Hodgkin Lymphoma Board Review Brad Kahl, MD 11/18/03

Hodgkin Lymphoma Board Review Brad Kahl, MD 11/18/03.
Dec 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hodgkin Lymphoma Board Review
Brad Kahl, MD
11/18/03

Hodgkin Lymphoma
Epidemiology Biology Classification Approach to the Patient

Hodgkin Lymphoma
Epidemiology– 14% of malignant lymphomas
– 0.5% of all malignancies
– approximately 8000 new cases/yr in US
– approximately 1500 deaths/yr
– over past 30 years age adjusted incidence rates declined appreciably mortality rates declined substantially

Trends in Cancer Mortality Rates, Men, 1973-1996
-80%
-70%
-60%
-50%
-40%
-30%
-20%
-10%
0%Testicular
Hodgkin's
Stomach
Mouth
Bladder
Larynx
Bladder
Colorectal
Pancreas
Leukemia

Trends in Cancer Mortality Rates, Women, 1973-
1996
-70%
-60%
-50%
-40%
-30%
-20%
-10%
0%Hodgkin's
Cervical
Stomach
Thyroid
Colorectal
Uterus
Mouth
Bladder
Ovary
Breast
Leukemia

Hodgkin Lymphoma
Epidemiology– men > women
– whites > blacks > Asians
– no clear risk factors, several implicated woodworking, farming familial risk
– Concordance for HD in twins 10/179 in monozygotic vs 0/187 in dizygotic twins
(Mack et al, NEJM 1995)

Hodgkin Lymphoma
Risk Factors con’t– HIV
increases risk for HD 8 fold
– HD not an AIDS defining illness NHL 113x KS 310x
– Unclear why risk for NHL so much greater in HIV patients
compared to HD

Hodgkin Lymphoma
Epstein Barr Virus– EBV DNA found in 50% RS cells
– pathogen or passenger– Increased risk for HD after infectious mono
(Hjalgrim et al, NEJM 2003)– Absolute risk 1/1000
– Median incubation time from mono to EBV+ HD 4.1 years
– No increased risk for EBV- HD after mono

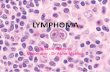
Reed-Sternberg Cell

Hodgkin Biology
Hodgkin’s Disease
– Reed-Sternberg cell is the malignant cell
1% of cells in a biopsy specimen
potent cytokine producing cell (at least 12 cytokines)
cytokines appear to drive the disease process
– remainder of cells are background inflammatory cells
lymphocytes, plasma cells, macrophages, eosinophils
– RS cell as the malignant cell
origin only worked out within the past 5 years

Hodgkin Biology
RS is a “crippled” germinal center B cell
– does not have normal B cell surface antigens
– micromanipulation of single RS followed by PCR demonstrates clonally rearranged, but non functional immunoglobulin genes
somatic mutations result in stop codon (no sIg)
no apoptotic death malignant transformation
– unclear how this occurs; ? EBV
– unclear how cells end up with RS phenotype

Hodgkin Lymphoma Classification
“Classic” Hodgkin’s Disease nodular sclerosis mixed cellularity lymphocyte depleted (very rare) classical lymphocyte rich
– HRS cells CD30 and CD15 positive nodular lymphocyte predominant
– HRS cells (L&H cells) have B cell markers CD 20 and surface Immunoglobulin

NLP Hodgkin Lymphoma
differs from classical HD clinically and histopathlogically
– preference for peripheral nodal sites
– early stage distribution
– late median time to recurrence
– late recurrences common
– low mortality from HD
– L&H cells
express CD 20 (B cell marker)
express surface Ig

Nodular Lymphocyte Predominant Hodgkin Lymphoma

Nodular Lymphocyte Predominant Hodgkin Lymphoma

Nodular Lymphocyte Predominant Hodgkin Lymphoma

Nodular Lymphocyte Predominant Hodgkin Lymphoma
Management– No consensus
often treated like classical hodgkins My view is “do not overtreat” as cure is unlikely and
as many deaths from second malignancies as from LPHD (possible related to HD therapy)
I believe watch and wait is reasonable Often can do IFRT to problem areas as they
appear Rituximab effective in relapse with ORR 85-100%.

