HIV CLINICAL ISSUES for Case Managers ADVANCED HIV CASE MANAGEMENT COURSE Leonard A. Sowah, MBChB, MPH Assistant Professor of Medicine Institute of Human Virology University of Maryland School of Medicine

HIV clinical issues for case managers
May 11, 2015
HIV patient outcomes have been shown to improve with appropriate support by case management. HIV case managers need to have a working understanding of clinical management issues to improve on the great work that they do for their patients. This presentation attempts to provide case managers with this information.
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

HIV CLINICAL ISSUES for Case Managers
ADVANCED HIV CASE MANAGEMENT
COURSELeonard A. Sowah, MBChB, MPH
Assistant Professor of Medicine
Institute of Human Virology
University of Maryland School of Medicine

HIV Virus Life Cycle
04/12/23

Clinical Course of HIV Infection
Acute or primary infection Rash Fever Flu like symptoms Fatigue Sore throat
Prolonged Asymptomatic Immune activation leads to CD4 cell decline
Early symptomatic phase Herpes zoster Increased risk of common infections HIV Dermatopathy
Advanced HIV or AIDS Opportunistic Infections

04/12/23
CD4 Cells
A type of white blood cell that carries the CD4 surface marker and helps the body fight infection. Also known as T-cells or T-helper cells. When infected by HIV, these cells incorporate HIV RNA into their DNA and subsequently manufacture new HIV particles.

HIV Viral Load
Viral load means how much HIV is in the patient’s bloodstream (also called HIV RNA).
“Undetectable viral load” means the amount of the virus is so low, the blood tests cant detect it.
Doctor’s use a combination of medicines to try and get the patient’s viral load to an undetectable level and keep it there.
Even when a viral load is extremely low or undetectable, the client should continue taking prescribed HIV medications.
04/12/23

04/12/23
AIDS - Acquired Immunodeficiency Syndrome
The most severe manifestation of HIV infection. Characterized by numerous opportunistic infections and malignancies or a CD4 cell count below 200/mm3, which, in the presence of HIV, constitutes a diagnosis of AIDS.

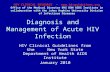
Course of HIV Infection
04/12/23

From CLIN INFECT DIS 30(S1):S5-S14. © 2000 by the Infectious Diseases Society of America. All rights reserved
04/12/23

Common Opportunistic Diseases in HIV
Pneumocystis pneumonia Oropharyngeal candidasis Pulmonary tuberculosis Herpes zoster Cryptococcal Meningitis CNS Toxoplasma Non Hodgkins Lymphoma HIV Encephalopathy
04/12/23

© 2012 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2
Causes of death in the HAART era
Current Opinion in Infectious Diseases. 25(1):36-41, February 2012.04/12/23

© 2006 AmericanAnnals of Internal Medicine. 145(6):397-406, September 19, 2006. College of Physicians. Published by American College of Physicians.
Causes of Death among Persons with AIDS in the HAART Era : New York City

VIRAL ENTRY AND REPLICATION Sources of HIV virus in
an infected person blood breast milk saliva semen tears vaginal fluids
Transmission has been documented only through
blood blood products sexual fluids Breast milk
04/12/23

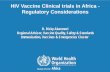
Current HIV drugs and their targets in the viral cell cycle
Fusion InhibitorsCCR5 Antagonist
NNRTIs & NRTIs
Protease Inhibitors
Integrase Inhibitors
Copyright © 2003 by the European Molecular Biology Organization04/12/23

Current FDA Approved HIV Medications
©2006 Community Research Initiative of New England. All Rights Reserved.
04/12/23

When to start therapy (DHHS Guidelines)
CD4 counts < 500 cells Observational data and cohort studies suggests clinical benefit for
patients treated with CD4 > 500 cells
History of AIDS-defining illness HIV-associated nephropathy (HIVAN) Pregnant women Hepatitis B co-infection Rapidly declining CD4 count High viral loads > 100,000 /ml
04/12/23

www.aidsetc.org
When to Start ART
Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts
Current recommendation: ART for all patients with CD4 <500 cells/µL
For patients with CD4 >500 cells/µL, 50% of the panel recommend ART, 50% consider ART to be optional
Randomized control trial (RTC) data support benefit of ART if CD4 350
No RTC data on benefit of ART at CD4 >350, but observational cohort data
04/12/23

