Whitepaper Hygiene and Compliance Part 1: How can hand-hygiene compliance be sustainably improved?

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Whitepaper
Hygiene and Compliance
Part 1:How can hand-hygiene compliance
be sustainably improved?

2g g g g g H Y G I E N E A N D C O M P L I A N C E
Hygiene the focus ofattention
Effective weapon in the battle against infections
The battle against the invisible enemy
In light of the world-wide spread of viral diseases, how is it pos-sible to effectively protect oneself from the transmission of dis-ease-causing pathogens? Since contagious diseases that may run a dangerous course for humans have become a regular compo-nent of reporting in the media, the subject of hygiene as an ef-fective prophylaxis of disease has been reinforced and is moving to the focus of public attention. But even beyond the infectious diseases of epidemic or pandemic proportions, experts consistently stress the importance of hy-giene within the realm of medical care. For instance as an ef-fective weapon against so-called nosocomial infections, that can appear in temporal connection with a stay at a hospital or other medical institution (hospital infections).
How exactly is hygiene defined in the medical sense?How is it put into practice in daily treatment?Are there concrete possibilities for optimization?And how effectively can these actually be applied inpractice?
To these questions the present Whitepaper will offer some an-swers in a concise and comprehensible form.
Hygiene – Reason and Purpose
Still it is useful to shed some light on this question. Only someone who precisely describes the meaning of hygiene and the interre-lation of its actions, can also successfully transform it into prac-tice and optimize it. Or stated differently: whoever wants to use hygiene as an effective weapon in the battle against infections, should ensure that they know their weapon well, in order to be able to engage it efficiently. So what exactly is understood by hygiene in the medical sense? Colloquially, and in its broadest sense, hygiene is often set equal with cleanliness. Experts consider a much more narrow definition. As a general consensus, medical hygiene can today be defined as “Doctrine on the prevention of diseases and the preservation and strengthening of health.”1
In this sense hygiene is in its whole not “just” a preparatory or accompanying step in actual treatment, but an essential compo-nent of patient care and medical prevention. It serves as an effec-tive controlling measure for illnesses and their spread.
3g g g g g H Y G I E N E A N D C O M P L I A N C E
Obligations of Hospital operators and hygiene responsible individuals
Not only financial damages threaten
Especially in consideration of an estimated 500,000 nosocomial infections yearly, in German clinics and hospitals alone, hygiene and its optimization are given a pivotal meaning in the realm of operational quality management in medical establishments.
Hygiene from a legal perspective
On the topic of hygiene, the legislation and jurisdiction in Ger-many have a clear position, and hold the operators of medical establishments, as well as those who are responsible for hygiene, accountable. The infection-protection law (lfSG) specifically em-phasizes the “direct responsibility of the responsible body and manager of […] health establishments as well as the individual in the prevention of communicable diseases.”2 And the federal supreme court of Germany counts hygiene as one of the fully controllable risks in medical practices and hospitals3.
A backdrop of improper organization and coordination of treat-ment events, to which conscientious hygiene management is counted, can lead to a reversal of the burden of proof in the scope of a legal dispute. The shift does not assume that the dan-ger stemming from the medical operation of the treating indi-vidual be concretely recognizable. In this case the patient does not have to prove the possible hygienic non-compliance of the hospital, instead the medical establishment stands on its own part responsible to convincingly prove the observance of all hy-giene regulations documented in the hygiene plan. Example: a patient is infected by a nosocomial infection and there-upon sues the hospital in which he was treated. If the medical establishment is not in the position to present convincing documentation for the concerned time period, for example in the form of a hygiene plan, out of which the regular performance of hand disinfection can be demonstrated, this could, under cir-cumstances, become expensive for the institution. Moreover, the image damages following such a process can be lastingly nega-tive to the hospital’s reputation and this way affect its business operation. In other words: the careful hygiene in hospitals and medical prac-tices should, beyond medical necessity, also from a legal perspec-tive become the highest priority.

