliative Care, 7(5), 1–8.
Jónsdóttir, H. (2008). Nursing care in the chronic phase of COPD: A callfor innovative disciplinary research. Journal of Clinical Nursing, 17(7B),272–290.
Lang, A., & Edwards, N. (2006). Safety in homecare: A background paper for roundtable discussion. Edmonton, AB, Canada: Canadian Patient Safety Institute.
Law, S. (2005, January). Liquid oxygen therapy at home: Report preparedfor AETMIS. Retrieved from http://www.inesss.qc.ca/fileadmin/doc/AETMIS/Rapports/Pneumologie/2004_08_res_en.pdf
Law, S., & Lehoux, P. (2004, June). Hospital technology at home—Portable oxygen therapy in COPD: Report prepared for AETMIS. Retrievedfrom http://www.inesss.qc.ca/fileadmin/doc/AETMIS/Rapports/Pneumologie/2004_03_res_en. pdf
Leff, B., Burton, L., Mader, S., Naughton, B., Burl, J., Inouye, S., . . . Burton, J. R.(2005). Hospital at home: Feasibility and outcomes of a program to providehospital-level care at home for acutely ill older patients. Annals of InternalMedicine, 143(11), 798–808.
López-Sendón, J. (2011). The heart failure epidemic. Medicographia, 33, 363–369.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

146 M. Macdonald et al.
Lundman, B., Brännström, M., Hägglund, L., & Strandberg, G. (2009). Fatigue inelderly with chronic heart failure: An under-recognized symptom. Aging Health,5(5), 619–624.
Luttik, M. L., Blaauwbroek, A., Dijker, A., & Jaarsma, T. (2007). Living with heartfailure: Partner perspectives. The Journal of Cardiovascular Nursing, 22(2),131–137.
Luttik, M. L., Jaarsma, T., Lesman, I., Sanderman, R., & Hagedoom, M. (2009).Quality of life in partners of people with congestive heart failure: Gender andinvolvement in care. Journal of Advanced Nursing, 65(7), 1442–1451.
Luttik, M. L., Lesman-Leegte, I., & Jaarsma, T. (2009). Quality of life and depressivesymptoms in heart failure patients and their partners: The impact of role andgender. Journal of Cardiac Failure, 15(7), 580–585.
Macdonald. M., & Lang, A. (2010). Safety in home care for unpaid caregivers:A scoping review. Retrieved from http://www.patientsafetyinstitute.ca/English/research/commissionedResearch/SafetyinHomeCare/Documents/MacDonald/MacDonald,%20Marilyn_Caregiver%20Safety_Final%20Report%20ENG.pdf
Mendoza, H., Martín, M. J., Garcia, A., Arós, F., Aizpuru, F., De Los Cobos, J. R., . . .
Cia, J. M. (2009). “Hospital at home” care model as an effective alternative inthe management of decompensated chronic heart failure. European Journal ofHeart Failure, 11(12), 1208–1213.
Michaels, C., & Meek, P. M. (2004). The language of breathing among individualswith chronic obstructive pulmonary disease. Heart & Lung: The Journal of Acuteand Clinical Care, 33(6), 390–400.
Mitchell, B. (2010). Electronic personal health records that promote self-managementin chronic illness. Online Journal of Issues in Nursing, 15(3).
Molloy, G. J., Johnston, D. W., & Witham, M. D. (2005). Family caregiving andcongestive heart failure. Review and analysis. European Journal of HeartFailure, 7(4), 592–603.
Morgan, A. L., Masoudi, F. A., Havranek, E. P., Jones, P. G. Peterson, P. N., Krumholz,H. M., . . . Rumsfield, J. S. (2006). Difficulty taking medications, depression, andhealth status in heart failure patients. Journal of Cardiac Failure, 12(1), 54–60.
Myers, S., Grant, R. W., Lugn, N. E., Holbert, B., & Kvedar, J. C. (2006). Impact ofhome-based monitoring on the care of patients with congestive heart failure.Home Health Care Management Practice, 18(6), 444–451.
Narsavage, G. L., & Chen, K. (2008). Factors related to depressed mood in adultswith COPD post-hospitalization. Home Healthcare Nurse: The Journal for theHome Care and Hospice Professional, 26(8), 474–482.
Nordtug, B., & Holen, A. (2011). Simlarities and differences in caring burden of homedwellers with partners suffering from chronic obstructive pulmonary disease ordementia. Home Health Care Management & Practice, 23(2), 93–101.
Polzien, G. (2007). Practical interventions to prevent or lower emergent care andrehospitalization. Home Healthcare Nurse, 25(7), 482–485.
Pressler, S. J., Gradus-Pizlo, I., Chubinski, S. D., Smith, G., Wheeler, S., Wu, J., &Sloan, R. (2009). Family caregiver outcomes in heart failure. American Journalof Critical Care, 18(2), 149–159.
Public Health Agency of Canada. (2012). Fast facts about chronic obstructivepulmonary disease. Retrieved from http://www.phac-aspc.gc.ca/cd-mc/publications/copd-mpoc/ff-rr- 2011-eng.php
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