Assessing Readiness for Therapy Knowledge about disease Prior adherence history Individual self efficacy Beliefs about Efficacy and safety of
ART regimen Age / income /education Drug use Dosing frequency Pill burden ????
J Gen. Intern Med 2002;17: 756 -76504/12/23

Choice of Initial Regimen
Efficacy Toxicity Clinical Co-morbidity Results of Genotypic resistance testing Substance abuse and psychiatric issues Potential for drug interactions Ease of Administration Consistency with patient lifestyle
04/12/23

Common Side Effects of HIV Meds
LipoatrophyLoss of fat in cheeks,
temples or extremities
Rashes
Increase in the amount of fat, cholesterol, or sugar in the blood that can lead to heart disease
LipodystrophyIncrease in abdominal size, breast size, and/or dorsocervical fat pad
(buffalo hump)
Nephrotoxicity, Kidney StonesKidney damage
HepatotoxicityLiver damage
Nausea, Diarrhea and Vomiting
AnemiaLow number of blood cells; causes fatigue
FACEFACE
BODYBODY
LIVERLIVER
SKINSKIN
HEARTHEART
KIDNEYSKIDNEYS
GUTGUT
BLOODBLOOD
NeuropathyNerve damage causing
strange sensations and pain, starting in the hands/feet
NERVESNERVES
Hyperlipidemia, High Cholesteroland High Glucose
Osteoporosis, OsteopeniaBone loss
BONESBONES

Immune-Reconstitution Inflammatory Syndrome (IRIS)
What is IRIS ? Paradoxical worsening of clinical symptoms
in a HIV positive patient upon therapy initiation from pre-existing infections.
10 – 25% of patients started on HAART Within 12 weeks of onset of HAART CD4 count of HAART start <100 cells/m3 Drop in viral load of > 2.5 log copies
04/12/23

Common Manifestations of IRIS
Anogenital Herpes virus infection Genital warts Molluscum contagiosum Shingles Tuberculosis MAC Infection PCP Hepatitis
Sources for pictures: http://www.medicinenet.com04/12/23

Perinatal HIV Transmission
Without antiretroviral (ARV) drugs during pregnancy, mother-to-child transmission (MTCT) has ranged from 16%–25% in North America and Europe.
21% transmission rate in the U.S. in 1994 before the standard zidovudine (ZDV) recommendation during pregnancy.
With this change in practice, transmission decreased to 11% in 1995.
Today, risk of perinatal transmission can be <2% with:
effective antiretroviral therapy (ART) elective cesarean section (C/S) as appropriate formula feeding
04/12/23

Hepatitis C and HIV
30 - 40% of HIV+ people in US also infected with HCV
More rapid progression of HCV (twice as fast) Little to no affect on HIV progression (still inconclusive) Complicates medication regimens Increases risk of perinatal transmission Incarceration and injection drug use settings have
co-infection rates >75% Treatment effectiveness is heavily determined by
genotype
04/12/23

Other Clinical Issues in HIV Care
Kidney Disease Hyperlipidemia Cardiovascular Disease Liver Disease COPD HIV Neuropathy Cognitive Impairments
04/12/23

End of Life Needs
Advanced Directives Power of attorney Disease management Hospice Care Comfort Care Insurance Issues
04/12/23

Summary
HIV viral replication can be suppressed with Anti Retroviral Therapy
Risk of development of drug resistance is high in non adherent patients.
Individualized choice of therapy regimen and when to initiate ART may reduce risk of treatment failure and development of resistance
Effective team work between case manager and HIV provider can reduce therapeutic failure and improve patient satisfaction
04/12/23

THANKS VERY MUCH
Related Documents