4g g g g g H Y G I E N E A N D C O M P L I A N C E
Initiatives for the promotion of hand hygiene
Compliance
“Five points of hand disinfection”
Hand-hygiene compliance on the test-bench
Among hygiene experts there is the far-reaching consensus that hand washing counts to the most powerful hygiene measures in the effective prevention of the spread of disease-causing agents within hospitals, and in this way guaranteeing a high hygienic standard.4 Furthering this, on the part of the world health organization WHO, and on a national level as well, there are targeted efforts which continue to present the enormous importance of medical hand disinfection and establish it as an effective means to further increase quality in patient care.
As an example, the German-wide hygiene project, “Action Clean Hands” (ASH), was started on January 1st, 2008 and pursues the goal of increasing general hand-hygiene compliance.
The term compliance has its roots in English with the general meaning of abiding to laws, regulations, and guide-lines. In the medical realm, compliance in hand hygiene describes abiding to hand disinfection guidelines, in the way they are specified in the hygiene plan, for example on the basis of recommendations of the WHO, which are binding for staff members in medical establishments.
The formulation of clear regulations for hospital staff in the im-plementation of hand disinfection, is an important instrument in the campaign of the ASH. In the “five points of hand disin-fection,” typical situations are defined, where hand disinfection should follow. Important is that, analogous to the suggestions of the WHO, an average amount of disinfection solution per patient day is not recommended. Instead the importance of situational, sensible hand hygiene is emphasized. Thus the following indica-tions for hand disinfection are envisaged:
• Before patient contact • Before aseptic activities • After contact with potentially infectious materials • After patient contact • After contact with surfaces in the immediate surroundings of the patient

