5/10/2017 1 Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM Johns Hopkins University School of Medicine University of New Mexico School of Medicine HIV Treatment Update Disclosures Consulting, Advisory Boards, and DSMBs Bristol-Myers Squibb Gilead Sciences Merck & Co. Theratechnologies ViiV Healthcare/GSK Research Support AbbVie Bristol-Myers Squibb Gilead Sciences Janssen Therapeutics Merck & Co. Sangamo BioSciences ViiV Healthcare/GSK

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

5/10/2017
1
Joel Gallant, MD, MPH
Southwest CARE CenterSanta Fe, NM
Johns Hopkins University School of MedicineUniversity of New Mexico School of Medicine
HIV Treatment Update
Disclosures
Consulting, Advisory Boards, and DSMBs
Bristol-Myers Squibb
Gilead Sciences
Merck & Co.
Theratechnologies
ViiV Healthcare/GSK
Research Support
AbbVie
Bristol-Myers Squibb
Gilead Sciences
Janssen Therapeutics
Merck & Co.
Sangamo BioSciences
ViiV Healthcare/GSK

5/10/2017
2
DHHS Guidelines, July 2016: What to Start
Recommended regimens
PI based DRV/r + (TDF/FTC or TAF/FTC)
INSTI based DTG + (TDF/FTC or TAF/FTC) DTG/ABC/3TC EVG/c/TDF/FTC or EVG/c/TAF/FTC RAL + (TDF/FTC or TAF/FTC)
Alternative regimens
NNRTI based EFV/TDF/FTC or EFV + TAF/FTC RPV/TDF/FTC or RPV/TAF/FTC (VL <100,000; CD4 >200)
PI based (ATV/c or ATV/r) + (TDF/FTC or TAF/FTC) (DRV/c or DRV/r) + ABC/3TC DRV/c + (TDF/FTC or TAF/FTC)
DHHS Guidelines for Antiretroviral Therapy in Adults and Adolescents, July 2016.
IAS–USA Guidelines, July 2016:What to Start
Günthard HF, et al. JAMA 2016;316:191-210.
Recommended Regimens
DTG/ABC/3TCDTG + FTC/TAFEVG/c/FTC/TAFRAL + FTC/TAF
Regimens When INSTIs are Not an Option
DRV/c or DRV/r + (FTC/TAF, FTC/TDF or ABC/3TC)EFV/FTC/TDFRPV/FTC/(TAF or TDF)

5/10/2017
3
LYMPHOCYTE
TFV
TFV
RENAL TUBULAR
CELL
RENAL TUBULAR
CELL
91% lower plasma TFV
HIV
PLASMAGI
TRACT
TDF(tenofovirdisoproxilfumarate)
300 mg
TAF(tenofovir
alafenamide)
25 mg
TAF vs. TDF: Mechanism of Action
1. Lee W et al. Antimicr Agents Chemo 2005;49:1898-906; 2. Birkus G, et al. Antimicr Agents Chemo 2007;51:543-50;3. Babusis D, et al. Mol Pharm 2013;10:459-66; 4. Ruane P, et al. JAIDS 2013;63:449-5; 5. Sax P, et al. JAIDS 2014;67:52-8; 6. Sax P, et al. Lancet 2015;385:2606-15.
GS 104/111: Initial ART with E/C/F/TAF v. E/C/F/TDF
Parallel, randomized, double-blind, active-controlled phase III studies
– 1o endpoint: VL < 50 at Wk 48 (FDA Snapshot)
Arribas JR, et al. CROI 2017. Abstract 453. Sax PE, et al. Lancet. 2015;385:2606-2615.
EVG/COBI/FTC/TAF(n = 866)
EVG/COBI/FTC/TDF(n = 867)
ART-naïve pts withVL ≥ 1000,
eGFR ≥ 50 mL/min(N = 1733)
Stratified by VL, CD4 count, geographic region
Wk 48Primary endpoint Wk 144

5/10/2017
4
Initial ART with E/C/F/TAF v. E/C/F/TDF:144 Week Efficacy
0
10
20
30
40
50
60
70
80
90
100
48 96 144 48 96 144 48 96 144
Treatment DifferenceWk 48: 2.0% (95% CI: -0.7% to 4.7%)
Wk 144: 4.2% (95% CI: 0.6% to 7.8%; P = .02)
E/C/F/TAF (N=886) E/C/F/TDF (N=867)
Virologic success Virologic Failure No data
Efficacy similar across subgroups, trending toward or significantly better with TAF in each group
– By baseline VL, baseline CD4, adherence, age, sex, race, region
Virologic failure with resistance by Wk 144: 1.4% in each arm
Arribas JR, et al. CROI 2017. Abstract 453. Sax PE, et al. Lancet. 2015;385:2606-2615.
Initial ART With E/C/F/TAF vs E/C/F/TDF:144 Week Safety Outcomes
More discontinuation for AEs with TDF vs TAF
– 3.3% vs 1.3% (P = .01)
Greater spine and hip BMD loss with TDF vs TAF
– 6 D/C’s for bone AEs in TDF arm vs 0 in TAF arm
TC, LDL, and HDL increases greater with TAF vs TDF
– Rates of lipid-modifying therapy initiation similar: 5.5% vs 5.8%
Med. eGFR increase lower with TAF vs TDF regimen: 1.6 vs 7.7 mL/min (P < .001)
Arribas JR, et al. CROI 2017. Abstract 453.
Renal Events Leading to Discontinuation, n
TAF(n = 866)
TDF(n = 867)
Proximal renal tubulopathy
0 4
Cr elevation or eGFR decrease
0 3
Renal failure 0 2
Nephropathy 0 1
Proteinuria 0 1
Bladder spasm 0 1
Total 0 12