Classic Hodgkin Lymphoma

Nodular Sclerosing Hodgkin Lymphoma

Mixed Cellularity Hodgkin Lymphoma

Nodular Lymphocyte Rich Classical Hodgkin Lymphoma

Lymphocyte Depleted Hodgkin Lymphoma

Hodgkin Lymphoma: approach to patient
staging evaluation H & P CBC, diff, plts ESR, LDH, albumin, LFT’s, Cr CT scans chest/abd/pelvis, CXR bone marrow evaluation (for stage IIB and higher) PET scan may be helpful PFTs, LVEF when clinically indicated Fertility counseling **lymphangiogram or laparotomy**

Cancer. 1982;49:2112.
Modified Ann Arbor Staging
Stage I Involvement of a single lymph node region
Stage II Involvement of 2 lymph node regions on the same side of the diaphragm
Stage III Involvement of lymph node regions on both sides of the diaphragm
Stage IV Multifocal involvement of 1 extralymphatic sites ± associated lymph nodes or isolated extralymphatic organ involvement with distant nodal involvement

Ann Arbor Staging System for Hodgkin's Disease
and Non-Hodgkin's Lymphoma
Stage I Stage II Stage III Stage IV
Reprinted with permission. Adapted from Skarin. Dana-Farber Cancer Institute Atlas of
Diagnostic Oncology. 1991.


Modified Ann Arbor Staging “E” designation for extranodal disease B symptoms
recurrent drenching night sweats during previous month unexplained, persistent, or recurrent fever with temps
above 38 C during the previous month unexplained weight loss of more than 10% of the body
weight during the previous 6 months
Criteria for bulk– 10 cm nodal mass
– mediastinal mass > 1/3 thorax diameter

Hodgkin Lymphoma: Prognostic Factors
Adverse prognostic features for stage I & II (EORTC data)
more than 3 nodal sites
bulky adenopathy
ESR > 50
B symptoms
invasion into critical organs
male
age > 40
MC or LD subtype
– should probably not receive XRT alone if any of the above present
(excessive relapse rate)

Hodgkin Lymphoma: Prognostic Factors
Independent adverse prognostic factors– advanced stage (III-IV)
male sex age > 45 albumin < 4 gm/dl HgB < 10.5 mg/dl stage IV disease WBC count > 15,000/mm3
lymphocyte count < 600/mm3
(Hasenclever et al, NEJM 339,1506-1514;1998)

Hodgkin Lymphoma: Prognostic Factors

Hodgkin Lymphoma: Biologic Prognostic Factors
Favorable– EBV in tumor cells
Unfavorable– Tissue eosinophila (NSHD)
– Lymphocyte depletion (NSHD)
– RS atypia (NSHD)
– Bcl-2 overexpression
– P53
– High proliferative rate

Hodgkin Lymphoma
Treatment– approach depends upon stage, prognostic
factors, and co-morbidities
– Stage I-II consider XRT, chemotherapy, or combined therapy
– Bulky stage I-II combined modality therapy, usually 6 cycles of
chemotherapy
– Stage III-IV ABVD x 6-8 cycles gold standard

Hodgkin Lymphoma
Results of Treatmentstage 5 year overall survival
–I 90%
–II 90%
–III 80%
–IV 65%

Hodgkin Lymphoma: Treatment of limited stage disease
Current general consensus is to administer CMT– ABVD x 4 (consider 6 cycles for bulk)
– Followed by IFRT
– Definite trend towards limiting the radiation field and possibly lowering the radiation dose due to concern over late effects
– Data from 2 large trials #1: Institute Nazionale Tumori
– Enrolled patients with stage I, IIA, IIA bulky, and IIEA
– Data presented at 2001 ASH meeting

Hodgkin Lymphoma: Treatment of limited stage disease

Hodgkin Lymphoma: Treatment of limited stage disease

Hodgkin Lymphoma: Treatment of limited stage disease
Study #2: Engart et al, JCO Oct 2003.– Included patients with limited stage HD and at
least one risk factor Bulky mediastinal disease Extranodal disease Massive splenic disease ESR > 50 and no B symptoms ESR > 30 and B symptoms More that 2 lymph node regions