5g g g g g H Y G I E N E A N D C O M P L I A N C E
Two methods of recording compliance
A further instrument in the campaign is the recording of hand-hygiene compliance with the goal of optimizing hand-disinfec-tion behaviors on the basis of the gathered data. In practice, this instrument is implemented with the help of two methods.
Method 1 – direct observation: Compliance is immediately and directly ascertained through standardized observation of the hos-pital staff, where the observation criteria correspond to the previ-ously mentioned indications.
Method 2 - recording consumption: Compliance is measured in-directly through the recording of the total consumption of alco-hol hand-disinfection solutions for every participating station in a hospital. Beyond the simple recording of consumption, follows assignment of stations to different areas, i.e. to intensive or non-intensive care stations.
The foundation of consumption measurements and documenta-tion forms the “HAND-KISS” module developed by the National Reference Center for Surveillance of Nosocomial Infections (NRZ).
For the year 2008 (acquisition period from January 1st to Decem-ber 31st, 2008) the following reference data were acquired for participating hospitals, i.e. stations.
Table 1: Annual list of intensive care stations in Germany
Year Number of Hospitals
Number of Stations
Patient days Yearly con-sumption, liters
Median patient day consump-tion, ml
hand dis-infection / patient day
2008 253 449 1.696.530 132.214 73 26
Table 2: Annual list of normal care stations in Germany
Year Number of Hospitals
Number of Stations
Patient days Yearly con-sumption, liters
Median patient day consump-tion, ml
hand dis-infection / patient day
2008 283 2799 22.811.422 399.478 16 6
6g g g g g H Y G I E N E A N D C O M P L I A N C E
The breaking point in hand-hygiene compliance: estimations instead of measurements
Critical observation: Compliance and recording in practice
Even if it is obvious that effective hand-hygiene management is necessary from both a medical and legal perspective, the imple-mentation in daily hospital practice still shows considerable room for improvement.6.
Besides other factors, the poor traceability of the actual per-formed hand-hygiene often forms the “breaking point”. How often doctors and caretakers actually disinfect their hands can rarely be reliably observed in the daily practice. Approximated es-timates instead of precise measurements are therefore often the only possibility for the hygiene officer, if he wants to determine the hand-hygiene compliance. An unsatisfactory situation for hy-giene as well as for the operational quality management of the medical establishment.
The problem of compliance, so worthy of improvement, is picked up by “Action Clean Hands”. Both of the methods used within the campaign - the direct observation of hand-hygiene compli-ance, as well as the recording of total consumption of hand-dis-infection solutions - demonstrate on the basis of their different starting points both benefits as well as disadvantages.
The big advantage of direct observations lies within the ability to evaluate, on-site, the compliance of clinic staff, on the basis of the “five points of hand disinfection”. Does the nurse disinfect her hands before she has contact with the patient and after she has touched the intravenous device near the patient? Questions such as these can be answered by direct observation. But an ex-haustive implementation of this method during the campaign and beyond that, in daily practice of the clinic, is countered by requiring a large number of staff, making it a costly endeavor. Additionally this method can lead to observation effects (Haw-thorne effect), which change the behavior of the observed under the circumstances, and in this way endanger the validity of the gathered data. Furthermore, it is conceivable that the observer may wrongly assign or interpret the observed happenings - even this could possibly weaken the conclusiveness of the observed results.
7g g g g g H Y G I E N E A N D C O M P L I A N C E
Direct observation: instant and costly
Measurement of total consumption does not provide differentiated data
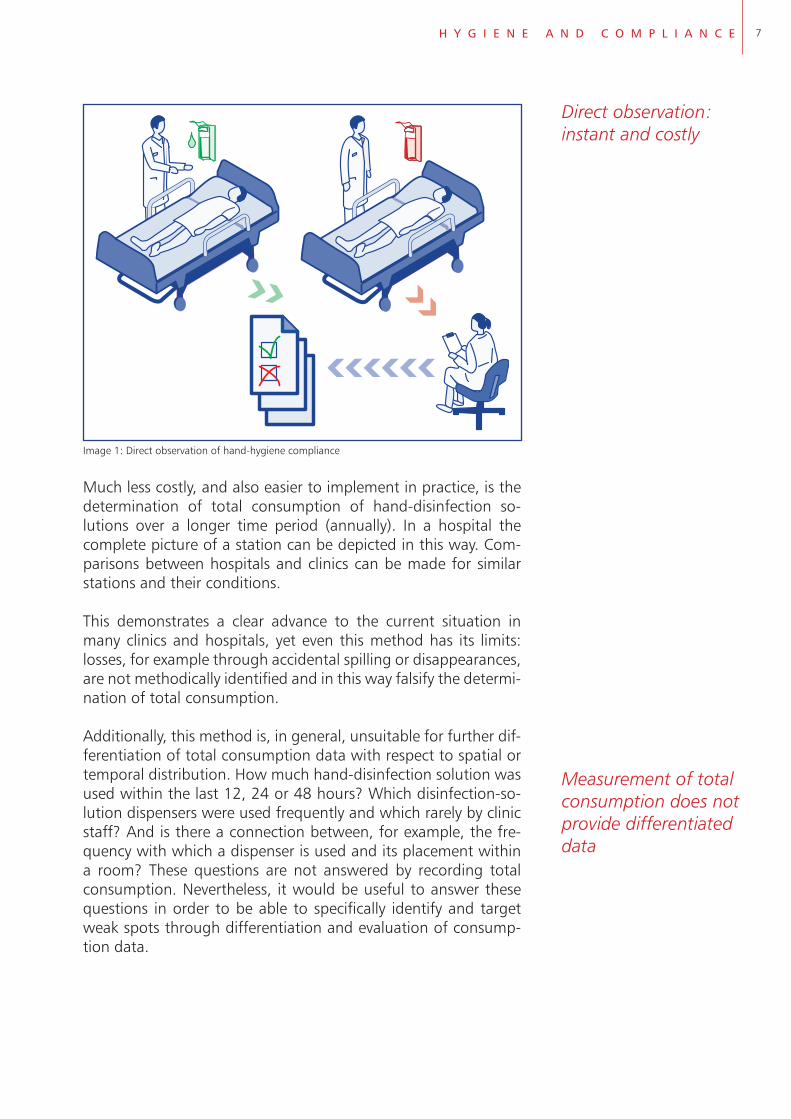
Image 1: Direct observation of hand-hygiene compliance
Much less costly, and also easier to implement in practice, is the determination of total consumption of hand-disinfection so-lutions over a longer time period (annually). In a hospital the complete picture of a station can be depicted in this way. Com-parisons between hospitals and clinics can be made for similar stations and their conditions.
This demonstrates a clear advance to the current situation in many clinics and hospitals, yet even this method has its limits: losses, for example through accidental spilling or disappearances, are not methodically identified and in this way falsify the determi-nation of total consumption.
Additionally, this method is, in general, unsuitable for further dif-ferentiation of total consumption data with respect to spatial or temporal distribution. How much hand-disinfection solution was used within the last 12, 24 or 48 hours? Which disinfection-so-lution dispensers were used frequently and which rarely by clinic staff? And is there a connection between, for example, the fre-quency with which a dispenser is used and its placement within a room? These questions are not answered by recording total consumption. Nevertheless, it would be useful to answer these questions in order to be able to specifically identify and target weak spots through differentiation and evaluation of consump-tion data.

8g g g g g H Y G I E N E A N D C O M P L I A N C E
STATION 1
STATION 2
STATION 3
∑9 l
Image 2: Indirect evaluation of compliance through total consumption analysis
Precise consumption records for lasting optimization of compliance
Where indirect determination of compliance via total consump-tion is limited by a differentiated analysis of possible weak spots in hand hygiene, the above previously described direct observa-tion method would be more effective. Particularly in sensitive risk areas of patient care, for example on an intensive care unit, it would be possible to specifically identify weak spots and in this way foundationally improve hygiene and operational qual-ity management. But non-intensive care stations can also profit from a differentiated measurement and documentation of com-pliance.
Considering the financial pressure in hospitals, the high time cost largely prevents this precise documentation from being a pos-sibility in daily practice.
How would it be possible to bypass the limitations of both methods in the recording of compliance? What possibilities are there for manageable, practical data collection in hand-hygiene compli-ance, that are sufficiently differentiated and thus convincing, but at the same time not falsified by observation effects?