5/10/2017
5
CD4 CountVL
ARIA: DTG/ABC/3TC vs. ATV/r + FTC/TDF in ART-Naive Women at Wk 48
Orrell C, et al. AIDS 2016. Abstract THAB0205LB. Johnson M, et al. HIV Glasgow 2016. Abstract P035. Hagins D, et al. IDWeek 2016. Abstract 949.
Outcome, % (n)DTG/ABC/3TC
(n = 248)ATV/r + FTC/TDF
(n = 247)Virologic nonresponse 6 (16) 14 (35)
No virologic data 12 (29) 15 (36)
0 4 8 12 16
3.1
10.5
17.8
FavorsDTG/ABC/3TC
Favors ATV/r +FTC/TDF
Overall Treatment Difference (95% CI)
20-16 -12 -8 -4
P = .005
DTG/ABC/3TC
VL
< 5
0 (%
)
Overall ≤ 100K > 100K ≤ 350 > 350
100
80
60
40
20
0
82
71
8374
80
64
85
7278
71
203/248
176/247
148/179
134/181
55/69
42/66
111/130
89/124
92/118
87/123
ATV/r + FTC/TDF
n/N =
Virologic Outcome
WAVES: Switch to E/C/F/TAF in Women at Wk 48
Open-label extension study
Hodder S, et al. CROI 2017. Abstract 443.
Virologic Outcome Treatment Difference(95% CI)
VL
< 5
0 (%
)
100
80
60
40
20
0
Switch to EVG/c/FTC/TAF (n = 159)
Continue ATV/r+FTC/TAF (n = 53)
Success Failure No Data
n= 150 46 3 2 6 5
9487
2 4 49
0 10 20
-20 -10
-1.2
7.5
19.4
FavorsE/c/F/TAF
Favors ATV/r+ FTC/TAF

5/10/2017
6
Integrase resistance in the U.S.
Transmitted INSTI resistance remains rare; rates of on-treatment INSTI resistance remains low[1-3]
CDC National HIV Surveillance System[1]:
– Prevalence of INSTI resistance through 2014: 65/14,468 (0.4%)
– Pre-ART prevalence of INSTI resistance (ie, transmitted): 2/4631 (0.04%)
UNC CFAR HIV Clinical Cohort[2]:
– 2015 INSTI resistance prevalence in 685 pts who began ART in 2007 or later: 1%
Modeling: assuming 0.1% rate of transmitted INSTI resistance and $250 cost per test: pre-ART INSTI resistance testing correlated with worse outcomes, higher costs vs no test[3]
1. Hernandez AL, et al. CROI 2017. Abstract 478. 2. Davy T, et al. CROI 2017. Abstract 483. 3. Koullias Y, et al. CROI 2017. Abstract 493.
Emergence of INSTI Resistance in Acute Infection Treated With DTG + FTC/TDF
45-yo man with PCP and ARS
Started DTG + FTC/TDF and discharged; readmitted to ICU several days later for hypoxia
VL increased after readmission despite adherence (including DOT in hospital); no divalent cation use
– DRV/r added, VL decreased
– Pneumonia improved; pt discharged
Rapid INSTI emergence by deep seq: eg, Q148K population increased from 0.0015% at Timepoint 1 to 20.9% at Timepoint 3
Fulcher JA, et al. CROI 2017. Abstract 500LB.
Days
0
200
400
600
800
1000
101
102
103
104
105
106
107
0 20 40 60 80 100
VL
(c
/mL
)
CD
4+
Co
un
t (cells/m
m3)
Initiated DTG/FTC/TDF; GT (clinical assay): RT: V118I, F214L; IN: Not Tested
Added DRV/RTV; GT (clinical assay): RT: M184V, V118I, F214L; IN: G163E
Time Points of IN Deep sequencing
1
23

5/10/2017
7
D:A:D: Exposure to ATV/r or DRV/r and Risk of CVD
Prospective analysis of pts followed from 1/1/09 (BL) to earliest CVD, last visit + 6 mos, or 2/1/16 (N = 35,711)– 1157 (3.2%) developed CVD
(MI, CVA, sudden cardiac death, invasive CV procedure)
Cumulative expos. to DRV/r, but not ATV/r, assoc. with increased CVD risk in multivariate analysis: 59% risk increase per 5-yrs’ DRV/r– Not mediated by dyslipidemia,
in contrast with 1st-generation PIs
Ryom L, et al. CROI 2017. Abstract 128LB.
CVD Risk per 5 Yrs of ARV Exposure, IRR (95% CI)
Model ATV/r DRV/r
Univariate1.25 (1.10-
1.43)1.93 (1.63-
2.28)
Multivariate
Baseline adjusted*
1.03 (0.90-1.18)
1.59 (1.33-1.91)
Time-updated adjusted*
1.01 (0.88-1.16)
1.53 (1.28-1.84)
*Adjusted for: BMI, CKD, DM, CD4, dyslipidemia.
Limitations: potential for unmeasured confounding; observational study; unable to distinguish between DRV/r800/100 mg QD vs DRV/r 600/100 mg BID
Initial Therapy:My choices for specific clinical scenarios
Scenario Regimens
Desires single-tablet regimen (STR) DTG/ABC/3TC EVG/c/FTC/TAF
STR doesn’t matter DTG + FTC/TAF
HBV Coinfection FTC/TAF-based regimen
Starting without resistance test results (DRV/c or DTG) + FTC/TAF
Desire for pregnancy RAL + (FTC/TDF or ABC/3TC) DRV/r + (FTC/TDF or ABC/3TC)
Questionable adherence DTG/ABC/3TC DRV/c + FTC/TAF
Tuberculosis EFV/FTC/TDF RAL 800 mg bid + (FTC/TDF or ABC/3TC)
Drug interactions (including HCV) DTG or RAL-based regimen