Home Care Safety Markers 147
Quinn, C. (2005). End-of-life care with the heart failure patient in home health: Acase study. Journal of Infusion Nursing, 28(6), 393–398.
Quinn, C. (2006). Low-technology heart failure care in home health: Improvingpatient outcomes. Home Healthcare Nurse: The Journal for the Home Care andHospice Professional, 24(8), 533–540.
Radai, M. M., Arad, M., Zlochiver, S., Krief, H., Engelman, T., & Abboud, S. (2008).A novel telemedicine system for monitoring congestive heart failure patients.Congestive Heart Failure, 14, 239–244.
Reinhard, S. C., Levine, C., & Samis, S. (2012). Home alone: Family caregiversproviding complex chronic care. Retrieved from http://www.aarp.org/home-family/caregiving/info-10-2012/home-alone-family-caregivers-providing-complex-chronic-care.html
Roberts, M. M., Leeder, S. R., & Robinson T. D. (2008). Nurse-led 24-h hotline forpatients with chronic obstructive pulmonary disease reduces hospital use andis safe. Internal Medicine Journal, 38, 334–340.
Rohrbaugh, M. J., Shoham, V., Cleary, A. A., Berman, J. S., & Ewy, G. A. (2009).Health consequences of partner distress in couples coping with heart failure.Heart & Lung: The Journal of Acute and Clinical Care, 38, 298–305.
Saunders, M. M. (2008). Factors associated with caregiver burden in heart failurefamily caregivers. Western Journal of Nursing Research, 30, 943–959.
Saunders, M. M. (2010). A comparison of employed and unemployed caregivers ofolder heart failure patients. Holistic Nursing Practice, 24(1), 16–22.
Sauvé, M. J., Lewis, W. R., Blankenbiller, M., Rickbaugh, B., & Pressler, S. J. (2009).Cognitive impairments in chronic heart failure: A case controlled study. Journalof Cardiac Failure, 15(1), 1–10.
Scherr, D., Kastner, P., Kollmann, A., Hallas, A., Auer, J., Krappinger, H., . . .
Fruhwald, F. M. (2009). Effect of home-based telemonitoring using mobilephone technology on the outcome of heart failure patients after an episode ofacute decompensation: Randomized controlled trial. Journal of Medical InternetResearch, 11(3), 1–12.
Schmidt, S., Sheikzadeh, S., Beil, B., Pattern, M., & Stettin, J. (2008). Acceptance oftelemonitoring to enhance medication compliance in patients with chronic heartfailure. Telemedicine and e-Health, 14(5), 426–433.
Slater, S. G., Neander, L., & Carey, G. (2006). Measuring quality of life outcomesthrough the use of home telehealth: Using a case study model in termi-nal heart failure patient. Home Health Care Management & Practice, 18(4),333–335.
Smith, L. (2010). Evaluation and treatment of depression in patients with heart failure.Journal of the American Academy of Nurse Practitioners, 22, 440–448.
Spence, A., Hasson, F., Waldron, M., Kernohan, G., McLaughlin, D., Cochrane, B.,& Watson, B. (2008). Active carers: Living with chronic obstructive pulmonarydisease. International Journal of Palliative Nursing, 14(8), 368–372.
Suwanno, J., Petpichetchian, W., Riegel, B., & Issaramalai, S. (2009). A model pre-dicting health status of patients with heart failure. The Journal of CardiovascularNursing, 24(2), 118–126.
Thorne, S., Kirkham, S. R., & O’Flynn-Magee, K. (2004). The analytic challengein interpretive description. International Journal for Qualitative Methods, 3(1),1–20.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014

148 M. Macdonald et al.
Triller, D., & Hamilton, R. A. (2007). Effect of pharmaceutical care services onoutcomes for home care patients with heart failure. American Journal ofHealth-System Pharmacy, 64, 2244–2249.
Upadaya, S., Lee, F. A., Saldarriaga, C., Verma, S., Sedrakyan, A., Nystrom, K., &Katz, S. D. (2004). Home continuous positive inotropic infusion as a bridge tocardiac transplantation in patients with end-stage heart failure. The Journal ofHeart and Lung Transplantation, 23(4), 466–472.
VanderSchaaf, K., Olson, K. L., Billups, S., Hartsfield, C. L., & Rice, M. (2010). Self-reported inhaler use in patients with chronic obstructive pulmonary disease.Respiratory Medicine, 104, 99–106.
Weeks, L. C., & Strudsholm, T. (2008). A scoping review of research on com-plementary and alternative medicine (CAM) and the mass media: Lookingback, moving forward. BMC Complementary and Alternative Medicine, 8, 43.doi:10.1186/1472-6882-8-43
Wilson, D. M., Ross, C., Goodridge, D., & Davis, P. (2008). The care needsof community-dwelling seniors suffering from advanced chronic obstructivepulmonary disease. Canadian Journal on Aging/La Revue canadienne duvieillissement, 27(4), 347–357.
Woolfe, P., McMillan, M., & Conway, J. (2007). The needs of caregivers of peoplewith COPD: A study. Australian Journal of Primary Health, 13(1), 28–35.
Yohannes, A. M., Willgoss, T. G., Baldwin, R. C., & Connolly, M. J. (2010). Depressionand anxiety in chronic heart failure and chronic obstructive pulmonary dis-ease: Prevalence, relevance, clinical implications and management principles.International Journal of Geriatric Psychiatry, 25, 1209–1221.
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
13:
00 0
8 O
ctob
er 2
014
Related Documents