9g g g g g H Y G I E N E A N D C O M P L I A N C E
Dispensers with a counter function allow differentiated measurements
Optimize operational quality and hygiene management
Identifying weak spots
A logical, practical method, and in this way easy to implement within a hospital, is offered by disinfection-solution dispensers with integrated counters. The functional principle is as easy as it is effective: when an outfitted dispenser is activated, it automati-cally activates the counter and documents the release of disinfec-tion solution.
In this way the frequency and use can be precisely determined for each individual dispenser. From the frequency of use, the total consumption of disinfection solution can again be calcu-lated. Usually one stroke corresponds to an amount of 1.5 ml, two strokes with a volume of 3.0 ml which corresponds to the recommended amount for hand disinfection, according to the Robert Koch Institute. For the responsible physician in the area of hygiene and hygiene specialists, this opens efficient possibilities to optimize operational quality and hygiene management.
As an example, the consumption profile per dispenser, per shift, per freely definable time period or even per patient day, can be easily determined and evaluated. The workload for the reading of the counters is proportional to the reading frequency - with shorter reading intervals the corresponding time cost of the data recording is increased. In contrast to the considerable investment of time resources required for a direct observation, even frequent counter readings are significantly less labor-intensive.
Image 3: Dispenser systems with counters for differentiated consumption measurements
Without large labor costs, rarely used dispensers, but also con-spicuous changes over the course of time, can be easily differ-entiated, identified, and evaluated in view of medically effective patient care.

10g g g g g H Y G I E N E A N D C O M P L I A N C E
Strengthening the legal position of hospitals
“Effectiveness gap”
On one hand, judging from experience, it is possible to see posi-tive effects for compliance already by simply gathering data7, on the other it is now possible to implement more specific optimiza-tion measures on the basis of more convincing data, ie. The more advantageous placement of dispensers in a room, or the educa-tion of specific employees.
Through precise measurement, the correlation between appear-ing infections, the dispenser-specific usage frequency and con-sumption amount can be determined. Do more infections appear temporally or spatially exactly then when disinfection-solution dispensers are used less frequently? The advantages of measur-ing by counter lie not only with the immediate acquisition of short-term “development trends” of hygiene behavior, but in particular in the long-term realm. While compliance in connec-tion with intervention measures, such as direct observation, will in many cases at first significantly better compliance, experience indicates that over the long-term, it often sinks to the level pri-or to implementation of the improvement measures8. With the counter function it is possible to notice a drop in compliance very quickly, and to further identify the weak spots, for example by implementing narrowly localized direct observation. This coordi-nated interaction between both methods forms the foundation for the development of effective countermeasures.
For the hospital, medically useful implementation of dispensers with integrated counters can also be an advantage from a le-gal perspective: in view of the medical establishment’s obligation for care, precise and differentiated documentation of consump-tion, and with that resilient proof of compliance, will noticeably strengthen the legal position of the hospital in the case of pos-sible disputes.
Conclusion
Hand-hygiene compliance is a typical example of the “effective-ness gap”9: Theoretically recognized as an important instrument in the avoidance of nosocomial infections, there remains much room for improvement in practice. Experience shows that hand disinfections in daily hospital practice are implemented much more rarely than the hygiene recommendations, guidelines and hygiene plans intend.
In order to permanently improve hand-hygiene compliance, foundational conditions must first be created: The quantitatively sufficient outfitting with disinfection-solution dispensers, and the specific education of hospital staff, in order to deeply impress the importance of hand hygiene on them.