5/10/2017
8
When to Start?: Guidelines
Symptoms CD4 <200
CD4 200-350
CD4 350-500
CD4 >500
US DHHS YES YES YES YES YES
IAS-USA YES YES YES YES YES
EACS YES YES YES YES YES
BHIVA (UK) YES YES YES YES YES
WHO YES YES YES YES YES
T.F.
• 28-year-old gay man presents with 3 days of fever, night sweats, lymphadenopathy, and sore throat. A rapid 4th
generation HIV test is positive
• Tested negative 6 months ago. Has been having condomless sex with multiple partners. He asked his primary care provider about PrEP and was told he would have to see “a specialist.”
• Otherwise in good health. Has well controlled depression on citalopram. He has been vaccinated against hepatitis B.
• Sees a nurse and case manager the day after diagnosis, and baseline lab tests are drawn. Has appointment with HIV provider in 10 days. Wants to start ART as soon as possible

5/10/2017
9
T.F.
When would you start ART?
1. After he keeps several clinic appointments (~3 months)
2. After baseline genotype results are available (~2-3 weeks)
3. At the HIV provider visit (10 days)
4. If creatinine is normal and HBsAg is negative (1-2 days)
5. Today
RAPID Start: Time to VL suppression by ART initiation strategy: SFGH 2006-2014
RAPID
RAPID vs. universal ART p<0.001
Universal ART
CD4-guided ART
Pro
po
rtio
n
<20
0 c/
mL N = 39
Pilcher CD, et al. J Acquir Immune Defic Syndr 2016

5/10/2017
10
Rapid Start:Potential regimens
Regimens to consider
DTG + FTC/TAF
EVG/c/FTC/TAF
DRV/c + FTC/TAF
Drugs to avoid
ABC (need HLA B*5701)
TDF (need eGFR)
RPV (need VL, CD4)
EFV, NVP (need genotype)
Switching Therapy

5/10/2017
11
Summary of TAF Switch Studies in Virologically Suppressed Patients
Trials:
GS-109: TDF-containing regimens to EVG/COBI/FTC/TAF
GS -112: Switch to EVG/COBI/FTC/TAF in patients with impaired renal function
GS-119: ART + DRV/r to EVG/COBI/FTC/TAF + DRV in ART-experienced patients
GS-1089: FTC/TDF to FTC/TAF
GS-1160: EFV/FTC/TDF to RPV/FTC/TAF
GS-1216: RPV/FTC/TDF to RPV/FTC/TAF
Results:
Noninferiority, with superiority in GS-109 (switch from EFV/FTC/TDF or ATV/r + FTC/TDF) and superiority in GS-119
Increase in bone density
Stability of eGFR (increase in GS-1089 and GS-112) with no tubular toxicity and decrease in overall and tubular proteinuria
.
-2.5 5.1
1.3
-5.3
-0.5
4.4
-10 0 10
GS 1089: Switch from F/TDF to F/TAFWeeks 48 and 96 Efficacy
FTC/TAF noninferior to FTC/TDF at Weeks 48 and 96
Raffi F, et al. HIV Glasgow, October 2016, Glasgow, UK, Presentation O125
FTC/TDF FTC/TAF
Pat
ient
s, %
94
05
93
26
89
29
89
1
10
0
20
40
60
80
100
Treatment Difference (95% CI)Virologic Outcome
48 48 4896 96 96Week
Wk 48
Wk 96
Success(< 50 copies/mL)
Failure No Virologic Data
FTC/TAF (n=333) FTC/TDF (n=330)

5/10/2017
12
-26
3
-4
-30
3
27
43 47
-50
-25
0
25
50
GS 1089: Switch from F/TDF to F/TAF Change in Renal Biomarkers at Weeks 48 and 96
All differences between treatments statistically significant (p <0.001)
Med
ian
% C
hang
e
UrineAlbumin:Cr
Urine Protein:Cr
Urineβ2M:Cr
UrineRBP:Cr
10 4
-20
-10
0
10
20
Med
ian
Cha
nge,
mL/
min
eGFR
FTC/TAF FTC/TDF
Raffi F, et al. HIV Glasgow, October 2016, Glasgow, UK, Presentation O125
GS 1089: Switch from F/TDF to F/TAF: Bone density changes through Week 96
321 310 300
320 310 306
294
297
287
292
321 309 300
317 305 303
293
296
288
289
FTC/TAF
FTC/TDF
n
Mea
n %
Cha
nge
(95%
CI)
Spine
WeekWeek
2.2
-0.2
p <0.001
Hip
1.9
-0.3
p <0.001
1.7
-0.1
1.2
-0.1
FTC/TAF FTC/TDF p value FTC/TAF FTC/TDF p value
≥ 3% increase 40% 18% < 0.001 29% 11% < 0.001
≥ 3% decrease 8% 19% < 0.001 6% 15% < 0.001
Raffi F, et al. HIV Glasgow, October 2016, Glasgow, UK, Presentation O125