Hodgkin Lymphoma: Treatment of limited stage disease

Hodgkin Lymphoma: Treatment of limited stage disease

Hodgkin Lymphoma: Treatment of limited stage disease
More acute toxicities in EFRT Late toxicities (second CA, cardiac, pulmonary)
not statistically different– Trend worse in EFRT arm
– Longer follow up will needed Conclusion from trials 1 and 2
– 4 cycles of chemotherapy plus IFRT equally effective to treatment plans including larger radiation fields

Hodgkin Lymphoma
Excess death rate (relative)* (SEER data)– 2 years: 5.6%
– 5 years: 8.8%
– 10 years: 14.3%
– 15 years: 19.4%
– 20 years: 23.9%
*compared to age and sex matched control
(deaths other than from Hodgkins)

Hodgkin Lymphoma: Late Complications
Radiotherapy appears to confer the most late risk
– Actuarial rate of second CA 1%/year with no plateau
– In one study the 25 year cumulative risk of breast CA was 16.3%
Current major focus of current clinical trials to to maintain high cure rate while minimizing late complication
shorter courses of chemotherapy with lower radiation doses in smaller fields
elimination of radiotherapy (some argue for this already)

Hodgkin Lymphoma
Current EORTC trial for stage I-II patients– EBVP x 6 + 36 Gy IF
– EBVP x 6 + 20 Gy IF
– EBVP x 6 (arm closed do to excessive relapse) Current GHSG trial for stage I-II patients
– ABVD x 4 + 30 Gy IF
– ABVD x 4 + 20 GY IF
– ABVD x 2 + 30 Gy IF
– ABVD x 2 + 20 GY IF

Hodgkin Lymphoma: Late Complications
Other Late Complications– depends upon treatment modality utilized
XRT vs. MOPP vs. ABVD vs. CMT
– issues depends upon the age of patient relative risks higher in younger patients absolute risks higher in older patients
– Risks of leukemia and infertility appear substantially lower using ABVD rather than MOPP Infertility 20% vs. 50-70%
– Pulmonary-Bleomycin, Cardiac-adriamycin

Hodgkin Lymphoma: Advanced Disease
More straightforward right now – ABVD is standard
– Treat until CR + 2 cycles up to maximum of 8
– No role for routine XRT after chemo (Aleman et al, NEJM June 2003)
– Common practice is to administer consolidative XRT to bulky mediastinal disease after chemo
Stanford V, BEACOPP being compared to ABVD in prospective clinical trials currently

Hodgkin Lymphoma: Stem Cell Transplant
Reserved for patients who relapse after chemotherapy (autologous)– Superior to additional conventional
chemotherapy in RCT (Schmitz et al, Lancet 2002)
Upfront transplant for poor prognosis disease does not appear superior (2 trials)
Beneficial for the small group of patients with primary refractory HD

Hodgkin Lymphoma: Stem Cell Transplant

Lymphoma and Pregnancy
4th most common malignancy among pregnant females (breast > cervical > ovarian)
no good evidence that pregnancy has a prognostic influence on the lymphoma (except Burkitts)
Staging Issues– CT scans and radioisotope scans contraindicated
– rely on PE, labs, CXR, US, MRI, and marrow

Lymphoma and Pregnancy
Therapy during pregnancy– choices will vary on case by case basis
– type of lymphoma, gestational age, personal beliefs
– therapeutic abortion vs watchful waiting vs limited XRT vs chemotherapy
Indolent NHL (rare) and some Hodgkins– will be able to defer therapy until after delivery

Lymphoma and Pregnancy
Aggressive NHL and Hodgkins requiring therapy– 2nd and 3rd trimester
data suggests can give combination chemotherapy with minimal risk to fetus (CHOP or ABVD)
need to plan delivery to avoid neutropenia and thrombocytopenia
– 1st trimester (most difficult situation) consider therapeutic abortion risk of fetal malformation with combination chemo
approximately 20%

Lymphoma and Pregnancy
Things to avoid– excessive XRT
maximum acceptable dose to fetus 10 Gy
– anti-metabolites methotrexate
– regimens heavy in alkylating agents MOPP
Related Documents