11g g g g g H Y G I E N E A N D C O M P L I A N C E
The alpha and omega: a convincing data pool
Optimization from both a medical and a legal standpoint
But how is a sufficient number of dispensers defined with con-sideration of the spatial conditions and peculiarities of a concrete station? Do all employees actually implement the required hand hygiene in daily practice?
This marks the start of the determination of hand-hygiene com-pliance. Only on the basis of a convincing data pool concerning hygiene behaviors, can these behaviors be optimized in practice.
Differentiated data about compliance for important indications is offered by direct observation. This measure can, however, be falsified through observation effects and cannot be implement-ed exhaustively over a longer time-period, since it is costly as a whole.
In contrast, for daily practice in hospitals, indirect determination of compliance through the recording of total disinfection-solu-tion consumption on one station is feasible. Considerable disad-vantage of this method: the necessary differentiated data for sus-tainable optimization of compliance are not accessible through this method.
Through the installation of dispensers with integrated counters, the previous methods of recording compliance will be effectively enhanced, and a string of disadvantages circumvented. In par-ticular over the long-term, the measurement via counter can economically and without large efforts, improve the determina-tion of compliance. Conspicuous changes in both temporal and spatial usage of dispensers can be quickly registered and with consideration of the circumstances, further identified through narrowly localized direct observation. Through the interaction of both methods, implementation of hand hygiene in the daily practice of hospitals can be more effectively determined, as pos-sible weak spots are identified and adequate countermeasures applied. Hygiene management can in this way be sustainably op-timized from both a medical and a legal standpoint.
Hand hygiene as an effective weapon against the spread of path-ogens should not just be theoretically recognized, but its imple-mentation in practice should be persistently propelled forwards: This target can move an important step closer through the ap-plication of dispenser systems with counters.

12g g g g g H Y G I E N E A N D C O M P L I A N C E
Table 3: Advantages and disadvantages of methods for the deter-mination of hand-hygiene compliance
Method Advantages Disadvantages
Direct observation Immediate determination of compliance is possible
Qualitative evaluation is possible; whether compli-ance for the required indications is met
Observation sheet can be flexibly adapted to research interests
Possible observation ef-fects endanger the data validity
Possible interpretation and allocation errors of the observer endanger the data validity
Short observation intervals heighten the danger of coincidence effects
Due to the observation sheet design no inquiry for temporal and spatial distribution of usage possible
High temporal and per-sonnel cost
Measuring total consump-tion
Small required effort simplifies practical implementation
Inter-hospital comparison of aggregate situation of similar stations possible
No differentiated records of compliance possible
No identification of losses Endangers the data validity
Precise consumption measurements (Dispensers with counters)
Differentiated quantitative data for compliance (spatial + temporal distribution of consumption)
Small required effort simplifies practical imple-mentation
Problem-free long-term observation to discover conspicuous changes
Measurement data is independent of possible errors in interpretation or allocation through an observer
Adherence to indications, for implemented hand disinfection can only be determined in combina-tion with direct observa-tion

13g g g g g H Y G I E N E A N D C O M P L I A N C E
References
1 Deutsche Gesellschaft für Hygiene und Mikrobiologie
2 Gesetz zur Verhütung und Bekämpfung von Infektions- krankheiten beim Menschen (Infektionsschutzgesetz - IfSG), § 1
3 BGH, Urteil vom 20. 3. 2007, AZ: VI ZR 158/06
4 Empfehlung der Kommission für Krankenhaushygiene und Infektionsprävention beim Robert Koch-Institut zur „Hände- hygiene“ im Bundesgesundheitsblatt 2000, 43, Seiten 230-233
5 Nationales Referenzzentrum für Surveillance (NRZ): Zusammenfassender Auszug aus den vom NRZ am 7. Juli 2009 veröffentlichen Daten für den Zeitraum vom 1. Januar bis 31.Dezember 2008
6 Robert Koch-Institut: Epidemiologisches Bulletin Nr. 34/ 22. August 2008, S. 288
7 Nationales Referenzzentrum für Surveillance von nosokomialen Infektionen, Modul HAND-KISS, http://www.nrzhygiene.de/surveillance/hand.htm, eingesehen am 6. Oktober 2009
8 Evidence Report/Technology Assessment Number 43, Prepared for Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services, www.ahrq.gov, Making Health Care Safer: A Critical Analysis of Patient Safety Practices, S. 112,
9 Robert Koch-Institut: Epidemiologisches Bulletin Nr. 34/ 22. August 2008, S. 288
14g g g g g H Y G I E N E A N D C O M P L I A N C E
Publication Information
PublisherOphardt Hygiene-Technik GmbH + Co KGLindenau 27 47661 Issum
Medical Business [email protected]
Medical Business Unit Director - John O`Malley [email protected] Tel.: +353-71 91-89380
Director of Business Development & Regulatory Affairs – Thomas Fröhling [email protected] Tel.: +49 (0)2835-18-62Fax: +49 (0)2835-18-2951444
Senior Executive Corporate Accounts - Klaus Zscherpe [email protected].: +49 (0)2835-18-0Fax: +49 (0)2835-18-77
Text Markus Hochkirchen
ArrangementPeter Hartinger
© Ophardt Hygiene-Technik, Oktober 2009All rights reserved. No part of this publication may be reproduced without prior written permission of the publisher.
Related Documents