5/10/2017
13
TDF to TAF switch
Advantages:
Increased eGFR
Decreased proteinuria
Improved bone density
Smaller pill size
Disadvantages:
Loss of TDF lipid effect
TAF will be more expensive than generic TDF
Günthard HF, et al. JAMA 2016;316:191-210.
IAS-USA recommendations: “If there is no increase in the price of TAF vs. that of TDF, switching from TDF to
TAF is reasonable even if patients are not experiencing TDF-related toxic effects.”
Alternative StrategiesUsing Approved Drugs

5/10/2017
14
SWORD 1 & 2: Switch From Suppressive ART to DTG + RPV
Open-label, multicenter phase III trials of pts with virologic suppression (N=1024) randomized to continue baseline ART vs switch to DTG + RPV
1 pt with confirmed criteria for virologic withdrawal at Wk 36 in DTG + RPV arm had K101K/E
– Documented nonadherence at VF
– Resuppressed with continued DTG + RPV
– No INSTI resistanceLlibre JM, et al. CROI 2017. Abstract 44LB.
Virologic Nonresponse
HIV-1 RNA< 50 c/mL
No Data
100
80
60
40
20
0
Pts
(%
)
95 95
< 1 15 4
Treatment difference: -0.2% (95% CI: -3.0% to 2.5%)
DTG + RPV (n=513)Baseline ART (n=511)
SWORD 1 & 2: Switch From Suppressive ART to DTG + RPV: Safety Outcomes
AE rates generally similar between arms through Wk52– Numerically higher rate of
drug-related grade 1/2 AEs with switch: 17% vs 2%
– Numerically higher rate of withdrawal for AEs with switch: 4% vs < 1%
No notable change in lipids through Wk 48 in either treatment arm
Llibre JM, et al. CROI 2017. Abstract 44LB.
Bone-specificalkaline
phosphatase
Osteocalcin Procollagen 1N-terminal propeptide
Bone Turnover Markers
DTG + RPV Baseline ART
0
20
60
40
80
Me
an
(µ
g/L
)
BaselineWk 48
15.912.9
100 BaselineWk 48
16.2 17.123.8
19.024.0 23.1
53.0
45.6
55.3 54.7
P < .001P < .001
P < .001

5/10/2017
15
PADDLE: Dolutegravir + Lamivudine for Treatment-Naive Pts
Cahn P, et al. AIDS 2016. Abstract FRAB0104LB.
Pt #
HIV-1 RNA (copies/mL)Screen BL Day 2 Day 4 Day 7 Day 10 Wk 2 Wk 3 Wk 4 Wk 6 Wk 8 Wk 12 Wk 24 Wk 36 Wk 48
1 5584 10,909 3701 383 101 71 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
2 8887 10,233 5671 318 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
3 67,335 151,569 37,604 1565 1178 266 97 53 < 50 < 50 < 50 < 50 < 50 < 50 < 50
4 99,291 148,370 11,797 3303 432 179 178 55 < 50 < 50 < 50 < 50 < 50 < 50 < 50
5 34,362 20,544 4680 1292 570 168 107 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
6 16,024 14,499 3754 1634 162 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
7 37,604 18,597 2948 819 61 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
8 25,071 24,368 6264 1377 Not done 268 105 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
9 14,707 10,832 Not done 516 202 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 SAE
10 10,679 7978 5671 318 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
11 50,089 273,676 160,974 68,129 3880 2247 784 290 288 147 < 50 < 50 < 50 < 50 < 50
12 13,508 64,103 3496 3296 135 351 351 84 67 < 50 < 50 < 50 < 50 < 50 < 50
13 28,093 33,829 37,350 26,343 539 268 61 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
14 15,348 15,151 3994 791 198 98 < 50 61 64 < 50 < 50 < 50 < 50 < 50 < 50
15 23,185 23,500 15,830 4217 192 69 < 50 < 50 < 50 Not done < 50 < 50 < 50 < 50 < 50
16 11,377 3910 370 97 143 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
17 39,100 25,828 11,879 1970 460 147 52 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
18 60,771 73,069 31,170 2174 692 358 156 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
19 82,803 106,320 35,517 2902 897 352 168 76 < 50 < 50 < 50 < 50 < 50 Virologic failure
20 5190 7368 3433 147 56 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50 < 50
ANRS 167 LAMIDOL: Switch to DTG + 3TC in Suppressed Pts
Noncomparative, open-label, single-arm multicenter trial
1o endpoint: therapeutic success at Wk 56 (ie, after 48 wks of dual therapy)
Therapeutic failure: VL > 50 interruption, lost to f/u, death
Joly V, et al. CROI 2017. Abstract 458.
DTG + 2 NRTI†
VL ≤ 50 x ≥ 2 yrson 1st-line ART;
≤ 2 ART modifications, except within 6 mosof study start; CD4
> 200 (N = 110)
Wk 8* Wk 56
*Pts with VL ≤ 50 proceeded to phase II. †In phase I, third agent in regimen replaced with DTG; baseline NRTI backbone maintained.
DTG + 3TC(n = 104)
Phase I Phase II
5/10/2017
16
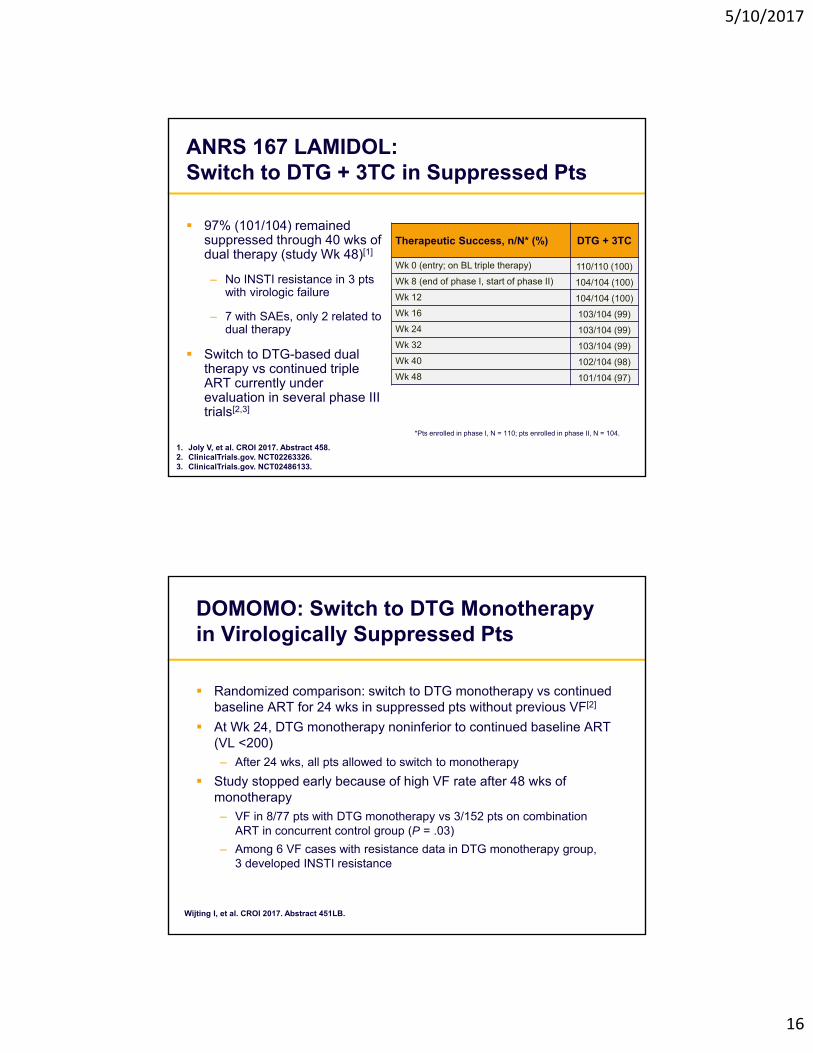
ANRS 167 LAMIDOL: Switch to DTG + 3TC in Suppressed Pts
97% (101/104) remained suppressed through 40 wks of dual therapy (study Wk 48)[1]
– No INSTI resistance in 3 pts with virologic failure
– 7 with SAEs, only 2 related to dual therapy
Switch to DTG-based dual therapy vs continued triple ART currently under evaluation in several phase III trials[2,3]
1. Joly V, et al. CROI 2017. Abstract 458. 2. ClinicalTrials.gov. NCT02263326. 3. ClinicalTrials.gov. NCT02486133.
Therapeutic Success, n/N* (%) DTG + 3TC
Wk 0 (entry; on BL triple therapy) 110/110 (100)
Wk 8 (end of phase I, start of phase II) 104/104 (100)
Wk 12 104/104 (100)
Wk 16 103/104 (99)
Wk 24 103/104 (99)
Wk 32 103/104 (99)
Wk 40 102/104 (98)
Wk 48 101/104 (97)
*Pts enrolled in phase I, N = 110; pts enrolled in phase II, N = 104.
DOMOMO: Switch to DTG Monotherapy in Virologically Suppressed Pts
Randomized comparison: switch to DTG monotherapy vs continued baseline ART for 24 wks in suppressed pts without previous VF[2]
At Wk 24, DTG monotherapy noninferior to continued baseline ART (VL <200)
– After 24 wks, all pts allowed to switch to monotherapy
Study stopped early because of high VF rate after 48 wks of monotherapy
– VF in 8/77 pts with DTG monotherapy vs 3/152 pts on combination ART in concurrent control group (P = .03)
– Among 6 VF cases with resistance data in DTG monotherapy group, 3 developed INSTI resistance
Wijting I, et al. CROI 2017. Abstract 451LB.

5/10/2017
17
Emergent INSTI Resistance After Switch to DTG Monotherapy
International, multicenter retrospective study – Evaluated virologically
suppressed pts switched to DTG monotherapy
– Pts with history of VF on INSTI and INSTI resistance excluded
11 of 122 pts (9%) switched to DTG monotherapy experienced VF– 9 of 11 had genotypic INSTI
resistance at VF
INSTI resistance pathways varied
Blanco JL, et al. CROI 2017. Abstract 42.
INSTI Resistance at VF
92Q/155H (n = 1)
97A/155H (n = 1)
155H/148R (n = 1)
118R (n = 2)
148K (n = 1)
148H (n = 2)
148R (n = 1)
Investigational Drugs

5/10/2017
18
Doravirine vs. DRV/r at Wk 48FDA Snapshot
Efficacy similar in both arms regardless of baseline VL or CD4 count
No resistance detected in pts with PDVF through Wk 48 in either arm
– n = 1 pt with noncompliance discontinued at Wk 24, developed DOR and FTC resistance
Molina JM, et al. CROI 2017. Abstract 45LB.
Virologic Nonresponse
Wk 48
HIV-1 RNA< 50 c/mL
No Data
100
80
60
40
20
0
Pts
(%
)
84 80
11 135 7
Treatment difference: 3.9% (95% CI: -1.6% to 9.4%)
DOR + 2 NRTIs (n = 383)DRV/r + 2 NRTIs (n = 383)
Doravirine vs DRV/r in Combination With FTC/TDF or ABC/3TC: Safety
Molina JM, et al. CROI 2017. Abstract 45LB.
AE, %DOR
(n = 383)DRV/r
(n = 383)
≥ 1 AE 80 78
Treatment-related AE 31 32
Serious AE 5 6
Discontinuation for AE 2 3
AEs of clinical interest Rash* Neuropsychiatric†
711
813
Fasting Lipid Δ From BL to Wk 48, mg/dL
DOR(n = 383)
DRV/r(n = 383)
LDL-c* -4.51 9.92
Non-HDL-c* -5.3 13.75
Cholesterol -1.37 17.9
Triglyceride -3.14 21.97
HDL-c 3.94 4.15
*Discontinued due to rash: n = 2 in DOR arm; n = 1 in DRV/r arm.†No discontinuation for neuropsychiatric conditions.
*P < .0001 for DOR vs DRV + RTV.

5/10/2017
19
Bictegravir + FTC/TAF vs DTG + FTC/TAF in Treatment-Naive Pts
Bictegravir: novel QD INSTI, active against most INSTI mutations, low DDI potential, half-life ~ 18 hrs, no food requirement with dosing, primarily metabolized by CYP3A4 and UGT1A1
Randomized, double-blind, active-controlled phase II trial
– Primary endpoint: VL < 50 at Wk 24
Open-label extension
Sax PE, et al. CROI 2017. Abstract 41. Sax PE, et al. Lancet HIV. 2017;[Epubahead of print]. Zhang H, et al. CROI 2017. Abstract 40.
Wk 48
BIC + FTC/TAF QD +Placebo for DTG QD
(n = 65)
DTG + FTC/TAF QD +Placebo for BIC QD
(n = 33)
Wk 24
ART-naive ptswith VL ≥ 1000;
CD4 ≥ 200;HBV and HCV negative
(N = 98)
Bictegravir + FTC/TAF vs DTG + FTC/TAF: Wk 24 and Wk 48 Efficacy (FDA Snapshot)
No drug resistance detected in either arm through Wk 48
Sax PE, et al. CROI 2017. Abstract 41.
Virologic Failure
Wk 48
Virologic Success
No Data
100
80
60
40
20
0
9791
2 6 2 3
Treatment difference: 6.4% (95% CI: -6% to 18.8%)
Virologic FailureWk 24
Virologic Success
No Data
100
80
60
40
20
0
Pts
(%
)
97 94
3 6 0 0
Treatment difference: 2.9% (95% CI: -8.5% to 14.2%)
BIC + FTC/TAF (n = 65) DTG + FTC/TAF (n = 33)

5/10/2017
20
Difficult to drawn conclusions on safety from small study, but 4 fully enrolled phase III trials in progress now evaluating efficacy, safety, tolerability of coformulated BIC/FTC/TAF
Bictegravir + FTC/TAF vs DTG + FTC/TAF: AEs and Lab Abnormalities
Sax PE, et al. CROI 2017. Abstract 41. Reproduced with permission.
Any Grade AE Occurring in ≥ 5% in Either Arm, %
BIC + FTC/TAF(n = 65)
DTG + FTC/TAF(n = 33)
Diarrhea 12 12
Nausea 8 12
Headache 8 3
URTI 8 0
Fatigue 6 6
Arthralgia 6 6
Chlamydial infection 6 3
Back pain 6 0
Furuncle 5 6
Flatulence 2 6
Gastroenteritis 2 6
Costochondritis 0 6
Hemorrhoids 0 6
Pruritus 0 6
Grade 2-4 Lab Abnormality ≥ 5% in Either Arm, %
BIC + FTC/TAF(n = 64*)
DTG + FTC/TAF(n = 32*)
Creatine kinase 13 9
AST 9 3
Hyperglycemia 8 13
ALT 6 0
LDL 6 9
Amylase 5 6
Hematuria 3 6
Glycosuria 2 6
*Pts with ≥ 1 post-BL laboratory assessment, excluding those not specified for all pts.
Sax PE, et al. CROI 2017. Abstract 41.
LATTE-2: IM cabotegravir + rilpivirineWeek 48 Results: VL <50 Snapshot (ITT-ME)
Margolis et al. AIDS 2016; Durban, South Africa. Abstract THAB0206LB.
Snapshot success
D1 W32
Q4W 99% 94%
Q8W 95% 95%
Oral 98% 91%Pro
po
rtio
n o
f p
atie
nts
wit
h
viro
log
ical
su
pp
ress
ion
, %
BL W-16 W-12 W-8 D1 W4 W8 W12 W16 W20 W24 W28 W32
Study visit
Induction period Maintenance period
W-4 W36 W40 W44 W48
Oral CAB induction (ME population) Oral CAB (n=56) Q4W IM (n=115) Q8W IM (n=115)

5/10/2017
21
LATTE-2 VL <50 at Week 48 ITT-ME (Snapshot)
Margolis et al. AIDS 2016; Durban, South Africa. Abstract THAB0206LB.
Oral IM
Virologic outcomes Treatment differences (95% CI)
-6.6 12.4
Q8W IM
-7.6 11.6
Q4W IM
Both Q8W and Q4W comparable to Oral CAB at Week 48a
2 subjects with resistance in 8 wk arm: 1 with INSTI mutations, 1 with NNRTI mutations
Active phosphorylated metabolite has prolonged intracellular half-life in PMBCs: 150-160 hrs
Exploratory study of single 10 mg oral dose in HIV infected volunteers
Potential for novel dosing or administration strategies
MK-8591: Long-acting NRTI
Grobler J, et al. 23rd CROI; Boston, MA; February 22-25, 2016. Abst. 98;Friedman E, et al. 23rd CROI; Boston, MA; February 22-25, 2016. Abst. 437LB.
-2.5
-2
-1.5
-1
-0.5
0
0.5
0 5 10 15 20
Ch
ang
e F
rom
Bas
elin
e V
L
(lo
g10
c/m
L)
Time (days)
TDF - 300 mg QD
TAF - 25 mg QD
MK-8591 - 10 mg QW

5/10/2017
22
Possible Long Acting SubdermalImplantable Devices for TAF Delivery
Gunawardana M et al. Antimicrob. Agents Chemother. 2015;59:3913-3919. Johnson L, et al. CROI 2016. #879.
• Silicone scaffold diffusion system1
• Long-acting biodegradable polycaprolactone thin-film membrane2
TMB-301: Long-Acting Ibalizumab in Pretreated Pts Infected With Multidrug-Resistant HIV
Humanized mAb to conformational epitope on CD4 receptor that blocks postattachment HIV entry into CD4 cells without altering normal cell function
Single-arm, open-label phase III trial
– Primary endpoint: ≥ 0.5 log10 VL decrease at Day 14
53% with resistance to all drugs from ≥ 3 classes; 68% with INSTI resistance
Lewis S, et al. CROI 2017. Abstract 449LB.
VL> 1000; on ART ≥ 6 mos, on stable ART ≥ 8 wks;
resistant to ≥ 1 ARV from 3 classes, sensitive to ≥ 1 ARV
for OBR (N = 40)
Wk 25
Ibalizumab2000 mg IV Day 7
(loading dose)Continue Failing ART
Days 0-14
Ibalizumab800 mg IV Day 21, Q2W
(maintenance dose)Switch to OBR
Day 14
Primary Endpoint:Day 14Control Period:
Day 0-7

5/10/2017
23
Efficacy, Safety of Ibalizumab Through 24 Wks
1o endpoint: 83% with ≥ 0.5 log10 VL decrease at Day 14 vs 3% at end of control period (P < .0001)
60% with ≥ 1.0 log10 VL decrease
Mean decrease by Day 14: 1.1 log10
9 pts reported 17 serious AEs
– 1 drug-related serious AE (IRIS) resulted in discontinuation
9 other pts discontinued
– Death (n = 4; liver failure, Kaposi sarcoma; end-stage AIDS, lymphoma)
– Consent withdrawal (n = 3)
– Lost to follow-up (n = 2)
No cases of anti-ibalizumabantibodies
Lewis S, et al. CROI 2017. Abstract 449LB.
Wk 24 Virologic OutcomeIbalizumab +
OBR
≥ 1.0 log10 VL decrease, % 55
≥ 2.0 log10 VL decrease, % 48
VL < 50, % 43
VL < 200, % 50
Mean VL decrease from baseline, log10
1.6
AgentMoA or
FormulationPhase
Dosing/Administration
Implications
GS-CA1[1] HIV capsid inhibitorPre-
clinical
Extended release, suitable for SC of solid
depot formulation
Potent ART with orthoganol resistance profile to existing ART; potential for long-acting formulation due to low aqueous solubility, high stability
GS-9131[2] NRTIPre-
clinical
Potential for once daily dosing
Potent ART active against NRTI RAMs K65R, L74V, M184V alone or in combination; minimal loss of susceptibility with 4 or more TAMs
MK-8591[3]
Nucleoside Reverse Transcriptase Translocation
Inhibitor (NRTTI)
Pre-clinica
l
10 mg QW PO; potential for extended duration
Comparable MK-8591 levels in animal rectal, vaginal tissue to TDF levels in tissues of human subjects highlights potential prophylaxis utility
GS-PI1[4] PIPre-
clinical
Potential for unboosted, once daily dosing
Potent ART with high barrier to resistance, including < 2-fold loss in potency against major PI RAMs, and 10-fold to 40-fold longer in vivo half life vs ATV or DRV
NANO-EFV, NANO-LPV[5]
Oral, lower dose SDN
InEFV: 50 mg QD, 21 dnLPV/RTV: 200/100 mg
BID, 7 d
Enhanced oral bioavailability suggests can reduce EFV, LPV dose by ~ 50% while maintaining PK
Additional Investigational Agents Reported at CROI 2017: Preclinical and Phase I
1. Tse WC, et al. CROI 2017. Abstract 38. 2. White KL, et al. CROI 2017. Abstract 436. 3. Grobler J, et al. CROI 2017. Abstract 435. 4. Link JO, et al. CROI 2017. Abstract 433. 5. Owen A, et al. CROI 2017. Abstract 39.
5/10/2017
24
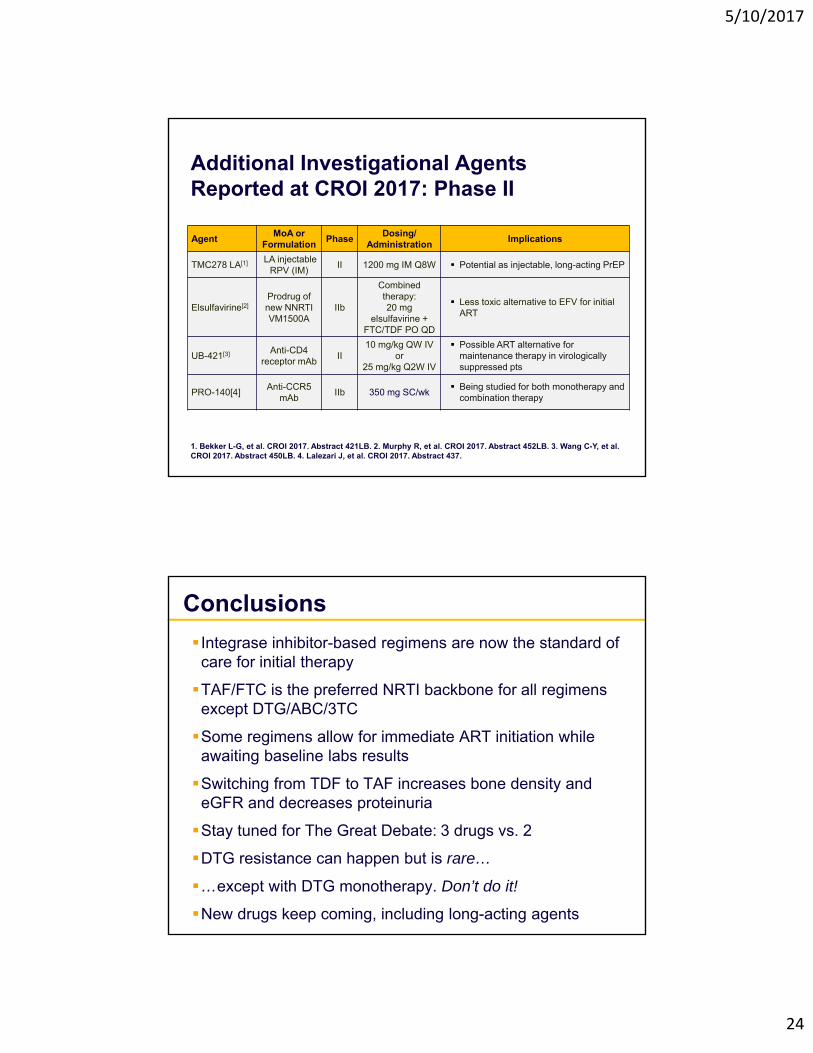
Additional Investigational Agents Reported at CROI 2017: Phase II
1. Bekker L-G, et al. CROI 2017. Abstract 421LB. 2. Murphy R, et al. CROI 2017. Abstract 452LB. 3. Wang C-Y, et al. CROI 2017. Abstract 450LB. 4. Lalezari J, et al. CROI 2017. Abstract 437.
AgentMoA or
FormulationPhase
Dosing/ Administration
Implications
TMC278 LA[1] LA injectable RPV (IM)
II 1200 mg IM Q8W Potential as injectable, long-acting PrEP
Elsulfavirine[2]Prodrug of new NNRTI VM1500A
IIb
Combined therapy: 20 mg
elsulfavirine + FTC/TDF PO QD
Less toxic alternative to EFV for initial ART
UB-421[3] Anti-CD4 receptor mAb
II10 mg/kg QW IV
or 25 mg/kg Q2W IV
Possible ART alternative for maintenance therapy in virologically suppressed pts
PRO-140[4]Anti-CCR5
mAbIIb 350 mg SC/wk
Being studied for both monotherapy and combination therapy
Conclusions
Integrase inhibitor-based regimens are now the standard of care for initial therapy
TAF/FTC is the preferred NRTI backbone for all regimens except DTG/ABC/3TC
Some regimens allow for immediate ART initiation while awaiting baseline labs results
Switching from TDF to TAF increases bone density and eGFR and decreases proteinuria
Stay tuned for The Great Debate: 3 drugs vs. 2
DTG resistance can happen but is rare…
…except with DTG monotherapy. Don’t do it!
New drugs keep coming, including long-acting agents

5/10/2017
25
Thank you!
Related Documents











